Key Points
- Major outbreaks of mpox – the infectious disease previously called monkeypox – are ongoing in a number of African countries, in particular the Democratic Republic of the Congo (DRC). In addition, several mpox cases linked to the DRC outbreak have now been identified in some non-African countries, including Sweden and Thailand. Due to these circumstances, in mid-August 2024, the World Health Organization (WHO) and the Africa Centres for Disease Control and Prevention (Africa CDC) each declared mpox to be a public health emergency requiring a globally coordinated response.
- This is the second time mpox has been declared an international emergency, with the first spanning 2022-2023. The current mpox outbreak centered in the DRC is being driven by the “clade I” strain of the virus, with a clade Ia variant that is primarily affecting children and a more recently identified clade Ib variant that is spreading primarily via sexual contact among adults. The previous international emergency was driven by a “clade II” strain, and primarily affected adult gay and bisexual men. Currently, there is ongoing transmission of both clades affecting mostly different geographic areas.
- The U.S. government has provided technical and financial assistance for mpox response in DRC and elsewhere for years. Following the emergency declarations it has increased this support, including by delivering 50,000 doses of mpox vaccine to the DRC and 10,000 doses to Nigeria, as well as providing $10 million in mpox response-specific funding. On September 24, President Biden also pledged to donate up to 1 million more vaccine doses and an additional $500 million in funding to support mpox response across Africa.
- Since the emergency declarations, the Africa CDC, WHO, and governments of affected countries have accelerated efforts to respond to the situation by developing updated response plans, mobilizing more funds and attention from policymakers, and working to obtain more mpox vaccine doses. Still, the response faces a number of challenges including an uncertain path to delivering mpox vaccines at scale, lack of access to prevention tools, poor health infrastructure in many affected areas along with ongoing conflicts and instability, and high levels of distrust and misinformation in affected communities.
- No cases of clade I mpox have been identified in the U.S. as of September 26, 2024, and the CDC estimates the risk to the general public in the U.S. from the current outbreak in African countries is very low. However, clade II mpox infections continue to occur in the U.S. primarily among adult gay and bisexual men, though case numbers have declined since the previous mpox emergency in 2022-2023.
Introduction
Major outbreaks of mpox are again raising significant international concern. The DRC in particular has reported a large increase in cases driven by the “clade I” strain of the mpox virus, including a “clade Ia” variant that is primarily affecting children and a more recently identified “clade Ib variant” that is spreading primarily via sexual contact among adults. Clade I cases are also being reported in some other African nations, and several cases of the clade Ib variant have now been identified in non-African countries. At the same time, there continue to be mpox cases caused by “clade II” mpox, which was the variant that led to an earlier public health emergency in 2022-2023 in many different regions and countries around the world, including in the U.S. The recent circumstances led to two public health emergency declarations: the Africa Centres for Disease Control and Prevention (Africa CDC) declared mpox to be a “public health emergency of continental security” (PHECS) for Africa on August 13, 2024, and the WHO Director-General declared the mpox outbreaks a “public health emergency of international concern” (PHEIC) on August 14, 2024.
This explainer answers key questions about the international response to date, including the U.S. government’s role globally, and identifies issues and challenges that may affect the response going forward. It also discusses how the global emergency might affect the U.S. and the current status of mpox circulation within the U.S. It will be updated as needed.
Key Questions
What is mpox?
Mpox is a disease caused through infection with the mpox virus (MPXV). The first human case of mpox was identified in 1970, and since then, the virus has caused intermittent outbreaks. It is considered endemic in several Central, East, and West African countries, where infections have traditionally occurred through exposure to rodents or other animals carrying the virus. Human-to-human spread is also possible, primarily through close contact such as skin-to-skin contact and sexual or other contact with infected body fluids. Mpox can also pass from mother to fetus during pregnancy and during or after birth. Mpox infections can lead to symptoms such as fever, headaches, and body aches, and the development of a rash with lesions. Some infections can cause severe illness and even death, and there is a higher risk for severe outcomes in those with weaker immune systems such as people with HIV who are not virally suppressed and children. In areas with poor health care infrastructure and a lack of access to prevention tools, testing, treatment, and supportive care, mpox can be more difficult to identify, treat, and contain.
In recent years, more sustained human-to-human transmission and larger mpox outbreaks have been recorded from two genetic families of mpox virus (known as clade I and clade II mpox viruses; see Box 1). Most notably, in 2022, an outbreak of clade II mpox virus emerged from West Africa and spread globally, eventually affecting more than 100 countries and causing over 100,000 reported cases, including over 30,000 cases in the U.S. alone. That global outbreak was declared a PHEIC by WHO between July 2022 and May 2023 , and also declared a public health emergency in the U.S. in August 2022, marking the first time mpox had become a significant public health threat in non-endemic countries. Adult gay and bisexual men, especially men of color, made up the vast majority of cases during that outbreak in the U.S.
Strains of mpox virus (MPXV) from both clades have continued to circulate in largely geographically separate sets of endemic African countries, with clade II mpox infections primarily found in West African and Southern African countries and clade I infections found in Central African countries, the DRC in particular. In addition, clade II infections continue to be identified in many countries outside endemic regions, including in the U.S., primarily in gay and bisexual men, though the number of reported cases has declined significantly since the 2022 global outbreak.
Box 1: Epidemiology of Mpox Virus (MPXV) Clades I and II
There are two main genetic families of MPXV, known as clade I and clade II, and each clade is divided into sub-clades (clade Ia, clade Ib, clade IIa, and clade IIb) based on genetic similarities and differences.
Historically, clade I MPXV infections have been identified primarily in Central African countries, the DRC in particular, while clade II MPXV infections have been identified primarily in West African countries. In 2022, clade II MPXV emerged from West Africa to cause a global outbreak, primarily spread via sexual contact among adult gay and bisexual men. While that outbreak subsided following its 2022 peak, new cases of clade II MPXV infection continue to be reported in a number of countries worldwide, including African countries and the U.S.
In recent years, clade Ia and clade Ib MPXV have been circulating concurrently in the DRC and in Africa, and some clade Ib infections have also been identified outside of Africa:
- Clade Ia MPXV: Infections continue to occur mostly in central DRC, affecting children exposed to infected animals with some additional ongoing human-to-human transmission due to close contact among family members or caregivers.
- Clade Ib MPXV: First described in 2023; infections have been found primarily in eastern DRC and neighboring African countries. This includes several countries reporting mpox cases for the first time ever, such as Burundi, Kenya, Rwanda, and Uganda. In areas affected by clade Ib, the majority of cases have occurred in adults and transmission appears to be sustained “largely, but not exclusively, through transmission linked to sexual contact and amplified in networks associated with commercial sex and sex workers.”
Available data suggest clade Ia MPXV infections are more likely to be severe cases and cause deaths than infections from clade IIa or clade IIb MPXV. While there is limited data on the severity of clade Ib, early indications are that it may not be as severe as clade Ia. Still, more data and studies are needed to fully understand the extent of biological and epidemiological differences across mpox sub-clades.
Why has mpox again been declared a public health emergency this year?
WHO and Africa CDC issued the emergency declarations due to the recent rapid rise in case numbers and expanded geographic reach of mpox. Of primary concern has been mpox in the DRC. In 2023, the DRC reported more than 14,000 suspected cases (three times as many as in 2022) and over 500 deaths from mpox. In 2024, these trends have accelerated, and in only the first half of this year, the country has reported over 14,000 suspected cases across 23 different provinces, with over 450 deaths. Children have been heavily affected in the DRC outbreaks, with an estimated 70% of mpox cases and 85% of mpox deaths in the country since 2022 occurring in children under 15.
Moreover, the emergence and rapid spread of a new strain of the mpox virus (known as clade Ib; see Box 1) that “appears to be spreading mainly through sexual networks” was first identified in eastern DRC in 2023 has not only caused a growing number of cases in the DRC, it has been found in a number of other countries in the region and outside Africa with one case detected in Sweden and one in Thailand. There are concerns that clade Ib virus may be more readily transmissible (including via sexual contact) compared to clade Ia, which could be contributing to the increased numbers of cases and the cross-border spread of the disease.
What has been the global response to the current mpox emergency?
Alongside its PHEIC declaration on August 14, WHO released $1.45 million from its Contingency Fund for Emergencies to help scale up the response in affected countries. On August 26, WHO issued a Global Mpox Strategic Preparedness and Response Plan (SPRP) that outlined a set of global, regional, and country level response steps and needs to address the spread of clade Ib in eastern DRC and to control outbreaks of clades I and II in the DRC and other African countries. The plan emphasized the need for better mpox surveillance, strengthening clinical care for the disease, more global cooperation to increase vaccine access, implementation of strategic vaccination efforts in populations at highest risk, and public health communication efforts and community empowerment.
Along with its declaration on August 13, Africa CDC requested $20 million for immediate mpox response needs (and reported it had been granted $10.4 million) from the African Union, and initially requested an additional $16 million from WHO and other international partners for a continent-wide response. The Africa CDC and WHO also launched a joint plan, the Mpox Continental Preparedness and Response Plan for Africa, covering the September 2024 through February 2025 period identifying the following:
- 10 “pillars” for the continental response including coordination and leadership, case management, vaccination, and logistics and financing;
- roles and responsibilities for the primary international organizations involved in the response, including Africa CDC, WHO, Gavi, the Vaccine Alliance, and UNICEF;
- the need for approximately $600 million to address the outbreak on the continent during the plan period (with 55% to be allocated to the mpox response in 14 affected countries and to boost readiness in 15 other countries at risk and 45% to be allocated to operational and technical support through partners), calling on donor governments, philanthropic organizations, and the private sector to provide this funding. Recent pledges from the U.S. and other donors totalled
In addition, Africa CDC activated its Public Health Emergency Operations Centre (PHEOC), initiated negotiations with pharmaceutical manufacturers and others to obtain mpox vaccines for use in outbreak response on the continent (see Box 2 for more on mpox vaccines), began supporting laboratory testing capacity building for mpox, and deployed epidemiologists to affected areas, among other activities.
Are mpox vaccines available, and are they getting to affected countries quickly?
There are several vaccines that can be used to prevent mpox (see Box 2). Africa CDC and WHO consider vaccines to be a key prevention tool for the response, and the joint Africa CDC and WHO continental response plan calls for enough vaccine doses to vaccinate 10 million people in African countries from September 2024 through February 2025. However, there are a limited number of vaccine doses available other than those already stockpiled by high-income countries.
Some high-income countries have agreed to donate vaccine doses from their existing stockpiles in support of the global response. For example, the European Commission announced a donation of 175,000 doses to Africa CDC, and Japan agreed to donate up to 3.5 million doses for response in the DRC. The U.S. has pledged to provide 1 million doses for the response, and has already delivered 50,000 doses to the DRC and 10,000 doses to Nigeria (see more on the U.S. role in mpox response below). In addition, Bavarian Nordic, the company that manufactures one of the mpox vaccines, pledged to donate 40,000 of the doses it has on hand to the DRC and to ramp up production of more doses for use in African countries in the coming months. Taken together, donors have pledged to provide a total of over 5.4 million doses of mpox vaccine for this response, according to WHO.
UNICEF and Gavi are also assisting in the process of acquiring vaccine doses and implementing vaccination in affected areas. Gavi announced it would redirect $2.9 million in funding to support mpox vaccinations in the DRC, and also is talking with vaccine manufacturers to help purchase doses directly, using funds drawn from its First Response Fund. Gavi is also helping coordinate the delivery of donated vaccines to countries in need. UNICEF reports that it is providing vaccination supplies and logistics support, health worker trainings, transportation, storage, and vaccine administration in the country.
As of September 24, 2024, 250,000 doses – 200,000 doses from the European Commission and Bavarian Nordic, along with the 50,000 doses from the U.S. – have arrived in the DRC. However, this is just a small fraction of the over 3 million doses that health authorities say are needed in the country in the near term. The DRC government announced it expects mpox vaccinations to begin in the country in the first week of October.
In other nearby countries reporting recent clade I mpox cases (such as Burundi, Rwanda, and Uganda), there is little information so far about if mpox vaccines will be provided in-country and when vaccinations may begin.
Box 2: Mpox vaccines and the international response
There are three vaccines, initially developed for smallpox prevention, that are considered effective in preventing mpox infection:
- MVA-BN: Also known under the brand names Jynneos, Imvamune, and Imvanex, it is manufactured by Bavarian Nordic in Denmark and licensed by a number of countries for use in adults for the prevention of mpox.1 The MVA-BN vaccine is administered in a two-dose series.
- ACAM2000: Manufactured by Emergent in the U.S., it has been made available for mpox prevention in adults under expanded access by the FDA in the U.S. The ACAM2000 vaccine is administered as a single dose.
- LC16m8: Manufactured by KM Biologics in Japan, it has been licensed by Japan for smallpox prevention in children and adults and authorized by Japan for use against mpox since 2022. The LC16m8 vaccine is administered as a single dose.
Africa CDC has primarily focused on acquiring MVA-BN and LC16m8 doses for African countries, and estimates that enough doses to vaccinate 10 million people on the continent are needed.1 In the U.S., a 2022 emergency use authorization issued by the FDA allows for the use of MVA-BN (JYNNEOS) vaccine in children and adolescents under some circumstances. WHO representatives have stated that the same vaccine could be used “off label” to vaccinate children and adolescents on the African continent during the current emergency response.
What assistance has the U.S. provided to the DRC for mpox response?
The U.S. government has long provided support to help DRC address mpox. For example, CDC has supported mpox research and response efforts in country for decades. Over the last few years, U.S. support for mpox response has included efforts to build laboratory testing capacity in-country, conduct mpox vaccine research, and training health care workers.
With the growth in mpox cases in the DRC and the emergency declarations from Africa CDC and WHO, the U.S. government has announced a number of additional actions. This includes a U.S. commitment to provide over $55 million in emergency health assistance through USAID and the U.S. CDC for mpox response in DRC and other affected countries in Africa, including $10 million in additional funding announced in August specifically for clade I mpox response efforts. Also, the U.S. donated 10,000 doses of mpox vaccine to Nigeria in August and delivered 50,000 doses of mpox vaccine to the DRC in September, along with additional support for vaccine delivery.
On September 24, President Biden stated the U.S. would increase its support over the coming months, and expects to provide over $500 million in additional assistance for the mpox response in African countries as well as donate as many as 1 million mpox vaccines in support of the response.
Besides its mpox-specific support, the U.S. government has also long provided significant amounts of global health and humanitarian assistance to the country, and recently stated it would be expanding assistance for broad humanitarian efforts in the DRC.
What are key challenges in responding to the current mpox emergency?
Addressing the current mpox emergency in the DRC and other affected countries in Africa poses a number of challenges, including:
- Limited testing, surveillance, and epidemiological capacity. There is a lack of point of care testing and laboratory capacity in many affected areas, which means many suspected cases of mpox may be undiagnosed and suspected cases unconfirmed. This is particularly true in regard to genomic sequencing. This hampers epidemiological investigations and leaves many questions unanswered about the current state of mpox in the DRC and elsewhere. More testing and epidemiological information on modes of disease transmission, risk factors, and disease severity associated with the different MPXV clades, as well as outcomes of pregnancy in women infected with different MPXV clades, would help authorities target response efforts.
- Difficulties with obtaining and distributing mpox vaccines at scale. There is currently a limited global supply of mpox vaccines, with many of the existing doses found only in national stockpiles of high-income countries so the response relies in large part on donations. Also, there is a lack of formal authorization to use these vaccines in a number of the affected countries in Africa and little data on the effectiveness of these vaccines against clade I mpox or their effectiveness in children. A new, large-scale vaccination campaign to reach the populations at greatest risk for mpox is also a challenge.
- Stigma and overlapping risks of mpox and HIV infection. There are relatively high rates of HIV infection in some mpox-affected countries in Africa, which raises concerns about the potential overlap in risks between these infectious diseases. Unsuppressed HIV infection could raise the risk for mpox transmission, especially in the context of sexual contact, and for development of more severe outcomes from mpox infection. In addition, both infections can lead to stigma for those affected, making the response more challenging. Therefore, ensuring public health authorities plan to address HIV and mpox in a coordinated fashion will be important.
- Health systems and health care workforce. Lack of access to health care and a limited health care workforce increase risks from mpox for individuals and communities. Linking mpox cases to health care services as early as possible and ensuring the health care workforce is adequately trained and supplied to address mpox improves outcomes.
- Travel restrictions. To date, countries have not put into place harsh restrictions on travel to and from areas affected by this mpox emergency. However, if the outbreak worsens and spreads to more countries, there is the potential for countries to impose travel bans or other restrictions, as has occurred during past outbreaks. There is little evidence to support the effectiveness of such restrictions in interrupting international transmission of mpox.
- Competing priorities amid instability, conflict, and community distrust. Many of the affected countries – the DRC in particular – face multiple simultaneous humanitarian crises, health emergencies, and other urgent issues in addition to mpox. This makes focusing attention on and implementing a response to mpox more challenging, especially in the context of limited resources. For example, in some affected areas in the DRC, there is a history of instability and conflict and an ongoing lack of trust in authorities in many communities, which complicates response and risk communication efforts particularly those focused on reaching the most at-risk populations.
How might this latest outbreak affect people in the U.S.?
Although cases of mpox due to clade II infections continue to occur in the U.S. (see below), so far no cases of mpox due to clade I infections – the genetic family linked to the current DRC outbreak – have been identified in the U.S. The U.S. CDC estimates that the risk to the general public from the current mpox outbreak in African countries remains very low. The CDC also estimates there is a low to moderate risk from the current DRC-based clade I outbreak for U.S. gay, bisexual and other men who have sex with men (MSM) who have more than one sexual partner as well as for people who have sex with MSM, regardless of gender, particularly if there is a history of travel to any of the African countries affected in the current mpox emergency.
In light of the evolving mpox situation in parts of Africa and the potential risk of imported cases, CDC has issued a travel warning for the DRC and has issued several health alerts for U.S. clinicians, which provide guidance on prevention strategies and also suggest a “heightened index of suspicion” for mpox in patients recently arriving from affected areas in Africa who demonstrate signs and symptoms consistent with the disease.
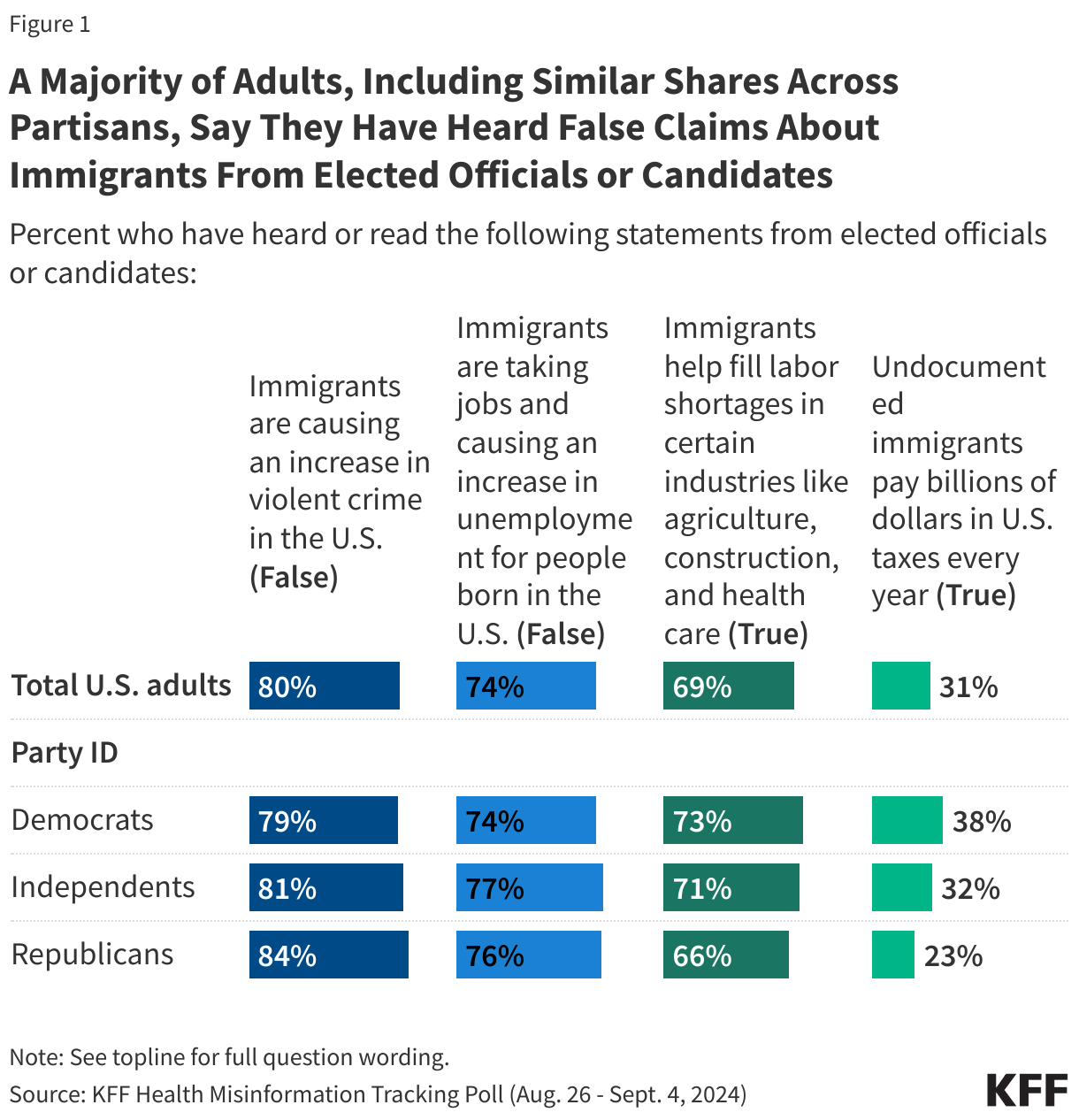
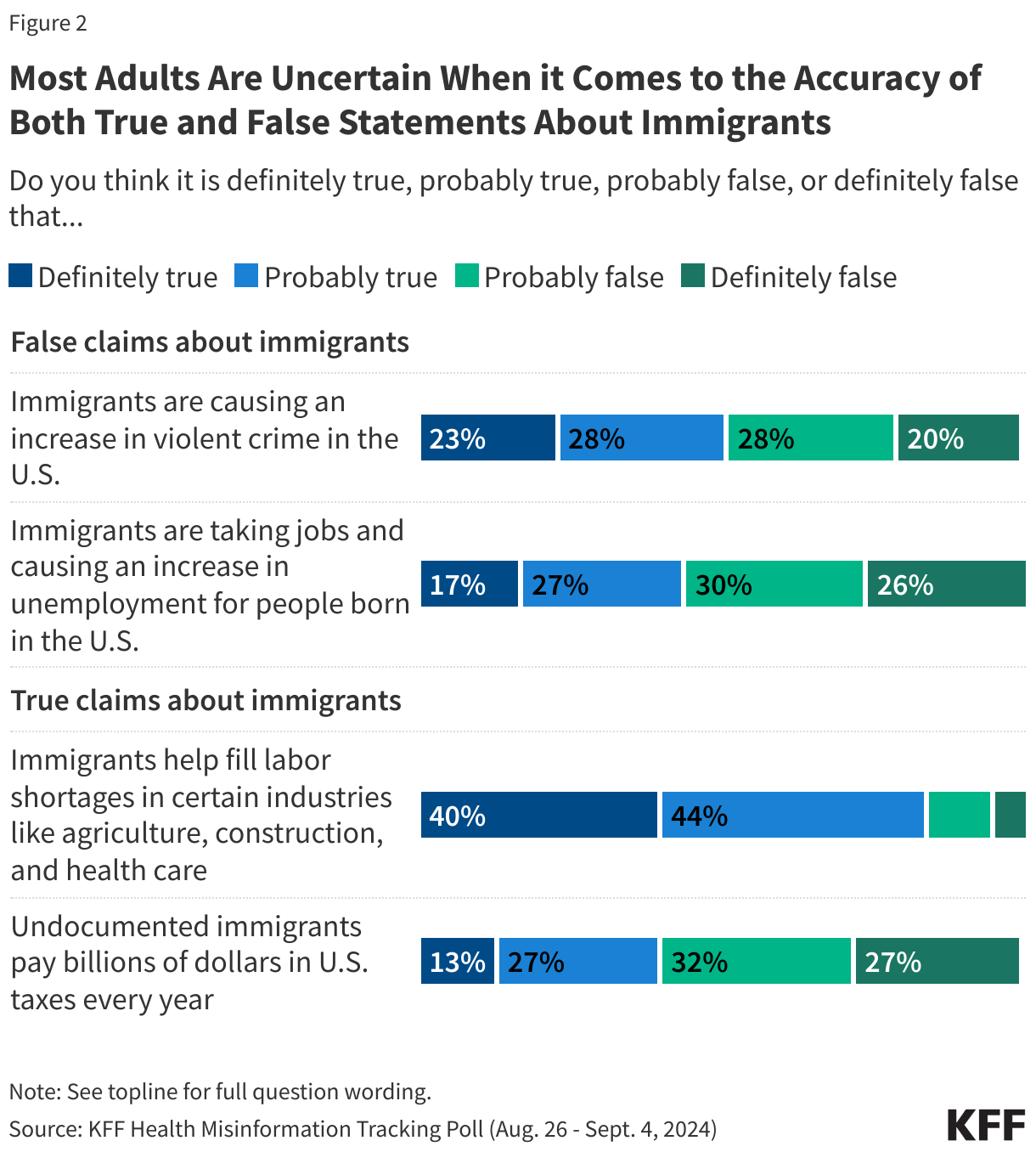
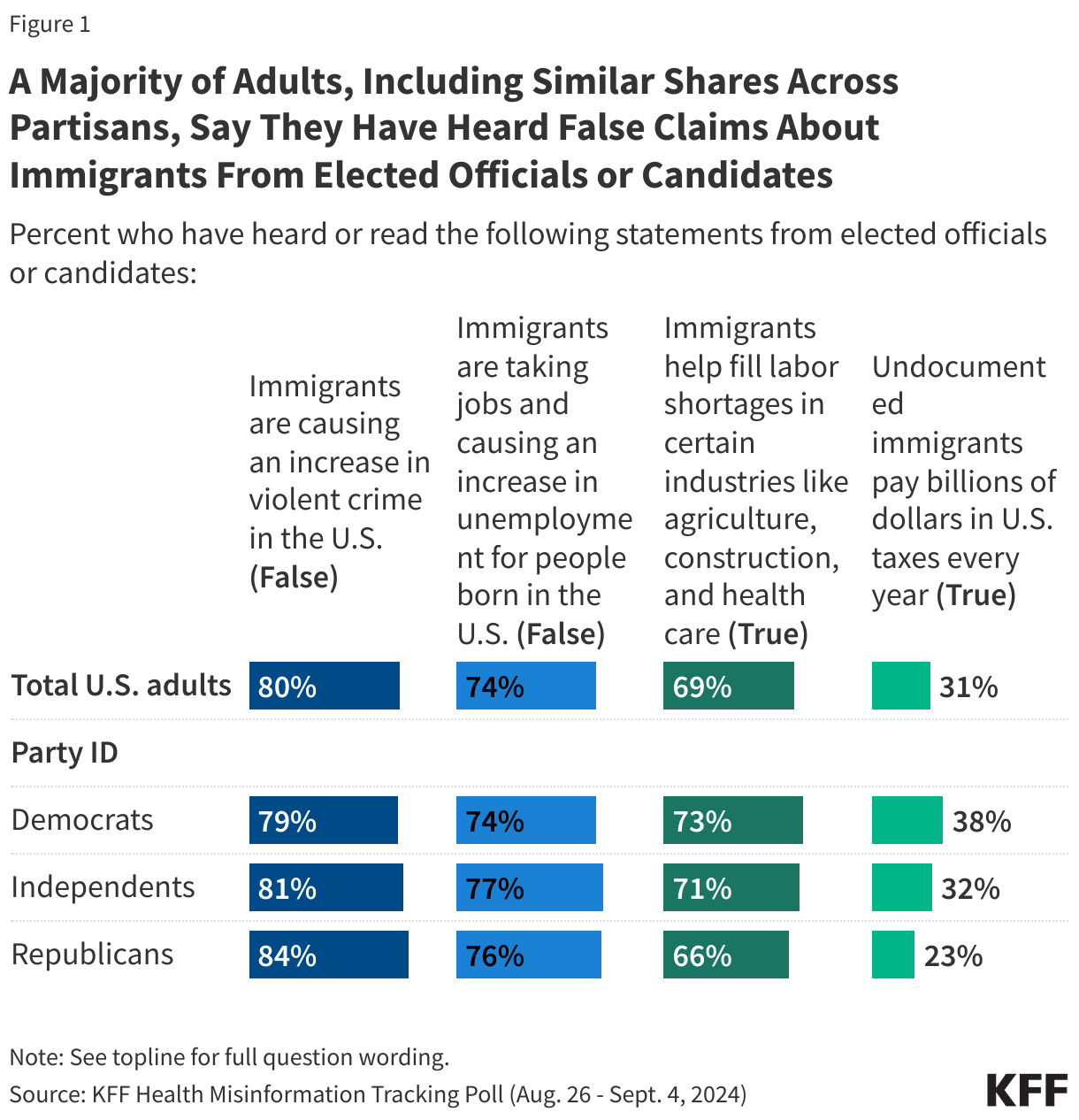
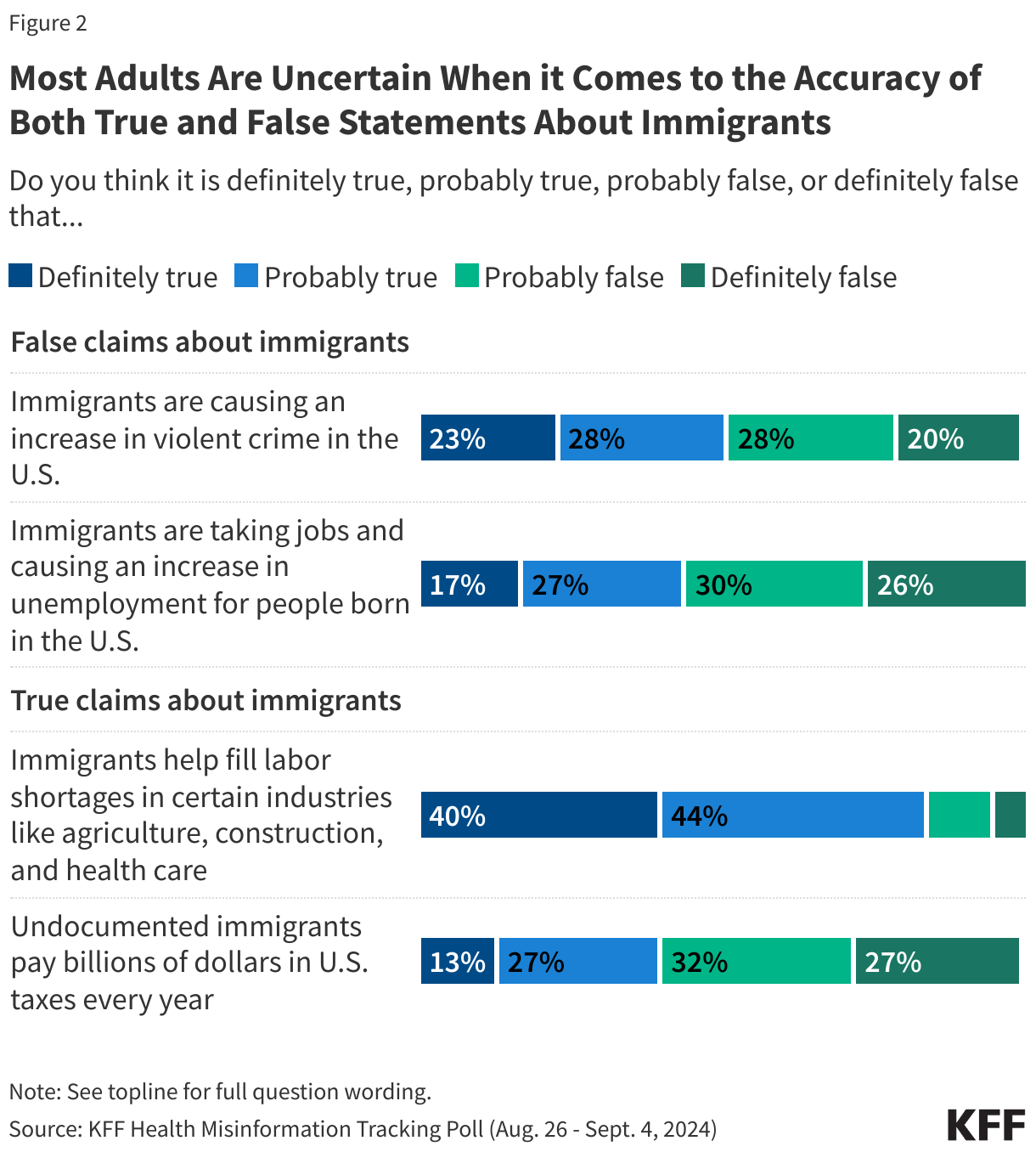
Given the rise in anti-immigrant rhetoric and a history of charged debates about travelers entering the U.S. during health emergencies, there is the potential for mpox to become politicized this election year, especially if cases linked to the ongoing outbreaks in Africa are eventually identified in the U.S.
What is the status of ongoing mpox circulation in the U.S.?
As mentioned above, in 2022-2023, the U.S. had over 30,000 mpox cases during the global outbreak of clade II mpox, which had initially emerged from West African countries. While case numbers have declined in the U.S. since 2022, some clade II mpox cases continue to be identified, with CDC reporting 1,968 mpox (clade II) cases so far this year nationwide as of September 1, 2024. These cases have primarily occurred among adult gay, bisexual and other men who have sex with men (MSM) who have multiple sexual partners, especially men of color and with people with HIV being disproportionately impacted. According to CDC, during the peak of the epidemic in 2022 over 99% of mpox clade II cases in the U.S. occurred among men, and of those, 94% were among men who had sexual contact with other men.




 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma