Background
Monkeypox is an infectious disease caused by the monkeypox virus, in the Orthopoxvirus genus, and is related to smallpox. The first human case was identified in 1970, and historically, it has primarily been found on the African continent, except in cases related to travel or imported animals. However, in May 2022, multiple cases were identified in several countries where monkeypox has not been endemic, including the United States (U.S.). This current outbreak is the largest ever in the U.S. and globally and marks the first time substantial local transmission has been reported in non-endemic countries across multiple continents. (See Box 1 for an overview of monkeypox illness, transmission and testing, prevention, and treatment.)
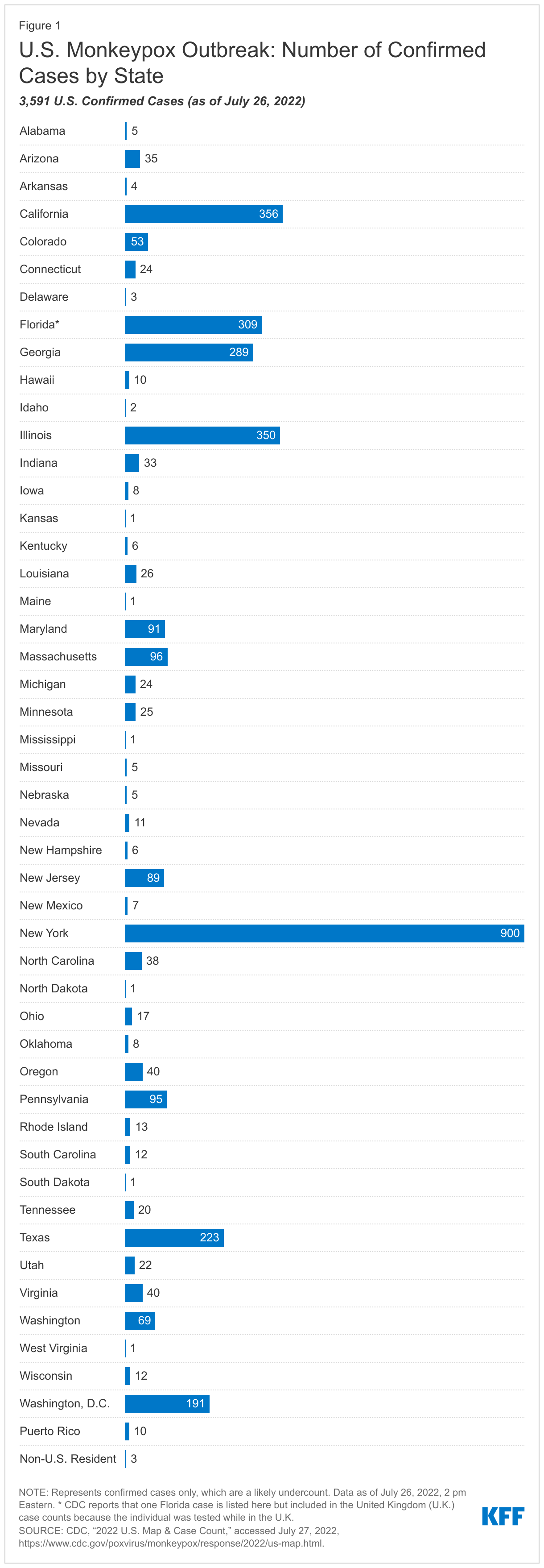
In the U.S., the first monkeypox case in the current outbreak was identified on May 18, 2022. As of July 26, 3,591 cases in 46 states, Puerto Rico, and Washington, D.C., have been diagnosed (see Figure 1); this represents 19% of 19,188 confirmed global cases. This number is likely a significant undercount due to a number of factors including: limited access to testing, particularly in the first few months of the outbreak; lag time between seeing a provider and having a case confirmed; knowledge gaps among providers; and stigma that may make individuals reluctant to seek medical care, especially when sores are in the genital or anal region and transmission may be associated with same-sex sexual encounters. Given the growing number of cases and considering other factors, on July 23, 2022, the World Health Organization (WHO) declared the monkeypox outbreak to be a Public Health Emergency of International Concern (PHEIC), and provided a set of recommendations on actions that governments and others can take to address the outbreak. Whether or not the U.S. follows suit and declares the outbreak to be a domestic public health emergency (PHE), remains to be seen. Doing so would allow for a range of flexibilities and potential access to funding, should this be needed. Confirmed cases are expected to continue to rise in the coming weeks, likely due to both an actual increase in the number of cases from ongoing transmission as well as improvements to testing and surveillance that capture more cases.
Almost all reported cases in the current U.S. outbreak (99% as of June 28, 2022) have been among gay, bisexual, and other men who have sex with men, who are considered most at risk at this time. However, monkeypox can be a risk to anyone, regardless of sexual orientation or sex/gender of sexual partners, and in the current outbreak, cases have been identified among transgender men and cisgender women. A few recent cases among children have also been identified.
This brief answers key questions about the U.S. outbreak to date and identifies issues that may affect the response going forward.
| Box 1: Monkeypox Overview |
| Illness | Transmission, Isolation, & Testing, and Isolation |
| Monkeypox can be a serious disease that causes illness and in some cases death (though no deaths have been reported in the U.S. from this current outbreak). There are two strains of the virus – a west African and a central African (Congo Basin) strain; the strain circulating in the current U.S. outbreak is the west African strain, which is less severe. Most cases in the U.S. have been mild to date, though the infection can be painful, and most hospitalizations that have occurred have been to treat pain. However, cases of monkeypox-related myocarditis and encephalitis also have been reported. Its incubation period is 1 to 2 weeks, and the first signs of illness following the incubation period may include symptoms common with a range of viral infections, including: - fever,
- headache,
- swollen lymph nodes,
- exhaustion, and
- body aches.
A severe rash and lesions typically follow. While lesions can occur anywhere on the body (e.g., hands, feet, chest, in the eyes), in the recent outbreak, they have commonly been found in the genital and anal regions, which can be painful. Those with weakened immune systems are more likely to get seriously ill and this may include people with HIV who are not virally suppressed. The illness typically lasts 2-4 weeks. | Monkeypox transmission between people can occur via:- direct contact with infected lesions, rashes, scabs or fluids (while some virus has been detected in samples, it is not yet known if transmission can occur via semen or vaginal fluid);
- contact with contaminated materials like clothing or linens;
- respiratory droplets from prolonged face-to-face contact (monkeypox is not thought be transmitted via respiratory aerosols as COVID-19 is); and
- across the placenta to the fetus among pregnant people.
People with monkeypox are infectious to others once symptoms begin and remain infectious until lesions form scabs, scabs fall off, and a fresh layer of skin forms. CDC recommends that people with monkeypox isolate until this point, which can take up to 4 weeks. There are steps individuals with monkeypox can take to limit exposure to others including, avoiding close contact with other people, including sexual activity, and not sharing potentially contaminated items, such linens, clothing, towels, and dishes, among other actions. Most testing for monkeypox currently relies on a general assay for Orthopoxvirus, but in the U.S., positive cases are presumed to be monkeypox per the CDC. In addition, Quest Diagnostics has developed a monkeypox specific test expected to be available in July. |
| Vaccines for Prevention | Antiviral Treatment |
In the United States there are two vaccines that can be used to prevent monkeypox: JYNNEOS and ACAM2000. JYNNEOS is FDA-approved for monkeypox and smallpox, while ACAM2000 is approved for smallpox but has been granted an expanded access Investigational New Drug (EA-IND) protocol to allow its use for monkeypox. Both vaccines are thought to be at least 85% effective at preventing monkeypox.- JYNNEOS is a two-dose series, while ACAM2000 requires a single dose but multiple punctures.
- While both vaccines are effective and CDC reports that most people have minor reactions, JYNNEOS has a lower risk profile, is less invasive administration than ACAM2000, and poses a lower risk to those administering the vaccine. Additionally, JYNNEOS is not contraindicated for people with conditions associated with being immunocompromised, including people with HIV, who are pregnant, or have other select conditions, as is the case with ACAM2000. As such the vaccination response in the U.S. has prioritized JYNNEOS.
The vaccines maybe used as either as pre-exposure prophylaxis (PrEP) or post-exposure prophylaxis (PEP) (note that this is PrEP and PEP for monkeypox, not HIV): - Vaccinating for PrEP means that an individual who is at risk of contracting monkeypox is vaccinated to prevent infection from occurring should they be exposed in the future. PrEP may also reduce severity of a breakthrough infection should one occur soon after vaccination.
- Using the vaccine for PEP means that an individual who is thought to have had a high-risk exposure to monkeypox is vaccinated to prevent infection or reduce severity of infection should it occur. The CDC states that vaccination given within 4 days from the date of exposure may prevent disease and that vaccination given between 4–14 days from date of exposure may reduce symptom severity.
- The CDC is also using the term PEP++ to describe the strategy of providing vaccinations to those with risk factors that might make them more likely to have been exposed to monkeypox even without a confirmed diagnosis, such as having had a higher risk activity in an area where monkeypox is spreading in the past 2 weeks.
| There are no available treatments that specifically target the monkeypox virus. However, as with vaccination, because the smallpox and monkeypox viruses are similar, smallpox antiviral treatments may be effective for treating monkeypox. Tecovirimat (TPOXX) is one such antiviral that has been approved for smallpox and is being made available for use as treatment for monkeypox via an expanded access Investigational New Drug (EA-IND) protocol, which requires providers to consult with the CDC or their state/local health department in order to prescribe it. |
Key Questions About the U.S. Response
When did the U.S. federal response to the outbreak begin?
After the first cases of monkeypox in this outbreak were identified (in the United Kingdom on May 6, 2022, and in the U.S. on May 18, 2022), the CDC and other agencies took initial response steps such as developing an updated case definition for monkeypox, providing advice to local, state, tribal, and territorial health departments on surveillance, reporting, and contact tracing, supporting diagnostic testing, and coordinating with international authorities and other countries. On June 28, 2022, 6 weeks after the first reported U.S. case, the White House announced a government-wide strategy and approach to scaling up vaccination and expanding testing capacity for monkeypox, and the CDC activated its Emergency Operations Center to enhance operational support including monitoring and coordination.
Some public health experts and advocates have criticized the administration’s response, saying the government did not act quickly enough or at sufficient scale and are now playing “catch up” in key response areas such as messaging and expanding access to vaccinations, testing, and treatments. Some expressed concern the federal government is repeating the missteps of its early response to the COVID-19 pandemic and warned the monkeypox outbreak could quickly grow even larger without additional testing, vaccinations, and particular focus on addressing equity issues. The administration has said it would continue to adapt the nation’s response as the situation develops.
What areas are the main focus of the U.S. response?
The federal government and state and local governments share responsibilities for responding to outbreaks such as monkeypox. The federal government’s response to date has been focused on several areas, including:
- securing and distributing vaccines and treatments;
- conducting and improving surveillance;
- increasing testing capacity and access;
- educating health care providers and the public;
- supporting research and development;
- coordinating with and supporting state, local and territorial responses;
- developing and pursuing research priorities; and
- engaging with affected communities and other stakeholders.
State and local jurisdictions also support many of these activities, with federal support and assistance. For example, some jurisdictions are working to facilitate health care providers’ access to testing, treatment, and vaccination, playing a role in communicating key information about the outbreak, and developing on-the-ground response networks. These responses, however, are variable across the country and more robust in some places than others. (See below discussion for more detail.)
What agencies are involved in the federal response?
The federal response is coordinated by the White House National Security Council’s Directorate on Global Health Security and Biodefense (also known as the White House Pandemic Preparedness Office) and involves the U.S. Department of Health and Human Services (HHS) and several of its operating divisions and offices. These include the Office of the Assistant Secretary for Preparedness and Response (ASPR, which includes the Strategic National Stockpile under the Office of Operations and Resources as well as the Biomedical Advanced Research and Development Authority (BARDA), the CDC, the Food and Drug Administration (FDA), and the National Institutes of Health (NIH). The White House Office of Science and Technology Policy (OSTP) also plays a role.
What is the status of monkeypox testing in the U.S.?
Testing for monkeypox (clinical samples taken from patients’ lesions and tested for the presence of an Orthopoxvirus or in some cases, specifically the monkeypox virus) currently takes place only in a set of authorized laboratories, and testing capacity has ramped up slowly. Initially, testing was done primarily at the CDC and other public health laboratories. More recently, testing has been expanded to commercial laboratories:
- As of June 28, 2022, 78 laboratories (mostly public health laboratories) in 48 states had the testing capacity to handle 10,000 Orthopoxvirus tests per week, up from 67 labs with a weekly capacity of 8,000 tests a week earlier.
- On June 22, 2022, HHS announced it had begun shipping CDC Orthopoxvirus tests to five commercial laboratory companies – Aegis Science, Labcorp, Mayo Clinic Laboratories, Quest Diagnostics and Sonic Healthcare – with the aim of increasing testing capacity and improving accessibility for providers and patients.
- As of July 18, Aegis Science, Labcorp, the Mayo Clinic Laboratories, and Sonic Healthcare had all begun testing using the CDC Orthopoxvirus test, with each of these labs providing a capacity of up to 10,000 tests per week.
- Since then, Quest Diagnostics announced they developed their own monkeypox-specific test (compared to the general Orthopoxvirus test) and expected to be able to run 30,000 of those tests per week by the end of July. Quest has stated that it would continue to work towards validating the general CDC Orthopoxvirus test as well, which would provide another testing option, and they expect that additional capacity to be available in August.
- Combining the public health laboratories and commercial sector, the total U.S. Orthopoxvirus or monkeypox virus testing capacity is currently 80,000 tests per week.
There have been some reports of access challenges to monkeypox testing, particularly prior to the commercial labs partnering with the CDC to offer tests. And now even with commercial labs offering the tests, not all providers are equipped or willing to perform specimen collection which contributes to ongoing barriers. Additionally, whereas testing performed at public health laboratories does not carry a cost for patients, tests performed by a commercial laboratory may have costs, which could be an issue particularly for patients who are under- or un-insured.
What is the status of the monkeypox vaccine supply in the U.S.?
Monkeypox vaccines can be used following a known or likely exposure (i.e., post-exposure prophylaxis or PEP) or as a preventive measure before an exposure occurs (i.e., pre-exposure prophylaxis or PrEP) (see Box 1 for more details).
Monkeypox vaccines are being made available through the Strategic National Stockpile. The U.S. currently has a limited supply of such doses, with just 65,000 JYNNEOS doses in the stockpile in late June. Additional doses have been ordered for delivery in the coming months, with 6.9 million doses of JYNNEOS expected to be available by mid-2023 (enough to vaccinate 3.5 million people), including approximately 1.9 million doses in 2022 (enough to vaccinate 950,000 people).
Of these, 5.5 million of the JYNNEOS doses were recently ordered by the U.S. government and come from an existing bulk vaccine order that HHS/BARDA has with vaccine-maker Bavarian Nordic though an existing ten-year contract. The contract allows the U.S. government to request that Bavarian Nordic “fill and finish” the equivalent of more than 15 million vaccine doses that the U.S. government purchased. Still, it is unclear whether the U.S. government plans to order more JYNNEOS doses through this contract beyond the 5.5 million doses already announced.
HHS also reported that the strategic national stockpile has more than 100 million doses of the ACAM2000 vaccine (a smallpox vaccine considered effective for monkeypox as well) available, though the JYNNEOS vaccine is preferred and recommended for most individuals.
Where and how have vaccine doses been distributed?
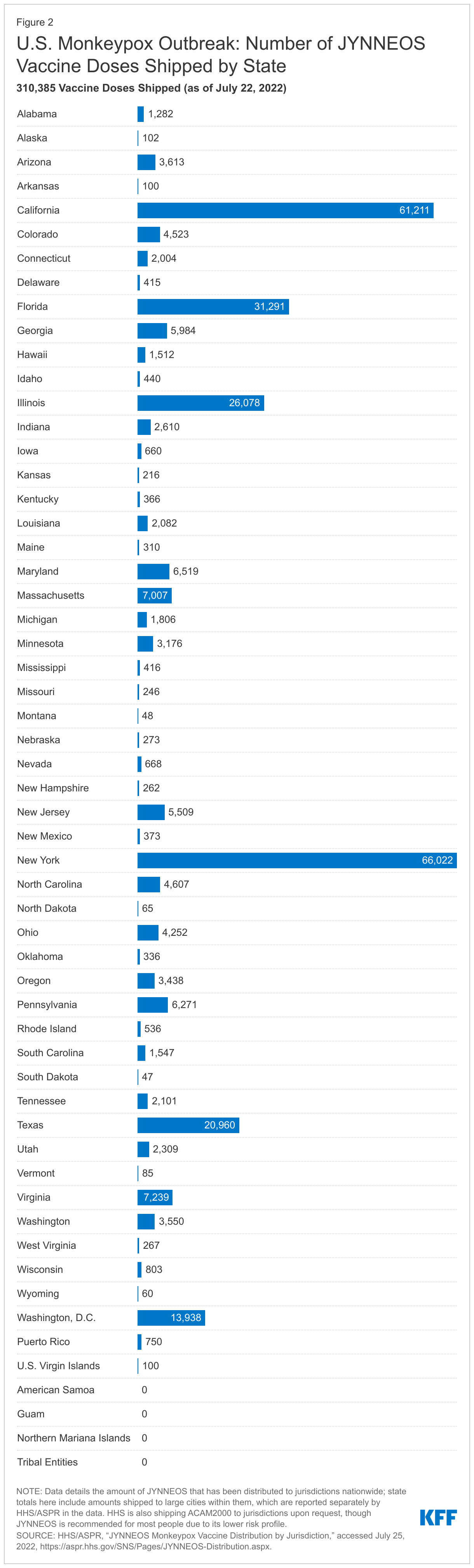
HHS reports that it began shipping JYNNEOS doses on May 21, 2022, and that as of July 22, 2022, it had allocated 333,218 doses (93% of which had been shipped) to all 50 states and seven jurisdictions/groups (American Samoa, Washington, D.C., Guam, the Northern Mariana Islands, Tribal Entities, Puerto Rico, and the U.S. Virgin Islands) from the strategic national stockpile. In addition to state-specific allocations, several large cities received additional doses. The largest number of doses have been allocated, thus far, to New York, followed by California, and then Florida. See Figure 2.
JYNNEOS doses are being allocated based on a “four-tier distribution strategy that prioritizes jurisdictions with the highest case rates of monkeypox. Within each tier, doses of JYNNEOS will be allocated based on the number of individuals at risk for monkeypox who also have pre-existing conditions, like HIV. Jurisdictions with higher cases counts and greater numbers of highly affected populations have been prioritized in initial allocation of the vaccines. Specifically, allocations in the current phase have been based on transmission (current and projected monkeypox cases) and prevalence of high risk populations, (i.e. men who have sex with men with HIV or who are eligible for HIV PrEP). To receive vaccine, jurisdictions must make requests to the CDC and draw down from their allocations, in most cases. The CDC has recommended that vaccines be provided to individuals with confirmed and presumed monkeypox exposure (as PEP and PEP++, respectively; see Box 1) while vaccine supply is limited, but some localities, such as New York City and Washington, DC, have made vaccination available more broadly to higher risk groups, such as gay and bisexual men and other men who have sex with men.
In addition, the ACAM2000 vaccine can be requested by jurisdictions. As of July 1, HHS reports that more than 800 doses of ACAM2000 have been distributed based on these requests.
What is the status of monkeypox treatment in the U.S.?
There are no available treatments that specifically target the monkeypox virus. However, because the smallpox and monkeypox viruses are similar, smallpox treatments may be effective for treating monkeypox. Currently, Ticoviromat (TPOXX), an antiviral approved for smallpox, is the treatment most likely to be prescribed for monkeypox infection in the U.S. under an expanded access Investigational New Drug (EA-IND) protocol. On July 1, 2022, HHS reported that the strategic national stockpile had over 1.7 million TPOXX antiviral treatment courses, and that it had deployed 300 courses from the strategic national stockpile by the end of June (it is unclear where these doses have been distributed).
Because TPOXX is only available under an EA-IND protocol for the treatment of monkeypox, its use has to be approved by the CDC. Partly for this reason, there have been many reports of providers facing lengthy and burdensome procedures for accessing treatment for their patients, creating a barrier for patients and a challenge for provider. In response to these challenges, on July 22, 2022, the CDC announced revisions to this process. While the CDC must still approve use of this treatment, the approval process has been somewhat streamlined by reducing “the number of required forms, patient samples, and photos & [giving] patients the option to see their doctor virtually.”
What federal funding is available for jurisdictions to respond to monkeypox?
So far, Congress has not provided any additional or emergency funding specifically for the monkeypox response. However, CDC has stated that several of their existing grants have flexibility to allow local jurisdictions to use funding for monkeypox as needed. These include four funding streams to date:
- Public Health Emergency Preparedness (PHEP) Cooperative Agreement: PHEP funding allows public health departments to “build and strengthen their abilities to effectively respond to a range of public health threats, including infectious diseases, natural disasters, and biological, chemical, nuclear, and radiological events.”
- Strengthening STD Prevention and Control for Health Departments (STD PCHD) Cooperative Agreement: STD PCHD funds support grantees efforts in addressing STDs including among priority populations including “adolescents and young adults, men who have sex with men, and pregnant women.”
- Epidemiology and Laboratory Capacity (ELC) Building for the Prevention of Emerging Infections Disease Cooperative Agreement: ELC funding supports grantee efforts “to detect, respond to, control, and prevent infectious diseases.”
- Community Health Workers for COVID Response and Resilient Communities (CCR): CCR funding provides “opportunities intended to put more trained [community health workers] CHWs in communities that have been hit hardest by COVID-19 and among populations at high risk for COVID-19 exposure, infection, and illness.”
What public communication and messaging efforts are being conducted about the outbreak?
Because this monkeypox outbreak has disproportionately affected gay, bisexual, and other men who have sex with men, messaging directed at this community is especially important, particularly when it accounts for the stigma and discrimination these communities experience. Accordingly, HHS has been reaching out to public health and provider communities as well as journalists working on LGBTQ issues to inform them about the evolving monkeypox outbreak and provide guidance on disease presentation, progression, testing, and treatment. The CDC is providing consultations with health departments on local epidemics, testing, vaccination, and treatment. The Biden administration has also met with advocates to elicit input and share information with trusted messengers. Additionally, CDC is providing messaging support to be shared with dating apps to raise awareness about monkeypox among gay, bisexual, and other men who have sex with men.
Public-facing messaging from the CDC and other public health authorities has focused on the fact that anyone can get monkeypox while acknowledging that the current outbreak has been concentrated among men who have sex with men. The agency has exercised caution in an effort not to marginalize those at increased risk, notably gay and bisexual men. One suggestion the CDC makes for partners engaging in monkeypox messaging is to “emphasize that anyone [emphasis theirs] can get monkeypox and promote it as a public health concern for all. Focusing on cases among gay and bisexual men may inadvertently stigmatize this population and create a false sense of safety among those who are not gay and bisexual men.” Some in the LGBTQ+ community have expressed concern that the efforts made to avoid stigmatizing this group have actually meant the true risk has been downplayed, resulting in the community not being adequately informed about monkeypox.
In addition to messaging from the federal government, some state and local health departments are reaching out to local providers and highly impacted communities (though the extent to which this is happening is varied), and some national efforts such as Greater than AIDS (operated by KFF) have developed targeted messaging for those at risk.
What key factors might impact the U.S. outbreak response going forward?
As the current monkeypox outbreak in the United States continues to unfold with reported cases climbing, a number of factors could impact the success of the federal approach to contain and address it, including: access to testing, vaccination, and treatment; funding and cost issues; community education and messaging; variation in responses across states/jurisdictions; and equity challenges.
Access to Testing
While testing is now scaling up, early on some criticized the federal government for not standing up widescale testing and engaging with national pharmacy and other partners. Testing plays a key role in tracking the outbreak and allowing those testing positive to take risk reduction measures, such as preventing ongoing transmission, accessing PEP (if possible) and notifying close contacts. It is also a first step towards accessing treatment, if needed and possible. Successful scale-up of testing means that patients and providers are aware of it and that barriers such as costs and stigma are managed. It is also important to note that while there is now commercial laboratory capacity, not all providers may be willing or able to conduct sample collection which could limit access for some. More broadly, whether the current scale-up of testing can keep pace with demand amidst the expanding outbreak is not yet known.
Access to Vaccination
Vaccine distribution has also been limited to date, and it is not yet clear how vaccine distribution will evolve over the coming months.
- Because jurisdictions are being prioritized for distribution based on certain factors, as discussed above, some will gain quicker access to vaccination than others. While the federal government distribution algorithm plays a central role in this, jurisdictional decisions about when and how many doses they request from the CDC may also be a factor. To the extent that some jurisdictions are slower to request vaccines compared to other jurisdictions, it could lead to delayed or restricted vaccine access.
- Federal and jurisdictional vaccine prioritization and allocation approaches also affect the speed and consistency of vaccine access across jurisdictions. The current emphasis on PEP/PEP++ is largely due to the supply of the preferred vaccine being highly limited at the moment and meeting the needs of those likely already exposed being considered more urgent. However, this approach limits access for high-risk individuals without a known exposure, which may be a missed opportunity for preventing disease and helping curb new infections. While some jurisdictions, such as New York City and Washington, D.C., have offered a limited supply of PrEP to persons at higher risk, many jurisdictions have not yet done so.
- Demand for vaccination currently seems to be far outpacing supply in various jurisdictions. In Washington, D.C., for example, on multiple occasions, the D.C. Department of Health opened vaccination appointments at a certain time with a limited number of spots (300 in the first instance) and seen those spots filled within a matter of minutes. Similar challenges, including traffic crashing the city website, were reported in New York City. However, once vaccination is more widespread, there may be a larger role for federal and local officials to play in encouraging uptake.
Available Funding and Coverage of Costs
It is unclear how much funding may be available for monkeypox under existing grants or how much more might be needed. Transparent tracking and reporting of how much funding is being used for this purpose may be useful and inform discussions if additional funding is needed.
Likewise, in the early weeks of the outbreak, certain costs of testing, treatment, and vaccination are being covered by the federal government, but it is possible this could shift over time. At this time, there is no cost to individuals for testing that occurs within public health laboratories or at the CDC. However, individuals may face costs for tests conducted through commercial sector labs, with actual amount determined by insurance coverage. Those without insurance or with high-cost sharing associated with their coverage could face more limited access to testing. Currently, vaccinations are being deployed from the strategic national stockpile and the vaccine itself is provided at no cost. Similarly, the cost of TPOXX is also currently covered. However, individuals may face costs for provider visits, hospitalization, and other lab tests run as part of treatment or diagnosis.
Variation in Local Responses
States and jurisdictions will likely see various levels of success in their ability to contain localized outbreaks due to differences in how they are responding (in some cases, for reasons outside their control) to the ongoing monkeypox outbreak. The differences include their access to and ability to distribute vaccines, approaches to distribution (e.g. as PEP or PrEP and to which priority groups), access to local public health testing – especially for the uninsured - robustness of local response networks, and the availability of funding. Jurisdictional success in addressing the outbreak may also vary based on their ability to communicate effectively with highly affected populations.
Equity Challenges
Health equity is a stated priority for the Biden administration, and working to limit disparities in access to health information, vaccination, and treatment will help curb the outbreak evenly across groups and reach those across sociodemographic lines (e.g., race, ethnicity, income, etc.). As with both HIV and COVID-19, health disparities have persisted, and there is a risk to see that repeated here. Anecdotal evidence suggest that this occurring with vaccinations in at least some settings already. With monkeypox vaccination and treatment now underway, monitoring vaccination and treatment data by race/ethnicity and other demographic characteristics will help to identify any emerging disparities early on, but thus far this data has not been made publicly available. Efforts to counter potential disparities could also be made at the outset through targeted outreach, including to people of color and transgender people, tailored messaging, ensuring broad access to testing, treatment, and vaccination, and leaning on trusted messengers.
Summary
While the U.S. response to monkeypox has ramped up over time, after early criticism, the outbreak is expanding significantly, and challenges remain. In particular, testing, vaccination, and treatment supply and access remain limited and varied across the country and among different population groups. The ability of the federal government to respond to these challenges over the next few months will be an important determinant in whether the U.S. is able to bring about an end to the outbreak or face the potential of monkeypox becoming an entrenched endemic disease domestically. While WHO has now designated this monkeypox outbreak as a PHEIC, the U.S. has so far not declared it a domestic public health emergency, though the administration is reportedly weighing the option. Whether the administration will elect to use this lever in the future is unknown, but doing so would allow for a range of flexibilities and potential access to funding, should be it be needed.