KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Poll: Large Majorities, Including Republicans, Oppose Discrimination Against Lesbian, Gay, Bisexual and Transgender People by Employers and Health Care Providers
Half Say Society Hasn’t Gone Far Enough in Accepting Transgender People
Large majorities of Americans think it should be illegal for either employers or health care providers to discriminate against people because they are lesbian, gay or bisexual, or transgender, a new KFF poll finds. This includes large majorities of Republicans, independents and Democrats across a range of questions about such discrimination.
The poll gauges the public’s views following two major developments this month that move in opposite directions on LGBTQ protections. First, the Trump administration finalized regulations removing protections based on sexual orientation and gender identity (including transgender status) in health care, arguing that the definition of sex does not extend to either. Then last week the U.S. Supreme Court ruled that gender identity and sexual orientation are protected under the definition of sex discrimination in the workplace.
The poll finds:
9 in 10 in ten adults agree with last week’s Supreme Court ruling, say it should be illegal for employers to fire or refuse to hire people because they are lesbian, gay, or bisexual (90%) or transgender (89%).
About 9 in 10 say it should be illegal for doctors or other health care providers to refuse to treat people because they are lesbian, gay, or bisexual (89%) or transgender (88%).
85% say it should be illegal for health insurance companies to refuse to pay for health care services for people who are transgender.
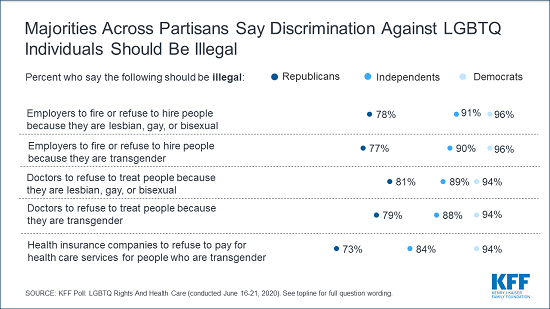
In each case, large majorities across partisan lines, including more than 7 in 10 Republicans, think such discrimination against LGBTQ people should be illegal.
Overall, nearly 7 in 10 adults say they support laws that ban discrimination based on whether a person is lesbian, gay, or bisexual (69%) or transgender (68%). This is similar to the share who support laws that ban discrimination based on race or ethnicity (71%) and only slightly smaller than the share who support laws banning discrimination against people with a disability (76%).
“Most Americans – including most Republicans — oppose discrimination against people who are lesbian, gay, bisexual, or transgender,” KFF President and CEO Drew Altman said. “The public is shifting more quickly on these issues than the political and legal landscapes are.”
Other findings include:
Most adults say that people who are transgender (79%) or are lesbian, gay or bisexual (74%) face at least some discrimination in the U.S. today. This is similar to the share who say the same about Black (84%) and Hispanic (77%) people. While still a majority, a smaller share of Republicans say each of these groups face at least some discrimination.
Half (49%) of the public says our society has “not gone far enough in accepting people who are transgender,” up 10 percentage points from a 2017 Pew Research Center Poll. In comparison, relatively few (15%) today say our society has “gone too far” in accepting people who are transgender, and a third (32%) say it “has been about right.” A similar share of Republicans say society has gone too far (30%) as say it has not gone far enough (24%).
More than a third of adults (36%) say they personally know someone who is transgender, including nearly half (46%) of those under age 30.
Designed and analyzed by public opinion researchers at KFF, the poll was conducted June 16-21 among a nationally representative random digit dial telephone sample of 1,001 adults using the SSRS Omnibus Poll. Interviews were conducted in English and Spanish by landline (263) and cell phone (738). The margin of sampling error is plus or minus 4 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
The Trump administration has taken several steps to roll back protections for LGBTQ people, including in health care. Most recently, on June 12th, the administration released a final rule on Section 1557 of the Affordable Care Act and other health regulations, removing protections based on sexual orientation and gender identity (including transgender status) in health care, arguing that the definition of sex does not extend to either. As a result of this rule, for example, health care insurers and providers could refuse to cover or treat someone who is transgender. Just three days later, however, the U.S. Supreme Court issued a landmark 6-3 decision, concluding that gender identity and sexual orientation are protected under the definition of sex discrimination in the workplace. While the Supreme Court decision pertains to employment and not health care, it likely has significant implications for the HHS rule. On June 22, 2020, a lawsuit was filed by several organizations using the Supreme Court decision to challenge the constitutionality of the Trump administration’s Section 1557 rule.
It is unclear if the Trump administration will move forward with the rule in light of the Supreme Court decision. If implemented, the rule would have significant implications for LGBTQ people, a population already facing challenges in accessing health care services. The latest KFF poll finds the rule is also at odds with public opinion. The poll, conducted among 1,001 U.S. adults immediately following the Supreme Court decision (June 16th–21st), finds a majority of the public supporting laws that ban discrimination based on whether a person is lesbian, gay, bisexual, or transgender and think it should be illegal for health care providers and health insurance companies to deny care for such individuals.
Partisans differ in whether society has gone too far or not far enough in accepting people who are transgender and in their views on how much discrimination LGBTQ individuals face. But majorities of Democrats, independents, and Republicans say they support laws banning discrimination based on whether a person is lesbian, gay, or bisexual (78%, 66%, and 62%) or transgender (77%, 63%, and 62%). In addition, more than eight in ten Democrats, independents, and Republicans say it should be illegal for doctors or other health care providers to refuse to treat people because they are lesbian, gay, bisexual, or transgender. Majorities (94% of Democrats, 84% of independents, and 73% of Republicans) also say it should be illegal for health insurance companies to refuse to pay for health care services for people who are transgender.
Half Say U.S. Hasn’t Gone Far Enough In Acceptance Of People who are Transgender
Half (49%) of U.S. adults say our society has “not gone far enough in accepting people who are transgender,” more than three times as many who say our society has “gone too far in accepting people who are transgender” (15%). About one-third (32%) say our society “has been about right” in accepting transgender individuals. This may mark a shift in attitudes in recent years with a larger share of individuals now saying society hasn’t gone far enough in accepting transgender people (up 10 percentage points from a 2017 Pew Research Center poll).
Figure 1: About Half Say Society Has Not Gone Far Enough In Accepting People Who Are Transgender
Attitudes about whether society has gone too far or not far enough in accepting people who are transgender are largely partisan, similar to where they were three years ago. Two-thirds of Democrats (65%) and half of independents say society has “not gone far enough”. One-fourth of Republicans (24%) agree while four in ten (42%) Republicans say society’s acceptance of transgender individuals “has been about right.” Three in ten Republicans say society has “gone too far” in its acceptance, compared to 14% of independents and 8% of Democrats.
While previous research has found generational differences in views towards transgender individuals, the latest KFF poll finds about half of adults – across all age groups – say society has “not gone far enough” in its acceptance of people who are transgender, as do six in ten people (60%) who say they personally know someone who is transgender (36% of total).
Figure 2: Partisans Divided In Whether Society Has Gone Too Far Or Not Far Enough Towards Accepting People Who Are Transgender
Do You Know Someone Who Is Transgender? Nearly Half Of 18–29 year olds Say They Do
More than one-third of U.S. adults (36%) say they personally know someone who is transgender. While substantial shares across racial groups (34% of white, non-Hispanic adults and 40% of non-white adults) and partisanship (29% of Republicans, 36% of Democrats, and 39% of independents) say they personally know someone, including themselves, who is transgender, there are large differences across age groups. Nearly half of 18-29 year olds (46%) and four in ten (41%) 30–44 year olds who say they know someone who is transgender compared to three in ten 45–64 year olds and 27% of adults 65 and older.
Majorities Say LGBTQ Individuals Face Discrimination
A majority of U.S. adults say transgender people (79%) and lesbian, gay, and bisexual people (74%) face at least some discrimination in the U.S. today. This is somewhat similar to the shares of the public who say there is at least some discrimination against Hispanic (77%) and Black people (84%) and considerably more than the share who say the same about white people (28%). Notably, nearly half (45%) of U.S. adults say there is “a lot” of discrimination against transgender individuals in society today, compared to 53% who say the same about Black individuals.
Figure 3: Large Shares Say Black, Transgender, Hispanic, And LGBTQ Individuals Face At Least Some Discrimination In the U.S.
A smaller share, but still a majority of Republicans, say there is at least some discrimination against Black people (72%), Hispanic people (59%), and people who are lesbian, gay, or bisexual (61%) or who are transgender (67%).
Table 1. Smaller Shares Of Republicans Say There Is At Least Some Discrimination Against Certain Groups
Percent who say there is at least some discrimination against the following groups in the U.S. today:
Democrats
Independents
Republicans
Black people
93%
83%
72%
People who are transgender
87
79
67
Hispanic people
89
76
59
People who are lesbian, gay, or bisexual
85
72
61
White people
17
34
37
Majorities Support Policies banning discrimination Against LGBTQ Individuals
A majority of the public think LGBTQ individuals should be protected from discrimination and support laws protecting them at about the same rate as they support laws protecting people who are discriminated against because of their race or ethnicity or because they have a disability.
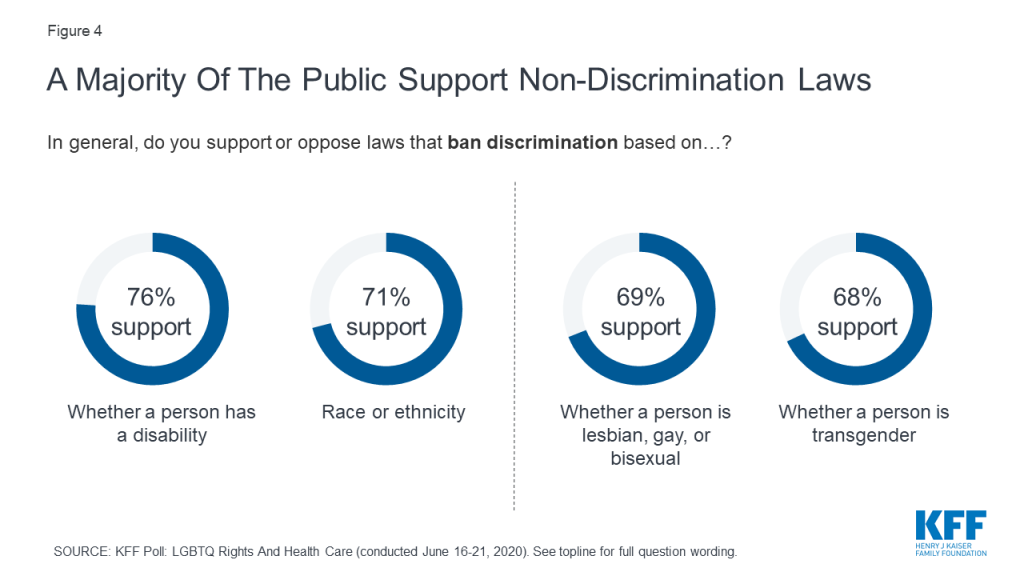
Nearly seven in ten individuals say they support laws that ban discrimination based on whether a person is lesbian, gay, or bisexual (69%) or transgender (68%). This is similar to the share who support laws that ban discrimination based on race or ethnicity (71%) and only slightly smaller than the share who support laws banning discrimination against people with a disability (76%).
Figure 4: A Majority Of The Public Support Non-Discrimination Laws
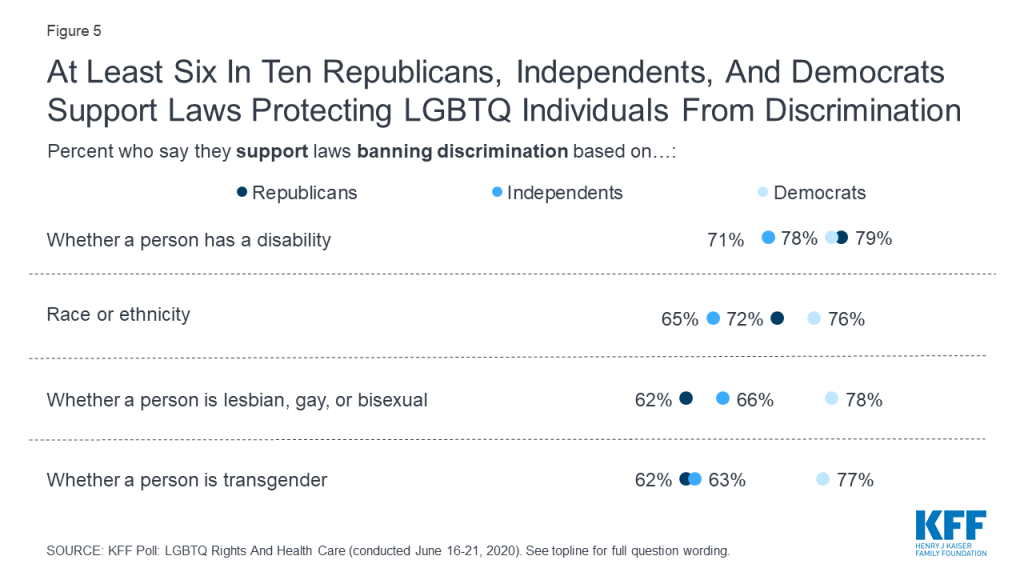
Laws protecting LGBTQ individuals from discrimination are supported by a majority of Democrats, independents, and Republicans, with at least six in ten across partisan groups saying they support laws banning discrimination based on whether a person is lesbian, gay or bisexual (78%, 66%, and 62%, respectively) or transgender (77%, 63%, and 62%, respectively).
Figure 5: At Least Six In Ten Republicans, Independents, And Democrats Support Laws Protecting LGBTQ Individuals From Discrimination
Large Majorities Think It Should Be Illegal For Employers and Health Care Providers To Discriminate Against LGBTQ People
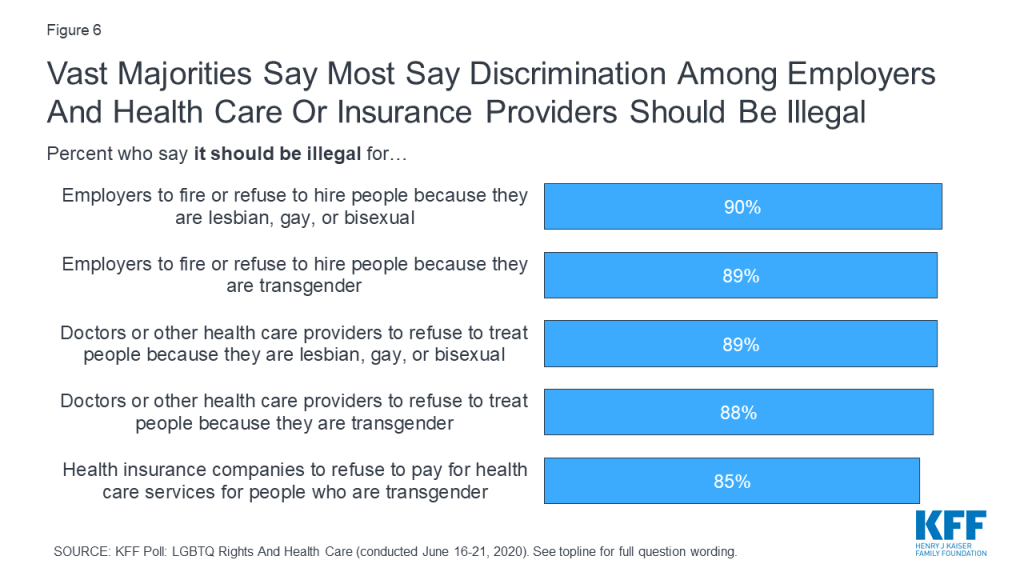
The vast majority of the public say it should be illegal for employers and health care providers to discriminate against people because they are lesbian, gay, bisexual or transgender. Nine in ten adults agree with last week’s Supreme Court ruling and say it should be illegal for employers to fire or refuse to hire people because they are lesbian, gay, or bisexual (90%) or transgender (89%). A large majority also say it should be illegal for doctors or other health care providers to refuse to treat people because they are lesbian, gay, or bisexual (89%) or transgender (88%). Eighty-five percent say it should be illegal for health insurance companies to refuse to pay for health care services for people who are transgender.
Figure 6: Vast Majorities Say Most Say Discrimination Among Employers And Health Care Or Insurance Providers Should Be Illegal
Majorities across partisanship say it should be illegal for employers, doctors and health care providers, and health insurance companies to be able to treat employees or patients differently because they are lesbian, gay, bisexual, or transgender.
Table 2: Majorities Across Partisans Say Discrimination Against LGBTQ Individuals Should Be Illegal
Should it be legal or illegal for…
Democrats
Independents
Republicans
…employers to fire or refuse to hire people because they are lesbian, gay, or bisexual
Legal
4%
7%
19%
Illegal
96
91
78
… employers to fire or refuse to hire people because they are transgender
Legal
4
8
18
Illegal
96
90
77
…doctors or other health care providers to refuse to treat people because they are lesbian, gay, or bisexual
Legal
5
9
17
Illegal
94
89
81
… doctors or other health care providers to refuse to treat people because they are transgender
Legal
6
10
18
Illegal
94
88
79
… health insurance companies to refuse to pay for health care services for people who are transgender
Legal
5
13
24
Illegal
94
84
73
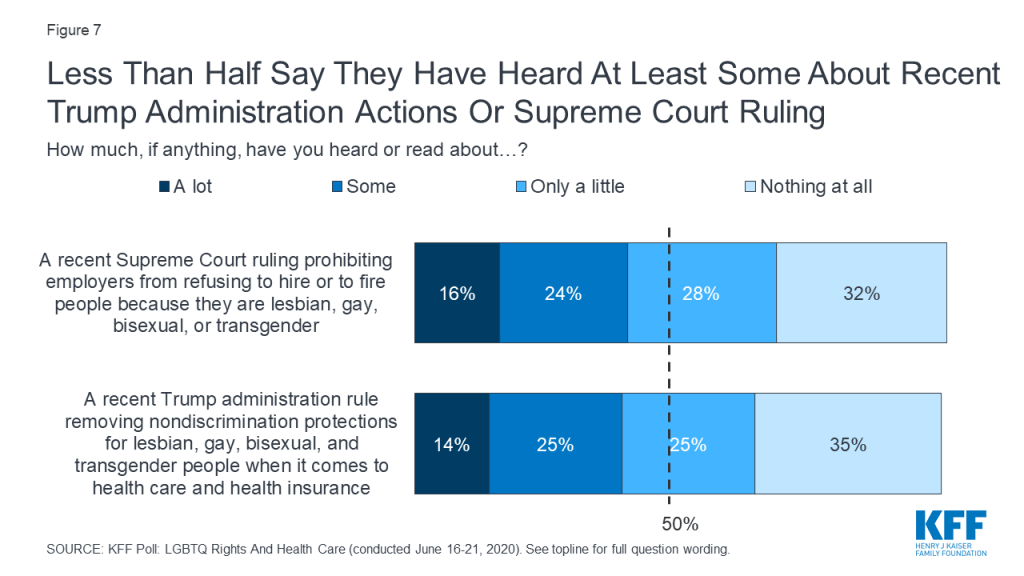
Despite the wide-reaching consequences of both of these actions, less than half of the public say they have heard at least some about either the recent Supreme Court ruling or the Trump administration rule. In fact, about one-third of U.S. adults say they have heard “nothing at all” about either the Supreme Court case prohibiting employment discrimination against LGBTQ individuals (32%) or the Trump administration actions removing protections for LGBTQ individuals when it comes to health care (35%).
Figure 7: Less Than Half Say They Have Heard At Least Some About Recent Trump Administration Actions Or Supreme Court Ruling
A smaller share of Republicans than Democrats say they have heard or read at least something about either the Supreme Court case (29% compared to 48%) or the Trump administration’s rule on LGBTQ access to health care (32% and 49%, respectively).
Methodology
This KFF LGBTQ Rights And Health Care Poll was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted June 16th to 21st, 2020 on the SSRS Omnibus Survey, among a nationally representative random digit dial telephone sample of 1,001 adults ages 18 and older, living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). Computer-assisted telephone interviews conducted by landline (263) and cell phone (738, including 504 who had no landline telephone) were carried out in English and Spanish by SSRS of Glen Mills, PA. Both the random digit dial landline and cell phone samples were provided by Marketing Systems Group (MSG). For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey, staff time was supported in part by the Elton John AIDS Foundation.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s March 2019 Current Population Survey (CPS) on sex, age, education, race, Hispanic origin, and region along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the July-December 2019 National Health Interview Survey. The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample, and design modifications, namely, the oversampling of prepaid cell phones and likelihood of non-response for the re-contacted sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 4 percentage points. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
To increase health care accessibility and limit risk of exposure during the COVID-19 pandemic, all fifty states and DC are expanding telehealth access for Medicaid beneficiaries. This issue brief highlights recently released federal guidance to assist Medicaid programs in developing telehealth policies in response to the COVID-19, discusses trends in state Medicaid activity to expand coverage and access to telehealth, and highlights state and federal activity support provider infrastructure and patient access to telehealth.
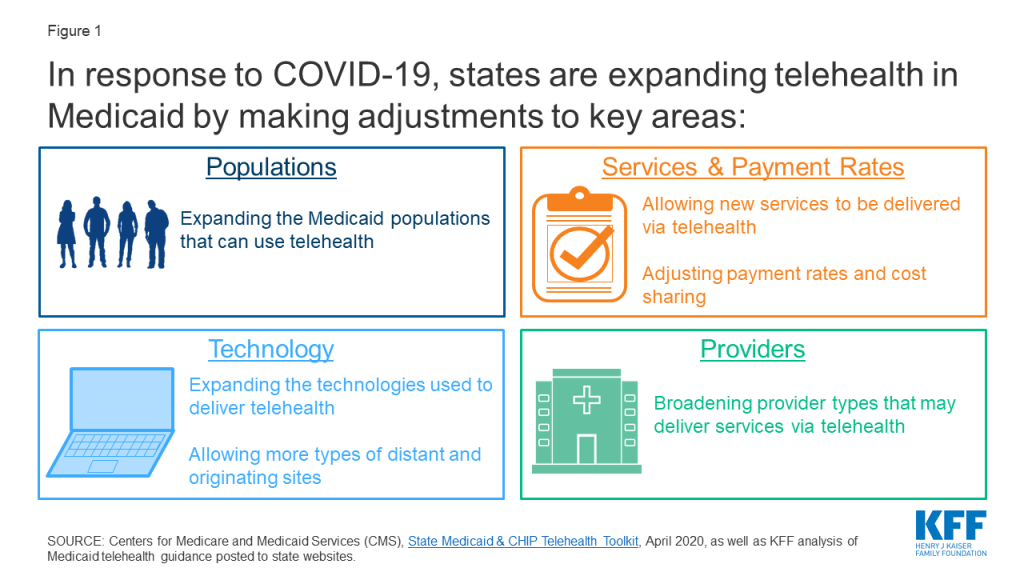
States have broad flexibility to determine whether and how to cover services delivered via telehealth in their Medicaid programs. Although states may apply to CMS for Medicaid emergency authorities (including Section 1135 waivers, Section 1915 (c) Appendix K strategies, and Disaster Relief SPAs), states can also take a wide range of additional actions to expand access to telehealth that do not require CMS approval. CMS has identified populations, services and payment rates, providers, technology, and managed care as key areas of telehealth for state consideration.
States are expanding telehealth access broadly and for specific services. States are waiving restrictions on distant and originating sites, modalities, and provider-patient relationships to better enable the use of telehealth. States are also issuing guidance focused on expanded telehealth access for specific services, including behavioral health; pediatric services; reproductive and maternal health services; services for beneficiaries with COVID-19; dentistry services; and speech therapy, physical therapy, and occupational therapy. Most of these Medicaid telehealth policy changes will expire with the end of the public health emergency, although states may opt to make some changes permanent.
States and the federal government are taking additional actions to increase provider and patient access to technologies required for telehealth. Medicaid beneficiaries face particular barriers to telehealth technology including internet service, and providers may also lack the necessary infrastructure. Federal financial support and state outreach efforts are facilitating increased access to these telehealth resources for Medicaid providers and patients.
Figure 1: In response to COVID-19, states are expanding telehealth in Medicaid by making adjustments to key areas:
Introduction
Telehealth can help limit risk of coronavirus exposure during the COVID-19 pandemic, and is important both for those who are unable to physically go to the doctor and more broadly when in-person visits are inadvisable. Telehealth can enable remote screening for those with COVID-19 symptoms, while patients with other health concerns can use telehealth to avoid potential viral exposure at health care facilities.
There are few federal requirements, or restrictions, involving coverage of telehealth in the Medicaid program.1 The federal Medicaid statute does not define telehealth as a specific service and CMS, prior to the COVID-19 pandemic, had issued little guidance on state use of telehealth. States have broad flexibility to determine whether to cover telehealth, which services to cover, geographic regions telehealth may be used, and how to reimburse providers for these services (including whether to require payment parity for services delivered via telehealth as compared to face-to-face services). If a state reimburses for services delivered via telehealth in the same way/amount that it pays for face-to-face visits, the state is not required to submit a separate state plan amendment (SPA) for coverage or reimbursement of these services.2 Telehealth coverage policies may differ between fee-for-service (FFS) Medicaid and Medicaid managed care. Although there are few federal Medicaid requirements involving the coverage of telehealth, Medicaid programs must follow other applicable federal and state laws and regulations including those related to patient privacy (e.g., HIPAA), prescribing, provider licensing, and scope of practice.
Prior to the COVID-19 pandemic, the use of telehealth in Medicaid was becoming more common, particularly to address barriers to care including insufficient provider supply (especially specialists), transportation barriers, rural access challenges,3 and stigma associated with receiving behavioral health care.4 All states had some form of Medicaid coverage for services delivered via telehealth, but reimbursement and regulation policies varied widely. As of February 2020, Medicaid programs in all fifty states and Washington, DC reimbursed some type of live video telehealth service delivery in FFS Medicaid programs; however, the scope of this coverage was inconsistent across states and many included restrictions on the type of services, providers, and originating sites. Most states prohibited or had no guidelines for audio-only telephone services. Fewer than half of states allowed the patient’s home to serve as the originating site, meaning that patients could access services via telehealth from their homes.5
This brief highlights recently released federal guidance to assist Medicaid programs in developing telehealth policies in response to the COVID-19, discusses trends in state Medicaid activity to expand coverage and access to telehealth, and highlights state and federal activity to support provider capacity to implement telehealth service delivery as well as strategies and activities to ensure patient access to these services. (Also see KFF’s Opportunity and Barriers for Telemedicine in the U.S. During the COVID-19 Emergency and Beyond.)
State Actions to Expand Medicaid Telehealth Coverage and Access
The Centers for Medicare and Medicaid Services (CMS) has released a COVID-19 FAQ document (last updated May 5, 2020) which notes the broad flexibility states have to cover telehealth through Medicaid and addresses flexibilities for telehealth payment rates, reporting, and managed care organizations (MCOs), among others. To further guide states in establishing new telehealth policies to increase access during the pandemic, CMS released a State Medicaid & CHIP Telehealth Toolkit on April 23, 2020. The toolkit identifies key areas of telehealth for state consideration:
Populations: Which Medicaid populations can receive services via telehealth? Do patients need to have an existing patient-provider relationship to receive services via telehealth?
Services and Payment Rates: Which services can be delivered via telehealth and how will these services be reimbursed? Are services delivered via telehealth subject to cost sharing requirements?
Providers: What types of providers can deliver services via telehealth and is any training required? Are any changes to licensing requirements or scopes of practice warranted?
Technology: What telehealth modalities (e.g. videoconference, audio-only phone) can be used to deliver services and what privacy laws need to be considered? What kinds of sites can serve as distant sites (provider location) and originating sites (patient location)?
Managed Care: Are managed care plans required to cover all services delivered via telehealth that are available in FFS Medicaid? Are cost sharing requirements different under managed care plans? Do managed care contracts need to be amended to extend the same flexibilities authorized under state plan, waiver (i.e., 1915(b) or 1915(c)), or demonstration (i.e., Section 1115)?6 Do managed care contracts need to be amended to reflect utilization of telehealth?
As referenced in the toolkit, states can broaden access to telehealth using Medicaid emergency authorities, which require CMS approval. As of June 15, 2020, 51 states (including DC) are using Section 1135 waivers to allow out-of-state providers with equivalent licensing in another state to provide care to Medicaid enrollees. Twelve states (including DC) are using Disaster-Relief SPAs to authorize telehealth payment variation and/or to include ancillary telehealth delivery costs. States are also using Section 1915 (c) Waiver Appendix K strategies to amend home and community-based services (HCBS) to broaden access to telehealth: 47 states (including DC) are permitting virtual eligibility assessments and service planning meetings and 44 states (including DC) are allowing electronic service delivery.
States have broad authority to take additional steps to expand coverage and access to services delivered via telehealth that may not require CMS approval, including modifications to Medicaid FFS policies and to MCO requirements. Most Medicaid telehealth policy changes made in response to COVID-19 will expire with the end of the public health emergency, although states may choose to make some changes permanent. As of June 15, 2020, 49 states (including DC) have issued specific guidance to expand coverage and access to telehealth in response to the pandemic. For example:7
States are expanding the Medicaid populations that can utilize telehealth. At least 11 states are waiving the requirement that provider-patient relationships be established in-person prior to the use of telehealth.
States are newly allowing certain services to be delivered via telehealth and are adjusting provider reimbursement rates and patient cost-sharing. At least 39 states (including DC) have established payment parity for at least some services delivered via telehealth as compared to face-to-face services. At least 20 states are waiving or lowering telehealth copayments (note that some states did not charge cost-sharing for any or all services prior to the pandemic). States are also making it easier to obtain patient consent for telehealth: for example, at least 4 states that previously required written consent are newly allowing verbal consent only.
States are broadening the provider types that may provide services via telehealth, including adding new providers and waiving licensing requirements. At least 11 states are allowing federally qualified health centers (FQHCs) and/or rural health clinics (RHCs) to provide services via telehealth. Given that Medicaid patients comprise a significant portion of these clinics’ patient populations, these rule changes could significantly impact the reach of telehealth under Medicaid.
States are expanding the technologies allowed for telehealth service delivery and the originating sites at which patients can receive services via telehealth. At least 26 states (including DC) are allowing the patient’s home to serve as the originating site. States are also expanding the modalities by which services can be delivered via telehealth. For example, at least 38 states are allowing some or all services to be provided via audio-only telephone communications.
In addition to the steps noted above, states are also issuing guidance to broaden telehealth access for specific services, including:
Behavioral health: Many states have issued guidance for behavioral health providers and are expanding telehealth access to behavioral health services, such as diagnostic evaluations, psychotherapy and medication-assisted treatment (MAT). Some states are broadening the practitioner/provider types that may provide behavioral health services via telehealth. States may impose different requirements on different behavioral health services. At least 41 states are allowing telehealth delivery of behavioral health services.8 Examples include the following:
Pennsylvania is newly allowing any practitioners who provide necessary behavioral health services to utilize telehealth. This change and other telehealth extensions in the state apply to behavioral health services delivered to Medicaid beneficiaries via FFS or through Behavioral Health MCOs.
Unlike many states that exclude all or most residential treatment services from those available via telehealth, Maryland is allowing substance use disorder (SUD) residential treatment programs to provide Medicaid services via telehealth until the end of the COVID-19 emergency.
Connecticut is requiring that enrollees be at Medicaid-enrolled originating sites to receive certain behavioral health services via telehealth (including psychiatric diagnostic evaluations and opioid treatment programs) but places no limitations on the originating site for telehealth delivery of individual therapy, family therapy, and psychotherapy with medication management.
Pediatric services: States are allowing the use of telehealth for Medicaid-funded well-child visits and services and are more likely to do so for children older than 24 months, in accordance with guidance from the American Academy of Pediatrics. At least 13 states have issued guidance for telehealth well-child and EPSDT visits.9
States such as Maine, North Carolina, and Rhode Island are allowing telehealth well-child visits delivered via FFS and/or through MCOs and require follow-up in-person visits as soon as possible. Kentucky requires the in-person follow-up visit to occur within 6 months of the end of the declared emergency.
States may newly allow other pediatric services to be delivered via telehealth—for example, Colorado has added pediatric behavioral therapy services to its list of eligible services to be delivered via telehealth.
Reproductive and maternal health services: Expanded access to telehealth service delivery in most states includes family planning services. States with extended Medicaid eligibility programs for family planning services may allow telehealth for these enrollees as well. For example,
North Carolina is allowing both traditional Medicaid beneficiaries and beneficiaries of its family planning Medicaid program to receive select family planning services via telehealth.
Alaska is newly allowing direct entry midwives to provide some services using telehealth.
Services for beneficiaries with COVID-19: States are issuing guidance to ensure that Medicaid beneficiaries with confirmed or suspected COVID-19 can receive services via telehealth. Examples include:
Louisiana and Nebraska have added reimbursement for telephonic evaluation and management services for Medicaid beneficiaries (including those covered by FFS and MCOs) actively experiencing symptoms of COVID-19.
Massachusetts has added a billing code for COVID-19 remote patient monitoring (RPM) for Medicaid beneficiaries with confirmed or suspected COVID-19 who are isolated at home or in a community-based setting. RPM is the electronic transmission of patient health data from the originating site to a provider at a distant site for assessment. Separate guidance clarifies that all Medicaid health plans in Massachusetts (including MCOs) are required to cover the new COVID-19 RPM bundle of services.
Dentistry services: Many states are expanding teledentistry in Medicaid, but often require these services to be provided using video technology and exclude audio-only delivery.
Maryland and Ohio are allowing dentists to utilize telehealth to provide limited problem-focused oral evaluations.
Kentucky is allowing for screenings, assessments, and examinations to be provided via teledentistry.
Speech therapy, physical therapy, and occupational therapy: At least 32 states cover telehealth delivery of speech therapy, physical therapy, and occupational therapy services.10 For example:
Missouri and Ohio have issued guidance on procedure codes for telehealth delivery of services that provide speech therapy, physical therapy, and occupational therapy. In both states, providers may use these codes to bill services provided to beneficiaries covered by FFS and MCOs.
Many state directives and guidance expanding telehealth in Medicaid apply to all delivery systems including managed care organizations (MCOs), although there is some variation. For example, Massachusetts requires that managed care entities provide all Medicaid services and provider flexibilities at the same level and rate as the state’s fee-for-service FFS program during the COVID-19 emergency. On the other hand, Florida acknowledges that its MCOs have broad flexibility to cover services delivered via telehealth and set their own requirements and rates, and the state’s telehealth policy applies only to its FFS delivery system. Florida is separately encouraging MCO plans to maximize the use of telehealth.
Activity to Support Provider Infrastructure and Patient Access to Telehealth in Medicaid
Both states and the federal government are taking action to support provider provision of telehealth broadly and Medicaid. Telehealth requires technology and internet access from both patients and providers that may not already be in place. The Coronavirus Aid, Relief, and Economic Security (CARES) Act appropriated $29 million annually for five years to the Telehealth Network Grant Program to fund telehealth technologies for nonprofit entities that provide direct services to rural and medically underserved areas. The Act also included $200 million for the Federal Communications Commission (FCC) that will fund the COVID-19 Telehealth Program, which provides financial support to nonprofit and public eligible health care providers for telecommunications services, information services, and devices necessary to provide critical connected care services. Although this program is not exclusive to Medicaid providers, the FCC has noted that funding decisions will take into account whether providers serve low-income patient populations and plan to target funding to high-risk and vulnerable patients. States can take additional action to facilitate provider use of telehealth. For example, providers in Washington can receive Zoom video conference licenses free of charge, with priority given to providers who serve a meaningful number of Medicaid clients.
States and the federal government are also increasing accessibility of telehealth for patients. Medicaid beneficiaries face particular barriers to accessing services via telehealth: in 2017, 26% of nonelderly, non-SSI, non-dual eligible Medicaid adults reported that they never use a computer and 25% reported that they do not use the internet. Further, adults in rural areas—which, as reported by the FCC, are significantly more likely to lack sufficient access to broadband internet—are also more likely to be covered by Medicaid than those in urban and other areas, with 24% of rural adults covered by Medicaid in 2015. To facilitate patient access to phone and internet services necessary for telehealth during the pandemic, the FCC has relaxed certain recertification, eligibility, and enrollment requirements for Lifeline, a federal program that provides subsidized phone and/or internet service to low-income households (enrollment in Medicaid, among other programs, makes one eligible for the program). States including Massachusetts and New York have issued resources to provide Medicaid beneficiaries with information about options for accessing technology required for telehealth. To further make telehealth more accessible to enrollees, the Office of Inspector General (OIG) has notified providers that they may reduce or waive cost-sharing obligations beneficiaries owe for services delivered via telehealth without being subject to OIG administrative sanctions. As of June 15, 2020, 18 states are broadly waiving cost sharing charges in their Medicaid programs and 20 have issued guidance to waive or lower telehealth copayments specifically (note that some states did not charge cost-sharing for any or all services prior to the pandemic).
Looking ahead
Prior to the pandemic, state coverage of telehealth in Medicaid varied widely. States took many factors into consideration including budget limitations, patient and provider acceptance, scope of practice laws, operational/technology challenges and costs for providers and patients, evidence around quality and effectiveness of services delivered via telehealth, concerns involving potential for fraud and abuse among others.11 Although state coverage of telehealth in Medicaid still varies widely, widespread changes to Medicaid telehealth policies undertaken during this public health emergency will provide additional information and evidence involving the use and effectiveness of telehealth. Although certain Medicaid telehealth policy changes may expire with the end of the public health emergency, states may consider making permanent some changes initiated in response to the COVID-19 crisis.
Data for the counts of states taking each action to expand telehealth access come from the Center for Connected Health Policy (last updated May 13, 2020), the Federation of State Medical Boards (last updated June 9, 2020), and KFF’s Medicaid Emergency Authority Tracker, as reported by Manatt Health (last updated June 15, 2020). Because these actions do not require CMS approval and are thus not posted in a single place, these counts may be incomplete. Further, states may have taken some actions prior to the COVID-19 pandemic, which may or may not be reflected in the counts. ↩︎
Every week we recap the past week in the coronavirus pandemic from our tracking, policy analysis, polling, and journalism.
The June 2020 KFF Health Tracking Poll finds a majority of the public (56%) say they are worried that recent protests may lead to an increase in coronavirus cases in their area. Democrats and Black adults – groups that are most likely to support the protests – are also among the most likely to say they are worried about the protests leading to an increase in coronavirus cases. About two in three Americans (64%) support the recent protests against police violence. The poll also reveals partisan differences in knowledge about the disparities faced by Black and Hispanic adults when it comes to health care and experiences with police. For example, Democrats are twice as likely as Republicans to know that Black Americans are more likely than White Americans to get sick or die from coronavirus (69% vs. 34%).
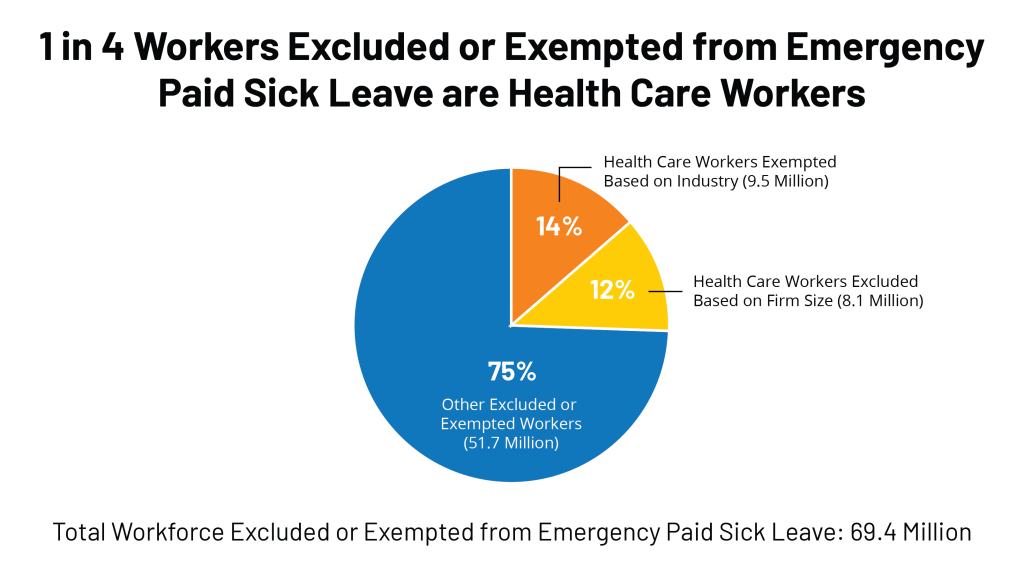
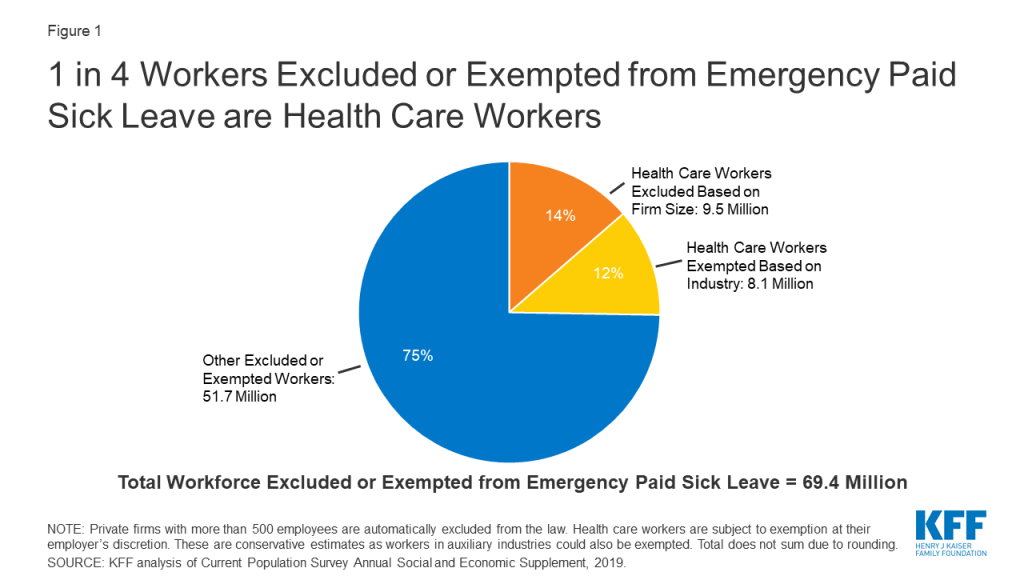
We also published new resources this week focusing on the pandemic’s impact on workers. One analysis finds that at least 69.4 million adult American workers – approximately four in 10 – are potentially ineligible for emergency paid sick leave benefits. Approximately 25% of those workers (17.7 million workers) are in the health care industry. Seventy-five percent of excluded or exempted health care workers are women, and 39% are people of color. A separate brief finds nearly one in four workers (24%) are considered at high risk of serious illness if they get infected by the novel coronavirus, highlighting the challenges that businesses, public offices and other employers face as they move toward reopening.
Here are the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: Total cases worldwide passed 8.3 million this week – with an increase of approximately 835,000 new confirmed cases between June 11 and June 17. There were approximately 27,500 new confirmed deaths worldwide between June 11 and June 17, bringing the total to approximately 449,000 confirmed deaths.
U.S. Cases and Deaths: There were nearly 163,000 confirmed cases between June 10 and June 17. Approximately 4,800 new confirmed deaths in the past week brought the total to nearly 118,000 confirmed deaths in the US.
U.S. Tests: There have been over 24.9 million total COVID-19 tests with results in the United States —with about 3.4 million added since June 10. In the past week, 1% of the total U.S. population was tested.
Race/Ethnicity Data: The demographics dashboard in our State Data and Policy Actions to Address Coronavirus tracker has been updated. Black individuals made up a higher share of cases/deaths compared to their share of the population in 31 of 47 states reporting cases and 32 of 43 states reporting deaths. More than half of deaths were among Black people in 2 states – Louisiana and Mississippi. Meanwhile, 75% of those who have died in Washington D.C. due to COVID-19 were Black. Hispanic individuals made up a higher share of cases compared to their share of the total population in 35 of 44 states reporting cases. COVID-19 continues to have a sharp, disproportionate impact on American Indian/Alaska Native and Asian people as well in some states.
Adults at Higher Risk of Serious Illness if Infected with Coronavirus: 38% of all U.S. adults are at risk of serious illness if infected with coronavirus (92,560,223 total) due to their age (65 and over) or pre-existing medical condition. Of those at higher risk, 45% are at increased risk of serious illness if infected with coronavirus due to their existing medical condition such as such as heart disease, diabetes, lung disease, uncontrolled asthma or obesity. Among nonelderly adults — low-income, American Indian/Alaska Native & Black adults have a higher risk of serious illness if infected with coronavirus. In both cases – for race and household income – the higher risk of serious illness if infected with coronavirus is chiefly due to a higher prevalence of underlying health conditions and longstanding disparities in health care and other socio-economic factors.
Social Distancing: 51 states have eased at least one social distancing measure.
Stay At Home Order: Original stay at home order in 7 states, stay at home order eased or lifted in 38 states, no action in 6 states
Mandatory Quarantine for Travelers: Original traveler quarantine mandate in place in 9 states, traveler quarantine mandate eased or lifted in 16 states, no action in 26 states
Non-Essential Business Closures: Some or all non-essential businesses permitted to reopen (some with reduced capacity) in 46 states, no action in 5 states
Large Gatherings Ban: Original gathering ban/limit in place in 10 states, gathering/ban limit eased or lifted in 40 states, no action in 1 states
State-Mandated School Closures: Closed in 6 states, closed for school year in 37 states, recommended closure in 1 state, recommended closure for school year in 6 states, rescinded in 1 state
Restaurant Limits: Original restaurant closures still in place in 4 states, restaurants re-opened to dine-in service (some with reduced capacity) in 46 states, no action in 1 state
Primary Election Postponement: Postponement in 15 states, no postponement in 36 states
Emergency Declaration: There are emergency declarations in all 51 states.
Waive Cost Sharing for COVID-19 Treatment: 3 states require, state-insurer agreement in 3 states; no action in 45 states
Free Cost Vaccine When Available: 9 states require, state-insurer agreement in 1 state, no action in 41 states
States Requires Waiver of Prior Authorization Requirements: For COVID-19 testing only in 5 states, for COVID-19 testing and treatment in 6 states, no action in 40 states
Early Prescription Refills: State requires in 18 states, no action in 33 states
Premium Payment Grace Period: Grace period extended for all policies in 4 states, grace period extended for COVID-19 diagnosis/impacts only in 4 states, expired in 8 states, no action in 35 states
Marketplace Special Enrollment Period: Marketplace special enrollment period still active in 5 states, ended in 7 states, no special enrollment period in 39 states
Paid Sick Leave: 13 states enacted, 2 proposed, no action in 36 states
38 states overall have taken mandatory action expanding access to telehealth services through private insurers, including:
New Requirements for Coverage of Telehealth Services: Parity with in-person services in 6 states, broad coverage of telehealth services in 6 states, limited coverage of telehealth services in 6 states, no action in 33 states
Waiving or Limiting Cost-Sharing for Telehealth Services: Waived for COVID-19 services only in 7 states, waived or limited for all services in 9 states, no action in 35 states
Reimbursement Parity for Telehealth and In-Person Services: Required for all services in 17 states, no action in 34 states
Require Expanded Options for Delivery of Telehealth Services: Yes in 35 states, for behavioral health services only in 1 state, no action in 15 states
Approved Section 1115 Waivers to Address COVID-19: 2 states (Washington and New Hampshire) have approved waivers
Approved Section 1135 Waivers: 51 states have approved waivers
Approved 1915 (c) Appendix K Waivers: 49 states have approved waivers
Approved State Plan Amendments (SPAs): 45 states have temporary changes approved under Medicaid or CHIP disaster relief SPAs, 1 state has an approved traditional SPA
Other State-Reported Medicaid Administrative Actions: 51 states report taking other administrative actions in their Medicaid programs to address COVID-19
Poll: 7 in 10 Black Americans Say They Have Experienced Incidents of Discrimination or Police Mistreatment in Their Lifetime, Including Nearly Half Who Felt Their Lives Were in Danger
Most Democrats See Racism and Police Violence as a Big Problem Nationally, While Most Republicans Instead View Violence by Protesters as a Big Problem
Most of the Public Favor a Range of Police Reforms to Curb Excessive Force, though Partisan Gaps Exist on Some Key Proposals
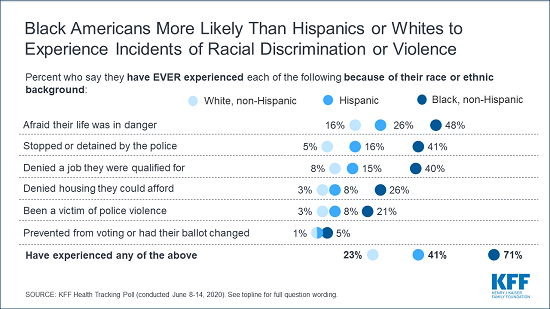
Amid nationwide protests against racial bias in law enforcement and beyond, a new KFF poll finds that the vast majority (71%) of Black Americans say they’ve experienced some form of racial discrimination or mistreatment during their lifetimes – including nearly half (48%) who say at one point that they felt their life was in danger because of their race.
When asked about interactions with law enforcement during their lifetimes, 4 in 10 (41%) Black Americans say they have been stopped or detained by police because of their race, and 1 in 5 Black adults (21%), including 3 in 10 Black men, say they have been a victim of police violence. A third as many Hispanics (8%) and relatively few Whites (3%) report such negative interactions with police over their lifetimes.
Blacks are also much more likely than Hispanics or Whites to say they have been denied a job for which they were qualified (40%, 15%, and 8%, respectively) or denied housing they could afford due to their race (26%, 8%, and 3%, respectively).
When asked about incidents just in the past year, 3 in 10 (30%) Black Americans say they personally experienced unfair treatment by police during traffic stops and other encounters. That is nearly three times the share of Hispanic Americans (11%) and ten times the share of White Americans (3%) who report such unfair treatment by police in the past year.
Fielded June 8-14, the poll probes into issues of racial and ethnic bias and discrimination and the national conversation about race sparked by recent deaths of Black Americans at the hands of police, as well as the subsequent protests, clashes, and in some cases, looting and vandalism.
The poll finds large shares of Americans view racism, police violence and violence caused by protestors as at least somewhat of a problem in the country today, though there are deep partisan divisions on these issues.
For example, most Democrats (82%) and independents (59%) say racism is a big problem nationally, while only a quarter (25%) of Republicans say so.
Democrats also are much more likely to say police violence is a big problem (65%) than to say violence caused by protesters is (24%). The opposite is true for Republicans, who are far more likely to say protester violence is a big problem (62%) than to say police violence is (14%).
Partisans also differ in their awareness about the COVID-19 epidemic’s disproportionate impact on Black and Hispanic communities and broader disparities in health care. For example, Democrats are twice as likely as Republicans to know that Black Americans are more likely than White Americans to get sick or die from coronavirus (69% vs. 34%).
Most of the Public Support Banning Chokeholds and No-Knock Warrants, Though Partisan Gaps Remain
The poll finds two key potential reforms that seek to reduce the excessive use of force by police officers are favored by a majority of the public, though Republicans are less supportive: banning police from using chokeholds and strangleholds (68% of the public, including 82% of Democrats, 70% of independents, and 52% of Republicans) and banning no-knock warrants that allow police to enter a person’s residence unannounced (52% of the public, including 65% of Democrats, 56% of independents and 34% of Republicans).
Bipartisan majorities support a range of other proposed reforms, including:
95% support requiring police to intervene and stop excessive force being used by other officers and to report those instances;
89% support requiring police to give a verbal warning, when possible, before shooting at a civilian;
76% support requiring states to publicly release disciplinary records for law enforcement officers; and
73% support allowing people to sue police officers if they feel they were subjected to excessive force.
Two Thirds of Public Supports Recent Protests against Police Violence
The poll finds two thirds of the public (64%) support the recent protests against police violence across the country, while three in ten oppose the protests (30%). Majorities across racial and ethnic groups support the protests, as do most Democrats (86%) and independents (67%), though most Republicans (57%) oppose them.
At the same time, a slight majority (56%) of the public say they are very or somewhat worried that protests may lead to an increase in coronavirus cases in their area. Democrats and Black Americans – groups that are most likely to support the protests – are also among the most likely to say they are worried about the protests leading to an increase in coronavirus cases (73% and 68% respectively).
Overall, 1 in 10 adults say they recently attended an event to protest police violence or in support of Black Lives Matter or other racial justice issues. About half (52%) of those who report attending a protest are under 30 years old, and a similar share (53%) are college graduates. Most identify as Democrats (46%) or independents (42%), with just 6% identifying as Republicans.
Designed and analyzed by public opinion researchers at KFF, the poll was conducted June 8-14 among a nationally representative random digit dial telephone sample of 1,296 adults. Interviews were conducted in English and Spanish by landline (297) and cell phone (999). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher. The margin of sampling error is plus or minus 4 percentage points for the sample of 811 White adults, plus or minus 9 percentage points for the sample of 211 Black adults, and plus or minus 8 percentage points for the sample of 177 Hispanic adults.
As with other payers, the coronavirus pandemic has resulted in financial strain for Medicaid providers. Some providers are dealing with both increased utilization and costs related to testing and treatment of COVID-19, while others are facing substantial losses in revenue as utilization has declined for non-urgent care. Medicaid providers include those that serve a high share of Medicaid enrollees and/or deliver services primarily financed by Medicaid, such as behavioral health or long-term care. These providers may face disproportionate risks to their continued financial viability as they may already have lower reimbursement levels relative to costs and lower operating margins. Within broad federal rules, states determine how Medicaid services are delivered and set reimbursement rates (or capitation payments for managed care).
In light of the pandemic, CMS has provided some guidance about options under current Medicaid rules that states can use to provide financial support for some providers. In addition, Congress has authorized $175 billion in new provider relief grants in the Coronavirus Aid, Relief, and Economic Security (CARES) Act and the Paycheck Protection Program and Health Care Enhancement Act to help bolster providers; however, the Administration’s plans to allocate those funds may not adequately address issues for providers that serve a disproportionate share of Medicaid enrollees. This brief provides an overview of how states currently reimburse providers and the challenges for Medicaid providers that have emerged from the pandemic and state budget issues. It presents new data on state actions to date to help bolster Medicaid providers dealing with the effects of COVID-19 and discusses support available for Medicaid providers from the federal provider relief fund.
What Challenges are Providers Facing Due to COVID-19?
Many Medicaid providers may be under fiscal strain as a result of the pandemic. Some providers are dealing with both increased utilization and costs related to testing and treatment of COVID-19, while others are facing substantial losses in revenue as utilization has declined for non-urgent care. For providers in states that rely heavily on managed care, states have made payments to the plans, but those funds may not be flowing to providers where utilization has decreased.
Medicaid providers may have been more fiscally vulnerable prior to the pandemic. Community health centers are a key source of primary care, and safety-net hospitals, including public hospitals and academic medical centers, provide a lot of emergency and inpatient hospital care for Medicaid enrollees. Safety-net hospitals and clinics as well as other providers that rely on Medicaid funding, including behavioral health providers, substance use disorder treatment providers, home and community-based service providers, children’s hospitals, pediatricians, and maternal health providers, may operate with lower operating margins and are vulnerable to fiscal stress from the pandemic. For example, recent data show that significant numbers of community health centers are closing, and federal fiscal relief from the Coronavirus Aid, Relief and Economic Security Act (CARES) and Paycheck Protection Program and Health Care Enhancement Act may not be sufficient to address financial and workforce issues that have been exacerbated by the pandemic.
How Does Medicaid Reimburse Providers Now?
Within broad federal rules, states have considerable flexibility in how they deliver and pay for services for Medicaid enrollees. States have latitude to determine provider payments so long as the payments are consistent with efficiency, economy, quality and access and safeguard against unnecessary utilization. Within these broad guidelines, provider payments must be sufficient to ensure Medicaid beneficiaries with access to care that is equal to others in the same geographic area. Over the years, beneficiaries and providers used this legal requirement, known as the “equal access provision,” to ensure that states use Medicaid provider payment rate setting methodologies that provide equal access. In 2015, however, the Supreme Court ruled in Armstrong v. Exceptional Child that providers could not bring lawsuits to enforce the equal access provision in federal court. Following the case, HHS issued regulations requiring states to measure access in fee-for-service delivery systems. Under the Trump Administration, HHS has proposed to rescind the regulations that require states to document access to care and service payment rates and include input from Medicaid providers, beneficiaries, and other stakeholders about the impact on access to care when proposing to reduce or restructure payment rates. That proposal is still pending at CMS.
Under current law, states can pay certain types of fee-for-service providers up to what Medicare would have paid in aggregate across the type and class of provider. States often use these upper payment limit (UPL) arrangements to direct supplemental payments to certain Medicaid providers to offer additional financial support. The use of UPL arrangements was under intense scrutiny at CMS prior to the pandemic, and the future of some of these arrangements is in question depending on the fate of the proposed Medicaid Fiscal Accountability Rule (MFAR) that is pending at CMS. If finalized as proposed, that rule would limit states’ ability to use supplemental payments and restrict what funds states can use for their state share of Medicaid spending. MFAR could affect existing Medicaid financing arrangements in most states, and there were over 4,000 comments on the proposed rule. The Health and Economic Recovery Omnibus Emergency Solutions Act (HEROES Act) passed by the House on May 15, prohibits the Secretary from taking any action to finalize or implement the proposed rule through the end of the public health emergency; that bill has not been taken up by the Senate to date.
Payments to Medicaid managed care organizations (MCOs) must be actuarially sound. Actuarial soundness means that “the capitation rates are projected to provide for all reasonable, appropriate, and attainable costs that are required under the terms of the contract and for the operation of the managed care plan for the time period and the population covered under the terms of the contract.” Unlike fee-for-service, capitation provides upfront fixed payments to plans for expected utilization of covered services, administrative costs, and profit. States generally pay the plans a capitation payment, but then the plans determine how to pay the providers in their network. Information is limited regarding the rates paid by plans to providers in managed care.
Under current MCO rules, states are prohibited from directing how a managed care plan pays its providers except for certain payment methodologies that have been approved and reviewed by CMS. States may require MCOs to adopt minimum or maximum provider payment fee schedules or provide uniform dollar or percentage increases for network providers that provide a particular service under the contract, as approved by CMS. States also can seek CMS approval to require MCOs to implement value-based purchasing models for provider reimbursement (e.g., pay for performance, bundled payments) or participate in multi-payer or Medicaid-specific delivery system reform or performance improvement initiatives. State directed payments must be based on utilization and delivery of services covered under the managed care plan contract. The proposed MCO rule pending at CMS would make some changes to minimum fee schedule arrangements for directed payments. The 2016 final rule phases out state supplemental pass-through provider payments in the capitation rates paid to managed care plans because these payments are not tied to the provision of services covered under plan contracts and therefore conflict with the actuarial soundness requirement. Specifically, the 2016 rule phases out pass-through payments to hospitals from 2017- 2027, and to physicians and nursing facilities from 2017-2022. The proposed rule would allow states to make new supplemental provider pass-through payments during a time-limited period when states are transitioning populations or services from fee-for-service to managed care.
What Are State Options Under Current Medicaid Rules to Support Providers?
To address current fiscal challenges faced by providers, states have various options to support providers directly or by directing plans to do so. CMS has described some of these options in its COVID-19 frequently asked questions and an informational bulletin on Medicaid managed care options for responding to COVID-19.
State Options to Financially Support Providers
COVID-Related Rate Increases and Payment Methodology Adjustments. States can increase provider rates to account for increased costs or decreased service utilization as a result of the public health emergency. For example, states could increase payments to providers that are seeing an influx of Medicaid patients due to the emergency, incurring additional costs related to COVID-19 like personal protective equipment (PPE) or additional staff, or experiencing decreased utilization but an increased cost per unit due to allocation of fixed costs or increase in patient acuity. States also could increase payments for services delivered via telehealth. Payment increases can be in the form of dollar or percentage increases in base payment rates or fee schedule amounts, rate add-ons, or supplemental payments. Depending on the Medicaid authority that states are using for the covered service, states are using Home and Community Based Services Waiver (HCBS) Appendix K, Disaster-Relief State Plan Amendments (SPAs) and Section 1115 demonstration waivers to adopt COVID-related rate increases for providers.
Payment Increases through Upper Payment Limit (UPL) Adjustments. States may be able to make adjustments within the bounds of the UPL ceiling to direct supplemental payments to providers during the emergency or potentially make changes to UPL demonstrations already submitted to CMS to support UPL estimates for the fiscal year. With regard to proposed increases to nursing facility rates, CMS guidance related to UPL demonstrations recognizes that states can use either a cost-based approach or a payment-based approach to comply with the UPL ceiling. Under a cost-based approach, an increase in nursing facility costs due to the emergency can be accounted for in the UPL ceiling. Under a payment-based approach, states can adjust the UPL ceiling to the extent that Medicare payment equivalents have increased. CMS guidance says that it will work with states if they are concerned about UPL calculations, but the guidance also notes that states cannot use Medicaid Disaster Relief SPAs to waive applicable UPLs, and payments still must meet all applicable legal requirements.
Advance and Interim Payments. CMS has said in recent guidance that under state plan authority, states can make periodic interim advance payments to providers to help providers remain viable during the emergency so that they are available when the emergency period is over. The interim payment methodology must describe how states will compute interim payment amounts for providers (e.g., based on the provider’s prior claims payment experience), and subsequently reconcile the interim payments with final payments for which providers are eligible based on billed claims. CMS has said that it will consider such requests on an expedited basis.
Retainer Payments. States can request authority to make retainer payments to certain habilitation and personal care providers to maintain capacity during the emergency. Unlike interim payments, which are made before services are provided and subsequently reconciled so that providers are paid only for services actually rendered, retainer payments allow providers to continue to bill and be paid for certain services that are authorized in person-centered service plans to enable providers to maintain capacity when circumstances prevent enrollees from actually receiving those services. For example, during the current pandemic, enrollees may not be able to receive in-person services due to self-quarantine rules. Such retainer payments are limited to personal care or attendant service providers while the enrollee is hospitalized or absent from their home. CMS has permitted states to make retainer payments since 2000, in Olmstead guidance, to equalize treatment of personal assistance services and nursing facility services, for which bed hold payments are permitted. In the Olmstead decision, the U.S. Supreme Court found that states have community integration obligations under the Americans with Disabilities Act. The 2000 guidance applies to personal assistance services provided through HCBS waivers, and CMS’s Section 1115 COVID-19 demonstration waiver template allows states to request authority for retainer payments to habilitation and personal care providers such as adult day health centers that have closed due to social distancing orders and could go out of business and be unavailable to provide services after the pandemic. The National Association of Medicaid Directors has requested additional flexibility from CMS to enable states to make retainer payments to a broader set of providers using Section 1115 waiver authority.
Directed Payment Through MCOs. States can direct that managed care plans make payments to their network providers using methodologies approved by CMS to further state goals and priorities, including COVID-19 response. This strategy can address the scenario in which states are making capitation payments to plans, but providers are not receiving reimbursement from plans due to decreased service utilization while social distancing measures are in place and non-urgent services are suspended. For example, states could require plans to adopt a uniform temporary increase in per-service provider payment amounts for services covered under the managed care contract, or states could combine different state directed payments to temporarily increase provider payments, according to recent CMS guidance.
CMS explains that state directed increased payments for actual utilization of services can preserve the availability of covered services for enrollees during a time when providers may be experiencing dramatic utilization declines or incurring additional costs due to the public health emergency. The guidance also says that states may use directed payments to address increased use of telehealth or other approaches to maintain access to care for all enrollees or specific subgroups with specialized needs during the emergency. States can direct payments to a class of providers, such as dental, behavioral health, home health and personal care, pediatric, federally-qualified health centers, or safety-net hospitals, to support providers that may serve a high proportion of Medicaid enrollees and may be disproportionately affected by the public health emergency. Directed payments must be appropriate and reasonable compared to the total payments the provider would have received in the absence of the public health emergency. For states that have approved directed payment proposals, CMS guidance says that states wishing to make changes to such arrangements in light of COVID-19 can submit an amended directed payment preprint and/or contract and rate certification amendments to CMS.
Section 1115 Waiver Disaster Relief Funds. In prior emergencies, states have used Section 1115 waivers to create disaster relief funds to support Medicaid providers experiencing high levels of uncompensated care or fiscal instability. For example, disaster waivers approved in response to Hurricane Katrina included uncompensated care funds for affected states. During the COVID-19 emergency, CMS told Washington that it would continue to review the state’s request to use Section 1115 authority to create a Disaster Relief Fund to cover costs associated with the treatment of uninsured individuals with COVID-19, housing, nutrition supports and other COVID related expenditures. During state stakeholder calls, CMS has said it will consider other available federal funds before approving state requests for Section 1115 authority for certain activities. For example, CMS pointed to relief funds available through CARES as rationale for not approving Washington’s request to cover treatment costs for the uninsured through Medicaid. However, the amount and allocation of those funds is still a question.
State Adoption of Provider Payment Policies During COVID-19
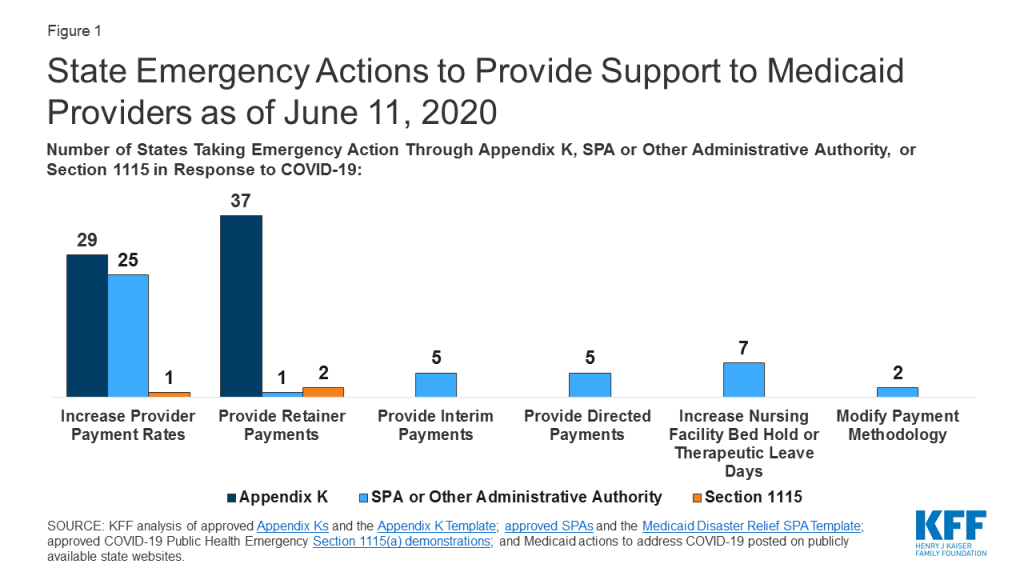
States have taken a number of actions to provide support to Medicaid providers in response to COVID-19 through Disaster-Relief State Plan Amendments (SPAs) and other administrative authorities, HCBS waiver Appendix K, and Section 1115 demonstration waivers. The Disaster-Relief SPA allows states to make temporary changes to their Medicaid state plans to address access and coverage issues during the COVID-19 emergency. States can also make changes through traditional SPAs (though no state to date has changed provider payment policies in response to COVID-19 using a traditional SPA) and can implement other changes under existing administrative authority that do not require SPA approval. Most Medicaid home and community-based services (HCBS) are provided through Section 1915 (c) waivers. Other states use Section 1115 to authorize HCBS that could have been provided under Section 1915 (c). States can use Section 1915 (c) waiver Appendix K to amend either of these HCBS waivers to respond to an emergency. CMS also developed a COVID-19 Section 1115 demonstration waiver template that identifies options for states to address the pandemic. The section below highlights the most common actions that states are taking regarding provider payment under these authorities (Figure 1).
Figure 1: State Emergency Actions to Provide Support to Medicaid Providers as of June 11, 2020
The most common policy adopted by states to support providers across service type and authority is increasing payment rates. As of June 11, 2020, twenty-five states have taken action to increase provider payment rates for state plan services through Disaster-Relief SPA or other administrative authority, 29 states have done so for HCBS waiver services using Appendix K, and one state is using a Section 1115 waiver to increase rates for HCBS.
States adopting temporary provider payment rate increases for state plan services using Disaster-Relief SPA or other administrative authority are most frequently targeting nursing facility services. Some states limit the additional payments to nursing facilities or patients with a COVID-19 diagnosis, while others apply them to all nursing facilities to account for increased costs related to staffing, equipment and cleaning as a result of the emergency. For example, some states are increasing facility per diem payments by a flat dollar amount or percentage (AL, CA, CO, KS, KY, LA, MT, NC, NM, OH, SC, WA, VA). Alabama also is providing an additional add-on cleaning fee. Arkansas adopted temporary supplemental payments that increase weekly pay of direct care workers in nursing facilities, intermediate care facilities, and psychiatric treatment centers; the payments include a base supplemental payment according to number of hours worked and an additional tiered acuity payment for those working in facilities with COVID-19 positive patients. Michigan is providing a $5,000 per bed supplemental payment in the first month for COVID-19 regional hub nursing facilities to address immediate infrastructure and staffing needs and a $200 per diem rate increase in subsequent months to account for the higher costs of caring for COVID-19 patients. Four states (CO, IL, MT, WV) are increasing payment rates for other institutional settings, such as ICF/IDDs, in light of COVID-19, using Disaster-Relief SPA or other administrative authority.
A couple of states have adopted temporary payment rate increases that apply to a range of providers. In March, Arizona passed legislation to increase payment rates for Medicaid physicians and dental providers, funded through a hospital assessment. Massachusetts has set up an $800 million dollar fund for Medicaid providers impacted by COVID-19, including hospitals, nursing facilities, physicians, community health centers, HCBS, and community behavioral health providers. For example, as part of this initiative, Massachusetts is increasing hospital rates by 20% for COVID-19 care and 7.5% for other hospital care. In addition, Tennessee is seeking federal approval to distribute $5 million in targeted payments to behavioral health providers to preserve the community mental health and substance use disorder provider network for Medicaid beneficiaries.
Among the 29 states using Appendix K to temporarily increase provider payment rates for HCBS waiver services, the types of services commonly targeted for increases are residential habilitation, home health, respite, personal care, and nursing. Five of these states (KY, LA, NE, WA, WY) have broad approval to increase rates for any services in some or all of their HCBS waivers, up to a cap; the approved caps range from 15% to 50% of current rates. Some states are increasing HCBS payment rates only or particularly in case where waiver enrollees are COVID-19 positive; an example is Wyoming. In addition, six states (AK, AR, DC, MI, NC, OK) have increased payments for state plan HCBS using Disaster-Relief SPA authority, and Washington has done so using Section 1115 demonstration waiver authority. State plan HCBS rate increases include targeted case management (AK), day habilitation (AR), skilled and/or private duty nursing (DC, OK), and home health and adult care homes (NC). Arkansas’s temporary supplemental payments for direct care workers in nursing facilities, described above, also apply to direct care workers in assisted living facilities and those providing home health and personal care services in the community. Michigan is adding a supplemental payment for providers of personal care and behavioral health treatment technician in-person services. Washington’s Section 1115 demonstration waiver allows the state to increase rates for Community First Choice attendant care services by up to 50 percent to maintain provider capacity during the public health emergency.
Many states are adopting retainer payments for HCBS (the only services for which they are available). Thirty-seven states have established retainer payments through Appendix K to support HCBS waiver service providers and address emergency-related issues. Two states (WA and NH) have an approved Section 1115 waiver that authorizes retainer payments for personal care and habilitation services provided under state plan authority. Vermont is only state providing temporary retainer payments to a broader set of Medicaid providers through existing authority to set provider payments under its Section 1115 waver. Vermont has a unique managed care-like delivery system in which the state Medicaid agency contracts with another state entity that operates as a non-risk prepaid health inpatient plan. Vermont’s temporary payment model gives providers the option to combine fee-for-service reimbursement with prospective monthly payments that are intended to reimburse providers for the difference between their long-term average monthly Medicaid fee-for-service revenues and the actual amount of Medicaid fee-for-service claims payments issued to them for services they continue to provide. After the state of emergency ends, up to 10% of prospective payments may be subject to recoupment based on the provider’s performance on access to care and financial impact metrics, except that providers that have been ordered to close as a result of the emergency and cannot provide remote services will not be subject to recoupment.
Few states are using interim or advance payments to support providers. Five states (AZ, CA, GA, NC, OK) have received approval through a Disaster-Relief SPA to make interim payments to providers. In North Carolina, any Medicaid-enrolled provider may request that their reimbursement be converted to an interim payment methodology. Arizona is providing interim payments to Medicaid-enrolled hospitals, while Oklahoma is providing interim payments to rural/ independent Medicaid-enrolled hospitals. Georgia is making interim payments to skilled nursing facilities. California is providing interim payments for non-narcotic treatment program and specialty metal health services.
A small number of states are using directed payments through MCOs or are working with MCOs to increase funding to providers during the emergency. Arizona’s March legislation includes directed payments to hospitals, funded through a hospital assessment. New Hampshire directed its MCOs to provide temporary add-on payments to safety net providers including federally qualified health centers, rural health centers, critical access hospitals, and providers of residential substance use disorder treatment, home health, personal care, and private duty nursing services. Tennessee has adopted temporary payment rate increases for community-based residential, personal care, attendant care, personal assistance and intensive behavioral treatment stabilization and treatment services and a temporary per diem add-on to community-based residential and personal care payment rates to account for direct support staff hazard pay, overtime, and PPE costs using its existing directed payment authority; these services are provided under a Section 1115 HCBS waiver. Washington is identifying behavioral health providers at financial risk and directing its MCOs to reach out and offer support, such as advance payments, adjustments to capitated contracts, or other relief on a case-by-case basis, such as release of provider enhancement funds or budget-based contracts. Colorado is encouraging its managed care entities to use alternative funding strategies to support community mental health centers, such as sub-capitated arrangements. Rhode Island is seeking Section 1115 approval to make pass-through payments to MCOs during the public health emergency to effectuate rate increases to hospitals and HCBS providers and retainer payments to personal care, habilitation, rehabilitation, and adult day HCBS providers, to the extent those payments are approved by CMS.
A limited number of states are using nursing facility bed hold increases and other payment methodology adjustments. Seven states have received approval through a Disaster-Relief SPA to increase the number of days they will provide payment to nursing facilities to reserve the bed of a beneficiary that is hospitalized or otherwise temporarily absent. Three states (HI, KY, OH) have received SPA approval to increase the number of nursing facility bed hold days, and three states (LA, OK, PA) have received approval to increase the number of therapeutic leave days. Utah is increasing both bed hold and therapeutic leave days. Two states are making other payment methodology changes in response to COVID-19. Kentucky has received approval through a Disaster-Relief SPA to temporarily avoid applying per diem rate sanctions to nursing facilities that are unable to meet medical record review thresholds to validate assignment of patients to reimbursement groups based on acuity during the public health emergency. To aid drive-through testing facilities, Washington received approval through a Disaster-Relief SPA to unbundle payments and instead set a flat rate for the handling and/or conveyance of specimens for transfer from the patient (other than in an office) to a laboratory.
How are Provider Relief Funds Supporting Medicaid Providers?
The Coronavirus Aid, Relief, and Economic Security (CARES) Act and the Paycheck Protection Program and Health Care Enhancement Act provide $175 billion in provider relief funds to reimburse eligible health care providers for health care related expenses or lost revenues that are attributable to coronavirus. The funds are available to reimburse providers for health care related expenses or lost revenues that are attributable to coronavirus. Specifically, funds are available for building or constructing temporary structures, leasing properties, medical supplies & equipment including PPE and testing supplies, increased workforce and trainings, emergency operation centers, retrofitting facilities, and surge capacity.
To date, $112.4 billion of these funds have been allocated to specific sets of providers. The $112.4 billion consists of $50 billion that HHS allocated in April to Medicare fee-for-service providers based on each provider’s share of total 2018 net patient revenue from all sources, plus $22 billion in tworounds of funding to hospitals that treated a high number of COVID-19 patients; $10 billion to rural providers (including hospitals, health clinics, and health centers); $4.9 billion for skilled nursing facilities; $500 million to Indian Health Service programs; $10 billion to safety net hospitals; and $15 billion to Medicaid/CHIP providers who did not receive funds in the distribution to Medicare fee-for-service providers.
Prior to the new $15 billion allocation, there had been concern that Medicaid providers were disadvantaged in the funding distribution to date, both in the amount of funding received and delays in allocations. HHS estimates that about 62% of all Medicaid/CHIP participating providers received funds as part of the $50B general allocation to Medicare fee-for-service providers based on net patient revenue from all sources distributed in April. An analysis of those funds shows that the distribution disadvantaged providers less reliant on private insurance payments (and therefore likely more reliant on Medicaid). This resulted because private insurance reimburses at a higher rate than public payers. Provider relief funds specifically allocated to Medicaid providers were not announced until June 2020. HHS notes that some of the earlier targeted funding allocations, including base payments to rural health clinics and rural community health centers, accounted for providers with no reported Medicare claims. To help allocate funds to Medicaid providers, CMS asked states to provide data on Medicaid provider revenues. Due to data reporting challenges, CMS instructed states to not include data for self-directed direct care providers (HCBS) and PACE organizations, making it unclear whether those provider types were sufficiently reflected in the funding allocation.
HHS estimates that close to one million Medicaid/CHIP providers are eligible for grants from the new $15 billion allocation for those who did not receive funds in the distribution to Medicare fee-for-service providers. According to HHS, payments to each provider will be at least 2% of reported gross revenue from patient care. While this is the same level provided to Medicare fee-for-service providers in the April distribution, Medicaid providers may have more narrow operating margins than providers that rely more heavily on private insurance and Medicare so it is unclear if the allocation will be adequate. The final amount will be determined after providers submit data, including the number of Medicaid patients served. The submission deadline is July 20. HHS anticipates that provider types potentially eligible for this funding include pediatricians, OB-GYNs, dentists, opioid treatment and behavioral health providers, assisted living facilities, and other HCBS providers. However, Medicaid providers who received any amount of funding, no matter how small, from the April distribution to providers who participate in Medicare fee-for-service cannot receive additional funds from the new Medicaid provider allocation. This could disadvantage providers highly reliant upon Medicaid, such as community health centers. Funding will be distributed directly to providers and will not flow through state Medicaid agencies.
The remaining $62.6 billion from the provider relief fund may not be sufficient for the other purposes identified by HHS, including paying for COVID-19 treatment costs for the uninsured and supporting other targeted provider groups affected by COVID-19.HHS has allocated an unspecified amount of the provider relief fund to reimburse providers for the cost of providing COVID-19 treatment to uninsured people at Medicare rates, until funding is exhausted. KFF has estimated that hospital costs alone could run between $13.9 billion to $41.8 billion – not taking into account costs incurred for services provided in other settings. The decision to use a portion of the limited pool of provider relief funds to cover COVID-19 treatment costs for the uninsured (instead of through new or expanded insurance coverage options) means that less funding will be available for other purposes identified by Congress and for direct support for Medicaid providers.
HHS’s website refers to “future provider relief funding, and HHS has stated that it is working on an additional allocation for dentists. It is unclear whether there will be further, separate allocations for other provider groups. The HEROES Act passed by the House would allocate additional money to the provider relief fund, specify a reimbursement formula that weights Medicaid reimbursement at 200% when determining net patient revenue, and require that not more than $10 billion of the provider relief fund be used to reimburse uncompensated care costs.
What is the Outlook?
While states have some have taken some action under existing Medicaid authority to help bolster providers using increased payment rates, retainer payments, interim payments, directed payments, and some other methods, these actions have been largely directed to nursing facilities and some targeted community based long-term services and supports providers. Fiscal relief provided through the CARES Act to temporarily increase the Medicaid match rate by 6.2 percentage points may help states make such payment adjustments in the short term. However, as the economic crisis continues, more individuals are likely to enroll in Medicaid while state revenues are expected to decline significantly. States that had projections available in late April were already anticipating Medicaid budget shortfalls in the next fiscal year. In prior economic downturns, states have turned to provider rate cuts, so it may be difficult in the current economic realities for states to continue to maintain or increase provider rates. At the same time, Congress has enacted legislation with $175 billion in provider relief grants. While these grants were designed to serve many purposes, the initial allocation of funds was disadvantageous to Medicaid providers. HHS recently announced that $15 billion has been set aside to more directly support Medicaid providers, and an unspecified amount has been allocated to reimburse providers for COVID-19 treatment costs for the uninsured. However, it is not clear if the current provider relief fund allocations will be sufficient to meet providers’ needs resulting from the pandemic. Congress will likely continue to debate additional funding for states through Medicaid and for providers. Without additional fiscal relief, states may be limited in their ability to support Medicaid providers and provider relief grants may not be adequate.
What options exist if you’ve lost your job-based health insurance?
As unemployment skyrockets due to the COVID-19 pandemic, tens of millions of people are at risk of losing their job-based health insurance. However, the majority of people are eligible for other forms of health insurance coverage.
Watch this two minute video to learn about the options: Medicaid, job-based coverage from a spouse or parent, ACA marketplace coverage, COBRA and short-term insurance plans.
A new KFF analysis finds that at least 69.4 million adult American workers – approximately four in 10 – are potentially ineligible for emergency paid sick leave benefits. Approximately 25% of those workers (17.7 million workers) are in the health care industry. Seventy-five percent of excluded or exempted health care workers are women.
The new emergency paid sick leave benefit that took effect in April as part of the Families First Coronavirus Response Act guarantees eligible workers up to 80 hours of paid leave for a health issue arising from coronavirus. However, the emergency paid sick leave provisions leave out a large swath of American workers by excluding those at private businesses with 500 or more employees, and offering broad exemptions for employers of emergency responders and health care workers regardless of firm size. Lack of comprehensive paid sick leave could result in workers having to choose between forgoing income or risking exposing their patients and colleagues to coronavirus.
Most (85%) health care and social assistance firms offer some form of paid leave as an employee benefit, but these programs typically require accrual and allow for an average of 7 to 8 days of sick leave, which is fewer than the number of days recommended by the CDC for recovery and quarantine from COVID-19. Fifteen percent of workers in these industries do not have any paid leave at all.
The emergency paid sick leave benefit that took effect in April as part of the Families First Coronavirus Response Act (FFCRA) guarantees eligible workers up to 80 hours of paid leave for a health issue arising from coronavirus. The Act represents the country’s first federal law aimed at providing workers paid leave, though it is set to expire at the end of 2020. In order to reduce the spread of coronavirus, the Centers for Disease Control and Prevention (CDC) has recommended that employers actively encourage employees who are exhibiting symptoms to stay home and maintain physical distancing. The new law temporarily provides short-term paid sick leave to as many as 86.3 million workers1 , according to our analysis of the Census Bureau’s 2019 Current Population Survey (CPS) Annual Social and Economic Supplement (ASEC). However, the emergency paid sick leave provisions leave out a large swath of American workers by excluding those at private businesses with 500 or more employees, and offering broad exemptions for employers of emergency responders and health care workers, regardless of firm size. While most health care employers offer paid sick leave to their workers, that leave usually requires accrual and may not be available to all workers or for as long as the emergency leave in the FFCRA.
While the legislation did not specify who would be classified as a health care worker, the Department of Labor (DOL) subsequently issued guidelines that permit many health care providers as well as a wide range of health-related entities to exempt their workers. Organizations responding to the COVID-19 pandemic, such as hospitals, doctors’ offices, clinics, residential facilities, medical schools, laboratories, pharmacies, and even contractors that provide services to these institutions, can be exempted. Should they choose the exemption, these employers are not required to offer emergency paid sick leave to either employees who provide direct patient care or who provide health-related services but do not have direct exposure to patients, such as janitors and food service workers.
In response to the gaps in emergency paid leave protections for health care and emergency response workers, the New York Attorney General has filed a lawsuit against the Trump Administration2 and several organizations have called on the Department of Labor to reconsider its expansive definitions of workers who may be exempted. Additionally, since the beginning of the pandemic, five states and 14 localities, plus Washington, DC, have enacted new emergency paid sick leave laws or expanded existing ones3 . On May 15, 2020, the House of Representatives passed the HEROES Act, legislation that would remove the federal FFCRA’s exclusion for private employers with 500 or more employees and the exemption for health care and emergency response workers, among several other coronavirus-related provisions. The bill is currently stalled in the Senate.
How Many Health Care Workers Do Not Have Access to the Coronavirus Emergency Paid Sick Leave?
Based on analysis of the 2019 CPS ASEC, we estimate that at least 69.4 million workers, or approximately four in ten workers, are potentially ineligible for emergency paid sick leave benefits. Approximately one in four (25%) of those workers works in the health care industry (Figure 1). In particular, the law automatically excludes the 9.5 million health care workers that work for a private employer with 500 or more employees (6% of the American workforce). An additional 8.1 million health care workers are subject to exemption (5% of the workforce) at their employer’s discretion. Taken together, as many as 17.7 million health care workers are not guaranteed access to emergency paid sick leave benefits under this law.
Figure 1: 1 in 4 Workers Excluded or Exempted from Emergency Paid Sick Leave are Health Care Workers
The CDC estimated in late May that more than 63,000 health care personnel had contracted COVID-19. Those working in the health care industry are of particular interest because of their increased risk of contracting the virus from infected patients as well as their potential to transmit the virus to patients at high risk of becoming seriously ill. While it is not known how many employers have elected not to offer emergency paid sick leave benefits under the exemption, we estimated the number of workers in the health care industries most likely to be excluded based on the DOL’s exemption criteria (see the Methodology section). This is a conservative estimate, as it does not include workers in some auxiliary services, such as industries that provide services necessary for the maintenance and operation of health care facilities and that can be exempted under the DOL’s guidance.
While most health care and social assistance firms offer paid sick leave as an employee benefit, whether voluntarily or state/locality-mandated, 15% of workers in these industries do not have any paid sick leave. Moreover, employer paid sick leave programstypically require accrual of time off and offer an average of 7 to 8 days of sick leave, which is fewer than the number of days recommended by the CDC for recovery and quarantine from COVID-19 for health care workers. By contrast, the FFCRA’s emergency paid sick leave law provides 2 weeks of paid sick leave, immediately available to all eligible workers, rendering it particularly valuable during this pandemic. Lack of comprehensive paid sick leave may discourage workers who have symptoms of coronavirus from staying home, potentially exposing their patients and co-workers to the virus.
Who are the Exempted and Excluded Health Care Workers?
Women make up the majority (75%) of the 17.7 million workers in the health care industry who are either automatically excluded from the new emergency paid sick leave law or subject to exemption (Figure 2). Nearly 4 in ten (39%) of them are people of color. Data suggest that due to higher rates of underlying health conditions, communities of color are at increased risk of serious illness if they contract COVID-19 and they face increased challenges related to health care access and social and economic factors. Other data find that communities of color are also experiencing higher rates of death from COVID-19. Additionally, about a quarter (24%) of the health care workforce excluded or subject to exemption are part-time workers, many of whom are less likely to receive any other type of paid leave benefit from their employer, as these benefits are often only available to full-time workers. Moreover, 18% are low-wage4 , for whom having to take unpaid leave when they are sick could put them in a difficult financial situation. Other research finds that lower-wage workers are also less likely to have access to other paid sick leave than higher-wage workers. For example, in 2019, only 47% of lower-income workers in private industry had access to paid sick leave, compared to 90% of higher-wage workers.
Figure 2: Characteristics of Health Care Industry Workers Excluded or Potentially Exempted from Emergency Paid Sick Leave
Many workers in the health care industry work in a setting where they may have exposure to patients and other health care workers (Table 1). More than four in ten (42%) work in hospitals, about a quarter (24%) work in long-term care facilities, which have been disproportionately affected by outbreaks of COVID-19, and about one in five (19%) work in physician offices and other outpatient care centers. Another 15% work outside of patient care settings, such as for the pharmaceutical industry, other medical supply companies, and a variety of other related health services.
Table 1: Worksites of the 17.7 Million Health Care Workers Who May Not Qualify for Emergency Paid Sick Leave
Hospitals
42%
Home, nursing, and residential care
24%
Home health care services
9
Nursing care facilities
9
Residential care facilities, without nursing
6
Physician offices and outpatient care
19%
Offices of physicians
9
Outpatient care centers
11
Medical and pharmaceutical manufacturing
7%
Pharmaceutical and medicine manufacturing
3
Medical equipment and supplies manufacturing
4
Other health care services
8%
SOURCE: KFF analysis of Current Population Survey Annual Social and Economic Supplement, 2019.
Discussion
Health care workers who continue to work while sick because they cannot afford to stay home without pay may face difficult tradeoffs between the need for an income and concerns about exposing patients or their colleagues. The FFCRA’s emergency paid sick leave provides an economic cushion that could allow health care workers to stay home when they are ill and help curb the spread of the pandemic. However, gaps in the law leave many workers without access, including 17.7 million health care workers. Health care workers without access to other types of paid leave may find it even more difficult to take time off work. Lack of paid sick leave could result in workers being forced to choose between going to work while they have symptoms and staying home without pay. Mediareportshave indicated that some health care workers are feeling the impact of the lack of access to emergency paid sick leave, with some worrying how they will pay their bills if they get sick with coronavirus and need to take time off work to recover.
New York’s lawsuit argues that the Department of Labor unlawfully allows for exemption of health care and emergency response workers. Additionally, the HEROES Act, passed by the House of Representatives in May 2020, attempts to close many of the gaps in access to emergency paid sick leave by extending the requirement to private firms with 500 or more employees and by removing the exemption for health care providers and emergency responders. These changes, if implemented, may make it easier for sick workers to stay home without losing pay and may help protect the others from exposure to COVID-19.
Methodology
This analysis is based on KFF analysis of the 2019 Community Population Survey Annual Social and Economic Supplement. We include self-employed workers, which make up about 9% of the workforce, and workers in the private sector, state and local governments, and the federal government. We define the health care and emergency response workforce as all individuals who earned at least $1,000 during the past year and indicated that their job was in one of the Census codes listed in Table 2. Excluded workers are those who work for a private firm with 500 or more employees and exempted workers are those who work in the health care or emergency response industries. Looking at industry rather than occupation allows for analysis that more closely resembles the broad exemptions as defined by the DOL, though this list does not include auxiliary industries necessary for the operation and maintenance of health care and emergency response entities, which may also be exempted. We did not include the offices of dentists, chiropractors, optometrists, or ‘other’ health practitioners, which employ an additional 1.4 million workers.
Table 2: Industry Classification Codes
Health Care
Census Code
Description
2190
Pharmaceutical and medicine manufacturing
3960
Medical equipment and supplies manufacturing
7970
Offices of physicians
8090
Outpatient care centers
8170
Home health care services
8180
Other health care services
8190
Hospitals
8270
Nursing care facilities
8290
Residential care facilities, without nursing
Emergency Response
8370
Individual and family services
8380
Community food and housing, and emergency services
9470
Justice, public order, and safety activities
SOURCE: Current Population Survey Annual Social and Economic Supplement, 2019. Codebook Appendix A.
Our estimates are based on 2019 employment data. In May 2019, 6 million people were unemployed. In May 2020, 21 million people were unemployed. ↩︎
In August 2020, the U.S. District Court for the Southern District of N.Y. ruled in favor of New York and in September 2020, the DOL amended the regulation to more narrowly define ‘health care worker.’↩︎
CA, CO, NY, OR, and WA. In CA: Long Beach, Los Angeles City and Co., Oakland, Sacramento City and County, San Francisco, San Jose, and Santa Rosa. San Mateo and Sonoma Counties have temporary emergency paid sick leave laws that are not included here because they only apply to certain employers in unincorporated parts of the county. In other states: Goshen, IN, Wilmington, NC, Philadelphia, PA, Burlington, VA, and Seattle, WA. Source: KFF analysis of A Better Balance Emergency Paid Sick Leave Tracker. Updated Oct. 2020. ↩︎
Low-wage refers to workers in the bottom 25% of earners, or less than $22,000 annually. ↩︎
Since the COVID-19 pandemic first surfaced in the United States, the number of cases and deaths in long-term care (LTC) facilities has been rising. As of June 4, 2020, over 43,000 COVID-19 related resident and staff deaths have been reported in nursing homes and other long-term care facilities, which is a conservative estimate because not all states publish these data. Among 41 states reporting COVID-19 LTC data at the state level, long-term care facility residents account for 50% or more of all COVID-19 deaths in 27 states. The increase in deaths among long-term care facility residents and staff has become an urgent concern for federal and state policymakers, the long-term care industry, family members of residents, residents themselves, and the general public.
In response to these concerns, on March 13, 2020, the Centers for Medicare & Medicaid Services (CMS) released guidance to limit the spread of the novel coronavirus to nursing home residents and staff, pertaining to visitors and staff screening. On April 2, CMS released guidance recommending universal use of facemasks by nursing home staff, and use of full Personal Protective Equipment (PPE) in facilities with known or suspected COVID-19 cases. As of May 8, nursing facilities are also required by CMS to report COVID-19 cases and deaths to the Centers for Disease Control and Prevention (CDC), and on May 18, CMS released guidance for states related to reopening nursing homes.
Notably, the CMS guidance and reporting requirements apply specifically to nursing facilities that fall under federal regulatory purview, leaving it to states to establish standards for assisted living facilities (ALFs) and other congregate living facilities. Assisted living facilities are home to over 800,000 mostly frail, elderly residents, who also face elevated risk of severe illness if they contract COVID-19, according to the CDC. While a great deal of attention has been paid to efforts to prevent and contain outbreaks of COVID-19 in nursing homes, assisted living facilities have been largely overlooked.
This analysis examines how states are regulating assisted living facilities in response to the COVID-19 pandemic, based on state-issued guidance for assisted living facilities on three key measures identified by CMS pertaining to visitors to facilities, daily staff screening, and universal use of PPE by facility staff, for each of the 50 states and DC. In addition, we tally state-level data on COVID-19 cases and deaths in assisted living facilities among states reporting such data as of June 8, 2020. The estimates reported here represent a subset of the COVID-19 cases and deaths data for long-term care facilities overall, as reported in other KFF analyses. (See Methods for details).
Key Takeaways
Ten states impose restrictions on assisted living facilities that are identical to those established by CMS for nursing facilities, i.e., prohibit visitors, require staff screening, and require staff use of PPE.
A majority of states prohibit visits to assisted living facilities (26 states plus DC) but recommend rather than require daily staff screening (27 states) and staff use of PPE (27 states).
Only 16 states report COVID-19 case and/or death data for assisted living facilities, either as a separate category (11 states) or combined with other long-term care facilities, other than nursing homes (5 states). Only 6 states report COVID-19 deaths occurring in assisted living facilities specifically.
Among the 11 states reporting COVID-19 cases for assisted living facilities specifically, a total of 7,703 cases among residents and staff have been reported. Among the six states reporting COVID-19 deaths for assisted living facilities specifically, a total of 643 deaths have been reported.
Variations in guidelines for assisted living facilities across states results in a patchwork of protections against COVID-19 that is likely to result in uneven effects across the country. However, given the paucity of state-reported data on case and death numbers in assisted living facilities specifically, the picture of disease incidence and mortality in these facilities is profoundly incomplete, and undoubtedly an undercount.
Guidance for Assisted Living Facilities Related to COVID-19 Varies across States
We found significant variation in COVID-19 guidance issued to assisted living facilities across states related to visitors, staff screening, and staff use of PPE.
Ten states impose restrictions on assisted living facilities which are identical to those established by CMS for nursing facilities, while other states are mixed in whether they require or recommend adherence to the guidelines in one or more of these areas (Table 1). A handful of states have not issued any guidance in one or more of these areas as of June 1, 2020, including one state (South Dakota) with no guidance issued in any of the three areas.
Visitors. More than half of all assisted living facilities in states and DC prohibit visitors (26 states plus DC), while 21 states recommend that assisted living facilities prohibit visitors, and two states provide no guidance on visitation to assisted living facilities (Figure 1).
Staff screening. More states recommend than require daily screening of staff for illness in assisted living facilities: 27 states recommend, and 17 states plus DC have this requirement. Six states have not issued guidance related to staff screening.
Use of personal protective equipment. More states recommend rather than require staff to use PPE in assisted living facilities: 27 states recommend, and 16 states plus DC require. Seven states have issued no guidance related to PPE use.
Figure 1: More Than Half of States and DC Prohibit Visitation to Assisted Living Facilities To Curb Coronavirus Infections; More Recommend Rather Than Require Screening and Use of PPE in ALFs
Relatively Few States Report COVID-19 Cases and Deaths Separately for Assisted Living Facilities
Our analysis shows that, as of June 8, 2020, 16 states report COVID-19 data for assisted living facilities, including 11 states that report data for assisted living facilities as its own category [CO, CT, FL, MA, MS, ND, NV, OH, RI, TX, UT] and five states that report COVID-19 data for assisted living facilities with congregate settings other than nursing homes, which are separately reported [CA, LA, NC, NY, SC]. Our analysis does not include data for the 23 states and DC that do not report COVID-19 data for assisted living facilities separately from nursing facilities; seven states that report data for nursing facilities, but not for assisted living facilities; and four states that do not report any state-level data.
COVID-19 Cases in Assisted Living Facilities
Among the 11 states [CO, CT, FL, MA, MS, ND, NV, OH, RI, TX, UT]reporting COVID-19 cases for assisted living facilities specifically, a total of 7,703 cases among residents and staff have been reported. This total includes 3,829 cases among residents, 1,135 cases among staff, and 2,739 cases among residents and staff not separately reported in two states [MA and UT].
Among the four states [CA, LA, NC, SC] that report COVID-19 cases occurring in a non-nursing facility category that includes, but is not limited to, assisted living facilities, a total of 3,386 COVID-19 cases have been reported among residents and staff. This includes 2,419 cases among residents and 967 cases among staff, with only three states reporting on the latter.
Covid-19 Deaths in Assisted Living Facilities
Among the six states [CO, CT, NV, RI, TX, MS] reporting COVID-19 deaths for assisted living facilities specifically, a total of 643 deaths have been reported. This includes 642 deaths among residents and one death among staff, with only two states (CO and NV) reporting on the latter.
Among the five states [CA, LA, NC, NY, SC] that report COVID-19 deaths in non-nursing facilities including, but not limited to, assisted living facilities, a total of 840 deaths have been reported. This includes 810 deaths among residents and 30 deaths among staff, with only three states reporting on the latter.
Discussion
With national attention focused on the rising number of COVID-19 deaths in nursing homes, this analysis takes a closer look at protections and COVID-19 cases and deaths in assisted living facilities. We found significant variation across states in assisted living facility regulations related to visitation, daily staff screening, and use of PPE, and a dearth of states reporting COVID-19 cases and deaths among residents and staff in these facilities specifically. In the majority of states, regulatory measures meant to protect assisted living facility residents and staff from COVID-19 infection are currently far less stringent than federal recommendations for nursing facilities. In the absence of uniform surveillance and reporting, little is known about the extent to which facilities are adhering to state guidelines or whether states are monitoring their enforcement.
In an effort to control outbreaks in LTC facilities, some states have instituted universal testing of nursing facility residents and staff. While some states, such as Connecticut and New York, now mandate universal testing of staff in both nursing homes and assisted living facilities, some state and national LTC associations are reporting that fewer states are testing both assisted living facilities residents and staff in addition to nursing facility residents and staff. Widespread adoption of universal testing in all LTC facilities and other congregate settings may not be possible, due to limited testing capacity nationwide. While regular screening of residents and staff for fever and respiratory symptoms is now a matter of protocol in most LTC facilities, screening only picks up symptomatic COVID-19 cases, whereas testing can identify asymptomatic carriers as well.
With many governors now moving toward relaxing restrictions that aim to slow the spread of coronavirus infections, some state guidance issued for assisted living facilities will soon expire (unless renewed). For example, executive orders issued by Michigan and Alabama will expire on June 26 and July 3, 2020, respectively. Other states, such as Arizona and North Carolina, have mandated that guidance pertaining to LTC facilities generally will expire upon termination of the state’s emergency declaration related to COVID-19. Ohio recently announced that visits to assisted living facilities will be allowed outdoors starting June 8, but visitors to nursing facilities will remain prohibited.
In terms of reporting of COVID-19 cases and deaths in long-term care facilities, the absence of uniform state reporting requirements for assisted living facilities makes it challenging to contextualize the numbers from the 16 states currently reporting such data separately from other types of long-term care facilities. For example, while CMS now reports the total number of resident beds in each nursing facility with COVID-19 cases, only three out of the 16 states reporting case and death data for assisted living facilities separate from nursing homes (Massachusetts, Connecticut, and North Dakota) also report the number of beds in each facility. This makes it challenging to examine the relationship between facility capacity and number of COVID-19 cases and deaths in assisted living facilities. Furthermore, total COVID-19 case and death counts for assisted living facilities would undoubtedly be much larger if data were released by all states, as CMS now requires for nursing homes nationwide.
This analysis confirms a patchwork state-based regulatory approach to establishing measures to limit the spread of coronavirus infection among assisted living facility residents and staff, and in reporting COVID-19 cases and deaths in assisted living facilities. This situation mirrors a larger national trend in the COVID-19 response, whereby some states have taken more aggressive actions than others and the federal government assumes a “backup” role. This state-by-state approach to the COVID-19 pandemic may result in uneven rates of illness, hospitalizations, and mortality among assisted living residents and staff across the country.
Methods
State Regulation of Assisted Living Facilities and COVID-19
To examine how states are regulating assisted living facilities in response to the COVID-19 pandemic, we collected and analyzed state-issued guidance for ALFs for each of the 50 states and District of Columbia. This information was posted in a variety of online locations across states: some regulatory guidance pertaining to long-term care facilities was posted on state-run websites dedicated to COVID-19-specific information and resources; some was posted on state Department of Health websites, some was stored on Governors’ websites, and some was posted on the websites of other state regulatory agencies, such as the Department of Human Services. State regulatory information was collected via Google keyword searches as well as targeted searches of government websites as listed above.
Regulatory information pertaining to ALFs was also conveyed in a variety of formats, including executive orders or press releases issued by state Governors’ offices, orders or guidance issued by state Public Health departments or other state regulatory agency (such as the Department of Human Services), or information or guidance appearing on state-run websites housing COVID-19-related information.
State regulatory information pertaining to ALFs was initially collected on a rolling basis via online search as detailed above between March 26 and April 20, 2020, and subsequently updated between May 29 and June 1, 2020, and is current as of June 1. Although best efforts were made, due to the wide variation in online location, presentation, and formatting of regulatory information pertaining to ALFs between states, it is possible that the research team inadvertently neglected to include some information, or was not aware of an update to information already collected. In some states, the regulatory guidance was directed to “long-term care” settings generally, in which case it was assumed to apply to ALFs.
State Reporting of COVID-19 Data for Assisted Living Facilities
To collect data on COVID-19 cases and deaths in ALFs, we reviewed public reporting of COVID-19 surveillance data displayed on applicable state-run websites in all states, and collected numbers of cases and deaths for ALFs in states where this data is reported separately from cases and deaths in LTC facilities generally, in order to exclude nursing facilities from our analysis. Not all states report cases and/or deaths in LTC facilities, and some only report this data for nursing homes. State data on COVID-19 cases and deaths was collected between June 5 and June 8, 2020, and is current as of June 8.
We included COVID-19 case and death data for states (n=11) that reported for ALFs specifically, as well as other states (n=5) that report ALF data separately from nursing facilities, but do so within a larger category that includes ALFs along with other non-nursing home facility types. The facility categories used by states reporting for ALFs under a broader classification are: Residential Care Facilities for the Elderly, Residential Care Facilities, Community Residential Care Facilities, Adult Residential Facilities, and Adult Care Facilities. We include these congregate facilities because assisted living facilities represent a large share of their total residents in many states. We intentionally exclude states reporting in broader categories that include nursing facilities because these numbers are reported to CMS separately and our goal is to understand the impact of COVID-19 in assisted living facilities to the extent this is possible with current data limitations.
Notably, not all states report data for both cases and deaths; some report only cases and others report only deaths. Not all states report for staff and residents; some report cases and/or deaths for residents only, and some states (n=2) report aggregate cases for residents and staff. Most states in our analysis (n=12) report cumulative case and death data, however four states (Florida, Mississippi, Utah, and North Dakota) report only active cases. States differ slightly in how many cases constitute a facility “outbreak” which triggers reporting – some states report data for facilities with just one active case, others begin reporting when two or greater cases are reported by facilities. States also differ in whether they report suspected COVID-19 cases and deaths, in addition to confirmed cases – some only report cases confirmed via diagnostic test. For the purpose of this analysis, we have included both suspected and confirmed COVID-19 cases and deaths reported. Additionally, four states (Massachusetts, Rhode Island, Utah, and California) report ranges of cases and/or deaths, versus specific counts. For these states, we used the median of the reported range, or 5 in the case of “5 or above” reported, and 31 for “greater than 30.”
Tables
Table 1: Guidance for Assisted Living Facilities Related to COVID-19, by State (Including DC)(as of June 1, 2020)
Visitation
Screening
Personal Protective Equipment
Alabama
Prohibit
Require
Require
Alaska
Recommend prohibit
Recommend
Recommend1
Arizona
Recommend prohibit
Require
Require
Arkansas
Prohibit
Require
Recommend
California
Prohibit
Recommend
Require
Colorado
Prohibit
Require
Require
Connecticut
No guidance
No guidance
Recommend
Delaware
Recommend prohibit
Recommend
Recommend2
District of Columbia
Prohibit
Require
Require
Florida
Prohibit
Require
Require
Georgia
Prohibit
Require
Require
Hawaii
Recommend prohibit
Recommend
Recommend
Idaho
Prohibit
Recommend
Recommend
Illinois
Recommend restrict
Require
Require
Indiana
Recommend prohibit
Recommend
Recommend
Iowa
Recommend prohibit
Require
Recommend
Kansas
Recommend prohibit
Recommend
Recommend
Kentucky
Recommend prohibit
Recommend
Recommend
Louisiana
Prohibit
Recommend
Recommend1
Maine
Recommend prohibit
Recommend
Recommend
Maryland
Recommend prohibit
Recommend
Recommend
Massachusetts
Prohibit
Recommend
Recommend
Michigan
Prohibit
Require
Require
Minnesota
Recommend prohibit
Recommend
Recommend
Mississippi
Prohibit
No guidance
Recommend
Missouri
Prohibit
Require
Require
Montana
Prohibit
Require
No guidance
Nebraska
Prohibit
No guidance
Recommend
Nevada
Recommend prohibit3
Recommend3
Recommend3
New Hampshire
Prohibit
Recommend
Require
New Jersey
Recommend prohibit
Recommend
Require
New Mexico
Prohibit
Recommend
Require
New York
Prohibit
Require
Require
North Carolina
Recommend prohibit
Recommend
Require
North Dakota
Recommend prohibit
Recommend
Recommend
Ohio
Prohibit4
Recommend
No guidance
Oklahoma
Prohibit
Recommend
No guidance
Oregon
Prohibit
Require
No guidance
Pennsylvania
Recommend prohibit
Recommend
Recommend
Rhode Island
Prohibit
No guidance
No guidance
South Carolina
Prohibit
Recommend
Recommend
South Dakota
No guidance
No guidance
No guidance
Tennessee
Prohibit
Recommend
Recommend5
Texas
Prohibit
Require
Require
Utah
Recommend prohibit
No guidance
Recommend
Vermont
Recommend prohibit
Require
Recommend
Virginia
Prohibit
Require
Require
Washington
Prohibit
Require
Recommend
West Virginia
Recommend prohibit
Recommend
Recommend
Wisconsin
Recommend prohibit
Recommend
No guidance
Wyoming
Recommend prohibit
Recommend
Recommend
NOTE: Blue highlights indicate states with requirements for ALFs that match CMS requirements for nursing facilities. Gray highlights indicate states with no guidance in specific area. 1PPE recommended for use with symptomatic residents. 2Recommend for staff providing direct care. 3Per official from the Division of Public and Behavioral Health, Nevada Dept. of Health and Human Services. 4The Governor announced a plan to lift the prohibition on visitation beginning on June 8, 2020 . 5PPE recommended when case identified.SOURCE: KFF analysis of state and DC long-term care facility guidance related to COVID-19; detailed methods available in KFF brief, “Under the Radar: States Vary in Regulating and Reporting COVID-19 in Assisted Living Facilities.”
Table 2: Number of States and DC With Specific Guidance for Assisted Living Facilities Related to COVID-19(as of June 1, 2020)
Visitation
Prohibit
27
Recommend prohibit
21
Recommend restrict
1
No guidance
2
Screening
Require
18
Recommend
27
No guidance
6
Staff use of personal protective equipment
Require
17
Recommend
27
No guidance
7
NOTE: Analysis includes 50 states and DC.SOURCE: KFF analysis of state and DC assisted living facility guidance related to COVID-19; detailed methods available in KFF brief, Under the Radar: States Vary in Regulating and Reporting COVID-19 in Assisted Living Facilities.”
Table 3: State Reporting of Assisted Living Facility Cases and Deaths Related to COVID-19(as of June 8, 2020)
Active or Cumulative Cases
Resident Cases
Resident Deaths
Staff Cases
Staff Deaths
Resident and Staff Cases
Assisted Living Facilities with known Cases
Number of states reporting
13
11
9
5
2
16
TOTAL
6,248
1,452
2,102
31
2,739
1,261
California1
Cumulative
1,168
472
682
30
–
96
Colorado
Cumulative
500
139
368
0
–
50
Connecticut
Cumulative
1,041
337
–
–
–
81
Florida
Active
758
–
447
–
–
281
Louisiana2
Cumulative
630
91
–
–
–
122
Massachusetts
Cumulative
–
–
–
–
2,726
206
Mississippi
Active
14
0
17
–
–
6
Nevada
Cumulative
98
23
44
1
–
28
New York3
Cumulative
–
169
–
–
–
58
North Carolina4
Cumulative
535
62
225
0
–
40
North Dakota
Active
13
–
10
–
–
10
Ohio
Cumulative
508
–
249
–
–
84
Rhode Island
Cumulative
161
29
–
–
–
8
South Carolina5
Cumulative
86
16
60
0
–
41
Texas
Cumulative
736
114
–
–
–
145
Utah
Active
–
–
–
–
13
5
NOTE: 1Cases and deaths in Residential Care Facilities for the Elderly. 2Cases and deaths in Adult Residential Facilities. 3Deaths in Adult Care Facilities. 4Cases and deaths in Residential Care Facilities. 5Cases and deaths in Community Residential Care Facilities.SOURCE: KFF analysis of state assisted living facility cases and deaths related to COVID-19; detailed methods available in KFF brief, “Under the Radar: States Vary in Regulating and Reporting COVID-19 in Assisted Living Facilities.”