KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
A new chart collection explores the impact of the coronavirus pandemic on the U.S. health care workforce, and finds that between February and April 2020, nearly 1.5 million health care jobs were lost. While more than 300,000 health services jobs were recovered in May 2020, mainly in dental offices, employment in some health care settings continued to decrease.
The rise in health care unemployment follows a sharp decline in utilization and revenue for non-emergency services. Many providers delayed or canceled appointments for routine care and elective procedures amid concerns that COVID-19 patients would overwhelm the health system; others closed their facilities entirely. Many patients also chose to forgo non-emergency care, presumably due to stay-at-home orders issued by local governments and fear of contracting the virus in health care settings.
Workers in ambulatory health care settings, like dental and physician’s offices, have been particularly hard-hit, accounting for more than half of total health care job losses between February and May 2020.
The chart collection also includes data on gender disparities and geographic variation in health care job loss, as well as a breakdown of job loss by sector.
The collection is part of the Peterson-KFF Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.
For more data, analysis, polling and journalism on the COVID-19 pandemic, visit our special resource page on kff.org.
In response to the widespread concerns about the high numbers of coronavirus cases and deaths in long-term care (LTC) facilities, CMS recently implemented new COVID-19 data reporting requirements for all federally certified nursing facilities. The newly-released federal data builds on state-reported data that has been included in many, but not all, states’ regular coronavirus reporting for several weeks. However, preliminary analysis indicates that the federal data will not reveal the full extent of the crisis in LTC facilities, as most states are reporting higher numbers of cases and/or deaths than appear in the federal data. This discrepancy is most likely due to the fact that the federal data only requires states to report cases and deaths after May 8th and is limited to cases and deaths in nursing facilities. State-reported data primarily reports cumulative cases and deaths across multiple types of long-term facilities. However, not all states have reported data, and data are not easily comparable across states. This brief explores the extent to which state and federal data on coronavirus in LTC facilities differ and discusses the likely causes for these differences. While federal reporting offers promise for analyzing the intersection of COVID-19 and LTC facilities, state data will continue to play a role in highlighting the scope of the crisis across facility types and trends in COVID-19 within these facilities over time.
Comparing federal and state data on COVID-19 and LTC
The federal government implemented a new reporting system for certified nursing facilities, requiring facilities in all states to report coronavirus cases and deaths among residents and staff. The federal data aims to produce current and uniform facility-level data for all states for both residents and staff, making it more comparable across states than the state-published data (Table 1). According to the federal requirements, nursing facilities must report data on confirmed coronavirus cases and deaths for residents and staff in all certified Medicare skilled nursing facilities and Medicaid nursing facilities. These data are to be reported at least once a week to the CDC using a standardized reporting portal called the CDC National Healthcare Safety Network (NHSN). This data is then shared with CMS and publicly reported. Facilities must also report outbreaks to residents, representatives, and families by next calendar day at 5pm. These notifications must follow a single confirmed infection in the facility, or 3+ residents and/or staff with respiratory symptoms that occur within 72 hours of each other.
Federal data released by CMS also includes additional information on facility resources and characteristics relevant to COVID-19 (Table 1). In addition to cases and deaths, CMS reports suspected coronavirus infections among residents and staff, total non-COVID deaths, personal protective equipment (PPE) supplies, ventilator capacity and availability, bed count, resident census, and testing access, among other variables. Many variables reported in the federal data are not reported by most states, making the federal data valuable for understanding more details about the crisis on the ground.
However, the federal data is not cumulative, which understates the full extent of the pandemic. The federal data does not require states to report data prior to May 8th, though facilities may report cumulative data prior to that period in their first reporting if they wish. Most state-published data report cumulative cases since the onset of the public health crisis (Table 1). Given high numbers of cases and deaths in nursing facilities as far back as March and April, the requirement to report as of May 8th may exclude a large number of cases that occurred during the “peak” of the curve in many states.
Additionally, federal reporting does not capture cases and deaths in other congregate settings, including assisted living facilities and other LTC settings. In contrast, most states include data on cases and deaths in other types of LTC facilities, including assisted living facilities, intermediate care facilities, group homes, and others (Table 1). Analysis of state data shows a notable number of cases and deaths in other LTC facilities.
Federal and state data also differ in their inclusion of recovered or resolved cases and outbreaks and suspected cases (Table 1). Seventeen states report data on recovered cases and resolved outbreaks, which is not reported in the federal data. Recovered cases refer to residents who previously tested positive for the virus, but have since recovered. Resolved outbreaks refer to facilities where there are no active cases for a specific period of time (in most cases, 14 days). Several of these states have also flagged facilities that are no longer undergoing an active outbreak. Understanding which facilities have successfully contained outbreaks can be helpful in understanding successful infection control policies. The number of recovered cases is also a valuable measure to understand the extent of the immediate crisis in facilities. Federal data does include suspected cases or deaths, while most states do not report this data.
Table 1: State and Federal Data Reporting on COVID-19 Cases and Deaths in Nursing Facilities
State Reporting (46 states + DC)
Federal Reporting(50 states + DC)
Number of states with publicly available data on cases
42 states + DC
50 states + DC
Number reporting facility-level data on cases
29 states + DC
50 states + DC
Number of states with publicly available data on deaths
40 states + DC
50 states + DC
Number reporting facility-level data on deaths
26 states + DC
50 states + DC
People included in case and/or death counts
Residents + staff: 30 states + DCResidents only: 9 statesUnspecified: 4 states
Residents + staff
Types of long-term care facilities included
Multiple LTCFs: 44 statesNursing facilities only: 2 states + DC
All certified Medicare skilled nursing facilities and Medicaid nursing facilities
Time period reported
Cumulative: 41 states + DCActive: 5 states
Varies, but at a minimum weekly cases and deaths starting May 8th
Frequency of data update
Daily: 23 states + DCAt least once/week: 18 statesUnclear: 5 states
Weekly
Includes suspected cases or deaths
8 states
50 states + DC
Includes recovered cases or resolved outbreaks
17 states
0 states
As of May 31st1 , the federal government is reporting about one-third fewer cases and deaths in long-term care facilities compared to the state data, reflecting differences in the scope of information included. Among the set of states for which there is both state and federal data, the federal data reports 37% fewer cases and 33% fewer deaths than state data. State data reports about 43,700 deaths for the 40 states reporting this data, while the federal data reports about 29,200 deaths among the same 40 states. State data reports about 217,400 cases for the 43 states reporting this data, while the federal data reports about 137,000 cases among the same 43 states.
Even including all states in the federal data, the federal data for 50 states plus DC is reporting less than three quarters of what the state data for 44 states reports nationally. Federal data reports 32,500 deaths and 155,700 cases among all states – about one-quarter fewer than the cases and deaths totals reported by states.
Five states report higher cases in federal data (Arkansas, Delaware, Michigan, North Dakota, and Wyoming); four states report higher deaths in federal data (Mississippi, Oklahoma, Oregon, and West Virginia). In most of these cases, the state data may be lower because it includes only resident (not staff) cases (AR, DE, MI) or only active cases (ND, MI, OR), and/or is based on a very small number of facilities in which a minor case undercount can sway percentages (WY). Other states, such as Oklahoma and West Virginia, may have data errors in the federal data, as the federal data currently reports a greater number of COVID deaths in nursing facilities than COVID deaths in the whole state. All other states report more cases and/or deaths than CMS reports. Most likely, this discrepancy is due to the reporting period (and whether cases/deaths prior to May 8th are reported) and types of facilities reflected in federal and state-published data.
Differences in the number of cases and deaths between the federal and state data lead to different conclusions about the extent to which the crisis is concentrated in LTC facilities. These differences are largely driven by the differences in time period and types of facilities reflected in the federal and state-published data. Based on the numbers reported in the state and federal data, as well as the total number of cases and deaths from our daily cases/deaths tracker, we calculated the share of total COVID cases and deaths in the state that can be attributed to LTC facilities. State-reported data shows that LTC facility cases account for 16% of coronavirus cases across 43 states, while the federally reported data shows that nursing facility cases account for 9% of cases. State-reported data shows that LTC facility deaths account for 45% of coronavirus cases across 41 states, while the federally reported data shows that nursing facility deaths account for 31% of deaths. This comparison varies across states. The following interactive maps show state-by-state comparisons of the share of total cases and deaths that can be attributed to LTC/nursing facilities reported in the state and federal data, respectively.
Notably, the federal government reports more COVID-19 deaths in Oklahoma and West Virginia’s long-term care facilities than total COVID deaths in those states as of May 31st. The analysis caps the share of deaths that can occur in LTC or nursing facilities at 100% of all COVID deaths in those states.
Interactive 1:
Interactive 2:
Looking Ahead
While early state reports on cases and deaths in LTC facilities were crucial in highlighting the scope of the problem in those settings and targeting policy to these hot spots, state-reported data has several limitations. Data on cases and deaths in long-term care facilities is still not reported for all states, and even among states reporting, is not directly comparable. Moreover, the state data generally does not include the additional indicators available in the federal data, including information on PPE availability and staffing shortages, which can help target policy responses.
Federal data offers great promise to address some of these limitations. At the same time, since the federal data was released, there have been severalreports of inaccurate data, including issues of reporting fatalities where there were none and undercounting fatalities in facilities with known fatalities. The federal data also reports two states that report a greater number of COVID deaths in long-term care facilities than total COVID deaths in the state. Analysis of facility-level data, paired to account for timing and case inclusion criteria, can shed light on the scale of data discrepancies between state and federal data. To some extent, if data errors in the federal data are present, it is unsurprising given the inherent challenges with setting up a new data reporting system. Fielding a large-scale, nationwide data collection effort can often take months, or even years. Over time, it is possible that data errors will be resolved in the federal data. However, the federal government has limited levers to require reporting for LTC facilities it does not regulate, and state data will continue to be valuable to understanding the full scope of the COVID-19 crisis in congregate settings.
Overall, given the fast-moving nature of the COVID-19 crisis and need for accurate, timely data, both the federal and state-reported data on COVID-19 and LTC will likely play an important role in understanding the trajectory of the pandemic.
Federal data is as of May 31st. The majority of state-reported data (41 states) is as of between May 27th and June 4th. ↩︎
News Release
Nearly One in Four Workers are at High Risk of Serious Illness with COVID-19, Posing Challenges for Employers as They Reopen
A new KFF analysis finds nearly one in four workers (24%) are considered at high risk of serious illness if they get infected by the novel coronavirus, highlighting the challenges that businesses, public offices and other employers face as they move toward reopening.
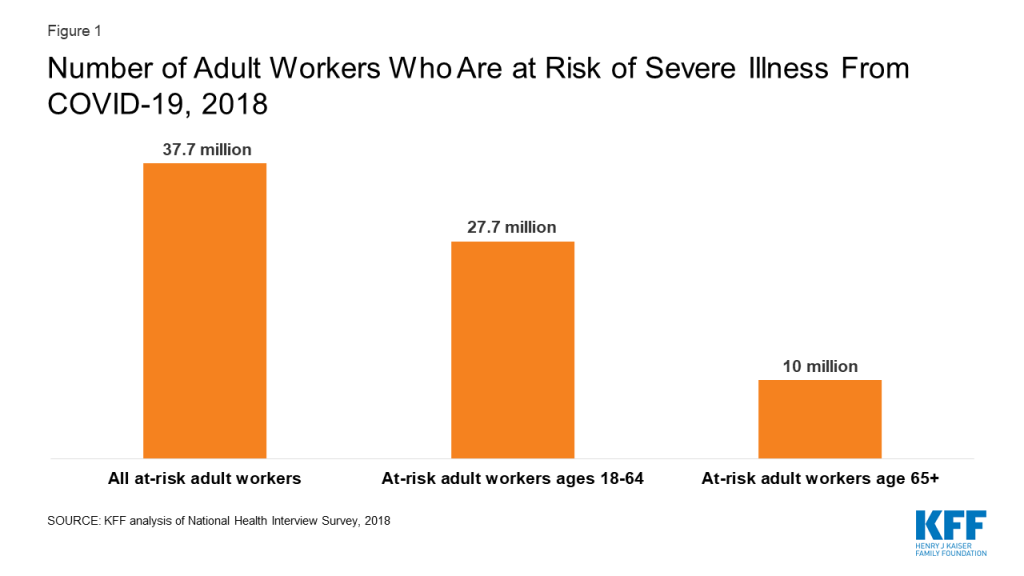
The analysis estimates 37.7 million workers (based on their work status in 2018) are at high risk of serious illness from COVID-19. This includes 10 million who are at least 65 years old and an additional 27.7 million who have pre-existing medical conditions that the Centers for Disease Control and Prevention (CDC) says put people at higher risk for severe illness from COVID-19. Many of these people may be out of work right now or working remotely, but would be at greater risk if they had to return to in-person work.
“As an employer, I know that employers are largely on their own to develop policies to reopen safely,” KFF President and CEO Drew Altman said. “These data suggest employers should take into account the higher risk some workers will face, allowing them to work at home where possible, to be tested and to minimize their risks if they return to work.”
The analysis also estimates that 12 million more at-risk adults who do not work themselves live in households with workers. For this group, indirect exposure could be just as serious of a risk as going to work themselves.
The estimates are based on KFF’s analysis of data from the 2018 National Health Interview Survey (NHIS). Workers deemed at high risk based on the CDC’s criteria include those who are at least 65 years old, as well as those with diabetes, heart disease, chronic obstructive pulmonary disease, asthma, a body mass index above 40, or have a functional limitation related to cancer.
More data, analysis, polling and journalism related to the COVID-19 epidemic is available at kff.org.
As states and employers continue to reopen businesses and public offices, important decisions are being made about how to keep workers safe from becoming infected with coronavirus at work or on their commutes to and from their homes. In addition, outbreaks of coronavirus at some businesses, such as food processing facilities and long-term care facilities, highlight the risks faced by essential workers who have continued to work outside the home. Safety considerations will be particularly important for those workers at greater risk of becoming seriously ill if they become infected with coronavirus. This caution applies to older workers in general, as well as to younger workers with certain medical conditions that put them at higher risk of serious illness if they become infected.
We use the National Health Information Survey (NHIS) to look at how many adult workers1 are at increased risk of severe illness if infected with coronavirus, based on risk factors identified by the Centers for Disease Control and Prevention (CDC). These risk factors include having diabetes, chronic obstructive pulmonary disease (COPD), heart disease, a body mass index (BMI) above 40, moderate to severe asthma, and a functional limitation due to cancer. All workers 65 and older also are considered at higher risk. The approach is similar to our prior work identifying at-risk adults and is described in more detail in the Methods.
Who are the At-Risk Workers?
We find that over 90 million adults are at greater risk for severe illness from COVID-19 due to underlying health conditions or age. Of these at-risk adults, we estimate that about 37.7 million were employed at a job or business in the prior year, including 10 million people age 65 and older (19.5% of adults age 65 and older, all of whom are considered at greater risk) and 27.7 million non-elderly adults (Figure 1). These at-risk workers comprise 24% of all adult workers.
Figure 1: Number of Adult Workers Who Are at Risk of Severe Illness From COVID-19, 2018
Among non-elderly adult workers, at-risk workers are older on average than non-elderly workers who are not at risk (average age of 45 versus 40), reflecting the fact that risk status chronic conditions or poor health increases with age. One-half of at-risk non-elderly adult workers are women, which is higher than the percentage (46%) of non-elderly adult workers who are not at risk.
Large shares of at-risk workers — 86% of non-elderly adult at risk workers and 61% of age 65 and older at-risk workers — work full-time (at least 35 hours per week). They have substantial connection to work and may face economic difficulties remaining absent from their jobs even if safety is a question.
The average annual earnings of non-elderly adult at-risk workers was $48,400 in 2018, somewhat lower than the average annual earnings for non-elderly adults workers who were not at risk ($51,900). The median annual earnings was $40,000 for both at-risk and not-at-risk adult non-elderly workers. One-quarter of non-elderly adult at-risk workers had annual earnings of less than $21,100.
The average annual earnings of workers age 65 and older was $49,100 in 2018; median annual earnings were $37,000. One-quarter of workers age 65 and older had annual earnings of less than $17,300.
The importance of at-risk workers’ earnings to themselves and to their families may put added pressure on them to continue to work or return to work even if their safety may be compromised. Not surprisingly, among both non-elderly at-risk workers and workers age 65 and older who live alone, earnings on average account for a very large share of their total annual incomes: 94% among non-elderly at-risk workers and 72% among older at-risk workers in 2018. For those living with others, the at-risk worker’s earnings on average comprised a substantial share of family income. Among non-elderly at-risk workers, their earnings accounted for 57% of family income in families of two or three and 50% in larger families. Among workers age 65 and older who live with others, the older worker’s earnings on average comprised 48% of family income.
Discussion
Most people, including at-risk workers, cannot afford to stay away from work for long periods of time. Some people at risk have likely continued to go to work outside their homes due to the nature of their jobs, perhaps as essential workers. Others may have been accommodated by remote work, which has taken hold to a remarkable degree but is not available to all workers. Some have lost their jobs or may be at risk of losing them. As more workplaces reopen there will be increasing pressures for all workers, including those at higher risk, to return to jobs or seek new jobs outside of their homes. This will raise issue both for employees concerned about their safety and for employers concerned about how to keep these workers safe.
In addition to at-risk people who are workers themselves, there are millions more at-risk adults who themselves are not workers but who live with workers. This indirect exposure could be just as serious of a risk as going to work themselves. We estimate that an additional 12 million at-risk adults who are not workers themselves live with at least one full-time worker. This includes 6.5 million people age 65 and older and about 5.5 million at risk non-elderly adults. This is a conservative estimate because additional non-working at-risk adults live with people who work part time or who are in and out of the work force. The safety of these family members will need to be part of the considerations for employees and employers as businesses continue to refine safety protocols and others reopen their workplaces.
State and local governments and employers themselves are wrestling with how to reopen businesses in the safest ways possible, with risks particularly high for workers who have pre-existing that make them more vulnerable to severe illness from COVID-19. Employers, workers, and governments may need to consider flexible and creative approaches to balance safety and business needs, but with such large number of workers meeting vulnerability criteria, there will be a continuing tension between the economic pressures facing families and businesses and the health and safety of millions of people.
Methods
This analysis uses data from the 2018 National Health Interview Survey (NHIS) to look at the share of workers who would be at increased risk of becoming seriously ill if they become infected with COVID-19. The analysis is similar to our previous [work], where we used the Behavioral Risk Factor Surveillance Survey (BRFSS) to estimate the number of adults who would be at increased risk if they were infected with coronavirus. In that study, we found that about 21% of non-elderly adults have one more of five risk factors that the Centers for Disease Control and Prevention (CDC) have identified as increased risk factors for those infected with coronavirus. The factors we were able to analyze were having diabetes, chronic obstructive pulmonary disease (COPD), heart disease, a body mass index (BMI) above 40, and asthma. In addition, the CDC criteria consider all people over age 65 to be at increased risk. In this brief we use similar information from the 2018 National Health Interview Survey (NHIS) to look at the share and characteristics of adults with these risk factors who are in the workforce.
We use NHIS rather than BRFSS for this analysis because it has more information about the earnings, income and family characteristics of the at-risk population, providing a fuller picture of the economic circumstances of these workers. The sample adult file in NHIS contains information about all of the same health conditions that we used in the previous study, plus the person file has information that allows us to include people who report being functionally limited due to cancer; CDC includes people with compromised immune systems, such as people undergoing treatment for cancer, as being at higher risk of serious illness if infected with coronavirus. With NHIS we find that 22% of non-elderly adults have one or more risk factors for becoming seriously ill with COVID-19, essentially the same share as we calculated under BRFSS. Including those with a functional limitation due to cancer accounts for less than one-half percentage point of this estimate. We note that one downside of using NHIS is that state-level analysis is not possible.
As with BRFSS study, the analysis identifies non-elderly people with one or more risk factors, but in two steps. One pass excludes asthma and the other includes it, and we use only a portion (62%) of the people whose only risk factor is asthma. Unlike our BRFSS analysis, here we incorporate the proportion by assigning risk status to 62% of those whose only risk factor is asthma. The assignment is done by sampling from the asthma risk only group in a way that increases the likelihood of selection with age. (See Zein et al.)
The purpose of the analysis is to look at people who may have difficult avoiding or delaying work if their safety may be compromised; we therefore attempted to focus the analysis on those with a significant amount of work, which we defined as workers who earned $5,000 or more at a job or business during the previous year. This threshold includes 94% of non-elderly adults and 88% of people age 65 and older with any work in the previous year.
We imputed full-time or part-time status for some observations with missing values. NHIS provides a file that multiply imputes family income, earnings and work status for survey respondents. This results in cases in which employment status and earnings are imputed for people who did not otherwise report being employed. Although NHIS contains several questions about hours worked (either in the previous period or usually), these questions do not contain information for respondents who were imputed to be workers and to have earnings. We imputed part-time/full-time status based on their annual earnings, separately for workers under age 65 and those 65 and older. More specifically, for cases where we had information on earnings and hours worked, we calculated the relative proportions of part-time and full-time workers in several earnings groups. We then randomly imputed yes or no for full-time status for the missing cases, using the probabilities associated with their income levels.
We calculated the share of earnings to family income, segmented by family size. For this analysis, we wanted to calculate the ratio for each worker in order to determine the importance of that worker’s earnings to the family. Doing this can create issues in cases where earnings are larger than family income, which can result in very high ratios of earnings to income, which inflate the overall average. To limit the impact of these situations, we capped the ratio associated with any worker to 1 (a worker’s earnings can account for 100 percent of family income but not more than that). A second issue is that the family incomes for some workers with significant earnings can be very low or even zero. This was the case for a small number of observations of at-risk workers (between 6 and 12 unweighted cases had earnings of $5000 or more and family income of less than $1,000. We excluded those cases when we calculated the ratios.
A person is considered to be a worker if they were employed at a job or business in the previous year and had at least $5,000 in annual earnings. ↩︎
Every Friday, we’re recapping the past week in the coronavirus pandemic from our tracking, policy analysis, polling, and journalism.
Certain parts of the U.S. are seeing spikes in COVID-19 cases, possibly spurred by states easing social distancing measures and large gatherings over Memorial Day weekend. A KHN article from this week explains that specific areas of California and certain counties in every Southern state have become “hot spots.”
Total coronavirus cases in the U.S. are still climbing, and this week the cumulative total surpassed 2 million. There have been over 114,000 total confirmed deaths in the U.S.
Here are more of the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: This week, total cases worldwide passed 7.5 million – with an increase of approximately 878,000 new confirmed cases between June 4 and June 11. There were approximately 30,000 new confirmed deaths worldwide between June 4 and June 11, bringing the total to approximately 421,000 confirmed deaths.
U.S. Cases and Deaths: Total confirmed cases in the US passed the 2 million mark this week, with approximately 151,000 new confirmed cases between June 4 and June 11. There were approximately 5,600 new confirmed deaths this week, bringing the total to nearly 114,000 confirmed deaths in the US.
U.S. Tests: There have been over 21.9 million total COVID-19 tests with results in the United States —with about 3.1 million added since June 4. In the last seven days, 1.0% of the total U.S. population was tested.
Social Distancing: 51 states have eased at least one social distancing measure.
Stay At Home Order: Original stay at home order in 9 states, stay at home order eased or lifted in 36 states, no action in 6 states
Mandatory Quarantine for Travelers: Original traveler quarantine mandate in place in 10 states, traveler quarantine mandate eased or lifted in 15 states, no action in 26 states
Non-Essential Business Closures: Some or all non-essential businesses permitted to reopen (some with reduced capacity) in 46 states, no action in 5 states
Large Gatherings Ban: Original gathering ban/limit in place in 14 states, gathering/ban limit eased or lifted in 36 states, no action in 1 states
State-Mandated School Closures: Closed in 7 states, closed for school year in 36 states, recommended closure in 1 state, recommended closure for school year in 6 states, rescinded in 1 state
Restaurant Limits: Original restaurant closures still in place in 8 states, restaurants re-opened to dine-in service (some with reduced capacity) in 42 states, no action in 1 state
Primary Election Postponement: Postponement in 14 states, cancelled in 1 state, no postponement in 36 states
Emergency Declaration: There are emergency declarations in all 51 states.
Waive Cost Sharing for COVID-19 Treatment: 3 states require, state-insurer agreement in 3 states; no action in 45 states
Free Cost Vaccine When Available: 9 states require, state-insurer agreement in 1 state, no action in 41 states
States Requires Waiver of Prior Authorization Requirements: For COVID-19 testing only in 5 states, for COVID-19 testing and treatment in 6 states, no action in 40 states
Early Prescription Refills: State requires in 18 states, no action in 33 states
Premium Payment Grace Period: Grace period extended for all policies in 4 states, grace period extended for COVID-19 diagnosis/impacts only in 4 states, expired in 8 states, no action in 35 states
Marketplace Special Enrollment Period: Marketplace special enrollment period still active in 6 states, ended in 6 states, no special enrollment period in 39 states
Paid Sick Leave: 13 states enacted, 2 proposed, no action in 36 states
38 states overall have taken mandatory action expanding access to telehealth services through private insurers, including:
New Requirements for Coverage of Telehealth Services: Parity with in-person services in 6 states, broad coverage of telehealth services in 6 states, limited coverage of telehealth services in 6 states, no action in 33 states
Waiving or Limiting Cost-Sharing for Telehealth Services: Waived for COVID-19 services only in 7 states, waived or limited for all services in 9 states, no action in 35 states
Reimbursement Parity for Telehealth and In-Person Services: Required for all services in 17 states, no action in 34 states
Require Expanded Options for Delivery of Telehealth Services: Yes in 35 states, for behavioral health services only in 1 state, no action in 15 states
Approved Section 1115 Waivers to Address COVID-19: 2 states (Washington and New Hampshire) have approved waivers
Approved Section 1135 Waivers: 51 states have approved waivers
Approved 1915 (c) Appendix K Waivers: 49 states have approved waivers
Approved State Plan Amendments (SPAs): 44 states have temporary changes approved under Medicaid or CHIP disaster relief SPAs, 1 state has an approved traditional SPA
Other State-Reported Medicaid Administrative Actions: 51 states report taking other administrative actions in their Medicaid programs to address COVID-19
Adults at Higher Risk of Serious Illness if Infected with Coronavirus: 38% of all U.S. adults are at risk of serious illness if infected with coronavirus (92,560,223 total) due to their age (65 and over) or pre-existing medical condition. Of those at higher risk, 45% are at increased risk of serious illness if infected with coronavirus due to their existing medical condition such as such as heart disease, diabetes, lung disease, uncontrolled asthma or obesity. Among nonelderly adults — low-income, American Indian/Alaska Native & Black adults have a higher risk of serious illness if infected with coronavirus. In both cases – for race and household income – the higher risk of serious illness if infected with coronavirus is chiefly due to a higher prevalence of underlying health conditions and longstanding disparities in health care and other socio-economic factors.
Finding Policy Responses to Rising Intimate Partner Violence during the Coronavirus Outbreak (Issue Brief)
How Could the Price of Remdesivir Impact Medicare Spending for COVID-19 Patients? (Issue Brief)
U.N. SG Guterres Comments On Global Coronavirus Response, Calls For More Investment In Food Security, Humanitarian Relief (KFF Daily Global Health Policy Report)
Trackers and Tools
Updated: State Data and Policy Actions to Address Coronavirus (Interactive)
Across the country, shelter at home orders and social distancing have helped slow the spread of the coronavirus outbreak in many communities. These measures, while helping to flatten the curve, also pose significant risk for those impacted by domestic or intimate partner violence (IPV). Under quarantines, household members, caregivers, and intimate partners are in close contact with one another, often unable to leave if a violent situation arises or escalates.
IPV during Emergencies
Nearly a third of all Americans experience IPV, used interchangeably with domestic violence (DV), within their lifetimes. IPV is defined as sexual violence, stalking, physical violence, and psychological aggression perpetrated by an intimate partner. Although IPV occurs across all demographics, some groups, such as women of color, people with disabilities, LGBTQ individuals, and pregnant women experience IPV at much higher rates. In addition to the risks associated with physical proximity caused by staying home, the economic impacts of the coronavirus pandemic could compound risk for IPV, particularly for women. Loss of jobs and income can exacerbate stress, risk of experiencing violence, or may make some people more financially dependent on an abusive partner.
While there is limited national data on the impact of the outbreak on IPV rates in the US during this time, some localized data is emerging. Examples in the US include Wilmington, North Carolina, where the DV shelter reported a 116% increase in calls from this same time last year, and Oregon, where calls to DV services have reportedly doubled since the emergency began. The National Domestic Violence Hotline has received calls and digital chats about abusive partners using COVID-19 as a scare tactic, such as preventing them from leaving the house or keeping them from seeking medical attention. A study of Los Angeles and Indianapolis police calls found an increase in DV calls, while calls for other crimes, such as burglary, decreased. The National Network to End Domestic Violence (NNEDV) reports hearing from state coalitions that chat and other digital services requests are up, while shelter requests are down.1 Understanding the full toll of the pandemic on IPV may take years, as cases of IPV are known to be undercounted and collecting data during a crisis can be more challenging.
DV service organizations are looking to research on IPV during and after natural disasters in developing guidance during this public health emergency. Natural disasters, similar to a public health crisis like COVID-19, involve threats to life and loss of loved ones, interruption of social systems and services, and a lack of socialization – all which have been linked to an increase in interpersonal violence against women and girls. Evidence suggests that requests for IPV services (particularly shelter) rise after the initial emergency of natural disasters have subsided.2 However, this will be challenging as it is estimated that there were more than 11,336 unmet requests per day for housing and emergency shelter from survivors of IPV last year, before the COVID-19 outbreak.
Policy Options to Support IPV Providers and Survivors
At the federal level, the Violence Against Women Act (VAWA), originally enacted more than 25 years ago, has been a foundational source of funding for resources and community responses to sexual and domestic violence. VAWA expired in 2018, and given the higher risk of IPV resulting from the pandemic, many have renewed the call for its reauthorization, which would ensure these funds continue to be available to address the fallout of the pandemic, particularly for shelters and hotlines. While some VAWA programs have been reappropriated and continue to be funded at their usual level, there are other policies and programs that consider the needs of IPV survivors and support organizations during COVID-19 including:
The CARES Act – The CARES Act includes some measures for addressing IPV, such as a moratorium on evictions for those in a covered housing program under VAWA. The act also builds on the existing Family Violence and Prevention Services Act (FVPSA) and provides $2 million for the National DV Hotline and awards $45 million to FVPSA formula grants, including for prevention efforts among Indian tribes and state DV coalitions.
The HEROES Act – The fourth proposed federal pandemic relief legislation, the HEROES Act, currently proposes to add $100 million for VAWA programs, such as transitional housing, which is expected to rise in demand as communities begin reopening. FVPSA programs would get an additional $50 million, $2 million of which will go to the National DV hotline. It would also authorize up to $100 million to community-based organizations to assist low-income women and survivors of domestic violence to protect their financial assets in the event of divorce from an abusive spouse. While the bill has passed the House, it is expected to be revised substantially if the Senate takes it up.
Telehealth and confidential mental health care – Many IPV programs provide mental health therapy and counseling by licensed practitioners by phone, over chat, or in person. Currently, many programs are looking to expand phone and digital communication abilities. While CMS has temporarily eased telehealth restrictions under HIPAA for some providers during the pandemic, clinicians who serve people affected by IPV must abide by stricter confidentiality laws. In particular, mental health clinicians that practice through DV response services cannot provide care over FaceTime or Skype, which have been approved by CMS for other telehealth services. Abusive partners can use technology to track and monitor those affected by IPV, making confidentiality particularly important for support services. Although each DV program must consider federal and state confidentiality laws, there are some platforms they can use to communicate with survivors.
Employer-based paid safe leave – Paid safe days allow people time off work to address issues stemming from sexual or domestic violence, such as physical recovery or obtaining legal or medical services, without losing pay. This can help protect job and financial security for those experiencing IPV. While there is no federal requirement for paid safe days, it has been proposed in federal legislation and is required by some state sick leave policies, typically as a component of an employer’s broader sick leave benefit.
Looking Forward
Some policymakers and DV providers are calling for increased support for IPV response services to help bridge gaps that already existed and address the aftermath of the Coronavirus pandemic. Emerging evidence and prior research shows that the pandemic and the economic fallout will place more people at risk for IPV. For them, the larger question is what the response of policymakers will be in the face of many competing community needs in the wake of the pandemic.
KFF private communication with the National Network to End Domestic Violence (NNEDV) ↩︎
This raises the question: How are swing counties affected by the pandemic? In this post, we compare coronavirus cases and death rates across counties in the U.S., based on 2012 and 2016 presidential election voting history, with a particular focus on swing counties. (more…)
In the Middle of the Coronavirus Pandemic: How have Swing Counties Fared?
Partisan divides have emerged along many dimensions of the coronavirus pandemic. Republicans are about three times more likely than Democrats to say their state is moving too slowly to reopen business and ease restrictions and Democrats are more likely than Republicans to report taking preventative measures like wearing masks in public. These partisan divides in opinions about the pandemic may be due in part to different partisan attitudes toward the public health response, as well as differences in COVID-19 prevalence between parts of the country. Indeed, as others have shown, the pandemic has hit Democratic counties harder than Republican counties.
This raises the question: How are swing counties affected by the pandemic? In this post, we compare coronavirus cases and death rates across counties in the U.S., based on 2012 and 2016 presidential election voting history, with a particular focus on swing counties. (more…)
Partisan divides have emerged along many dimensions of the coronavirus pandemic. Republicans are about three times more likely than Democrats to say their state is moving too slowly to reopen business and ease restrictions and Democrats are more likely than Republicans to report taking preventative measures like wearing masks in public. These partisan divides in opinions about the pandemic may be due in part to different partisan attitudes toward the public health response, as well as differences in COVID-19 prevalence between parts of the country. Indeed, as others have shown, the pandemic has hit Democratic counties harder than Republican counties.
This raises the question: How are swing counties affected by the pandemic? In this post, we compare coronavirus cases and death rates across counties in the U.S., based on 2012 and 2016 presidential election voting history, with a particular focus on swing counties. (more…)
Trends in Workplace Wellness Programs and Evolving Federal Standards
In 2019, 84% of large employers (200 or more workers) offering health benefits offered a workplace wellness program, such as those to help people lose weight, stop smoking, or provide lifestyle and behavioral coaching; in addition 4% of large offering firms have programs that exclusively do health screening, meaning in total almost 9 in 10 firms have some sort of workplace wellness program (88%). An estimated 63 million covered employees, including 59 million at large employers work for firms which offer health benefits and one of these workplace wellness programs.1 The Employer Health Benefit Survey (EHBS) has tracked the growth in workplace wellness programs from 2008 when about 70% of large employers (with 41 million covered employees) offered them. Overtime EHBS has changed the way it asks employers about their wellness and health screening offerings, for a detailed explanation see the Appendix.
Increasingly workplace wellness programs ask workers to disclose health information
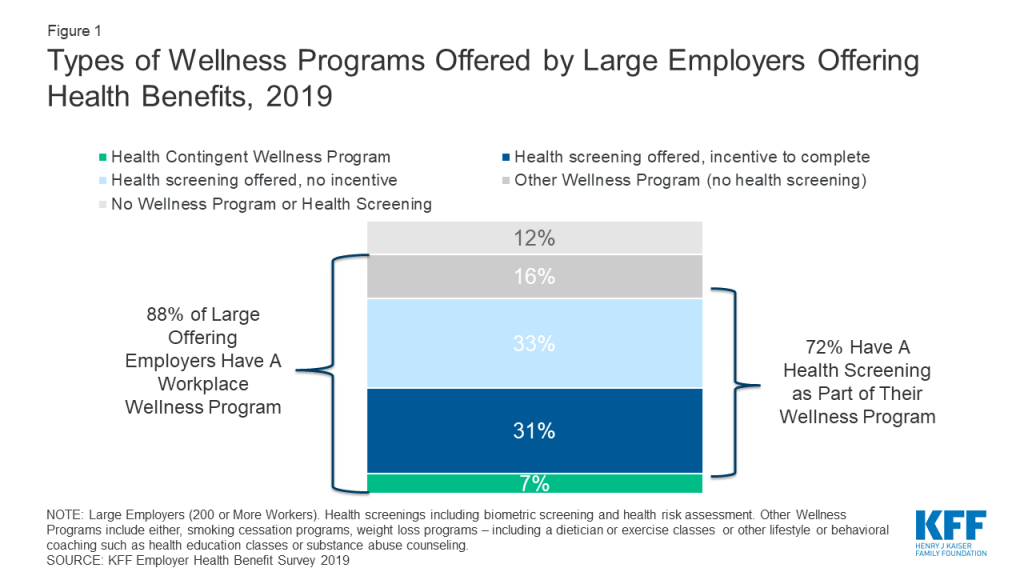
Most large employers ask employees to disclose extensive personal health information via a questionnaire, known as a health risk assessment (HRA), or through biometric screening (such as a physical examination or lab test), or both. In 2019, 72% of large firms that offer health benefits, employing 48 million covered employees, offered the opportunity to complete either an HRA, biometric screening, or both. (Figure 1)
Figure 1: Types of Wellness Programs Offered by Large Employers Offering Health Benefits, 2019
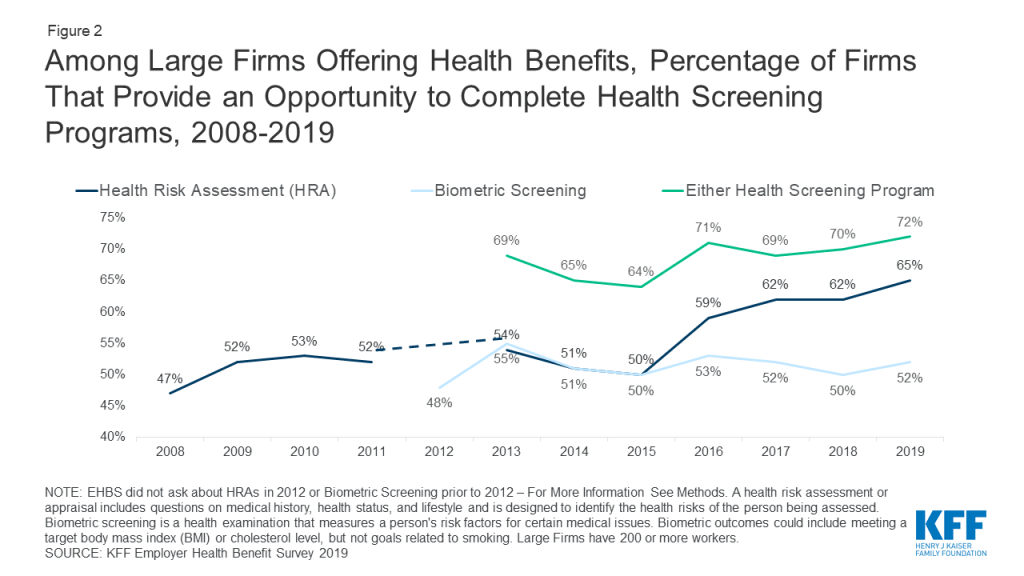
Use of HRAs has increased among large employers offering health benefits – from 47% in 2008 to 65% in 2019. (Figure 2) In 2012, the first year the EHBS asked about biometric screening 48% of large firms offered a biometric screening program similar to 52% in 2019. In addition, large employers and their health plans collect information through wearable technologies (18% in 2019). In total, 42 million covered employees worked at a large employer who had one of these screening programs that involves disclosure of personal health information.
Figure 2: Among Large Firms Offering Health Benefits, Percentage of Firms That Provide an Opportunity to Complete Health Screening Programs, 2008-2019
Financial incentives to complete health screenings
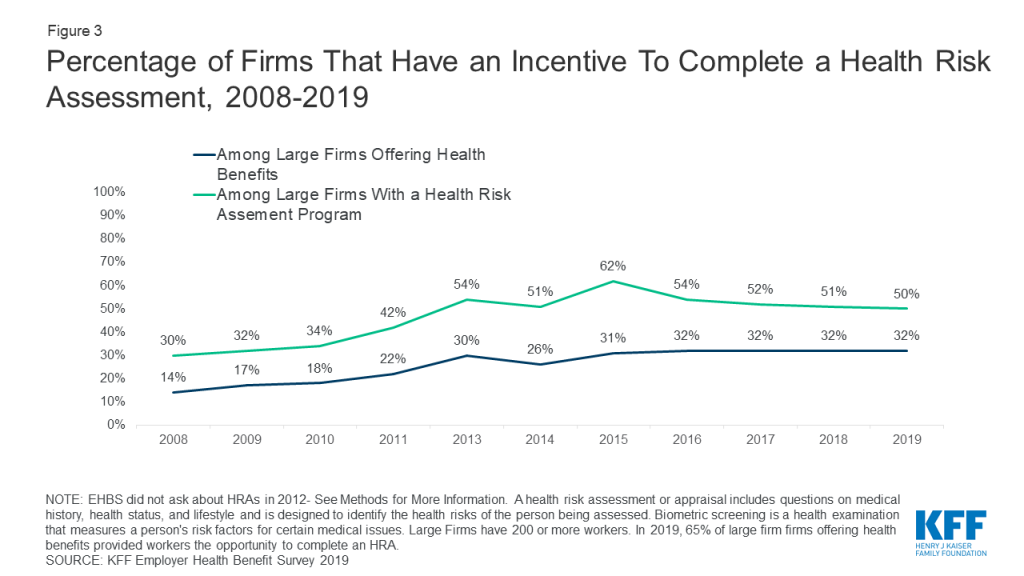
Employers that offer health risk assessments in their wellness programs increasingly use financial incentives to encourage workers to disclose health information. (Figure 3) In 2019, almost a third (32%) of large firms offering health benefits offered incentives to complete a HRA, compared to 14% in 2008.
Figure 3: Percentage of Firms That Have an Incentive To Complete a Health Risk Assessment, 2008-2019
A small percent of large offering employers (7%) offer incentives to not only disclose health information but also to achieve biometric outcomes such as a target BMI or cholesterol level. These so-called health contingent wellness programs were authorized by federal regulation in 2006, and later by the Affordable Care Act (see timeline). The share of large employers offering so-called health contingent wellness programs has remained about the same since 2012.
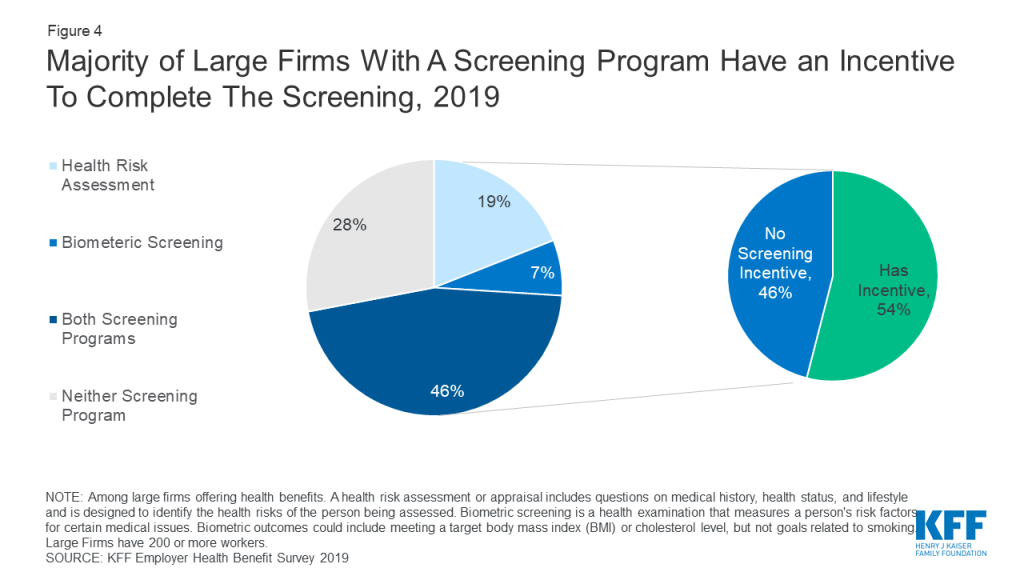
Overall, among large employer wellness programs with health screening, including health-contingent programs, a majority (54%) apply financial incentives for participants to complete the health screening and disclose health information. (Figure 4) Nearly 28 million covered workers are in these firms. In some cases, these incentives or penalties may also apply to workers not enrolled in the health plan (34%) or an enrolled worker’s spouse (49%).
Figure 4: Majority of Large Firms With A Screening Program Have an Incentive To Complete The Screening, 2019
Size and effectiveness of financial incentives
In 2019, 20% of large firms with a wellness or health screening incentive had a maximum incentive of more than a $1,000. On average, the maximum value of the incentive was $783. Firms may provide incentives in a variety formats, including discounts or surcharges to the employee’s health premium contribution, cash, or merchandise. Incentives may reward or penalize workers for combination of activities.
We can get a sense of the size of these incentives/penalties by comparing the average premium contribution for single coverage to the average maximum reward. At firms with a wellness program incentive, covered workers’ pay $1,357 per year for single coverage premiums, not quite twice as much the maximum average penalty or incentive of $783. There is tremendous variation in employer incentives, but at some firms wellness penalties can be a significant cost for covered workers.
Participation in wellness screening programs is not high, even with incentives. A previous analysis of the 2016 Employer Health Benefit Survey, found that at large firms with an incentive for completing a health risk assessment, 50% of workers complete the assessment compared to 31% at firms with no incentive. Most large employers (61%) say either that financial incentives are either “not at all effective” or only “somewhat effective” in encouraging employee participation in wellness programs, or they don’t know if incentives are effective.
Workers may opt not to participate in wellness programs to protect the privacy of their health information, because they don’t find the program convenient, and/or for other reasons. To the extent wellness program incentives trigger financial penalties for non-participation, workers may find them burdensome, as a recent legal challenge demonstrates.
Yale University Health Expectation Program (HEP)
In 2017, Yale University implemented a new employee wellness program for its unionized clerical, technical, food service, and maintenance staff and their spouses. Employees and spouses covered by Yale medical plans are automatically enrolled in HEP, and then must follow screening recommendations. Those diagnosed with or having risk factors for certain conditions (such as diabetes, hypertension, or hyperlipidemia) can also be required to participate in a health coaching program. Trestle Tree is the wellness vendor that administers the health coaching program in partnership with a second vendor, HealthMine, which receives all health data on workers covered by the program. In addition to data collected through screening, health insurance claims data, including pharmacy claims, for all health plan enrollees is regularly transferred to HealthMine, regardless of whether enrollees participate in HEP.
Members may opt out of participating in HEP if they pay a weekly fee of $25, or $1,300 for the entire year, which is deducted from their paycheck. The average annual salary for a Yale food service worker is reportedly less than $37,000. HEP participants who don’t comply with the program are also subject to the $25 weekly fee. In one reported case, a campus cook and breast cancer survivor who had undergone bilateral mastectomy was nonetheless told she would be fined $25/week unless she had a mammogram.
In 2019, this employee and several others brought a class action suit against Yale University, arguing that it coerces employees and their spouses to turn over health information in violation of the ADA and GINA, federal laws that permit collection of personal health information by employers only through voluntary wellness programs.
In response, Yale points out this wellness program was agreed to by the union as part of its collectively bargained health benefits package. Under the agreement, the HEP took effect in 2017, when EEOC regulations permitting wellness financial incentives were still in effect. Yale also argues the wellness program financial incentive is modest and does not render the choice to participate as involuntary.
Federal rules applicable to wellness program incentives
Questions about the permissibility of these workplace wellness incentives under federal law are ongoing. Two federal employment nondiscrimination laws – the Americans with Disabilities Act of 1990 (ADA) and the Genetic Information Nondiscrimination Act of 2008 (GINA) – prohibit employers from making inquiries about employee health information or genetic information with limited exceptions, including through voluntary workplace wellness programs. Initially, regulations and enforcement guidance defined “voluntary” wellness programs to be those that neither require participation nor penalize employees for nonparticipation. In 2016, new federal regulations issued by the Equal Employment Opportunity Commission (EEOC) re-defined voluntary wellness programs to include those that impose financial incentives up to 30% of the cost of self-only coverage (or more than $2,100, based on the average cost of self-only group health plan coverage in 2019). The agency asserted that it did so to permit wellness program incentives consistent with those permitted under the Affordable Care Act (ACA) [see box], but that nonetheless “prevent economic coercion that could render provision of medical information involuntary.” However, a federal district court found that EEOC did not provide sufficient justification for its wellness program incentives limits, and ruled this change in the definition of “voluntariness” to be arbitrary and capricious. EEOC repealed the financial incentive provisions of its ADA and GINA wellness rules in December 2018. The Agency’s regulatory agenda indicates further rulemaking on wellness is planned.
Meanwhile, other provisions of the ADA and GINA wellness rules remain in effect for all workplace wellness programs that make disability-related inquiries or conduct medical examinations. Such programs must be “reasonably designed.” Among other requirements, reasonably designed programs must provide employees with advanced notice clearly explaining what medical information will be obtained, how the medical information will be used, who will receive the medical information, the restrictions on its disclosure, and methods the employer/wellness program uses to prevent improper disclosure of medical information. In addition, programs must be reasonably designed to promote health or prevent disease.
HIPAA, ACA, and Workplace Wellness Incentives
Since enactment of the Health Insurance Portability and Accountability Act of 1996 (HIPAA), group health plans have been prohibited from discriminating (varying eligibility or premium contribution) based on health status. HIPAA permitted an exception to the nondiscrimination requirement: group health plans can vary premiums or cost sharing through workplace wellness programs. Regulations in 2006 permitted employers to offer so-called health-contingent wellness programs that vary premium contributions on the ability of employees to meet biometric targets, such as normal weight or blood sugar, as long as wellness programs meet other standards, including limits on the amount of financial incentives. The regulation did not limit other incentives to participate that were not tied to meeting health outcomes.
In 2010, the Affordable Care Act codified the 2006 regulations and specified that incentives under health-contingent workplace wellness programs could be as much as 30% of the cost of the group health plan (employer plus employee share). Final regulations implementing the 2010 workplace wellness provisions were published in 2013. Again, regulations did not limit other wellness program incentives to participate that were not tied to meeting heath outcomes, but did specify that compliance with ACA wellness program requirements does not mean the program complies with other federal employment nondiscrimination laws, including the ADA and GINA.
Since these statutory and regulatory changes permitting health-contingent wellness program incentives, few employers have adopted this type of wellness program. In 2019, 7% of large employers offered health contingent wellness programs.
Health information collected through reasonably designed wellness programs can be used to provide meaningful feedback or advice to employees about their health or risk status; health information collected through wellness programs can also be used, in aggregated form, to design effective disease management programs or treatments. However, the EEOC regulations specify that a wellness program is not reasonably designed if it exists mainly to shift costs from the employer to targeted employees based on their health, or to simply give an employer information to estimate future health care costs.
Among large firms with a screening program in 2018, 62% report using information from their screening programs to target health promotion programs or communications, 53% use information to design new programs, 43% use information to measure health plan costs, 67% use information to understand employee health risks, and 24% use information as the basis for an incentive program
Discussion
Despite the prevalence of workplace wellness programs, numerous studies find limited evidence of their effectiveness in promoting health or preventing disease. There are considerable challenges with measuring the impacts of workplace wellness program. First, healthier individuals are more likely to participate in wellness programs, making it hard to determine if differences in health outcomes reflect program effectiveness or the people who elect to participate. Secondly, workplace programs come in many shapes and sizes, with many programs focusing more on health screening than health promotion programs.
Recently two randomized controlled trials found limited improvements in health outcomes from employer wellness programs. The first trial, conducted at the University of Illinois, found that implementing a $200 incentive increased participation in the health screening from 46.9% to 62.5% of employees. Employees completing screening were able to participate in health coaching, disease management and wellness classes. After a year, the program did not find any impacts on medical spending, absenteeism, and health outcomes between participants and the control group. Individuals who participated in the program were more likely to complete a health screening and say that management cared about their health and wellbeing. One consequence of the programs was that lower wage workers were more likely to be penalized, exacerbating concerns about affordability.
A second trial, involving 20 worksites for a large US warehouse retail company did not find improvements in health outcomes, spending, or utilization over an 18-month period. The intervention did find an 8% percentage point increase in the share of employees who regularly exercised and their self-reported health status. Workers were eligible for up to $250 dollars in rewards if they participated in a wellness vendor’s programs, including nutrition and exercise classes.
Federal law permits collection of health information from workers through voluntary workplace wellness programs, and the EEOC has given notice it will revisit the issue of incentives in future rulemaking. How federal standards for wellness incentives evolve remains to be seen. Even as standards evolve, though, most large employer wellness programs continue to collect personal health information, and most of these screening programs incentivize workers to provide it. When incentives are applied to the premium contribution for group health benefits, failure to participate in wellness programs can substantially increase the cost workers would otherwise pay for their health coverage.
Methods
The KFF Employer Health Benefits Survey is an annual, nationally representative sample of non-federal public and private employers with three or more employees. The survey asks extensive questions about the firm characteristic and the benefits they offer. In 2019, 2,012 firms completed the full survey, including 1,133 firms with 200 or more employees. While less than 2% of firms have 200 or more employees, 73% of covered workers work at these firms. Therefore, the smallest firms dominate any statistics weighted by the number of employers. For this reason, most statistics are reported for just larger firms. For more information on the Employer Health Benefit Survey see here.
Every year we review and revise the questions asked in the employer health benefit survey. Questions are adapted to changes in the marketplace, to improve the clarity and ease for respondents, or to reduce the overall burden of the survey. Given the rapidly changing landscape of employer wellness and health screening programs, these questions saw several revisions over the last decade, with a major revision in 2014. Changes to question wording can have an effect on estimates. In this analysis we reported trends of comparable questions over time, the exact question wording are provided here. In some years we elected not to ask a question in order to make space for other topics. In addition, interviewers are provided notes to address common questions for respondents, the notes provided for any given question are available on request. These notes typically have minor changes every year and are infrequently read to respondents.
Health Risk Assessment
Between 2008 and 2011: “Does your firm give its employees the option to complete a health risk appraisal or health risk assessment? A health risk assessment or appraisal includes questions on medical history, health status, and lifestyle and is designed to identify the health risks of the person being assessed.”
2013 and 2014: “Does your firm provide the opportunity for employees to complete a health risk appraisal or health risk assessment? A health risk assessment or appraisal includes questions on medical history, health status, and lifestyle and is designed to identify the health risks of the person being assessed.”
Since2015: “A health risk assessment includes questions on medical history and lifestyle and is designed to identify a person’s health risks. Does your firm or insurer provide an opportunity to complete a health risk appraisal or assessment?
Biometric Screening
Between 2013 and 2014: Which of the following wellness or health promotion programs does your firm or any of your health plans offer to at least some employees: Biometric Screening?
Biometric screening is an in-person health examination conducted by a health professional to 2015: measure an employee’s risk factors such as cholesterol, blood pressure, and body mass index. Does your firm or insurer provide an opportunity, or ask employees, to complete biometric screening to identify health issues that the employee may have?
Since 2016: Biometric screening is an in-person health examination conducted by a health professional to measure an employee’s risk factors such as cholesterol, blood pressure, and body mass index. Does your firm or insurer provide an opportunity for employees to complete a biometric screening?
Incentives for Health Risk Assessments
Between 2008 and 2009: Does your firm offer financial incentives to employees that complete a health risk appraisal or health risk assessment?
Between 2010 and 2014: Does your firm offer financial incentives to employees that complete a health risk appraisal or health risk assessment, anything from premium discounts to cash?
Since 2015: Does your firm use incentives or penalties to encourage employees to complete a health risk assessment?
Incentives for Biometric Screening Programs
Between 2013 and 2014: Are employees rewarded or penalized financially based on whether they meet specified biometric outcomes such as meeting a target body mass index (or BMI) or cholesterol level? Please do NOT include incentives or penalties related to smoking or tobacco use in answering this question.
Since 2015: Does your firm use incentives or penalties that encourage employees to complete biometric screening?
Wellness and Health Promotion Programs
Since 2015: Which of the following wellness or health promotion activities does your firm, any of your health plans, or 3rd party vendors offer to at least some employees? Please select all that apply.
a. Programs to help employees stop smoking or using tobacco
b. Programs to help employees lose weight, including monitored exercise programs, nutrition counseling or an on – site dietician (Note: Online programs count only if the program is interactive. Walking clubs count if they are structured.)
c. Other lifestyle or behavioral coaching, such as health education classes, stress – management or substance abuse counseling (If needed: Including for opioids.)
Between 2012 and 2014: Which of the following wellness or health promotion programs does your firm or any of your health plans offer to at least some employees?
a. Weight loss program
c. Smoking cessation program
d. Lifestyle or behavioral coaching (other than smoking cessation)
f. Classes in nutrition or healthy living
Between 2008 and 2011: Which of the following wellness programs or benefits does your firm or any of your health plans offer to at least some employees?
a. weight loss programs
c. smoking cessation program
d. personal health coaching
e. classes in nutrition or healthy living
Between 2005 and 2006: Does your firm offer any of the following wellness programs to your employees?
a. fitness programs or on-site health club facilities
b. smoking cessation
d. weight loss
Appendix
Timeline of Federal Policy Related to Wellness Programs
July 1990
Americans With Disabilities Act (ADA) enacted. Prohibits employment discrimination based on disability and prohibits employers from making any medical inquiries of/about employees with few exceptions, including through “voluntary” wellness programs.
EEOC enforcement guidance states that “voluntary” means that the employer neither requires participation in the program, nor penalizes employees who do not participate.
1996
Health Insurance Portability and Accountability Act (HIPAA) enacted.
Prohibits group health plans from conditioning eligibility or premium contribution for group health benefits on health status (nondiscrimination). Wellness exception permits premium discounts or rebates or modification of otherwise applicable cost sharing in return for adherence to programs of health promotion and disease prevention
1997
Clinton Administration final HIPAA regulation clarifies that wellness program incentives cannot vary premiums or cost sharing based on achieving a health status-related factor.
Dec 2006
Bush Administration final nondiscrimination and wellness regulation reinterprets wellness exception to permit health-outcomes-based incentives that vary premium and cost sharing based on a health status-related factor. Health-outcomes based wellness programs are allowed if the financial incentive does not exceed 20% of the health plan cost (employer + employee share), and if the wellness program is reasonably designed and offered to all similarly situated individuals. Other “participatory” wellness programs that do not vary premiums or cost sharing based on health status factors are not subject to this standard. The regulation specifies that wellness program compliance with these standards Compliance with this section is not determinative of compliance with any other State or Federal law, such as the Americans with Disabilities Act.
May 2008
Genetic Information Nondiscrimination Act (GINA) enacted. Prohibits discrimination in health insurance and in employment based on genetic information, defined to include results of a genetic test and information about family history. Health insurers, plans, and employers are also prohibited from requesting or requiring genetic information of an individual or an individual’s family members, with limited exceptions, including voluntary wellness programs.
Mar 2010
Affordable Care Act (ACA) enacted. Codifies 2006 regulatory standards for health-outcomes based wellness programs and increases permissible financial incentives to 30% of total health plan cost, or up to 50% if tobacco cessation incentives are included.
Nov 2010
EEOC final rule on GINA clarifies that wellness programs may not offer a financial incentive for completion of a health risk assessment that includes questions about family medical history or other genetic information.
Jun 2013
Obama Administration final rule on ACA wellness standards. Specifies that workplace wellness program compliance with these standards is not determinative of compliance with any other State or Federal law, including the ADA.
May 2016
EEOC final rule to amend ADA and GINA regulations and enforcement guidance with respect to workplace wellness programs that collect personal health information. Voluntary programs can use incentives, up to 30% of cost of self-only coverage, to encourage participation. Reasonably designed programs that collect health information must meet other standards relating to permitted uses of collected health information, prior notice to employees, and health data privacy protections
Aug 2017
In response to AARP challenge, Federal court finds 2016 rule is arbitrary and capricious because EEOC did not provide sufficient reasoning to justify the incentive limit for workplace wellness programs. The court later issued an order vacating the incentive portion of the rule, effective 1/1/2019.
Dec 2018
EEOC repeals portions of ADA and GINA wellness rules permitting financial incentives. Other portions establishing standards relating to permitted uses of health information, notice to employees, and privacy remain in force.
Spring 2019
EEOC includes revisions to ADA and GINA wellness rules on the agency’s regulatory agenda for 2019.
Endnotes
Half of small firms (3-199) worker offer a wellness programs (https://modern.kff.org/report-section/ehbs-2019-section-12-health-and-wellness-programs/) This brief focuses on the programs offered by large employers, because these firm are more likely to sponsor and administer their programs directly and they manage benefits for the majority of covered workers. ↩︎
A new Coronavirus Policy Watchpost from KFF explores how state responses to limit abortion access during the COVID-19 pandemic has drawn renewed attention to the provision of medication abortion using telemedicine approaches. Medication abortion via telemedicine is a method that can be used to safely provide women with access to abortion care while social distancing, preserving personal protective equipment, and limiting risk of exposure to coronavirus.
A new telemedicine protocol –“no-test” medication abortions– has been developed in response to COVID-19. This approach, based on studies conducted outside the US demonstrating its safety, enables many patients to safely obtain abortions without needing in-person tests or exams. This approach, along with other telemedicine protocols, however, would not be available in many states because of state laws and policies that prohibit its use.
Currently, in 23 states, providers could adopt this method to offer medication abortion because there are not laws or policies that prohibit its use. However, in other states, laws explicitly ban telemedicine abortions or make them impractical by requiring the prescribing clinician to be physically present with the patient, ultrasounds before abortions, or in-person counseling.