KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
The KFF Health Misinformation Tracking Poll Pilot examines U.S. adults’ use of and trust in different media sources and their exposure to and belief in a series of health-related misinformation claims, including false statements related to COVID-19 and vaccines, reproductive health, and firearm safety. The Health Misinformation Tracking Poll will work in tandem with KFF’s forthcoming Health Misinformation Monitor, a detailed report of the landscape of health misinformation messages circulating among the public, probing the impact of misinformation documented in the monitor to help inform and strengthen efforts aimed at addressing misinformation in health. Both the Misinformation Tracking Poll and the Monitor are part of a new program on health misinformation and trust being developed at KFF. This snapshot from our initial pilot poll provides a look at the survey results among Black adults1 and their implications for addressing health-related misinformation among this community. Other snapshot reports provide similar insights into addressing misinformation among Hispanic adults and among rural residents. These snapshot reports are aimed at helping organizations in the U.S. working to combat health-related misinformation and rebuild trust in the media, public health, and scientific communities.
Key Takeaways for the Field
When it comes to health misinformation, few Black adults are convinced that widely circulated falsehoods are true, while much larger shares are doubtful or uncertain, providing an opportunity for intervention. When presented with specific items of health misinformation, few Black adults (between 4% and 15%) say they believe them to be “definitely true.” Modest shares (between 14% and 36%) recognize each of these claims to be “definitely false.” Similar to adults overall, when it comes to their tendency to believe false health-related statements, most Black adults fall somewhere in the middle of the spectrum, with large shares saying each claim is “probably true” or “probably false.” While most Black adults do not ardently believe the health misinformation examined in the survey, the exposure to these false and inaccurate claims may contribute to uncertainty and doubt when it comes to individual health care behaviors and choices. This more uncertain middle group may offer an opportunity for focused outreach and interventions.
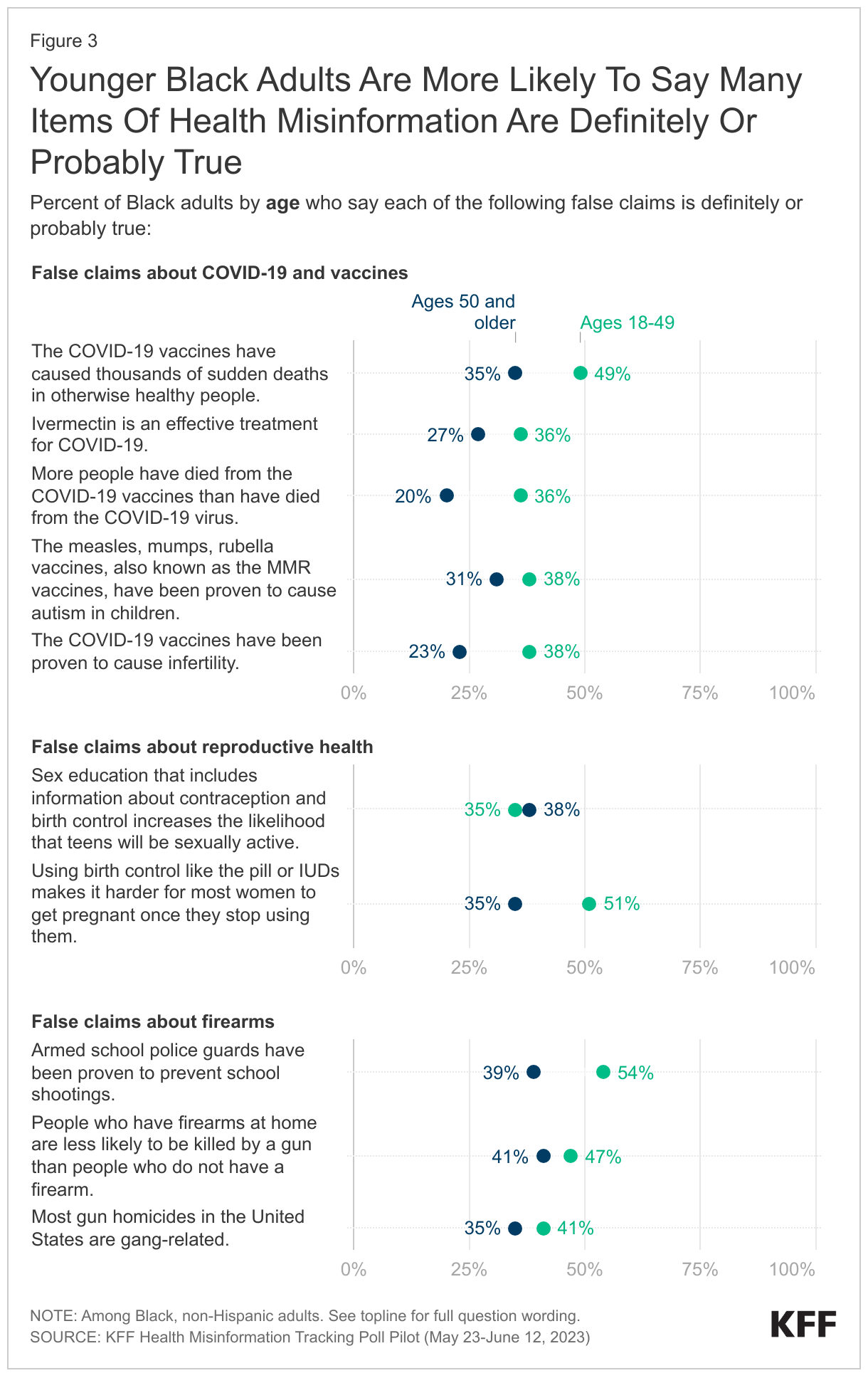
Among Black adults, some groups – including younger adults and those without a college degree – are more inclined to believe certain types of health misinformation than others, suggesting it may be helpful to target interventions to these groups. Black adults under age 50 are much more likely to say items of misinformation related to COVID-19 and vaccines are definitely or probably true compared to their older counterparts. As with adults overall, there are also large differences among Black adults in their propensity to believe health misinformation claims across educational attainment, with those without a college degree generally being more likely to say that the health misinformation items examined in the survey are definitely or probably true. This suggests that interventions aimed at preventing misinformation from taking hold may need to take a person’s broader experiences, education, and knowledge base into account.
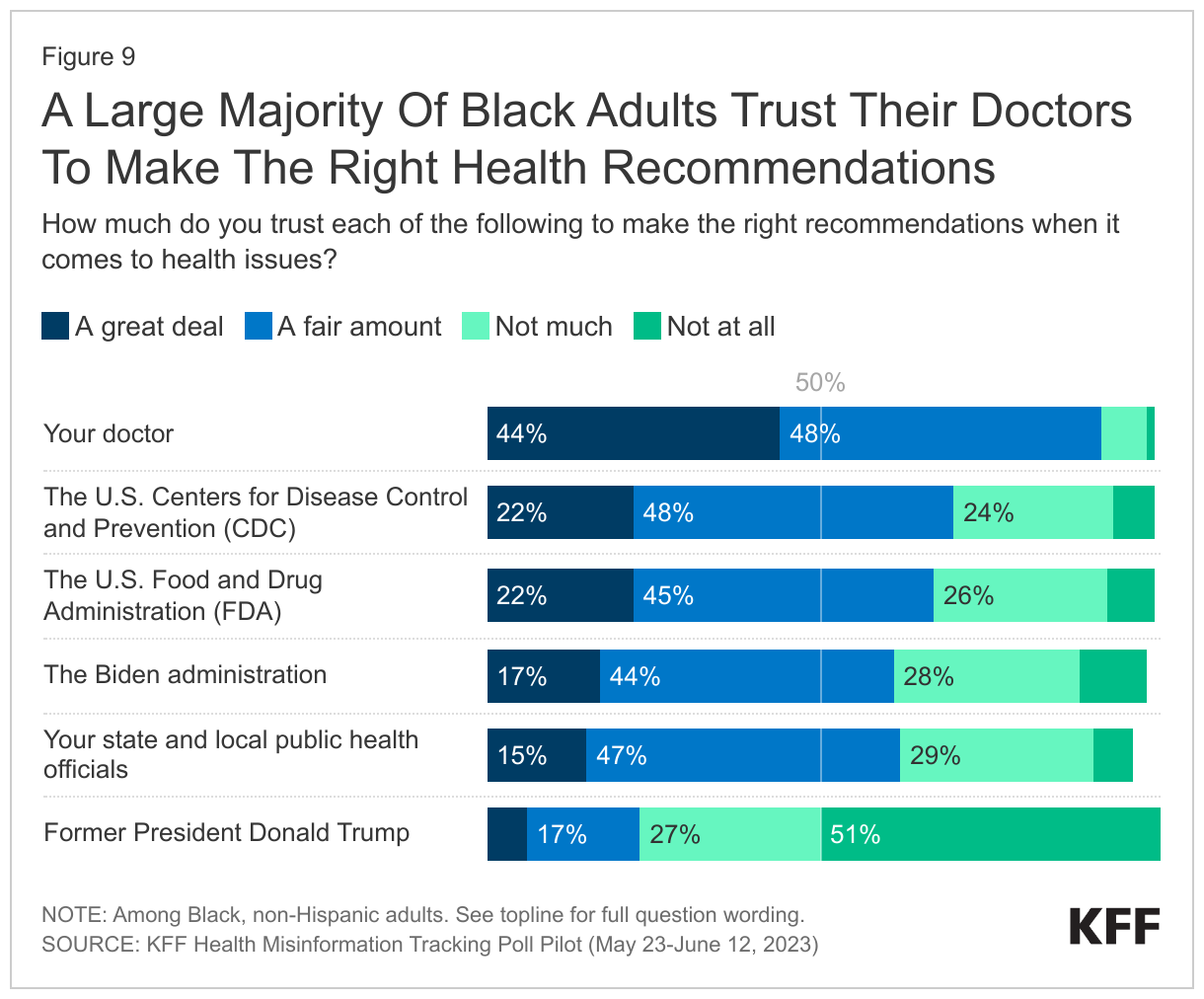
Personal connections maintain an outsized importance when it comes to trusted information. Black adults say that their doctors are their most trusted sources of health information. Notably, a majority of Black adults also trust the CDC, FDA, their state and local public health officials, and the Biden administration to make the right recommendations when it comes to health issues, showing potential for these official government agencies to be effective messengers to Black individuals and communities.
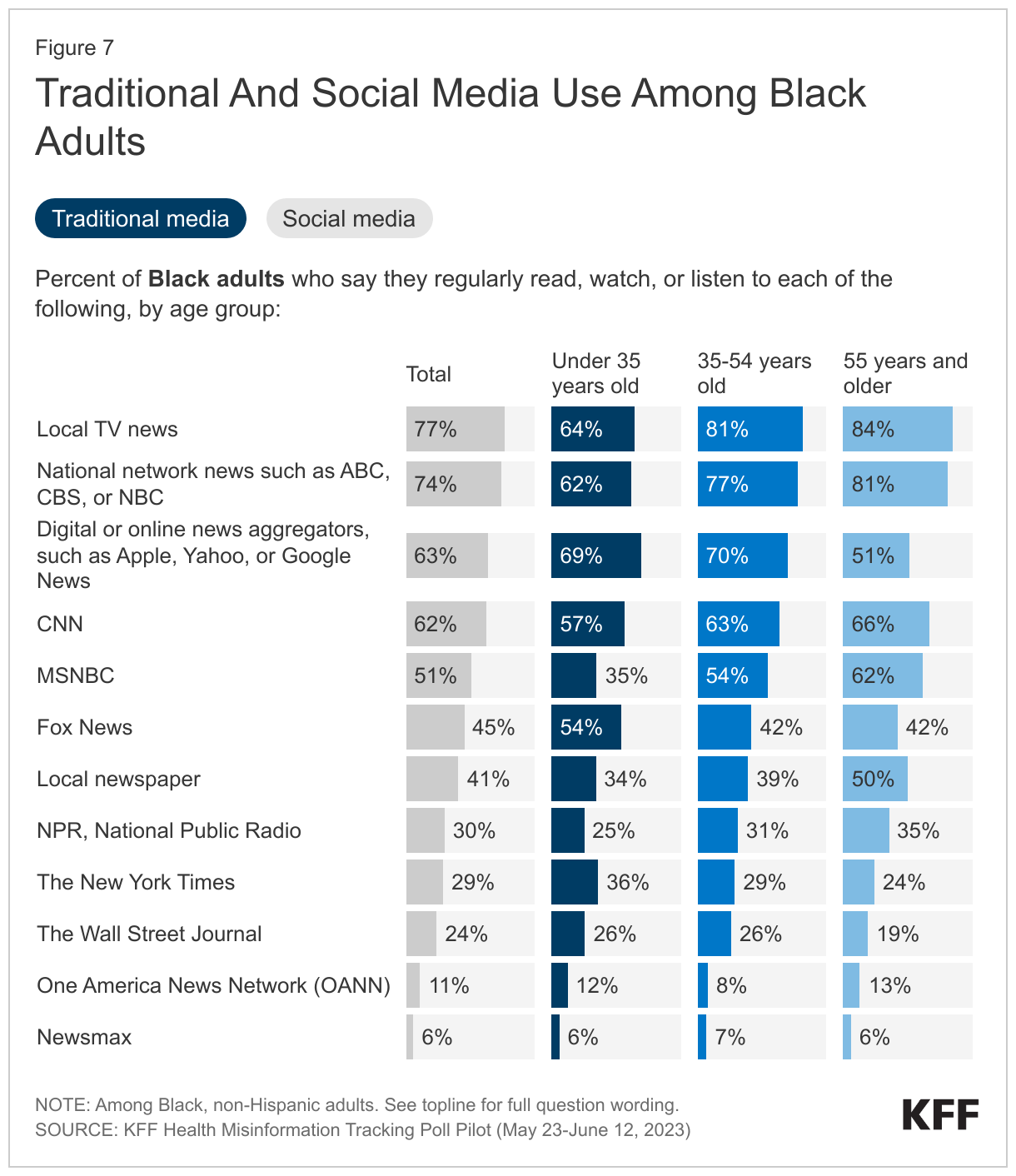
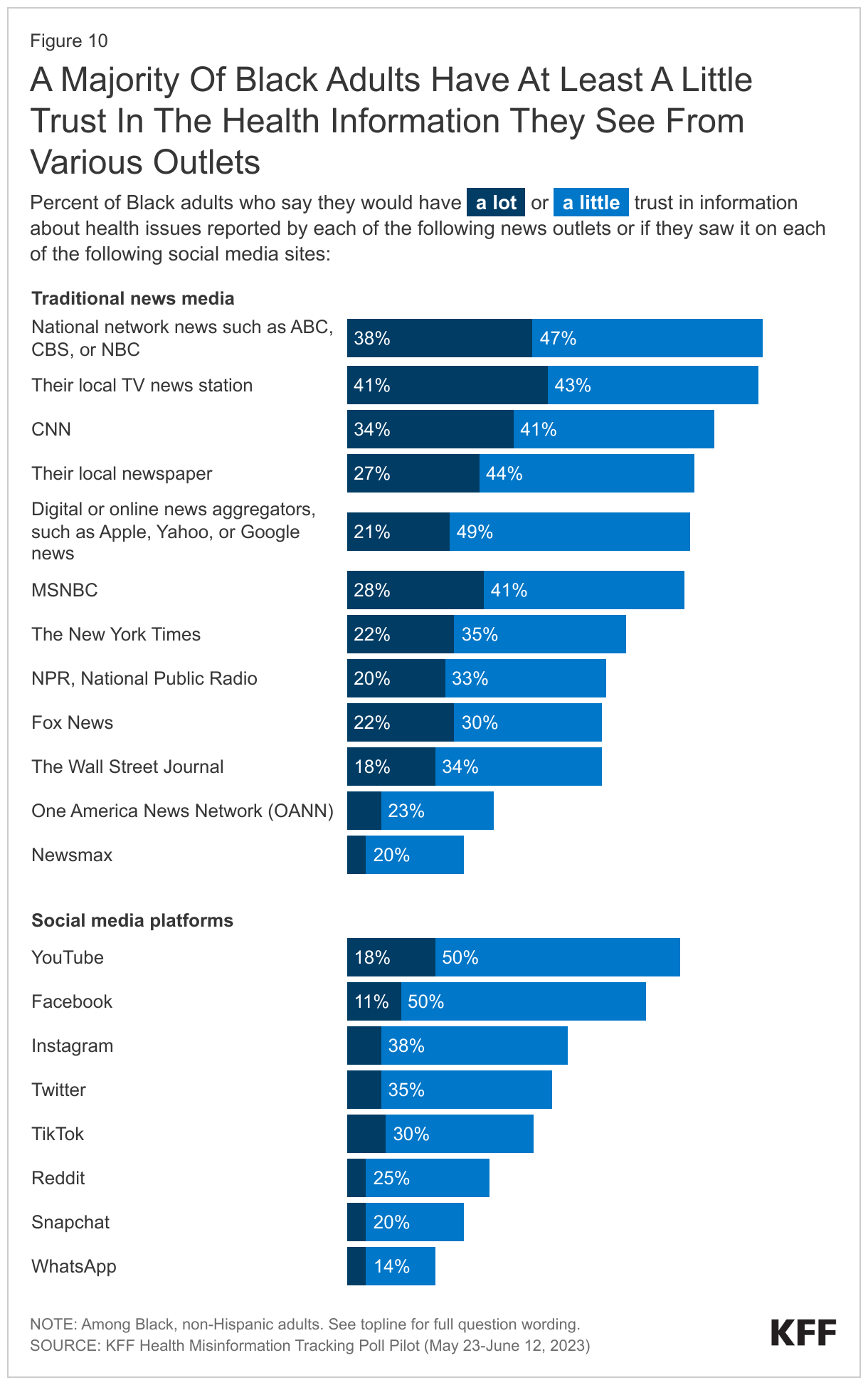
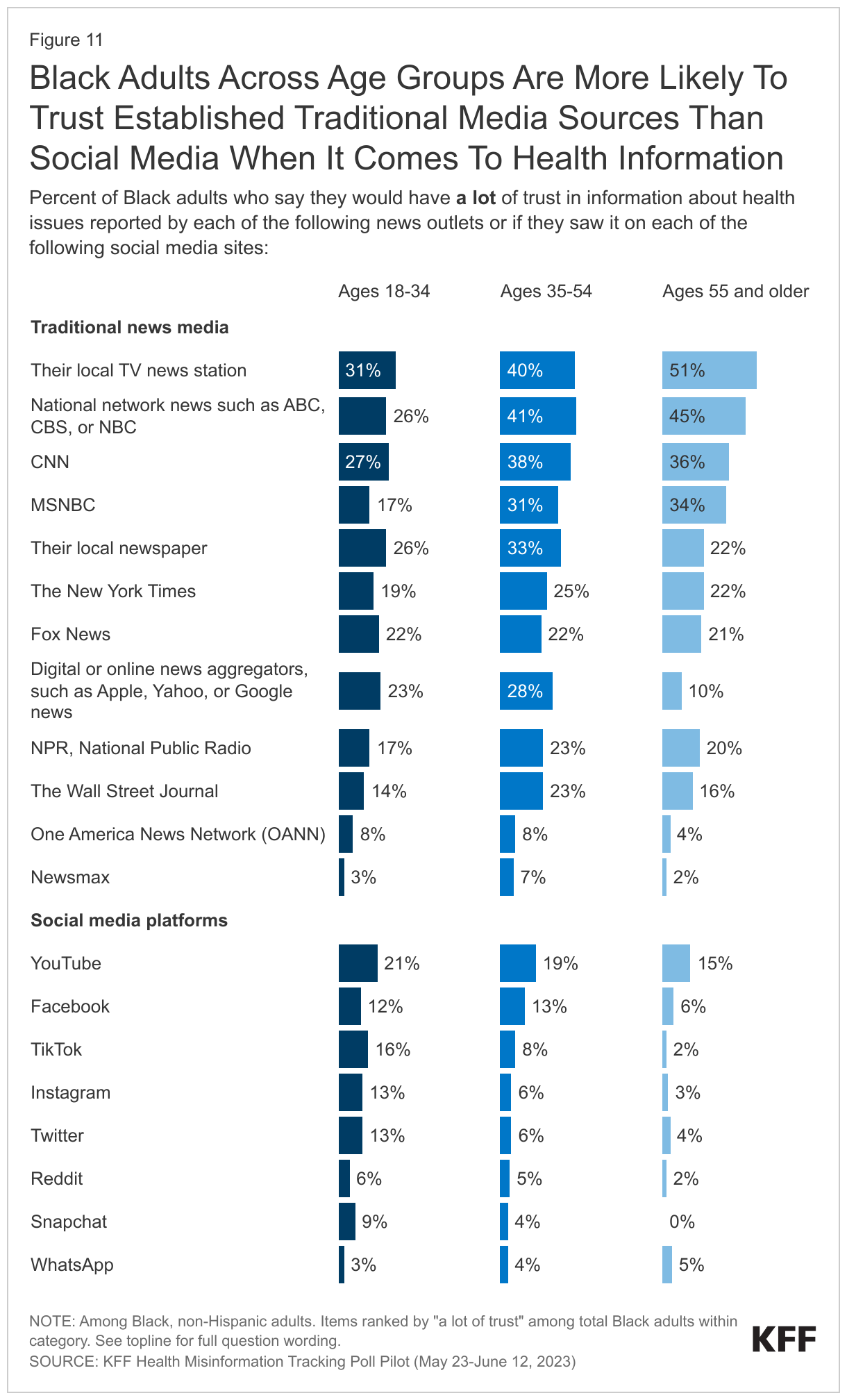
Local TV news and national network news are promising ways to reach Black audiences with accurate information. Large shares of Black adults across age groups say they watch these sources regularly and would trust health information they report, ranking relatively high compared to other news sources. Online digital news aggregators, CNN, and MSNBC are also regular news sources for at least half of Black adults, though fewer say they have a lot of trust in health information reported by these sources.
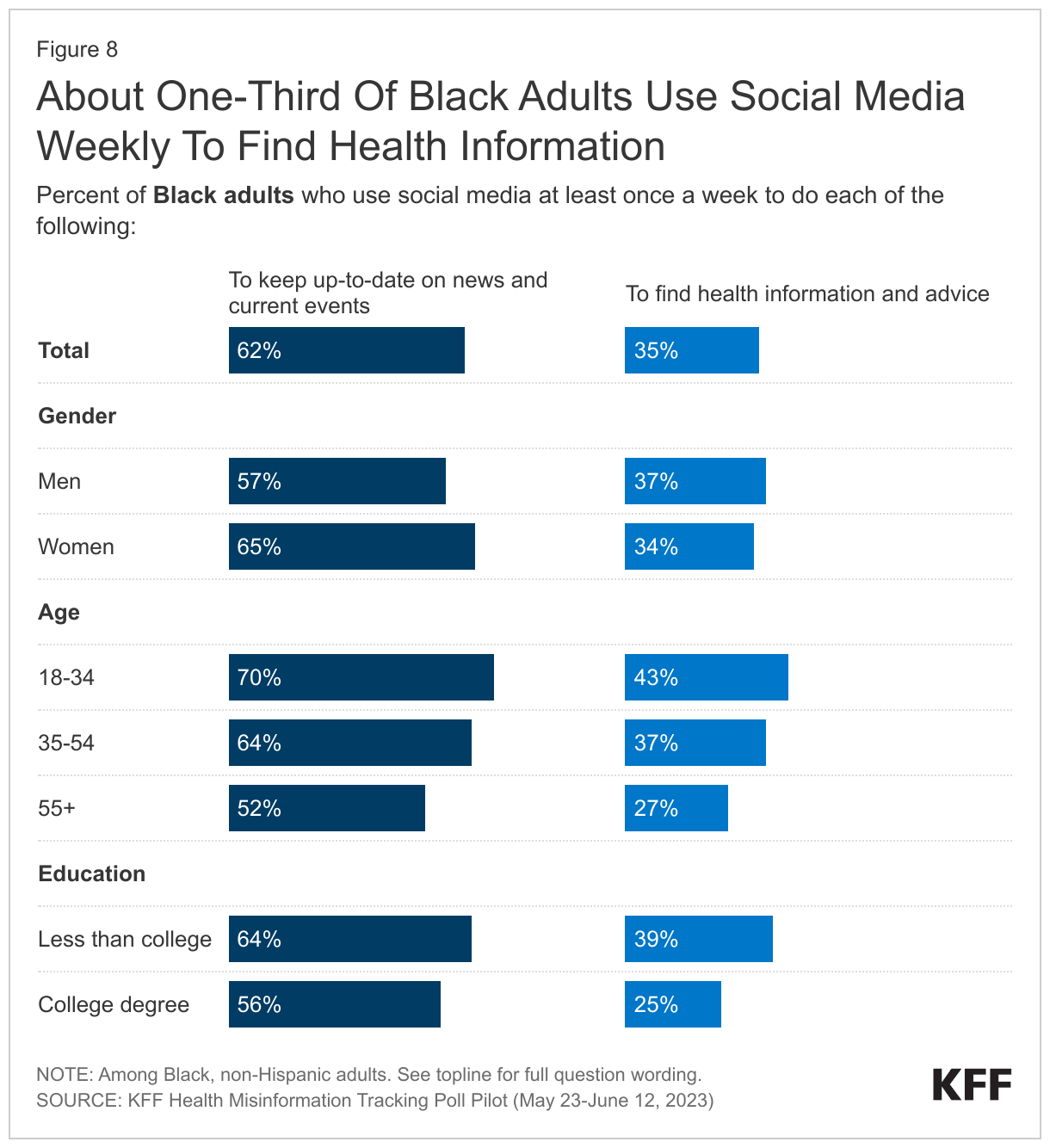
Many Black adults report regularly using social media platforms for news and current events, though fewer say they actively seek out health information on social media and few express a lot of trust in health information seen on social media. Among these platforms, Facebook and YouTube are the most widely used and have the reported highest relative levels of trust.
Social media may be the best way to reach younger Black adults, but don’t count traditional media out. Black adults under age 35 are more likely to use social media, with majorities saying they use YouTube, Instagram, Facebook, and TikTok at least once a week, and four in ten saying they use social media at least weekly to find health information and advice, higher than for other age groups. However, majorities in this age range also say they regularly rely on local TV news and network news for information. Legacy in traditional news media remains, as younger adults report being more trusting of the information they see about health issues reported by some sources of news media rather than social media platforms.
Exposure to and Belief in Health Misinformation
While notable shares of Black adults are coming across health-related misinformation, relatively few are buying into specific false claims about COVID-19, reproductive health, and firearm violence and safety examined in the KFF Misinformation Tracking Poll Pilot. Similar to adults overall, only small shares of Black adults (15% or less) are convinced that specific items of misinformation asked about in the poll are “definitely true.” Somewhat larger shares (between 14% and 36%) reject these misinformation items as “definitely false,” yet most Black adults are in a middle group that express some uncertainty saying these false claims or “probably true” or “probably false.”
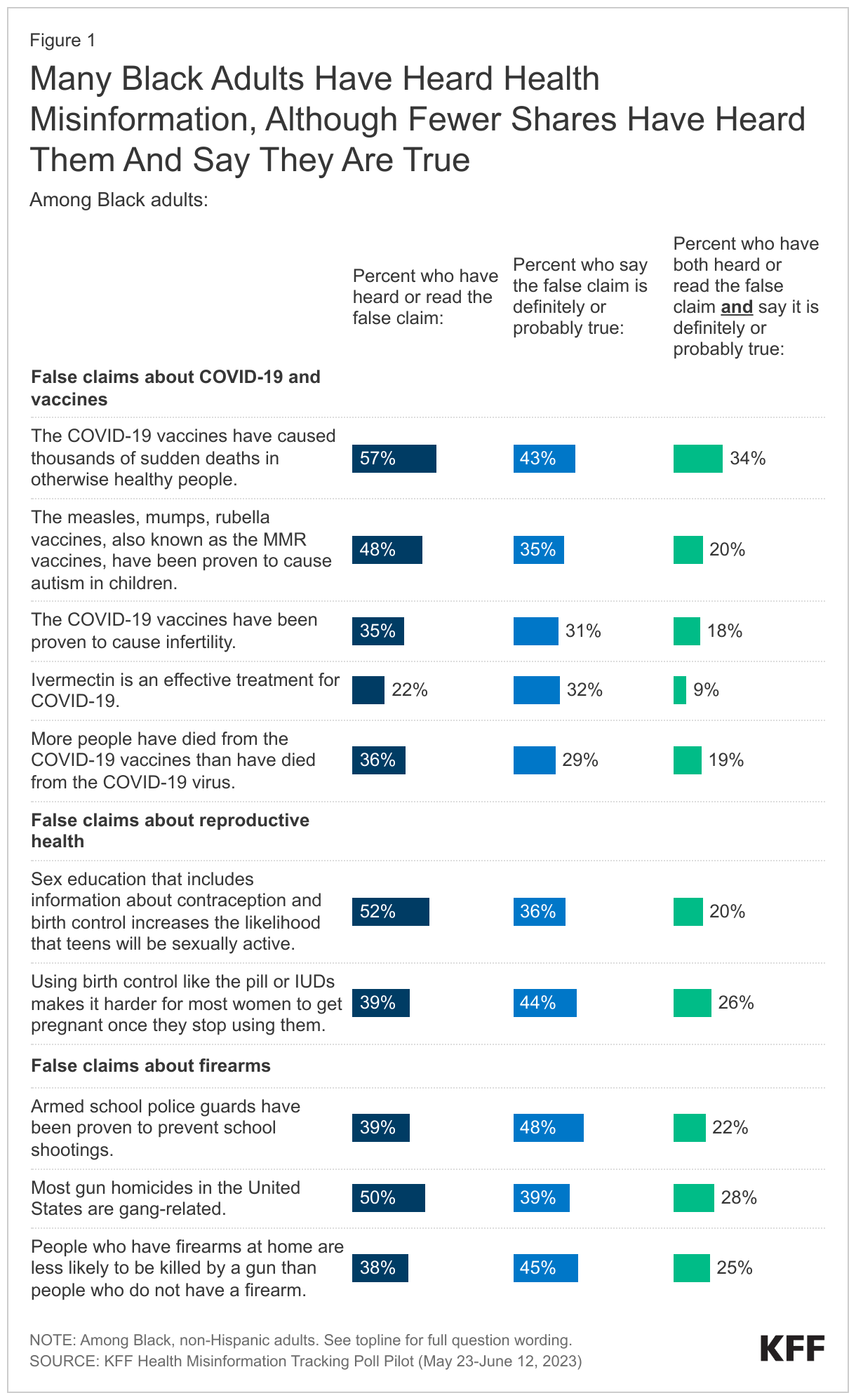
Between one in five and three in five Black adults have heard each of the pieces of health misinformation included in the survey. The most commonly heard items are that “COVID-19 vaccines have caused thousands of sudden deaths in otherwise healthy people,” “Sex education that includes information about contraception and birth control increases the likelihood that teens will be sexually active,” and “Most gun homicides in the U.S. are gang related.” Exposure to specific claims of health misinformation varies by age, gender, and education, with young Black adults and college educated Black adults being more likely to have heard pieces of COVID-19 misinformation.
Regardless of whether they have heard or read specific items of misinformation, the survey also asked people whether they think each claim is definitely true, probably true, probably false, or definitely false. For most of the misinformation items included in the survey, between three in ten and half of Black adults say they are “definitely” or “probably true.” Combining these measures, smaller shares of Black adults (between one in ten and one-third) both have heard each claim and believe it is probably or definitely true.
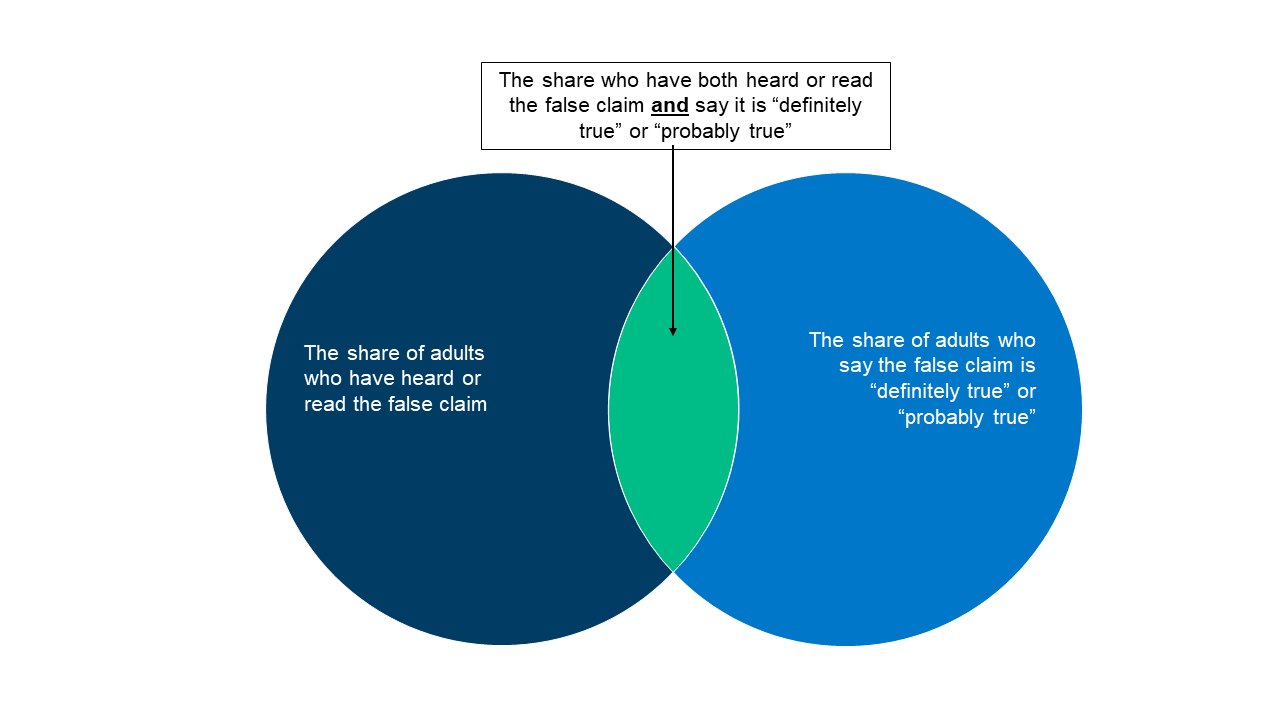
Measures of Health Misinformation
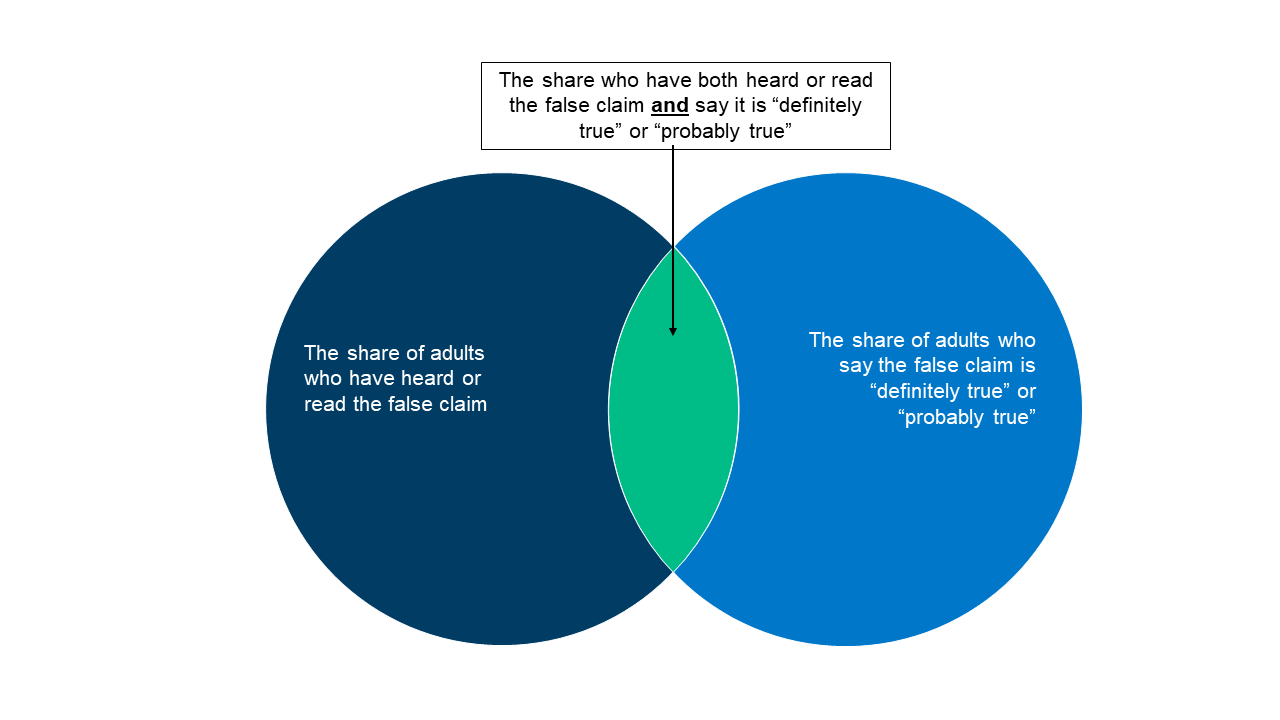
This report examines three measures of health misinformation among the public. Adults were asked whether they had heard or read specific, false health-related statements. Regardless of whether they have heard or read specific items of misinformation, all were asked whether they thought each claim was definitely true, probably true, probably false, or definitely false. We then combined these two measures to examine the share who have heard the false claims and believe it is definitely or probably true.
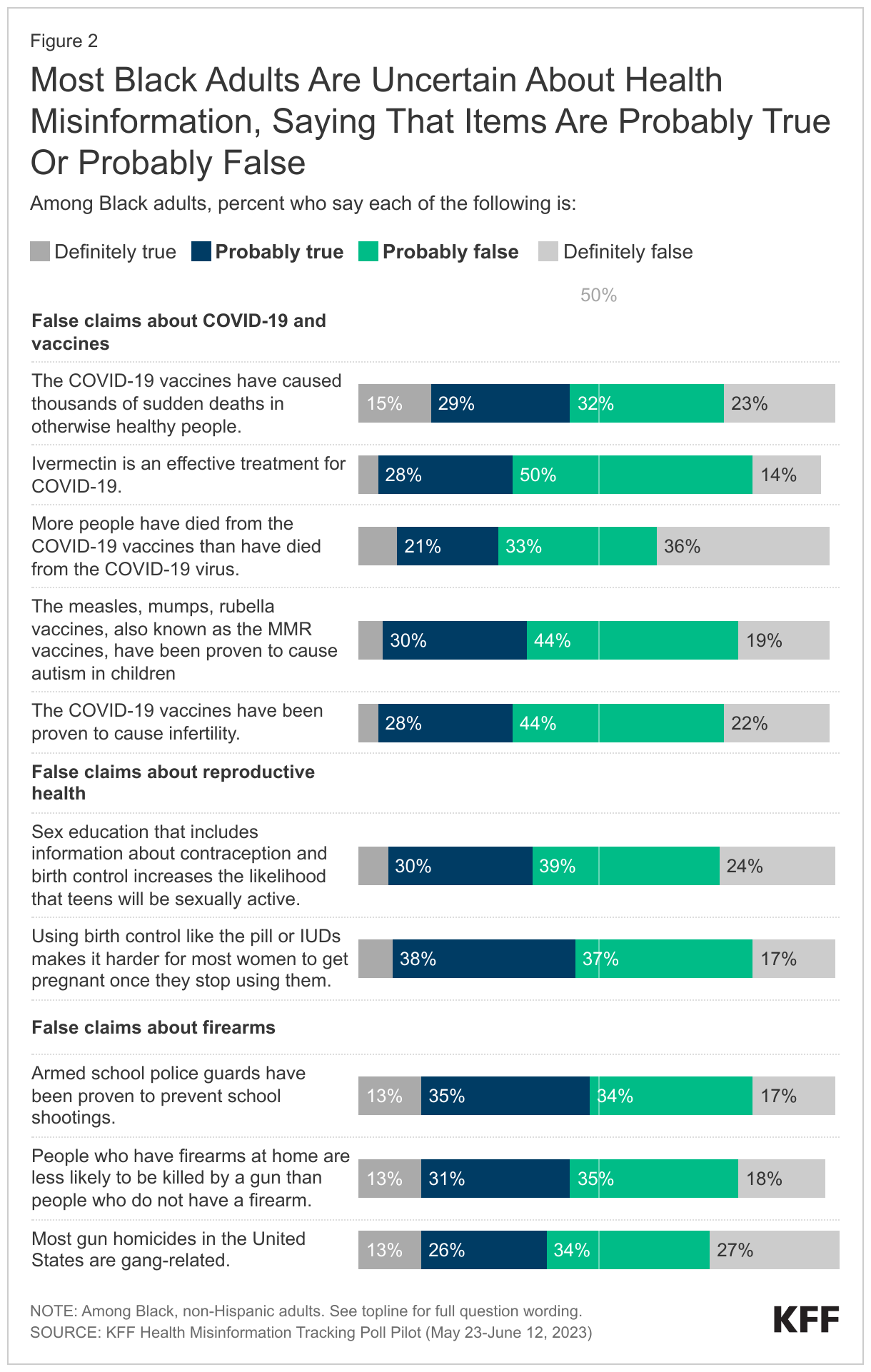
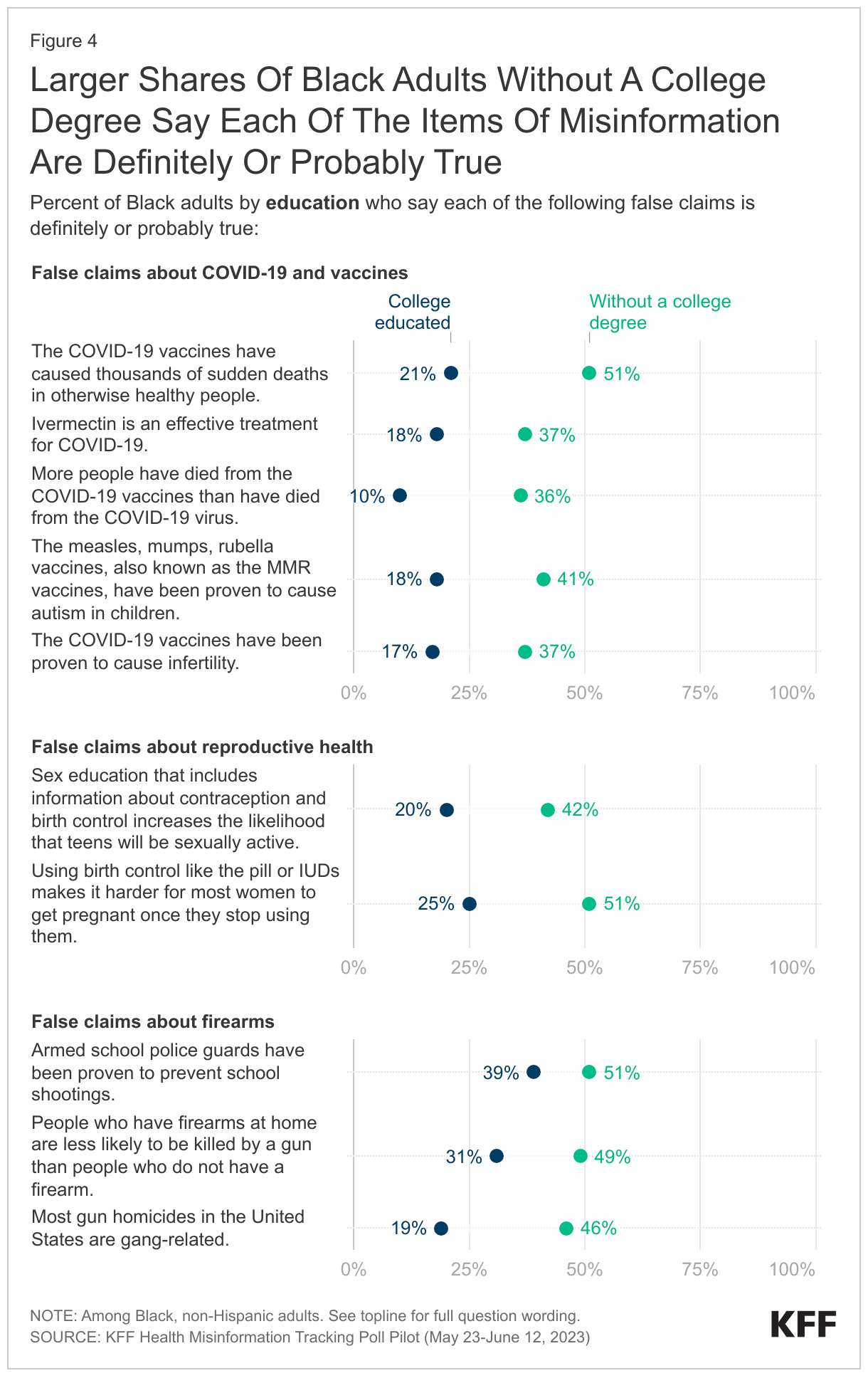
Large shares of Black adults express uncertainty about the truthfulness of the false claims tested in the survey, with majorities saying each is either “probably true” or “probably false.” Small shares – about one-third or fewer – recognize any of the claims as “definitely false,” and fewer than one in five say that any of these claims are “definitely true.” Black adults without a college degree are particularly likely to express uncertainty about many of these claims.
The figures below show the shares of Black adults by age group and education level who believe each of the false claims is definitely or probably true. Generally, younger Black adults and those without a college degree are more likely than their older and college educated counterparts to say each of the items of misinformation examined in the survey are definitely or probably true.
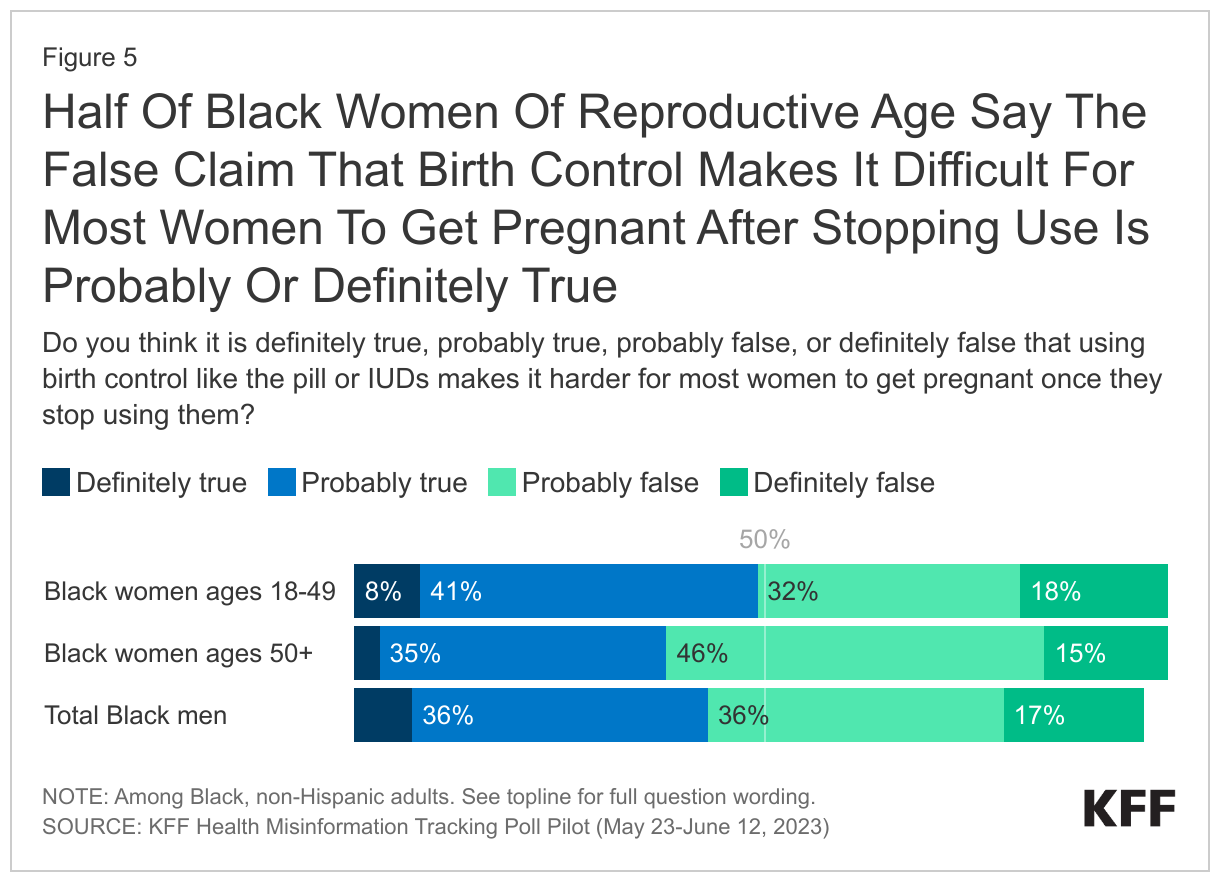
Notably, about half of Black women of reproductive age (ages 18-49) say it is probably or definitely true that using hormonal birth control makes it harder for most women to get pregnant after ceasing birth control use. Older Black women lean more towards saying the statement is false, though just 15% of Black women ages 50 and older say the statement is “definitely false,” and nearly half (46%) say it is “probably false.”
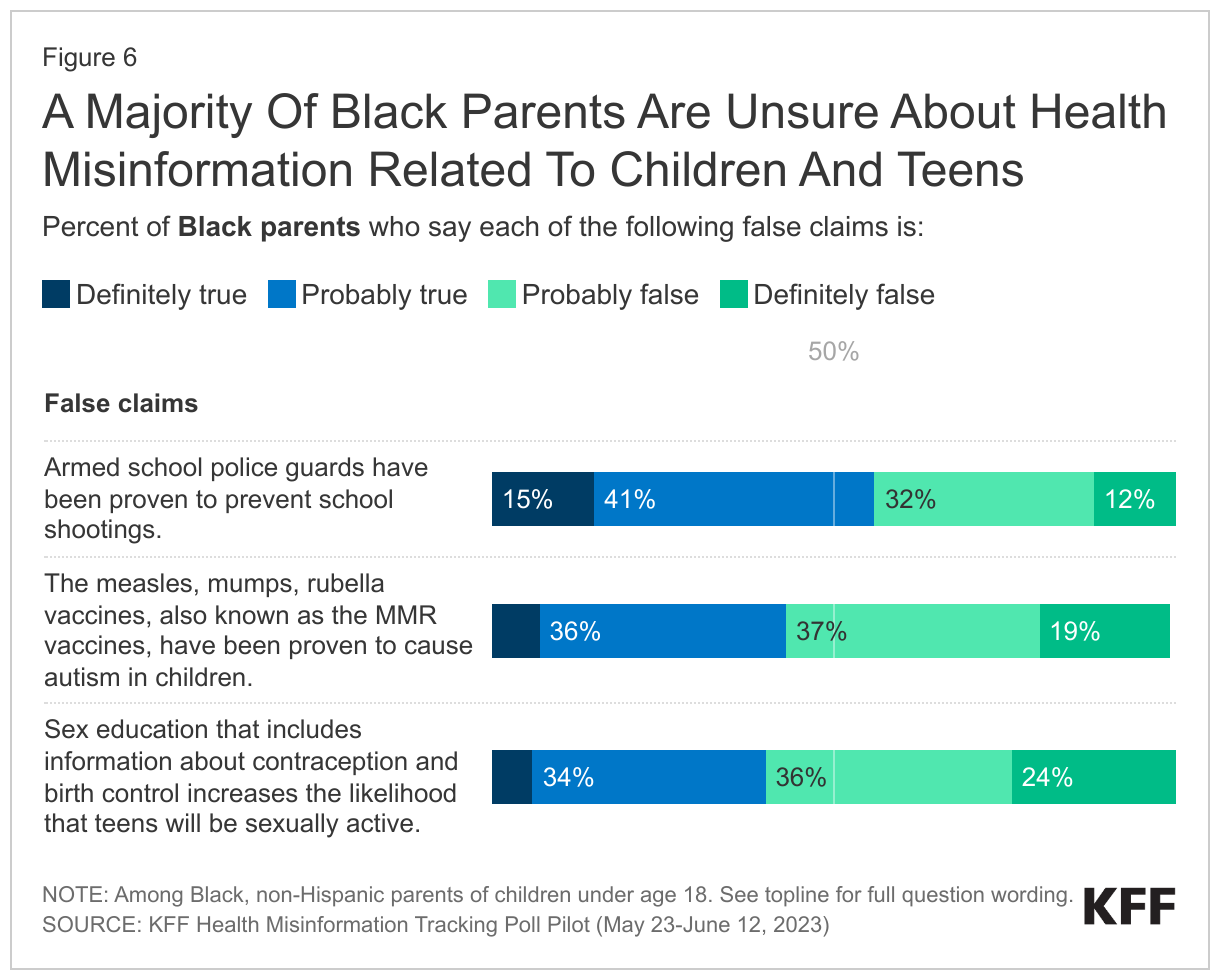
Most Black parents are unsure about some of the misinformation items examined in the survey related to children, teens, and schools, with majorities saying it is “probably true” or “probably false” that armed school guards have been proven to prevent school shootings, that the MMR vaccines cause autism in children, and that sex education that includes information about contraception increases the likelihood that teens will be sexually active. One in four Black parents say the final claim is “definitely false.”
Media Consumption and Trust
Consumption of News, Social Media, and Health Information
Television is the most commonly reported medium for news consumption among Black adults ages 35 and over, with large majorities saying they regularly watch local news and national network news, and more than half saying they are regular viewers of CNN and MSNBC. Among younger Black adults, seven in ten say they regularly use digital news aggregators that draw on multiple news sources, and more than half report regularly watching various TV news sources.
Social media use, not surprisingly, varies by age among Black adults as well. A majority of Black adults across age groups report using Facebook and YouTube at least once per week, but larger shares of Black adults under age 35 say they regularly use Instagram (79%), TikTok (62%), Snapchat (49%) and Twitter (41%) compared to their older counterparts.
Regardless of preferred social media platform, many (62%) Black adults say they use social media at least once a week to keep up-to-date on news and current events. This rises to seven in ten Black adults under age 35. One-third of Black adults also say they use social media at least weekly to find health information and advice. Younger Black adults and those without a college degree are more likely than their counterparts to use social media for health advice and information.
Trust in Sources of Information
Doctors with personal relationships are the most trusted sources of health information for Black adults, with the vast majority saying they trust their doctor a great deal or a fair amount to make the right recommendations when it comes to health issues. Notably, a majority of Black adults have at least “a fair amount” of trust in the CDC, FDA, Biden administration, and state and local public health officials to make the right health recommendations. Fewer Black adults (22%) have at least a fair amount of trust in former President Donald Trump to make the right recommendations on health issues.
There are a range of sources that Black adults find at least somewhat trustworthy when it comes to health information. Majorities say they would trust health information at least a little if it was reported by most TV news sources asked about in the survey, including local and network news, CNN, MSNBC, and Fox News. At least half also say they would trust health information reported in their local newspaper, the New York Times, Wall Street Journal, or NPR. While no source garners “a lot” of trust from a majority of Black adults, at least one-third say they would trust health information “a lot” if it were reported by their local TV news station, national network news, or CNN.
Despite high use of social media platforms, fewer than one in five say that they would have “a lot of trust” in information related to health if they saw it on these platforms. Notably, however, majorities say they would trust health information at least a little if they saw it on Facebook or YouTube, and about four in ten or more say the same about Instagram, Twitter, and TikTok.
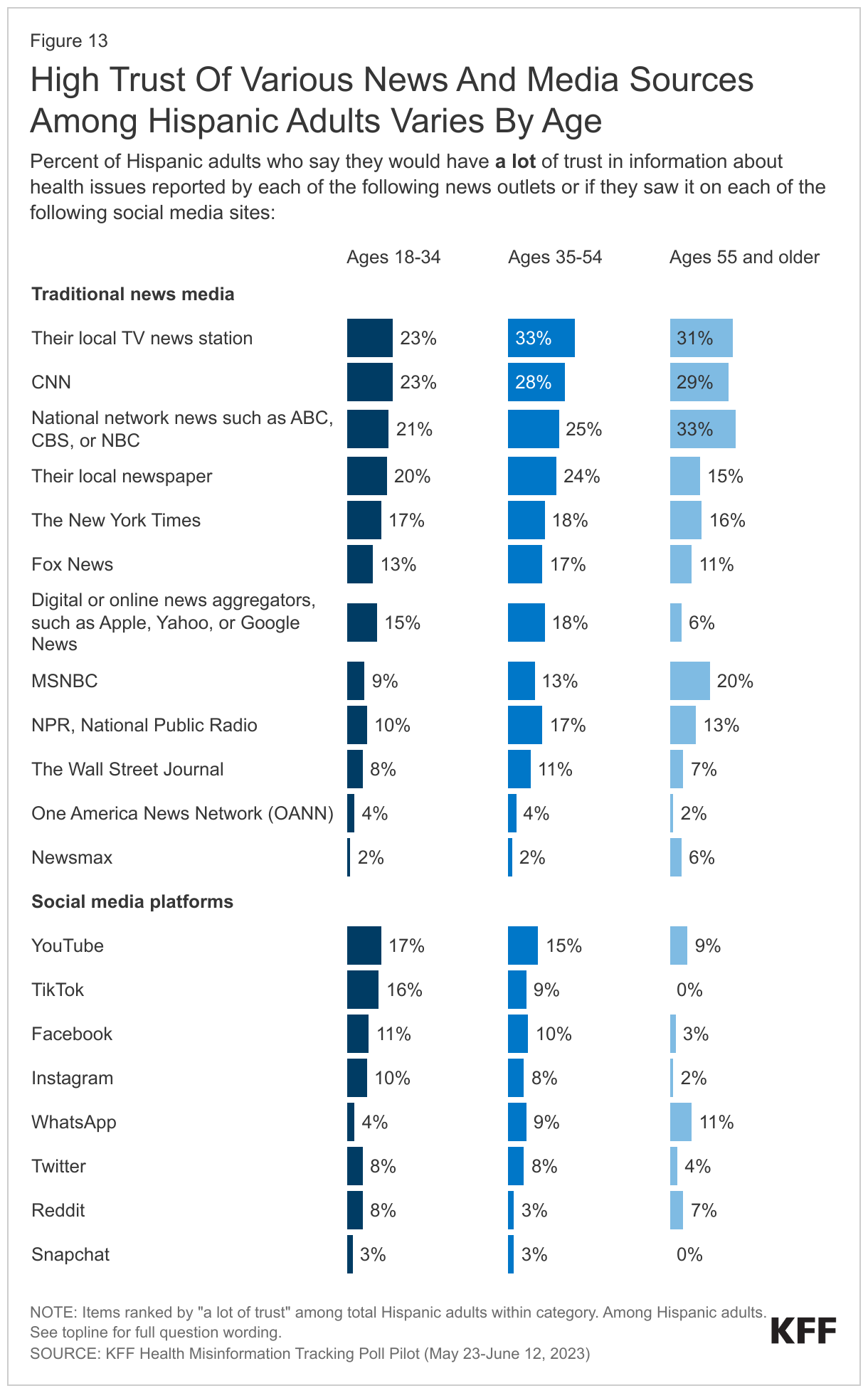
Looking at trust in news and social media sources among Black adults across age groups, local TV news stations and network news rank among the highest for trust in health information. However, across the board, few young Black adults say they would have “a lot” of trust in the health information from any source. Despite high use of social media among younger adults, Black adults under age 35 are more likely to say they would have “a lot” of trust in the health information they may come across on various traditional news sources than social media platforms such as YouTube (21%), TikTok (16%), Instagram (13%), and Twitter (13%).
Support for this work was provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methodology
This KFF Health Misinformation Tracking Poll Pilot was designed and analyzed by public opinion researchers at KFF. The survey was conducted May 23 – June 12, 2023, online and by telephone among a nationally representative sample of N=2,007 U.S. adults in English (1,881) and in Spanish (126). The sample includes 1,532 adults reached through the SSRS Opinion Panel either online or over the phone (n=78 in Spanish). The SSRS Opinion Panel is a nationally representative probability-based panel for which panel members are recruited randomly in one of two ways: (a) Through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Groups (MSG) through the U.S. Postal Service’s Computerized Delivery Sequence (CDS); (b) from a dual-frame random digit dial (RDD) sample provided by MSG. For the online panel component, invitations were sent to panel members by email followed by up to three reminder emails. 1,445 panel members completed the survey online and panel members who do not use the internet were reached by phone (87).
Another 475 (n=48 in Spanish) interviews were conducted from a random digit dial telephone sample of prepaid cell phone numbers obtained through MSG. Phone numbers used for the prepaid cell phone component were randomly generated from a cell phone sampling frame with disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification was based on incidence of the race/ethnicity groups within each frame. Respondents in the prepaid phone samples received a $15 incentive by check received by mail, and panel respondents received a $5 electronic gift card incentive (some harder-to-reach groups received a $10 electronic gift card).
The online questionnaire included two questions designed to establish that respondents were paying attention. Cases that failed both attention check questions, those with over 30% item non-response, and cases with a length less than one quarter of the mean length by mode were flagged and reviewed. Cases were removed from the data if they failed two or more of these quality checks. Based on this criterion, 0 cases were removed.
The combined cell phone and panel samples were weighted to match the sample’s demographics to the national U.S. adult population using data from the Census Bureau’s 2021 Current Population Survey (CPS). Weighting parameters included sex, age, education, race/ethnicity, region, and education. The sample was weighted to match patterns of civic engagement from the September 2017 Volunteering and Civic Life Supplement data from the CPS and to match frequency of internet use from the National Public Opinion Reference Survey (NPORS) for Pew Research Center. Finally, the sample was weighted to match patterns of political party identification based on a parameter derived from recent ABS polls conducted by SSRS polls. The weights take into account differences in the probability of selection for each sample type (prepaid cell phone and panel). This includes adjustment for the sample design and geographic stratification of the cell phone sample, within household probability of selection, and the design of the panel-recruitment procedure.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. KFF public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Support for this work was provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Group
N (unweighted)
M.O.S.E.
Total
2,007
± 3 percentage points
Race/Ethnicity
Black, non-Hispanic
510
± 6 percentage points
Hispanic
514
± 6 percentage points
White, non-Hispanic
866
± 4 percentage points
Black adults by age
Ages 18-34
148
± 11 percentage points
Ages 35-54
197
± 10 percentage points
Ages 55 and older
164
± 10 percentage points
Black adults by educational attainment
Less than a college degree
392
± 7 percentage points
College graduates
116
± 12 percentage points
Endnotes
In race/ethnicity analysis throughout this report Black adults are non-Hispanic. Persons of Hispanic origin may be of any race but are categorized as Hispanic; White adults are non-Hispanic. Sample sizes for other race and ethnic groups were too small for analysis but are included in the total sample.nu00a0 ↩︎
The KFF Health Misinformation Tracking Poll Pilot examines U.S. adults’ use of and trust in different media sources and their exposure to and belief in a series of health-related misinformation claims, including false statements related to COVID-19 and vaccines, reproductive health, and firearm safety. The Health Misinformation Tracking Poll will work in tandem with KFF’s forthcoming Health Misinformation Monitor, a detailed report of the landscape of health misinformation messages circulating among the public, probing the impact of misinformation documented in the monitor to help inform and strengthen efforts aimed at addressing misinformation in health. Both the Misinformation Tracking Poll and the Monitor are part of a new program on health misinformation and trust being developed at KFF. This snapshot from our initial pilot poll provides a look at the survey results among Hispanic adults1 and their implications for addressing health-related misinformation among this community. Other snapshot reports provide similar insights into addressing misinformation among Black adults and among rural residents. These snapshot reports are aimed at helping organizations in the U.S. working to combat health-related misinformation and rebuild trust in the media, public health, and scientific communities.
Key Takeaways for the Field
While large shares of Hispanic adults have heard many widely circulated falsehoods related to COVID-19, reproductive health, and guns, few are convinced that these falsehoods are true, providing an opportunity for intervention. When presented with specific items of health misinformation, few Hispanic adults (one in ten or fewer for all items except for one) say they believe them to be “definitely true,” while modest shares (between 13% and 37%) recognize each to be “definitely false.” Similar to adults overall, most Hispanic adults fall somewhere in the uncertain middle, saying each claim is “probably true” or “probably false.” While few Hispanic adults are convinced of these false and inaccurate claims, exposure to multiple pieces of health misinformation may contribute to uncertainty and doubt which could impact their health care decisions.
Hispanic adults with lower levels of educational attainment are more inclined to believe certain false claims related to health, suggesting that efforts to address health misinformation need to be accessible to Hispanic adults with differing levels of education. This finding is consistent with the public overall, as those without a college degree are more susceptible to believing certain types of health misinformation. In addition to differences by educational attainment, partisanship plays a big role, as Republican-leaning and independent Hispanic adults are more likely to believe many health-related falsehoods than those who lean toward the Democratic party.
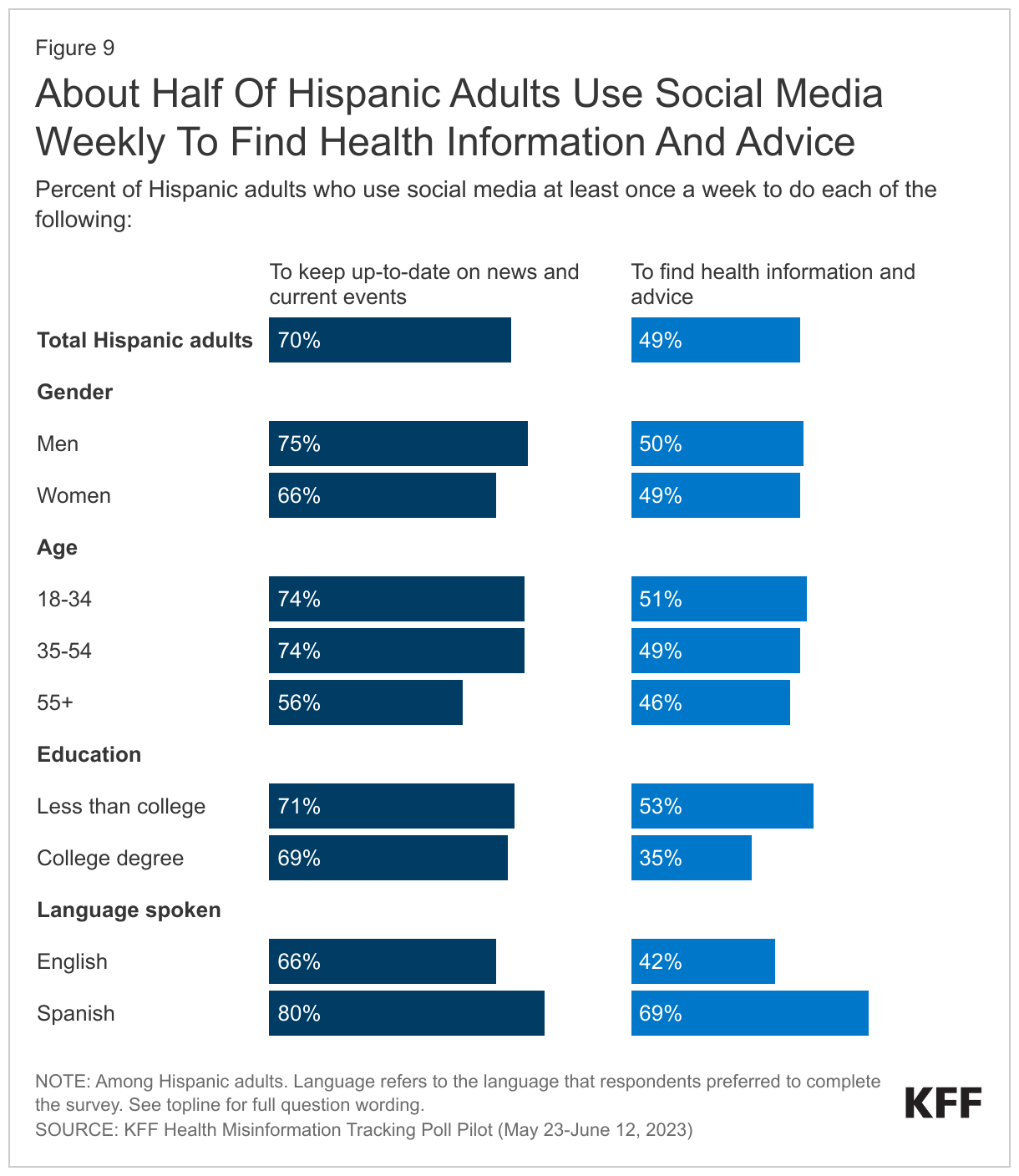
Social media is an especially prominent source of health information for Hispanic adults, particularly those without a college degree and those who primarily speak Spanish. About half of Hispanic adults say they use social media at least once a week to find health information and advice, more than three times the share of White adults who say they do this. The share of Hispanic adults who use social media at least weekly for health information rises to 53% among Hispanic adults without a college degree and nearly seven in ten (69%) among Spanish speakers2 . Given the large shares that seek health information and advice via social media, it may present a particularly important avenue for organizations addressing misinformation among Hispanic adults.
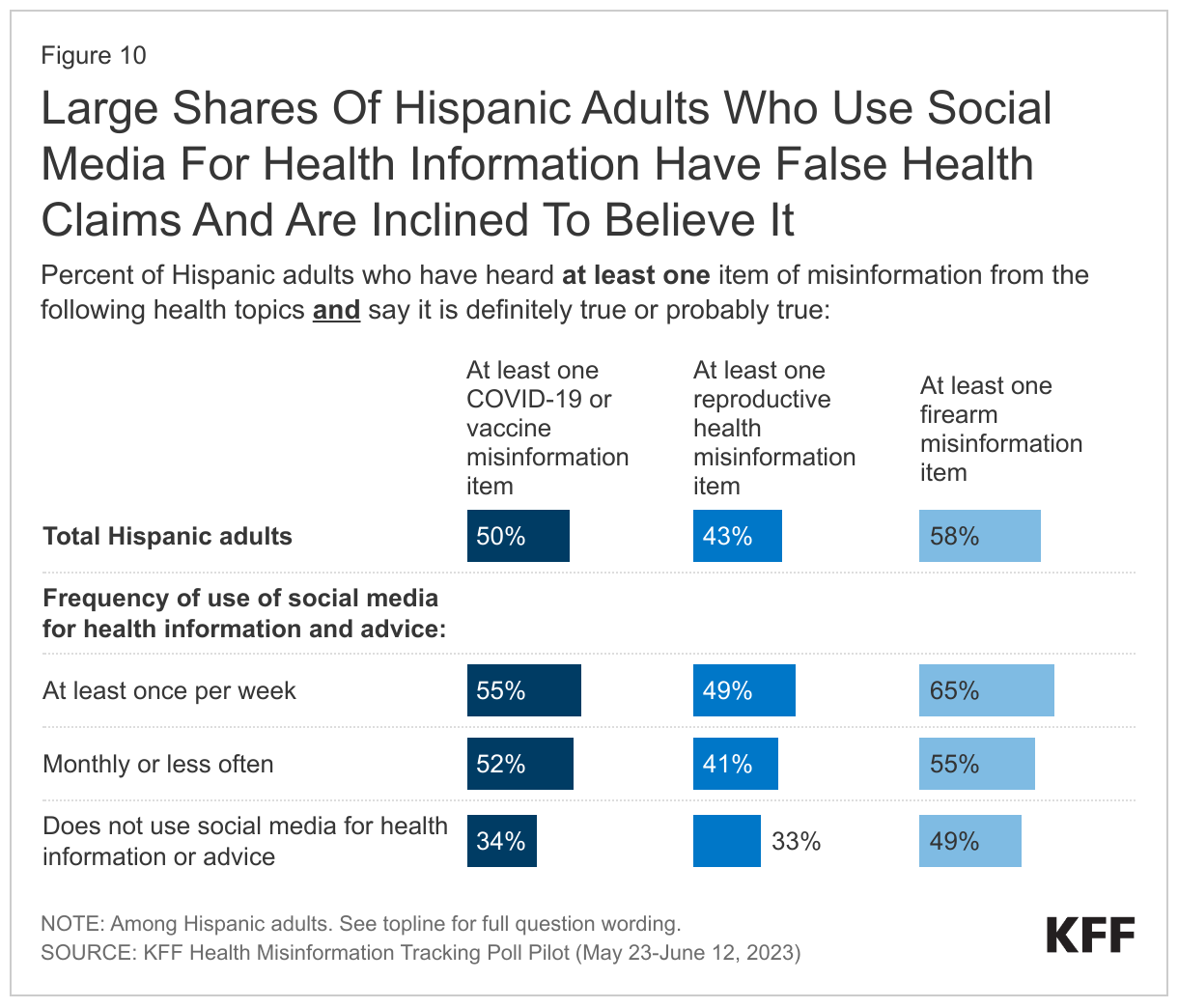
Although few Hispanic adults say they would have a lot of trust in health information posted on social media, those who use social media for health advice are more open to believing health misinformation than those who don’t. While it is frequently cited as a source, few — less than one in six — Hispanic adults say they would have a lot of trust in information about health issues if they saw it on any social media platform included on the survey. However, those who rely on social media at least occasionally for health advice are more likely than those who do not seek health information on social media to have heard and believe at least one item of COVID-19 and vaccine misinformation and at least one reproductive health misinformation item. Health information and advice from social media – though it may not be entirely trusted – may nonetheless plant seeds of doubt and confusion over what information is accurate and what is false.
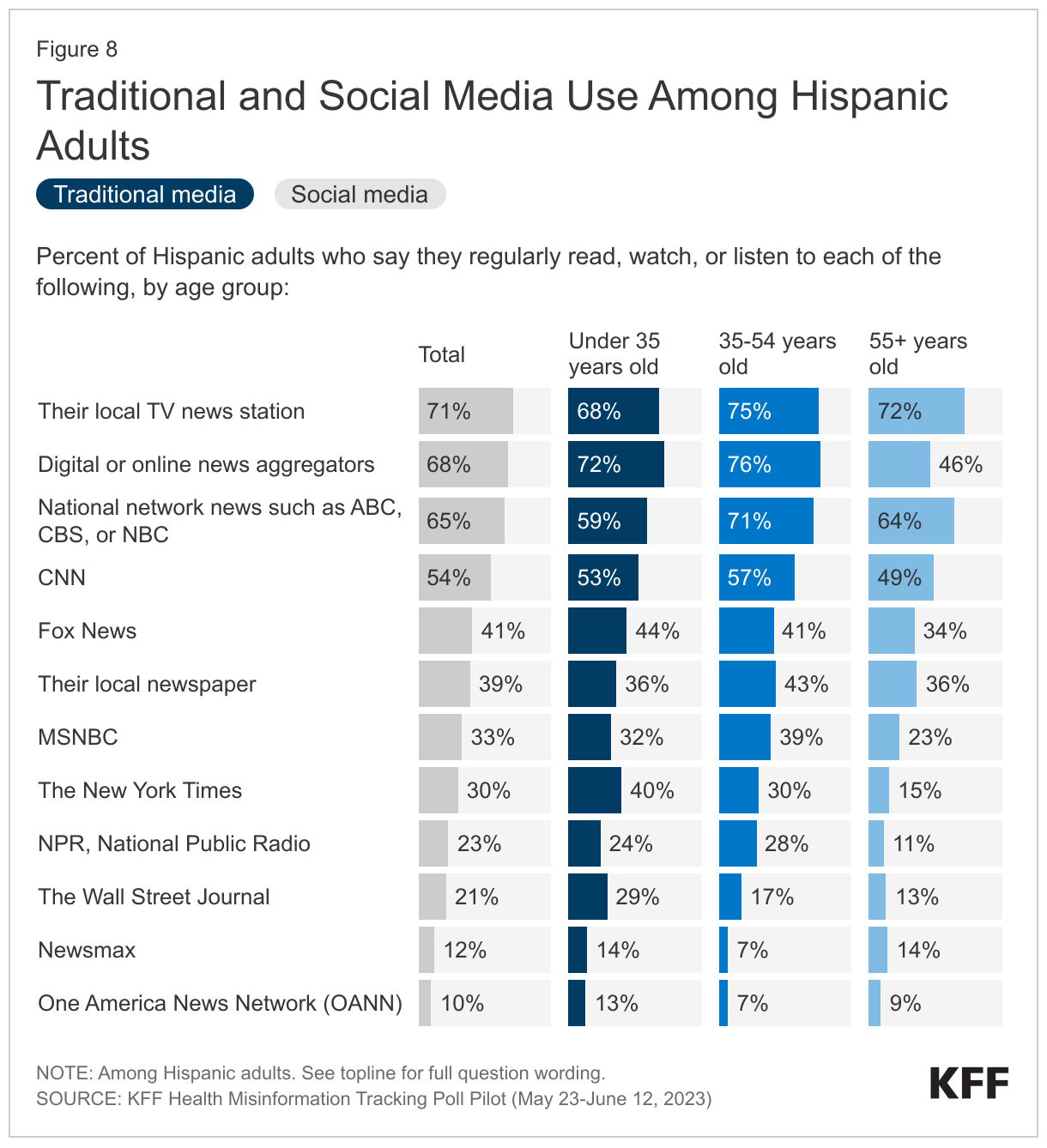
Though social media use is popular among large shares of Hispanic adults, traditional media viewership and readership are also high, and some sources such as local TV news and network news are far more likely to be trusted. Television is among the most commonly reported medium for news consumption among Hispanic adults across age groups with majorities reporting regularly watching local news and national network news. These traditional news sources are also more likely to be trusted with about one in four Hispanic adults saying they would have “a lot” of trust in health information they report, suggesting that they may offer an opportunity for efforts to address misinformation.
Spanish-speaking adults are most trusting of Spanish-language news sources and are much more likely to use WhatsApp than Hispanic adults who primarily speak English. When asked to say in their own words, what is the one news source they trust the most to provide them with reliable information, more than one in four (28%) Spanish-speaking Hispanic adults name Telemundo or Univision, while fewer name various specific English-language sources. Spanish-language sources, both news and commonly used platforms such as WhatsApp, can be useful tools for addressing misinformation among Spanish-speakers, especially in light of this population’s reliance on social media for health information and advice.
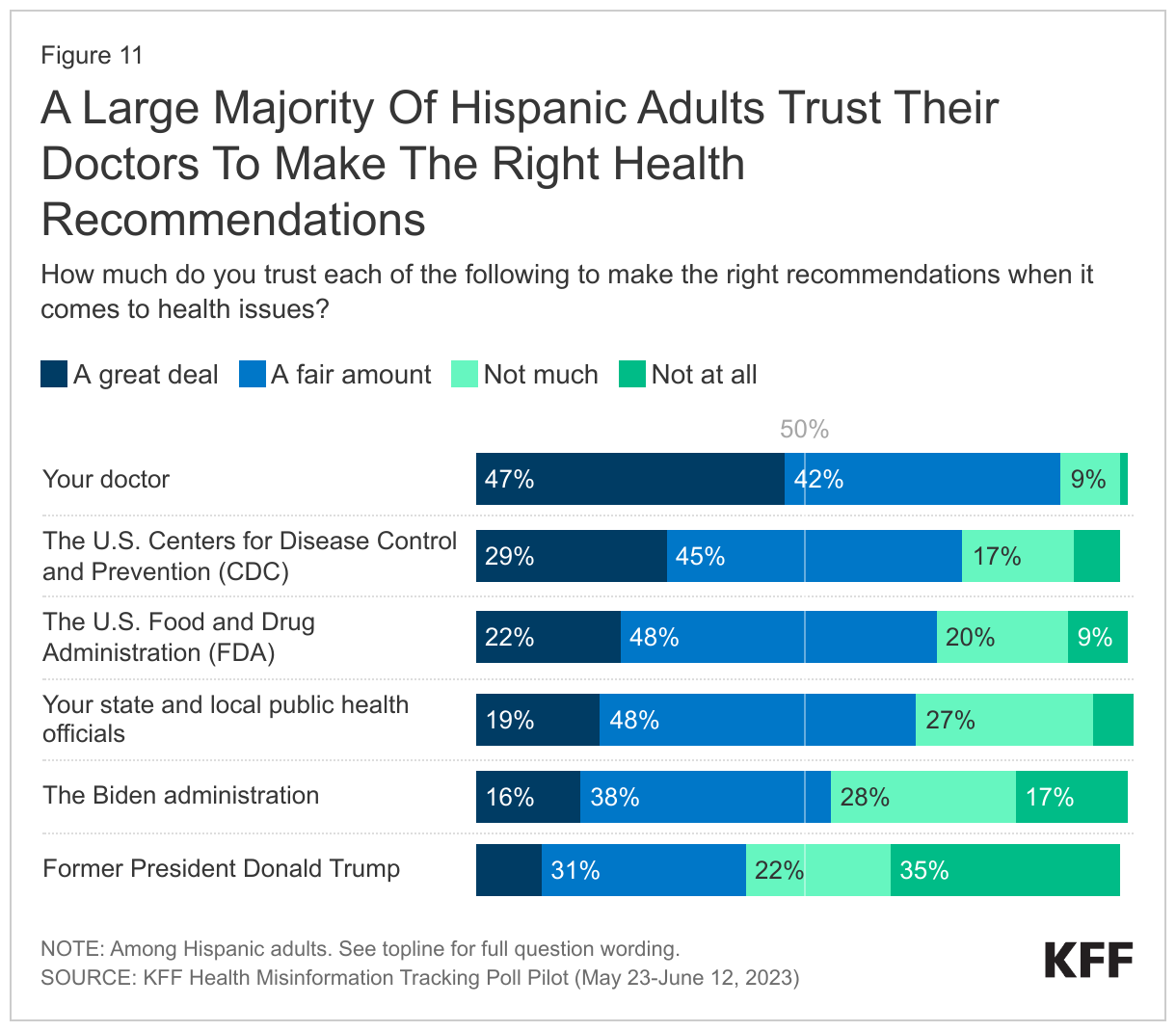
Hispanic adults are generally trusting of the CDC, FDA, and local public health officials when it comes to health recommendations, though personal doctors are by far the most trusted messengers, highlighting the importance of personal connections. More than two-thirds of Hispanic adults have at least a fair amount of trust in the CDC, the FDA, and in their state and local public health officials to make the right recommendation on health issues and a slight majority express trust in the health recommendations from the Biden Administration. However, mirroring adults overall, personal doctors are by far the most trusted among Hispanic adults, highlighting the opportunity medical professionals have in utilizing the personal connections they have with patients to reinforce accurate health information and dispel false and inaccurate claims.
Exposure to and Belief in Health Misinformation
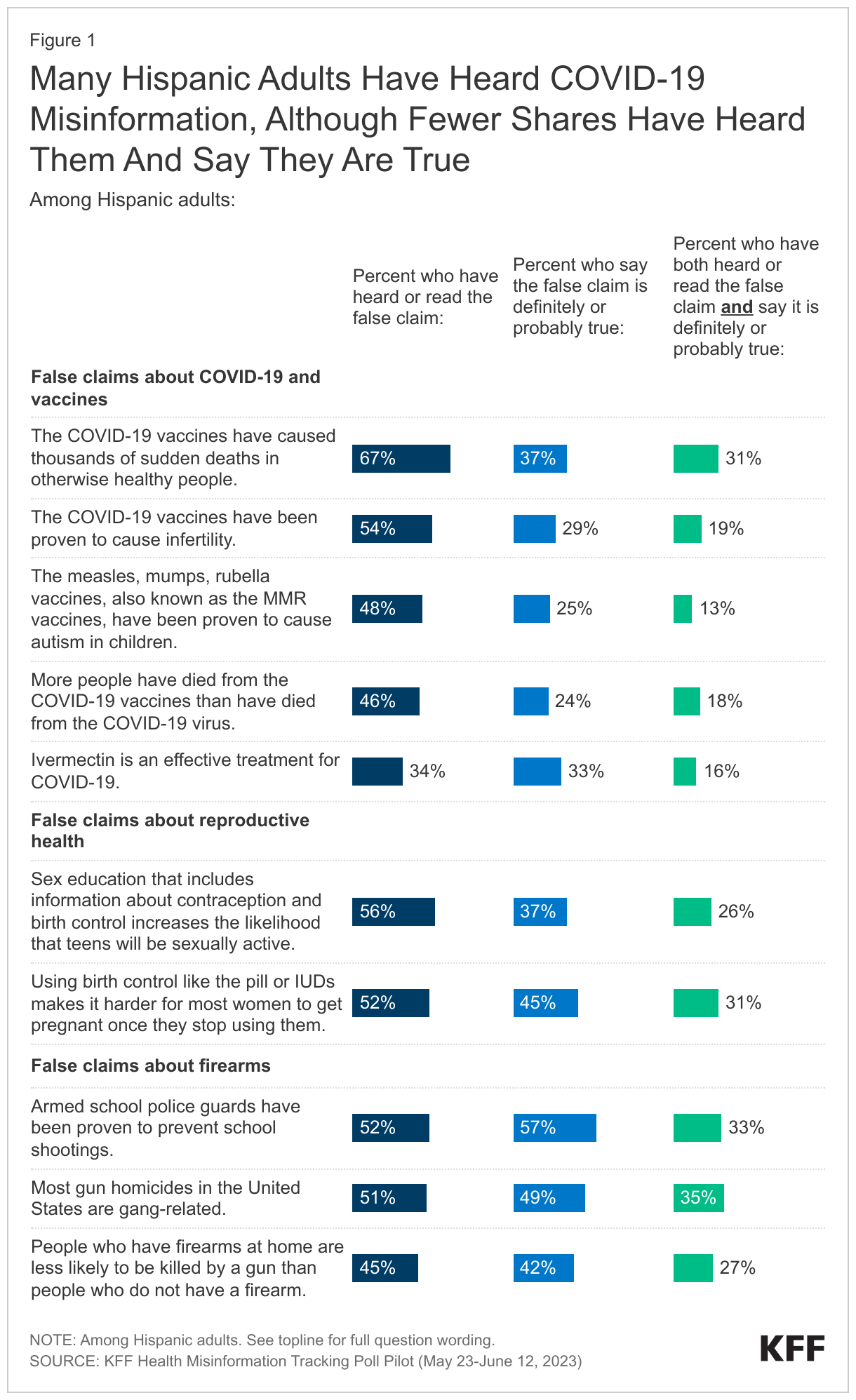
The KFF Health Misinformation Tracking Poll Pilot finds that, similar to adults overall, notable shares of Hispanic adults have been exposed to health-related misinformation. However, relatively few (10% or fewer on all items except for one at 17%) are convinced that the health misinformation claims included in the survey are “definitely true.” Modest shares (between 13% and 37%) fully reject these misinformation items as “definitely false.” Similar to the public overall, large shares of Hispanic adults are in a larger “muddled middle” group saying that false claims are “probably true” or “probably false.”
Between about one-third and two-thirds of Hispanic adults have heard each of the items of health misinformation included in the survey. Notably, two-thirds of Hispanic adults (67%) say they have heard the false claim that COVID-19 vaccines have caused thousands of sudden deaths in otherwise healthy people. Majorities say they have heard that sex education that includes information about contraception and birth control increases the likelihood that teens will be sexually active (56%), and that the COVID-19 vaccines have been proven to cause infertility (54%). Among Hispanic adults, certain groups are more likely to say they have encountered certain topics of health misinformation. For example, young Hispanic women are more likely than their older counterparts to say they have heard the false claim that using birth control like the pill or IUDs makes it harder for most women to get pregnant once they stop using them.
Regardless of whether they have heard or read specific items of misinformation, the survey also asked people whether they think each claim is definitely true, probably true, probably false, or definitely false. For most of the misinformation items included in the survey, between about one-quarter and six in ten Hispanic adults say they are “definitely” or “probably true.” Combining these measures, smaller shares of Hispanic adults (between one in ten and three in ten) both have heard each claim and believe it is probably or definitely true.
Measures of Health Misinformation
This report examines three measures of health misinformation among the public. Adults were asked whether they had heard or read specific false health-related statements. Regardless of whether they have heard or read specific items of misinformation, all were asked whether they thought each claim was definitely true, probably true, probably false, or definitely false. We then combined these two measures to examine the share who have heard the false claims and believe it is definitely or probably true.
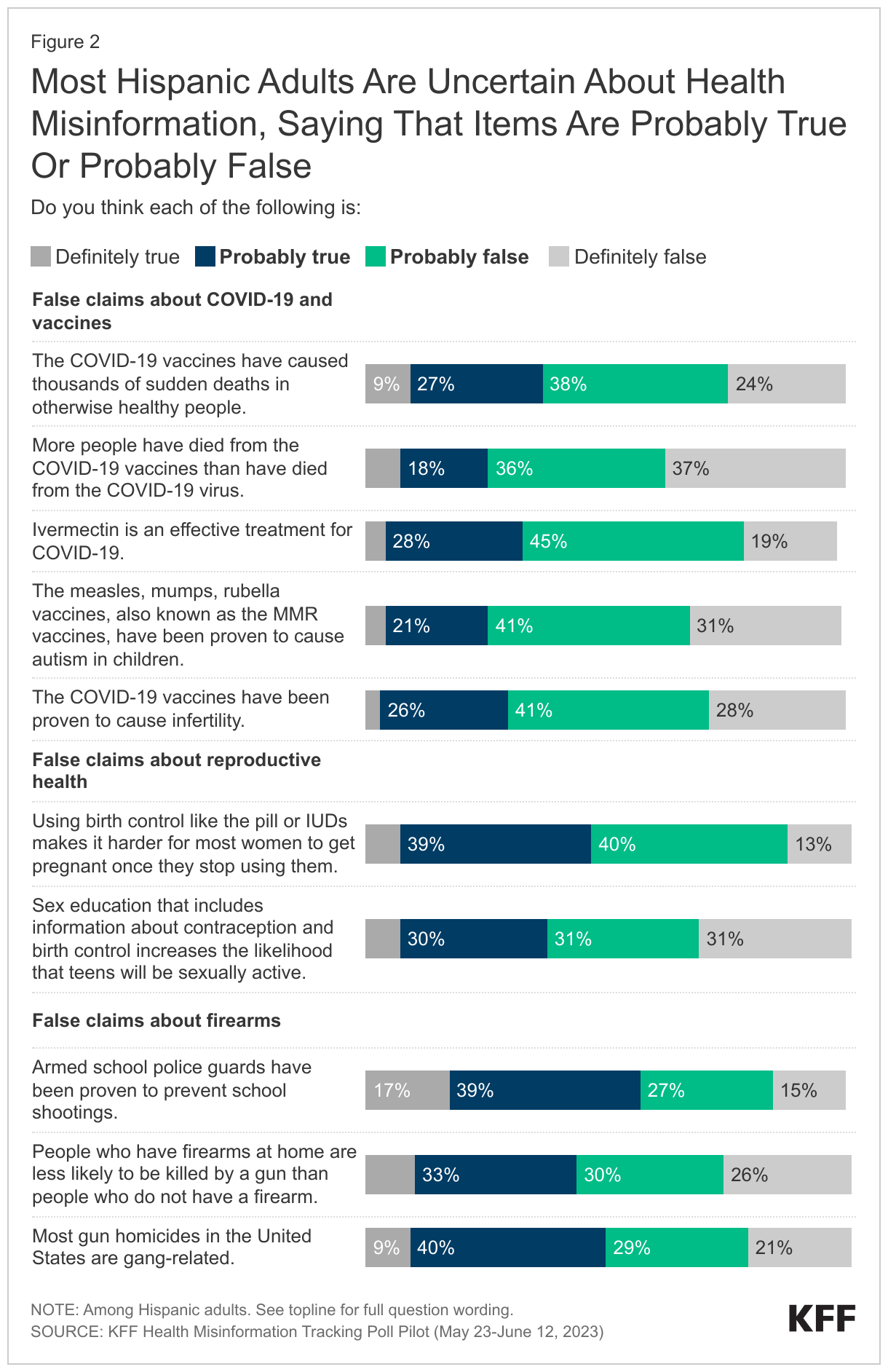
Most Hispanic adults have some doubt or uncertainty about the whether the misinformation claims tested in the survey are true or not, with majorities saying each is either “probably true” or “probably false.” On all items except one at 17%, one in ten Hispanic adults or fewer say that the false claims are “definitely true.”
The largest shares of Hispanic adults express belief in two falsities related to firearms: about six in ten (57%) Hispanic adults say that the false claim that “armed school police guards have been proved to prevent school shootings” is “definitely” or “probably true,” and half (49%) say that the false claim that “most gun homicides in the U.S. are gang-related” is “definitely” or “probably true.” Hispanic adults who say they or someone in their household is a gun owner are just as likely as those who do not live with a gun owner to say each of these gun-related falsities is “probably” or “definitely true.”
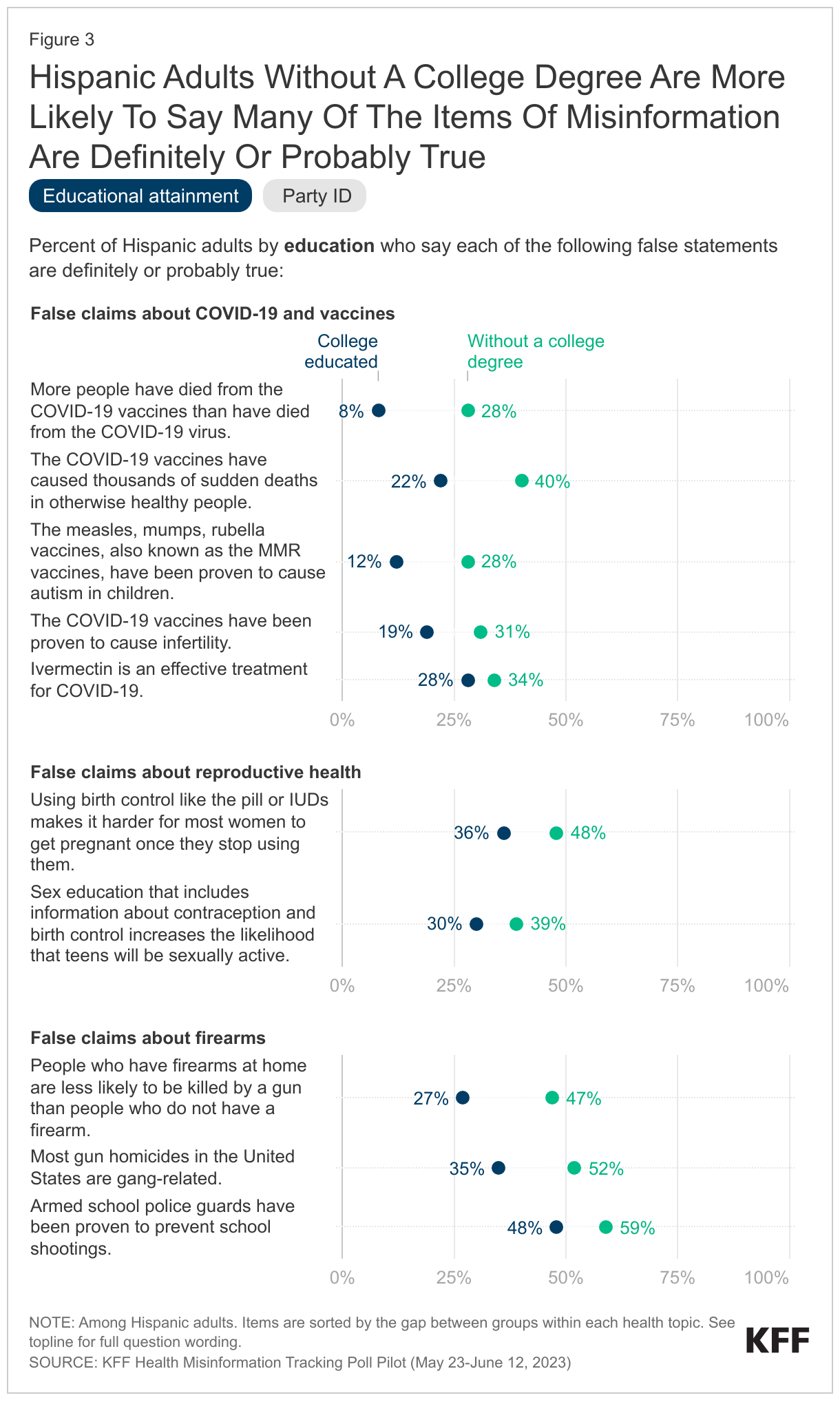
The figures below show the assessments of the verity of each of the claims by Hispanic adults by educational attainment and partisanship. Generally, Hispanic adults without a college degree are more likely than their college educated counterparts to say most of the items of misinformation examined in the survey are definitely or probably true. Consistent with patterns among the public overall, Hispanic adults who identify as Republicans or lean towards the Republican Partytand out as being more likely than Democratic-leaning Hispanic adults to say most of the misinformation items are probably or definitely true. For most of the health falsities explored in this survey, there were no significant differences among Hispanic adults by primary language or nativity (U.S.-born vs. foreign-born) in their assessments.
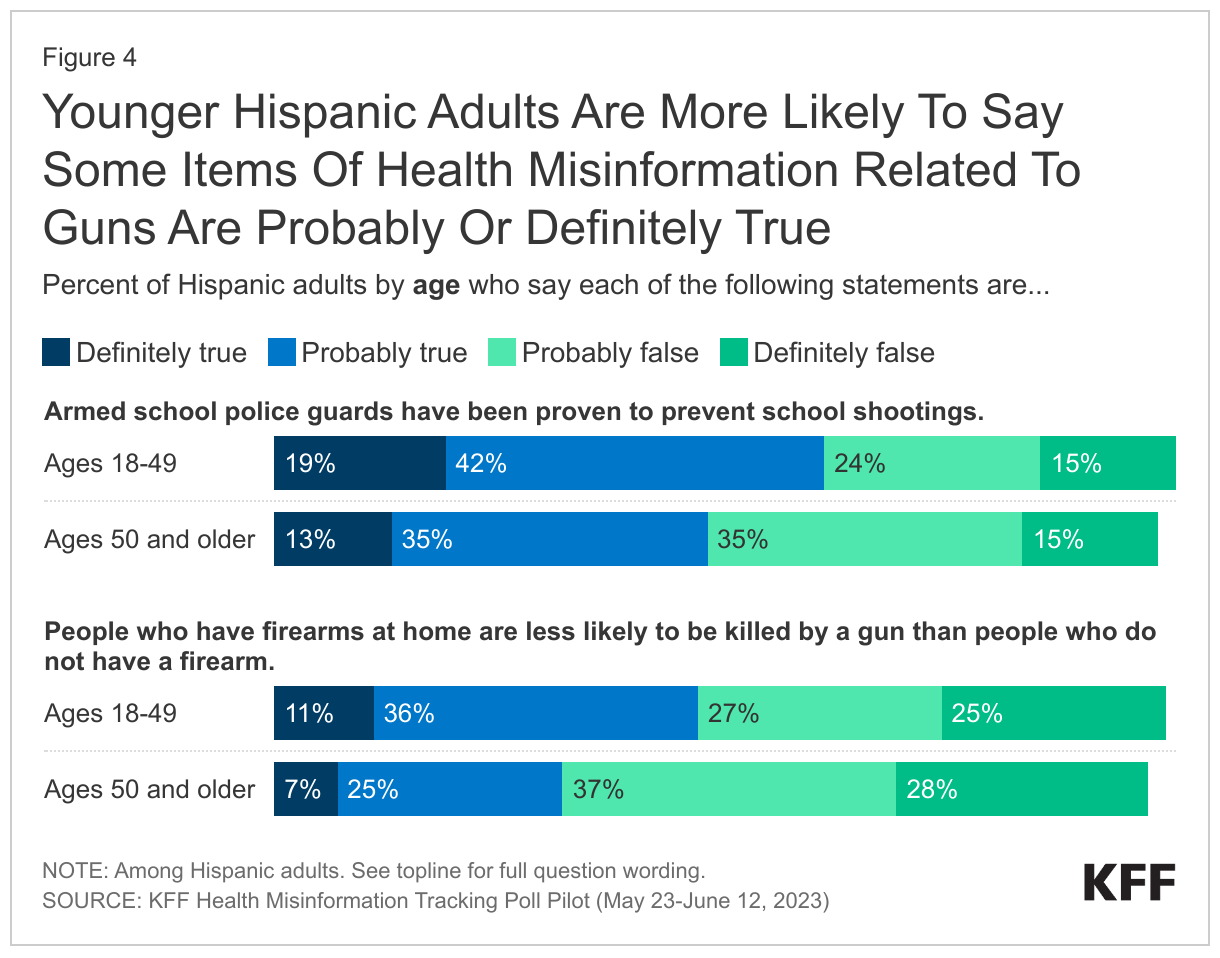
There are fewer notable differences across age groups when it comes to Hispanic adults’ assessments of the verity of misinformation statements related to COVID-19, though those under the age of 50 are more likely to believe some falsities related to guns. A majority of Hispanic adults under age 50 say that it is “definitely” or “probably true” that armed school police guards have been proven to prevent school shootings, compared to about half of Hispanic adults ages 50 and older. Similarly, Hispanic adults under age 50 are more likely than older Hispanic adults to say it is true that people with firearms at home are less likely to be killed by a gun than people who do not have a firearm. For both of these false statements, this difference is mostly driven by the larger share of younger adults who say the statements are “probably true.”
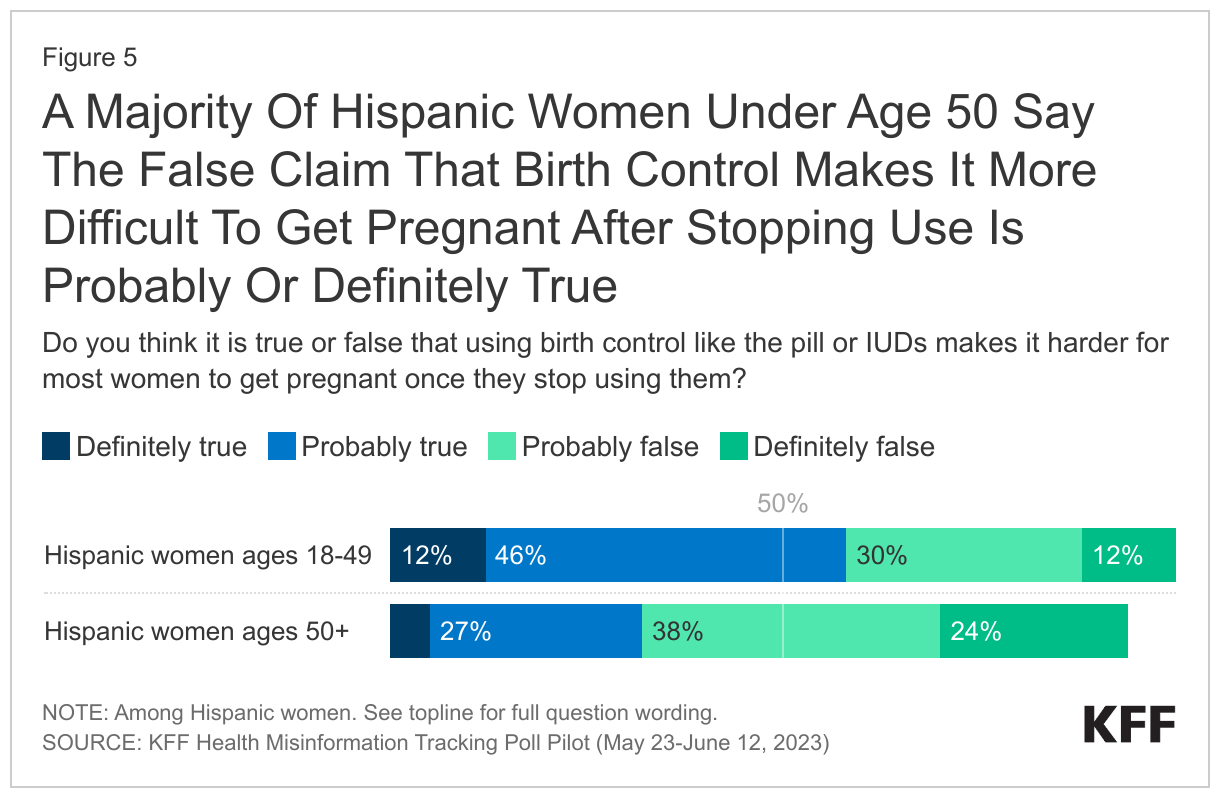
A majority of Hispanic women of reproductive age (ages 18 to 49) say it is probably or definitely true that using hormonal birth control makes it harder for most women to get pregnant after ceasing birth control use, while most Hispanic women ages 50 or older say it is probably or definitely false.
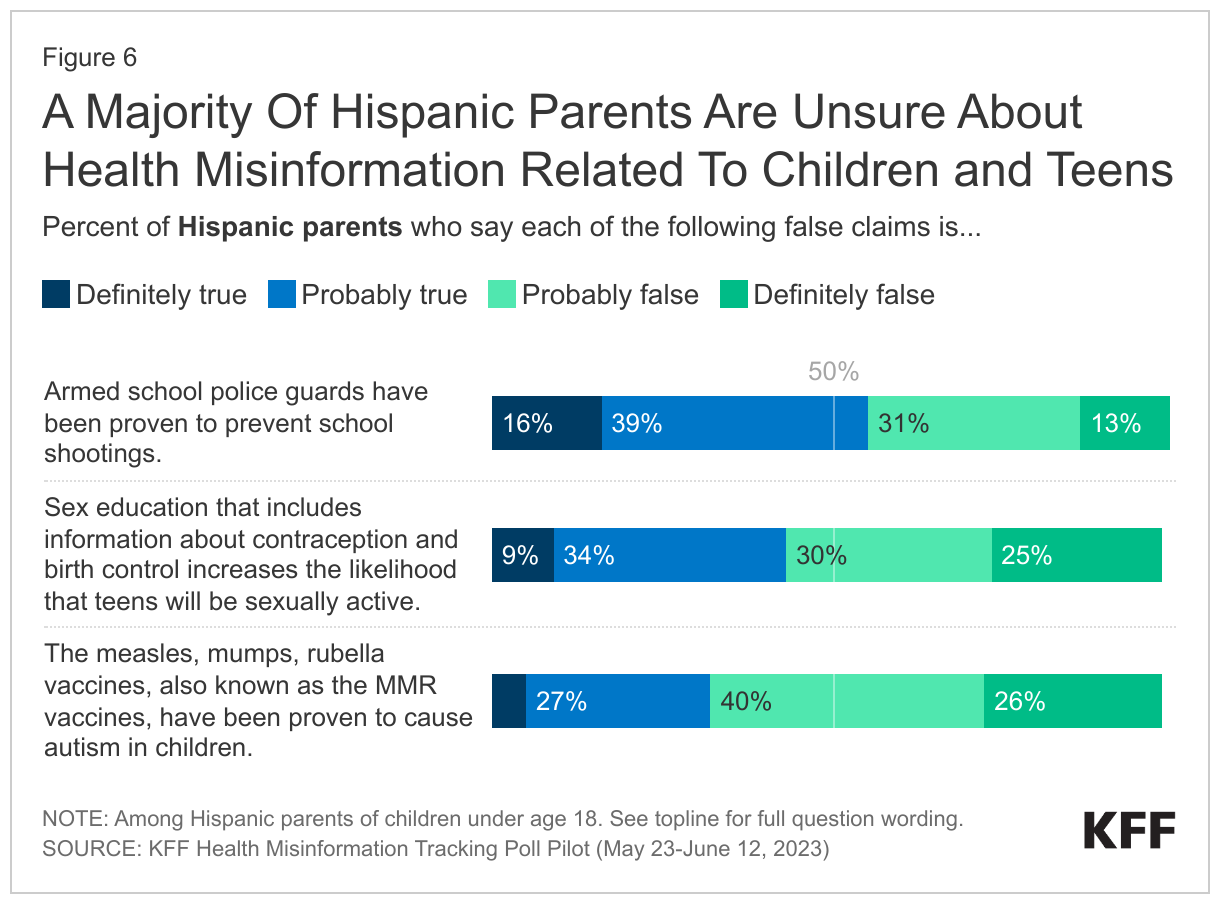
Most Hispanic parents are unsure about some of the misinformation items examined in the survey related to children, teens, and schools, with a majority saying it is “probably true” or “probably false” that armed school guards have been proven to prevent school shootings, that the MMR vaccines cause autism in children, and that sex education with information regarding contraception increases the likelihood that teens will be sexually active. About one in four Hispanic parents (26%) say it is “definitely false” that MMR vaccines cause autism or that comprehensive sex education increases the likelihood that teens would be sexually active (25%).
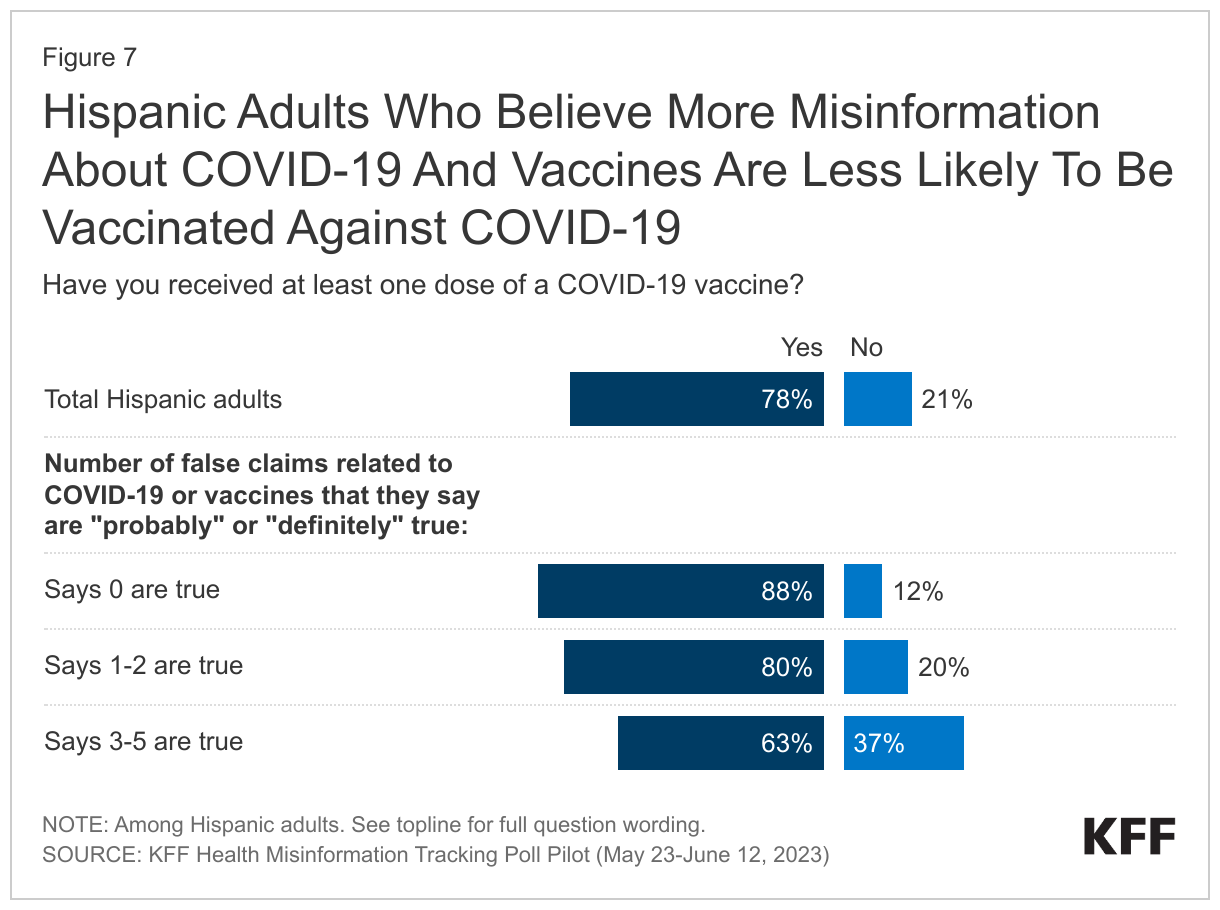
When it comes to COVID-19 and vaccines, belief in misinformation is correlated with Hispanic adults’ individual vaccination status: while nearly nine in ten Hispanic adults who indicate that none of the items of vaccine or COVID misinformation presented are true are vaccinated against COVID-19, fewer (63%) Hispanic adults who believe between 3 and 5 items of COVID misinformation say they are vaccinated against the virus.
Media Consumption and Trust
Consumption of News, Social Media, and Health Information
Television is the most commonly reported medium for news consumption among Hispanic adults across age groups with large majorities saying they regularly watch local news and national network news. For Hispanic adults under age 55, digital news aggregators that draw on multiple news sources are consumed on par with television news. Few Hispanic adults across age groups report regular consumption of conservative national news networks such as OANN or Newsmax, though about four in ten Hispanic adults under age 55 and about a third of those age 55 or older say they regularly watch Fox News.
Social media use, not surprisingly, varies by age among Hispanic adults as well. At least seven in ten Hispanic adults across age groups say they use Facebook at least once per week. A majority of Hispanic adults under age 55 also regularly use YouTube and Instagram. At least one-third of Hispanic adults across age groups use WhatsApp at least weekly, rising to 87% of Spanish-speaking Hispanic adults, likely reflecting high international use of this app. Hispanic adults under age 35 are much more likely than those 35 and older to regularly use Instagram TikTok (61%), Snapchat (52%), and Reddit (26%).
When asked to say in their own words, what is the one news source they trust the most to provide them with reliable information, regardless of the sources asked about explicitly in the survey, more than one-third (28%) of Spanish-speaking Hispanic adults say Telemundo or Univision, while fewer name various specific English-language sources. In-language sources, both news and commonly used platforms such as WhatsApp, can be useful tools for addressing misinformation among Spanish-speakers and the Hispanic community generally.
Regardless of preferred social media platform, seven in ten Hispanic adults use social media at least once a week to stay up to date on news and current events. This rises to three-fourths of Hispanic adults under age 35 and eight in ten Hispanic adults who primarily speak Spanish. Half of Hispanic adults (49%) – compared to just 15% of White adults and about a third of Black adults – use social media regularly to find health information and advice. Similar shares across age report this, but this rises to half (52%) of Hispanic adults without college degrees and seven in ten (69%) Hispanic adults who primarily speak Spanish.
Among Hispanic adults, the use of social media, even occasionally, for health information and advice is correlated with hearing and believing items of health misinformation. For example, at least half of Hispanic adults who use social media for health information and advice say that they have heard at least one of the false COVID-19 or vaccine claims tested in the survey and think it is definitely or probably true, compared to about one-third of those who don’t use social media for health advice.
Trust in Sources of Information
Doctors with personal relationships are the most trusted sources of health information for Hispanic adults, with the vast majority saying they trust their doctor “a great deal” or a “fair amount” to make the right recommendations when it comes to health issues. Notably, a large majority of Hispanic adults have at least “a fair amount” of trust in the CDC, FDA, and their local public health officials. Hispanic adults are more divided when it comes to trust in health recommendations from the Biden administration and former President Trump, with a slight majority saying they would have at least a fair amount of trust in the Biden administration to make the right health recommendations, while four in ten would have at least a fair amount of trust in former President Trump. Democratic-leaning Hispanic adults are more trusting of the current administration, while Republican-leaning Hispanic adults are more trusting of the former president’s recommendations. Overall, recommendations from government agencies are deemed trustworthy but even more likely to be trusted when presented by their personal doctors. Health recommendations from political actors are unlikely to be trusted by those of the opposing partisan persuasion.
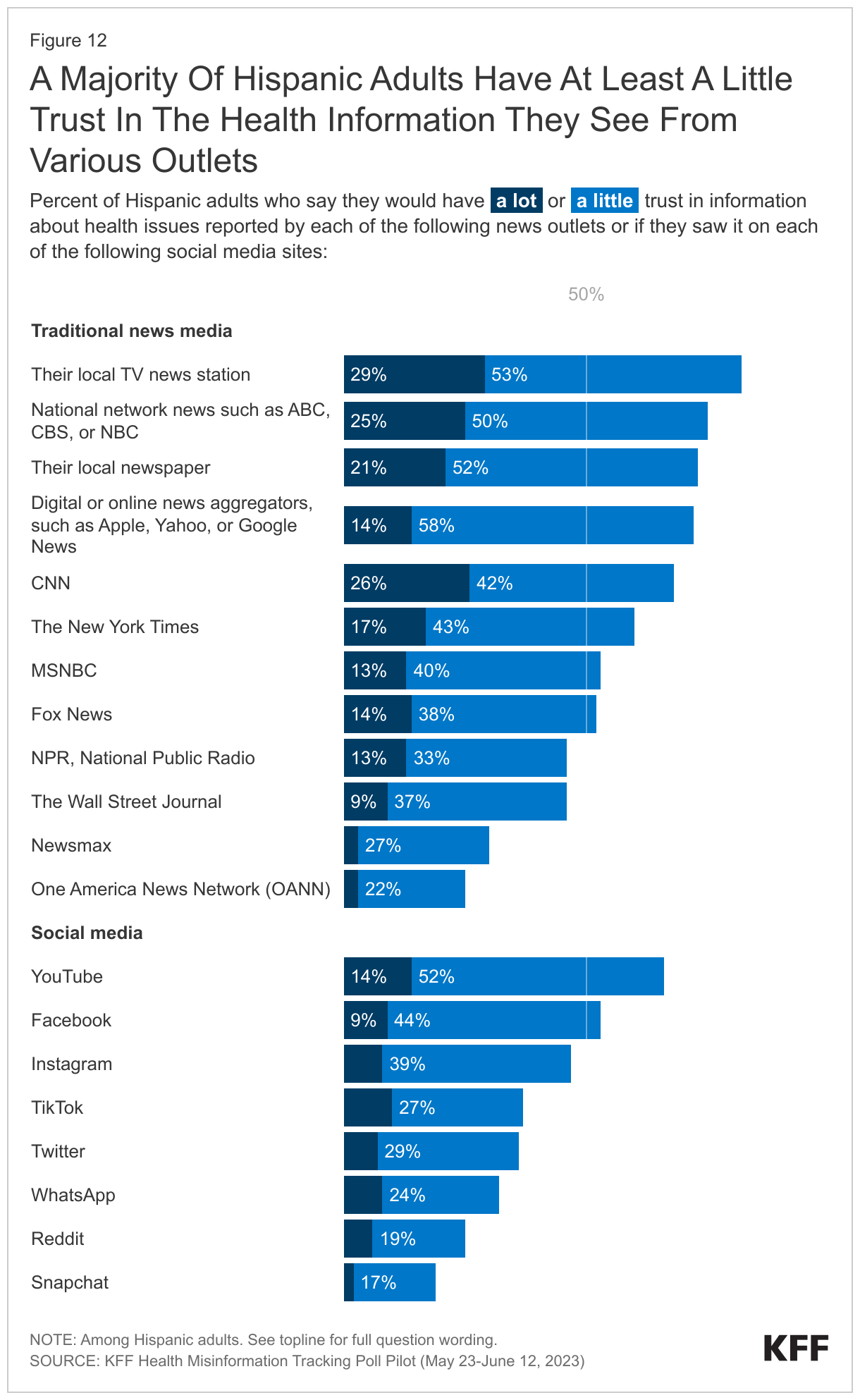
There are a range of news sources and platforms that Hispanic adults find at least somewhat trustworthy when it comes to health information. At least half say they would trust health information at least a little if it was reported by most TV news sources including local and network news, CNN, MSNBC, and Fox News. Nearly three in four also say they would have at least a little trust in health information reported in their local newspaper and six in ten say they would trust it if they saw it reported by the New York Times. While no source garners “a lot” of trust from a majority of Hispanic adults, at least one-quarter say they would trust health information “a lot” if it were reported by their local TV news station, national network news, or CNN.
Despite high use of social media platforms, fewer than one in six Hispanic adults say that they would have “a lot of trust” in health information if they saw it on these platforms. Two-thirds say they would trust health information at least a little if they saw it on YouTube, and about half say the same about Facebook and Instagram. Notably, WhatsApp – despite being used at least once per week by half of Hispanic adults – ranks low in terms of how much health information would be trusted on the platform, with just 8% of total Hispanic adults saying they would trust information on the platform “a lot,” rising to 12% among users of the app.
Support for this work was provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methodology
This KFF Health Misinformation Tracking Poll Pilot was designed and analyzed by public opinion researchers at KFF. The survey was conducted May 23 – June 12, 2023, online and by telephone among a nationally representative sample of N=2,007 U.S. adults in English (1,881) and in Spanish (126). The sample includes 1,532 adults reached through the SSRS Opinion Panel either online or over the phone (n=78 in Spanish). The SSRS Opinion Panel is a nationally representative probability-based panel for which panel members are recruited randomly in one of two ways: (a) Through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Groups (MSG) through the U.S. Postal Service’s Computerized Delivery Sequence (CDS); (b) from a dual-frame random digit dial (RDD) sample provided by MSG. For the online panel component, invitations were sent to panel members by email followed by up to three reminder emails. 1,445 panel members completed the survey online and panel members who do not use the internet were reached by phone (87).
Another 475 (n=48 in Spanish) interviews were conducted from a random digit dial telephone sample of prepaid cell phone numbers obtained through MSG. Phone numbers used for the prepaid cell phone component were randomly generated from a cell phone sampling frame with disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification was based on incidence of the race/ethnicity groups within each frame. Respondents in the prepaid phone samples received a $15 incentive by check received by mail, and panel respondents received a $5 electronic gift card incentive (some harder-to-reach groups received a $10 electronic gift card).
The online questionnaire included two questions designed to establish that respondents were paying attention. Cases that failed both attention check questions, those with over 30% item non-response, and cases with a length less than one quarter of the mean length by mode were flagged and reviewed. Cases were removed from the data if they failed two or more of these quality checks. Based on this criterion, 0 cases were removed.
The combined cell phone and panel samples were weighted to match the sample’s demographics to the national U.S. adult population using data from the Census Bureau’s 2021 Current Population Survey (CPS). Weighting parameters included sex, age, education, race/ethnicity, region, and education. The sample was weighted to match patterns of civic engagement from the September 2017 Volunteering and Civic Life Supplement data from the CPS and to match frequency of internet use from the National Public Opinion Reference Survey (NPORS) for Pew Research Center. Finally, the sample was weighted to match patterns of political party identification based on a parameter derived from recent ABS polls conducted by SSRS polls. The weights take into account differences in the probability of selection for each sample type (prepaid cell phone and panel). This includes adjustment for the sample design and geographic stratification of the cell phone sample, within household probability of selection, and the design of the panel-recruitment procedure.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. KFF public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Support for this work was provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Group
N (unweighted)
M.O.S.E.
Total
2,007
± 3 percentage points
Race/Ethnicity
Hispanic
514
± 6 percentage points
Black, non-Hispanic
510
± 6 percentage points
White, non-Hispanic
866
± 4 percentage points
Hispanic adults by age
Ages 18-34
205
± 9 percentage points
Ages 35-54
208
± 9 percentage points
Ages 55 and older
100
± 13 percentage points
Hispanic adults by educational attainment
Less than a college degree
372
± 7 percentage points
College graduates
141
± 11 percentage points
Endnotes
In race/ethnicity analysis throughout this report, persons of Hispanic origin may be of any race but are categorized as Hispanic; Black adults are non-Hispanic; White adults are non-Hispanic. Sample sizes for other race and ethnic groups were too small for analysis but are included in the total sample.nu00a0 ↩︎
Spanish-speaking Hispanic adults are those who identified as Hispanic and opted to complete the survey in Spanish. ↩︎
KFF Examines Challenges in Navigating Coverage for Opill, the First Over-the-Counter Daily Oral Contraceptive Pill, Coming to Market Next Year
States’ Experiences Covering Other Forms of Over-the-Counter Contraception Suggest Significant Obstacles to Affordability, Implementation, and Coverage
As Opill—the first over-the-counter daily oral contraceptive pill in the United States—is expected to be available for purchase in early 2024, new research conducted by KFF examines barriers to its accessibility for consumers and challenges in providing insurance coverage for it.
Based on interviews with nearly 80 representatives from private insurance plans, state Medicaid programs, chain pharmacies, and other key groups, the report provides a deeper view into the operational challenges in expanding access to coverage of over-the-counter contraceptive pills.
Although the new over-the-counter birth control pill could broaden access to contraceptive options across the country, KFF interviews with experts uncovered that consumers are likely to face some hurdles if they seek to have their plan cover the costs. According to the interviewees, the extent to which Opill can expand contraceptive options will depend on several factors, including clear state and federal policies and protocols, insurance coverage, pharmacy engagement, pharmacy stocking and signage, cost, and broad-scale public awareness and education.
Perrigo, Opill’s manufacturer, has yet to announce the price of the contraceptive, which will have implications for affordability, particularly if Opill is not covered by insurance or Medicaid.
While states could require coverage of Opill in fully insured health plans, only a federal requirement would reach self-insured plans, which cover most people with employer-sponsored health coverage. A federal requirement would also apply to states that do not have existing over-the-counter contraceptive coverage requirements. Under the Affordable Care Act, health plans are generally required to cover a wide range of preventive services with no patient co-pays, including contraceptives with a prescription.
In states where over-the-counter contraceptive methods are covered without a prescription by Medicaid or private plans, consumers will generally need to get Opill at the pharmacy counter for their plan to cover it. In some private health plans, consumers may be able to pay for Opill up front and then seek reimbursement from the plan, but that could be financially and administratively burdensome for consumers and is reportedly rarely used for other over-the-counter drugs available without a prescription.
Insurance Coverage of OTC Oral Contraceptives: Lessons from Field is based on interviews conducted from January to August 2023, with nearly 80 experts and key players such as pharmacists, health plans, and state Medicaid officials involved in the coverage and provision of over-the-counter contraception in IL, NJ, NM, NY, OR, UT, and WA. States were selected based on whether they had implemented insurance coverage of over-the-counter contraception without a prescription or expanded the scope of pharmacist practice.
Join us tomorrow, September 15th, at 12:30pm ET for a discussion of insurance coverage of over-the-counter birth control pills, which will include a presentation of the discoveries in this report.
Also, learn more about over-the-counter contraceptive pills in the brief Over-the-Counter Oral Contraceptive Pills, an overview of over-the-counter oral contraceptives and laws and policies related to insurance coverage.
In July 2023, the U.S. Food and Drug Administration (FDA) approved the first over-the-counter (OTC) daily oral contraceptive pill, Opill. Despite years of OTC access to contraception such as Plan B and condoms, there has been little research on how private insurance plans or Medicaid programs cover non-prescribed OTC contraception and whether they do so without cost-sharing. Currently, federal law requires most private health insurance plans and Medicaid expansion programs to cover, without cost-sharing, the full range of FDA-approved contraceptive methods. Health plans usually require a prescription to indicate medical necessity and trigger coverage, including for methods that do not require a prescription to purchase. Traditional Medicaid programs are required to cover family planning services without cost-sharing, though states have flexibility in which contraceptive methods they cover.
Earlier this year, the Biden administration issued an executive order directing the U.S. Departments of Labor, Health and Human Services, and Treasury to consider new actions to improve access to affordable contraception, which includes promoting increased access to and coverage of OTC contraception at no costs to consumers. Currently, the guidance from these three agencies “encourages” private plans to cover OTC contraceptives without cost-sharing but does not require it.
Six states, however, have passed laws requiring state-regulated health plans to cover, without cost-sharing, certain OTC contraception without a prescription and seven states use state-only funds to provide this coverage for Medicaid enrollees. Twenty-seven states and D.C. have expanded pharmacist prescribing of at least some contraceptive methods, which could facilitate coverage of OTC methods but few pharmacists have training or time, and those that do, are not compensated for counseling patients.
This report is based on 35 structured interviews conducted from January to August 2023, with nearly 80 experts and key players such as pharmacists, health plans, and state Medicaid officials involved in the coverage and provision of OTC contraception in seven states with one or more of these coverage approaches (IL, NJ, NM, NY, OR, UT, and WA). It discusses the challenges and opportunities identified by the interviewees that they have experienced regarding coverage under private health insurance and Medicaid and reviews potential options for operationalizing insurance coverage of non-prescribed OTC contraception such as Opill. These experiences are also informed by recent policies that required plans to pay for OTC COVID tests and more recently by interest in expanding access to Narcan, now available without a prescription.
With the imminent availability of Opill and the possibility of a new OTC oral contraceptive pill in the near future, the issue of coverage has been raised by many stakeholders. While some states have moved forward with coverage requirements for OTC contraceptives, operational issues and concerns such as pharmacy and pharmacists’ capacity to submit claims for OTC products, a lack of uniformity and oversight of health plans’ billing protocols, and low awareness of these policies remain as implementation challenges. While required coverage of OTC contraception without a prescription and without patient cost-sharing would increase access, it could also create a precedent for coverage of other OTC treatments, raising issues of cost for insurers and state Medicaid programs.
Key Takeaways
Across the spectrum of stakeholders interviewed, there is interest and engagement about the potential of an over-the-counter (OTC) contraceptive pill to broaden access to contraceptive options, but many raised concerns about challenges related to affordability, implementation, and coverage options based on experiences in several states.
In states where OTC methods are currently covered without a prescription by Medicaid or private plans, consumers generally need to obtain OTC contraception at the pharmacy counter, where they can show evidence of coverage and get their pharmacy claim processed. In some private health plans, consumers can pay for OTC contraception up front and then seek reimbursement from the plan, but that could be financially and administratively burdensome for consumers and is rarely used.
Interviewees indicated that there has been little specific outreach about this covered benefit to pharmacies in states where OTC contraception, such as emergency contraception and condoms, is covered without a prescription in private insurance or for Medicaid enrollees. Health plan interviewees reported that they receive few claims for non-prescribed OTC contraception, which could be due to low awareness of the benefit and how to bill for it. Few plans provide information about the benefit in their enrollee-facing information.
State Medicaid programs need to submit a State Plan Amendment (SPA) to the Centers for Medicare & Medicaid Services (CMS) to cover OTC drugs and products. After obtaining this authorization, states can determine which OTC drugs and products their Medicaid programs will cover. However, federal Medicaid law requires a prescription to cover all drugs, even those that are available without a prescription. A few states have chosen to use their own funds, without federal matching dollars, to pay for OTC contraceptives for Medicaid enrollees without a prescription. Federal funds will remain unavailable to cover OTC drugs without a prescription unless Congress amends the federal Medicaid law.
In states where coverage for OTC contraception is provided without a prescription, interviewees noted that billing protocols for OTC contraception vary widely by health insurance plan and even within state Medicaid programs, leading to confusion for some pharmacists. States/state agencies do not usually determine the billing mechanism to be used.
Some interviewees raised the importance of addressing quantity limits for OTC contraception. Interviewed health plans and a national PBM suggested that quantity limits have the potential to control fraud, waste, and abuse, which they cited as leading to higher costs for insurers.
There has been limited communication about billing for non-prescribed OTC contraception between pharmacies, PBMs, health plans, and state insurance departments. Many interviewees from these sectors expressed that the mechanics of these state laws and how to operationalize them are unclear.
While several interviewees expressed confidence that their current billing process for other non-prescribed OTC contraception can easily accommodate, most state-level discussions on insurance coverage of this product are in the preliminary stages.
In some states, pharmacist prescribing plays an integral intermediary role in access to contraception where a prescription is required for coverage by removing the need to obtain a prescription from a physician or other prescriber. However, challenges and shortcomings with this approach persist, such as pharmacist time constraints, training requirements, and low or no payment from health plans for pharmacists’ services.
When interviewees were asked what general suggestions they had for how to best implement coverage for Opill without a prescription, many stressed the importance of having a standardized billing process to help facilitate the transition to covering OTC contraception such as without a prescription as well as the role of clearer federal guidance regarding what plans are required to cover.
While state actions to increase access to non-prescribed OTC contraception without cost-sharing can be meaningful for people with private insurance, the reach of these actions is limited, in large part because the majority of those with private health insurance are enrolled in self-funded employer plans, which are not subject to state insurance requirements.
The extent to which OTC contraceptive pills can broaden the availability of effective contraceptives to those who seek them will depend on many factors including state and federal policies, pharmacy engagement, pharmacy stocking and signage, religious refusals, affordability, and insurance coverage, as well as public awareness and education.
This work was supported by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Report
This report is based on 35 structured interviews conducted from January to August 2023, with nearly 80 experts and key players such as pharmacists, health plans, and state Medicaid officials involved in the coverage and provision of OTC contraception in seven states with one or more of these coverage approaches (IL, NJ, NM, NY, OR, UT, and WA). It discusses the challenges and opportunities identified by the interviewees that they have experienced regarding coverage under private health insurance and Medicaid and reviews potential options for operationalizing insurance coverage of non-prescribed OTC contraception such as Opill. These experiences are also informed by recent policies that required plans to pay for OTC COVID tests and more recently by interest in expanding access to Narcan, now available without a prescription:
Oral contraceptives are the most commonly used method of reversible contraception in the U.S. Oral contraceptive pills were first approved for prescription use by the U.S. Food and Drug Administration (FDA) in 1960. In July 2023, the FDA approved Opill, the first daily oral contraceptive pill available over-the-counter (OTC) without a clinician or provider’s prescription. It is expected to be available in early 2024.
OTC status is an FDA designation meaning that a drug or product is available without needing a prescription from a health care provider. The ability to access oral contraceptives without a prescription from a clinician can save time spent on travel, at a clinician’s office, and off work or school. Studies suggest that OTC access to oral contraceptives would increase the use of contraception, facilitate continuity of use, and reduce the risk of unintended pregnancy.
Most drugs available OTC today were initially labeled and approved as prescription-only medications. Other commonly known OTC drugs that were previously only available with a prescription include levonorgestrel emergency contraceptive pills; smoking cessation aids such as Nicorette; several brands of allergy medications such as Claritin D, Allegra, and Zyrtec; heartburn medication such as Prilosec; and Narcan nasal spray, the most recent product to switch from prescription to OTC status before Opill, which is used to treat opioid overdoses.
Levonorgestrel emergency contraceptive (EC) pills, marketed as Plan BOne-Step and other brands, are a form of backup birth control intended to be taken within three days after unprotected sex or contraceptive failure to prevent pregnancy. They were the first contraceptive pills to have switched from prescription to OTC status, in 2006. While EC pills were originally FDA-approved for OTC use by people ages 17 and older, the FDA removed the point-of-sale age requirement in 2014. Unlike daily oral contraceptives, EC pills are not intended for daily use.
Other contraceptive products that are available over the counter without a prescription include external condoms, spermicides, and contraceptive sponges. These non-hormonal contraceptive methods are less effective than oral contraception at preventing pregnancy. The FDA’s approval of Opill will make it the most effective method of contraception available over the counter intended for regular use.
FDA Prescription-to-OTC Switch Process
The FDA requires applicants to conduct extensive testing, often over several years, of products and labeling before they can be approved for OTC use. Opill’s application was approved through the “RX-to-OTC switch” pathway, which is available for drugs that have already been approved by the FDA, like Opill, by submitting a New Drug Application (NDA). Medications may be eligible for OTC status if the FDA determines that they can be used appropriately by consumers for self-diagnosed conditions; they do not require a clinician for safe and effective use; and they have a low potential for misuse and abuse. Applicants typically must conduct studies to assess whether consumers are able to comprehend the product’s labeling and use the product safely and appropriately without the supervision of a clinician.
Opill, a daily progestin-only oral contraceptive, was initially approved for prescription use by the FDA in 1973 (manufactured by Pfizer under the brand name Ovrette). HRA Pharma acquired the rights to Opill in 2015 and began the research process required to apply to the FDA for an Rx-to-OTC switch, including label comprehension studies and self-selection actual use trials. HRA Pharma, subsequently acquired by Perrigo in April 2022, submitted its application to move Opill over the counter in July 2022.
In addition to review by the FDA itself, the process often also entails review by independent advisory committees comprised of scientific experts and consumer representatives. In May 2023, after reviewing evidence and hearing public testimony, FDA advisory committees unanimously voted in favor of the FDA moving Opill over the counter. Although the FDA is not required to follow advisory committees’ recommendations, they typically do. The FDA approved Opill for OTC use on July 13, 2023, without age restrictions, and the manufacturer reports that it will be available in stores and online in early 2024. Consumers will be able to purchase a pack of one, two, three, or six months’ worth of pills, depending on availability.
Although it is farther behind in the process, another pharmaceutical company, Cadence, is working toward FDA approval of an OTC version of its combined (progestin and estrogen) oral contraceptive pill, Zena. Cadence is reported to be considering a different FDA pathway to OTC status that has been proposed by the Biden administration.
Federal and State Laws on Coverage of OTC Contraception
MEDICAID
Medicaid is the joint federal/state health insurance program for people with low incomes. Federal law requires state Medicaid programs to cover family planning services and supplies without cost-sharing, but they are not required to cover OTC products (with a few exceptions) or to cover OTC contraception without a prescription. States cannot obtain federal matching dollars for covering a medication without a prescription, but they may opt to use state-only funds to cover OTC drug benefits without a prescription.
Seven states (CA (effective in 2024), IL, MD, MI, NJ, NY, and WA) cover, with state funds, at least some OTC contraceptive methods without a prescription for Medicaid enrollees. Note that New Jersey Medicaid’s coverage of non-prescribed OTC contraception applies to fee-for-service (FFS) enrollees only, which represent 2% of enrollees in the state. With the exception of California, coverage is specific to emergency contraception or condoms in these states, so these programs may not include Opill without a change in policy. (See Over-the-Counter Oral Contraceptive Pills for the coverage details of these and other state Medicaid programs.)
PRIVATE INSURANCE
The Affordable Care Act (ACA) requires most private health plans (individual, small group, and large group) to cover recommended preventive services without cost-sharing. The ACA tasks the Health Resources and Services Administration (HRSA) with recommending coverage requirements for a range of preventive services for women, which initially consisted of eight recommendations that included contraceptive services and supplies, identified by a committee of the Institute of Medicine in 2011. The initial HRSA 2011 recommendation included the language “as prescribed” in reference to the coverage requirement for contraception. Today, the Women’s Preventive Services Initiative (WPSI) is the expert body currently commissioned by HRSA to issue and update preventive clinical recommendations for women. WPSI updated its contraceptive coverage recommendation in 2021 and it does not include a prescription requirement for coverage of contraception. HRSA dropped the prescription requirement in its language when the preventive services guidelines were updated and posted. Currently, “as prescribed” is only referenced in the U.S. Departments of Labor, HHS, and Treasury (“tri-agency”) federal FAQs.
In addition to the federal ACA requirements, six states (CA (effective in 2024), MD, NJ, NM, NY, and WA) have laws or regulations requiring state-regulated private health insurance plans (individual and fully-insured employer-sponsored plans) to cover, without cost-sharing, OTC contraception without a prescription. Nationally, 65% of workers with employer-sponsored insurance are enrolled in a self-funded plan; therefore, the majority of people with employer-sponsored insurance who live in states that require coverage of OTC contraception without a prescription are not guaranteed this coverage. While the language of New York’s law is specific to emergency contraception, the other state laws apply to a broad range of contraception. The language of these laws, with the exception of New York’s, is broad enough to include a daily oral contraceptive pill such as Opill without a change in policy. (See Over-the-Counter Oral Contraceptive Pills for the details of these state laws and others that require coverage without a prescription.)
Illinois and Oregon require private health plans to cover OTC contraception; however, while these laws do not state that a prescription is required in order for it to be covered by insurance, the laws also do not explicitly stipulate that plans must cover them without a prescription. While federal law applies to all private plans, state law applies to only individual plans and fully-insured employer plans.
Pharmacist Prescribing
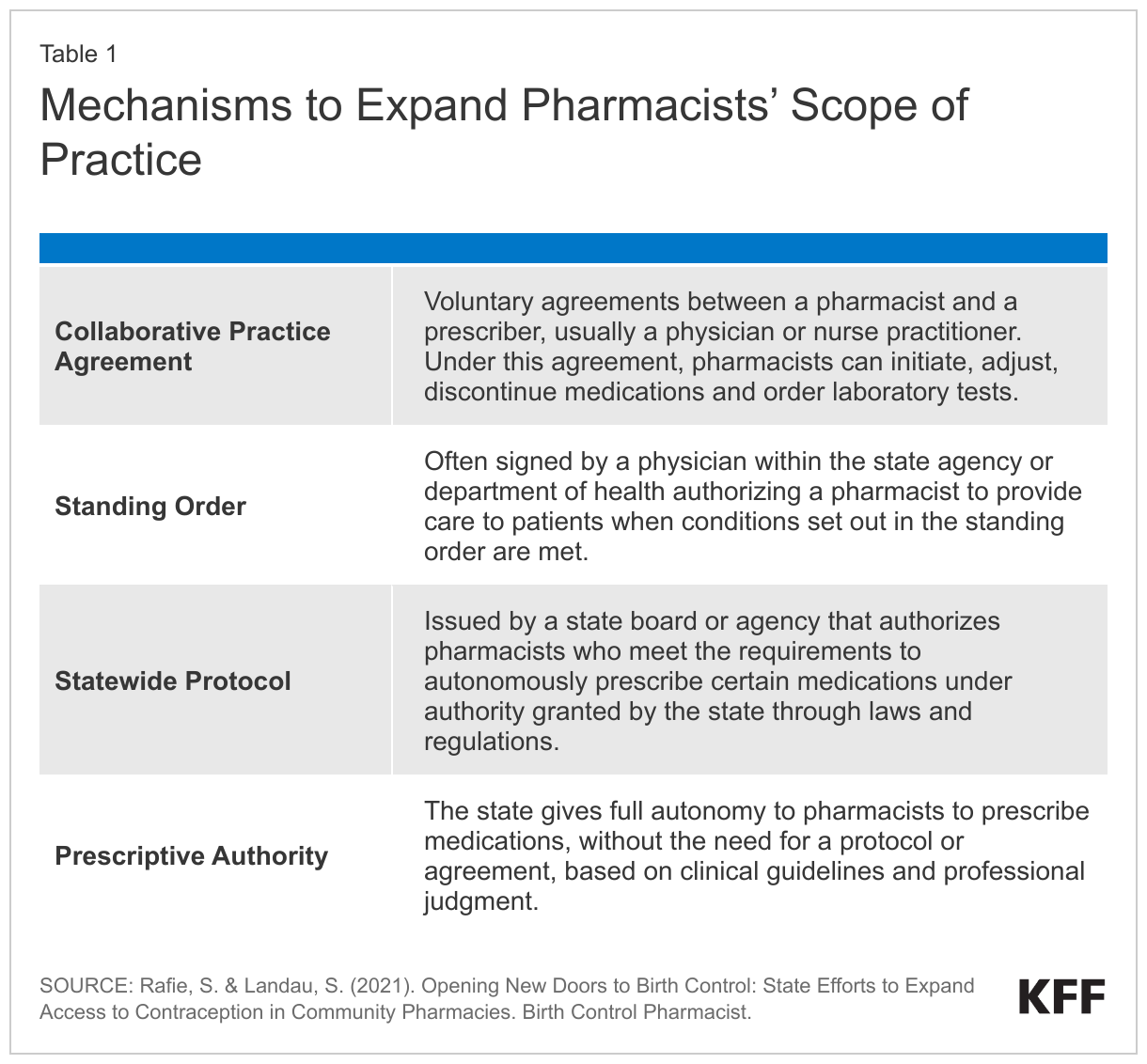
In states where coverage of OTC contraception without a prescription is not possible, not required, or where billing requirements are unclear, pharmacist prescribing is a relatively novel approach that can help expand access and bridge that gap. States, rather than the federal government, establish standards that determine the scope of practice and services that may be provided by different types of licensed health practitioners practicing in that state. Twenty-seven states and D.C., including all seven in this study, have passed laws permitting pharmacists to prescribe certain methods of contraception, including OTC contraception, or to dispense it pursuant to a standing order or collaborative practice agreement (discussed in more detail later in the report). In these states, consumers can obtain a prescription for contraception, including OTC methods, at a participating pharmacy without the need for a visit to a clinic or doctor’s office. Expanded scope of practice can help facilitate private insurance and Medicaid coverage of these products and research demonstrates that it can increaseaccess to contraception and help prevent unintended pregnancies.
However, many states do not have laws that permit pharmacist prescribing, and in the states that do, there are many limitations with pharmacy prescribing, including low pharmacy and pharmacist take-up, pharmacist training requirements, and patient counseling and evaluation requirements, which are typically provided without payment from health plans. Although the FDA did not place an age restriction on access to Opill, some states place age restrictions on pharmacists prescribing contraception to people under the age of 18. Additionally, a consumer who wants pharmacist-prescribed contraception is not able to do so outside of pharmacy hours or when the pharmacist is unavailable to provide this service. Because pharmacist prescribing is still a clinical model and patients in most states must disclose personal health data during the consultation, this approach may present barriers for people who do not wish to interact with the health care system.
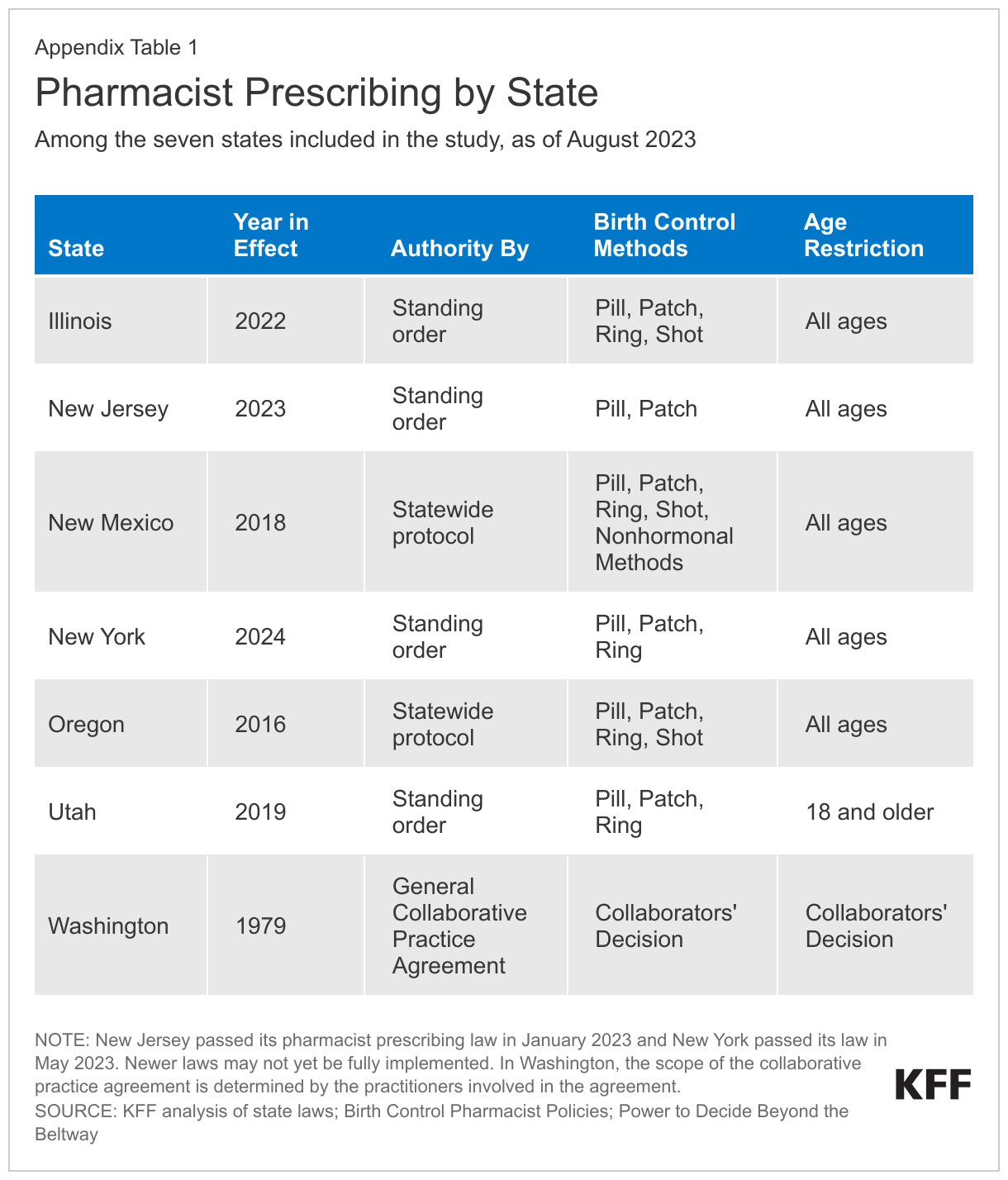
To identify experiences and approaches for plans to cover OTC contraceptives, key players in states that require or allow for private insurance or Medicaid coverage of OTC contraception without a prescription, including some that allow pharmacists to prescribe contraception, were interviewed. After identifying states that implemented at least one of these insurance coverage or pharmacist prescribing policies, while also factoring in interviewing logistics, seven states were included in the project: Illinois, New Jersey, New Mexico, New York, Oregon, Utah, and Washington.
From January 2023 through August 2023, KFF staff completed 35 interviews with nearly 80 experts from state Medicaid programs, the Centers for Medicare and Medicaid Services (CMS), state insurance departments, private health insurance plans, Medicaid managed care organizations (MCOs), chain pharmacies, independent pharmacies, a pharmacy benefit manager (PBM), and trade associations, as well as pharmacists and contraceptive access advocates.
The information collected from the interviews highlights state policies and strategies that have been used to operationalize Medicaid and private insurance coverage of OTC contraception such as Opill, as well as identifies the approaches and challenges to help inform state and federal efforts to address coverage for Opill. To preserve interviewees’ confidentiality, individual names, affiliations, and states are not provided. (See the Methods section for more details.)
State-Funded Coverage of OTC Contraceptives Without a Prescription for Medicaid Enrollees
The specifics of coverage of family planning services and supplies vary across Medicaid programs. Four of the seven states that participated in the study confirmed they pay for non-prescribed OTC contraception for Medicaid enrollees (IL, NJ, NY, and WA). (As mentioned above, New Jersey’s coverage applies only to FFS enrollees.) Because federal Medicaid law requires a prescription to trigger coverage of drugs and products, these coverage policies are entirely state-funded. New Jersey and New York only cover non-prescribed OTC emergency contraceptive pills while Illinois and Washington cover non-prescribed OTC emergency contraceptive pills and other OTC contraceptives such as condoms.
In states that cover non-prescribed OTC contraception for Medicaid enrollees using state-only funds, there are generally two mechanisms pharmacists use to bill for them and get reimbursed from the state.
Universal National Provider Identifier (NPI) number:NPIs are unique, 10-digit numbers issued by CMS that identify individual providers or health care entities, such as pharmacies, which are used for billing purposes. Across the Medicaid programs that cover non-prescribed OTC contraception using state funds, this is the most common mechanism pharmacists use to submit a claim without enrollee cost-sharing. According to interviewees, this process involves the pharmacist entering a dummy, blank, or state-specific universal NPI in the prescriber field. It is used by three state Medicaid programs and some MCOs in the study.
Pharmacy NPI: In this process, the pharmacist enters the pharmacy’s NPI in the prescriber field. It is used by one state Medicaid program and several Medicaid MCOs, and it was formerly used by one state Medicaid program that used to cover non-prescribed OTC emergency contraception but no longer does.
While each of the four state Medicaid programs published billing guidance and/or resources on the coverage benefit, pharmacist and consumer awareness of the benefit is generally low. Pharmacist training and billing guidance vary across states. Some state Medicaid programs are unaware of any issues with their billing mechanism for non-prescribed OTC emergency contraception, but others have cited that some pharmacists are unaware or unsure of the billing process for contraception despite billing guidance provided through pharmacy handbooks, newsletters, and email or fax blasts. As one pharmacist pointed out, part of the confusion stems from the fact that they are dealing with many plans and there is no standardized method of communicating this information or a single source for a pharmacist to find this information.
“The consumer will attempt to obtain [OTC] contraception at a pharmacy, and the pharmacist turns them away because they’re unable. They either think that they cannot dispense it without a prescription, or they feel Medicaid requires a prescription [for coverage]. Some of them just don’t know how to do it.”
–State Medicaid official
Billing mechanisms can also differ between traditional FFS Medicaid and MCOs. For example, in one state Medicaid program, pharmacists billing for non-prescribed OTC contraception are instructed to use a dummy NPI number in the prescriber field for their FFS program, the pharmacy’s NPI for one MCO, and dummy NPIs for other MCOs. These different billing mechanisms can lead to pharmacist confusion and additional administrative burdens.
Most state Medicaid programs studied indicated they have not recently reviewed claims data for non-prescribed OTC contraception or do not know how often claims are submitted for it. State Medicaid programs do not directly advertise the benefits to beneficiaries outside of the member handbook. Several pharmacists corroborated that awareness of this benefit among pharmacists and consumers is low.
One of the three states that does not currently cover OTC contraceptives for Medicaid enrollees discontinued funding for non-prescribed contraception in 2016. The program was reportedly discontinued due to lack of utilization, and one pharmacy owner mentioned the process was tedious for both pharmacists and patients. The program was administered through the state health department and was paid for using state funds and involved pharmacists billing Medicaid using the pharmacy’s NPI. State Medicaid officials have not discussed restarting the program.
In general, Medicaid fee-for-service enrollees cannot file a claim if they did not obtain point-of-sale coverage for non-prescribed OTC emergency contraception. However, an FQHC-based Medicaid MCO in one state that covers non-prescribed OTC contraception reported that enrollees can purchase the OTC contraceptive out-of-pocket and then submit a receipt to the MCO for reimbursement.
Private Insurance Coverage of OTC Contraceptives Without a Prescription
The project included four of the states that currently require state-regulated private health insurance plans to cover at least some methods of OTC contraception without a prescription (NJ, NM, NY, and WA). Oregon and Illinois, also included in the study, have laws requiring coverage of OTC contraception, but coverage without a prescription is not explicit and interpretation of the laws varies. Nonetheless, some health plans in these states do cover OTC contraception without a prescription.
In states where private insurers are required to cover OTC contraception without a prescription, there are generally two pathways for consumers to receive coverage.
Obtaining the OTC contraceptive product at the pharmacy counter: The private plans interviewed said that consumers can bring their OTC products to the pharmacy counter and the pharmacist would then submit a claim to the plan using their own national provider identifier (NPI) number, pharmacy NPI number, or dummy NPI depending on the plan and state protocol. Enrollees usually must purchase it from an in-network pharmacy in order for it to be covered. This approach is similar to how pharmacists billed for at-home COVID-19 tests in many situations.
Purchasing the OTC contraceptive product at the cashier outside of the pharmacy and getting reimbursed: One private plan mentioned that consumers can also purchase the product outside of a pharmacy setting and then submit a claim with the receipt to their insurance company for reimbursement, similar to the reimbursement mechanism that was used for some at-home COVID-19 tests. While this option generally expands access to coverage in certain situations, such as when a pharmacy inside a store is closed, it could pose financial and logistical barriers by requiring enrollees to pay the cost upfront and navigate the plan’s reimbursement process, which may require the enrollees to include a prescription number.
Some health plans voluntarily provide coverage for OTC contraceptives without a prescription in states that do not mandate coverage. The state insurance department for one state without an OTC contraceptive coverage requirement noted there are a few private health plans that voluntarily cover non-prescribed OTC contraception. Corroborating this notion, one private health insurance carrier that operates in a state where coverage of non-prescribed OTC contraceptives is required also voluntarily extends the same coverage in the three other states where the carrier operates, which do not have this requirement, as long as the drug or product is included on the drug formulary. A formulary is the list of drugs covered by a specific health insurance plan. If a drug is not listed on a plan’s formulary, it is likely not covered by the plan and the enrollee would need to pay out-of-pocket for it.
Despite state coverage requirements, the health plans in the study indicated that claims for non-prescribed OTC contraception are rare, suggesting a lack of awareness of this covered benefit among pharmacists and health plan enrollees. Indeed, two independent pharmacy owners in a state with this coverage requirement indicated that they were unaware of or unfamiliar with this private insurance policy. Representatives from another state’s insurance department stated that it is the health plans’ responsibility to inform their members of any new benefits to which they are entitled. Some state insurance departments indicated that health plans are required to notify their enrollees that this coverage is available or include the information in their membership materials, though the details of how and where that information is communicated is largely up to the plan.
Some contraceptive access advocates cited concerns that raising consumer awareness and expectations about this covered benefit without better operational structures could generate confusion among enrollees with employer-sponsored insurance. Coverage requirements for OTC contraception only apply to state-regulated private health plans (individual and fully-insured employer-sponsored plans). However, the majority of covered workers are enrolled in self-funded plans, to which state coverage requirements do not apply. Two national advocates, who also work with state-level advocates, noted that broadly promoting coverage awareness can misguide and mislead many consumers who are in self-funded plans into thinking they are guaranteed this coverage because self-funded and fully-insured plans typically look the same to the enrollee so they may not know they are in a self-funded plan. Some states, such as Colorado, Maryland, and New Jersey, require insurance cards to indicate whether the plan is regulated by the state, but most states do not.
Even with state laws requiring coverage, insurance commissioners have not issued guidance on how private health plans should process claims for non-prescribed OTC contraception. Representatives from one state’s department of insurance confirmed that billing mechanisms for OTC contraceptives vary across health plans, with some plans having their pharmacy networks set up to detect the products as zero cost-sharing and others requiring enrollees to submit claims to the insurer for reimbursement. The various ways of billing private insurance can consequently lead to pharmacist confusion.
“Working in the community setting, we are incredibly busy. Having to look up a separate way to do the same thing takes a lot of time.”
– Pharmacist from a regional retail pharmacy chain
State compliance and enforcement efforts vary. One state department of insurance addresses compliance on a case-by-case basis, primarily relying on complaints from consumers or providers to trigger a compliance review. This state insurance department noted that while there was some confusion among insurers about the mechanics of the coverage law when it took effect, they have received very few complaints. Another state insurance department takes a different approach to ensuring compliance with state coverage laws by conducting systematic reviews periodically, in addition to addressing individual complaints they receive from consumers and providers, which they note are rare. However, a pharmacist and a representative from a pharmacy chain noted that even with state mandates, getting payers to operationalize coverage is difficult.
“Even though we’ll have a bill that says it’s supposed to be covered, the plans don’t necessarily start covering it. We’ve seen that with the extended supply [of hormonal contraception].”
– Clinical pharmacist and national pharmacist educator
Pharmacy Benefit Managers
Pharmacy benefit managers (PBMs) are third-party administrators contracted by health plans that perform a variety of financial and clinical services for both private insurance plans and Medicaid programs, including negotiating discounts on medications for health plans and employers, establishing prescription drug formularies, and adjudicating pharmacy claims. PBMs play a role in the provision of OTC contraception by determining what tier of a drug formulary it is placed on, which impacts enrollee cost-sharing amounts; determining pharmacy reimbursement amounts, which impacts the willingness of a pharmacy to sell a particular drug or product; processing enrollee claims; and conducting pharmacy oversight of claims to ensure proper billing techniques.
Billing for OTC contraceptives varies across PBMs. PBMs help establish standard formulary processes while ensuring the insurers and pharmacies they contract with abide by state and federal policies. One national PBM interviewee noted that coverage for OTC drugs typically requires a prescription in order for the claim to adjudicate through their pharmacy system. In states with laws that require private insurers to cover non-prescribed OTC contraceptives, a health plan interviewee explained that their members need to mail in receipts to be reimbursed for the out-of-pocket purchase. However, as other interviewees shared, there have been few claims for these non-prescribed OTC contraceptives.
Both payers/PBMs and pharmacies experience challenges with claims submission due to historical systems and processes that were not built for widespread coverage of non-prescription products. For example, one health plan explained that most chain pharmacy systems require an NPI to submit a claim and that most payer claim systems also require an NPI to adjudicate the claim. While the payer could in theory opt not to require an NPI, the pharmacy system would still require it. As a result of these collective limitations, workarounds at the pharmacy and health plan level may be necessary when billing for non-prescribed OTC contraception, creating additional burden on community pharmacy staff.
Some pharmacists are concerned that billing health plans for non-prescribed OTC contraceptives may trigger an audit from PBMs. Some pharmacists said they worry about being audited by PBMs, as these billing mechanisms appear to contradict the training they have received about billing thoroughly and carefully to avoid auditing. One pharmacy chain representative shared this concern as well since failed audits can result in penalties and loss of compensation for pharmacies. However, representatives from a private health insurance plan and a Medicaid managed care organization stated that their PBM excluded OTC categories from being auditable.
Some pharmacists also reported being concerned about potential legal liability for billing without a prescription. When a pharmacist uses their NPI, the pharmacy’s NPI, or a dummy NPI to bill for an OTC drug, it can give the impression that a prescription has been written for it. Some pharmacists in these states raised concerns about potential legal liability in the event that a patient claims a pharmacist made a mistake because no prescription was actually written.
Clear communication between PBMs, health plans, and pharmacies can help facilitate coverage for OTC contraceptives. The health plan above noted that their PBM notified network pharmacies that coverage for OTC contraceptives is a new capability that pharmacies in the state must comply with. The PBM also sent out billing guidance on how to bill for OTC contraceptives. Clear communication can help reduce confusion about different billing mechanisms and alleviate concerns about being audited.
The Role of Pharmacist Prescribing
Four (NM, OR, UT, and WA) of the seven states in the study currently permit pharmacists to prescribe contraception; two states (IL and NJ) recently passed pharmacist prescribing laws and are still in the process of implementing them; and one state (NY) passed a pharmacist prescribing law in May 2023 that will take effect at the end of 2024. (See Appendix Table 1 for details on each state’s law.)
Pharmacist prescribing plays a key role in coverage of contraception without cost-sharing in some states. Many interviewees stated that pharmacist prescriptive authority helps expand access to reproductive health care. Prescribing authority varies by state and is typically issued through a standing order, collaborative practice agreement, statewide protocol, or full prescriptive authority (Table 1). Where this is an option, pharmacist prescribing helps reduce barriers to accessing contraception by removing the need to visit a clinician to obtain a prescription, and for people without insurance, it can be less expensive than getting a prescription from a clinician.
Uptake of prescriptive authority has been low among pharmacists in some states, in part because of the training requirements. In many states, including one in the study, pharmacists graduating from the state university’s pharmacy school earn prescriptive authority upon graduation. However, prescriptive authority for hormonal contraception usually involves continuing education which takes time and resources outside the standard responsibilities of a pharmacist. An executive pharmacy director for a Medicaid managed care organization stated that even though their state allows pharmacists to prescribe hormonal contraceptives via a standing order, it is uncommon for pharmacists to use this option.
While pharmacist prescribing can promote access to contraception, shortcomings of this approach may persist for several reasons. The most commonly cited reasons include:
Lack of or limited compensation for consultation is a barrier to participation in pharmacist prescribing. Most pharmacists and independent community pharmacy leadership mentioned that pharmacists in their state are not incentivized to prescribe or dispense hormonal contraception due to the lack of payment from health plans for the service. Several pharmacy interviewees cited challenges getting private insurance to compensate pharmacists for this service. This challenge is in part due to the fact that insurance companies typically do not recognize pharmacists as providers and adhere to credentialing and enrollment processes that are typically reserved for traditional health care providers vs. pharmacists. While pharmacies are reimbursed for the cost of the drug, pharmacist services for patient counseling and evaluation, prescribing, and other administrative services associated with providing this service are often not compensated by payers or are paid at a low rate. Representatives from a pharmacy chain said that when pharmacy services are paid, whether the payment goes to the pharmacy or to the pharmacist depends on the arrangement pharmacists have with their employer. One pharmacist noted that payment typically goes to the pharmacy rather than to the pharmacist. Lack of or low compensation can sometimes lead pharmacies to charge patients consultation fees in lieu of payer compensation, which is at odds with the goal of the ACA and Medicaid to eliminate financial barriers to contraceptive services for patients. One pharmacy interviewee reported that they do not prescribe many OTC products for this reason:
“Economically, it doesn’t work out because [patients are] paying $80 [in consultation fees] to get a product that they would pay $50 for [without insurance coverage].”
–Independent pharmacy owner
Lack of prescriptive authority where it is permitted: As mentioned above, it may be difficult to locate pharmacies with at least one prescribing pharmacist, even in states with many prescribing pharmacists. One interviewee said their data showed pharmacist prescribing is more prevalent in urban areas than rural areas. Since prescriptive ability is optional to most pharmacists, consumers may encounter inconsistent availability of pharmacists willing or able to prescribe hormonal contraception. This gap is particularly prevalent in rural areas that already face declining access to pharmacies. However, other studies suggest that pharmacists in rural communities are just as likely to prescribe contraceptives as those in urban communities.
Lack of time: The role and scope of pharmacists in health care has rapidly expanded over the years, with a growing number of pharmacists dispensing medication, administering vaccines, and counseling patients, among other services. Several interviewees expressed that prescribing contraceptives and adjudicating coverage for OTC contraceptives adds another layer of responsibility for pharmacists who are already overstretched. The process often involves a pharmacist consultation, drug utilization review, blood pressure check, and patient education, all of which take time to complete and can interrupt workflow. For these reasons, even if there are pharmacists who can prescribe at a pharmacy, patients may have to wait to obtain a prescription for contraception. Additionally, pharmacists are generally required to enroll as a Medicaid provider in order for Medicaid to compensate for their services, which can be a burdensome process depending on the state.
When asked what suggestions they would have for other states considering implementing pharmacist prescribing, some pharmacy interviewees noted the importance of having input from pharmacies and pharmacists when developing and implementing legislation and regulations.
Considerations for Covering OTC Oral Contraceptive Pills
Discussions about coverage of an OTC daily oral contraceptive pill without a prescription have barely begun at the state level. The FDA approved the daily oral contraceptive pill, Opill, for OTC use at the end of the interview fielding period. Interviewees were asked what steps, if any, they have taken in anticipation of or in reaction to FDA approval of an OTC daily oral contraceptive pill, including agency, health plan, or pharmacy discussions, or any concrete plans. For the most part, these discussions have not yet begun or are in their very early phases. Among those that have begun planning, several interviewees expressed confidence that their current system for billing for other OTC contraception such as Plan B without a prescription is a feasible way to bill for an OTC daily oral contraceptive and that they do not believe any additional steps would need to be taken to change billing and claims systems. Private health insurance plans and a state insurance department interviewed indicated that while there have been some discussions about coverage for an OTC oral contraceptive without a prescription, they have not yet taken any concrete actions. Interviewees, including a state department of insurance, mentioned the importance of involving health care providers with clinical expertise, especially pharmacists, in efforts to expand coverage. Since their interview, one state reported it has begun a provider outreach campaign to understand barriers at the pharmacy level, particularly those in smaller towns, rural areas, and tribal communities, and is developing a communications campaign to help ensure any barriers to OTC uptake are addressed by the time Opill comes to market.
The importance of clear federal guidance about any plan coverage requirements for OTC contraception was cited by many interviewees when asked for suggestions on how to best implement coverage approaches without a prescription. One interviewee from a state insurance department noted that their state relies heavily on federal action for implementing changes for new drug coverage. Representatives for a national PBM echoed that federal guidance would be helpful, and another representative for a national health plan trade group emphasized that communication related to coverage policies from the federal government needs to be clear and cannot be confusing for patients, providers, and plans. One pharmacy interviewee commented that direction from the federal government on coverage without a prescription is mutually beneficial all around. Contraceptive access advocates noted that lack of consistency in the language between what the ACA regulations require plans to cover and the tri-agency FAQs has led to differing interpretations of policy and lack of clarity on what can be enforced.
One pharmacy chain indicated that it is currently working with the U.S. Department of Health and Human Services (HHS) to try to create a payment pathway at the federal level for pharmacist prescribing, a fallback approach to coverage where coverage without a prescription is not an option.
“Anything that’s dictated nationally versus state-by-state is always a win for the patient, and quite frankly, it’s always a win for the pharmacy.”
–Representative from a pharmacy chain
CMS has begun preparations to accommodate coverage of OTC contraception in Medicaid, but some form of a prescription is still required to obtain federal matching funds. CMS, the federal agency that administers Medicaid in partnership with state governments/Medicaid agencies, has issued guidance on how states can leverage expanded scope of pharmacist practice to cover OTC medications such as contraception. They suggest using broad and general language in their state plan regarding Medicaid coverage of OTC drugs. States submit state plan amendments (SPAs) to CMS when they plan to make changes in how they administer Medicaid program activities and are seeking federal approval to draw down federal funds or federal matching dollars for those services.
In response to the FDA approval of OTC Narcan nasal spray in March 2023, and in anticipation of the FDA approving a daily OTC oral contraceptive, CMS has encouraged state Medicaid programs to use broad implementation language in their state plan and list which therapeutic categories are covered on their state website or other public-facing documents to prevent the need for states to submit a new SPA each time their state wishes to cover an OTC drug. For example, CMS approved SPAs from Delaware, Montana, Florida, and Illinois indicating their intent to broadly cover OTC drugs. The billing mechanisms for covering these OTC products vary by state and still require the NPI field to be filled out. CMS leaders believe that this method can be leveraged by any state because even prior to Narcan’s OTC approval, all states had a protocol in place to allow pharmacists to dispense at least some drugs, for example, through a state health official’s standing order. Some state Medicaid programs also used this approach to cover at-home COVID-19 tests.
This approach is different than state Medicaid programs using state-only funds to cover OTC contraception without a clinician’s prescription. States only receive federal matching funds for OTC contraception if it is prescribed by an authorized prescriber.
Nearly all pharmacy interviewees recommended that states considering coverage for OTC contraception should include a billing structure that adequately compensates pharmacists for their services since pharmacies are not typically paid for submitting claims for non-prescribed products. A national PBM indicated that it is currently considering potential billing mechanisms for Opill and has begun partnering with its clients and pharmacies to effectuate this coverage. This PBM and a national PBM trade association also stressed that modernizing the pharmacy claims process and having a standardized billing process in place would facilitate the transition to covering OTC contraception such as Opill without a prescription.
Submitting Pharmacy Claims to Health Plans
There are several steps involved in a pharmacy submitting a claim to a health plan or PBM (see Appendix Table 2). While the processing of a pharmacy claim, from submission by the pharmacy to the return claim arriving back at the pharmacy, occurs, on average, within 3 to 4 seconds, it can take several minutes (or longer if there are problems) for the pharmacist or technician to enter all the billing information. Despite the time and resources expended to submit a claim, pharmacies are not typically paid for providing this service for non-prescribed over-the-counter medications.
Quantity limits are another consideration in coverage for OTC contraception without a prescription.Opill will be sold in packages of one-, two-, three-, and six-month supplies. Having an extended supply of oral contraception is associated with better adherence and lower rates of unintended pregnancy. Several states require plans to cover an extended supply of contraception, such as six or 12 months at a time. However, several interviewees, including some health plans and a national PBM, suggested that prohibitions on quantity limits could contribute to increased waste and costs.
“One of the big learnings we heard from our plans is that there needs to be some guardrails. If there are no quantity limits or other constraints, people could buy bulk male condoms, for example, and then resell them. It actually has happened.”
–Representative from a national health insurance trade association
While interviewees did not report these types of incidents with OTC emergency contraceptive pills, which are a closer parallel to Opill than condoms, this is an issue that at least some interviewees are thinking about in preparation for insurance coverage of Opill. On the other hand, some advocates are concerned that quantity limits can create access barriers for consumers in the event that their pack of pills gets damaged, lost, or left behind.
Stocking decisions and signage can increase opportunities for coverage. Although a few states, such as Washington and Massachusetts, require pharmacies to stock contraceptive medications such as Plan B, pharmacies in most other states will decide whether or not to carry Opill. Stocking also has implications for insurance coverage because most plans provide more coverage for drugs purchased at an in-network pharmacy than at an out-of-network pharmacy, and in some cases such as with health maintenance organizations (HMOs), drugs and services are not covered by out-of-network providers at all.
Pharmacies’ decisions on where to stock OTC contraceptives will also play a role in access, both for those with and without insurance. Some pharmacies decide to put OTC contraceptives behind the pharmacy counter or in a locked cabinet on the shelf due to shoplifting concerns. Some interviewees noted that this type of placement in a pharmacy may make it more difficult to access the contraceptives and that some consumers may have confidentiality concerns, particularly for young people and those living in smaller towns and rural areas. On the other hand, one pharmacist interviewee said that having consumers come to the pharmacy counter to obtain OTC contraception allows the pharmacist to help them understand if the product is the best option for them, understand how to use it, and assess if it is covered by their insurance.
“There is a perception that these medications, Plan B and Opill, are more likely at risk for shoplifting. So even if they do have them out at the OTC area, they could be placed behind the locked cabinet. Think about the barrier, right? We have to go and actually ask somebody to be able to have access to it.”
–Representative from a national pharmacy benefits manager
Posting signage about the availability of OTC contraception and whether it may be covered by insurance could help increase consumer awareness and uptake. An interviewee suggested that some pharmacies may be voluntarily posting signage on the shelf where emergency contraception is stocked to inform customers that if they take the product to the pharmacy counter, the pharmacist may be able to bill insurance for it, rather than the customer having to pay for it entirely out-of-pocket. A pharmacist interviewee noted that posting this type of signage may be more difficult for chain pharmacies because they typically require upper management approval for any content that is posted in their pharmacies.
Pharmacist religious refusals can also impact access to contraception in general. Multiple interviewees in the study cited religious beliefs and refusals as common barriers to accessing hormonal contraceptives through the pharmacy in at least some parts of the state, typically in rural areas and small towns. While some health plans and pharmacies try to find a second prescribing pharmacist at the pharmacy, these refusals and objections have reportedly led to delays in patient access. Even in states where a prescription is not needed for insurance coverage of OTC contraception, a pharmacist may still refuse to process the claim.
Outreach and education to pharmacies, pharmacists, and patients will be critical in fully realizing the potential of an OTC daily oral contraceptive, as discussed by several state Medicaid programs, private health plans, pharmacists, and advocates. The insights gleaned from these interviews suggest that there is a role for a variety of stakeholders including consumer advocates, health plans, state Medicaid programs, PBMs, pharmacies, and pharmacists when it comes to informing consumers of this new product and insurance coverage for it.
“If you keep [Opill] locked up, which I’m imagining will be in some of these retailers, and nobody speaks about it, I don’t know how successful it will be. I hope that they’re going to have a good campaign to help educate everybody about it.”
–Community pharmacist
Contraceptive access advocates expressed that both the availability of OTC contraceptives and having plan coverage of these products can especially benefit communities that have historically faced a myriad of barriers to accessing and affording contraception. They encourage policymakers at the state and federal level to evaluate all possible options for covering OTC contraceptives, with special attention to addressing the concerns facing communities without a pharmacy or people that experience other barriers to access.
“Affordability is an equity issue. We want to make sure [Opill] is not just going to people who have privilege or who could have gotten it through other mechanisms and that it’s really reaching the communities with systemic barriers in place due to inequities in our healthcare system and in our society.”
–Representative from national contraceptive access advocacy group
States have a variety of policy options if they seek to increase access to non-prescribed OTC contraception for individuals with private insurance. More states can continue passing laws requiring state-regulated health insurance plans to cover, without cost-sharing, OTC contraception without a prescription. Using broad language when developing laws and regulations, as some states have already done, can promote coverage of more drugs and products, such as Opill, emergency contraception, and non-hormonal methods such as condoms. Additionally, state laws requiring health plans to cover an extended supply of contraceptives, including those obtained over the counter without a prescription, could reduce burdens associated with having to order or go to the pharmacy every month. While these policies can increase opportunities for OTC contraceptive coverage for those who reside in those states, these policies only apply to those enrolled in state-regulated plans. States do not have the authority to require coverage for specific benefits in self-funded plans, which is the type of plan the majority of individuals with employer-sponsored coverage are enrolled in.
State Medicaid programs that do not currently have a SPA allowing broad coverage of OTC drugs will need to submit a SPA to CMS to cover OTC contraceptives (with a prescription). States that wish to cover Opill without a prescription for Medicaid enrollees may opt to use state-only funds. Most states that currently cover OTC contraception without a prescription for Medicaid enrollees only cover OTC emergency contraception and condoms, so policy changes would be required to permit coverage of a daily oral contraceptive pill such as Opill.
Expanding pharmacists’ scope of practice to permit them to prescribe contraception or enter into a standing order or other statewide protocol to dispense OTC contraception is another approach some states have taken. This approach still involves a prescription, but it can satisfy the prescription requirement to obtain coverage for the product and reduce some of the barriers often associated with having to obtain a prescription from a clinician.
Federal Policy Options
While state actions to increase access to non-prescribed OTC contraception without cost-sharing are meaningful for people who are eligible for that coverage, their reach is limited. The vast majority of states have not taken action to expand insurance coverage of OTC contraception without the need for a prescription. While some additional states may act on their own to develop systems and protocols to facilitate coverage of OTC methods without the need for a prescription, other states do not have the political climate to pass contraceptive coverage requirements in general, including OTC. Additionally, these coverage requirements will only apply to state-regulated health plans. Absent federal guidance or legislation, coverage requirements will continue to vary by state and by plan type.
At the federal level, in 2022, legislation was introduced in the U.S. House and Senate called the Affordability is Access Act that would require private health insurance plans to cover, without cost-sharing, FDA-approved OTC contraception purchased without a prescription. The legislation was re-introduced in 2023, shortly after the FDA advisory committees voted to recommend approval of Opill; however, its passage is unlikely in the current political climate.
Although the ACA requires most private health plans to cover, without cost-sharing, the full range of FDA-approved contraceptive methods, which includes OTC contraception, there is currently no specific requirement or policy that they be covered without a prescription. A prescription requirement is currently mentioned in federal FAQs clarifying ACA coverage requirements, with the most recent one issued by the Biden administration in July 2022. The FAQ references coverage of emergency contraception and states that plans must cover OTC contraceptives when the product is prescribed. It also states that plans are “encouraged to cover OTC emergency contraceptives with no cost-sharing when they are purchased without a prescription.” In June 2023, President Biden issued an executive order directing the U.S. Departments of Labor, Health and Human Services, and Treasury to consider new actions to improve access to affordable OTC contraception, including no-cost coverage. What those actions may look like and when they will occur is not yet known.
New federal guidance clarifying that coverage be provided with or without a prescription and without cost-sharing could have the effect of increasing access to non-prescribed OTC contraception such as Opill to the majority of people with private health insurance. Federal guidance under the preventive services contraceptive coverage requirements would apply to those in self-funded employer plans, as well as individual and other state-regulated plans and standardize OTC coverage for contraceptives across the country.
Medicaid programs, particularly for non-expansion populations, have considerable leeway in determining what benefits, including contraceptive methods, are covered. Although all state Medicaid programs cover outpatient prescription drugs, they are not required to do so. With limited exceptions (e.g., prenatal vitamins and certain tobacco cessation products), they are also not required to cover OTC drugs, but the majority of states do. CMS has indicated it could facilitate coverage of OTC contraception by approving SPAs permitting states to cover OTC drugs and products broadly. However, a prescription for OTC drugs is needed in order for the state to draw down federal matching funds. Congress would need to amend the federal Medicaid statute to require coverage of OTC products without a prescription. Absent that, states could adopt pharmacist prescribing to fulfill the prescription requirement.
Conclusion
As new products come to market through OTC availability, the issues of cost and coverage are raised by payors and consumers alike. In the case of COVID tests there was a rapid adoption of no cost coverage, but there was a national pandemic emergency and a cross cutting will from stakeholders across the spectrum to do what was possible to expand access to the tests. Currently, for insurers to pay for an OTC product, some kind of prescription is typically needed for the plan to process a claim. There is no national requirement that OTC contraceptive drugs and products be covered without a prescription, although some states and plans have moved forward to implement coverage absent a federal requirement.
There has been some level of bipartisan support for the availability of an OTC contraceptive pill, but there is less agreement about whether these methods should fall under the ACA’s no cost coverage requirement and be covered free of cost to policyholders. A policy that requires plans to cover OTC drugs without the requirement for a prescription will likely also have implications for the coverage and payment for other drugs that have OTC status beyond contraceptives and will shape the actions of plans, public programs, pharmacies, and policyholders alike.
While some of the interviewees for this project expressed that their state coverage laws for non-prescribed OTC contraception have increased access to some degree, most cited extensive challenges and confusion over the implementation of these laws. Issues cited include the mechanics of billing for a medication that is not accompanied by a prescription, lack of awareness about these laws (for health plans, pharmacists, and enrollees); and reliance on pharmacist prescribing as a fallback approach in states that allow it. From the perspective of many interviewees, these challenges have limited the impact of these coverage laws to meaningfully increase access to non-prescribed OTC contraception. Additionally, state benefit requirements only apply to fully-insured plans and do not apply to self-funded employer plans, which are only regulated by federal law.
Some interviewees expressed that uniform coverage of OTC oral contraceptives under private plans and Medicaid can only be achieved with federal action to clarify that no prescription is needed for coverage without cost-sharing. They commented on the importance for states with requirements for coverage to communicate about the availability of these benefits with health plans, pharmacies, and consumers to increase awareness and therefore access. Some interviewees noted that eliminating the prescription requirement for OTC oral contraceptives could also expand their availability, particularly to low-income individuals who may not have the resources to purchase the products directly.
The extent to which OTC contraceptive pills can broaden the availability of effective contraceptives to those who seek them will depend on many factors including state and federal policies, pharmacy engagement, public awareness and education, affordability, as well as the implementation of systems of coverage. Absent federal guidance or regulations, the availability of private insurance and Medicaid coverage of OTC contraception without a prescription will continue to depend on the state in which one lives and, if covered by employer-sponsored insurance, the plan’s funding structure.
KFF thanks all of the interviewees for sharing their time, expertise, insights, and feedback throughout the course of this project. All interviewees who agreed to be identified are listed below. The authors would also like to thank Donald F. Downing (University of Washington School of Pharmacy) for his contributions to this project.
AHIP (formerly America’s Health Insurance Plans)Ashley Seyfarth, PharmD, Owner, Kare DrugCat Livingston, MD, MPH, Medical Director, Health Share of OregonChristine Gilroy, MD, Chief Medical Officer, Express ScriptsIllinois Department of Healthcare and Family ServicesJenny Arnold, PharmD, CEO, Washington State Pharmacy AssociationNew Mexico MedicaidNew York State MedicaidRobyn Elliott, Managing Partner, Public Policy PartnersSally Rafie, PharmD, Founder, Birth Control PharmacistTara Pfund, PharmD, Product Manager, AssureCareVictoria Nichols, Free the Pill Project Director, Ibis Reproductive HealthWashington State Health Care Authority
Methods
KFF staff identified states and a wide range of stakeholders that are involved in aspects of the decision-making, implementation, and oversight of coverage of OTC contraceptive methods. States were selected based on whether they had implemented insurance coverage of OTC contraception without a prescription and/or expanded the scope of pharmacist practice.
To inform interviews with Medicaid officials, KFF contracted with Health Management Associates (HMA) to assist in identifying key officials from state Medicaid programs and facilitating contact with them. HMA also provided feedback on interview guides and this analysis written by KFF, and provided clarification and guidance regarding pharmacy industry policies, processes, and terminology.
Potential interviewees were contacted by KFF or HMA via email. Follow-up emails were sent to those who did not respond. KFF consulted with several experts in the fields of pharmacy and policy to develop interview guides, which were tailored to the type of industry/agency and provided to interviewees prior to the interviews. Interviews were conducted virtually (except one that was completed in writing) by the KFF research team and lasted 30 to 60 minutes. Some interviews had multiple representatives from one agency, company, or organization, while others had a single interviewee. Interviewees representing smaller private industries and organizations were offered a $200 gift card incentive to participate.
Interviewees were asked to review the draft report and provide their feedback prior to publication, which most did.
To ensure interviewee confidentiality, interviewees were instructed that they would not be personally recognized unless given express consent. For this reason, neither interviewee names nor affiliations are included in this report.
Appendix
Appendix Table 2: Steps to Submitting a Pharmacy Claim
1. Pharmacy enters information required to bill insurance into its computer system, including the patient’s insurance, the drug or product, the prescriber’s national provider identification number (NPI), and other relevant information. This can be performed by a pharmacist, pharmacy technician, or clerk.
2. Pharmacy submits the claim using the National Council for Prescription Drug Programs (NCPDP)’s standard. NCPDP sets the HIPAA standard for pharmacy claims.
3. The claim reaches what is referred to as a “switch,” which acts as a gate keeper to ensure the claim reaches the correct pharmacy benefit manager (PBM) or other payer.
4. The claim contains values associated with the patient that identifies the PBM/payer the claim should be sent to.
BIN – Bank Identification Number
PCN – Processor Control Number
Group# – Group Number is not always required; some plans only use BIN & PCN
Member ID
5. The PBM/payer receives the claim for processing.
6. After processing, the PBM/payer returns the claim back to the originating pharmacy through the “switch” with either an approval or a denial. There are other processes that might require the PBM/payer to return a claim containing more information before final processing.
7. An approved claim will provide the pharmacy with the amount being paid and the amount of copayment to collect from the patient (if any).
8. Actual payment to the pharmacy (money transfer) occurs at a later date based on the parties’ contractual agreement.
SOURCE: Kevin Gorospe, PharmD, Principal, Gorospe Solutions LLC
The FDA has approved and authorized updated COVID-19 vaccines for the fall, and CDC has recommended them for everyone, ages 6 months and older. This recommendation comes as COVID-19 hospitalizations, and likely cases, are on the rise. The fall will also mark the first time that COVID-19 vaccines will be commercialized – that is, transitioned to the commercial market for their manufacturing, procurement and pricing. Up until this point, the federal government had purchased all COVID-19 vaccines and provided them free of charge to anyone, regardless of insurance coverage or ability to pay.
While the average price paid by the federal government for the most recent COVID-19 booster was about $29/dose, vaccine manufactures have indicated that they will charge $110-$130 per dose, or 3-4 times as much, on the commercial market. This has raised concerns about how those who are uninsured will access COVID-19 vaccines going forward, particularly given the potential for adverse effects on individual and population-level health. While virtually everyone with public and private insurance is guaranteed free access to any CDC recommended vaccine, including for COVID-19, this is not the case for the more than 23 million uninsured non-elderly adults in the United States, a number that may be increasing due to the unwinding of the pandemic-era continuous enrollment policy in Medicaid. Uninsured adults are disproportionately low income, people of color, and in poorer health, including being more likely to be hospitalized for avoidable health conditions and to experience declines in their overall health than those who are insured.
The federal government and vaccine manufactures have announced plans for a temporary approach to support access to the COVID-19 vaccine for uninsured adults. This policy watch provides an overview of how uninsured adults currently access recommended vaccines, how they have accessed COVID-19 vaccines thus far, including what is known about their vaccine uptake, and proposed plans to provide COVID-19 vaccines to uninsured adults this fall and beyond. It does not focus on uninsured and underinsured children who are guaranteed free access to all recommended vaccines through the Vaccines for Children Program.
How do uninsured adults access and pay for recommended vaccines now?
For adults who are uninsured in the United States, there is no guaranteed access to free vaccines recommended for routine use. The federal government does purchase a limited number of recommended vaccines directly for uninsured and other qualifying adults through funding that comes from Section 317 of the Public Health Services Act. Section 317 is a discretionary program, dependent upon annual appropriations from Congress, and its funding is used both for purchasing recommended vaccines and for supporting the nation’s immunization infrastructure. As a discretionary program, funding does not necessarily match need or cost, or take into account the introduction of a new vaccine (such as for COVID-19 or RSV). Because of these limits, some states supplement their Section 317 funds with state funds in order to reach more people. To be eligible to receive free vaccines through the Section 317 program, adults must be uninsured, have no vaccine coverage, or be vaccinated as part of a public health response such as a mass vaccination campaign. Free vaccines are largely distributed through state and local health departments and community health centers. Uninsured adults who are unable to access free vaccines must pay out of pocket for the full cost of the vaccines or receive them on a sliding fee scale at certain safety net providers.
How have uninsured adults accessed COVID-19 vaccines up until this point?
During the COVID-19 pandemic emergency, the federal government spent billions of dollars in emergency funds to purchase COVID-19 vaccines, including boosters, to provide them free of charge to the public. Vaccines were distributed widely, through federal and state public vaccine distribution centers, pharmacies, and health centers, which were instrumental in prioritizing hard to reach communities during this time. In addition, states were given a temporary option to provide Medicaid coverage for COVID-19 vaccines to uninsured individuals and receive 100% federal matching funds to cover the costs of providing care. This coverage option ended when the public health emergency declaration ended in May.
What do we know about uptake of COVID-19 vaccines among uninsured adults?
Among adults between the ages of 18 and 65, and despite COVID-19 vaccines being free to all up until this point, those who are uninsured are much less likely to have been vaccinated compared to those who are insured (54% vs 75%), based on recent KFF polling. This difference in uptake may reflect several factors, including systemic barriers to accessing care among uninsured individuals, different views of vaccination, and other challenges.
What is the ‘Vaccines for Adults’ program proposed by the Biden administration?
The Biden administration has twice proposed to Congress in its annual budget request the creation of a new “Vaccines for Adults” (VFA) program to provide uninsured adults with access to all recommended vaccines, including COVID-19 vaccines, at no cost. Congress has not acted on these proposals. As a result, the administration has proposed a temporary “Bridge Access” program to provide COVID-19 vaccines to uninsured adults on a limited basis (see below).
What is the HHS Bridge Access Program?
To address concerns about COVID-19 vaccine access among uninsured adults this fall, the administration announced a new “Bridge Access Program” earlier this year. It will operate as a “public-private partnership to help maintain uninsured individuals’ access to COVID-19 care at their local pharmacies, through existing public health infrastructure, and at their local health centers.” Financed with $1.1 billion in funds already appropriated during the COVID-19 emergency (funds will be used for both vaccines and treatments), the program is largely managed by the CDC and has two main components:
Vaccines will be purchased through the CDC’s Section 317 program and distributed through that network of local health departments and health centers. The Health Services and Resources Administration will provide additional support to health centers to ensure equitable access to vaccines and treatments.
CDC will partner with three pharmacy chains (CVS, Walgreens, and eTrueNorth) and provide them with a per-dose payment to support vaccine administration costs, as was done during the public health emergency. This component of the program relies on vaccine manufacturers providing COVID-19 vaccines at no cost to uninsured people, as they have announced (see below).
CDC has indicated that vaccines under the program will begin to be available within 48 hours of being recommended by CDC. The program is temporary and will run through December 2024.
Will vaccine manufacturers help provide COVID-19 vaccines to the uninsured?
Many vaccine and drug manufacturers offer patient assistance programs to support those without insurance or with limited means in accessing their products; however, these programs vary in terms of eligibility and application process. Both Pfizer and Moderna have announced that they intend to provide their vaccines at no cost to uninsured individuals, though details are not yet available.
Discussion
During the COVID-19 pandemic emergency, the federal government spent billions of dollars in emergency funds to purchase COVID-19 vaccines, including boosters, to provide free of charge regardless of insurance status or ability to pay. As COVID-19 vaccines enter the commercial market for the first time, uninsured adults will no longer be guaranteed access to these vaccines at no cost. To address this in the short term, the federal government announced a “Bridge Access Program” that relies, in part, on vaccine manufacturers providing free vaccines to uninsured individuals. Still, full details on these efforts are not yet available. And, while participating pharmacies will be required to conduct outreach to underserved communities, ensuring eligible people know about the program will be a challenge. Given that uninsured adults are disproportionately low income and people of color and that COVID-19 vaccine uptake among uninsured adults is already lower than among those with insurance, concerns about cost and lack of awareness about the availability of free vaccines could present additional barriers to vaccination and further exacerbate existing disparities in uptake and health status. Moreover, these temporary approaches do not address access to vaccines beyond COVID-19, such as for flu or RSV, and underscore the broader challenge faced by those who are uninsured in accessing preventive health services.
Medicare Advantage enrollment has grown rapidly in recent years, and in 2023, more than half (51%) of all eligible Medicare beneficiaries are in a Medicare Advantage plan. Most Medicare Advantage enrollees, and most Medicare beneficiaries, live in metropolitan areas. To understand the role of Medicare Advantage in rural areas, this analysis examines trends in enrollment, plan availability and premiums in less populated counties.
Medicare Advantage enrollment is lower, but has grown more rapidly in recent years in rural areas than in metropolitan areas. In 2023, 40% of all eligible Medicare beneficiaries in rural counties are enrolled in a Medicare Advantage plan, nearly four times the share in 2010 (11%). Rural Medicare Advantage enrollees can choose from among 27 plans, on average, which is triple the number of plans available just five years ago. In rural counties, like all areas, most Medicare Advantage enrollees are in a plan that charges no additional premium, other than the Part B premium.
Medicare Advantage in Rural Areas
Medicare Advantage enrollment has quadrupled in rural areas since 2010 and reached 40% in 2023.
In 2023, a smaller share (40%) of Medicare beneficiaries in rural areas – counties with less than 10,000 people – are enrolled in a Medicare Advantage plan than Medicare beneficiaries in micropolitan (10,000 to 50,000 people) or metropolitan (at least 50,000 people) areas (44% and 53%, respectively). Though Medicare Advantage enrollment is lowest in rural areas, it has grown more rapidly in these counties, nearly quadrupling from 11% of eligible Medicare beneficiaries in 2010 to 40% in 2023. Over the same period, the share of Medicare beneficiaries enrolled in a Medicare Advantage plan in micropolitan areas nearly tripled (from 15% to 44%), and nearly doubled in metropolitan areas (from 27% to 53%).
In 2023, more than 1.8 million Medicare beneficiaries in rural areas are enrolled in a Medicare Advantage plan, more than four times the number enrolled in 2010 (400,000). In metropolitan areas, enrollment increased from 9.7 million in 2010 to 26.3 million in 2023 and in micropolitan areas, enrollment rose from nearly 700,000 in 2010 to 2.6 million in 2023 (Appendix Table 1). The growth in enrollment translates into an average annual increase of 12% in rural areas and 11% in micropolitan areas, compared with 8% in metropolitan areas between 2010 and 2023.
The average Medicare beneficiary living in a rural county can choose among 27 Medicare Advantage plans, triple the number of plans offered five years ago.
Across all areas, the number of Medicare Advantage plans available to the average Medicare beneficiary have risen steadily since 2018, after holding relatively constant in earlier years. In 2023, the average Medicare beneficiary in a rural area has 27 Medicare Advantage plans to choose from, which is three times more than the number of plans available in 2018 (9 plans). This is similar to the growth in micropolitan areas, where the average Medicare beneficiary has access to 31 plans in 2023, compared to 11 plans in 2018. In contrast, the average Medicare beneficiary in a metropolitan area can choose from substantially more plans – 46 in 2023, just over double the number in 2018 (22 plans) (Figure 2).
In 2023, the average Medicare beneficiary living in a rural area can choose among Medicare Advantage plans offered by six firms, twice the number of firms offering plans in these counties in 2018.
Since 2018, the average number of firms offering Medicare Advantage plans has increased in all areas. The average Medicare beneficiary in a rural area can choose from plans offered by six firms in 2023, which is double the number of firms offering plans in these areas in 2018 (3 firms). The trend in the number of firms offering plans in micropolitan areas is similar, rising from three in 2018 to six in 2023. The number of firms offering plans has been consistently higher in metropolitan areas than in other geographic areas, rising from six firms in 2018 to ten firms in 2023 (Figure 3).
More than two-thirds (69%) of Medicare Advantage enrollees in rural areas are in a plan that requires no premium other than the Part B premium.
A somewhat smaller share of enrollees in rural (69%) and micropolitan (66%) counties pay no additional premium compared with enrollees in metropolitan areas (75%) (Figure 4). Medicare Advantage plans may impose a premium for the cost of Medicare-covered services above payments made by the federal government to the plans, as well as the cost of prescription drug coverage. Most Medicare Advantage plans offer extra benefits for no additional premium.
Since 2015, the share of Medicare Advantage enrollees in plans with no additional premium has increased steadily in all areas. Growth has been fastest in rural areas where the share of enrollees in plans with no additional premium increased from 21% in 2015 to 69% in 2023. Growth has been similarly rapid in micropolitan areas, rising from 24% in 2015 to 66% in 2023. In metropolitan areas, the share of enrollees in plans with no additional premium has been consistently higher than in rural or micropolitan areas, but has increased more slowly, rising from 53% in 2015 to 75% in 2023 (Appendix Table 2).
Discussion
Medicare Advantage enrollment and plan availability in rural areas have increased rapidly in recent years, as they have in more populated counties. Private plans often provide supplemental benefits to enrollees for no additional premium (other than the Part B premium), including some coverage of dental, vision, and hearing services, as well as reduced cost sharing compared to traditional Medicare without a supplemental plan. At the same time, Medicare Advantage plans may use provider networks, limiting coverage of services delivered by out-of-network providers. Provider networks may impose barriers to people living in rural areas who already face challenges obtaining health care services because of fewer providers and longer travel distances. Despite recent growth, Medicare Advantage enrollment in rural areas remains lower than enrollment in more populated areas. This could be the result of fewer investments in marketing and outreach in these areas by Medicare Advantage insurers, because financial returns are lower given the smaller population of potential enrollees. As Medicare Advantage enrollment continues to grow, understanding how plans differ across metropolitan, micropolitan and rural areas will be increasingly relevant to assessing how well private plans meet the needs of their enrollees.
Jeannie Fuglesten Biniek and Tricia Neuman are with KFF. Gabrielle Clerveau was with KFF at the time this brief was written. Anthony Damico is an independent consultant.
As states unwind the Medicaid continuous enrollment provision, data show that large shares of people are being disenrolled for paperwork or procedural reasons as opposed to being determined ineligible. These high procedural disenrollment rates are raising concerns that many people who remain eligible for Medicaid may, nevertheless, be losing coverage. But, there are different procedural disenrollment rates being reported that can be confusing to interpret. This policy watch explains how the different rates are calculated, provides insights for interpreting the data, and describes steps the Centers for Medicare and Medicaid Services (CMS) and states are taking to reduce procedural disenrollments.
What are procedural disenrollments?
Procedural disenrollments occur when there is no definitive determination of ineligibility. Procedural disenrollments may happen because enrollees do not receive renewal notices or face barriers to completing the redetermination process, such as not understanding what steps need to be taken. In some cases, people may be procedurally disenrolled because eligibility workers are not able to process documents enrollees have submitted before cases are automatically closed. Some enrollees may know they are no longer eligible, perhaps because of an increase in income or other change in circumstance, and do not respond to the renewal request so the state cannot make a definitive determination that the person is no longer eligible. While some states are reporting reasons for procedural terminations that indicate whether someone may be over income or did not respond, these data are limited. The main concern with procedural disenrollments is that many people losing Medicaid for these paperwork reasons may still be eligible and do not have another source of health coverage.
How are the procedural disenrollment rates calculated and how should different rates be interpreted?
Different procedural disenrollment rates are being reported for states because of differences in how those rates are calculated. When calculating procedural disenrollment rates, the denominator and timeframe matter. A procedural disenrollment rate calculated using total disenrollments as the denominator is going to be higher than a rate that uses all initiated renewals, which includes enrollees whose coverage was renewed as well as cases that remain pending, as the denominator. Additionally, a cumulative procedural disenrollment rate based on all reported renewal data since the start of the unwinding period is going to differ from one that is cohort based and reflects only procedural disenrollments for a single month. The cumulative procedural disenrollment rate reported by KFF, 73% as of September 5, 2023, uses total disenrollments as the denominator, highlighting that a substantial majority of disenrollments are for paperwork reasons rather than for people being definitively determined ineligible. In contrast, the cumulative procedural disenrollment rate using all initiated renewals as the denominator is 20%, reflecting the fact that many people have had their coverage renewed (Figure 1).
Reporting procedural disenrollments as a share of total disenrollments isolates procedural disenrollments and can help to identify systems or other issues. High procedural disenrollment rates using this methodology may reflect problems with mail delivery, backlogs in processing returned forms, or problems complying with federal regulations related to processing redeterminations. In contrast, states with lower procedural disenrollments as a share of total disenrollments may have more effective processes and procedures for contacting enrollees; they may provide a longer timeframe for enrollees to respond; or they may have more robust systems that streamline the process for returning renewal forms or submitting documentation.
Examining procedural disenrollments as a share of people renewed or the share of all initiated renewals can provide important context for understanding the data. States that are renewing large shares of people each month or that are holding redetermination cases open to give enrollees more time to respond may have lower overall disenrollment rates, even if their procedural disenrollment rates as a share of total disenrollments are high. An example is the District of Columbia, which has a 90% procedural disenrollment rate as a share of total disenrollments that drops to just 27% when calculated as a share of total completed renewals because DC is renewing coverage for 70% of enrollees (Figure 2). While some states, such as Texas, have procedural disenrollment rates that are higher than the national average for each measure, other states, such as Michigan, have rates that are lower.
How are CMS and states addressing high procedural disenrollment rates?
CMS has sent letters to states identifying concerns with high procedural disenrollment rates and potential systems issues contributing to inappropriate procedural terminations. On August 9, 2023, CMS sent letters to states expressing general concern over procedural disenrollment rates and urging states to take action to reduce those rates. CMS flagged 28 states where the agency deemed the procedural disenrollment rate to be too high. The rates reported in the letters were for May 2023 only, using total renewals initiated in the month as the denominator, and CMS defined a high procedural disenrollment rate as greater than 10%, More recently, CMS sent a letter to state Medicaid Directors on August 30, 2023 identifying a potential issue related to how some states are processing ex parte renewals (i.e., renewals that make use of electronic data sources documenting income and other circumstances) that could be contributing to inappropriate procedural terminations for some individuals, including children. According to the letter, any state that is out of compliance with federal rules must implement a mitigation strategy until the issue is fixed, reinstate coverage for all individuals who were improperly terminated for procedural reasons, and pause procedural disenrollments for individuals who may be affected.
Most states have adopted at least some of theflexibilities CMS has made available during the unwinding period aimed at reducing procedural disenrollment rates. More recently but prior to the release of the CMS letters, some states extended renewal notice timelines by 30 days to give people additional time to respond and to give states additional time to reach out to enrollees who have not yet responded. Other states temporarily paused procedural disenrollments for certain cohorts or for all enrollees. In light of the recent CMS letters, states can be expected to adopt additional strategies to reduce procedural disenrollments.
Enhanced Marketplace subsidies have continued to drive up enrollment in the individual market, and the loss of Medicaid coverage by millions of people could contribute to this trend, according to a new KFF analysis. Meanwhile, enrollment in non-ACA-compliant plans is at a record low.
As of early 2023, an estimated 18.2 million people have individual market coverage, the highest since 2016. Individual market enrollment grew by about 29% between early 2020 and early 2023 — a result of enhanced subsidies introduced by the Inflation Reduction Act, increased outreach, and an extended enrollment period.
This enrollment growth could continue in 2023 as states resume Medicaid disenrollments amid the unwinding of the continuous enrollment provision. Some of the people losing Medicaid coverage may be eligible for subsidies on the ACA Marketplaces.
Due in part to the enhanced subsidies, about 4 in 5 individual market enrollees have subsidized coverage — the highest share since the ACA was implemented.
The number of people in non-compliant plans has fallen each year and could decrease further due to the Biden Administration’s proposed rule that would reverse the expansion of short-term plans. An estimated 1.2 million people were in non-ACA-compliant plans in mid-2022, compared to 5.7 million in mid-2015. These short-term plans often do not include certain benefits or coverage for pre-existing conditions and can impose a dollar limit on insurance coverage.
If unsubsidized premiums rise in 2024 due to higher health care prices and utilization, enhanced subsidies could shield most individual market enrollees from increases in their monthly payments.
With Marketplace enrollment at a record high in early 2023, the upcoming open enrollment period could be among the busiest yet. In addition to Marketplace enrollees renewing coverage, uninsured people and those buying individual coverage off-Marketplace – as well as those losing Medicaid coverage as the pandemic-era continuous enrollment provision unwinds – may want to check if they are eligible for expanded subsidies under the Inflation Reduction Act.
This analysis looks at how many people are signed up for each type of individual market coverage—both on- and off-Marketplace and with or without subsidies—as of early 2023. The number of people enrolled in compliant and non-compliant plans was also evaluated up to 2022, the latest year this data is publicly available. A key takeaway from this analysis is that as Marketplace enrollment has reached record highs with enhanced premium assistance, fewer people are buying coverage off-Marketplace, but the overall individual market is nonetheless growing.
Individual market enrollment continues to grow, driven by enhanced subsidies. As of early 2023, an estimated 18.2 million people have individual market coverage, the highest since 2016 (Figure 1). The individual health insurance market grew rapidly in the early years of ACA implementation, reaching nearly 20 million people in early 2015, nearly double the approximately 11 million signed up before the ACA. However, these enrollment gains were partially offset by subsequent declines driven by steep premium increases, particularly among people not receiving subsidies. By early 2020, the individual market had declined to about 14 million enrollees.
During this period of decreasing individual market enrollment, subsidized enrollment increased from 2017-2019 which corresponds with the Trump Administration ending federal cost-sharing reduction (CSR) payments; this led to insurers “silver loading” premiums for CSRs and increased premium subsidies for some.
With passage of enhanced subsidies in the American Rescue Plan Act (ARPA), combined with boosted outreach and an extended enrollment period, 2021 marked the first year since 2015 when there was an increase in individual market enrollment. Individual market enrollment grew about 5% from 14.1 million in first quarter 2020 to 14.9 million in first quarter 2021.
The ARPA’s subsidies didn’t simply bring people from off-Marketplace plans to the Marketplace; the subsidies also helped bring overall individual market enrollment higher, up to 18.2 million in early 2023, an increase of about 29% from early 2020.
Now, with enhanced subsidies in place, the vast majority of people buying individual market coverage are subsidized. The Inflation Reduction Act continues the ARPA subsidies without interruption for another three years through 2025. That means premiums are capped for people with incomes over 400% of the poverty level ($120,000 for a family of 4 in 2024) who were ineligible for subsidies previously, and those who were already eligible for subsidies are paying even less than they were before. Overall, about 4 in 5 individual market enrollees are now subsidized (Figure 2) – the highest share since the ACA was implemented – and some of those who aren’t receiving a subsidy might find they are eligible if they moved onto the Marketplace.
Heading into 2024 open enrollment, we estimate there are still about 2.5 million people buying unsubsidized coverage off-Marketplace, including some in non-ACA-compliant plans (like grandfathered and short-term plans). Early 2023 off-Marketplace enrollment decreased by 20% compared to early 2022. Despite Trump Administration efforts to promote non-compliant coverage, the number of people in non-compliant plans has fallen each year.
While enrollment in non-ACA-compliant plans is at a record low, a substantial number continue enrolling in non-compliant plans. Using federal risk adjustment data and data compiled by Mark Farrah Associates, we estimate 1.2 million people were in non-ACA-compliant plans in mid-2022, compared to 5.7 million in mid-2015 (Figure 3). Although we don’t yet have complete 2023 data, it’s likely ACA-compliant enrollment (both on- and off-Marketplace) is currently at a record high and that non-compliant enrollment is at a record low.
Non-compliant short-term plans often do not include certain benefits or coverage for pre-existing conditions, and can impose a dollar limit on insurance coverage. For example, of short-term plans reviewed, none covered maternity care, most didn’t cover prescription drugs, about half didn’t include mental health or substance use treatment, and most imposed a dollar limit on covered services or drugs. The Biden Administration’s proposed rule, which would reverse Trump Administration’s expansion of short-term plans, may further reduce enrollment in non-compliant plans if it is finalized.
The share of individual market enrollment in ACA compliant plans has increased to 93% in mid-2022 compared to 71% in mid-2015. These data are only available through mid-2022, and non-compliant enrollment may have fallen even further in 2023.
Some off-Marketplace enrollees will find they are still ineligible for subsidies, even with enhanced subsidies. Undocumented immigrants and people with affordable offers of employer coverage are ineligible for Marketplace subsidies. Additionally, although there is no longer an upper income limit for subsidies, people with higher incomes who would pay less than 8.5% of their income for an unsubsidized benchmark silver plan do not qualify for subsidies because their premium isn’t high enough to trigger financial help. Even so, some of the latter group may find it advantageous to purchase on the Marketplace because if they experience midyear changes in their income or other circumstances, they may begin receiving subsidies mid-year without changing plans or they could retroactively claim a subsidy when they file taxes.
Yet others who were previously ineligible for Marketplace subsidies may now be eligible. For example, the Biden Administration’s fix to the “family glitch” means dependents of workers, who have affordable self-only coverage but unaffordable family coverage through their employers, can get Marketplace subsidies starting in 2023.
Marketplace enrollment data are as of the first quarter of 2023. In the second quarter of 2023, states started to disenroll people from Medicaid, some of whom may be signing up for subsidized Marketplace coverage.
How might future premium increases affect people in the individual market? Looking back over the last ten years of the ACA, changes in individual market enrollment closely mirror changes in what people had to pay for coverage. In years when premiums were rising steeply from 2016-2018, unsubsidized individual market enrollment fell. When premiums held mostly steady from 2019 to 2020, so did individual market enrollment. Then, as new subsidies became available in 2021-2023, individual market enrollment picked up again, driven by an increase in the number of subsidized enrollees.
Heading into 2024, we may see unsubsidized premiums rise, pushed up by rising health care prices and utilization. However, unlike when premiums rose in past years, the Inflation Reduction Act’s enhanced subsidies could shield the vast majority of individual market enrollees from increases, even those with higher incomes. In fact, some people who aren’t subsidized in 2023 may find premium increases in 2024 make them newly eligible for subsidies (if their benchmark premium rises above 8.5% of their income). But, to take advantage of subsidies, they would need to shop on the Marketplace during open enrollment.
Methods
Federal enrollment and risk adjustment data were combined with administrative data insurers report to state regulators, as compiled by Mark Farrah Associates, to determine the number of enrollees in each type of individual market coverage. Early effectuated enrollment reports (available for years 2015-2023) were used to determine the number of on-Marketplace and subsidized enrollees. Risk adjustment data (available for years 2014-2022) were used to determine the total number of enrollees in ACA-compliant plans. The number of compliant enrollees in Massachusetts and Vermont in 2015-2021 and Massachusetts in 2022 was estimated using a ratio of total Exchange enrollment to total compliant enrollment in all the other states.
Mark Farrah Associates data were used to estimate the total number of enrollees in the individual market. Because some plans do not file quarterly data, we adjust these plans’ enrollment numbers based on enrollment changes seen in plans that do file quarterly. We also remove likely Children’s Health Insurance Program, or CHIP, enrollees from the individual market total.
As the Biden administration begins the process of negotiating prices for 10 costly drugs on behalf of Medicare and its beneficiaries as authorized in last year’s Inflation Reduction Act, KFF Executive Vice President for Health Policy Larry Levitt probes some likely arguments against it in this op-ed column in The New York Times. The column also examines the policy and political implications of the debate and pending legal challenges.