Racial and Ethnic Disparities in Mental Health Care: Findings from the KFF Survey of Racism, Discrimination and Health
Key Takeaways
In the wake of the COVID-19 pandemic, 90% of U.S. adults say the country is facing a mental health crisis and many reported major impacts of severe mental health problems on their families, according to a KFF/CNN survey. Additionally, drug overdose deaths sharply increased amid the pandemic and suicide deaths rose. People of color have been disproportionately affected by the rises in drug overdose and suicide deaths. People of color also are more likely to report experiences of racism and discrimination, which are associated with worse mental health and well-being. Reports of any mental illness in the past year remain lower among Hispanic, Black, and Asian adults compared to White adults. However, mental illness among people of color may be underdiagnosed due to the lack of culturally sensitive screening tools, coupled with structural barriers to care, with previous research pointing to racial disparities in receipt of mental health services.
This brief examines disparities in mental health care by race and ethnicity and other factors based on data from the 2023 KFF Racism, Discrimination and Health Survey, a large, nationally representative survey based on responses from over 6,000 adults. The survey provides unique data on access to the health care system and how factors such as racism and discrimination impact these experiences and overall health and well-being. Key findings include:
Among adults who report fair or poor mental health, White adults (50%) are more likely to say they received mental health services in the past three years compared with Black (39%) and Hispanic adults (36%). Across racial and ethnic groups, about half of all adults (53%) who report that they received mental health services said they were very or extremely helpful.
Adults identify cost concerns and scheduling difficulties as primary barriers to mental health care, and Hispanic, Black, and Asian adults disproportionately report additional challenges, such as finding a provider who can understand their background and experiences, lack of information, or stigma or embarrassment. Among adults who received or tried to receive mental health care, Asian (55%), and Black (46%) adults are more likely to report difficulty finding a provider who could understand their background and experiences compared to their White counterparts (38%). Among those who thought they needed mental health care but did not try to find a provider, Hispanic adults are more likely than White adults to say the main reason was they didn’t know how to find a provider (24% vs. 11%) and/or that they were afraid or embarrassed to seek care (30% vs. 18%).
Adults who report unfair treatment or negative experiences with a provider are twice as likely as those without these experiences to say they went without needed mental health care. Four in ten (41%) adults who report they were treated unfairly or with disrespect by a health care provider and about one-third (35%) of adults who say they’ve had at least one negative experience with a health care provider say they did not get mental health services they thought they needed compared to smaller shares of those who do not report these experiences (18% and 15%, respectively).
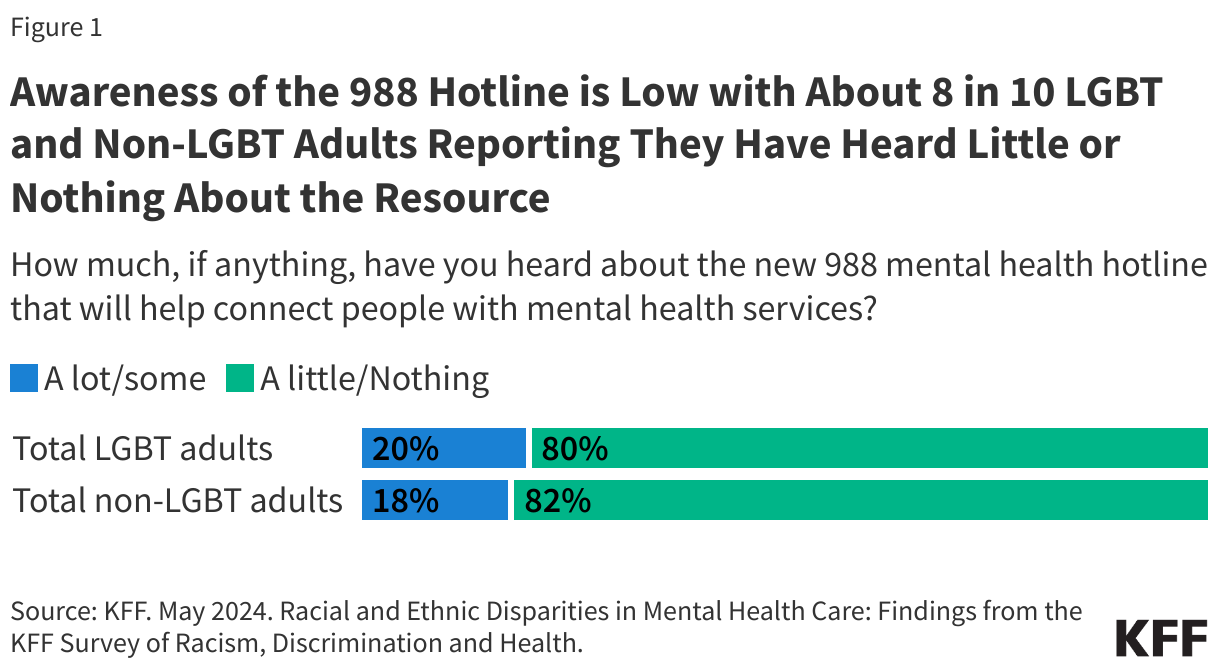
Reported awareness of the 9-8-8 mental health hotline remains low overall, particularly among Black, Hispanic, and Asian adults. As of Summer 2023, about one in five (18%) adults say they have heard a lot or some about 9-8-8, with Black (16%), Hispanic (11%), and Asian (13%) adults less likely to say they have heard about 9-8-8 than White adults (21%). At the same time, about one in five (21%) adults say they or a family member has ever experienced a severe mental health crisis that resulted in serious consequences such as homelessness, hospitalization, incarceration, self-harm, or suicide, with this share rising to 39% among young (ages 18-29) White adults.
Findings from the 2023 KFF Racism, Discrimination and Health Survey highlight barriers to mental health care, including costs and difficulties finding providers, with people of color citing additional challenges such as difficulty finding providers with shared background and experiences, lack of information, and stigma and embarrassment. These findings also point to areas of focus that may help address barriers to mental health care, such as diversifying the mental health care workforce and enhancing knowledge of culturally competent care among mental health care providers. Additionally, focused outreach and education efforts among specific communities may address awareness of mental health resources and stigma associated with mental health care. Findings from the 2023 KFF survey offer insight into the interactions of people of color with the mental health care system at a time when they are experiencing disproportionate increases in deaths by drug overdose and suicide and ongoing impacts of racism and discrimination.
Use of Mental Health Services
Receipt of mental health services varied across demographics and by insurance status leading up to the pandemic. As reported in KFF analyses, prior to the pandemic Black adults with moderate to severe symptoms of anxiety and/or depression were less likely than their White peers to receive mental health services. Similarly, among adults with moderate to severe symptoms of anxiety and/or depression, young adults, men, uninsured individuals, and individuals without a usual source of care were less likely than their respective counterparts to receive mental health services.
The 2023 KFF survey data show that about one quarter (23%) of adults say they have received mental health services from a doctor, counselor, or other mental health professional in the past three years. This share rises to 45% among those who report fair or poor mental health status, compared with about one in five (19%) of those who say they have good to excellent health.
Among adults who report fair or poor mental health, White adults (50%) are more likely to say they received mental health services in the past three years compared with Black (39%) and Hispanic adults (36%) (Figure 1). Additionally, among those who report fair or poor mental health status, U.S.-born adults (48%) are more likely than their immigrant counterparts (26%) to report receiving mental health services, and insured adults with fair or poor mental health status are more likely than those who are uninsured to say they received mental health services (48% vs. 27%).

About half of adults (53%) who report that they received mental health services said they were very or extremely helpful (Figure 2). The remaining 47% said they were somewhat, not too, or not at all helpful. Adults with self-reported fair or poor mental health status were less likely than those with better reported mental health status to say that the services they received were very or extremely helpful (41% vs. 59%), although this could reflect improved self-reported mental health status among those who found the services helpful.

Barriers to Accessing Mental Health Services
Prior research shows that many adults report unmet mental health needs and face barriers to accessing mental health services. Common barriers to accessing mental health care include costs, not knowing where to obtain care, limited provider options, and limited acceptance of insurance among providers. People of color face increased access barriers due to a range of factors, such as the lack of a diverse mental health care workforce, the absence of culturally informed treatment options, and stereotypes and discrimination associated with poor mental health.
Across racial and ethnic groups, about one in five adults say there was a time in the past three years when they thought they might need mental health services or medication but did not receive them. This share rises to about half (48%) among those with self-reported fair or poor mental health status, with about four in ten or more White (53%), Black (47%), and Hispanic (39%) adults who report fair or poor mental health saying they went without mental health services or medication that they thought they needed in the past three years (Figure 3).

Adults who report unfair treatment by or negative experiences with a health care provider are more likely to say they went without needed mental health care. As previously reported, Black, Hispanic, AIAN, and Asian adults report higher levels of unfair treatment when seeking health care than their White counterparts. Adults who say they were treated unfairly or with disrespect by a health care provider are more likely to report not getting mental health services they thought they needed compared to those who do not report unfair treatment (41% vs. 18%) (Figure 4), and this difference persists among those with self-reported fair or poor mental health status (67% vs. 40%). Similarly, adults who say they’ve had at least one negative experience with a health care provider, such as a provider assuming something about them without asking, suggesting they were personally to blame for a health problem, ignoring a direct request or question, or refusing to prescribe pain medication they thought they needed are more likely to report not getting mental health services they thought they needed compared to adults who did not report a negative experience (35%. vs 15%). This difference also persists among those with self-reported fair or poor mental health status (56% vs. 37%).

Among adults who say they needed but went without mental health services, about half (48%) say they tried to find a mental health care provider, while the remaining half (52%) say they did not. Additionally, seven in ten parents with children who they thought might need mental health services or medication but went without them in the past three years (or 14% of all parents) say they tried to find a provider for their child.
Adults who received or tried to find a mental health care provider for themselves or their children identified scheduling delays, difficulty finding a provider who could understand their background and experiences, and concerns about affordability or coverage as challenges. Overall, 32% of adults received mental health services or tried to find a mental health care provider for themselves or their children in the past three years. Among these adults, about four in ten say that it was very or somewhat difficult to find a mental health care provider who could treat them in a timely manner (44%), understand and relate to their background and experiences (41%), or who they could afford (41%), and 36% say it was very or somewhat difficult to find one who would take their insurance. Compared to their White counterparts (38%), Asian (55%), and Black (46%) adults are more likely to report difficulty finding a provider who could understand their background and experiences (Figure 5).

Concerns about costs and scheduling difficulties are primary reasons cited for not trying to find a mental health care provider among those who say they needed mental health care. A total of 12% of adults thought they or their children needed mental health services in the past three years but report they did not try to find a provider. Among these adults, the main reasons they say they did not try to find a provider were because they thought it would be too expensive (37%), they were too busy or could not take the time off (31%), or they didn’t think it would help (29%). Somewhat smaller shares say they were afraid or embarrassed to seek care (21%), did not know how to find a provider (15%), or did not think they could find a provider with a shared background or experiences (14%) (Figure 6). Hispanic adults who thought they or their children needed mental health services but did not try to find a provider are more likely than their White peers to say the main reason was because they didn’t know how to find a provider (24% vs. 11%) or that they were afraid or embarrassed to seek care (30% vs. 18%). Black adults who thought they or their children needed mental health services but did not try to find a provider are more likely than their White peers to say the main reason was because they didn’t think they would find one who shared their background and experiences (21% vs. 10%).

Mental Health Crises and Awareness of 9-8-8 Mental Health Hotline
Since the launch of the federally mandated crisis number, 9-8-8, awareness remains low overall, particularly among Black, Hispanic, and Asian adults. In July 2022, 9-8-8 became available to all landline and cell phone users, providing a single three-digit number to access a network of over 200 local and state funded crisis centers where those in need may receive crisis counseling, resources and referrals. While national answer rates increased alongside increases in call volume after the implementation of 9-8-8, awareness of the hotline remains low overall. As of Summer 2023, about one in five (18%) adults say they have heard a lot or some about 9-8-8, with Black (16%), Hispanic (11%), and Asian (13%) adults less likely to say they have heard about 9-8-8 than White adults (21%) (Figure 7). Immigrant adults and adults with limited English proficiency also are less likely to say they have heard about 9-8-8 compared to those who are U.S.-born and English proficient.

Low awareness of the 9-8-8 hotline comes at a time when about one in five adults (21%) say they or a family member ever experienced a severe mental health crisis that resulted in serious consequences such as homelessness, hospitalization, incarceration, self-harm, or suicide (Figure 8). White adults (24%) are more likely to report having had or having a family member who has had a severe mental health crisis compared to Asian (9%), Hispanic (16%), and Black adults (18%), a difference that is largely driven by higher rates among White adults who are younger and have lower incomes. Younger adults (ages 18-29) are more likely to say they or a family member who experienced a severe mental crisis resulted in one of these consequences across racial and ethnic groups, with this share rising to about four in ten young White adults (39%). Similarly, among lower income adults ($40,000 annually or less), about a third (34%) of White adults report this experience compared with lower shares of Hispanic (18%), Black (19%), and Asian (11%) adults.