As of July 2025, about 1.2 million people live in nursing facilities (referred to as nursing homes) and about one in five are in a nursing home in a rural area. This is similar to the share of the total U.S. population that lives in rural areas (20%) and slightly lower than the share of all adults 65 or older living in rural areas (24%). Nursing homes provide medical and personal care services for older adults and younger people with disabilities.Rural populations are older than urban populations and rural residents have a higher level of disability than their urban counterparts. The older demographic and higher rates of disability among rural populations contribute to a greater need for nursing homes and other long-term care services in rural communities.
Medicaid is the primary payer for nursing home care in the US. The 2025 reconciliation law, signed into law on July 4th, 2025, is projected to reduce federal Medicaid spending by $911 billion over ten years, according to the Congressional Budget Office, resulting in an estimated reduction of $137 billion in federal Medicaid spending in rural areas, according to KFF analysis. The law also includes $50 billion in funding for a new “rural health transformation program”, though these funds are unlikely to offset the Medicaid cuts to rural areas and few states have included proposals for nursing homes in rural areas in their applications. The reconciliation law also delayed implementation of a Biden-era rule intended to help address long-standing concerns about staffing shortages and the quality of care in nursing homes until 2034. A Texas judge overturned key requirements from the rule in April 2025; and the Trump Administration rescinded the rule in December 2025. Some of the changes to Medicaid financing could also have implications for nursing homes.
This analysis compares the characteristics of nursing homes in rural areas with those in urban areas. This brief uses data from Nursing Home Compare, a publicly available dataset that provides a snapshot of information on quality of care in each nursing home. This analysis categorizes nursing homes as remote rural, rural adjacent to metro areas (or “other rural”), and urban based on 2024 Urban Influence Codes from the USDA. See methods for more information on how rural categories were calculated. State-level data are also available on State Health Facts, KFF’s data repository with downloadable health indicators. Key takeaways from the analysis include:
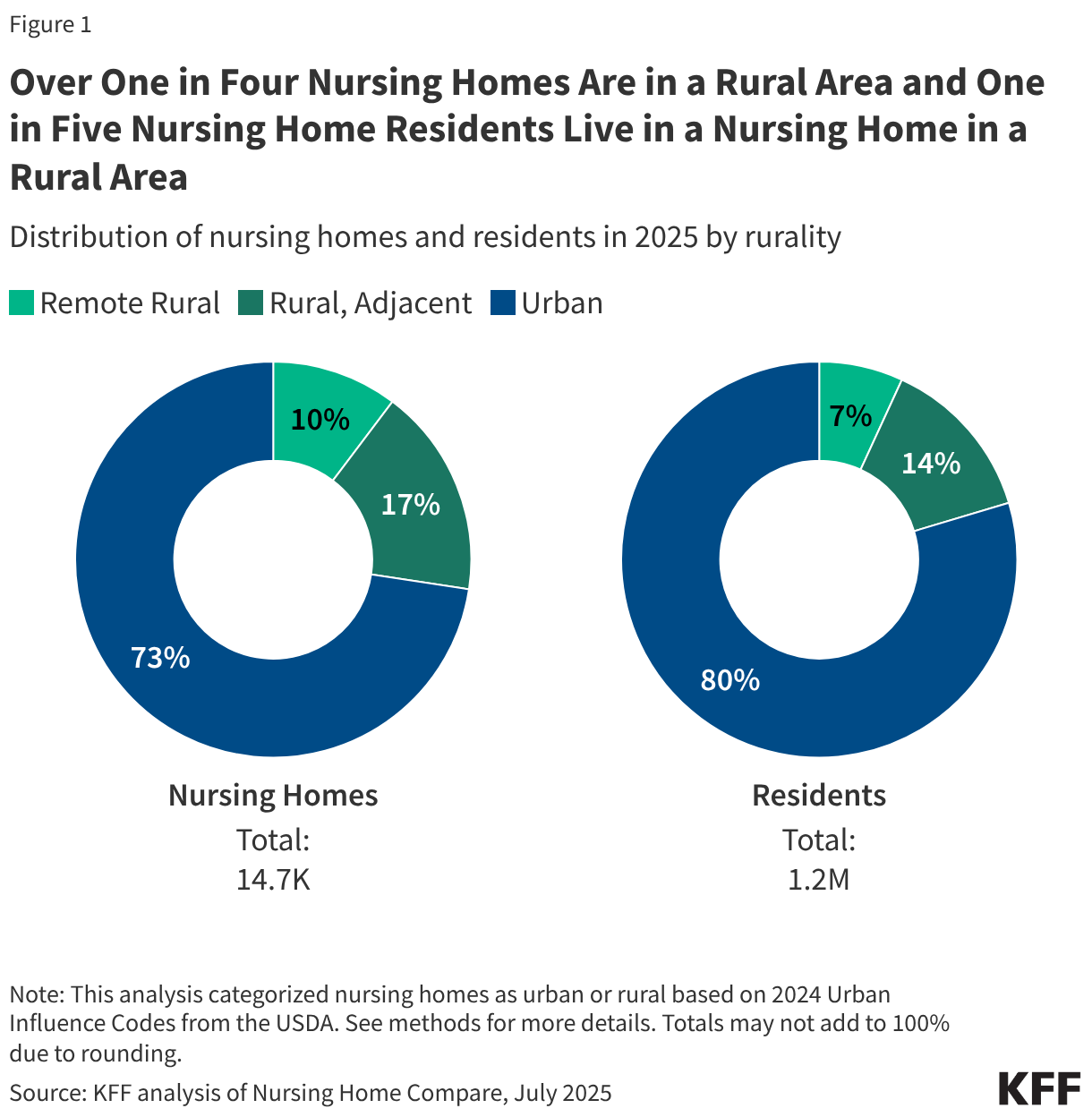
- Over one in four (27%) Medicaid and/or Medicare certified nursing facilities (referred to as nursing homes) are in a rural area and one in five (20%) residents live in a nursing home in a rural area (Figure 1). To be certified to serve Medicare or Medicaid patients, nursing homes are inspected regularly by state survey agencies in accordance with the Centers for Medicare & Medicaid Services (CMS) guidance.
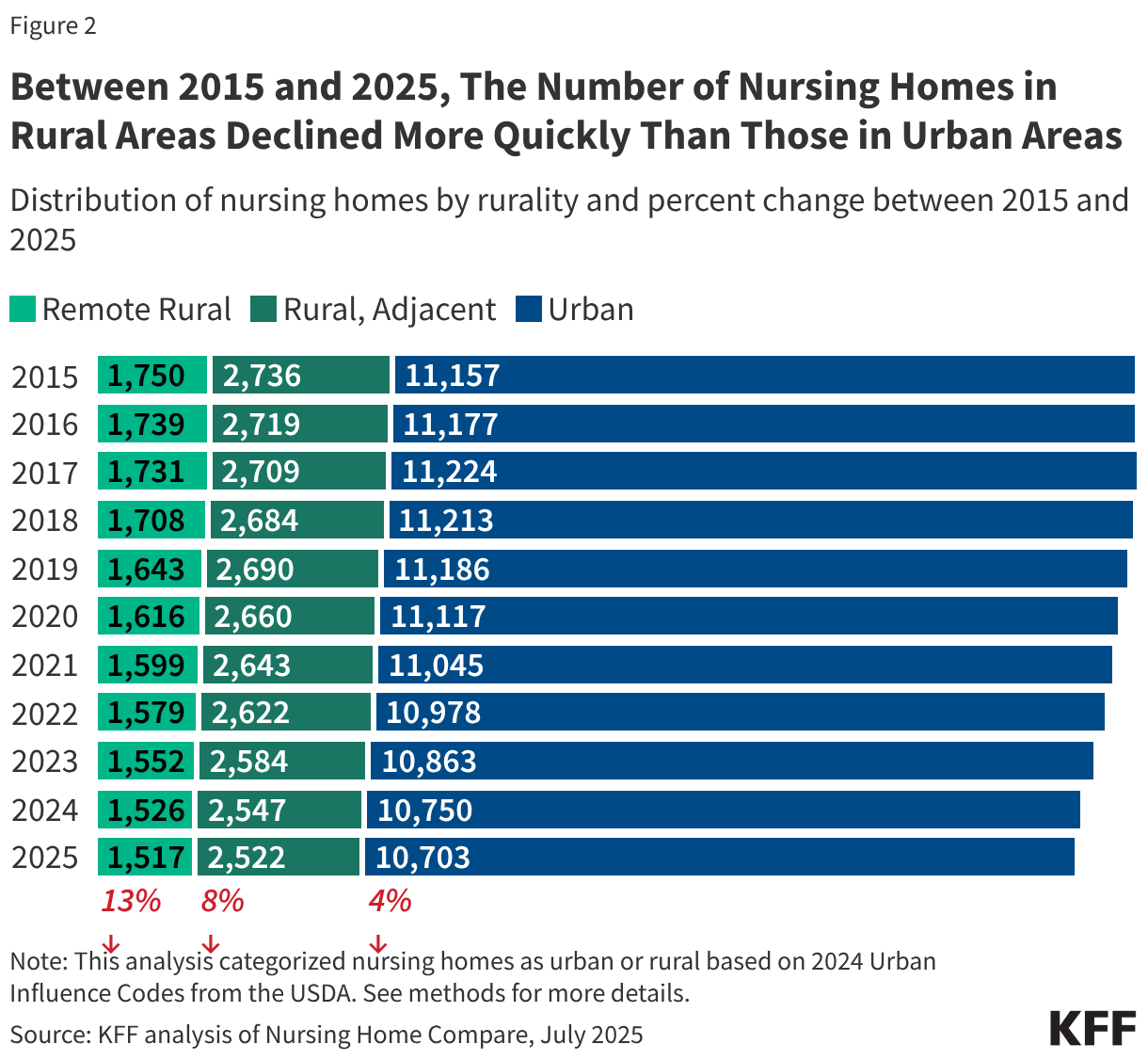
- Between 2015 and 2025, the number of nursing homes in rural areas decreased faster than nursing homes in urban areas (Figure 2).
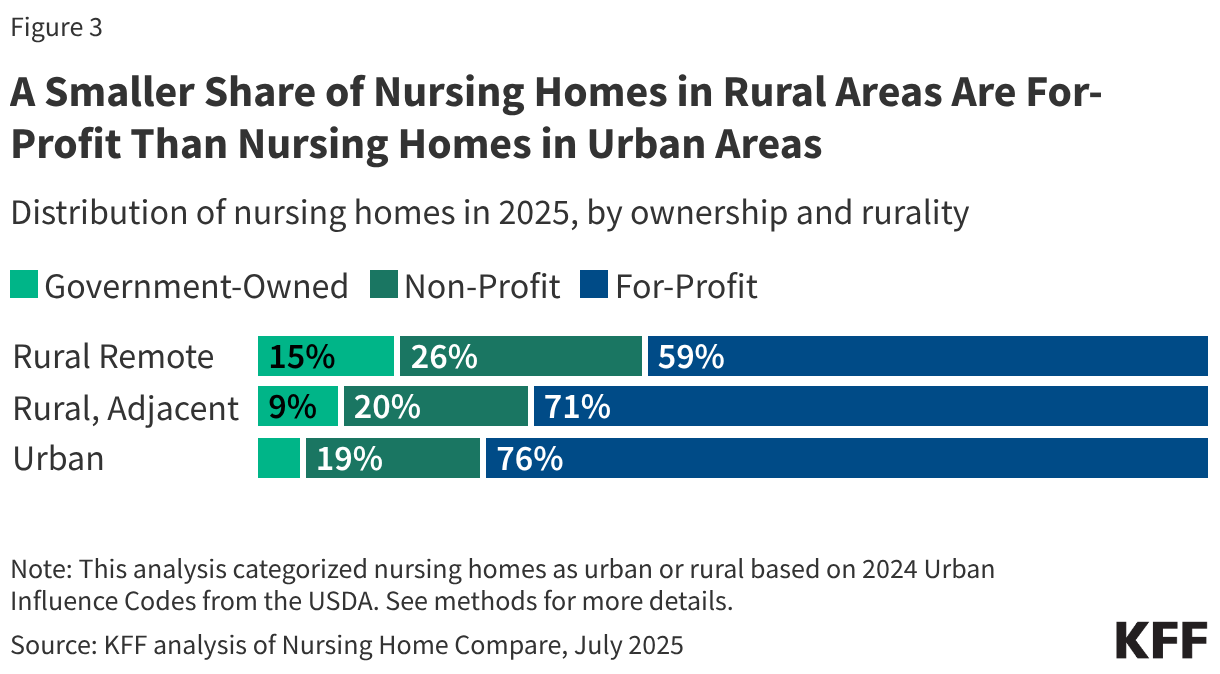
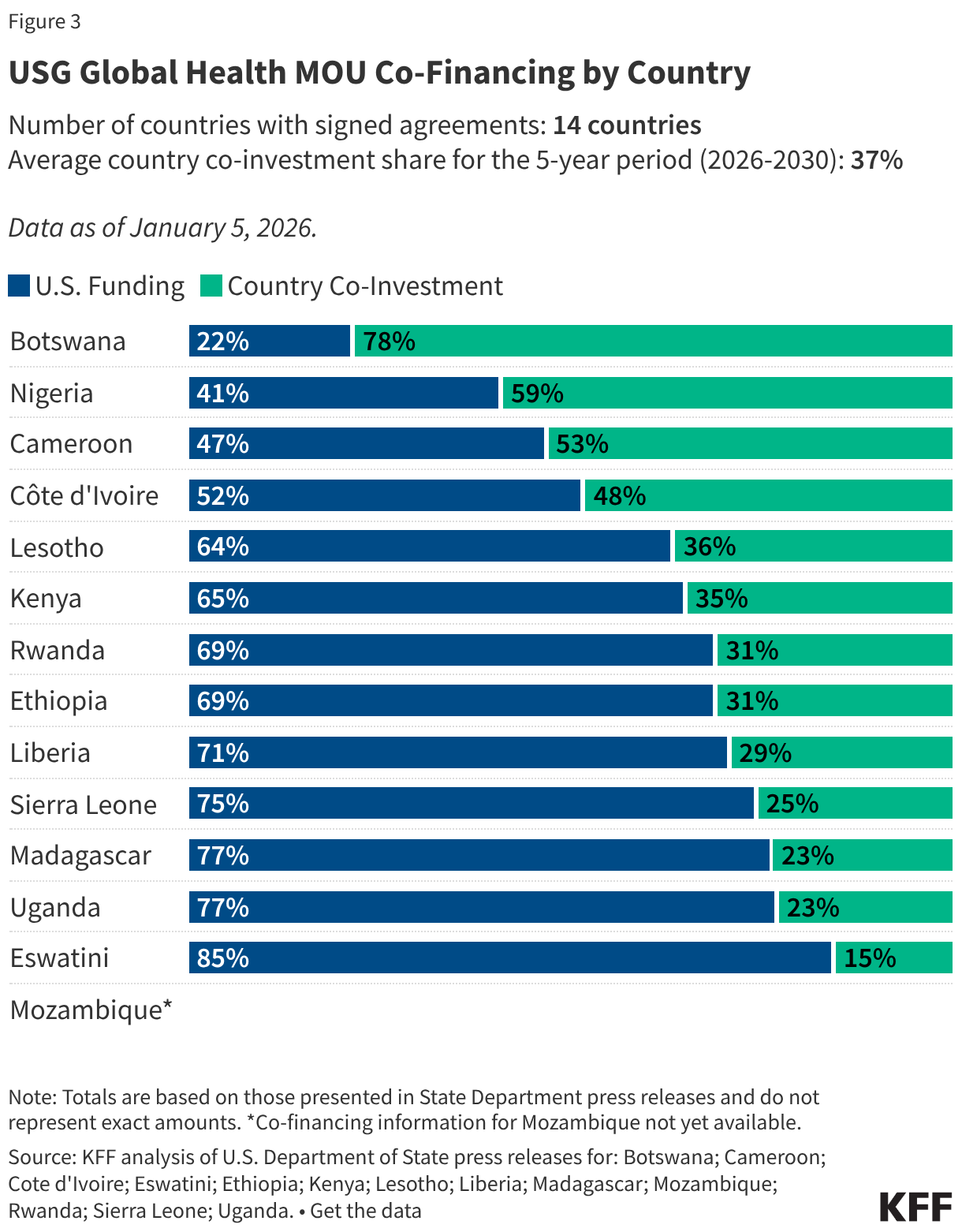
- A smaller share of nursing homes in rural areas are for-profit when compared to nursing homes in urban areas (Figure 3).
- Nursing homes in rural areas and nursing homes in urban areas have similar staffing levels and similar rates of deficiencies that cause actual harm or immediate jeopardy to residents.
Over one in four nursing homes are in a rural area and one in five residents live in a nursing home in a rural area (Figure 1). There are about 4,000 nursing homes in rural areas that are home to over 250,000 nursing home residents. These nursing homes account for about 27% of all nursing homes, with 10% in remote rural areas and 17% in rural areas adjacent to urban areas (or “other rural”). While over one-quarter of nursing homes are in rural areas, a smaller share of residents (20%) lives in these nursing homes because the average nursing home in a rural area is smaller than the average nursing home in an urban area (85 beds vs. 115 beds, data not shown). About 7% of nursing home residents live in nursing homes in remote rural areas and the other 14% live in nursing homes in other rural areas (totals do not add to 20% due to rounding). In eight states, at least half of nursing home residents live in nursing homes in rural areas (VT, WY, SD, MS, MT, IA, NE, and ND).
Between 2015 and 2025, the number of nursing homes in rural areas declined more quickly than those in urban areas (Figure 2). Between 2015 and 2025, the total number of nursing homes in the US dropped by 6%, from 15,643 to 14,742. Half of the decline occurred in rural areas (447 out of 901 nursing homes). The number of nursing homes in remote rural areas decreased the fastest (13% decline) when compared to nursing homes in other rural areas (8% decline) or urban areas (4% decline). These declines reflect the net number of nursing homes, which accounts for closures and openings.
During this time, the number of residents declined even more quickly. There was a 19% decline in nursing home residents living in remote rural areas; a 12% decline among those living in other rural areas; and an 8% decline among those living in urban areas. It is not clear what contributed to the decline in nursing homes and residents, but Medicaid as a whole has been providing home care to more people and spending on home care has increased more quickly than spending on institutional care.
A smaller share of nursing homes in rural areas are for-profit than nursing homes in urban areas (Figure 3). A smaller share of nursing homes in remote rural areas are for-profit (59%) than those in other rural areas (71%) or urban areas (76%). Additionally, a larger share of nursing homes in remote rural areas are non-profit (26%) than those in other rural areas (20%) or urban areas (19%). Similarly, a larger share of nursing homes in remote rural areas are government-owned (15%) than those in other rural areas (9%) or urban areas (5%).
In many other ways, nursing homes in rural areas are similar to nursing homes in urban areas.
- Nursing homes in rural areas and nursing homes in urban areas have relatively similar payer distributions. Nursing homes in rural areas report that 66% of residents have Medicaid as their primary payer and nursing homes in urban areas report that 63% of residents have Medicaid as their primary payer. Similarly, 10% of residents in nursing homes in rural areas have Medicare as their primary payer and 15% of those living in nursing homes in urban areas have Medicare as their primary payer. (Medicare does not generally cover long-term care services but does cover up to 100 days of skilled nursing facility care following a qualifying hospital stay.) Nursing homes in rural areas report that 24% of their residents have another primary payer (such as private insurance or out-of-pocket) and nursing homes in urban areas report that 23% of residents have another primary payer.
- Similarly, nursing homes in rural areas and nursing homes in urban areas report similar shares of nursing homes with deficiencies that cause actual harm or immediate jeopardy to residents (27% vs. 29%).
- Staffing levels in nursing homes in rural areas and nursing homes in urban areas are similar as well: 58% of nursing homes in rural areas and 64% of nursing homes in urban areas report an average of at least 3.5 total nursing hours per resident per day. This is consistent with prior research that found that similar shares of nursing homes in rural areas (20%) and nursing homes in urban areas (18%) would have met the requirements in the now-rescinded Biden-era staffing rule intended to help address long-standing concerns about staffing shortages and the quality of care in nursing homes.
Methods
Nursing Home Compare: Nursing Home Compare is a publicly available dataset that provides a snapshot of information on quality of care and key characteristics for approximately 14,900 Medicare and/or Medicaid-certified nursing homes.The data in this analysis is from July 2025.
Defining Rurality in Nursing Home Compare: Nursing homes in urban areas are defined as those in a metropolitan area, while nursing homes in rural areas are defined as those in nonmetropolitan areas. A metropolitan area is a county or group of counties that contains at least one urban area with a population of 50,000 or more people. Nonmetropolitan areas include micropolitan areas—which are counties or groups of counties that contain at least one urban area with a population of at least 10,000 but less than 50,000—and noncore areas (areas that are neither metropolitan nor micropolitan). This brief also breaks rural areas into those that are adjacent to metropolitan areas (defined as “other rural” in this brief) and those that are not adjacent to metropolitan counties (defined as “remote rural” areas in this brief).
This analysis categorized counties and county equivalents based on 2024 Urban Influence Codes from the USDA, as follows:
Urban
- 1: Large metro (in a metro area with at least 1 million residents)
- 4: Small metro (in a metro area with fewer than 1 million residents)
Rural, adjacent to a metro area (“other rural”)
- 2: Micropolitan, adjacent to a large metro area
- 3: Noncore, adjacent to a large metro area
- 5: Micropolitan, adjacent to a small metro area
- 6: Noncore, adjacent to a small metro area
Rural, not adjacent to a metro area (“rural remote”)
- 7: Micropolitan, not adjacent to a metro area
- 8: Noncore, not adjacent to a metro area and contains a town of at least 5,000 residents
- 9: Noncore, not adjacent to a metro area and does not contain a town of at least 5,000 residents
Deficiencies in Nursing Homes: Health care deficiencies in nursing homes are evaluated on two elements:
- The scope of the deficiency (such as whether the deficiency was isolated to one person or was widespread across the nursing home)
- The severity of the deficiency (such as whether an individual suffered actual harm or immediate jeopardy)
Deficiencies are assigned a Scope/Severity score ranging from letters A through L, with each letter corresponding to a unique combination of scope and severity. This analysis looks at only at deficiencies that cause actual harm or immediate jeopardy, which corresponds with values G through L. The Centers for Medicare and Medicaid Services defines "actual harm" as a "deficiency that results in a negative outcome that has negatively affected the resident's ability to achieve the individual's highest functional status. "Immediate jeopardy" is defined as a deficiency that "has caused (or is likely to cause) serious injury, harm, impairment, or death to a resident receiving care in the nursing home." CMS’ definition of “serious” deficiencies varies slightly from the definition in this analysis. CMS excludes deficiencies with score “G” and includes deficiencies with score “F” for certain deficiencies that represent a “substandard quality of care.”
This work was supported in part by The John A. Hartford Foundation. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.