KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Hulu’s new miniseries “Dopesick” was built on journalism, and its creators hope it will spark a renewed public discussion about the nation’s opioid crisis, show executives said during a recent panel discussion hosted by KFF’s Kaiser Health News and Hulu.
The event brought together the lead creative powers behind the show along with a journalist from KHN and a policy expert from KFF to unpack the making of “Dopesick” and what the show has to say about the origins of the opioid crisis. KFF’s journalists and policy experts have been tracking the devastating epidemic with on-the-ground stories as well as data-driven analyses for a number of years. The panelists brought their different lenses — creative, journalistic and policy — to focus on the devastating impact of opioids on ordinary Americans and the often ineffective efforts to combat this continuing public health emergency.
The panel discussion, moderated by Chaseedaw Giles, KHN’s digital strategy and audience engagement editor, featured executive producer, writer and showrunner Danny Strong; journalist Beth Macy, who authored the book on which the show is based; KHN correspondent Aneri Pattani, who has reported extensively on opioid policy, substance use and mental health; and KFF senior policy analyst Nirmita Panchal, whose analytical work focuses on mental health and substance use.
“What was unique about my collaboration with Beth is that the journalism side of the process never ended,” Strong said. “We would do interviews together, people would leak documents to us. … It was this unusual process in which we were writing a scripted drama and then simultaneously doing active investigative journalism.”
Macy, who was in the show’s writers’ room full time, said writers would incorporate into scripts revelations from newly released court filings in ongoing cases against Purdue Pharma, the company behind the drug OxyContin, which features prominently in the eight-episode miniseries.
“New documents were coming out all the time,” Macy said. “We would take turns — you go through this, I’ll go through this. And then we would all report back to Danny and decide what the best highlights were.”
In a 40-minute discussion, the panelists explored a wide range of topics about the show and the real-life opioid crisis it depicts, weaving in stories from people Pattani has interviewed for KHN radio and print pieces and findings from Panchal’s analyses. Topics included:
• How the show employed the tools of fiction, such as composite characters, to tell a larger truth
• The important role played by medication-assisted treatment, which combines medications with counseling and behavioral therapy in the treatment of opioid addiction
• The current state of the opioid crisis, marked by a record-high 93,000 deaths from drug overdoses in 2020; the expansion of the problem beyond largely rural, white communities; and the rise of highly addictive synthetic opioids like fentanyl
• The role of politics in the funding for, and availability of, different types of treatment
The economic fallout and social isolation of the COVID-19 pandemic have exacerbated the opioid epidemic, Panchal said. She noted that about 1 in 3 people now say they are experiencing anxiety and depression, compared to about 1 in 10 before the pandemic.
“The job loss, financial hardship, poor mental health — these are things that can often go hand in hand with substance use,” Panchal said.
Pattani noted that there are divisions among political leaders at all levels about how best to tackle the opioid crisis, with some pushing for more medication-assisted treatment, others favoring traditional rehab centers and some emphasizing a criminal justice approach to the problem.
Everyone is representing a district that has constituents affected by this,” she said. “I haven’t talked to a politician who says we don’t need to address the opioid epidemic, but I think they all disagree on how.”
“Dopesick” premiered on Hulu Oct. 13, with new installments of the miniseries available on Hulu every Wednesday. The panel discussion, recorded in KFF’s Washington, D.C., offices without a live audience due to COVID-19, can be viewed anytime on kff.org.
About KFF and KHN
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
About Hulu and “Dopesick”
From Executive Producer Danny Strong and starring and executive-produced by Michael Keaton, “Dopesick” examines how one company triggered the worst drug epidemic in American history. The series takes viewers to the epicenter of America’s struggle with opioid addiction, from the boardrooms of Big Pharma to a distressed Virginia mining community, to the hallways of the Drug Enforcement Administration. Defying all odds, heroes will emerge in an intense and thrilling ride to take down the craven corporate forces behind this national crisis and their allies. The limited series is inspired by The New York Times bestseller by Beth Macy.
The eight-episode series stars Michael Keaton, Peter Sarsgaard, Michael Stuhlbarg, Will Poulter and John Hoogenakker, with Kaitlyn Dever and Rosario Dawson. Guest stars include Phillipa Soo and Jake McDorman.
“Dopesick” is written by Emmy winner Danny Strong (“Empire,” “Recount,” “Game Change”) and directed by Oscar winner Barry Levinson (“Paterno,” “Rain Man”). Executive producers for “Dopesick” include Strong, John Goldwyn (“Dexter”), Keaton, Levinson, Warren Littlefield (“The Handmaid’s Tale,” “Fargo,” “The Old Man”), Beth Macy (“Dopesick”) and Karen Rosenfelt (“Twilight”).
This brief reviews final 2022 premium rate filings for Marketplace-participating individual market insurers in all 50 states and the District of Columbia. Although the ACA individual market represents a small share of the privately insured population, the rate filings for this market are detailed and publicly accessible, making them a useful source of information on how health insurers are thinking about their likely costs for the next year.
Most of the 311 rate filings reviewed,We find that most insurers expect spending and utilization to return to pre-pandemic levels in 2022 and do not expect COVID-19 to affect costs in the individual market. A majority of rate changes for 2022 are moderate, with most insurers posting premium increases or decreases of a few percentage points.
The brief is available on the Peterson-KFF Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.
The October KFF Health Tracking Poll finds one in five adults in the U.S. report receiving ongoing support for daily activities such as bathing, dressing, or remembering medications, and a similar share say they are providing those type of services for a close friend or family member. About one in five adults (18%) also say they or a family member need either new or additional support from paid nurses or aides beyond what they are currently getting. The most common reason why people haven’t gotten the support they need is cost. More than three-fourths of those who say they need more help (14% of all adults) say “not being able to afford the cost of the care” is a reason why they or their family member has not received the additional support from paid nurses or aides.
Many unpaid caregivers say providing support to friends or family members has caused them to worry or stress (77%), experience worsening of their own mental health (50%), financial strain due to inability to work (42%), or worsening of their own physical health (38%). Unpaid caregivers are more likely to be racial and ethnic minorities, those with lower education, and report lower levels of household income.
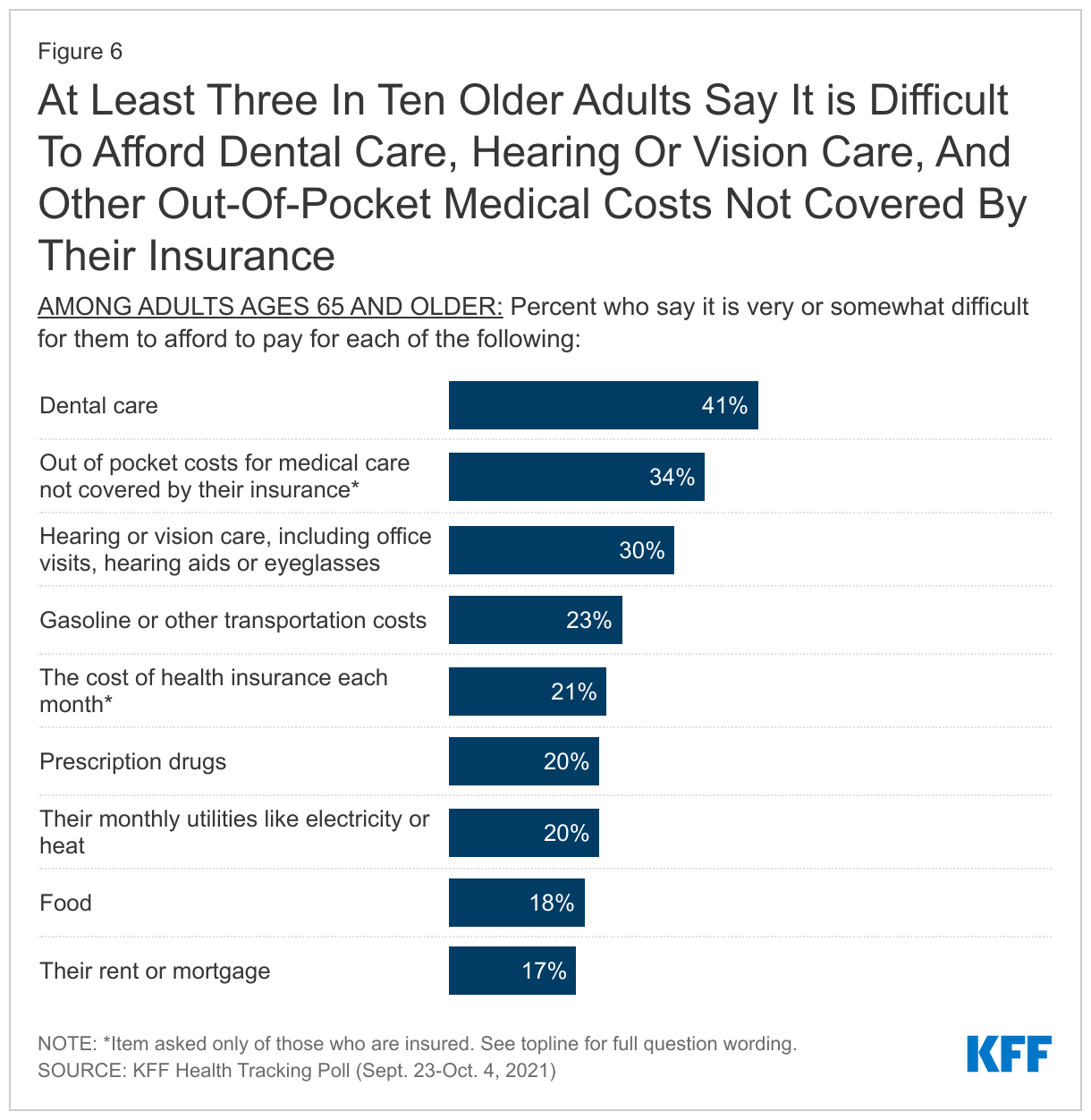
Significant shares of older adults in the U.S. report difficulty paying for various aspects of health care, especially services not generally covered by Medicare. Four in ten older adults (41%) report difficulty paying for dental care while three in ten report difficulty affording hearing or vision care (30%). Dental, vision, and hearing coverage are three benefits not generally covered by Medicare but are part of Democratic lawmakers’ proposals as part of the reconciliation spending package.
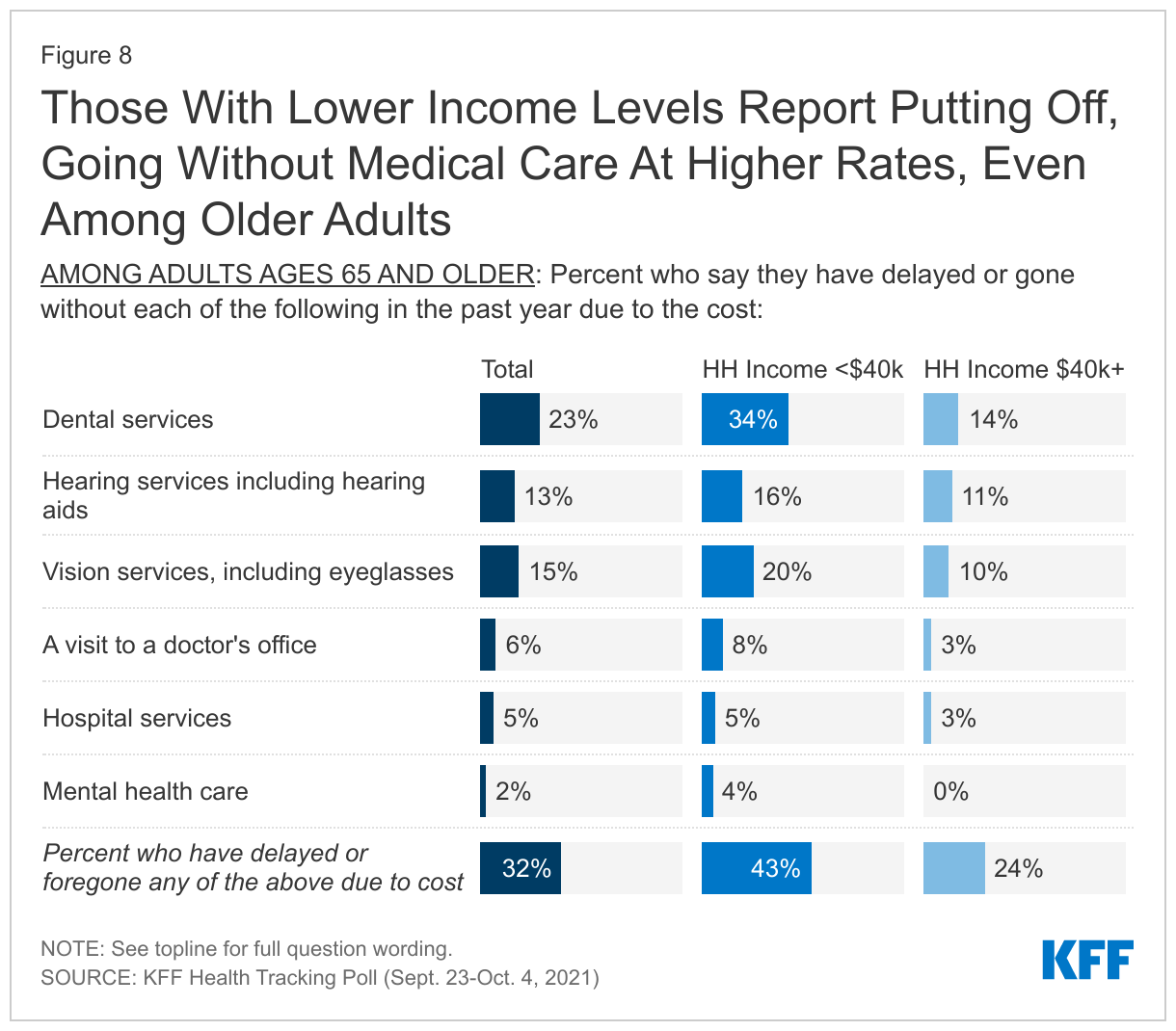
Many older adults who are eligible for Medicare also report putting off or foregoing medical care due to costs. While Medicare helps older adults pay for routine doctor visits and hospital stays, substantial shares of lower income older adults report putting off or foregoing services not covered by Medicare. Overall, more than four in ten older adults in households earning less than $40,000 annually report delaying or going without some form of medical care over the past year due to costs (compared to 24% of older adults with household incomes over $40,000), including dental care (34%), vision care (20%), and hearing services including hearing aids (16%).
With substantial shares of the public reporting financial strains associated with help with everyday activities for themselves or family members, and seniors reporting difficulty paying for some health care expenses, the latest KFF poll finds broad support for many of the proposals in the reconciliation package being currently discussed in Congress.
Home And Community Based Services
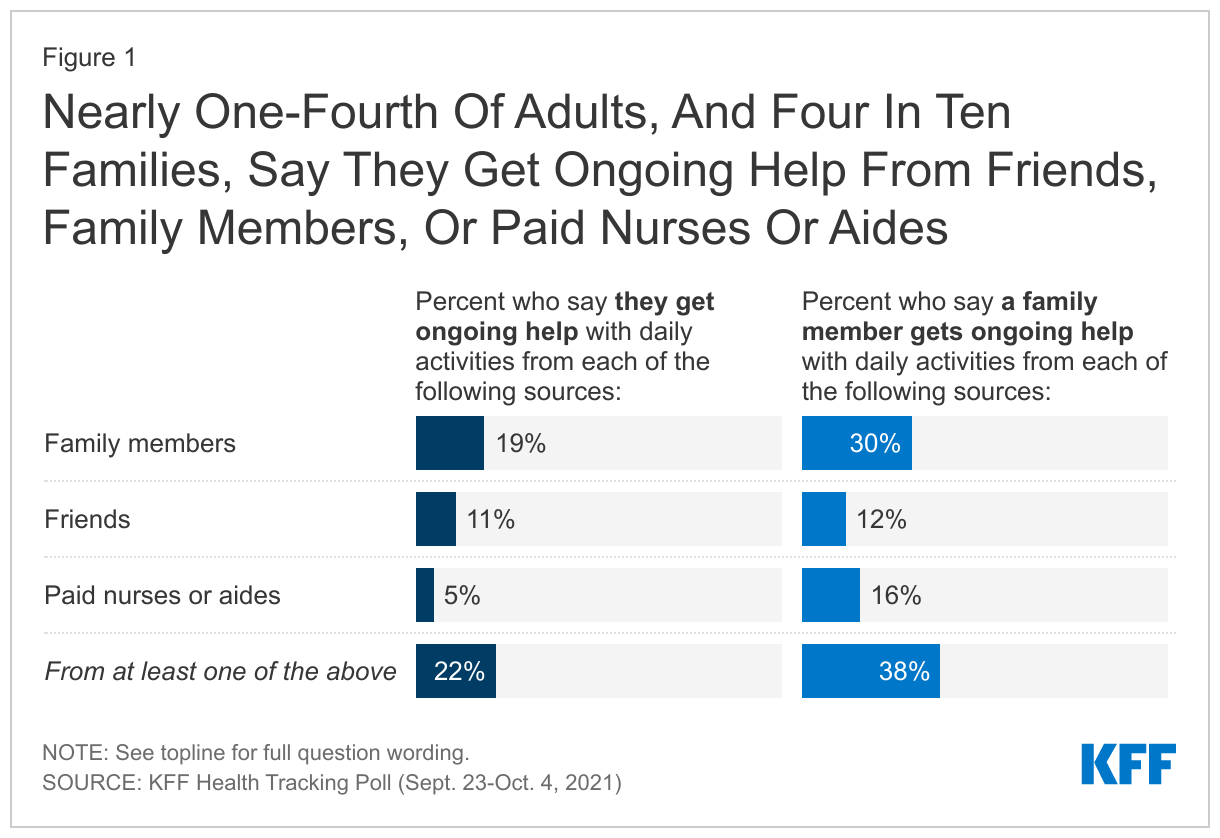
One in five adults, including 27% of adults 65 and older, say they are currently receiving ongoing support with everyday activities from either a family member (19%), a friend (11%), or paid nurses or aides (5%). Additionally, nearly four in ten (38%) adults say a family member gets ongoing help from at least one of these sources including another family member (30%), paid nurses or aides (16%) or friends (12%).
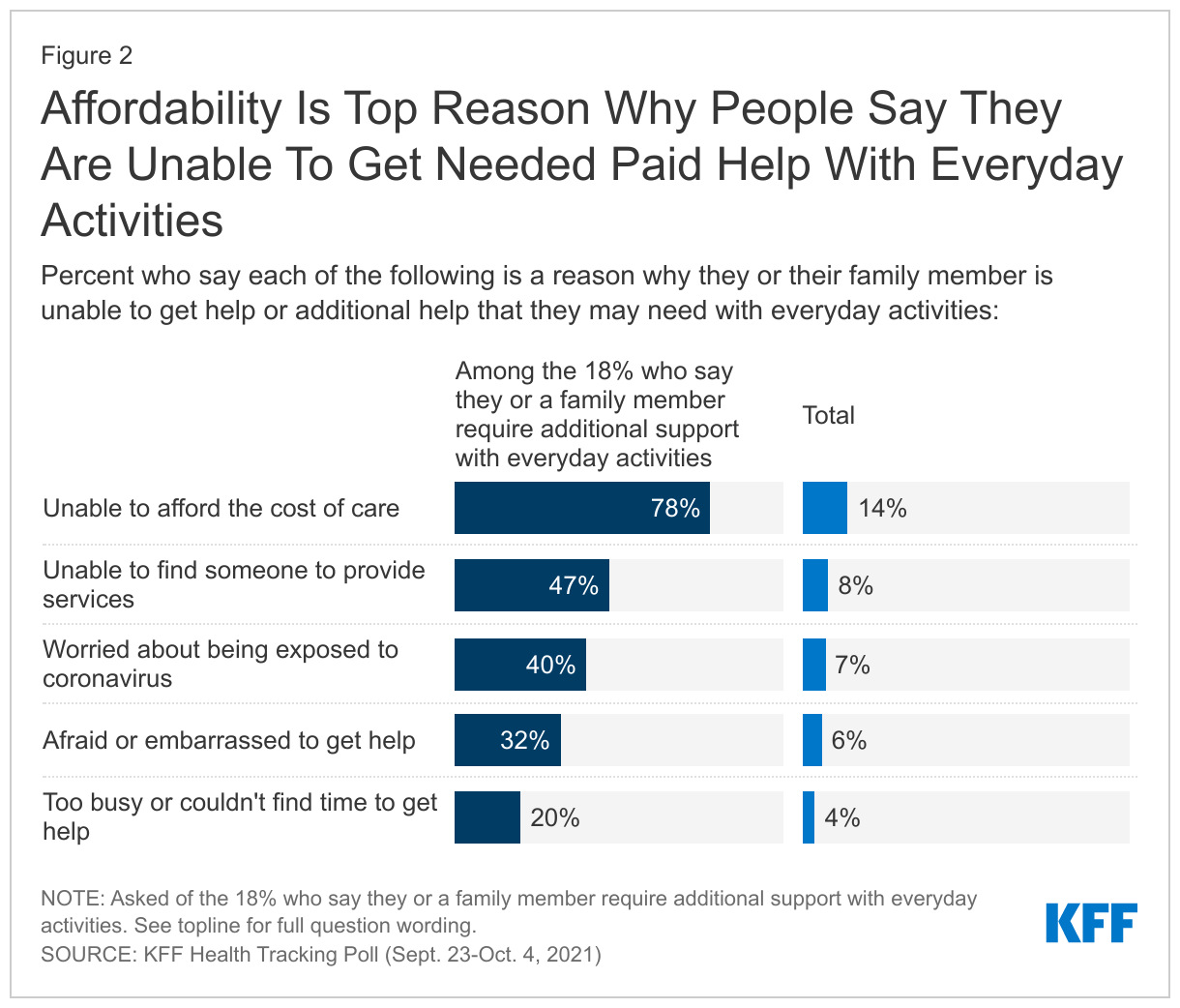
About one in five adults (18%) say they or a family member need either new or additional support from paid nurses or aides beyond what they are currently getting. The most common reason why people haven’t gotten the support they need is cost. More than three-fourths of those who say they need more help (14% of all adults) say “not being able to afford the cost of the care” is a reason why they or their family member has not received the additional support from paid nurses or aides. Other reasons include not being able to find someone to provide the services (47%, or 8% of all adults)1 , being worried about being exposed to coronavirus (40%, 7% of all adults), being afraid or embarrassed to get help (32%, 6%), or being too busy or unable to find the time to get help (20%, 4%).
With many reporting difficulty paying for cost of home and community based care, the poll also gauged support for Democratic proposals to increase funding to Medicaid to pay workers and expand home and community-based services (HCBS). Medicaid is the primary payer for long-term services and supports (LTSS), including home and community-based services (HCBS), that help seniors and people with disabilities with daily self-care and independent living needs. Majorities across partisans (79% total, 95% of Democrats, 76% of independents, 67% of Republicans) support increased funding to Medicaid to pay workers and expand home and community-based services (HCBS).
The toll On Unpaid Caregivers
With Congress discussing possible new tax credits to help with home and community based care, one in five adults (21%) say they are currently providing unpaid support with everyday activities to either a friend or family member, excluding the type of care young children need. Majorities across partisans also favor new tax credit to help people pay for such care (82% total, 94% of Democrats, 80% of independents, 73% of Republicans).
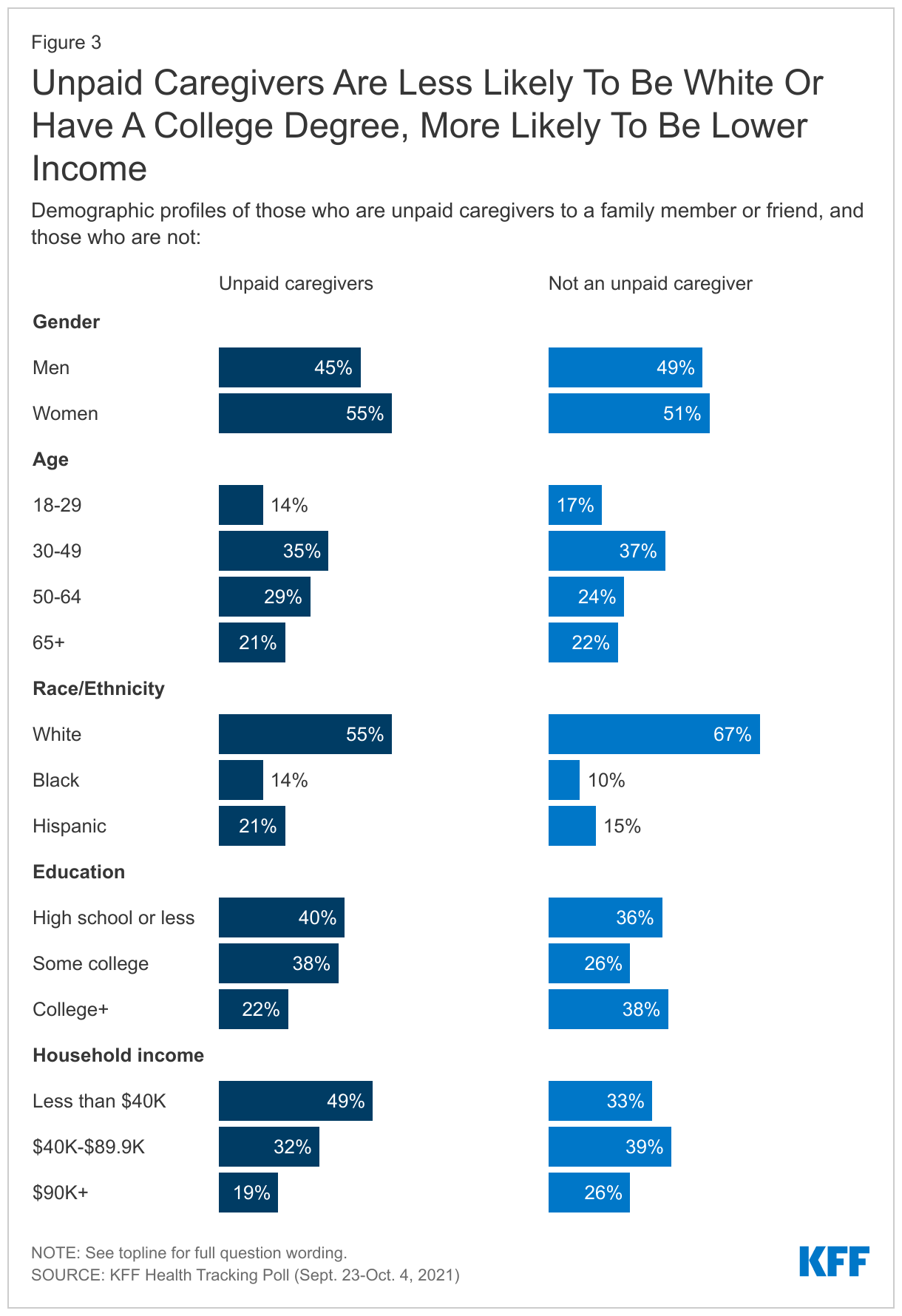
The KFF October Tracking Poll finds unpaid caregivers are more likely to be Black or Hispanic (14% and 21%) compared to those who are not unpaid caregivers (10% and 15%). About eight in ten unpaid caregivers to family and friends do not have a college degree, and about half have household incomes under $40,000.
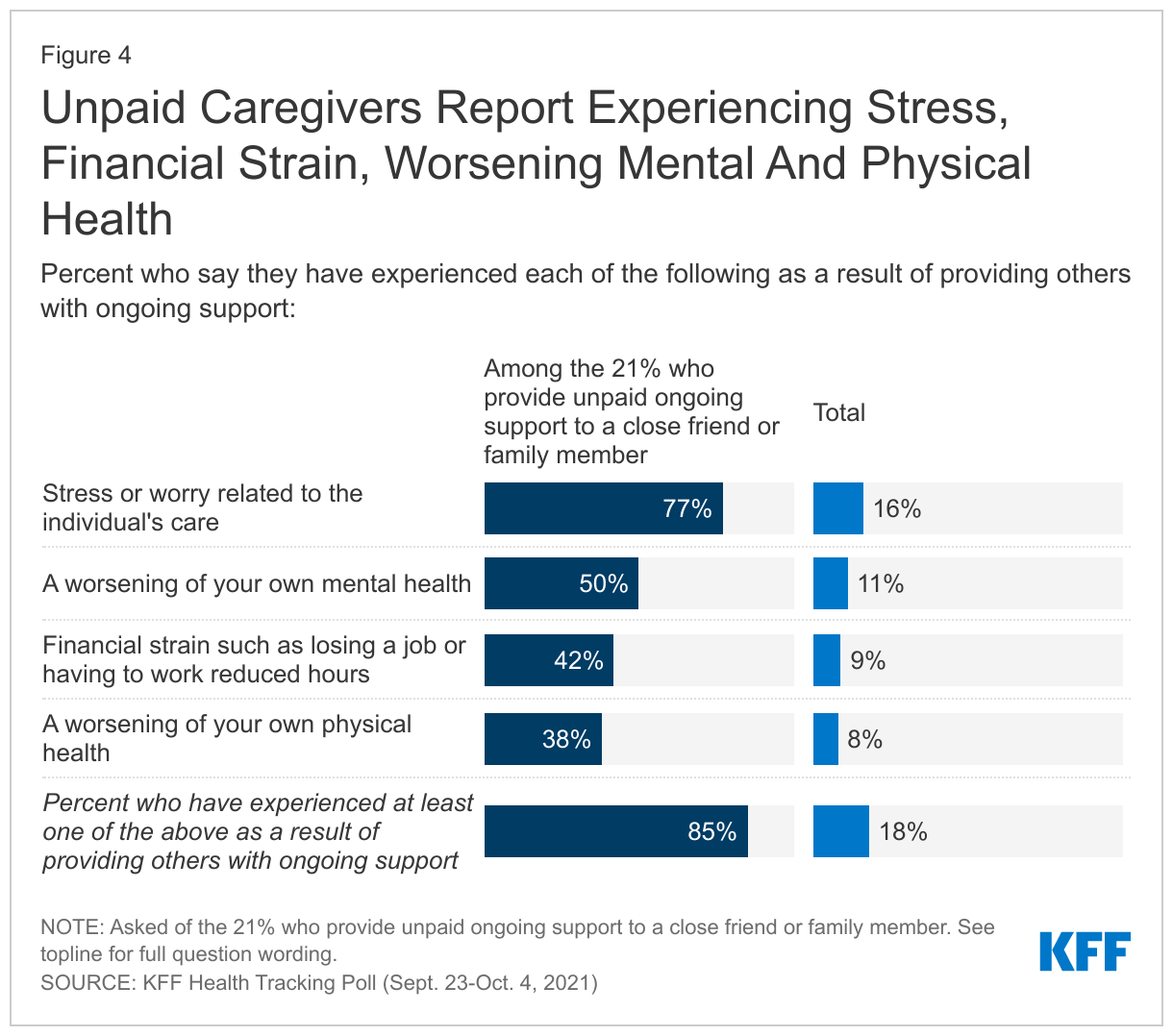
Consistent with recent focus groups conducted by KFF, the poll finds most unpaid caregivers (85%, 18% of all adults) report experiencing at least one of several negative outcomes due to their caregiving responsibilities. Over three-fourths of unpaid caregivers (16% of all adults) say they have experienced stress or worry related to the care of the individual they are caring for, with an additional half (11% of all adults) say they have experienced a worsening of their own mental health as a result of providing this ongoing support. About four in ten (9% of total) say they have experienced financial strain, such as losing a job or having to work reduced hours. A similar share (38% and 8% of total) also say they have experienced a worsening of their own physical health.
Expanding Medicare Benefits
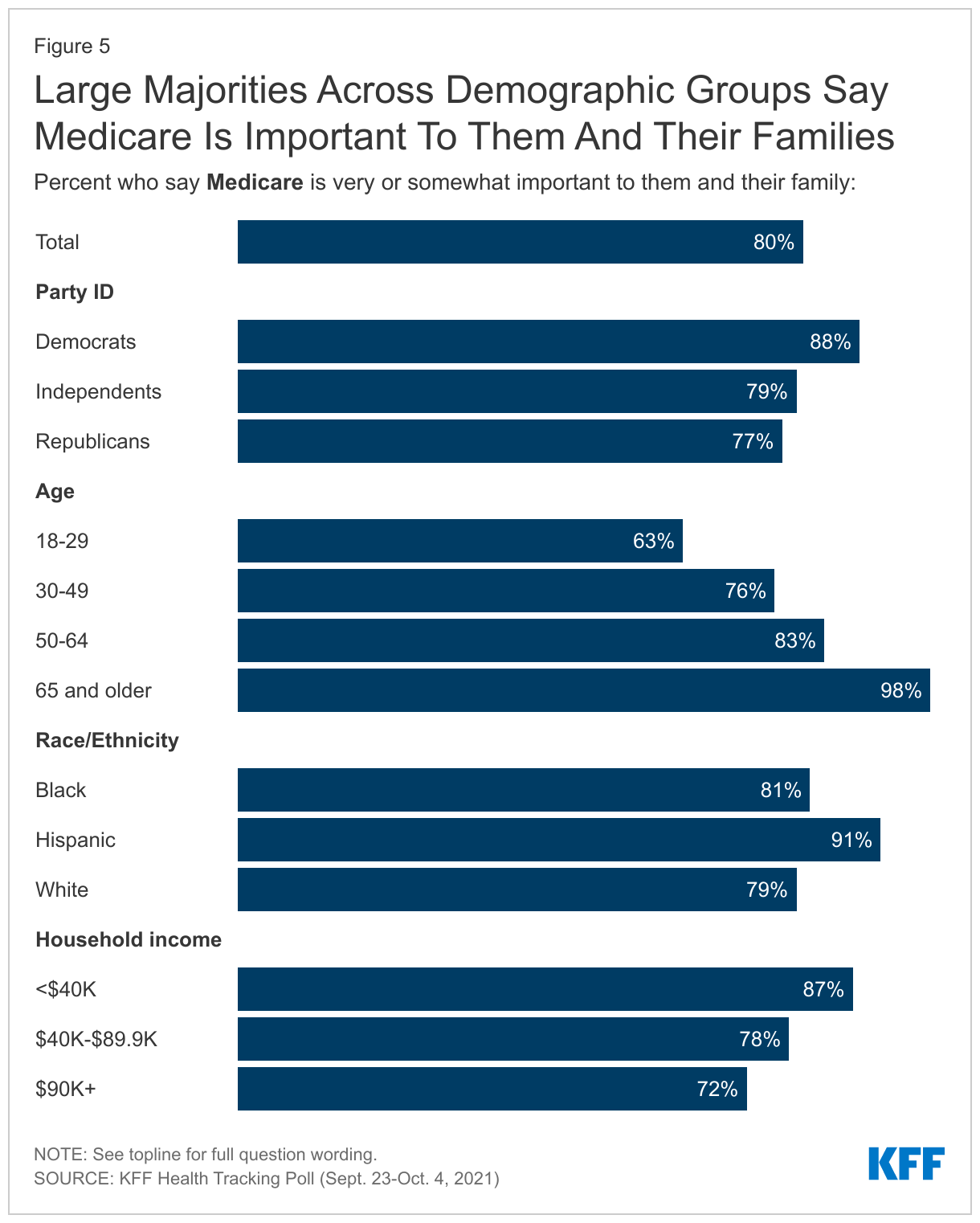
With Congress debating changes to the current Medicare program, eight in ten adults—and nearly all older adults—say Medicare is important to them and their family members. This includes at least seven in ten adults across partisanship, income groups, and racial and ethnic identity.
Significant shares of older adults in the U.S. report difficulty paying for various aspects of health care, especially services not generally covered by Medicare.2 Four in ten older adults (41%) report difficulty paying for dental care while three in ten report difficulty affording hearing or vision care (30%). Two in ten report difficulty affording their prescription drugs. Additionally, one-third report difficulty affording their out-of-pocket health care costs and one in five report the same about their monthly health insurance costs – shares comparable to those who report difficulty affording other household expenses such as rent or mortgage, gasoline, monthly utilities, or food and groceries.
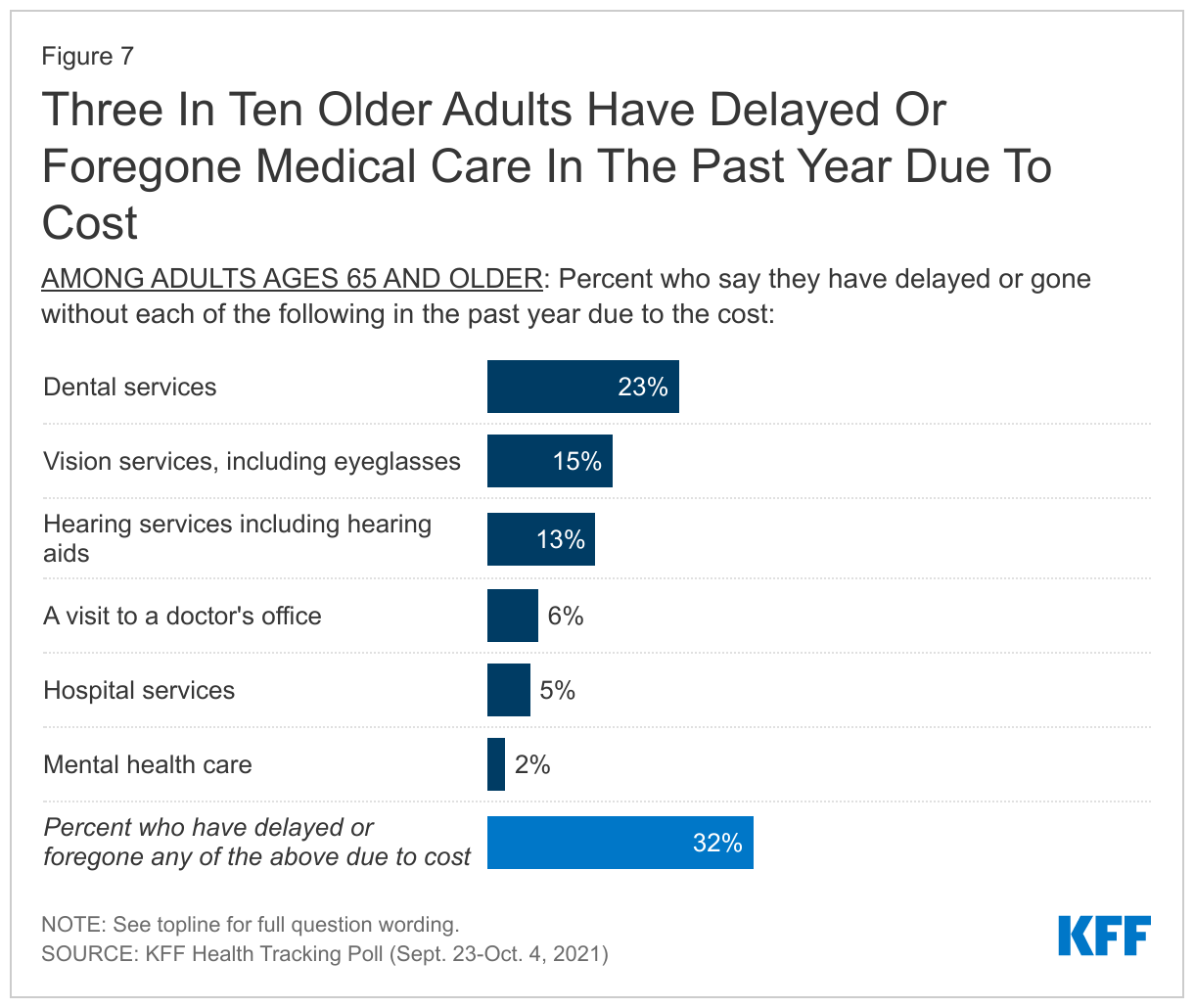
Dental services are the most common type of medical care that people have delayed or gone without with about with about one in four (23%) of adults ages 65 and older saying they have put off dental care in the past year due to cost. This is followed by vision services or eyeglasses (15%) and hearing aids (13%). Dental, vision, and hearing coverage are three benefits not generally covered by Medicare.
Few older adults report delaying or going without a doctor’s office visit (6%), hospital services (5%) or mental health care (2%) due to cost. Overall, three in ten adults 65 and older report delaying or going without certain medical care during the past year due to cost (32%).
Even among older adults who are eligible for Medicare, those with lower incomes report delaying or going without care at higher rates. More than four in ten older adults in households earning less than $40,000 annually report delaying or going without some form of medical care over the past year due to costs (compared to 24% of older adults with household incomes over $40,000). While Medicare helps older adults pay for routine doctor visits and hospital stays, substantial shares of lower income older adults report putting off or foregoing dental care (34%), vision care (20%), and hearing services including hearing aids (16%) that are not generally covered by Medicare.3
A large majority of the public (90%) favor expanding Medicare coverage to include dental, vision, and hearing coverage, including 97% of Democrats, 90% of independents, and 85% of Republicans. This proposal is also largely favored by adults 65 and older, including 96% of those in that age group who identify as Democrats or Democratic-leaning and 82% of their Republican counterparts. Proposals aimed at curbing the price individuals have to pay for their prescription drugs are favored by majorities of the public with at least eight in ten overall and at least three-fourths across partisans saying they favor each of the proposals asked about. Eighty-eight percent of adults favor limiting how much drug companies can increase the price for prescription drugs each year to not outpace the rate of inflation (including 93% of Democrats, 86% of independents, 89% of Republicans) and a similar share (85%) favor placing an annual limit on out-of-pocket prescription drug costs for people on Medicare (favored by 88% of Democrats, 85% of independents, 84% of Republicans). The proposed changes to Medicare drug negotiations as part of the reconciliation package poll findings were released earlier this week.
The Affordable Care Act
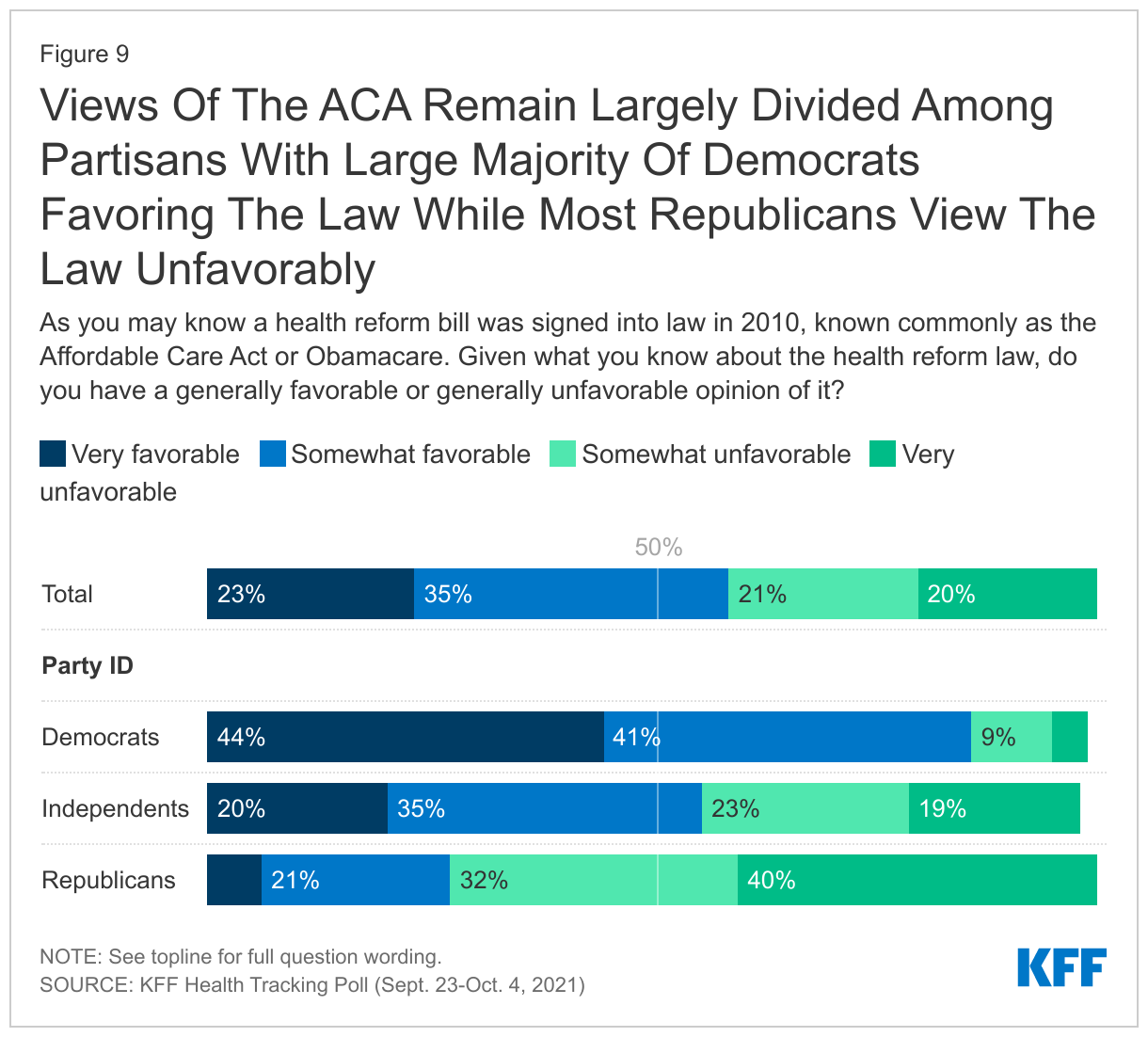
Views of the 2010 Affordable Care Act are still largely driven by party identification with nearly nine in ten Democrats saying they view the law favorably, while three-fourths of Republicans say they hold an unfavorable view. Independents are slightly more favorable than unfavorable with more than half saying they hold a positive opinion of the ACA. KFF has been polling on the ACA since its passage and since 2017 views have been more favorable than unfavorable but still sharply divided on party lines.
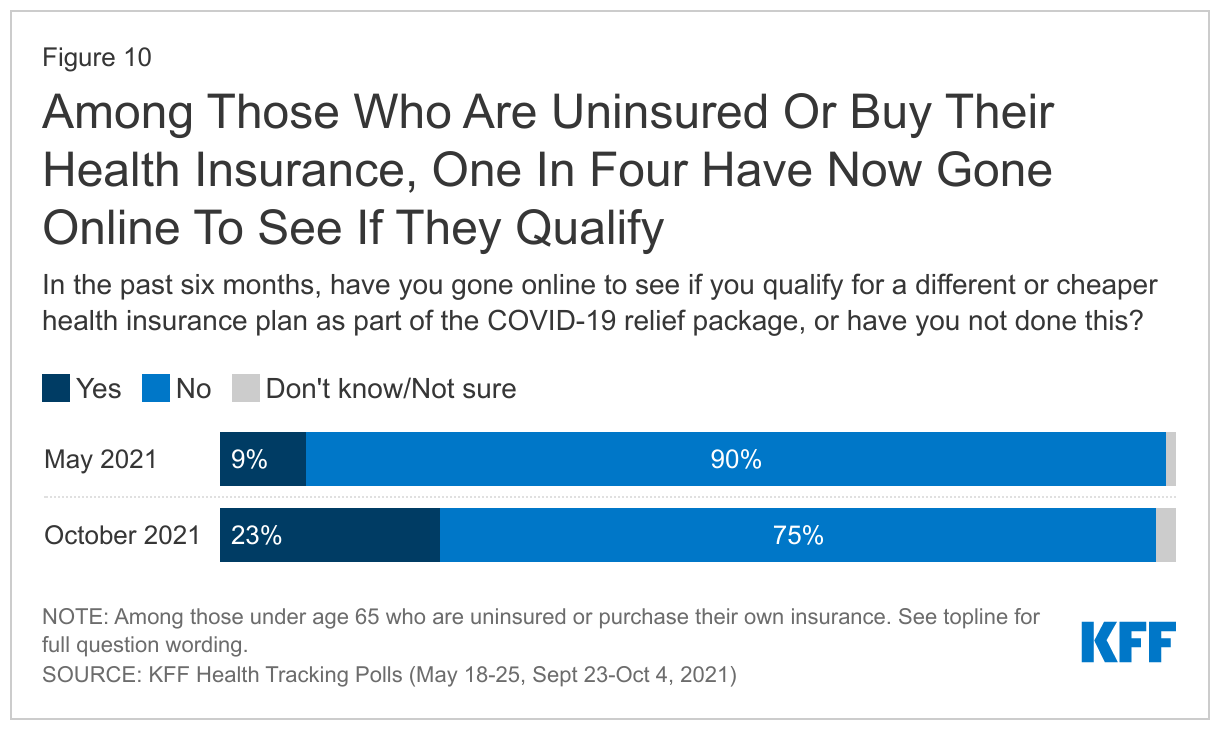
The COVID relief bill passed in early March 2021 providing additional financial help for people who buy their own health insurance coverage. Previous KFF polling found that a small minority of those likely eligible for additional financial help or coverage reporting going online to see if they qualify for a different or cheaper health insurance plan.
Among those under 65 years old, nine percent of those who are either uninsured or buy their own coverage reported going online in the in the two months before mid-May 2021 to see if they qualify for a different or cheaper health insurance plan or Medicaid as part of the COVID relief package. Four months later, the latest KFF polling finds that about one in four (23%) of those likely eligible for this assistance have gone online to see if they qualify, though majorities (75%) still have not.
In addition, changes to health insurance coverage provided under the Affordable Care Act continue to be seen through a partisan lens, with overwhelming majorities of Democrats and smaller majorities of Republicans expressing support. Overall, eight in ten adults favor making permanent the financial help to low- and moderate- income Americans who buy their own health insurance coverage (94% of Democrats, 79% of independents, 63% of Republicans). Three in four favor the federal government stepping in to provide insurance options for lower income people living in states that haven’t expanded their Medicaid programs (94% of Democrats, 76% of independents) but this is supported by a small majority (54%) of Republicans.
While the poll finds broad support for many of the Democratic proposed changes to the country’s health care system including the ACA, Medicaid, and Medicare, the poll did not ask about the potential costs and savings associated with each provision, or the size and scope of Democrats’ broader legislative plan, which includes many provisions unrelated to health care.
Methodology
The KFF Health Tracking Poll was conducted in English and Spanish with a nationally representative sample of 1,146 U.S. adults aged 18 or older, including an oversample of 474 adults ages 65 and older. The survey was conducted online and via phone from September 23-October 4, 2021, combining sample from two online probability-based panels and telephone samples recruited from random digit dialing (RDD). Sampling, data collection, weighting and tabulation were managed by SSRS of Glen Mills, PA in close collaboration with Kaiser Family Foundation researchers. The KFF team developed the questionnaire, analyzed the data and contributed financing for the survey.
Panel surveys were conducted through two online panels: (1) The SSRS Opinion Panel, a representative probability-based panel of U.S. adults ages 18 and older, recruited using the SSRS Omnibus poll (a weekly dual-frame RDD telephone survey) and through address-based sampling (ABS) (n=939). (2) The IPSOS KnowledgePanel, a probability-based online panel of U.S. adults ages 18 and older recruited through ABS targeting panelist (n=85). In order to reach adults 65 and older, a group less likely to be reached through an online panel, as well as those who do not have access to the internet, 122 interviews were completed by telephone, (including 79 among those who had previously indicated they do not use the internet).
The combined online, cell phone, and landline sample was weighted to match the sample demographics to estimates for the national population. A multi-stage weighting process was used to adjust for the fact that not all survey respondents were selected with the same probabilities and to account for systematic non-response. In the first weighting stage, adjustments were made regarding the probabilities of selection to the two web panels, and for probability of selection and non-response to the telephone callback samples. Each of these surveys were probability samples of the U.S. adult population that were weighted to the Census Bureau’s March 2020 Current Population Survey (CPS), by gender, age, race/ethnicity, education, and Census region. The data were also weighted to match internet usage metrics based on the U.S. Census’s 2019 American Community Survey, civic engagement metrics based on the September 2019 CPS Volunteering and Civic Life Supplement, and to match party identification within age groups from previous KFF RDD samples.
All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 4 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Group
N (unweighted)
M.O.S.E.
Total
1,146
± 4 percentage points
Age
18-64
672
± 5 percentage points
65+
474
± 7 percentage points
Party Identification
Democrats
476
± 6 percentage points
Republicans
231
± 8 percentage points
Independents
322
± 7 percentage points
Endnotes
A shortage of direct care workers predated and has been intensified by the COVID-19 pandemic, characterized by low wages and limited opportunities for career advancement. The direct care workforce is disproportionately female and Black. Debate in Congress to increase funding for Medicaid HCBS is aimed at strengthening the direct care workforce. ↩︎
In this column for the JAMA Health Forum, Larry Levitt explores why the Medicaid “coverage gap” still exists in 12 states that have not expanded their Medicaid programs under the Affordable Care Act, why it matters, and why eliminating it could prove challenging.
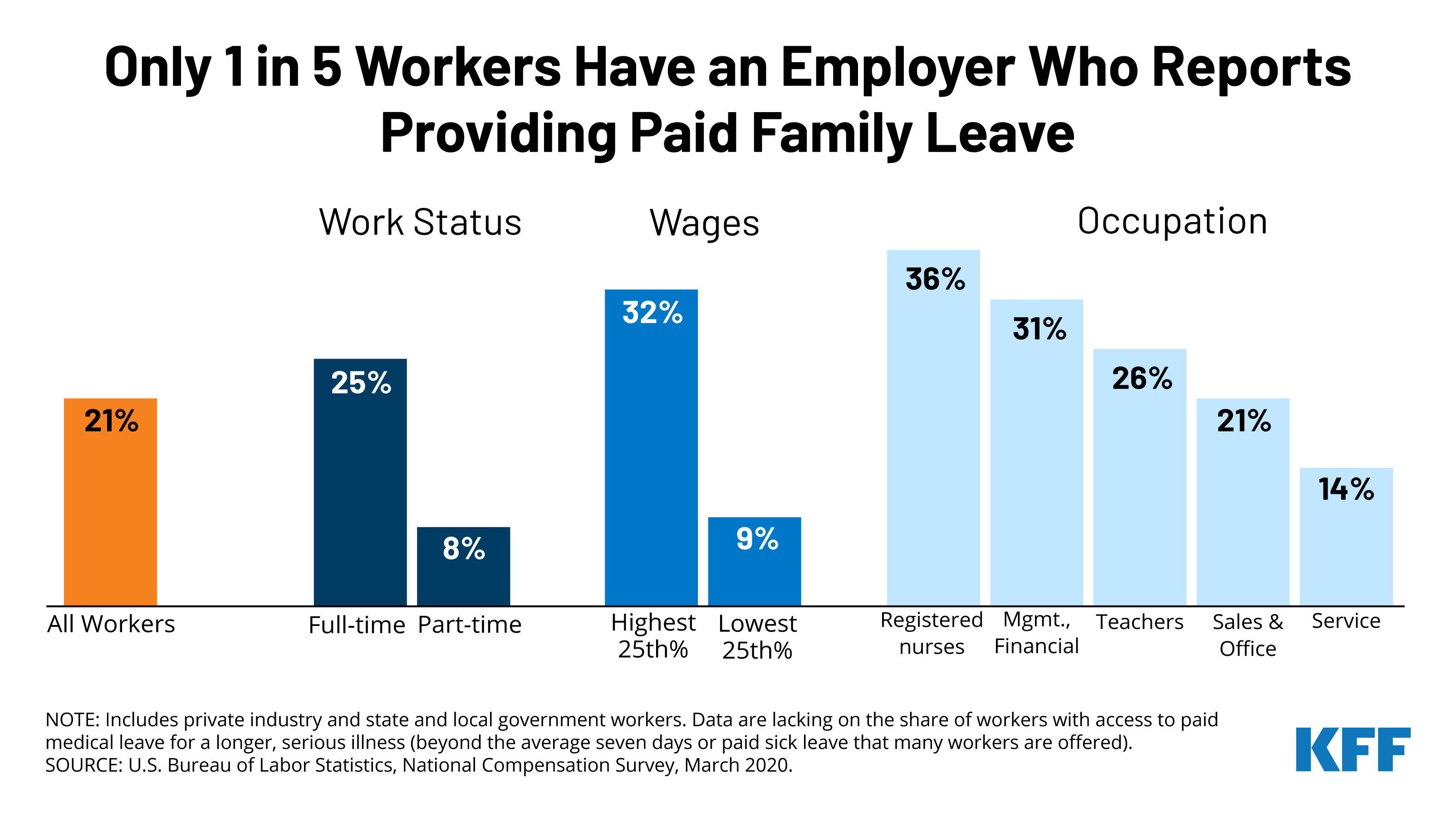
Most people will need to take time off work to care for themselves or their families at some point, but only one in five (21%) workers have access to paid family leave through their employer. That share is even lower for low-wage and part-time workers, and in certain occupations.
Congress is considering creating a universal paid family and medical leave program as part of the Build Back Better Act, which Democrats are looking to pass through the budget reconciliation process relying on Democratic votes. The proposal guarantees 12 weeks of paid family and medical leave annually to all workers in the United States for several qualifying reasons, including welcoming a new child, recovering from a serious illness, and caring for a seriously ill family member. It’s unclear how the program would be financed or whether more changes will be made as pressure to reduce the cost of the social spending package could limit the bill’s scope.
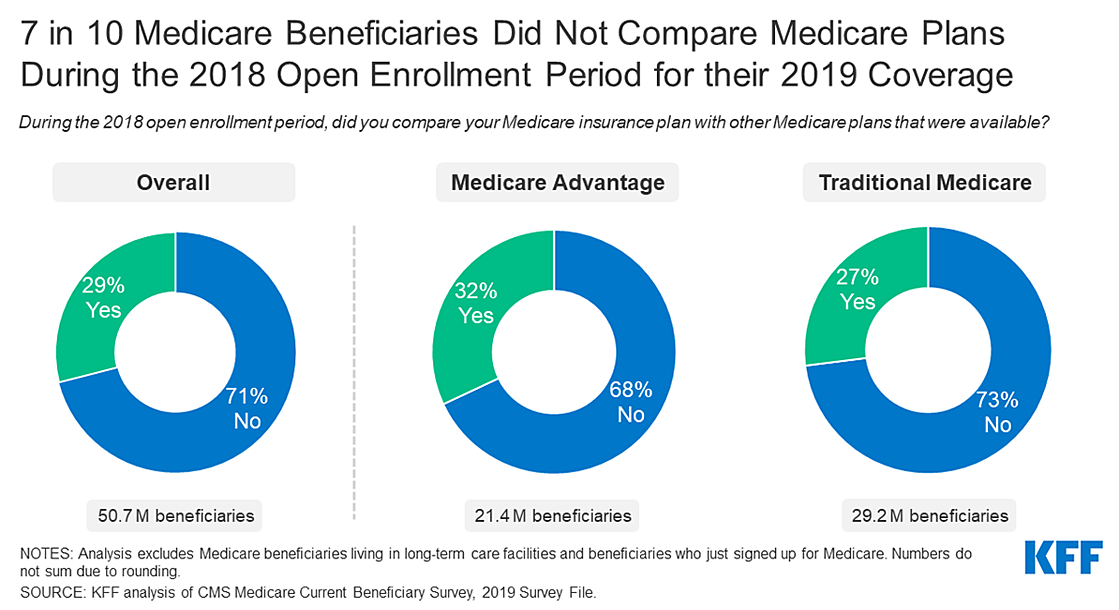
With the Medicare open enrollment period set to begin October 15, a new KFF analysis finds that 7 in 10 beneficiaries (71%) say that they didn’t compare their coverage options during a recent open enrollment season. Twenty-nine percent said they did compare Medicare plans.
But not shopping around can have a big impact on enrollees’ coverage and costs. The Centers for Medicare & Medicaid Services (CMS) recommends that beneficiaries review and compare Medicare plans each year.
The new analysis examines the share of Medicare beneficiaries who compared plans during the 2018 open enrollment period for coverage in 2019, the share who compared drug coverage in Medicare Advantage and stand-alone drug plans, and variation by demographic characteristics, based on an analysis of the 2019 Medicare Current Beneficiary Survey (the most recent year available).
Other key findings include:
• The share of beneficiaries who said they did not compare their options was higher among beneficiaries who are Black (74%) and Hispanic (79%), ages 85 and older (84%), with low incomes (85%), and those enrolled in both Medicare and Medicaid (87%).
• When it comes to Part D drug coverage, 81 percent of Medicare Advantage drug plan enrollees and 72 percent of Medicare stand-alone drug plan enrollees said they did not compare drug coverage offered by their current plan to other plans.
• Nearly half (47%) of all beneficiaries with Medicare said they had never visited the official Medicare website for information, 53 percent reported they had never called the 1-800-MEDICARE helpline and 31 percent said they did not read the Medicare & You handbook.
Medicare beneficiaries with traditional Medicare can compare and switch Medicare Part D stand-alone prescription drug plans or join a Medicare Advantage plan, the privately run alternative to traditional Medicare. At the same time, enrollees in Medicare Advantage can compare and switch Medicare Advantage plans or elect coverage under traditional Medicare with or without a stand-alone drug plan.
Coverage and costs vary widely among both Medicare Advantage plans and Part D prescription drug plans. Plans can change from one year to the next, as can beneficiaries’ health care needs, which could lead to unexpected and avoidable costs, and disruptions in care for beneficiaries who stay put and do not at least review their options annually.
With much attention on the public’s view on Medicare drug price negotiations, the latest KFF Tracking Poll finds large majorities support allowing the federal government to negotiate and this support holds steady even after the public is provided the arguments being presented by parties on both sides of the legislative debate (83% total, 95% of Democrats, 82% of independents, and 71% of Republicans).
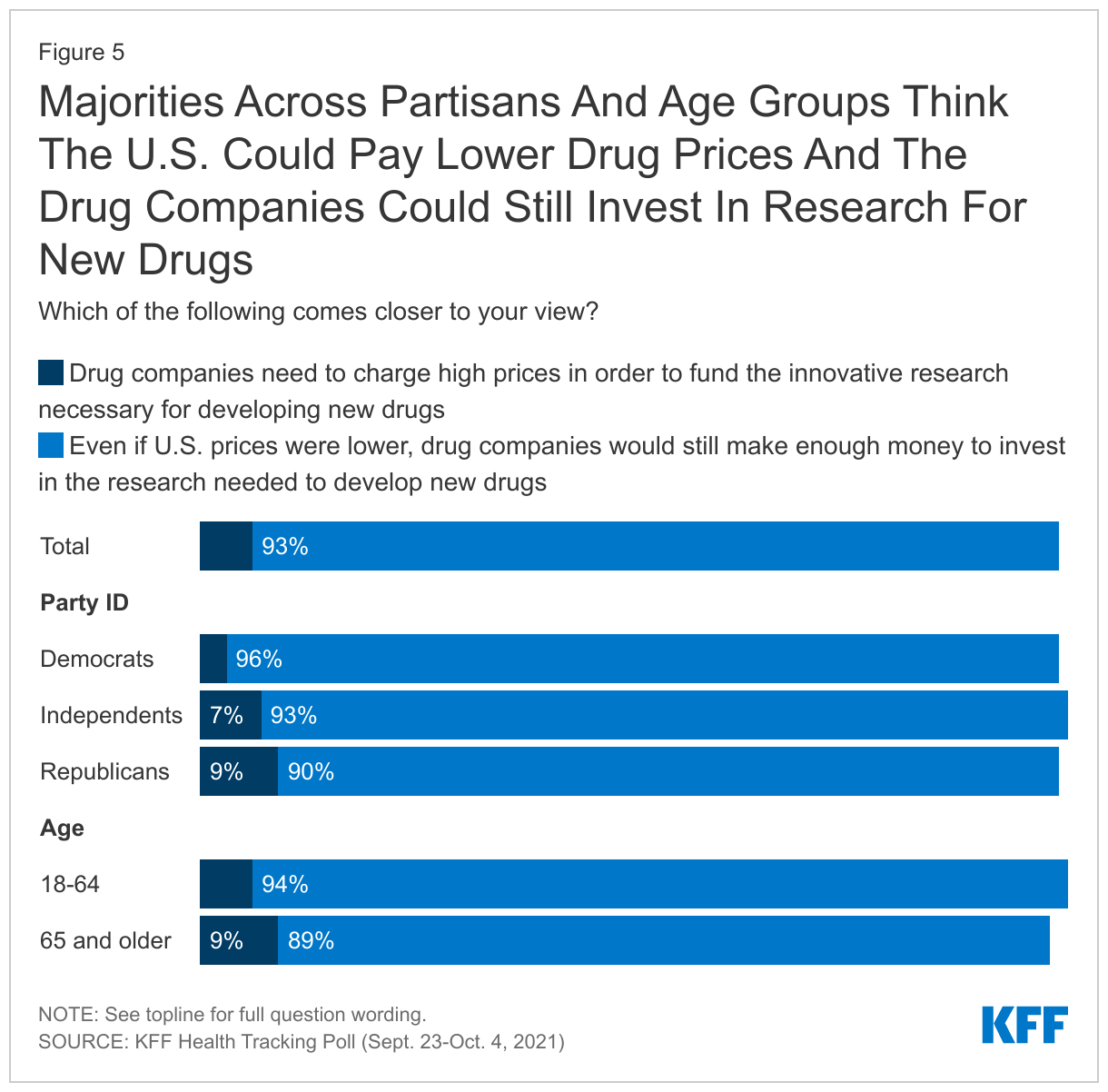
Most adults – across partisans – don’t believe high drug prices are needed for drug companies to invest in new research instead agreeing that “even if U.S. prices were lower, drug companies would still make enough money to invest in the research needed to develop new drugs.” The results suggest that while hearing individual arguments may shift some views, the public still largely favors allowing Medicare drug negotiations when presented with the entirety of the public debate.
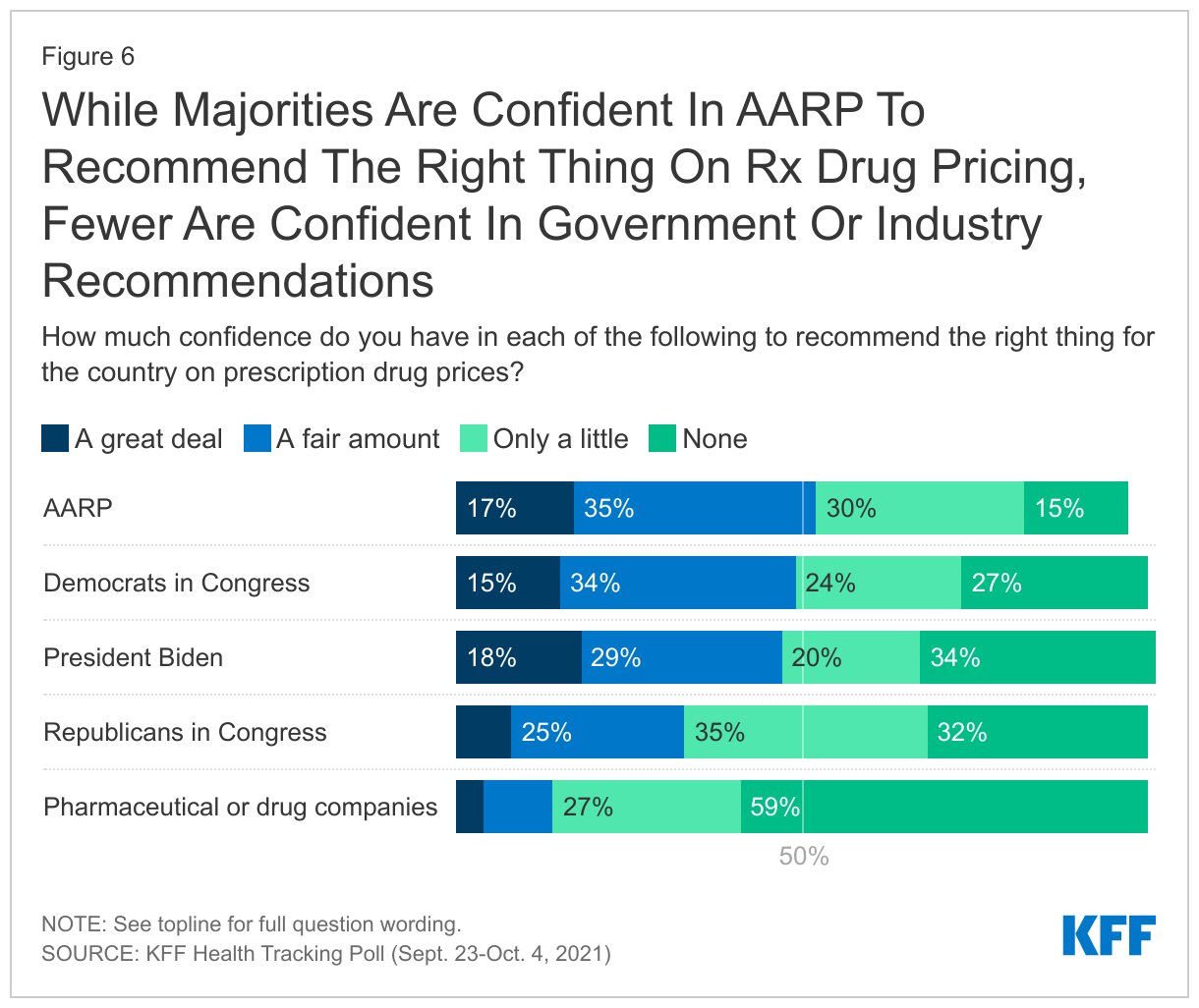
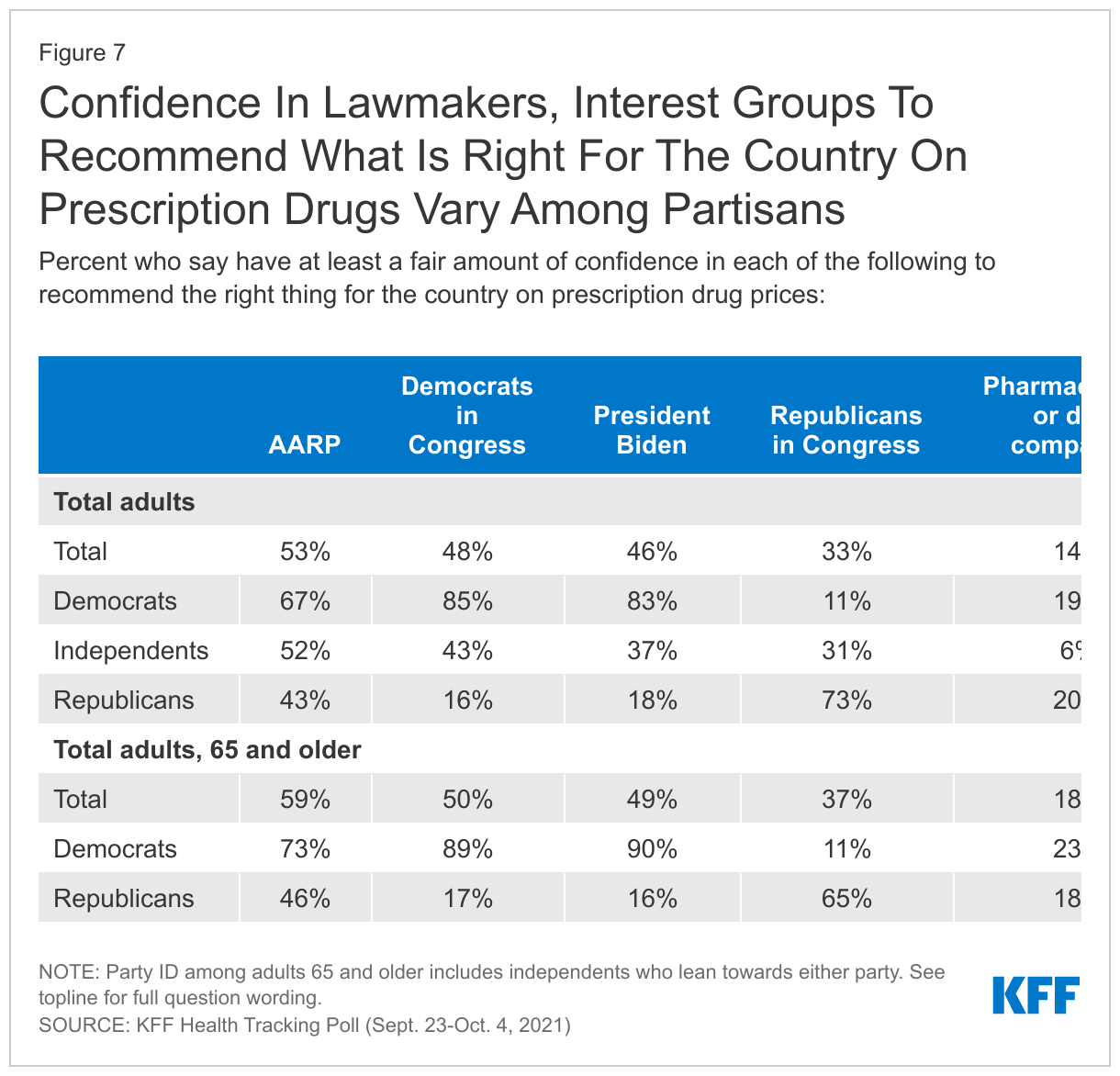
As the debate over how to address prescription drugs continues, less than half of the public say they have confidence in President Biden or either party in Congress to recommend the right thing for the country on prescription drug prices, but Democratic lawmakers fare better than Republican ones. Among interest groups, AARP garners a slight majority of adults saying they are confident in the organization’s ability to recommend the right thing for the country on prescription drug pricing while fewer (14%) have the same level of confidence in pharmaceutical companies.
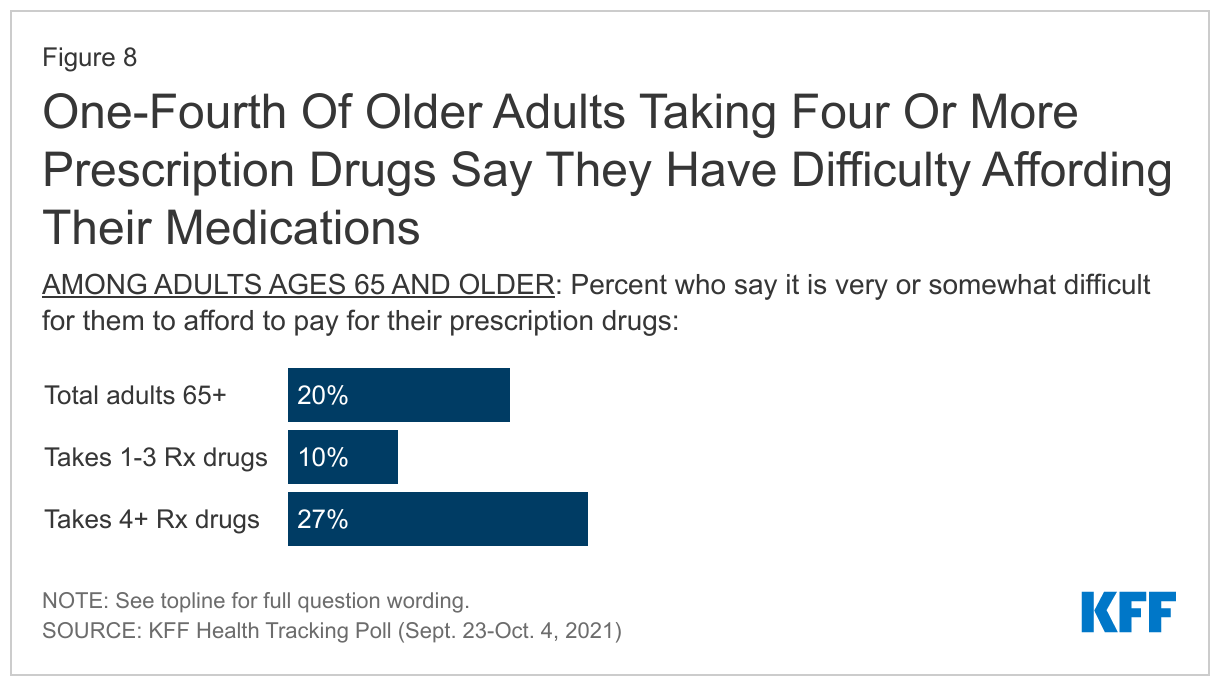
While 85% of adults ages 65 and older report having some type of insurance that helps pay for prescription drugs, one in five older adults still report difficulty affording their prescription drugs, including 17% of older adults with some type of prescription drug coverage. The share who report difficulty affording prescription drugs increases to more than one in four among adults 65 and older who take four or more prescription drugs.
Public Favors Medicare Drug Negotiations
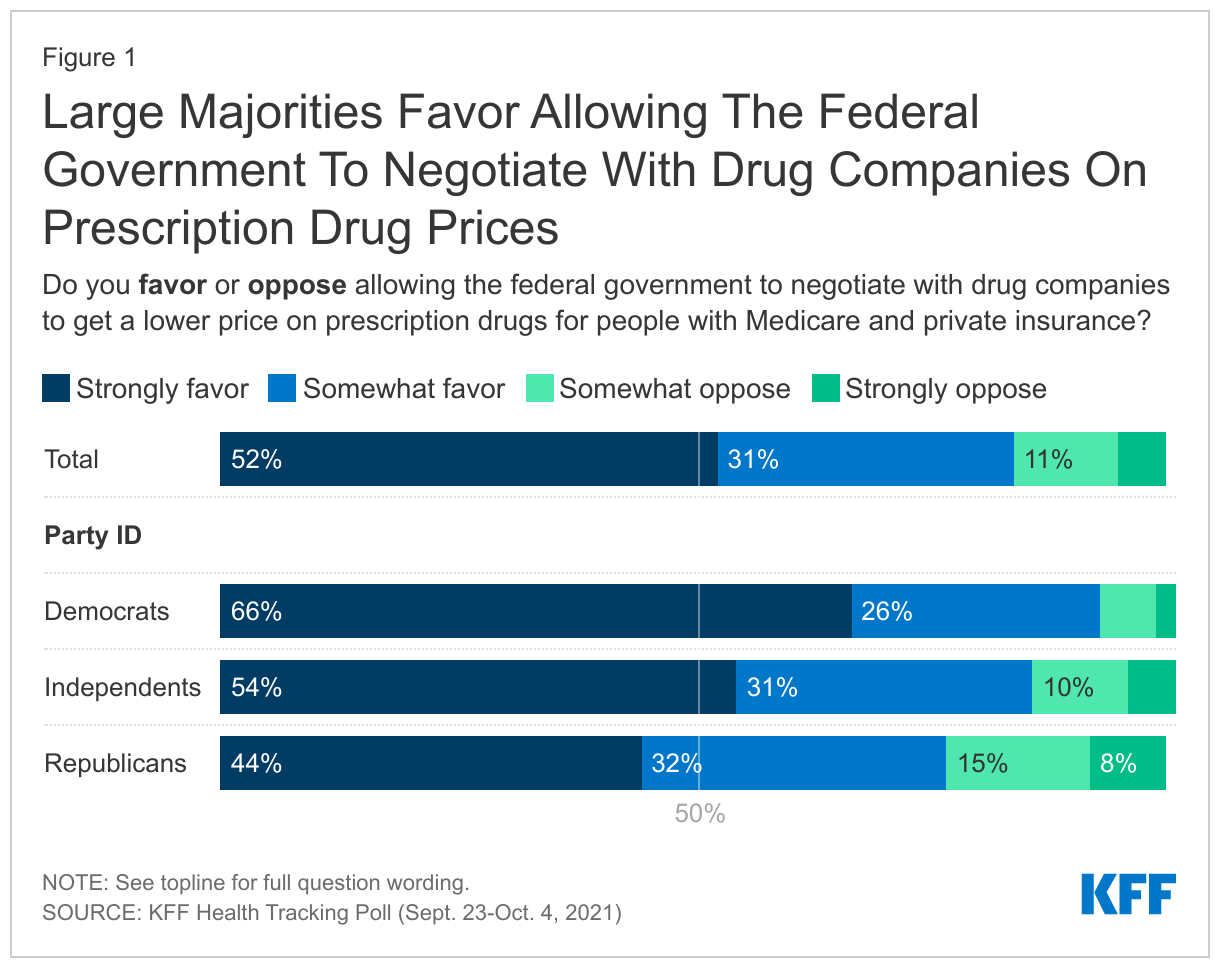
About eight in ten U.S. adults (83%) and adults 65 and older (78%) say they think the cost of prescription drugs is “unreasonable.” Lowering prescription drug prices in the U.S. has been a health care policy priority for decades and earlier this year, it topped the list of health care issues the public wanted Congress to tackle. One proposal aimed at lowering the cost of prescription drugs is to allow the federal government to negotiate the price of prescription drugs for people on Medicare and private insurance.
The Democrats’ budget reconciliation package includes a proposal to allow the federal government to negotiate prescription drug prices on behalf of Medicare beneficiaries and people enrolled in private plans. The proposal, which has been part of previous legislative proposals and previously estimated by The Congressional Budget Office (CBO) to result in about $450 billion in savings to Medicare1 , has met strong opposition from the pharmaceutical industry, as well as some lawmakers. Yet, the proposal is largely popular among the public across partisans as well as among seniors, the group most directly impacted by such legislation. Eight in ten adults (83%) say they either “strongly favor” or “somewhat favor” allowing the federal government to negotiate with drug companies as do 84% of older adults (65 and older), including the vast majority (93%) of those ages 65 and older who identify as either a Democrat or lean Democratic, and three-fourths (76%) of older adults who are Republican or lean Republican.
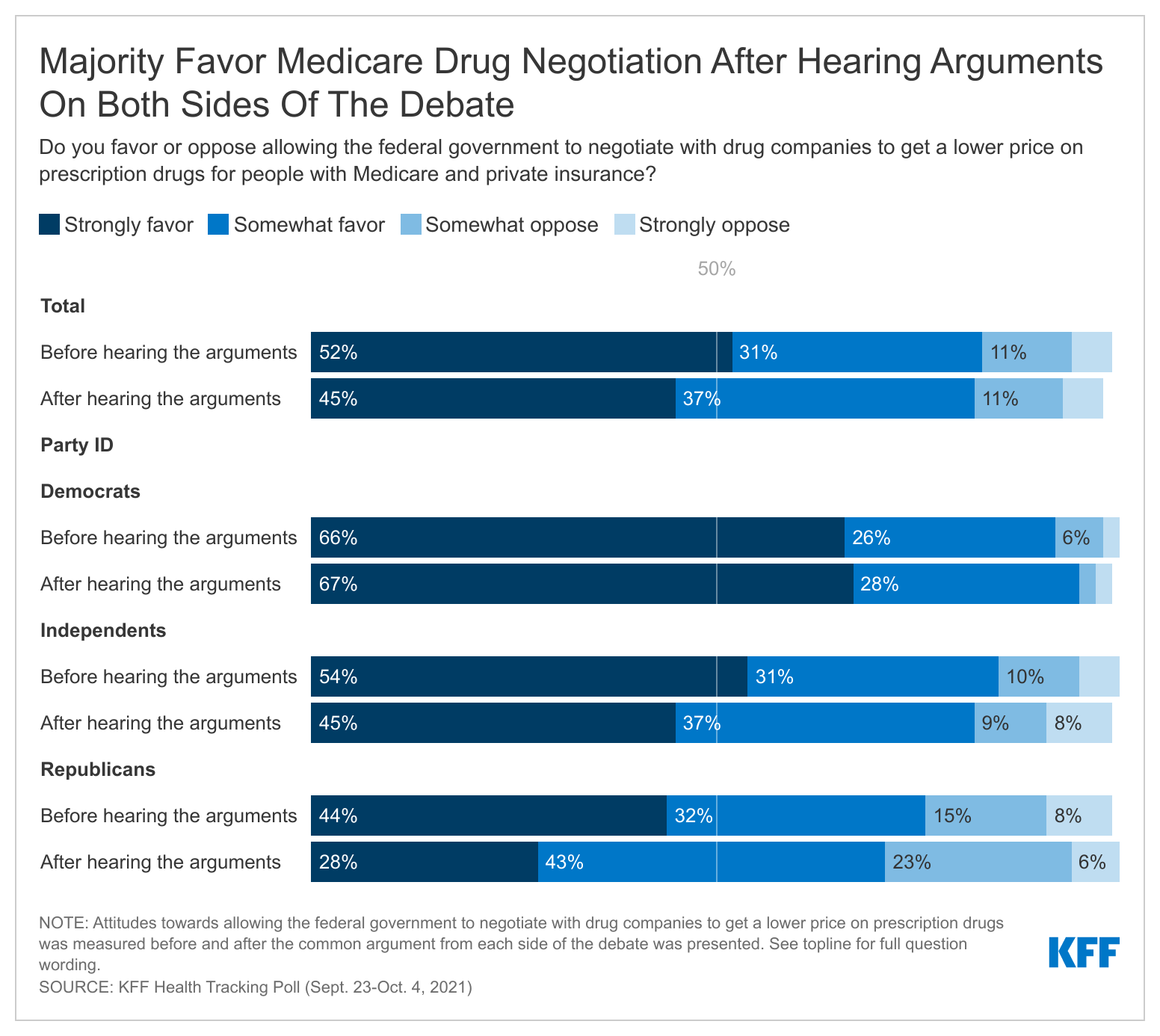
Previous KFF polls have found that some attitudes are malleable on this issue as the public hears arguments from either side of the debate around Medicare drug price negotiations. The latest poll finds that when the public are presented with the main arguments being made by advocates on both sides of the debate, the shift in opinion is modest and support for negotiation remains high. After gauging initial support allowing the federal government to negotiate prices with drug companies, the poll presented respondents with arguments both for and against the proposal.
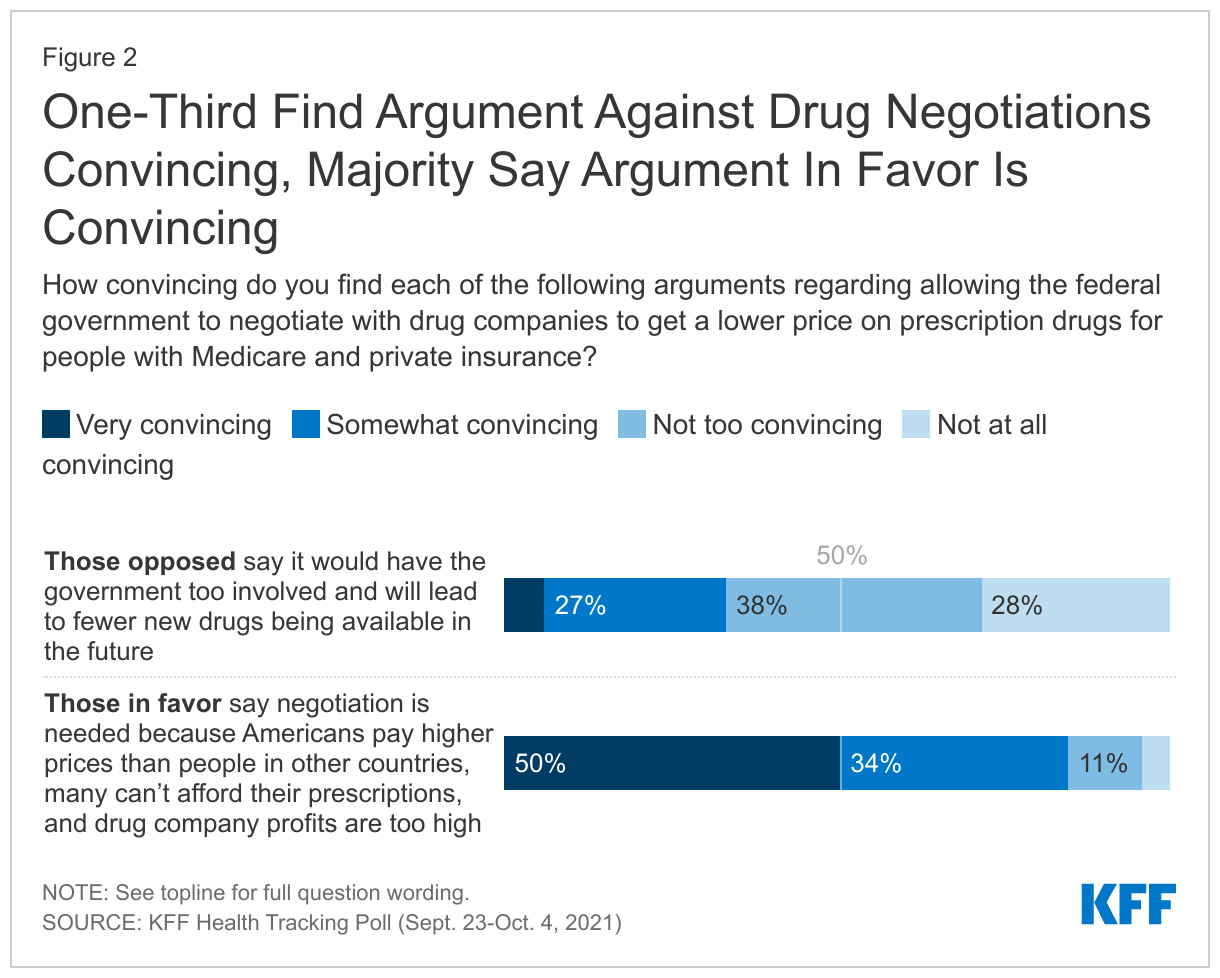
Argument against: People opposed to allowing the federal government to negotiate prices with drug companies say this would have the government too involved and will lead to fewer new drugs being available in the future.
Argument in favor: People in favor of allowing the federal government to negotiate prices with drug companies say this is needed because Americans pay higher prices than people in other countries, many can’t afford their prescriptions, and drug company profits are too high.
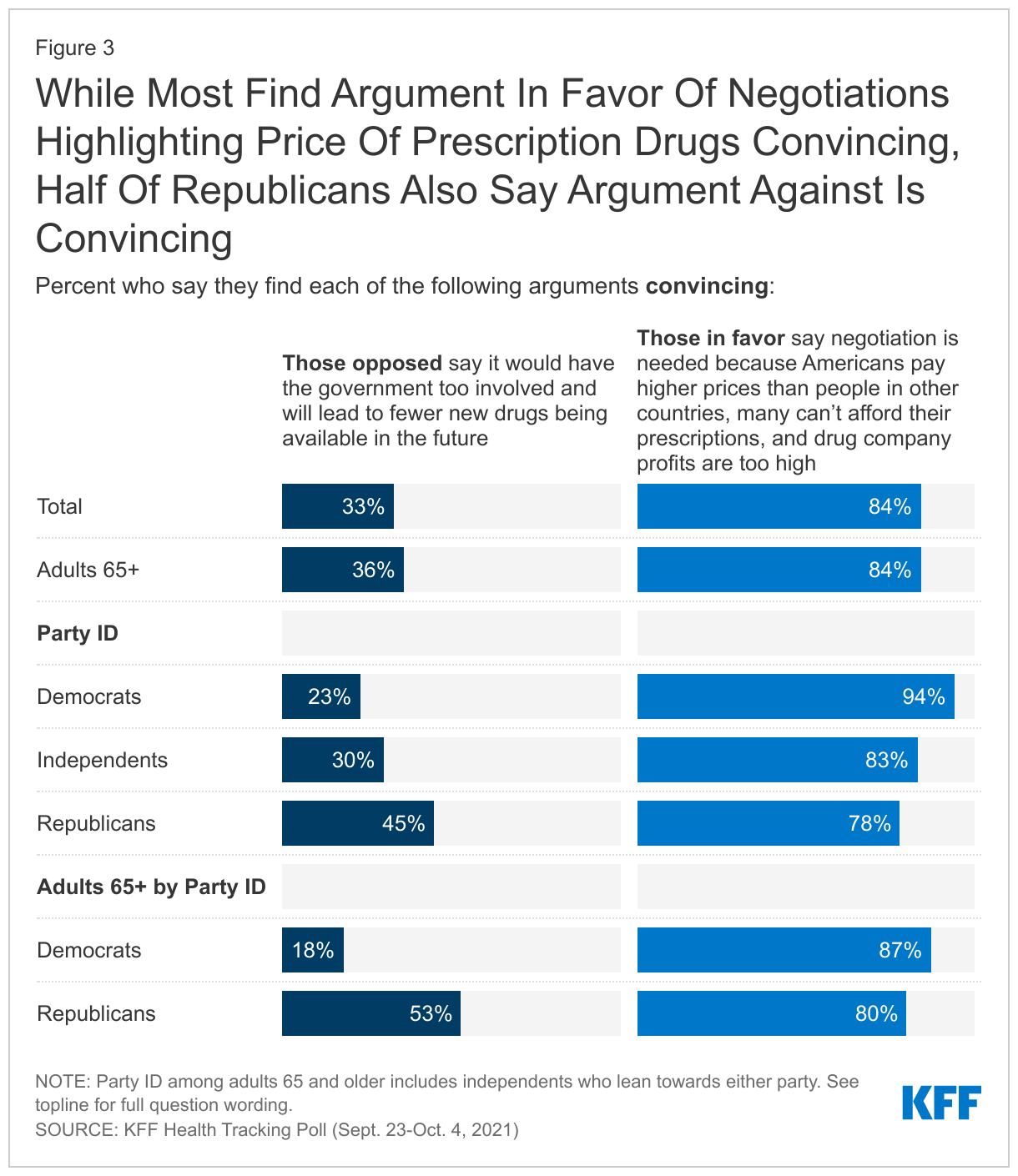
One-third of the public say the argument from those opposed to drug price negotiations is convincing compared to a large majority (84%) who say they found the argument from those in favor convincing.
Majorities of all adults as well as those 65 and older, across partisans, say they found the argument in favor of drug negotiations convincing while a smaller share said the same about the argument against the drug negotiations. Nearly half (45%) of all Republicans said the argument from those opposed, which highlights the increased role of the government and the drug companies’ stance that this will lead to fewer drugs coming to market, is also convincing. More than half (53%) of adults 65 and older who are Republican or Republican-leaning say they found the argument against drug negotiations convincing, compared to 18% of Democrat or Democratic-leaning older adults.
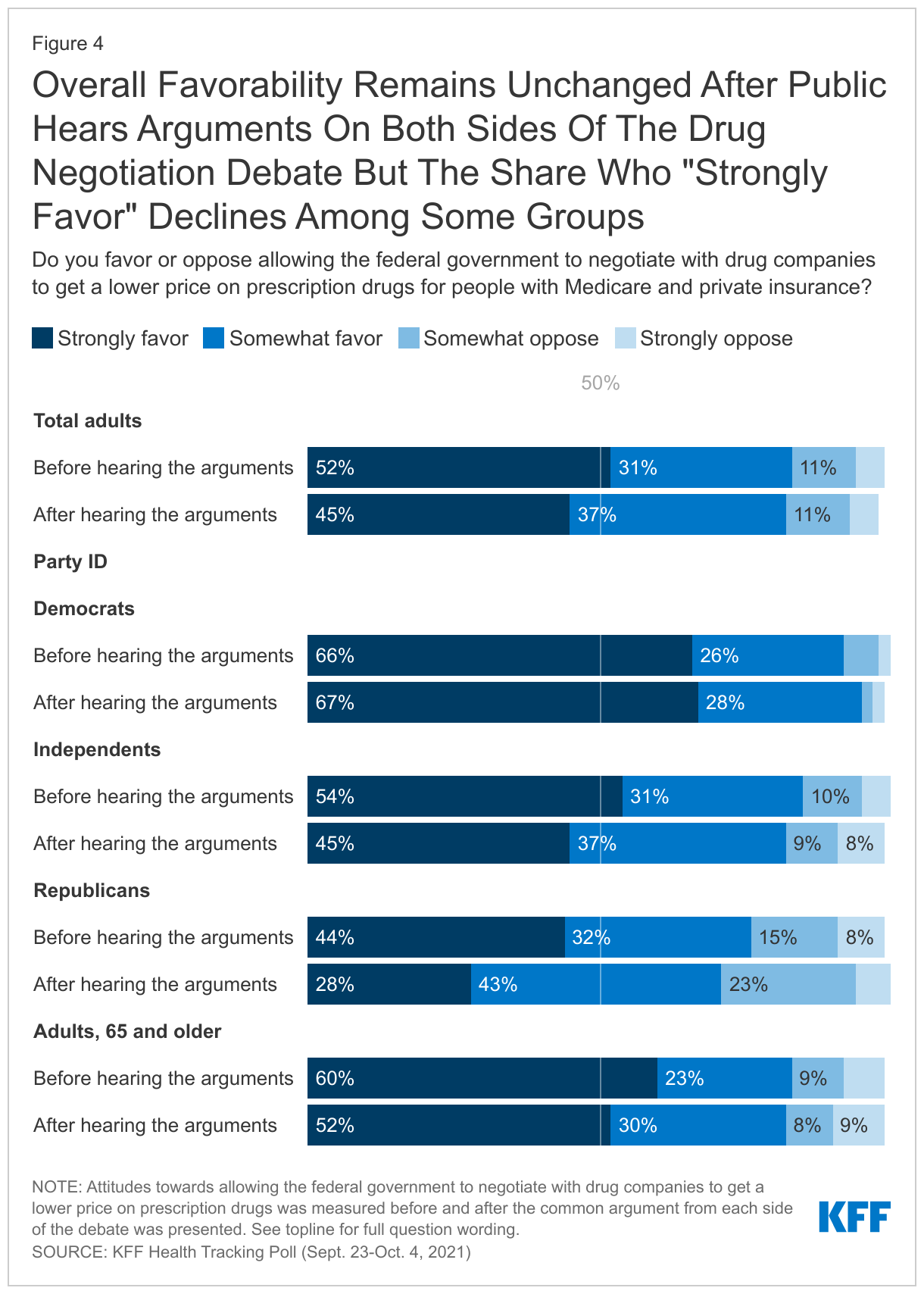
After hearing the arguments for and against the proposal to allow the federal government to negotiate prices with drug companies, attitudes remained relatively unchanged with a majority continuing to favor this proposal. While overall favorability stays the about same, there are some small shifts among groups especially in the share who “strongly favor” this proposal. For example, overall Republican support for drug negotiations decreases five percentage points but there is a large shift among those who say they “strongly favor” after hearing both arguments (44% to 28%). But even so, a majority of Republicans (71%) continue to support the proposal after hearing the arguments.
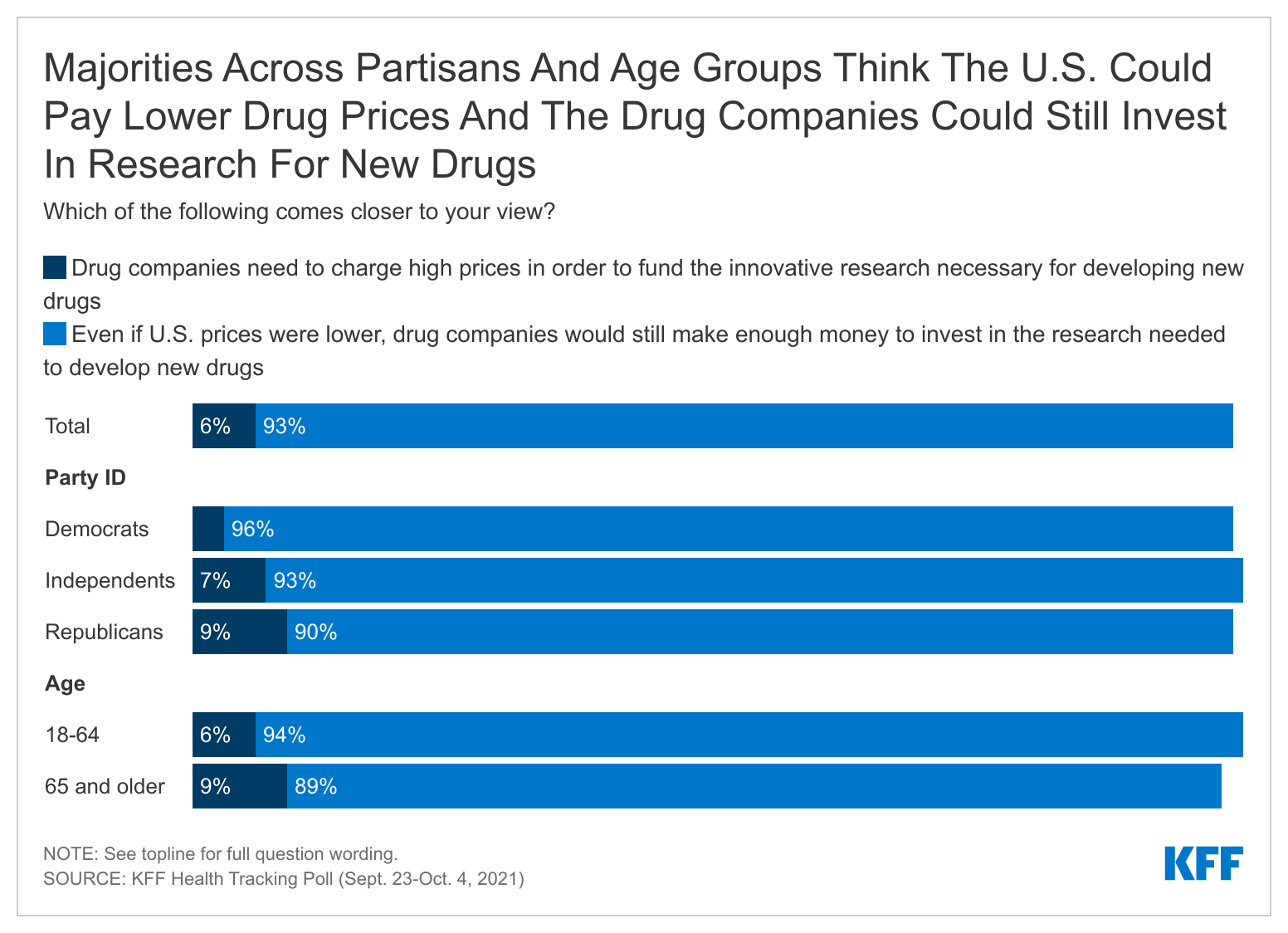
The pharmaceutical industry has argued that allowing the federal government to negotiate prescription drug prices will lead to less research and development of new prescription drugs. KFF polling finds few people (6%) saying they think “drug companies need to charge high prices in order to fund the innovative research necessary for developing new drugs” while a large majority (93%) say “that even if U.S. prices were lower, drug companies would still make enough money to invest in the research needed to develop new drugs” comes closer to their view. This view is consistent across partisanship and age groups.
Few Have Public’s Confidence To Recommend The Right Thing On Prescription Drug Pricing
Neither President Biden nor members of either party in Congress has gained the full confidence of the public to do what’s right for the country on prescription drug pricing. Slightly less than half of the public say they have “a great deal” or “a fair amount” of confidence in President Biden (46%) or Democrats in Congress (48%) to recommend the right thing for the country on prescription drug prices. One-third of the public (33%) say they have at least a fair amount of confidence in Republicans in Congress and few are confident that pharmaceutical companies will recommend the right thing (14%).
A slight majority of adults are confident in AARP’s ability to recommend the right thing for the country on prescription drug pricing. AARP is a non-partisan interest group focusing on the issues that impact adults over the age of 50 that has strongly advocated for Medicare drug negotiations.
AARP also has the confidence of older adults with about six in ten adults 65 and older saying they have at least “a fair amount” of confidence in AARP to recommend what is right for the country on prescription drugs.
One In Five Seniors Struggle Affording Prescription Drugs
The latest KFF Health Tracking Poll finds that 85% of adults ages 65 and older report having some type of insurance that helps pay for prescription drugs. Even still, one in five older adults report difficulty affording their prescription drugs, including 17% of older adults with some type of prescription drug coverage. The share who report difficulty affording prescription drugs increases to more than one in four among adults 65 and older who take four or more prescription drugs.
Methodology
The KFF Health Tracking Poll was conducted in English and Spanish with a nationally representative sample of 1,146 U.S. adults aged 18 or older, including an oversample of 474 adults ages 65 and older. The survey was conducted online and via phone from September 23-October 4, 2021, combining sample from two online probability-based panels and telephone samples recruited from random digit dialing (RDD). Sampling, data collection, weighting and tabulation were managed by SSRS of Glen Mills, PA in close collaboration with Kaiser Family Foundation researchers. The KFF team developed the questionnaire, analyzed the data and contributed financing for the survey.
Panel surveys were conducted through two online panels: (1) The SSRS Opinion Panel, a representative probability-based panel of U.S. adults ages 18 and older, recruited using the SSRS Omnibus poll (a weekly dual-frame RDD telephone survey) and through address-based sampling (ABS) (n=939). (2) The IPSOS KnowledgePanel, a probability-based online panel of U.S. adults ages 18 and older recruited through ABS targeting panelist (n=85). In order to reach adults 65 and older, a group less likely to be reached through an online panel, as well as those who do not have access to the internet, 122 interviews were completed by telephone, (including 79 among those who had previously indicated they do not use the internet).
The combined online, cell phone, and landline sample was weighted to match the sample demographics to estimates for the national population. A multi-stage weighting process was used to adjust for the fact that not all survey respondents were selected with the same probabilities and to account for systematic non-response. In the first weighting stage, adjustments were made regarding the probabilities of selection to the two web panels, and for probability of selection and non-response to the telephone callback samples. Each of these surveys were probability samples of the U.S. adult population that were weighted to the Census Bureau’s March 2020 Current Population Survey (CPS), by gender, age, race/ethnicity, education, and Census region. The data were also weighted to match internet usage metrics based on the U.S. Census’s 2019 American Community Survey, civic engagement metrics based on the September 2019 CPS Volunteering and Civic Life Supplement, and to match party identification within age groups from previous KFF RDD samples.
All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 4 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Most of the Public Lacks Confidence that President Biden, Congressional Democrats or Republicans Will Do the Right Thing on Drug Prices
Allowing the federal government to negotiate with drug companies to lower drug prices for Medicare beneficiaries and people enrolled in private plans – a key cost-saving proposal in the Democrats’ massive reconciliation bill – is favored by large majorities across political partisans, even after they hear arguments from both sides, a new KFF Health Tracking Poll finds.
Initially 83% of the public say they favor allowing the federal government to negotiate with drug companies to lower drug prices on behalf of people enrolled in Medicare beneficiaries and private plans. This includes 91% of Democrats, 85% of independents, and 76% of Republicans, as well as majorities of seniors (84%), who would be most affected by such a provision.
To gauge the potential impact of a national debate over the proposal, the survey asked the public to assess a summary of key arguments being made for and against the plan. Those arguments do little to move the share of the public that favors or opposes the proposal, though affected the intensity of support among Republicans. While Republican support held steady (76% to 71%), the share who “strongly favor” it dipped (44% to 28%).
When asked specifically about each argument, most (84%) of the public, including three-quarters (78%) of Republicans, say the argument in favor – “this is needed because Americans pay higher prices than people in other countries, many can’t afford their prescriptions, and drug company profits are too high” – is convincing.
On the other side, a third (33%) say the argument against – “this would have the government too involved and will lead to fewer new drugs being available in the future” – is convincing. This includes nearly half (45%) of Republicans.
The public also rejects the argument that high prices are necessary for supporting research into new drugs.
When asked which comes closer to their view, 93%, including 90% of Republicans, say “that even if U.S. prices were lower, drug companies would still make enough money to invest in the research needed to develop new drugs”, while just 6% say that “drug companies need to charge high prices in order to fund the innovative research necessary for developing new drugs.”
The poll also reveals that the public does not have a lot of confidence in Washington to address the issue. Less than half the public say they have confidence in President Biden (46%) and Democrats in Congress (48%) to recommend the right thing on prescription drug prices, while a third say they have confidence in Republicans in Congress (33%).
Among key interest groups, more say they are confident in the recommendations of AARP (53%), which has strongly advocated for drug-price negotiations, than say so about drug companies (14%).
Additional findings from the KFF Health Tracking Poll will be released later this week.
Designed and analyzed by public opinion researchers at KFF, the KFF Health Tracking Poll was conducted from September 23-October 4 among a nationally representative sample of 1,146 adults including an oversample of adults, 65 and older (474). Interviews were conducted in English and Spanish online (1,024) and by telephone (122). The margin of sampling error is plus or minus 4 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
In Focus Groups, Direct Care Workers and Unpaid Caregivers Describe Low-Wage, Physically-Challenging Work That is Often Mentally Overwhelming and Marked By Uncertainty
In recent focus group interviews, 32 paid direct care workers and unpaid caregivers who assist seniors and people with disabilities with self-care and household activities describe daily work defined by low pay, physical demands and mental stress that has been made worse by the pandemic.
KFF conducted the four focus groups in July and August 2021 with 24 direct care workers and eight unpaid caregivers to help provide context for the ongoing debate in Congress about increasing federal funding for Medicaid home and community-based services (HCBS). Medicaid is the nation’s primary payer for such services. Among other uses, new funding could help raise wages for direct care workers, provide training opportunities and offer supports to family caregivers such as respite care and peer supports.
Key takeaways from the focus groups include:
These jobs are mentally demanding as well as physically taxing. Paid caregivers reported that the mental demands of their jobs had intensified during COVID-19. Among other things, they cited the fear of infecting their clients or bringing the virus home to infect their families. Unpaid family caregivers described the mental demands associated with caregiving as often “overwhelming.”
Uncertainty is a constant. A number of paid caregivers described regularly experiencing uncertainty about whether they would be able to leave work at the end of their shift due to staffing shortages and scheduling challenges that were exacerbated by the pandemic. (It is unclear how vaccination mandates might contribute to workforce shortages, as participants in the paid direct care worker groups were divided about whether to receive the COVID-19 vaccine.)
Caregivers feel there is a mismatch between their work and their wages. Paid direct care workers universally agreed that their wages are low and do not reflect the demands of their jobs. They described their financial situation as “getting by” and “living paycheck to paycheck.” Some participants in the unpaid caregiver group said the demands of caregiving made it impossible to have paid work.
The racially and geographically diverse group of focus group participants worked in a range of job types, both full- and part-time, and cared for people with a variety of disabilities and long-term care needs. The report presents key highlights from the focus groups including caregiver characteristics; physical and mental caregiving demands; the impact of workforce shortages; wages, finances, and opportunities for advancement; and what caregivers would like policymakers to know about their work. While these focus groups are not necessarily generalizable to all caregivers, they can provide insight into their experiences to help inform current policy debates.
The American Rescue Plan Act (ARPA), passed earlier this year, provides states with a one-year, 10 percentage point increase in federal Medicaid matching funds (FMAP) for HCBS. Congress is currently debating efforts to increase federal matching funds, without a time limit, for state spending on Medicaid HCBS as part of an overall budget reconciliation package, although the final funding amount remains in flux as policymakers weigh competing priorities.
The COVID-19 pandemic has intensified longstanding issues surrounding the unmet need for home and community-based services (HCBS) among seniors and people with disabilities and shortages in the direct care workforce that provides these services. The Biden Administration recently announced that it will require vaccination for staff in Medicaid and Medicare certified home health agencies, along with nursing homes and other health care settings. However, a notable share of direct care workers are vaccine hesitant, so new requirements may exacerbate existing staff shortages. Efforts to develop policies to expand HCBS and strengthen the direct care workforce have centered on Medicaid as the primary payer for these services. The American Rescue Plan Act (ARPA), passed earlier this year, provides states with a one year 10 percentage point increase in federal Medicaid matching funds (FMAP) for HCBS. Congress is currently debating efforts to build on the ARPA investments as part of an overall budget reconciliation package, and the final funding amount remains in flux as policymakers weigh competing priorities.
To help inform the ongoing debate, KFF conducted four focus groups in July and August 2021 with direct care workers and unpaid caregivers who provide HCBS, assisting seniors and people with disabilities with daily self-care and household activities. These focus groups are not necessarily generalizable to all caregivers, but can provide insight into their experiences to help inform current policy debates. Key findings include the following:
In addition to physical demands, paid caregivers reported that their jobs had mental demands, which intensified during the pandemic. A number of unpaid family caregivers explained that the mental demands associated with caregiving were often “overwhelming.”
A number of paid caregivers described regularly experiencing uncertainty about whether they would be able to leave work at the end of their shift due to staffing shortages and scheduling challenges, which were exacerbated by the pandemic. It is unclear how vaccination mandates might contribute to workforce shortages, as participants in the paid direct care worker groups were divided about whether to receive the COVID-19 vaccine. While the majority of those weighing in on this issue were vaccinated, a vocal minority were unvaccinated. Among the unvaccinated, some expressed hesitancy, while at least one said their opposition was strong enough to lead them to leave their job if faced with an employer mandate.
It is perhaps not surprising, but participants in the paid direct care worker groups universally agreed that their wages are low and do not reflect the demands of their jobs. They described their financial situation as “getting by” and “living paycheck to paycheck.” Those who live in a household with two wage earners universally noted that their spouse was the “primary breadwinner” and observed that their earnings alone were not enough to support a family. Some participants in the unpaid caregiver group said that their caregiving demands made it impossible for them to have paid work.
Efforts to develop policies to expand HCBS and strengthen the direct care workforce have centered on Medicaid as the primary payer for these services. The American Rescue Plan Act, passed earlier this year, provides states with a one year 10 percentage point increase in federal Medicaid matching funds (FMAP) for HCBS. President Biden then proposed a landmark $400 billion federal investment in Medicaid HCBS as part of his American Jobs Plan. Funding in the current House bill has been reduced to $190 billion, the majority of which would be available as a permanent seven percentage point FMAP increase for HCBS for states that choose to participate and meet program requirements. This legislation is part of the overall budget reconciliation package, and the final funding amount remains in flux as policymakers weigh competing priorities.
To help inform the ongoing debate, KFF conducted four focus groups in July and August 2021 with direct care workers and unpaid caregivers who provide HCBS, assisting seniors and people with disabilities with daily self-care and household activities. The groups included a total of 24 paid direct care workers and eight unpaid caregivers. Participants worked in a range of job types and cared for people with a variety of disabilities and long-term care needs. We sought diversity in how long people had worked as caregivers, those working full vs. part-time, and racial/ethnic background. We also sought to recruit people primarily serving Medicaid enrollees. All groups were held by online video conference, allowing for participation from states across the country.1 KFF worked with PerryUndem Research/Communication to conduct the focus groups.
This issue brief presents findings from the focus groups including caregiver characteristics; physical and mental caregiving demands; the impact of workforce shortages; wages, finances, and opportunities for advancement; and what caregivers would like policymakers to know about their work.
Who are caregivers?
The paid direct care workers in our focus groups generally reflect the national data in terms of gender, race/ethnicity, and full vs. part-time work status. Box 1 describes national data about caregiver demographics. Most of our focus group participants are women and included people who identified as white, Black, Hispanic, and Asian. They work in a variety of job types, including home health aides, personal care attendants, direct service professionals (DSPs), and certified nursing assistants, and most work full-time. Workers’ years of experience ranges from less than one to over 25 years, with most having worked between one and five years in the field. Most are employed by provider agencies, though a few worked for state agencies, and some were hired directly by clients who self-direct their Medicaid services.
The direct care worker focus group participants care for people with a range of disabilities and in a variety of community-based settings. Their clients include seniors, including some with dementia; nonelderly adults with physical disabilities such as Parkinson’s disease, cerebral palsy, multiple sclerosis, and spina bifida; children and adults with intellectual or developmental disabilities (I/DD) such as Down’s syndrome and autism; children who are medically fragile; and people with mental illness. They work in individual client homes, group homes, day programs, and schools. The number of clients per week ranged from one to more than five. The vast majority of participants reported that their clients receive services covered by Medicaid.
Many focus group participants who are paid caregivers started as unpaid family caregivers. Several participants described being drawn to caregiving jobs for their paid employment because they had first experienced taking care of family members (including young children or siblings as well as relatives with disabilities) and/or had seen relatives who worked in paid caregiving jobs and were able to “make a difference” in their clients’ lives. A male direct care worker in Texas observed, “[y]ou have to have a service-oriented, nurturing, caring spirit and be genuinely interested in helping out [the] person. . . that you’re assisting.” A frequently cited attribute for success on the job was “patience.” Others underscored the importance of “social skills,” both in terms of establishing rapport and “creati[ing] a bond with [your] client” and in communicating with family members.
“I love being able to help people. . . So I think just seeing the positive effects of what I’m doing, even it’s something small, how big of a difference it makes for somebody. I love that. It’s such a good thing for me.” – 24-year-old female paid caregiver in Pennsylvania
“[S]ome of these patients, they value your company. Like they’re lonely so that’s what gives me the most gratification. . .” – 34-year-old female paid caregiver in New York
Nearly all participants in the unpaid caregiver group were women and described themselves as the primary caregiver for someone receiving Medicaid, typically a family member. This group was about evenly divided between people who identified as white or Black. They care for seniors with physical disabilities and/or dementia, and nonelderly people with autism, serious mental illness, and physical disabilities. Some had paid employment, either full or part-time, in addition to their caregiving responsibilities. They describe Medicaid as helpful in covering doctor visits, prescriptions, medical tests, supplies, transportation, and home health aide services. Transportation to medical appointments and daily supplies such as gloves, wipes, and adult diapers were cited as items that participants would find expensive to cover out-of-pocket without Medicaid. A couple of participants noted that Medicaid home health aide services allowed them to do paid work as well.
Participants in the unpaid family caregiver group experienced a variety of circumstances that led to them assuming their caregiving roles. Some were parents of a child born with I/DD and had been caregiving since their child’s birth and into adulthood. A woman in Florida described the sudden onset of her adult daughter’s caregiving needs: her daughter had been living on her own and working when she began experiencing symptoms that led to discovery of a brain tumor. She now lives with her mother and requires constant care. Several participants who are caring for aging parents observed that they expected to be caregiving eventually but had not anticipated their parents to need care as soon as they did. Most participants in the unpaid caregiver were not formally trained as caregivers and reported varied experiences with accessing the information and resources they needed to support them in their caregiving roles. Some had one-time training when they began caregiving, while others had no training. Participants generally agreed that information was not easy to find and required time and persistence to pursue. Several cited their family member’s doctor as the most helpful source of information about available resources.
“I just feel like there’s not anyone out there that, you know, helps us and guides us in the right direction for what we need or what we want.” – 56-year-old female unpaid caregiver in Ohio
“I was able to learn a lot just by talking to someone at the Senior Resource Center, which has helped tremendously.” – 60-year-old female unpaid caregiver in Minnesota
Box 1: National Characteristics of Paid and Unpaid Caregivers
National data show that the paid long-term care workforce is disproportionately low-wage, female, and Black. Aides and personal care workers are much more likely to be low-wage earners, compared to other types of long-term care workers, such as health care providers and social and behavioral health workers. Across care settings, 70% of aides and personal care workers earn less than $30,000 (the 40th percentile of overall long-term care worker earnings). Aides and personal care workers also are more likely to live in poverty than other types of long-term care workers (15% versus 6%). Just under 60% of home health workers and 62% of aides and personal care workers are employed full-time. The vast majority (88%) of aides and personal care workers are female, and nearly half are Black or Hispanic (32% and 16%, respectively). Another analysis shows that, while most (60%) health care workers with direct patient contact working in long-term care settings have private health insurance, 21% have Medicaid or other public coverage, and 14% are uninsured.2
The majority of unpaid family caregivers are white and female. A 2020 AARP survey found that over 20 percent of Americans (about 53 million people) had cared for a relative or friend in the past year, up from about 43.5 million people in 2015. Six in 10 family caregivers are white (61%), 17% percent are Hispanic, 14% are Black, 5% are Asian/Pacific Islander, and 3% identify another race/ethnicity including multiracial. Just over 60 percent of family caregivers are female, and over half are age 50 or older. Over half are caring for a parent, and the average duration of caregiving is 4.5 years. One in 5 family caregivers reports high financial strain as a result of caregiving, and 45% have experienced at least one negative financial impact due to caregiving, such as taking on more debt. Just over 60 percent of family caregivers have paid employment, with most of this group reporting that caregiving has impacted their work.
The pandemic has affected both paid and unpaid caregivers. A 2020 survey found that over half of DSPs reported that their work life was “worse or much worse” since the pandemic. Another 2020 survey found that unpaid family caregivers scored significantly worse on well-being measures (such as anxiety and depression) compared to non-caregivers. Family caregivers also were more likely to report increased worries about food and financial security since the pandemic began, compared to non-caregivers. Additionally, family caregivers reported that the pandemic made it more difficult to perform caregiving.
What are the physical and mental demands of caregiving?
Participants in the paid direct care worker groups described daily caregiving work involving a variety of physical demands. Typical tasks include helping clients with eating, bathing, and toileting; preparing meals, doing laundry and other household chores; and managing medications. They described the physical demands of their jobs, including lifting and transferring patients in and out of bed and wheelchairs. Other common job characteristics included long hours and unpredictable schedules.
“The physicals demands. . . include the transporting of the. . . patients. . . who were bedridden [to the bathroom]… we didn’t have the bed lift to really lift them up, we would have to do it ourselves and. . . it would be a lot.” – 21-year-old male paid caregiver in New York
“The most strenuous job was when [client] would have her behavior, she would lay down on the ground and she was 250 pounds and just lay there.” – 51-year-old female paid caregiver in Florida
Participants in the paid direct care worker groups also described their jobs’ mental demands, which intensified during the pandemic. Several said that they “love” their work but also acknowledged that everyone is not well suited for the demands of caregiving jobs. They described the demands of caring for clients with challenging behaviors. They cited increased stress especially in the pandemic’s early days. Participants described the uncertainty of working during the pandemic and fear of infecting their clients or bringing the virus home to infect their families.
“It’s hard to get a break, and eventually you just kind of get worn out over the course of the day.” – 78-year-old male paid caregiver in California
“Mentally, you just feel like. . . you can never just sit down and. . . regroup. . . You always feel like there’s something to do, especially with COVID adding more things onto your daily schedule. . . it’s very hectic.” – 21-year-old male paid caregiver in New York
“When the pandemic hit everything shut down…[Clients] could not understand why, and you had to sit there and try to explain to them…they would get frustrated at me, curse me, and spit at me.” – 51-year-old female paid caregiver in Florida
“I would say that my anxiety is honestly probably an all-time high…How do you social distance as a home health care aide?…It makes life challenging, it makes, you know my job challenging, riding the subway is a challenge. There were a lot of times where I was not taking mass transit and that was an additional cost to me.” – 42-year-old male paid caregiver in New York
Similarly, participants in the unpaid caregiver group recounted a range of daily caregiving duties with a variety of physical demands. They assist with preparing meals, bathing, dressing, running errands, laundry, managing medication, and monitoring to ensure safety and prevent falls. Nearly all participants live with the person for whom they care. Many noted that they “don’t really get breaks” from their caregiving duties. Participants described relying on other family members to fill in when they needed someone to cover their caregiving responsibilities, rather than formal respite care.
Participants in the unpaid family caregiver group also explained the mental demands associated with caregiving, which they often described as “overwhelming.” They described the all-encompassing nature of their caregiving role, which existed prior to the pandemic. Participants described caregiving during the pandemic as “scary,” “extremely busy,” “very stressful,” and “a nightmare.” Several had experienced COVID-19 infections themselves or in their households. A 60 year old woman in Minnesota lost her stepmother to COVID-19, which led to her having to assume caregiving responsibilities for her father.
“It’s always a challenge. It is tiring emotionally, physically.” – 51-year-old male unpaid caregiver in California
“I just find it very stressful, very challenging sometimes. . .to find a moment for ourselves because it can be so overwhelming.” – 42-year-old female unpaid caregiver in Illinois
“I never thought I’d feel this tired.” – 44-year-old female unpaid caregiver in Illinois
“I would say it’s been kind of a nightmare for us. My son is autistic…he has some tumors on his brain and he gets very violent and so through the whole pandemic, he was not able to do all of the things that he used to… it was very hard for him to be stuck in the house and not get to go places.” – 56-year-old female unpaid caregiver in Ohio
How are caregivers affected by workforce shortages?
Several participants in the paid direct care worker groups described regularly experiencing uncertainty about whether they would be able to leave work at the end of their shift due to staffing shortages and shifts not being filled if a worker called out. These issues existed prior to the COVID-19 pandemic. A few participants mentioned the toll that working overnight shifts took on their schedules, especially when balancing another job and/or school. Some participants had regular weekly hours, while others said that their schedules changed from week to week, and they did not know their schedule for the upcoming week until a couple of days before the week started.
“It’s mostly common that we have a shortage of staff in most states…I definitely agree like I would start a certain time and wouldn’t know if I [would] leave… Having a shortage doesn’t help either, so if your relief doesn’t come and there is a shortage, you’re just working.” – 21-year-old male paid caregiver in New York
“Some Tuesday mornings when I think I’m going home at six, the owner would call and say, two of them had to go to the doctor, so I would never come home until Wednesday night.” – 51-year-old female paid caregiver in Florida
On the other hand, participants who provide self-directed services said that they and their clients enjoyed the flexibility to decide how to allocate their allotted hours during the week. Self-direction is a service delivery model that typically allows beneficiaries to select and dismiss their direct care workers, determine worker schedules, set worker payment rates, and/or allocate their service budgets.
“I can be with [my client] for 30 hours a week. We can divide that up any way we want to… how it fits our schedules best. . . it’s very flexible.” – 60-year-old male paid caregiver in Texas
The COVID-19 pandemic created additional scheduling challenges and intensified pre-existing staffing shortages for paid direct care workers. Participants agreed that COVID-19 led some of their colleagues to leave their caregiving jobs for fear of getting sick themselves or bringing the disease home to a family member and observed that staffing shortages intensified during the pandemic. Those working in group homes found that they had to increase staffing during the day when outside day programs shut down due to stay-at-home orders, and clients were suddenly at home during the day. Participants also underscored that “social distancing is impossible” when helping clients with personal care needs.
“You never knew who was going to call out. So you always stayed prepared. You always had an extra overnight bag ready just in case.” – 51-year-old female paid caregiver in Florida
“A lot of the [day] programs were closed. So instead of us having an eight-hour break where [group home residents] went to program, now we had to fill the first shift…Not only in the home that I supervise, there was other homes where there was call offs, so I found myself going to assist other people.” – 42-year-old female paid caregiver in Missouri
Unpaid caregivers also were affected by the pandemic’s disruption of in-home and day program services on which some unpaid caregivers relied so that they could work outside the home. A 56 year old woman in Ohio had to leave her paid employment to care for her adult son with autism after the pandemic began and his day program closed. A 42 year old woman in Florida said that her adult daughter’s home health aide stopped coming during the early days of the pandemic, but services later resumed. A couple of participants noted that they no longer had the same home health aide coming consistently since the pandemic, which created additional disruption and required additional time to orient new aides. Others described discontinuing in-home services during the pandemic due to fear of infection.
“I had to quit working, because he was no longer in school anymore… we were transitioning into the adult program, and then could only go back one day, and then it shut down… I wasn’t able to go back to work.” – 56-year-old female unpaid caregiver in Ohio
It is unclear how vaccination mandates might contribute to workforce shortages, as participants in the paid direct care worker groups were divided about whether to receive the COVID-19 vaccine. While the majority of those weighing in on this issue were vaccinated, a vocal minority were unvaccinated. Among the unvaccinated, some expressed hesitation, while at least one said that their opposition was strong enough to lead them to leave their job if faced with an employer mandate. A number of participants described contracting COVID-19 themselves or working where there were outbreaks among staff or clients, but these experiences did not necessarily mean that they wanted to be vaccinated. A female paid caregiver in California had just learned that her employer was adopting a vaccine mandate and was preparing to leave her job rather than comply. A female paid caregiver in Maryland who had had COVID-19 said that she did not want to be vaccinated due to “anxiety” and seeing family members who were vaccinated experiencing breakthrough infections. A female paid caregiver in Missouri said that she did not want the COVID-19 vaccine after becoming ill when she received a flu vaccine. Participants noted that clients increasingly were requesting workers who are vaccinated to fill open shifts. Unlike the division among participants in the paid caregiver groups, those in the unpaid family caregiver group generally were supportive of vaccination.
“I don’t know if I was going to be having a job next month because they wanted everybody to be, all their workers to be vaccinated.” – 41-year-old female paid caregiver in California
“I’m not getting vaccinated. . . I just don’t trust it.” – 45-year-old female paid caregiver in Maryland
“I am not vaccinated. But I’ve noticed that when they do call me to offer shifts, sometimes the agency may say this particular consumer will prefer someone who has been vaccinated. So, you know, the consumer does have the right to specify it. For my own personal reasons, I’m just a little hesitant right now.” – 24-year-old female paid caregiver in Pennsylvania
Participants in the paid direct care worker groups who were vaccinated cited the benefits they saw for themselves as well as their clients. A male paid caregiver in Texas who has diabetes reported getting vaccinated as soon as he was eligible, while a female paid caregiver in New Jersey said that she felt comfortable getting the vaccine after doing her own research and preferred that route to getting vaccinated through her employer. One paid caregiver in Texas working with immune compromised children was frustrated that some families were not getting vaccines despite additional risks to their children
“I got the vaccination because my job required it, but I was going to get it anyway as soon as I was in line. I was in line as a senior. But I got it earlier because I was in line first as a caregiver.” – 66-year-old female paid caregiver in Pennsylvania
“I got [the COVID-19 vaccine] at the nearby hospital… I did it on my own terms because I don’t want to put my own family at risk, especially my grandmother, and my other clients… [Clients] feel more comfortable with someone that’s vaccinated in their home.” – 22-year-old female paid caregiver in New Jersey
“I’m diabetic so when I got the chance to get vaccinated at the beginning of this year, I didn’t doubt it.” – 54-year-old male paid caregiver in Texas
How do caregivers feel about their wages, overall finances, and opportunities for advancement?
Perhaps not surprisingly, participants in the paid direct care worker groups universally agreed that their wages were low and did not reflect the demands of their jobs. They described their financial situation as “getting by” and “living paycheck to paycheck.” Those who live in a household with two wage earners universally noted that their spouse was the “primary breadwinner” and observed that their earnings alone were not enough to support a family. Some noted that they had been able to earn additional money by picking up extra hours during the pandemic when colleagues called out, though they also noted the additional stress of working more long shifts. On the other hand, one woman described the financial challenges her family faced during the pandemic when her husband was out of work and their income was limited to her caregiving wages. Full-time employees generally reported access to employer-sponsored health insurance, and some employers offered retirement savings plans. Some but not all had paid vacation days, and most did not have paid sick leave.
Participants in the paid direct care worker groups generally did not receive raises and expressed the desire to have good job performance recognized with wage increases. Those who had asked for raises generally reported that their employers said that this was not feasible due to low Medicaid reimbursement rates. A 24 year old female paid caregiver in Pennsylvania who had been working at her employer for four years said that small hourly increases were available based on an annual evaluation: “based on your performance, they’ll give you like maybe an extra 30 cents an hour, an extra 20 cents.” She reported that her employer had been in business for 17 years, and during that time the starting hourly rate had increased only from $9 to $10.
“You’re not going to get rich, you know, and it’s not about that, it’s more of. . . I know that I’m going to be helping people at the end of the day. . .” – 41-year-old female paid caregiver in California
“We’re over worked and underpaid. And it’s not really an easy job. . . This job is not for the weak. You have to love what you do.” – 51-year-old female paid caregiver in Florida
“[O]bviously we need money. . . to support ourselves, that’s how we get by, we pay bills, we eat. . . put food on the table and put clothes on our back. But you [have] got to do this. . . because you love to do it, and that’s the only way that you’ll be able to get through those 12, 24 hour shifts sometimes.” – 21-year-old male paid caregiver in New York
“[T]o grow a family, yes, it is necessary to have two incomes, because as a home health [aide]. . . even though. . . we live here in Texas, it’s not very expensive, [but] it’s not enough to raise a family.” – 54-year-old male paid caregiver in Texas
Participants in the paid direct care worker groups are interested in opportunities for training that lead to wage increases and the ability to advance in their careers. Some participants said that their employers offered online or in-person training on topics such as safe lifting practices, allergy management, and tracheotomy and gastrointestinal tube care and that they were paid for their training time. However, these trainings did not appear to be tied to wage increases or career advancement, and most participants did not feel that their jobs offered a career ladder to higher wages based on increased skills or job responsibilities.
“With my company there is no real career advancement… there is no training program to move you into let’s say a managerial role… [I]t’s not like. . . somebody ever sits me down for my annual review and says. . . okay, where do you see yourself in two or three years. . . I’ve never had a conversation like that. . . I don’t think those conversations are typical.” – 42-year-old male paid caregiver in New York
Some participants in the unpaid caregiver group have paid employment in addition to their caregiving, while others said that their caregiving demands made it impossible for them to work. Those that are working often described their outside jobs (often from home) as a break from caregiving, though they also noted difficulty in balancing their paid employment with their caregiving responsibilities. A 42 year old woman in Florida who cares for her adult daughter noted that she lost a job due to her inability to focus, which led to mistakes, because she was preoccupied with her daughter’s needs. Others agreed with her description of “always being in caretaker mode.” She has now found another job but noted that she is unable to go to work or take her younger daughter to school if the home health aide for her adult daughter does not show up on time. A 44-year-old woman in Illinois who cares for her adult brother with serious mental illness and a brain tumor said that her caregiving responsibilities only allowed her to work part-time.
“I had another job, but I was let go because I couldn’t focus. I was making so many mistakes… [T]his job I have now is working from home, but that makes it ten times harder for me to focus because [my daughter is] right in the next room.” – 42-year-old female unpaid caregiver in Florida.
What is Congress considering to support caregivers and what do caregivers want policy makers to understand?
The Congressional debate about the overall budget reconciliation package and the amount of new federal funding for Medicaid HCBS is continuing. President Biden proposed $400 billion in new federal funds for Medicaid HCBS, while the current House bill includes $190 billion. Box 2 describes key provisions of the new funding as they relate to paid and unpaid caregivers.
Box 2: Key Provisions in the Current House Bill Related to Caregivers
Most of the new Medicaid HCBS funds in the House budget reconciliation bill are dedicated to a new “HCBS Improvement Program,” which would provide states with a permanent seven percentage point increase in federal Medicaid matching funds for HCBS. To qualify for the enhanced funds, states would have to engage in certain activities to expand Medicaid HCBS and strengthen the direct care workforce.
A number of the activities tied to the proposed enhanced federal HCBS funds focus specifically on paid and unpaid caregivers. For example, states would have to provide supports to family caregivers, such as respite care, caregiver assessments, peer supports, or paid family caregiving. States also would have to update, and increase as appropriate, HCBS payment rates to support the recruitment and retention of direct care workers, and review these rates every three years. Payment rate increases would have to be at least proportionately passed through to direct care workers. States would have to update qualification standards and develop training opportunities for HCBS providers and provide resources for family caregivers. States also would have to monitor and report on factors such as direct care worker wages, benefits, turnover, and vacancy rates.
Under the new program, states also could receive an increase in the federal matching rate for administrative costs, from 50% to 80%, through September 2031, for activities such as modifying provider rate setting processes, adopting or improving training programs for direct care workers and family caregivers, and adopting or enhancing registries to connect HCBS enrollees and direct care workers. Additionally, states could receive another two percentage point increase in federal Medicaid HCBS matching funds for two years if states adopt certain activities to support self-direction. These activities include developing a worker registry to help enrollees find workers; recruiting and training independent providers; supporting enrollees who self-direct services by processing worker timesheets and payments; and supporting family caregivers as paid providers.
Participants in the paid direct care worker groups cited improving wages as the top issue for policymakers to address. There was a general feeling of being “overworked and underpaid,” which existed prior to the pandemic. Participants emphasized the importance of any reimbursement rate increases being passed through to direct care worker wages. Participants also supported increased training, especially if tied to career advancement and higher wages, and access to the equipment and supplies they need to perform their jobs safely.
“I think [higher wages] would attract more people to the job. . . having more money. . . within your pocket would allow more people. . . to be able to sustain themselves and not be discouraged from. . . not being paid enough” – 21-year-old male paid caregiver in New York
“if [policymakers] do give an increase to whatever the reimbursement rate to the agencies is, maybe they could specify something in their contract just to say, you know, caregivers should be making at least this amount.” – 24-year-old female paid caregiver in Pennsylvania
Participants in the unpaid caregiver group asked for recognition of the value of the services that they provide for their family members. They all said that they wanted to keep their family members at home and were willing to provide the caregiving necessary to avoid having them institutionalized. At the same time, they did not think that people who have not had the experience of family caregiving fully understand the challenges it presents. One suggested providing tax credits to family caregivers to recognize that in-home care is less expensive than nursing home care. Other suggestions included additional opportunities for community integration and a centralized website with current information about caregiver supports. They also emphasized that policies should be flexible enough to recognize that each person has unique needs to be met and administrative burdens to access services should be minimized.
“Nobody knows how much you’re sacrificing for yourself to take care of somebody else… I would never want to put my parents or my son in a nursing home… And I just think that a lot of people just don’t understand what it is that we go through.” – 56-year-old female unpaid caregiver in Ohio
“There’s people in different degrees of caregiving, lower-level, higher levels, and so those need to be taken into consideration. Those that really have severely disabled [family members], whether it’s emotionally or physically, they need to have the support…it’s a 24/7-hour job. They need to be supported through whatever means necessary.” – 51-year-old male unpaid caregiver in California
“Keeping somebody out of a nursing home really reduces the cost; I’d like them to recognize that us as caregivers are really saving tons of money, we’re providing good quality service, keeping our loved ones with us.” – 60-year-old female unpaid caregiver in Minnesota
Looking Ahead
The COVID-19 pandemic has intensified long-standing issues related to the unmet need for HCBS, such as growth in the aging population and direct care workforce shortages. Many states used Medicaid emergency authorities to support HCBS providers during the pandemic by increasing reimbursement rates and/or offering retainer payments. CMS guidance encourages states to identify any temporary policy changes adopted under emergency authorities that increased access to HCBS and to consider making those changes permanent. However, states’ ability to do so could be limited by budgetary constraints. While the American Rescue Plan Act provides a temporary increase in federal matching funds for Medicaid HCBS, the expiration of this increase after one year could limit states’ ability to adopt longer-term HCBS program expansions.
Congressional debate about the overall budget reconciliation package and the amount of new federal funding for Medicaid HCBS is continuing. President Biden proposed $400 billion in new federal funds for Medicaid HCBS, while the current House bill includes $190 billion.
The major HCBS program in the bill would increase federal matching funds, without a time-limit, for state spending on Medicaid HCBS. To qualify for the new funds, states would have to take certain actions, a number of which are relevant to addressing issues raised by caregivers in our focus groups. For example, states would have to review, and update as necessary, HCBS provider reimbursement rates every three years, and any rate increases would have to be passed through to direct care workers. These actions could help to address issues with low wages cited by focus group participants. To receive the new funds, states also would have to develop training opportunities for paid HCBS providers as well as for unpaid family caregivers, which could help to address needs in these areas expressed by focus group participants. Another set of activities under the new program centers on states providing supports to family caregivers, such as respite care, caregiver assessments, peer supports, or payment as providers. Participants in the unpaid caregiver group cited these areas as gaps in which additional resources and supports are needed. How much the reconciliation package does to address the concerns raised by caregivers will depend in large part on the level of funding committed. There is pressure to reduce the overall price tag in the package, and planned HCBS expansions could be reduced further as they compete with other priorities.
Participants in the paid direct care worker groups live in Alabama, California, Florida, Illinois, Missouri, New Jersey, New York, Pennsylvania, South Carolina, Texas, and Washington. Participants in the unpaid family caregiver group live in California, Florida, Illinois, Minnesota, New York, Ohio, and Oregon. ↩︎