KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
The high cost of emergency care may impact patients’ ability to afford treatment, with almost half of US adults reporting they have delayed care due to costs. This analysis uses 2019 insurance claims data from the Merative MarketScan Commercial Database, which captures privately insured individuals with large employer health plans, to assess the total and out-of-pocket costs of emergency department visits for this group, overall and by diagnosis and severity level. It also looks at which services contribute most to the costs of emergency department visits and examine regional variation in emergency department costs and provides a demographic profile of consumers who visited the emergency department.
It find that enrollees spend $646 out-of-pocket, on average, for an emergency department visit. The most expensive components of most emergency department visits include evaluation and management charges, imaging, and laboratory studies. Cost varies by disease, visit complexity, and geographic region.
More Than 4 in 10 Republicans and a Third of Parents Now Oppose Schools Requiring Children to Get Vaccinated for Measles and Other Illness, Up Since the COVID-19 Pandemic Began
About 4 in 10 Seniors Have Gotten the New COVID-19 Booster; Many Vaccinated Adults Who Have Not Gotten the Booster are Skeptical of Its Value
Amid controversies around the COVID-19 vaccine and growing distrust of public health authorities, more than four in ten Republicans and Republican-leaning independents, and a third of parents, now say they oppose requiring children in public schools to receive some childhood vaccines, up since 2019, a new KFF COVID-19 Vaccine Monitor survey finds.
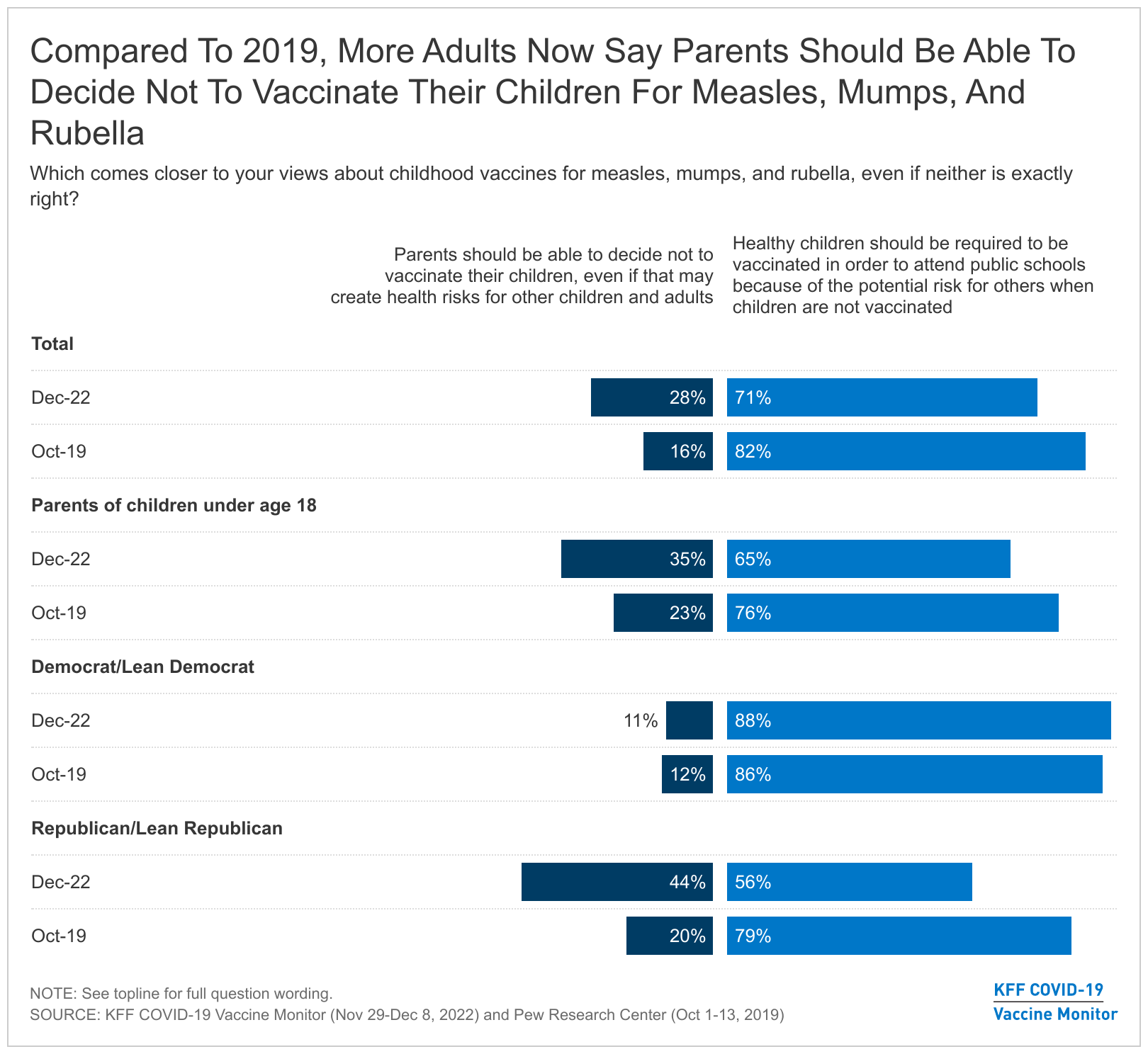
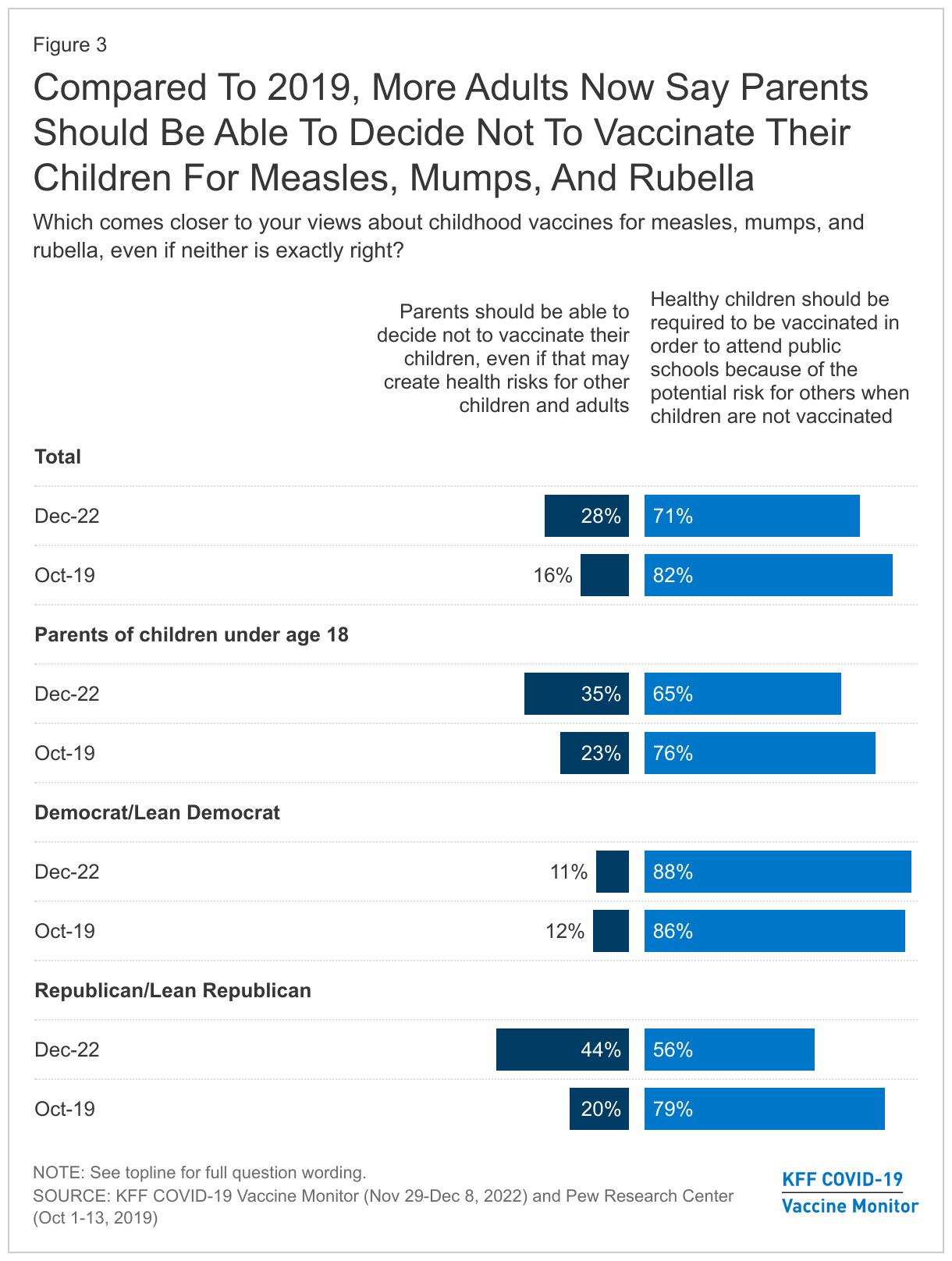
Overall, nearly three in ten adults (28%) nationally now say that parents should be able to decide not to vaccinate their children for measles, mumps, and rubella rather than those vaccinations being required to attend public schools, up from 16% in a 2019 Pew Research Center poll conducted before the COVID-19 pandemic. Among parents, opposition to requiring those childhood vaccines now stands at 35%, up from 23% in 2019.
While most of the public still say that healthy children should be required to get those vaccines to attend public schools (71%), that share is down from 82% in 2019.
The growing opposition stems largely from shifts among people who identify as Republican or lean Republican, with 44% now saying parents should be able to opt out of those childhood vaccines, up from 20% in 2019. In contrast, the vast majority of Democrats and those who lean Democratic support requiring the vaccines for public school students (88%), little changed from 2019 (86%).
Currently, all states and the District of Columbia require children to be vaccinated against certain diseases, including measles and rubella, in order to attend public schools, though exemptions are allowed in certain circumstances.
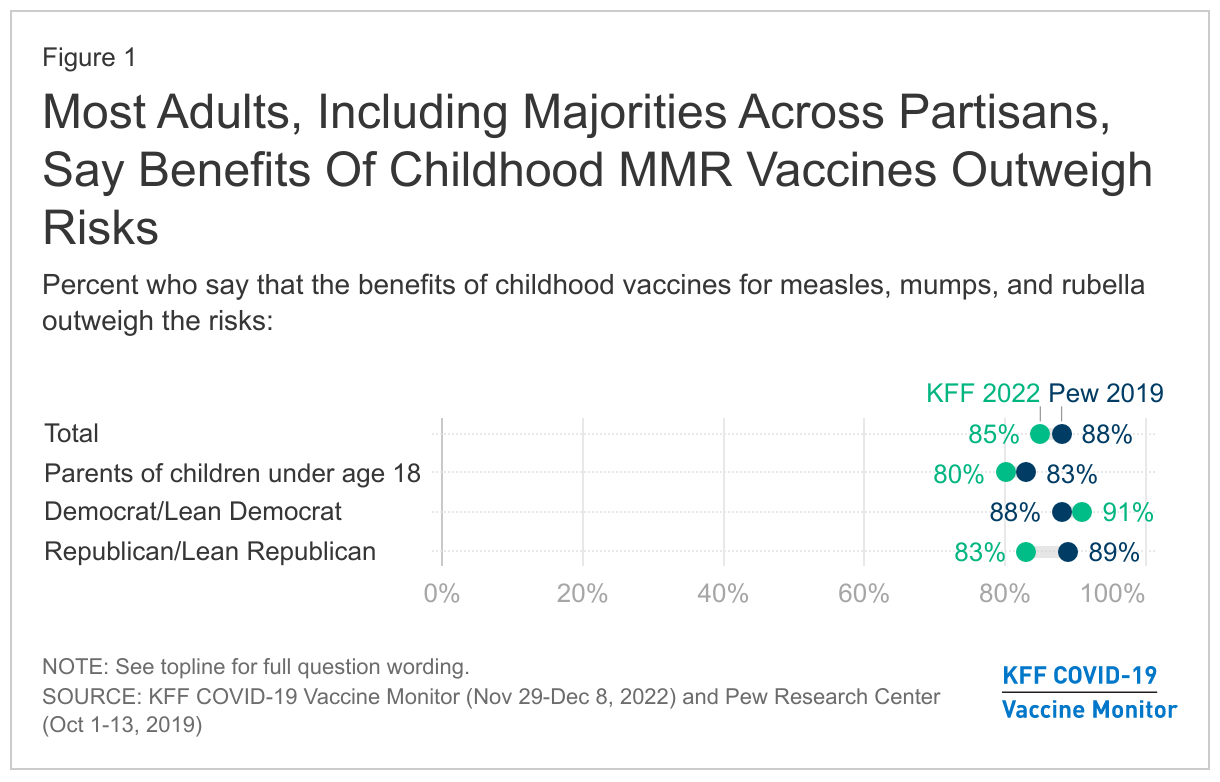
Despite growing opposition to requiring childhood vaccines, the new survey captures only modest shifts in the public’s view of their value. Today 85% of the public and 80% of parents say the benefits of the measles, mumps and rubella vaccines outweigh their risks, little changed from 2019, when 88% of the public and 83% of parents felt that way.
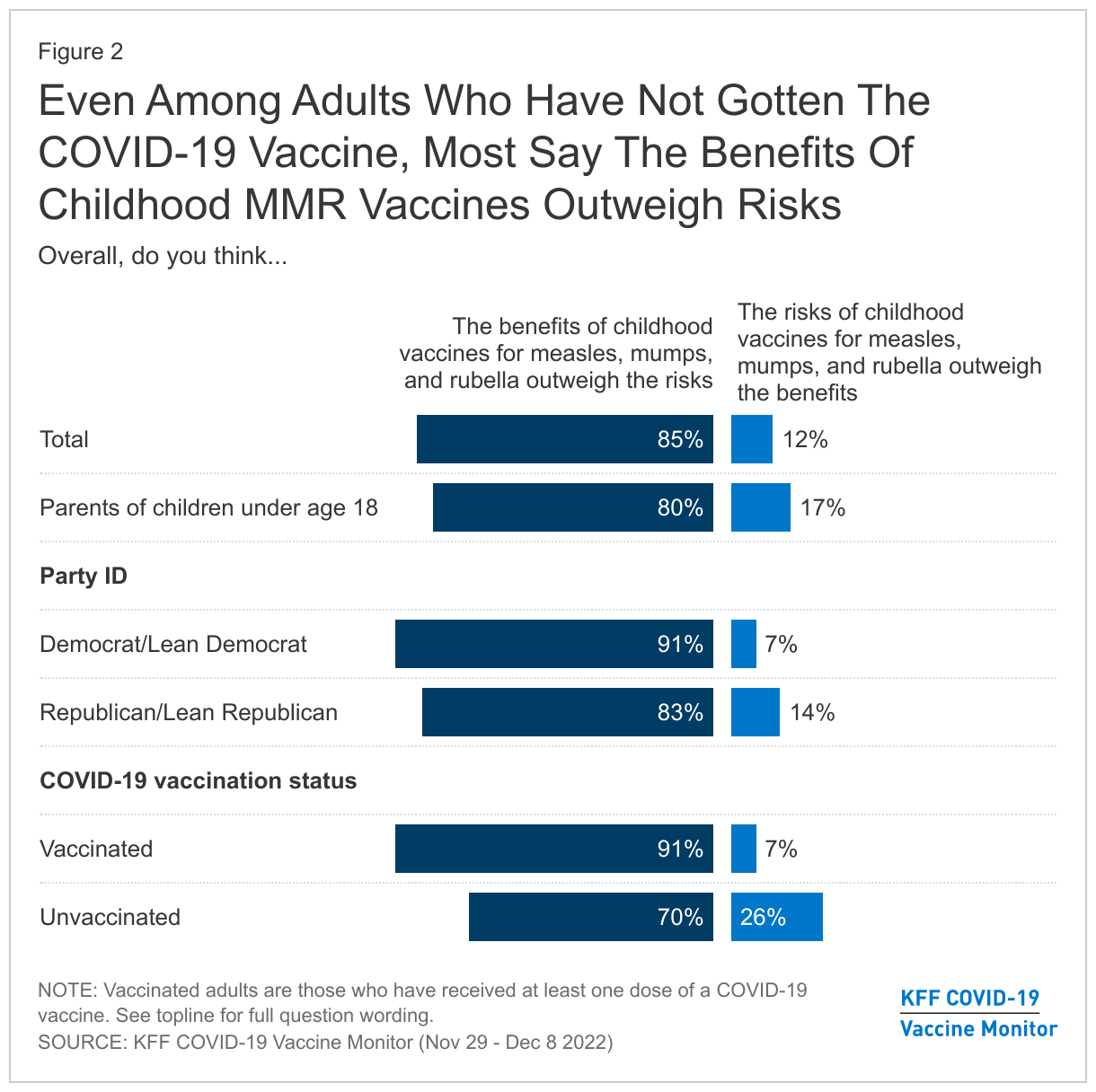
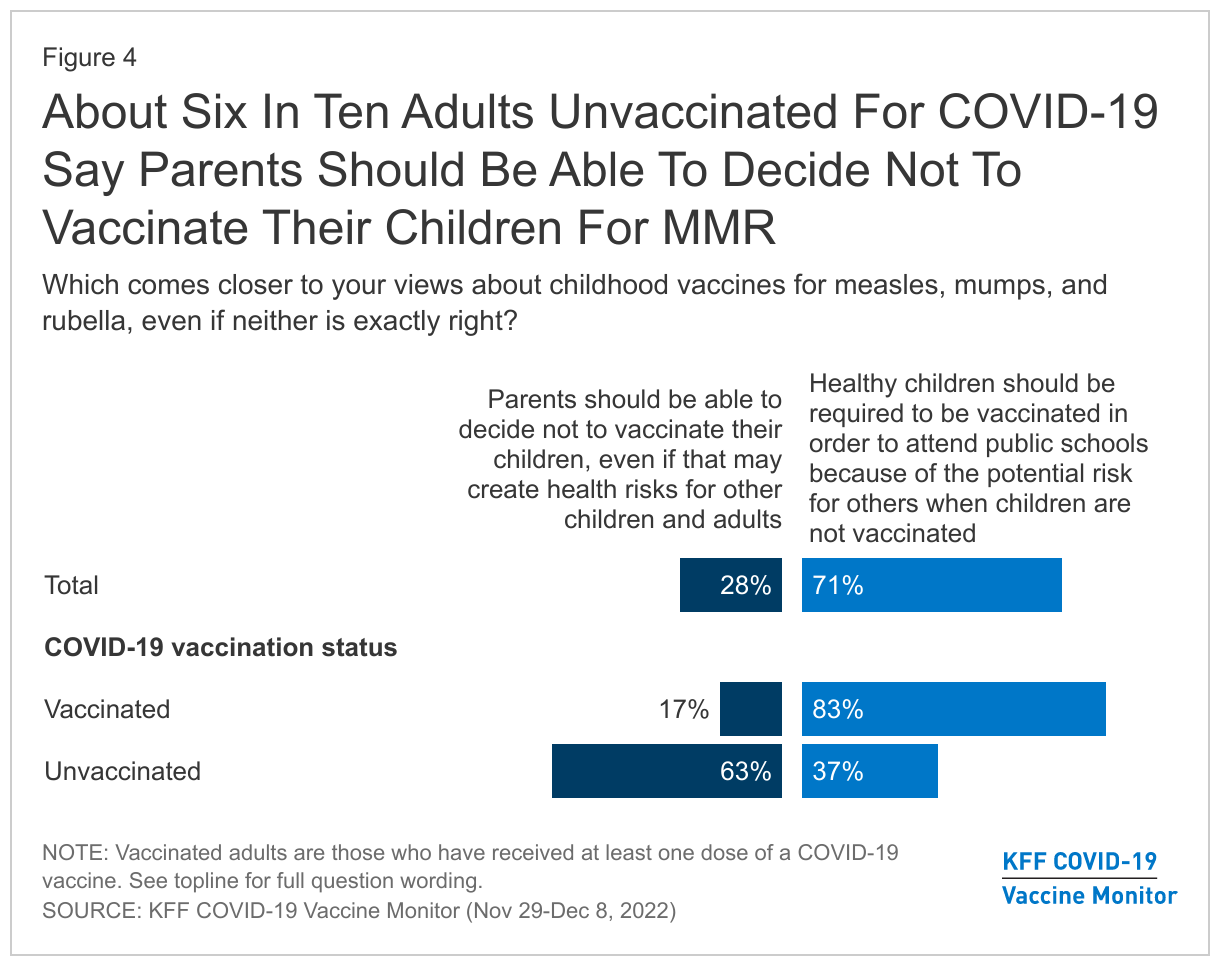
Even among people who have not gotten a COVID-19 vaccine, a large majority (70%) say the benefits of these childhood vaccines outweigh the risks, though one in four (26%) say the risks outweigh the benefits.
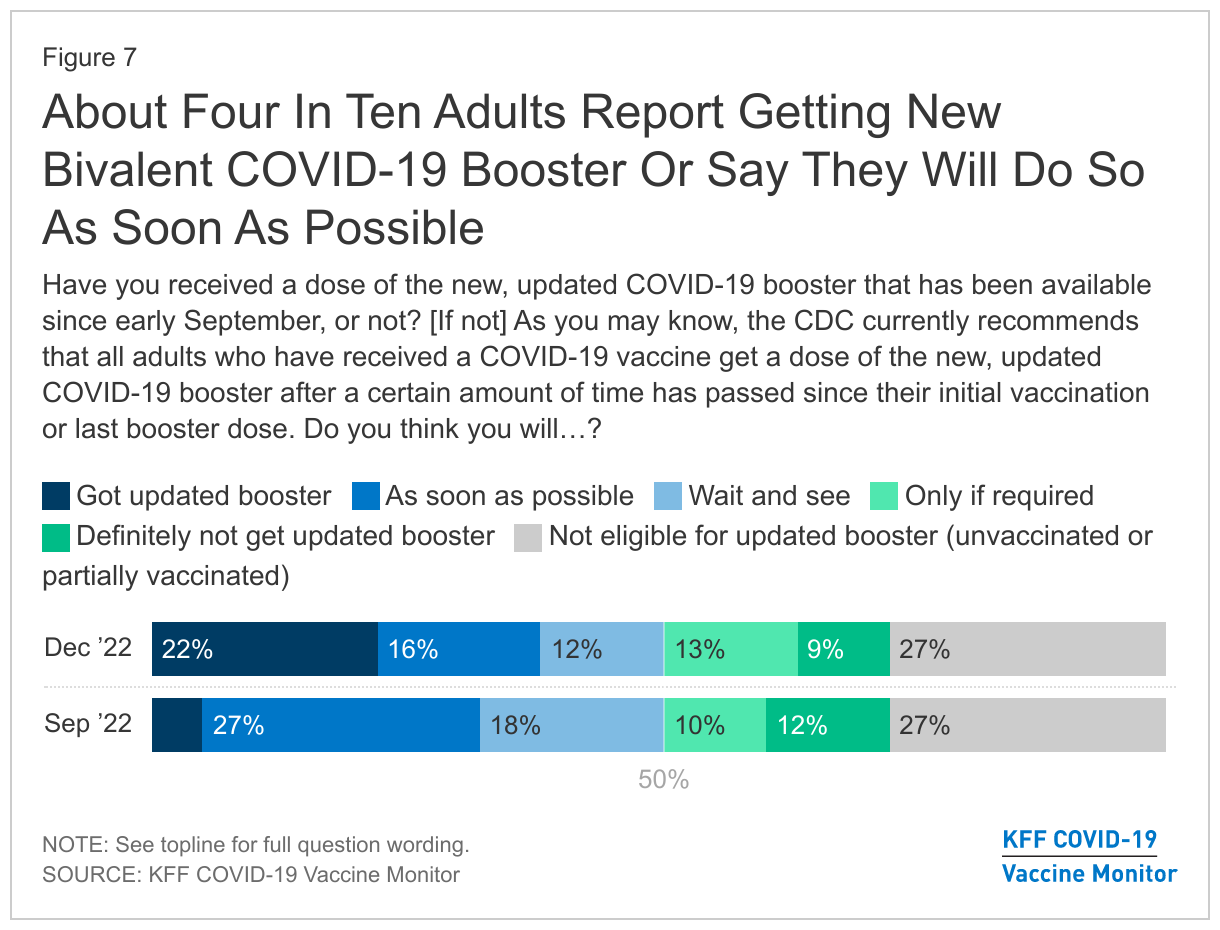
The new survey also finds that about four in ten adults report that they either have already gotten the recommended bivalent booster shot (22%) or say they will get it as soon as they can (16%). The bivalent booster targets both the original and omicron COVID-19 strains and has been available since September.
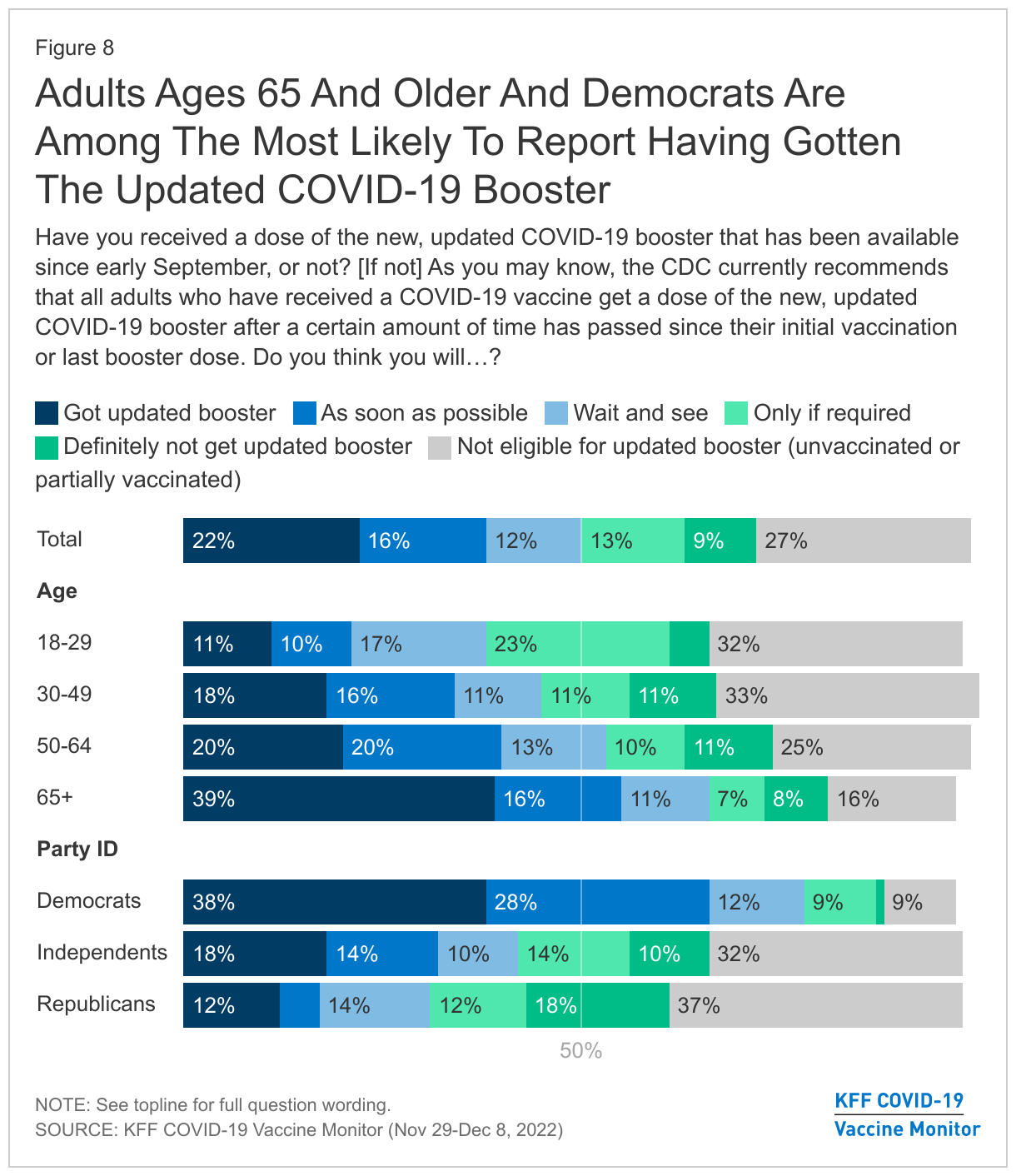
Among adults ages 65 and older, who face higher risks from COVID-19, about four in ten (39%) say they have already gotten the bivalent booster, and another 16% say they intend to do so as soon as possible. Still, this currently leaves more than half of older adults without the protection of the bivalent booster.
Democrats (38%) are much more likely than independents (18%) or Republicans (12%) to say that they’ve gotten the new booster.
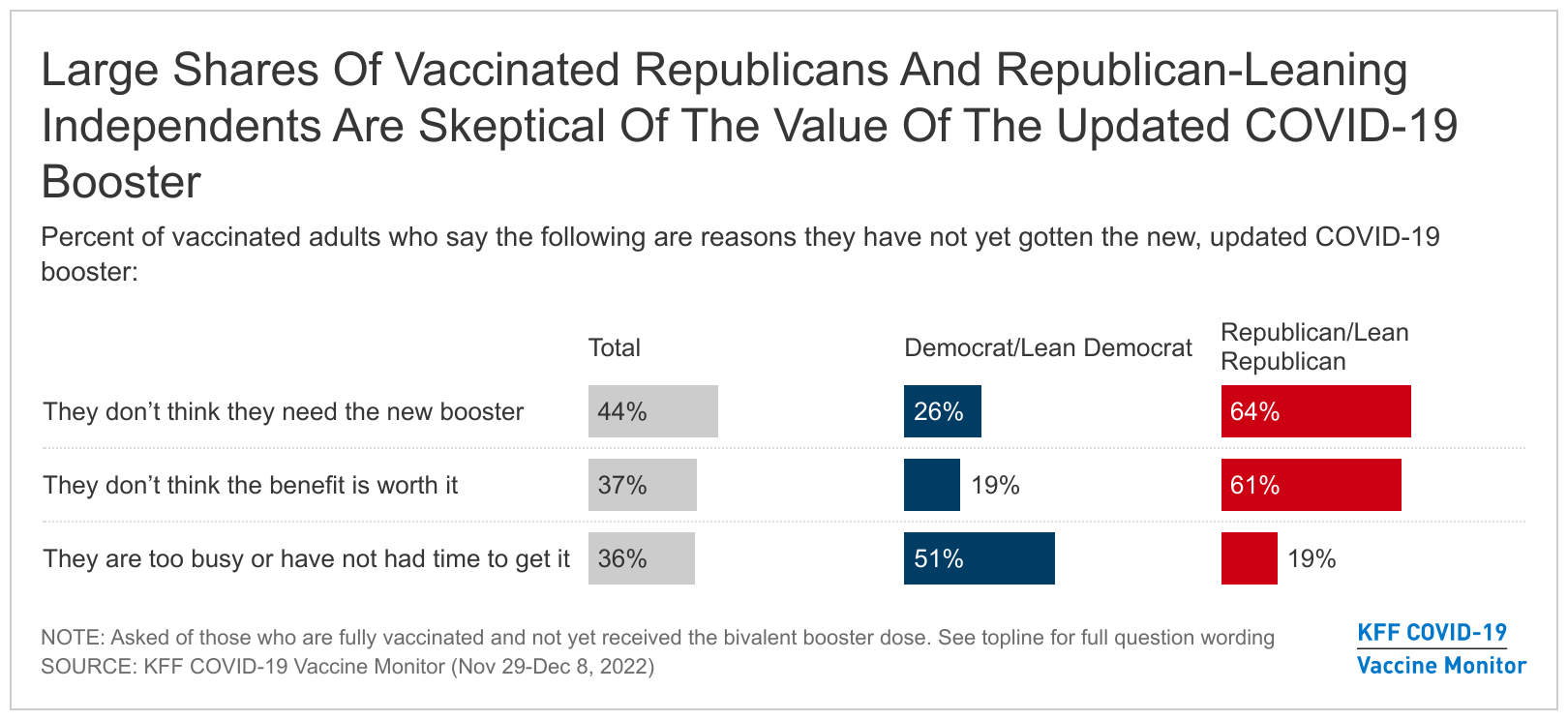
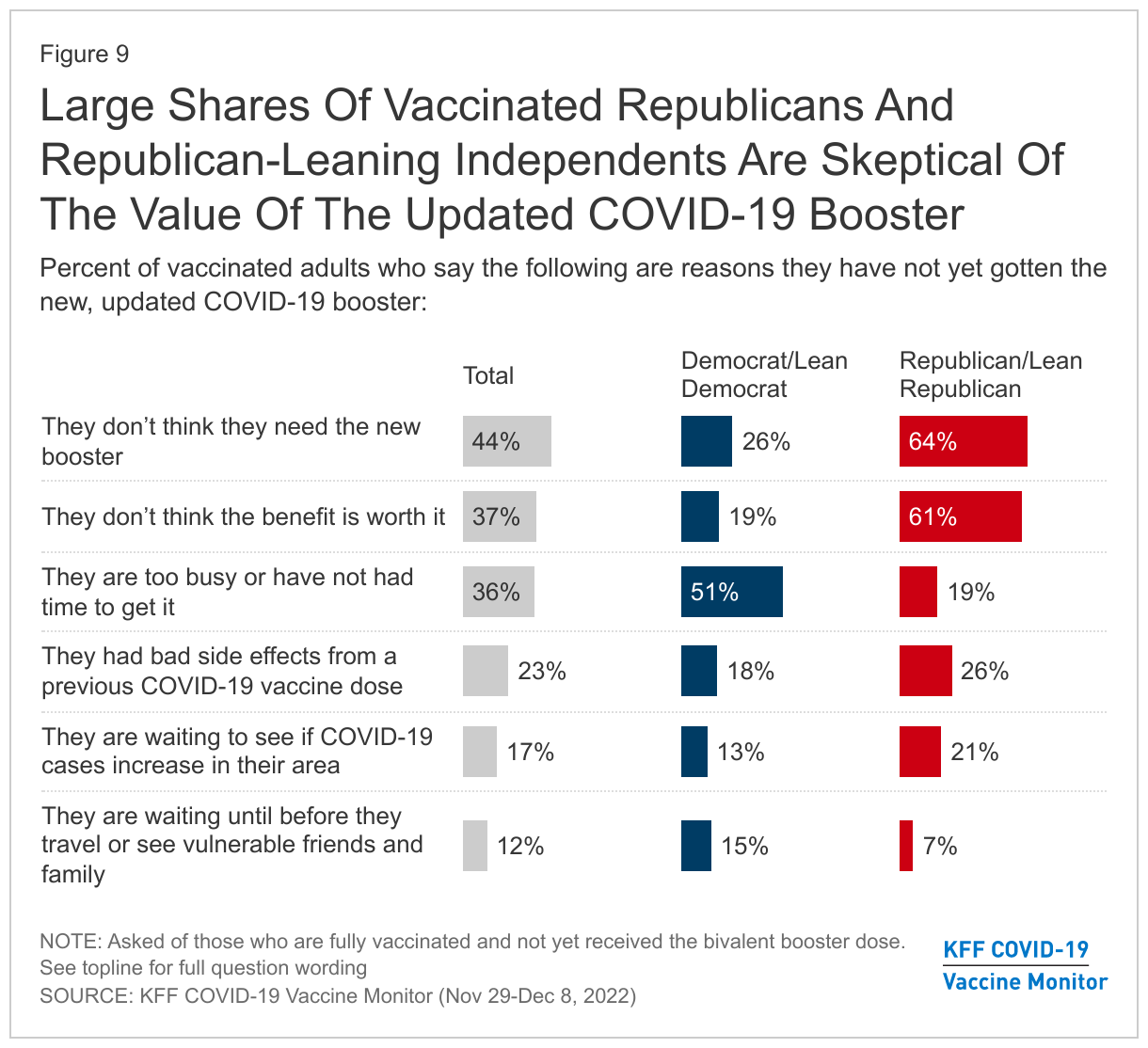
Vaccinated adults who have not gotten a bivalent booster are largely skeptical about its value. Among this group, more than four in ten (44%) say they don’t think they need the new booster, and more than a third (37%) say that they don’t think its benefits are worth it. A similar share (36%) say they are too busy and haven’t had time to get it.
Fewer cite other reasons such as bad side effects from earlier COVID-19 vaccines (23%), waiting to see if cases increase in their area (17%), or waiting until they travel or see vulnerable family and friends (12%).
Among those ages 65 and older who are vaccinated but have not gotten the updated booster, about a third say that they don’t think they need it (36%) and that they don’t think the benefit of the updated booster is worth it (36%). About one in four (23%) say they have been too busy or have not had time to get the new booster yet.
Most vaccinated Republicans or Republican-leaning independents who haven’t gotten the new booster say that they don’t think they need it (64%) or that its benefits are not worth it (61%). Among vaccinated Democrats and Democratic-leaning independents who have not gotten the updated booster, the top reason is being too busy (51%).
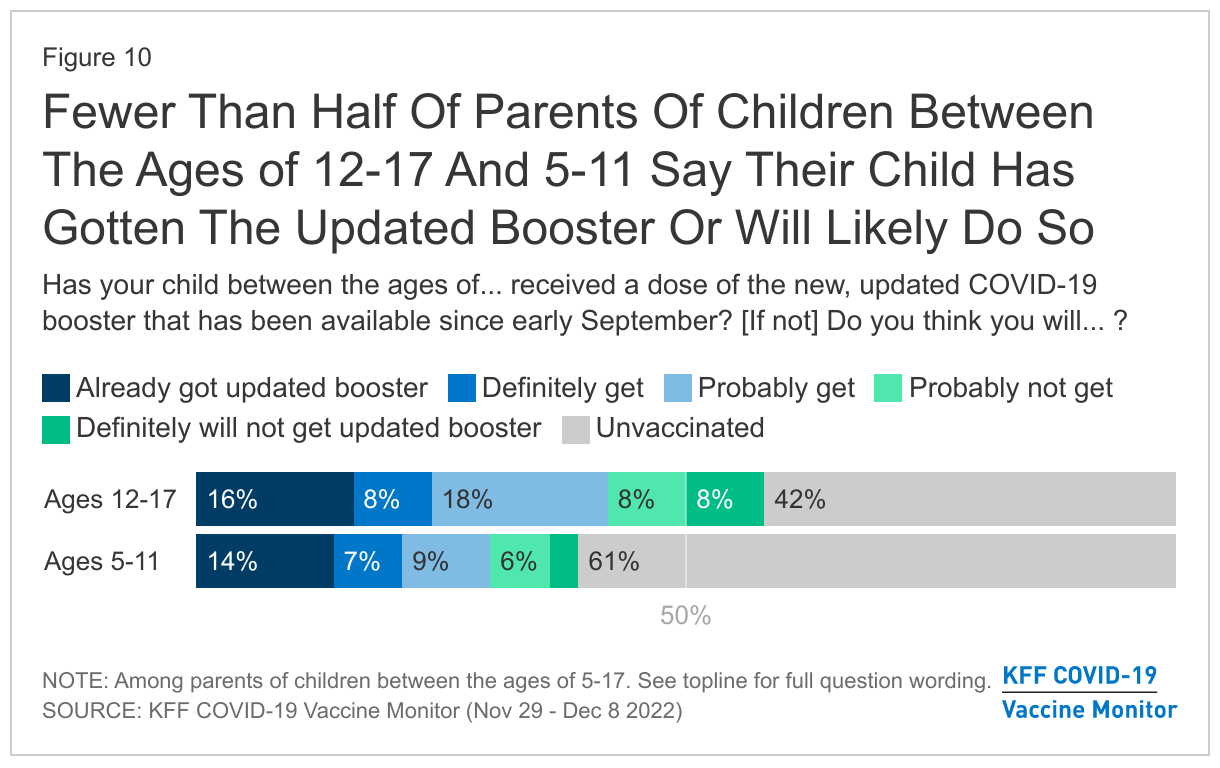
Relatively small shares of parents of children ages 12-17 (16%) and children ages 5-11 (14%) say their child has already received a bivalent booster. At least half of parents in each age group say either that their child is not vaccinated or that they definitely won’t get their child boosted.
Parents Are Now At Least as Likely to Worry Their Children Will Get RSV or the Flu as COVID-19
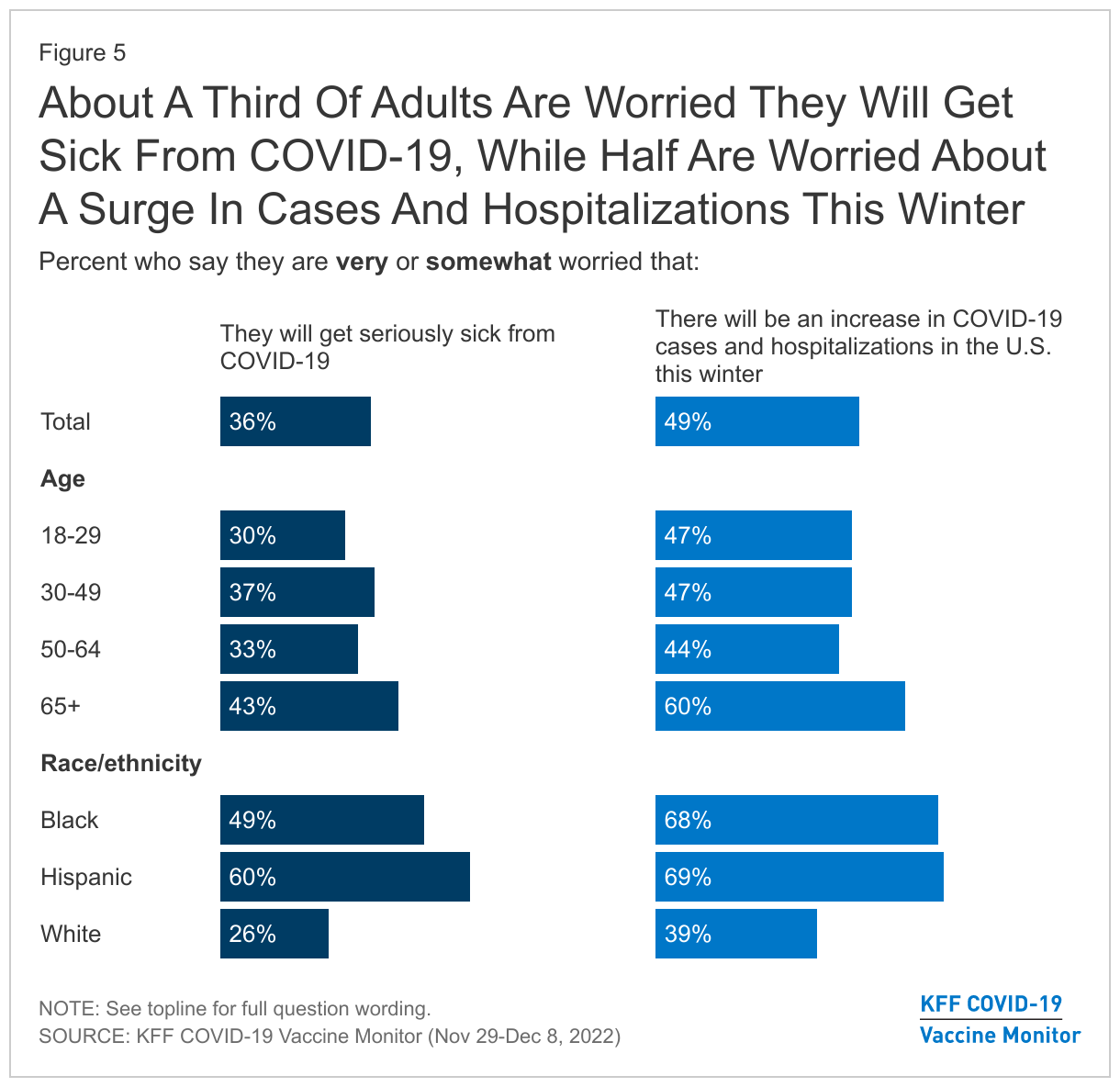
About half (49%) of adults nationally say that they are worried there will be an increase in COVID-19 cases and hospitalizations in the U.S., though just about a third (36%) say they are worried they personally will get seriously sick from the virus. As in the past, Black and Hispanic adults, as well as people over age 65, are among the groups most likely to worry about getting seriously ill.
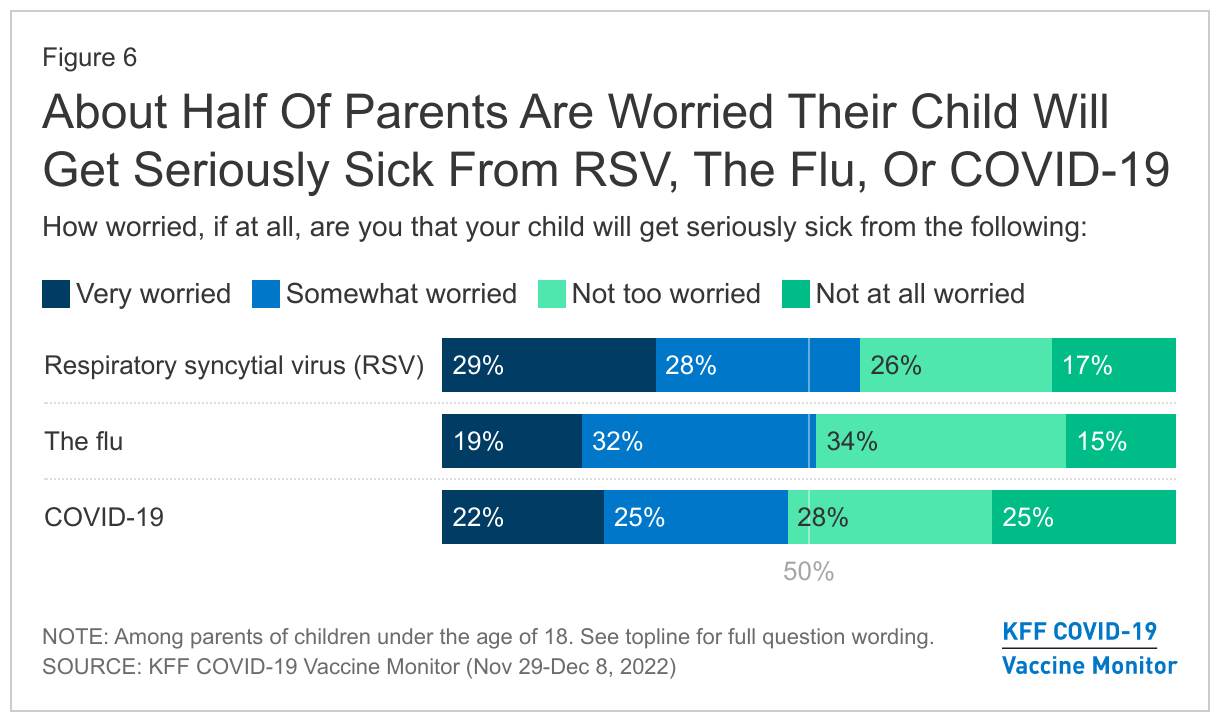
Amid reports about rising flu and RSV cases, parents are now at least as likely to worry about their children getting sick from those illnesses as from COVID-19. Roughly half of parents say they are at least somewhat worried that their children will get sick from RSV (56%), the flu (51%) and COVID-19 (47%).
Designed and analyzed by public opinion researchers at KFF, the Vaccine Monitor survey was conducted from Nov. 29 – Dec. 8, 2022, online and by telephone among a nationally representative sample of 1,259 adults, in English and in Spanish. The margin of sampling error is plus or minus 4 percentage points for the full sample. For results based on other subgroups, the margin of sampling error may be higher.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and acceptance, information needs, trusted messengers and messages, as well as the public’s experiences with vaccination.
While most of the public continue to have confidence in the benefits of childhood vaccines for measles, mumps, and rubella, the experience of the COVID-19 pandemic and debates over vaccine requirements and mandates appear to have had an impact on public attitudes towards MMR vaccine requirements for public schools. The latest KFF COVID-19 Vaccine Monitor survey finds that about seven in ten adults (71%) say healthy children should be required to get vaccinated for MMR in order to attend public schools, down from 82% who said the same in an October 2019 Pew Research Center poll. Almost three in ten (28%) now say that parents should be able to decide not to vaccinate their school-age children, even if this creates health risks for others, up from 16% in 2019. Among Republicans and Republican-leaning independents, there has been a 24 percentage-point increase in the share who hold this view (from 20% to 44%).
With COVID-19 cases rising across the country, just about a third of adults say they are worried they will get seriously sick from COVID-19, though nearly half of the public say they are worried about an increase in COVID-19 cases and hospitalizations in the U.S. this winter. As previous KFF surveys have repeatedly found, Black and Hispanic adults continue to be more concerned about the pandemic compared to White adults, with about two-thirds of Black adults (68%) and Hispanic adults (69%) saying they are worried about an increase in cases and hospitalizations this winter, compared to about four in ten White adults who say the same. Older adults are more likely than those under age 65 to say they are worried they will get seriously sick from COVID-19 (43% vs. 34%) and that cases and hospitalizations will rise this winter (60% vs. 46%).
As the country faces a “tripledemic”, with a surge in flu and RSV (respiratory syncytial virus) cases accompanying the rise in COVID-19 cases, many parents are now concerned about not one, but all three of these viruses. About half of parents are worried their child will get seriously sick from COVID-19 or the flu. A slight majority of parents (56%) say they are worried their child will get seriously sick from RSV – rising to more than seven in ten parents with a child under the age of 5 (73%), an age group that is particularly vulnerable to RSV.
Though many no longer see COVID-19 as a uniquely urgent threat, public health officials continue to encourage vaccination and emphasize the importance of the updated bivalent booster to help prevent serious illness and death from COVID-19, particularly in light of holiday gathering and travel. However, public uptake of the updated booster is relatively tepid, with just about one in five adults saying they have already gotten it. Democrats (38%) and adults ages 65 and older (39%) have been more eager, with about four in ten saying have already gotten the updated COVID-19 booster which has been available since September. Fewer young adults under the age of 30 (11%) and Republicans (12%) report having gotten an updated booster dose.
Though public health officials have stressed the importance of the updated COVID-19 booster for older adults who are more vulnerable to complications from a COVID infection, more than half of adults ages 65 and older have not yet gotten the updated booster. About a third (36%) of vaccinated adults ages 65 and older who have not yet gotten the bivalent booster say they don’t think they need it (36%) and a similar share say they don’t think the benefit of the updated booster is worth it.
Vaccinated Republicans and Republican-leaning independents are particularly skeptical of the value of the updated booster with about two-thirds of those who have not yet gotten it saying they don’t think they need it (64%) and that the benefit is not worth it (61%) while Democrats are most likely to say they have been too busy or haven’t had the time to get the update booster (51%).
The Impact Of COVID-19 On Attitudes Towards Other Childhood Vaccines
Despite the politicization of the COVID-19 vaccine and decreasing levels of trust in the FDA and CDC, most adults (85%) say the benefits of childhood vaccines for measles, mumps, and rubella (MMR) outweigh the risks, with little change from the share who said the same in a Pew Research Center poll in 2019 (88%). Though there were no significant differences across partisans in 2019, our survey finds that Republicans and Republican-leaning independents are now less likely than their Democratic counterparts believe the benefits of MMR vaccines outweigh the risks (83% vs. 91%).
While most parents of children under age 18 (80%) say they think the benefits of childhood MMR vaccines outweigh the risks, about one in six parents (17%) think the risks of these vaccines outweigh the benefits. Among adults who have not gotten vaccinated for COVID-19, about one in four (26%) say the risks of childhood vaccines for measles, mumps, and rubella outweigh the benefits. Nonetheless, it remains notable that even among adults who have not gotten the COVID-19 vaccine, most (70%) say the benefits of childhood MMR vaccines outweigh the risks.
While confidence in the benefits of childhood MMR vaccines remains high, the debate over COVID-19 vaccine mandates may have had some spillover effects on attitudes towards requiring MMR vaccines for children attending public school. Currently, all states and the District of Columbia require children to be vaccinated against certain diseases, including measles and rubella, in order to attend public schools, though exemptions are allowed in certain circumstances. Yet, there has been a notable decrease since 2019 in the share of adults who say “healthy children should be required to be vaccinated (for MMR) in order to attend public schools because of the potential risk for others when children are not vaccinated,” with 71% saying they should be required to do so, an 11 percentage point decrease from a October 2019 Pew Research Center poll. Almost three in ten (28%) now say parents “should be able to decide not to vaccinate their children, even if that may create health risks for other children and adults,” an increase from 16% in 2019.
This decrease in support for MMR vaccine requirements for children in public schools is driven by Republicans and Republican-leaning independents – just a slight majority of Republicans (56%) say healthy children should be required to be vaccinated to attend public schools, a 23 percentage-point decline from 2019 when about eight in ten expressed support for such a requirement. More than four in ten Republicans and Republican-leaning independents (44%) now say that parents should be able to decide not to vaccinate their children, up from 20% in 2019. This compares to 11% of Democratic-leaning parents who say the same, a share that has held steady since 2019.
Among parents of children under age 18, about two-thirds (65%) think healthy children should be required to be vaccinated to attend public schools, down from 76% who said the same in 2019. One-third (35%) of parents now believe parents should be able to decide not to vaccinate their children, up from 23% in 2019.
While we cannot know the pre-pandemic attitudes that adults who are currently not vaccinated for COVID-19 held about childhood MMR vaccines, most (63%) of these adults unvaccinated for COVID-19 say that parents should be able to decide not to vaccinate their children, even if that creates health risks for children and adults. Just about four in ten (37%) adults who are not vaccinated for COVID-19 say that healthy children should be required to be vaccinated in order to attend public school.
COVID-19 And Other Winter Illnesses
With reports of COVID-19 cases increasing across the country, just about a third of adults (36%) say they are worried that they will get seriously sick from COVID-19, similar to the share which expressed this concern in January (34% worried) amidst the initial omicron surge in the U.S., but up from November 2021 (30% worried) before the omicron variant became widespread. However, about half of the public (49%) say they are worried that there will be an increase in COVID-19 cases and hospitalizations this year. Adults ages 65 and older, who are more vulnerable to negative outcomes from a COVID-19 infection, are more likely than younger adults to express worry about a winter COVID-19 surge (60% vs. 46%) and to worry that they will get seriously sick from the virus (43% vs. 34%).
As previous KFF surveys have found time and time again, people of color continue to be more concerned about the pandemic compared to White adults. The December KFF COVID-19 Vaccine Monitor survey finds that about two-thirds of Black adults (68%) and Hispanic adults (69%) say they are very worried about an increase in COVID-19 cases and hospitalizations this winter, compared to about four in ten White adults (39%) who express the same concern. Black and Hispanic adults (49% and 60%, respectively) are also more likely than White adults (26%) to worry that they will personally get seriously sick from the virus.
Worries About COVID-19 And Other Winter Viruses In Children
This winter has not only brought reports of increasing COVID-19 cases, but also widespreadreports of a surge in flu and RSV cases, particularly among children. In a sign that COVID-19 is changing from being a singular concern to part of the landscape of different illnesses people worry about, parents’ worries about their children getting sick from COVID this winter are about on par with their worries about other viruses like flu and RSV. About half of parents (47%) say they are “very” or “somewhat” worried that their children will get seriously sick from COVID-19 and a similar share (51%) say they are worried their children will get seriously sick from the flu. A slight majority of parents (56%) say they are worried their child will get seriously sick from RSV – rising to 73% of parents with children under the age of 5, who are particularly vulnerable to RSV. Notably, despite half of parents saying they are worried their child may get seriously sick from the flu, just a third of parents (34%) say their child has gotten a flu shot for the current flu season.
Uptake Of The Updated Bivalent COVID-19 Booster
Although for many people COVID-19 may be less of an urgent concern this winter, public health officials continue to emphasize the importance of boosters in reducing the risk of serious illness and death particularly among the most vulnerable. Despite this, the public’s response to the new bivalent booster has been somewhat lackluster. About four in ten adults say they have either received the updated bivalent COVID-19 booster dose (22%)1 , which has been available since September, or say they plan to get the new booster as soon as possible (16%). About one in ten adults say they want to “wait and see” before getting the new booster (12%), while a similar share (13%) say they will only get it if they are required to do so. A further 9% say they will definitely not get the new updated booster while about one in four adults (27%) are unvaccinated or only partially vaccinated, and therefore not eligible for the updated bivalent booster dose.
KFF’s September COVID-19 Vaccine Monitor survey, fielded shortly after the new updated booster was made available, found that more than a third of older adults ages 65 and older said they intended to get the updated booster as soon as possible. This month’s survey finds that many of these older adults remain eager, with four in ten adults ages 65 and older (39%) saying they have already gotten the updated COVID-19 booster while 16% say they will do so as soon as they can. However, this still leaves more than half of older adults, who are more vulnerable to complications from a COVID infection, without the protection of the updated booster.
Democrats also seem eager to get the updated booster with about four in ten (38%) saying they have already done so. Indeed, Democrats are three times as likely as Republicans to report having already gotten the updated COVID-19 booster (38% vs. 12%). Notably, about three in ten Republicans say they will only get the updated booster if they are required to do so (12%) or say they will “definitely not” get the new COVID-19 booster dose (18%). A further 37% of Republicans are unvaccinated or only partially vaccinated and therefore not eligible for the new updated COVID-19 booster dose.
Vaccinated adults who have not yet gotten a dose of the bivalent COVID-19 booster cite a variety of reasons for not getting the updated booster; about four in ten (44%) say they do not think they need it and about a third (37%) say they do not think the benefit is worth it. About a third (36%) say they have been too busy or have not had the time to get it, while about one in four (23%) say they have not gotten the updated booster because they had bad side effects from a previous COVID-19 vaccine dose. About one in six (17%) vaccinated adults who have not gotten the updated booster say they have not done so because they are waiting to see if COVID-19 cases increase in their area, while 12% say they are waiting until before they travel or see vulnerable family and friends to get the updated booster.
Though public health officials have stressed the importance of the updated COVID-19 booster for older adults, who are more vulnerable to complications from a COVID infection, about one third (36%) of vaccinated adults ages 65 and older who have not yet gotten the booster say they don’t think they need it (36%) and a similar share say they don’t think the benefit of the updated booster is worth it. About one in four (23%) vaccinated adults ages 65 and older say they have not gotten the updated booster because they have been too busy or have not had time to get it yet.
Notably, at least six in ten vaccinated Republicans or Republican leaning independents who have not yet gotten the updated booster say they haven’t done so because they don’t think they need it (64%) or do not think the benefit is worth it (61%). Among vaccinated Democrats or Democratic-leaning independents who have not yet gotten the updated booster, the most common reason for not yet doing so is having been too busy or not having the time to get it (51%).
About one in four parents of teenagers ages 12 to 17 say their child has already gotten the updated COVID-19 booster (16%) or that they will definitely be doing so (8%). A further 18% say their teen will probably get the update booster. Notably, about four in ten parents of teenagers say their 12-17 year old is not vaccinated for COVID-19 and therefore not eligible to get the updated bivalent booster.
Among parents of younger children between the ages of 5 and 11, six in ten (61%) say their child is unvaccinated and therefore not eligible for the new COVID-19 booster. About one in five parents say their 5 to 11 year old has either gotten the updated booster (14%) or will definitely be doing so (7%), while a further 9% say their child will probably get the updated booster.
Methodology
This KFF COVID-19 Vaccine Monitor Poll was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted November 29 – December 8, 2022, online and by telephone among a nationally representative sample of 1,259 U.S. adults in English (1,203) and in Spanish (56). The sample includes 1,029 adults reached through the SSRS Opinion Panel[1] either online or over the phone (n=32 in Spanish). The SSRS Opinion Panel is a nationally representative probability-based panel where panel members are recruited randomly in one of two ways: (a) Through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Groups (MSG) through the U.S. Postal Service’s Computerized Delivery Sequence (CDS); (b) from a dual-frame random digit dial (RDD) sample provided by MSG. For the online panel component, invitations were sent to panel members by email followed by up to three reminder emails. 1,004 panel members completed the survey online and panel members who do not use the internet were reached by phone (n=25).
Another 230 (n=24 in Spanish) interviews were conducted from a random digit dial telephone sample of prepaid cell phone numbers obtained through MSG. Phone numbers used for the prepaid cell phone component were randomly generated from a cell phone sampling frame with disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification was based on incidence of the race/ethnicity groups within each frame. Respondents in the phone samples received a $15 incentive via a check received by mail, and web respondents received a $5 electronic gift card incentive (some harder-to-reach groups received a $10 electronic gift card).
The online questionnaire included two questions designed to establish that respondents were paying attention. Cases that failed both attention check questions, those with over 30% item non-response, and cases with a length less than one quarter of the mean length by mode were flagged and reviewed. Cases were removed from the data if they failed two or more of these quality checks. Based on this criterion, one case was removed.
The combined cell phone and panel samples were weighted to match the sample’s demographics to the national U.S. adult population using data from the Census Bureau’s 2021 Current Population Survey (CPS). Weighting parameters included sex, age, education, race/ethnicity, region, and education. The sample was weighted to match patterns of civic engagement from the September 2017 Volunteering and Civic Life Supplement data from the CPS and to match frequency of internet use from the National Public Opinion Reference Survey (NPORS) for Pew Research Center. Finally, the sample was weighted to match patterns of political party identification based on a parameter derived from recent ABS polls conducted by SSRS polls. The weights take into account differences in the probability of selection for each sample type (prepaid cell phone and panel). This includes adjustment for the sample design and geographic stratification of the cell phone sample, within household probability of selection, and the design of the panel-recruitment procedure.
The margin of sampling error including the design effect for the full sample is plus or minus 4 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Group
N (unweighted)
M.O.S.E.
Total
1,259
± 4 percentage points
Race/Ethnicity
White, non-Hispanic
771
± 5 percentage points
Black, non-Hispanic
190
± 10 percentage points
Hispanic
226
± 9 percentage points
Party identification
Democrat
463
± 6 percentage points
Republican
327
± 7 percentage points
Independent
297
± 8 percentage points
Parents
Total parents
377
± 7 percentage points
Parent with a child ages 6 months through 4 years old
133
± 11 percentage points
Parent with a child ages 5-11
201
± 9 percentage points
Parent with a child ages 12-17
193
± 10 percentage points
Endnotes
KFF’s COVID-19 Vaccine Monitor data on vaccine and bivalent booster uptake is based on self-reported responses and may differ data from the Centers for Disease Control which is based on administered doses reported by specific jurisdictions and providers. ↩︎
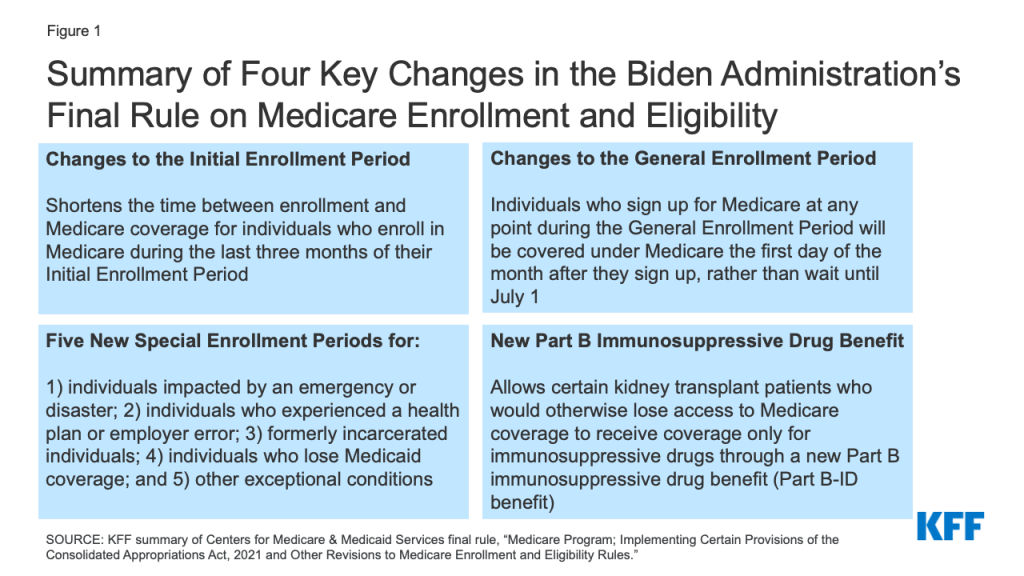
The Centers for Medicare & Medicaid Services (CMS) issued a final rule on October 28, 2022 to implement several changes in Medicare enrollment and eligibility that were included in the Consolidated Appropriations Act of 2021 (CAA). These changes are designed to minimize gaps in coverage for people who sign up for Medicare and improve access to care by shortening the gap between Medicare enrollment and coverage; creating new Special Enrollment Periods for individuals whose coverage would otherwise be delayed due to challenging circumstances, such as a natural disaster; and extending coverage of immunosuppressive drugs for certain beneficiaries with end-stage renal disease (ESRD) who would otherwise lose coverage for these drugs after their kidney transplant.
This brief highlights four key changes related to Medicare enrollment and eligibility under the final rule, and summarizes the estimated impact of these provisions on coverage and costs. These provisions are expected to reduce gaps in coverage for people when they first sign up for Medicare, and have a negligible impact on Medicare spending, according to CMS estimates.
Figure 1: Summary of Four Key Changes in the Biden Administration’s Final Rule on Medicare Enrollment and Eligibility
1. The final rule accelerates the start of Medicare coverage for beneficiaries who enroll during the Initial Enrollment Period
Individuals have several opportunities to enroll in Medicare. They can enroll when they first become eligible for Medicare during the Initial Enrollment Period, during the annual General Enrollment Period, or during a Special Enrollment Period. People are generally advised to sign up for Medicare during their Initial Enrollment Period, unless they have group health plan coverage from an employer. Individuals with insurance coverage through the Marketplace or COBRA are also advised to sign up for Medicare during their Initial Enrollment Period. Depending upon when they enroll in Medicare, individuals may face a gap in coverage and late enrollment penalties. Late enrollment penalties are added to a beneficiary’s monthly premium costs for the remainder of their Medicare enrollment. For Medicare Part B, 10% is added to the standard Part B monthly premium for each 12-month period a beneficiary delays enrollment in Part B. The new rule reduces the gaps in coverage between the date of enrollment and coverage during both the Initial Enrollment and General Enrollment Periods, effective January 1, 2023.
Policy prior to January 1, 2023
When an individual is turning 65, their first opportunity to sign up for Medicare is during a 7-month window called the Initial Enrollment Period. This period spans three months before the month of their 65th birthday, the month of their birthday, and three months after it. When Medicare coverage begins depends on when an individual enrolls during their Initial Enrollment Period. Under the policy in effect prior to January 1, 2023, individuals who enrolled during the last three months of their Initial Enrollment Period could face gaps between signing up and the start of Medicare coverage:
If an individual signs up for Medicare during any of the first 3 months, their coverage begins the first day of the month they turn 65. If a beneficiary signs up during the month they turn 65, coverage starts the first day of the following month.
If they sign up 1 month after they become eligible, coverage begins 2 months later, and if they sign up 2 or 3 months after they become eligible, coverage begins 3 months later.
New policy
This rule shortens the time between enrollment and Medicare coverage for individuals who enroll in Medicare during the last three months of their Initial Enrollment Period. Individuals who sign up for Medicare during the last three months of their Initial Enrollment Period will be covered under Medicare the first day of the month following the month in which they enroll.
Examples of how this new policy will affect Medicare coverage
Mary turned 65 on April 1, 2022, before the new rule took effect. Her 7-month Initial Enrollment Period started three months before her birthday (January) and ended three months after the month she turned 65 (July). Mary signed up for Medicare on July 1, the seventh month of her Initial Enrollment Period. Her Medicare coverage started on October 1, leaving her without Medicare coverage for three months after she enrolled in Medicare, and six months after her 65th
Mary’s younger sister, Anne, is turning 65 on April 1, 2023. Under this new rule, if Anne enrolls in Medicare on July 1, 2023, the seventh month of her Initial Enrollment Period, her Medicare coverage will take effect on August 1 (the first day of the month following enrollment), a shorter gap in coverage than her older sister Mary experienced before the final rule took effect.
2. The final rule shortens the gap between enrollment and Medicare coverage for beneficiaries who enroll during the General Enrollment Period
Policy prior to January 1, 2023
If an individual misses their Initial Enrollment Period for Medicare, they can enroll during the General Enrollment Period, which runs from January 1 to March 31 each year. Under the policy in effect until January 1, 2023, for individuals who enrolled at any point during the General Enrollment Period, Medicare coverage would begin on July 1, resulting in up to a six-month gap between Medicare enrollment and the start of coverage.
New policy
Individuals who sign up for Medicare at any point during the General Enrollment Period will be covered under Medicare the first day of the month after they sign up, rather than waiting until July 1.
Examples of how this new policy will affect Medicare coverage
John’s 65th birthday was June 15, 2021 (prior to the effective date of the new rule), but he missed his 7-month Initial Enrollment Period, which started three months before his birthday in March 2021 and ended September 2021. His next opportunity to enroll in Medicare was during the next General Enrollment Period, between January 1 and March 31, 2022. John signed up for Medicare during the first week of January, and his Medicare coverage started on July 1, leaving him without Medicare coverage for more than a year after his 65th birthday and six months after he signed up during the General Enrollment Period.
John’s brother, Mike, turned 65 on June 15, 2022. He also missed the opportunity to enroll in Medicare during his Initial Enrollment Period and instead plans to sign up during the next General Enrollment period, January-March 2023. If Mike signs up during January, his coverage will begin the following month, on February 1, 2023, rather than on July 1, as it would have under the old policy. The final rule will reduce the number of months people like Mike would have to wait to be covered by Medicare.
3. The final rule establishes new Special Enrollment Periods to reduce gaps in coverage for people who missed their Medicare enrollment period due to certain circumstances
Medicare’s Special Enrollment Periods allow beneficiaries to sign up for Medicare Part B and Premium-Part A or change the type of Medicare coverage they have under certain situations, without being subject to a late enrollment penalty. The time period for enrollment under these Special Enrollment Period, as well as the types of coverage changes that can be made, vary based on circumstances. For example, individuals who did not enroll in Medicare during their Initial Enrollment Period because they received health insurance through a qualified group health plan have an 8-month Special Enrollment Period to sign up for Medicare after they stop working or lose their group health plan coverage. Examples of other circumstances that grant existing Medicare beneficiaries a Special Enrollment Period to change their coverage include moving into or out of a facility (e.g., skilled nursing facility) or if Medicare terminates the beneficiary’s current Medicare Advantage plan. Generally, during a Special Enrollment Period, Medicare coverage, or the change in coverage, begins the first day of the month following enrollment.
Policy prior to January 1, 2023
Prior to the enactment of the Consolidated Appropriations Act of 2021, CMS did not have broad authority to create new Special Enrollment Periods, which potentially created gaps in coverage for individuals seeking to enroll in Medicare who had extenuating circumstances not specified in law (such as those listed above). As a result, some individuals with extenuating circumstances beyond their control, such as someone living in an area struck by a disaster, could miss their Initial Enrollment Period for Medicare and be subject to a late enrollment penalty as a result.
New policy
The Consolidated Appropriations Act of 2021 gives CMS the authority to create new Special Enrollment Periods for individuals who meet certain exceptional conditions. Using this authority, CMS finalized five new Special Enrollment Periods in this final rule that will provide people who missed a Medicare enrollment period because of exceptional circumstances an opportunity to enroll without having to wait for the General Enrollment Period. These Special Enrollment Periods are generally effective for circumstances that occur on or after January 1, 2023, and Medicare coverage will begin the first day of the month following the month of enrollment. For all of these Special Enrollment Periods, individuals will not be subject to a late enrollment penalty.
Individuals impacted by an emergency or disaster: The rule creates a Special Enrollment Period for individuals who missed an enrollment opportunity because they were impacted by certain government-declared emergencies and disasters. To qualify, an individual must demonstrate that they themselves, their authorized representative, legal guardian, or a person who makes health care decisions on behalf of them, lives in (or lived) in that impacted area. This Special Enrollment Period will begin on the date an emergency or disaster is declared and ends 6 months after the declaration has ended.
Individuals who experienced a health plan or employer error: This Special Enrollment Period is intended for individuals who did not enroll in Medicare because of misrepresentation by, or incorrect information from their employer, a group health plan, or agents and brokers of health plans. These individuals can enroll in Medicare without penalty starting from the date they notify the Social Security Administration of this error up to 6 months later.
Formerly incarcerated individuals: This Special Enrollment Period affects: (1) individuals who become newly eligible for Medicare while incarcerated who miss their Initial Enrollment Period while incarcerated; and (2) individuals who were enrolled in Medicare prior to their incarceration, who stop paying their Medicare premiums during incarceration (because Medicare does not cover services during incarceration), and have their Medicare coverage terminated. Both groups of individuals are required to enroll or re-enroll during the General Enrollment Period once they are no longer incarcerated and face a gap in coverage and penalty for late enrollment. This new Special Enrollment Period allows incarcerated individuals who become newly eligible for Medicare to enroll, and current Medicare beneficiaries who drop Medicare coverage while incarcerated to re-enroll, starting the day they’re released and up to 12 months later.
Individuals who lose Medicaid coverage: This Special Enrollment Period applies to Medicare-eligible individuals who lose Medicaid eligibility on or after January 1, 2023 or the end of the COVID-19 public health emergency (whichever is earlier). Under this Special Enrollment Period, Medicaid enrollees who lose Medicaid eligibility may sign up for Medicare without paying a late enrollment penalty, if they enroll at any time from the date they are notified that their Medicaid eligibility will be terminated up to 6 months after Medicaid eligibility ends. This new Special Enrollment Period was created in response to the expected disenrollment of many Medicaid enrollees who turned 65 during the public health emergency but did not lose their Medicaid coverage on account of requirements in the Families First Coronavirus Response Act. This law required Medicaid programs to keep people continuously enrolled through the end of the month in which the COVID-19 public health emergency ends, in exchange for enhanced federal funding. The public health emergency is currently in effect until January 11, 2023, and is expected to be extended again.
Other exceptional conditions: Under this rule, if an individual has an extenuating circumstance that caused them to miss a Medicare enrollment period, CMS can grant them a Special Enrollment Period on a case-by-case basis. The duration for this Special Enrollment Period can vary but will be no less than 6 months.
Examples of how these changes will affect Medicare coverage
Vanessa assists in making health care decisions on behalf of her mother. In August 2023, the governor in Vanessa’s state declares a state of emergency because of a hurricane affecting the county where she lives. Due to the impact of the hurricane, she is unable to help her mother, who lives in a state that was not affected by the hurricane, sign up for Medicare during her Initial Enrollment Period. This new policy will allow Vanessa to help her mom sign up for Medicare up to 6 months after the end of the emergency, reducing the gap between Medicare enrollment and coverage her mother would have otherwise faced, and eliminating any late-enrollment penalties that would otherwise have applied.
Robert, a 65-year-old man, is enrolled in Medicaid because of his low income. He does not have any dependent children or disabilities and is only eligible for Medicaid through the Affordable Care Act. He turned 65 in June 1, 2022 but did not enroll in Medicare because he was still enrolled in Medicaid. Prior to his 65th birthday, his state was supposed to send out a letter saying that he would no longer be eligible for Medicaid through the Affordable Care Act, but that he would be eligible for Medicare. However, his state doesn’t send the letter until after the public health emergency ends and Robert has missed his Initial Enrollment Period (March 2022-September 2022). This new rule will allow him to sign up for Medicare from the date he receives the letter notifying him of his Medicaid termination up to 6 months after his Medicaid benefits are terminated, without paying the late enrollment penalty or waiting until the next General Enrollment Period in 2024 to sign up.
4. The final rule extends Medicare coverage of immunosuppressive drugs for certain kidney transplant patients
Adults under the age of 65 with end-stage renal disease (ESRD) qualify for Medicare coverage on the basis of their ESRD diagnosis. Medicare covers all of their covered medical services, not just those related to their ESRD, including kidney transplants, which requires immunosuppressive drugs to prevent the body from rejecting the transplanted kidney. In 2022, there were more than 230,000 Medicare beneficiaries under age 65 with ESRD, including those who qualified on the basis of their ESRD only, representing about 3% of beneficiaries under age 65.
Policy prior to January 1, 2023
When a Medicare beneficiary under the age of 65 with ESRD receives a kidney transplant, their Medicare coverage has ended 36 months after the month in which they received their transplant, unless they’re eligible for Medicare on another basis, such as turning 65 or having a disability. Termination of Medicare coverage can lead to gaps in coverage and adverse health outcomes (e.g., organ rejection) for patients who have received a kidney transplant and continue to need immunosuppressive drugs beyond the point at which their Medicare coverage ends, unless they are able to obtain coverage through another source.
New policy
The final rule allows certain Medicare beneficiaries who have undergone a kidney transplant and would otherwise lose access to Medicare coverage beyond the 36-month post-transplant period to receive coverage only for immunosuppressive drugs after this point through a new Part B benefit referred to as the immunosuppressive drug benefit, or the Part B-ID benefit. Beneficiaries who qualify for the new Part B-ID benefit will not receive coverage for Medicare-covered items and services other than immunosuppressive drugs. The monthly premium for this benefit ($97.10 for 2023) will be less than the standard Part B premium ($164.90 in 2023) and will be higher for those with higher incomes. The standard Part B deductible will apply ($226 in 2023), after which beneficiaries will be responsible for 20% coinsurance for immunosuppressive drugs. There are no late enrollment penalties regardless of when an individual enrolls in the benefit. The rule also allows low-income beneficiaries who are eligible for the Part B-ID benefit to enroll in the Medicare Savings Programs if they qualify, which will help to alleviate the financial burden of costs associated with the new Part B-ID benefit.
If a beneficiary’s Medicare coverage ends before January 1, 2023, they can enroll in the new immunosuppressive drug benefit from October 1, 2022 through December 31, 2022 and coverage will start on January 1, 2023. If a beneficiary’s coverage ends on or after January 1, 2023, they can enroll at any time afterwards, and coverage will begin the month their Part A benefits ends.
Eligible beneficiaries: To be eligible for the new Part B-ID benefit, a beneficiary must be enrolled, or previously enrolled, in Medicare on the basis of their ESRD status, undergo a kidney transplant, and NOT be enrolled, or expect to be enrolled, in certain specific forms of health insurance or other programs that cover immunosuppressive drugs. For example, individuals enrolled in a group health plan, TRICARE for Life program, or a state plan that provides benefits for immunosuppressive drugs will not qualify for this new benefit. Additionally, beneficiaries who become eligible for Medicare based on other reasons (e.g., turning 65, having a disability) will not be eligible for this benefit because they have access to broader Medicare coverage.
Example of how this new Policy will affect Medicare coverage
Janet is a 35-year-old who became eligible for Medicare because she was diagnosed with ESRD. She received a kidney transplant on January 1, 2019. Her Medicare coverage terminated on January 1, 2022, 36 months after her transplant, because she did not meet other criteria to remain on Medicare. Since then, she has been uninsured and lacked coverage for her immunosuppressive drugs. Under this new policy, Janet will be able to sign up to receive Medicare coverage for her immunosuppressive drugs through this new Part B-ID benefit. She can sign up starting on October 1, 2022, and her coverage will begin January 1, 2023.
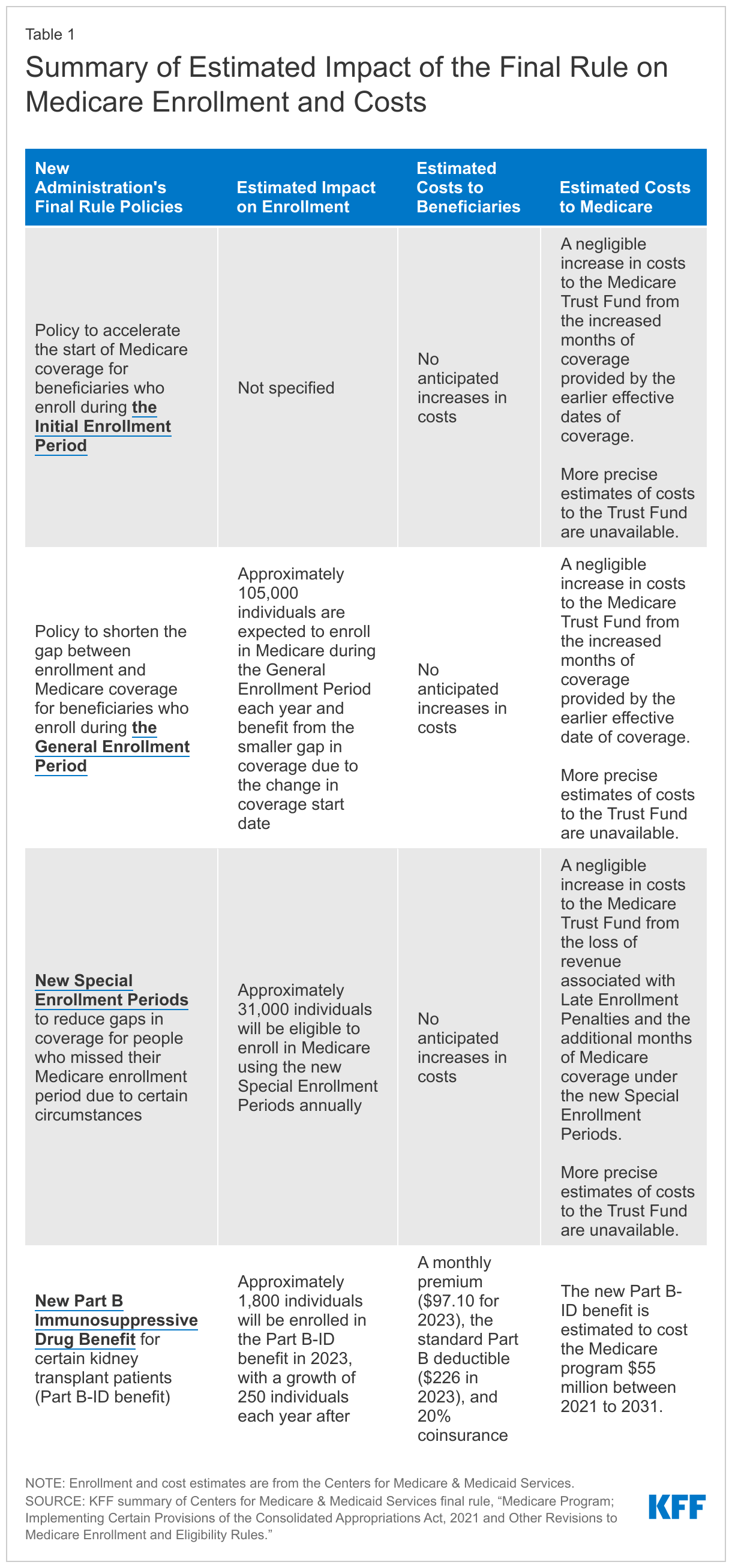
What is the estimated impact of the final rule on Medicare enrollment and costs?
These provisions of the final rule are expected to improve gaps in Medicare coverage with minimal impact on Medicare spending. Table 1 provides an overview of CMS’s estimates on the number of individuals impacted, costs to beneficiaries, and costs to Medicare resulting from these changes.
Medicaid is the nation’s single largest health insurance program, and Medicaid enrollment has grown since the start of the COVID-19 pandemic. Early in the pandemic marked what many described as one the most severe economic downturns in United States (US) history. The pandemic-induced recession looked different from historical recessions in a number of ways and was the first downturn with the Affordable Care Act’s (ACA) coverage expansions in place. Of the newly unemployed, many were projected to enroll in Medicaid or take up exchange-based health insurance coverage (though many also were temporarily furloughed and had their employer-sponsored health benefits continued). While the job market has recovered substantially, there have been large layoffs recently at high-profile companies and there are fears that another recession could be on the horizon. This brief reviews what we know about Medicaid enrollment changes during economic downturns, examines unemployment-linked Medicaid enrollments early on in the COVID-19 pandemic, and considers the implications for the unwinding of the national public health emergency (PHE).
How does Medicaid enrollment change during economic downturns?
Medicaid enrollment typically increases during economic downturns. Medicaid is a counter-cyclical program, meaning that more people become eligible and enroll during economic downturns; at the same time, states may face declines in revenues that make it difficult to fund the state share of funding for the program. Historically, increases in the national unemployment rate have been associated with increases in Medicaid enrollment. Medicaid enrollment increased sharply following both the 2001-2002 recession and the Great Recession, and enrollment growth has been a primary driver of total Medicaid spending over the past decade. In the 2007-2009 Great Recession, before the passage of the ACA and expanded Medicaid eligibility for low-income adults, Medicaid enrollment increased by 21% (2.6 million), from 6.8% in 2007 to 8.1% in 2009 among working aged (19-64) adults. Further, rising unemployment during the Great Recession was associated with declining private coverage and increased Medicaid enrollment among persons with private coverage in the previous year.
During the Great Recession, Medicaid enrollment was concentrated in states with more expansive eligibility guidelines based on an analysis that created an index and relied on state upper income limits and categorical eligibility rules. States with more expansive guidelines also experienced smaller increases in cost-related barriers to care associated with rising unemployment in the Great Recession because a larger share of people losing private coverage due to job loss were able to transition to Medicaid. Prior to the implementation of the ACA Medicaid expansion, Medicaid eligibility levels for parents were low (national median eligibility level for parents was 64% of the federal poverty level (FPL) in 2013) and only a small group of states had coverage for childless adults through Section 1115 waivers. Unlike the recent pandemic-induced recession, the MOE requirements tied to the fiscal relief during the Great Recession did not include a continuous enrollment requirement, though states could not make eligibility or enrollment processes more restrictive. The Great Recession also predated the passage of the ACA, which expanded Medicaid eligibility and established tax credits for people buying individual insurance through the ACA marketplace.
How did the ACA and expanding Medicaid make it easier for the unemployed to enroll in Medicaid?
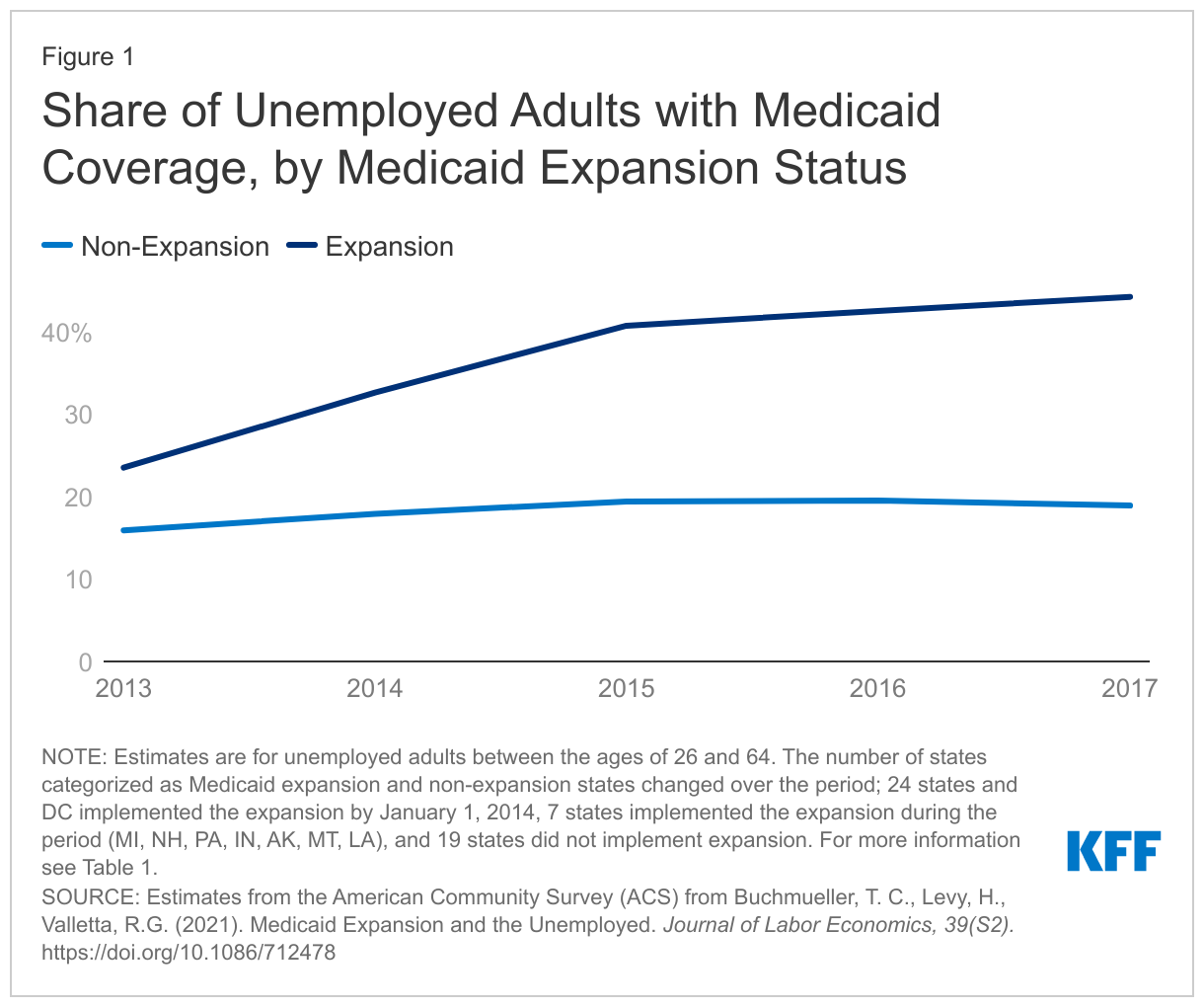
The ACA created new coverage pathways in Medicaid and streamlined Medicaid enrollment processes, making it easier for the unemployed to enroll in Medicaid.State adoption of the ACA’s Medicaid expansion expanded Medicaid eligibility for nearly all adults up to 138% FPL ($23,030 for a family of three in 2022). The expanded eligibility guidelines made it easier for more people who lost their jobs to qualify for Medicaid because categorical requirements such as parental status were no longer a part of eligibility determination. Following the ACA’s Medicaid expansion, Medicaid enrollment among the unemployed in states that adopted Medicaid expansion increased from 23.5% in 2013 to 44.2% in 2017 (Figure 1). After states expanded Medicaid, becoming unemployed was less of a risk factor for becoming uninsured. According to the Bureau of Labor Statistics, an individual is classified as unemployed if they are currently jobless but are available to work and have actively looked for work in the past 4 weeks.
How did Medicaid enrollment change early in the COVID-19 pandemic?
Medicaid enrollment has increased to record highs during the current COVID-19 PHE. To provide broad fiscal relief to states while preventing coverage losses during the pandemic, Congress passed the Families First Coronavirus Response Act (FFCRA) early in the pandemic to provide a 6.2 percentage point increase in the federal Medicaid match rate (“FMAP”) for states that meet certain “maintenance of eligibility” (MOE) requirements, including a continuous enrollment requirement. The COVID-19 recession had different implications for Medicaid enrollment compared to the Great Recession due to its unique health implications, the MOE continuous enrollment requirement, and the passage of the ACA. While Medicaid enrollment is higher in states that have expanded Medicaid under the ACA, the continuous enrollment requirement during the PHE has resulted in substantial enrollment increases in all states.
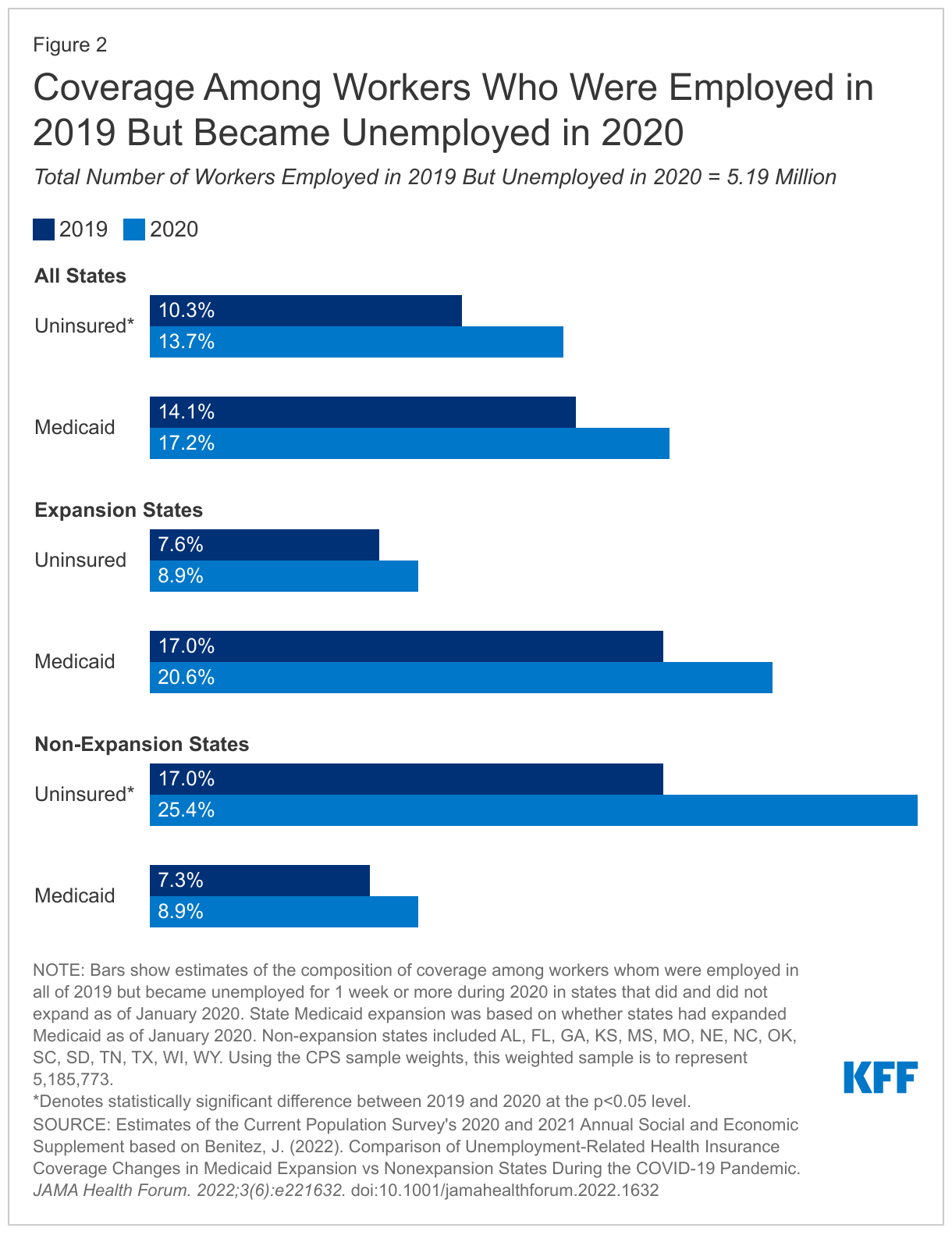
Medicaid enrollment increases were concentrated in states with expanded eligibility guidelines in place at the start of the pandemic. An analysis of the Current Population Survey’s Annual Social and Economic Supplement (CPS ASEC) examined coverage trends among adult workers that were employed in 2019 and became newly unemployed in 2020, the first year of the pandemic, compared to workers who were employed in 2019 and remained employed in 2020. Among newly unemployed workers, Medicaid enrollment increased 3.1 percentage points overall, with a larger increase in expansion states (from 17.0% in 2019 to 20.6% in 2020) compared to non-expansion states (from 7.3% in 2019 to 8.9% in 2020) (Figure 2). In addition, uninsurance increased by 1.3 percentage points (from 7.6% in 2019 to 8.9% in 2020) in Medicaid expansion states but increased by 8.4 percentage points (from 17.0% in 2019 to 25.4% in 2020) in non-expansion states among newly unemployed workers. Workers that became unemployed—including temporary layoffs and furloughs—in Medicaid expansion states during the pandemic year were 70% less likely to become uninsured compared to workers that became unemployed in states that did not expand Medicaid.
What to watch looking ahead?
While the PHE end date remains uncertain, it is expected to have significant implications for Medicaid enrollment. Following the end of the PHE and continuous enrollment requirement, Medicaid redeterminations will resume, and individuals may lose Medicaid coverage if they are no longer eligible or are unable to navigate administrative barriers despite remaining eligible. Some individuals who gained Medicaid when they became unemployed may have gained new employment and now have income too high to qualify for Medicaid. They may have access to employer-based health insurance (or already be enrolled in such coverage), or now be eligible for ACA Marketplace coverage with premium assistance. Other individuals may have regained employment but may still qualify for Medicaid if they are employed in a low-wage job. Some individuals may also no longer be in the laborforce because of the longer-run effects of COVID-19 infections like long-COVID as well as additional caretaking or childcare responsibilities. To avoid becoming uninsured, individuals will need to transition to other available coverage if they are no longer eligible for Medicaid or renew Medicaid coverage.
While state fiscal conditions have vastly improved since the pandemic began, recent economic developments have raised concerns and heightened uncertainty. States’ longer-term fiscal outlooks remain uncertain due to recent economic turmoil, including rising inflation, the Russian invasion of Ukraine, supply chain issues, along with tapering federal fiscal relief. There have also been warning signs signaling the US could be headed for another recession. The findings described here suggest, in the event of future employment losses, Medicaid can serve as an important safety net to prevent coverage loss following unemployment, and that the safety net is stronger in those states that have expanded Medicaid under the ACA.
Joseph Benitez (@j_a_benitez) is currently a non-residential visiting scholar working with KFF’s Program on Medicaid and the Uninsured.
A new KFF analysis finds that the President’s Emergency Plan for AIDS Relief (PEPFAR), the U.S. global HIV/AIDS response and the largest commitment by any nation to address a single disease in history, is associated with improvements in key economic and educational outcomes in countries that received PEPFAR support. Specifically, the program may have helped to grow per capita GDP and reduce the shares of girls and boys who are out of school.
PEPFAR may have a direct economic stimulus effect. The aid program was associated with a 2.1 percentage point increase in the GDP per capita growth rate over the study period, compared to what would have been expected in the absence of the program. The program was also associated with a 9.2 percentage point decline in primary school-age girls not in school. The share of boys of primary school age who were out of school also declined by 8 percentage points in PEPFAR countries.
These findings contribute to existing evidence that PEPFAR, which was not designed as an economic or educational program, has a positive impact on non-health outcomes. The findings also suggest that investments in vertical health programs—those focused on one issue or disease—can have knock-on effects that support broader economic development goals and improvements, which is vital in an era of constrained aid budgets.
For the analysis, researchers studied a data set of 157 low- and middle- income countries. The group included 90 countries that had received PEPFAR support and 67 counties that had received minimal or no PEPFAR support, between 2004 and 2018.
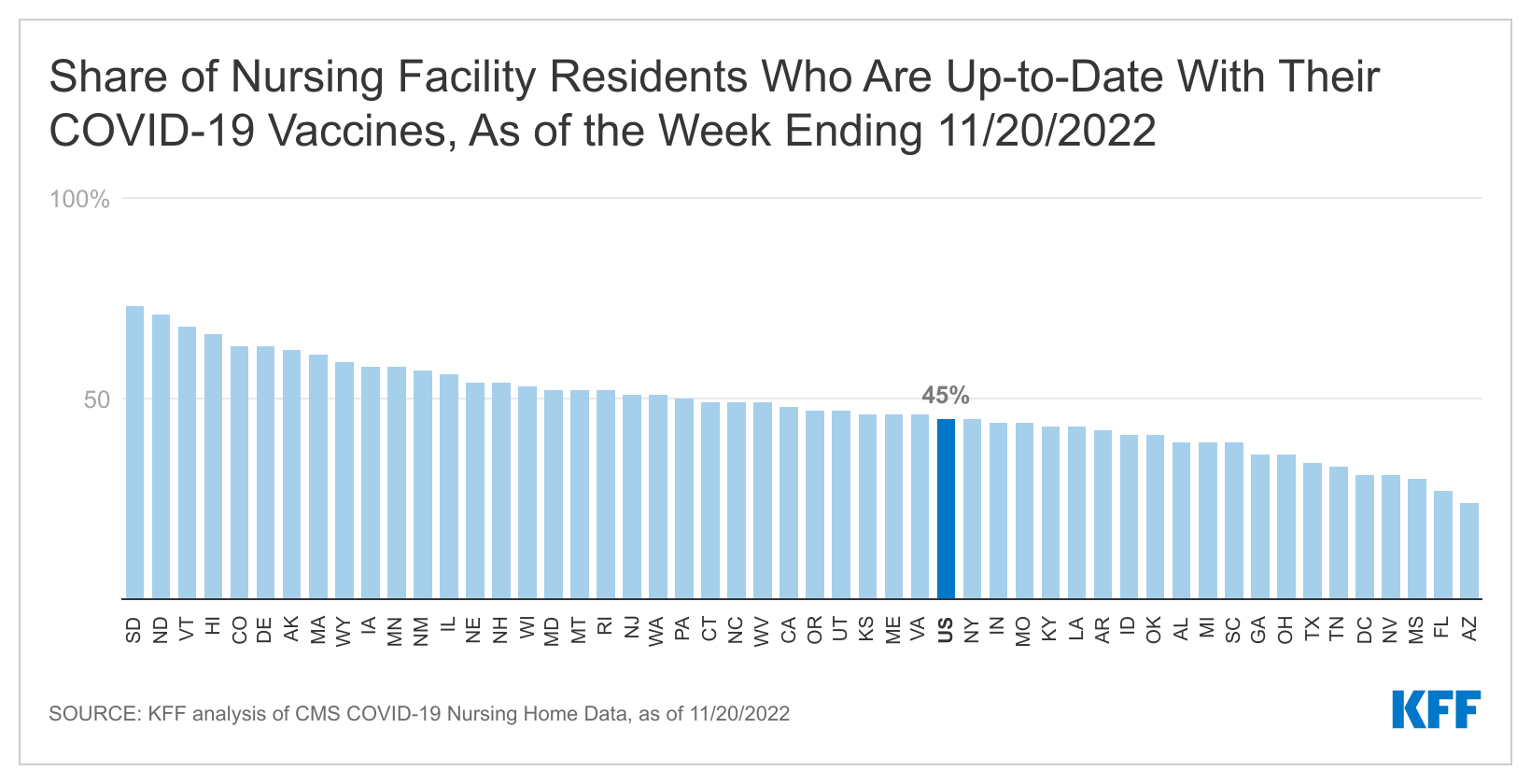
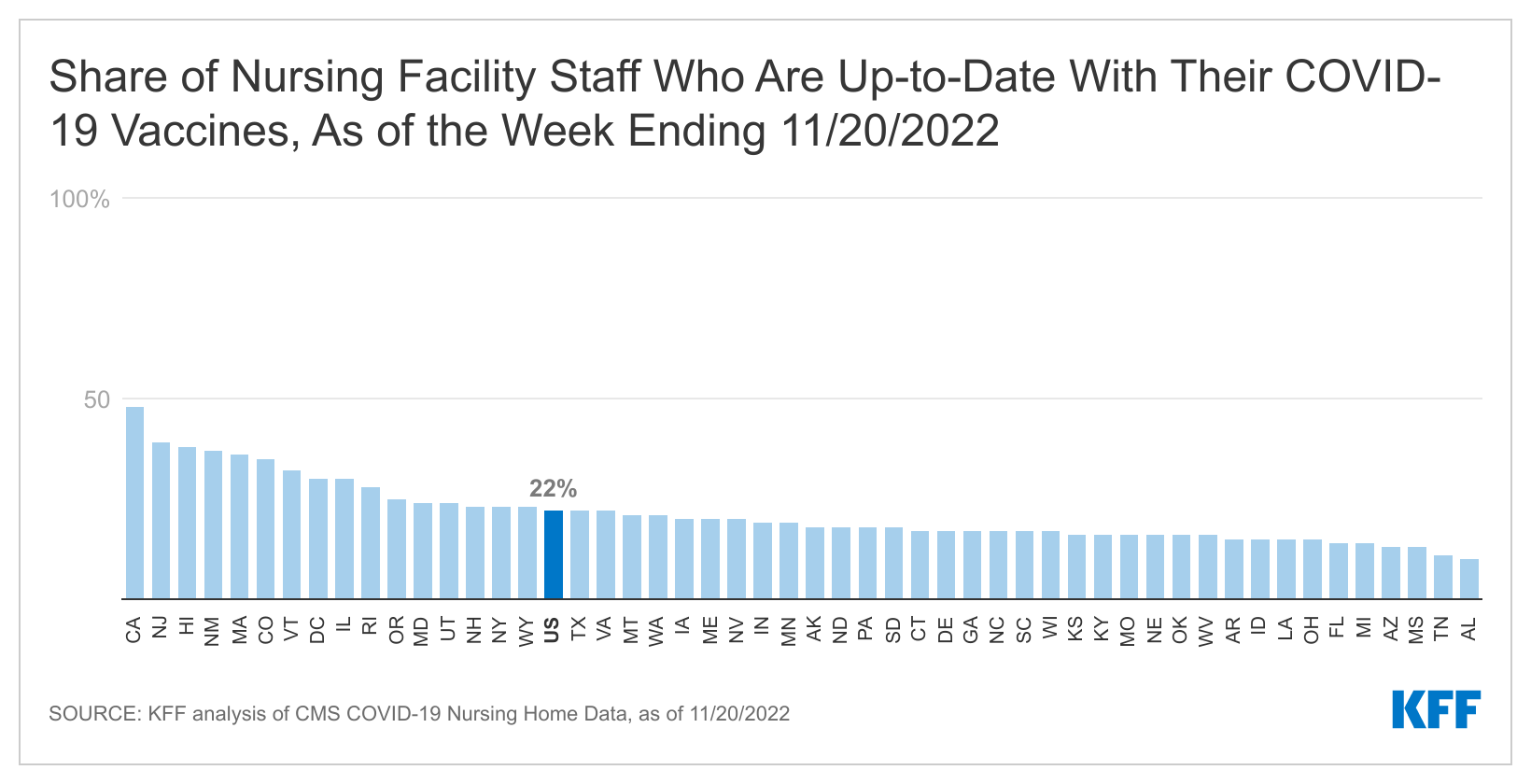
As winter approaches, a new KFF analysis finds that less than half (45%) of all nursing facility residents and less than a quarter of staff (22%) are up to date with their COVID-19 vaccinations. That is a sharp drop from the 87 percent of nursing facility residents and staff who completed their primary vaccination series.
The U.S. Centers for Disease Control and Prevention (CDC) now defines being up to date as “having received a bivalent booster or having received a final shot of the original vaccines less than two months ago.”
Federal vaccine clinics and health care worker vaccine mandates contributed to high initial vaccination rates among nursing facility residents and staff. But without ongoing federal initiatives, fewer people may stay up to date with their vaccines.
The share of residents who are up to date ranged from 73 percent in South Dakota to 24 percent in Arizona. Among nursing home staff, the share ranged from 48 percent in California to 10 percent in Alabama.
PEPFAR, the U.S. global HIV program, is the largest commitment by any nation to address a single disease in history. In addition to impacts on HIV, studies have shown that PEPFAR has had broader health impacts, including in the area of maternal and child health. Whether it has also had impacts beyond health, such as in broader economic and educational gains, is less known but could have important implications for the future of the program. If found to support these other areas, it suggests that investments in a vertical health program can have knock-on effects that support broader economic development goals and improvements, a finding that has particular relevance in an era of constrained aid budgets. Here, we examine PEPFAR’s association with five non-health outcomes: the GDP growth rate per capita; the share of girls and share of boys, respectively, who are out of school; and female and male employment rates. We find that:
PEPFAR was associated with significant, positive improvement in three of the five measures assessed over the 2004-2018 period, while findings for the other two outcomes were inconclusive.
PEPFAR countries experienced an increase in the GDP per capita growth rate that was greater than what would otherwise be expected in PEPFAR’s absence. Specifically, the growth rate was 2.1 percentage points higher over the period. This effect was greater in countries with “Country Operational Plans,” which engage in more intensive planning and generally have greater financial investment from PEPFAR.
In addition, the share of girls of primary school age who were not in school declined significantly over the period, falling by more than 9 percentage points, an effect that was greater in COP and high investment countries. This result was also found for boys – the share out of school fell by 8 percentage points.
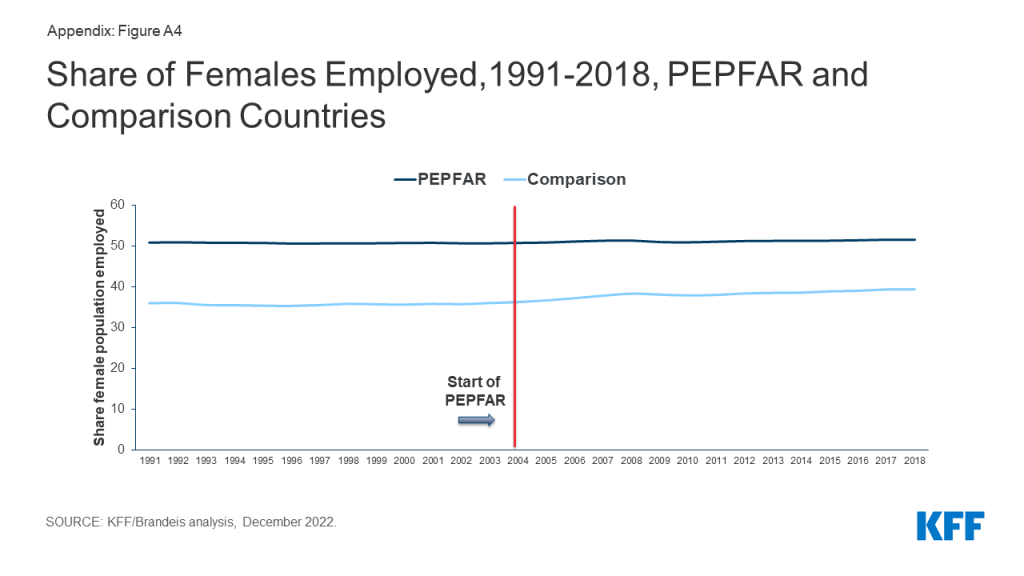
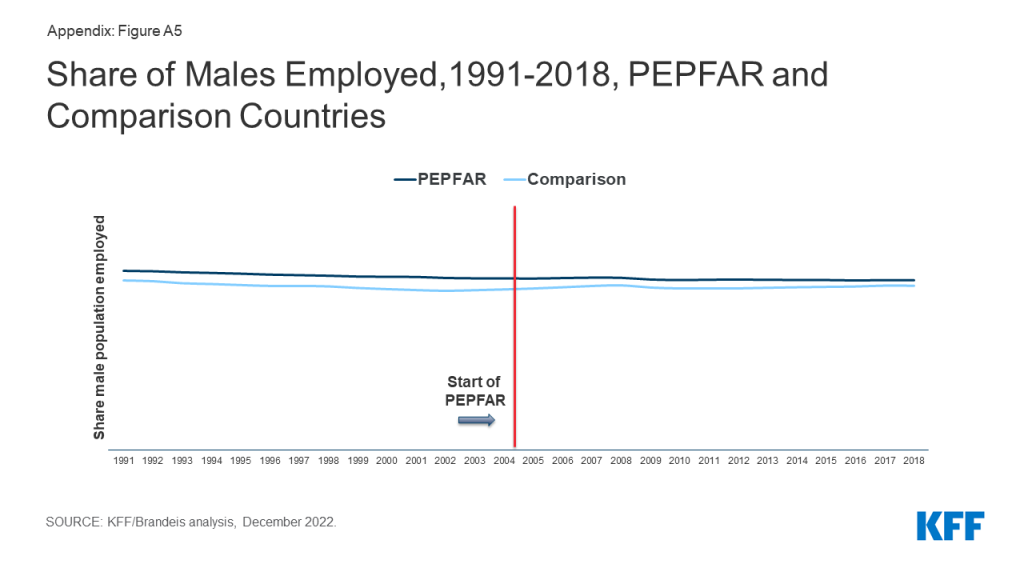
The was no significant effect detected on labor force participation for either females or males over the period.
Overall, these findings further contribute to the evidence base that PEPFAR’s investments have been correlated with positive, non-health outcomes.
Introduction
PEPFAR is the largest commitment by any nation to address a single disease. Since its launch in 2003, the U.S. government has provided close to $90 billion in bilateral assistance to address HIV in low and middle income countries (LMICs), and PEPFAR has been credited with saving millions of lives and helping to change the trajectory of the global HIV epidemic. In a prior analysis, we found that PEPFAR has contributed to large, significant reductions in all-cause mortality, suggesting a mortality effect beyond HIV.1 More recently, we found that PEPFAR has had significant, positive, health spillover effects in the area of maternal and child health, including reductions in maternal and child mortality and increases in childhood immunization rates.2
Whether PEPFAR has also had any spillover effects beyond health, however, has been less studied, and, while such an impact is plausible, it is not a given. On the one hand, PEPFAR, as a vertical, disease-specific initiative, was not designed to be an economic or educational program, and its goals are HIV-focused and targeted. On the other, the program has recognized that providing economic and educational support, such as in its DREAMS program focused on adolescent girls and young women, is important for addressing the drivers of the HIV epidemic (although its direct support for such interventions is limited and only began after 2014).3,4 In addition, external aid may also act as a direct economic stimulus in countries, impacting their GDP.5 More broadly, studies have found that health investments are correlated with educational attainment and economic growth, including, for example, by enabling children to stay in school longer and by supporting adults to join and/or remain in the labor force.6In this analysis, we seek to assess whether PEPFAR has had impacts beyond health by examining changes in five economic and educational outcomes in PEPFAR countries: the GDP growth rate; the share of girls and share of boys, respectively, who are out of school; and female and male employment rates (see Box). If PEPFAR is found to support these other areas, it suggests that investments in a vertical health program can have knock-on effects that support broader economic and development goals and improvements, a finding that has particular relevance in an era of constrained aid budgets.
Box: Outcome Measures
1. GDP per capita growth (annual % change)
2. Share of girls out of school
3. Share of boys out of school
4. Female employment rate
5. Male employment rate
The existing literature on PEPFAR’s impact in these areas is limited though there is evidence of such an effect. In a study of 21 countries in sub-Saharan Africa, including 10 PEPFAR focus countries and 11 control countries, Wagner, Barofsky, and Sood found that PEPFAR was associated with a significant increase in male employment, though not with female employment, between 2004 and 2010.7 Kim and Whang, in a study of 15 PEPFAR focus and 121 control countries, found that PEPFAR was associated with increases in the GDP growth rate in focus countries between 2003 and 2009.8 Finally, an analysis by the Bipartisan Policy Center found that GDP per capita and average output per worker were higher in countries with greater PEPFAR investment compared to countries with low or no investment between 2004 and 2016.9 Other studies have looked more generally at the relationship between HIV interventions, particularly antiretroviral therapy, and economic outcomes, though not at PEPFAR’s role specifically, and also found positive correlations.10 No studies were identified that have examined the relationship between PEPFAR and educational attainment, although several have more generally assessed the impact of HIV on the education of children, demonstrating the epidemic’s deleterious effects.11
For the current analysis, we look at a larger set of countries and over a longer period of time than the prior analyses identified. We use a difference-in-difference quasi-experimental design to analyze the change in each of these outcomes in 90 PEPFAR countries between 2004, the first year in which PEPFAR funding began, and 2018, compared to a comparison group of 67 low- and middle- income countries (See methodology for more detail). We tested several different model specifications. Our final model controls for numerous baseline variables that may also be expected to influence these outcomes and which help to make the PEPFAR and non-PEPFAR country groups more comparable. Despite the strengths of the difference-in-difference model design, however, it is still possible that there may be other, unobservable ways in which comparison countries differed from PEPFAR countries which could account for our results. In addition, we are unable to determine causality, which could operate in either direction (e.g., better health results in greater economic growth or greater economic growth improves health), as has been noted in the broader health economics literature.12
Findings
We find that PEPFAR was positively associated with three of the five economic and educational outcomes examined, while its association with the remaining two is inconclusive:
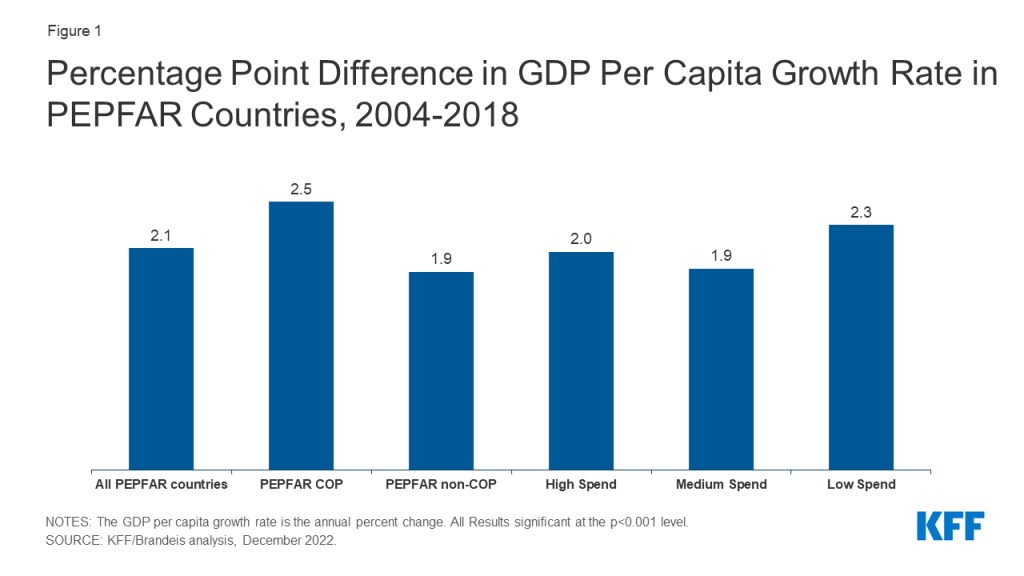
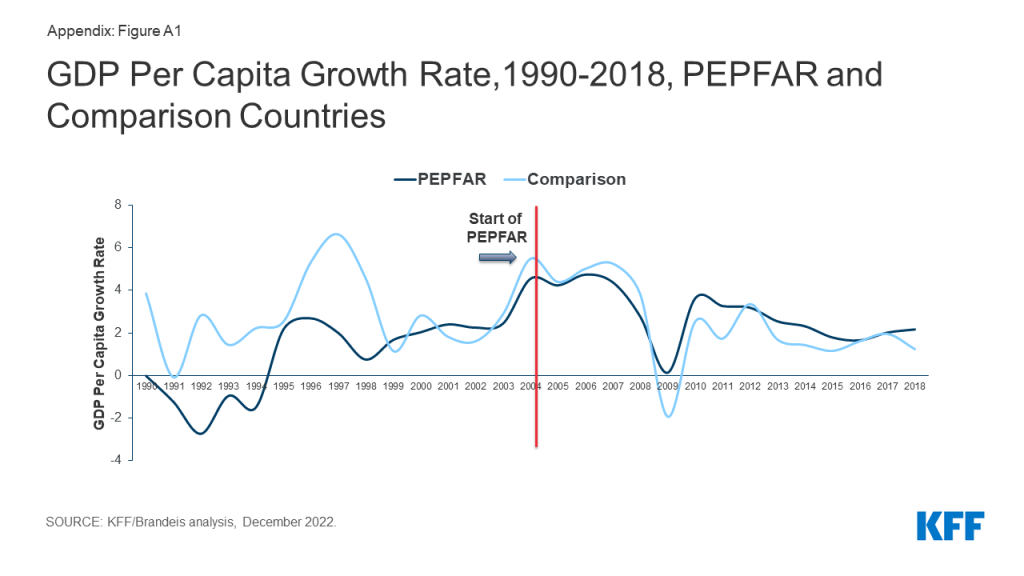
Between 2004 and 2018, PEPFAR was associated with a 2.1 percentage point increase in the GDP growth rate per capita over the period, compared to what would have been expected in the absence of the program. This percentage point change translates into a 45.7% increase in the GDP per capita growth rate. Looking at the broader trend, prior to PEPFAR’s initiation, the GDP per capita growth rate in comparison countries was generally higher than the rate in PEPFAR countries. This pattern began to change just a few years after PEPFAR’s initiation, near the time of the 2008 global financial crisis, when the growth rate in comparison countries fell below that of PEPFAR countries. While it is possible that the financial crisis affected PEPFAR and comparison countries differently, our model is designed to control for this possibility. We also examined the period before 1999, given the volatility in the GDP growth rate in both PEPFAR and comparison countries, which appears to be influenced by a subset of outlier countries; after removing these countries from our analysis, the results remain significant (See Figure 1, Tables 5-6, and Appendix).
Figure 1: Percentage Point Difference in GDP Per Capita Growth Rate in PEPFAR Countries, 2004-2018
PEPFAR’s estimated effect on the GDP growth rate per capita over the period was even greater in “COP” countries. The increase in the GDP growth rate per capita was 2.5 percentage points in COP countries, or a 61.5% increase over the period. These countries engage in more intensive planning and programming by preparing an annual PEPFAR Country Operational Plan (COP), compared to other PEPFAR countries, and generally receive greater funding; indeed, countries with more intensive spending saw greater change than their comparisons (See Figure 1 and Tables 5-6).
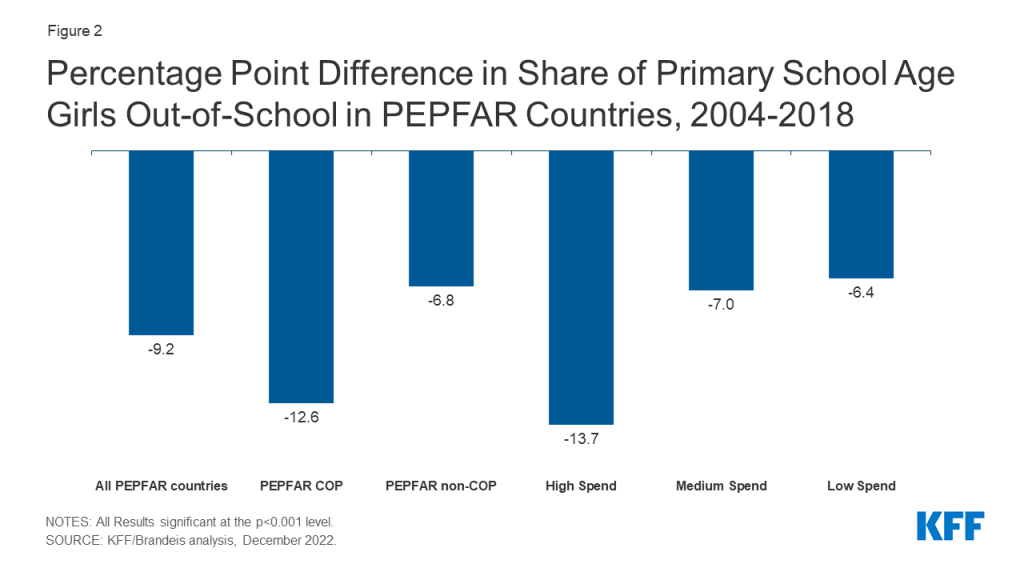
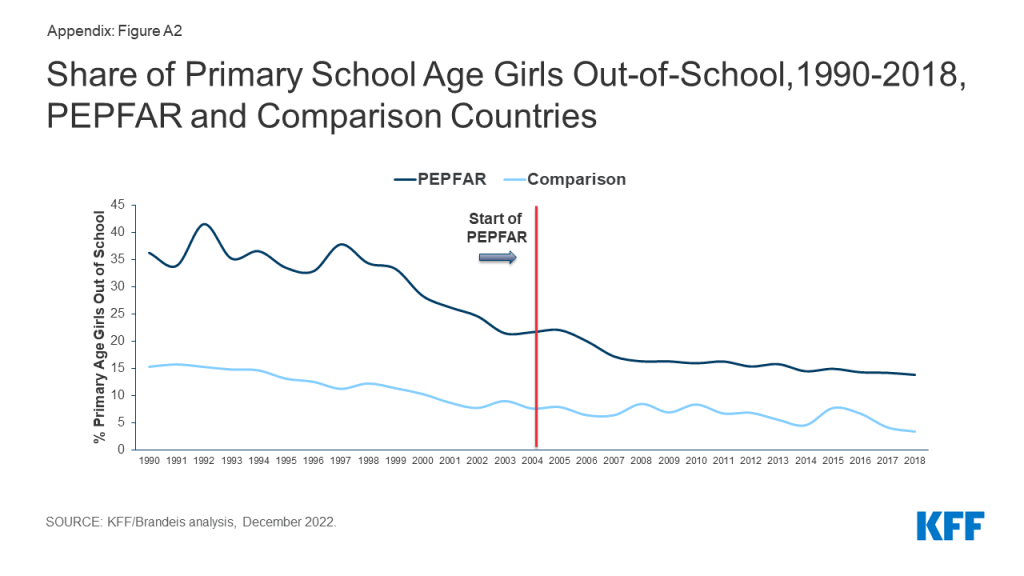
PEPFAR was also associated with a decline of 9.2 percentage points in the out-of-school rate for girls of primary school over the period. This represents a decline in the share of girls not in school of 42.4%. This effect was strongest in COP countries and in countries with greater PEPFAR investment. The large time trend shows that, prior to PEPFAR, the share of girls out of school was much higher in PEPFAR countries, relative to comparison countries. Following the introduction of the program, these rates began to converge (see Figure 2, Tables 5-6, and Appendix).
Figure 2: Percentage Point Difference in Share of Primary School Age Girls Out-of-School in PEPFAR Countries, 2004-2018
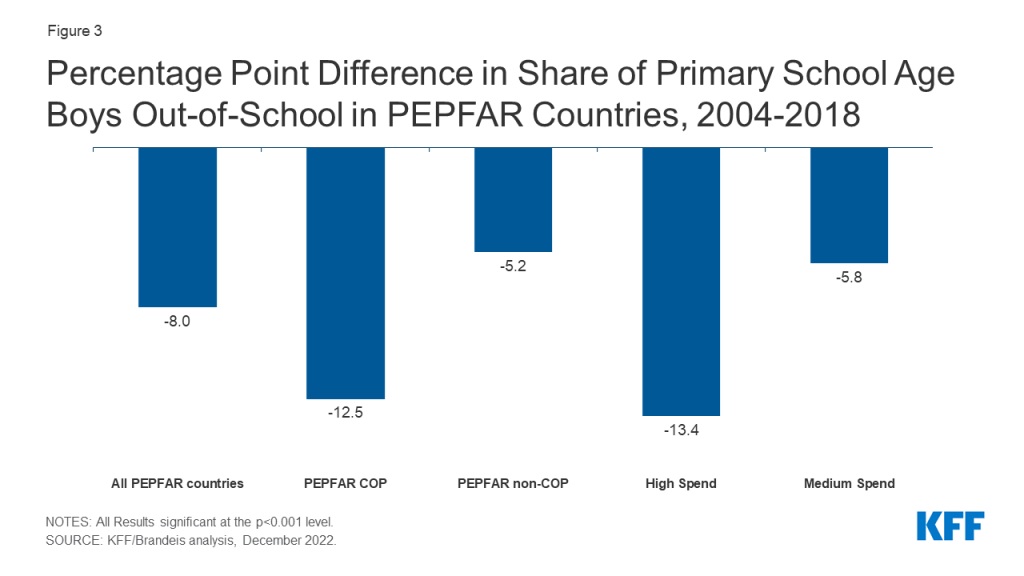
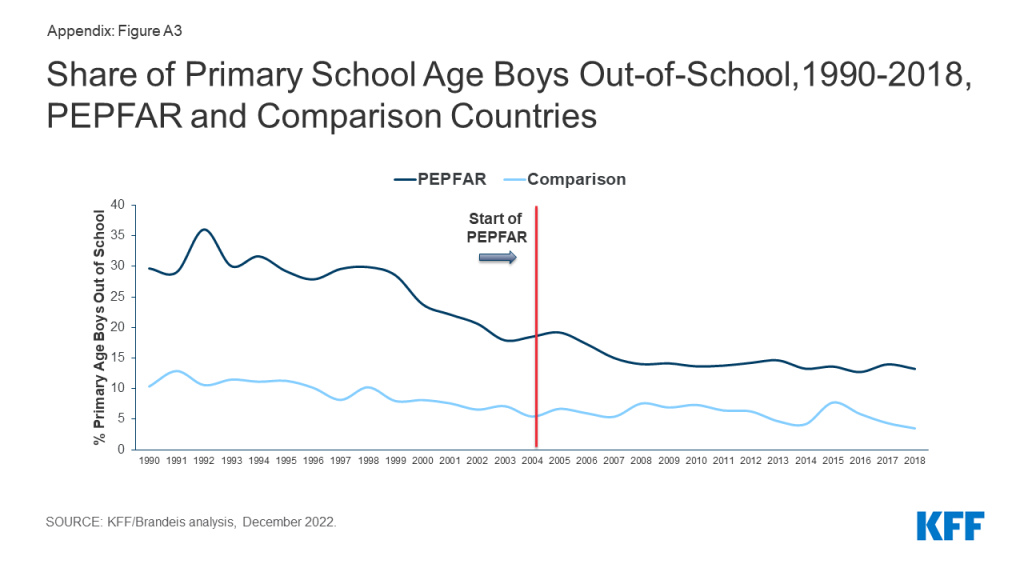
Similarly, the share of boys of primary school age who were out-of-school also declined in PEPFAR countries, by 8 percentage points relative to what would be expected. This represents a decline of 43.1%. As with girls, the effect was stronger in COP countries and in countries with greater PEPFAR investment and the broader trend was similar to that of girls (see Figure 3, Tables 5-6, and Appendix).
Figure 3: Percentage Point Difference in Share of Primary School Age Boys Out-of-School in PEPFAR Countries, 2004-2018
By contrast, PEPFAR’s effect on employment rates for both females and males is inconclusive. Our findings for employment rates for females and males, respectively, were not statistically significant (we only report final results significant at the p < 0.001 level). More generally, the rates of employment for both females and males were essentially flat over the entire 1990-2018 period for PEPFAR and comparison countries (and higher for female employment in PEPFAR countries even before PEPFAR’s initiation). (see Tables 5-6 and Appendix).
Implications
Our findings confirm the prior literature demonstrating a relationship between PEPFAR and economic growth.13 We show that these impacts are most pronounced in COP countries, which also receive the highest levels of PEPFAR investment. These effects could be due to the direct economic stimulus of PEPFAR assistance on low and middle income economies; in general, PEPFAR funding as a share of GDP in COP countries was under one percent in most years, though in some, it ranged between 1-2%.14 We also demonstrate the impacts of PEPFAR on two measures not previously reported in the literature – a decrease in the share of girls and of boys, of primary school age, who were out-of-school. Again, PEPFAR impacts were greatest in COP countries. We do not, however, find evidence of a relationship between PEPFAR and rates of employment for females and males (our findings were not significant). While increases in both GDP growth rates and educational engagement may be expected to result in increased labor participation, such impacts may take many years before they become evident or may be influenced by other factors. Still, this area warrants further exploration.
While our findings regarding GDP growth rates per capita and educational engagement are strong, and despite the strengths of the difference-in-difference model design, it is possible that there may be other, unobservable ways in which comparison countries differed from PEPFAR countries, which could account for our results. As mentioned above, for example, it is possible that the financial crisis affected PEPFAR and comparison countries differently, although our model design attempts to control for this possibility. In addition, it is possible that patterns within a subset of countries could be driving the overall trend. Future analysis could seek to explore other factors that may contribute to these findings as well as the country-level effects for these measures. It could also further explore the different pathways that may help to explain the relationships between PEPFAR support and improved economic and educational outcomes.
Overall, these findings further contribute to the evidence base that PEPFAR’s investments have also been correlated with positive, non-health outcomes. Given tight budgets and ongoing questions about the future trajectories of global health efforts more broadly and PEPFAR specifically, such findings indicate that a large, vertical health program which has been shown to have significant health impacts, may also contribute to broader economic and development goals.
Methods
We used a difference-in-difference15 , quasi-experimental design to estimate a “treatment effect” (PEPFAR), compared to a group without the intervention (the counterfactual). The difference-in-difference design compares the before and after change in outcomes for the treatment group to the before and after change in outcomes for the comparison group. We constructed a panel data set for 157 low- and middle- income countries between 1990 and 2018. Our PEPFAR group included 90 countries that had received PEPFAR support (between 2004 and 2018). Our comparison group included 67 low- and middle-income countries that had not received any PEPFAR support or had received minimal PEPFAR support (<$1M over the period or <$.05 per capita) between 2004 and 2018. The pre-intervention period was 1990 to 2003 and post intervention period was 2004 to 2018. Data on PEPFAR spending by country were obtained from the U.S. government’s https://foreignassistance.gov/ database and represent U.S. fiscal year disbursements; data for other measures were obtained from the World Bank’s World Development Indicator database and the Institute for Health Metrics and Evaluation (IHME) database, unless otherwise noted. Our outcomes of interest, their definitions, and sources are listed in Table 1. Baseline variables (for 2004) and sources are listed in Table 2 and model specifications examined in Table 3. Table 4 provides baseline means for all outcome variables. Final results are presented in Tables 5-6.
Table 1: Outcome Variables
Variable
Definition
1. GDP per capita growth (annual %)
Annual percentage growth rate of GDP per capita based on constant local currency. GDP per capita is gross domestic product divided by midyear population.
2. Children out of school, female (% of female primary school age)
Percentage of female primary-school-age children who are not enrolled in primary or secondary school.
3. Children out of school, male (% of male primary school age)
Percentage of male primary-school-age children who are not enrolled in primary or secondary school.
4. Employment to population ratio, 15+, female (%)
Proportion of a country’s female population that is employed, defined as persons of working age who, during a short reference period, were engaged in any activity to produce goods or provide services for pay or profit, whether at work during the reference period (i.e. who worked in a job for at least one hour) or not at work due to temporary absence from a job, or to working-time arrangements.
5. Employment to population ratio, 15+, male (%)
Proportion of a country’s male population that is employed, defined as persons of working age who, during a short reference period, were engaged in any activity to produce goods or provide services for pay or profit, whether at work during the reference period (i.e. who worked in a job for at least one hour) or not at work due to temporary absence from a job, or to working-time arrangements.
United Nations, Department of Economic and Social Affairs, Population Division (2019). World Population Prospects 2019, Online Edition. Rev, https://population.un.org/wpp/
We explored several difference-in-difference model specifications, compared to an unadjusted model (see Table 3). Each specification controlled for numerous baseline variables that may be expected to influence the outcome of interest to help make the non-PEPFAR group more comparable to the PEPFAR group. Baseline means for outcome variables are provided in Table 4. Final results are presented in Tables 5-6 and are from model specification #3, and significance is only reported in the analysis for results at the p<0.001 level. The appendix provides trend data for each outcome variable in PEPFAR and comparison countries over the full study period.–
Table 3: Model Specifications
Model
Difference-in Difference Specification
1
Unadjusted model
2
Includes baseline variables 1-9
3
Includes baseline variables 1-11
4
Includes baseline variables 1-9 and yearly per capita donor spending on health (non-PEPFAR) by all donors
Despite the strengths of the difference-in-difference design, there are limitations to this approach. While we adjusted for numerous baseline factors that could be correlated with our outcomes of interest, there may be other, unobservable factors that are not captured here. Similarly, while our baseline factors are also intended to adjust for selection bias, there may be other ways in which comparison countries differed from PEPFAR countries (and factors which influenced which countries received PEPFAR support), which could bias the estimates.–
Table 4: Baseline Means, PEPFAR Countries, 2004
Outcome Measure
All PEPFAR countries
COP countries
Non-COP countries
High spending
Medium spending
Low spending
GDP Per Capita growth (% change)
4.5
4.1
4.8
3.3
5.6
4.7
Primary Age Females Out of School (%)
21.7
21.3
21.9
26.0
15.5
26.0
Primary Age Males Out of School (%)
18.5
19.1
18.1
23.7
12.5
20.9
Female Employment (%)
50.7
56.2
47.7
55.0
50.8
46.1
Male Employment (%)
69.8
70.9
69.2
70.2
68.1
71.1
Table 5: Estimates of PEPFAR’s Impact by Measure, 2004-2018
(Percentage point difference-in-difference from means; standard errors in parentheses)
Outcome Measure
All PEPFAR countries
COP countries
Non-COP countries
High spending
Medium spending
Low spending
GDP per capita growth (% change)
2.072***
2.504***
1.853***
2.037***
1.882***
2.288***
(0.434)
(0.615)
(0.499)
(0.582)
(0.569)
(0.569)
Primary Age Females Out of School (%)
-9.185***
-12.580***
-6.781***
-13.663***
-6.969***
-6.352***
(1.143)
(1.304)
(1.134)
(1.439)
(1.437)
(1.479)
Primary Age Males Out of School (%)
-7.962***
-12.508***
-5.196***
-13.374***
-5.766***
-4.336**
(1.031)
(1.171)
(1.029)
(1.302)
(1.301)
(1.338)
Female Employment (%)
-2.416*
-3.313**
-1.952
-1.763
-3.601**
-1.777
(0.991)
(1.102)
(1.013)
(1.298)
(1.258)
(1.284)
Male Employment (%)
-1.657**
-1.650*
-1.660*
-1.180
-2.582**
-1.125
(0.625)
(0.644)
(0.694)
(0.814)
(0.788)
(0.805)
***p < 0.001 **p < 0.01 *p < 0.05
Table 6: Estimates of PEPFAR’s Impact by Measure, 2004-2018(Percent change from Mean)
Outcome Measure
All PEPFAR countries
COP countries
Non-COP countries
High spending
Medium spending
Low spending
GDP Per Capita (% change)
45.7%***
61.5%***
38.7%***
62.1%***
33.4%***
49.1%***
Primary Age Females Out of School (%)
-42.4%***
-59.2%***
-31.0%***
-52.5%***
-44.9%***
-24.5%***
Primary Age Males Out of School (%)
-43.1%***
-65.3%***
-28.7%***
-56.3%***
-46.1%***
-20.8%**
Female Employment (%)
-4.8%*
-5.9%**
-4.1%
-3.2%
-7.1%**
-3.9%
Male Employment (%)
-2.4%**
-2.3%*
-2.4%*
-1.7%
-3.8%**
-1.6%
***p < 0.001 **p < 0.01 *p < 0.05
Jen Kates is with KFF. William Crown, Allyala Nandakumar, Gary Gaumer and Dhwani Hariharan are with Brandeis University.
Appendix
Figure A1: GDP Per Capita Growth Rate,1990-2018, PEPFAR and Comparison CountriesFigure A2: Share of Primary School Age Girls Out-of-School,1990-2018, PEPFAR and Comparison CountriesFigure A3: Share of Primary School Age Boys Out-of-School,1990-2018, PEPFAR and Comparison CountriesFigure A4: Share of Females Employed,1991-2018, PEPFAR and Comparison CountriesFigure A5: Share of Males Employed,1991-2018, PEPFAR and Comparison Countries
Wagner Z, Barofsky J, Sood N, “PEPFAR funding associated with an increase in employment among males in ten sub-Saharan African countries,” Health Affairs, 2015 Jun, 34(6): 946-953. ↩︎
See, for example: Remes J, Wilson M, Ramdorai A, How investing in health has a significant economic payoff for developing economies, Brookings, July 2020, available at: https://www.brookings.edu/blog/future-development/2020/07/21/how-investing-in-health-has-a-significant-economic-payoff-for-developing-economies/; World Bank, Human Capital Project, available at: https://www.worldbank.org/en/publication/human-capital; Piabuo S, Tieguhong J, “Health expenditure and economic growth – a review of the literature and an analysis between the economic community for central African states (CEMAC) and selected African countries,” Health Econ Rev, 2017 Dec, 7(23); Vogl T, Education and health in developing economies, Working Papers 1453, Princeton University, Woodrow Wilson School of Public and International Affairs; Bloom D, Khoury A, Kufenko V, Prettner K, “Spurring economic growth through human development: research results and guidance for policymakers,” Population and Development Review, 2021 Jun, 47(2): 377-409; Bloom D, Kuhn M, Prettner K, Health and economic growth, 2018, IZA DP No. 11939, available at: https://www.iza.org/publications/dp/11939/health-and-economic-growth; Collin M, Weil D, The effect of increasing human capital investment on economic growth and poverty: a simulation exercise, World Bank, WPS8590, 2018, available at: https://openknowledge.worldbank.org/handle/10986/30463. ↩︎
Wagner Z, Barofsky J, Sood N, “PEPFAR funding associated with an increase in employment among males in ten sub-Saharan African countries.” Health Affairs, 2015 Jun, 34(6): 946-953. ↩︎
Kim Y, Whang T, “The effects of the President’s Emergency Plan for AIDS Relief on the economies and domestic politics of focus countries”, Global Economic Review, 2017 Aug, 46(4), 441-463. ↩︎
See, for example: Bor J, Tanser F, Newell M, Barnighausen T, “In a study of a population cohort in South Africa, HIV patients on antiretrovirals had nearly full recovery of employment”, Health Affairs, 2012 July, 31(7),1459-1469; Resch S, Korenromp E, Stover J, Blakley M, Krubiner C, Thorien K, Hecht R, Atun R, “Economic returns to investment in AIDS treatment in low and middle income countries,” PLoS ONE 2011 Oct, 6(10): e25310; Thirumurthy H, Galárraga O, Larson B, Rosen S, “HIV treatment produces economic returns through increased work and education, and warrants continued US support,” Health Affairs, 2012 Jul, 31(7):1470-7; McLaren Z, Bor J, Tanser F, Barnighausen T, Economic stimulus from public health programs: externalities from mass AIDS treatment provision in South Africa, September 2019, available at: https://mdsoar.org/handle/11603/23512. ↩︎
See, for example, Zivin JG, Thirumurthy H, Goldstein M, “AIDS treatment and intrahousehold resource allocation: children’s nutrition and schooling in Kenya,” J Public Econ, 2009 Aug, 93(7-8):1008-1015; Guo Y, Li X, Sherr L, “The impact of HIV/AIDS on children’s educational outcome: a critical review of global literature,” AIDS Care, 2012 April,24(8):993-1012. ↩︎
See discussions in: Bloom D, Khoury A, Kufenko V, Prettner K, “Spurring economic growth through human development: research results and guidance for policymakers,” Population and Development Review, 2021 Jun, 47(2): 377-409; Bloom D, Kuhn M, Prettner K, Health and economic growth, 2018, IZA DP No. 11939, available at: https://www.iza.org/publications/dp/11939/health-and-economic-growth; Weil D, “Health and economic growth”, ch. 03, p. 623-682 in, Handbook of Economic Growth, 2014, vol. 2: 623-682. ↩︎
Gertler P, Martinez S, Premand P, Rawlings L, Vermeersch C. Impact evaluation in practice, second edition. 2016, Washington, DC: Inter-American Development Bank and World Bank. Available at: https://openknowledge.worldbank.org/handle/10986/25030. ↩︎
An updated Peterson-KFF Health System Tracker analysis shows the United States experienced a second year of decline in life expectancy in 2021 while other comparably large, wealthy countries saw a rebound in life expectancy since the onset of the COVID-19 pandemic in 2019. Over recent decades, life expectancy has improved by much more in peer nations than it has in the U.S. The COVID-19 pandemic has increased mortality and premature death rates in the U.S. by more than it did in most peer countries, widening a gap that already existed before the pandemic. While the U.S. has the lowest life expectancy among comparable countries, it far outspends its peers on health care. In 2021, the U.S. spent over $4,000 more per capita on health care than the next highest spending country.
If the federal government runs out of money to purchase COVID-19 vaccines, the per-dose price likely would skyrocket and could increase spending on vaccines by billions of dollars a year, a new KFF analysis finds.
To date, the federal government has spent more than $30 billion on COVID-19 vaccines to encourage their development, guarantee a market, and ensure that the public can access them at no charge. The Biden administration has said it can no longer afford to purchase additional doses if Congress does not provide more funds, shifting the burden to the commercial market.
Vaccine makers Pfizer and Moderna have announced that the anticipated commercial price per dose of their vaccines would likely be between $82 and $130 per dose – roughly three to four times what the federal government has paid, according to the KFF analysis.
If payers end up paying those prices for one dose per adult, the analysis estimates that the total cost of purchasing booster shots commercially would run between $6.2 billion and $29.7 billion a year, depending on price and how many people nationally get the vaccine or booster.
Put another way, the federal government could purchase enough bivalent booster shots to serve all adults nationally at its current per-dose price for $7.5 billion, about what it would cost to purchase doses for just a quarter of adults at the higher commercial per-dose price.
While it is possible insurers and other payers could negotiate discounts from the prices suggested by the manufacturers, they will have limited leverage because they will generally be required to cover all recommended vaccines and boosters.
Even after vaccines are purchased commercially, most people with health insurance should still be able to access COVID-19 vaccines without any cost-sharing, and the higher per-dose price would be borne by public and private insurers, including Medicare and Medicaid. For private insurers and their enrollees, these costs could push premiums upward.
People who are uninsured would lose guaranteed access to free COVID-19 vaccines, and the high cost of getting one at the commercial price could discourage some from getting them.