KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Poll: As States Start to Ease Coronavirus Restrictions, Few Americans Expect to Stay in Hotels or Fly This Summer, Though Most Plan to Visit a Doctor, Get a Hair Cut and Dine Out
Deep Partisan Differences on Almost Every Dimension of Coronavirus: Republicans are More than Three Times as Likely as Democrats to Say Their State is Moving Too Slowly to Ease Restrictions
Most of the Public, including Most Swing Voters, Disapprove of President Trump’s Coronavirus Response and Overall Job Performance; President Earns Higher Ratings on the Economy
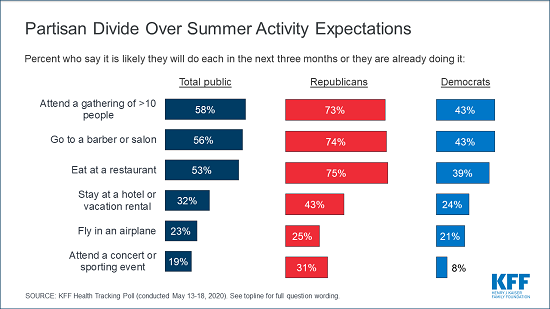
Even as many states start to lift restrictions on businesses and social gatherings, most Americans are expecting the coronavirus pandemic to upend their summers, with few saying they expect to stay in a hotel (32%), fly (23%), or attend a concert or sporting event (19%) during the next three months, the latest KFF Health Tracking Poll finds.
Larger shares of the public say they are likely to engage in other routine activities, including 82% who say they expect to visit a doctor or dentist in person over the next three months. Most say they expect to attend a gathering of at least 10 people (58%), visit a salon or barber (56%), or eat in person at a restaurant (53%).
Democrats are more wary than Republicans and independents about engaging in most of these activities – just one example of a deep partisan divide that colors Americans’ views about the coronavirus crisis.
“There is one pandemic, but Americans increasingly view both the gravity of it and what should be done about it through red- and blue-colored glasses,” KFF President and CEO Drew Altman said. “It’s a sad comment that partisan division, not national unity, is becoming a defining feature of the American response to coronavirus.”
Fewer than half of Democrats say they expect to attend larger gatherings (43%), visit a barber or salon (43%), or eat at a restaurant (39%) over the next three months, while most Republicans and independents say they are already doing these activities or expect to do them soon.
While minorities across party lines say they would stay at a hotel or vacation rental, fly, or attend a concert or sporting event in the coming months, Republican are more likely than Democrats to say they expect to do each of those activities.
Other examples of the partisan divide include:
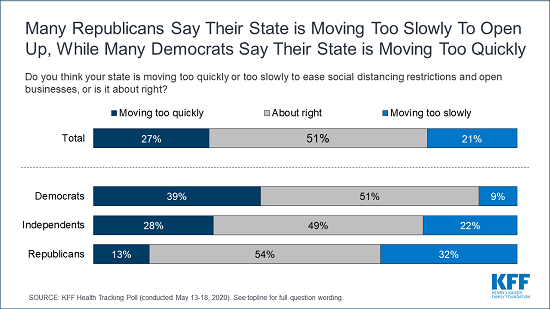
More than three times as many Republicans (32%) as Democrats (9%) say their state is moving “too slowly” to ease social distancing restrictions and reopen businesses, while Democrats are three times as likely as Republicans to say their state is moving “too quickly” (39% and 13%, respectively). Independents are more evenly split with 28% saying “too quickly” and 22% saying “too slowly.”
Democrats (70%) are about twice as likely as Republicans (37%) to say they wear a protective mask “every time” they leave their house and might be in contact with others. Among the public overall, about three quarters of adults say they wear a mask every time (52%) or most of the time (21%).
Most people (72%) think President Trump should wear a mask when meeting with other people. This includes a large majority (88%) of Democrats but only about half of Republicans (48%).
Two thirds of Republicans either say that the coronavirus pandemic isn’t a major problem (20%) or that the “worst is behind us” (45%), while most Democrats (70%) and half of independents say “the worst is yet to come.” Half of adults overall say “the worst is yet to come,” nearly twice the share (28%) who say “the worst is behind us.”
Most of the Public and Most Swing Voters Disapprove of President Trump’s Coronavirus Response
The public’s rating of President Trump’s job performance on coronavirus has fallen, with slightly more Americans now disapproving (52%) than approving (46%) after tilting positive six weeks earlier. Similar shares now disapprove of President Trump’s performance on health care (51%) and overall (52%). In contrast, most of the public (57%) approve of his performance on the economy.
While most Republicans approve and most Democrats disapprove of President Trump’s performance across the board, independents are conflicted. Most disapprove of his overall performance (54%) and on coronavirus (52%) and health care (51%), but most approve on his performance on the economy (59%).
The crucial group of “swing voters,” who are not yet certain about their presidential vote in November, are also negative in their assessments of President Trump’s presidency. Six in 10 swing voters (59%) disapprove of the president’s overall job performance, and similar shares disapprove of his handling of coronavirus (61%) and health care (58%). Swing voters remain positive in their assessments of his handling of the economy (59% approve).
With less than six months before the 2020 presidential election, the poll finds the economy and health care remain the top two election issues, with roughly equal shares naming the economy (25%) and health care (23%) as the most important issue in their vote for president. The coronavirus pandemic, which affects both health care and the economy, ranks third (17%).
The economy stands out by far as Republicans’ top issue, with 40% saying it is the most important to their vote. In comparison, just 13% of Democrats cite the economy as their top issue, ranking it third behind health care (32%) and the coronavirus pandemic (29%).
Swing voters rank health care (30%) and the economy (25%) as the top issues, followed by the coronavirus pandemic (19%).
Designed and analyzed by public opinion researchers at KFF, the poll was conducted May 13-18 among a nationally representative random digit dial telephone sample of 1,189 adults. Interviews were conducted in English and Spanish by landline (283) and cell phone (906). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
KFF will release additional findings from this poll in the coming days.
COVID-19 has the potential to deeply impact PEPFAR countries, especially those in sub-Saharan Africa and, as such, affect PEPFAR’s future trajectory.
As the largest U.S. global health program, PEPFAR is in a unique position to respond to COVID-19, but the outbreak also raises urgent new questions for PEPFAR, as well as underscores existing challenges.
PEPFAR has moved to respond quickly, accelerating prior strategies that could serve to minimize disruption and promote continuity of HIV care, such as multi-month dispensing of antiretrovirals; implementing new strategies, such as telemedicine; and allowing for some program flexibility in reporting requirements, staffing, and funding re-allocation.
Despite these steps, there are likely to be additional disruptions and need for further guidance, flexibilities and, potentially, new resources for PEPFAR which, to date, has not received additional support through the emergency measures passed by the U.S. Congress.
Introduction
The potential for the COVID-19 pandemic to significantly affect the health and development of low- and middle-income countries (LMICs), particularly those in sub-Saharan Africa, has serious implications for PEPFAR, the President’s Emergency Plan for AIDS Relief. PEPFAR is the U.S. government’s flagship global health effort, credited with saving millions of lives and helping to change the trajectory of the global HIV epidemic. As of May 17, coronavirus cases have been reported in all PEPFAR countries1 , with cases rising rapidly in some (see Table 1), and many are in lockdown or have instituted other social distancing measures. Most of these countries lack robust health systems and have limited preparedness and readiness capacity to respond to COVID-19. Given PEPFAR’s large country footprint, expertise and country infrastructure, the program is in a unique position to respond to COVID-19.
However, the outbreak also raises urgent new challenges for the program, as well as amplifies existing ones, given the potential for it to halt or even reverse hard-won HIV-related gains and alter the global health landscape. While PEPFAR has taken steps to respond to the outbreak, it is still unclear if these will be enough or if additional measures will be taken. To date, while emergency funding has been provided for certain global efforts and to domestic HIV programs by the U.S. Congress, no new resources have been provided to PEPFAR. As COVID-19 continues to impact the countries within which PEPFAR operates, this issue brief examines the potential implications for PEPFAR, the steps the program has taken to respond to the outbreak, and issues at stake.
Table 1: COVID-19 Cases in 25 PEPFAR Countries
Country
# of COVID-19 Case(as of May 17, 2020)
Angola
48
Botswana
25
Burundi
23
Cameroon
3,105
Côte d’Ivoire
2,109
Democratic Rep. of the Congo
1,455
Dominican Republic
12,314
Eswatini
203
Ethiopia
317
Haiti
456
Kenya
887
Lesotho
1
Malawi
70
Mozambique
137
Namibia
16
Nigeria
5,959
Rwanda
292
South Africa
15,515
South Sudan
290
Tanzania
509
Uganda
227
Ukraine
18,291
Vietnam
320
Zambia
753
Zimbabwe
44
Total
63,366
NOTES: Includes 25 countries required to develop PEPFAR Country Operating Plans (COPs). Includes confirmed and presumed positive COVID-19 cases.SOURCE: KFF. COVID-19 Coronavirus Tracker.
PEPFAR Snapshot
PEPFAR is funded at approximately $5 billion per year (not including contributions to the Global Fund to Fight AIDS, Tuberculosis and Malaria), making it the largest U.S. global health program and largest in the world devoted to a single disease. As of September 2019, PEPFAR is estimated to have provided life-saving antiretroviral medications to more than 15 million people, supported testing services for nearly 80 million, and prevented more than 2.6 million babies from being born with HIV.
While PEPFAR support reaches more than 50 countries, the program focuses most of its efforts on a subset of 25 countries.2 These 25 countries represent nearly 65% of people living with HIV (see Table 2). PEPFAR activities focus on expanding access to HIV prevention, treatment, and care interventions. These include provision of HIV testing, antiretroviral treatment, pre-exposure prophylaxis, voluntary male circumcision (VMMC), condoms, and prevention programming focused on certain populations, including adolescent girls and young women. PEPFAR also provides broader health systems support in countries, including investments in health workforce and laboratory capacity.
While significant progress has been made, prior to the outbreak, only a limited number of PEPFAR’s countries were on target to meet global HIV milestones, including the UNAIDS 90-90-90 targets (by 2020, 90% of people with HIV would know their status; 90% of people diagnosed with HIV would be on treatment; and 90% of those on treatment would be virally suppressed), or PEPFAR’s own goal of achieving epidemic control by 2020 (defined by PEPFAR to be when new HIV infections fall below deaths from all causes among people with HIV). Other challenges facing PEPFAR that pre-date the outbreak include:
Concern about U.S. funding fatigue amidst a growing global funding gap;
Promise versus reality of domestic resource mobilization;
Interdependence of PEPFAR’s and the Global Fund’s successes and donor coordination more broadly;
How to optimally reach marginalized populations and those most at risk for HIV; and
Converging timelines of the expiration of PEPFAR’s current strategy, the next U.S presidential and congressional elections, and the lead-up to PEPFAR’s next reauthorization.
Table 2: HIV Indicators for 25 PEPFAR Countries
Treatment Cascade
Country
Number of People Living with HIV(2018)
HIV Prevalence(2018)
HIV Incidence-to-Prevalence Ratio(2018)
HIV Incidence-to-Mortality Ratio(2018)
% People living with HIV who know their status(2018)
% People living with HIV receiving ART(2018)
% People living with HIV who have suppressed viral loads(2018)
HIV Incidence per 1000 Population(2018)
Angola
330,000
2
8.45
1.71
42
42
–
1.01
Botswana
370,000
20.3
2.31
1.24
91
83
81
4.36
Burundi
82,000
1
2.03
0.63
–
80
–
0.16
Cameroon
540,000
3.6
4.37
1.04
74
52
–
1.02
Cote d’Ivoire
460,000
2.6
3.67
0.79
63
55
41
0.7
Democratic Rep. of the Congo
450,000
0.8
4.13
1.1
62
57
–
0.21
Dominican Republic
70,000
0.9
3.92
1.72
82
56
37
0.26
Eswatini
210,000
27.3
3.78
2.03
92
86
81
8.62
Ethiopia
690,000
1
3.28
1.48
79
65
–
0.24
Haiti
160,000
2
4.63
1.9
67
58
–
0.69
Kenya
1,600,000
4.7
2.94
1.26
89
68
–
1.02
Lesotho
340,000
23.6
3.87
1.29
86
61
57
7.8
Malawi
1,000,000
9.2
3.65
2.04
90
78
69
2.28
Mozambique
2,200,000
12.6
6.64
2.05
72
56
–
5.25
Namibia
200,000
11.8
3.05
1.51
91
92
87
2.82
Nigeria
1,900,000
1.5
6.57
1.73
67
53
42
0.65
Rwanda
220,000
2.5
1.59
0.86
94
87
74
0.29
South Africa
7,700,000
20.4
3.08
1.88
90
62
54
4.94
South Sudan
190,000
2.5
9.93
1.71
24
16
–
1.56
Tanzania
1,600,000
4.6
4.64
2.13
78
71
62
1.41
Uganda
1,400,000
5.7
3.82
1.56
84
72
64
1.4
Ukraine
240,000
1
5.26
1.69
71
52
48
0.28
Vietnam
230,000
0.3
2.48
1.01
–
65
–
0.06
Zambia
1,200,000
11.3
3.89
1.94
87
78
59
2.97
Zimbabwe
1,300,000
12.7
2.93
1.34
90
88
–
2.79
Global
37,900,000
0.8
4.6
1.71
79
62
53
0.24
Global Target
–
–
<3.0
<1
90
81
73
<1
# Countries Meeting Target
–
–
6
3
7
5
4
10
NOTES: Includes 25 countries required to develop PEPFAR Country Operating Plans (COPs). HIV data is for all ages unless otherwise specified. HIV prevalence data is for adults (ages 15-49). Percentages for the treatment cascade global targets are based on the 90-90-90 global targets.SOURCES: U.S. Department of State, “Where We Work — PEPFAR” webpage, https://www.state.gov/where-we-work-pepfar/. UNAIDS, AIDSInfo database, accessed May 2020. UNAIDS, Global AIDS Update 2019, December 2019. UNAIDS, “Ratio of new HIV infections to number of people living with HIV improving”, April 2020. UNAIDS, “Making the End of AIDS Real: Consensus building around what we mean by epidemic control”, October 2017.
HIV & COVID-19
COVID-19 has introduced particular challenges for the HIV response. First, while there is no evidence that people with HIV are at greater risk of SARS-CoV-2 infection, the virus that causes COVID-19, those with underlying health conditions, including uncontrolled HIV, are at greater risk of developing more severe disease if infected. Second, the very health systems and services that people with and at risk for HIV rely on could be disrupted, potentially affecting access to and continuity of critical medications, care, and other services. Third, lockdowns and other social distancing measures may also affect the ability of those with HIV to access services or exacerbate factors that put people at risk for HIV, including interpersonal and/or gender-based violence (IPV/GBV). New modeling estimates from the WHO and UNAIDS show that there could be half a million additional deaths from AIDS-related illnesses and significant increases in mother-to-child HIV transmission in sub-Saharan Africa if more is not done to mitigate service interruptions.
Disruptions in supply chains for antiretrovirals, rapid tests, and other key commodities related to HIV services;
Reductions in HIV program personnel due to evacuations or redeployment to address COVID-19; and suspension of some prevention services, such as voluntary medical male circumcision;
Anticipation of increased use of laboratory facilities and lab staff for SARS-CoV-2 testing, which could impact HIV testing and lab capacity;
Lack of personal protective equipment (PPE) for health workers.
Concerns that physical distancing measures and health system pressures will prevent people with and at risk for HIV from seeking services, including treatment and testing, and about the potential for clinic closures;
Barriers to effective telehealth services, especially for youth; and
Concerns about potential food insecurity and resulting poor nutrition, which can negatively affect antiretroviral therapy and can be particularly detrimental to pregnant and breastfeeding women.
PEPFAR’s Response to COVID-19
PEPFAR has identified four key priorities to guide its programming during the outbreak: ensuring continuity of care for people living with HIV, particularly antiretroviral treatment; leveraging PEPFAR’s infrastructure to respond to COVID-19; reducing risk of exposure to staff and clients; and providing program flexibility.
PEPFAR also began providing technical guidance to the field, first released on March 20, and updated regularly. The guidance addresses multiple areas, including: maintenance of antiretroviral treatment; HIV testing; prevention, including provision of PrEP, especially for those who are most vulnerable; particular needs of women, children and families; co-infection/ co-morbidities (e.g., tuberculosis); integration of services, such as HIV and family planning; IPV/GBV; and supply chain challenges and laboratory capacity issues (see Table 3). It provides a number of strategies that can be used by country and regional teams to adapt to the new realities of COVID-19.
Some are strategies PEPFAR has already been working to prioritize and are now being accelerated by the outbreak, such as multi-month dispensing (MMD) of antiretrovirals and health care worker (HCW) task shifting/sharing. These are part of PEPFAR’s larger move to differentiated service delivery, an approach to providing services that aims to meet the diverse needs of clients, while also reducing the burden on health facilities and improving health outcomes. Others are designed to respond to the acute situation of COVID-19 and reduce the risk of transmission, such as encouraging telehealth, cancelation of most in-person activities, and health care worker re-training in Infection Prevention and Control (IPC) and training on COVID-19. The guidance also indicates where flexibilities are permitted, including extensions of reporting periods, and indicates that requests to utilize HIV resources to also respond to COVID-19 can be made.
Facilities should minimize patient contact and reduce non-essential visits.
Clinics to consider staggering appointments and streamlining clinic flow; HIV patients should be seen in clinics that are dedicated for HIV treatment.
Telehealth (e.g., phone calls, SMS, WhatsApp, social media, and other digital platforms) should be used to communicate with HIV clients.
Facilities should maximize 6-month refills for ARVs where stock is available.
Clients should preferably receive drug supplies (e.g., ARVs, PrEP, HIV self-tests, other medicines for chronic conditions) outside of the facility setting (e.g., home deliveries, community or private pharmacies, pop-up pharmacies, automated lockers, or community pickups).
Additional steps should be taken to prepare for clinic closures.
Beyond any Chief of Mission directive, involvement in larger U.S. government COVID-19 response should be based on and limited to the intersection of HIV, HIV/TB, and COVID; PEPFAR Coordination Offices should stay abreast of ways in which PEPFAR program investments are being leveraged for the larger U.S. COVID-19 response and potential adaptations necessary to implement the PEPFAR program safely; PEPFAR Coordination Offices are not responsible for coordinating the larger U.S. COVID-19 response.
Human Resources for Health
PEPFAR-supported health care workers (HCWs) should be prepared to continue to deliver essential HIV services.
Staff should be prepared for task shifting/sharing of essential services where allowed and be prepared to be repurposed or redeployed, including to enable provision of services outside of facilities; staff should work with local governments to allow emergency task-shifting where formal policies are not in place.
Depending on role, HCWs should be trained to screen HIV patients for COVID-19 and refer for testing and treatment based on in-country guidance for COVID-19 cases.
HCWs should receive refresher training in Infection Prevention and Control (IPC) and steps should be taken to protect their safety (e.g., secure authorization from local authorities for continued work, support staff to avoid public transportation, reduce in-person contact).
Limit home visits to those “absolutely essential.”
Direct HCW-patient interactions for HIV services should not take place where routine adequate PPE is not available (e.g., gloves).
HIV Treatment
Accelerate and complete scale up of 3 to 6 multi-month dispensing (MMD) of ARVs, where available.
ARV distribution for all people living with HIV should be decentralized.
Phone or electronic follow-up encouraged to support adherence/assess side effects for those initiating treatment, to continue peer support for youth, and for other purposes related to HIV treatment.
Routine viral load monitoring in stable patients may be delayed.
HIV Prevention
Packaging of condoms and lubricants, and at larger than normal quantities, should be supplied to extent possible; distribution points should be modified to reflect social distancing.
PrEP should continue as part of comprehensive prevention; MMD should be allowed.
New VMMCs may be delayed or paused, depending on host government guidance/policies on social distancing; post-operative follow up should continue.
Phone and digital platforms should be utilized for general HIV prevention services, as well as for PrEP and VMMC follow up.
HIV Testing
Adapt HIV testing services to host country government directives or policies on social distancing.
Maximize use of self-testing outside of the clinic setting through decentralized distribution approaches (e.g., peer home delivery, private/community pharmacies).
Prioritize clinical-based testing for those most in need (e.g., in antenatal settings, diagnostic testing for individuals presenting with suspected HIV, individuals with TB/STIs/malnutrition; early infant diagnosis (EID) detection, passive partner/index/family testing, in certain key population programs).
Testing should not take place where routine adequate PPE is not available (e.g., gloves).
Recommended recency testing be temporarily paused at health facilities and laboratories.
Shortages of rapid test kits have been reported.
TB
Programs should continue to screen and test for TB in high prevalence areas and consider testing for both TB and COVID-19 in people living with HIV, especially in people presenting with fever and cough.
PEPFAR-supported TB contact investigations should make efforts to use mobile/virtual platforms; community-based testing and active TB case-finding strategies among people with HIV should follow local/national COVID-19 guidance on movement restriction/social distance/continuity of operations; if mobile and virtual platforms cannot be used and it is not safe for HCWs to conduct contact investigations in the community, contact-tracing/case-finding for TB may need to be deferred.
People with HIV should be provided with the full or remaining course of their drugs for TB-HIV or drugs for TB prevention.
Phone consultations for people with HIV-TB should be used, where possible.
Women’s Health
Voluntary family planning services continue as an essential service.
HIV services integrated with contraceptive services should be streamlined to avoid patient visits to facilities or optimally use time when in clinic.
Multi-month provision of oral contraceptives and condoms should be provided and optimal schedules for long-acting contraceptives should be developed between client and provider (note: PEPFAR cannot be used to procure contraceptives; they are made available to PEPFAR-supported programs through collaboration with national family planning programs, USAID, and other donors).
Problems with contraceptive supply chains have been noted; country teams advised to include contraceptives on lists of essential drugs allowed into countries while shipments are restricted; integrating FP and HIV supply chain management and distribution may also help ensure contraceptives are available for HIV-affected populations.
Cervical cancer screening outside of same-day/same-site ART clinical services should be limited; screening done as part of routine ART visit may continue; high-grade lesion treatment can continue.
Maternal Child Health
Women should follow local/national guidelines for ANC testing; options to limit or reduce time spent in clinic settings should be considered (e.g., providing services in community settings, bundling services); regular retesting for HIV is encouraged, if feasible.
HIV self-testing can be used for pregnant and breastfeeding women; women screening positive should be fast-tracked for confirmatory testing and treatment services.
PrEP should continue to be offered and MMD should be considered.
Consider offering newborn prophylaxis in case of home/community births.
EID should continue as an essential service with proper precautions.
Expand phone/SMS support to mothers and infants.
DREAMS
Contact with DREAMS participants should be maintained via phone/SMS/WhatsApp/digital platforms, depending on country and local context.
Group-based activities should follow local guidelines for mass gatherings.
Where feasible, facility-based DREAMS services should be offered in community with appropriate social distancing.
IPV/GBV
Teams should advocate with host governments to designate child protection and GBV responders; work with local entities and donors to update directories of response services; ensure that PEPFAR staff have information on resources and can support clients experiencing violence.
Children
Many stipulations noted above apply to children and the guidance outlines additional recommendations given the special treatment, testing, and prevention needs of children.
Orphans and Vulnerable Children (OVC) activities can continue and can be conducted virtually, including for treatment literacy and adherence support, linkages to food supplementation/assistance, hygiene supplies, and distance learning opportunities; staff encouraged to incorporate COVID-19 prevention messaging and resources, per host country government guidelines, into virtual support to households; enrollment can continue to extent possible and certain populations should be prioritized, including children and adolescents living with HIV; HIV-exposed infants; and infants, children, and adolescents exposed to abuse, harm, or violence.
Laboratory
Some countries are experiencing delays for HIV test kits and consumables; orders should be placed at least one month earlier than usual.
Due to recent WHO and FDA guidance on emergency use authorization for HIV viral load, EID, and TB-related instruments for SARS-CoV-2 testing, there is potential for increased demand on diagnostic networks; teams should anticipate increased use of instruments, facilities, consumables, and PPE for COVID-19, HIV, and TB-related testing and prepare for staff diversions or reductions in lab and other staff.
Laboratories should prioritize testing based on local policies and needs; HIV-related testing should be prioritized for certain populations (e.g., EID, viral load services for children and pregnant and breastfeeding women, non-virally suppressed adults).
If HIV and COVID-19-related testing need to be conducted on same instrument, SOPs for testing prioritization should be developed in collaboration with host country government and other stakeholders.
Use of existing national laboratory capacity, systems, and networks for COVID-related testing encouraged; funding dedicated for HIV and TB testing should not be reallocated for COVID-19; any additional costs for COVID-19 testing should be paid using country-specific COVID-19 supplemental funds from other sources.
Supply Chain/Commodities
Country programs advised to assess current stocks of antiretrovirals and develop distribution plans with goal to distribute drugs so each client has enough for at least 3 months; PEPFAR working to ensure HIV commodity supplies; USAID coordinating with Global Fund to Fight AIDS, Tuberculosis and Malaria to prevent stock outs; country teams should work with host country governments to ensure MMD policies communicated to providers, facilities, pharmacies, and supply chain actors.
Delays expected for ARVs due to majority of U.S.-FDA approved ARV manufacturers in India; facilities have experienced interruptions due reduced capacity and logistical challenges during lockdown.
Should additional stock be necessary for acceleration of 6-month MMD, teams should notify proper U.S. government staff.
PEPFAR cannot ensure appropriate and adequate supply of PPE; teams asked to seek alternative sources.
NOTE: This table highlights a selection of issues; see guidance for more detail.SOURCE: PEPFAR. PEPFAR Technical Guidance in Context of COVID-19 Pandemic (May 13, 2020).
While the guidance is being regularly updated to address emerging issues, there are potential gaps or questions that exist. For instance, the guidance calls for an acceleration of antiretroviral MMD and, while it notes the challenges in achieving MMD goals for people with HIV in an expedited timeframe, it will be important to monitor how supply chain disruptions, lockdowns/restrictions in movement, and the rapid scale-up will impact MMD across populations and countries. Additionally, the extent to which decentralization and telehealth can be implemented in all settings, especially those with hard-to-reach populations, will be important to assess as well and may require other measures to support continuity of care. The guidance also calls for staff in health care settings to have proper personal protective equipment (PPE), although it does not indicate these can be secured amid shortages and restrictions on purchasing with U.S. assistance dollars.
PEPFAR’s responses also will depend upon host government approaches to COVID-19 mitigation and ensuring the continuity of HIV services during the outbreak. To date, the governments of several PEPFAR countries have issued their own guidance for HIV services amid the pandemic. Further, while PEPFAR has stated that program flexibility is a key goal at this time, there may be a need for more specificity about what is permitted. Finally, as PEPFAR works to maintain its current levels of service, particularly antiretroviral treatment, amid the new challenges of COVID-19, there could be considerable resource implications. While Congress has provided emergency COVID-19 funding to domestic HIV programs, it has not yet provided such funding to PEPFAR.
Questions Ahead
Despite the ongoing uncertainties regarding COVID-19’s impact in PEPFAR countries, it is highly likely that there will be significant implications for PEPFAR in both the short- and long-term. Some of these pre-date COVID-19 but are exacerbated by the outbreak; others are new concerns and challenges. Key questions to consider include:
What guardrails and warning systems can be put in place to help ensure the needs of people with HIV, particularly for antiretroviral treatment, are being met in real time as the COVID-19 outbreak worsens?
Will additional flexibilities, or clarification about existing flexibilities, be provided, including around the ability to reallocate current budgets?
Will additional resources be provided and how far will they go in meeting needs? How will those resource needs be quantified?
How will the decentralization of services and responses to COVID-19, including telehealth, carry forward after the pandemic?
How can the PEPFAR platform be leveraged to respond to COVID-19 without affecting HIV services? Can marginal investments be made in PEPFAR’s infrastructure, such as its laboratory networks and equipment, that are more cost-effective than building new systems to respond to COVID-19?
Will HIV trajectories in PEPFAR countries be impacted? Will ground be lost?
Will the larger landscape of HIV donor funding, which was already strained, be further impacted?
What does this mean for shifts to domestic HIV funding (which has been an increasing priority for PEPFAR and the U.S. government more broadly)? Are transitions away from PEPFAR funding by countries even more unlikely now, depending on the economic damage done by COVID?
How will COVID-19 contribute to and shape PEPFAR’s future role, including tensions between a laser focus on HIV and a broader focus on building health systems in PEPFAR-supported countries?
As the pandemic continues to unfold and health systems are tested and pushed further than most countries have experienced in modern history, the impact of COVID-19 on people with and at risk for HIV, and the programs and systems that serve them, will come into focus, as will the implications for PEPFAR. Should PEPFAR’s early response to COVID-19 be sustained, leveraged, and adequately resourced, it could help to bolster protections for people with HIV during the pandemic and contribute to the broader response in countries. On the other hand, the pandemic could potentially reshape PEPFAR and the broader HIV policy landscape for the years to come.
Sweden’s response to the novel coronavirus has been simultaneously praised and criticized by public health experts. In an article for Foreign Affairs, KFF’s Josh Michaud discusses the merits and risks associated with Sweden’s hands-off approach to the pandemic.
Community health centers are a national network of safety net primary care providers that fill an important role in national, state, and local responses to the coronavirus pandemic. Health centers primarily contribute to response efforts by providing tests, triaging patients, and reducing the burden on hospitals, although they also play a role in addressing demand for behavioral health services and continuing primary care for patients with chronic conditions. Patients at health centers are disproportionately low-income and people of color, groups especially hard hit by the pandemic. Among the roughly 28 million patients served by health centers, 91% are low-income and 63% are racial or ethnic minorities. Like other outpatient health care providers, health centers are having to adjust to stay-at-home orders, drops in patient visits for non-essential health care, and workforce challenges. This brief presents findings from new data collected by the Health Resources and Services Administration (HRSA) to provide insights into how health centers are adapting their services in response to the pandemic and how coronavirus is affecting their operations and long-term financial outlook with patient visits and revenue from those visits dropping precipitously. (For more detail on the data underlying this Data Note, see the text box at the end of the brief.)
COVID-19 Testing at Health Centers
Nine out of ten (90%) health centers are providing COVID-19 tests, and in 16 states and DC, all health centers are providing tests. Of those that provide testing, the majority (67%) offer walk-up or drive-through testing as of May 8, which can expand access to testing. In the week preceding May 8, health centers reported providing 127,816 tests, with 36,155 patients (28%) testing positive, roughly double the national positive test rate of 13% during a similar period.
People of color represented more than half of all people tested (57%) and confirmed cases (56%) at health centers. Among all individuals receiving tests, 24% were White and 57% were among people of color, including 32% who were Hispanic and 16% who were Black (Table 1). Race/ethnicity was unknown for about 1 in 5 tests (19%) and 1 in 4 confirmed cases (24%). Hispanics made up a higher share of positive tests, compared to their share of total tested patients (42% vs. 32%), while White patients made up a slightly lower share of positive tests compared to their share of total tested patients (19% vs. 24%). The ability of health centers to report testing data by race/ethnicity is important for broader efforts to ensure access to COVID-19 testing for people of color and to address disparities that existed prior to COVID-19 and may be widening due to the pandemic.
Table 1: Share of COVID-19 Tests and Confirmed Cases at Health Centers by Race and Ethnicity, Week Ending May 8, 2020
Race/Ethnicity
Percent of Tests
Percent of Positive Tests
White
23.7%
19.5%
Hispanic
32.2%
42.5%
Black
15.8%
7.0%
Asian
1.9%
1.1%
American Indian/Alaska Native
1.1%
0.3%
Native Hawaiian/Other Pacific Islander
0.4%
0.4%
More than One Race
5.9%
4.8%
Unknown Race/Ethnicity
19.0%
24.4%
Total
100%
100%
NOTES: Persons of Hispanic origin may be of any race. For this analysis, Hispanic patients include those who report Hispanic ethnicity and White, Black, or unknown race. Patients classified as White or Black are non-Hispanic. Other racial categories include both Hispanic and non-Hispanic individuals.SOURCES: HRSA. Health Center COVID-19 Survey. Latest data for the week ending May 8, 2020.
Effects of Coronavirus on Health Center Operations
Despite ramping up testing and virtual visits, health centers are reporting steep declines in patient visits and many staff who are unable to work. Health center organizations reported a 43% drop in the number of patient visits compared to before the pandemic, as many people across the country are avoiding non-essential trips to health care providers. The drop in visits comes even after health centers have been increasing the number of telehealth visits, with health centers conducting roughly half (51%) of visits virtually or over the phone. Additionally, health centers report that 11% of staff are not working due to exposure to the coronavirus, lack of protective equipment, site closures, or family obligations, among other reasons.
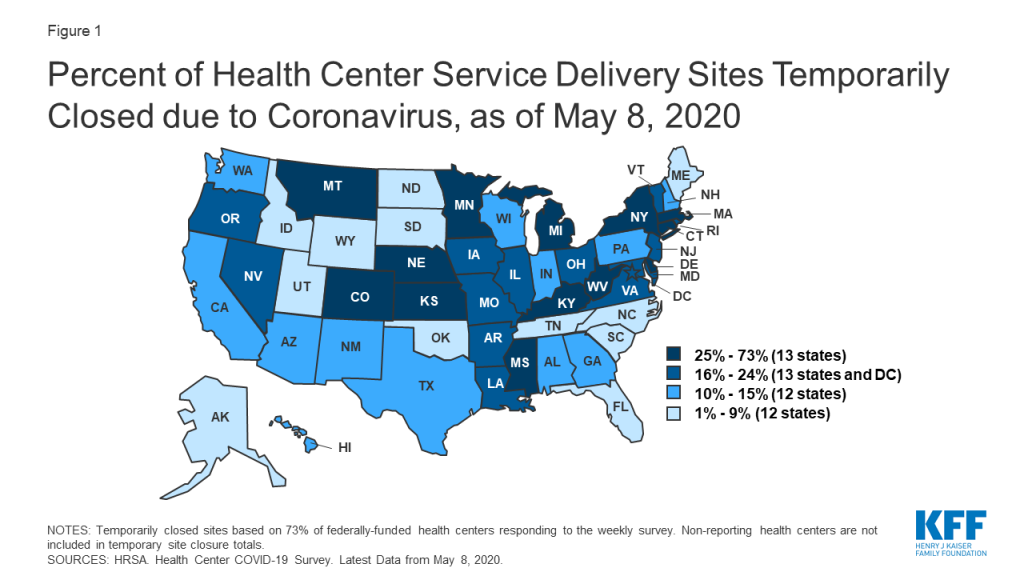
There have been 1,954 temporary health center site closures due to repercussions from the coronavirus as of May 8. Most health centers operate multiple service delivery sites – in 2018, 1,362 health centers operated 11,744 sites. The number of temporary site closures likely undercounts total closures, given that more than a quarter of health centers did not respond to the survey and are not included in the total. The survey data also do not provide details on the types of sites that have closed, such as whether the closed sites are brick-and-mortar, mobile vans, or school-based clinics. Still, site closures are occurring in states hard hit by the virus as well as in states less affected. Connecticut, close to the epicenter of the pandemic in the US, has seen nearly three-quarters (73%) of its sites closed, while Kentucky and Mississippi, which had fewer cases, have each seen 49% of sites closed. At least one-third of sites have closed in Nebraska (48%), Kansas (36%), West Virginia (36%), and Michigan (33%).
Figure 1: Percent of Health Center Service Delivery Sites Temporarily Closed due to Coronavirus, as of May 8, 2020
Financial Challenges
Health centers have received $1.98 billion in rapid response grants from the federal government, though more financial support may be needed to sustain services. These grants include $100 million in emergency grant funding and $1.3 billion through the Coronavirus Aid, Relief and Economic Security Act (CARES) that can be used to support response efforts, including buying testing materials and personal protective equipment (PPE), as well as to maintain or increase health center capacity generally. In early May, health centers received $583 million in grants to support COVID-19 testing capacity through the Paycheck Protection Program and Health Care Enhancement Act. All federally-funded health centers received each of these grants through an expedited awards process based on the size of the health center patient population and the number of uninsured patients reported to the Uniform Data System. While this funding is significant in aiding the coronavirus response, the combined $1.98 billion in additional appropriations represents just 7% of total health center revenues in 2018 (the most recent year of data available). Although data on the impact of the pandemic on overall health center finances are not available, the majority of health center revenues (68%) come from patient visits, and the drop in those visits could be contributing to a roughly 30% decrease in health center revenues. Adding to the uncertainty for health centers’ finances is the Community Health Center Fund (CHCF), an important source of federal funding representing $4 billion of the $5.6 billion appropriated to health centers in FY 2019. The CHCF has been extended through November – though it has not been reauthorized longer term as of mid-May 2020.
The effects of patient declines and staffing issues could have major implications for health centers even after the pandemic. Leading up to the pandemic, the two most commonly cited challenges for health centers were financial and workforce issues, both of which have been exacerbated by the economic effects of the coronavirus. The precipitous drop in patient volume has likely led to steep declines in patient care revenue that may contribute to future financial instability. Depending on how long the crisis lasts, some of the temporary site closures and staff reductions could become permanent, further exacerbating long-standing health care access issues in communities served by health centers.
Conclusion
Health centers will continue to play an important role in responding to the coronavirus pandemic and in providing access to care for communities disproportionately affected by COVID-19, especially as job losses mount and the number of people who are uninsured or covered by Medicaid rises. However, key findings from the HRSA survey highlight the significant operational challenges health centers are facing, which threaten their longer-term financial viability. While the emergency federal funding provided so far has aided health centers’ coronavirus response, secure future funding will also be important to maintain the long-term viability of the primary care safety net after the pandemic is over.
About the Health Center COVID-19 Data
In April 2020, HRSA began a weekly, rapid-response survey of all federally-funded health centers to track the impact of the coronavirus on health centers and identify needs for training, technical assistance, funding, and other resources. The survey instrument asks health centers to report on experiences from the previous week. All findings are reported at the health center organization level, although most health center organizations operate multiple clinic sites. Unless otherwise specified, all results discussed in this Data Note report findings at the health center organization (versus site) level. HRSA reports findings from the data as unweighted totals and percentages that do not account for non-responding health centers. The most recent survey data in this report is based on responses from the week ending May 8, 2020, with 1,011 (73%) federally-funded health centers responding to the survey.
Many states that shared budget projections in response to a new KFF survey of state Medicaid officials report that they expect to see Medicaid budget shortfalls due to rising Medicaid spending and enrollment as people lose jobs amid the coronavirus pandemic and more people enroll in the government health insurance program for low-income people.
KFF conducted the rapid survey of Medicaid directors in all 50 states and the District of Columbia with Health Management Associates (HMA), drawing responses from 38 states. Some states were still in the process of gathering data to understand the implications of the coronavirus at the time of the survey, and did not have updated enrollment and/or spending projections yet for FY 2020 and/or FY 2021.
The survey findings come at a time when Congress is considering an additional increase in the federal match rate available to states for Medicaid. Without additional federal support, state budgets for the forthcoming fiscal year – which begins July 1 for most states – will likely include significant spending cuts, including for Medicaid, at a time when demand for services is growing, the survey suggests.
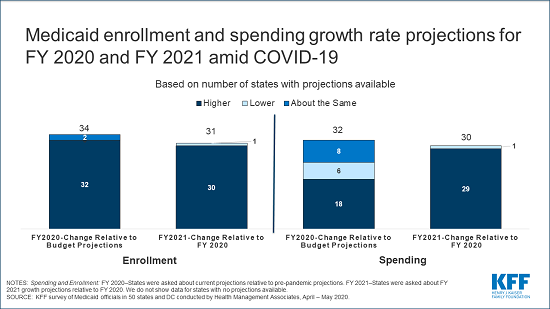
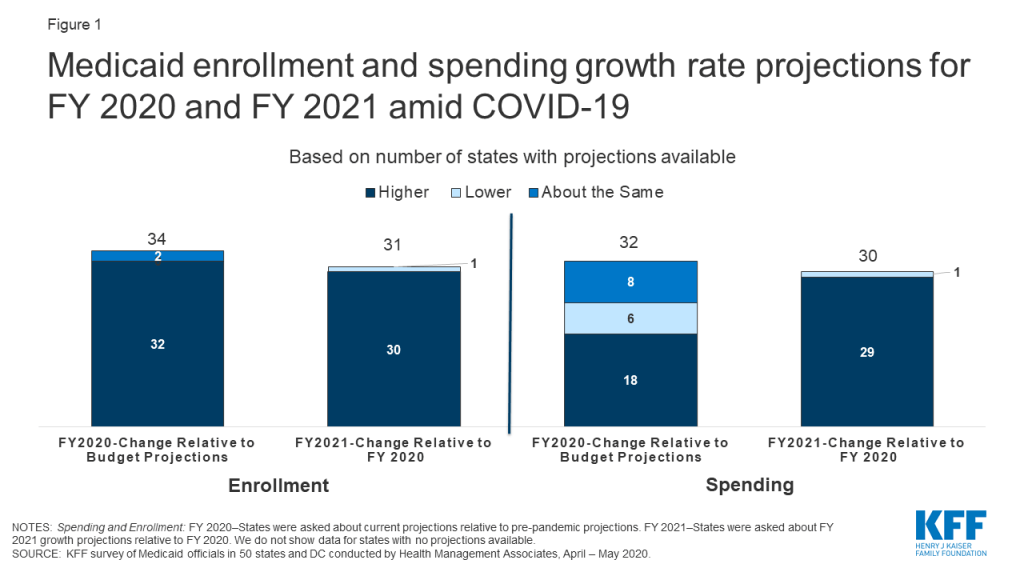
Overall, nearly all states with enrollment projections and over half of states with spending projections for FY 2020 anticipate growth rates to exceed pre-pandemic estimates for the current fiscal year. Nearly all states with projections anticipate that both enrollment and spending will grow more quickly in FY 2021 than in FY 2020. For most states, the fiscal year begins on July 1.
As a result of the accelerating enrollment and spending, 17 of 19 states that had budget projections reported that a budget shortfall was “nearly certain” or “likely” for the upcoming state fiscal year. Because Medicaid is financed with a combination of federal and state funds, states would need to make substantial cuts to Medicaid to generate significant state budget savings.
Medicaid is a countercyclical program. During economic downturns more people enroll, increasing program spending at the same time that state tax revenues may be falling. The Families First Coronavirus Response Act (FFCRA) authorized a 6.2 percentage point increase in the federal match rate (“FMAP”) to provide support to state Medicaid programs and fiscal relief for states if states comply with certain maintenance of eligibility requirements that would ensure continuous coverage for current enrollees.
Even with the additional help, state budgets are expected to be severely strained in the coming fiscal year, the survey shows. Legislation introduced on May 12 in the House would increase the FMAP by 14 percentage points from July 1, 2020 through June 30, 2021. But the future of the legislation, and prospects for additional federal support for states and Medicaid more generally, remain uncertain.
For the full report, as well as other data and analyses regarding Medicaid and COVID-19, visit kff.org.
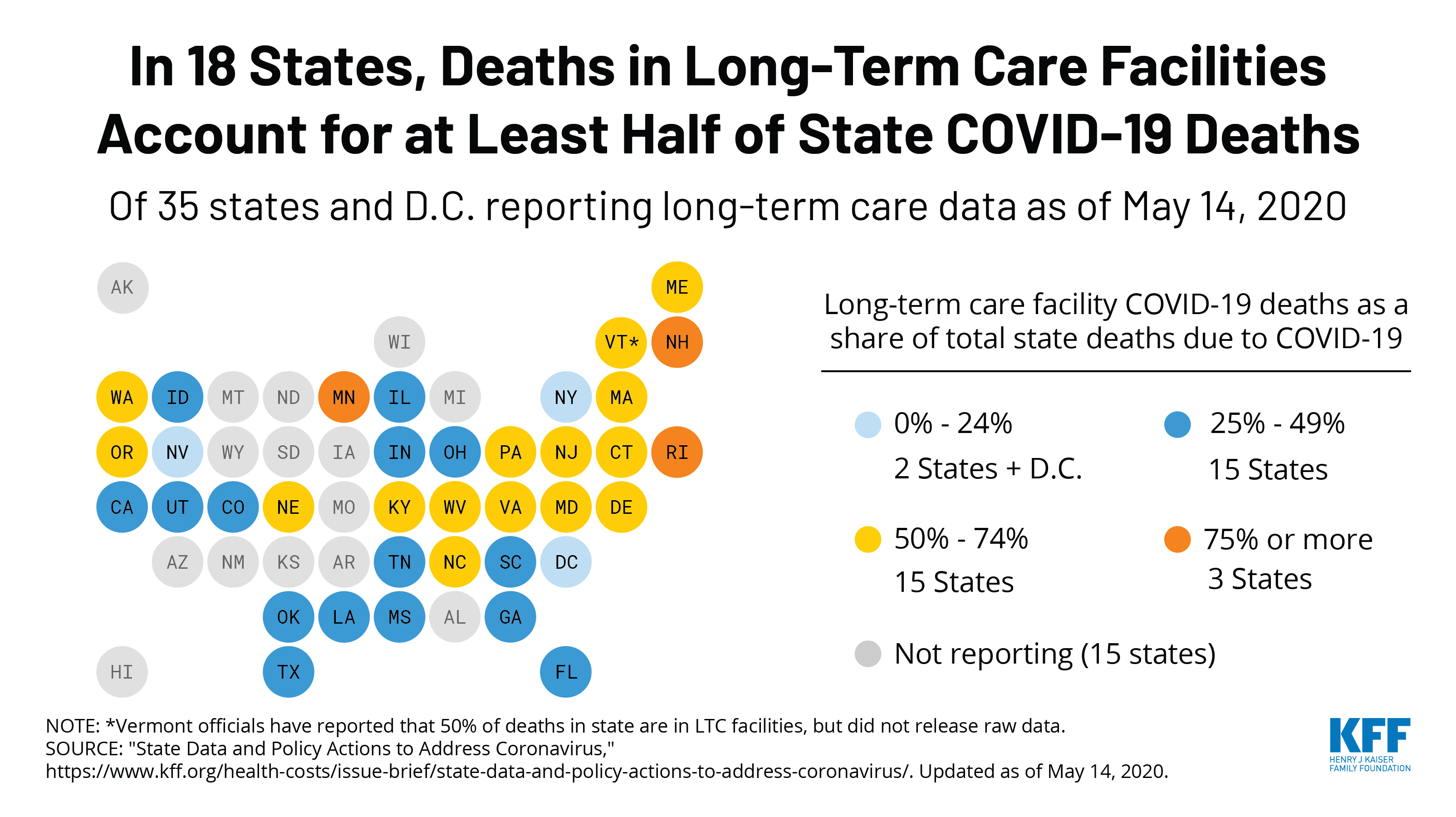
Every Friday, we’re recapping the latest on the coronavirus from our tracking, policy analysis, polling, and journalism. Total coronavirus cases in the U.S. are still climbing, and this week increased by 160,000, bringing the cumulative total of cases past 1.4 million. This week, approximately 10,000 people died from COVID-19 in the U.S., bringing the total to 85,700. Across 36 states reporting this data yesterday, 41% of deaths due to COVID-19 occurred in long-term care facilities.
Meanwhile, since last Thursday, eight more states have allowed some or all non-essential businesses (some with reduced capacity) to reopen since May 7. Restaurants have reopened to dine-in service in 5 states.
Here are more of the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: This week, total coronavirus cases worldwide passed 4.4 million – with approximately 596,000 new confirmed cases added between May 8 to May 14. There were approximately 33,000 new, confirmed deaths due to COVID-19 worldwide between May 7 and May 14.
U.S. Cases and Deaths: There have been over 1.4 million total confirmed coronavirus cases in the U.S. There were approximately 161,000 new confirmed cases and 10,000 confirmed deaths due to COVID-19 in the United States between May 7 and May 14.
U.S. Tests: There have been almost 10 million total COVID-19 tests with results in the United States — with over 1.9 million added since May 7. 13.9% of the total tests were positive. There have been 30.4 tests with results per 1,000 people in the U.S.
Social Distancing: 37 states have eased at least one social distancing measure.
Stay At Home Order: Original stay at home order in place in 29 states, stay at home order eased or lifted in 16 states, no action in 6 states
Mandatory Quarantine for Travelers: Original traveler quarantine mandate in place in 20 states, traveler quarantine mandate eased or lifted in 3 states, no action in 28 states
Non-Essential Business Closures: Original non-essential business closures still in place in 14 states, some or all non-essential business permitted to reopen (some with reduced capacity) in 31 states, no action in 6 states
Large Gatherings Ban: original gathering ban/limit in place in 39 states, gathering/ban limit eased or lifted in 10 states, no action in 2 states
State-Mandated School Closures: Closed in 7 states, closed for school year in 36 states, recommended closure in 1 state, recommended closure for school year in 6 states, rescinded in 1 state
Restaurant Limits: Original restaurant closures still in place in 30 states, restaurants re-opened to dine-in service in 20 states, no action in 1 state
Primary Election Postponement: Postponement in 14 states, cancelled in 1 state, no postponement in 36 states
Emergency Declaration: There are emergency declarations in all states and D.C.
Waive Cost Sharing for COVID-19 Treatment: 3 states require, state-insurer agreement in 3 states; no action in 45 states
Free Cost Vaccine When Available: 9 states require, state-insurer agreement in 1 state, no action in 41 states
States Requires Waiver of Prior Authorization Requirements: For COVID-19 testing only in 5 states, for COVID-19 testing and treatment in 6 states, no action in 40 states
Early Prescription Refills: State requires in 18 states, no action in 33 states
Premium Payment Grace Period: Grace period extended for all policies in 11 states, grace period extended for COVID-19 diagnosis/impacts only in 5 states, no action in 35 states
Marketplace Special Enrollment Period: Marketplace special enrollment period in 12 states, no special enrollment period in 39 states
Paid Sick Leave: 13 states enacted, 2 proposed, no action in 36 states
38 states have taken action to expand access to telehealth services, such as
New Requirements for Coverage of Telehealth Services: Parity with in-person services in 6 states, broad coverage of telehealth services in 6 states, limited coverage of telehealth services in 5states, no action in 34 states
Waiving or Limiting Cost-Sharing for Telehealth Services: Waived for COVID-19 services only in 7 states, waived or limited for all services in 9 states, no action in 35 states
Reimbursement Parity for Telehealth and In-Person Services: Required for all services in 17 states, no action in 34 states
Require Expanded Options for Delivery of Telehealth Services: Yes in 35 states, for behavioral health services only in 1 state, no action in 35 states
Approved Section 1115 Waivers to Address COVID-19: 1 state has an approved waiver
Approved Section 1135 Waivers: 51 states have approved waivers
Approved 1915 (c) Appendix K Waivers: 42 states have approved waivers
Approved State Plan Amendments (SPAs): 32 states have temporary changes approved under Medicaid or CHIP disaster relief SPAs, 1 state has an approved traditional SPA
Other State-Reported Medicaid Administrative Actions: 51 states report taking other administrative actions in their Medicaid programs to address COVID-19
Adults at Higher Risk of Serious Illness if Infected with Coronavirus: 38% of all U.S. adults are at risk of serious illness if infected with coronavirus (92,560,223 total) due to their age (65 and over) or pre-existing medical condition. Of those at higher risk, 45% are at increased risk of serious illness if infected with coronavirus due to their existing medical condition such as such as heart disease, diabetes, lung disease, uncontrolled asthma or obesity. Among nonelderly adults — low-income, American Indian/Alaska Native & Black adults have a higher risk of serious illness if infected with coronavirus. In both cases – for race and household income – the higher risk of serious illness if infected with coronavirus is chiefly due to a higher prevalence of underlying health conditions and longstanding disparities in health care and other socio-economic factors.
How Can Lessons from Medicaid Help Connect People to Unemployment Insurance? (Issue Brief)
Global Funding Across U.S. COVID-19 Supplemental Funding Bills (Issue Brief)
Opportunities and Barriers for Telemedicine in the U.S. During the COVID-19 Emergency and Beyond (Issue Brief)
N. Security Council Works To Find Common Ground On COVID-19, Cease Fire Resolution; WHO’s Nabarro Warns Of ‘Fracture In Global Leadership’ (KFF Daily Global Health Policy Report)
The coronavirus pandemic has generated both a public health crisis and an economic crisis, with major implications for Medicaid, a countercyclical program. During economic downturns, more people enroll in Medicaid, increasing program spending at the same time state tax revenues may be falling. To help support states as enrollment in Medicaid grows and ensure existing enrollees maintain continuous coverage, the Families First Coronavirus Response Act (FFCRA) authorized a 6.2 percentage point increase in the federal match rate (“FMAP”) (retroactive to January 1, 2020) available if states meet certain “maintenance of eligibility” (MOE) requirements.
This brief provides some early insights into the current picture of Medicaid spending and enrollment, as Congress considers providing additional fiscal relief through the federal Medicaid match rate. It is based on a rapid survey conducted by the Kaiser Family Foundation (KFF) and Health Management Associates (HMA) of Medicaid directors in all 50 states and the District of Columbia. A total of 38 states responded to the survey. Some states were still in the process of gathering data to understand the implications of the coronavirus at the time of this survey and did not have updated enrollment and/or spending projections yet for state fiscal year (FY) 2020 and/or FY 2021. Overall, nearly all states with enrollment projections and over half of states with spending projections anticipate FY 2020 growth rates to exceed pre-pandemic estimates. Nearly all states with projections anticipate FY 2021 growth rates to exceed rates in FY 2020 for both enrollment and spending (Figure 1). For most states, the fiscal year begins on July 1.
Figure 1: Medicaid enrollment and spending growth rate projections for FY 2020 and FY 2021 amid COVID-19
Overview
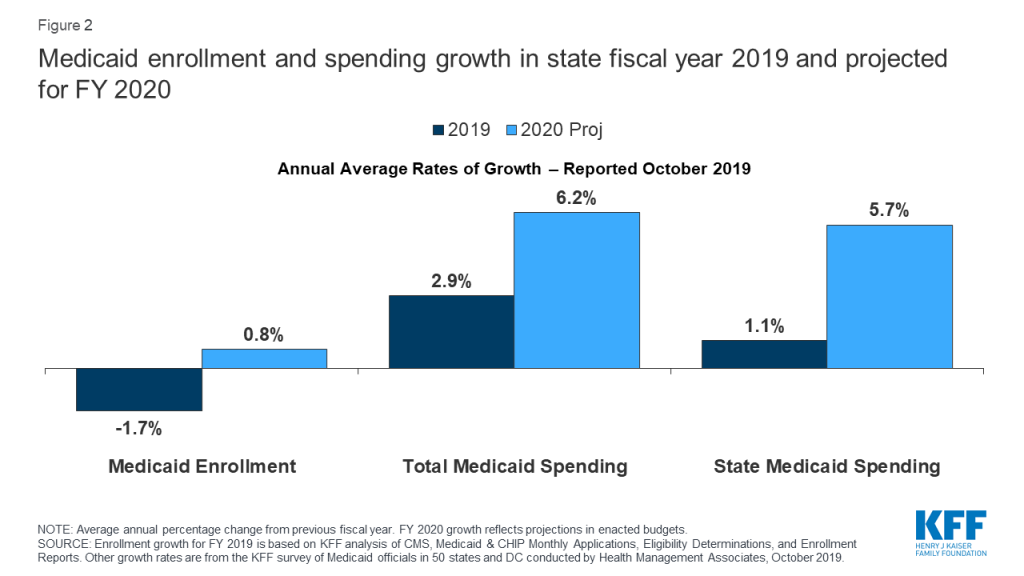
At the start of FY 2020, states anticipated relatively flat enrollment growth but modest total and state Medicaid spending growth (Figure 2). When states adopted budgets for FY 2020, states attributed flat enrollment projections primarily to a robust economy. States also pointed to changes in renewal processes, new functionality of upgraded eligibility systems, and enhanced verifications and data matching efforts as contributors to enrollment declines. While states expected flat enrollment growth to mitigate total Medicaid spending growth, states also reported that higher costs for prescription drugs, provider rate increases, and costs for the seniors and people with disabilities (including increased utilization of long-term services and supports) would put upward pressure on total Medicaid spending.
Figure 2: Medicaid enrollment and spending growth in state fiscal year 2019 and projected for FY 2020
The economic implications from the coronavirus pandemic are stark with unemployment rates up and state revenues down. April data show that the U.S. economy lost 20.5 million jobs and the unemployment rate increased to 14.7 percent. The Congressional Budget Office (CBO) estimates that the unemployment rate will average 15 percent during the second and third quarters of 2020, up from less than 4 percent in the first quarter. CBO expects the unemployment rate to decline somewhat but remain at 9.5 percent by the end of 2021 (about 6 percentage points higher than the rate in CBO’s economic projection produced in January 2020). Often individuals lose job-based health insurance coverage when they experience job loss. A recent KFF analysis shows that by January 2021, when unemployment insurance benefits cease for most people who lost jobs between March 1 and May 2, 2020, nearly 17 million people could be newly eligible for Medicaid and about 6 million eligible for marketplace subsidies (assuming individuals in this group have not found work as by that time) . Preliminary data show that state April 2020 revenues may be down 20 percent to 50 percent from April last year and down significantly relative to pre-pandemic projections. Drops in revenues coupled with increased demand for spending to address the public health emergency is generating budget shortfalls across states. A CBO letter to the Chair of the House Budget Committee affirms that without further funding from the federal government, states will need to increase taxes or reduce spending as a result of the pandemic and these actions would result in lower spending and higher job loss.
During economic downturns, enrollment and spending in Medicaid grow. During downturns, more individuals lose jobs and income and enroll in Medicaid. While demand for Medicaid and other services typically increases during downturns, state revenues generally fall. For example, during the Great recession, the unemployment rate peaked at 10 percent in October 2009 and Medicaid spending and enrollment growth peaked at 7.6 percent and 7.8 percent, respectively, in 2009 as well. At that time, a temporary increase in the Medicaid FMAP rate was used to provide rapid fiscal relief to states. This approach leveraged Medicaid’s existing financing structure to provide federal funds to states more quickly and efficiently than establishing a new program or allocating money from a new funding stream. It also reduced the need for states to cut Medicaid spending to fill state budget gaps and included MOE provisions for states to be eligible for enhanced match. Because Medicaid is funded from a combination of federal and state funds, states need to make substantial cuts to Medicaid to generate state savings. For example, for a state with a 50 percent match rate, a $100 cut to Medicaid will reduce state spending by $50 and federal spending by $50. However, for the ACA expansion population, a $100 reduction will yield only $10 in state savings and reduce federal spending by $90 (as the federal match rate is set at 90 percent for newly eligible expansion adults).
The Families First Coronavirus Response Act, amended by the Coronavirus Aid, Relief, and Economic Security (CARES) Act, authorizes a 6.2 percentage point increase in federal Medicaid matching funds to help states respond to the COVID-19 pandemic. The additional funds are available to states from January 1, 2020 through the quarter in which the public health emergency period ends, provided that states meet certain conditions. The HHS Secretary declared COVID-19 a nationwide public health emergency on January 31, 2020, retroactive to January 27, 2020. The public health emergency ends when the Secretary declares that the emergency no longer exists or after 90 days, whichever happens first, although the Secretary can renew the public health emergency declaration for subsequent periods. The public health emergency was extended on April 26 for another 90 days. Increased federal matching funds support states in responding to the increased need for services, such as testing and treatment during the COVID-19 public health emergency, as well as increased enrollment as more people lose income and qualify for Medicaid during the economic downturn.
States must meet five maintenance of eligibility (MOE) conditions that ensure continued coverage for current enrollees to receive the enhanced federal matching funds during the COVID-19 public health emergency. States must apply Medicaid eligibility standards, methodologies, and procedures that are no more restrictive, and states cannot increase premiums relative to what was in effect on January 1, 2020. States also must cover coronavirus testing and COVID-19 treatment, including vaccines, specialized equipment, and therapies, without cost-sharing while they receive the increased funds. States also cannot increase political subdivisions’ contributions to the non-federal share of Medicaid costs beyond what was required on March 11, 2020. Finally, states must provide continuous eligibility through the end of the month in which the public health emergency ends for those enrolled as of March 18, 2020 unless the person ceases to be a state resident, becomes deceased, or requests a voluntary coverage termination. Medicaid eligibility during this time must continue “regardless of any changes in circumstances or redeterminations at scheduled renewals that would otherwise result in termination.” Recent guidance from CMS states that, under the MOE, states that accept the FMAP increase cannot increase cost-sharing.
Key Findings
Enrollment Trends
Compared to pre-pandemic estimates, nearly all states with projections anticipate higher enrollment growth in FY 2020 and continued growth into FY 2021. We asked states about their current projections for monthly Medicaid enrollment for May 2020 relative to projections made prior to the pandemic as well as the direction and drivers of enrollment into FY 2021. Not surprisingly, nearly all states with projections (32 of 34) anticipate that current FY 2020 enrollment growth will exceed pre-pandemic enrollment projections and 30 of 31 states anticipate that enrollment growth in FY 2021 will outpace the current fiscal year.
States attribute higher enrollment projections in FY 2020 and FY 2021 to the worsening economy and the effects of the MOE. The effects of the economy in recent months and expectations that these conditions will get worse were major factors in state enrollment projections. In addition, states reported that the MOE was also a factor. MOE requirements eliminate the usual enrollment churn that occurs when some individuals lose eligibility and are dis-enrolled from Medicaid each month. However, even when states can resume eligibility redeterminations, given the magnitude of the economic crisis, many individuals are likely to retain eligibility because their income will continue to fall below Medicaid income eligibility thresholds. In the past, some eligibility churn was attributable to individuals losing coverage due to barriers maintaining coverage at renewal or when states conducted periodic data matches between renewals. Prior to the pandemic, these types of barriers were potentially depressing enrollment for some individuals who remained eligible. Beyond the conditions to access the enhanced funding, some states are implementing actions to expand eligibility and make it easier to apply such as allowing for self-attestation of eligibility criteria, eliminating premiums, expanding the use of presumptive eligibility, or otherwise simplifying application processes.
Spending Trends
Over half of states with projections anticipate that FY 2020 spending growth will be higher than spending growth projections made prior to the pandemic. Similar to other health care payers, the spending picture for Medicaid for the remainder of FY 2020 is somewhat mixed. Over half of states with projections (18 of 32) expect FY 2020 total Medicaid spending to exceed pre-pandemic projections while eight states anticipate no material change. The remaining six states expect somewhat lower spending in FY 2020 due to public health emergency restrictions halting non-urgent services and otherwise resulting in lower utilization of health care services. Some states with managed care noted that without adjustments in capitation rates, reductions in utilization will not reduce overall costs while increases in enrollment will continue to drive expenditures up. Without available claims data to review, many states could not anticipate how lower costs attributable to lower utilization would compare to costs related to increased enrollment and new/unanticipated expenditures related to COVID testing and treatment.
States also reported policy actions to expand access to services and increase payment rates for selected providers. Some states pointed to actions that could put upward pressure on spending and potentially offset expenditure reductions due to decreased utilization. Such actions include waiving copayments and prior authorization requirements, allowing early pharmacy refills, expanded telehealth services and reimbursement rates, and increasing provider rates particularly for hospitals, nursing facilities, and other long-term services providers. Examples of reimbursement adjustments include bumps for COVID-positive nursing facility residents or a hospital DRG add-on of 20 percent for COVID-19 positive enrollees.
For FY 2021, nearly all states with projections (29 of 30) anticipate that total Medicaid spending rates will continue to increase over FY 2020 spending rates, primarily due to increases in enrollment. In addition, states anticipate upticks in utilization for new enrollees and previously enrolled individuals (catch-up for depressed utilization in FY 2020) and pressure to address provider reimbursement issues will contribute to expenditure growth in FY 2021. A few states also pointed to the expected continuation of telehealth expenditures. While not asked about projections beyond FY 2021, at least one state commented that economic impacts and higher enrollment growth will likely continue beyond FY 2021.
Expected Budget Shortfall
Four in ten states with projections (13 of 33) reported currently projecting a Medicaid budget shortfall for FY 2020. A few states said that the combination of a supplemental appropriation and the additional federal support from the FMAP increase will help to address potential Medicaid budget shortfalls in FY 2020. However, a number of states reported that FY 2020 budgets were still in flux and broader reductions in overall state revenues may require reductions in Medicaid and other state programs. At least one state reported administrative reductions like hiring freezes and deferment of non-essential contracts.
Among the states with projections available, nearly all reported a budget shortfall is “almost certain” or “likely” for FY 2021 (17 of 19 states). Two other states reported a “50-50” chance of a Medicaid budget shortfall for FY 2021. No states reported that that a FY 2021 budget shortfall was “not likely” or “almost certain no shortfall.”
Looking Ahead
The FFCRA temporary FMAP increase has already provided fiscal relief to states facing mounting budget pressures from the pandemic. Enhancing that relief by further increasing the temporary FMAP rate and extending its duration could provide greater fiscal stability to states and support the costs of growing increases in enrollment as the economy worsens, at increased federal cost. Multiple state groups including the National Governors Association and the National Association of State Medicaid Directors have called for a further increase in the FMAP. The House bill introduced on May 12, 2020 would increase the FMAP by 14 percentage points from July 1, 2020 through June 30, 2021. Without certainty of additional federal support, many states will need to develop balanced budgets for the fiscal year beginning on July 1 (for most states) that could likely include significant spending cuts, including for Medicaid programs, at a time when demand for services is growing. We will continue to track state changes to Medicaid in response to the pandemic and will be fielding a more detailed survey of Medicaid programs this summer to capture assumptions about Medicaid spending and enrollment as well as policy changes that were included in state fiscal year (FY) 2021 budgets.
The COVID-19 emergency presents significant risks for the over 5 million individuals who self-identify as American Indian and Alaska Native (AIAN) alone or in combination with another race. AIAN people live across the country, but are concentrated in certain states, with roughly half living in seven states (CA, OK, AZ, TX, NM, WA, and NY). Under treaties and laws, the federal government has a unique responsibility to provide health care services to AIAN people. AIAN people face disproportionate risks from the COVID-19 outbreak given significant underlying disparities in health, social, and economic factors. Addressing their needs as part of COVID-19 response efforts will be key for preventing further widening of these disparities and fulfilling the federal government’s federal trust responsibility.
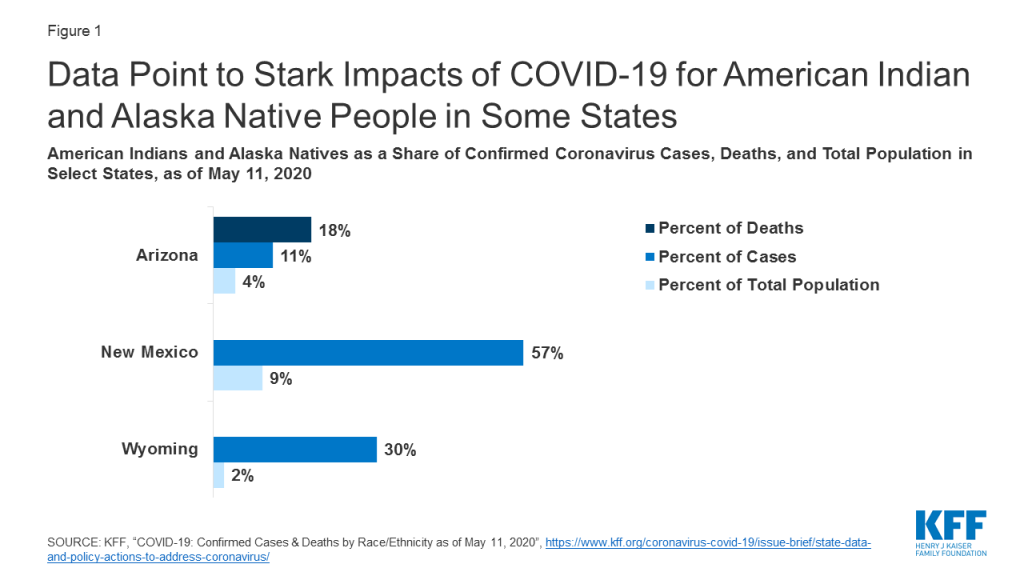
Data point to stark impacts of COVID-19 for AIAN people in some states. For example, as of May 11th, AIAN people made up 18% of deaths and 11% of cases compared to 4% of the total population in Arizona, 57% of cases compared to 9% of the total population in New Mexico, and 30% of cases compared to 2% of the total population in Wyoming, and (Figure 1). As of May 10th, the Indian Health Service (IHS) reported nearly 5,500 positive cases from IHS, Tribal, and urban Indian facilities, including over 3,300 among the Navajo Nation, which spans Arizona, New Mexico, and Utah.
Figure 1: Data Point to Stark Impacts of COVID-19 for American Indian and Alaska Native People in Some States
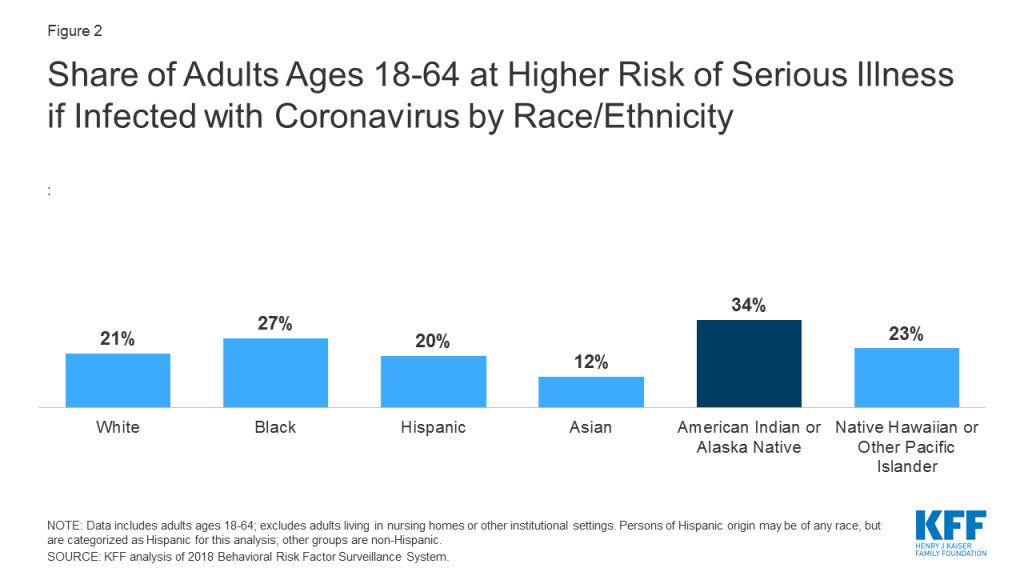
Coronavirus presents significant health risks for AIAN people because they face large underlying health disparities. AIAN people have disproportionately high rates of many health conditions that may put them at higher risk for serious illness if they contract coronavirus, including diabetes, heart disease, asthma, and obesity. Analysis examining how many adults are at higher risk for experiencing serious illness if they are infected with coronavirus based on CDC’s identified health risk factors finds that 34% of AIAN nonelderly adults are at risk of serious illness compared to 21% of White nonelderly adults (Figure 2). Living conditions also put AIAN people at increased risk for exposure to the disease. For example, compared to other groups, AIAN individuals are more likely to lack access to clean water and plumbing and to live in substandard and crowded housing situations, limiting the ability to practice frequent hand washing and social distancing.
Figure 2: Share of Adults Ages 18-64 at Higher Risk of Serious Illness if Infected with Coronavirus by Race/Ethnicity
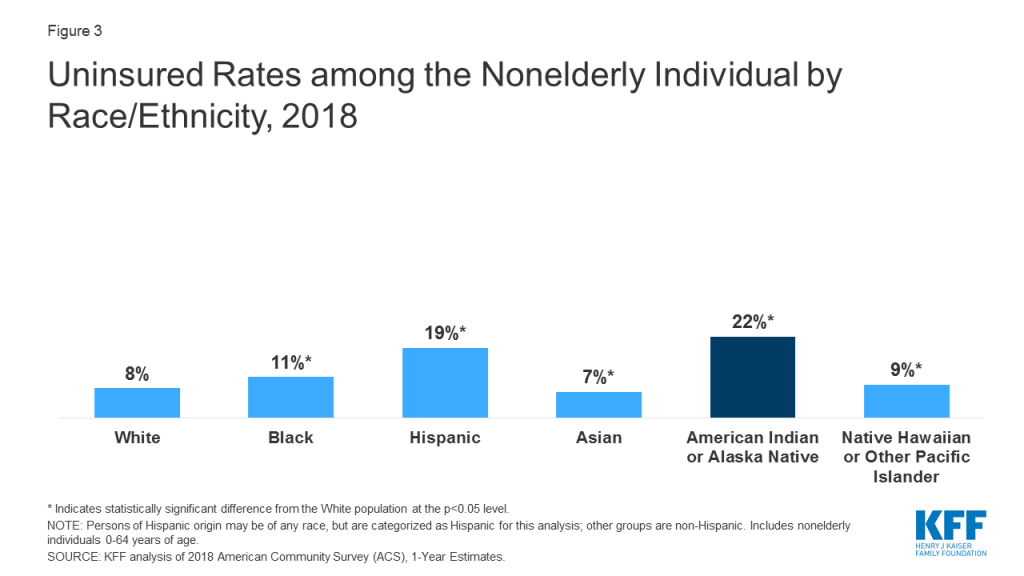
AIAN people face barriers to health care that may make it challenging to obtain coronavirus testing and treatment services. IHS is the primary vehicle through which the federal government fulfills its responsibility to provide health care services to AIAN people. However, IHS historically has been underfunded to meet their health care needs. Moreover, not all individuals who identify as AIAN are able to access services through IHS. IHS services generally are limited to members of or descendants of members of federally recognized Tribes. However, not all individuals who self-identify as AIAN belong to a federally recognized Tribe. Further, while many AIAN people live in rural areas, the majority live outside of Tribal areas, which can make it challenging to access an IHS provider. Give the limitations of IHS, Medicaid and other sources of health insurance remain important for expanding access to care for AIAN people. They also provide revenue that enhances capacity at IHS and Tribal facilities. However, as of 2018, 22% of AIAN nonelderly people were uninsured, the highest of all racial and ethnic groups (Figure 3). Reflecting the limitations of IHS and the high uninsured rate for AIAN people, they face increased challenges accessing care. For example, AIAN nonelderly adults are more likely compared to their White counterparts to have not seen a doctor in the past year due to cost (19% vs. 13%) and to have delayed care for other reasons (36% vs. 19%).
Figure 3: Uninsured Rates among the Nonelderly Individual by Race/Ethnicity, 2018
Coronavirus also may lead to disproportionate financial challenges for AIAN people. Over one in four (26%) nonelderly AIAN people have income below poverty, leaving them with limited ability to absorb income decreases that may result from the COVID-19 crisis. In addition, Tribes have lost key sources of revenue to support operations and services due to the halting of businesses and services in response to social distancing policies.
Addressing the needs of AIAN people as part of COVID-19 response efforts will be key to prevent further widening of their already large health and economic disparities and fulfilling the federal trust responsibility provide health care to AIAN people. The federal government has provided relief and support for federally recognized Tribes and Tribal business entities through the Coronavirus Aid Relief and Economic Security Act, including roughly $1 billion in additional IHS funding. Looking ahead, it will be important to assess the extent to which resources are adequate to address the needs of AIAN people and communities, including providing access to testing and treatment, support for health care providers, resources to mitigate risks associated with living conditions, culturally appropriate outreach and education, and financial relief. Moreover, comprehensive data will be key for understanding how the COVID-19 outbreak is affecting AIAN people, directing resources to meet needs, and measuring effects of response and relief efforts.