KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
As the first doses of the new COVID-19 vaccine are delivered to health care workers and other early recipients, many Americans are eager to know not only when the vaccine will be available to them but also whether they will be able to get it at no cost.
The answer is that providers are not allowed to charge patients who get the vaccine, at least during the public health emergency, KFF experts write in a new issue brief. But it will be important to drive home that message to the public since some patients have been left with unexpected bills for COVID testing and treatment in spite of federal rules and programs, as well as voluntary efforts by insurers, designed to cover such costs.
Through Operation Warp Speed, the federal government has purchased hundreds of millions of doses of COVID-19 vaccines that are being distributed to providers at no cost. In turn, providers must agree to not charge for the vaccine itself. While providers can charge for the cost of administering the vaccine, private insurance and public programs will cover 100 percent of that cost during the public health emergency.
People who are uninsured also will not be charged for the vaccine. Providers who wish to be reimbursed for administering the vaccine must bill the federal government and cannot bill uninsured individuals. It will be important for the federal government to develop plans to strictly enforce these requirements to ensure that the public receives the vaccine for free as intended.
In the issue brief, KFF experts highlight the laws and regulations that are in place to ensure access to free COVID-19 vaccines for individuals regardless of their insurance status and explain how vaccine administration costs will be covered in private insurance, Medicare and Medicaid, and for the uninsured.
There will be many challenges convincing people to get the COVID-19 vaccine. Fear over unexpected costs need not be one of them.
As the initial COVID-19 vaccine doses become available to the public, it will be important to ensure people are aware that they can get the vaccine for free. New rules and legislative changes enacted since the pandemic hit eliminated cost sharing for the vaccine. However, people may still be concerned about costs because of their experiences getting COVID-19 tests and treatment. Despite rules requiring that COVID-19 tests be provided without cost sharing, some insured patients have faced unexpected out-of-pocket costs, and some uninsured patients have been left with large bills for COVID-19 treatment even with a Department of Health and Human Services’ (HHS) program in place that is intended to cover those costs. Patients were left with these bills due to gaps in the protections that Congress and the Trump administration put in place early in the COVID-19 pandemic. These gaps may lead some people to worry they could face unexpected out-of-pocket costs for the vaccine too. While making sure people trust that the vaccine is safe will be the highest priority, it will also be important to make sure that experiences with unexpected costs for COVID-19 testing or treatment do not deter people from getting vaccinated.
Loopholes that have led to out-of-pocket costs for COVID-19 testing
Gaps in the Families First Coronavirus Response Act (FFCRA) and the Coronavirus Aid, Relief, and Economic Security (CARES) Act leave some patients with private insurance unprotected when they get a COVID-19 test from an out-of-network provider—those providers are not limited in what they can charge patients and are allowed to bill patients directly for the entire cost of testing and related services, leaving insured patients to submit claims for reimbursement themselves. Federal law also does not prohibit out-of-network providers from balance billing for COVID-19 tests and related services. Instead, the law requires providers to publicly post their cash charges for testing and related services and requires insurers to reimburse the providers at their cash price if posted, but the law is silent on what insurers must pay for COVID-19 tests and related services rendered by out-of-network providers if no cash price has been posted. Additionally, COVID-19 testing may not qualify for coverage by private insurance if it is deemed to not be medically necessary, for example, testing for travel or employment. Patients with Medicare have more comprehensive coverage for COVID-19 testing with no cost sharing. This also is true for Medicaid enrollees while states are receiving enhanced federal matching funds tied to the COVID-19 public health emergency. After the public health emergency is lifted, some Medicaid enrollees may face nominal cost sharing, and some Medicaid adults (low-income parents, pregnant women, seniors, and people with disabilities who do not receive an “alternative benefit plan”) may not have coverage unless states choose to cover diagnostic tests.
Lack of comprehensive protections against out-of-pocket costs for COVID-19 treatment
In contrast to COVID-19 testing, there are few federal requirements related to COVID-19 treatment. For example, no changes were made to Medicare cost sharing rules, meaning that Medicare beneficiaries in traditional Medicare could face more than $1,400 in cost sharing if they are hospitalized for COVID-19 and do not have supplemental coverage, while those in Medicare Advantage could face higher or lower costs for a hospitalization depending on their plan. According to CMS guidance, Medicare Advantage plans may waive or reduce cost sharing for COVID-19-related treatments, and most Medicare Advantage insurers have announced that they are temporarily waiving such costs, but this is not required. While many private health insurers are also voluntarily and temporarily waiving cost sharing for COVID-19 treatment costs, privately insured patients—particularly those covered by self-insured employer-sponsored health plans—could face significant out-of-pocket expenses if they require hospitalization or other treatment for COVID-19. Additionally, privately insured patients with a confirmed or presumptive case of COVID-19 do have some protections against balance billing by out-of-network providers if the provider received federal grant funds intended to provide economic assistance during the pandemic. However, patients may not be aware of this protection and it is not clear how it is being enforced. Additional requirements were added to protect Medicaid beneficiaries from cost sharing for COVID-19 treatment. Similar to COVID-19 testing, state Medicaid agencies may not require cost sharing for COVID-19 treatment while receiving additional federal funding that is tied to the public health emergency. Once that requirement ends, Medicaid programs will be permitted to require nominal cost sharing.
Limitations in protections for uninsured COVID-19 patients
The Trump administration established a program through the federal Provider Relief Fund, to reimburse providers for care for uninsured COVID-19 patients, but narrow eligibility rules and voluntary participation by providers has limited the program’s reach. For example, only patients with a primary diagnosis of COVID-19 are eligible. Hospitalgroups have noted that this is particularly a problem for patients with sepsis caused by COVID-19. In those cases, coding protocols dictate that patients are coded with sepsis as their primary diagnosis and not COVID-19. Importantly, uninsured patients are not entitled to have their claims submitted to this program. Providers can decide on a case-by-case basis whether to submit claims; otherwise providers are not limited in what they can charge or try to collect from uninsured patients for COVID-19 testing or treatment. Providers that submit COVID-19 testing or treatment claims to this program are reimbursed based on Medicare rates.
Protections from cost sharing for COVID-19 vaccines
The federal government has purchased hundreds of millions of doses of COVID-19 vaccines through Operation Warp Speed, and those doses will be distributed at no cost to providers. Providers participating in the federal COVID-19 Vaccination program must agree to not charge for the federally purchased vaccine itself. Both private insurance and public programs will cover 100% of the administration fee, and providers cannot bill payers for the vaccine itself. Uninsured patients will not be charged for the vaccine and providers who wish to be reimbursed for vaccine administration must bill the federal government and cannot bill uninsured individuals. It will be important for the Trump administration and incoming Biden administration to develop plans to strictly enforce these requirements on insurers and providers to ensure that the public receives the vaccine for free as intended. The federal government should also put mechanisms in place so that any noncompliance that results in a bill to a patient can be resolved without cost or administrative burden for the patient.
As discussed in a recent KFF brief, laws and regulations ensure access to free COVID-19 vaccines for individuals regardless of their insurance status, although some of these protections are in effect only during the public health emergency or for the initial doses purchased through the COVID-19 Vaccination Program.
Private insurance: Private insurance subject to the Affordable Care Act’s requirement for plans to cover preventive services will have to cover the COVID-19 vaccine and, during the public health emergency, that requirement extends to vaccines administered by out-of-network providers. A combination of federal standards also limited what providers can charge for COVID-19 vaccine administration if they are out-of-network; federal regulation establishes Medicare rates as a reasonable reimbursement rate for the COVID-19 vaccine and administration fee. In addition, to receive or administer COVID-19 vaccines, providers must enroll in the federal COVID-19 Vaccination Program; conditions for participating in this program prohibit balance billing of insured patients for any amounts not covered by their insurance.
Medicare: Medicare beneficiaries will have coverage for the vaccine with no cost sharing through Medicare Part B.
Medicaid: Medicaid must cover the vaccine with no cost sharing as long as states are receiving enhanced federal funding that is tied to the public health emergency. People with limited Medicaid coverage (for example, coverage for family planning benefits only) are not covered by this requirement and are instead considered to be uninsured for the purposes of COVID-19 vaccination. Once states are no longer receiving additional federal funds tied to the public health emergency, COVID-19 vaccine coverage would be optional for some adults. If states did not opt to cover COVID-19 vaccines, those adults would likely be considered to be uninsured for the COVID-19 vaccine. While the FFCRA rules do not apply to CHIP, states must cover recommended vaccines for children with no cost sharing in their CHIP programs.
Uninsured: People who are uninsured or do not have coverage for vaccines can obtain the vaccine for free from any provider administering the initial doses funded by the government. Providers that participate in the CDC COVID-19 Vaccination Program must agree to not seek any reimbursement from a vaccine recipient. Instead, providers can bill the Provider Relief Fund for reimbursement of vaccine administration costs for people who are uninsured. About $25 billion remains in the fund that will be used to reimburse providers for vaccine distribution, although that fund has also been used to provide grants to providers and to reimburse for care for uninsured COVID-19 patients. Once federally purchased doses through the COVID-19 Vaccination Program are used up, uninsured patients and others who do not have coverage for the COVID-19 vaccine could face out-of-pocket costs for both the vaccine and its administration.
It will be important for vaccination information campaigns to educate the public about the COVID-19 vaccine with the clear message that the initial doses will be free to everyone. Without this assurance, some people may worry they will face out-of-pocket costs for the vaccine. The CDC should also ensure that Vaccine Program providers know that they cannot directly bill patients for COVID-19 vaccine administration. This will help avoid billing errors and noncompliance with federal requirements. There will be many challenges convincing people to get the vaccine. Fear over unexpected costs need not be one of them.
Poll: Large Majorities Now Say They Wear Masks Regularly and Can Continue Social Distancing for At Least Six Months if Needed, though Republicans Remain Less Likely to Take Such Precautions
At Least Two-thirds of the Public Favor Changes to Expand Coverage and Negotiate Drug Prices Put Forward by President-Elect Biden
As winter sets in and COVID-19 cases and deaths reach records in most parts of the country, more Americans say they wear masks every time they leave home now (73%) than said so in May (52%), a new KFF Health Tracking Poll finds.
A small minority (11%) say they wear masks only some of the time or never. This group is more likely to be white (70%), male (65%) and Republican (54%).
In addition, 7 in 10 Americans (70%) say that they can continue to follow social distancing guidelines to limit COVID-19’s spread for at least another six months if necessary. Only small shares say they could follow such guidelines less than another month (4%) or not at all (9%).
There are big partisan differences, with an overwhelming majority of Democrats (87%) and just half of Republicans (50%) saying they can follow these guidelines at least six months or until a vaccine is widely available. One in five (20%) Republicans say they can’t follow the guidelines at all.
The willingness to wear masks and follow social distancing comes as two thirds (68%) of the public worry that they or someone in their family will get sick from coronavirus. This marks the highest level of concern recorded since KFF began asking the question in February. As in the past, Democrats worry more about this risk than Republicans.
In addition, half (51%) of adults say that worry or stress related to the pandemic has had a negative impact of their mental health, similar to July (53%). This includes a quarter (25%) who say it has had a major impact. Women and young adults are more likely than men and older adults to report negative mental health impacts.
Fielded just before the Food and Drug Administration approved any COVID-19 vaccines, the poll finds half (51%) of the public say the “worst is yet to come” in the pandemic, up from a low of 38% in September. Democrats are more than twice as likely as Republicans to feel that way (72% v. 32%), with independents in the middle (50%).
“Republican denialism mirroring President Trump, even in the face of a growing epidemic in red states, has become a real public health challenge that the incoming administration will need to take on,” KFF President and CEO Drew Altman said.
The poll also gauges the public’s views on several proposals to negotiate drug prices and to expand access to affordable health coverage that President-elect Biden promoted during the 2020 campaign.
On drug prices, nearly 9 in 10 (89%) favor allowing the federal government to negotiate with drug companies to get a lower price for both Medicare and private insurance. This includes large shares of Republicans (84%) and independents (87%) as well as nearly all Democrats (97%).
On coverage expansions, large majorities support guaranteeing health insurance coverage to lower-income people in states that have not expanded their Medicaid program under the Affordable Care Act (76%); having a government-administered “public option” heath plan available to all Americans (71%); expanding government financial help for those who buy their own insurance on the ACA marketplace (66%); and lowering the age when people become eligible for Medicare from 65 to 60 (65%).
There is a wider partisan divide on the coverage proposals, with Democrats generally most supportive and Republicans least supportive – though about half of Republicans favor guaranteeing coverage to low-income people in states that have not expanded Medicaid (54%) and lowering Medicare’s age of eligibility (51%).
A large majority (80%) – including majorities across parties – also favor protecting patients from surprise medical bills from out-of-network providers, which is the subject of bi-partisan legislation being worked on in Congress.
As part of his campaign, President-elect Biden focused on protecting and building upon the Affordable Care Act to expand access to affordable health coverage. Most of the public wants the incoming administration and Congress either to build on the ACA (48%) or keep it as is (14%). Fewer want to scale it back (9%) or repeal it entirely (20%).
As with the ACA overall, there are large partisan divisions, with most Democrats and independents wanting to build on what the law does or keep it as is, while most Republicans want to scale it back or repeal it entirely.
Designed and analyzed by public opinion researchers at KFF, the survey was conducted from Nov. 30-Dec. 8 among a nationally representative random digit dial telephone sample of 1,676 adults, including oversamples of adults who are Black (390) or Hispanic (298). Interviews were conducted in English and Spanish by landline (391) and cell phone (1,285). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher
As the country hits record numbers of cases, hospitalizations, and deaths, pessimism about the trajectory of the coronavirus pandemic continues to increase. Half of adults now say the worst is yet to come, returning to levels measured in May. Moreover, the share of the public who say they are worried that they or someone in their family will get sick from coronavirus is at its highest point since KFF began tracking this question in February (68%).
With a COVID-19 vaccine on the horizon, most adults (70%) say they can continue adhering to social distancing guidelines for six months or more, or until a vaccine is widely available. As some states and localities impose new stay-at-home orders and place restrictions on some businesses in efforts to limit the spread of coronavirus, about four in ten adults think their state has about the right amount of restrictions on businesses and on individuals. About half of Democrats (49%) say their state does not have enough restrictions on businesses, while half of Republicans (50%) say their state has too many restrictions.
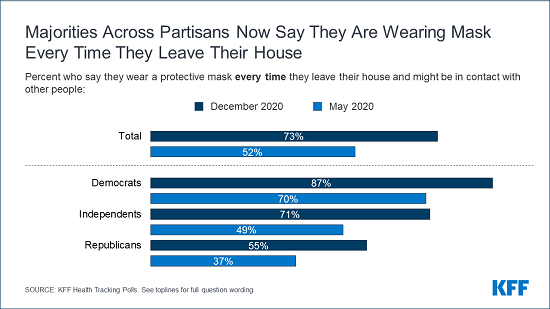
Compared to May, a larger share now say they wear a mask every time they leave home (73%, up 21 percentage points since May, including increases across partisans and age groups).
Reflecting the large share who say they consistently wear face masks, most of the public think wearing a mask to help prevent the spread of COVID-19 is part of everyone’s responsibility (73%), though Republicans are more divided with half saying it is everyone’s responsibility to help protect the health of others and 45% saying it is a personal choice.
Majorities of the public want the incoming Biden administration and Congress to either build on the Affordable Care Act (ACA) or keep it as it is (62%), though partisans differ. There is bipartisan support for President-elect Biden’s proposal to allow the federal government to negotiate with drug companies to get a lower price on medications (89%). While majorities of the public favor guaranteeing health insurance coverage to lower-income people whose states have not expanded their Medicaid program (76%), establishing a public option (71%), expanding government financial help for those who buy their own insurance on the marketplace (66%) and lowering the Medicare eligibility age to 60 (65%), fewer Republicans are supportive of these proposals.
Growing Pessimism About The Coronavirus Outbreak
With coronavirus cases and hospitalizations at record highs across the country, the latest KFF Health Tracking Poll finds the public feeling increasingly negative about the trajectory of the pandemic. Half of adults (51%) think the worst is yet to come – an increase from September and October when about four in ten thought the worst was still ahead. One quarter of the public (25%) say the worst of the outbreak is behind us and about one in five say they do not think coronavirus is or will be a major problem in the U.S. (19%).
Among partisans, seven in ten Democrats (72%) say the worst is yet to come. Notably, about a third (32%) of Republicans now say the worst of the pandemic is yet to come, twice as many as in October (15%). Among independents, half say the worst of coronavirus is yet to come (50%) while 28% say that the worst is behind us. About six in ten Black adults (62%) – a group that has been disproportionally affected by coronavirus – say the worst of the coronavirus outbreak is yet to come while about half of White adults (53%) and four in ten Hispanic adults (41%) say the same.
Figure 1: Half Of Adults Say The Worst Of The Coronavirus Outbreak Is Yet To Come
The U.S. recently hit a COVID-19 daily death record, with more than 3,000 people dying from the disease in a single day. Three in ten adults say they are “very worried” they or a family member will get sick from coronavirus and a further 38% say they are “somewhat worried”. About eight in ten Democrats say they are worried they or a family member will get sick, including 42% who are “very worried”. While a majority of independents (68%) say they are at least “somewhat worried” that they or a family member will get sick from coronavirus, fewer than half of Republicans express this concern (46%).
Notably, about three in four Black adults (75%) and Hispanic adults (77%) say they are worried they or a family member will get sick from coronavirus while about two in three White adults (64%) express this concern.
Figure 2: Majorities Of Democrats And Independents Are Worried That They Or Someone In Their Family Will Get Sick From Coronavirus
Amidst the worsening outbreak, the share of the public who say they are “very worried” or “somewhat worried” that they or someone in their family will get sick from coronavirus is at its highest point since KFF began tracking this question in February, with 68% now saying they are worried. The share of Democrats and independents who say they are worried they or a family member will get sick was similar in October but lower in April when slight majorities said they were worried (56% of Democrats, 54% of independents). Since early April, fewer than half of Republicans have said they are worried they or a family member will get sick from coronavirus.
Figure 3: Compared To February, Larger Shares Across Partisans Say They Are Worried They Or A Family Member Will Get Ill From Coronavirus
Ten months after coronavirus began spreading through the country, half of adults (51%) say worry or stress related to the pandemic has had a negative impact on their mental health, including one in four who say it has had a major impact. This is similar to the share in July who said pandemic-related stress and worry had a negative impact on their mental health (53%), and higher than the share who said the same in May (39%). Women are more likely than men to say their mental health has been negatively impacted by the coronavirus outbreak (57% vs. 44%). Similarly, younger adults ages 18 to 29 are more likely than their older counterparts to say stress and worry about the pandemic has had a negative impact on their mental health. The economic impacts of the pandemic are also taking a toll as six in ten adults whose household lost a job or income due to the pandemic say stress and worry related to coronavirus has had a negative impact on their mental health.
Figure 4: About Six In Ten Women, Young Adults, Black Adults, And Those Who Have Had Financial Impact Report Mental Health Impact
With the promise of a vaccine on the horizon, seven in ten adults say they can continue to follow social distancing guidelines for more than six months or until a vaccine is widely available. Majorities of Democrats (87%) and independents (68%) say they can keep following social distancing guidelines for another six months or longer or until a vaccine is available, and half of Republicans say the same. Notably, one in five Republicans say they cannot follow social distancing guidelines at all.
Figure 5: Most Say They Can Keep Up Social Distancing Guidelines For More Than Six Months, Or Until A Vaccine Is Widely Available
The reluctance of some Republicans to follow social distancing guidelines may stem from the perception that the seriousness of coronavirus is being exaggerated. Overall, the public is divided on whether news coverage of coronavirus is exaggerating its seriousness (35%) or presenting it correctly (36%), while one in four think the seriousness of coronavirus is underestimated (25%).
Partisans Are Divided On State Restrictions For Businesses, Individuals
In response to rising cases, some states and localities have instituted stay-at-home orders and placed restrictions on some businesses in an attempt to slow the spread of coronavirus. Four in ten adults say their state has about the right amount of restrictions on businesses (40%) and on individuals (42%) in its efforts to slow the outbreak. However, about a third of the public think their state does not have enough restrictions on businesses (32%) and individuals (36%), while one in four say their state has too many restrictions on businesses and one in five say there are too many restrictions on individuals.
There is a stark partisan divide on this issue. While about half of Democrats (49%) say their state does not have enough restrictions on businesses, a similar share of Republicans (50%) say their state has too many restrictions. Similarly, while a slight majority of Democrats (53%) say their state does not have enough restrictions on individuals in its efforts to limit the spread of coronavirus, about four in ten Republicans (43%) say their state has too many restrictions. Among independents, pluralities say their state has about the right amount of restrictions on businesses (45%) and on individuals (42%).
Figure 6: About Half Of Democrats Think Their State Currently Does Not Have Enough Restrictions On Businesses, Individuals
Larger Shares Of The Public Now Wearing Masks Every Time They Leave Home Than in May
Recentmediacoverage has highlighted the politicization of face mask use. Overall, about three in four adults say they wear a protective mask every time they leave their house and may be in contact with other people (73%). While large majorities across partisans – including three in four Republicans (76%) – say they use a mask at least “most of the time” they leave home, large shares of Democrats (87%), and independents (71%) say they wear a protective mask every time they leave their house, compared to fewer Republicans (55%).
Figure 7: Majorities Across Parties Say They Wear A Protective Mask Every Time They Leave Their House
Compared to May, there has been a marked increase in the share of the adults who say they wear a mask every time they leave home. About three in four adults now say they wear a mask every time, up 21 percentage points since May. The share who say they wear a protective mask every time they leave home has increased by double digit percentage points across partisans and across age groups since May.
Figure 8: Compared to May, Public Is Now Much More Likely To Say They Wear A Mask Every Time They Leave Home
Who is not regularly wearing face masks?
With mask mandates in place in many parts of the country, most of the public say they are wearing masks at least most of the time they leave home and may be in contact with other people. However, a small minority of the public (11%) say they wear protective masks only some of the time of never. This group is disproportionately White (70%), male (65%), and Republican (54%), and is more likely to have no college education compared to those who report wearing masks more consistently.
The reported increase in consistent mask use reflects the attitude held by 73% of adults that wearing a mask to prevent the spread of COVID-19 is “part of everyone’s responsibility to protect the health of others.” While an overwhelming majority of Democrats (93%) and a large majority of independents (70%) say wearing a mask is everyone’s responsibility to protect public health, Republicans are more divided on this issue with half (50%) saying it is everyone’s responsibility and a similar share saying it is a personal choice (45%).
Figure 9: About Seven In Ten Say Wearing A Mask Is Part Of Everyone’s Responsibility To Prevent The Spread Of COVID-19
The view of mask wearing as a personal choice or a part of everyone’s responsibility appears related to personal mask use. Those who think wearing a mask to prevent the spread of COVID-19 is everyone’s responsibility are more than twice as likely as those who think it is a personal choice to say they wear a mask every time they leave their house and may come in to contact with others (85% vs. 37%).
Figure 10: Those Who See Wearing A Mask As A Personal Choice Are Far Less Likely To Say They Wear One Every Time They Leave Home
Most of the public correctly knows that wearing a face mask can help limit the spread of coronavirus (78%) and that wearing a face mask is not harmful to your health (77%). Last month, the Centers for Disease Control stated that wearing a mask can help provide protection from the coronavirus for the wearer. Most adults think that is indeed the case with 70% saying a face mask helps protect them from coronavirus.
Figure 11: Most Of The Public Know The Public Health Benefits Of Wearing A Masks To Help Limit The Spread Of Coronavirus
Nonetheless, though most of the public knows these key facts about face mask use as a preventative measure against coronavirus, a third hold at least one misconception. Notably, a majority of Republicans (54%) hold at least one misconception about face masks, including 44% who say wearing a face mask does not help protect you from coronavirus. Among adults who believe at least one misconception about face masks, six in ten (61%) say they think the seriousness of coronavirus is being exaggerated and half say wearing a mask is a personal choice (50%).
Table 1: Misconceptions of Coronavirus Face Mask Use by Party Identification
Total
Party ID
Democrats
Independents
Republicans
Percent who believe in at least one misconception:
34%
14%
38%
54%
Percent who say:
…wearing a face mask does not help protect you from coronavirus
25
6
29
44
…wearing a face mask is harmful to your health
21
8
22
34
…wearing a face mask does not help limit the spread of coronavirus
17
4
19
33
President-Elect Biden’s Potential Health Care Agenda
While addressing the pandemic will undoubtedly be a top priority for the incoming Biden administration, there are other health care proposals – some of which have bipartisan support – that may also serve as cornerstones in Biden’s health care agenda.
Two health care priorities that have bipartisan support are price transparency and legislation aimed at curbing surprise medical bills. President Trump recently announced new transparency requirements which will require employer-based group health plans to disclose price and cost-sharing information to enrollees, and Congress is working on a bi-partisan bill to protect patients from surprise out-of-network medical bills. There is some hope that the legislation to address surprise bills will pass Congress before the end of the year. The latest KFF polling finds large majorities of the public – including majorities across partisans – favor making information about the price of doctors’ visits, tests, and procedures more available to patients (93%) and favor legislation aimed at protecting patients from high out-of-network surprise medical bills (80%).
Figure 12: Large Majorities Favor Price Transparency, Action To Protect Patients From Surprise Medical Bills
Majorities of the public also favor many of the key health care proposals put forth by President-elect Joe Biden including large shares that favor allowing the federal government to negotiate with drug companies to get a lower price on medications that would apply to both Medicare and private insurance (89%). Support is high across partisans with more than eight in ten Democrats (97%), independents (87%) and Republicans (84%) supporting this proposal. A majority across partisans also favor guaranteeing health insurance coverage to lower-income people whose states have not expanded their Medicaid programs (76% overall, 95% of Democrats, 74% of independents, and 54% of Republicans). Overall, a majority also favor other aspects of President-elect Biden’s health care agenda asked about including about seven in ten overall who favor having a government-administered heath plan available as a public option to all Americans (71%), and about two-thirds who favor expanding government financial help for those who buy their own insurance on the marketplace (66%), and lowering the age when people become eligible for Medicare from 65 to 60 (65%).
Figure 13: Majorities Favor Key Health Care Proposals Put Forward By President-Elect Joe Biden
However, Democrats and Republicans diverge on Biden’s proposals that are aimed at expanding health care coverage. While an overwhelming majority of Democrats (95%) favor guaranteeing health insurance coverage to lower-income people whose states have not expanded their Medicaid program, a smaller majority of Republicans (54%) support this proposal. Likewise, more than nine in ten Democrats support a public option compared to less than half of Republicans who say the same (92% vs. 45%).
Currently, most adults only qualify for Medicare health care benefits once they reach the age of 65. Nearly two-thirds of adults – including majorities of Democrats and independents and half of Republicans – favor Biden’s proposal to lower the age when people become eligible for Medicare from 65 to 60. While seven in ten adults ages 18 to 64 (70%) support lowering the Medicare eligibility age to 60, fewer than half of adults 65 and over (46%) favor this proposal.
Table 2:Support for President-Elect Biden’s Proposed Health Care Policies
Percent who say they favor each of the following health care proposals:
Total
Party ID
Democrats
Independents
Republicans
Allowing the federal government to negotiate with drug companies to get a lower price on medications that would apply to both Medicare and private insurance
89%
97%
87%
84%
Guaranteeing health insurance coverage to lower-income people whose states have not expanded their Medicaid program
76
95
74
54
Having a government-administered health plan, sometimes called a public option, that would compete with private health insurance plans and be available as an option to all Americans
71
92
71
45
Expanding government financial help for those who buy their own insurance on the marketplace
66
84
64
48
Lowering the age when people become eligible for Medicare from 65 to 60
65
79
61
51
Most Want To Build On The ACA Or Keep It As Is
In November, the Supreme Court heard arguments in the California v. Texas case challenging the constitutionality of the 2010 Affordable Care Act. The Trump administration submitted a brief in this case asking the Supreme Court to overturn the law. President-elect Joe Biden repeatedly voiced his support for the Affordable Care Act during his campaign and recently selected California Attorney General Xavier Becerra, who has been a strong defender of the ACA in court, as his pick for Secretary of Health and Human Services. The latest KFF Heath Tracking poll finds about half of the public (53%) have a favorable view of the ACA while 34% have an unfavorable view of the law.
Figure 14: Larger Shares Of The Public View The ACA Favorably Than Unfavorably
Building on the ACA has been a focal point for Joe Biden’s presidential bid, as he has proposed creating a government-run public option health care plan that will compete with private insurers and be available for all Americans. Nearly half of adults want the incoming presidential administration and Congress to build on what the ACA does (48%). A smaller share want to keep the law as it is (14%) and about three in ten want to either scale back what the law does (9%) or repeal it entirely (20%). Partisans differ on these approaches, with three in four Democrats wanting the incoming administration and Congress to build on what the law does (74%) and six in ten Republicans wanting the law to be scaled back (15%) or repealed entirely (44%).
Figure 15: Most Want To Build On The ACA Or Keep It As Is, Though Partisans Differ
The Trump administration both shortened the open enrollment period for the ACA marketplaces and decreased funding for marketing and outreach efforts that publicize the enrollment period, eligibility, and process. With the enrollment deadline in many states having just recently passed and in other states quickly approaching, the latest KFF Health Tracking poll finds that just one in seven adults under age 65 who either buy their own insurance or are uninsured, and thus likely the target for ACA marketplace plans, are aware of the correct closing date for enrollment (14%). A possible action the incoming Biden administration may take to help further strengthen the ACA would be to restore funding for marketing and outreach to help Americans who want to buy their own insurance through the ACA marketplaces.
Figure 16: Few Know The Marketplace Deadline For Signing Up For Their Own Health Insurance
Methodology
This KFF Health Tracking Poll was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted November 30- December 8, 2020, among a nationally representative random digit dial telephone sample of 1,676 adults ages 18 and older (including interviews from 298 Hispanic adults and 390 non-Hispanic Black adults), living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). Phone numbers used for this study were randomly generated from cell phone and landline sampling frames, with an overlapping frame design, and disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. The sample also includes interviews completed with respondents who had previously completed an interview on the KFF Tracking Poll (n =267) or an interview on the SSRS Omnibus poll (and other RDD polls) and identified as Hispanic (n = 80; including 14 in Spanish) or non-Hispanic Black (n=179). Computer-assisted telephone interviews conducted by landline (391) and cell phone (1,285, including 947 who had no landline telephone) were carried out in English and Spanish by SSRS of Glen Mills, PA. To efficiently obtain a sample of lower-income and non-White respondents, the sample also included an oversample of prepaid (pay-as-you-go) telephone numbers (25% of the cell phone sample consisted of prepaid numbers) Both the random digit dial landline and cell phone samples were provided by Marketing Systems Group (MSG). For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s 2019 U.S. American Community Survey (ACS), on sex, age, education, race, Hispanic origin, and region, within race-groups, along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the January- June 2019 National Health Interview Survey. The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample, and design modifications, namely, the oversampling of prepaid cell phones and likelihood of non-response for the re-contacted sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
To help support states and promote stability of coverage amidst the COVID-19 pandemic, the Families First Coronavirus Response Act (FFCRA) provides a 6.2 percentage point increase in the federal share of certain Medicaid spending with requirements to meet certain maintenance of eligibility (MOE) requirements that include ensuring continuous coverage for current enrollees. Under a new Interim Final Rule (IFR), The Centers for Medicare and Medicaid Services (CMS) has reinterpreted the MOE to allow states to decrease benefits, increase cost-sharing, and in some cases, terminate enrollment for people considered not “validly enrolled” or change eligibility groups while still receiving increased federal matching funds. The MOE requirements are tied to the Public Health Emergency (PHE) period, but specific requirements expire at different times. This brief provides an overview of these MOE requirements, examines what happens when the MOE expires, and discusses key issues to consider looking ahead. Key findings include the following:
Under the IFR, as of November 2, 2020, states are now allowed to increase cost-sharing and eliminate optional benefits and still be in compliance with MOE requirements. In addition, states are required to transition most enrollees determined ineligible for their current coverage to different coverage pathways for which they are eligible if such a transition is in the same tier of coverage (though it may cover fewer benefits or have higher patient cost-sharing).
CMS has also released an informational bulletin for states affirming current eligibility renewal and redetermination rules but has not yet provided additional guidance on policies for the end of the PHE. Clear guidance with sufficient lead time will be key for helping states establish policies and processes to clear renewal backlogs when the MOE requirements end.
The change in Presidential administration will have implications for MOE requirements, states and beneficiaries. The new Biden Administration will face decisions around continuing to extend the PHE, revising the current MOE rules and about guidance for renewals post PHE. The incoming administration could also work with Congress to pass legislation to extend the amount and duration of the fiscal relief and MOE.
What are the MOE requirements for states?
The FFCRA provides a 6.2 percentage point increase in the federal share of Medicaid spending with requirements to maintain eligibility. The increase does not apply to Affordable Care Act (ACA) Medicaid expansion adults, for whom states continue to receive a 90% federal matching rate. The Federal Medical Assistance Percentage (FMAP) increase was retroactive to January 1, 2020, and is in place until the end of the quarter in which the PHE ends.
The law requires states to meet certain MOE requirements as a condition of receiving the enhanced funding. States must apply Medicaid eligibility standards, methodologies, and procedures that are no more restrictive than those in effect on January 1, 2020. States cannot increase Medicaid premiums above those in effect on January 1, 2020.1,2,3 States must cover coronavirus testing and COVID-19 treatment services, including vaccines, without cost-sharing. States cannot increase political subdivisions’ contributions to the non-federal share of Medicaid costs beyond what was required on March 1, 2020.4
The MOE requirements also provide continuous coverage for current enrollees. Specifically, states must provide continuous eligibility through the end of the month in which the PHE ends for those enrolled as of March 18, 2020, or at any time thereafter during the PHE period. In guidance to states through FAQs, CMS originally interpreted the MOE to allow states to act on changes in circumstances to move individuals into eligibility categories that provide additional benefits but prohibited states from moving individuals into eligibility categories with fewer benefits.5 The original guidance further prohibited states from increasing cost-sharing or restricting benefits.
CMS released an IFR updating (and in some instances reversing) its interpretation of the MOE continuous coverage requirements effective November 2, 2020.6While most enrollees may not be disenrolled until the end of the month in which the PHE ends, this rule reverses prior guidance and requires states to follow regular program rules on changes in circumstances by moving beneficiaries to an eligibility category with coverage within the same “tier” or into a category with more comprehensive coverage (but not to a lower tier of coverage) if they are determined ineligible for their current coverage.7 This could result in some changes in benefit packages or cost-sharing which were not permitted under the original guidance.8 The rule defines three “tiers” of coverage: minimum essential coverage (MEC);9 coverage that is not MEC but includes COVID-19 testing and treatment services, and more limited benefit packages that do not include COVID-19 testing and treatment (e.g., family planning). If an enrollee is determined no longer eligible for Medicaid under any eligibility pathway, states must maintain the same coverage through the end of the month in which the PHE ends. 10 States also cannot disenroll individuals for procedural reasons such as failure to respond to notices requesting additional information. Table 1 provides selected examples of eligibility, benefits, and cost-sharing changes under the interim final rule.
Table 1: Selected Examples of Medicaid Eligibility Changes Under the FMAP MOE
If ineligible for another full-benefit group, remain in low-income child group.
Young adult turns 21
Continue providing EPSDT
Stop providing EPSDT
ACA expansion adult turns 65
Remain enrolled in expansion group. Add Medicare Savings Program (MSP) group if eligible for Medicare cost-sharing assistance
Terminate expansion group enrollment and enroll in another full-benefit Medicaid group if eligible. Also enroll in MSP group if eligible.
If ineligible for another full-benefit Medicaid group or MSP, continue expansion group enrollment (even if receiving Medicare).
Woman reaches end of 60 day post-partum period
Remain enrolled in pregnant woman group
If eligible for another full benefit group, such as ACA expansion, and benefit package for new group is the same or more generous than pregnant woman benefit package, move to new group.
If pregnant women benefit package is not MEC but does include COVID testing and treatment, and person is ineligible for any full benefit group, remain enrolled in pregnant woman group.
Nursing home resident has increased income
Do not increase patient liability (cost-sharing)
Increase patient liability (cost-sharing)
Person receiving LTSS moves from community to nursing home
Do not decrease personal needs allowance (do not increase cost-sharing)
Decrease personal needs allowance (resulting in increased cost-sharing)
Child or pregnant woman loses qualifying immigration status in states that opt to waive 5-year bar
Move from full benefit group to emergency Medicaid only
Same outcome as under prior guidance.
Person loses eligibility for family planning group or another limited benefit package that is not MEC and does not cover COVID testing and treatment
Remain enrolled in limited benefit package unless eligible for a full benefit group
Remain enrolled in limited benefit group, unless eligible for group with MEC or COVID testing and treatment (do not move to another limited benefit package group).
Person fails to respond to state request for additional information (such as follow up to quarterly wage data check)
Remain enrolled in current group (do not terminate eligibility on a procedural basis).
The rule allows states to terminate Medicaid coverage during the PHE for those not “validly enrolled.” CMS describes the rule as a presumption that most people are “validly enrolled” with limited exceptions11 but also allows states to terminate coverage for individuals not “validly enrolled,” defined as those who have been convicted of fraud or have a formal finding of abuse that is material to the eligibility determination or by agency error. These rules apply to all initial eligibility determinations as well as to redeterminations and renewals that were completed prior to March 18, 2020. The rule also confirms that individuals determined presumptively eligible but who have not yet received a final eligibility determination are not “validly enrolled.” Prior to terminating coverage of anyone not “validly enrolled,” states must follow regular Medicaid rules, including reviewing all other potential bases of eligibility and providing advance notice and the opportunity for a fair hearing. States are also allowed to terminate coverage for those who are no longer residents under limited circumstances12 as well as anyone who is deceased.
The IFR reverses earlier guidance by allowing states to make benefit and cost-sharing changes and continue to receive the FMAP bump. States may eliminate optional benefits as well as change the scope of benefits, such as service authorization criteria. States may also establish or increase cost-sharing and increase the patient liability amount for those receiving long-term services and supports (LTSS) under post-eligibility treatment of income rules.
By drawing down the enhanced federal funds, states are indicating to CMS that they will comply with the MOE conditions.13 CMS will not require a separate demonstration of compliance from states but will allow states to passively attest by drawing down the funds. If CMS later determines that the state does not satisfy all of the conditions, the state must return the enhanced funds.14 CMS has stated it is not aware of any states not taking enhanced federal funds.15
Beyond the MOE requirements, states can streamline eligibility and enrollment processes to help connect people to coverage more quickly, and many are doing so through emergency authorities. Nearly all (47) states are making changes to streamline eligibility and/or enrollment through State Plan Amendments (SPAs) or other administrative authority beyond what is required to access the enhanced federal funding. States can make changes through a regular SPA or Disaster-Relief SPA as well as other authorities. States have flexibility to expand eligibility or modify eligibility rules, eliminate or waive premiums, and streamline application and enrollment processes. Specific actions states are taking include expanding Medicaid coverage to optional groups, allowing increased used of self-attestation to expedite enrollment, eliminating premiums, as well as expanded use of presumptive eligibility.
What happens when MOE requirements end?
The MOE requirements are tied to the COVID-19 PHE period, but specific requirements expire at different times (Appendix Table 1). The PHE ends when the Secretary declares that the emergency no longer exists, or after 90 days, whichever happens first, although the Secretary can renew the PHE declaration for subsequent periods.16 The most recent declaration extended the PHE until January 20, 2021. The Department of Health and Human Services (HHS) has not specified if the PHE will be renewed again, but if not already extended, the incoming Biden Administration is expected to extend the PHE in response to increasing coronavirus cases across the country. The requirement for states to provide continuous eligibility to enrollees expires the last day of the month in which the PHE ends (“continuous eligibility period”). The other four MOE requirements and the enhanced FMAP funding last through the end of the quarter in which the PHE ends (“MOE period”). State policy changes to streamline eligibility and enrollment through Disaster-Relief SPAs will also expire at the end of the PHE. As such, states may consider whether to continue those changes through regular SPA authority or revert to pre-pandemic policies. Changes that states have made to verification processes through a verification plan disaster addendum, such as accepting self-attestation for eligibility criteria, are also tied to the emergency period, but the exact end date varies based on state option.
After the end of the PHE, states must resume renewals and redeterminations in accordance with current Medicaid rules. These rules differ somewhat for enrollees whose eligibility is based on modified adjusted gross income (MAGI groups, including pregnant women, low-income parents, and low-income children) and non-MAGI enrollees (groups where eligibility is based on old age or disability).
States must first conduct an ex parte (passive) renewal based on available data sources. If a passive renewal is unsuccessful, states must send a prepopulated form that requests any needed information to MAGI enrollees while states can choose to send a prepopulated form to non-MAGI enrollees.
If eligibility is terminated due to failure to timely respond to a renewal request, states must provide a 90 day reconsideration window where individuals in MAGI groups can provide the necessary information to re-establish eligibility without completing a new application; the 90-day reconsideration period is optional for non-MAGI groups. 17
For MAGI populations, states may only renew eligibility once every 12 months unless the state receives information from the beneficiary or through data sources indicating a change in circumstances that may affect eligibility. Eligibility for non-MAGI groups must be renewed at least once every 12 months, and more frequently at state option.
All enrollees must report changes in circumstances that may affect eligibility in a timely manner, and states must promptly address any changes by redetermining eligibility.18 Federal rules also generally require states to use current income and determine eligibility on “all bases” before determining an enrollee ineligible.19 States must provide beneficiaries with advance written notice of the termination at least 10 days in advance and inform the individual of their right to a fair hearing.20
CMS issued an informational bulletin on December 4, 2020, that reiterates these current renewal and redetermination rules for states but does not address processes at the end of the PHE. CMS is encouraging states to conduct renewals and redeterminations to the extent possible during the PHE and plans to issue more specific guidance later about the end of the PHE.21 This guidance could include more specific instructions to states about policies and processes for addressing redetermination and renewal backlogs that may have accumulated during the PHE, when data matches for income must be conducted, when to determine current income (for example, when states must conduct another updated eligibility determination to check for subsequent changes in circumstances for individuals who maintained eligibility only due to the MOE), and what notices will be required when the PHE ends. Prior to the PHE, CMS had encouraged states to enhance verification processes and conduct periodic data checks, which may have contributed to enrollment declines.
What are the key questions looking ahead?
How will states implement requirements and options in the new IFR? It is unclear how many individuals will be transitioned to alternative eligibility pathways within the same coverage tier, how enrollees will be notified of such a change, and how administratively challenging such transitions will be for states. The recent CMS bulletin also affirms current rules that if an individual is determined eligible following a change in circumstances, states can start a new 12-month renewal period if all other eligibility criteria can be verified. While few states have used this option, more states may use this option to help stagger renewals following the end of the PHE. In addition, it will be important to watch if states restrict benefits or increase cost-sharing, particularly as Governors develop budgets for the upcoming fiscal year and states continue to face economic pressures and reduced revenues.
Will the PHE be extended and for how long? The current PHE declaration expires on January 20, 2021, and it is expected it will be extended either by the current Administration or under by the Biden Administration for at least another 90 days. If the PHE is not extended, continuous coverage requirements will end on January 31, 2021, and the enhanced FMAP and other MOE requirements will expire on March 31, 2021. State eligibility and enrollment flexibilities through Disaster-Relief SPAs during the PHE will also expire. Providing more transparency or clarity on how long the PHE is likely to remain in place will be helpful to states as they prepare for when continuous coverage and other MOE requirements end.
Will CMS issue additional guidance to help states manage backlogs and establish redetermination policies and processes when the MOE requirements expire? States will have a backlog of renewals and redeterminations for individuals whose renewal date fell during the continuous eligibility period when MOE requirements end. The Medicaid and CHIP Payment Advisory Commission (MACPAC) sent a letter to HHS requesting that states be provided with at least 90 days’ notice prior to the end of the PHE to plan for the end of enhanced federal match rate. The letter also requests clear guidance for states for returning to normal in a “manner that best protects and minimizes disruption for Medicaid beneficiaries, providers, plans, and states.” Although federal rules specify certain requirements related to renewals and periodic eligibility verifications, states will be looking for additional guidance from CMS about rules related to processing renewals and redeterminations when the PHE ends. For example, when the ACA went into effect and states faced an influx of enrollment and new MAGI rules, CMS provided states the option to delay renewals.22,23
Are there things states can do to prepare for the end of the PHE? States can alleviate potential backlogs at the end of the PHE by continuing to process ex parte renewals and extend eligibility for an additional 12 months or start new 12-month coverage periods following a change in circumstance. To streamline these determinations, states may use electronic data from other benefit programs, such as SNAP, to verify income.24 States can also proactively work to update addresses through the U.S. Postal Service National Change of Address Database as well as work with managed care plans to update address information and minimize disruptions for enrollees after the PHE ends. As of January 2020, only ten states reported proactively updating addresses.25 In addition, states may encourage the use of online accounts to maintain up to date enrollee information, allow enrollees to view notices online and to reduce administrative workload.26
Will there be changes to the amount and duration of the fiscal relief and MOE requirements?
President-elect Biden has indicated support for further increasing the FMAP and may try to work with Congress to enact legislation, though Republican leaders have generally been opposed to substantial increases in state and local assistance during the pandemic and economic crisis. The Health and Economic Recovery Omnibus Emergency Solutions (HEROES) Act passed by the House in May and then updated and passed again in October would increase the enhanced FMAP to 14% effective through September 2021 to support states as the COVID-19 pandemic continues. Congress could also consider alternative options to target the relief to states experiencing higher enrollment increases. However, it remains unclear if Congress will provide additional relief through the FMAP or if they will revisit the MOE requirements as part of another coronavirus relief package.
A temporary 6.2 percentage point increase in the regular federal matching rate. To receive the enhanced match states must comply with maintenance of eligibility requirements.
Requires states to provide continuous eligibility for those enrolled prior to or during the emergency, regardless of changes in circumstances, unless the individual requests termination or ceases to be a resident.
States cannot implement more restrictive eligibility policies or procedures and states cannot increase Medicaid premiums. States also must cover coronavirus testing and COVID-19 treatment without cost-sharing. States also cannot increase political subdivisions’ contributions to the non-federal share of Medicaid costs.
January 1, 2020 and March 1, 2020 (for political subdivision contributions)
Allows states to make temporary changes to address eligibility, enrollment, premiums, cost-sharing, benefits, payments, and other policies differing from their approved state plan during the COVID-19 emergency. States may not make changes that restrict or limit payment, services, or eligibility or otherwise burden beneficiaries and providers.
January 1, 2020 (using Section 1135 waiver authority) or later date elected by state
End of public health emergency or earlier date elected by state
Allows states to amend their Medicaid state plans, which govern program elements such as coverage groups, covered services, provider reimbursement methodologies, and administrative activities.
1st day of quarter in which SPA is submitted to CMS or later date elected by state
Continues until subsequently amended or terminated
Allows states to operate Medicaid programs without regard to specific statutory or regulatory provisions to furnish medical assistance in a manner intended to protect, to the greatest extent possible, the health, safety, and welfare of individuals and providers who may be affected by COVID-19.
March 1, 2020 or later date elected by state and approved by CMS
60 days after public health emergency ends or earlier date approved by CMS
Except that a state could receive the enhanced funds from March 18 through April 17, 2020 if a premium in effect during that period was higher than those in effect on January 1, 2020. This provided a 30-day grace period for states to restore premiums to the amount required on January 1, 2020. CMS, Families First Coronavirus Response Act, Coronavirus Aid, Relief, and Economic Security Act Frequently Asked Questions, question 23, https://www.medicaid.gov/state-resource-center/downloads/covid-19-section-6008-CARES-faqs.pdf. ↩︎
This applies only to cost-sharing, such as copayments; states may still not increase or impose new premiums throughout the duration of the MOE period as required by the separate MOE provision at Families First Coronavirus Response Act, Section 6008 (b)(2). ↩︎
“Minimum essential coverage” (MEC) describes the health insurance that individuals must maintain to comply with the ACA’s individual mandate. IRS regulations and CMS guidance provide that most Medicaid benefit packages generally qualify as MEC and specify when certain limited benefit packages, such as family planning services, tuberculosis services and pregnancy-related services, do not qualify as MEC. CMS, State Health Official Letter: Minimum Essential Coverage, (November 7, 2014), https://www.medicaid.gov/federal-policy-guidance/downloads/sho-14-002.pdf. ↩︎
The rule separately provides that states that opt to cover lawfully present children and pregnant women who otherwise would be subject to the 5-year bar must move those enrollees to emergency Medicaid if they no longer meet lawfully present criteria. ↩︎
The COVID-19 pandemic has posed significant challenges for health systems and access to care in the United States, including for people with HIV and the systems that serve them. To better understand pandemic’s impact on HIV, we surveyed the nation’s directly funded Ryan White providers. Ryan White, the federal HIV safety net program, serves over half of those in the country diagnosed with the disease, providing outpatient HIV care and support services. Our key findings are as follows:
Respondents described an immediate pivot to new ways of providing HIV care and prevention during the early months of the pandemic.
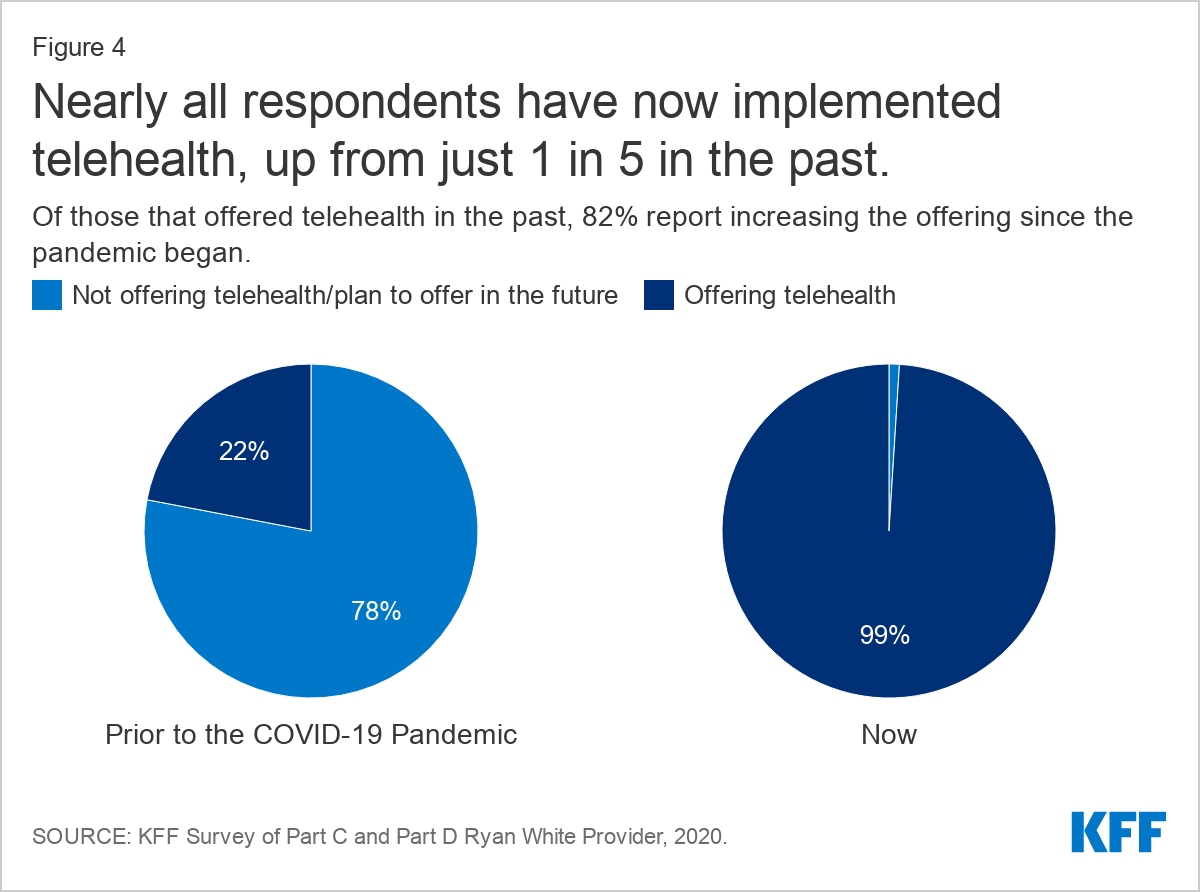
Nearly all are now offering telehealth services (99%), up from 22% in the past, and are conducting about half of patient visits virtually, on average. However, the “digital divide” means telehealth services are not an option for all patients.
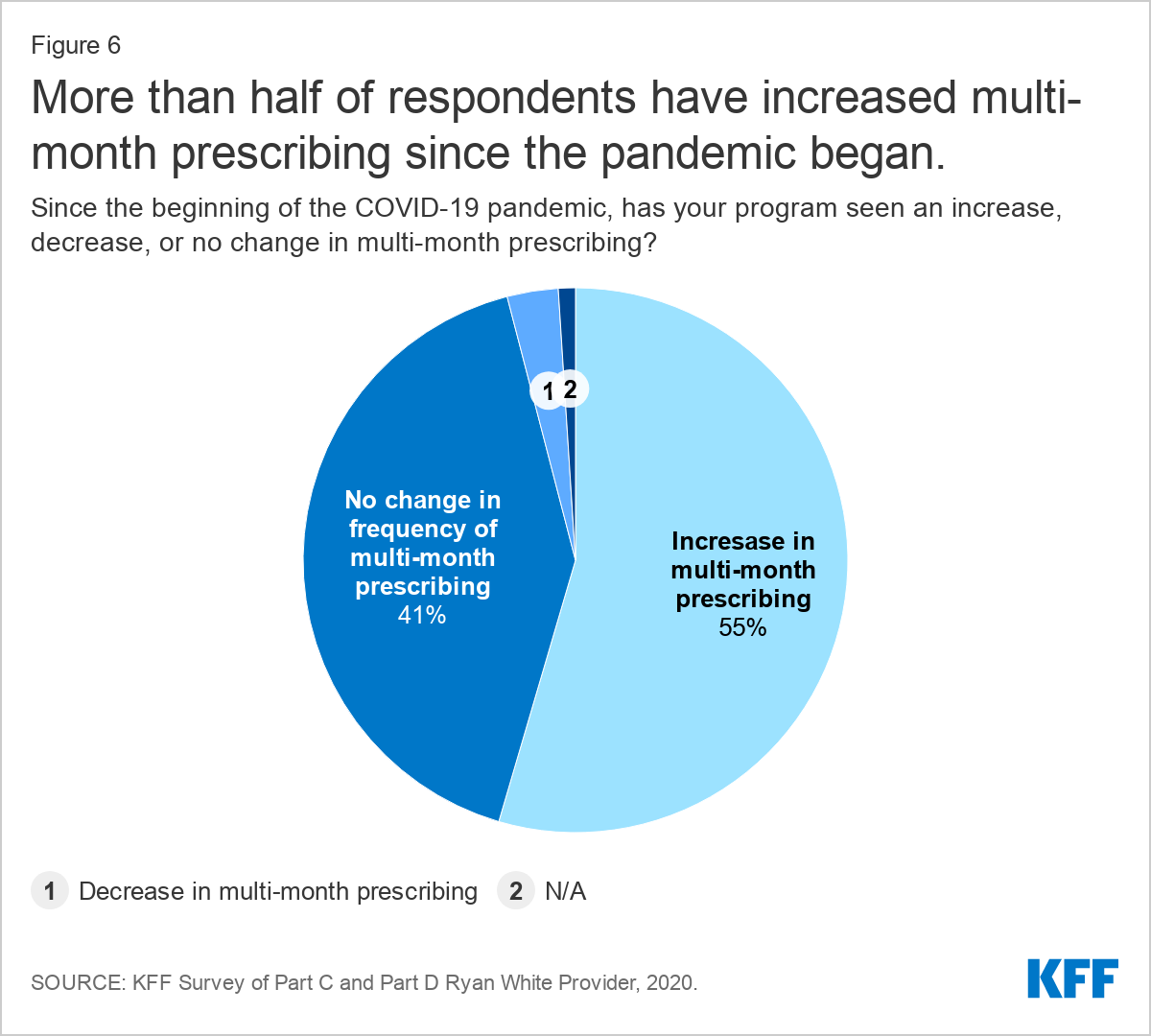
Most (89%) are offering multi-month prescriptions for antiretrovirals (ARVs), and half reported that this practice has increased due to COVID-19.
Seven in ten (70%) are conducting onsite COVID-19 testing.
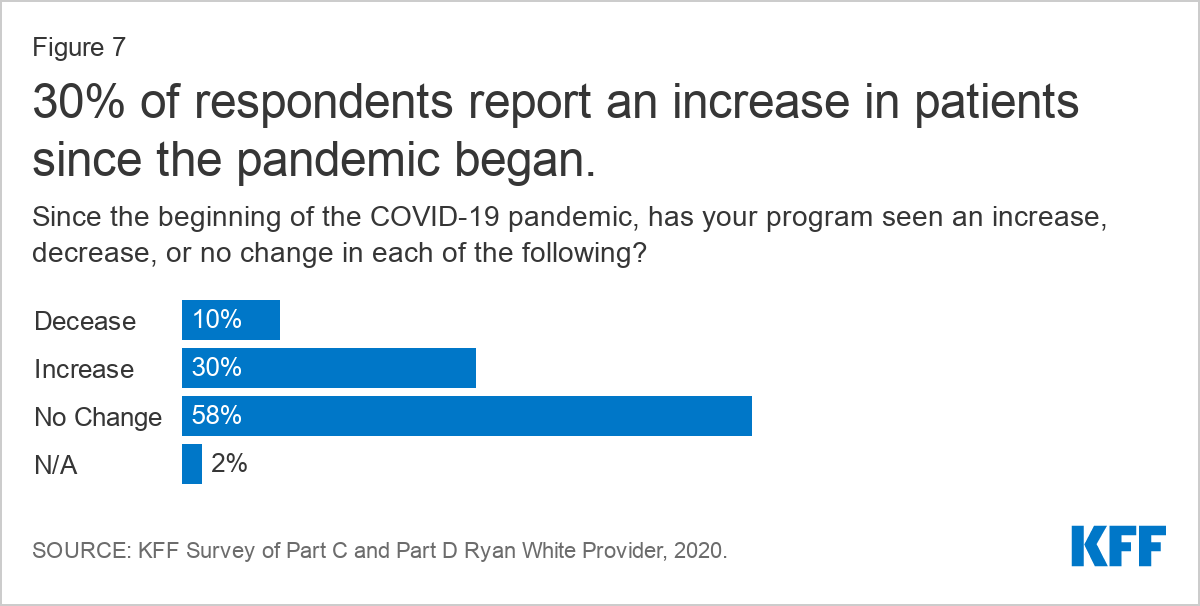
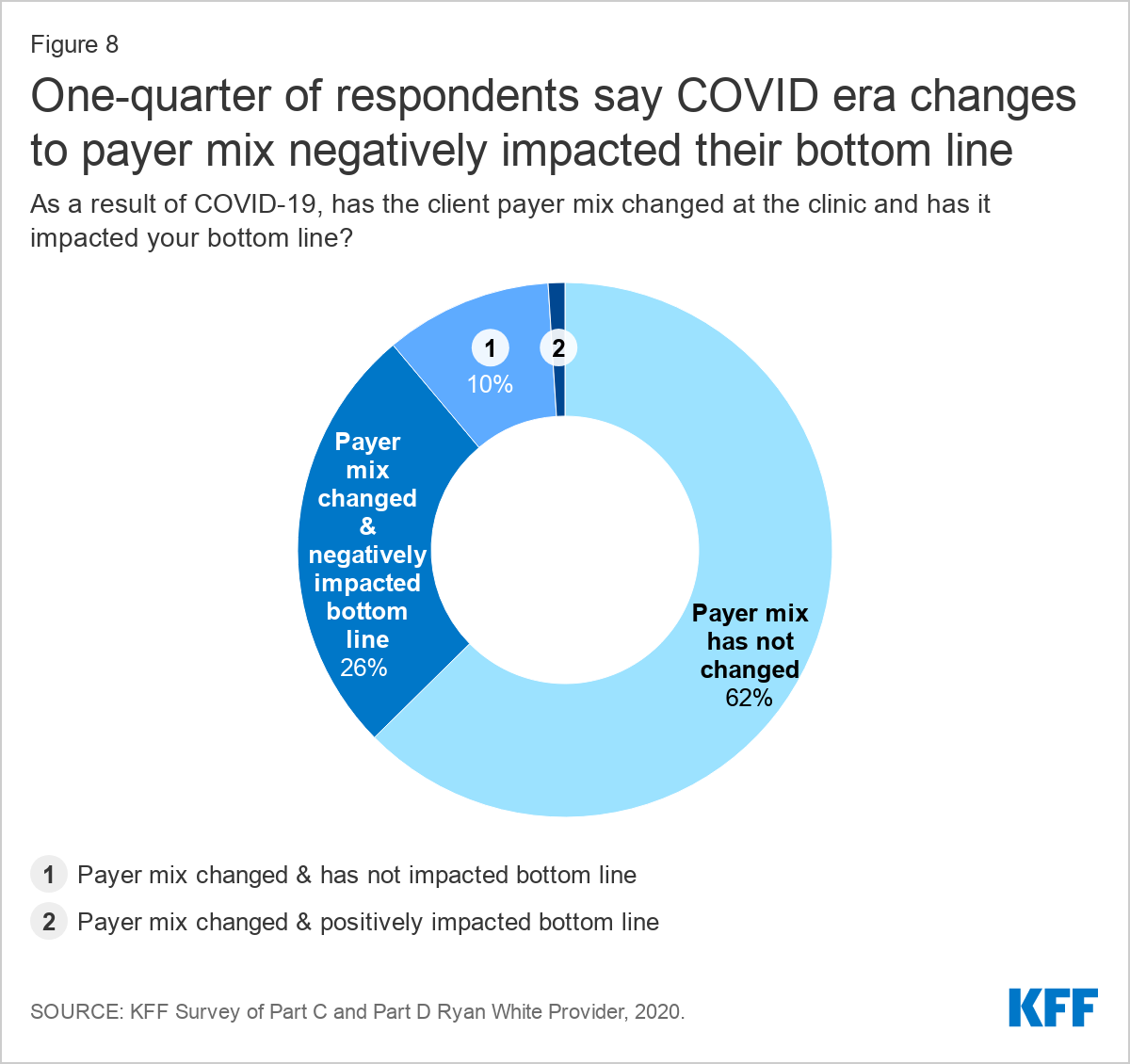
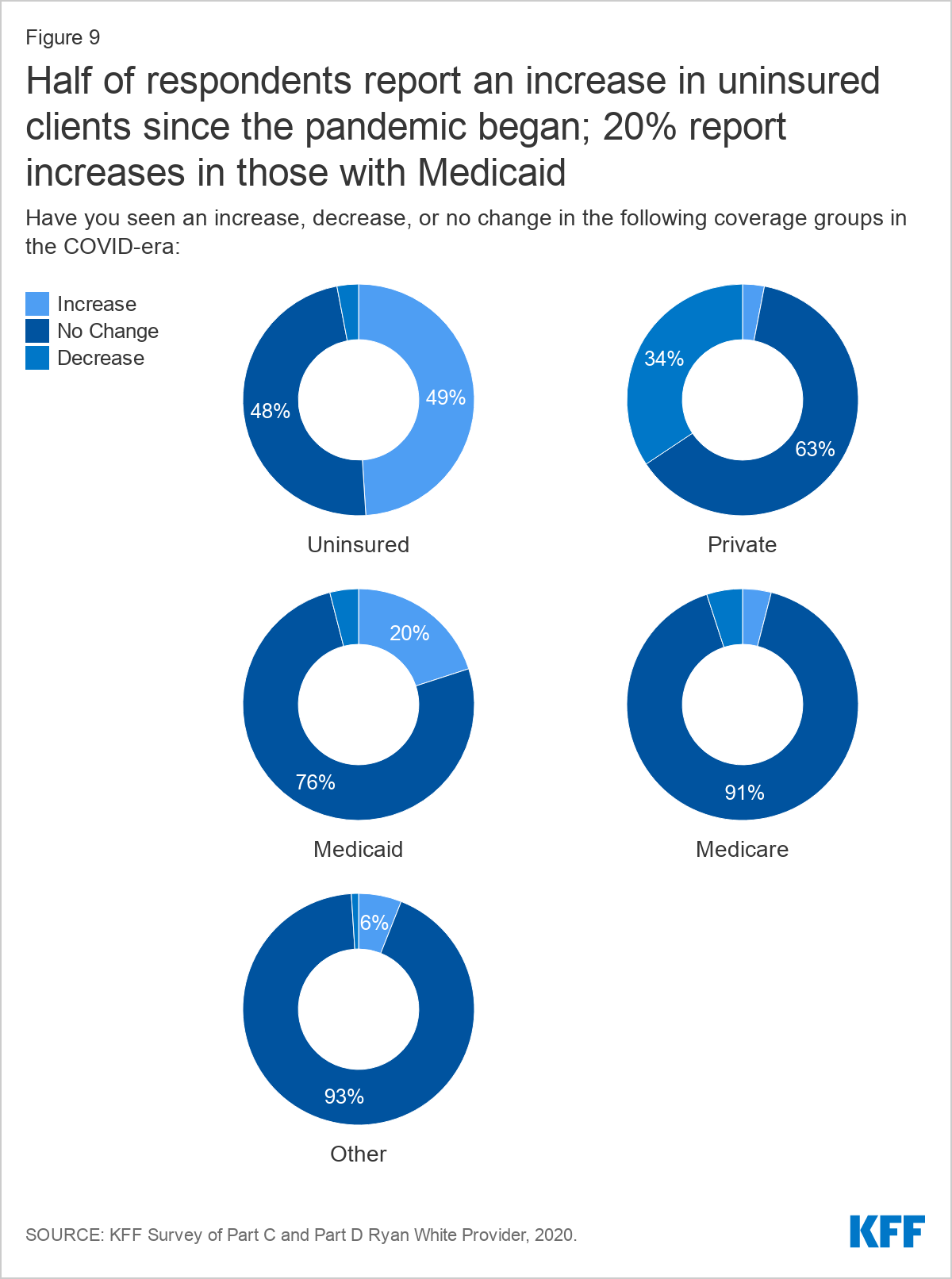
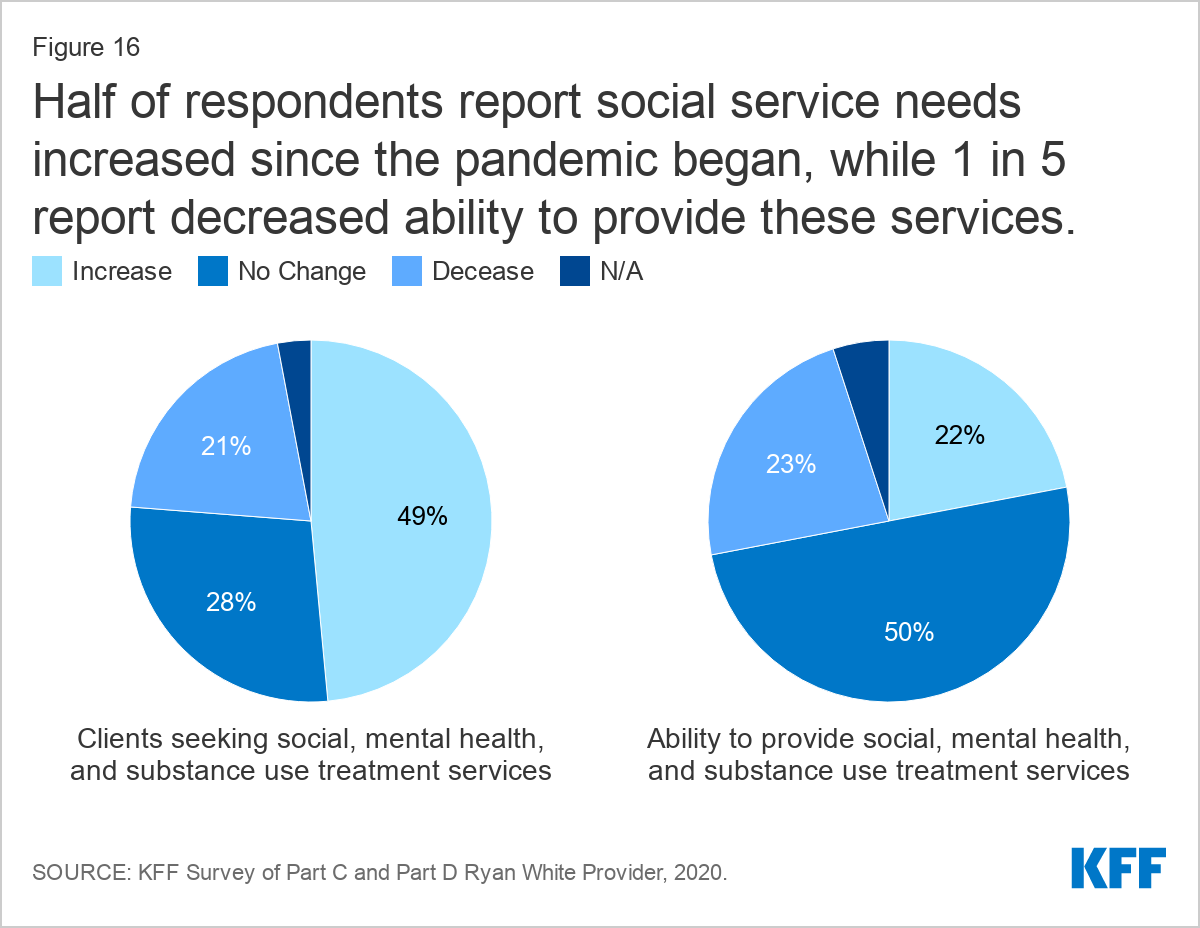
Nearly one-third (30%) reported an increase in new clients and nearly 40% of respondents saw a change in payer mix, primarily an increase in clients who were uninsured, followed by private coverage losses, and then increases in clients with Medicaid.
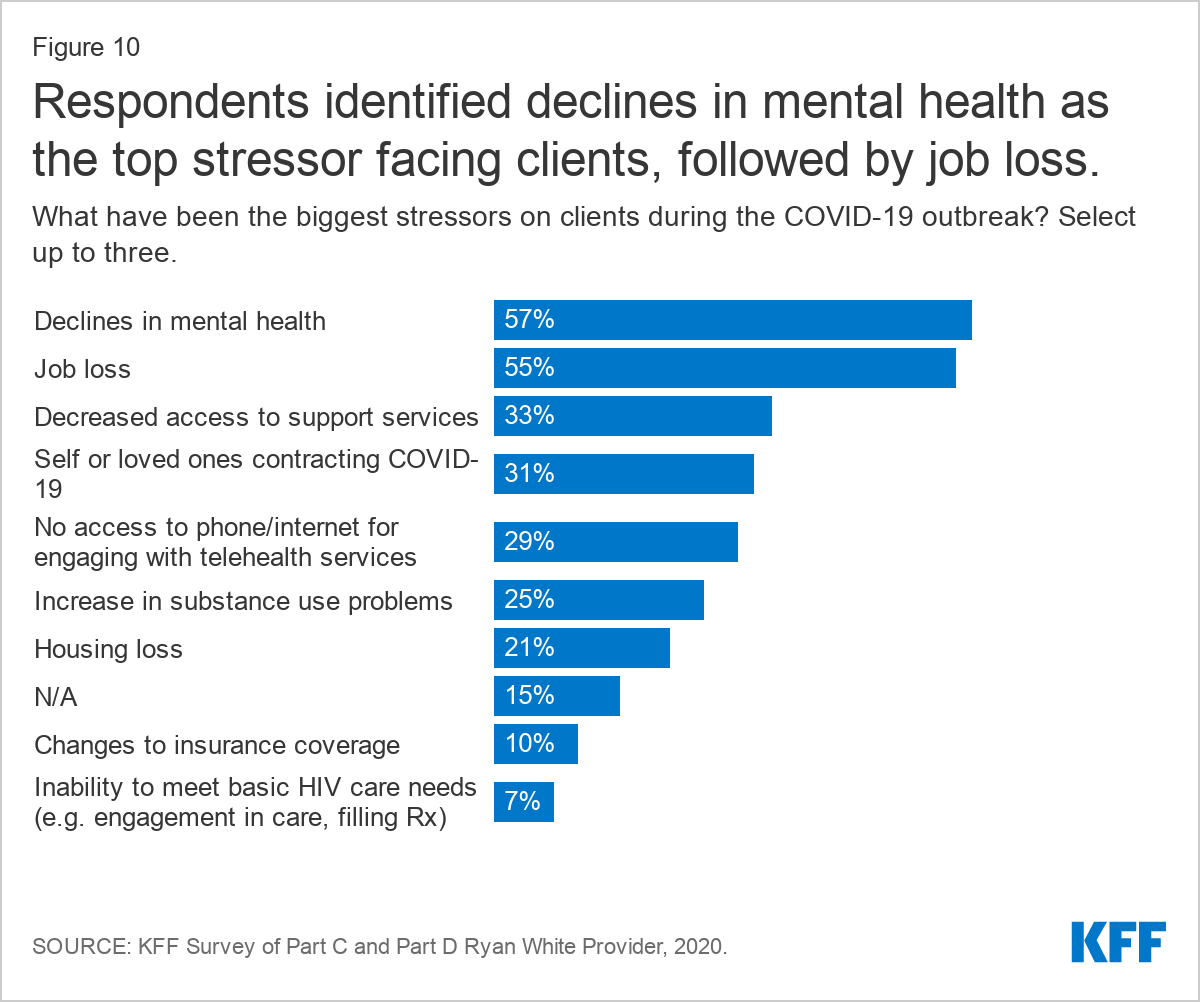
Respondents report that clients face significant stress and uncertainty amidst the pandemic, noting declines in mental health, job loss, and decreased access to support services, among other challenges.
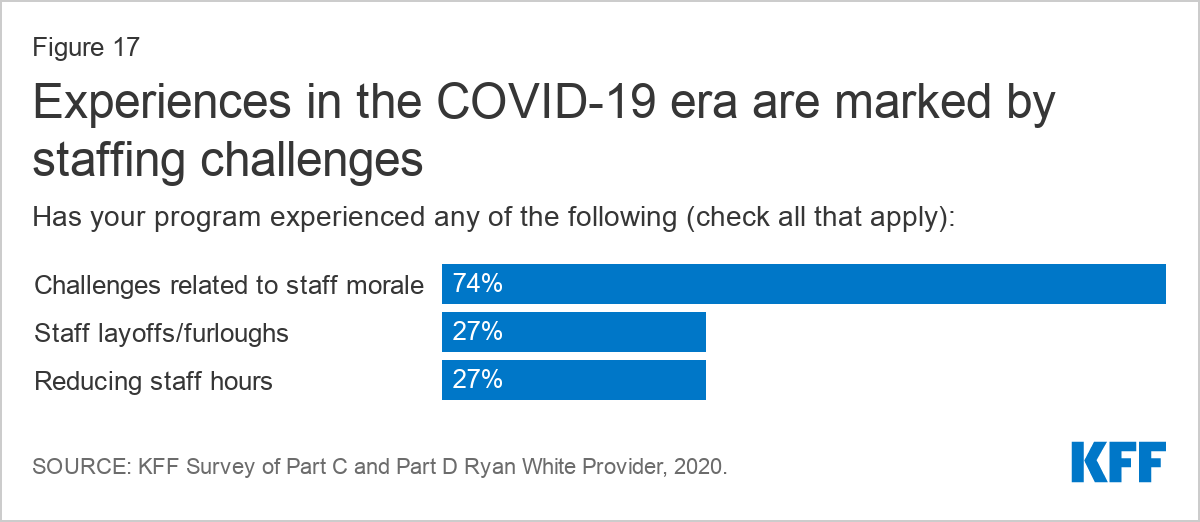
Respondents also experienced significant challenges related to staffing. More than one-quarter (27%) reported staff layoffs or furloughs and the same share reduced staff hours. Moreover, staff morale was a challenge reported by three-quarters (74%) of respondents.
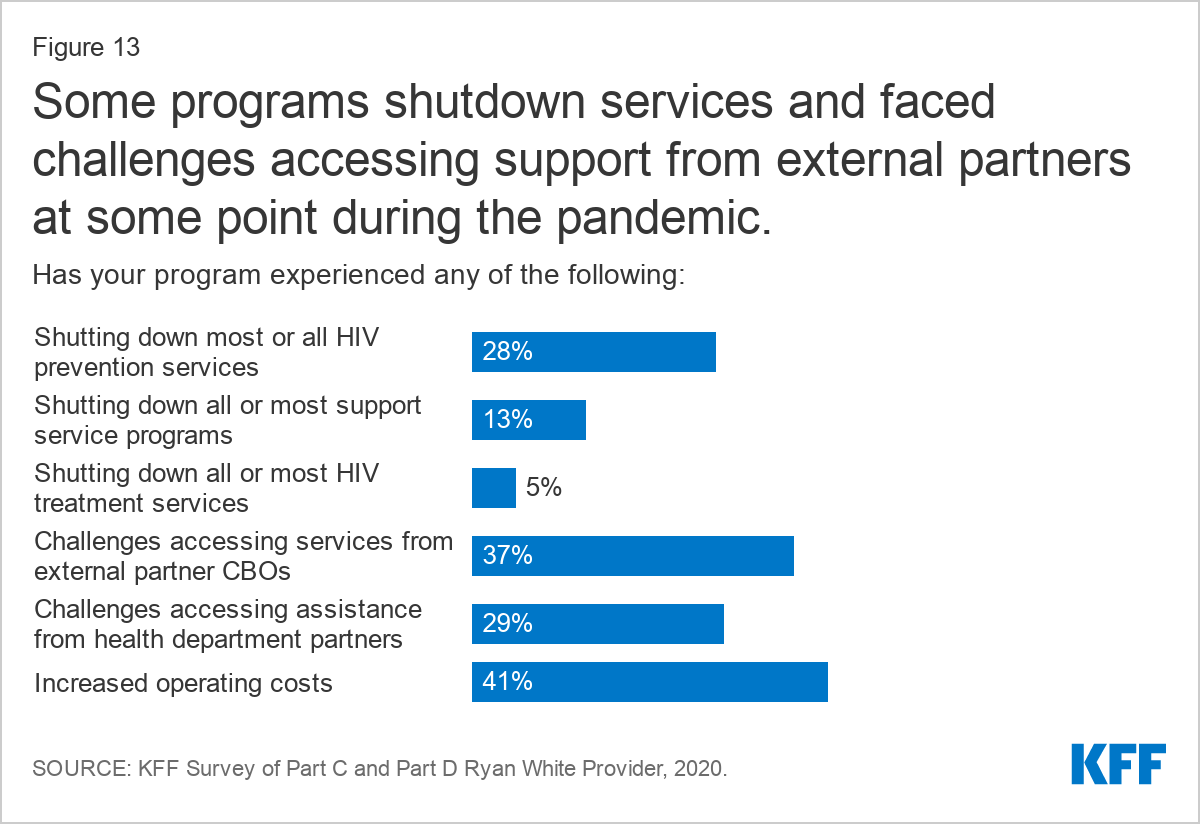
Operating challenges were common, including for the 28% who shut down all or most of their HIV prevention services in response to the pandemic. Other challenges included difficulty connecting with service partners and increased costs.
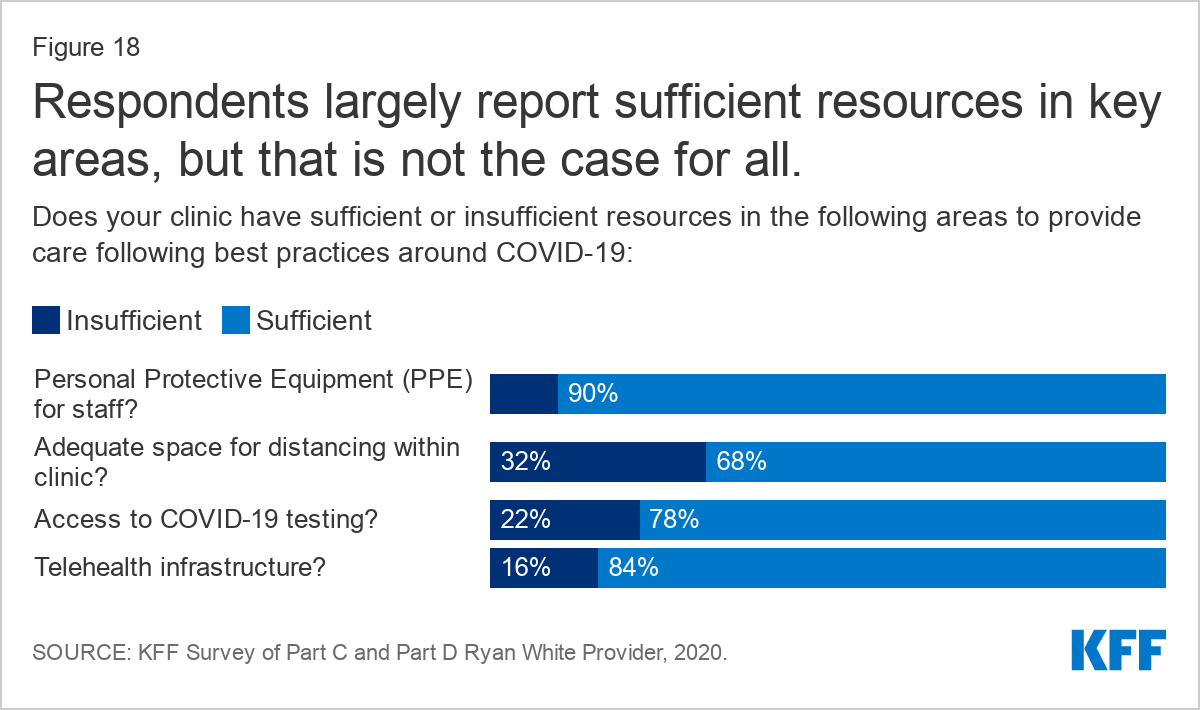
Following COVID-era public health guidelines remains a challenge for some who experience inadequate clinical space for social distancing (32%), insufficient access to COVID-19 testing (22%)and insufficient PPE (10%).
However, despite these historic challenges, respondents largely report adjusting to a “new normal” and significant resiliency in adapting to new ways of providing care.
Issue Brief
Introduction
The COVID-19 pandemic has posed significant challenges for health systems and access to care in the United States, including for people with HIV and the systems that serve them. While it does not appear that people with well controlled HIV are at greater risk for more severe complications associated with COVID-19, 4 in 10 people with HIV in the U.S. do not have sustained viral suppression and CDC suggests that those with a low CD4 count or not on antiretroviral treatment could be at higher risk. In addition, many of the individuals invested in the nation’s HIV response – especially those with an expertise in infectious disease – have shifted at least some of their attention away from HIV to focus on the pandemic.
To better understand how COVID-19 has affected the HIV service delivery environment and people with HIV, we surveyed the nation’s Ryan White-funded providers. The Ryan White HIV/AIDS Program is the largest federal program designed specifically for people with HIV in the U.S., serving over half of those in the country diagnosed with the disease. It provides outpatient care and support services to individuals and families affected by HIV, functioning as the “payer of last resort” by filling the gaps for those who have no other source of coverage or face coverage limits or cost barriers. Funding is provided to states, cities, and providers throughout the country. In addition, recognizing the new stresses the pandemic might mean for Ryan White and people with HIV, Congress appropriated $90 million in emergency supplemental funding for the program through the CARES Act.
Methods
Between August 18, 2020 and September 4, 2020 we surveyed directly funded Ryan White HIV/AIDS Program medical provider grantees (i.e. those funded through Part C or Part D). We identified all Part C and Part D grantees funded in FY2020 using publicly available grantee data. In total we identified 390 unduplicated grantees. The named contact for each grantee organization was sent a confidential survey using Survey Monkey containing closed and open-ended questions. We received 161 responses and 8 bounce backs, representing a 42% response rate. Raw survey data was downloaded and analyzed using Excel. Open-ended qualitative responses were analyzed using an inductive framing approach.
While all respondents received Ryan White funding to provide HIV care and treatment, many also received funding from other sources, including to conduct HIV prevention activities. Survey questions and responses are not limited to activities carried out using Ryan White funding.
Respondent Characteristics
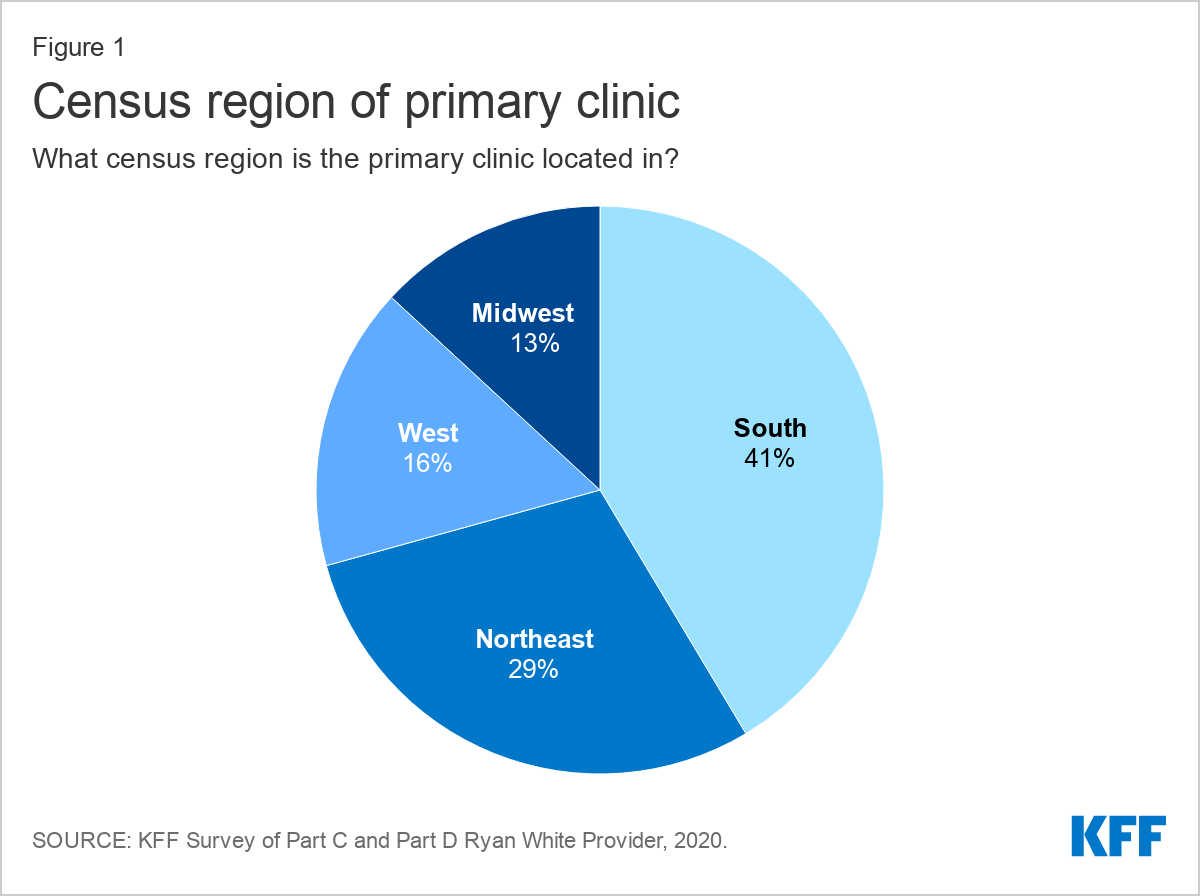
Respondent organizations were located in 38 states, Washington, D.C., and Puerto Rico. A plurality of respondents (41%) were based in the Southern U.S, followed by the Northeast (29%), the West (16%), and the Midwest (13%).
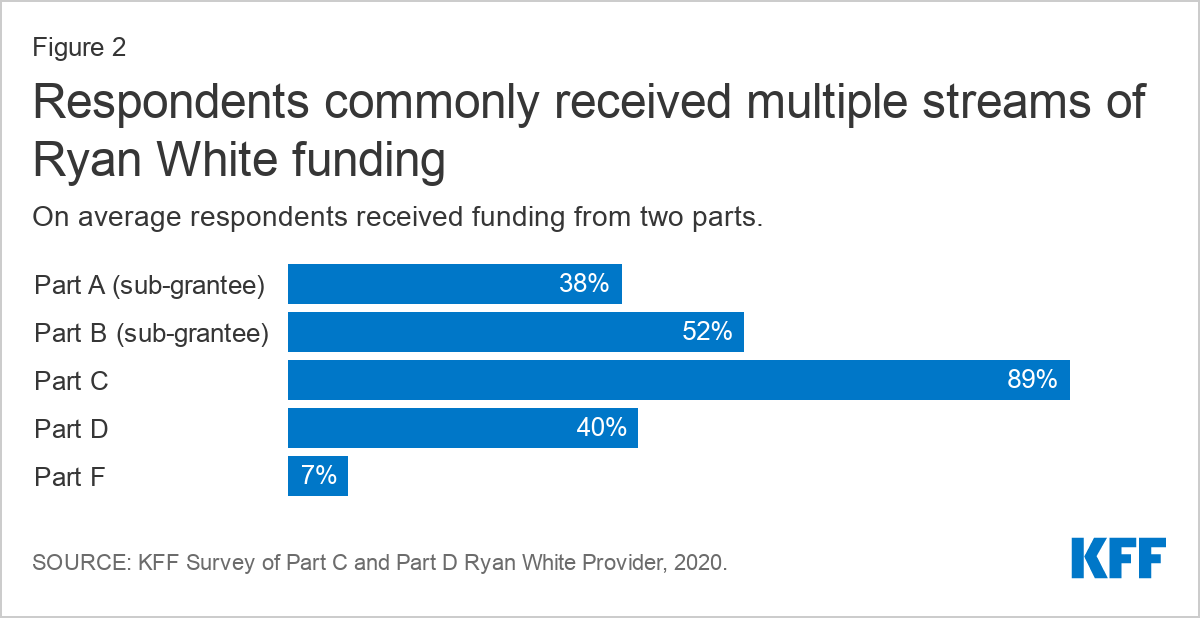
Respondents reported receiving funding from a range of Ryan White Program parts, with many reporting funding from multiple streams (two on average). The most common funding stream was from Part C (89%, funding for community-based organizations providing outpatient HIV health and support services), followed by Part B as a sub grantee (52%, funding directed to states). Forty percent (40%) were Part D grantees (funding for community based ambulatory programs focusing on family-centered care and support services for women, infants, children, and youth with HIV). Smaller shares received funding from Part A as a sub-grantee (38%, funding directed to hard hit urban areas) and Part F (7%, funding for dental care).
Findings
Changes to Services
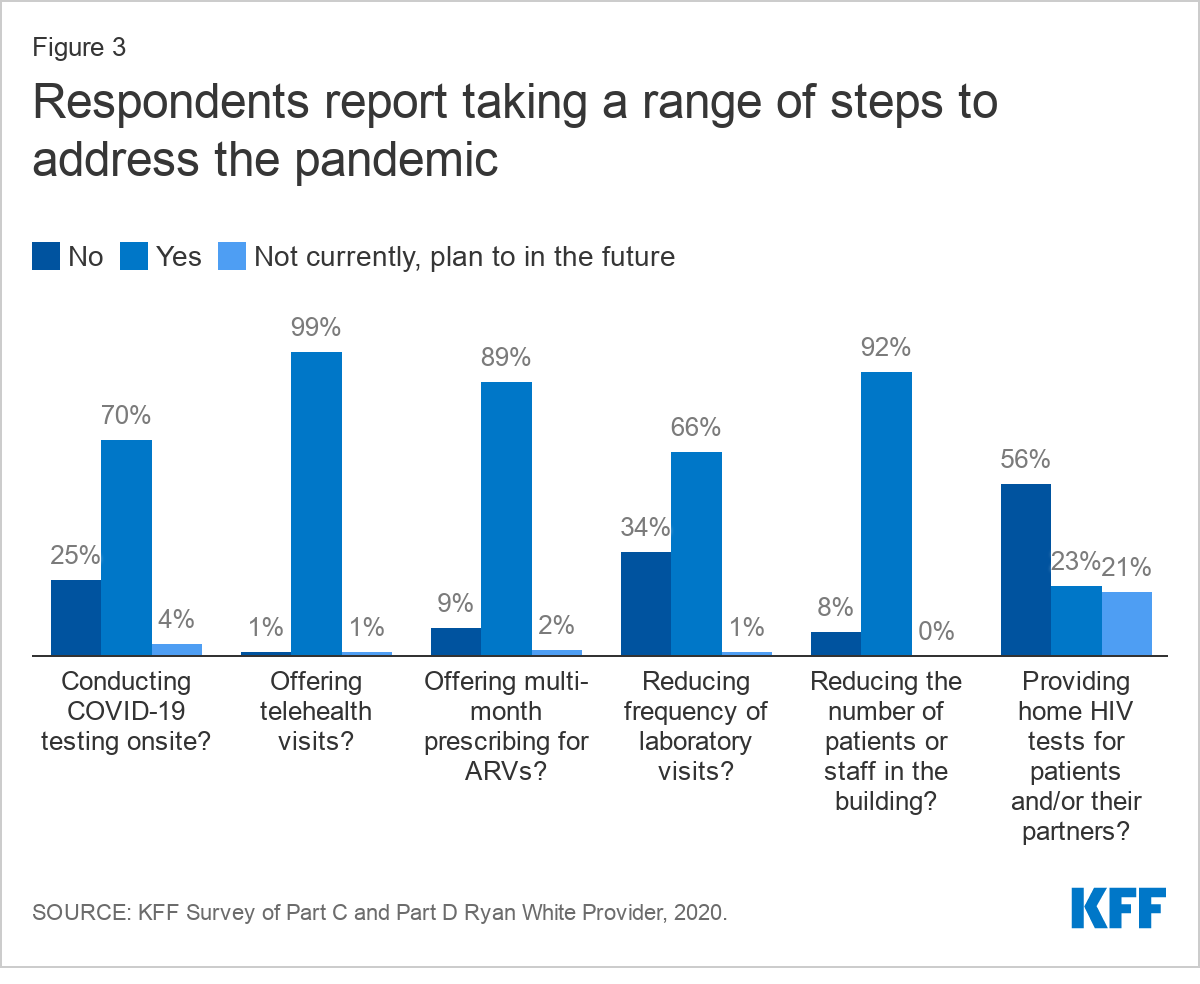
Providers reported significant program changes made in response to the COVID-19 pandemic and described an immediate pivot to new ways of providing HIV care and prevention. Nearly all reported offering telehealth services (99%) and reducing the number of staff or patients in the building at one time (92%). Most reported offering multi-month prescriptions for antiretrovirals (ARVs) (89%), conducting onsite COVID-19 testing (70%), and reducing frequency of laboratory visits (66%). Over half (56%) reported providing clients with home HIV tests, with an additional 21% planning to offer home HIV tests in the future. Respondents described tinkering with new offerings and service closures to find the right balance for their clinic and patient population.
“We have less onsite primary care visits but increased telehealth visits. Decreased support groups onsite, but increased teletherapy with individual clients. We have adjusted with workarounds to keep our clients engaged, frequent wellness checks, and supplied with resources, including COVID supplies.” --Part A, B, C, and D grantee, Midwest
Virtually all providers reported now using telehealth, compared to 22% who did so before COVID-19. Leveraging telehealth was one of the most common COVID-era changes made by providers, with virtually all (99%) saying they offer this service. Of those that did offer telehealth in the past, most (82%) reported expanding telehealth due to COVID-19. Respondents described that this was easier for those who had pre-existing telehealth infrastructure before the pandemic, while some who lacked this prior experience struggled with implementation.
“The transition to Telehealth and use of other virtual platforms that worked effectively and were HIPAA complaint, was a challenge. There were significant delays in even getting the needed equipment due to backorders…” --Part A, B, and C grantee, West
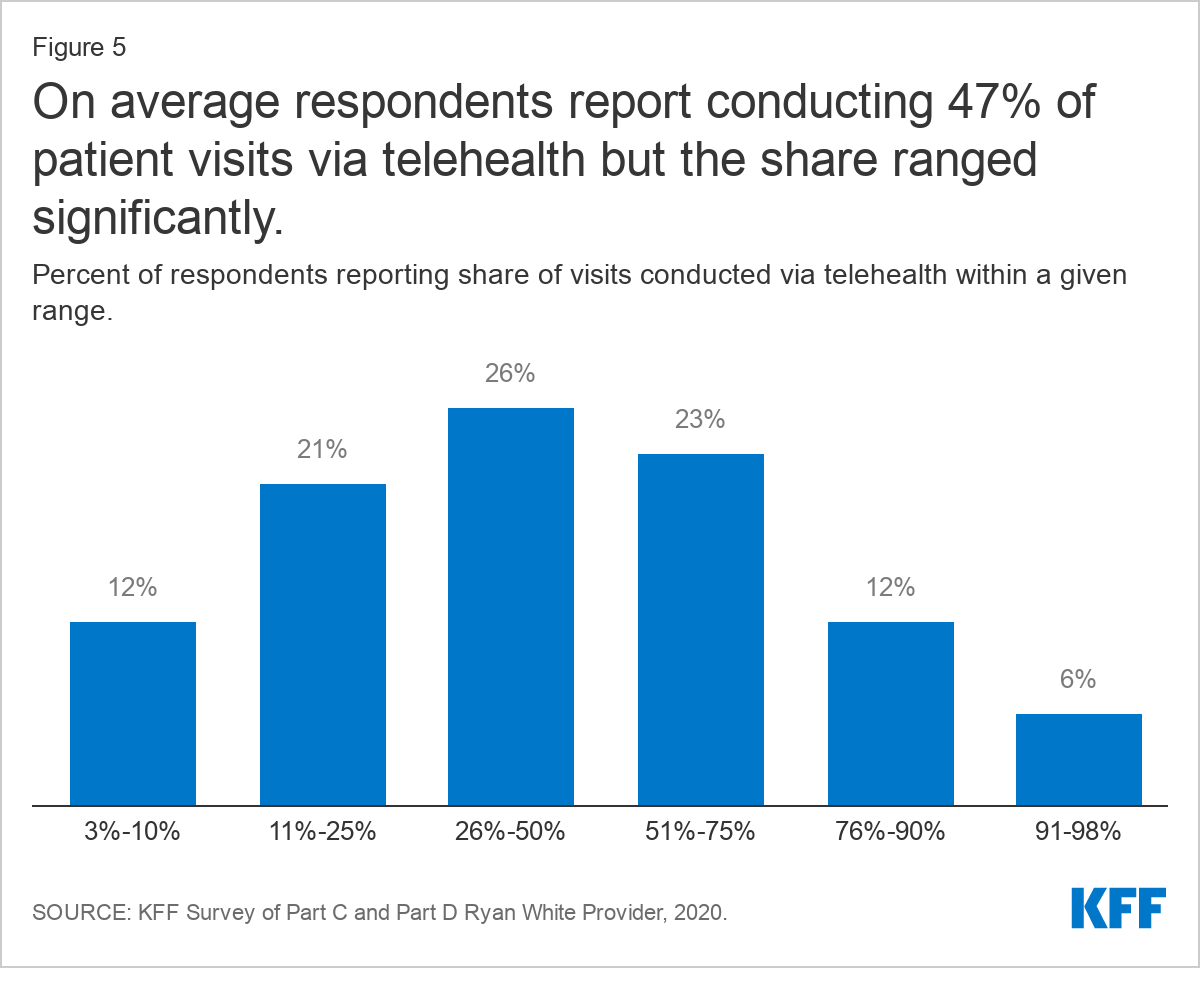
On average, providers now report conducting about half (47%) of patient visits through telehealth (including via video and phone) but that share varied significantly. Forty-one percent (41%) of respondents report using telehealth more than 50% of the time and 6% report using it more than 90% of the time. Six percent (6%) of respondents reported using telehealth more lightly, for less than 10% of visits. In addition to infrastructure challenges, some who reported less frequent use of telehealth were limited by institutional policy. As one provider said, “our larger health care system has been unable (because of security issues) to let us do video visits, only telephone. I believe video would greatly improve these interactions.”
Respondents generally expressed that integrating telehealth services more widely into their practices was an important step forward, not just in providing care during the pandemic, but that they would retain the practice in the long term. Many explained that they were able to connect with historically hard to reach populations and others said they were able to stretch scarce provider time further. Some stated that retention in care had improved and “no shows” declined as a result. They described learning how to make telehealth work best for their patients and saw it as a critical tool for maintaining care during the pandemic.
"I think that telemedicine has been an invaluable tool that has enabled us to stay in contact with patients during this uncertain time and while it is efficient and convenient, we still need to work doubly hard to connect and relate to our patients. We need to project through our screens the compassion and concern we have for them, to continually reassure them, and ensure that they continue to receive quality care regardless of how it is delivered. Patients have been responsive to telehealth as evidenced by show rates over the past 4+ months which is a good indicator that retention in care and viral suppression can be maintained and/or improved." --Part B, C, and D grantee, South
However, many also discussed the “digital divide, noting telehealth only worked well for certain patient populations, with respondents largely agreeing on who was best and worst served (see Table 1).
“Telehealth is working for our practice. We do face barriers with connection problems, and older patients that are not technically knowledgeable…We also have patients that are not on unlimited plans. Telehealth has helped our bottom line. We are able to reach some patients, younger group, that otherwise are not easy to reach.” --Part C grantee, South
Table 1: Respondents Generally Agreed on Which Groups Most Benefited from/Struggled with Telehealth
Most Benefited
Most Struggled
Younger populations/tech savvy individuals
Older populations/less tech savvy individuals
Those in rural areas with limited transportation (with tech access)
Those without internet/computer/smartphone access, those with limited phone data, including those in rural areas without broadband & cell infrastructure
Those with childcare responsibilities
Unstably housed individuals
Medically uncomplicated and stable individuals
Medically complex and vulnerable individuals
Some historically harder to reach patients
Those who lack privacy to make calls
Those penalized for taking time off at work
Those in need of translation services
Established patients
New patients
Some reported taking steps to address technology gaps, including offering technical support, and by providing clients with phones, phone cards, data plans, internet access, and mobile hotspots. In addition, some described offering telehealth or technology training for staff and patients, sometimes focusing on a specific population, such as seniors. In many cases, respondents used supplemental Ryan White Funding provided through the CARES Act (see Box 1) to cover these costs.
Box 1: Respondent’s Reported Use of CARES Act Funding
Areas bolded denote the most common responses, mentioned by multiple respondents. (Alphabetical Order)
COVID-19 best practices consulting, infection control review, COVID-19 educational materials for patients
COVID-19 testing
Emergency financial assistance
Housing/rental assistance, isolation lodging, utilities for clients, clinic rent
Infrastructure changes (e.g. to support telehealth, to provide for social distancing)
Marketing/outreach of HIV care and COVID-19 testing
Medical supplies for clinic and for clients (e.g. BP cuff, thermometer, pulse ox machines)
Medical transportation, new vehicle for patient and meal transport
PPE, sanitation supplies/services, Plexiglas, partitions, and air purifiers
Premium assistance and medications (OTC medications, ARVs)
Staff salaries for existing staff/prevent layoffs and salaries to support new staff: E.g. Home health care providers (medical assistant), case management/medical case management, full and part-time physicians and nurses (including to assist with overflow from infectious diseases physicians occupied by COVID-19 response), telehealth coordinators, medical triage staff for COVID-19 screening, mental/behavioral health and social service support staff, peer advocate, community healthcare workers, COVID-19 nurse staffed to work with HIV positive clients.
Supplies and care packages for clients (in some cases mailed to clients): E.g. masks, sanitizer, coloring books/pens, gas cards, clothing, gift cards for basic supplies (e.g. food, cleaning supplies, personal hygiene products etc.)
Telehealth infrastructure: E.g. tablets, computers, phones, phone cards, phone service/mobile hot spots for clients, licenses (e.g. for Doxy.me and Zoom), webcams, microphones, and computers.
Note: The Coronavirus Aid, Relief, and Economic Security, or CARES, Act was the third major legislative initiative to address the COVID-19 Pandemic. Additional information available here.
Providers noted that while telehealth is well suited for certain types of visits, it is inadequate for others. Generally, providers explained it worked well for routine visits or follow-up care, and prescription drug refills. Some thought it was also working well for behavioral health/social work, though others thought social service visits worked better in person. One stated “Telehealth has been especially important for maintaining mental health services.”
"Telehealth is working well for medical follow up, case management and eligibility appointments for individuals who are stable and virally suppressed..." --Part A, B, and C grantee, West
As time has gone on and it has become clear that there will not be an immediate end to the pandemic, some respondents expressed concern about patients being without in-person visits or laboratory services in the long term. They believed conducting all services via telehealth as a stopgap measure was reasonable at first, but several respondents described now wanting to bring patients back onsite for at least some in person care, for both clinical and reimbursement reasons. Some also worried that reliance on telehealth in the long term could increase patient isolation. Others worried providers “would miss things” by not seeing patients in-person for extend periods of time.
"…While initially medical care visits were easily provided through telehealth, there is more concern amongst providers, as the time drags on. They are concerned about actually having the opportunity to examine patients and also to monitor labs..." --Part B, C, and D grantee, South
"Telehealth is very helpful. No-show rates decreased. Only challenge is to bring in those pts with co-morbidities who have not been seen face-to-face for over 6 months now. Providers want them to come in at least once, then continue telehealth. Pts with comorbidities need to be closely monitored." --Part A and C grantee, Northeast
Just a few respondents had a more pessimistic view of telehealth overall and were unable to get past seeing it as inferior way to practice medicine. They believed that telehealth didn’t allow them to gather critical health information or, in one case, that the technology actually got in the way of the visit.
"Telehealth is good reassurance for patients, but it has not been very helpful in terms of HIV primary care -- we cannot get vital signs and monitor BP, we don't have labs, and we cannot as easily connect pts to in-clinic resources. It feels "better than nothing" but doesn't feel like the highest quality of care…" --Part C grantee, Northeast
While some described being able to leverage telehealth to conduct more visits and generate additional revenue, most described reimbursement challenges. A primary issue hinged on the fact that payers would reimburse for video but not telephonic visits, while many patients preferred or only had technology to support phone calls. One provider noted that they could bill for their time but not collect facility fees with telehealth visits.
Multi-month dispensing of HIV medications was offered by nine in ten (89%) respondents, with many saying they have increased this practice. More than half (54%) say that the practice has increased since the pandemic began, though a large share (41%) report no change.
In addition to multi-month prescribing, respondents also reported offering new options to facilitate access to medications. Some are now offering home delivery of medications, often by clinic staff such as case workers, and others are more heavily using mail order prescription delivery services.
Changes to Patient Population
Nearly one-third of respondents (30%) reported an increase in new patients since the pandemic began. Some respondents believed they were seeing more clients because engagement and retention in care was easier for certain individuals through new telehealth offerings, though it may also be due to increasing need and coverage losses.
Two respondents noted that some HIV positive clients who had previously fallen out of care, reengaged with the health system in the wake of the pandemic, fearful of what becoming infected with COVID-19 might mean for them.
"We've seen an increase in patients who had been out of care returning to care over COVID fears…" --Part A and D grantee, South
"…Because we were a COVID testing site early on we did see an increase in patients that had fallen out of their HIV care coming to the COVID testing and asking also about getting back into HIV care, because they were concerned about being vulnerable to COVID." --Part A and C grantee, South
Nearly 40% of respondents reported changes to their payer mix. Respondents were asked whether their clinic saw a change in overall payer mix as a result of the pandemic, that is, have clients gained or lost insurance coverage. Payer mix can impact clinic bottom line and certain care experiences. While most (62%) reported that they have not seen a change in payer mix, nearly 40% have seen a shift, with more than one quarter (26%) saying the change has negatively impacted their bottom line. One in ten said that payer mix has changed, but it has not impacted bottom line. Only 1% of respondents reported a payer mix change with a positive bottom line impact.
When asked about specific changes experienced under the pandemic, respondents reported even higher rates of coverage changes. About half of respondents (49%) reported an increase in uninsured patients, one-third (34%) reported decreases in clients with private coverage, and 20% reported increases in clients with Medicaid coverage. Fluctuations in Medicare and other coverage were smaller.
There were differences in client coverage changes reported by respondents in Medicaid expansion states compared to those in non-expansion states (or in states that had not yet implemented expansion). While large shares of respondents reported increases in uninsured clients across the board, this was somewhat less common among respondents in Medicaid expansion states compared to those in states that had not expanded their programs (45% v 55%). This could be attributed to increases in Medicaid coverage and less of decline in private coverage among clients in expansion state. Twenty-eight percent (28%) of respondents in expansion states reported increases in clients with Medicaid coverage, while just 9% of those in non-expansion states reported Medicaid increases. Twenty-nine percent (29%) of those in expansion states and 43% of those in non-expansion states reported declines in clients with private coverage.
Table 2: Share of Respondents Reporting Coverage Changes in The COVID Era, by Medicaid Expansion Status
Uninsured
Private
Medicaid
Medicare
Other
Exp.
Non-Exp.
Exp.
Non-Exp.
Exp.
Non-Exp.
Exp.
Non-Exp.
Exp.
Non-Exp.
Increase
45%
55%
2%
5%
28%
9%
4%
3%
7%
5%
Decrease
3%
3%
29%
43%
2%
7%
3%
7%
0%
3%
No Change
52%
41%
69%
52%
70%
84%
92%
90%
93%
92%
Impact on Clients
Respondents reported that clients faced significant stress and uncertainty amidst the pandemic and noted that these experiences translated to increased social service needs. Respondents were asked to select the three most significant stressors impacting their clients from a list. The top stressor, identified by 57% of respondents, was declines in client mental health, followed by job loss (55%) and decreased access to support services (33%). Also ranked highly were lack of access to technology to support telehealth encounters (29%) and increases in substance use problems (25%). Housing loss was a top stressor identified by one in five respondents (21%). Smaller shares pointed to insurance loss (10%) and inability to meet HIV care needs (7%). Those who selected “other” (15%) most commonly expanded their answer to identify fear, isolation, and stress related to the pandemic as the biggest challenges facing their clients, including for those working in high risk settings. Other stressors for patients included food insecurity and inability to safely use transportation. Some were also concerned about patients who were afraid to return to care due to possible COVID exposure, including those who are immunocompromised.
"For many of our HIV+ patients, engaging with staff and medical providers is the only actual in person engagement that they have. In the era of COVID, many clients have expressed increased feeling of isolation, anxiety and/or depression."--Part A, B and C grantee, West
"A number of our patients work (as nutrition aides and CNAs) in local nursing homes heavily impacted by the pandemic. Others work at grocery stores, restaurants and in other "essential worker" roles. The stress of reporting to work in an environment with increased potential for COVID exposure has been a big stressor." --Part B and C grantee, Northeast
"Immunocompromised patients are afraid to come in and be exposed to COVID-19. We have offered COVID testing as part of their appointment and they seem to feel safer knowing people are testing as they come to their appointments."--Part C grantee, West
Respondents described that some patients and staff adjusted smoothly to the changes brought on by the COVID-19 pandemic while others had a more challenging time. When asked to consider how well clients’ needs were being met compared to pre-COVID times, nearly equal shares, said that needs were being met somewhat more sufficiently (24%), somewhat less sufficiently (23%), that there had been no change (24%), or that the experience had been mixed ( 22%). In a separate question, respondents elaborated, that those patients better engaged in care in the COVID-era compared to the past were largely individuals who adapted well to telehealth services. Those who most struggled were patients with increased social service needs or those who did not adapt easily to telehealth.
"We transitioned to virtual care for all services during late March/early April, then returned to full on-site services in May…In terms of HIV care, our capacity is similar but patients have higher needs due to the financial and behavioral stresses of the COVID pandemic. In addition, layoffs affecting clinical staff have impacted the clinical workflow." --Part A and C grantee, Northeast
Respondents were similarly split as to how retention in HIV care during the pandemic compared to experiences in the past. A plurality reported no change in retention in care (38%) and similar shares reported a slight improvement (25%) or slight decline (28%). Improvements in retention were sometimes attributed to leveraging telehealth while some attributed drops in retention to more limited access to social support groups and in person services.
Operating Challenges
Despite the steps respondents report taking to maintain care and prevention opportunities during the pandemic, operating challenges were common. For instance, four in ten respondents (41%) reported that they were facing increased operating costs.
Additionally, more than one-quarter (28%) report shutting down all or most of their HIV prevention services at some point in response to the pandemic. Smaller shares shuttered HIV care services at some point during the pandemic (5%). More than one in ten (13%) shut down all or most support services at some point.
Large shares of respondents also reported difficulty connecting with service partners. Challenges accessing services from community-based organizations were reported by 37% of respondents and 29% reported challenges accessing assistance from health department partners.
While some providers reduced HIV services or ran into barriers with access to partner organizations, others offered creative approaches to continuing these activities, such as opening a testing hotline and outfitting a van for parking lot HIV testing. (See Box 2: Best Practices Identified by Respondents.)
Box 2: Respondent Identified Best Practices in the COVID-era
Telehealth
Providing training
Getting staff buy-in
Getting technology to patients
Offer drive through appointments to help clients set up their phones for telehealth
Clinical
Scheduling labs in advance to reduce waiting
Provision of home HIV (and STI) testing
Staff delivery of prescription medication (e.g. case managers, patient navigators)
Imbedding nurse practitioner in call center
On call weekend coverage for mental health services and medical case management
Purchased medical van (with CARES Act funding) to bring care to patients
Increase flexibility of where patients can get labs drawn
Operating a testing hotline
Outfitting van for parking lot HIV testing
Social services
Extensive case management to maintain contact
Use of taxi vouchers/Uber/Lyft for appointments
Use of “psycho-educational” Zoom groups to address social isolation
Case managers picked up food bank packages and provide contactless delivery to clients
Administrative
Administrative staff working from home
Other
Coordination between patient care navigators and local health department linkage to care program to help reconnect unstably housed populations
"We have continued to provide HIV testing at our site but have not been able to go to partner agencies to provide testing. With less testing encounters, our opportunity to educate on PrEP reduced. We quickly implemented telehealth services for medical care and behavioral health." --Part A, B, and C grantee, South
Most respondents (61%) reported a decreased ability to provide HIV testing during the pandemic and a similar share (64%) reported decreased demand. Smaller shares reported increased capacity (4%) and increased demand (9%). Some worried this drop off in HIV testing would lead to a “surge” of potentially late diagnoses later on. Others expressed concern that decreased HIV testing would impact grant deliverables and future funding.
"We saw a decrease in new [HIV] diagnoses and transfers into care…[W]e are concerned about potentially higher #'s of undiagnosed cases or new patients who haven't yet engaged with us due to COVID19 and worry about a 'surge' of diagnoses later in the year with potentially delayed diagnosis." --Part A, B, and C grantee, South
Some respondents (25%) reported a decline in their ability to offer PrEP, as well as declines in clients seeking these services (47%). Most (56%) had seen no change in their ability to offer PrEP and a smaller share saw an increased capacity (7%). One in ten (11%) reported an increase in demand for PrEP services.
Meeting social service needs was a challenge for some at a time when many saw increased need among clients. Half of respondents (49%) reported increased social, mental health, and substance use service needs during the pandemic. While half retained or increased their ability to provide these support services, nearly one-quarter (23%) reported this capacity had declined.
Staffing challenges were common among respondents. Possibly related to service closures, over one-quarter (27%) of respondents reported staff layoffs or furloughs and the same share reported reducing staff hours. Respondents also described that infection control efforts lead to increased workload, in some cases making meeting grant demands challenging. Likewise, closure of certain activities, such as HIV testing, also presented barriers for meeting grant deliverables for some.
Moreover, staff morale was a challenge reported by three-quarters (74%) of respondents. Respondents described substantial trauma, fear, and strain related to working in healthcare during the COVID-19 pandemic, with one respondent reporting that at least half of their staff had contracted the infection and had significant trauma. Some reported staff had resigned due to fear of COVID-19. In addition to the stress of providing health services during the pandemic, staff also struggled personally as they balanced home and family responsibilities. Many staff faced strain related to increased workload due to staffing limitations, infection control work, and as their peers were diverted to aid with COVID response. Additionally, divisions between staff who were able to work from home and staff required to be on site were reported by some.
"Our organization was hit hard by covid and the refrigerated trailers holding dead bodies were parked outside our clinic. Many staff still struggle with the trauma of working through the pandemic and knowing seeing so many people die. At least half the staff contracted covid and about 1/4 had someone die from covid." --Part C and D grantee, Northeast
"Reduced volume of billable visits with same levels of staffing and increased workload on infection control, PPE, etc. has been a significant financial and morale strain." --Part C grantee, Midwest
"Staff is very stressed out and feeling isolated despite attempts to stay connected with regular zoom calls. Difficult to sustain enthusiasm for projects or services." --Part C and D grantee, West
"COVID has taken a very significant emotional toll on our HIV staff. Many love their jobs because of the support they are able to offer our clients. Having face to face session severely limited has made them feel that their jobs are much less rewarding, which just adds to the rest of the personal and professional stress they are dealing with. Even though we are healthcare providers, well trained in universal precautions, when a staff member of client was actually diagnosed with COVID, there was a great deal of anxiety and even some panic regarding staff risk of infection." --Part A, B, and C grantee, West
"Staff morale is down. People have personal challenges with kids, parents, etc. Many staff have contracted COVID or been exposed to it." --Part A and C grantee, South
"Reduced volume of billable visits with same levels of staffing and increased workload on infection control, PPE, etc. has been a significant financial and morale strain." --Part C grantee, Midwest
While most respondents report sufficient resources in key areas to maintain COVID-era public health practices and safe work and clinical environments, critical gaps remained for many.
The most common gap, identified by one-third (32%) of respondents, was inadequate space for social distancing within the clinic. Respondents elaborated that lack of space was particularly concerning for staff sand patient safety. Potentially related to office crowding, 16% reported insufficient telehealth infrastructure.
"Lack of physical space to coordinate new services (COVID) and social distancing. Staff are sitting on top of each other and the waiting room is jammed with both healthy and sick people. Staff morale!!" --Part B and C grantee, Midwest
One in five (22%) reported insufficient access to COVID-19 testingIn some cases this appears to have meant lack of access to testing altogether but other respondents expressed that while they had access to COVID-19 testing, long result delays meant that testing access was inadequate.
One in ten (10%) respondents reported insufficient PPE for staff six months into the pandemic, including difficulty accessing items like N-95 masks and sanitizer. Others noted that while they have sufficient PPE now, they were very low resourced early on and worry the supplies could be hard come by again. As one respondent said the “future is hard to predict.” In some cases, respondents associated insufficient resources to operate safely with low staff morale.
"PPE supplies remain a moving target. We currently have enough, that may change. But the available supply for purchase is slowing catching up with demand…" --Part A and C grantee, South
"All of the items listed above are sufficient today. However, as we continue with COVID-19 in the months to come, these items like PPE, telehealth equipment, etc. might be insufficient." --Part A, B and C grantee, West
Many respondents who were able to adapt to follow public health guidelines, reported using CARES Act funding to do so. For example, respondents purchased telehealth equipment for themselves and clients, purchased masks and sanitation supplies, and modified their clinical spaces (see Box 1 for a detail on how respondents used CARES Act funding).
Discussion
The majority of Ryan White grantee respondents reported a quick pivot to new ways of providing HIV care and prevention in the COVID-era. They rapidly made significant changes to their operations, in some cases shutting services down all together but more commonly, introducing new offerings such as telehealth and multi-month prescribing. Some faced challenges when these changes were first implemented, including being unsure of how much of operations to shut down, struggling through technology learning curves, and dealing with staffing difficulties but many described eventually finding their footing and reopening to some degree within a “new normal.” Many respondents saw the supplemental Ryan White CARES Act funding as critical to their ability to adjust to new service and staffing needs and some worried about its continued availability as the pandemic wears on. However, some continued to struggle, including at least one respondent who has yet to reopen for any in person visits.
"Our ability to provide services was impacted significantly in March during the initial phases of transition to telehealth. Since then, our outreach, retention in care, and viral suppression rates have recovered to pre-pandemic levels due to extensive outreach efforts on the part of our staff and the successful implementation of telehealth." --Part C and D grantee, Northeast
"Initially, we struggled to make sure services continued to be available. Now we the changes and innovations we have made will make a lasting positive impact on our Program and services." --Part B and C grantee, Northeast
Most found that the new ways of providing care, worked very well for certain patients, including in retaining some previously hard to reach patients in care, and many foresee continuing such practices in the long-term. However, respondents also worried that some patients were being left behind and were concerned that as the pandemic wears on, medicine practiced exclusively virtually will cause problems. Respondents were especially eager to get patients back in for laboratory testing.
Additionally, many faced a shifting payer mix, struggled with engaging with community partners, and some continued to lack basic COVID era necessities, such as PPE. Patient and staff well-being was a top concern for most respondents. Both groups were dealing with significant stress and trauma. Respondents were very mixed in how well they believed they were able to meet client needs and retain them in care during the pandemic. However, despite the clear strain the pandemic has taking on clinical staff, most report resiliency and are figuring out how to best operate during an extraordinary time.
"While it has been challenging at times, it has definitely highlighted the resiliency of our clients and our staff!" --Part A, B and C grantee, South
This work was supported in part by the Elton John AIDS Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
The first Americans were vaccinated today as COVID-19 vaccines are being distributed across the country. A new KFF review of states’ releases and statements about their vaccination priorities finds that most states are following the Centers for Disease Control and Prevention’s (CDC) Advisory Committee on Immunization Practices recommendations for the highest priority group (health care workers and long-term care residents), with some choosing to start with one of the populations in the first weeks as they await more supply.
The review does find a handful of states have decided to include additional populations, like law enforcement, prisoners and those who are homeless in the initial priority group. More than 20 states are further segmenting the priority group of health care workers and long-term care residents based on criteria such as risk of exposure and underlying health conditions.
Most states are still developing plans for their later priorities, for which tough decisions will have to be made between essential workers, seniors, and those with high-risk medical conditions, given what is expected to be ongoing limitations in vaccine supply. But several states already differ from what the CDC is likely to recommend according to the review.
The pandemic and resulting economic crisis have upended any expectations about what health spending, utilization, and the subsequent financial performance of insurers might have looked like this year. The unprecedented decrease in health care spending and utilization in the spring led to rising margins and profits for many insurers. In the summer and fall of this year, spending and service utilization rebounded as patients returned for routine and elective care, adding to costs associated with testing and treating patients with COVID-19. Job losses and economic instability have driven increased enrollment in Medicaid broadly and increases in Medicaid managed care but seemingly modest changes in enrollment in the group and individual markets thus far.
In this brief, we analyze third quarter data from 2018 to 2020 to examine how insurance markets performed financially through the end of September, as the pandemic continued and health care utilization climbed back towards previous levels. We use financial data reported by insurance companies to the National Association of Insurance Commissioners (NAIC) and compiled by Mark Farrah Associates to look at average medical loss ratios and gross margins in the Medicare Advantage, Medicaid managed care, individual (non-group), and fully-insured group (employer) health insurance markets through the third quarter of each year. Third quarter data is year-to-date from January 1 – September 30. A more detailed description of each market is included in the Appendix.
By the end of September, average margins across these four markets remained relatively high (and loss ratios relatively low or flat) compared to the same point in recent years. These findings suggest that many insurers have remained profitable even as both COVID-related and non-COVID care increased in the third quarter of 2020. The results for the individual and group markets continue to indicate that commercial insurers are going to owe substantial rebates to consumers again next year under the Affordable Care Act’s (ACA) Medical Loss Ratio provision. For Medicaid, application of risk sharing arrangements that many states have in place may ultimately reduce overall margins calculated in the quarterly data.
Gross Margins
One way to assess insurer financial performance is to examine average gross margins per member per month, or the average amount by which premium income exceeds claims costs per enrollee in a given month. Gross margins are an indicator of financial performance, but positive margins do not necessarily translate into profitability since they do not account for administrative expenses. However, a sharp increase in margins from one year to the next, without a commensurate increase in administrative costs, would indicate that these health insurance markets have become more profitable during the pandemic.
Insurers are still required to cover the full cost of coronavirus testing and many have continued to voluntarily waive out-of-pocket costs for coronavirus treatment. Still, insurers have seen their claims costs fall and margins increase relative to 2019.
At the end of the third quarter of 2020, average gross margins among individual market and fully-insured group market plans were 21% and 24% higher, respectively, than at the same point last year. Gross margins among Medicare Advantage plans were 35% higher through the third quarter compared to 2019. (Gross margins per member per month for Medicare Advantage plans tend to be higher than for other health insurance markets mainly because Medicare covers an older, sicker population with higher average costs).
Average gross margins for managed care organizations (MCOs) in the Medicaid market were more than twice as high through the third quarter of 2020 as they were through the third quarter of 2019 (a 109% increase). However, compared to the other markets, margins in the Medicaid MCO market are lower because while rates must be actuarially sound, payment rates in Medicaid tend to be lower than other markets. States typically use a variety of mechanisms to adjust plan risk, incentivize performance and ensure payments are not too high or too low, including various options to modify their capitation rates or use risk sharing mechanisms. CMS has provided guidance about options to adjust payments for MCOs during the pandemic, since states and plans could not have reasonably predicted the changes in utilization and spending that have occurred. Many of these adjustments that states can make may occur retrospectively and may not be reflected in the quarterly data.
Medical Loss Ratios
Another way to assess insurer financial performance is to look at medical loss ratios, or the percent of premium income that insurers pay out in the form of medical claims. Generally, lower medical loss ratios mean that insurers have more income remaining after paying medical costs to use for administrative costs or keep as profits. Each health insurance market has different administrative needs and costs, so low loss ratios in one market do not necessarily mean that market is more profitable than another market. However, in a given market, if administrative costs hold mostly constant from one year to the next, a drop in medical loss ratios would imply that plans are becoming more profitable.
Medical loss ratios are used in state and federal insurance regulation in a variety of ways. In the commercial insurance (individual and group) markets, insurers must issue rebates to individuals and businesses if their loss ratios fail to reach minimum standards set by the ACA. Medicare Advantage insurers are required to report loss ratios at the contract level; they are also required to issue rebates to the federal government if their MLRs fall short of required levels and are subject to additional penalties if they fail to meet loss ratio requirements for multiple consecutive years in a row. For Medicaid MCOs, CMS requires states to develop capitation rates for Medicaid to achieve an MLR of at least 85%. There is no federal requirement for Medicaid plans to pay remittances if they fail to meet their MLR threshold, but a majority of states that contract with MCOs do require remittances always or in some cases.
The medical loss ratios shown in this issue brief differ from the definition of MLR in the ACA and CMS Medicaid managed care final rule, which makes some adjustments for quality improvement and taxes, and do not account for reinsurance, risk corridors, or risk adjustment payments. The chart below shows simple medical loss ratios, or the share of premium income that insurers pay out in claims, without any modifications (Figure 2). Average loss ratios in the Medicare Advantage market decreased four percentage points through the first nine months of 2020 relative to the same period in 2019, and average loss ratios in the Medicaid managed care market decreased by an average of seven percentage points, but still on average met the 85% minimum even without accounting for potential adjustments. Group market loss ratios decreased by an average of three percentage points compared to the same point last year.
Average individual market loss ratios also decreased four percentage points in 2020 compared to the third quarter of last year. Loss ratios in the individual market were already quite low and insurers in the market recently issued record-large rebates to consumers based on their experience in 2017, 2018, and 2019.
Discussion
Just as we found in our mid-year analysis, it still appears that health insurers in most markets have become more profitable during the pandemic, though we can’t measure profits directly without administrative cost data. Across all four markets we examined, average gross margins are higher and medical loss ratios are lower than they were at this point last year.
The return of elective and routine care this fall, coupled with the continued costs of testing and treating patients with COVID-19, contributed to slightly higher loss ratios in the Medicare Advantage and group markets in the third quarter compared to the second quarter this year, but increases in claims costs from June through September did not offset the sharp drop earlier in the year. Average medical loss ratios among individual market plans remained more stable this past quarter and are still well below the 80% threshold established by the ACA. Loss ratios in the Medicaid MCO market are lower this year; however, margins in the Medicaid MCO market are low relative to the other markets, and data do not reflect implementation of existing or newly imposed risk sharing mechanisms.
It remains to be seen whether spending and use will change substantially in late 2020. Insurers may see their claims costs fall again this winter as the pandemic worsens and more enrollees delay care due to social distancing restrictions or general fear of contracting the virus. Record numbers of COVID-19 tests and hospitalizations will likely increase claims costs for some insurers though. Insurers are still generally required to cover the entire cost of COVID-19 testing, and many have extended their waivers on cost-sharing for COVID-19 treatment through the end of the year. (The impact of COVID-19 hospitalizations on Medicaid MCO finances will vary by state, since states have multiple options to address the cost of COVID-19 treatment for beneficiaries).
Medicare Advantage insurers that fall short of required loss ratio requirements for multiple years face additional penalties, including the possibility of being terminated. Some Medicare Advantage insurers may take this opportunity to start offering more benefits than they currently do, which are popular and attract enrollees. For Medicaid MCOs, given all the options that states have to modify payments and risk agreements during the pandemic, it is unlikely that these plans will be left with unexpected surpluses or fail to reach their state’s MLR threshold this year.
ACA medical loss ratio rebates in 2021 likely will be exceptionally large across commercial markets. Rebates to consumers are calculated using a three-year average of medical loss ratios, meaning that 2021 rebates will be based on insurer performance in 2018, 2019, and 2020. Individual market insurers were quite profitable in 2018 and 2019, so even if insurers have very high claims costs in the last three months of 2020, these insurers will likely owe large rebates to consumers. Group market insurers may also owe larger rebates to employers and employees than plans have in typical years, as loss ratios are still lower than previous year.
Methods
We analyzed insurer-reported financial data from Health Coverage Portal TM, a market database maintained by Mark Farrah Associates, which includes information from the National Association of Insurance Commissioners (NAIC). We used the “Exhibit of Premiums, Enrollment, and Utilization” report for this analysis. The dataset analyzed in this report does not include NAIC plans licensed as life insurance or California HMOs regulated by California’s Department of Managed Health Care. Additionally, for Medicaid, there are four states (Arizona, California, New York, and Oregon) that have different reporting practices and therefore consistently only have partial NAIC data available.
We excluded plans that filed negative enrollment, premiums, or claims, or reported more than 1,000 hospital inpatient days per 1,000 enrollees. We only included plans that were categorized as having a “medical” focus in our analysis and exclude “specialty” plans which are categorized as “ancillary or supplemental benefit plans.” We corrected for plans that did not file “member months” in the annual statement but did file current year membership by imputing these values.
The group market in this analysis only includes fully insured plans.1 Premiums to Medicare Advantage plans do not include payments for Medicare Part D benefits. NAIC defines “Medicaid” as “business where the reporting entity charges a premium and agrees to cover the full medical costs of Medicaid subscribers.” This explicitly excludes Administrative Service Only (ASO) plans. We only use “medical” focused plans to help exclude any specialty plans; however, prepaid ambulatory health plans (PAHPs), prepaid inpatient health plans (PIHPs), or Programs of All-Inclusive Care for the Elderly (PACE) plans may be included in the analysis due to NAIC’s definition of Medicaid. We compared the NAIC plans from the second quarter of 2018 to the plans in the Center for Medicare and Medicaid Services’ Medicaid Managed Care Enrollment Report and removed three plans from our analysis that did not offer comprehensive Medicaid acute services. However, CMS enrollment data is not available for 2019 or 2020, so we were not able to compare for the other years.
Gross margins were calculated by subtracting the sum of total incurred claims from the sum of unadjusted health premiums earned and dividing by the total number of members in each market. Therefore, calculations represent trends in each market, not for individual plans. Premiums for Medicare Advantage plans primarily consist of federal payments made to plans for Medicare-covered benefits and include any additional amounts plans may choose to charge their enrollees. Premiums for the individual market were not adjusted to account for rebates required to be remitted to enrollees. Premiums for Medicaid do not reflect contractual adjustments related to risk corridors or other risk-sharing adjustments.
To calculate medical loss ratios, we divided the market-wide sum of total incurred claims by the sum of all unadjusted health premiums earned. Medical loss ratios in this analysis are simple loss ratios and do not adjust for quality improvement expenses, taxes, or risk program payments. For example, the 2016 CMS managed care final rule (CMS-2390-F) allows managed care plans to adjust their medical loss ratio calculations to account for quality improvement expenditures and the removal of estimated Medicaid taxes, licensing, and regulatory fee from the revenues when submitting data to CMS. It should be noted that other organizations and agencies use claims and premiums reported in the “Statement of Revenues & Expenses” for their medical loss ratio calculations.
Appendix
Individual Market. The individual market, which accounted for more than 13 million people in 2019, includes coverage purchased by individuals and families through the Affordable Care Act’s exchanges (Marketplaces) as well as coverage purchased directly off-exchange, which includes both plans complying with the ACA’s rules and non-compliant coverage. (e.g., grandfathered policies purchased before the ACA went into effect and some short-term plans). The federal government provides subsidies for low-income people in the Marketplace and includes measures, such as risk adjustment, to help limit the financial liability of insurers. Insurers in the individual market receive premium payments from enrollees, plus any federal subsidies for people in the Marketplaces.
Group Market. The fully-insured group market serves employers and their employees that are enrolled in fully-insured health plans. This market includes both small and large group plans, but excludes employer-sponsored insurance plans that are completely or partially self-funded, which account for 61% of all workers with employer-sponsored insurance. Roughly 30 million people were enrolled in fully-insured group market plans in 2019. Plans typically receive premium payments from both employers and their employees. While both average claims and average premiums for enrollees in the group market have increased, the market has been relatively stable for insurers over the past decade.
Medicaid Managed Care. The Medicaid Managed Care market includes managed care organizations (MCOs) that contract with state Medicaid programs to deliver Medicaid services to enrollees. More than two-thirds (around 54 million people) of all Medicaid beneficiaries nationally receive most or all of their care from risk-based MCOs. There is significant variation across states with regards to services that are covered by MCOs.
KFF defines comprehensive MCOs as those that provide comprehensive Medicaid acute care services and, in some cases, long-term services and supports as well. This excludes prepaid ambulatory health plans (PAHPs), prepaid inpatient health plans (PIHPs), and Programs of All-Inclusive Care for the Elderly (PACE). However, NAIC defines “Medicaid” as “business where the reporting entity charges a premium and agrees to cover the full medical costs of Medicaid subscribers” and only explicitly excludes Administrative Service Only (ASO) plans from their reporting. While we only use “medical” focus plans to help exclude any specialty plans, PAHPs, PIHPs and PACE plans may not be excluded due to NAIC’s definition of Medicaid. Additionally, for Medicaid, there are four states (Arizona, California, New York, and Oregon) that have different reporting practices and therefore consistently only have partial NAIC data available.
Mark Farrah Associates Health Coverage Portal TM includes data from fully capitated risk-based MCOs as well as non-comprehensive Primary Care Case Management (PCCM) plans and some specialty plans. PCCM plans have lower capitated payments than comprehensive MCO agreements because a primary care physician is paid a smaller flat fee for case management and care coordination responsibilities, but the remainder of services an enrollee receives are delivered on a Fee-For-Service agreement.
Medicare Advantage. The Medicare Advantage market provides Medicare-covered benefits through private plans to more than 24 million Medicare beneficiaries in 2020, with enrollment projected to increase to nearly half of all Medicare beneficiaries by the end of the decade. The federal government makes risk-adjusted payments (higher payments for sicker enrollees and lower payments for healthier enrollees) to plans (averaging $11,545 per enrollee in 2019) to cover the cost of benefits covered under Medicare Parts A and B, with additional payments for costs associated for prescription drug coverage. Some plans charge enrollees an additional premium. The majority of Medicare Advantage plans offer supplemental benefits, such as dental, vision and hearing.
Endnotes
61% of workers with employer-sponsored insurance are enrolled in a plan that is completely or partially self-funded. The group market in this analysis only includes fully-insured group plans.
↩︎
A new chart collection looks at how internet access may affect health care in the U.S., as more providers turn to telemedicine during the pandemic. An estimated 25 million Americans – about 8% of the population – lack access to internet at home. Hispanic and Black Americans, seniors, rural residents, and those living in poverty are more likely than other groups to lack internet access.
The chart collection is available on the Peterson-KFF Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.
KFF Launches New COVID-19 Vaccine Monitor to Track the Public’s Confidence in the Vaccine and Experiences for the Duration of the Pandemic
First Survey Finds Enthusiasm for Getting Vaccinated Varies Across the Public; Most Fall into “As Soon As Possible” and “Wait and See” Categories, While Some Say “Only if Required” and “Definitely Not”
Republicans and Black Americans are More Likely to Be Hesitant but Even Among These Groups Reasons Vary
KFF has launched a new COVID-19 Vaccine Monitor to dive deeply into the public’s views about the vaccine and experiences getting it for as long as the pandemic lasts.
First results released today show that Americans’ enthusiasm for getting a COVID-19 vaccination varies substantially across groups, with Republicans and Black Americans among those most hesitant.
Overall, 71% of the public says they definitely or probably would get a vaccine, up from 63% in September. Still about a quarter (27%) of the public is vaccine hesitant, saying they probably (12%) or definitely (15%) would not get a COVID-19 vaccination even if it were available for free and deemed safe by scientists.
Hesitancy remains highest among Republicans (42%), those ages 30-49 (36%), rural residents (35%), and Black adults (35%), a group that has been disproportionately affected by the pandemic.
Some Black adults are hesitant for reasons that could change with more information. For example: 71% of those who say they won’t get vaccinated say a major reason is that they are worried about possible side effects (which are expected to be mild) and half (50%) say they worry they could get COVID-19 from the vaccine. But nearly as many hesitant Black adults (47%) say they are hesitant to get the COVID-19 vaccine because they don’t trust vaccines in general.
Among another large group of the hesitant – Republicans – top reasons for not getting vaccinated may be tougher to change, including believing the dangers of COVID-19 have been exaggerated (57% of hesitant Republicans cite this as a major reason), and that they don’t trust the government to ensure a vaccine is safe and effective (56%). Nearly as many (54%) also worry about possible side effects.
“Many who are hesitant are in wait-and-see mode, and their concerns include worries about side effects and whether the vaccine can cause COVID-19, which may dissipate as people get more information and see the vaccine introduced successfully among people they know,” KFF President and CEO Drew Altman said.
The initial Monitor survey identifies four broad categories of enthusiasm for getting a vaccination that pose different messaging challenges:
A third of the public (34%) are in the most enthusiastic “as soon as possible” group, who want to get vaccinated as soon as they can. This group is disproportionately made up of Democrats, seniors, white adults, and people with college degrees. Some in this group may become frustrated if they are not among the priority groups receiving early vaccinations.
The “wait and see” group is the largest, comprising 39% of the public, and generally want to see how vaccinations work for other people before getting it themselves. This group looks like the public at large, and their willingness to get vaccinated may depend on what they learn during its initial rollout, including news reports about its effectiveness, safety and side effects.
The “only if required” group is the smallest, representing 9% of the public, and say they would only get vaccinated if required for work, school or other activities. Most (61%) of this group are essential workers who work outside their homes during the pandemic, a category considered high risk for exposure.
The most resistant group, representing 15% of the public, says they would “definitely not” get vaccinated, even if it were deemed safe and available for free. This group is disproportionately made up of Republicans and of people with no more than a high-school level education.
“Many Americans who are hesitant are simply reserving judgment before they are ready to get vaccinated. However, nearly one in four Republicans don’t want to get vaccinated because they don’t believe COVID poses a serious threat,” KFF Executive Vice President Mollyann Brodie said. “It will be a real challenge to undo COVID denialism among this slice of President Trump’s political base.”
Those who are more hesitant to get vaccinated for COVID-19 are also more likely to harbor misconceptions about the pandemic and related public health measures, which may make them less receptive to public health messages generally, including those about the importance of vaccinations.
For example, two-thirds (68%) of the “definitely not” group and more than a third (37%) of the “only if required” group incorrectly believe that wearing a face mask does not protect the wearer from coronavirus. Similarly, more than half (54%) of the “definitely not” group and about three in ten (29%) of the “only if required” group believe that wearing a face mask is harmful to one’s health.
Personal Health Care Providers are the Public’s Most Trusted Sources for Vaccine Information
As with many health topics, the poll finds people’s personal health care providers are at the top of the list as a trusted source of vaccine information, ahead of any national, state, or local messengers.
More than eight in ten (85%) say they trust their own doctor or health care provider to provide reliable information on a COVID-19 vaccine, while about seven in ten also trust national messengers like the U.S. Centers for Disease Control and Prevention (73%), the Food and Drug Administration (70%), and Director of the National Institute of Allergy and Infectious Diseases, Dr. Anthony Fauci (68%), as well as their local public health department (70%).
Somewhat fewer, but still a majority, put at least a fair amount of trust in their state government officials (58%), President-elect Joe Biden (57%), and pharmaceutical companies (53%), while about a third (34%) say they trust President Trump.
Trust in personal doctors is high among all racial and ethnic groups and across partisan groups. When it comes to government sources of information, however, a much larger share of Democrats than Republicans say they trust such sources to provide reliable information about a COVID-19 vaccine, with independents generally falling in the middle.
The survey suggests the race to develop a vaccine is helping to improve the public’s views of pharmaceutical companies. Most (58%) of the public say that drug companies working on a COVID-19 vaccine are equally interested in the public good and making a profit. That contrasts sharply with the public’s view in July that found the majority of the public (76%) say drug makers generally care mostly about profits.
Designed and analyzed by public opinion researchers at KFF, the survey was conducted from Nov. 30-Dec. 8 among a nationally representative random digit dial telephone sample of 1,676 adults, including oversamples of adults who are Black (390) or Hispanic (298). Interviews were conducted in English and Spanish by landline (391) and cell phone (1,285). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and focus groups, this project will track the dynamic nature of public reactions as vaccine development unfolds, including vaccine confidence and hesitancy, trusted messengers and messages, as well as the public’s experiences with vaccination as distribution begins.