Navigating the Unwinding of Medicaid Continuous Enrollment: A Look at Enrollee Experiences
Report
During the COVID-19 pandemic, states kept people continuously enrolled in Medicaid in exchange for enhanced federal funding. Leading up to the unwinding, many enrollees were unaware of the upcoming renewals and when informed, worried about losing coverage. With the end of the continuous enrollment provision on March 31, 2023, states are part-way through the process of redetermining eligibility for people enrolled in Medicaid and disenrolling those who are either no longer eligible or who are unable to complete the renewal process. States are in different places in terms of how many enrollees have been redetermined and are experiencing different outcomes in terms of the share of enrollees who have been disenrolled or renewed. According to KFF tracking, six months into the unwinding (at the time of our focus groups), states had reported renewal outcomes for one in three Medicaid enrollees, and 16 million had their renewed coverage and nearly 9 million had been disenrolled. These numbers continue to rise as states move through the unwinding period.
To better understand the experiences of Medicaid enrollees who have completed the renewal process since the start of the unwinding period, KFF conducted five virtual focus groups in September to learn about their experiences with Medicaid, awareness of the end of the continuous enrollment provision, experiences renewing their coverage since the start of the unwinding, and if they were disenrolled, efforts to regain Medicaid or transition to other coverage. Key findings from our groups include the following:
- Awareness that Medicaid coverage had been protected during the pandemic and that disenrollments had begun again in their state varied among participants.
- Among participants who successfully renewed their Medicaid coverage, most found the process quick and easy, especially when done online. However, even among those that renewed coverage, some reported barriers to completing or submitting paperwork and faced long processing times. Some also experienced problems with understanding notices and other communications from the states as well as challenges getting through to call centers.
- Participants who were disenrolled reported that they lost their coverage for a variety of reasons, and some who thought they were still eligible did not know why they had been disenrolled. Many who were disenrolled encountered an array of communication problems. Several faced substantial out-of-pocket costs for medically necessary care during gaps in coverage and needed one-on-one assistance from caseworkers and community-based organizations to help them with attempts to regain Medicaid coverage. After losing Medicaid, some participants obtained coverage through the Affordable Care Act (ACA) Marketplace or their employer, but others remained uninsured.
- Overwhelmingly, participants valued Medicaid coverage and pointed to health and financial consequences if Medicaid or other coverage were not available. Participants said that losing Medicaid would be “devastating” due to loss of access to “lifesaving” prescriptions and treatments. They believed that losing Medicaid would cause a serious decline in their physical and mental health and expressed anxiety at the thought of no longer having Medicaid coverage for themselves or their children.
Focus group participants’ experiences show that while the renewal process can be easy and seamless for some individuals, for others the process may be complicated and result in confusion and termination of coverage. As unwinding continues, these enrollee experiences can help inform policy makers about opportunities to improve communication and outreach, simplify notices, provide assistance with renewals including through call centers, and help enrollees who were disenrolled regain Medicaid if eligible or transition to other coverage if no longer eligible.
Information About The Focus Group Participants
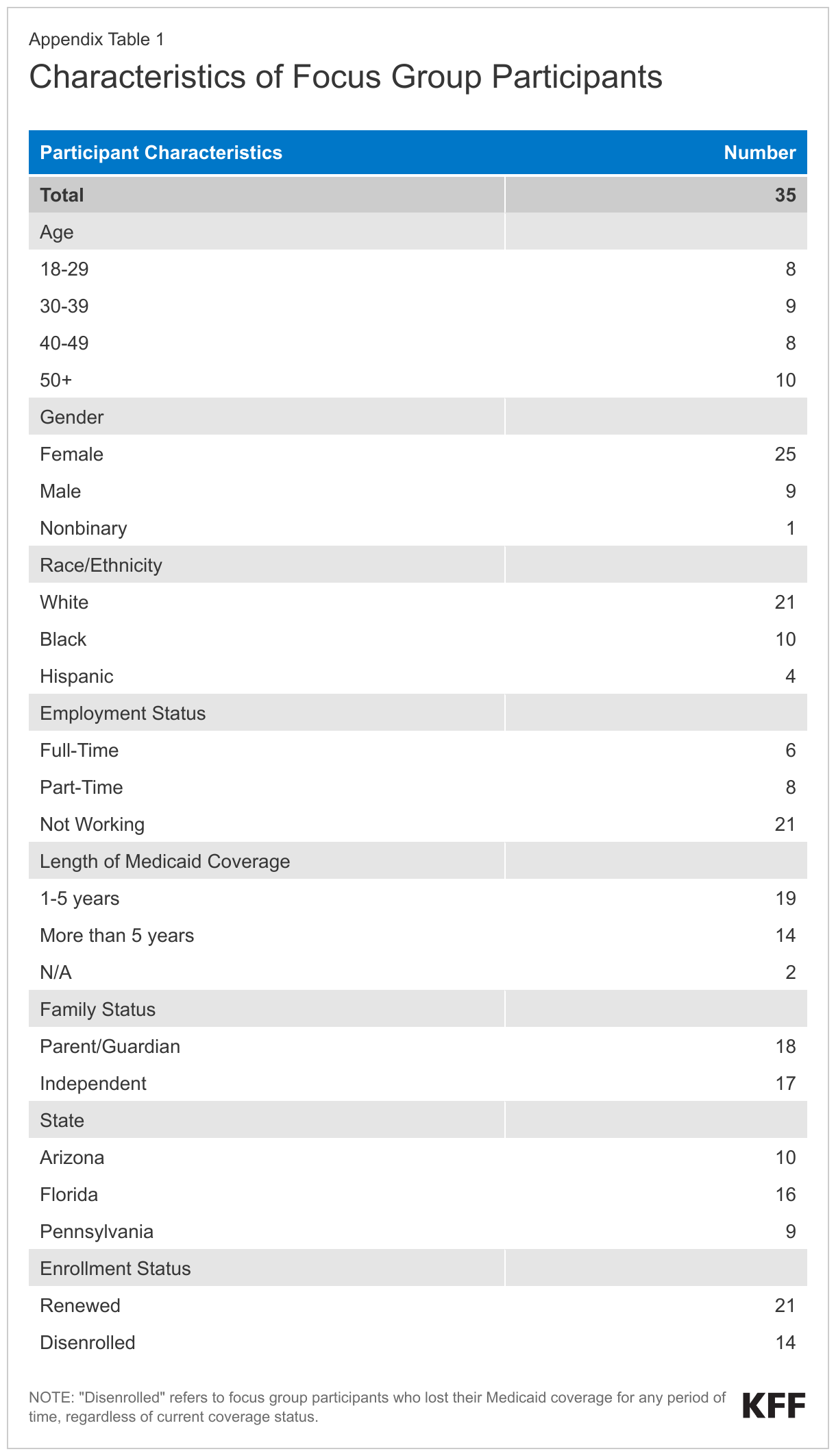
Groups included 35 adults from three states (Arizona, Florida, and Pennsylvania) who self-identified as having Medicaid coverage for themselves or had children enrolled in Medicaid. KFF worked with PerryUndem Research/Communication to conduct the focus groups. Participants included a mix of adults by gender, race/ethnicity, age, length of time enrolled on Medicaid, and work and family status. Groups were generally stratified by those who were able to renew coverage and those who had been disenrolled. Some individuals who were disenrolled from Medicaid were recruited with the assistance of local advocacy organizations. Individuals who were able to participate in our groups needed to have completed the Medicaid renewal process since April, have two hours of time, a quiet space, a computer, and internet. These characteristics alone may not fully represent many Medicaid enrollees, so findings may not be generalizable to the entire Medicaid population. See Appendix Table 1 for demographic details about the participants.
Key Themes
Current Health Status of Medicaid Enrollees
Many participants were managing an array of physical and mental health conditions, as well as financial difficulties. Focus group participants reported a range of health conditions including chronic pain, HIV, diabetes, substance use disorders, epilepsy, and anxiety and depression. To manage these conditions, participants need medications and receive ongoing therapy. Some participants noted the challenges of managing chronic health conditions on top of financial pressures that were exacerbated by rising prices. Due to Medicaid’s eligibility requirements, the people going through the renewal process, by definition, have low incomes and are more likely to experience financial distress.
“I’m looking for work, and I’m having a hard time because I don’t have a lot of office experience … And then I have also some other health issues that have come about, such as; I need to have surgery, I need to have a right hip replacement.”
44-year-old, Black female,(Pennsylvania)
“I see a counselor once a week for my anxiety. I’m military and it has caused me to have some mental health issues.”
26-year-old, Black female(Florida)
“I’m HIV positive. I feel as though the medication that I am on is not helping as much as it used to. I also have heart issues where two years ago I suffered a major heart attack … I just feel like it’s just one of those moments in my life where; why does it always have to be such a hard struggle?”
51-year-old, White female(Pennsylvania)
“I’ve recently had a foot surgery in March, and I have another surgery scheduled in October. I deal with some chronic pain issues so one of my doctors is a pain specialist and a podiatrist that [I see] at least once a month.”
55-year-old, Black female(Arizona)
Experience With Medicaid
Participants valued Medicaid coverage and noted that it enables them to access health care services, mental health services, and medications for themselves and their children. Those with serious chronic health conditions and health needs, such as diabetes, HIV, and asthma, said having Medicaid means they can get medications and have regular doctor’s visits to manage their conditions. Others used Medicaid to access mental health or substance use disorder treatment. In a number of cases, enrollees said Medicaid coverage has provided access to necessary surgeries and treatments, such as foot surgery or a CPAP machine for sleep apnea. Some had Medicaid coverage due to pregnancy or serious disabilities. Parents in the groups valued being able to access preventive and primary care, treatment for more serious conditions, mental and behavioral health services, and dental care for their children. For these parents, Medicaid provided peace of mind knowing that unexpected health costs would be covered for children.
“I’ve had some substance abuse issues and it pays for my methadone … So that helps me with that drastically. I have used the behavioral health for myself as well for my son when he was having some issues getting back into the school.”
40-year-old, White female(Arizona)
“I have in the last year seen several specialists, primary care, as well as an Urgent Care visit. And then my son is diabetic, so he actually has like a regular condition that he has to see a doctor every month and get prescriptions every month.”
38-year-old, White female(Arizona)
“The biggest thing is just the insurance that the kids are covered … I really hated periods where a kid might get hurt or would’ve gotten hurt, and I was scared to take them for help because I was wondering how much it was going to cost.”
29-year-old, Black female(Florida)
Participants specifically commented that Medicaid’s limited out-of-pocket costs enabled them to get the care they needed, though some mentioned difficulty finding doctors who accept Medicaid. Participants expressed appreciation that they were able to access medications and treatment that would otherwise be too expensive. Some participants said that before they had Medicaid, they would forgo procedures or not take medications as prescribed (such as cutting pills in half) because these treatments would cost hundreds or thousands of dollars they could not afford. While participants noted some issues related to access to care and providers, such as prior authorization and difficulty finding doctors who accept Medicaid, most said Medicaid covers the services they need.
“I had to go to the hospital because my leg started swelling and then having Cellulitis … I was in there for like three days on IV antibiotics. I was pretty impressed with it, just because, you know, I don’t pay anything, which is really nice.”
34-year-old, White male (Arizona)
“My job currently doesn’t offer insurance … So it impacts me financially … being able to go to the doctor like worry-free without having to pay extra costs, and copays and things like that.”
29-year-old, White male(Pennsylvania)
“I battle severe depression and anxiety … my medication is very expensive. (With) mental health issues, I’ve gone to the doctor more probably than I ever have in my life with this insurance.”
55-year-old, Black female(Arizona)
“My son has microscopic tubes in his ear, he was getting constant infections. Without it [Medicaid], it would’ve cost us thousands, thousands, and thousands for that surgery.”
41-year-old, Hispanic male(Florida)
Participants also said that Medicaid coverage helps them stay healthy enough to work. Working participants noted that being able to maintain their health was integral to being able to continue to work. Medicaid coverage allowed them to address health conditions that if left untreated may have impacted their ability to meet the physical demands of their jobs. Others said having Medicaid made it easier for them to work because they did not need to find jobs that provided insurance, allowing them to take available jobs to get back on their feet and to provide for their families.
“I had a torn meniscus recently and a sprained ACL and being that I’m an Instacart worker, without the Medicaid I wouldn’t have been able to see the specialist and get the treatment that I needed in order to get back to work. So Medicaid has played a big role for me, because I definitely wouldn’t be able to afford the cost.”
33-year-old, Black female(Florida)
“I think Medicaid helps you because you need your health before you need anything. As far as for me, like I said I have some health issues that I deal with on a daily basis, but it does help me, it keeps me going.”
44-year-old, Black female(Pennsylvania)
Awareness of the Continuous Enrollment Provision
Awareness varied among participants that Medicaid coverage had been protected during the pandemic and that disenrollments had begun again in their state. Many participants said they did not know about the continuous enrollment provision in place during the pandemic and some were unaware that these protections had come to an end. Others were aware of the policy change, having learned about it through news sources, posters in their providers’ offices, or through notices received in their online accounts or mailed to them by the Medicaid agency. Whether they had heard about the policy change or not, most participants knew that they needed to renew their Medicaid coverage. Some were not concerned about the law changing and renewals because they felt certain they would continue to qualify.
“I never heard of anything [about disenrollments resuming], but nothing really changed for me because I’m on disability. So my income doesn’t change at all, so it didn’t really affect me at all.”
44-year-old, White male(Pennsylvania)
“I actually heard about it on the local news channel. And I’m unsure if I got anything in the mail about it … I was on it prior to COVID so it didn’t really affect me one-way or the next.”
34-year-old, Black female(Pennsylvania)
“If I remember correctly that the PCP sent me a letter warning me that … I was waiting for the packet, and that came like a month before when they were gonna kick everybody off. My doctor was more on top of it than the actual Medicaid office.”
34-year-old, White male(Arizona)
“I received correspondence, and I think I also logged in because I heard about it that it was not going to auto renew anymore. So I logged into my portal to see what it said.“
32-year-old, Hispanic female(Arizona)
Renewal Experiences
Among participants who successfully renewed their Medicaid coverage, most found the process quick and easy, especially when done online. Participants completed their renewal in multiple ways including using online portals, sending back paper renewal forms in the mail, calling a caseworker and completing over the phone, or submitting paperwork in person at a local Medicaid office. While most participants who were able to renew their coverage said they received some communication from the Medicaid agency alerting them to the need to renew, some said they did not receive a notice, but were aware of their renewal date because they had set up calendar reminders or proactively checked their online accounts. Many participants who had successful renewal experiences described the process as easy. Most participants who had their coverage renewed reported completing their renewal online, and most expressed satisfaction with how quickly they were able to complete the process. However, those who have access to computers who were able to participate in our virtual focus groups may be more likely to be able to complete an online renewal process. While the availability of online renewals may help to streamline the process for some, not all Medicaid enrollees have internet access or are comfortable using online technology.
“I would say the only time that I interact with [the online account] is when it’s time to renew and get e-mail text message something, saying it’s time to renew. I just log in, click through everything, and then it’s done. It’s pretty convenient.”
39-year-old, White individual(Arizona)
“I actually got a call after I got the letter and I just talked to them on the phone and it like, well, nothing’s changed and they’re like, okay, you’re fine then. It was pretty painless.”
63-year-old, Black female(Arizona)
“Filling out the process online, it’s lengthy, but I understand it, I know what I have to provide and what they’re asking of me.“
41-year-old, Hispanic male(Florida)
“It’s much easier now just not having to sit in the office or, you know wait, and the wait, you know, just it’s easier to do it everything online.“
33-year-old, Black female(Pennsylvania)
Some, however, reported barriers to completing or submitting paperwork or said they experienced long processing times. A few participants who sought to complete their renewal online were unable to upload certain documents and had to fax the documents or go in person to a local office to submit the paperwork. One participant who renewed her son’s coverage expressed being surprised at having to renew the coverage earlier in the year than she had previously. Some participants noted the time it took the state to confirm their ongoing eligibility was longer than for renewals they had completed prior to the COVID-19 pandemic, potentially reflecting administrative backlogs in their state. While some of the problems people faced were consistent across states, there was variation, particularly in processing times. Additionally, in states where workers at county offices processed renewals, people’s experiences differed depending on where they lived, with people in some areas reporting more problems than those in other areas.
“This particular one took a lot more, a lot longer. It took like 2 months, 2 ½ months to get an answer.”
41-year-old, Hispanic male(Florida)
“I was so surprised when the renewal came up over the summer because I’m used to renewing at the end of the year.”
51-year-old, White female(Florida)
“I had a change in my income and my residency and so they wanted a form of income verification, and for some reason it wouldn’t upload on their system … So I had to physically drop it off at the location.”
38-year-old, White female(Arizona)
“Somehow along the way, they lost the paperwork in the office. Because they did that, I had to now wait … thank God I took pictures of it and everything but it was a real pain in the ass.”
51-year-old, White female(Pennsylvania)
Even among participants who successfully renewed their coverage, they reported problems with notices and other communications from the states as well as challenges getting through to call centers. Most participants who renewed their coverage said the notices they received were mostly clear and somewhat easy to understand; however, some participants complained that the notices contained duplicate information or used “legalese” that was not so easy to understand. Others noted it is difficult to distinguish between important renewal notices and other mailings they often receive about Medicaid. Several participants noted sometimes they receive renewal notices very close to the deadlines to submit the required forms. These enrollees said that getting the notices earlier to allow more time to respond would help to avoid gaps in coverage. And, when it comes to calling the Medicaid agency, while most participants who called said they were able to get the help they needed from Medicaid call centers, several agreed that it was necessary to call first thing in the morning to get their calls answered. Otherwise, wait times would be hours and sometimes calls were not answered at all. Some also noted that calling earlier in the day often meant getting more knowledgeable staff who could more easily resolve their issues.
“They’re [the notices] fairly easy to understand. Sometimes they have a little bit too much sort of legalese, the jargon is just a little bit too heavy on that … I feel like some of it could be clearer.”
63-year-old, Black female(Arizona)
“Maybe send a letter out maybe 60 days prior to renewal so that you’re not losing those benefits, because they want you to apply like 30 days prior to the expiration date. Sometimes they get backed up and you’re at risk, not the person that’s processing your documents.”
33-year-old, Black female(Florida)
“If you’re not like on the phone calling consistently like 10, 15 sometimes 20 minutes prior to them calling, so that you can be one of the first people to be answered, you might as well wait until the next day to call. Because I’ve waited longer than two hours before, and still have not had my phone call answered. The phones still hadn’t been picked up.”
26-year-old, Black female(Florida)
“Sometimes, I even use the automated system on my phone just to call, and it’s really convenient to call and it’s fast. “
33-year-old, Hispanic female(Arizona)
Experience Among Enrollees Who Were Disenrolled
Participants who were disenrolled lost their coverage for a variety of reasons, including being no longer eligible, though some who thought they were still eligible did not know why they had been disenrolled. Some participants were disenrolled for procedural reasons related to missed notices and systems issues. In some cases, participants said they did not receive renewal notices and were not aware they had been disenrolled, but in one case, a participant missed the renewal notice because it came outside of her normal renewal period and she did not realize she needed to respond to maintain her coverage. Another participant described ongoing problems trying to update his address and lost coverage because the notice was sent to the old address. Others were found ineligible due to increases in their income. While some generally understood why they had been disenrolled, others said they were confused as to why they lost coverage. In one case, a woman was disenrolled shortly after giving birth despite being told she would have postpartum coverage for one year.
“I feel like I missed it because it wasn’t my normal renewal date, and I didn’t think that’s what it was … Because it wasn’t the time that I would expect the renewal to be. That’s probably why I skipped over it.“
43-year-old, Black female(Florida)
“When I go in the Compass Account it says; my case is closed, and then it still has my previous address, that I’ve made multiple, you know attempts [to update my address]. And because it’s not changed to a different office I can’t log into the correct account.“
29-year-old, White male(Pennsylvania)
“I actually never went through the renewal application … I just did the calculations and realized that I wouldn’t qualify so I didn’t go through with the application.”
25-year-old, White female(Pennsylvania)
“You get [Family Support Services] telling you that you, a woman who has a child, they should be covered for one year. Then when you talk to somebody else it’s three months; so it’s just been one confusing mess. She got dropped right when she had the baby … I just don’t understand it.“
50-year-old, White female, speaking on behalf of her children(Florida)
“It’ll be nice if the notice came earlier and just kind of more clear on the criteria.“
34-year-old, White male(Arizona)
Many who were disenrolled encountered an array of communication problems. A common theme among those who were disenrolled is that they faced challenges receiving and understanding notices and had difficulties contacting Medicaid to try and have their coverage reinstated. In addition to not receiving or missing notices, several participants complained that they did not know why they or a family member had been disenrolled. In several cases, participants said they did not receive a notice to renew their coverage or a notice indicating their coverage had been terminated and did not realize they had lost their coverage until they went to fill a prescription or went to see a provider. Others claimed to have gotten incorrect information from Medicaid agencies when they called to ask about their coverage. For several, the communications problems persisted when they sought to appeal the agency’s decision. Information on how to continue benefits during an appeal, what steps were involved in appealing the decision, and information on what to expect during the fair hearing once the date was set were either not clear or not provided at all.
“We basically got terminated from Medicaid for no reason. You know just got cut off … we didn’t get called, we didn’t get [a] notice.”
43-year-old, White female(Florida)
“When I went for my prescriptions they were like, you don’t have insurance. I’m like well what are you talking about, I have insurance, I got my prescriptions last month.”
45-year-old, White female(Pennsylvania)
“I did think I would get some kind of notice … we got no notice, we had no idea [her son had been disenrolled]. So I was scrambling to try to find him something, because … he needs his meds, he needs his services.”
65-year-old, White female, speaking on behalf of her 28-year-old son(Florida)
“They [Medicaid agency] said he’s on until May 31st 2024. I waited 10 days and called back just to be sure. He’s on till May 31st 2024. I go June 1st to get his insulin from the pharmacy and he has no Medicaid.”
71-year-old, White female, speaking on behalf of her 19-year-old grandson(Florida)
“I’m going to have a hearing … I got a packet saying what all was gonna happen. I didn’t get the packet like that the first time. And they claimed that your address changed, no, my address didn’t change, nothing has changed; I just didn’t get that letter.”
64-year-old, Black female(Arizona)
While some participants who were disenrolled were able to reenroll in Medicaid quickly, others faced gaps in coverage. A few participants who realized they missed their renewal date were able to reapply and reenroll in Medicaid within a month of being disenrolled. However, others had to reach out multiple times to their Medicaid agency or turn to a local advocacy group to get help getting their coverage reinstated. These participants faced longer gaps in their coverage because of their temporary disenrollments. Others were not able to get their Medicaid reinstated despite believing they or their family members were still eligible.
“The guy I had talked to through one of the 1-800 numbers, he was very nice, he’s like; I’m going to submit this to your caseworker … I didn’t think it would work, you know and he did it. Within 24 hours I had insurance again.“
45-year-old, White female(Pennsylvania)
“I went about like three, almost three months I’d say with a gap in the insurance, just because of the hassle trying to switch it [his address].“
29-year-old, White male(Pennsylvania)
“I talked to [local advocates] on the 23rd [of August], by the 25th his Medicaid was reinstated. Although, they didn’t notify me to sign up for a plan until the 29th. So, I don’t know what’s been paid for in August.”
65-year-old, White female, speaking on behalf of her 28-year-old son(Florida)
Some participants who lost their coverage have faced substantial out-of-pocket costs for medically necessary care or have gone without care because they could not afford it. Losing their coverage left participants scrambling to find ways to continue to access the medications and treatment they or their family members needed. While some were able to pay out of pocket temporarily for needed medications, many could not get the medications or care they needed because it was too expensive. This disruption in care was stressful, and in some cases, led to declines in physical or mental health. Some participants who lost their Medicaid coverage and took medications regularly to manage chronic health conditions were trying to stretch supplies they had left while they worked to have their coverage reinstated or obtain other coverage. But one participant who was speaking on behalf of her diabetic grandson was worried about what would happen if he was still uninsured when they ran out of insulin.
“At this point I was off my seizure meds for about a week, week and a half, you know dealing with this whole issue.”
45-year-old, White female(Pennsylvania)
“[My children] couldn’t go for their physical for school. They couldn’t get the dental appointments that I scheduled. The [behavioral] therapy stopped, so I couldn’t get [therapy] for my daughter who has autism, who needs her AD therapy.”
43-year-old, White female(Florida)
“I just had a baby and I think I was going through post-partum depression. So not being able to get that covered it was … it’s a period where I was down and depressed because I didn’t have that medication.“
21-year-old, White female(Florida)
“And then she was sick the other month … Urgent Care was $125 just to walk in the door … that’s where we found out she didn’t have insurance, and we ended up leaving.“
50-year-old, White female, speaking on behalf of her children(Florida)
“We just called around to pharmacies to find … the cheapest price [for her son’s medication] that we could find to be able to pay for it, because we couldn’t let that happen to him [go without medication] … It was about $150.“
65-year-old, White female, speaking on behalf of her 28-year-old son(Florida)
Participants sought one-on-one assistance from caseworkers and community-based organizations to help them try to regain Medicaid coverage. Some of the participants who were disenrolled had complex situations and ongoing and significant health and mental health needs. When they were unable to regain coverage on their own, they turned to legal aid and other community-based organizations for help. Several said they did not think they would have been able to resolve issues or navigate appeals without the help they received. A few participants with less complex situations were also able to get in touch with Medicaid agents who helped them regain coverage.
“I went to a program … they had an attorney that will work with you if you had any issues like with AHCCS or the state. I had to give them authorization to work on my case and that’s how I got in contact with the attorney that helped me. So somehow she pulled strings and I got my insurance back and then I was compensated for all the copays that I had paid for my medication.”
64-year-old, Black female(Arizona)
“She would do phone interviews with me once a week to get back on [Medicaid] and be a mediator and call on the third-party line, and we would try to do it together.”
50-year-old, White female, speaking on behalf of her children(Florida)
“It seems like it’s they bombard you with enough paper you can’t figure out what to do next; and like I say if I didn’t get the help I do, we’d be lost.”
71-year-old, White female, speaking on behalf of her 19-year-old grandson(Florida )
After losing Medicaid, some participants obtained coverage through the Marketplace or their employer, but others remained uninsured, resorting to accessing care at clinics with sliding scale payments. While most participants who were disenrolled had either regained Medicaid coverage or were actively trying to reenroll in Medicaid, some were able to transition to other coverage through their employer or through the Marketplace. People no longer eligible for Medicaid and without access to employer coverage should generally be eligible for subsidized coverage through the ACA Marketplace, though some may fall into the “coverage gap” in states that have not expanded Medicaid under the ACA. Those who obtained Marketplace coverage were generally satisfied with the monthly premiums, but one participant who enrolled in the plan offered by his employer said having to pay premiums and copayments were expenses he did not have with Medicaid that he would now have to factor into his budget. Similarly, a participant whose children were transitioned to the state’s Children’s Health Insurance Program (CHIP) expressed frustration at having to pay a monthly premium that felt unaffordable on an already tight budget. Some participants became uninsured—one because her postpartum coverage was terminated although she is still eligible and she had not been able to get her coverage reinstated, and another who could not find plans with affordable premiums in the Marketplace. Those who became uninsured said they would use sliding fee scale clinics to access needed care or would rely on churches and other charity organizations to help pay for medications.
“It’s like an income-based, it’s basically a clinic … So it’s not good, I’m not going to say it’s bad healthcare, but it’s not, I mean everybody is going there. Everyone is going there because everyone’s in-between.”
50-year-old, White female, speaking on behalf of her children(Florida)
“It’s a burden, like who can afford KidCare? I was like, I’m barely paying my rent … you really want me to pay KidCare?”
43-year-old, White female(Florida)
“I’d go to the Lutheran Church and I tell them; hey guys, I need you to pass the hat … Next thing I know we have a new meter and we have strips and one of the guys at church, and they won’t tell me who has Amazon sending us a hundred strips a month. That’s not enough for him to be tested six times a day, but, still that’s a lot of help.“
71-year-old, White female, speaking on behalf of her 19-year-old diabetic grandson(Florida)
“I was able to roll onto Pennie and so my monthly premium is I think $3.70 … I’m really pleased with it so far. I’ve been on it for just about a month and a half now, but so far it’s been a really easy transition.”
25-year-old, White female(Pennsylvania)
“I got [insurance] through my employer, Blue Cross Blue Shield, that’s what I have right now … that’s just a bill I’ve never had, but now I have to pay, so yeah just have to factor it in now.”
34-year-old, White male(Arizona)
“I started getting calls from Marketplace and they said … $800 is what I would have to pay, so that just went in one ear and came out another.”
64-year-old, Black female(Arizona)
Consequences of Losing Medicaid Coverage
Losing Medicaid coverage could have significant consequences for the ability of participants to maintain their physical and mental health. Across all groups, participants said that losing Medicaid would be devastating and would prevent them from being able to continue to access the prescriptions or treatments they need. Participants stressed that the prescriptions and treatments covered by Medicaid are “lifesaving;” they believed that losing Medicaid would cause a serious decline in their physical and mental health and expressed anxiety at the thought of no longer having Medicaid coverage for themselves or their children.
“My son who is diabetic, he would probably be dead, because his medication is like 800 dollars a month and he has to see a doctor every other month.”
38-year-old, White female(Arizona)
“My son goes to counseling, so that would stop … My daughter has asthma, so there is a potential, you know, serious complications that could come with that.”
33-year-old, Black female(Pennsylvania)
“If I don’t have access to the medication that I need, to the prescriptions that I have; then it’s like significantly life altering in a very bad way … I just feel like it’s important to convey that having a way for low-income-people to access healthcare is absolutely essential.”
39-year-old, White individual(Arizona)
“I’ve got some cardiac issues and dental issues, and so it would mean a lot. It would … just cause some mental health issues, because I would start getting worried about those kind of things like that. So, and my health, physically [and] mentally, might decline.”
57-year-old, White male(Pennsylvania)
“For me it would be just kind of a scary process because as you get older, it’s just more things that go on, and it’s like playing Russian Roulette if you don’t have insurance. You’re just kind of out there, you know, at any point you might have to go to the hospital; you know it’s just a lot of different possibilities … So, it would be kind of a lot of anxiety.”
63-year-old, Black female(Arizona)
Looking Ahead
As states continue the process of redetermining eligibility for the over 94 million people who were enrolled in Medicaid at the start of the unwinding period, the experiences of focus group participants highlight both where processes are working well, but also where policies and systems create barriers to completing the renewal process and maintaining coverage for those who remain eligible. Providing multiple ways for people to complete their renewal, including through online accounts, as well as communicating early and clearly and through more than one mode about actions enrollees need to take can help ensure they complete the renewal process within the specified timeframes. Additionally, improving access to call centers for those who have questions or need assistance and connecting those who have been disenrolled to resources and in-person assistance may help to promote continued coverage through Medicaid or seamless transitions to other coverage.
Participants in these groups and across the Medicaid program have a broad range of health care needs, and Medicaid provides comprehensive coverage with no or low out of pocket costs. Without Medicaid or other coverage, many individuals could face severe health and financial consequences. Addressing the barriers to maintaining Medicaid coverage for those who remain eligible and facilitating enrollment into other coverage for those who are no longer eligible could reduce the negative outcomes from experiencing gaps in health coverage or from losing coverage altogether.
Appendix