KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Since the COVID-19 pandemic first surfaced in the United States, the number of cases and deaths in long-term care (LTC) facilities has been rising. As of August 20, 2020, over 70,000 COVID-19 related resident and staff deaths have been reported in nursing homes and other long-term care facilities, which is a conservative estimate because not all states publish these data. The increase in deaths among long-term care facility residents and staff has become an urgent concern for federal and state policymakers, the long-term care industry, family members of residents, residents themselves, and the general public.
While COVID-19 outbreaks and deaths in nursing homes have received a fair amount of attention, assisted living facilities (ALFs), which are home to over 800,000 mostly frail, elderly residents, have been largely overlooked. Unlike nursing homes, assisted living facilities are not federally regulated, leaving states to decide whether or not to publicly report data or to impose restrictions to protect residents. This analysis examines the impact of COVID-19 on assisted living facilities as well as changes over time, using state-level data on COVID-19 cases and deaths reported in early June 2020, and again in early August. These counts are a subset of the state-level COVID-19 cases and deaths in all long-term care facilities, including nursing homes, as reported in other KFF analyses. (See Methods for details).
Less Than Half of All States Report COVID-19 Cases in Assisted Living Facilities and Even Fewer Report Deaths
As of August 2020, 19 states identify COVID-19 cases or deaths specific to assisted living facilities, an increase of four states since June 2020. Of these 19 states, 13 [CO, CT, FL, KY, MA, NV, ND, OH, PA, RI, TN, TX, UT] report COVID-19 data for assisted living facilities in its own, distinct category, and 6 [CA, GA, LA, NC, NY, SC] report COVID-19 data for assisted living facilities along with congregate settings other than nursing homes (Tables 1 and 2). This leaves 31 states and DC that do not identify COVID-19 cases and deaths occurring in assisted living facilities specifically, as of August 2020.
18 of the 19 states report COVID-19 cases in assisted living facilities: As of August 2020, 18 states report COVID-19 cases in assisted living facilities, either in its own distinct category (13 states) or combined with other congregate, non-nursing facilities (5 states), and report either cumulatively (13 states) or active cases only (5 states). Of these 18 states, 14 report cases among residents and staff separately, 2 report cases among residents and staff combined, and 2 report cases among residents only.
14 of the 19 states report COVID-19 deaths in assisted living facilities: As of August 2020, 14 states report COVID-19 deaths in assisted living facilities, either in its own distinct category (8 states) or combined with other congregate settings other than nursing homes (6 states), and report either cumulatively (12 states) or only among facilities with ongoing outbreaks (2 states). Of these 14 states, 7 report deaths among residents and staff separately, and 7 states report deaths among residents only
COVID-19 Cases and Deaths in Assisted Living Facilities Have Increased, With a Notable Increase in Cases Among Staff
CASES:As of early August 2020, a total of 22,080 COVID-19 cases have been reported among residents and staff in assisted living facilities, based on the 18 states reporting COVID-19 cases data. This total reflects both the number of cases among 14 states that were reporting this information in June and the addition of 4 states that started reporting since then. Among the 14 states that reported COVID-19 cases in both June and August, the number of cases among residents and staff has increased by 66% and the number of cases among residents only has increased by 63%. This is an undercount because it is based on data reported by a minority of states.
As of early August 2020, a total of 7,626 cases were reported among assisted living staff in the 14 states reporting staff cases, including 6 states that started reporting since June. Among the 8 states that reported in both June and August, the number of staff cases has increased by 156% from 2,085 to 5,333 cases in early August.
DEATHS: As of early August 2020, a total of 2,651 deaths among residents and staff have been reported in the 14 states that identify COVID-19 deaths specific to assisted living facilities, including the 10 states that reported deaths in both June and August, and 4 states that started reporting since June. Among the 10 states that reported deaths in both June and August, the total number of deaths increased by 59% from 1,483 to 2,356 deaths in early August. The majority of reported COVID-19 deaths are among assisted living facility residents (2,257); a relatively small number represent deaths among staff (99).
As of early August 2020, a total of 99 deaths were reported among assisted living staff in the 7 states reporting staff deaths, including 2 states that started reporting since June. Among the 5 states that reported in both June and August, the number of deaths has increased by 219% from 31 to 99 deaths in early August.
In the 10 states reporting cumulative COVID-19 CASE numbers for assisted living facilities in both June and August, the percentage increase in the aggregate number of COVID-19 cases in the population overall was significantly greater than the percentage increase in aggregate resident and staff cases in ALFs (223% versus 61%). But the opposite is true in the states reporting cumulative deaths in assisted living facilities. In the nine states reporting cumulative DEATH data for assisted living facilities separately from nursing homes, the aggregate percentage increase in COVID-19 deaths occurring in the overall population in these states was roughly half of the increase in resident and staff deaths occurring in ALFs between June and August (36% vs. 60%).
Discussion
Despite intense scrutiny of the number of COVID-19 cases and deaths in nursing facility settings, less than half of all states are reporting data for COVID-19 in assisted living facilities specifically. As a result, it is difficult to know the extent to which residents and staff in assisted living facilities have been affected by COVID-19 or the extent to which interventions are urgently needed. Our analysis finds a significant increase in COVID-19 cases and deaths among residents and staff in assisted living facilities in the two-month period between June and August. The rise in cases among staff is especially noteworthy. Notably, four out of five states [CA, FL, NV, SC] with the largest increase in cases among staff are also considered “hotspot” states with widespread community transmission. The rise in COVID-19 cases among staff is most likely to disproportionately affect female, Black, and low-wage workers, based on a recent analysis.
Since COVID-19 data for assisted living facilities are reported separately from nursing facilities by a minority of states, the counts of cases and deaths presented in this analysis are undoubtedly conservative. Compounding this data limitation, states that do report for assisted living facilities separately from nursing homes vary significantly in what they report: some states report cases, but not deaths, and some do not report cases or deaths among staff. In fact, only seven states separately report deaths among staff working in assisted living facilities. Additionally, while some states (e.g., NY, LA) have been reporting cumulative case and death data dating back to early March, others do not specify the start date of their retrospective data reporting, leading to potential undercounts of cases and deaths that have occurred since the beginning of the pandemic. The reporting of active cases only by some states (such as Florida) is likely to result in an undercount of the true magnitude of cases and deaths since the numbers do not take into account cases and deaths that may have occurred but are no longer active.
Overall, the incomplete system of state-level reporting of COVID-19 data in assisted living facilities results in an incomplete picture of disease incidence and mortality among staff and residents in these facilities. Based on data from the states that do report, outbreaks in assisted living facilities, and protections for residents and staff, warrant more careful attention.
Tables
Table 1:
–
Methods
To collect data on COVID-19 cases and deaths in ALFs, we reviewed public reporting of COVID-19 surveillance data displayed on applicable state-run websites in all states, and collected numbers of cases and deaths for ALFs in states where this data is reported separately from cases and deaths in LTC facilities generally, in order to exclude nursing facilities from our analysis. Not all states report COVID-19 data for LTC facilities, and some only report this data for nursing homes. For this analysis, we collected state data on COVID-19 cases and deaths between June 5 and June 8, 2020, and between August 3 and August 6, 2020.
We included COVID-19 case and death data for each state (n=13) that reported for ALFs specifically, as well as other states (n=6) that report ALF data separately from nursing facilities, but do so within a larger category that includes ALFs along with other non-nursing home facility types, such as residential care facilities, personal care homes, and adult care facilities. We included these congregate facilities because assisted living facilities represent a large share of their total residents in many states. We intentionally excluded states reporting in broader categories that include nursing homes because these numbers are reported to CMS separately and our goal is to understand the impact of COVID-19 in assisted living facilities to the extent this is possible with current data limitations.
In order to compare increases in COVID-19 cases and deaths overall to increases in cases and deaths occurring in ALFs over the study period, we calculated the percent increases in cases and deaths occurring between June 8 and August 6, 2020 in the 11 states reporting cumulative ALF data in both the beginning and end of the study period, using the state data section of the KFF COVID-19 Coronavirus Tracker.
Notably, states vary widely in reporting data for cases and deaths. Among the 18 states that report ALF cases, 2 states report aggregate cases for residents and staff, 14 states report cases for residents and staff separately, and 2 states report cases for residents only. Among the 14 states that report ALF deaths, 7 states report deaths for residents and staff separately and 7 states report deaths for residents only. Since June, Connecticut and Texas, which were previously reporting cases and deaths for residents only, are now reporting staff cases, but not staff deaths (Texas) and cases and deaths for residents and staff separately (Connecticut). Most states in our analysis (n=14) report cumulative case and death data, however five states (Florida, North Carolina, North Dakota, Tennessee, Utah) report only active cases, which may lead to a significant undercount of cases and deaths that are no longer active. Within the two-month period, North Carolina switched from reporting cumulative cases to active cases.
States differ slightly in how many cases constitute a facility “outbreak” which triggers reporting – some states report data for facilities with just one active case, others begin reporting when two or more cases are reported by facilities. States also differ in whether they report suspected COVID-19 cases and deaths, in addition to confirmed cases – some only report cases confirmed via diagnostic test. For the purpose of this analysis, we have included both suspected and confirmed COVID-19 cases and deaths reported. Additionally, four states (Massachusetts, Rhode Island, Utah, and California) report ranges of cases and/or deaths, versus specific counts. For these states, we used the median of the reported range, or 5 in the case of “5 or above” reported, and 31 for “greater than 30”.
Long-term care (LTC) facilities have experienced a disproportionate share of deaths during the COVID-19 pandemic. The most recently available data show long-term care facilities making up 8% of all coronavirus cases, but more than 40% of all COVID-19 deaths. This analysis evaluates trends of long-term care cases and deaths between April and August 2020 to evaluate where and when the pandemic has hit long-term care facilities the hardest, how the share of cases and deaths attributed to long-term care facilities has changed over time, and whether states continue to report new cases and deaths in these facilities at the same rate now as they did back in April.
This analysis presents trends in long-term care data for states that have reported long-term care cases (35 states) and deaths (36 states) since early April 2020 (see methods and limitations for more details). Federally available, facility-specific data was not used for this analysis because facilities were not required to begin reporting until May 8, which would miss peaks in cases and deaths in April and May. Key findings from our analysis include:
Nationally, reported cumulative cases and deaths in long-term care facilities have increased over time, increasing from 10,000 deaths and 50,000 cases in mid-April to over 70,000 deaths and nearly 400,000 cases in mid-August. However, trends in cases and deaths vary notably across states. (Interactives 1 and 2). Some states, such as New York and Massachusetts, experienced a surge of long-term care cases and deaths that peaked and plateaued much earlier than other states where long-term cases and deaths were first reported in later months and have continued to climb, such as Texas and North Carolina (Interactives 1 and 2).
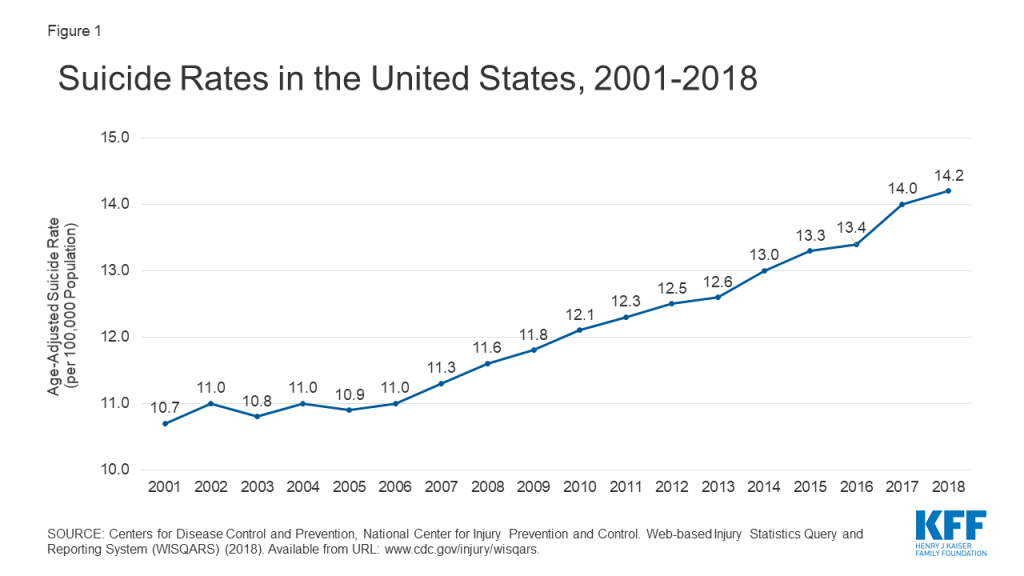
Nationally, the share of deaths attributed to LTC facilities has stayed relatively constant since May, but the share of cases attributed to LTC facilities has decreased over time (Figures 1 and 2). The decreasing share of cases attributed to long-term care facilities is likely due broader availability of testing that contributed to the identification of more cases in the general population, particularly in younger age groups, in June and July.
Nationally, the number of new LTC cases and deaths peaked in April, decreased in May and June, before rising in July, followed by a rise in new LTC deaths in August (Figure 3 and Table 2). These patterns of new LTC cases and deaths generally follow the patterns of cases and deaths that we have seen nationally, indicating a strong connection between community spread with cases and deaths in long-term care facilities. Recent analysis on cases in hotspot states supports this notion as well. A key distinction here is the number of new LTC cases per 100,000 residents in July and August was much lower than new LTC cases in April and May, which differs from the national pattern where new cases in the summer months were higher than new cases in April and May. (Figure 3).
Issue Brief
1. How do trends in total cases and deaths in long-term care facilities vary by state?
Total cases and deaths in long-term care facilities have increased over time, with notable differences across states (Interactives 1 and 2). Examining visual trend lines in cumulative cases and deaths since April indicates that there are some states, such as New York, Massachusetts, New Jersey, and Connecticut, that have “flattened the curve”, while other states, such as California, Texas, Georgia, and Ohio, have continued to see a rise in long-term care cases and deaths (Interactives 1 and 2).
As of August 20th, states with the highest burden of COVID-19 long-term care cases and deaths per 100,000 state residents were among those that experienced the earliest peaks in both long-term care and overall cases and deaths (Table 1). New Jersey, Massachusetts, Louisiana, Rhode Island, and Connecticut had the highest burden of cases and deaths in LTC facilities per 100,000 state residents (>250 cases per 100,000 residents and >40 deaths per 100,000 residents) among all states that report data. With the exception of Louisiana, these states were also among the states that experienced relatively large numbers of long-term care cases and deaths in the earlier months of the pandemic (Interactives 1 and 2, Table 2).
In contrast, while long-term care cases and deaths in states like California and Texas continued to rise into the summer months, after other states had flattened their curve (Interactives 1 and 2, Table 2), these states experienced a smaller number of long-term care cases and deaths per 100,000 residents (11-12 deaths and 118 cases per 100,000 state residents) than states that peaked in March/April (>40 deaths and >250 cases per 100,000 state residents) (Table 1). With the number of cases and deaths in these states continuing to rise, it will be important to re-assess the extent to which this finding holds over time.
Interactive 1:
–
Interactive 2:
–
2. How has the national share of deaths and cases attributed to long-term care facilities changed over time?
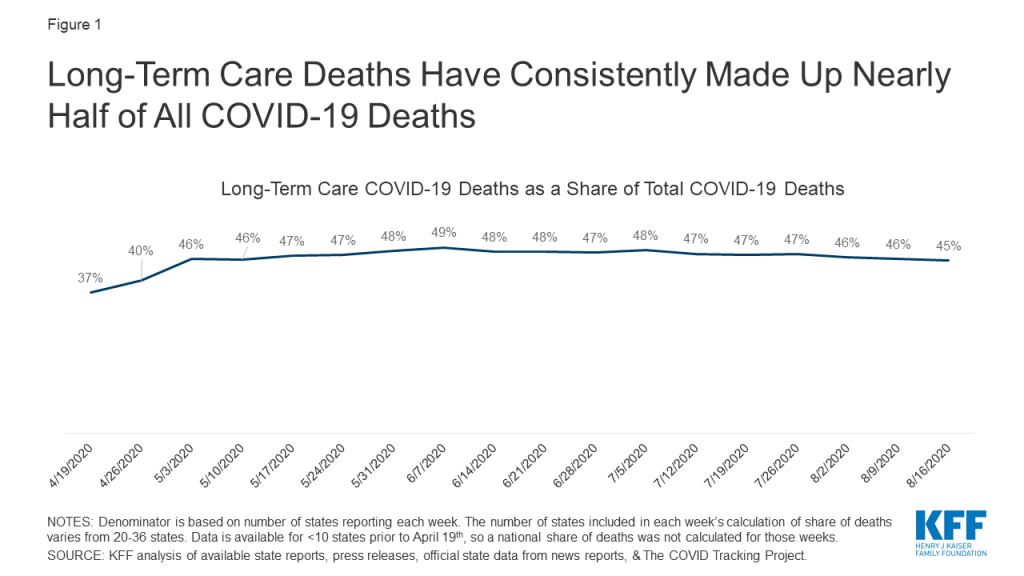
Nationally, the share of deaths attributed to long-term care facilities has stayed relatively constant over time (Figure 1). The share of reported deaths attributed to long-term care facilities increased from 37% the week of April 19th to 46% the week of May 3rd and has stayed relatively constant since then. The increase in share of deaths attributed to LTC facilities from April to May may be attributed to better reporting (Figure 1). Notably, 7 additional states started reporting data on deaths between the week of April 19th and the week of May 3rd.
Figure 1: Long-Term Care Deaths Have Consistently Made Up Nearly Half of All COVID-19 Deaths
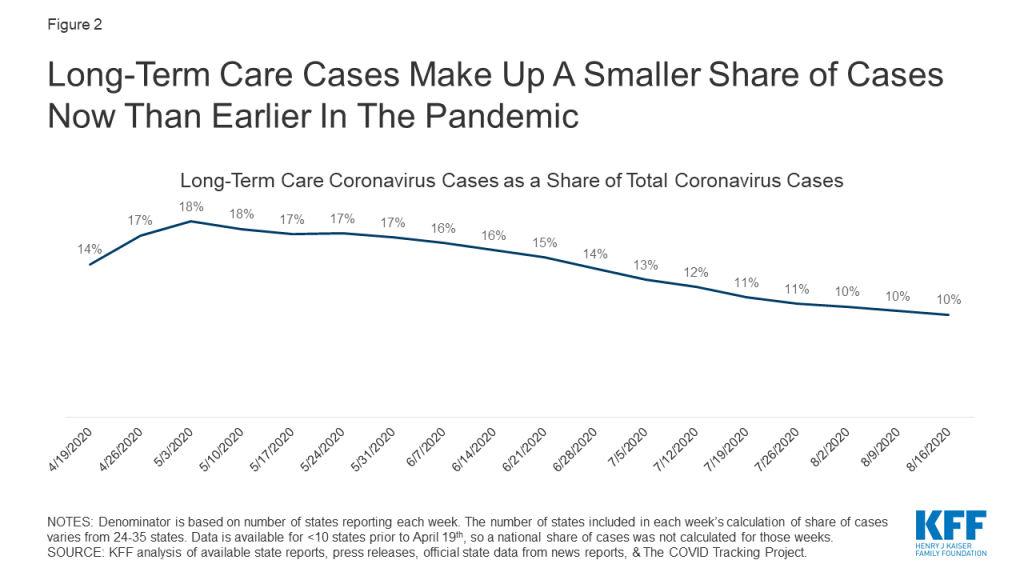
In contrast, the share of cases attributed to long-term care facilities has decreased over time. When long-term care data began to be reported by more states in mid-April, 1 in every 7 coronavirus cases was a long-term care facility resident or staff member. By the beginning of May, that share had increased to nearly 1 of every 5 cases. However, since then, the share of cases attributed to residents and staff in long-term care facilities has decreased. The most recent data from mid-August show that 1 in every 10 cases is a long-term care facility case (Figure 2). This decrease can likely be attributed to an increase in testing of the general population, most likely due to the increased community transmission that occurred in June and July.These new cases primarily skewed towards a younger population, so share of cases attributed to long-term care facilities has decreased.
Figure 2: Long-Term Care Cases Make Up A Smaller Share of Cases Now Than Earlier In The Pandemic
3. What has happened with new cases and deaths in long-term care facilities nationally and at the state-level?
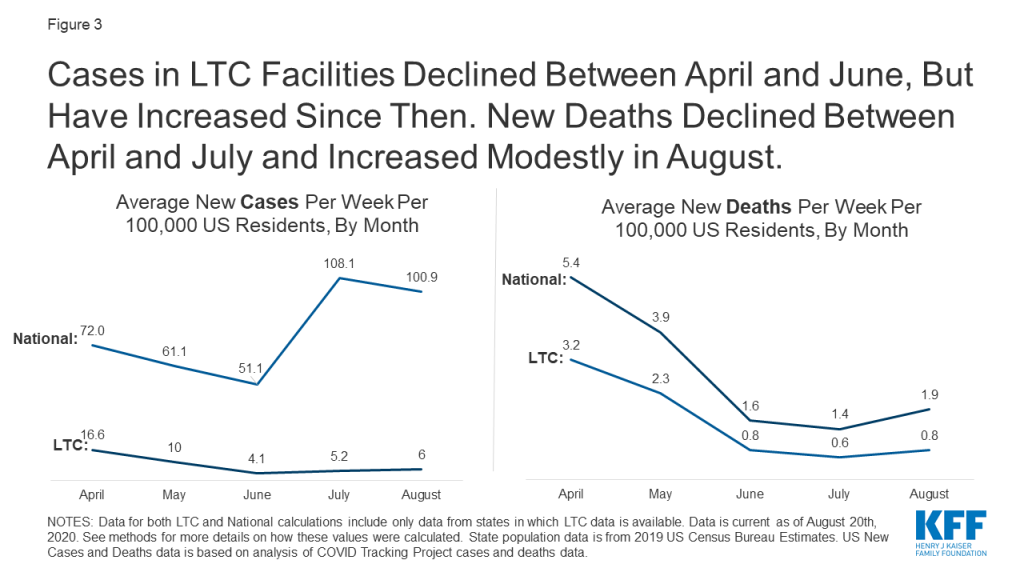
Nationally, new reported long-term care cases per week were the highest in April and decreased through May and June, before increasing again in July and August. (Figure 3 and Table 2). The number of new long-term care cases nationwide decreased from April to May (16.6 cases to 10.0 cases per 100,000 US residents) and again in June (4.1 cases per 100,000 US residents). However, beginning in July, new cases began to rise again (5.2 cases per 100,000 US residents) and again in August to 6.0 new long-term care cases per 100,000 US residents.
Figure 3: Cases in LTC Facilities Declined Between April and June, But Have Increased Since Then. New Deaths Declined Between April and July and Increased Modestly in August
New reported long-term care COVID-19 deaths per week were the highest in April, decreased through May, June, and July, before increasing modestly in August (Figure 3 and Table 2). New weekly long-term care deaths decreased from April to May (3.2 deaths to 2.3 deaths per 100,000 US residents), to June (0.8 deaths per 100,000 US residents), to July (to 0.6 deaths per 100,000 US residents) before increasing slightly in August to 0.8 deaths per 100,000 US residents.
The number of new LTC cases and deaths per 100,000 US residents was overall lower in July and August than in April and May. This pattern of new LTC cases differs from national new case trends, while the pattern of new LTC deaths is similar to national new death trends (Figure 3 and Table 2). New LTC outbreaks were more severe in the earliest months of the outbreak (primarily in the Northeast) than in more recent months, based on the lower number of new LTC cases and deaths per week (Figure 3 and Table 2). This pattern mirrors new deaths nationally, but is in contrast to national new case trends where, new cases in the general population were higher in July and August than in April and May (Figure 3). It is important to continue to track new LTC cases and deaths in the coming months to understand if we are at the beginning of a continued increase in new LTC cases and deaths that will outpace the rate of new cases and deaths identified in April and May.
Trends in long-term care facilities may mirror trends in community outbreaks, but may also be affected by measures that have been put in place to mitigate the impact of the pandemic on residents and staff. Trends of new cases and deaths, as well as recent analysis of cases and deaths by hotspot state status, support the idea that increased community transmission plays a role in increasing cases and deaths in long-term care facilities. However, nationally, long-term care facilities have seen less severe outbreaks now than they did earlier in the pandemic. While the severity of long-term care cases and outbreaks have decreased, potentially as a result of policies restricting visitors, implementing universal testing of staff and residents, and greater social distancing in communities, it will be important to look at burden of cases/deaths and new cases/deaths again if states experience a rise in cases and deaths in the community.
Tables
Table 1: Long-Term Care Coronavirus Cases and Deaths Per 100,000 Residents As of August 20th, 2020
State
Long-Term Care Cases Per 100,000US and State Residents
Long-Term Care Deaths Per 100,000US and State Residents
US TOTAL
128 cases per 100,000 US residents(35 states)
23 cases per 100,000 US residents(36 states)
Alabama
148 per 100,00 State Residents
N/A
Arkansas
42
N/A
California
118
12 per 100,000 State Residents
Colorado
88
13
Connecticut
287
91
Delaware
127
37
District of Columbia
147
24
Florida
N/A
19
Georgia
170
19
Idaho
105
10
Illinois
208
34
Indiana
148
27
Iowa
N/A
17
Kansas
57
7
Kentucky
112
12
Louisiana
319
42
Maryland
244
35
Massachusetts
356
82
Michigan
123
21
Minnesota
74
23
Mississippi
154
31
Nevada
78
7
New Jersey
425
79
New York
N/A
34
North Carolina
103
12
North Dakota
N/A
9
Ohio
138
22
Oklahoma
73
7
Oregon
43
5
Pennsylvania
194
40
Rhode Island
280
76
South Carolina
127
18
Tennessee
74
6
Texas
118
11
Utah
66
5
Vermont
38
N/A
Virginia
105
15
Washington
82
13
Wisconsin
28
7
NOTES: All state data is “per 100,000 State Residents”. See methods for more details on how these values were calculated. State population data is from 2019 US Census Bureau Estimates.
Table 2: Average New LTC Cases and Deaths Per Week Per 100,000 Residents, By Month
State
Average New Cases Per Week Per 100,000US and State Residents
Average New Deaths Per Week Per 100,000US and State Residents
April
May
June
July
August
April
May
June
July
August
US TOTAL
16.6(24 states)
10.0(31 states)
4.1(35 states)
5.2(35 states)
6.0(34 states)
3.2(20 states)
2.3(31 states)
0.8(36 states)
0.6(36 states)
0.8(35 states)
Alabama
5.7
7.3
7.3
8.4
9.6
Arkansas
1.3
1.4
2.7
4.3
California
8.8
7.1
3.6
8.7
7.9
0.8
0.5
0.7
0.5
Colorado
9.7
6.2
1.6
1.1
1.2
1.1
1.0
0.4
0.2
0.1
Connecticut
52.8
22.9
2.9
1.8
0.8
12.3
9.1
1.7
0.8
0.1
Delaware
7.7
13.7
6.0
1.0
1.5
2.4
3.0
2.3
0.9
0.1
District of Columbia
9.4
16.8
4.3
1.9
1.6
4.0
3.4
0.3
0.2
Florida
0.8
0.8
0.7
1.0
2.1
Georgia
12.0
7.5
4.4
9.4
11.4
1.1
1.1
0.5
0.8
1.3
Idaho
2.1
9.1
14.8
0.1
0.7
1.2
Illinois
22.5
17.8
7.9
4.0
4.0
3.1
3.3
1.4
0.6
0.5
Indiana
8.6
3.7
15.1
2.8
2.0
0.8
1.7
0.9
Iowa
1.2
0.7
0.7
0.8
Kansas
1.6
2.0
2.3
4.8
0.3
0.4
0.2
0.3
Kentucky
4.5
5.1
5.3
8.4
0.5
0.7
0.5
0.3
Louisiana
15.5
15.5
8.1
18.1
23.0
3.1
2.2
1.1
1.1
3.0
Maryland
16.9
11.2
5.0
4.9
2.9
2.2
0.5
0.3
Massachusetts
57.7
29.3
6.1
2.4
3.0
11.3
7.2
2.5
1.2
1.0
Michigan
1.9
1.8
3.0
0.2
0.4
0.3
Minnesota
5.2
7.3
2.3
0.9
2.9
2.1
1.1
0.4
0.5
Mississippi
8.0
8.3
5.8
7.1
11.7
0.9
2.1
1.0
1.6
2.3
Nevada
8.0
3.2
2.0
4.3
5.7
0.3
0.5
0.2
0.2
0.5
New Jersey
72.5
35.8
7.0
3.2
0.6
13.5
6.6
1.4
0.8
1.0
New York
0.8
2.7
0.3
0.2
0.1
North Carolina
4.7
4.3
3.5
5.1
10.0
0.7
0.7
0.5
0.3
1.0
North Dakota
0.2
0.3
0.3
Ohio
19.0
9.6
4.1
6.2
7.6
1.6
0.9
0.7
0.7
Oklahoma
5.2
3.3
1.5
3.3
5.4
0.5
0.5
0.1
0.2
0.4
Oregon
2.3
2.5
3.7
0.3
0.2
0.3
Pennsylvania
19.5
14.9
5.8
4.1
4.0
4.2
3.3
2.0
0.6
0.6
Rhode Island
36.9
24.4
5.3
1.2
2.6
2.9
8.3
3.6
0.7
0.2
South Carolina
5.0
5.8
2.8
9.7
12.0
0.6
0.7
0.5
1.4
1.9
Tennessee
2.7
1.9
0.9
3.7
13.5
0.2
0.3
0.1
0.1
0.9
Texas
1.4
2.0
16.1
9.9
0.2
0.2
0.9
1.3
Utah
2.1
3.6
5.9
3.8
0.2
0.2
0.5
0.4
Vermont
0.6
5.2
2.2
0.7
Virginia
4.9
8.6
5.3
3.3
3.8
0.4
1.7
0.8
0.3
0.4
Washington
2.5
2.5
3.8
0.4
0.3
0.6
Wisconsin
2.6
1.9
1.1
0.7
1.2
0.5
0.3
0.1
0.2
NOTES: National values are per 100,000 US residents. State values are per 100,000 state residents. Data is current as of August 20th, 2020. See methods for more details on how these values were calculated. State population data is from 2019 US Census Bureau Estimates.
Table 3: Variations in State Reporting of Long-Term Care Facility Cases and Deaths Related to COVID-19
State
What is reported?
Who is included in counts?
What types of long-term care facilities are included?
How often is/was data updated?
Additional State Data Notes
Alabama
Cases
Residents and Staff
Long-term care facilities
Daily
Arkansas
Cases and Deaths
Residents
Nursing Homes
Daily
Stopped updating number of cases at the end of July. Now only reports share of cases in nursing homes. Started reporting number of deaths in nursing homes at the beginning of August. Deaths are not included in this analysis due to short time period of availability.
California
Cases and Deaths
Residents and Staff
Nursing Homes, Residential Care Facilities for the Elderly, and Adult Residential Facilities (ARF)
Daily
4/23-5/14: Includes resident/staff cases/deaths in nursing homes5/19: Drop in cases from 9908 to 9869 because of exclusion of staff cases. Added other types of LTCF cases and deaths.5/25-present: Includes staff & other LTCFs.
Colorado
Cases and Deaths
Residents and Staff
Nursing Homes and Assisted Living Facilities
Weekly
Connecticut
Cases and Deaths
Residents and Staff
Nursing Homes and Assisted Living Facilities
Weekly
4/16: Cases and deaths in nursing home residents4/29: Added cases in assisted living facilities5/13: Added deaths in assisted living facilities7/14: Includes cumulative staff cases and deaths since 6/17 in NH and 7/1 in ALFs.7/21: Drop in cases from 10,166 to 10,1378/11: Number of facilities with outbreaks drops from 307 to 306
Delaware
Cases and Deaths
Residents
Long-term care facilities
Daily
Latest data on Staff cases/deaths is from June 26th – 461 staff cases and 1 staff death. Not included in counts due to inconsistent reporting of staff data.7/3: Drop in cases from 1,164 to 1,1547/10: Drop in deaths from 335 to 334 due to exclusion of resident who was found to be member of independent living facility
District of Columbia
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
6/9: Drop in deaths from 165 to 1578/20: Drop in cases from 1055 to 1034Previously, data was updated daily reports via spreadsheet. In recent weeks, data is updated more irregularly.
Florida
Deaths
Residents and Staff
Long-term care facilities
Daily
Only active cases are reported, so cumulative cases cannot be trended.
Georgia
Cases and Deaths
Residents and Staff
Nursing homes, Assisted Living Communities and Personal Care Homes
Daily
Idaho
Cases and Deaths
Residents and Staff
Nursing Home, Assisted Living Facility, or Intermediate Care Facility
Weekly
Illinois
Cases and Deaths
Residents and Staff
Long-term care facilities
Weekly
Indiana
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
4/26 – 7/19: Cases and deaths in residents in long-term care facilities from 4/26-7/197/26 – present: Staff cases and deaths added to counts
Iowa
Deaths
Residents and Staff
Long-term care facilities
Daily
Only active cases are reported, so cumulative cases cannot be trended.
Kansas
Cases and Deaths
Residents and Staff
Long-term care facilities
Previously reported data in summary PDF; now reports data as part of Cluster Summary dashboard
Kentucky
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
Louisiana
Cases and Deaths
Residents and Staff
Long-term care facilities
Weekly
3/29 – 5/10: nursing home resident cases/deaths5/18: staff cases added to countsLA also reports Adult Residential Care cases/deaths, but those are not reported consistently, so they are not included in this analysis to make trended data more reliable
Maryland
Cases and Deaths
Residents and Staff
Long-term care facilities
Weekly
Massachusetts
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
Michigan
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
Active cases only reported up till 6/14Deaths data fluctuates due to data reconciliation.
Minnesota
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
Mississippi
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
Nevada
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
New Jersey
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
New York
Deaths
Residents and Staff
Long-term care facilities
Daily
Deaths that occurred outside of facility are not counted. This excludes hospital deaths.
North Carolina
Cases and Deaths
Residents and Staff
Long-term care facilities
Multiple times per week
North Dakota
Deaths
Residents and Staff
Long-term care facilities
Daily
Only active cases are reported, so cumulative cases cannot be trended.
Ohio
Cases and Deaths
Residents and Staff
Long-term care facilities
Weekly
369 deaths reported prior to April 15th
Oklahoma
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
Oregon
Cases and Deaths
Residents and Staff
Care facilities, Senior living communities, and Congregate Living Settings
Weekly
Active cases, deaths, and outbreaks were reported until 6/21
Pennsylvania
Cases and Deaths
Residents and Staff
Nursing Homes and Personal Care Homes
Daily
Rhode Island
Cases and Deaths
Residents and Staff
Long-term care facilities
Weekly
South Carolina
Cases and Deaths
Residents and Staff
Long-term care facilities
Multiple times per week
Tennessee
Cases and Deaths
Residents and Staff
Long-term care facilities
6/12: cases and deaths drop from 1325 to 1055 and 155 to 1327/29: Aggregated & corrected data is reported, accounting for hike in cases & deaths
Texas
Cases and Deaths
Residents and Staff
Nursing Homes and Assisted Living Facilities
Daily
Staff cases are as of August 6th.
Utah
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
Vermont
Cases
Residents and Staff
Long-term care facilities
Weekly
7/22: Cases drop from 407 to 4057/29: Vermont began reporting congregate care/living settings separately from other outbreaks accounting for large drop in reported cases
Virginia
Cases and Deaths
Residents and Staff
Long-term care facilities
Daily
Washington
Cases and Deaths
Residents and Staff
Nursing Homes, Assisted Living Facilities, Adult Family Home
Weekly
7/12: Deaths drop from 820 to 815
Wisconsin
Cases and Deaths
Residents and Staff
Nursing Homes and Assisted Living Facilities
Daily
SOURCE: KFF analysis of available state reports, press releases, press conferences, official state data from news reports, and The COVID Tracking Project
Methods
This analysis is based on data from 38 states plus Washington DC, for a total of 39 states. Within these 39 states, we were able to trend long-term care cases in 35 states and long-term care deaths in 36 states. Data was trended as far back as internal records and publicly available historical data allowed. States were chosen based on where we could reliably trend data. States were excluded from this analysis if they do not report data on cases and deaths in long-term care facilities, if their data is sourced from sporadically released media reports, or if there were data quality issues. The 12 states excluded from the analysis were excluded for the following reasons:
Alaska, Arizona, Hawaii, Missouri, Montana, New Mexico, South Dakota – Not reporting cases and deaths in long-term care facilities
Maine, Nebraska, New Hampshire, Wyoming – Data on cases and deaths in long-term care facilities are sourced from sporadic media reports
West Virginia – State-reported data has severe data quality issues
For all states, we trended the subset of data that would give us the longest reliable trend line. Notable examples of this include Louisiana, where data from non-nursing home long-term care facilities were excluded because they were not consistently reported. In Delaware, data excludes staff cases because that data was not reported consistently. For this reason, this analysis should not be used to identify state-level or national data on total long-term care cases and deaths. The most recent data on total cases and deaths in long-term care facilities can be located here.
Table 1: Long-Term Care Coronavirus Cases and Deaths Per 100,000 US and State Residents As of August 20th, 2020
This table presents the burden of long-term care cases and deaths that each state has experienced as of August 20th, 2020. Total population data was taken from 2019 state population estimates from the US Census Bureau. The latest long-term care cases/deaths data available was used to calculate the burden of cases and deaths experienced by each state. National long-term care case burden was calculated by summing US population from 35 states that reported case data, dividing total cases by total population in those 35 states, and multiplying by 100,000 to find the value per 100,000 US residents. National long-term care deaths burden was calculated similarly by using data from 36 states that report LTC deaths.
Table 2: Average New LTC Cases and Deaths Per Week Per 100,000 US and State Residents, By Month
Total population data was taken from 2019 state population estimates from the US Census Bureau. The first week of available data for each state was not included in this analysis since the first week of data does not reflect a single week of cases/deaths, but rather all cases and deaths that have occurred up to that point. New cases and deaths were calculated for each week thereafter, and then averaged for all of the weeks within the month. April, June, and July reflect 4 weeks of data. May reflects 5 weeks of data. August reflects 3 weeks of data. These average new cases were converted to represent cases and deaths per 100,000 state residents to allow for easier comparison across states. National new cases and national new deaths were calculated by averaging new cases and new deaths across states. See limitations for more details on this process.
Limitations
There were several possible approaches to this analysis, all of which posed major limitations. This analysis could be limited to the time period where most major states are reporting, which would limit the time period of this analysis to mid-June to present day. However, this approach would miss the major peaks in states such as Massachusetts, Connecticut, and New Jersey. Another option was to limit the analysis to states where we had the earliest weeks of data available. However, this approach would exclude Texas, Michigan, Maryland, and several other states where data was not available until at least several weeks after other states began reporting. Deaths in the states that would have been excluded in this approach make up 30% of all long-term care deaths due to COVID-19. This analysis could have also used the federally reported data, but this would have limited the time period of analysis as well.
Due to data availability and quality issues, we were unable to include all states in this analysis. Thus, all national calculations in this analysis are subject to data availability. In particular, national calculations of new cases and deaths in Table 2 are limited by varying numbers of states included in each week and month, the differences in policies across states, and the lack of reporting comparability. However, given the data limitations, this is the best approximation of new cases and deaths per month.
We conducted a sensitivity analysis for the analysis in Table 2 to see how much using different states in each month affected both the raw Ns and the direction of the trend. Our sensitivity analysis found no notable differences. When looking at the same set of 23 states for new cases and 19 states for new deaths from April to August, we found similar trends as when looking at all available states in respective months. As mentioned above, this method excludes several major states, such as Texas, Michigan, and Maryland.
Another key limitation is related to data on cases. Two large states – Florida and New York – do not report data on cumulative cases. Thus, the national numbers we present for case data are not truly nationally representative. These states report a large number of deaths, so they have likely experienced similarly large numbers of cases.
On July 24, 2020, President Trump signed four executive orders related to prescription drug costs. All four orders will require regulatory action by the Administration before they can be implemented. Three of the four executive orders were released publicly – one pertaining to prescription drug importation, one pertaining to Medicare Part D drug rebates, and one pertaining to the cost of insulin and injectable epinephrine in federally qualified health centers. The fourth executive order, referred to by the President as the “most favored nation” proposal, that uses international reference prices to lower drug costs in the U.S., was not released with the others. Instead, the President announced he would give pharmaceutical companies 30 days to come up with an alternative approach before that order would take effect.
Those 30 days have now passed, and the executive order has still not been released. According to press reports, the pharmaceutical industry has put together an alternative proposal, but it is not known whether the proposal has been presented to the White House, nor whether the President will accept the industry’s proposal and drop the “most favored nation” proposal. The President has continued to tweet and talk about this proposal, including at some length on the opening day of the Republican National Convention. According to the President’s statement at the signing ceremony, the executive order would ensure that the U.S. pays no more for pharmaceuticals than other countries.
While the content of this executive order has not been released to the public, a portion of the textthat was captured by a photographer during the President’s signing ceremony indicates that it may be similar to a proposal announced by the Administration in October of 2018 in an advance notice of proposed rulemaking (ANPRM). Under the 2018 proposal, Medicare would test a model that uses lower drug prices from several foreign countries to set payments for drugs that are covered under Medicare Part B, with the aim of paying 126% of what other countries pay, down from 180% currently. Medicare Part B covers a limited set of prescription drugs that are administered in outpatient settings, such as physician offices and hospital outpatient departments, mainly high-cost drugs used to treat serious illnesses such as cancer or rheumatoid arthritis. As proposed, the model would have no direct impact on the price of drugs covered under Medicare Part D or private insurance.
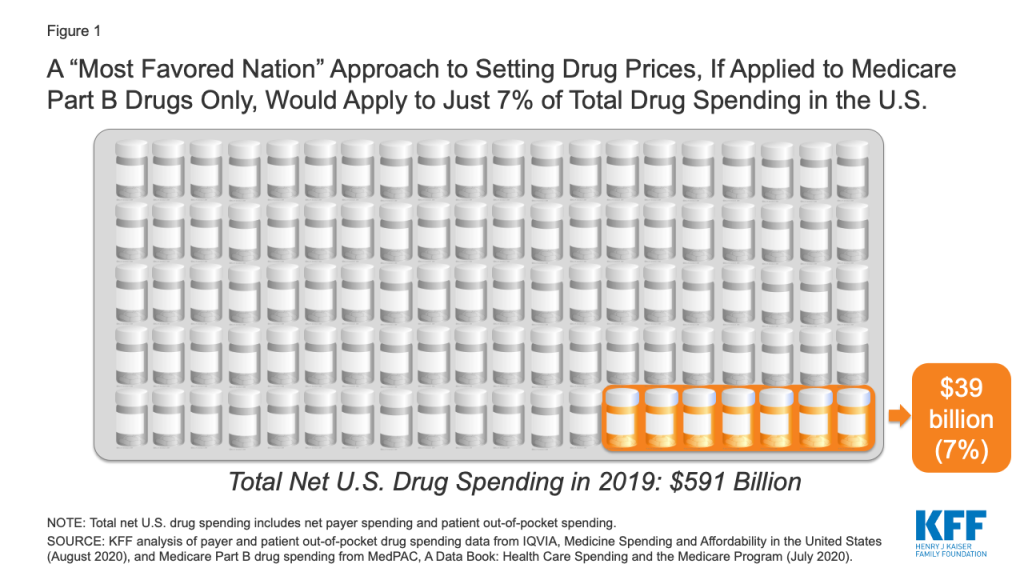
If the new executive order is similar to the 2018 proposal, and applies only to Medicare Part B drug spending, it would apply to just 7% of total national spending on prescription drugs, according to our analysis (Figure 1).
Figure 1: A “Most Favored Nation” Approach to Setting Drug Prices, If Applied to Medicare Part B Drugs Only, Would Apply to Just 7% of Total Drug Spending in the U.S.
If a “most favored nation” approach was limited to setting prices for prescription drugs covered by Medicare Part B only, it could lower drug costs for approximately 4 million Medicare beneficiaries, based on the number of people who used Part B drugs in 2018 (just 7% of all 60 million beneficiaries covered by Medicare). However, it would have no direct impact on the lion’s share of drug spending under Medicare for prescriptions filled by the 45 million beneficiaries covered under Medicare Part D, nor would it lower drug costs for the 157 million people with employer coverage or for millions more with other insurance coverage or no coverage whatsoever.
Methods
To calculate the share of total drug spending accounted for by Medicare Part B drug spending, we used data from IQVIA, Medicine Spending and Affordability in the United States: Understanding Patients’ Costs for Medicines (August 2020) and MedPAC, A Data Book: Health Care Spending and the Medicare Program (July 2020). According to IQVIA, total net payer spending on prescription drugs in 2019, including both retail and non-retail settings, was $509 billion, and patient out-of-pocket spending on drugs, both retail and non-retail, was an additional $82 billion, for a total of $591 billion in total net payer and patient drug spending in 2019. According to MedPAC, Medicare Part B drug spending was $35 billion in 2018. We trended this 2018 estimate forward to 2019 using the 11% average annual growth rate in Part B spending between 2009 and 2018, as reported by MedPAC, to derive an estimated Part B drug spending amount for 2019 of $39 billion. This $39 billion estimate formed the numerator and the $591 billion IQVIA estimate formed the denominator for our calculation of total drug spending accounted for by Medicare Part B drug spending in 2019.
States have taken a number of Medicaid policy actions to address the impact of COVID-19 on seniors and people with disabilities, many of whom rely on long-term services and supports (LTSS) to meet daily needs and are at increased risk of adverse health outcomes if infected with coronavirus. Medicaid is the primary source of coverage for LTSS, financing over half of these services in 2018. Collectively these actions could expand access to coverage (by enhancing financial and functional eligibility criteria and streamlining enrollment), expand access to long-term care services (by adding new benefits and increasing utilization limits), and bolster providers (through increased reimbursement or retainer payments). Increased funding may be required to extend community-based care more broadly and additional enrollee protections and oversight could be achieved through strengthened reporting requirements. This issue brief identifies state actions taken as of August 21, 2020 and implications for future consideration.
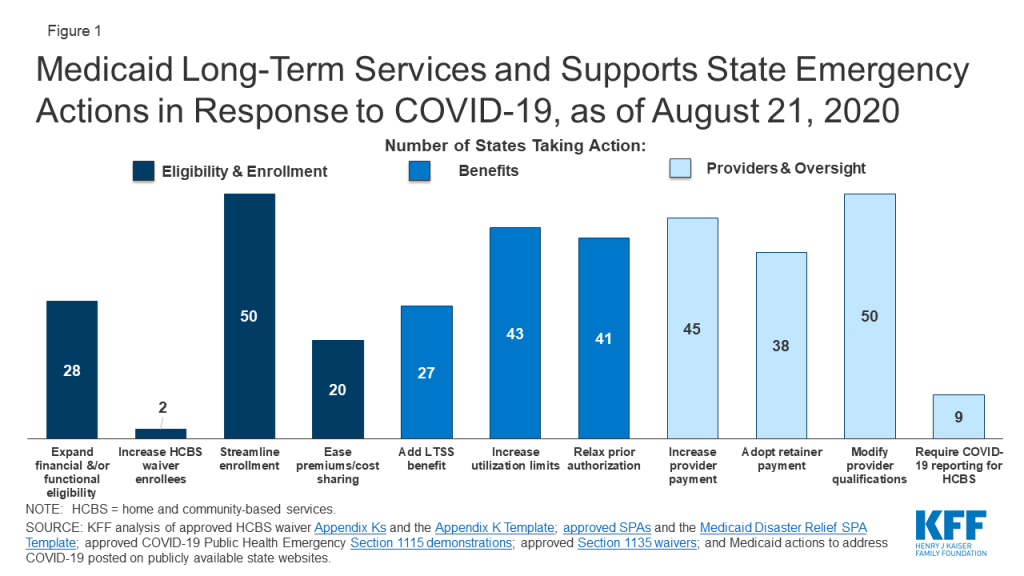
States have taken a number of emergency LTSS actions related to Medicaid eligibility, benefits and providers (Figure 1). Over half of states have expanded eligibility criteria for seniors and people with disabilities, while few states have increased the total number of HCBS waiver enrollees served. Nearly all states have streamlined enrollment processes, and over one-third of states have eased premium and/or cost-sharing requirements for seniors and people with disabilities. Just over half of states have added a new LTSS benefit to meet enrollee needs during the emergency; most benefit expansions are home and community-based services (HCBS). Most states have increased service utilization limits and relaxed prior authorization requirements. Nearly all states have increased provider payment rates for at least one LTSS and modified provider qualifications, and many have adopted retainer payments. Among states with provider payment rate increases, just over half have increased institutional rates, while about two-thirds have increased rates for at least some HCBS. Few states have required reporting on COVID-19 cases and deaths for HCBS enrollees and/or settings. CMS has adopted separate COVID-19 reporting requirements for nursing facilities.
Figure 1: Medicaid Long-Term Services and Supports State Emergency Actions in Response to COVID-19, as of August 21, 2020
The duration of the public health emergency has implications for policy actions adopted under Medicaid emergency authorities as well as the availability of enhanced federal funding provided through the matching rate increase. Many state policy changes have been adopted through temporary authorities that will expire after the public health emergency declaration ends, which will lead policymakers to assess whether any policies can or should be retained and transitioned to other authorities. In addition, some policy changes in response to the pandemic may be difficult for states to sustain without additional federal financial support beyond the 6.2 percentage point increase in federal Medicaid matching funds authorized by Congress during the public health emergency, as states are facing revenue declines and budget shortfalls.
A great deal of attention has been focused on the impact of COVID-19 in nursing homes, given the disproportionate number of cases and deaths among residents and staff nationally, with less attention on community-based residential settings. The Trump Administration has issued guidance about how nursing homes should respond to the pandemic, announced the formation of an independent commission to assess nursing home response, and adopted new reporting requirements for COVID-19 cases and deaths in nursing homes. To date, less attention to COVID-19 cases and deaths generally has been paid to community-based residential settings, such as group homes, where the pandemic presents similar risks to Medicaid enrollees and providers due to the highly transmissible nature of the coronavirus, the congregate nature of the settings, and the close contact that many workers have with residents. Data about COVID-19 cases and deaths in both institutional and community-based congregate settings may allow policymakers to more fully assess the impact across populations at increased risk of adverse health outcomes. The pandemic also may exacerbate the need for HCBS waiver services, which already are subject to waiting lists in a number of states. For example, elderly parents sickened by COVID-19 may no longer be able to provide care for their adult children with disabilities. Beyond the pandemic, the coming age wave makes LTSS and Medicaid’s role as the primary payer likely to be policy issues faced by the next Administration, in addition to the continuing effects of the pandemic and economic crisis.
Introduction
As the COVID-19 pandemic continues, states have taken a number of Medicaid policy actions to address the impact on seniors and people with disabilities, many of whom rely on long-term services and supports (LTSS) to meet daily needs and are at increased risk of adverse health outcomes if infected with coronavirus. Medicaid covers nearly 7.4 million seniors and almost 11.1 million people who are eligible based on a disability as of 2014. These enrollees may be at increased risk for adverse health outcomes if infected with coronavirus due to their older age, underlying health conditions, and/or residence in congregate settings, such as nursing homes, intermediate care facilities for people with intellectual or developmental disabilities (I/DD), or group homes. In addition, many seniors and people with disabilities rely on Medicaid LTSS to meet daily self-care and independent living needs, which makes it important for their coverage and access to care to continue uninterrupted during the pandemic.
Many state policy changes related to Medicaid LTSS have been adopted through temporary authorities that, according to CMS guidance, will expire when the Health and Human Services Secretary’s COVID-19 public health emergency declaration ends. This will lead policymakers to assess whether any changes can or should be retained and transitioned to other authorities. The public health emergency declaration currently is set to expire on October 23, 2020. While some state actions have been supported by the 6.2 percentage point increase in federal Medicaid matching funds authorized by Congress during the public health emergency, policy changes may be difficult for states to sustain without additional federal financial support, given the severity and expected longevity of the economic crisis resulting from the pandemic. The amount of fiscal relief to states from the increase in federal matching funds depends on the duration of the public health emergency, while the economic consequences of the pandemic are likely to persist beyond the public health emergency period. The current increase in federal matching funds could offset or reduce state spending but is unlikely to fully offset state revenue declines and address budget shortfalls.
The election will have implications for LTSS issues, and Medicaid’s role as its primary payer, given the effects of the pandemic, the resulting economic crisis, and the coming age wave. Democratic Presidential nominee Joe Biden recently released a plan to increase access to Medicaid home and community-based services (HCBS), while the Trump Administration has proposed a Medicaid program-wide federal financing cap in the President’s FY 2020 budget and is asking the Supreme Court to invalidate the entire Affordable Care Act, including provisions that allows states to expand Medicaid HCBS. This issue brief identifies trends in state policy actions related to Medicaid for seniors and people with disabilities and LTSS as of August 21, 2020. These include actions to expand eligibility and streamline enrollment, ease premium and/or cost-sharing requirements, enhance benefits, increase provider payment, modify provider qualifications, and alter reporting requirements.
Key Findings
States are adopting Medicaid policies targeted to seniors, people with disabilities, and LTSS in response to the pandemic through a variety of authorities that have different expiration dates. These authorities include Disaster-Relief State Plan Amendments (SPAs), traditional SPAs, other administrative authorities, HCBS waiver Appendix K, Section 1115 demonstration waivers, and Section 1135 waivers. The beginning and ending dates vary by authority (Appendix Table 1).
Eligibility and Enrollment
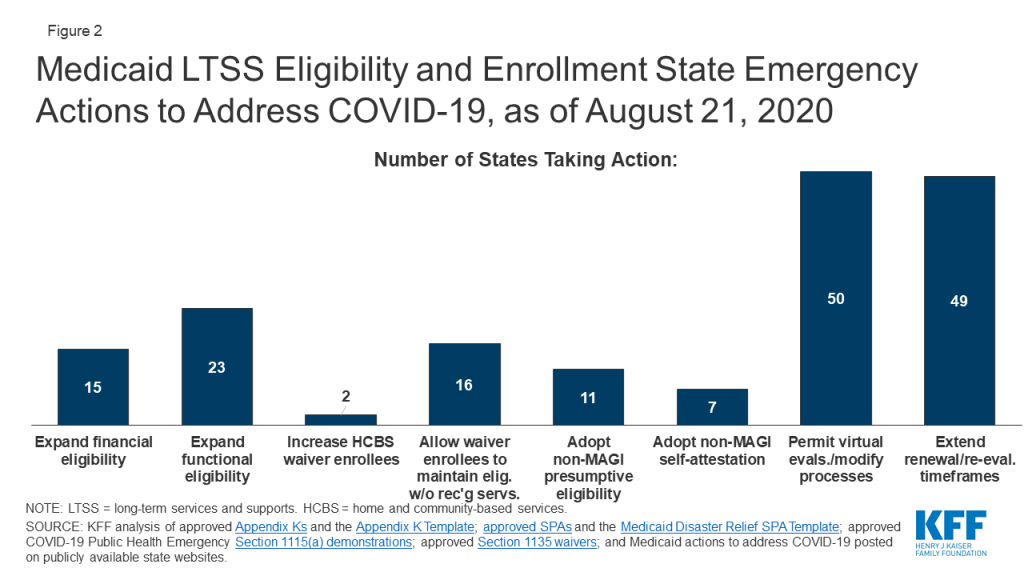
Fifteen states are expanding financial eligibility limits for seniors and people who qualify for Medicaid based on a disability to increase access to coverage during the public health emergency (Figure 2). Coverage groups where eligibility is based on old age or disability (known as “non-MAGI groups”) have income limits, and at state option, also may have asset limits. State actions to expand financial eligibility in these pathways include applying less restrictive income or asset methodologies and/or increasing HCBS waiver cost limits during the emergency period. For example, North Carolina is disregarding increases in assets for all non-MAGI groups until after the emergency period ends, and Massachusetts is allowing people with disabilities to obtain a temporary hardship waiver of the medically needy spend down requirement during the public health emergency. In addition, North Carolina and Washington are modifying financial eligibility criteria for some HCBS to cover beneficiaries who would otherwise not be eligible.
Figure 2: Medicaid LTSS Eligibility and Enrollment State Emergency Actions to Address COVID-19, as of August 21, 2020
Less than half of states (23) are expanding functional eligibility criteria to help more people qualify for coverage based on a disability during the emergency period (Figure 2). In addition to meeting financial eligibility criteria, coverage groups related to disability status require individuals to meet functional criteria, for example, based on the extent of their self-care needs. Missouri expanded coverage to adults who test positive for coronavirus by considering it a qualifying disability for its aged/blind/disabled pathway.1 Indiana is giving HCBS waiver enrollment priority to people with COVID-19 or who are presumed positive from its waiting lists for waivers that provide non-residential supports for people with I/DD, while other states are temporarily modifying HCBS waiver functional eligibility targeting criteria. In addition, 13 states are modifying HCBS waiver assessment requirements to allow individuals to begin receiving services before a functional eligibility evaluation is completed (no data shown).
Maryland and Utah are increasing the total number of individuals served in HCBS waivers during the emergency period (Figure 2). Maryland is increasing the number of individuals served in its waiver for children with autism spectrum disorder; Utah is increasing the number of individuals served by a waiver for people transitioning from institutions to the community. Unlike state plan coverage groups, states can limit the number of people who enroll in waivers, which can result in waiting lists when the number of people seeking services exceeds the number of waiver slots available. States acknowledged that the pandemic may exacerbate the need for HCBS waiver services; for example, Pennsylvania noted that many people on its waiver waiting list have aging caregivers who may not be able to continue providing care if they develop COVID-19. However, few states have been able to increase the number of waiver enrollees served in response to the pandemic. In addition, 16 states are allowing individuals to maintain HCBS waiver eligibility without receiving services, which can keep enrollees connected to coverage while services are interrupted due to provider shortages or restrictions due to state stay-at-home orders or while individuals are receiving inpatient treatment during the pandemic (Figure 2).
Nearly all states are taking at least one action to streamline eligibility determinations to expedite enrollment in coverage for seniors and people with disabilities during the emergency. Eleven states are allowing hospitals to make presumptive eligibility determinations for non-MAGI groups during the emergency, which can help connect people to coverage at the time they seek medical treatment (Figure 2). Seven states are allowing applicants in non-MAGI pathways to self-attest to financial and/or functional eligibility requirements in lieu of requiring documentation before determining eligibility (Figure 2). The most frequent action in this area is permitting virtual evaluations to determine HCBS waiver functional eligibility and/or otherwise modifying processes for HCBS waiver level of care evaluations and reevaluations to account for social distancing during the pandemic, adopted by 50 states (Figure 2).
Almost all states are extending eligibility renewal due dates during the pandemic to keep people connected to coverage and enable states to focus limited state agency staff time on responding to the emergency. Forty-nine states are extending reassessment and reevaluation due dates for one or more HCBS waivers (Figure 2). Pennsylvania is extending eligibility renewal deadlines for non-MAGI populations to every 12 months. As one of the conditions of receiving the enhanced federal matching funds under the Families First Coronavirus Response Act, states must provide continuous eligibility for individuals enrolled on or after March 18, 2020 through the end of the month in which the public health emergency ends.2
Premiums and Cost-Sharing
States are eliminating or easing premiums and cost-sharing requirements to help seniors and people with disabilities remain in coverage and facilitate access to services during the pandemic. More than one-third of states are eliminating or waiving premiums in Medicaid pathways that offer buy-in coverage for working people with disabilities, while a couple of states are easing cost-sharing requirements (Figure 1). Connecticut is suspending copayments for individuals who are dually eligible for Medicare and Medicaid. Rhode Island has adopted a policy that helps ensure that people with short-term nursing home stays will have a community-based residence to which they can return post-discharge by allowing enrollees to receive a home maintenance allowance throughout the public health emergency. This policy accounts for the financial cost of maintaining a home in the community by reducing the amount that these enrollees must pay out-of-pocket for institutional care and applies to individuals who were institutionalized for less than six months as of March 1, 2020, and unable to be discharged home due to COVID-19.
Benefits
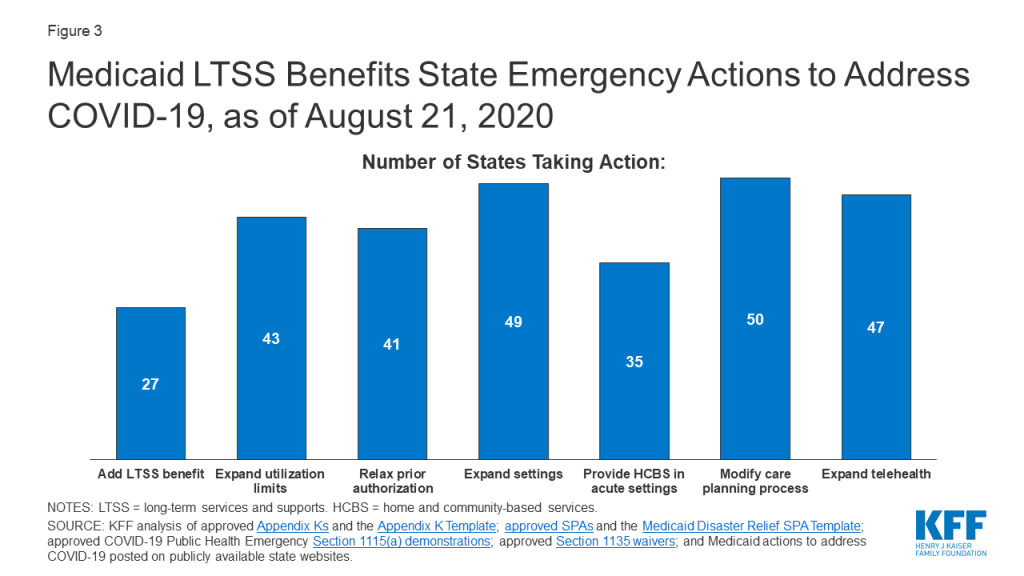
About half of states (27) are temporarily adding new services to their regular LTSS benefit packages to meet enrollee needs during the public health emergency (Figure 3). Nearly all state actions in this area relate to expanding the benefit packages available under HCBS waivers and/or Section 1915 (i) state plan HCBS. Frequently added services include home-delivered meals; medical supplies, equipment, and appliances; and assistive technology. Some states are adding other services to address the emergency. For example, Washington is adding wellness education to help HCBS waiver enrollees manage chronic conditions, avoid health risks and be informed about COVID-19. Indiana is adding rent and food reimbursement to help enrollees in an I/DD waiver offset the costs of room and board for an unrelated, live-in caregiver during the emergency. On the institutional LTSS side, Ohio has created a new benefit, Health Care Isolation Centers. These services are provided in specialized COVID-19 facilities to individuals who have been discharged from hospitals but continue to need medical and isolation care that cannot be provided in the community or their former congregate setting.
Figure 3: Medicaid LTSS Benefits State Emergency Actions to Address COVID-19, as of August 21, 2020
While the majority of benefits changes are expansions, one state is restricting benefits, and many are restricting visitors in HCBS settings in efforts to contain coronavirus spread (no data shown). Washington has authority to suspend specialized add-on nursing home services like habilitation during an emergency to protect the health of residents and staff. Similar to CMS guidance restricting visitors in nursing homes, 40 states are not allowing any visitors in at least some HCBS waiver residential settings to minimize the spread of infection.
Most states (43) are temporarily modifying utilization limits for covered services to ensure that enrollees can access services and address health and welfare issues during the emergency (Figure 3). Among these states, most are allowing utilization limits to be exceeded for HCBS waiver and/or state plan services. For example, Arkansas is removing its limit on physician visits in nursing homes, and Ohio is lifting hour and day limits on private duty nursing services post-discharge. In addition, 31 states are temporarily modifying the scope of HCBS waiver covered services to account for needs created by the pandemic (no data shown). For example, Tennessee is adding HCBS waiver services to support individuals with I/DD with shopping, hygiene, meal preparation and money management. By contrast, North Carolina, Rhode Island and Washington are restricting utilization of HCBS services (no data shown). All three states have Section 1115 waivers that allow them to vary the amount, duration, and scope of services based on population needs. In addition, North Carolina and Washington may target services on a less than statewide basis.
Most states (41) are suspending prior authorization requirements to ensure access to HCBS waiver and/or state plan services during the emergency (Figure 3). For example, Connecticut is waiving prior authorization for home health services, Maryland is suspending prior authorization for remote patient monitoring, and Nebraska is waiving prior authorization for transfers to post-acute long-term acute care hospitals, acute inpatient rehabilitation, or skilled nursing facility care. In addition, eight states are allowing other licensed providers to order home health services for state plan HCBS in addition to physicians (no data shown).
Nearly all states are expanding the settings where enrollees can receive HCBS to account for disruptions due to COVID-19 (Figure 3). Among these states, 49 are temporarily expanding the settings where HCBS waiver services can be provided during the public health emergency to include providing services in hotels, shelters, schools and churches, as needed. In addition, 35 states are allowing individuals in short-term inpatient settings to receive HCBS to provide communication and behavioral supports (Figure 3). Most states have adopted this policy for one or more HCBS waivers, and a couple are doing so for state plan HCBS: Alaska is allowing Community First Choice attendant care services to be provided in acute care hospitals, and Oregon is temporarily allowing payment for state plan HCBS, including home-based habilitation, behavioral habilitation, and psychosocial rehabilitation services, to individuals in an inpatient setting.
Nearly all states (50) are modifying care-planning processes to accommodate social distancing and facilitate access to services during the emergency (Figure 3). Examples of frequently adopted policy changes in this area include modifying the person-centered plan development process for HCBS waiver services, adjusting functional assessment requirements used to determine service levels, and adding electronic document signing. Other policy changes in this area include allowing verbal consent instead of a written signature for HCBS service plans and allowing the face-to-face encounter for home health services to take place up to one year after an individual begins receiving services. North Carolina and Washington are allowing for the provision of LTSS to individuals impacted by the emergency even if the services are not updated timely in the care plan. Michigan is extending service authorizations in person-centered service plans for state plan HCBS throughout the duration of the public health emergency.
Nearly all states have expanded the delivery of HCBS via telehealth (Figure 3). Forty-seven states are adding electronic service delivery methods to continue providing HCBS waiver and state plan in-home services remotely. Minnesota is allowing state plan group therapy and rehabilitative services to be provided via telehealth. Oregon is allowing adding telehealth delivery of state plan home-based habilitation, behavioral habilitation, and psychosocial rehabilitation services. Connecticut is allowing for telephonic check-ins in lieu of face-to-face assistance for certain mental health HCBS waiver enrollees. DC is also covering services provided remotely to state plan HCBS recipients, such as wellness checks and therapeutic activities.
Provider Payment
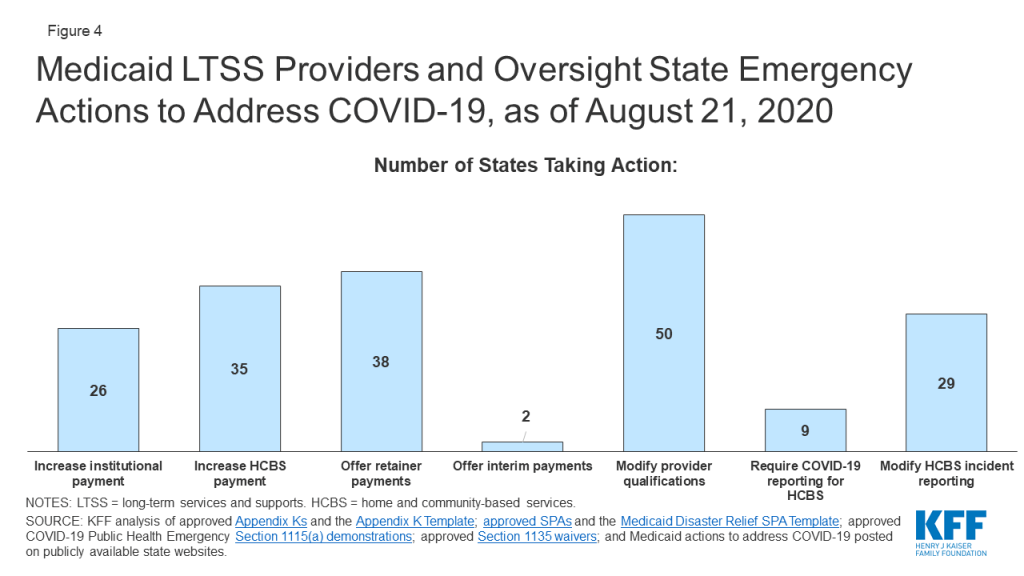
Just over half of states are increasing institutional LTSS payment rates (Figure 4). Among these 26 states, 24 have increased rates for nursing homes, which have been disproportionately affected by the COVID-19 pandemic, and five states are doing so for intermediate care facilities for people with intellectual or developmental disabilities or other institutional settings (no data shown). Most states are implementing per diem or percentage rate increases, while a few states are increasing the number of days for which facilities can receive bed hold payments to account for absences due to COVID-19 treatment. Alabama also is providing an additional add-on cleaning fee. Kentucky is temporarily pausing per diem rate sanctions to nursing facilities that are unable to meet medical record review thresholds to validate assignment of patients to reimbursement groups based on acuity during the public health emergency.
Figure 4: Medicaid LTSS Providers and Oversight State Emergency Actions to Address COVID-19, as of August 21, 2020
Some states limit the additional payments to facilities or patients with a COVID-19 diagnosis, while others apply them to all nursing facilities to account for increased costs related to staffing, equipment and cleaning as a result of the emergency (no data shown). For example, Michigan is providing a $5,000 per bed supplemental payment in the first month for COVID-19 regional hub nursing facilities to address immediate infrastructure and staffing needs and a $200 per diem rate increase in subsequent months to account for the higher costs of caring for COVID-19 patients.
A couple of states specifically have included pay increases for direct care workers in nursing homes and/or other institutional settings (no data shown). Arkansas adopted temporary supplemental payments that increase direct care workers’ weekly pay by a base supplemental payment according to number of hours worked and an additional tiered acuity payment for those working in facilities with COVID-19 positive patients. Texas’ nursing facility payment rates increase includes a pay increase for direct care workers and an increase for supply and dietary costs.
Just over two-thirds of states (35) are increasing provider payment rates for at least some HCBS state plan or waiver services during the public health emergency (Figure 4). For example, Alabama is increasing waiver payment rates for personal care, adult companion, respite, and skilled nursing care to account for overtime pay, staffing needs and infection control supplies. Louisiana has received approval to increase payments for all services provided under its Community Choices Waiver for elderly and disabled adults by up to 50% as needed to maintain staffing. States increasing payment rates for HCBS provided under state plan authority include targeted case management (AK), day habilitation (AR), skilled and/or private duty nursing (DC, OK), and home health and adult care homes (NC). Arkansas’s temporary supplemental payments for direct care workers in nursing facilities also apply to direct care workers in assisted living facilities and those providing home health and personal care services in the community. Michigan adopted a supplemental payment for providers of personal care and behavioral health treatment technician in-person services. Washington’s Section 1115 demonstration waiver allows the state to increase rates for Community First Choice attendant care services by up to 50 percent to maintain provider capacity during the public health emergency. In addition, Tennessee has adopted temporary payment rate increases for community-based residential, personal care, attendant care, personal assistance and intensive behavioral treatment stabilization and treatment services and a temporary per diem add-on to community-based residential and personal care payment rates to account for direct support staff hazard pay, overtime, and PPE costs using its existing directed payment authority; these services are provided under a Section 1115 HCBS waiver.
Among the states adopting LTSS provider payment increases, 18 states have increased rates for both institutional and community-based services (no data shown). Ten states have increased provider payments for only institutional services, while 17 states have increased rates for HCBS only.
About three-quarters of states are adopting retainer payments for HCBS providers (Figure 4). Thirty-eight states have adopted retainer payments for providers offering HCBS through waiver and/or state plan authorities. For example, Washington and New Hampshire have an approved Section 1115 waiver that authorizes retainer payments for personal care and habilitation services provided under state plan authority.
Two states are making interim payments to LTSS providers (Figure 4). Among these states, North Carolina allows any Medicaid-enrolled provider to request that their reimbursement be converted to an interim payment methodology, while Georgia is making interim payments to skilled nursing facilities.
Provider Qualifications
Nearly all states (50) are temporarily modifying HCBS state plan and/or waiver provider qualifications in response to potential staff shortages and increased demand due to COVID-19 (Figure 4). Frequently adopted policies in this area include temporarily permitting payment for HCBS waiver services rendered by family caregivers or other legally responsible relatives during the emergency (if not already permitted in the waiver), adopted by 38 states (no data shown). Twenty-three states are waiving conflict of interest rules and allowing case management entities to also be direct service providers for HCBS waiver enrollees during the emergency (no data shown). In addition, all states have adopted modified provider screening requirements through Section 1135 waiver authority, which may apply to LTSS providers as well as other providers.
Reporting and Oversight
Few states are adopting reporting requirements for COVID-19 cases and deaths among HCBS enrollees (Figure 4). CMS is requiring all nursing facilities to report COVID-19 cases and deaths as of May 8, 2020, but just nine states are requiring reporting of COVID-19 cases among HCBS waiver enrollees. HCBS waiver enrollees living in congregate settings such as group homes are likely to experience increased risk from coronavirus infection similar to individuals in nursing homes. In addition to the CMS nursing home reporting requirements, three states (AZ, CT, IN) have adopted their own reporting requirements related to COVID-19 cases and deaths for long-term care facilities. For example, Connecticut requires managed residential communities and nursing homes to provide daily COVID-19 status reports. Arizona also requires reporting on COVID-19 cases and deaths from group homes.
Twenty-nine states are temporarily modifying HCBS waiver incident reporting requirements and other participant safeguards during the public health emergency (Figure 4). This allows states to focus their administrative efforts on the COVID-19 response. However, there are potential risks for enrollees as incident reporting is a requirement for HCBS programs to protect enrollees from abuse, neglect and injury and to ensure their health and safety. Twenty-eight states are delaying submitting HCBS waiver enrollment and spending reports to CMS and/or are suspending data collection for performance measures other than health and welfare (no data shown). In addition, forty-seven states are suspending pre-admission screening and annual resident review requirements for nursing facilities (no data shown).
Looking Ahead
The duration of the public health emergency has implications for policy actions adopted under Medicaid emergency authorities as well as the availability of enhanced federal funding provided through the match rate increase. Many state policy changes have been adopted through temporary authorities that will expire after the public health emergency declaration ends, which will lead policymakers to assess whether any policies can or should be retained and transitioned to other authorities. In addition, some policy changes in response to the pandemic may be difficult for states to sustain without additional federal financial support beyond the 6.2 percentage point increase in federal Medicaid matching funds authorized by Congress during the public health emergency, as states are facing revenue declines and budget shortfalls.
A great deal of attention has been focused on the impact of COVID-19 in nursing homes, given the disproportionate number of cases and deaths among residents and staff nationally with less attention on community-based residential settings. The Trump Administration has issued guidance about how nursing homes should respond to the pandemic, announced the formation of an independent commission to assess nursing home response, and adopted new reporting requirements for COVID-19 cases and deaths in nursing homes. To date, less attention to COVID-19 cases and deaths generally has been paid to community-based residential settings, such as group homes, where the pandemic presents similar risks to Medicaid enrollees and providers due to the highly transmissible nature of the coronavirus, the congregate nature of the setting, and the close contact that many workers have with residents. Data about COVID-19 cases and deaths in both institutional and community-based congregate settings may allow policymakers to more fully assess the impact across populations at increased risk of adverse health outcomes. The pandemic also may exacerbate the need for HCBS waiver services, which already are subject to waiting lists in a number of states. For example, elderly parents sickened by COVID-19 may no longer be able to provide care for their adult children with disabilities. Beyond the pandemic, the coming age wave makes LTSS and Medicaid’s role as the primary payer likely to be policy issues faced by the next Administration, in addition to the continuing effects of the pandemic and economic crisis.
Appendix
Appendix Table 1: Medicaid Emergency Authorities
Authority
Description
Start Date
End Date
Disaster-Relief SPA
Allows states to make temporary changes to address eligibility, enrollment, premiums, cost-sharing, benefits, payments, and other policies differing from their approved state plan during the COVID-19 emergency. States may not make changes that restrict or limit payment, services, or eligibility or otherwise burden beneficiaries and providers.
1/1/20 (using Section 1135 waiver authority) or later date elected by state
End of public health emergency or earlier date elected by state
Traditional SPA
Allows states to amend their Medicaid state plans, which govern program elements such as coverage groups, covered services, provider reimbursement methodologies, and administrative activities.
1st day of quarter in which SPA is submitted to CMS or later date elected by state
Continues until subsequently amended or terminated
HCBS Waiver Appendix K
Allows state to amend Section 1915 (c) or Section 1115 HCBS waiver provisions related to eligibility, services, payment, provider qualifications, level of care evaluations, person-centered service plans, incident reporting, settings, and other policies to respond to emergency.
1/27/20 or later date elected by state and approved by CMS
1/26/21 or earlier date elected by state
Section 1115 Demonstration Waiver
Allows states operate to Medicaid programs without regard to specific statutory or regulatory provisions to furnish medical assistance in a manner intended to protect, to the greatest extent possible, the health, safety, and welfare of individuals and providers who may be affected by COVID-19.
3/1/20 or later date elected by state and approved by CMS
60 days after public health emergency ends or earlier date approved by CMS
Section 1135 Waiver
Allows states to operate Medicaid programs without regard to certain fee-for-service prior authorization, LTSS authorization and assessment, fair hearing procedural and timeline, provider enrollment, reporting and oversight, and other requirements, to ensure that sufficient health care items and services are available to meet enrollee needs and that providers are reimbursed.
3/1/20
End of public health emergency, per CMS guidance
SOURCE: KFF analysis of Medicaid emergency authorities and CMS guidance.
Endnotes
Missouri elects the Section 209 (b) option to apply Medicaid financial and/or functional eligibility rules to SSI beneficiaries that differ from federal SSI rules. KFF, Medicaid Financial Eligibility for Seniors and People with Disabilities: Findings from a 50-State Survey (June 2019), https://modern.kff.org/report-section/medicaid-financial-eligibility-for-seniors-and-people-with-disabilities-findings-from-a-50-state-survey-issue-brief/. In its COVID-19 Frequently Asked Questions, CMS notes that “[i]n making disability determinations, a state must generally use the same definition of disability as used for supplemental security income (SSI). A positive diagnosis for COVID-19 is not a per se disability under SSI criteria and therefore cannot be the sole basis of a determination of disability for purposes of Medicaid eligibility.” CMS, COVID-19 Frequently Asked Questions (FAQs) for State Medicaid and Children’s Health Insurance Program (CHIP) Agencies at II.C.2 (last updated June 30, 2020), https://www.medicaid.gov/state-resource-center/Downloads/covid-19-faqs.pdf. ↩︎
States generally must maintain Medicaid eligibility through the end of the month in which the public health emergency period ends for all individuals enrolled on or after March 18 2020, as a condition of receiving the 6.2 percentage point increase in federal matching funds. KFF, Key Questions About the New Increase in Federal Medical Matching Funds for COVID-19 (May 2020), https://modern.kff.org/coronavirus-covid-19/issue-brief/key-questions-about-the-new-increase-in-federal-medicaid-matching-funds-for-covid-19/. CMS has clarified that states are not prohibited from conducting regular eligibility renewals during this period, but as a condition of receiving the enhanced federal matching funds, states cannot terminate coverage for any Medicaid beneficiary enrolled on or after March 18 2020, unless the individual is no longer a state resident or requests voluntary termination. CMS, Families First Coronavirus Response Act – Increased FMAP FAQs, question B.11 (updated as of 4/13/2020), https://www.medicaid.gov/state-resource-center/downloads/covid-19-section-6008-faqs.pdf. ↩︎
Amid the coronavirus pandemic, half of Americans report that their mental health has been negatively impacted due to related stress and worry. Many are, or will be, struggling with mental health challenges due to anxiety, social isolation, loss of loved ones, and job losses – potentially leading to increased mental health care needs over the long term.
A new issue brief examines where President Trump and Democratic presidential nominee Joe Biden stand on key aspects of the nation’s mental health and substance use challenges. Key points include:
Opioid epidemic. President Trump declared a national public health emergency in 2017 and has renewed it repeatedly since then. His proposed 2021 budget would decrease total funding to the Substance Abuse and Mental Health Services Administration and to Medicaid, the nation’s largest payer for mental health services and main contributor for substance use disorder services. Vice President Biden’s campaign website features a five-point plan to address the opioid crisis that would increase access to services, curb unnecessary opioid prescriptions, and hold pharmaceutical companies accountable for their role in the crisis.
Suicide prevention. Both candidates’ suicide prevention plans focus on veterans, with President Trump creating a task force to tackle the issue and proposing to boost the Veterans Administration (VA) budget for suicide prevention. Vice President Biden proposes to expand and strengthen veterans’ mental health programs inside and outside the VA, as well as strengthen programs aimed at reducing suicide among LGBTQ teenagers.
Mental health parity. Vice President Biden’s campaign vows to redouble efforts to enforce existing mental health parity laws and expand funding for mental health, but has not offered specific plans. President Trump’s campaign website does not address mental health parity. His administration is seeking to overturn the Affordable Care Act, which would substantially limit the scope of parity rules.
Mental health workforce. Neither candidate specifically addresses mental health workforce shortages on their campaign websites. However, President Trump’s 2021 budget proposal includes a 24% increase for behavior health workforce development programs, and Vice President Biden’s education plan would double the number of psychologists, counselors and other mental health professionals in schools.
The brief draws on each candidates’ campaign website, news coverage, public statements and budget proposals. It is part of KFF’s ongoing efforts to provide useful information related to the health policy issues relevant for the 2020 elections, including policy analysis, polling, and journalism. Find more on our Election 2020 resource page.
KFF also has compiled state-specific data on mental health and substance use on more than 20 indicators, with mental health state fact sheets available profiling each state, as well as an updated look at how the COVID-19 pandemic is affecting Americans’ mental health.
Amid the COVID-19 pandemic, many Americans are struggling with mental health challenges. In a recent KFF poll, majority (53%) of adults in the United States reported that their mental health has been negatively impacted due to worry and stress over the virus. Additionally, more than one in three adults in the U.S. reported symptoms of anxiety or depressive disorder during the pandemic, up from roughly one in ten in 2019. As the virus continues to spread, the pandemic will likely lead to increased mental health care needs and significantly impact the well-being of people in the U.S. Under the Trump administration, the recently-passed Coronavirus Aid, Relief, and Economic Security Act (CARES Act) may address some of these needs.
Mental health was already a key public health issue. In recent years, growing numbers of Americans have reported being depressed, and deaths due to drug or alcohol abuse, or suicide have increased. In 2017-2018, nearly 17 million adults and an additional 3 million adolescents had a major depressive episode in the past year, and over 10 million adults with mental illness had serious thoughts of suicide in the past year. Nearly 14 million adults reported an unmet need for mental health or substance use treatment, with many citing cost as a barrier.
The 2020 presidential election could have a substantial effect on the United States’ response to growing mental health needs and long-term policy for addressing this public health challenge. This issue brief examines the presumptive 2020 presidential candidates’ positions on mental health and substance use disorders. Specifically, we analyzed candidate positions on suicide prevention, mental health workforce issues, mental health parity enforcement, and the opioid epidemic. We synthesize policy positions for President Donald Trump and the presumed Democratic nominee, Former Vice President Joe Biden.
We identified candidate positions first by gathering information directly from campaign platforms as stated on candidate websites. Where information was not available on former Vice President Biden’s website, we supplemented with information his campaign supplied in a survey conducted by Mental Health for US, a nonpartisan coalition of organizations working in mental health and addiction policy. President Trump did not participate in the survey as of this brief’s publication, so we also reviewed news coverage of his campaign from the last year and his proposed 2021 budget for mention of these mental health-related topics. While candidates may have made other statements about mental health and substance use disorders, we do not aim to capture all comments ever made but instead focus on the candidates’ stated platforms.
The candidate platforms differ in both the amount of attention paid to mental health and their approaches to addressing these issues. Election outcomes thus have potentially large implications for policy direction in these areas of mental health and substance use funding, service delivery, and access.
Rising Suicide Rates & Suicide Prevention
Due to necessary social distancing, many people are experiencing isolation, distress, and barriers to accessing mental health services. Historically, national crisis hotlines have seen a spike in calls during distressing nationals events, and as the pandemic continues, calls to hotlines are on the rise. There is particular concern about suicidal ideation during this time, as isolation is a risk factor for suicide. In 2018, over 48,000 Americans died by suicide1 , and in 2017-2018, over ten million American adults (4.3%) reported having serious thoughts of suicide in the past year. Suicide is one of the top ten causes of death in the U.S. and accounts for majority of firearm deaths. Moreover, the Centers for Disease Control and Prevention (CDC) documents a substantial increase in the national suicide rate over time, with the age-adjusted suicide rate rising from 10.7 per 100,000 people in 2001 to 14.2 per 100,000 people in 2018 (Figure 1). Among working-age Americans (ages 16-64 years), the suicide rate rose by 40% over the same period. Both presidential candidates have offered suicide prevention plans with particular attention paid towards veterans, one subgroup at higher risk of suicide than the general population.
Figure 1: Suicide Rates in the United States, 2001 – 2018
President Trump’s suicide prevention plan focuses on the veteran population. His campaign website spotlights his 2019 executive order creating a task force dedicated to preventing suicides among veterans, and his proposed 2021 budget for the Department of Veterans Affairs allocates roughly 30% more in funding for suicide prevention among veterans than the 2020 enacted budget. Separately, in President Trump’s proposed 2021 budget for SAMHSA, he includes a small increase in funding for specific grant-based suicide prevention programs.
Former Vice President Biden’s suicide prevention plan is primarily focused on the veteran population. His campaign website details several initiatives that he would implement within the Veterans Affairs health system, which would increase funding for mental health services, streamline the initiation of mental health treatment, and increase the number of mental health staff practicing in VA hospitals. Former Vice President Biden’s plan states that he would also establish a national center of excellence for reducing veteran suicide to develop and implement suicide prevention strategies outside of the VA health system, and that he would address risk factors for suicide such as PTSD and sexual assault among current and former service members, though details on possible approaches are not provided. Additionally, in the context of the youth LGBTQ community, former Vice President Biden states that he will strengthen suicide prevention programs for teens, but does not provide specific details.
Mental Health Workforce Shortages
The need for mental health care is expected to increase in light of the coronavirus pandemic. Due to ongoing, widespread efforts to slow the spread of the virus by means of social distancing, an increasing number of mental health providers are offering services through telehealth, but those with limited capacity to do so may be scaling back their practices. Meanwhile, many individuals seeking mental health care are already unable to access care in a timely manner due to provider shortages across the country. Nationwide, nearly 117 million people are in a mental health provider shortage area, and less than 30% of the need for psychiatrists is being met.2 Furthermore, HRSA projects there will be a nationwide shortfall of over 12,500 adult psychiatrists and over 11,500 addiction counselors by the year 2030. Access to pediatric providers is particularly problematic, with 70% of counties in the U.S. having no practicing child psychiatrist. Neither candidate has provided specific details on how they will increase the mental health workforce to address the lack of providers.
President Trump’s campaign website does not specifically address mental health workforce shortages. However, his 2021 budget proposal for HRSA indicates roughly a 24% increase in funding for behavioral health workforce development programs from 2019 to 2020, which would not change for 2021.
Former Vice President Biden’s campaign website does not specifically address mental health workforce shortages. However, in the context of his education plan, he states he will double the number of psychologists, guidance counselors, and other mental health professionals in schools. In a survey by Mental Health for US, former Vice President Biden states that he will increase funding for the National Health Service Corps and create partnerships between health centers, high schools, and community colleges in order to encourage youth to pursue health care jobs. He also adds that he will build on legislation such as the 21st Century Cures Act and the Opioid Workforce Act of 2019, which address the shortage of mental health and substance use disorder providers.
Mental Health Parity
There is a focus on addressing access barriers for services many people need in relation to the coronavirus pandemic, such as potentially high cost-sharing for testing and treatment. Access to mental health and substance use disorder services is also a key need to address, and has its own challenges due to lingering issues with mental health parity. The Mental Health Parity and Addiction Equity Act (MHPAEA) was passed in 2008, requiring insurer coverage of mental health and substance use disorder services in a way that is equivalent to coverage for medical and surgical services. The law prohibits most group health plans that offer coverage for mental health and substance use conditions from imposing treatment limitations and financial requirements on those benefits that are stricter than for medical and surgical benefits. The 2010 Affordable Care Act (ACA) expanded MHPAEA’s reach by requiring coverage of behavioral health services as an “essential health benefit” in many private health plans (a notable exception being large employer plans) and extending parity requirements to the small group, individual, and Medicaid managed care markets. Since the MHPAEA took effect, changes in the use of mental health services have been modest. Additionally, while research has documented an effect of parity on equalizing quantitative treatment limitations and cost sharing, it has been more difficult to measure and regulate the law’s effect on non-quantifiable treatment limitations, such as prior authorization and network adequacy, which are also supposed to be provided at parity. Questions remain as to how to improve parity enforcement; so far, both candidates have offered limited details.
President Trump’s campaign website does not address parity for mental health services. The Trump administration has joined Texas and several other states in Texas v. U.S. (known as California v. Texas by the Supreme Court, which recently agreed to hear the case), arguing that the ACA should be invalidated, an outcome that would substantially limit the scope of parity rules and eliminate the essential health benefit requirement. The Trump administration has also expanded the allowed duration of short-term health plans, which do not have to comply with ACA requirements, typically do not cover mental health services, and generally exclude people with pre-existing conditions such as serious mental illnesses.
Former Vice President Biden’s campaign website says that, as president, he would “redouble” efforts to enforce existing mental health parity laws and expand funding for mental health. He points to his previous role in implementing the MHPAEA but does not specify which actions his administration would take to further enforcement.
The Opioid Epidemic and Drug Overdoses
Preliminary data shows that deaths due to drug overdose are increasing during the coronavirus pandemic. This may be a result of necessary lockdowns, barriers to care, and the economic recession. Prior to the pandemic, deaths due to opioid overdose saw large increases, from 2.9 deaths per 100,000 people in 1999 to 14.6 deaths per 100,000 people in 2018 (Figure 2). In response to the growing opioid epidemic, the Department of Health and Human Services declared a public health emergency in 2017 and introduced five strategies: 1) improving access to treatment, 2) increasing use of drugs to reverse overdoses, 3) public health surveillance, 4) research on pain and addiction, and 5) identifying better practices to manage pain. In recent years, several indicators have shown some improvement in opioid misuse or overdose, but rising rates of use or misuse of illicit drugs—including methamphetamine, cocaine, and benzodiazepines—have broadened the scope of the addiction crisis. Each presidential candidate has proposed strategies to address the opioid epidemic and substance use disorder going forward, including details on making medication-assisted treatment3 more widely available.
Figure 2: Opioid Overdose Death Rate in the United States, 1999-2018
President Trump’s reelection campaign website states that addressing the opioid epidemic has been a priority for his administration, which declared the crisis a national public health emergency in late 2017 and has since renewed the declaration every 90 days. He also signed legislation approving additional grant funds to combat the opioid epidemic, including the SUPPORT for Patients and Community Act. However, President Trump’s proposed 2021 budget would continue to decrease total funding for both the Substance Abuse and Mental Health Services Administration (SAMHSA) and Medicaid – the U.S.’s largest payer for mental health services and a main contributor for substance use disorder services. Despite these overall cuts, the proposed budget for SAMHSA includes a small increase in state grants to address opioid use disorders, and the proposed budget for Medicaid includes increased funding over ten years for states to extend postpartum coverage for women with substance use disorders. The proposed budget for opioid response programs in rural areas under the Health Resources and Services Administration (HRSA) remains flat for 2020 and 2021, but down from 2019.
Former Vice President Biden’s campaign website outlines a detailed, five-point plan to address the opioid crisis. First, it states how he will monitor and hold pharmaceutical companies accountable for their role in the crisis, notably by banning pharmaceutical companies from financially incentivizing prescriptions and appointing an “Opioid Crisis Accountability Coordinator” to work with both federal and state-level efforts. Second, former Vice President Biden states that he will increase access to substance use disorder services through a $125 billion investment over a ten-year period. These investments will include making medication-assisted treatment universally accessible by 2025 by building on the 21st Century Cures Act; providing funding to underserved communities with high rates of substance use disorder; and increasing funding for the National Institutes of Health’s Helping to End Addiction Long-Term research initiative. His third point indicates several ways he intends to stop the unnecessary prescription of opioids, including having states require prescriber participation in prescription drug monitoring programs and supporting the use of alternative pain treatments and development of less addictive pain medications. The final two points of former Vice President Biden’s statement focus on reducing the amount of illicit drugs entering the U.S. and diverting incarceration based solely on drug use to drug courts and treatment services.
Discussion
As the novel coronavirus pandemic continues, it spotlights the importance of mental health issues in the lead-up to the 2020 election. The pandemic is expected to not only exacerbate the existing mental health issues and barriers to care that people face, but to also increase the need for already limited mental health services. President Trump and former Vice President Biden have taken stances on several mental health issues, including the opioid crisis, rising suicide rates, and – to a more limited extent – parity in coverage for mental health services and nationwide shortages in the mental health workforce.
Suicide Prevention: Both of the presumptive 2020 presidential candidates give special attention to veterans in their suicide prevention plans and plan to expand access to mental health services through the VA health system.
Mental Health Workforce: Former Vice President Biden supports increasing the mental health workforce, including expansion of national service organizations such as the National Health Service Corps.
Mental Health Parity: The candidates do not provide specific plans to enforce the mental health parity requirements of the MHPAEA and ACA, and President Trump, more broadly, is arguing in court that the ACA should be invalidated.
Opioids: Both President Trump and former Vice President Biden have presented plans to expand access to treatment services such as medication-assisted treatment programs. In addition to this, former Vice President Biden emphasizes holding pharmaceutical companies and drug manufacturers accountable and intends to stop the overprescribing of opioids.
Beyond the candidates’ specific plans, a number of major election issues have implications for mental health, including immigration, gun violence, and the future of the ACA.
The subjects of immigration and border security remain prominent in President Trump’s reelection campaign. Several mental health experts have weighed in on the Trump administration’s policy of separating families at the U.S.’s southern border, raising concerns that children separated from their parents and detained at border facilities may be at substantially elevated risk of developing mental health conditions. Former Vice President Biden has stated he would end current practices of long-term detention, separating families, and workplace immigration raids.
President Trump has responded to recent mass shootings by arguing that gun violence is best addressed as a mental health issue. The Trump administration has considered researching whether technological devices can be used to monitor people with mental illnesses in order to prevent them from committing violent acts. However, most scientific evidence does not support a direct link between mental illness and gun violence, and instead suggests that people with mental illness are more likely to be victims of violence than perpetrators. Former Vice President Biden supports stronger gun control, including universal background checks and an assault weapons ban.
The future of the ACA remains uncertain, as the Trump administration has joined Texas and several other states in pushing to invalidate the law in Texas v. U.S. Because the ACA’s provisions require insurers to cover mental health care and substance abuse treatment, a ruling against the law would likely reduce access to these services for many Americans. Particularly if the ACA is struck down, these actions may limit the federal administration’s capacity to reduce opioid overdose deaths and suicide rates, and would undermine efforts to achieve parity for mental health coverage. Former Vice President Biden has criticized efforts to have the ACA invalidated. In an open letter written to President Trump on the tenth anniversary of the ACA, the former vice president highlighted the ACA’s role as a safety net during the coronavirus pandemic and the potential impacts of dismantling it. Former Vice President Biden’s proposed health care plan includes public option programs that would preserve ACA marketplaces and increase subsidies for marketplace plans.
This work was supported in part by Well Being Trust. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
KFF analysis of Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) (2018). Accessed at: https://webappa.cdc.gov/sasweb/ncipc/mortrate.html↩︎
This refers to Health Professional Shortage Areas (HPSA), which are used to identify areas and population groups within the United States that are experiencing a shortage of health professionals. There are three categories of HPSA designation based on the health discipline that is experiencing a shortage: 1) primary medical; 2) dental; and 3) mental health. The primary factor used to determine a HPSA designation is the number of health professionals relative to the population with consideration of high need. Federal regulations stipulate that, in order to be considered as having a shortage of providers, an area must have a population-to-provider ratio of a certain threshold. For mental health, the population to provider ratio must be at least 30,000 to 1 (20,000 to 1 if there are unusually high needs in the community). More information is available here: https://data.hrsa.gov/topics/health-workforce/shortage-areas↩︎
Every Friday we recap the past week in the coronavirus pandemic from our tracking, policy analysis, polling, and journalism.
With the Democratic National Convention held this week and the Republican National Convention scheduled for next, the 2020 general election season is officially kicking off and brings an even greater focus on the country’s coronavirus pandemic response as a campaign issue. KFF’s survey research team wrote a Policy Watch post analyzing voters’ increasingly negative opinions of President Trump’s handling of the pandemic, with the caveat that the President continues to garner strong support among his base of Republican voters – even those living in areas disproportionately impacted by the virus.
KFF traditionally produces content on where the candidates stand on the key health policy issues facing the country. This election year is no different, but the global pandemic has overshadowed other key issues that may have had more attention. The new slideshow, Health Care and the 2020 Presidential Election, compares President Trump’s record and former Vice President Joe Biden’s proposals on several issues, including the slide below on the COVID-19 response.
Here are the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: Total cases worldwide surpassed 22 million this week – with an increase of approximately 1.8 million new confirmed cases in the past seven days. There were also approximately 43,500 new confirmed deaths worldwide, bringing the total to nearly 794,000 confirmed deaths.
U.S. Cases and Deaths: Total confirmed cases in the U.S. reached nearly 5.6 million this week. There was an approximate increase of 325,000 confirmed cases between August 14 and August 20. Over 7,000 confirmed deaths in the past week brought the total in the United States to over 174,000.
Race/Ethnicity Data: As of August 17, Black individuals made up a higher share of cases/deaths compared to their share of the population in 31 of 49 states reporting cases and 32 of 46 states reporting deaths. In 6 states (MI, MO, IL, WI, KS, and ME) the share of COVID-19 related deaths among Black people was at least two times higher than their share of the total population. Hispanic individuals made up a higher share of cases compared to their share of the total population in 36 of 46 states reporting cases. In 5 states (NE, WI, MN, NH and SD), Hispanic peoples’ share of cases was more than 3 times their share of the population. COVID-19 continues to have a sharp, disproportionate impact on American Indian/Alaska Native as well as Asian people in some states.
Face Mask Requirements– Enhanced requirements: CT, GA, MS• Social Distancing Measures– Extended: GA, HI, FL, MS, NV– Paused: No states– Rolled back: NY– New restrictions: IL, OR
The Affordable Care Act’s preventive care provisions eliminated out-of-pockets costs for contraception for many insured women, but some are still paying these out-of-pocket costs.
In an article for Contraception: X, KFF’s Brittni Frederiksen, Matthew Rae, and Alina Salganicoff examine large employer plans to identify which types and brands of oral contraceptive pills have the largest shares of oral contraceptive users with out-of-pocket spending and which oral contraceptives have the highest average annual out-of-pocket costs.
The authors found 10% of oral contraceptive users in large employer plans still had out-of-pocket costs in 2018.
Brand name oral contraceptives with generic alternatives had the largest share of users with annual out-of-pocket spending and the three drugs with highest average annual out-of-pocket spending were brand names without generic alternatives.
President Trump and Democratic nominee Joe Biden hold widely divergent views on health issues, with the president’s record and response to the coronavirus pandemic likely to play a central role in November’s elections.
A new KFF side-by-side comparison examines President Trump’s record and former Vice President Biden’s positions across a wide range of key health issues, including the response to the pandemic, the Affordable Care Act marketplace, Medicaid, Medicare, drug prices, reproductive health, HIV, mental health and opioids, immigration and health coverage, and health costs.
The resource provides a concise overview of the candidates’ positions on a range of health policy issues. While the Biden campaign has put forward many specific proposals, the Trump campaign has offered few new proposals for addressing health care in a second term and is instead running on his record in office.
It is part of KFF’s ongoing efforts to provide useful information related to the health policy issues relevant for the 2020 elections, including policy analysis, polling, and journalism. Find more on our Election 2020 resource page.