Introduction
The U.S. Congress, the legislative body of the U.S. government (USG), plays an important role in determining and shaping the government’s global health policy and programs. Although only one of many USG entities involved in global health, its engagement has been particularly notable over the last 20 years, which have been marked by unprecedented bipartisan support for U.S. global health efforts and resulted in the authorization of the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), the U.S. government’s coordinated response to global HIV and the largest program focused on a single global health issue in the world, as well as the appropriation of significantly increased funding. It has also played a key role in the U.S. response to recent global health emergencies, including Ebola, Zika, and COVID-19 as well as increasing U.S. support for global health security and pandemic preparedness and response efforts. Indeed, Congress fulfills a key role in U.S. global health policy by setting the broad parameters and priorities of U.S. global health programs, determining their funding levels, and overseeing the implementation and effectiveness of supported efforts. Its activities in this area are complemented and influenced to varying degrees by those of numerous stakeholder groups and individuals that, while not examined in this primer, are key actors in the policymaking process. Such stakeholders include: advocates, the private sector, think tanks, academic institutions, religious communities and organizations, people directly affected by global health issues (such as people living with HIV), and others.
To help shed light on Congress’ role in global health, this primer provides an overview of its engagement in this area, aiming to provide a basic framework with which congressional efforts may be understood. First, it examines the structure of Congress and its role and key activities in global health, which range from authorizing the creation of and providing funding for U.S. global health programs to engaging in program oversight and confirming presidential appointees to lead these efforts. It then illustrates these by examining selected legislative activities for two global health examples: the creation and evolution of PEPFAR and the 2014/2015 Ebola outbreak in West Africa. Finally, it discusses opportunities and challenges related to congressional engagement in global health going forward.
Structure
Congressional engagement in global health is carried out by the two chambers of Congress – the U.S. House of Representatives and the U.S. Senate – and their members, committees, and caucuses. This work is supported by a cadre of congressional staff as well as legislative branch agencies and offices (e.g., the Congressional Budget Office (CBO), the Government Accountability Office (GAO), and the Congressional Research Service (CRS)).
Chambers
The U.S. House of Representatives (the House) and the U.S. Senate (the Senate) debate and vote on legislation, including legislation related to global health, among other activities. The House is the larger body, whose members represent 435 congressional districts, which are distributed across states based on population during the most recent census; House members are up for re-election every two years. The Senate has 100 members, two from each state, who are up for re-election every six years.
Members
Each chamber is made up of individuals who have been elected to serve as members of Congress for certain periods of time (see Box 1). Members’ engagement in global health may include a variety of actions, such as: sending official correspondence (e.g., to the Executive Branch or to congressional colleagues individually or via “Dear Colleague” letters1 ), speaking publicly and/or privately, participating in congressional delegations to the field, issuing press releases, introducing or co-sponsoring legislation, and, most importantly, voting on legislation. (It is important to keep in mind that legislation may be a product of negotiations with the Executive Branch.)
Box 1: The 117th Congress
Every two years, a new term of Congress is convened, initiating a new two year period of legislative activity. Each year within this period is a congressional session. The current Congress, known as the 117th Congress, was convened on January 3, 2021, and will end on January 3, 2023. Its membership is made up of the following:
- Representatives: 435 elected members2 of the House who serve two–year terms; all are up for election every two years.
- Senators: 100 members of the Senate who serve six-year terms; a third of senators are up for election every two years.
- Democratic majority in House and Senate: The House has 212 Republicans and 220 Democrats.* The Senate has 50 Republicans, 48 Democrats, and 2 Independents who caucus with the Democrats; Democrats hold the majority due to the tie-breaking vote of the Vice President, a Democrat.
- Members who are: women (147); African-Americans (57); Hispanic or Latino (54); of Asian, South Asian, or Pacific Islander ancestry (21); American Indian (Native American) (5).*
- Members who served or are serving in the U.S. military: 91.*
NOTES: * As of Aug. 5, 2021; at that time, there were three vacant seats in the House, and additionally, four delegates are Democrats, and one delegate and the Resident Commissioner of Puerto Rico are Republicans.SOURCE: CRS, Membership of the 117th Congress: A Profile, Aug. 5, 2021 update.
Committees
Within each chamber, the work of Congress is generally performed by smaller groups of members, known as committees. Committees examine issues under their jurisdiction and may also consider and vote on legislation. Passage of a piece of legislation by a committee allows it to be brought before the chamber as a whole. Currently, the Senate has 16 standing (permanent) committees and four select and special committees, which may be permanent or temporary and typically “examine emerging issues that do not fit clearly within existing standing committee jurisdictions or cut across jurisdictional boundaries.” The House has 20 standing committees and five select committees.3 Additionally, there are four joint committees of the House and Senate, which are permanent, bicameral entities that do not consider legislation but rather carry out studies and certain administrative functions for Congress. Although the organization of committees in each chamber is rooted in a 1946 law that originally laid out similar committees in each chamber, the committee structure has evolved over time, leading to more variation across committees and chambers.4
There are more than ten congressional committees whose work relates to global health,5 although a smaller subset of six committees has primary jurisdiction over most global health programs and funding. These six are: the House Committee on Foreign Affairs (HFAC), the Senate Committee on Foreign Relations (SFRC), the House Committee on Energy and Commerce (E&C Committee), the Senate Committee on Health, Education, Labor, and Pensions (HELP Committee); and the House and Senate Committees on Appropriations (Approps. Committees). See Table 2 for an overview of jurisdiction by committee. Also see Appendix A for an overview of key committees and subcommittees’ leadership as well as a listing of members serving on these during the 117th Congress.
Caucuses
Members of Congress may also establish formal or informal groups of members, known as caucuses, focused on specific topics.6 Caucuses may be bipartisan (drawing their membership from both Democrats and Republicans) and bicameral (including members from both chambers), but they do not have to be. Among current caucuses, there are nearly 10 related to global health, including: the Congressional Global Health Caucus, the Congressional HIV/AIDS Caucus, the Tuberculosis Elimination Caucus, the Congressional Caucus on Malaria and Neglected Tropical Diseases, the Senate Caucus on Malaria and Neglected Tropical Diseases, the House Hunger Caucus, the Senate Hunger Caucus, and the COVID-19 Global Vaccination Caucus. See Appendix B for a listing of global health-related caucuses and their leadership during the 117th Congress.
Role and Key Activities
Congress is responsible for determining the broad outlines and priorities of U.S. global health efforts, providing funding for USG agencies and departments to carry them out, and overseeing the conduct and impact of these efforts. Congress fulfills this role through an array of activities, which generally fall under two broad umbrellas: introducing, considering, and passing legislation and carrying out oversight activities, including confirming presidential appointees to key USG global health positions.
Legislation
Legislation considered by Congress may be either a resolution or a bill, each of which serves different functions.7 These types of legislation are described below, and Table 1 provides several examples of global health-related legislation.
Resolutions
Resolutions often recognize or commemorate a person, day, or issue or express a position on an issue but generally do not become law (i.e., most are non-binding), though there are some that may be more similar to bills. For example, a resolution “recognizing the importance of sustained United States leadership to accelerating global progress against maternal and child malnutrition and supporting the commitment of the United States Agency for International Development to reducing global malnutrition through the Multi-Sectoral Nutrition Strategy” was passed by the Senate in 2020, as was a similar resolution in the House.8
Resolutions are generally one of three types: a simple resolution, a concurrent resolution, and a joint resolution. Simple and concurrent resolutions are used most often with regard to specific global health issues and have similar functions: A simple resolution usually expresses the sentiments of the chamber of Congress that voted for its passage, while a concurrent resolution also serves this function (as well as sometimes being used for congressional administrative matters) but is voted upon by both chambers. For example, the Senate passed a simple resolution on “supporting the goal and ideals of World Polio Day and commending the international community and others for their effort to prevent and eradicate polio” in 2014, while the House and the Senate passed a concurrent resolution to address a matter affecting the operation of both chambers, specifically correcting the enrollment (final agreed form) of a bill addressing U.S. global HIV, TB, and malaria activities.9 On the other hand, unlike the other two types, a joint resolution may have the force of law if it passes both chambers and is subsequently submitted to and signed by the President. In such cases, it is more similar to a bill. Joint resolutions, however, differ from bills in the ways in which they are used and with regard to the content they generally address: joint resolutions are often used to propose changes to current law that are relatively minor, temporary, or short-term in nature, and are also sometimes used to create temporary bodies or commissions. In general, joint resolutions are used less often with specific regard to global health and, rather, are used to address broader matters (like budget matters) that may impact global health.
Bills
Bills, which may become law if they pass both chambers and are subsequently submitted to and signed by the President, usually either function to authorize U.S. funding, programs, and activities or to appropriate U.S. funding for such programs and activities (see below).
| Table 1: Examples of Global Health-Related Legislation |
| Resolutions10 |
| Simple: A resolution designating the month of November 2005 as the “Month of Global Health”. Concurrent: A concurrent resolution to correct the enrollment of H.R. 1298. Joint: A joint resolution expressing the sense of the Congress with respect to international efforts to further a revolution in child health. Joint: Continuing Appropriations Resolution, 2015, which provided funding to respond to the outbreak of the Ebola virus in Africa, among other things. |
| Authorization Bills11 |
| Public Health Service Act of 1944 and Foreign Assistance Act of 1961: established the main agencies that carry out global health activities and specified where and how funds should be directed. International Health Research Act of 1960: provided for international cooperation in health research, research training, and research planning and also authorized the Secretary of the U.S. Department of Health and Human Services (HHS) to enter into international cooperative agreements for biomedical and health activities. Global AIDS and Tuberculosis Relief Act of 2000: helped lead to the creation of the Global Fund to Fight AIDS, Tuberculosis, and Malaria (an independent, multilateral financing entity designed to raise significant new resources to combat HIV, TB, and malaria in low- and middle-income countries) by directing the Secretary of the Treasury to enter into negotiations with other donors to establish a Trust Fund for AIDS at the World Bank. U.S. Leadership Against HIV/AIDS, Tuberculosis, and Malaria Act of 2003: authorized the creation of PEPFAR and provided for expanded U.S. government efforts to address global HIV, TB, and malaria by authorizing up to $15 billion in funding over five years (Fiscal Year (FY) 2004 – FY 2008) for efforts to address these diseases and for U.S. contributions to the Global Fund. Tom Lantos and Henry J. Hyde U.S. Global Leadership Against HIV/AIDS, Tuberculosis, and Malaria Act of 2008: reauthorized PEPFAR and provided for expanded U.S. global HIV, TB, and malaria efforts by authorizing up to $48 billion in funding over five (more) years (FY 2009 – FY 2013) for these efforts and for U.S. contributions to the Global Fund. PEPFAR Stewardship and Oversight Act of 2013: reauthorized PEPFAR for another five years (FY 2014 –FY 2018). Senator Paul Simon Water for the World Act of 2014: established the position of the Global Water Coordinator at USAID and outlines priorities for USG efforts that provide first-time or improved access to safe drinking water, sanitation, and hygiene (WASH) in developing countries. PEPFAR Extension Act of 2018: reauthorized PEPFAR for another five years (FY 2019 – FY 2023). |
| Appropriations Bills12 |
| Department of Defense (DoD) Appropriations Acts: provided funding for the first time to support DoD HIV research efforts in 1986 and DoD HIV prevention efforts among African militaries in 2001, effectively creating new DoD HIV efforts that today have a global reach. Supplemental Appropriations Act, 2010: provided $2.9 billion in emergency funding to support disaster relief and reconstruction efforts in Haiti after a major earthquake struck there in 2010. |
Authorization Bills
An authorization bill may lay out congressional priorities for global health programs, including approaches/strategies, focus countries, target groups (vulnerable populations), and targets (keeping in mind that legislation may be the result of negotiations with the Executive Branch). It may also broadly create and/or modify the policies and organization of USG global health efforts and drive support for the creation/growth of new global health organizations internationally. For example, the U.S. Leadership Against HIV/AIDS, Tuberculosis, and Malaria Act of 2003 (Leadership Act) authorized and institutionalized the President’s Emergency Plan for AIDS Relief (PEPFAR) program by: authorizing the expansion of U.S. global efforts to address HIV, TB, and malaria in low- and middle-income countries through U.S. bilateral assistance as well as U.S. contributions to the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund, which is an independent, multilateral financing entity designed to raise significant new resources to combat HIV, TB, and malaria in low- and middle-income countries); outlining PEPFAR’s organizational structure as a coordinated, whole-of-government response to global HIV, including establishing the position of the U.S. Global AIDS Coordinator; and defining the key priorities and policies of the program. Later, the Tom Lantos and Henry J. Hyde U.S. Global Leadership Against HIV/AIDS, Tuberculosis, and Malaria Act of 2008 (Lantos-Hyde Act) reauthorized these efforts for five more years and redefined the priorities and policies of the PEPFAR program. Additionally, as sometimes happens with legislation, the Act also included provisions (such as codifying the position of the U.S. Global Malaria Coordinator and requiring a five-year global malaria strategy) that had appeared in other proposed legislation.13 See the KFF brief on PEPFAR reauthorization.
An authorization bill may also define the period during which such activities may be operated and provide guidance on the amount of funding to be provided. Still, while specifying an authorized level of funding in an authorization bill may be indicative of congressional intent to appropriate funding at certain levels, funding is actually appropriated through appropriations bills, and Congress is not required to appropriate the level of funding that is authorized for a discretionary program (see Box 2 and further discussion below). In some instances, Congress may appropriate more funding than authorized (see Box 3), while in others, it may appropriate less. For example, in the Leadership Act of 2003, Congress authorized up to $15 billion for U.S. global HIV, TB, and malaria efforts, including bilateral assistance as well as U.S. contributions to the Global Fund, from FY 2004 through FY 2008, but ultimately, it appropriated nearly $19.8 billion for these efforts during that period.14 On the other hand, in the Lantos-Hyde Act of 2008, Congress authorized up to $48 billion for these same efforts from FY 2009 through FY 2013 but, ultimately, appropriated just under $37.2 billion for them during that period.15
Box 2: Discretionary and Direct (Mandatory) Spending
There are two types of spending (funding) that make up the U.S. federal budget: discretionary and direct; each type is subject to different processes and controls in the budget process.
Discretionary spending is provided through the annual appropriations process, which is a legislative process for determining the level of funding to be spent on certain U.S. government activities. Global health funding falls under this type, since U.S. government global health activities are discretionary programs.
Direct spending, also often referred to as mandatory funding, is generally provided outside of the annual appropriations process. This type mostly involves funding for entitlement programs, such as Social Security and Medicare, and interest payments on the U.S. national debt.16
Appropriations Bills
An appropriations bill provides funding for specific programs and activities. Because support for all U.S. global health programs is considered discretionary (versus direct – or mandatory – funding), funding is typically determined (appropriated) on an annual basis by Congress; see Box 2 for more information on these two different kinds of federal spending.
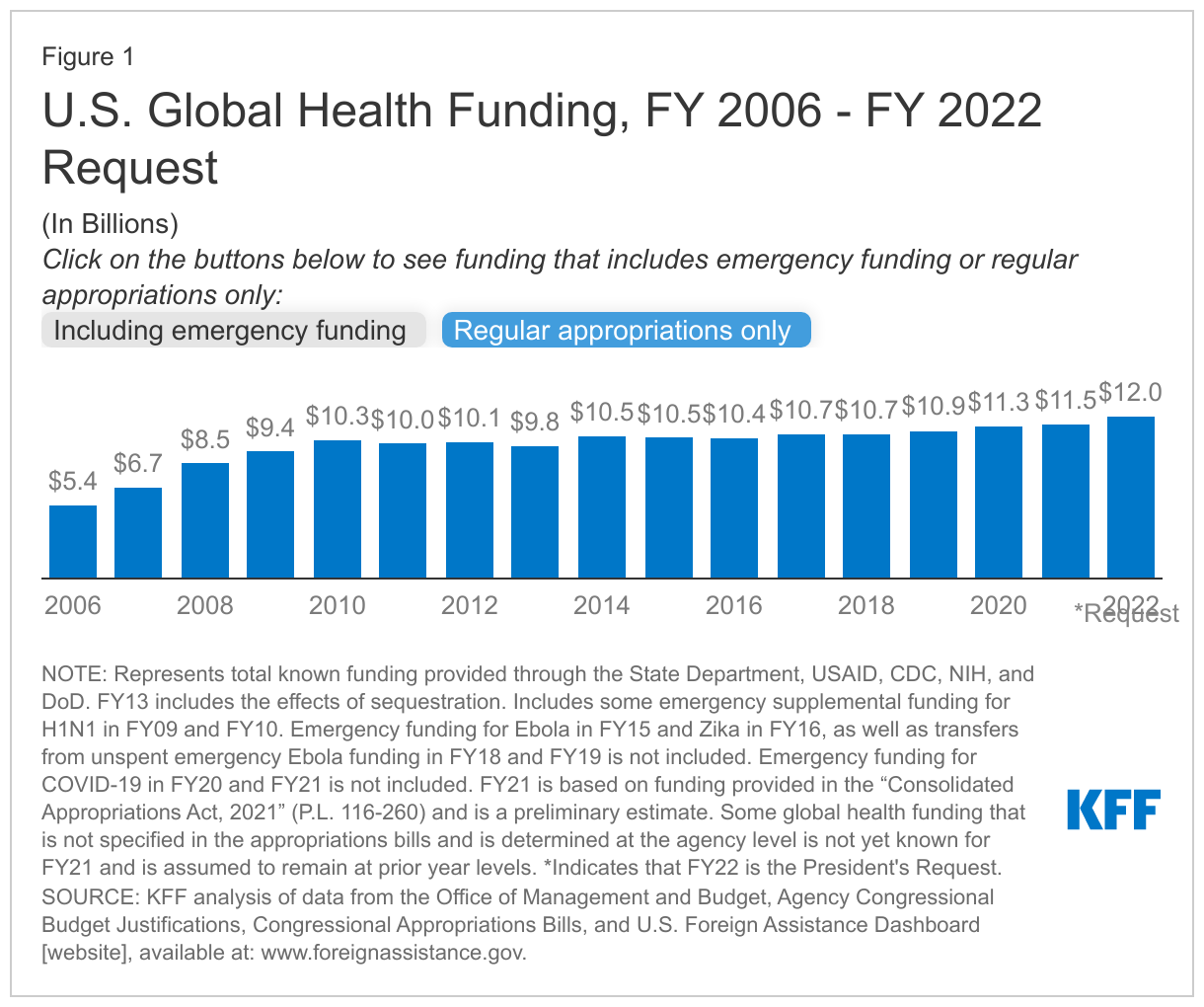
Over time, particularly in the last decade, Congress has increased levels of funding for global health, making the U.S. government the largest donor to global health in the world. However, since FY 2010, non-emergency U.S. funding for global health has remained relatively flat (see Figure 1).17 In recent years, it has provided higher levels than requested in the President’s Budget for regular appropriations, and it has also supported supplemental appropriations for emergency humanitarian, health, and pandemic responses.
Box 3: The Two-Step Process of Authorization/Appropriations
Established by House and Senate rules, the two-step process of authorization/appropriations supports the linkages between the authorizing and appropriating committees of each chamber. Authorizing legislation is “intended to provide guidance to appropriators as to a general amount and under what conditions funding might be provided to an agency or program” before appropriations may be made.18
For foreign assistance specifically – including global health assistance, this two-step process is also required by law. Still, this requirement is often waived by Congress, since it has not passed comprehensive foreign assistance authorization legislation since 1987. (Some instances of limited authorization legislation for specific programs, including global health programs such as PEPFAR, exist, but these are less frequent occurrences than the use of waivers for the process.)
Thus, absent an authorization bill, an appropriations bill can have the effect of authorizing the creation of a new program when providing funding for a specific activity for the first time and/or authorizing the continued operation of an existing program by providing continued funding for its activities.
- Regular appropriations. Each year, bills referred to as “regular appropriations bills” outline funding for government programs and activities, including for U.S. global health activities, within specified USG agencies and departments for a single fiscal year. For example, the Department of State, Foreign Operations, & Related Programs Appropriations Act (SFOPS bill) provides funding for USAID, the Department of State, and the Millennium Challenge Corporation (MCC), while the Departments of Labor, Health and Human Services, and Education, & Related Agencies Appropriations Act (Labor/HHS bill) provides funding for CDC, NIH, and FDA, among others. In some years, Congress may pass some or all regular appropriations bills individually or as part of a larger bill that bundles them together during vote consideration (an “omnibus” bill). In others, it may not pass some or all of these bills, instead opting to pass a “continuing resolution” that, generally, maintains U.S. funding at the prior fiscal year’s levels.Typically, at least five regular appropriations bills include components of global health activities carried out by more than 15 USG entities; these bills are the SFOPS bill; Labor/HHS bill; Department of Defense Appropriations Act; Agriculture, Rural Development, Food and Drug Administration, and Related Agencies Appropriations Act; and Financial Services and General Government Appropriations Act.19
- Supplemental appropriations. Less frequently, a bill referred to as a “supplemental appropriations bill” may provide additional funding to agencies to support emergency activities or other urgent needs that must be filled before the passage of the next fiscal year’s regular appropriations bills.20 For example, supplemental appropriations that included global health components supported funding for the USG’s response to unforeseen events, crises, and humanitarian disasters, such as the 2009 H1N1 pandemic, the 2010 Haiti earthquake, the 2014-2015 Ebola outbreak in West Africa, the 2015-2016 Zika outbreak, and the ongoing COVID-19 pandemic.21
Key Provisions and Reports
While these two kinds of bills – authorization and appropriations bills – are intended to be interrelated as part of a two-step process where each type fulfills a different function, Congress has increasingly used these bills for similar purposes (with the caveat that appropriations bills remain the only legislative vehicle for providing funding).
As a consequence, Congress now may (and often does) include provisions in both authorization and appropriations legislation that provide specific guidance or requirements for how funding be spent and/or how USG global health programs be implemented. These provisions may include spending directives as well as other legislative requirements and restrictions, which are discussed below.
- Spending directives. These may relate to certain bilateral global health programs as well as U.S. contributions to certain multilateral/international organizations. For example, in the Consolidated Appropriations Act of 2021 (which included the SFOPS bill), Congress provided guidance on the amount of funding to be directed to the U.S. contribution to the U.N. Population Fund (UNFPA) by stating that $32.5 million should be made available for this purpose.22
- Other legislative requirements and restrictions. These may range from requiring regular reporting to Congress on global health efforts to the development of five-year strategies on a specific global health issue to the conduct of programs to accordance with specific guidelines. For example, Congress requires USG global family planning/reproductive health (FP/RH) funding only be used to support organizations that “offer, either directly or through referral to, or information about access to, a broad range of family planning methods and services” through a provision known as the DeConcini Amendment in the SFOPS bill each year.23
Additionally, congressional committees with jurisdiction over global health-related legislation may also issue reports on legislation. While these reports are not binding and do not have the force of law, they may offer more specific guidance to the Executive and Judicial Branches (and other audiences) about how Congress would like to see a piece of legislation interpreted and more specifics about certain aspects of the legislation.24
Oversight
Congressional oversight of government programs, including for global health, is generally the purview of the committee or committees with responsibility for reviewing the activities and performance of departments and agencies under their jurisdiction (see Table 2 for key committees’ jurisdiction related to global health). Their oversight activities may include the following:
- Holding hearings. Hearings can draw public and congressional attention to recent developments and issues as well as inform the legislative process. For example, in the context of global health, Congress held several hearings on malaria in 2004 and 2005 that drew attention to and questioned key aspects of USAID’s approach to addressing malaria, such as the small proportion of U.S. malaria support devoted to buying and distributing commodities (e.g., bed nets and antimalarial drugs) as well as its overall impact and effectiveness.25 Later, in 2006, another congressional hearing reviewed changes that had been made to the USAID malaria program in 2005, when (among other things) the agency began to operationalize the newly-created President’s Malaria Initiative (PMI), which President Bush had launched in 2005 to expand U.S. global malaria efforts, and direct more funding to commodities.26
- Reviewing legislatively-mandated reports to Congress. This provides an opportunity for members and their staff to evaluate the status of efforts relative to legislative benchmarks. For example, the Executive Branch submits annual reports to Congress on the PEPFAR program and periodic reports to Congress on USAID health research & development (R&D) activities, among other things.27
- Approving changes to program funding allocations through the review of congressional notifications (known as CNs) from USG agencies. CNs provide some flexibility to agencies when circumstances necessitate changes to how funding is to be spent after Congress has already appropriated funding; the CN process provides Congress with a chance to review, evaluate, and approve such changes with regard to certain funding. This could include, for example, a CN requesting a change in the amount of funding planned to support activities related to a particular global health area in a specific country.28
- Reviewing the rules, regulations, and policies promulgated by departments and agencies to implement laws, policies, and congressional recommendations.29 Such review may help to influence the final form these implementing mechanisms take. Congress may also exercise its authority to disapprove rules and regulations, though this authority “has been little used by Congress.”30
- Issuing congressional reports. Congressional committees may issue reports on issues under their jurisdiction that they are investigating.31 For example, in 2006, the then-House Committee on Government Reform issued a committee report based on a study conducted by its Subcommittee on National Security, Emerging Threats, and International Relations, which examined strengthening disease surveillance. Though the report’s findings and recommendations focused on improving U.S. domestic disease surveillance in order to detect global threats, it also discussed global disease outbreaks and select USG global disease surveillance efforts, such as the Department of Defense’s Global Emerging Infections Surveillance and Response System (GEIS).32
- Approving treaties proposed and negotiated by the Executive Branch. Before the U.S. may officially accede to a treaty, the President must submit the treaty to the Senate for its advice and consent; with the Senate’s approval, the President may then proceed with ratifying the treaty.33 For example, the Senate approved the Food Aid Convention (FAC, a treaty negotiated in 1999 that aimed to “ensure that the international community can respond to emergency food situations, as well as ongoing food needs in developing nations” and that also “promotes food security, especially for vulnerable populations”34 ), allowing the U.S. to ratify the treaty in 2001. More recently, the Senate approved the FAC’s successor, the Food Assistance Convention (the FAC expired in 2003), allowing the U.S. to ratify the treaty in 2012, the same year in which it was negotiated.35
- Confirming presidential appointees. A function reserved to the Senate, providing advice and consent on the nominations of individuals for certain key global health-related positions within the USG allows the Senate to review and question each nominated individual’s priorities for and approach to their position. See below for further discussion.
| Table 2: Jurisdiction of Key Congressional Committees Related to Global Health |
| House Foreign Affairs (HFAC) and Senate Foreign Relations (SFRC) |
| Responsible for oversight and legislation relating to foreign assistance, including programs operated by the Department of State, USAID, and the Millennium Challenge Corporation (MCC). SFRC is also responsible for confirmation of presidential appointees at these agencies. Key HFAC Subcommittees: - Africa, Global Health, and Global Human Rights
- International Development, International Organizations, and Global Corporate Social Impact
Key SFRC Subcommittees: - Africa and Global Health Policy (with responsibility for disease outbreak and response)
- Multilateral International Development, Multilateral Institutions, and International Economic, Energy, and Environmental Policy (with responsibility for international organizations, including the United Nations and its agencies)
- State Department and USAID Management, International Operations, and Bilateral International Development (with responsibility for State, USAID, MCC, Peace Corps)
- Western Hemisphere, Transnational Crime, Civilian Security, Democracy, Human Rights, and Global Women’s Issues
|
| House E&C Committee and Senate HELP Committee |
| Responsible for oversight and legislation related to a number of areas of health care, including biomedical research, public health, and the regulation of drugs. The HELP Committee is also responsible for confirmation of presidential appointees at the Centers for Disease Control and Prevention (CDC), National Institutes of Health (NIH), and Food and Drug Administration (FDA). Key House E&C Subcommittee: Key Senate HELP Subcommittees: - Children and Families
- Primary Health and Retirement Security
|
| House and Senate Appropriations Committees |
| Responsible for oversight and appropriation of funds to USG global health efforts. Key House Appropriations Subcommittees: - Defense
- Labor, Health and Human Services, Education, and Related Agencies (with responsibility for CDC and NIH)
- State, Foreign Operations, and Related Programs (with responsibility for State and USAID)
Key Senate Appropriations Subcommittees: - Defense
- Labor, Health and Human Services, Education, and Related Agencies (with responsibility for CDC and NIH)
- State, Foreign Operations, and Related Programs (with responsibility for State and USAID)
|
| NOTES: State means the Department of State, USAID is the U.S. Agency for International Development, MCC is the Millennium Challenge Corporation, CDC is the U.S. Centers for Disease Control and Prevention, NIH is the National Institutes for Health. |
Confirmation of Key USG Officials
As required by the U.S. Constitution and law, people appointed by the president to certain positions within the USG may only be confirmed with the advice and consent of the Senate.36 With regard to global health, a number of positions with federal departments and agencies require such confirmation. Some of these positions are mainly or entirely focused on global health (e.g., the U.S. Global AIDS Coordinator, who holds the diplomatic rank of Ambassador-at-Large, at the State Department; the Assistant Administrator for the Bureau for Global Health at USAID), while other positions are generally focused on global development but include global health in their purview (e.g., the Administrator of USAID). Still other positions requiring Senate confirmation have a broader portfolio that includes global health among many other issues (e.g., the Secretary of Health and Human Services).
The confirmation process, which involves both the committee with jurisdiction and the Senate as a whole, proceeds at varying speeds, depending on the nominee, the position for which they are nominated, questions or concerns raised about their nomination by a Senator(s) (if any), and the broader political context and timing of the nomination. Generally, the relevant committee is responsible for gathering information about a nominee, and it may or may not hold a hearing related to the nomination before deciding whether or not to recommend the nominee to the full Senate for a vote.37 (See also the PEPFAR example below.)
Member Engagement
Additionally, members of Congress may individually weigh in on the conduct of USG global health efforts in various ways (e.g., by drafting letters to USG officials about global health issues/programs, as 98 members did in 2009 when they sent a letter to President Obama in which they urged him to request at least $1.75 billion for the U.S. contribution to the Global Fund as part of his FY 2011 budget request38 ), and congressional member and staff delegations may visit sites of USG global health efforts during official visits overseas.
Examples of Congressional Engagement
PEPFAR
Though the history of congressional engagement in global HIV spans several decades, Congress has become substantially more involved in responding to the epidemic over the past 20 years. It has employed a variety of legislative tools and activities – from legislation to hearings to caucuses – in its efforts to shape and reshape the USG response to global HIV, leading up to and through PEPFAR.
Legislation
While PEPFAR is widely seen as a signature initiative of President George W. Bush, some members of Congress had already begun laying legislative groundwork for an expanded U.S. global HIV effort and crafting legislation that served as an early blueprint for PEPFAR. Just four months after President Bush announced his intention to create PEPFAR during his 2003 State of the Union Address, Congress passed legislation authorizing the program at up to $15 billion in funding for U.S. global HIV, TB, and malaria efforts over five years; since then, the program has been reauthorized three times (see Table 1). PEPFAR illustrates how global health endeavors evolve over time, requiring Congress, as well as the Administration and non-government stakeholders, to navigate conflicting approaches, disparate priorities, and changing budget environments; this is reflected, for example, in the evolving content of PEPFAR’s authorizing legislation over time, as well as PEPFAR’s appropriations history. Each authorization has addressed different aspects of policy and programming, with Congress spelling out spending directives as well as other requirements and restrictions for PEPFAR activities through these pieces of legislation. For example, the Leadership Act of 2003 included a spending directive that required not less than 10% of HIV funding be spent on orphans and other children affected by or vulnerable to HIV/AIDS (a provision which remains in force today), and the Lantos-Hyde Act of 2008 required additional PEPFAR reporting to Congress, including a report by the Comptroller General about the coordination of USG global HIV efforts and the impact of PEPFAR funding and programs on other USG global health programming.39 In addition, whereas Congress appropriated substantially more funding in PEPFAR’s first five year period than the $15 billion authorized for the program, it appropriated significantly less than that authorized in its next five years and has essentially flat-funded the program since, reflecting a dramatically changed budget context.
Oversight
Congressional oversight of PEPFAR takes many forms, including: public hearings; review of reports to Congress that describe, for example, how appropriated funding has been spent and documenting progress toward congressionally-mandated targets for PEPFAR efforts; the creation of at least two congressional caucuses focused specifically on global HIV (along with other caucuses addressing broader global health issues that have also worked to address HIV); congressional participation on delegations to the field; and the engagement of individual members in a variety of activities. With regard to the latter, the substantial engagement of a number of members of Congress has, historically, been important in advancing not only related legislation but also in both buttressing as well as challenging USG policy, programming, and goals related to HIV: Over the years, a number of members have written letters to leaders in the Executive Branch about PEPFAR activities, spoken on the floor of the House and Senate at length about HIV, and engaged with the HIV community and, more broadly, the global health community through a variety of fora.
Additionally, of particular importance in the context of PEPFAR oversight is the Senate confirmation of the leader of PEPFAR, known as the U.S. Global AIDS Coordinator. A novel approach to coordinating U.S. global health efforts related to a single issue at the time of the position’s creation, the Coordinator oversees U.S. global HIV efforts across USG departments and agencies but is based at the U.S. Department of State; however, the Coordinator exercises significant authority over HIV funds across USG agencies, which remains a unique attribute of the position relative to leaders of other USG disease-specific programs. While the person who will lead PEPFAR is appointed by the president, the position is among those that must be confirmed with the advice and consent of the Senate.
West Africa Ebola Outbreak
By the latter half of 2014, congressional attention to the then-rapidly-expanding outbreak of Ebola virus disease in West Africa grew quickly, and the ensuing flurry of congressional activity provides a snapshot of the varied ways in which Congress may engage with a global health issue. The Ebola outbreak began to garner more attention in the U.S., and specifically on Capitol Hill, after the infection of two American health workers overseas who were working with Ebola-infected patients was announced in July 2014. At about the same time, the non-governmental organization Medicins San Frontieres (MSF) issued a global call for help, stating that “Ebola is no longer a public health issue limited to Guinea [the country where the outbreak began]. It is affecting the whole of West Africa.”40
In the years following that, congressional efforts were wide-ranging and included public hearings, legislation (both binding and non-binding), and member engagement on the issue (e.g., several members called for more information about and increased USG actions in response to the outbreak). Some key activities are described below.
Legislation
Several pieces of legislation related to the Ebola outbreak, including non-binding resolutions and appropriations bills, were passed by Congress (or in the case of resolutions, by one or more chamber of Congress). For example, in September 2014, the Senate passed a resolution that recognized the outbreak as a “severe threat” to populations, government, and economies across Africa and potentially beyond, and also that month, Congress passed a continuing appropriations resolution that provided continued funding for USG agency efforts, including greater funding for accelerating Ebola research and development activities as well as the USG response to the outbreak.41 Subsequently, in November 2014, President Obama requested $6.18 billion in emergency funding for Ebola.42 Then-Chairwoman of the Senate Appropriations Committee, Senator Barbara A. Mikulski (D-MD) stated at that time, “Ebola, in my mind, meets the criteria for emergency spending. It’s sudden. It’s urgent. It’s unforeseen. And it’s temporary.”43 Shortly thereafter, in December 2014, Congress passed an omnibus appropriations bill that included $5.4 billion in emergency funding for Ebola response and recovery efforts, of which $3.7 billion was specifically designated for international efforts.44 Attention then turned to oversight of this funding, specifically to how agencies planned to spend the funds provided by Congress. As with other USG global health funding, Ebola funding was governed by various spending directives and other congressional guidance, and agencies had to seek congressional approval (through CNs) as their spending plans changed over time.45
Oversight
Congressional efforts to oversee the U.S. government’s response to the West Africa Ebola outbreak were multifaceted and included public hearings, the approval of changes in planned funding allocations across certain agencies, and the engagement of individual members as well as caucuses in a variety of activities. In 2014 alone, five congressional committees (or their subcommittees) convened eight public hearings on the Ebola outbreak, beginning in early August 2014; see Table 3. As the outbreak grew and attention to it increased both within policy circles and in the U.S. more broadly, congressional and public attendance at hearings steadily increased.46 Congress also authorized the repurposing of funds by agencies to respond to the Ebola outbreak, which was accomplished through the CN process when, for example, DoD requested and received congressional approval to spend up to $750 million in previously-appropriated but leftover war funds on its Ebola outbreak response.47 With regard to individual member engagement, various members spoke about Ebola in floor speeches on the House and Senate floors, discussed the need for greater USG resources and an intensified organizational response to the outbreak, and participated in public events that focused on Ebola through caucuses and other organizations.48
| Table 3: Congressional Hearings on the West Africa Ebola Outbreak in 2014 |
| Date | Committee(s)49 | Hearing Title |
| Aug. 7 | HFAC subcommittee | “Combating the Ebola Threat” |
| Sept. 16 | Senate HELP; Senate Approps. | “Ebola in West Africa: A Global Challenge and Public Health Threat” |
| Sept. 17 | HFAC subcommittee | “Global Efforts to Fight Ebola” |
| Oct. 15 | House E&C subcommittee | “Examining the U.S. Public Health Response to the Ebola Outbreak” |
| Nov. 12 | Senate Approps. | “ U.S. Government Response: Fighting Ebola and Protecting America” |
| Nov. 13 | HFAC | “Combating Ebola in West Africa: The International Response” |
| Nov. 18 | HFAC subcommittee | “Fighting Ebola: A Ground-Level View” |
| Dec. 10 | SFRC subcommittee | “The Ebola Epidemic: The Keys to Success for the International Response” |
Looking Ahead
Congressional engagement has a significant impact on the USG's role in global health. Over the last 20 years alone, bipartisan congressional support for global health has led to expanded U.S. efforts to address global HIV, TB, and malaria, in particular (among other things, such as global health security), including significantly increased funding, and also respond to global health emergencies, such as pandemic influenza, Ebola, Zika, and COVID-19. Congress, through the array of activities carried out by its congressional committees, caucuses, and individual members, has played and will continue to play an important role in shaping and overseeing U.S. global health efforts. Key issues and opportunities going forward include:
- educating new and continuing members and staff about USG global health efforts, recent developments, and the role of Congress;
- maintaining and strengthening bipartisan support for USG global health programs and funding, given the shifting make-up of Congress over time and in light of current fiscal constraints;
- assessing USG support for multilateral engagement, innovative financing mechanisms, and public-private partnerships, given their role in leveraging USG global health funding and resources;
- ensuring that the legislative framework for USG global health programs is responsive to an evolving global health environment as well as U.S. interests and considerations; and
- providing ongoing oversight, particularly as USG global health efforts are increasingly transitioned to partner countries (i.e., as country ownership is heightened) in order to ensure transparency, accountability, and sustainability in these activities.