KFF COVID-19 Vaccine Monitor: Views On The Pandemic At Two Years
Findings
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and acceptance, information needs, trusted messengers and messages, as well as the public’s experiences with vaccination.
Key Findings:
- With pandemic-related restrictions being lifted in many states as well as local areas and remaining mask mandates set to expire soon, most of the public (59%) say they have personally returned to doing some of their pre-pandemic activities, but not all, or say they are still doing very few of the activities they were doing before the pandemic. Two years into the pandemic, about a quarter of adults say they have basically returned to normal while one in seven say they never changed their activity level during the pandemic.
- With people returning to some pre-pandemic activities, majorities still report wearing masks in public indoor areas. Eight in ten adults say they’ve worn a mask in public indoors at least some of the time in the last 30 days. Similarly, most say people should continue to wear masks in some public places to minimize the spread of COVID-19 and avoid another surge in cases (59%) while four in ten say people should stop wearing masks in public so things can get back to normal. Views of the federal mask mandate on airplanes and public transit are divided, with half of the public wanting the mandate extended and half wanting it to expire.
- Larger shares of Democrats and vaccinated adults report they’ve been wearing masks and want others to continue doing so, while most Republicans and unvaccinated adults are eager to return to normal and lift mask mandates. Further, compared to their counterparts, Black adults, Hispanic adults, and those with lower incomes are less likely to say they’ve returned to normal, more likely to say they’re wearing masks frequently, and much more likely to say people should continue to wear masks to minimize the spread of the virus and prevent another surge. With Black and Hispanic adults and those with lower-incomes more likely to work in jobs that are highly impacted by COVID-19, the survey finds that they’re more likely to show concerns over reopening and unmasking measures.
- The pandemic has taken a heavy toll on adults and children over the last two years with many reporting difficulties balancing their child’s education and their work, household finances, and mental or physical health. Six in ten parents say the pandemic has negatively affected their children’s schooling and over half saying the same about their children’s mental health. In addition, half of adults overall say their own personal mental health has been negatively affected, and four in ten say the same about their physical health and their financial situation. Those with lower incomes are more likely to report a negative impact on their finances, while young adults are more likely than older adults to say the pandemic had a negative impact on their mental and physical health as well as their employment situation.
- Asked to say in their own words what has been the biggest challenge and/or any positive change brought about by the pandemic over the past two years, the top responses on both the negative and positive side related to human interactions and relationships or lack thereof. On the negative side, 27% say the hardest thing has been isolation and not seeing people. When asked if anything has changed for the better because of the pandemic, 24% say they’re closer to their family or spent more time with their families.
How Ready Is The Public To Return To “Normal” And Who Is More Hesitant About Lifting Mask Restrictions?
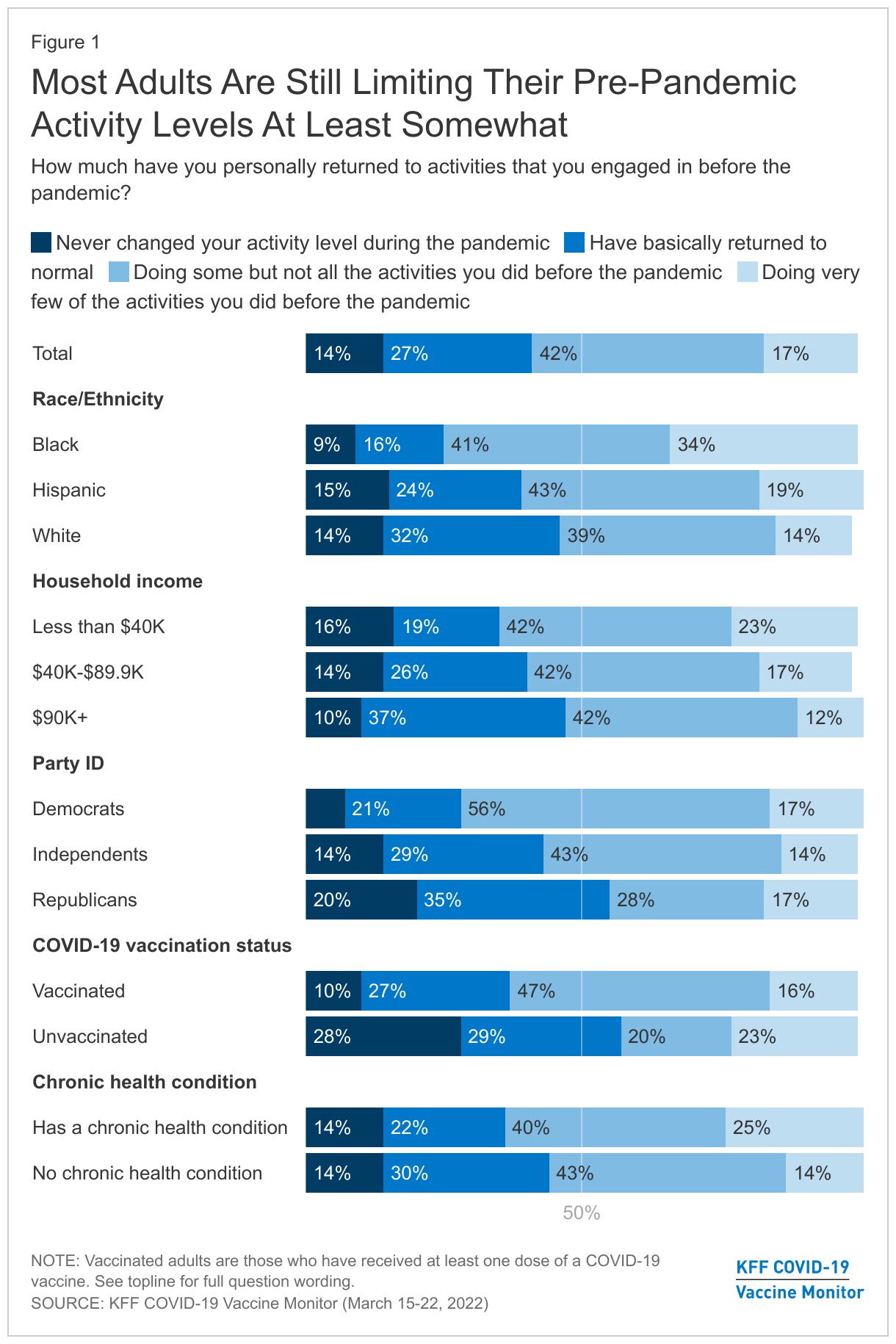
The latest analysis from a KFF COVID-19 Vaccine Monitor survey1 finds that as the omicron surge recedes, a majority of adults say they are limiting their activity levels from pre-pandemic at least somewhat in order to protect themselves from COVID, with 42% who are doing some but not all the activities they did before the pandemic and 17% who are doing very few of the activities they did before COVID-19. Around four in ten adults say they have basically returned to normal in terms of activities that they engaged in before the pandemic (27%) or that they never changed their activity level to begin with (14%).
Unvaccinated adults (57%), Republicans (55%), and White adults (47%) are the groups most likely to say they never changed activity levels or have basically returned to normal. Nearly half of those with household incomes of $90,000 or more say the same. Black adults (34%), those with a chronic condition that puts them at higher risk for COVID-19 (25%), and those living in households with incomes less than $40,000 (23%) are the most likely to say they are doing very few of the activities they did before the pandemic.
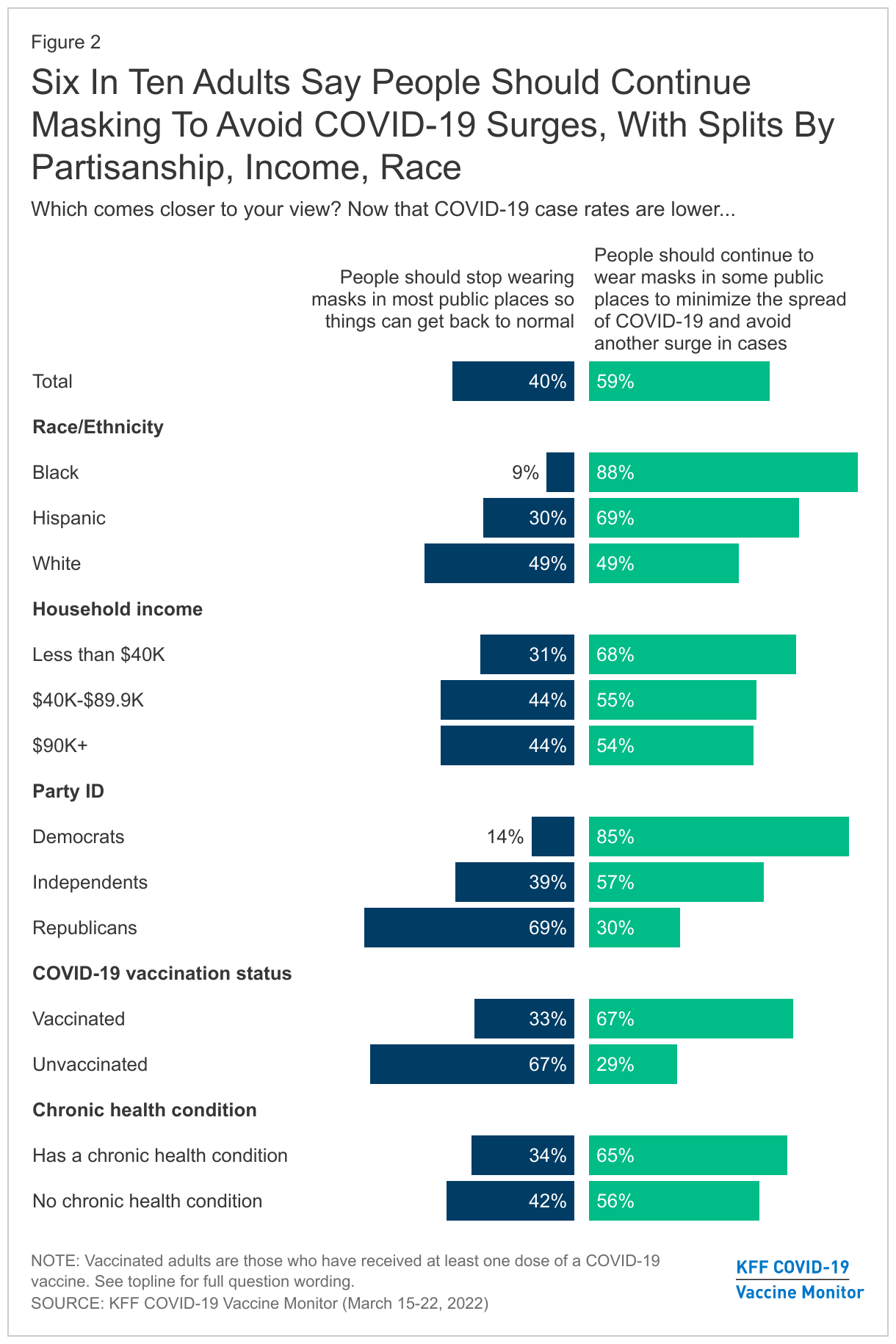
About six in ten adults (59%) say that now that COVID-19 case rates are lower, people should continue to wear masks in some public places to minimize the spread and avoid another surge in cases, while four in ten say that people should stop wearing masks in most public places so things can go back to normal. There are significant divides not only by partisanship, and vaccination status, but also by race, ethnicity, and income.
Eight-five percent of Democrats say that people should continue to wear masks, as do 57% of independents and 67% of vaccinated adults. Around seven in ten Republicans (69%) say that people should stop wearing masks so that things can return to normal, as do 67% of unvaccinated adults.
While White adults are split (49% say people should stop wearing masks, 49% say they should continue to wear them in some public places), large majorities of Black adults (88%) and Hispanic adults (69%) say that people should continue to wear masks in some public places to minimize the spread of COVID-19. Around two-thirds of those with a household income of less than $40,000 a year (68%) say the same, compared to 55% of those with an income between $40,000-$89,900 and 54% of those with an income of $90,000 or more. This finding that people of color are more likely to support continued mask wearing may reflect larger shares of Black and Hispanic adults being employed in service industries compared to White adults, putting them at an increased risk of exposure to COVID-19.
This finding is consistent with previous Vaccine Monitor surveys, which found Black and Hispanic adults were more likely to be worried that they personally will contract COVID-19, as well as be worried that someone in their family or their child will get sick. Black and Hispanic adults, as well as those with lower incomes were also more likely to say they don’t get paid time off if they get COVID-19.
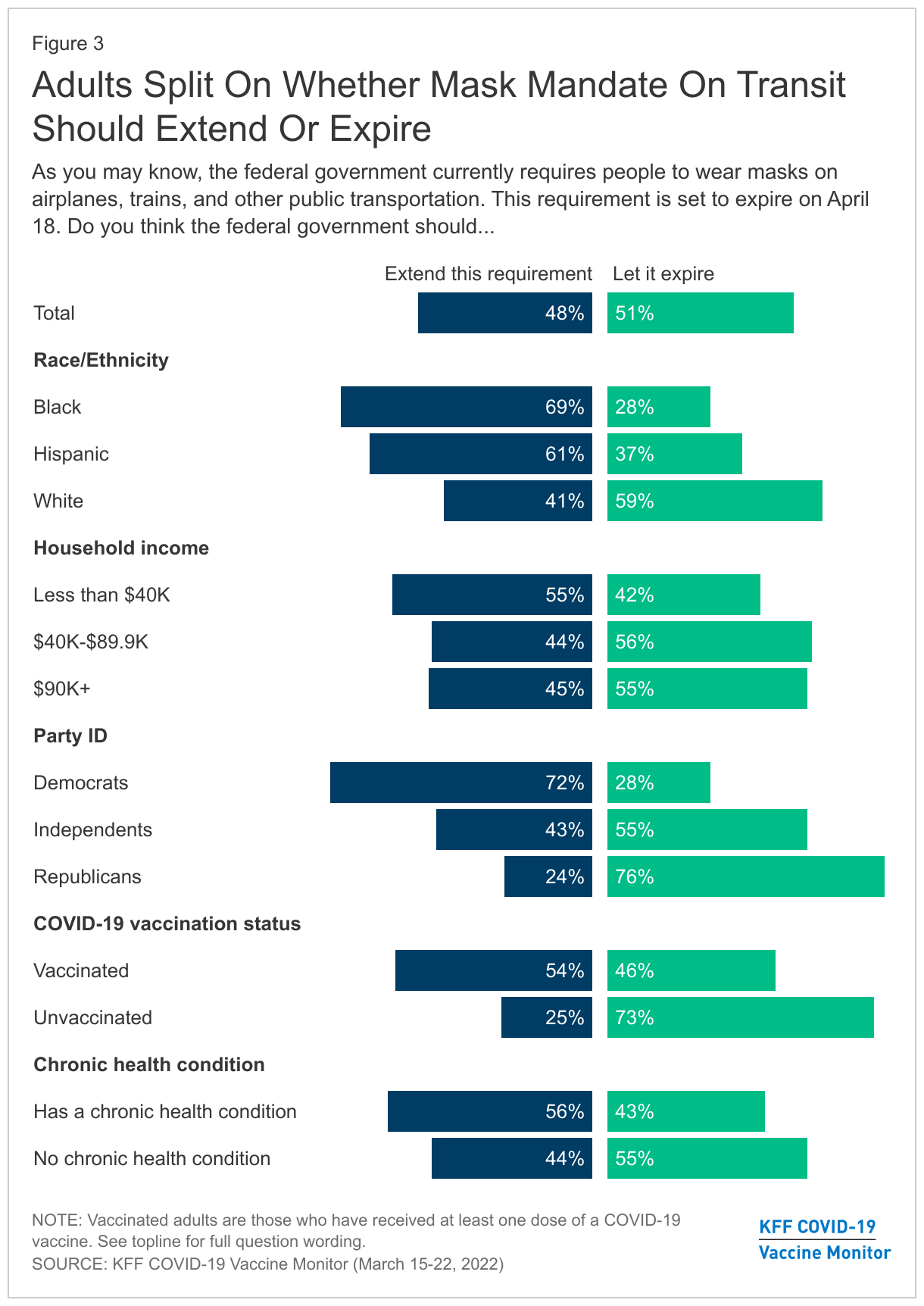
On the more specific question of mandating masks on public transportation, the public is more evenly divided. The federal government currently requires people to wear masks on airplanes, trains, and other public transportation. With this requirement set to expire on April 18, adults are split on whether the federal government should let the requirement expire (51%) or extend the requirement (48%).
Majorities of Democrats (72%) and vaccinated adults (54%) support extending the masking requirement on transportation. By contrast, three-quarters of Republicans (76%) and unvaccinated adults (73%), and over half of independents (55%) would prefer to let the requirement expire on April 18.
However, preferences for this federal mandate extend beyond partisanship and vaccination status, with lower income adults and people of color voicing support for keeping the requirement after April 18. At least six in ten of Black (69%) and Hispanic adults (61%) say the federal government should extend the requirement, compared to 41% of White adults. Over half of adults with lower incomes (55%) want to extend the masking requirement, compared to 44% of those with a household income of between $40,000-$89,900, and 45% of those with an income of $90,000 or more. Similar to views of general masking, this divide by racial and ethnic groups as well as income groups may reflect those most likely to be working in areas where they would be exposed to COVID-19 without mask mandates.
Those with chronic conditions are also more likely to support extending the federal mask mandate on transportation (56%), while more than half (55%) of those without chronic conditions want to let the mandate expire.
current MASK USAGE
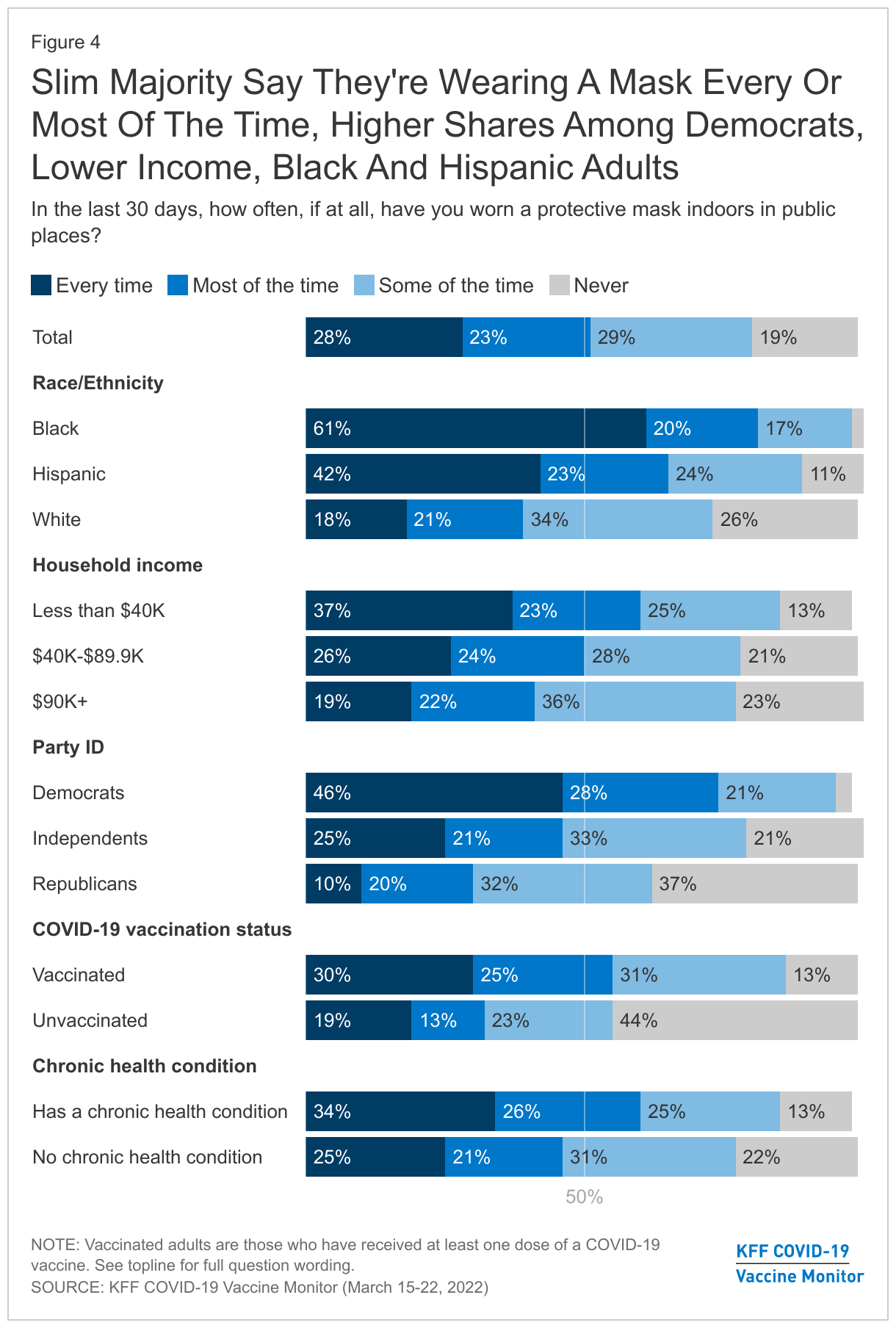
Most adults report continuing to wear a mask at least sometimes in public places. Around half of adults (51%) say that in the past 30 days they wore a mask every time or most of the time when indoors in public places, including 28% who say they wore one every time. Another 29% say they wore a mask some of the time, and 19% say they never wore a mask indoors in public places.
In line with attitudes about mask requirements on transportation, Democrats are more likely to say they always or mostly wore a mask indoors in the past 30 days (75%), compared to independents (46%) and Republicans (30%).
Two-thirds of unvaccinated adults say they have been wearing a mask some of the time or never have worn a mask indoors in the past 30 days (67%), while one-third (32%) report wearing one every or most of the time. A majority of vaccinated adults say they wore a mask every or most of the time (56%).
Showing differences by race and ethnicity, twice the share of Black adults compared to White adults report wearing a mask always or most of the time in the past 30 days (80% vs. 39%). Around two-thirds of Hispanic adults say the same (65%).
The Pandemic’s Toll On Families Two Years In
IMPACTs ON MENTAL, PHYSICAL, and FINANCIAL HEALTH
The survey finds the pandemic has taken a heavy toll on adults and children over the last two years. Whether it comes to their education, work, finances, mental or physical health, many – regardless of race, ethnicity and income – report feeling the negative effects of the pandemic.
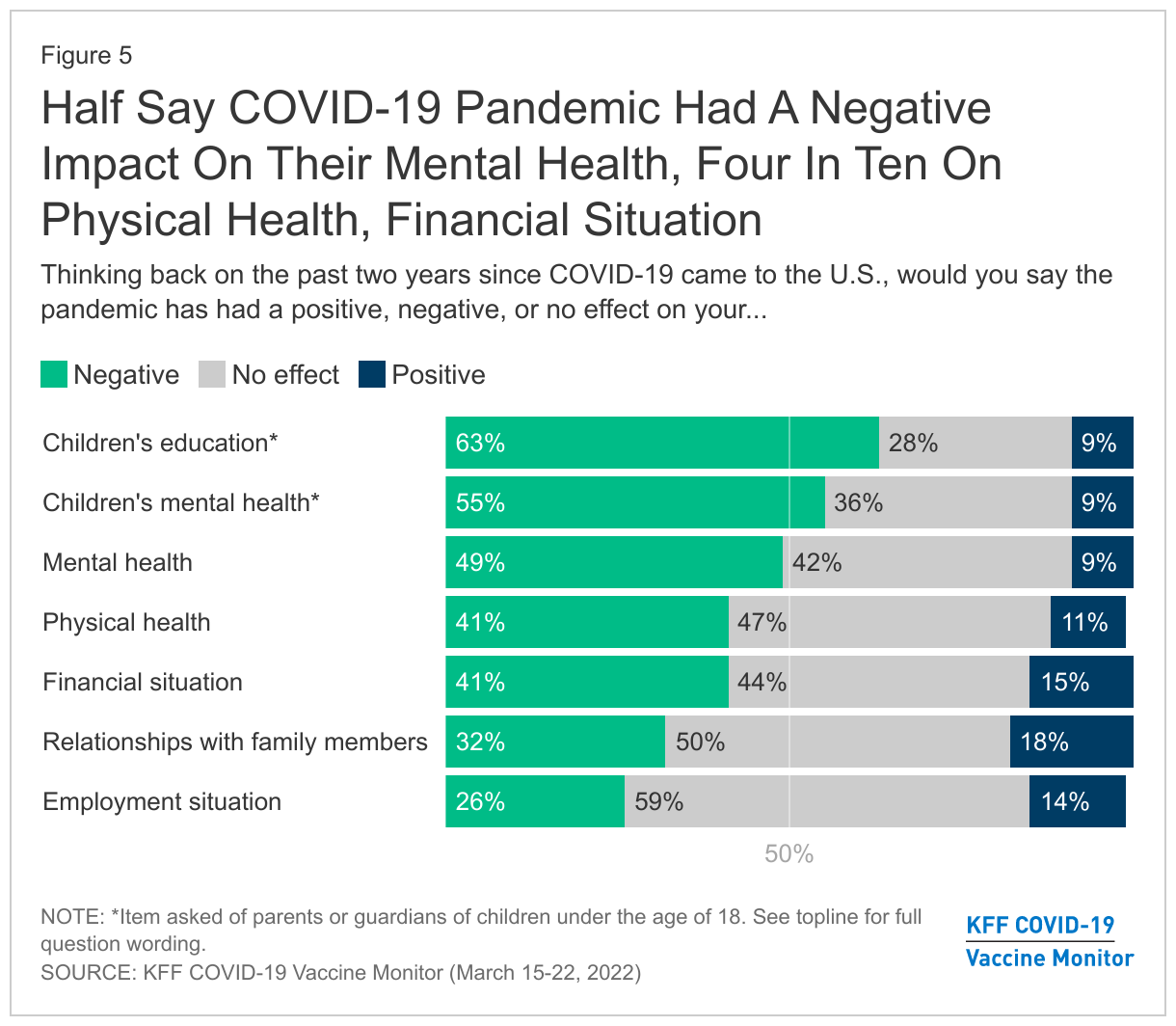
The most common negative effects of the pandemic, as reported by parents, are about their children’s education and mental health. Almost two-thirds of parents say that the pandemic has negatively affected their children’s education (63%), with 28% saying it had no effect, and 9% who report it had a positive effect. Moreover, over half (55%) of parents say the pandemic has had a negative impact on their children’s mental health, compared to 36% who say it made no difference, and 9% saying it had a positive effect.
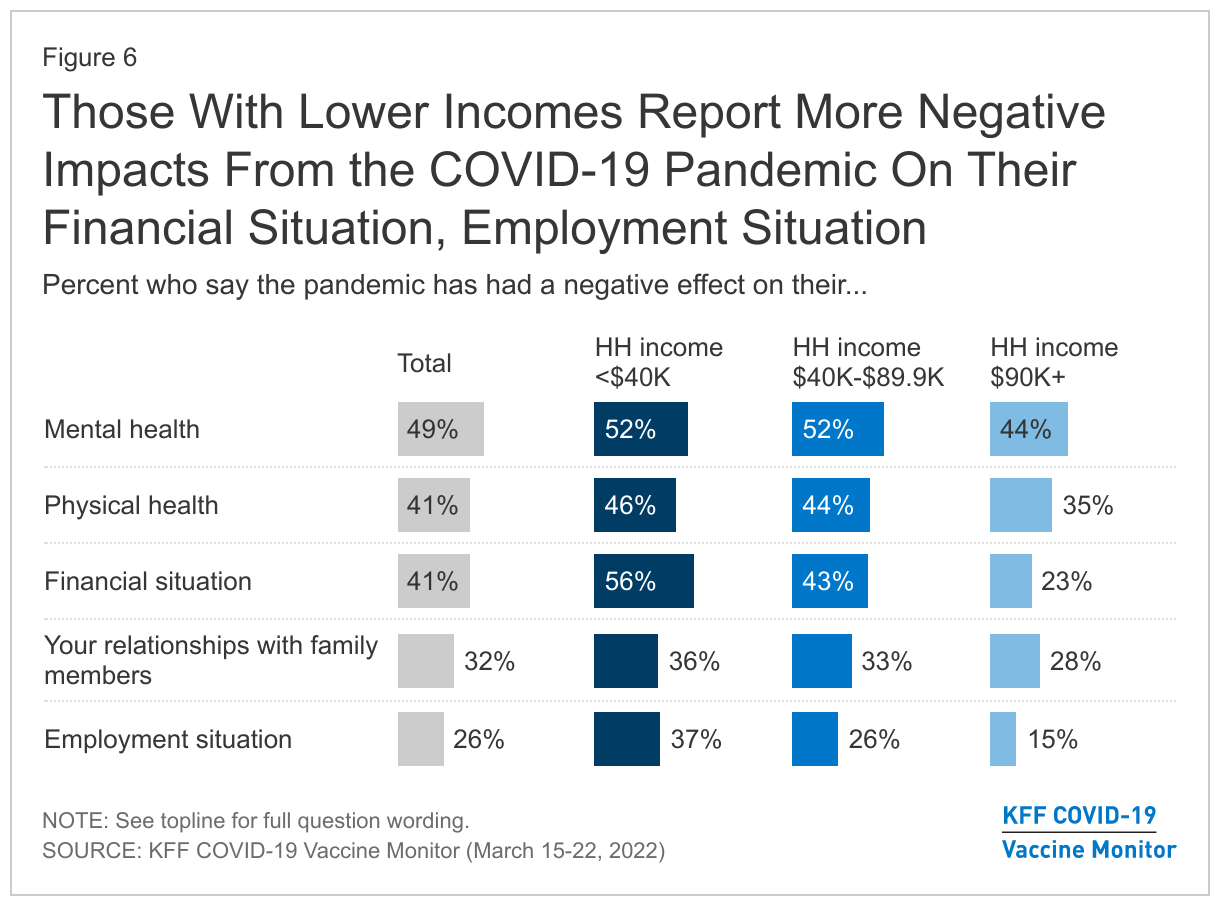
Among all adults, half say the pandemic has had a negative effect on their personal mental health (49%), and 41% say it has had a negative impact on their physical health. Few say it has had a positive effect on either their physical (11%) or mental health (9%).
About four in ten adults say the pandemic had a negative impact on their financial situation (41%) while a similar share report it had no impact (44%), with 15% who say it had a positive impact. One-quarter of adults say the pandemic has had a negative impact on their employment situation (26%), with 59% who report it has not had an impact.
Results are more mixed when it comes to the pandemic’s effect on family relationships. Around a third say the pandemic has had a negative impact on their relationships with family members (32%) while 18% say it has had a positive impact. Half say it has not had any impact one way or another.
Adults in households with lower incomes report being harder hit by the pandemic, especially when it comes to financial and employment impacts. Adults with a household income of less than $40,000 a year are more likely to say the pandemic has had a negative impact on their financial situation (56%), compared to 43% of those with an income of between $40,000 and $90,000 and 23% of those with a household income of $90,000 or more a year.
In addition, the share of those with lower incomes who say the pandemic had a negative impact on their employment situation (37%) is more than twice the share of those with annual incomes greater than $90,000 (15%).
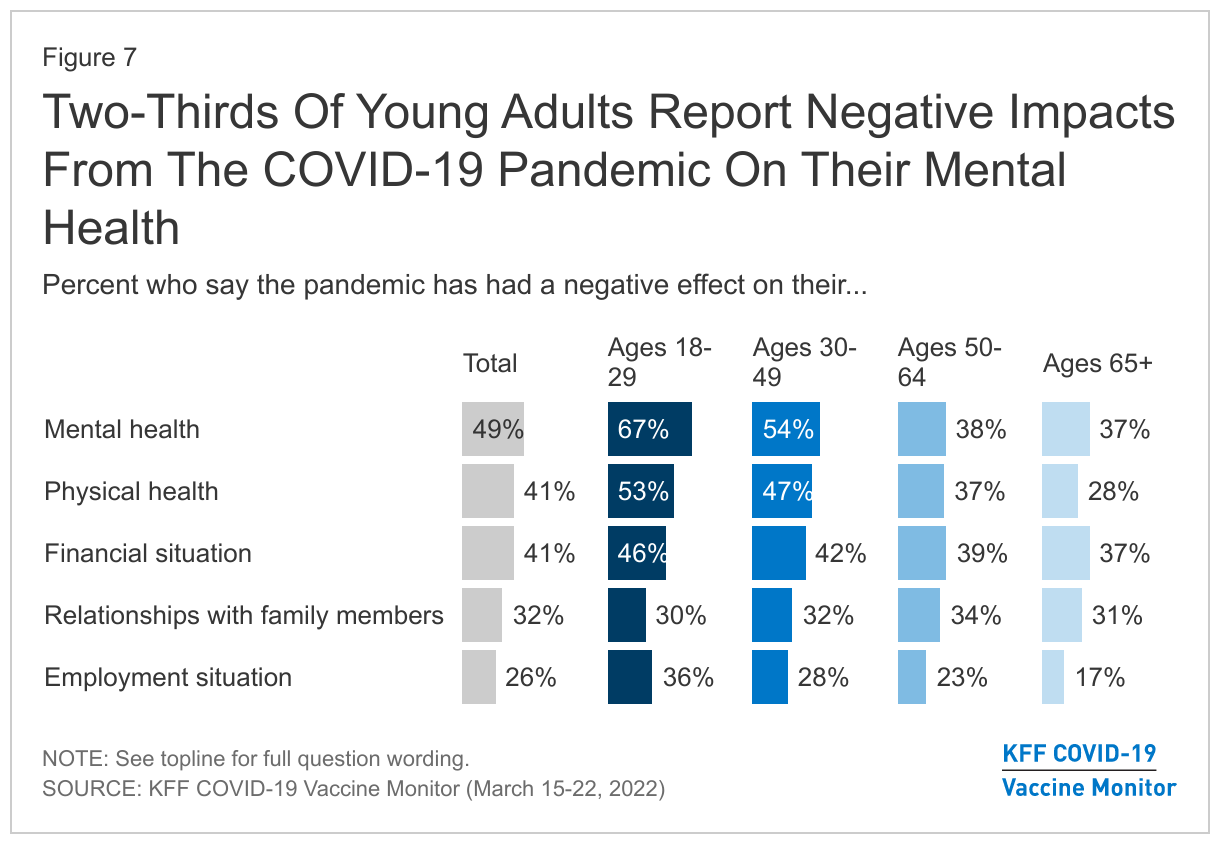
Younger people also report disproportionate effects from the COVID-19 pandemic, especially when it comes to their mental and physical health. Two-thirds of young adults aged 18-29 (67%) report that the pandemic has had a negative impact on their mental health, compared to just over half of 30-49 year-olds (54%), and under four in ten 50-64 year-olds (38%) and those over the age of 65 (37%).
Young adults are also more likely to report difficulties with their physical health due to the pandemic, with 53% of those under 30 reporting a negative impact, 47% of those 30-49, 37% of those 50-64, and 28% of those over the age of 65. In addition, larger shares of young adults report negative effects on their employment situation (36%) compared to older adults, including those ages 50-64 (23%) and those 65 and older (17%).
PANDEMIC IMPACTS: IN THEIR OWN WORDS
In their own words, when asked about the biggest challenge and/or positive change brought about by the pandemic over the past two years, the top responses regarding both negative and positive effects were related to human interactions and relationships, or the lack thereof.
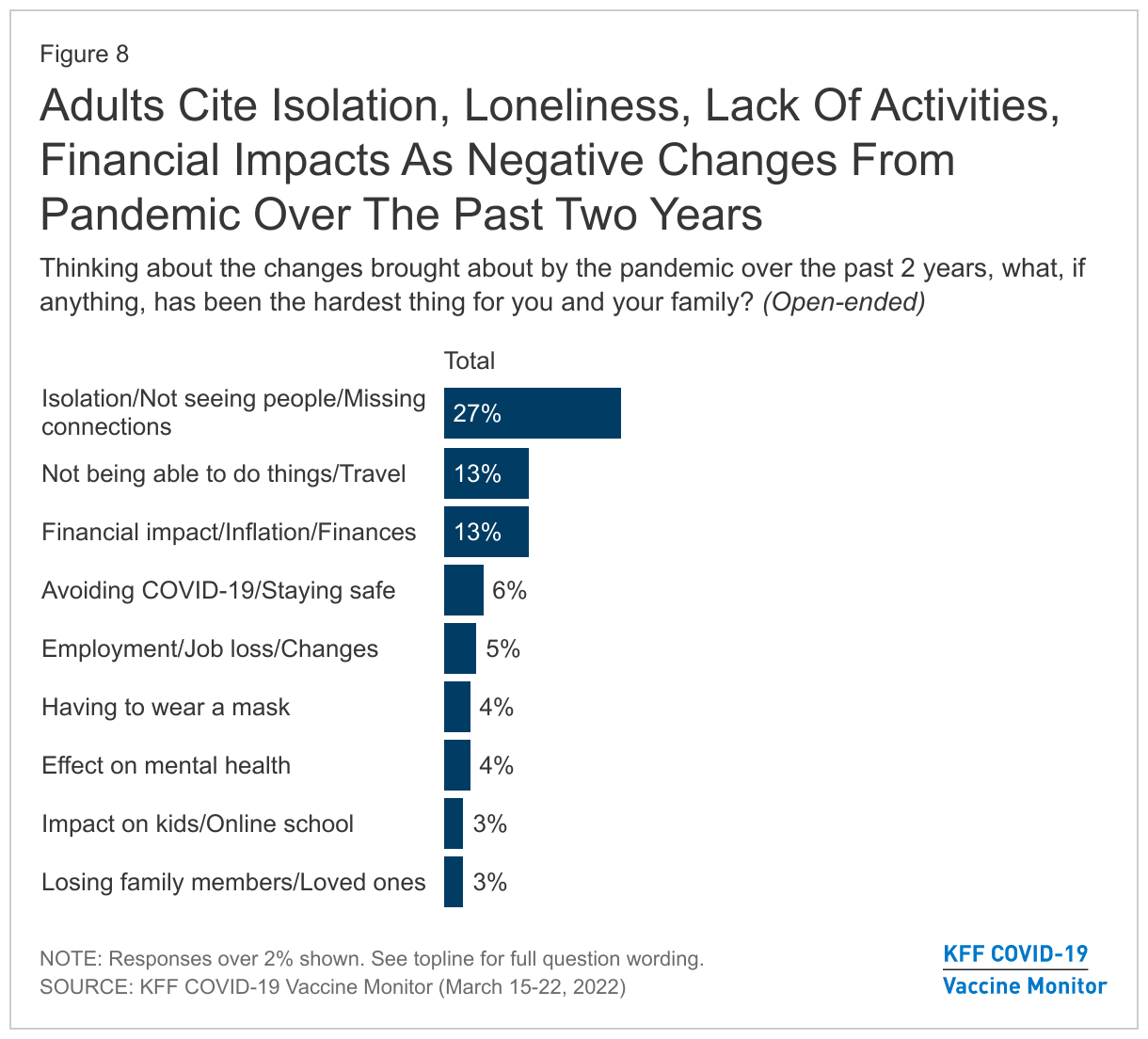
When asked about changes that have been brought about by the pandemic over the past two years, 27% say the hardest thing has been isolation and not seeing people. Another 13% say they have struggled with not being able to do things or travel, and 13% cite the financial impact, including inflation.
Some say the hardest part has been avoiding COVID-19 and staying safe (6%), employment changes and job loss (5%), having to wear a mask (4%), the effect on mental health (4%), the impact on kids and online schooling (3%), and losing family members and loved ones (3%).
In their own words: Thinking about the changes brought about by the pandemic over the past two years, what, if anything, has been the hardest thing for you and your family?“
Being evicted and still not recovered financially.” – 43 year old, male, White, Democrat, South Carolina
“Not allowed to be with my wife when she was hospitalized with stage 4 cancer.” – 65 year old, male, White, Republican, Arkansas
“Finances, health, loss of family members, being hospitalized, lasting effects. My family's going through things because of the whole COVID thing. Their finances are going down and they're struggling; I had to leave my apartment - everything was chaotic.” – 31 year old, female, White, Independent, Tennessee
“Concern over preexisting conditions.” – 24 year old, female, Asian, Democrat, Illinois
“Deal with all mandates and restrictions.” – 30 year old, male, Hispanic, independent, Indiana
“Just the online schooling, I had to quit work to stay at home.” – 31 year old, female, White, Democrat, Ohio
“Division over what's real or not and what we should follow.” – 25 year old, male, Hispanic, Republican, Florida
“Having to wear masks everywhere, it’s terrible.” – 24 year old, male, White, Independent, Michigan
“Inability to visit elderly parents.” – 63 year old, male, White, Independent, Florida
“Getting clear information about it and how best to manage through the maze of many, many authorities giving advice about Covid.” – 90 year old, female, Black, Democrat, New York
“Mask mandates and business closures, especially as a truck driver.” – 58 year old, male, White, independent, South Dakota
“Medical debt, inability to work from disabilities exacerbated or initiated by covid.” – 31 year old, other, White, independent, Oregon
“Loss of non-family social relationships.” – 22 year old, female, White, Democrat, New York
“Mental health got a lot worse due to distancing people from each other.” – 38 year old, male, White, independent, Illinois
“The grief of people dying.” – 39 year old, female, White, independent, Texas
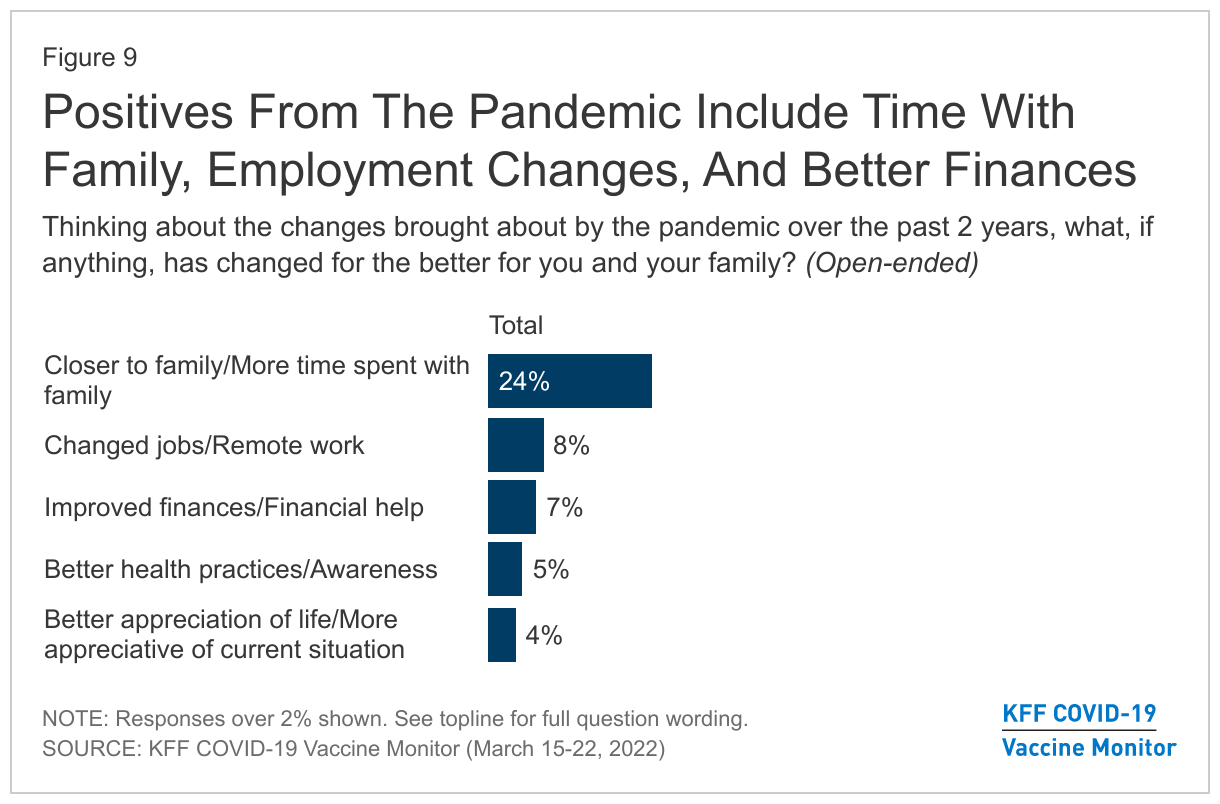
When asked if anything has changed for the better in the last two years, 24% say they are closer to their family or have spent more time with their families. Some (8%) also say that job changes or remote work were a positive change, 7% cited improvements in their financial situation, 5% said they had better health practices or awareness, and 4% cited a general appreciation of life or their current situation. A third of respondents said nothing changed for the better.
In their own words: Thinking about the changes brought about by the pandemic over the past two years, what, if anything, has changed for the better for you and your family?“
Being able to use telehealth communications for doctors and by doing a lot of things by phone and email now, very convenient for families.” – 25 year old, female, White, independent, Kentucky
“Closer bonding with family and more stability with work life.” – 30 year old, male, Asian, independent, Texas
“Eating more prepared meals from home and saving money.” – 66 year old, female, White, Republican, Illinois
“Better handwashing and wearing a mask has helped with overall health.” – 66 year old, male, White, Democrat, California
“Gives me a good excuse to get out of dinner with in-laws.” – 37 year old, other, Hispanic, independent, Pennsylvania
“It helped cherish the moments you have with each other and to be less wasteful. Realize that habits/behaviors can change all the time; make the best changes.” – 39 year old, female, Black, Democrat, Tennessee
“The stimulus checks helped keep me out of debt.” – 52 year old, female, White, independent, Colorado
“More remote opportunities in education and employment.” – 21 year old, male, White, Democrat, Maryland
Methodology
This KFF Health Tracking Poll/COVID-19 Vaccine Monitor was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted March 15-22, 2022 online and by telephone among a nationally representative sample of 1,243 U.S. adults, conducted in English (1,188) and in Spanish (55). The sample includes 1,004 adults reached through the SSRS Opinion Panel either online or over the phone (n=39 in Spanish). The SSRS Opinion Panel is a nationally representative probability-based panel where panel members are recruited randomly in one of two ways: (a) Through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Groups (MSG) through the U.S. Postal Service’s Computerized Delivery Sequence (CDS); (b) from a dual-frame random digit dial (RDD) sample provided by MSG. For the online panel component, invitations were sent to panel members by email followed by up to three reminder emails. 974 panel members completed the survey online and panel members who do not use the internet were reached by phone (30).
Another 239 (n=16 in Spanish) interviews were conducted from a random digit dial telephone sample of prepaid cell phone numbers obtained through MSG. Phone numbers used for the prepaid cell phone component were randomly generated from a cell phone sampling frame with disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification was based on incidence of the race/ethnicity groups within each frame.
The combined cell phone and panel samples were weighted to match the sample’s demographics to the national U.S. adult population using data from the Census Bureau’s 2021 Current Population Survey (CPS). Weighting parameters included sex, age, education, race/ethnicity, region, and education. The sample was also weighted to match patterns of civic engagement from the September 2017 Volunteering and Civic Life Supplement data from the CPS. The sample was also weighted to match frequency of internet use from the National Public Opinion Reference Survey (NPORS) for Pew Research Center. The weights take into account differences in the probability of selection for each sample type (prepaid cell phone and panel). This includes adjustment for the sample design and geographic stratification of the cell phone sample, within household probability of selection, and the design of the panel-recruitment procedure.
The margin of sampling error including the design effect for the full sample is plus or minus 4 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
This work was supported in part by grants from the Chan Zuckerberg Initiative DAF (an advised fund of Silicon Valley Community Foundation), the Ford Foundation, and the Molina Family Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
| Group | N (unweighted) | M.O.S.E. |
| Total | 1,243 | ± 4 percentage points |
| COVID-19 vaccination status | ||
| Have gotten at least one dose of the COVID-19 vaccine | 981 | ± 4 percentage points |
| Have not gotten the COVID-19 vaccine | 259 | ± 7 percentage points |
| Race/Ethnicity | ||
| White, non-Hispanic | 748 | ± 5 percentage points |
| Black, non-Hispanic | 188 | ± 10 percentage points |
| Hispanic | 213 | ± 9 percentage points |
| Party identification | ||
| Democrat | 396 | ± 6 percentage points |
| Republican | 321 | ± 7 percentage points |
| Independent | 310 | ± 8 percentage points |
| Registered voters | ||
| Total voters | 1,036 | ± 4 percentage points |
| Democratic voters | 351 | ± 7 percentage points |
| Republican voters | 293 | ± 7 percentage points |
| Independent voters | 253 | ± 9 percentage points |
Endnotes
- The latest data from the KFF COVID-19 Vaccine Monitor includes interviews conducted over the phone and online using a probability-based sample. ↩︎