KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Note: To get the latest data on Medicaid enrollment, disenrollment, and procedural disenrollments, visit KFF’s Medicaid Enrollment and Unwinding Tracker.The analysis below uses CMS data about Medicaid and CHIP enrollment through December 2022, providing information about Medicaid enrollment levels during the pandemic.
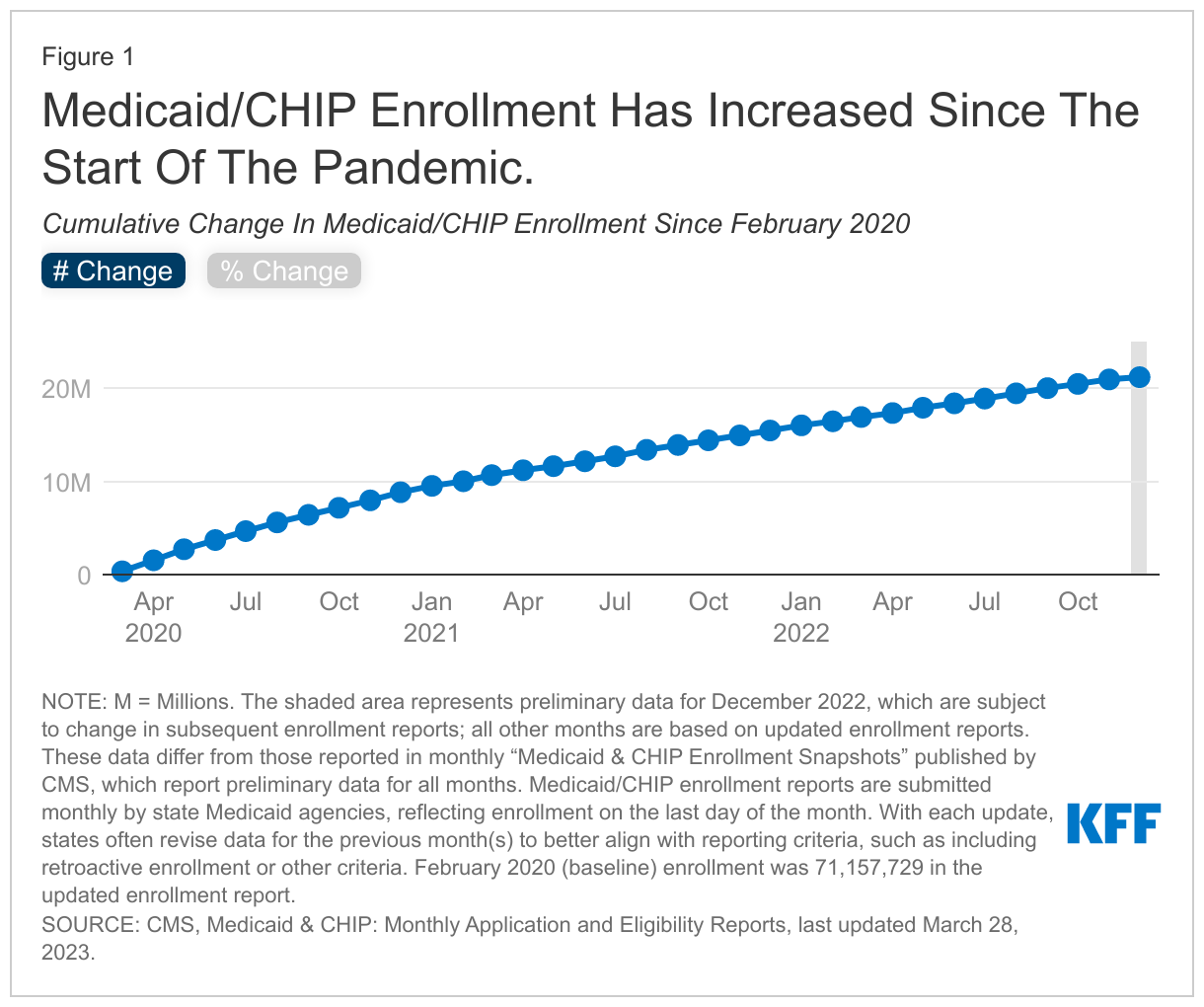
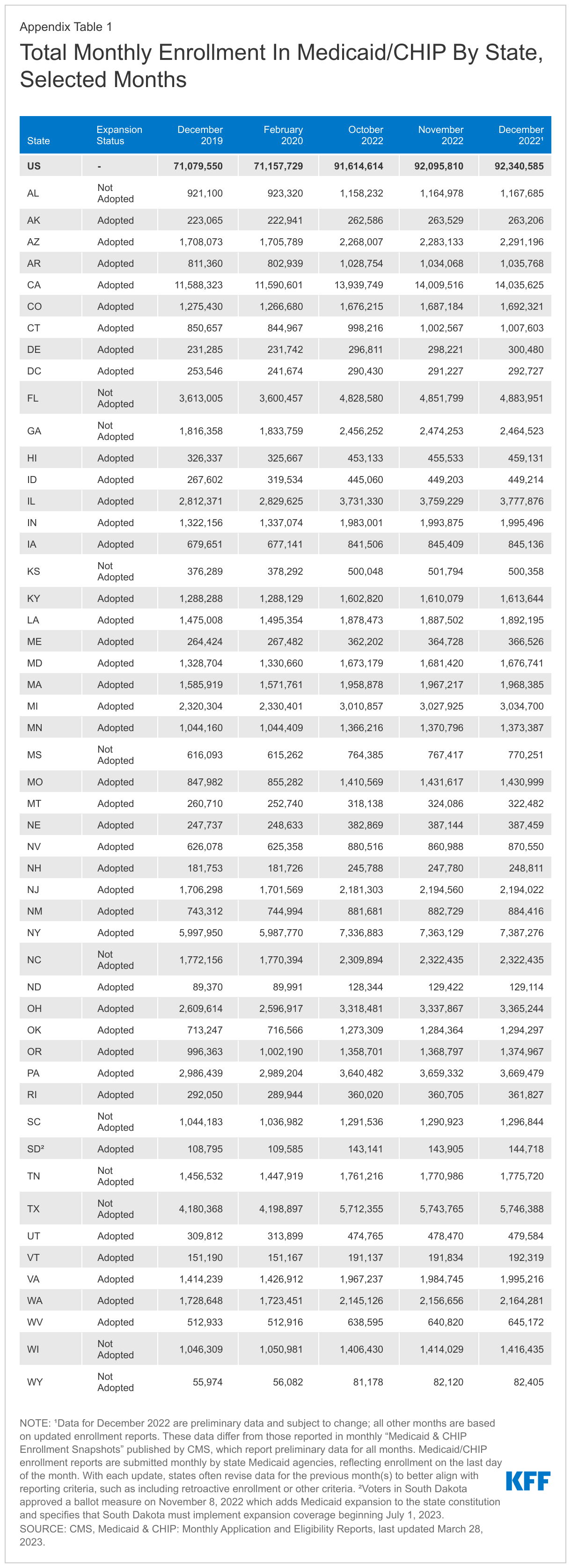
This data note looks at national and state-by-state Medicaid and CHIP enrollment data through December 2022. After declines in enrollment from 2017 through 2019, preliminary data for December 2022 show that total Medicaid/CHIP enrollment grew to 92.3 million, an increase of 21.2 million from enrollment in February 2020 (29.8%), right before the pandemic and when enrollment began to steadily increase (Figure 1).1 Increases in enrollment may reflect changes in the economy, changes in policy (like recent adoption of the Medicaid expansion in the Affordable Care Act), and the temporary continuous enrollment provision created by the Families First Coronavirus Response Act (FFCRA). Under the continuous enrollment provision, states generally cannot disenroll Medicaid enrollees while the provision is still in effect and in exchange, states receive a temporary increase in the federal Medicaid match rate. The continuous enrollment provision has halted churning in Medicaid – the temporary loss of coverage in which enrollees disenroll and then re-enroll within a short period of time – in addition to preventing Medicaid coverage loss during the pandemic. As part of the Consolidated Appropriations Act, signed into law in December 2022, Congress set an end to the continuous enrollment provision on March 31, 2023, and will phase down the enhanced federal Medicaid matching funds through December 2023. States that accept the enhanced federal funding can resume disenrollments beginning in April 2023 but must meet certain reporting and other requirements during the unwinding process. KFF estimates that Medicaid/CHIP enrollment will reach roughly 95 million enrollees in March 2023 before states may resume disenrollments during the “unwinding” of the continuous enrollment provision.
The information in this data note is based on KFF analysis of the Centers for Medicare and Medicaid Services (CMS) Performance Indicator Project Data. Medicaid/CHIP enrollment data are submitted monthly by state Medicaid agencies and, with each monthly update, states often revise the previous months’ enrollment to include retroactive enrollment and to better align with reporting criteria. Except for the latest month’s enrollment (December 2022), this brief reports data from the updated enrollment reports for all other months to reflect the most current enrollment data possible. However, the data presented in this brief will differ from those presented in monthly Medicaid and CHIP Enrollment Snapshots published by CMS, which use exclusively preliminary enrollment reports for all months.
Medicaid/CHIP enrollment increased following the implementation of the Affordable Care Act (ACA) but was declining in the two years prior to the pandemic. Following the implementation of the ACA Medicaid expansion to low-income adults in 2014, there were large increases in Medicaid and CHIP enrollment across states that followed steady growth in coverage of children over the past decade. These increases reflected enrollment among newly eligible adults in states that implemented the expansion as well as enrollment among previously eligible adults and children due to enhanced outreach and enrollment efforts and updated enrollment procedures tied to the ACA. This trend began reversing when enrollment started to decline in 2018 and continued to decline in 2019. Total enrollment fell from 73.3 million in December 2017 to 71.0 million in December 2019, a decline of 2.3 million people or 3.1%. Month-to-month enrollment declines slowed but continued until February 2020. The declines in enrollment, in part, reflected a robust economy, but experiences in some states suggested that they may have also reflected enrollment losses among people who were still eligible for coverage due to challenges completing enrollment or renewal processes.
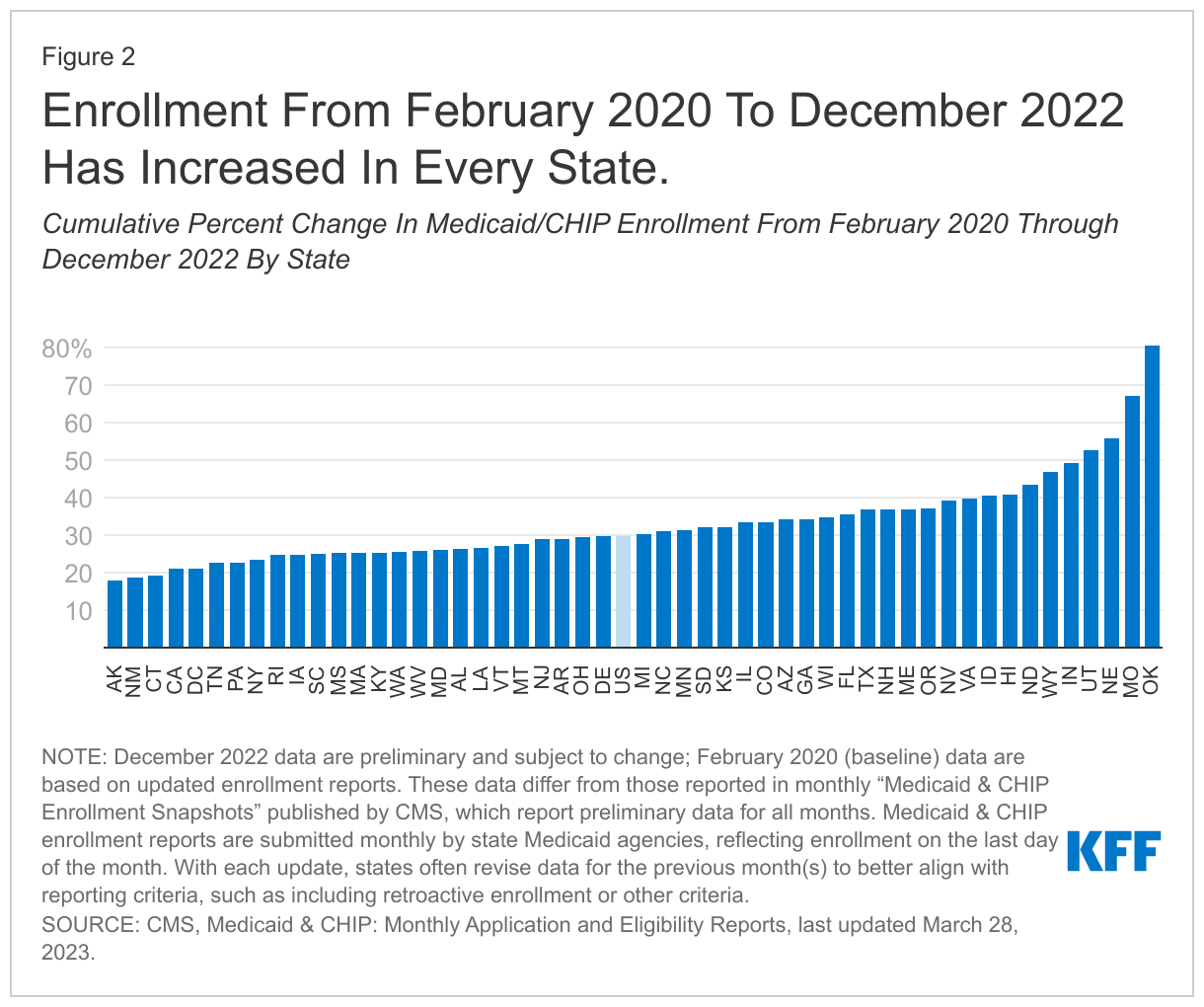
Data show that Medicaid/CHIP enrollment is increasing amid the coronavirus pandemic, growing by 21.2 million enrollees or 29.8% from February 2020 to December 2022. Over this period, all states experienced total Medicaid/CHIP enrollment growth ranging from 18.1% to 80.6% (Figure 2).2 The state with the largest growth since February 2020, Oklahoma, implemented the Medicaid expansion on July 1, 2021. Four other states have implemented expansion since 2020 – Utah and Idaho in January 2020, Nebraska in October 2020, and Missouri (where the state began to process applications3 in October with coverage retroactive to 7/1/2021) – contributing to higher-than-average rates of enrollment growth in these states as well.
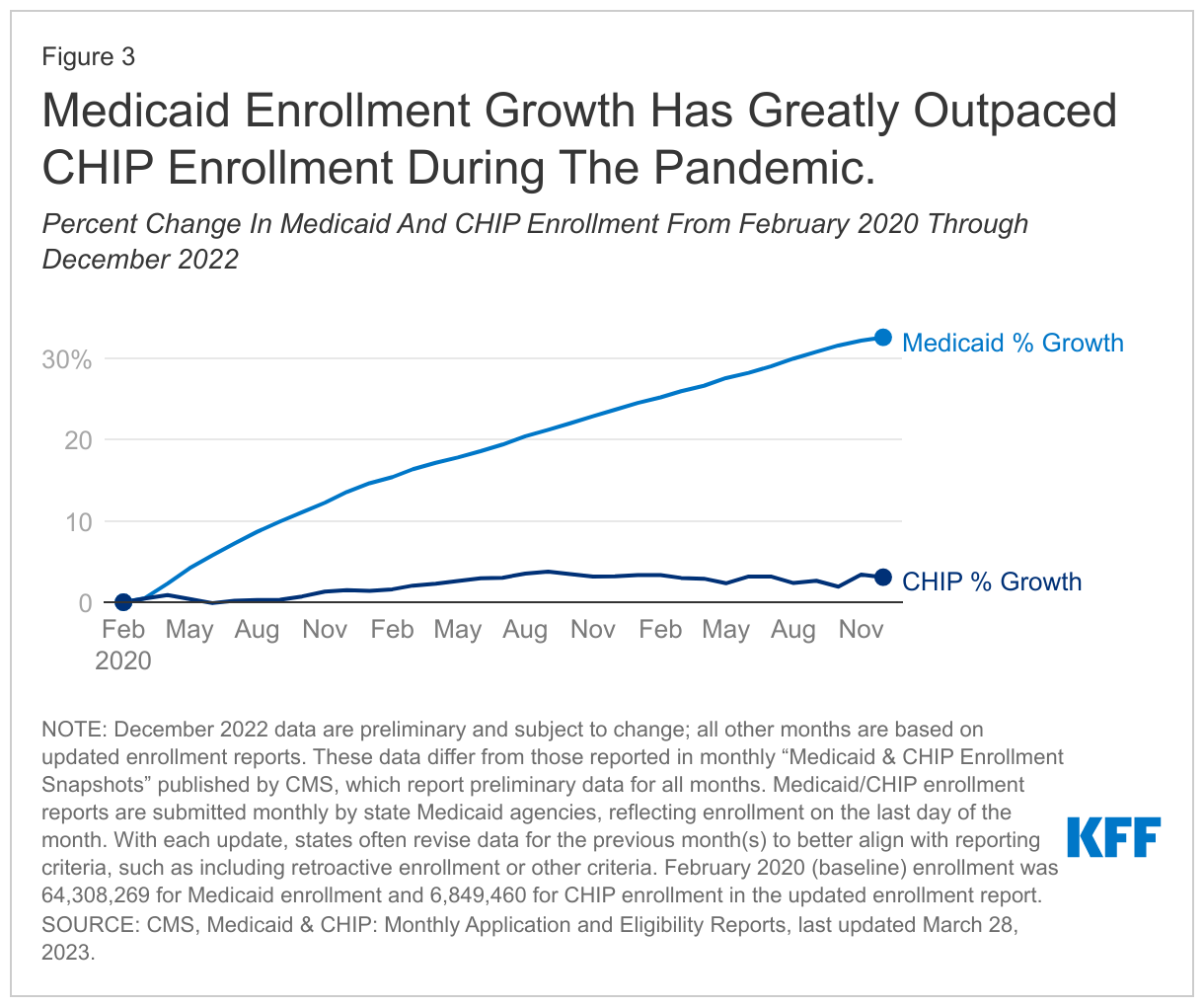
Virtually all growth was concentrated in Medicaid, which grew by 32.6% (21.0 million enrollees) from February 2020 to December 2022 data (Figure 3). Conversely, CHIP has seen less enrollment growth since February 2020 (3.1% or 211,000 enrollees) and several states (17) have seen declines in CHIP enrollment from February 2020 through December 2022 reports. These declines in CHIP enrollment for some states could reflect changes in family income, causing children to move from CHIP to Medicaid coverage. As discussed below, all states reported increases in child enrollment for Medicaid/CHIP overall during this time period.
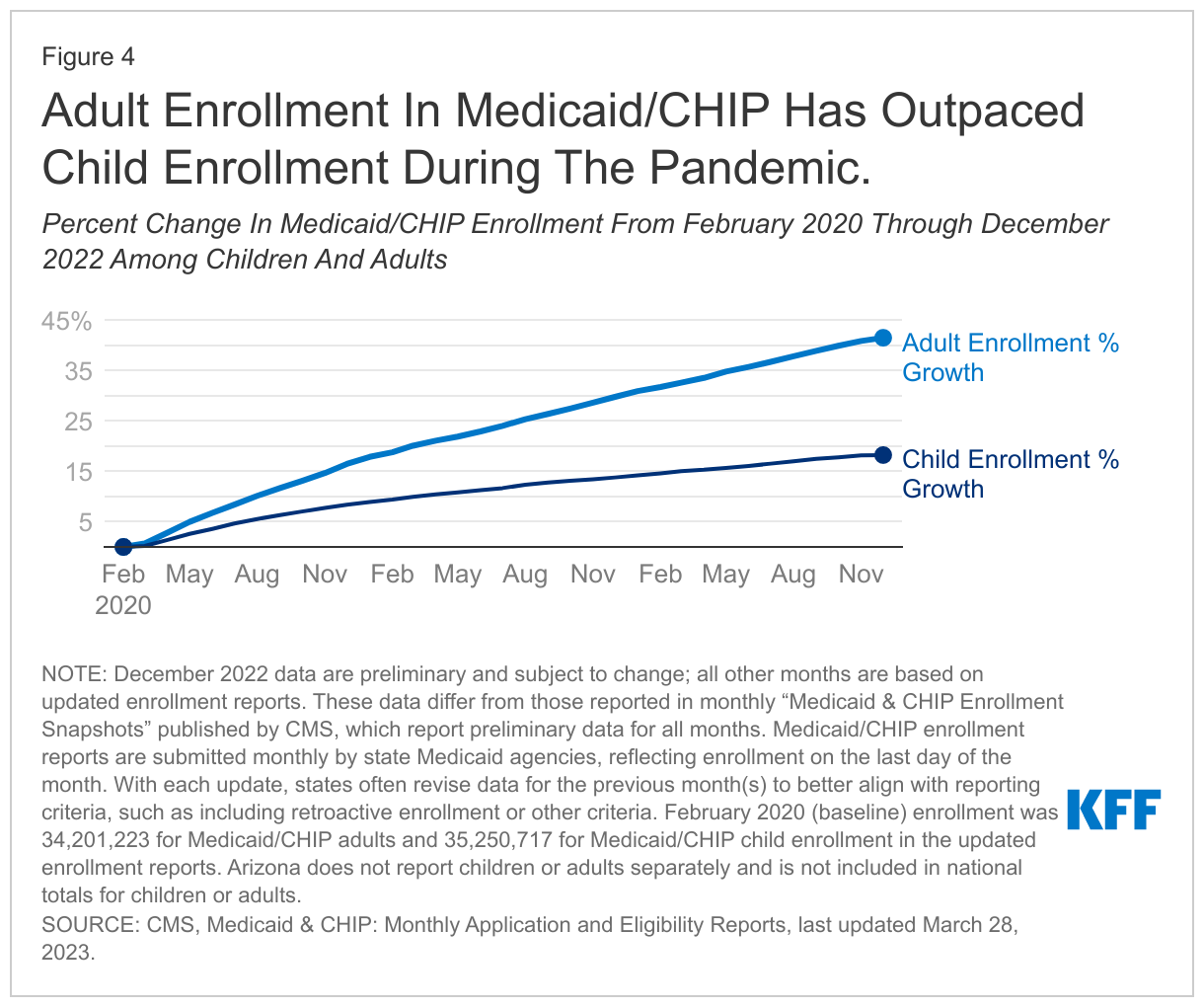
Adult enrollment in Medicaid/CHIP has increased rapidly during the pandemic, growing by 41.5% from February 2020 through December 2022 enrollment reports (Figure 4). This growth amounts to an additional 14.2 million adults in the 49 states and DC that report adult/child monthly enrollment (Arizona does not report children or adults separately). As mentioned above, five states began newly enrolling expansion adults since January 2020 (Idaho, Missouri, Nebraska, Oklahoma, and Utah), contributing to increased adult enrollment. Child enrollment grew as well, but at a slower pace: 18.2% or 6.4 million enrollees in the same period. Still, every state reporting these data saw an increase in child Medicaid/CHIP enrollment from February 2020, despite declines in CHIP enrollment in some states (as discussed above).
Many could lose coverage as states resume disenrollments starting in April 2023, once the continuous enrollment provision expires. As part of the Consolidated Appropriations Act, signed into law in December 2022, Congress set an end to the continuous enrollment provision on March 31, 2023, allowing states to resume disenrollments in April 2023, though states must meet certain reporting and other requirements during the unwinding process. plan to take the full 12 to 14 months allowed by CMS for completing redeterminations and returning to normal operations, though some states will complete the process more quickly, with five states planning to take 9 to 12 months and one state planning to take less than 9 months (data are currently unavailable for two states, Ohio and Texas). During this time, millions could be disenrolled from Medicaid if they no longer qualify or if they face administrative barriers during renewal even if they continue to be eligible. How states manage the large volume of redeterminations during the “unwinding” of the continuous enrollment provision, as well as how states engage with enrollees and other stakeholders, will impact the continuity of coverage for millions of Medicaid enrollees.
Medicaid/CHIP enrollment reports are submitted monthly by state Medicaid agencies, reflecting enrollment on the last day of the month. With each update, states often revise data for the previous month(s) to better align with reporting criteria, such as including retroactive enrollment or other criteria. December 2022 data are preliminary and subject to change; all other months presented in this brief are based on updated enrollment reports. The data presented in this brief differ from those reported in monthly “Medicaid & CHIP Enrollment Snapshots” published by CMS, which use exclusively preliminary enrollment reports for all data reported. ↩︎
Although all states report an increase in Medicaid/CHIP enrollment from February 2020 through December 2022, some states have occasionally reported month-to-month decreases in their updated enrollment reports starting in late 2020 and into 2022 (AK, CT, DE, ID, IL, IN, KS, KY, LA, MT, NM, ND, PA, RI, UT, and WV). Generally, these month-to-month declines appear sporadic and so do not likely represent a trend. In July 2021, Kentucky’s total Medicaid/CHIP enrollment decreased by 6.7% and the state attributed the decrease to removing individuals who had been receiving temporary coverage under the state’s presumptive eligibility policy during the pandemic, according to the CMS Enrollment Snapshot for July 2021. Month-to-month decreases in Medicaid/CHIP enrollment generally represent data reporting issues that have not yet been resolved by states, or they may represent data reporting corrections where historical data has not yet been corrected. Nine states (AK, GA, IA, KS, MD, MO, MT, NJ, and ND) reported a decline in total Medicaid/CHIP enrollment from the updated November 2022 report to the preliminary December 2022 report. These declines were generally small and reflect preliminary enrollment data for December 2022, which is typically updated in subsequent enrollment reports as states update their enrollment counts (for example, to better capture retroactive enrollment or to better align with CMS’s reporting criteria). In many cases, updated reports show slight increases in enrollment from preliminary reports. ↩︎
Missouri has also expanded Medicaid since 2020. Medicaid coverage under expansion began when the state started processing applications in October 2021, with coverage retroactive to July 1, 2021, consistent with a state supreme court order. However, news reports indicate that the state was slow to process applications and enroll newly eligible expansion adults, although the state has worked with CMS to streamline the enrollment process and had made improvements in average application processing times as of September 2022. The state has still had higher-than-average enrollment increases from February even prior to implementing expansion. ↩︎
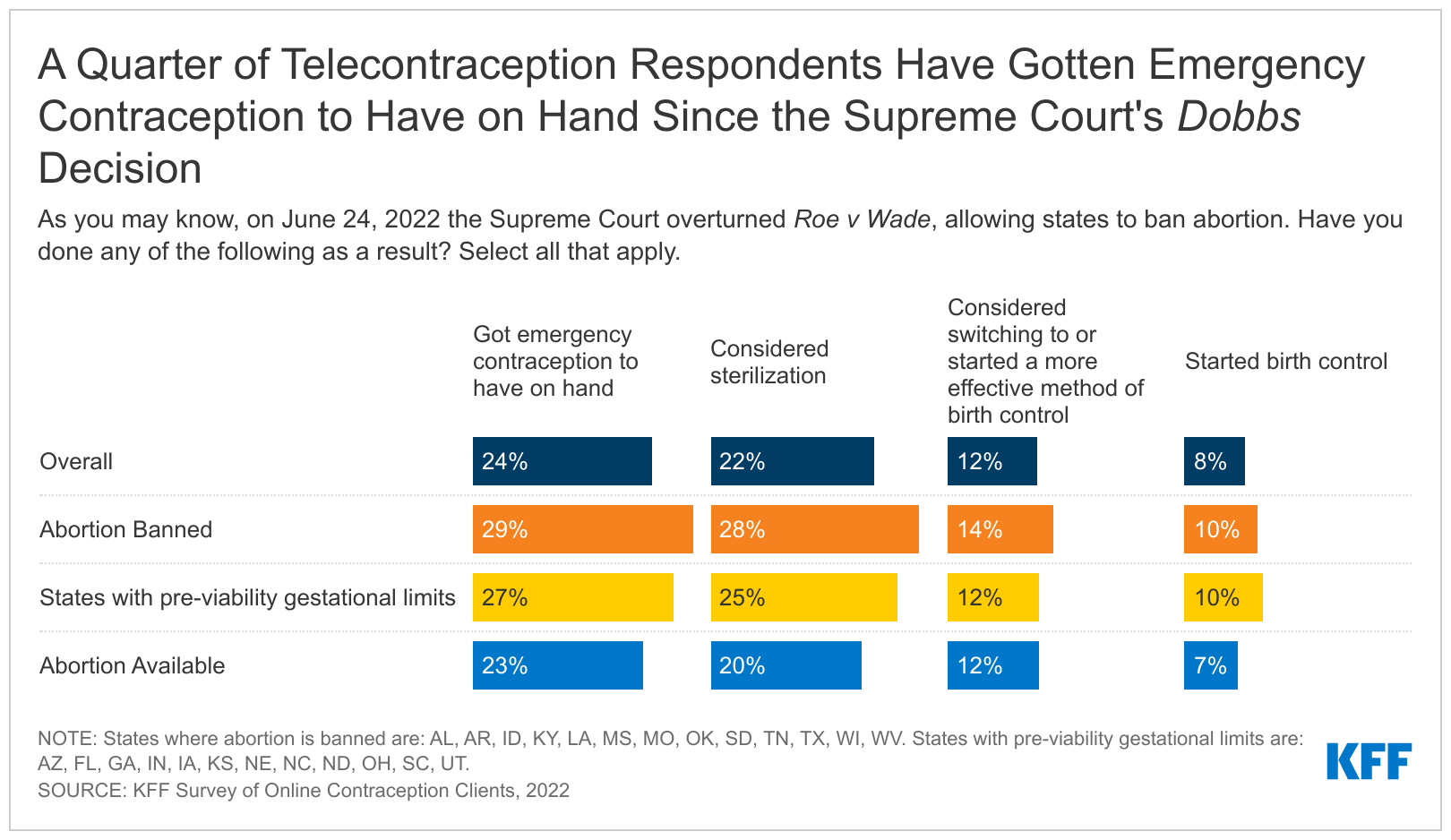
According to a new KFF survey with a nonprobability sample of clients from four online sources of contraception, one in four clients said they got emergency contraception to have on hand because of the Supreme Court’s decision to overturn Roe v. Wade. Additionally, more than a fifth (22%) said they have considered sterilization, 12% reported that they considered switching to or started using a more effective method of birth control, and eight percent said that they began to use birth control because of the Dobbs decision. These findings were consistent across states regardless of whether or not abortion was banned.
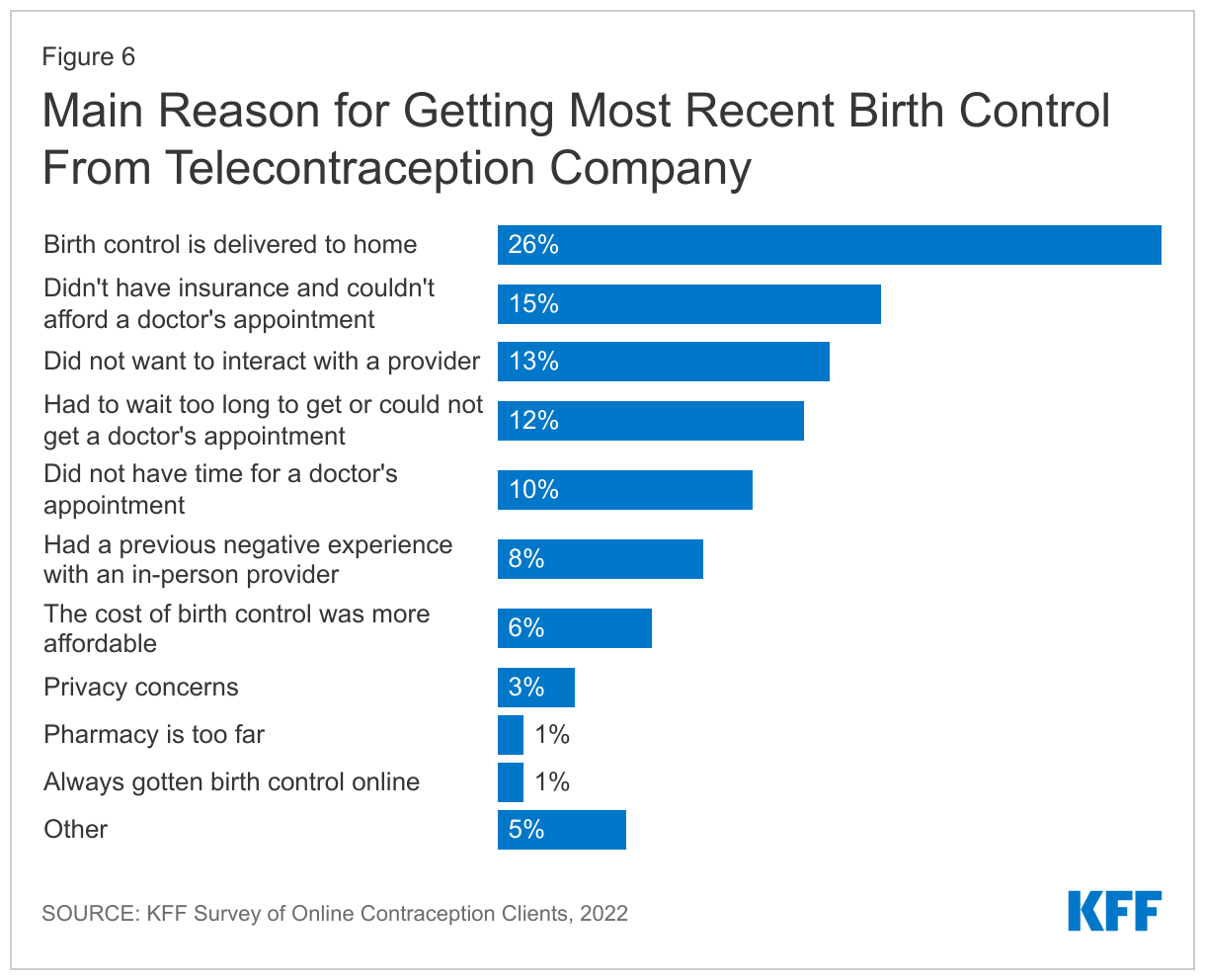
Respondents said they turned to telecontraception companies for birth control for various reasons, but the most frequently cited reason is that the birth control is delivered to their home (26%). Others noted privacy, difficulties getting appointments, and prior negative interactions with in-person care. Larger shares of LGBT+ individuals compared to non-LGBT+ cited a previous negative experience with an in-person provider as their main reason for getting their most recent birth control prescription online (11% vs. 7%). Nearly one in five (18%) respondents cited the COVID-19 pandemic as the reason they first accessed birth control online.
These findings come from the KFF Survey of Online Contraception Clients, which was sent to active contraceptive clients over the age of 18 who had received contraception from their company in the past year (272,800 clients) by each of the four participating telecontraception companies. The survey was fielded from October 13 to December 8, 2022. A total of 5,925 telecontraception clients participated in the survey. This survey is based on a nonprobability sample and so its results are not generalizable to all telecontraception users. Learn more about who uses telecontraception and why in the brief, “Who Uses Telecontraception and Why? A Closer Look at Clients of Four Telecontraception Companies.”
Based on the findings of a non-probability sample of 6,000 survey respondents from four telecontraception companies, the leading reason respondents cite for getting their most recent birth control via telecontraception is that it is delivered to their home (26%). Others cite privacy, difficulties getting appointments, and prior negative interactions with in-person care. Nearly one in five (18%) of respondents cited the COVID-19 pandemic as the reason they first accessed birth control online.
The vast majority of respondents using telecontraception are women and two-thirds are 35 and younger, including larger shares who don’t have health insurance or who are LGBT+ compared to a nationally representative sample of contraceptive users in U.S. population.
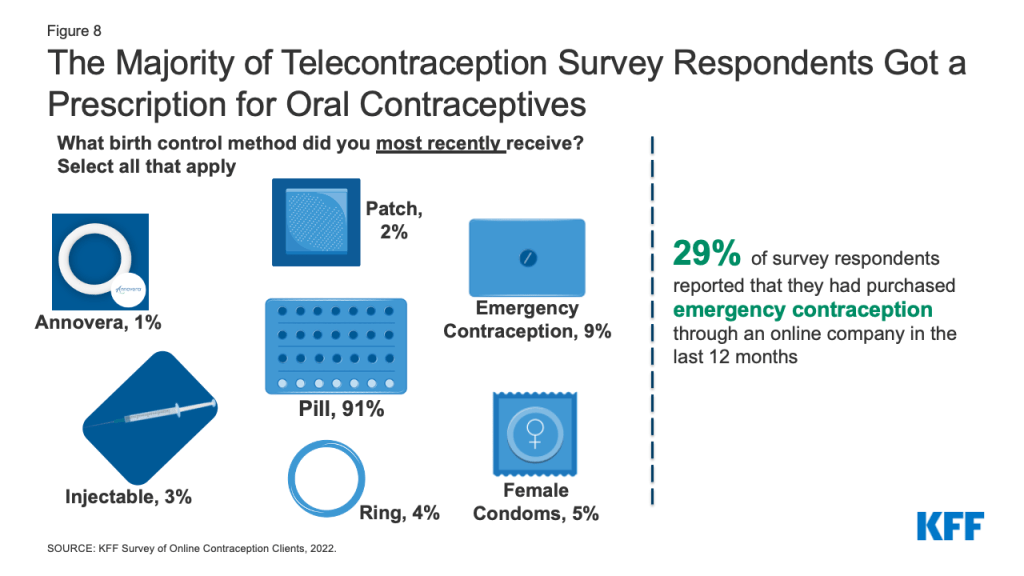
The most frequently received contraceptive method reported by telecontraception respondents is oral contraceptives (91%), followed by emergency contraceptive pills (9%). Nearly three in ten (29%) respondents overall say they purchased emergency contraception through an online company in the last 12 months.
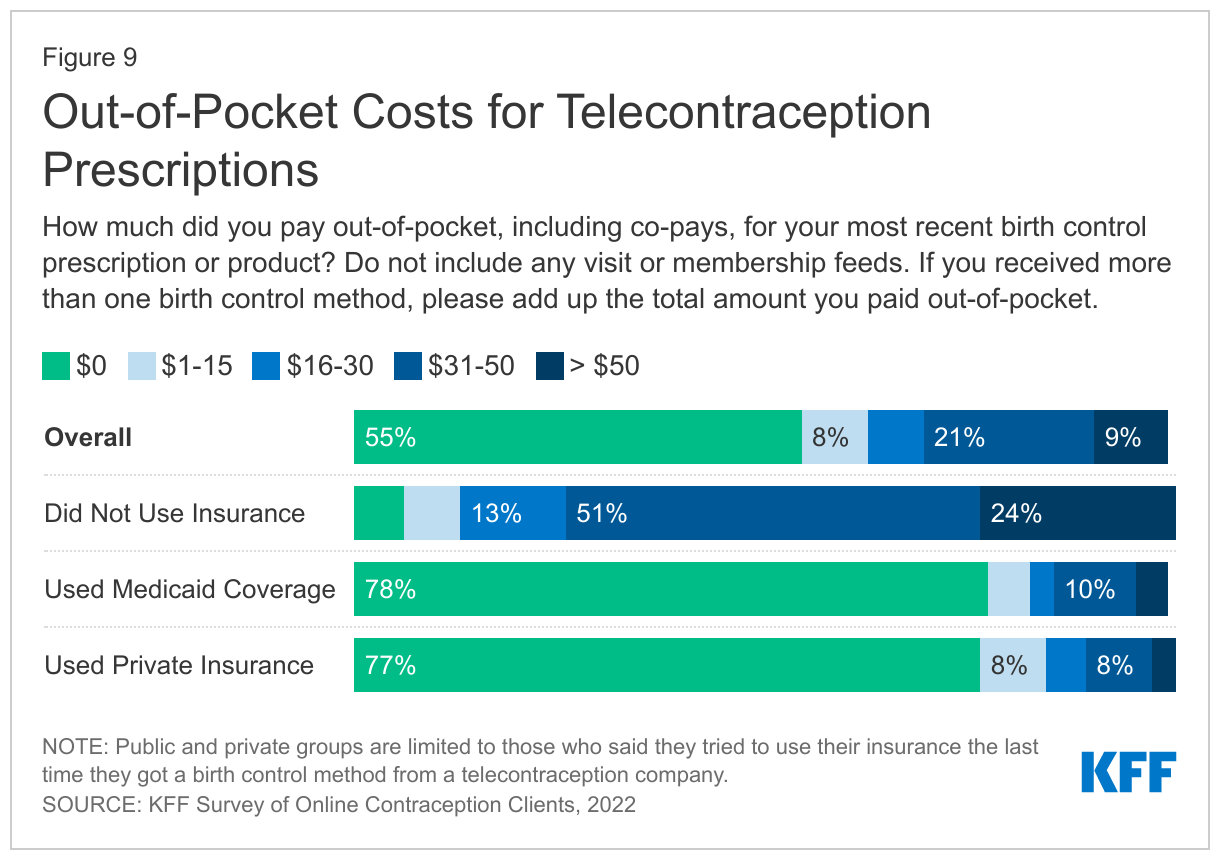
About three in four respondents with private insurance or Medicaid who tried to use their insurance for telecontraception paid nothing out-of-pocket for their birth control method. Half (51%) of those who did not use insurance paid between $31 and $50 and about a quarter (24%) paid over $50 for their birth control. The companies do charge a consultation or membership fee for all of their users and this cost is not covered by insurance.
Four in ten (43%) respondents say they do not have a regular doctor and one in five (20%) have never had an in-person birth control visit.
Almost a quarter (24%) of respondents report they have gotten emergency contraception to have on hand and over a fifth (22%) have considered sterilization in response to the Supreme Court’s decision to overturn Roe v Wade. These findings were fairly consistent across states regardless of whether abortion was banned or not.
Introduction
In recent years there has been increased interest in making contraception more accessible, particularly outside of traditional clinical settings. These efforts have gained urgency in wake of the Supreme Court decision in Dobbs v Jackson Women’s Health, which overturned Roe v. Wade, and the COVID-19 pandemic. However, even prior to both of these events, online companies had started to offer consumers the option of having contraceptives delivered to their home without needing to go for an in-person healthcare visit. While only a small share of people say they have used these online platforms, companies have reported a rapid growth in clients during the COVID-19 pandemic and an increase in emergency contraception orders since the Dobbs decision. There has been very little research to date on who uses telecontraception and why they choose to get their birth control online aside from a recent study focused on one online platform. In order to learn more about who is using telecontraception in the Fall of 2022, KFF conducted a survey of current clients from four telecontraception companies. The responses from individuals who responded to the survey across the four companies have been combined to give a snapshot of who is using telecontraception.
Methods
The KFF Survey of Online Contraception Clients was designed and analyzed by researchers at KFF. The survey was conducted via SurveyMonkey using a unique survey link that was sent to four telecontraception companies who then sent the link to their active contraceptive clients over the age of 18 who had received contraception from their company in the past year (272,800 clients). The survey was fielded from October 13 to December 8, 2022. A total of 5,925 telecontraception clients participated in the survey. Clients had an opportunity to be entered into a drawing for twelve $100 Amazon gift cards (three for each company) by submitting their email after completing the survey.
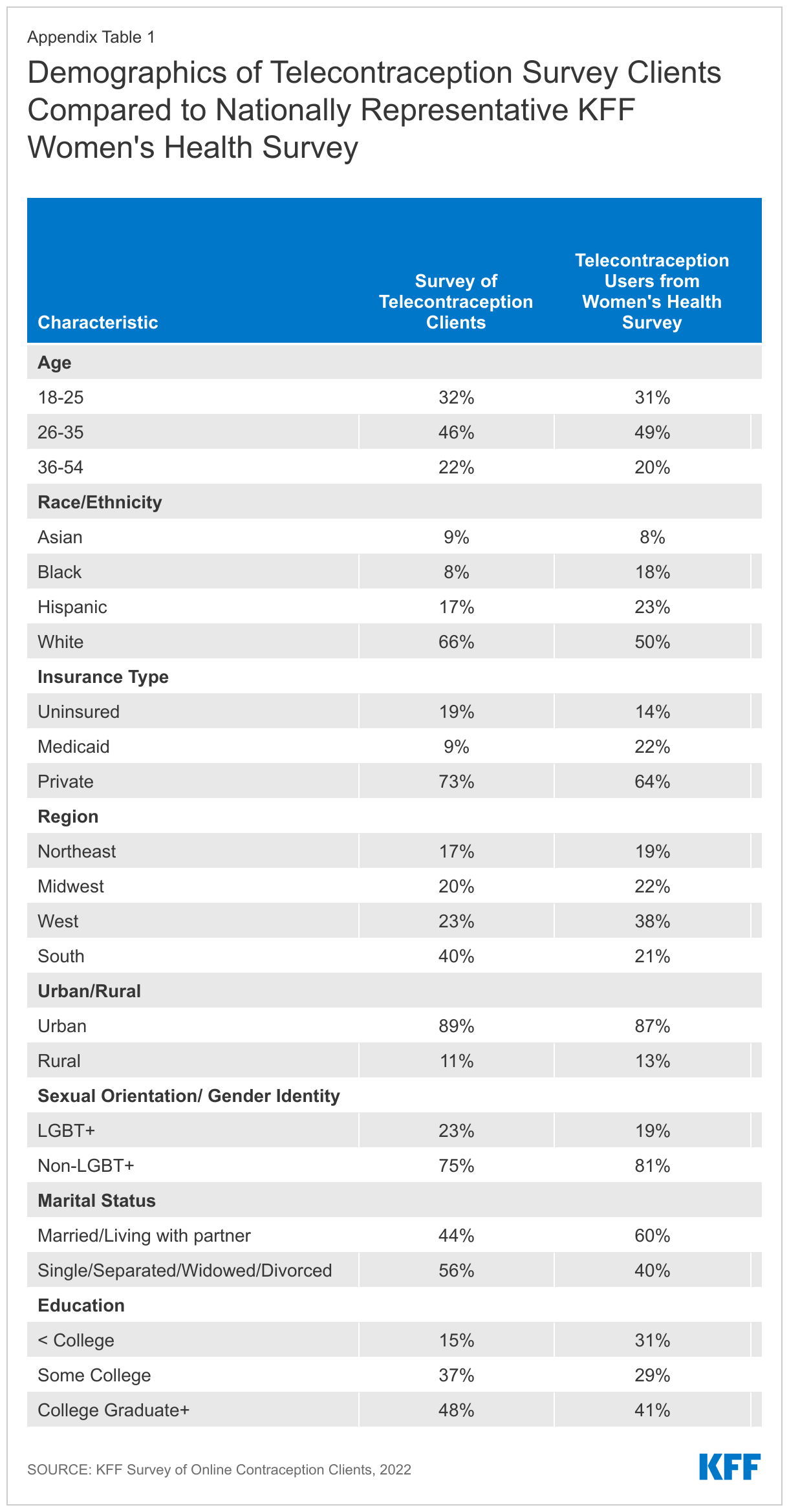
This survey is a non-probability sample based on telecontraception clients that responded to the survey from the four companies. There were not large differences in demographics and survey responses across the four companies surveyed, so the data for survey respondents from all four companies were combined to give an overall picture of telecontraception clients. These data were collected using a non-probability sampling frame, and the results are not necessarily representative of the broader population that receives online contraception. However, the overall demographics of telecontraception clients from this sample closely matched a similar sample of women who said they have received a prescription or obtained a health care service from an online company in the prior 12 months obtained from KFF’s 2022 Women’s Health Survey, a nationally representative sample of women (See Appendix Table 1). Therefore, no additional adjustments, such as weighting, were made to the sample.
Demographics of Telecontraception Survey Respondents
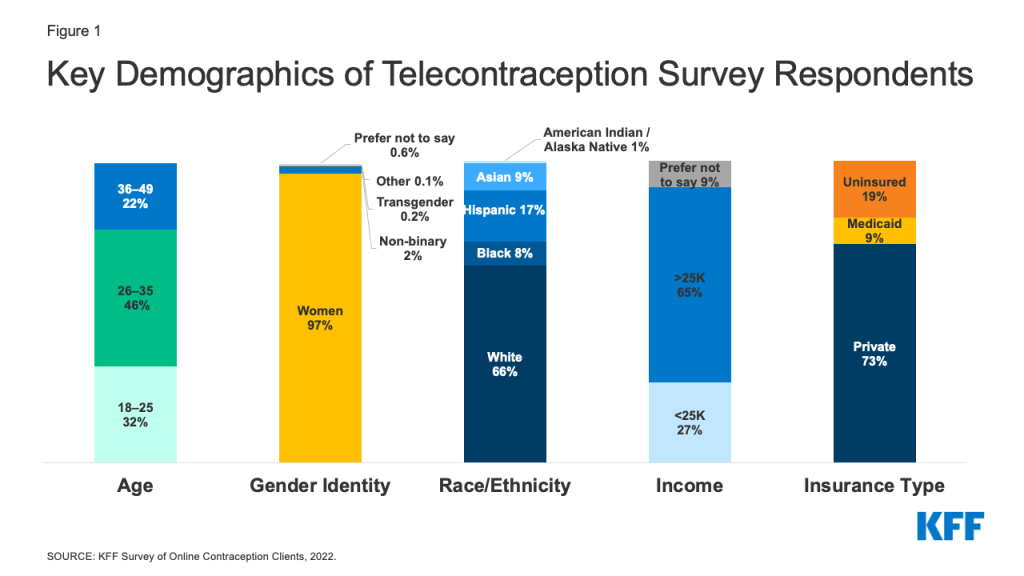
This report presents a snapshot of telecontraception clients of four companies who responded to the KFF survey. The vast majority (97%) of responding telecontraception clients identify as women, while 2% are non-binary, 1% prefer not to say, and less than 1% identify as men, transgender or another gender. The four companies surveyed for this project do not offer male condoms, which explains why there are so few male clients in the sample.
Telecontraception clients responding to this survey ranged in age from 18-54. The largest share of those using telecontraception are between the ages of 26-35 (46%), about a third are ages 18-25 (32%), and over one in five are ages 36-54 (22%). Compared to females using short acting reversible contraception (such as the pill, injectables, patches or condoms, (SARC)) from the nationally representative KFF Women’s Health Survey, larger shares of telecontraception respondents fell in the 26-35 age range (46% vs. 35%) and smaller shares fell in the 36-54 age range (22% vs. 35%).
The majority of telecontraception survey respondents are White (66%), 17% are Hispanic, less than one in ten are Asian (9%), Black (8%), and American Indian/Alaska Native (1%). Larger shares of telecontraception respondents were White compared to those using SARC nationally (66% vs. 55%). Nearly two-thirds (65%) of telecontraception survey respondents earn more than $25,000 a year, while over one in four (27%) earn less than $25,000 a year, and another 9% prefer not to say (Figure 1).
Figure 1: Key Demographics of Telecontraception Survey Respondents
Seven in ten respondents have private insurance (73%), about one in ten (9%) have Medicaid coverage, and almost one in five (19%) are uninsured. Compared to our nationally representative sample of SARC users, the share of those in the survey who have Medicaid coverage is smaller (9% vs. 20% nationally) and those who are without insurance is larger (19% in this survey vs. 9% nationally).
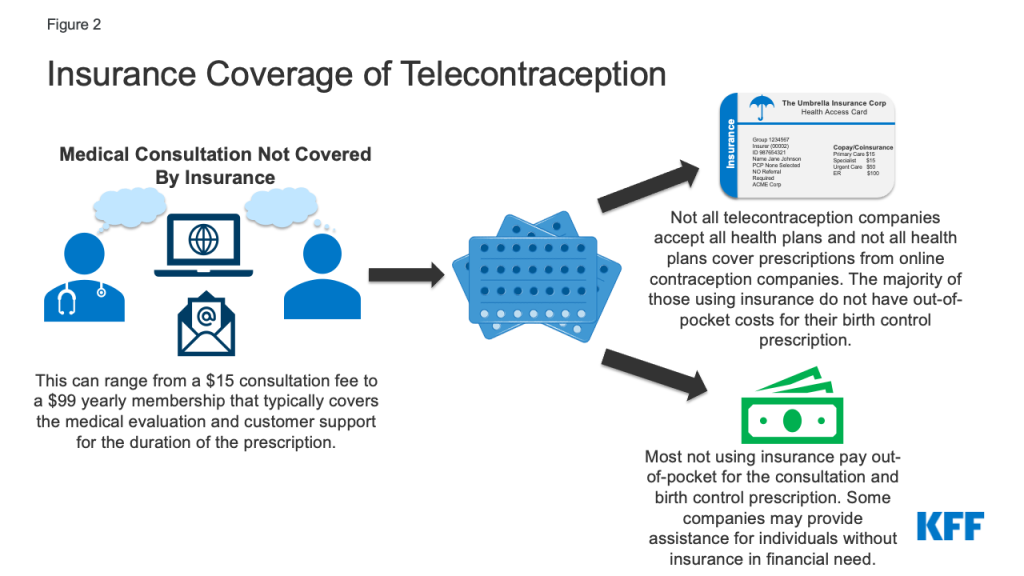
Figure 2: Insurance Coverage of Telecontraception
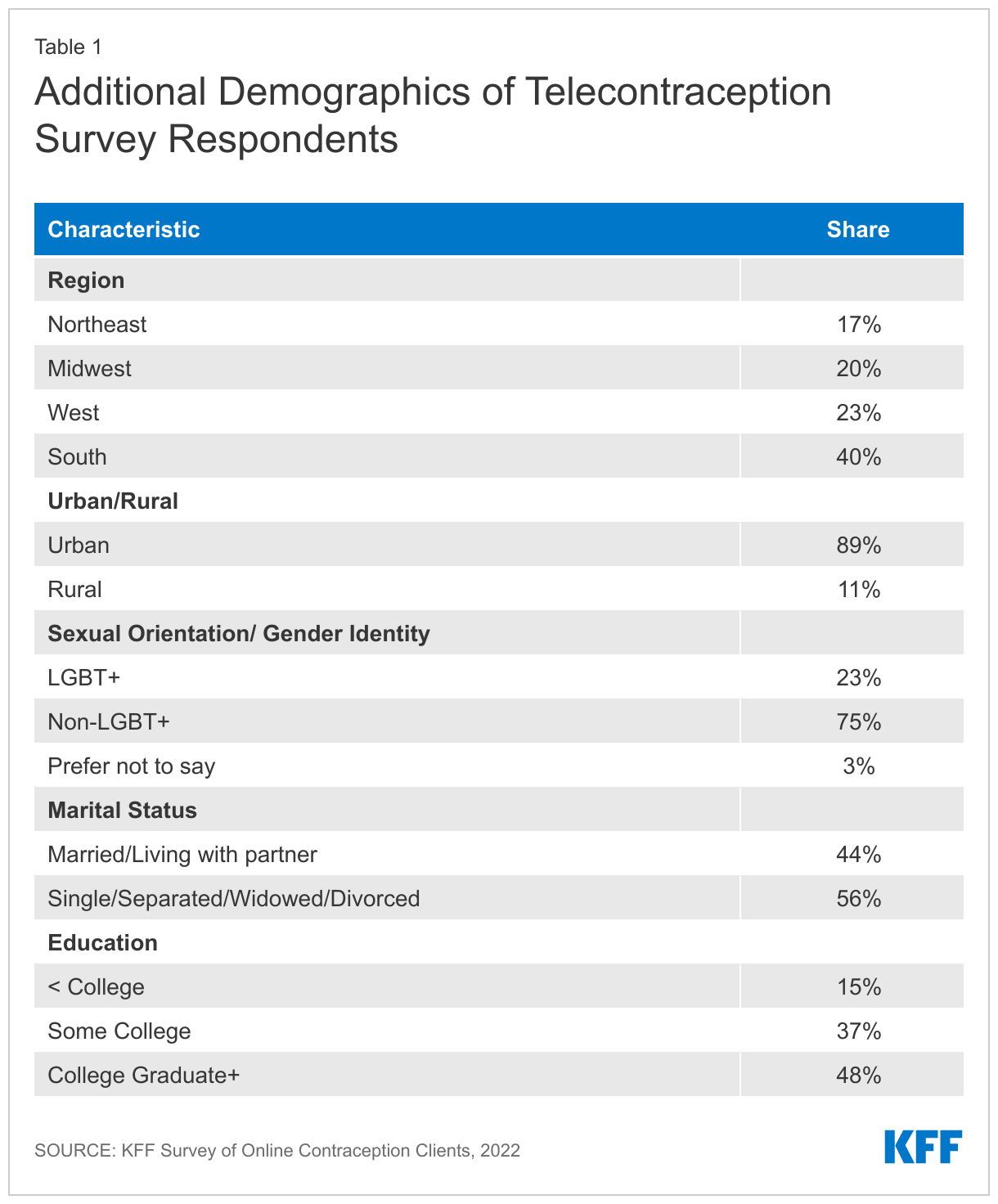
The largest share of respondents live in the South (40%), nearly a quarter are in the West (23%), one in five reside in the Midwest (20%), and 17% live in the Northeast United States, which is very similar to SARC users in our nationally representative sample (Appendix Table 1).
Nearly a quarter (23%) of respondents are LGBT+, three-quarters are non-LGBT+ (75%), and 3% prefer not to say. The share of respondents who are LGBT+ is slightly higher than the share of females who use SARC and identify as LGBT+ (23% vs. 17%).
Finally, a larger share of respondents are single, separated, widowed, or divorced compared to married or living with a partner (56% vs. 44%) and eight in ten have some college education compared to 15% with less than a college education (85% vs. 15%) (Table 1). Smaller shares of SARC users nationally are single, separated, widowed or divorced (42% vs. 56%) and larger shares of telecontraception respondents have some college education compared to SARC users nationally (85% vs. 75%).
Experiences with Telecontraception
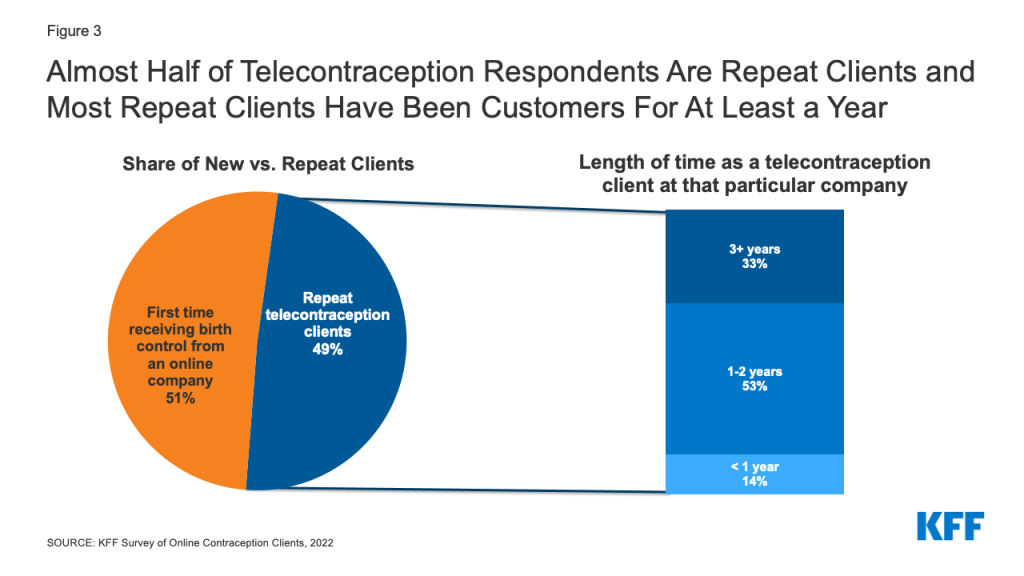
While telecontraception may be a new avenue for accessing contraception for many, nearly half (49%) of all telecontraception clients who responded to the survey say this is not the first time they have received their birth control from an online contraception company. Among those who have received birth control multiple times from an online contraception provider, the majority (86%) have been clients at the company for which they completed the survey for at least a year (Figure 3). The length of time people had been clients varied by company, with the majority of respondents at two of the companies saying they had been clients for at least a year (Company A = 85% and Company B = 95%), while about half of respondents at the other two companies say they have been clients for at least a year (Company C = 45% and Company D = 51%). All of the participating companies have been in business for a number of years.
Figure 3: Almost Half of Telecontraception Respondents Are Repeat Clients and Most Repeat Clients Have Been Customers For At Least a Year
One in five (20%) respondents say they have received birth control from at least one additional telecontraception company. This also differed by company, with Company A and Company B having smaller shares of respondents who have received birth control from a different online company (18% and 14%, respectively) compared to respondents at Company C and Company D (54% and 65%, respectively).
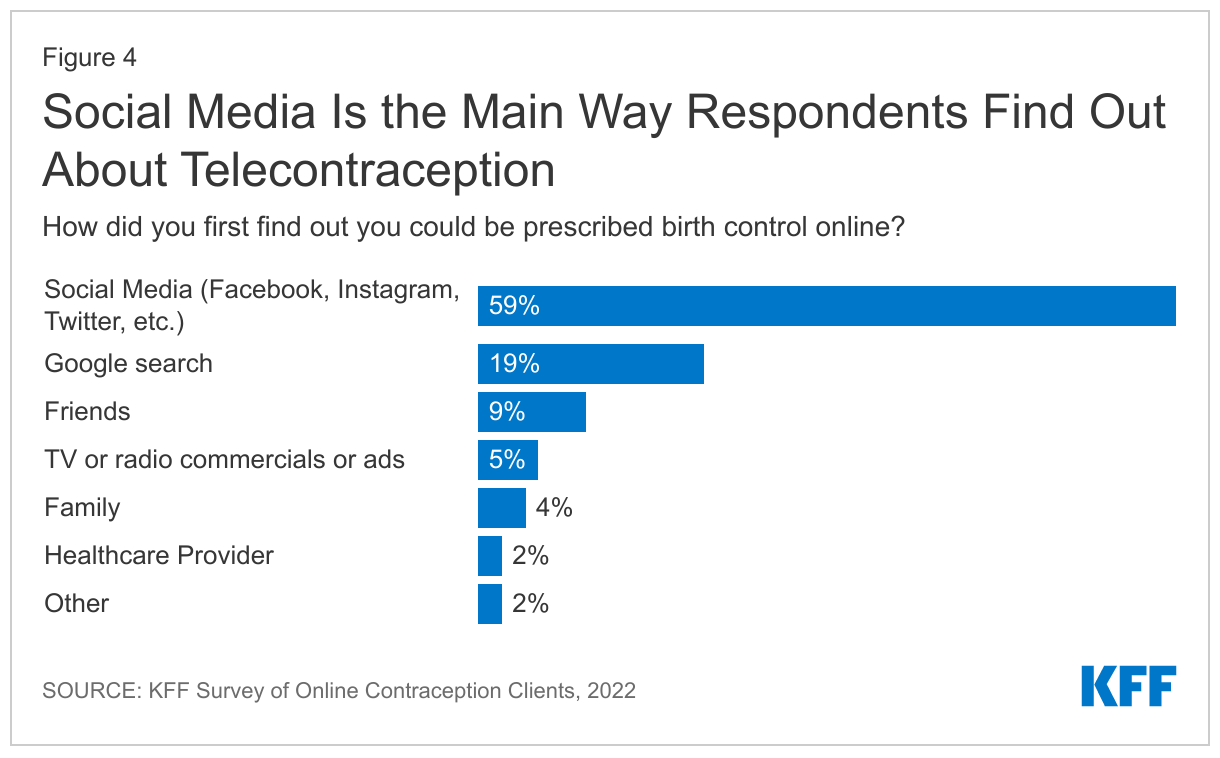
Many telecontraception companies utilize paid search engine marketing and social media to advertise and the majority of respondents say they first found out they could be prescribed birth control online through social media (59%), followed by Google search (19%), friends (9%), family (4%), and a healthcare provider (2%) (Figure 4).
Reasons for Accessing Birth Control Online
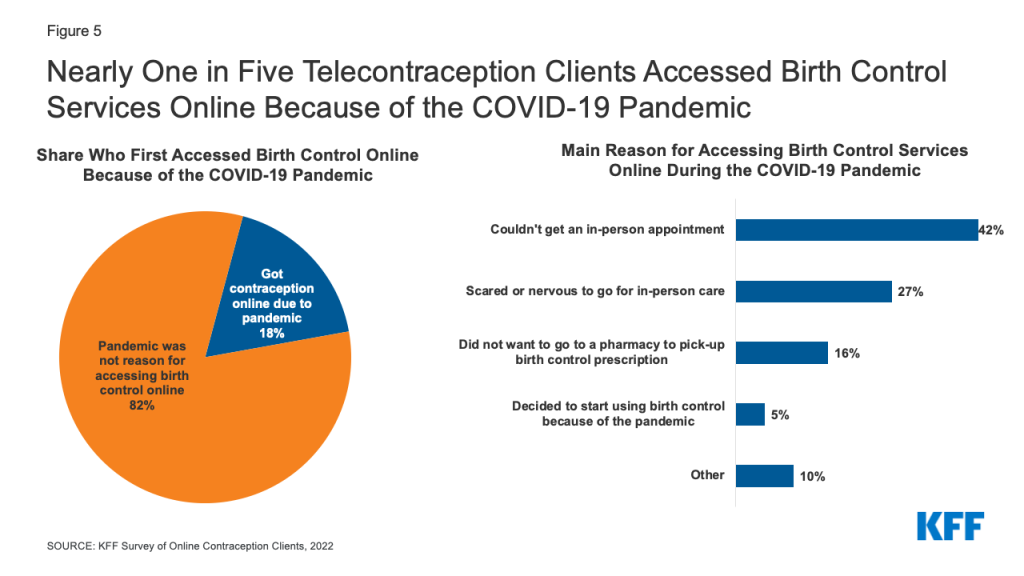
Although, telecontraception companies have reported they have seen a proliferation of clients due to the COVID-19 pandemic, most (82%) respondents say the pandemic was not the reason they accessed birth control online. Only one in five (18%) respondents say they first accessed birth control online because of the COVID-19 pandemic. Among those who first accessed birth control online because of the COVID-19 pandemic, the most widely cited reason was they could not get an in-person appointment (42%), followed by just over a quarter (27%) who were scared or nervous to go for in-person care, and 16% did not want to go to a pharmacy to pick-up their birth control prescription. A small share (5%) say they decided to start using birth control because of the pandemic and another one in ten cited another reason (Figure 5).
Figure 5: Nearly One in Five Telecontraception Clients Accessed Birth Control Services Online Because of the COVID-19 Pandemic
Among all respondents, the most frequent reason people cite for getting their most recent birth control via telecontraception is that the birth control is delivered to their home (26%). The second most frequent reason they say is they didn’t have insurance and couldn’t afford a doctor’s appointment (15%). Other reasons include not being able to get a doctor’s appointment (12%) or not having time for a doctor’s appointment (10%), as well as not wanting to interact with a provider (13%) or having a previous negative experience with an in-person provider (8%). Larger shares of LGBT+ individuals compared to non-LGBT+ cite a previous negative experience with an in-person provider as their main reason for getting their most recent birth control prescription via telecontraception (11% vs. 7%).
Among all respondents, smaller shares say the cost of birth control was more affordable (6%), they had privacy concerns (3%), a pharmacy is too far (1%), or they have always gotten birth control online (1%), and 5% cite some other reason (Figure 6).
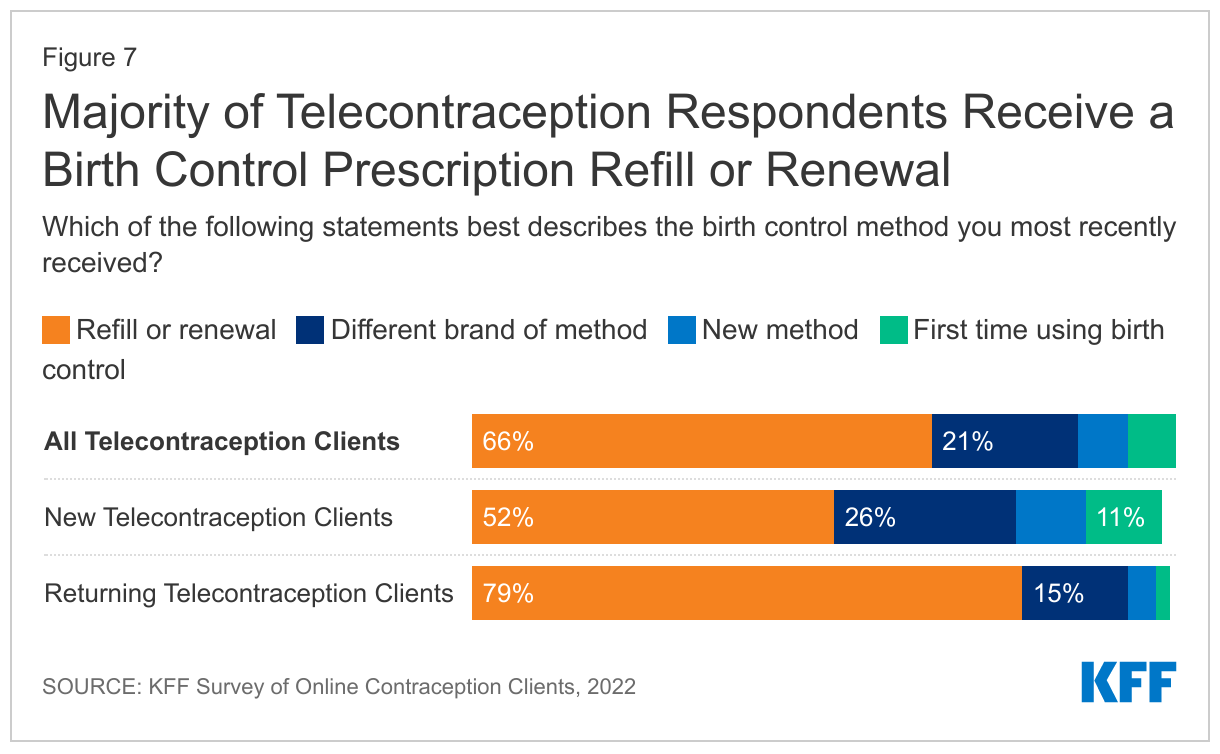
Individuals accessing telecontraception can get new prescriptions for contraception via a telehealth visit (typically asynchronous) with an online provider or refill an existing prescription. The majority of respondents (66%) say they most recently refilled or renewed a birth control prescription they were already using. Just over one in five (21%) say they obtained a different brand of their previous birth control method, like an oral contraceptive brand, or possibly a generic. Only 7% of respondents say they received a new birth control method and another 7% say the prescription they most recently received was their first time ever using birth control.
Compared to respondents who had previously received birth control online, smaller shares of respondents receiving birth control for the first time from a telecontraception company say their most recent birth control method was a refill or renewal (52% vs. 79%). Larger shares of new telecontraception clients compared to returning clients say they got a different brand of their previous method (26% vs. 15%) or got a new birth control method (10% vs. 4%). Just over one in ten (11%) new telecontraception clients say this was their first time ever using birth control (Figure 7).
Contraceptive Methods Prescribed
Among respondents, the most frequently obtained contraceptive method is oral contraceptives (91%), followed by emergency contraceptive pills (9%) (Figure 8). Five percent of respondents received female condoms, 4% monthly contraceptive rings, 3% injectable contraception, 2% contraceptive patch, and 1% received the one-year ring, Annovera. One in ten (10%) respondents most recently obtained more than one contraceptive method and 95% of those who got more than one contraceptive method received emergency contraception and almost one third (31%) got female condoms. Female condoms and emergency contraception are often included as add-ons at the end of an order. Nearly three in ten (29%) respondents overall say they purchased emergency contraception through an online company in the last 12 months.
Figure 8: The Majority of Telecontraception Survey Respondents Got a Prescription for Oral Contraceptives
Cost and Coverage
Since 2012, the ACA’s contraceptive coverage requirement has required all new private plans to cover FDA-approved contraceptive methods for women without cost-sharing from a participating provider. For individuals with Medicaid coverage, family planning services have been a mandatory benefit category that all state programs must cover without any cost-sharing, but services must be obtained from a Medicaid-participating provider. One of the companies that participated in this survey does not accept Medicaid and the other three do, but do not accept Medicaid in all states.
When asked how much they had to pay out-of-pocket, including co-pays, for their most recent birth control prescription or product, the majority of respondents say they did not have to pay anything (55%). For those with some out-of-pocket costs, just over one in five (21%) paid $31-50, 9% paid more than $50, 8% paid $1-15, and 7% paid $16-30 (Figure 9). However, this varied significantly among those with some type of health insurance coverage and those without insurance (See Insurance Coverage of Telecontraception above). About three in four individuals with private insurance or Medicaid who tried to use their coverage paid nothing out-of-pocket for their birth control compared to only 6% of individuals without insurance who had no out-of-pocket costs. Some companies provide free birth control for women without insurance who are in financial need. The largest share of those without insurance (51%) paid $31-50 and about a quarter (24%) paid over $50 for their birth control prescription or product. Individuals without insurance could get free or low-cost birth control from a federally funded Title X clinic or federally qualified health center, however, they may choose to pay for telecontraception for other reasons like convenience.
Despite the requirement that most private insurance plans cover contraceptive services and supplies free of cost-sharing, there may be multiple reasons individuals with private insurance may have out-of-pocket costs. The telecontraception company may not have had a contract with their insurance plan, the telecontraception company could have been considered out of network, or the client might be enrolled in a plan that is exempt from the contraceptive coverage requirements, such as those that are grandfathered, or those with coverage through an employer that is exempt on religious grounds.
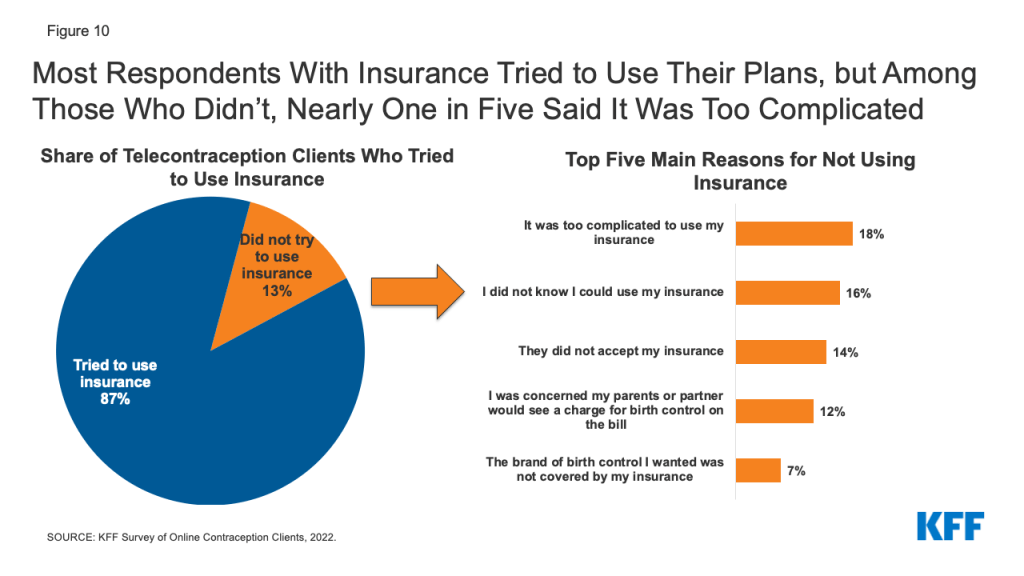
When asked about the last time they got a birth control method from a telecontraception company, the majority (87%) of insured respondents tried to use their insurance, while 13% did not (Figure 10). The top reason for not trying to use insurance was it was too complicated (18%). Another 16% of those who did not try to use their insurance say they did not know they could use their coverage. One in seven (14%) say the telecontraception company did not accept their insurance, while 12% did not try to use their insurance because they were concerned their parents or partner would see a charge for birth control. Seven percent say the brand of birth control they wanted was not covered by their insurance. Other reasons specified for not trying to use insurance included: the price was affordable without insurance, they hadn’t had a chance to update their insurance information, and they didn’t want their insurer to know about their birth control use.
Figure 10: Most Respondents With Insurance Tried to Use Their Plans, but Among Those Who Didn’t, One in Five Said It Was Too Complicated
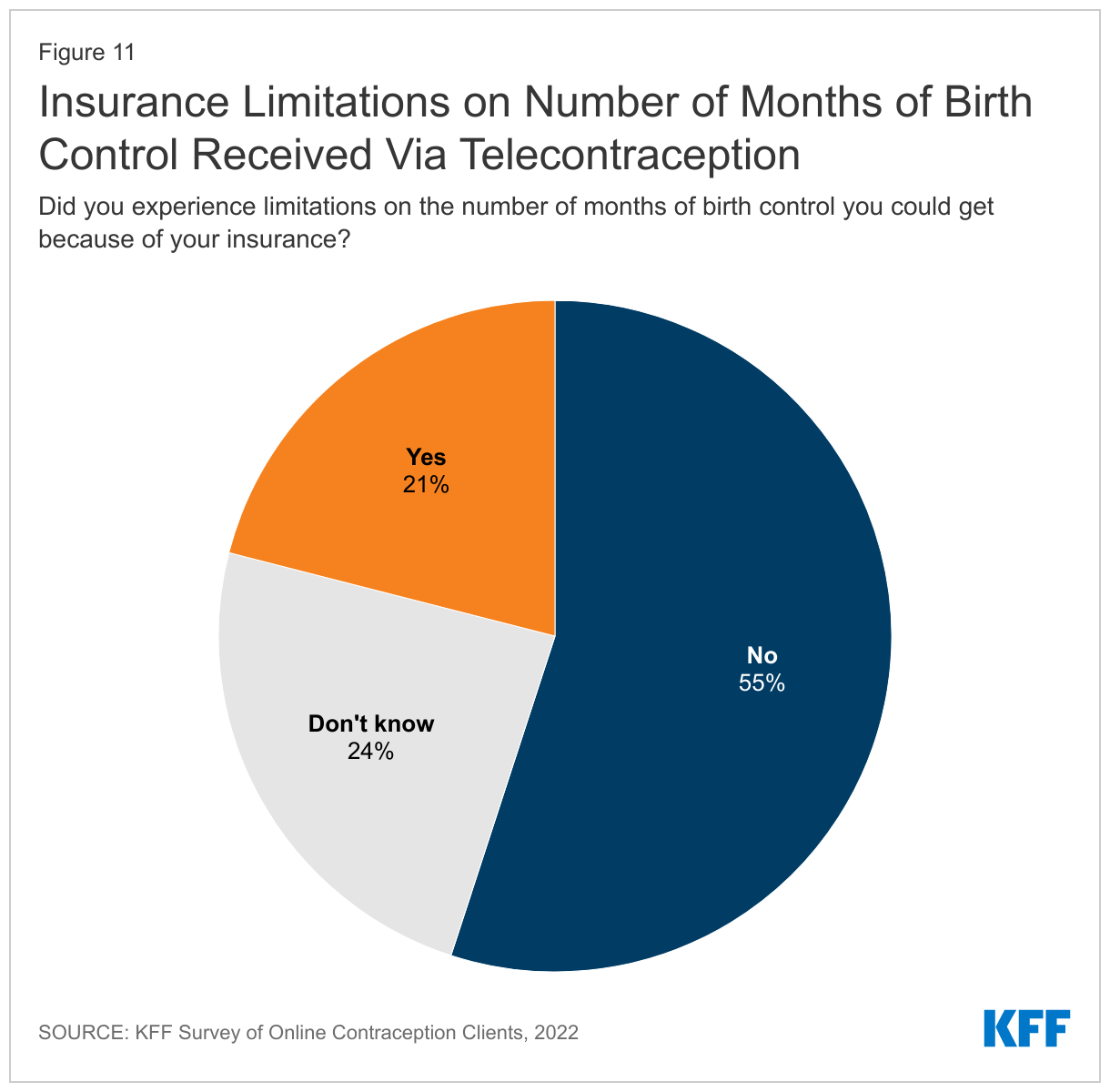
For individuals who tried to use their insurance for their telecontraception prescription, one in five (21%) say their insurance imposed limitations on the number of months of birth control they could get, while the majority (55%) did not experience limitations (Figure 11). About a quarter of respondents who tried to use their insurance did not know if they experienced limitations on the number of months of birth control they could get. The share reporting that they experiencing limitation did not differ between those with private insurance or Medicaid (data not shown).
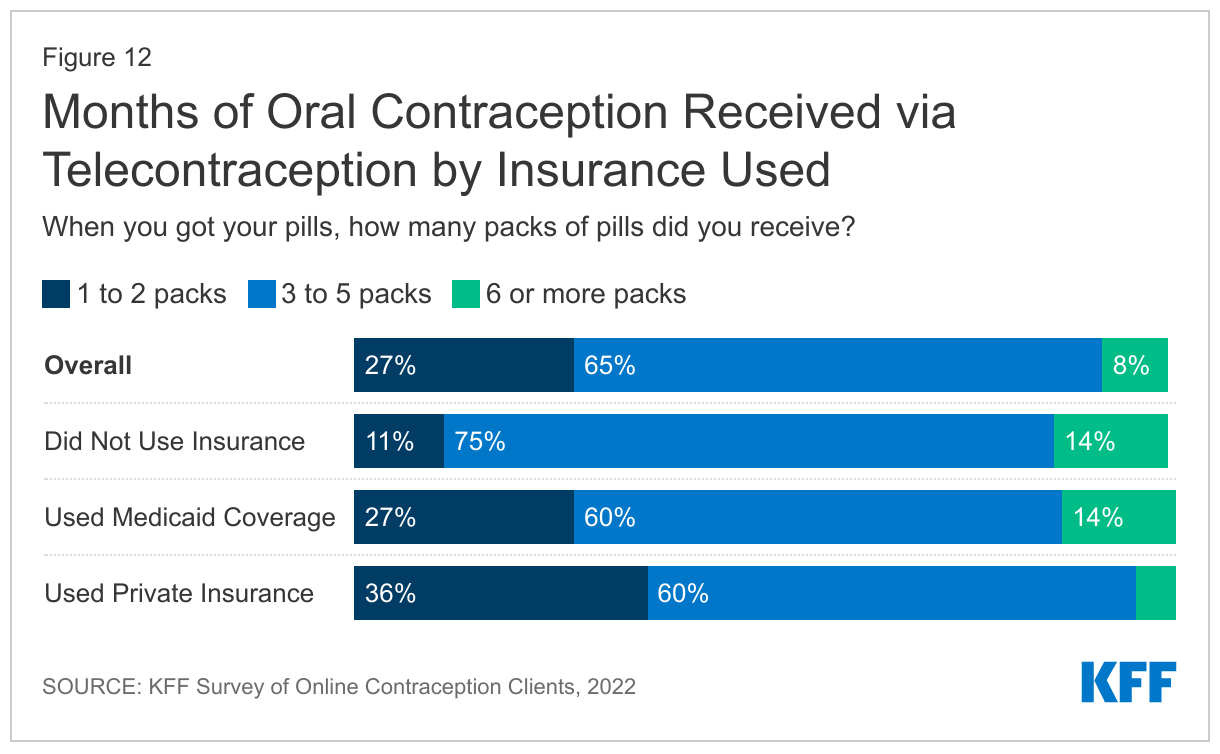
The largest share of respondents (65%) prescribed oral contraceptives say they receive three to five packs of pills at a time. While research has shown that best practice is to offer oral contraceptive users an extended supply of oral contraceptive pills such as a 12 month supply, few women receive a 12-month supply of contraceptives. Eight percent of respondents say they get 6 or more packs at a time, while 27% receive one to two packs at a time.
However, there are significant differences between those without insurance and those with Medicaid coverage compared to private insurance. Larger shares of respondents who used their Medicaid coverage (14%) or those that did not use insurance (13%) received six or more packs of pills compared to just 5% of those using private insurance (Figure 12). Currently, Medicaid programs in sixteen states and DC cover a 12-month supply of oral contraceptives at a time, which likely explains the larger share of individuals with Medicaid coverage receiving a 12-month supply. Some of the telecontraception companies also offer contraception at a discounted price if a larger number of packs at purchased at one time, which may be why a larger share of individuals without insurance received 6 or more packs. Twenty states and DC require state regulated insurers to cover an extended supply of contraceptives at one time, but this policy doesn’t include all plans (such as those that are self-funded) and there are still issues with implementation in getting insurance to cover more than 1 to 3 months of contraception at a time due to health plans’ concern over waste and increased costs.
Experiences Using Telecontraception
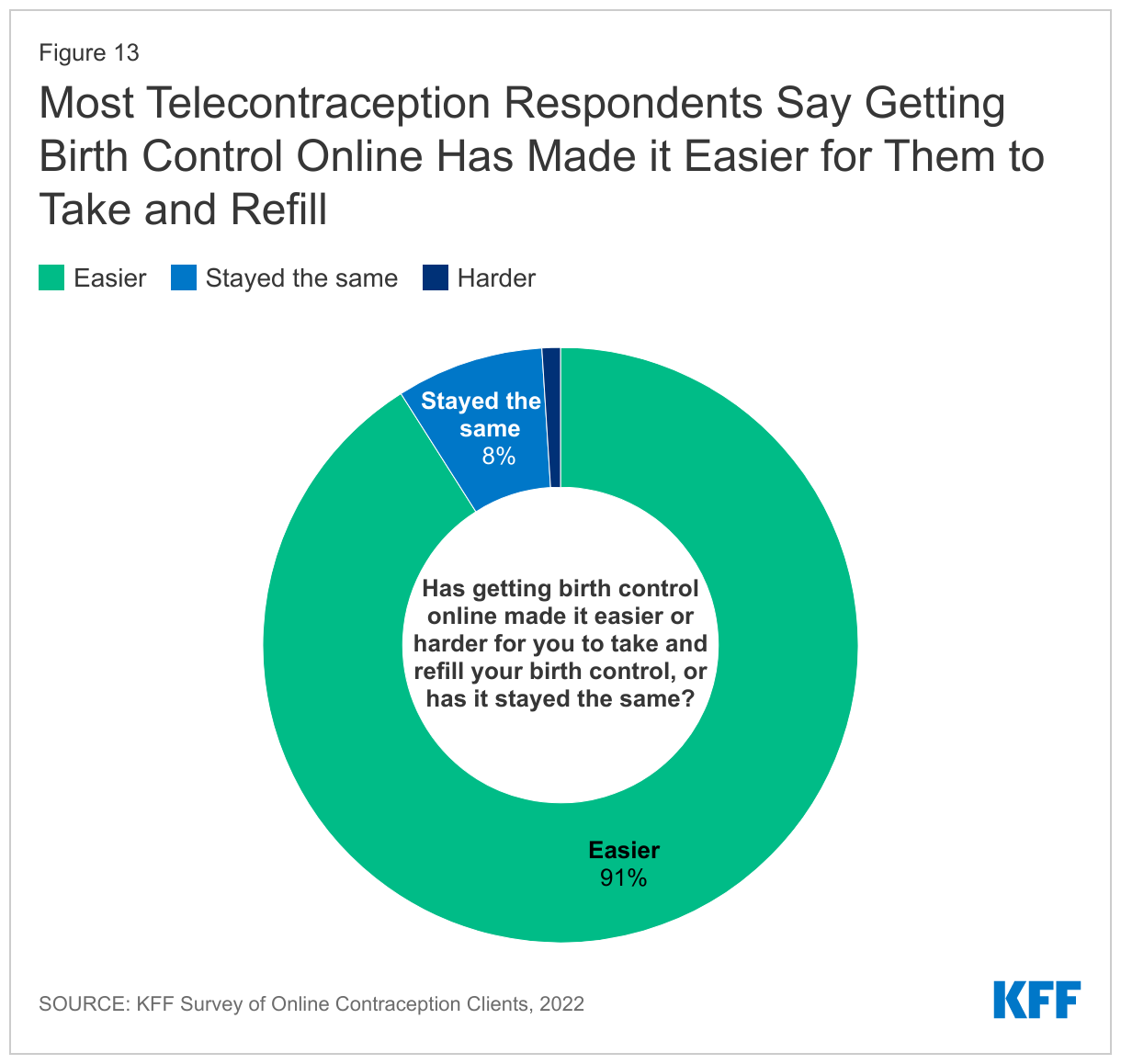
The telecontraception clients responding to this survey were largely satisfied with the services they received and felt that telecontraception made it easier for them to take and refill their birth control. Ninety-one percent of survey respondents report that getting their contraception through an online company has made it easier for them to take or get refills for their birth control, while only 1% report it has made it harder. Eight percent say there has been no change (Figure 13). Individuals that are able to continuously take and refill their birth control with little to no barriers are less likely to have an unwanted pregnancy.
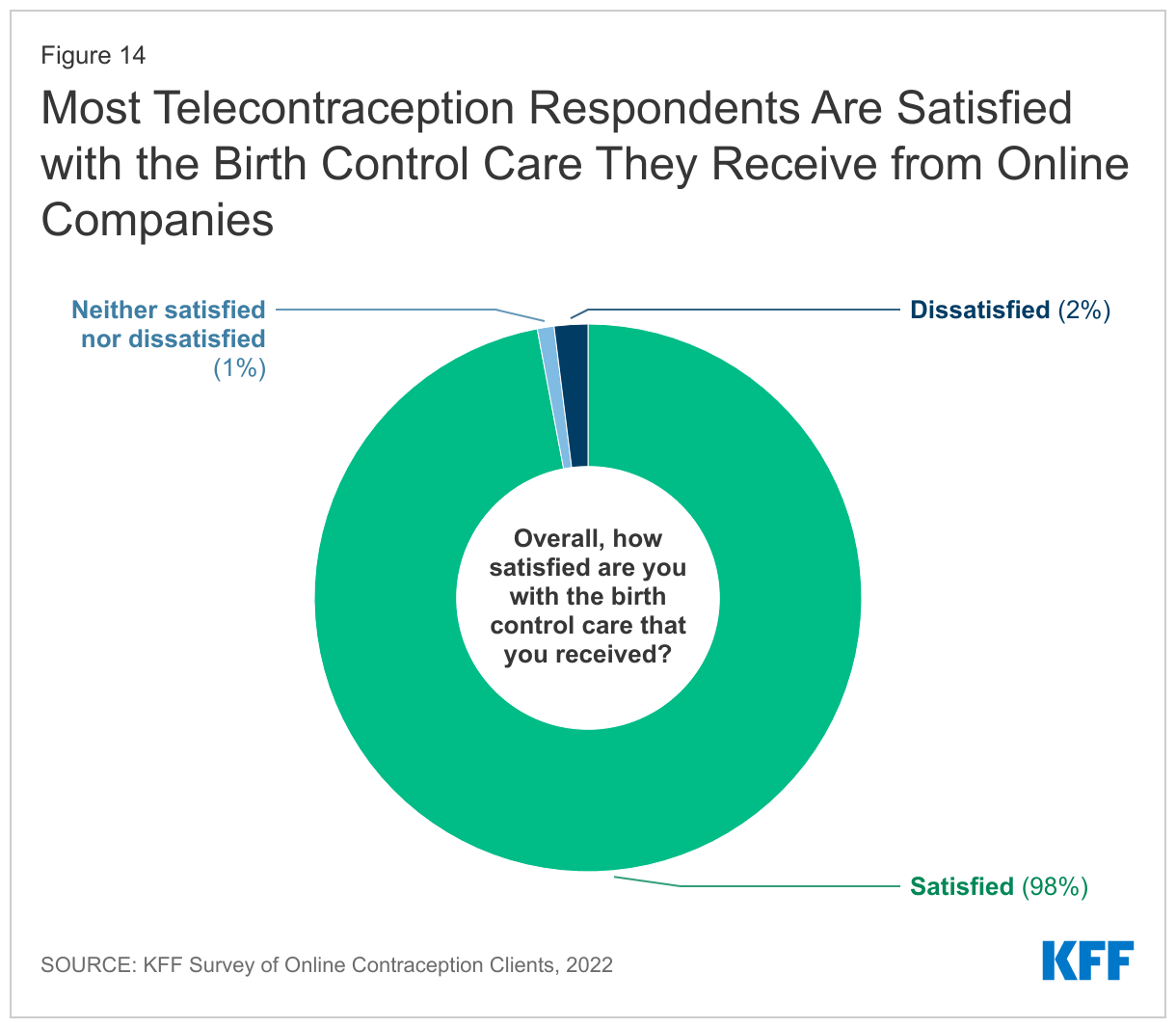
The majority (98%) of respondents report they are satisfied with the birth control care they received from the telecontraception companies (Figure 14). Across the four companies, between 93% to 98% say they were satisfied with their care. Two percent of respondents report they are dissatisfied with the care they received, and 1% report they are neither satisfied nor dissatisfied.
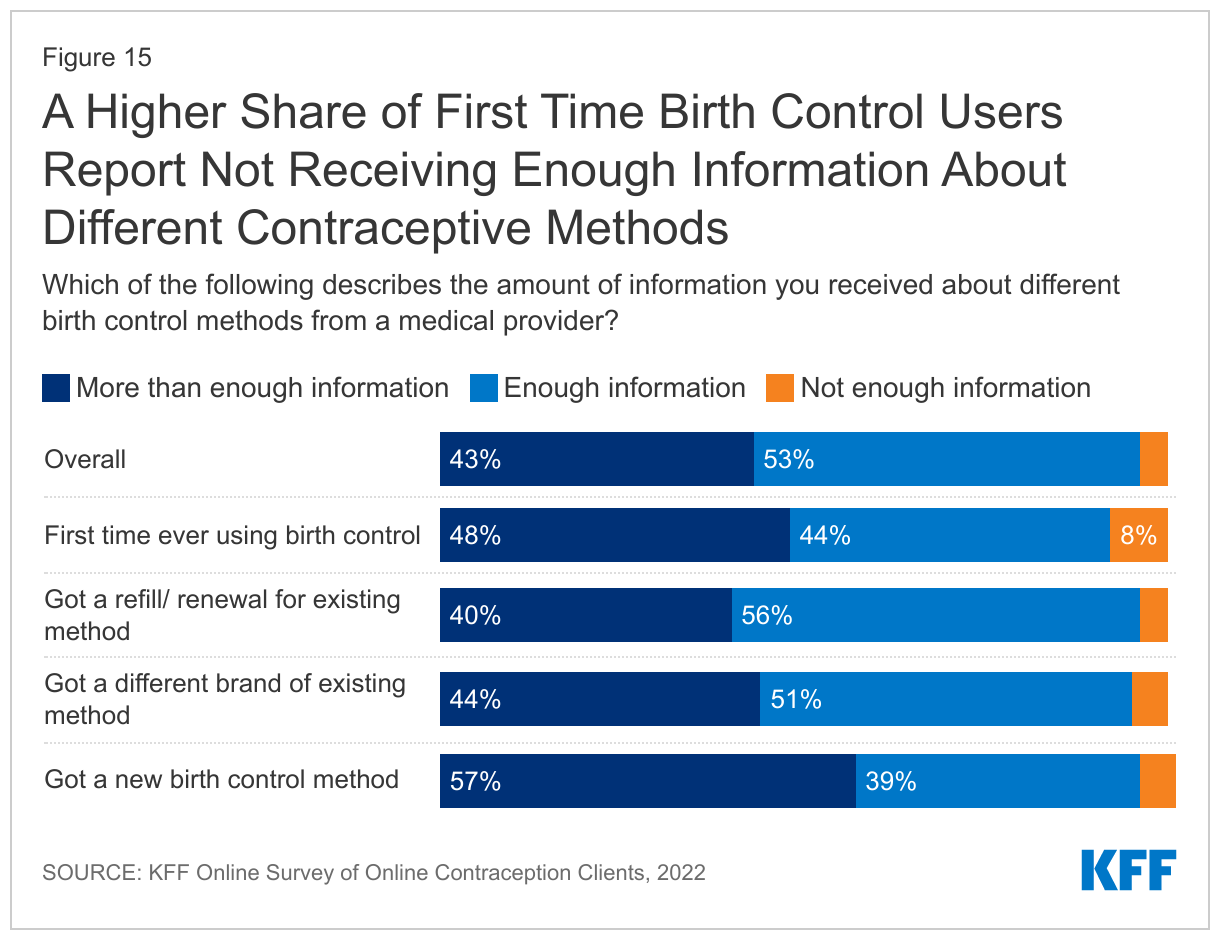
Most respondents say they received enough information about different birth control methods from a medical provider at the company of their choice. Half (53%) report they got enough information, and another 43% report they received more than enough information. Only 4% report they did not get enough information—across companies, this share ranged from 4% to 11%. However, a higher share of respondents who were using a birth control method for the first time report they did not get enough information (8%) compared to those getting a different brand (5%), a new method (5%), or a refill (4%) (Figure 15).
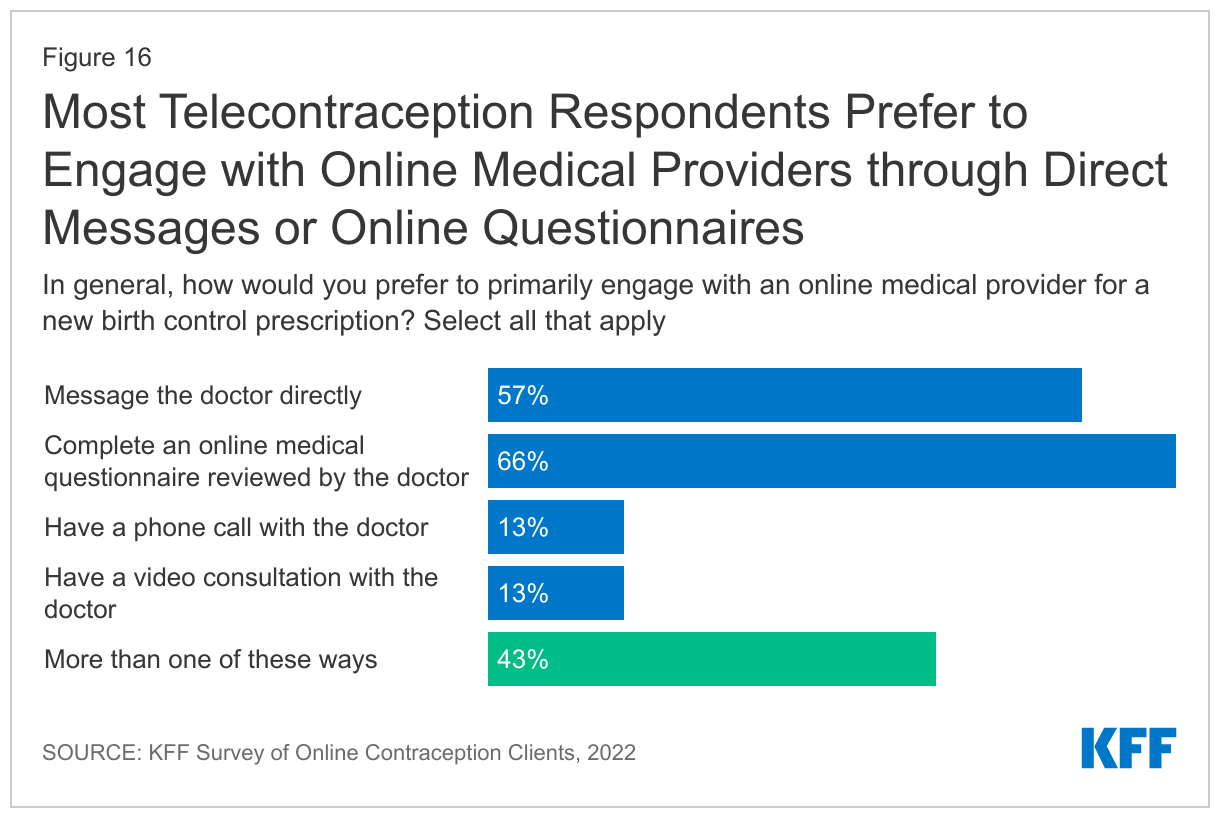
Telecontraception clients generally receive birth control prescriptions by filling out a health questionnaire meant to screen for birth control contraindications, such as high blood pressure, smoking status, or a history of strokes. These questionnaires are then reviewed by healthcare providers, and depending on the policies of the state they reside in, the provider will communicate with the patient via text or chat or will have a video call with the patient to determine whether they are a good candidate for birth control and what method or brand they should use. Survey respondents were asked how they would prefer to engage with online medical providers when obtaining a new birth control prescription, and 57% prefer to message the online medical provider directly. Thirteen percent prefer video calls and 13% prefer phone calls. Sixty-six percent report they prefer filling out an online questionnaire that was reviewed by the medical provider. Four in ten (43%) would prefer to be able to engage with an online medical provider in more than one of these ways (Figure 16).
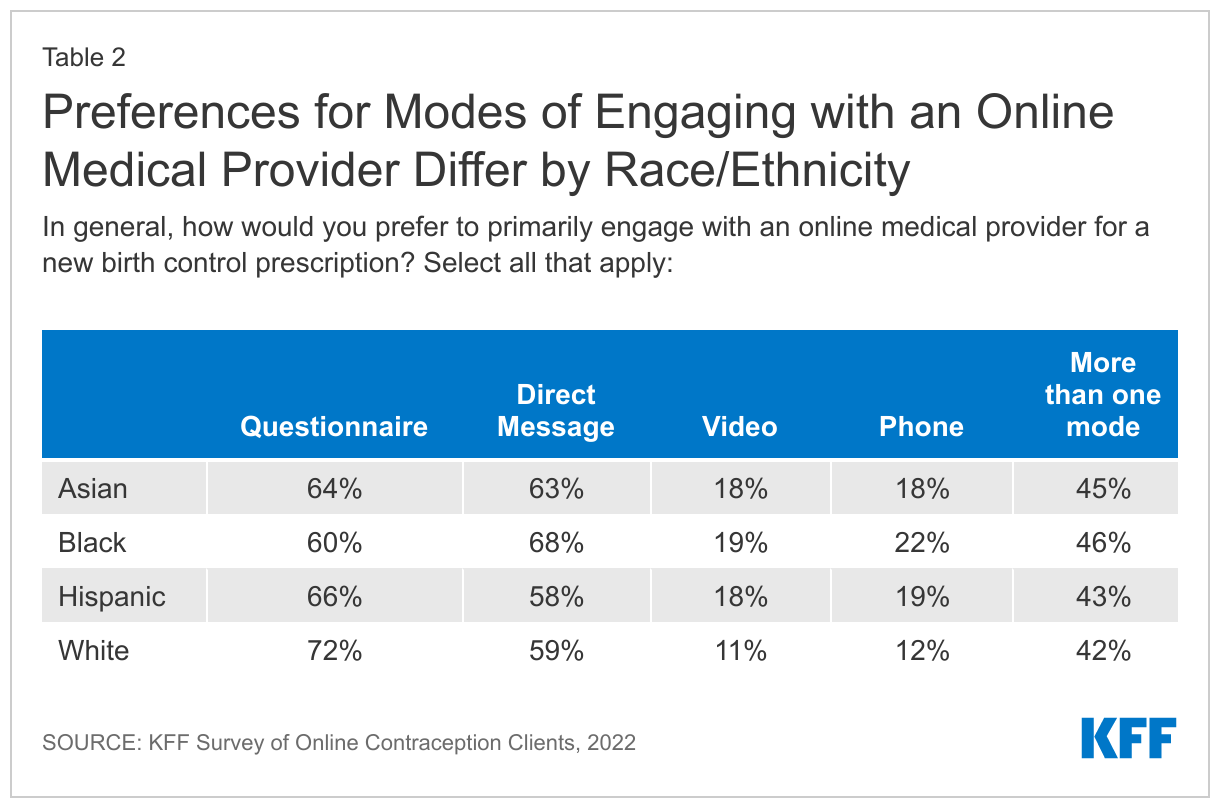
A somewhat higher share of Black respondents said they prefer to primarily engage with online medical providers via direct message compared to White respondents, and higher shares of Black, Hispanic and Asian respondents prefer to engage providers via video calls or phone calls. Somewhat higher shares of White respondents said they preferred to primarily engage with providers via a questionnaire (Table 2).
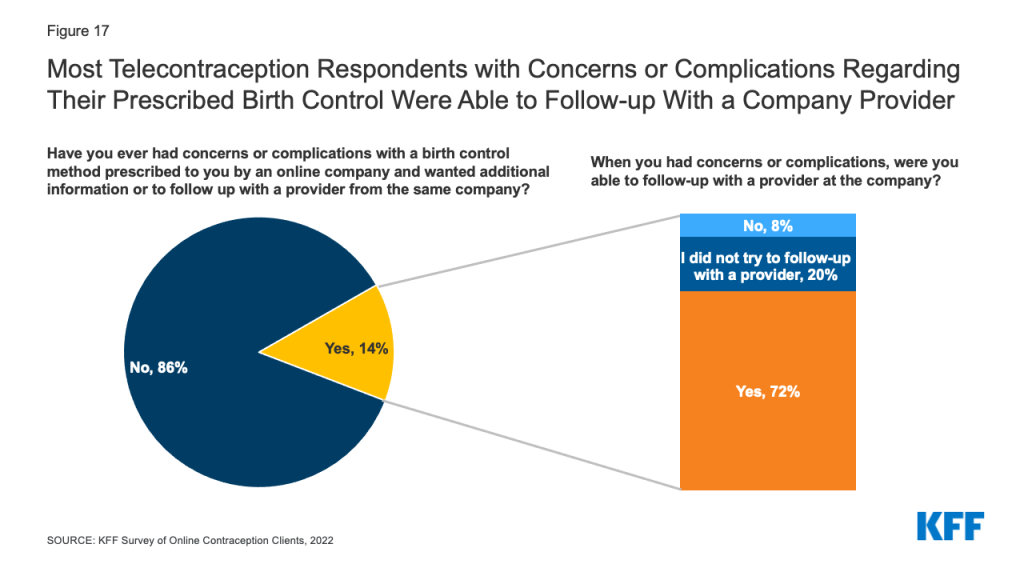
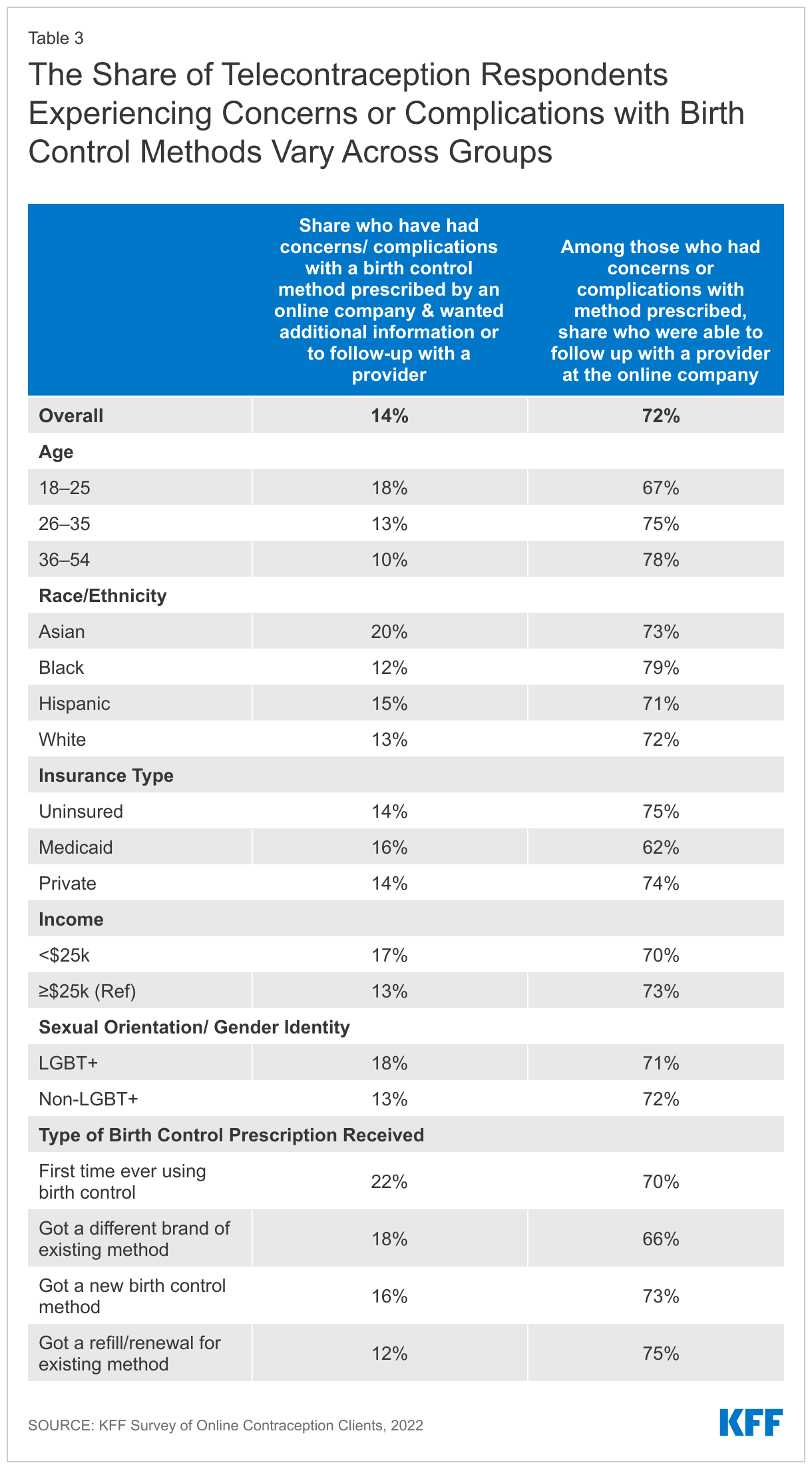
Overall, 14% of respondents report that they had had concerns or complications with a birth control method they had been prescribed through an online platform and wanted additional information or a follow with a medical provider (Figure 17). Among those who had concerns or complications, 72% report they were able to follow up with a provider at the company and another 20% say they never tried to follow up, and eight percent say they were not able to follow up. Larger shares of Asian respondents (20%) and respondents ages 18-25 (18%) report having a concern or complication with a birth control method prescribed through an online platform compared to White respondents (13%) and older respondents (10% of those over age 36) (Table 3). Additionally, larger shares of those getting birth control for the first time or getting a new method or different brand say they had concerns or complications with their method compared to those getting a refill or renewal.
Figure 17: Most Telecontraception Respondents with Concerns or Complications Regarding Their Prescribed Birth Control Were Able to Follow-up With a Company Provider
Connections to the Health Care System
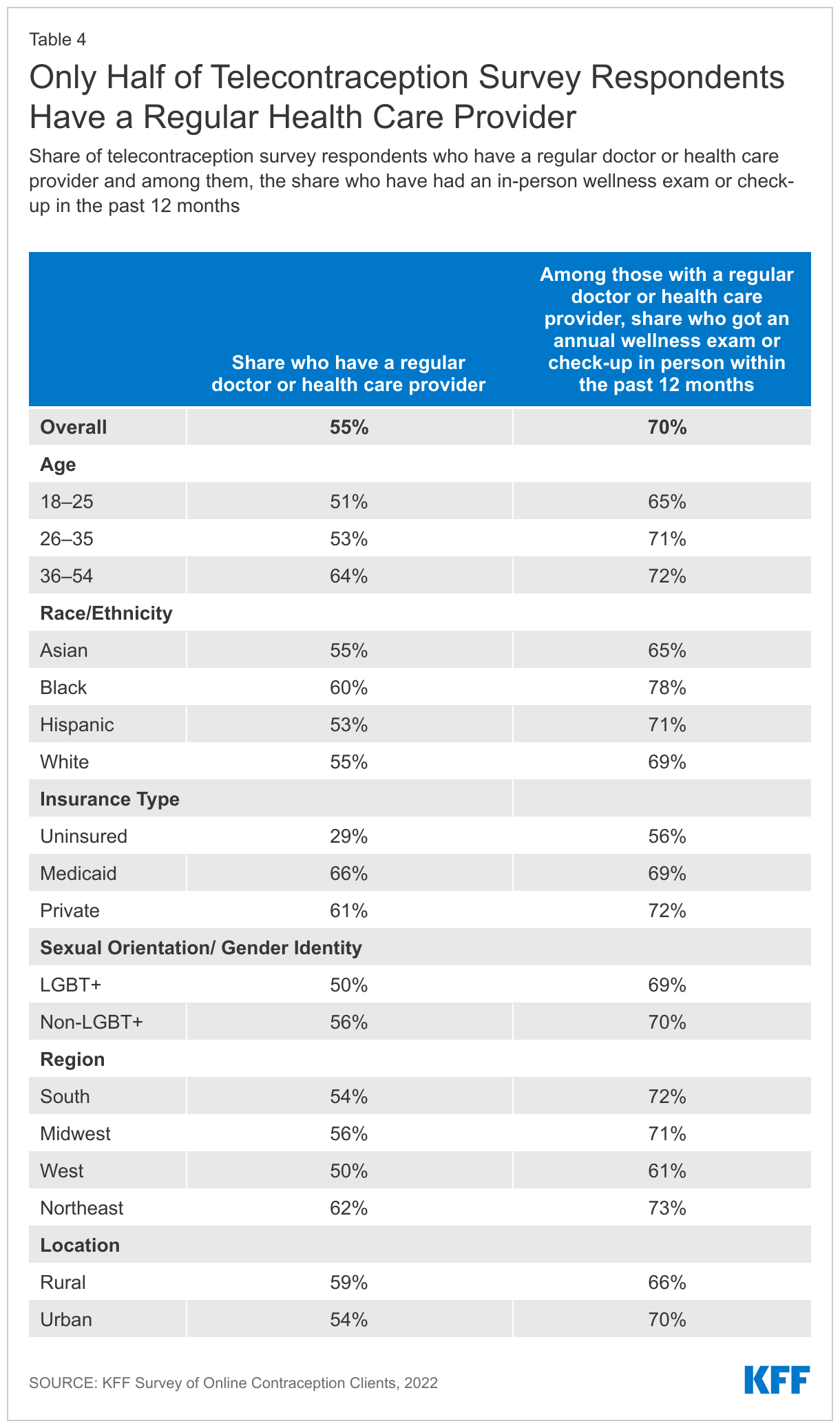
For some, interacting with a telecontraception provider may be their only interaction with a health care provider, while others may use telecontraception for a convenient way to get birth control, but have other connections to the health care system through a brick-and-mortar clinic. Over half (55%) of respondents report they have a regular doctor or health care provider they usually see when they are sick or need routine care. Four in ten (43%) say they do not have a regular doctor, and another 3% say they were not sure. The share without a regular doctor is much higher than women overall in the U.S. (43% vs. 18%). Larger shares of younger respondents compared to older and LGBT+ individuals compared to non-LGBT+ do not have a regular doctor or health care provider. Nearly seven in ten respondents without insurance say they do not have a regular health care provider. Larger shares of Black respondents compared to White respondents and respondents in the Northeastern part of the U.S. compared to all other regions of the country say they have a regular doctor.
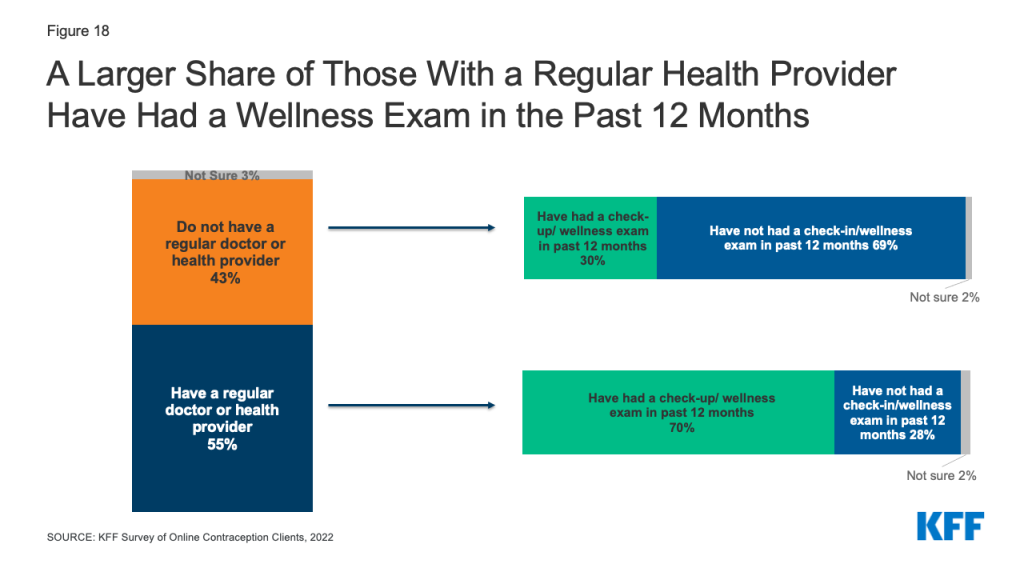
Regular check-ups give patients the opportunity to talk with their health care providers about a broad range of issues, such as preventive health services, role of lifestyle factors on health, and management of chronic health issues. Fifty-two percent of respondents say they have received an in-person annual wellness exam or check up in the past twelve months, while 46% have not. Among those who have a regular doctor or health care provider, 70% report they received an in-person annual exam or check-up in the past 12 months compared to just 30% of those without a regular doctor or health care provider (Figure 18 and Table 4).
Figure 18: A Larger Share of Those With a Regular Health Provider Have Had a Wellness Exam in the Past 12 Months
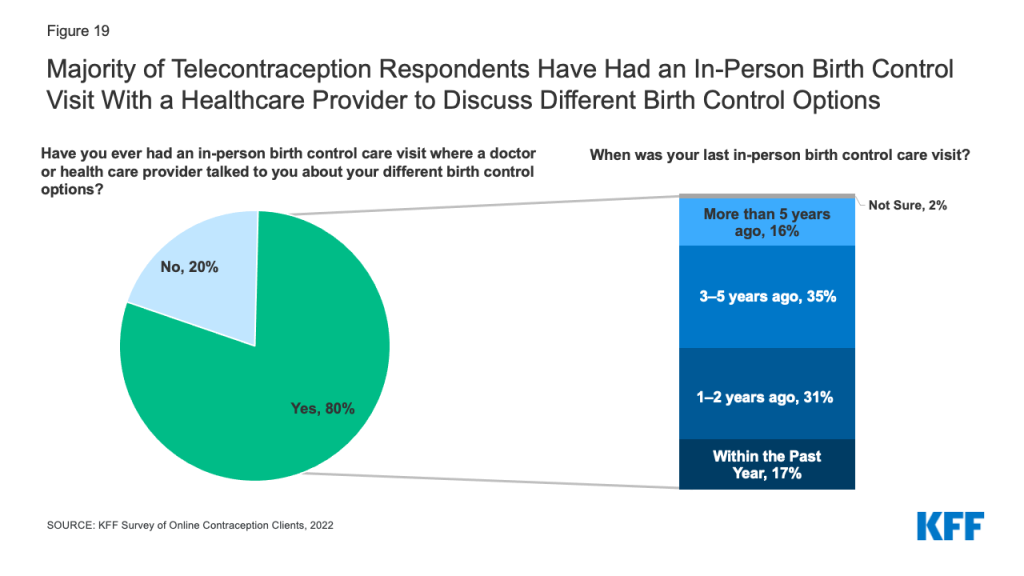
Eighty percent of respondents say they have had had an in-person birth control care visit where a doctor or health care provider had talked to them about their different birth control options at some point in their lives. Among this group, 17% say their last in-person visit was in the past year and 31% say it was one to two years ago. Another 35% report their last visit was in the last three to five years, and 16% say it was more than five years (Figure 19).
Figure 19: Majority of Telecontraception Respondents Have Had an In-Person Birth Control Visit With a Healthcare Provider to Discuss Different Birth Control Options
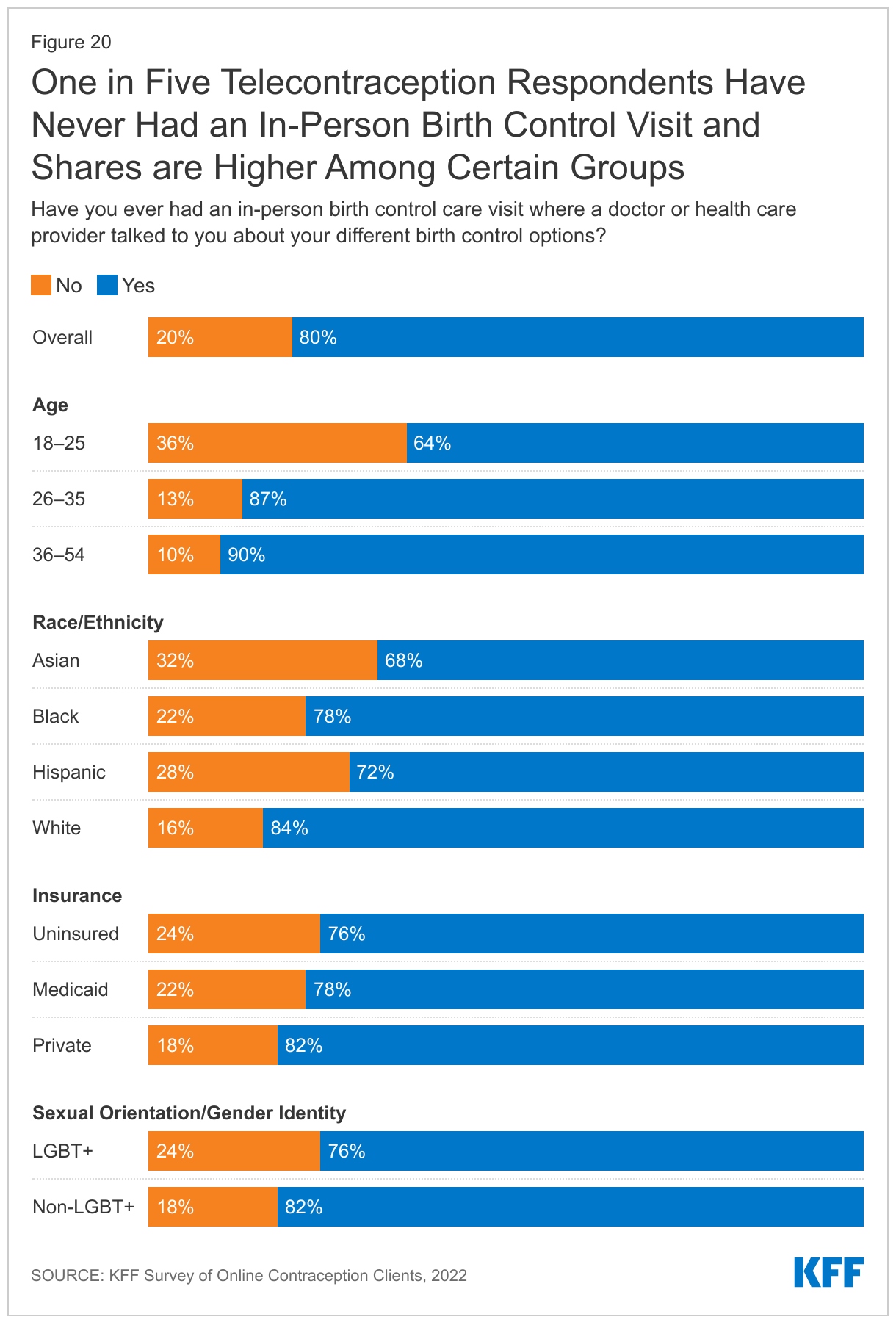
One in five (20%) telecontraception respondents report they have never had an in-person birth control visit (Figure 20). Higher shares of respondents ages 18-25 (36%), respondents who identify as LGBT+ (24%), those with Medicaid coverage (22%), and those who are uninsured (24%) report they had never had an in-person visit compared to respondents ages 26–35 and 36–49, those who identify as non-LGBT+, and those with private insurance. Over a third (32%) of Asian respondents and 28% of Hispanic respondents also say they have never had an in-person birth control visit, compared to 22% of Black respondents and 16% of White respondents.
Post-Roe Actions
On June 24, 2022 the Supreme Court issued their decision in Dobbs vs Jackson Women’s Health, and overturned Roe v Wade, which eliminated the federal constitutional standard that had protected the right to abortion. Now states can set their own policies banning or protecting abortion rights. As of April 2023, 13 states have banned abortion. After the Dobbs decision, telecontraception companies reported an influx of emergency contraception orders.
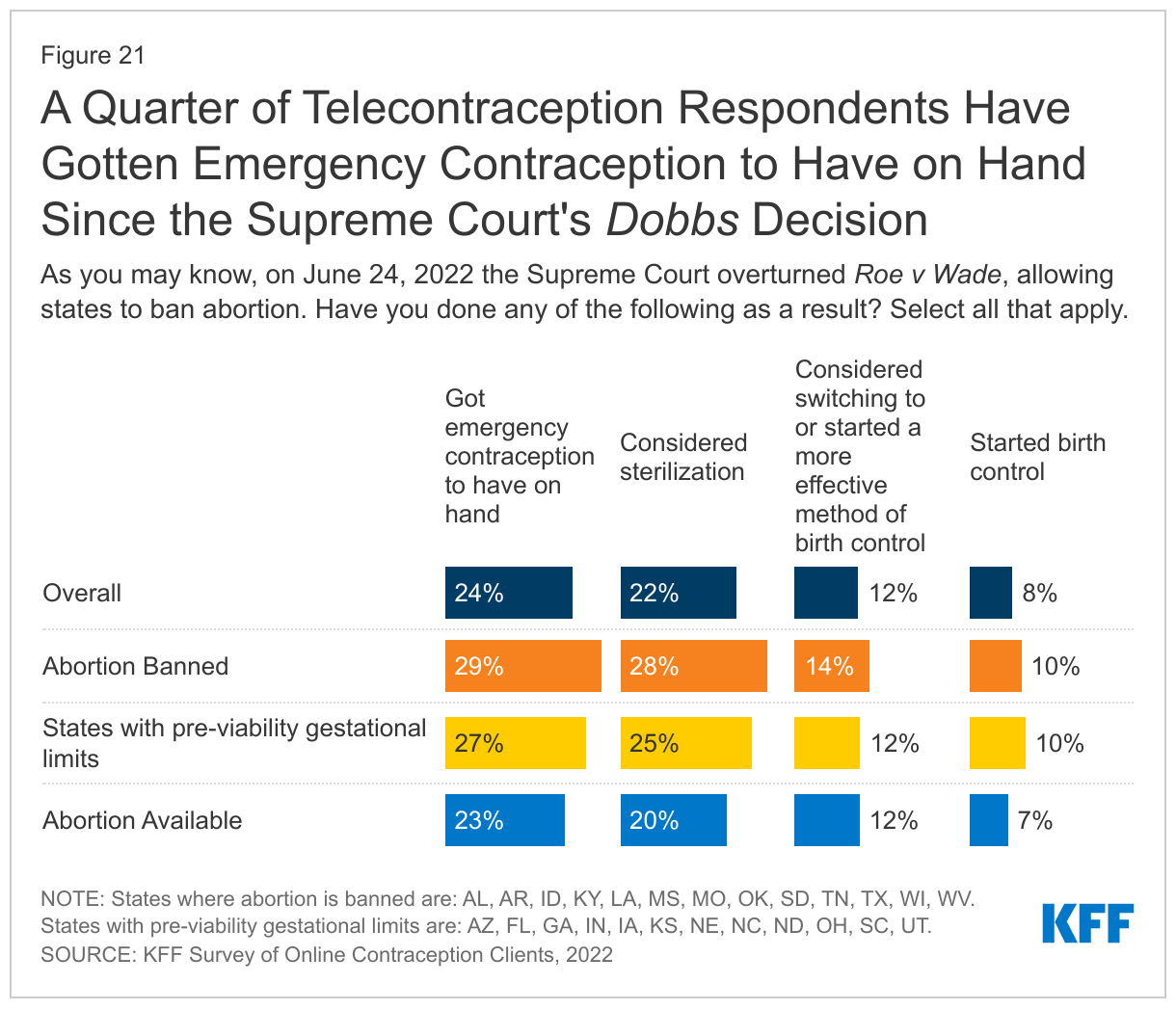
In response to the ruling, almost a quarter (24%) of respondents report that they have gotten emergency contraception to have on hand and over a fifth (22%) have considered sterilization. Twelve percent report that they have considered switching to or have started a more effective method of birth control, and eight percent have started using birth control due to the Dobbs decision (Figure 21). These findings were fairly consistent across states regardless of whether abortion was banned or not.
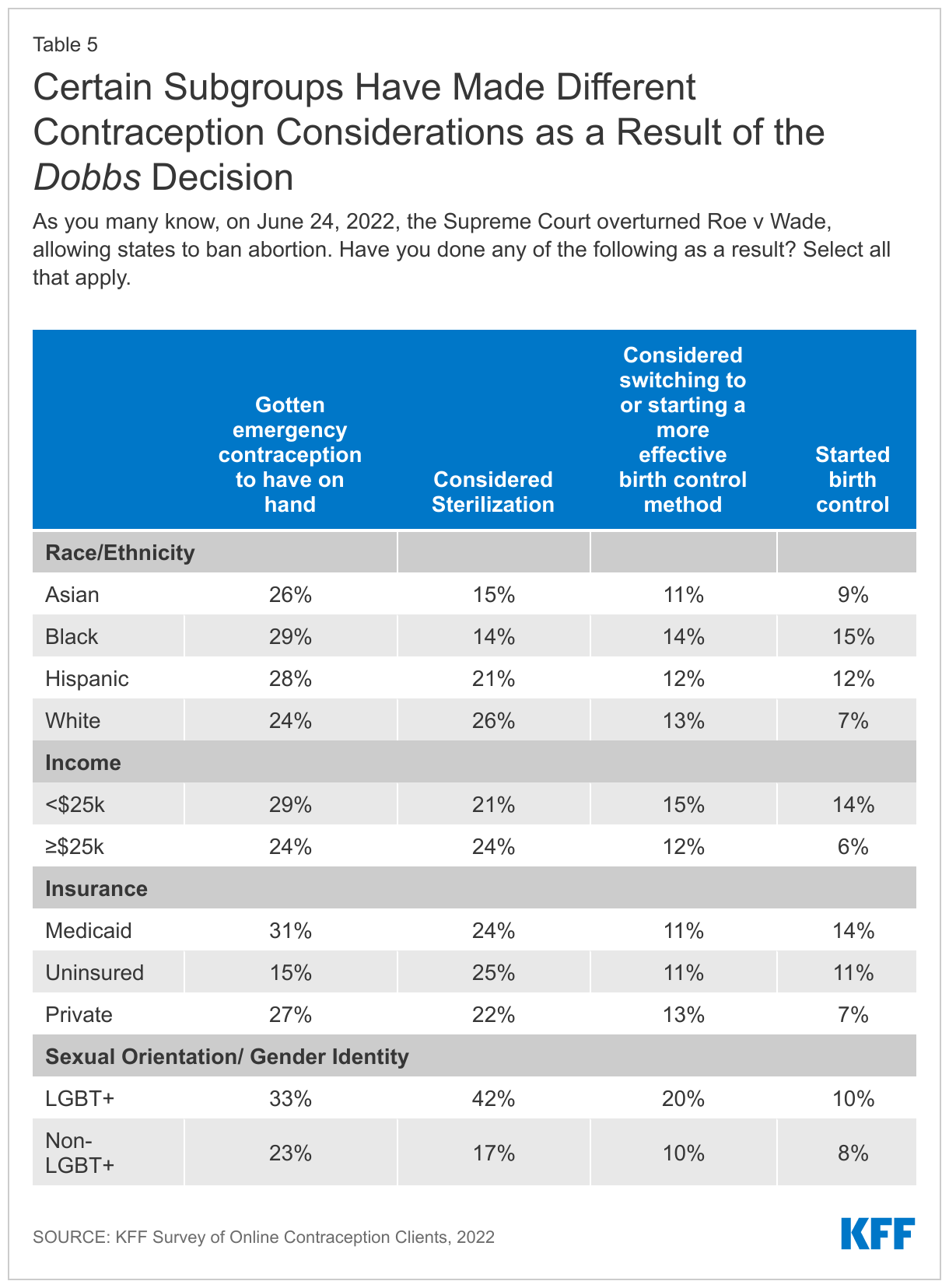
There were some differences in these contraceptive considerations or actions by certain subgroups like race/ethnicity, income, insurance type, and sexual orientation (Table 5). Smaller shares of Black and Hispanic respondents (14% and 21%) compared to White respondents (26%) say they had considered sterilization in the wake of the Dobbs decision, but larger shares of Black and Hispanic respondents say they started birth control (15% and 12%) compared to White respondents (7%). Larger shares of those with lower incomes compared to higher incomes (14% vs. 6%) and those with Medicaid coverage or those without insurance (14% and 11% vs. 7%) compared to those with private insurance say they started birth control. A larger share of LGBT+ individuals compared to non-LGBT+ individuals say they got emergency contraception to have on hand (33% vs. 23%), considered sterilization (43% vs. 17%), and considered switching to or starting a more effective birth control method (20% vs. 10%) after Roe v Wade was overturned.
Looking Forward
While telecontraception remains a relatively new avenue for accessing contraception and only a small share of people say they have accessed services through these platforms, it has been difficult to know the characteristics of telecontraception users and what their experience has been like. Those who responded to this survey are generally satisfied with their experience, say telecontraception has made it easier for them to get their birth control, and they appear to be getting enough information about different birth control methods. However, this is a limited convenience sample and may not be representative of the larger population of telecontraception clients. Telecontraception has provided a way for people to get their birth control without having to leave their home, which has been helpful for many during the COVID-19 pandemic. However, some are left paying out-of-pocket, especially those without insurance, for birth control methods that would otherwise be covered free of charge at a federally funded clinic or through their insurance. In addition, all users must pay a membership or consultation fee, even though their insurance or Medicaid would cover the full cost of a visit and supply if they went to an in-network provider. Many of those accessing contraception online do not have a regular doctor or have never had an in-person birth control visit, so this may be the only information they are getting about birth control methods. Because there are a limited number of birth control methods for them to choose from, telecontraception may not be a good fit for those wanting long-acting reversible contraceptive methods or more comprehensive contraceptive counseling. However, for those who use reversible hormonal methods or seek emergency contraceptive pills, telecontraception offers privacy and convenience, which is valued by the respondents of this survey.
As reproductive health policies and abortion access becomes more restrictive in some states, online companies may play a greater role in expanding access to sexual and reproductive health care.
This work was supported in part by Arnold Ventures. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
We would like to thank Nurx, The Pill Club, Twentyeight Health, and Pandia Health for working with us on this project.
Medicare is a primary source of health insurance coverage for several million people younger than age sixty-five who have long-term disabilities.
Published in the journal Health Affairs, this analysis compared measures of access to care, cost concerns, and satisfaction with care for beneficiaries younger than age sixty-five versus those ages sixty-five and older, using the 2019 Medicare Current Beneficiary Survey. It also compared beneficiaries in traditional Medicare with those in Medicare Advantage, given that a growing share of younger beneficiaries with disabilities are enrolled in private plans.
It finds that Medicare beneficiaries younger than age sixty-five reported worse access to care, more cost concerns, and lower satisfaction with care than beneficiaries ages sixty-five and older, regardless of their type of Medicare coverage. Among beneficiaries younger than age sixty-five in traditional Medicare, the share reporting cost concerns was highest among those without supplemental coverage.
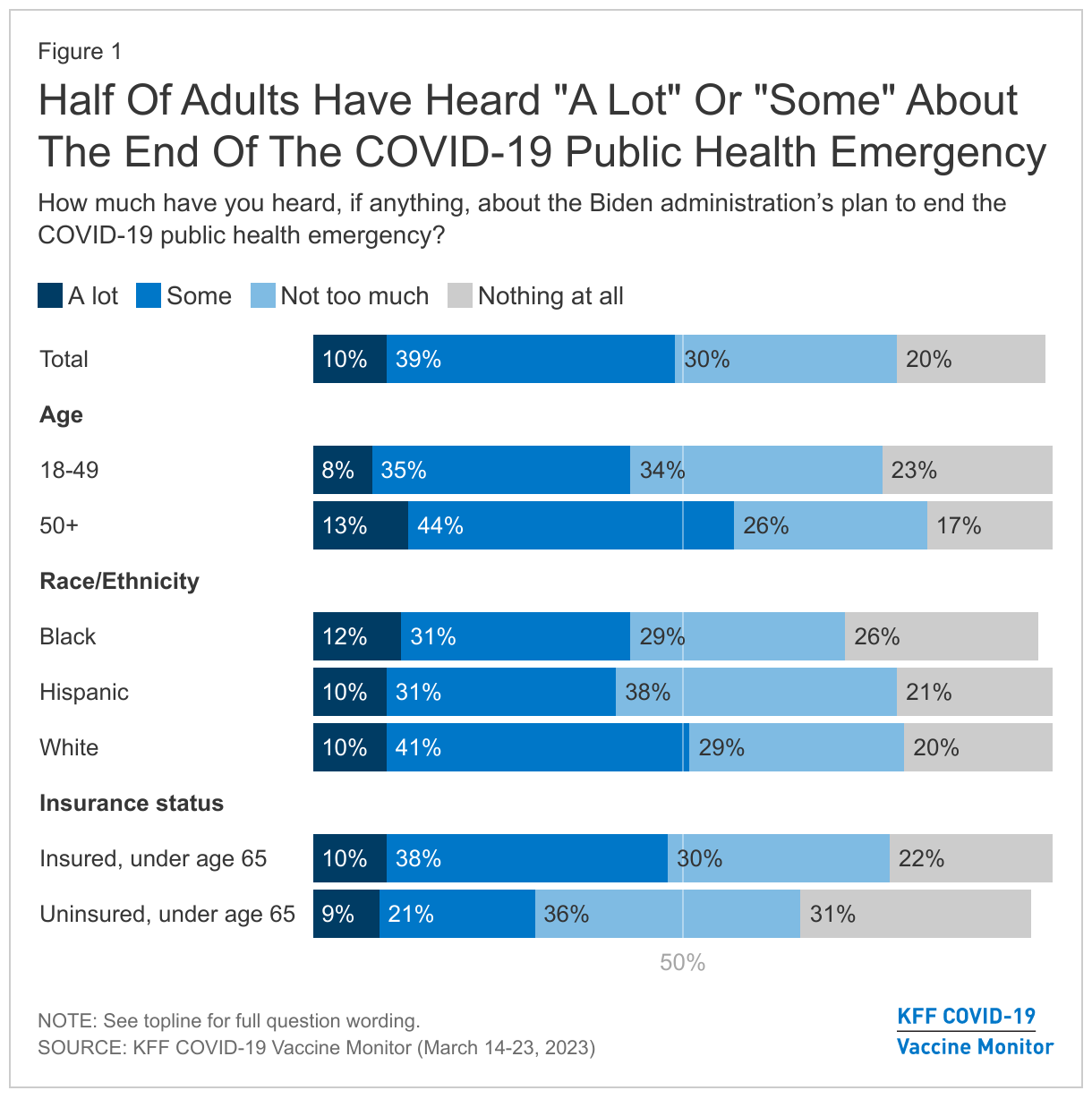
With the end of the public health emergency (PHE) and the impacts that will have on the health care system, one in five adults have heard “nothing at all” about the Biden administration’s plan to end the COVID-19 PHE. Six in ten (59%) adults think the end of the PHE will have “no impact” on them and their family and almost half (46%) say it won’t have an impact on the country overall. The end of the PHE is a bigger concern to some groups who have been more negatively affected by the coronavirus pandemic, including people of color and those with lower household incomes.
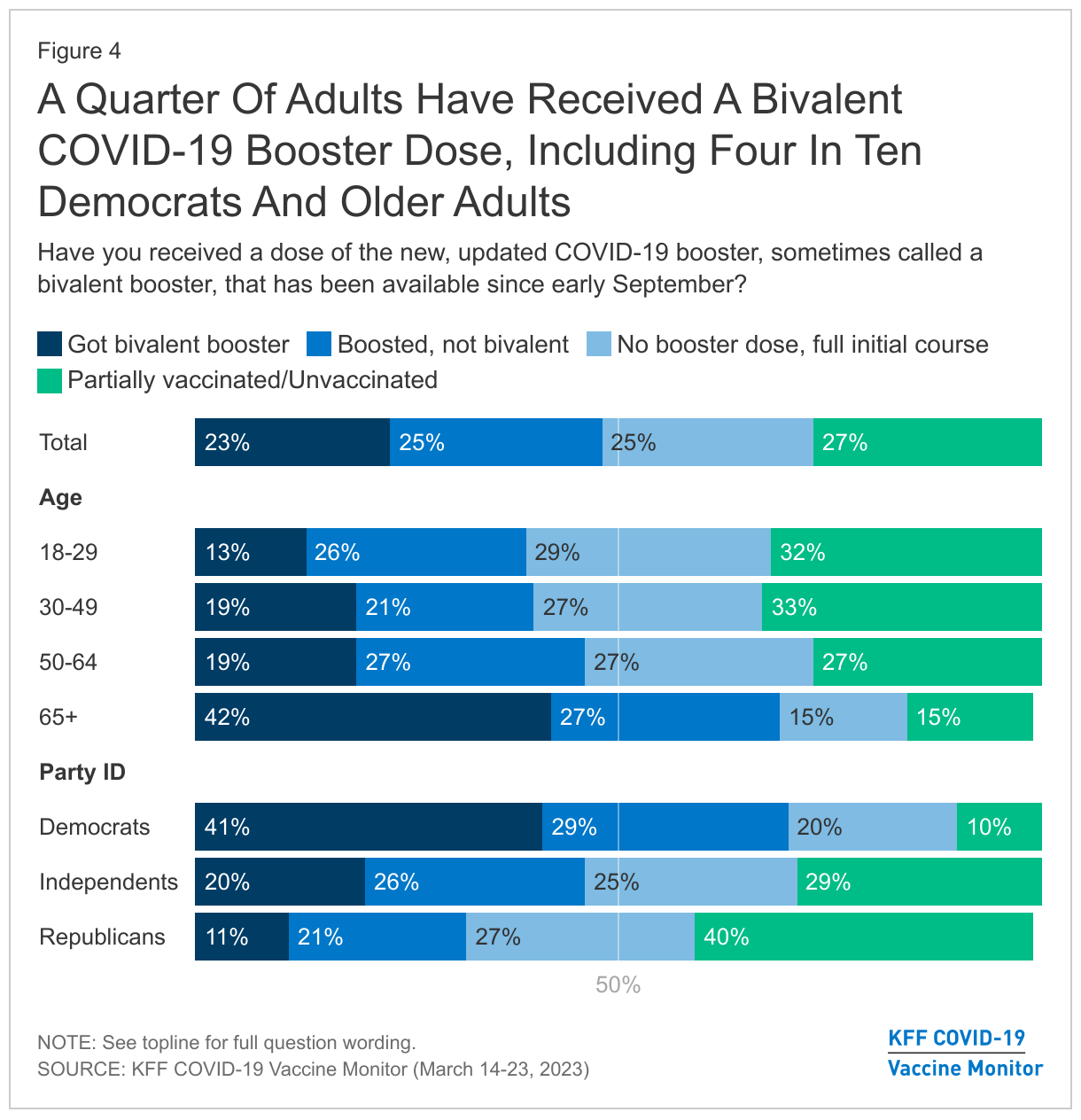
The latest KFF COVID-19 Vaccine Monitor reports a quarter of adults (23%) saying they have received the bivalent booster, the most recent version of the COVID-19 vaccine that became available in September 2022. As discussions surrounding the timing of boosters continue, about half of adults say they’re likely to get a COVID-19 vaccine annually if one was offered in that time frame, like a flu shot, including one in three (32%) who say they’re “very likely” to get an annual COVID-19 vaccine. Vaccinated adults and those who already receive annual flu shots are among the largest shares to say they’re likely to get an annual COVID-19 booster.
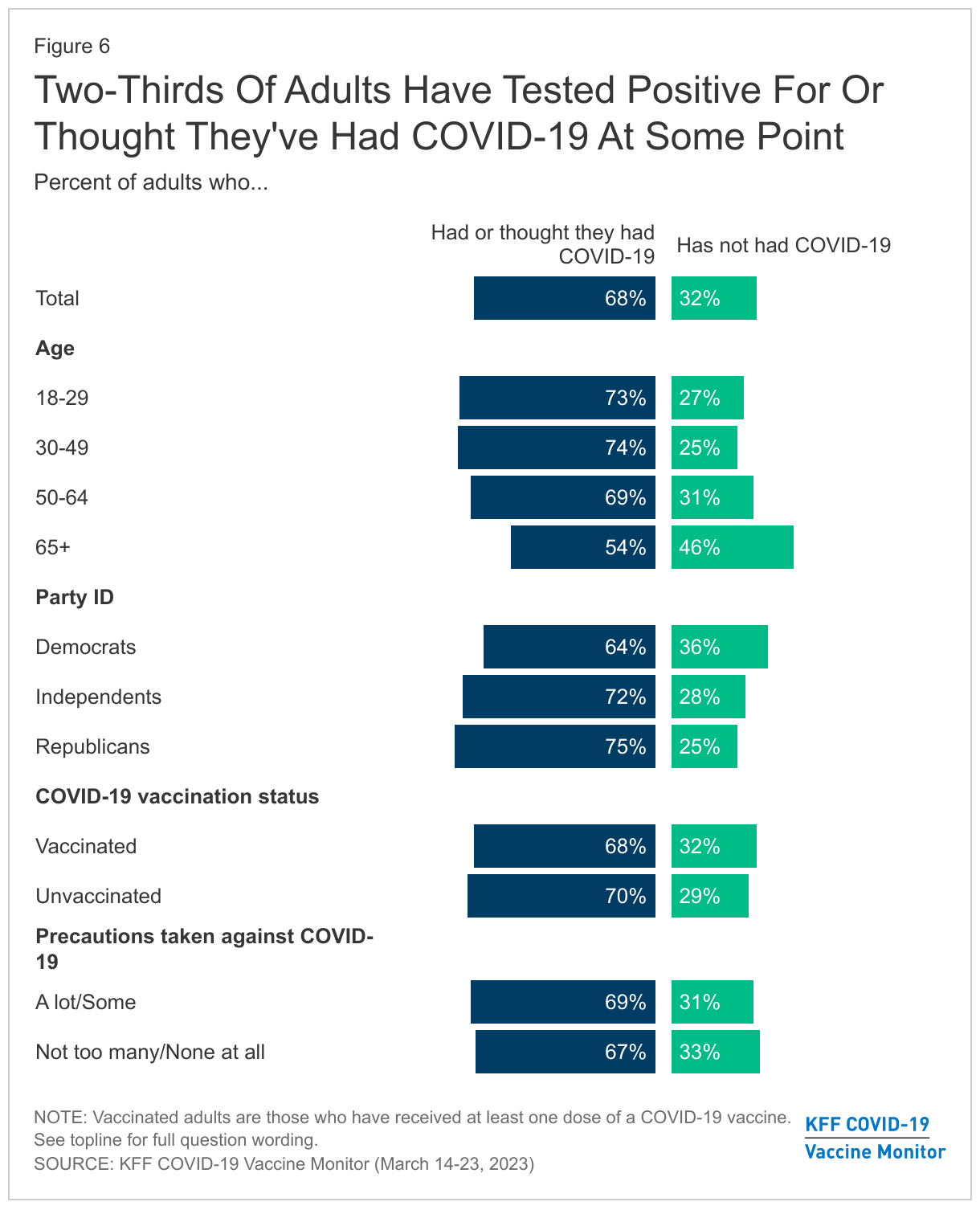
About two-thirds of U.S. adults say they have either tested positive for COVID-19 (55%) or thought they had it even if they didn’t test positive (13%). This leaves around one-third of adults who don’t think they have had COVID-19. When it comes to who hasn’t had COVID yet, smaller shares of those ages 65 and older and Democrats report testing positive for or thinking they’ve had the virus at some point.
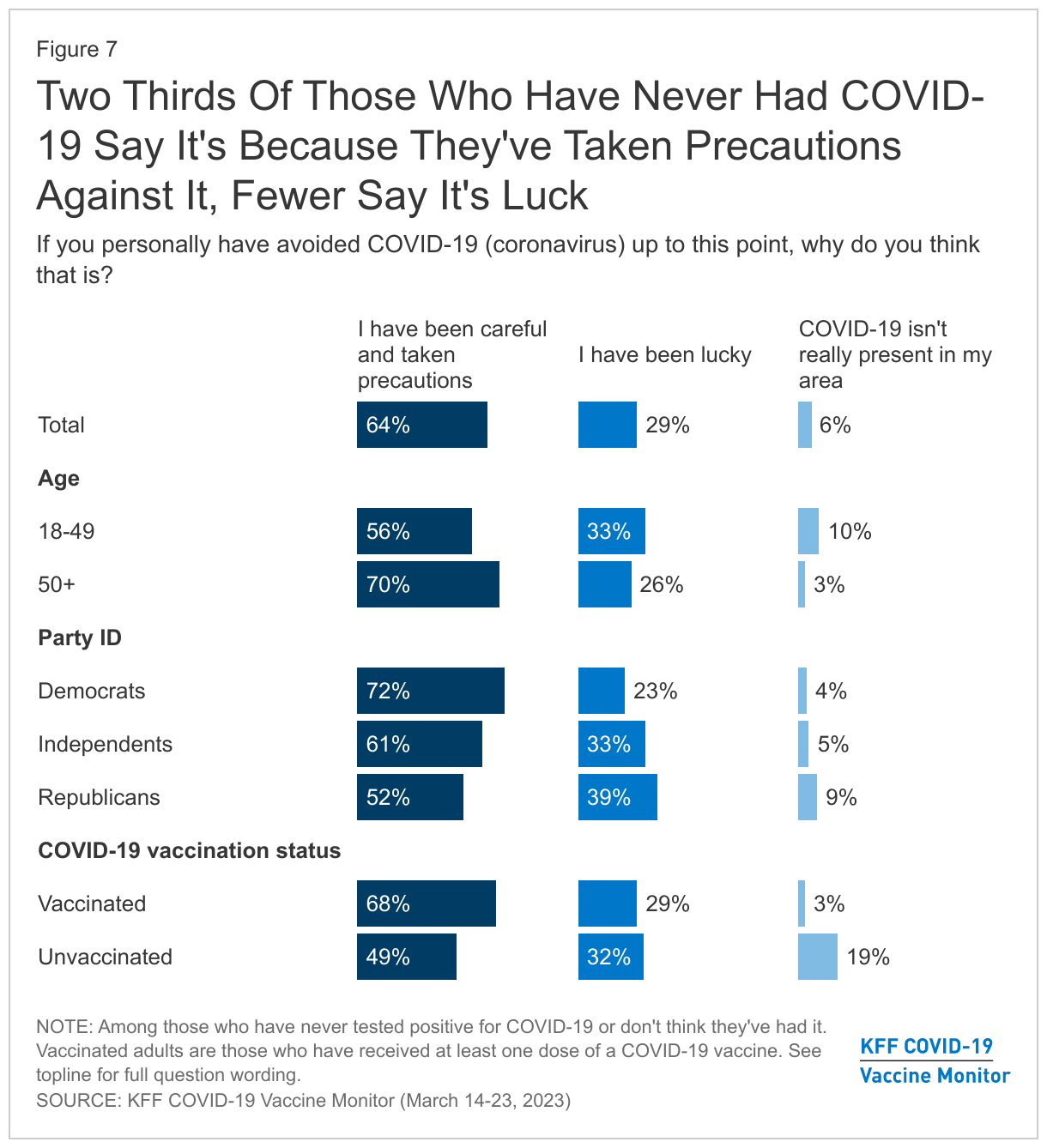
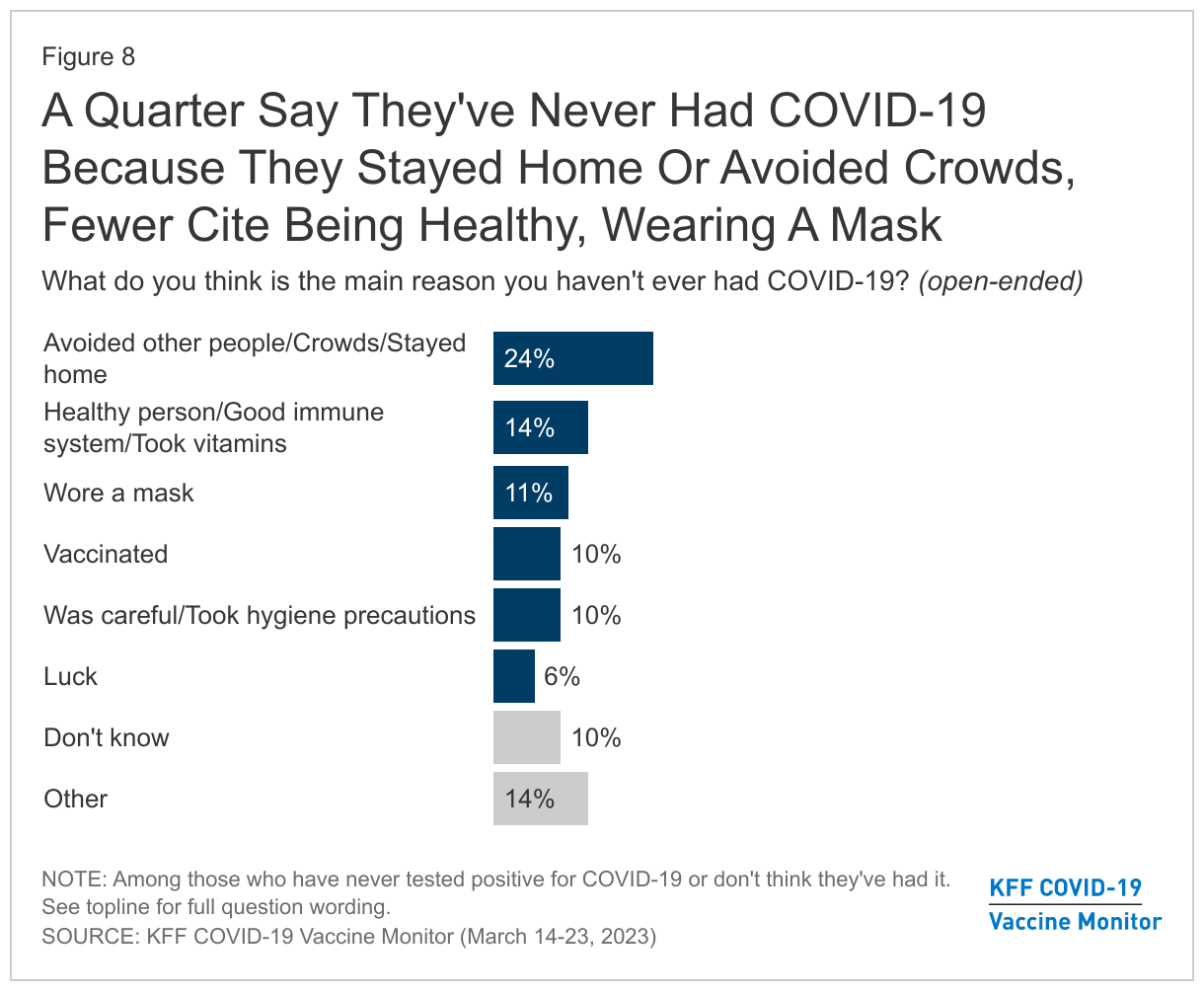
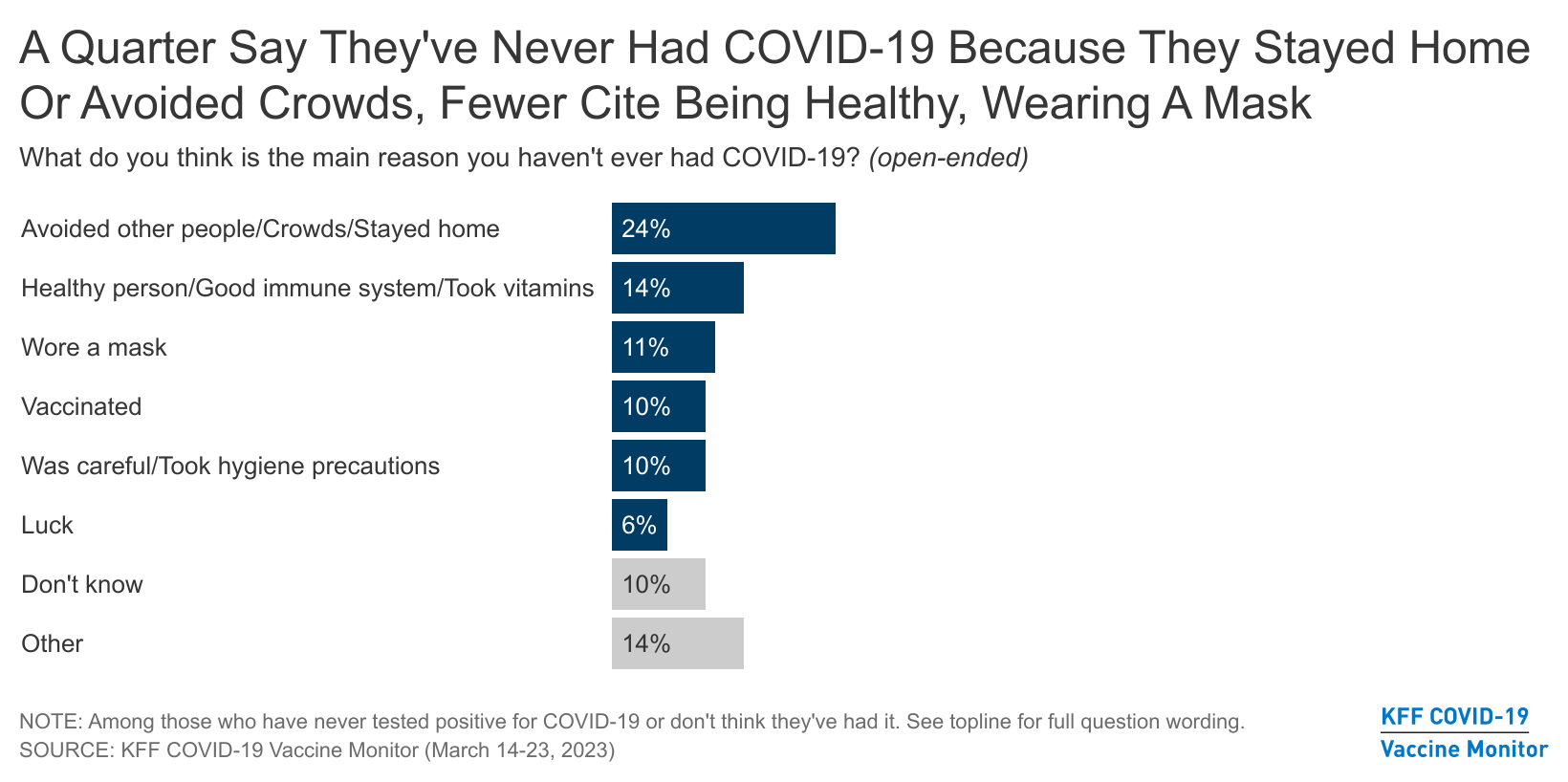
When those who say they’ve never had COVID are asked to say, in their own words, why they believe they haven’t been infected, 24% say they’ve avoided other people and crowds or stayed home. Another 14% say they’re generally healthy or have a good immune system. Around one in ten say they haven’t had COVID because they wore a mask (11%), they were vaccinated (10%), or they were generally careful and took hygiene precautions (10%). Fewer than one in ten (6%) say they were lucky. Similar shares across partisan lines cite avoiding people and staying home as their reasoning for never having COVID-19, but larger shares of Republicans than Democrats say they’re healthy with a good immune system (22% v. 5%) while larger shares of Democrats than Republicans say wearing a mask was the main reason they haven’t contracted the virus (20% v. 1%).
The Ending Of The Public Health Emergency
On May 11, 2023, the Biden administration intends to end the national emergency and public health declarations related to the COVID-19 pandemic. The emergency declarations, which were put in place by President Donald Trump in early 2020, giving the federal government flexibility to waive or modify certain requirements in a range of areas, including in the Medicare, Medicaid, and CHIP programs, and in private health insurance.
One in five adults have heard “nothing at all” when it comes to the Biden administration’s plan to end the COVID-19 public health emergency (PHE), with an additional 30% saying they’ve heard “not too much.” That leaves around half of adults saying they have heard at least “some” about the end of the PHE, including 10% who have heard “a lot.”
Older adults have been one of the most highly impacted groups by COVID-19 – adults ages 50 and older are more likely to have heard “a lot” or “some” about the end of the public health emergency, with 57% who say so, compared to 42% of those under 50.
Another impacted group by the pandemic, the uninsured, are less likely to have heard about the end of the PHE. Almost half (48%) of insured adults under the age of 65 have heard “a lot” or “some” about the plan to end the PHE, compared to 31% of those without insurance.
Less than half of Black adults (43%) and Hispanic adults (42%) have heard at least “some” about the end of the PHE, compared to half of White adults (51%). Similar shares of Democrats, Republicans, and independents have heard at least “some” about the end of the PHE.
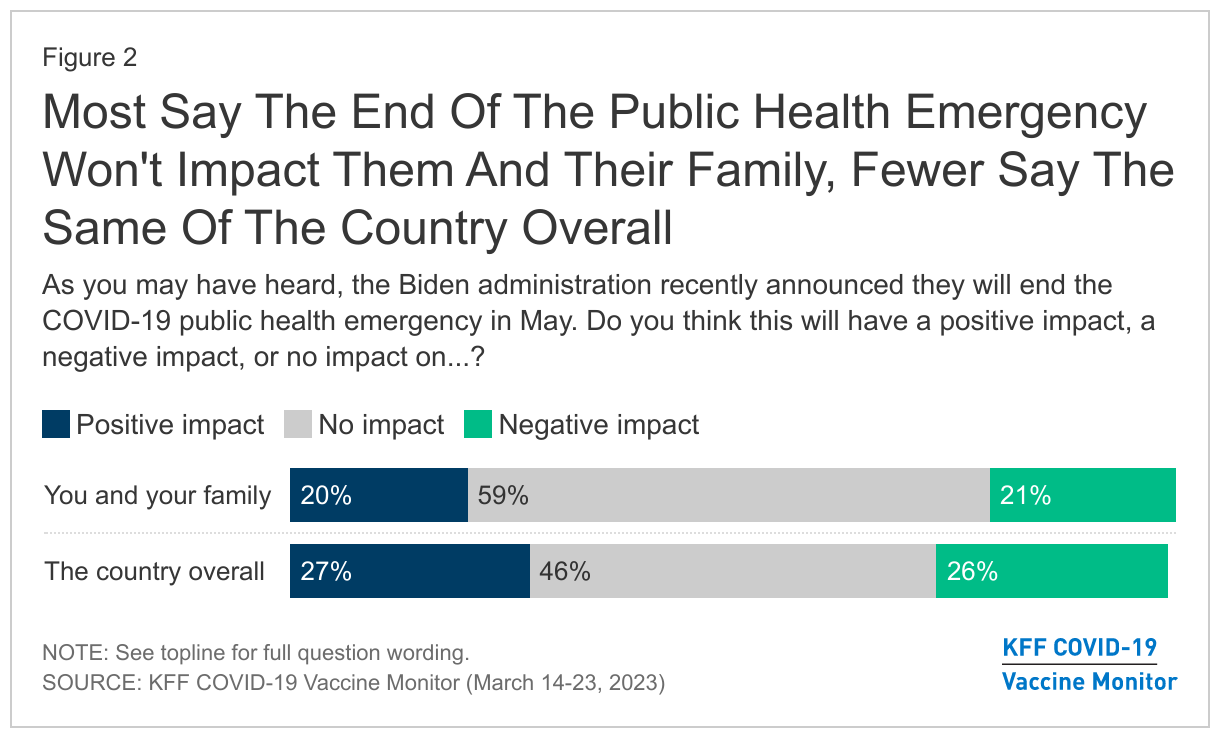
Six in ten (59%) adults think the end of the COVID PHE will have “no impact” on them and their family and almost half (46%) say it won’t have an impact on the country overall.
Similar shares say they think the end of the public health emergency will have a “positive impact” (20%) or a “negative impact” (21%) on them and their family. About a quarter of the public (27%) say it will have a “positive impact” on the country, while another quarter (26%) think the end of the public health emergency will have a “negative impact” on the country overall.
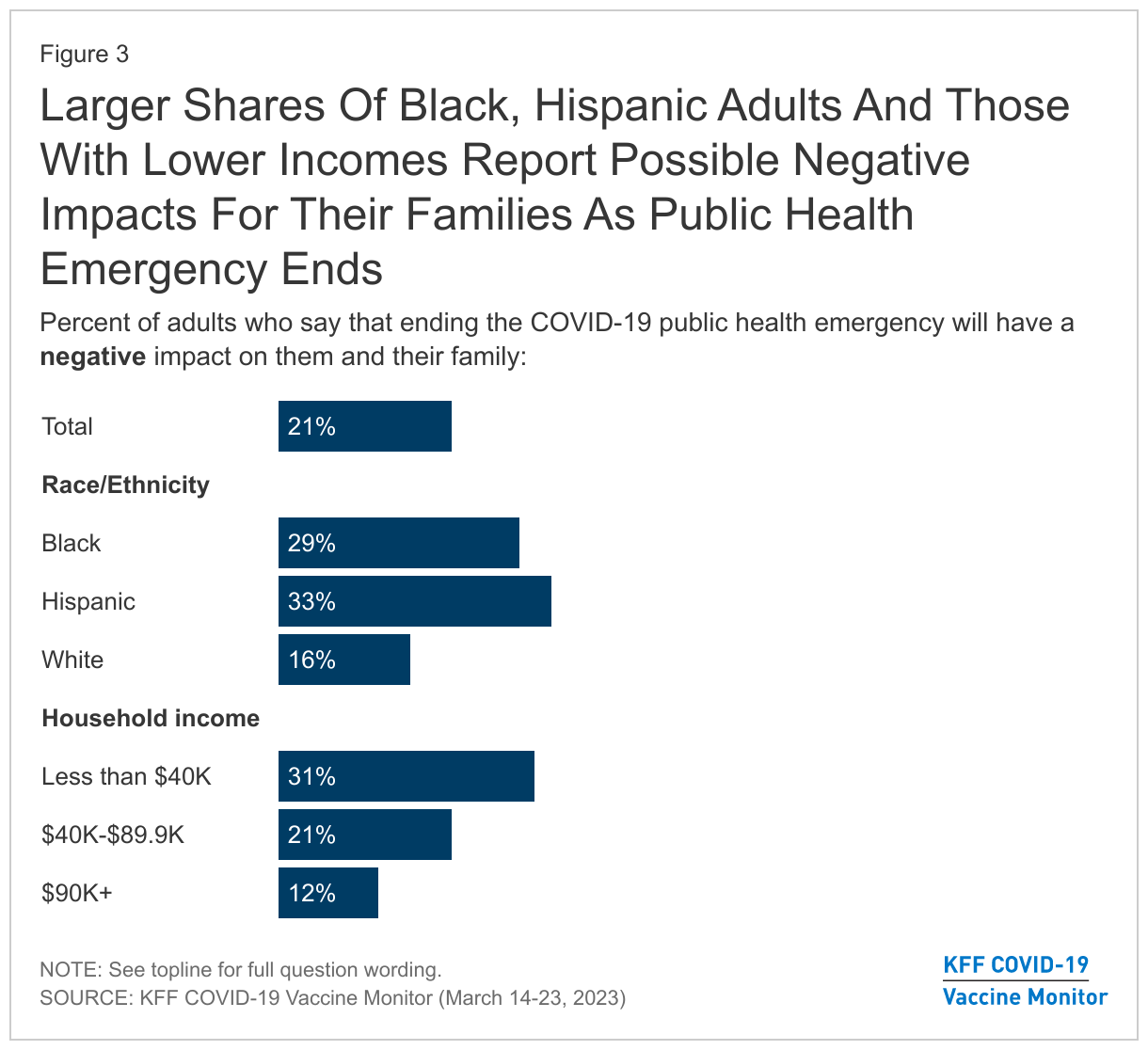
The end of the PHE is a bigger concern to some groups who have been more negatively affected by the coronavirus pandemic, with around three in ten Black adults (29%) and one-third of Hispanic adults reporting that the end of the COVID-19 public health emergency will have a negative impact on them and their family, compared to 16% of White adults. Three in ten adults (31%) living in households with incomes of less than $40,000 say the end of the PHE will have a negative impact on them and their family, compared to one in ten of those with incomes of $90,000 or more.
The Future Of Bivalent Boosters in the U.S.
The latest KFF COVID-19 Vaccine Monitor reports a quarter of adults (23%) saying they have received the bivalent booster, the most recent version of the COVID-19 vaccine that became available in September 2022. Slightly more than half of the public say they have either received an older booster dose but not the most recent version (25%) or received initial full course of vaccines but no booster doses (25%). One in four adults in the U.S. report being unvaccinated or partially vaccinated.
Adults ages 65 and older and Democrats are among the groups with the largest shares saying they have gotten the bivalent booster dose, with around four in ten who report getting their shot (42% of those ages 65 and older, and 41% of Democrats).
The Food and Drug Administration has begun discussions of what the future of the COVID-19 vaccinations will look like for Americans and how often booster doses will be available. One possibility presented by the FDA would be for the COVID-19 vaccine to be offered annually, like the flu shot, as the impact of COVID-19 booster doses have been shown to fade after about six months.
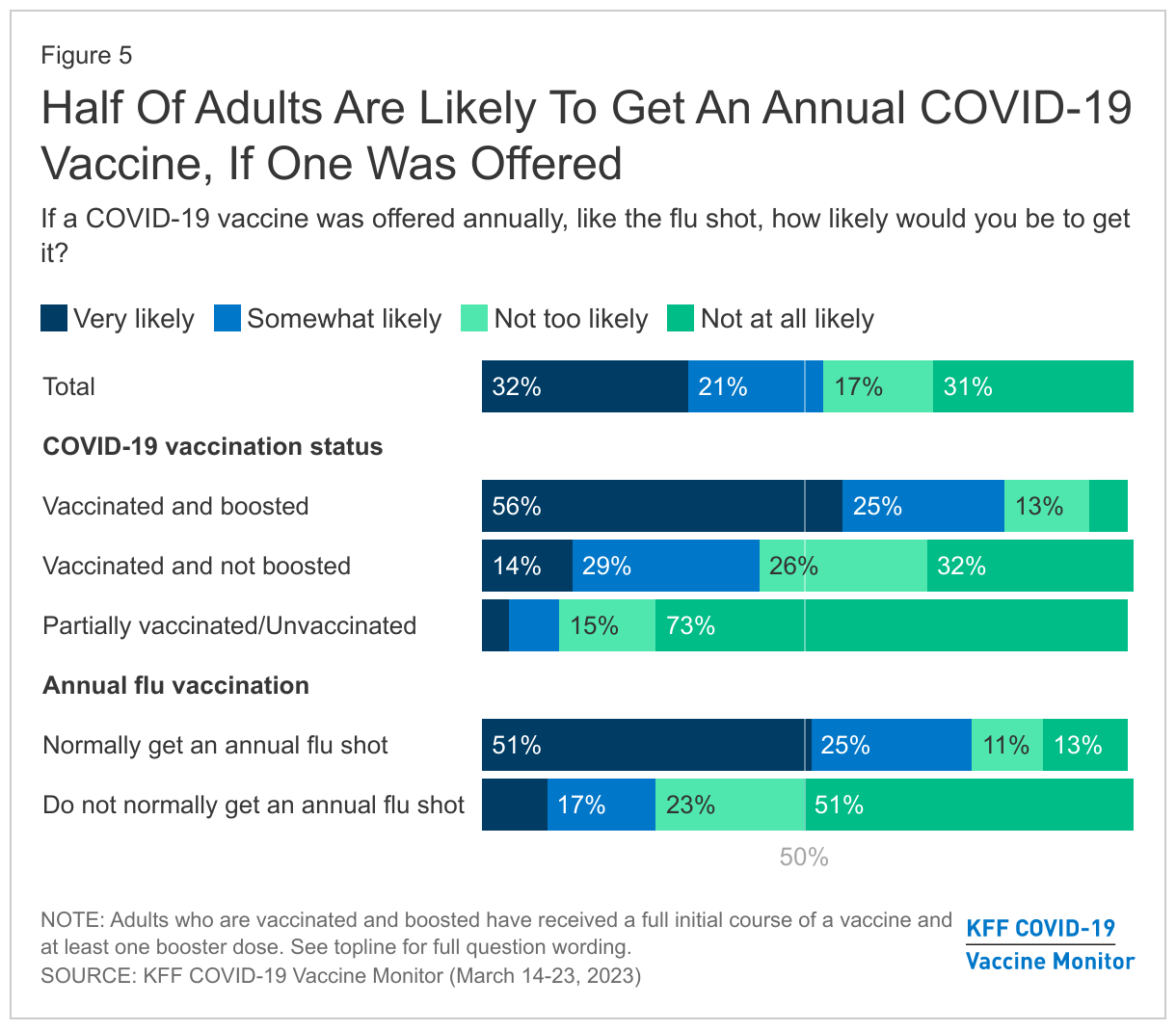
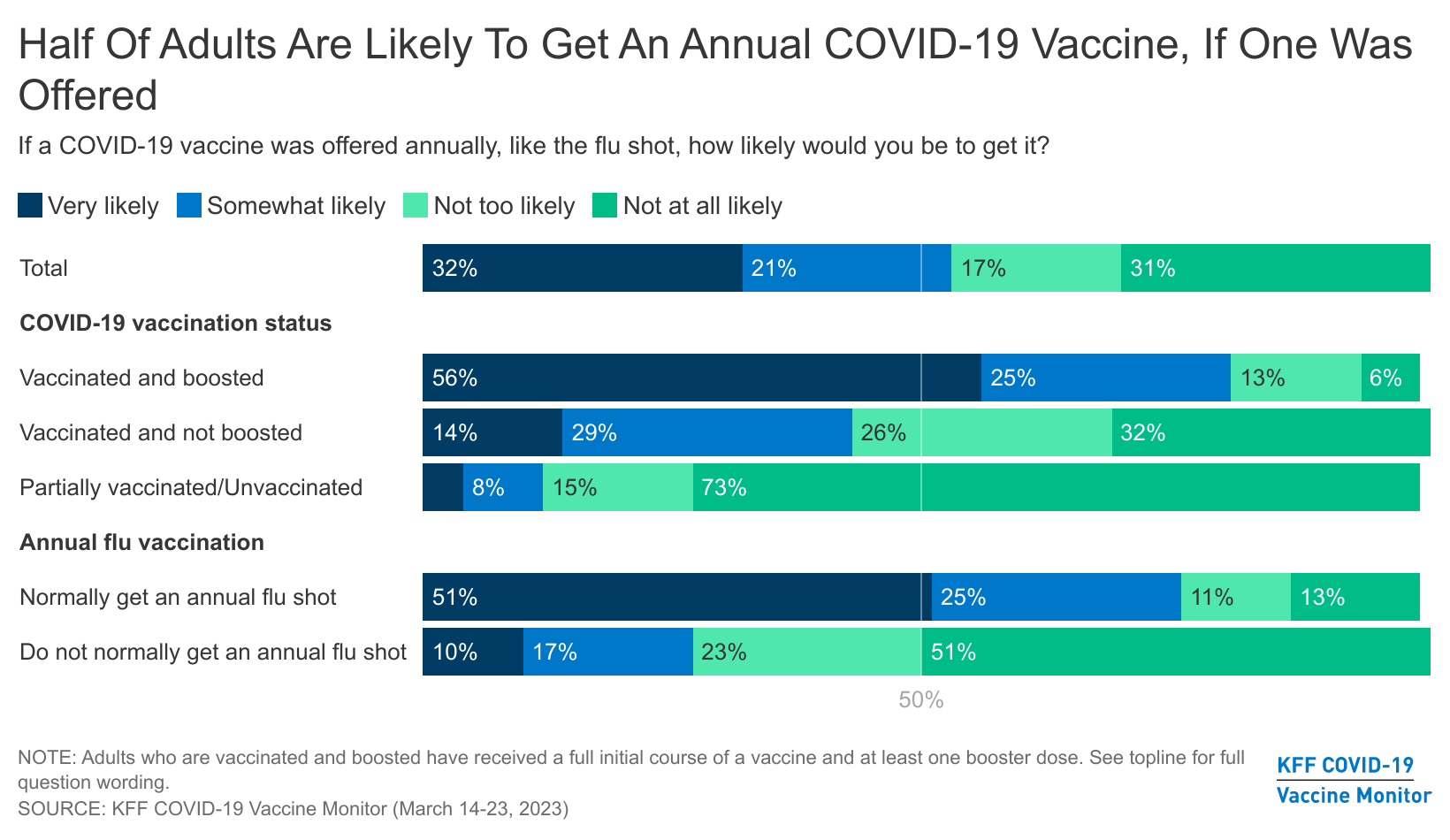
About half of adults say they’re likely to get a COVID-19 vaccine annually if one was offered in that time frame, like a flu shot, including one in three (32%) who say they’re “very likely” to get an annual COVID-19 vaccine. Vaccinated adults, especially those who have received a booster dose, are among the most likely to say they’d get a COVID-19 vaccine annually. Eight in ten adults who have received a booster dose of the vaccine say they would be likely to get an annual vaccine, including more than half who say they are “very likely.” Among the vaccinated adults who have not received the suggested boosters, willingness to get an annual vaccine lags, with less than half (42%) saying they would be likely to get an annual COVID-19 vaccine. In addition, about one in ten of those who are only partially vaccinated or unvaccinated say they would be likely to get a COVID-19 vaccine annually.
Those who get annual flu shots are more likely than those who don’t normally get flu shots to say they would be likely to get an annual COVID-19 vaccine. Three-fourths (76%) of those who say they normally get an annual flu vaccine (which is about 53% of all adults) say they’d be likely to get one, compared to 26% who don’t normally get their annual flu shot. About half (51%) of those who don’t get an annual flu vaccine say they’re “not at all likely” to get an annual COVID-19 vaccine.
People Report Various Reasons For Never Having COVID-19
About two-thirds of U.S. adults say they have either tested positive for COVID-19 (55%) or thought they had it even if they didn’t test positive (13%). This leaves around one-third of adults who don’t think they have had COVID-19. The share of adults who don’t think they have had COVID-19 increases to nearly half of adults 65 and older, a group that had earlier access to vaccines and booster doses due to increased risks and complications from the virus.
A slightly larger share of Democrats compared to Republicans say they don’t think they have had COVID-19 (36% v. 25%), which may be related to both higher vaccination rates among Democrats as well as that group being more likely to report taking “a lot” of precautions (54% v. 24%) to not get sick.
Notably, there is no difference in the share who say they’ve had COVID between vaccinated and unvaccinated adults (68% v. 70%). There is also no difference in the share who say they’ve had COVID between groups who report taking “a lot” or “some” precautions against COVID-19 (such as wearing a mask or avoiding large crowds) versus those who report taking “not too many” or no precautions at all (69% v. 67%).
Most people (64%) who haven’t had COVID-19 think they have avoided the virus because they have been careful and taken precautions. This is more than twice the share who attribute their lack of illness to being lucky (29%). Less than one in ten (6%) say COVID isn’t really present in their area.
Most Democrats (72%), adults ages 50 and older (70%), and vaccinated adults (68%) who haven’t gotten sick attribute it to being careful and taking precautions. While half of Republicans who haven’t gotten sick also say it is because they have been careful, about four in ten (39%) cite being lucky as their reason for not getting COVID.
Larger shares of unvaccinated adults than those who are vaccinated say that COVID isn’t really present in their area (19% of unvaccinated adults v. 3% of vaccinated adults).
When those who haven’t gotten COVID were asked to provide what they think the main reason was in their own words, about a quarter (24%) offer responses related to avoiding other people and crowds or staying home. Another 14% attribute it to the fact that they’re generally healthy or have a good immune system. Around one in ten think they haven’t had COVID because they wore a mask (11%), they were vaccinated (10%), or they were generally careful and took hygiene precautions (10%). Fewer than one in ten (6%) offer responses related to them being lucky.
Similar shares across partisan lines cite avoiding people and staying home as their reasoning for never having COVID-19, but larger shares of Republicans than Democrats say they’re healthy with a good immune system (22% v. 5%) while larger shares of Democrats than Republicans say wearing a mask was the main reason they haven’t contracted the virus (20% v. 1%).
In their own words: “What do you think is the main reason you haven’t ever had COVID-19?”
“I practice safety measures such as wearing a mask, washing my hands, and sanitizing, and I received all my vaccine shots.” – 21 year-old, female, Hispanic, California, vaccinated
“I think it is B.S.” – 63 year-old, male, White, California, unvaccinated
“Because I have not been around people and up until recently, I masked all day. Plus the fact that I have gotten all of the vaccines.” – 69 year-old, female, Black, South Carolina, vaccinated
“Because I practice holistic medicine.” – 30 year-old, female, Black, North Carolina, unvaccinated
“Because I stay away from crowds. I do my shopping or laundry, I only go out when I have to, and I wear a mask.” – 55 year-old, male, Black, New York, vaccinated
“Lucky, maybe use of mouthwash.” – 66 year-old, male, White, Illinois, vaccinated
“I didn’t go out as much and I take supplements to strengthen my immune system.” – 21 year-old, female, Hispanic, Texas, vaccinated
“Masks and the fact that I am terrified of getting sick helps me to prevent spreading germs.” – 22 year-old, female, Hispanic, Maryland, vaccinated
Methodology
This KFF Health Tracking Poll/COVID-19 Vaccine Monitor Poll was designed and analyzed by public opinion researchers at KFF. The survey was conducted March 14-23, 2023, online and by telephone among a nationally representative sample of 1,271 U.S. adults in English (1,198) and in Spanish (73). The sample includes 986 adults reached through the SSRS Opinion Panel either online or over the phone (n=33 in Spanish). The SSRS Opinion Panel is a nationally representative probability-based panel where panel members are recruited randomly in one of two ways: (a) Through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Groups (MSG) through the U.S. Postal Service’s Computerized Delivery Sequence (CDS); (b) from a dual-frame random digit dial (RDD) sample provided by MSG. For the online panel component, invitations were sent to panel members by email followed by up to three reminder emails. 961 panel members completed the survey online and panel members who do not use the internet were reached by phone (25).
Another 285 (n=40 in Spanish) interviews were conducted from a random digit dial telephone sample of prepaid cell phone numbers obtained through MSG. Phone numbers used for the prepaid cell phone component were randomly generated from a cell phone sampling frame with disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification was based on incidence of the race/ethnicity groups within each frame. Respondents in the phone samples received a $15 incentive via a check received by mail, and web respondents received a $5 electronic gift card incentive (some harder-to-reach groups received a $10 electronic gift card).
The online questionnaire included two questions designed to establish that respondents were paying attention. Cases that failed both attention check questions, those with over 30% item non-response, and cases with a length less than one quarter of the mean length by mode were flagged and reviewed. Cases were removed from the data if they failed two or more of these quality checks. Based on this criterion, no cases were removed.
The combined cell phone and panel samples were weighted to match the sample’s demographics to the national U.S. adult population using data from the Census Bureau’s 2021 Current Population Survey (CPS). Weighting parameters included sex, age, education, race/ethnicity, region, and education. The sample was weighted to match patterns of civic engagement from the September 2017 Volunteering and Civic Life Supplement data from the CPS and to match frequency of internet use from the National Public Opinion Reference Survey (NPORS) for Pew Research Center. Finally, the sample was weighted to match patterns of political party identification based on a parameter derived from recent ABS polls conducted by SSRS polls. The weights take into account differences in the probability of selection for each sample type (prepaid cell phone and panel). This includes adjustment for the sample design and geographic stratification of the cell phone sample, within household probability of selection, and the design of the panel-recruitment procedure.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. KFF public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
More than three years into the COVID-19 pandemic, about half (53%) the public says they would likely get an annual COVID-19 vaccine if offered similar to an annual flu shot, the latest KFF COVID-19 Vaccine Monitor finds. This includes about a third (32%) who would be “very likely” to do so.
The findings provide a window into the potential uptake of an annual COVID-19 vaccine, which the Food and Drug Administration has raised as a potential option to provide future protection from the virus.
Larger shares of people who typically get an annual flu shot (76%) say they are likely to get an annual COVID-19 vaccine than those who don’t normally get a flu shot (26%).Not surprisingly, the vast majority (81%) of people who are already vaccinated and boosted against COVID-19 say they would be likely to get an annual shot. About four in 10 (42%) of those who have been vaccinated but not boosted say they would at least somewhat likely get an annual shot, while about three-quarters (73%) of those who are unvaccinated or only partially vaccinated say are “not at all likely” to get an annual shot.
COVID-Free?
Nearly a third (32%) of all adults nationally say they have never tested positive for COVID-19 or never thought they’ve had the virus, and the new survey examines their experiences.This never-had-it group includes nearly half (46%) of adults ages 65 and older, who generally had earlier access to the vaccines due to their high risks. A larger share of Democrats (36%) than Republicans (25%) say they’ve never gotten the COVID-19, while the shares are similar among those who were vaccinated (32%) and unvaccinated (29%).Almost two thirds (64%) of those in the never-had-it group attribute their success in avoiding the virus to being careful and taking precautions, more than twice the share that say they were lucky (29%). In comparison, few (6%) believe it is because COVID-19 isn’t really present in their area.
When asked to say in their own words the main reason why they think they haven’t gotten COVID-19, about a quarter (24%) cite avoiding crowds or staying home. Other reasons include having a good immune system and generally being healthy (14%), wearing masks (11%), being vaccinated (10%), and generally being careful and taking precautions (10%). A small share (6%) say they believe it was good luck.
Other findings include:
Nearly a quarter (23%) of adults say they’ve gotten the latest bivalent COVID-19 booster, which has been available since September. Similar shares say they have received an earlier booster shot (25%) or have gotten their initial course of vaccinations but no booster (25%). That leaves slightly more than a quarter (27%) who say that they are either partially vaccinated or not vaccinated at all.
Half (49%) of adults say they’ve heard at least something about the Biden administration’s plan to end the COVID-19 public health emergency on May 11.
Similar shares of the public say that the end of the public health emergency will have a positive (20%) or negative (21%) impact on them and their families, though most (59%) say that it will have no impact. Larger shares of Hispanic (33%) and Black (29%) adults, as well as those in low-income households (31%), say the emergency’s end will hurt them and their families.
Designed and analyzed by public opinion researchers at KFF, the survey was conducted from March 14-23, 2023, online and by telephone among a nationally representative sample of 1,271 U.S. adults, in English and in Spanish. The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on other subgroups, the margin of sampling error may be higher.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and acceptance, information needs, trusted messengers and messages, as well as the public’s experiences with vaccination.
The Trump Administration aimed to reshape the Medicaid program by newly approving Section 1115 waivers that included work and reporting requirements as a condition of Medicaid eligibility. However, courts struck down many of these requirements and the Biden Administration withdrew these provisions in all states that had approvals. After these withdrawals, in April 2022 the Supreme Court dismissed pending appeals in cases that had found work requirement approvals unlawful. However, these provisions remain in place in Georgia, as a Federal District Court judge vacated the Administration’s rescission of work and premium requirements in the Georgia Pathways waiver. Additionally, other states have indicated they may pursue work requirement waivers in the future, and some Congressional Republicans have recently discussed a federal Medicaid work requirement. This Waiver Watch summarizes the recent history of work requirements, the current status of Georgia’s waiver, and key state and federal issues to watch.
What is the recent history and current status of work requirements in Medicaid?
In a departure from previous administrations, the Trump Administration approved Section 1115 waivers that conditioned Medicaid coverage on meeting work and reporting requirements, but the Biden Administration withdrew these approvals. Thirteen waivers with work requirements had been approved during the Trump administration. Following the Biden Administration’s withdrawals, in April 2022 the Supreme Court dismissed pending appeals in cases that had found work requirement approvals unlawful. The Supreme Court’s dismissal does not preclude future presidential administrations from approving new Section 1115 work requirements. To survive an expected legal challenge, the administrative record in any future approvals would likely have to support the conclusion that such waivers would further Medicaid program objectives.
As most Medicaid enrollees are already working or face barriers to work, work and reporting requirements may result in coverage loss among eligible enrollees without increasing employment. Prior to the pandemic, the majority (63%) of non-elderly adult Medicaid enrollees who did not qualify based on a disability were already working full- or part-time. Most who were not working would likely meet exemptions from work requirement policies (e.g., had an illness or disability or were attending school), leaving just 7% of these enrollees to whom work requirement policies could be directed. Although few Medicaid work and reporting requirements were ultimately implemented due to litigation, state withdrawals, and/or pauses during the COVID-19 pandemic, available implementation data from Arkansas suggests that these requirements were confusing to enrollees and result in substantial coverage loss, including among eligible individuals.
What is the status of Georgia’s waiver?
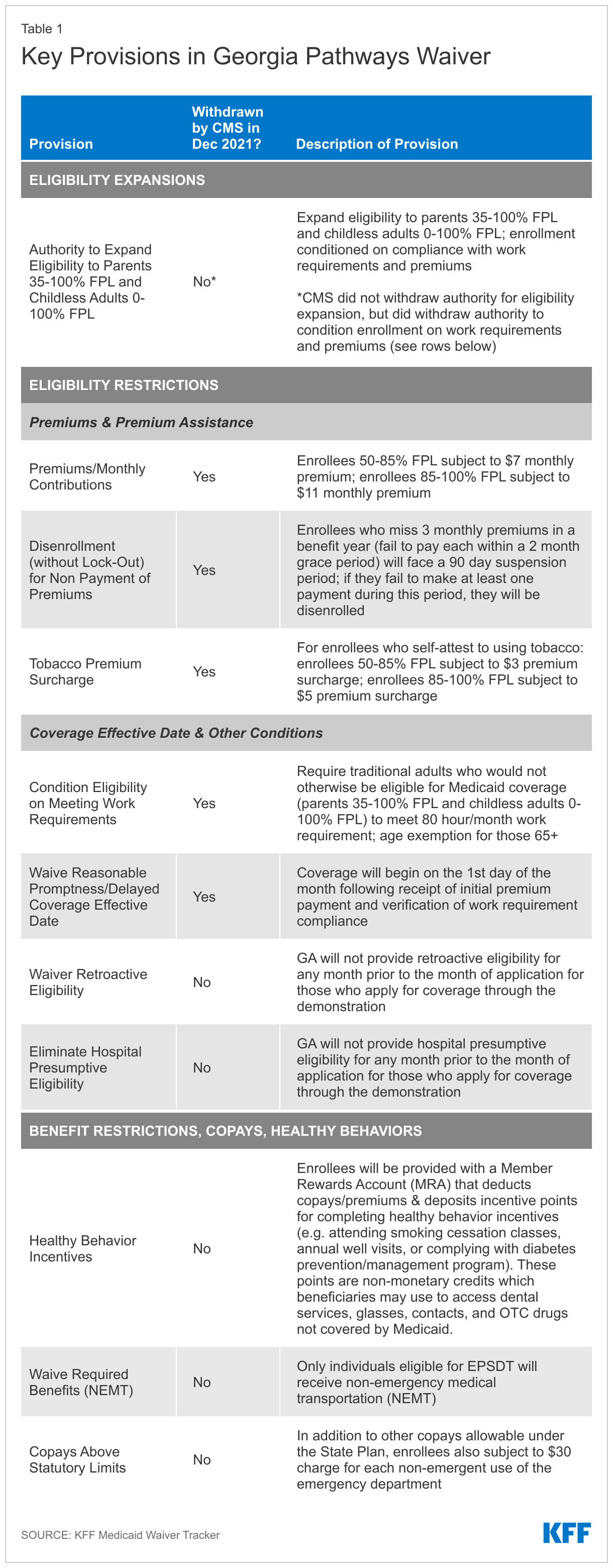
Although CMS withdrew the work and premium requirement components of Georgia’s waiver, these provisions remain in place after a federal judge vacated the CMS rescission. In December 2021, CMS rescinded work requirement and premium authorities that the Trump Administration had approved as part of a limited coverage expansion in Georgia’s waiver—an action that the state subsequently challenged in court. In August 2022, a Federal District Court judge issued a decision in favor of the state, vacating CMS’s rescission thus reinstating these provisions. Although CMS generally reserves the right to withdraw waiver authorities at any time, the judge found that its rescission of Georgia’s waiver provisions was arbitrary and capricious due to agency errors, including that it failed to weigh that the waiver would have increased Medicaid coverage. CMS did not appeal this decision. Georgia Governor Brian Kemp allocated $52 million in his proposed state fiscal year (FY) 2024 budget to implement the Georgia Pathways program beginning July 1, 2023.
Once implemented, Georgia’s waiver will expand eligibility to 100% of the federal poverty level (FPL), with initial and continued enrollment conditioned on meeting work and premium requirements. These and other provisions of the Georgia Pathways waiver, including additional eligibility and benefit restrictions, are summarized in more detail in Table 1. The work requirement would apply to enrollees below age 65, with “good cause exceptions” (for those who cannot fulfill the requirement in a given month due to a circumstance such as a family emergency) and “reasonable accommodations” (to enable individuals with disabilities to meet the requirement) available. The state originally estimated that the Georgia Pathways waiver would provide coverage to about 64,000 individuals—significantly less than the estimated 269,000 uninsured individuals in the Medicaid coverage gap (parents with incomes that exceed Medicaid eligibility levels but are below the FPL, plus childless adults with incomes below the FPL) who could be covered if Georgia adopted the ACA Medicaid expansion.
What are key issues to watch?
Looking ahead, key questions to watch will play out at the state and federal levels:
How will implementation of the Georgia waiver go? It remains to be seen exactly how many currently uninsured individuals under 100% FPL will meet the work (as well as premium) requirements necessary to enroll in the new coverage program. Looking ahead, Section 1115 monitoring and evaluation requirements will require Georgia to track and report the number of enrollees who gain and maintain coverage.
Will other states pursue work requirements? Several other states have indicated they may pursue work requirements, but unlike Georgia, these states have already adopted Medicaid expansion and would not be adding new coverage. In February 2023, Arkansas Governor Sarah Huckabee Sanders directed the state to submit a new work requirement waiver request with a proposed effective date of January 2024. In both Iowa and West Virginia (two states that did not previously pursue work requirement waivers), proposed state legislation would direct eachstate to seek waivers that include work requirements and to resubmit such requests periodically until approval. Finally, in March 2023, North Carolina Governor Roy Cooper signed a law that would direct the state to expand Medicaid (contingent on appropriations in the biennial budget), and to seek approval to apply a work requirement to this population if there is ever any indication that the federal government would approve such a waiver. Because these states all propose applying a work requirement to an existing Medicaid population rather than to a new coverage group as in Georgia, it is unclear if the rationale that the Federal District Court ruling used in Georgia would apply. While the Biden Administration does not believe work requirements further Medicaid objectives, a future presidential administration could revisit these waiver provisions. However, any future work requirements approved would likely face legal challenges.
Will there be debate over federal legislation related to Medicaid work requirements? Ahead of federal budget debates, Congressional Republicans have indicated that they will rely on a budget outline that would require Medicaid enrollees to work, or look for work, in order to receive coverage (in addition to other Medicaid programmatic cuts); recently, Republican Speaker of the House Kevin McCarthy highlighted work requirements as a policy to reduce the debt limit. Previously, Republican attempts in 2017 to allow states to require work as a condition of Medicaid eligibility (as part of the ACA repeal and replace debate) were unsuccessful. While some policymakers favor work requirements as a policy, they are unlikely to result in significant savings or result in large increases in enrollee employment rates, since the vast majority of Medicaid enrollees are already working or would likely qualify for exemptions.
The Africa Centers for Disease Control and Prevention (Africa CDC) works to build the capacity of public health institutions across Africa to strengthen the timeliness and effectiveness of public health responses. First envisioned a decade ago, the 2014 West African Ebola outbreak accelerated its creation and it was formally approved as a specialized technical entity of the African Union (AU) in 2016. While it originally operated as an arm of the AU, with the aim of establishing a new regionally owned and managed “public health order for Africa” it has grown in prominence and role including being recognized as helping to lead the African continent’s response to COVID-19. In 2022, the AU revised the foundational statute for Africa CDC to transform the institution from a specialized technical agency of the AU to an autonomous public health body. As the global community increasingly focuses on strengthening global health security in advance of future pandemics and health emergencies, there is growing recognition that Africa CDC occupies an especially strategic position with respect to pandemic preparedness and response.
This brief reviews the history of Africa CDC, describing its structure, funding and operations to date, including U.S. government engagement, as well as challenges and opportunities for the institution moving forward. It is based on analysis of the literature and interviews with experts.
Creation and Evolution of Africa CDC
While African leaders officially recognized the need for the creation of an Africa-wide public health agency in 2013, it was the 2014 West African Ebola outbreak that drove home this need and accelerated the process. After formal approval by the AU in 2016, Africa CDC was officially launched in January 2017. The Africa CDC’s founding statute declared that the agency would function as an organ of the African Union and like the AU, it is based in Addis Ababa. In early 2017, Cameroon-born Dr. John Nkengasong, a longtime public health official at the U.S. Centers for Disease Control and Prevention (CDC), was named the first head of Africa CDC. Nkengasong is cited by key informants as a driving force in Africa CDC’s launch and maturation.
AU member states have primary responsibility for public health activities within their borders. Much like the U.S. Centers for Disease Control and Prevention, Africa CDC plays a normative, coordinating and capacity-building role. This encompasses work in a number of areas, as directed by its founding statute, including early warning and response, pandemic preparedness and response, mapping hazards and risks, supporting emergency responses, promoting partnership and collaboration on health, harmonizing disease control and prevention policies, and building public health capacity (including field epidemiology and laboratory capacity). The founding statute directs Africa CDC to establish and work through regional collaborating centers representing the five major sub-regions on the continent: Central Africa, Eastern Africa, Northern Africa, Southern Africa, and Western Africa.
Africa CDC was minimally staffed at its outset, with U.S. CDC seconding two technical experts to work alongside Nkengasong to get the agency up and running. Its initial focus was in supporting the development of regional capacity for syndromic surveillance (i.e., monitoring of illnesses to provide early warning of disease spread). In recent years, as external funding has increased (see below) and the agency’s remit has expanded, staffing has substantially grown, with one key informant referring to the increase on staffing as “exponential.” With financing from China, Africa CDC now has a new headquarters in Addis Ababa which will include an emergency operations center, a data center, a laboratory, and other facilities.
The founding statute also directs Africa CDC to collaborate with the World Health Organization and other partners to enhance coordination and avoid overlap. Prior to the formal launch of Africa CDC, the African Union Commission and WHO executed a framework of collaboration to guide and inform the working relationship between Africa CDC and WHO, as the respective constituencies of the two organizations differ in some respects. Africa CDC’s geographic remit is more extensive than WHO’s, as several AU member states (including Djibouti, Somalia, Libya, Morocco, Sahwari Republic, and Tunisia) are not members of WHO’s AFRO region. Another difference is that while WHO’s African regional office works primarily through Ministers of Health, Africa CDC, as a body of the AU, has a direct line to, and ability to convene, African Heads of State.
Although created by the African Union, it was initially expected that the agency would operate somewhat independently of the AU bureaucracy. In practice, however, the AU often exercised close oversight and control over such functions as hiring, approval of travel and agency communications, which proved challenging to Africa CDC’s need for flexibility and rapid response to emerging health issues. External support assisted the agency in gaining agility and capacity in the early years, including funding from the Bill & Melinda Gates Foundation to accelerate the hiring of key personnel and to support strategic planning. Africa CDC (with support from the U.S. CDC) also leveraged the hiring capacity of the African Field Epidemiology Network (AFENET), a non-profit network that works to build capacity for public health functions, to strengthen epidemiological capacity across the region. After COVID-19, there was a broad recognition of the need for greater autonomy at the agency, which led to the AU’s decision in 2022 to clarify and institutionalize the independent nature of Africa CDC.
After Nkengasong left in 2022, following his U.S. Senate confirmation as U.S. Ambassador-at-Large and global HIV/AIDS coordinator, Dr. Ahmed Ogwell Ouma, a Kenyan epidemiologist, served as acting director. In February 2023, African heads of state approved Dr. Jean Kaseya, a Congolese public health expert, to serve as the first Director General of the newly autonomous Africa CDC.
Box 1: Africa CDC – A Timeline
July 2013: AU formally acknowledges the need for creation of Africa CDC
January 2014: AU Heads of State endorse initial concept for Africa CDC
January 2015 AU Heads of State request implementation roadmap for Africa CDC
January 2016: AU Heads of State ratify governing statute of Africa CDC
February 2016: U.S. CDC places technical staff at Africa CDC
May 2016: Africa CDC Governing Board selects John Nkengasong as first Director and authorizes creation of 5 regional collaborating centers
2017: Africa CDC launches first strategic plan for 2017-2021
January 2018: AU Heads of State approve organizational structure for Africa CDC
2018: Africa CDC maps laboratory capacity in 10 African countries
2018: Africa CDC deploys experts to respond to Ebola outbreak in DRC, to cholera outbreaks in Cameroon and Zimbabwe, to chikungunya in Sudan, and to Rift Valley fever in Kenya
2019: Africa CDC deploys experts to respond to Ebola outbreak in DRC, the Rift Valley fever outbreak in Kenya, and multiple outbreaks in Sudan
2019: Africa CDC finalizes frameworks for public health workforce, national public health institutes, and control of antimicrobial resistance
2019: Africa CDC acquires the Journal of Public Health in Africa to serve as a platform for timely information sharing
February 2020: Africa CDC establishes Africa Taskforce for Novel Coronavirus
March 2020: Africa Joint Continental Strategy for COVID-19 outbreak launched
March 2020: AU Heads of State hold emergency meeting on COVID-19 outbreak
March 2020: Africa CDC publishes first of what will be regular scientific and public policy updates on COVID-19
July 2020: African health and finance ministers meet to assess the status of COVID-19 control across the region
August 2020: Africa CDC, AU, the African Export-Import Bank and the United Nations Commission for Africa launch the African Vaccine Acquisition Trust (AVAT), with the World Bank joining later as a partner
January 2021: Africa CDC issues framework for fair, equitable and timely allocation of COVID-19 vaccines across the region
June 2022: John Nkengsong formally leaves Africa CDC after being sworn is as U.S. Ambassador-at-Large for Global Health Diplomacy and Global AIDS
July 2022: AU formally elevates the status of Africa CDC from a technical arm of the AU to an autonomous public health agency
January 2023: Africa CDC’s new headquarters is inaugurated
February 2023: African heads of state select Dr. Jean Kaseya as Director General of Africa CDC
March 2023: Africa CDC publicly releases its Second Strategic Plan (2022-2026)
Africa CDC Operations
Africa CDC is governed by a 15-person board, consisting of 10 health ministers (two per each of the five regions), two representatives of the African Union Commission, two nominees of the Commission chair, and one regional health organization. The Board directs and approves the agency’s strategy, operations, budget, and other key governance activities. There is also a 25-person advisory council, which reports to/informs the Board and provides technical guidance to Africa CDC.
The agency uses a decentralized model that relies on the work and cooperation of national health institutions, which are incorporated in each AU member state. As noted above, Africa CDC has established five regional collaborating centers in Central Africa, Eastern Africa, Northern Africa, Southern Africa, and Western Africa, which it funds, intended to serve as hubs for the strengthening and coordination of Africa CDC’s surveillance, preparedness and emergency response activities and to enable sub-regional approaches to disease outbreaks and other public health priorities. The regional collaborating centers are in various stages of development, with some becoming fully operational only in 2021.
Building robust laboratory capacity across the region – a pillar of pandemic preparedness – has been a major area of work for Africa CDC. Informed by an early mapping exercise of laboratory capacity gaps in Africa, Africa CDC provided laboratory workforce training and capacity-building support focused on preventing and addressing antimicrobial resistance. Through its Regional Integrated Surveillance and Laboratory Network (RISLNET), Africa CDC is working to establish harmonized standards to improve quality control and facilitate the sharing and timely, strategic use of public health data. These efforts have helped close gaps in disease detection in the region and accelerated the steady strengthening of laboratory systems in Africa. While these lab-focused efforts ultimately rely on the laboratory systems and professionals in AU member states, Africa CDC has helped to train laboratory workers and create a coordinated, linked regional laboratory network.
The agency also works to establish public health norms, partnerships and coordination mechanisms. For example, in July 2022, Africa CDC called on all African countries centers to respond to future health emergencies. It also provides a platform for the development of regional public health policies, such as the Africa Medical Supplies Platform, created in 2020 which pools and shares health resources and commodities. Africa CDC also enters into strategic partnerships to benefit the region, such as its Memorandum of Understanding with FIND to increase access to diagnostic tools as well as its close working relationship with the African Society for Laboratory Medicine (ASLM).
U.S. Government Collaboration with Africa CDC
The U.S. Government played a foundational role in the early days of Africa CDC, facilitated by having Dr. Nkengasong as its first director, and continues to serve as a central technical partner for the organization. U.S. CDC entered a Memorandum of Understanding with Africa CDC in 2015 and the following year placed two senior staff at Africa CDC. Alongside Nkengasong, these staff served as the organization’s early nucleus. Expertise from the U.S. CDC helped shape and direct the creation of syndromic surveillance systems across the region. U.S. CDC also supported Africa CDC’s early efforts to develop a strategic public health plan for the region. While the U.S. CDC has provided much of the U.S. Government’s support for Africa CDC, other arms of the U.S. government, such as the Department of Defense (primarily via the Defense Threat Reduction Agency, DTRA), have also provided technical and financial support (more information below in the Funding section).
With its long history of delivering technical support to health systems in Africa, U.S. CDC has supported Africa CDC in strengthening the public health workforce, with a particular focus on creating a network of trained epidemiologists capable of addressing outbreaks that cross national borders. This close working relationship has enabled Africa CDC to leverage U.S. CDC’s existing investments in the region’s laboratory capacity, disease surveillance, and response preparedness. Using a cooperative agreement with the African Field Epidemiology Network, U.S. CDC hired 10 graduates of the epidemiology program to work at Africa CDC in its early years.
In March 2022, the U.S. Government renewed its partnership with Africa CDC by entering into a new Memorandum of Understanding. The MOU outlines several priority areas for engagement, including building the capacity of national health institutes and regional collaborating centers, especially with regard to surveillance, public health information exchange, early outbreak warning systems, and development of testing and diagnostics capacity. Strengthening the public health workforce is also prioritized as an area of collaboration under the new MOU. The U.S. Government has also pledged to support the purchase and distribution of key health commodities, to advance next-generation molecular sequencing capacity, and to aid in expanding vaccine manufacturing capacity in Africa.
Funding of Africa CDC
Although Africa CDC was initially created as an arm of the AU, informants indicate that the AU has provided only minimal direct funding to the agency, although it has covered the salary costs for certain personnel. This has meant that external donors have, to date, been the primary source of funding for Africa CDC, with contributions to the organization surging during the COVID-19 pandemic.
The U.S. government has provided in-kind support to Africa CDC since 2015, with annual support ranging from approximately $1 million to about $3 million. Financial support from the U.S. government has come from the U.S. CDC, with some additional funding from DTRA. Early funding from the U.S. CDC helped in organizational strategic planning, the hiring of field epidemiologists, and the hiring of technical and administrative staff. In 2018, the U.S. Government announced an initial $150 million in support to national health institutes in Africa. In 2020, the U.S. CDC joined together with the Bill & Melinda Gates Foundation, Microsoft, Illumina, and Oxford Nanopore Technologies to launch a $100 million Africa Pathogen Genomics Initiative to improve disease surveillance and emergency response.
China is another key government donor to the Africa CDC (specific funding amounts are not publicly available), including support for the construction of the new Africa CDC headquarters building in Addis Ababa. China, sometimes in concert with the U.S. CDC, has also provided in-kind health workforce training, national regulatory capacity-building, and support for laboratory systems across the region. The U.S. and China have in the past formally collaborated in supporting Africa CDC, reflected in a Memorandum of Understanding signed in 2016.
Table 1: Selected Africa CDC Donor Funding Announcements Since 2020
Funder
Amount
Year
Purpose
Source
World Bank
$100 million
2022
Enhance technical capacity and strengthen Africa CDC’s institutional framework “to intensify support to African countries in preparing for, detecting, and responding to disease outbreaks and public health emergencies.”
Enable Africa CDC to “provide technical assistance and capacity building support in combating the COVID-19 pandemic and mitigating its impact in 37 African Development Fund eligible African Union Member States.”
To support Africa CDC’s work in emergency preparedness and response, the Africa CDC Health Economics Unit (HEU), improve COVID-19 vaccination coverage, and to build national and regional institutional capacity for addressing health challenges..
To help purchase COVID-19 vaccines, enable vaccine delivery and administration, develop a workforce to support continental vaccine manufacturing, and strengthen the Africa CDC.
For a four year partnership project to help “strengthen the capacity of Africa CDC to prepare for and respond to public health threats in Africa…facilitate harmonised surveillance and disease intelligence, and support the implementation of the public health workforce strategy”.
Four-year partnership to expand access to next-generation genomic sequencing tools and expertise designed to strengthen public health surveillance and laboratory networks across Africa.
NOTES: Not a complete list of grants; based on publicly available announcements of funding to and partnerships with Africa CDC made since 2020.
While a detailed budget is not available, a number of donors have provided funding to African CDC since the start of the pandemic to help with various aspects of COVID-19 response activities such as vaccine purchases and distribution, investments in public health workforce, laboratory strengthening, and a number of other areas (see Table 1). Major donors over this time period have included the MasterCard Foundation ($1.5 billion), the World Bank ($100 million), the Gates Foundation along with the US CDC and other partners ($100 million), the African Development Bank ($27.3 million), and the European Union (€10 million). Africa CDC has also leveraged other financial sources to advance its mission, such as using a financing facility established by the African Export-Import Bank to procure COVID-19 vaccines. Moving forward, Africa CDC is also a potential recipient of donor funds directed from the new Pandemic Fund housed at the World Bank, although it had as of February 2023, not been approved as one of the Fund’s “Implementing Entities” to which funds can be provided.
Africa CDC and its role in disease outbreaks, including COVID-19
Africa CDC plays prominent leadership and operational roles during outbreak response efforts on the African continent. For example, during the Ebola outbreak in the Democratic Republic of Congo (DRC) in 2018-2020, Africa CDC collaborated with the DRC government and WHO on contact tracing initiatives, laboratory services, and the training of thousands of healthcare workers and traditional healers – all in the context of a fragile security situation and under exacting political scrutiny.
The COVID-19 emergency accelerated the work of Africa CDC and raised its profile as a public health leader – regionally but also globally. With Africa CDC in place when COVID-19 emerged, the region was spared the need to invent mechanisms for collaboration and information-sharing in response to the pandemic.
Africa CDC helped catalyze an early, coordinated response to COVID-19. By February 2020, at a time when the U.S. Government was assuring Americans that COVID-19 posed little danger, Africa CDC spearheaded the creation of a joint continental strategy to respond to the pandemic, with 55 countries agreeing to harmonize their COVID-19 approaches and strategies. An Africa Task Force for Coronavirus (AFTCOR) was established in February 2020, meeting bi-weekly thereafter.
Africa CDC also served as a regional source of public health information on COVID-19, providing a central data hub for member-state reported data on cases, deaths, recoveries, tests and vaccination uptake, developing and disseminating issue briefs on important aspects of the COVID-19 pandemic and serving as a media information hub. It also tracked news and social media channels to identify and address vaccine-related disinformation and misinformation.
Africa’s laboratory capacity – a major focus of Africa CDC’s work prior to COVID-19 – has been cited as a key part of the COVID-19 response not only on the continent, supporting training of laboratory personnel, but also for providing early COVID data to the global community before other labs. Nigeria sequenced and broadly disseminated the first African SARS-CoV-2 genome, the Network for Genomic Surveillance South Africa discovered the Beta variant, and genome-sequencing efforts in Botswana and South Africa led to identification of the Omicron variant.
In addition, Africa CDC spearheaded the procurement of essential COVID-19 commodities for the continent. In the very early stages of the pandemic, when countries across the world were competing for personal protective equipment and ventilators, Africa CDC negotiated with regional airlines, whose planes were grounded at the time, to deliver scarce commodities to the region. In August 2020, Africa CDC joined with partners to establish the African Vaccine Acquisition Team (AVAT) to serve as a centralized purchasing agent for COVID-19 vaccines for the region. Through AVAT, the African Union made multiple purchases of COVID-19 vaccines for use across the region, including 110 million doses of the Moderna mRNA vaccine in 2021.
As the COVID-19 Vaccines Global Access (COVAX) initiative began delivering vaccines to African countries in 2021, Africa CDC helped countries in ensuring fair, equitable and timely allocation of vaccines. More recently, in 2022, it brokered an agreement with Pfizer for the purchase of the COVID-19 therapeutic Paxlovid.
Africa CDC also supported innovative means to deliver COVID-19 interventions and to address vaccine hesitation or misinformation. For example, Africa CDC launched the Partnership to Accelerate COVID-19 Testing in Africa (PACT), recruiting and training thousands of community health workers to provide community education and link people to COVID-19 testing and vaccination services and fielded a vaccine perception survey in 2020 to inform and guide vaccination campaigns.
Future Challenges and Opportunities for Africa CDC
It is an important moment of transition for Africa CDC as a new Director General takes the helm and the agency undergoes the process of becoming a fully autonomous organization after years of working within AU systems and oversight. Africa CDC has recently released its new strategic plan (for 2022-2026), which outlines the agency’s strategic objectives and goals as it looks ahead after helping to mount a continent-wide response to a historic pandemic.
Expert informants uniformly expressed admiration for the rapid progress that Africa CDC has made in building its capacity, elevating its profile, and influencing regional public health policies and practice. In particular, the Africa CDC has played a key role in raising the visibility of pandemic preparedness across the region and in marshalling high-level political support for public health measures. However, as indicated in the agency’s new strategic plan document and information provided by expert informants, a number of questions remain regarding how robustly staffed and supported certain functions of the Africa CDC are and how it can best fulfill the vision outlined in its founding charter. These include:
Mobilizing sufficient and sustainable financing: Donor funding has been central to establishing and growing the Africa CDC. However, Africa CDC’s reliance on external financing carries risks with respect to sustainability, and it could be facing more restricted funding in the coming years, as COVID-19 response activities wind down and societal and political attention on public health preparedness wanes. Some have called for increased contributions from AU member states – though it is unclear how willing and able governments across the region are to provide more for the agency over the coming years – as well other potential funding sources such as a continent-wide tax on airline tickets, an idea proposed by the incoming Africa CDC Director General.
Building capacity of key national and regional actors: Africa CDC is most able to be successful and implement its vision and strategy when it has strong partners and robust institutions at the national and regional levels, including effective national health systems. However, given the economic, societal, and budgetary effects of the pandemic and resulting constraints on public spending in many African countries, the investments and support for national and regional health institutions is uncertain in the coming years. In particular, informants pointed to the importance of building up stronger regional collaborating centers in partnership with Africa CDC, given that at present, the quality and capacity of these regional bodies varies considerably across the continent and some are still relatively nascent.
Maintaining hard-won goodwill and support: According to informants, Africa CDC has generated extraordinary goodwill across the region and in a relatively short time has become a remarkably influential public health institution. Many report that effective leadership helped build this reputation and expand influence, along with the impact of it work, it responsiveness, and success in communication. With a new leader taking the helm and the public health response in the region entering a new phase, informants advised that the agency will face challenges in building on its past successes and navigating the next phase. These include successfully leveraging the capacities and lessons derived from the COVID-19 response to continue to build robust regional pandemic preparedness, maintaining good relations with the AU and political leaders across the region, recruiting high-quality staff, implementing a code of conduct to govern its operations, and building the systems for follow through on Africa CDC’s autonomous status.
Strengthening transparency and accountability: The transparency of transnational mechanisms for global health and development is recognized as a growing global priority. While Africa CDC’s web portal provides a wealth of information on organizational activities, relevant news items, and some epidemiological information, the site does not make readily available details about other important aspects of the organization such as governance and funding. In fact, there is no public source to turn to for key Africa CDC organizational characteristics such as staff size, organizational charts, governing board minutes, budgets, and other areas. Similarly, while Africa CDC has articulated a number of goals and targets (such as providing 10 million COVID-19 tests in four months or recruiting and deploying 1 million community health workers for contact tracing), target and goal information remains limited and it is not clear whether stated goals have been met. Publicly available annual reports (through 2019) provide extensive information on outputs (e.g. number of laboratory professionals trained, strategic frameworks developed, public health staff deployed to address outbreaks) but less information on outcomes and impact. As it transitions to greater organizational autonomy, providing more accessible information about key aspects of its work could help diverse stakeholders understand and engage with the organization.
Navigating difficult political issues: In its early years, Africa CDC has understandably focused on core technical activities and fundamental public health capacity gaps, and its work on pandemic response has generally avoided being politicized or generated protests and pushback from member countries. However, this could change over time over time. For example, the U.S. CDC, a model for Africa CDC, has experienced numerous political controversies for its work on diverse public health matters such as adolescent health, gun violence, contraception, and COVID-19 measures, with U.S. states having varied rules and approaches to many of these issues. It is possible Africa CDC could similarly face complicated political issues linked to public health over which its member states have differing opinions and regulations. For example, as several African countries have taken steps to establish their own national vaccine manufacturing capacity, with the aim of avoiding a repeat of vaccine shortages that challenged the regional COVID-19 response, Africa CDC has cautioned countries to go more slowly, warning against the potential of a glut in vaccine capacity while other commodity priorities, such as diagnostics, are less prioritized. More broadly, Africa CDC’s commitment to support the establishment of robust vaccine manufacturing capacity and to ensure regional access to essential health commodities, for example, could touch on matters of considerable international political dispute. The recent appointment of the new Africa CDC Director General led to complaints about a lack of transparency and politicization from some African countries. Other public matters, such as the optimal strategy for preventing and controlling HIV and other sexually transmitted diseases, are often the source of political disagreements. Maintaining political support amid expanding ambitions could mean increasingly navigating politically difficult issues.
Clarifying and strengthening the relationship with WHO: Key informants observed that Africa CDC’s relationship with WHO’s Africa regional office (WHO AFRO) can be complicated, as the mandates of the two organizations have sometimes overlapped and it has not always been clear which has primary responsibility for certain activities or how their separate efforts integrate together. Informants indicated that over time, Africa CDC and WHO AFRO have developed a mostly productive working relationship that was bolstered during the COVID-19 response, with regular information sharing and coordination meetings held between the leaders of the two organizations over the course of the pandemic. Even so, Africa CDC and WHO AFRO differ in important ways, which has implications for their relationship going forward. While WHO is a global entity with regional representation via AFRO, Africa CDC is an African institution. While WHO works primarily at the level of Ministries of Health, Africa CDC derives authority through the AU from Heads of State. According to informants there is an opportunity for these two important institutions to strengthen their partnership and joint work going forward, though doing so will likely require communication and diplomacy on the part of leadership and continued attention to defining respective roles in order to avoid duplication and unnecessary friction.
Sustaining and further strengthening the partnership with the U.S. Government: The Biden Administration has indicated that it regards Africa CDC as a key partner, as reflected by the updated Memorandum of Understanding between the agency and the U.S. government. The U.S. has also made clear its commitment to building robust pandemic preparedness capacity in low- and middle-income countries, through advocacy for and early funding of the Pandemic Fund at the World Bank and by the establishment at the State Department of a Bureau of Global Health Security and Diplomacy, along with its ongoing financial and technical support to global health security programs including many efforts in the African region. This alignment of interests and priorities offers potential avenues for building on and further strengthening U.S. support for the work of Africa CDC.
This work was supported in part by the Hilton Foundation. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Josh Michaud is with KFF. Michael Isbell is an independent consultant.
In this JAMA Forum column, KFF’s Larry Levitt examines the growing role of private insurance companies in public programs, including Medicare Advantage and Medicaid managed care, and the tradeoffs that result.
With a divided Congress expected to weigh spending cuts during its debt ceiling and budget debates, the latest KFF Health Tracking Poll finds that the public has broad concerns about Medicare’s sustainability for the future but mostly views the debate about Medicare cuts as largely politics.
About eight in 10 (81%) adults – including similar shares of Democrats, independents and Republicans – say they worry Medicare will not be able to provide the same level of benefits in the future as it provides to seniors today. Many (73%) believe changes need to be made to Medicare to keep it going. At the same time, a large majority (79%) says the back-and-forth between Republicans and Democrats about Medicare cuts is more about both sides playing politics, while one in five (19%) say the debate reflects actual policy plans.
Overall, about eight in 10 adults (81%) view Medicare positively, including similarly large majorities of Democrats, independents and Republicans. Three in four (76%) also view the Medicaid program favorably, including two-thirds of Republicans (65%). Most (69%) say that Medicaid is working well for the low-income people it covers, including similar shares across partisans.About two thirds (66%) of the public say they have a connection to the Medicaid program, either because they have been covered through Medicaid or because they have a child, family member or close friend who has. Republicans with a personal connection to Medicaid are more likely than those who lack such a connection to view the program favorably (70% v. 55%).
In addition, most of the public view Medicaid primarily as a health insurance program (61%) rather than a welfare program (37%), though there are partisan differences. Most Democrats (79%) and independents (60%) view Medicaid primarily as health insurance, while Republicans are narrowly more likely to view it as a welfare program (54% v. 45%). Among Republicans, those with a personal connection to Medicaid mostly view it as health care (55%), while those without such a connection mostly view it as welfare (73%).
Other findings include:
Most of the public views the Affordable Care Act (ACA) favorably (62%), though with a big partisan divide. Most Republicans (70%) continue to hold unfavorable views of the law, while most Democrats (90%) have favorable views.
About two-thirds (65%) of people living in the 10 states that have not approved the ACA’s Medicaid expansion want their state to do so to cover more low-income uninsured residents.
METHODOLOGYDesigned and analyzed by public opinion researchers at KFF, the survey was conducted from March 14-23, 2023, online and by telephone among a nationally representative sample of 1,271 U.S. adults, in English and in Spanish. The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on other subgroups, the margin of sampling error may be higher.