Key Takeaways
- The Kaiser Family Foundation has conducted the KFF Women’s Health Survey approximately every four years since 2001 to provide a look into the range of women’s health care experiences, especially those that are not typically addressed by most surveys. The election year provided a unique opportunity to ask a nationally representative sample of 3,661 women and 1,144 men ages 18-64 about seven women’s health policies likely to be discussed with Democrats in power and how much of a priority they should be for the new President and Congress.
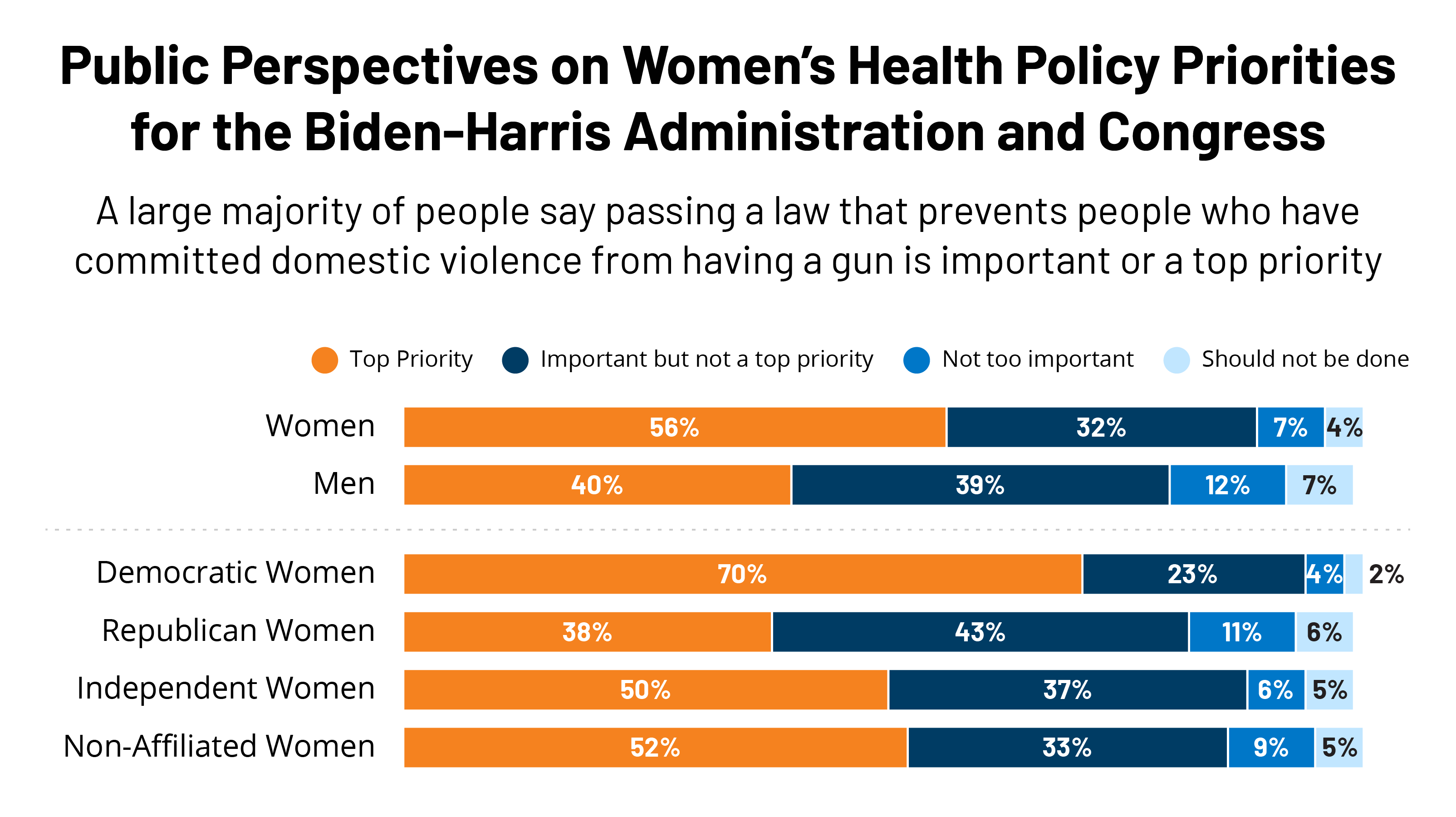
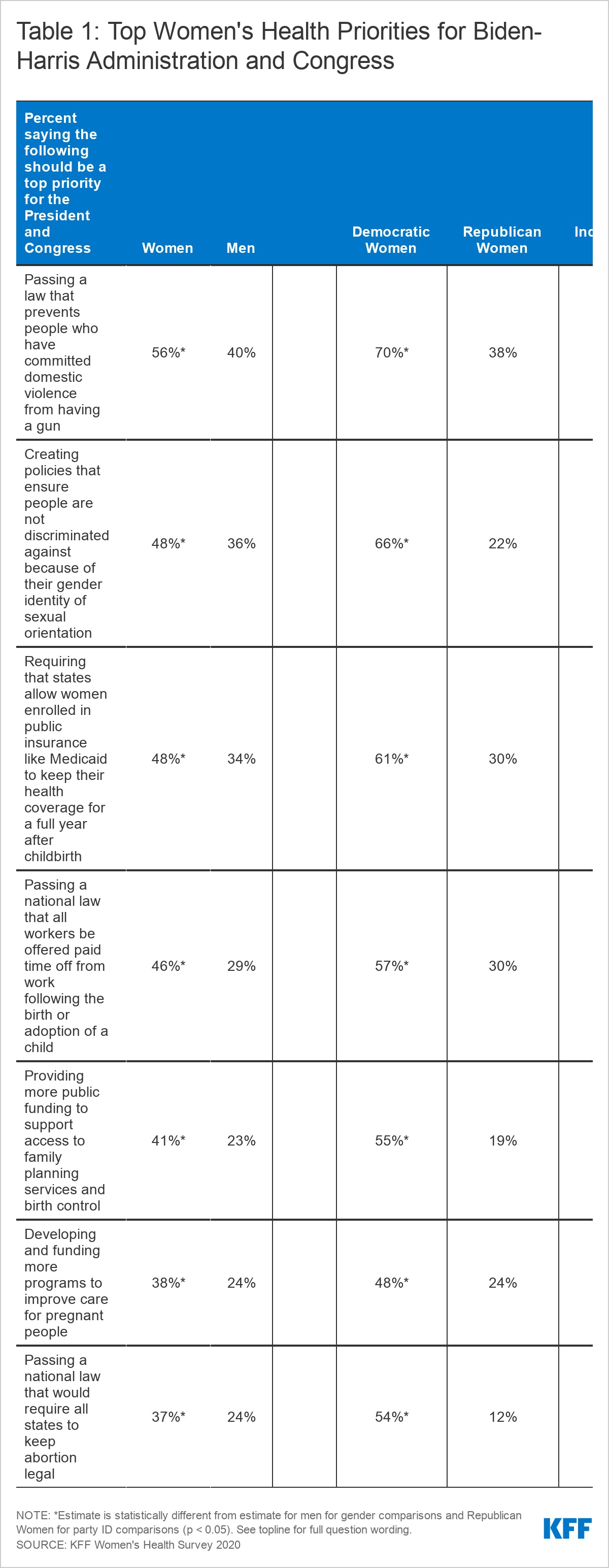
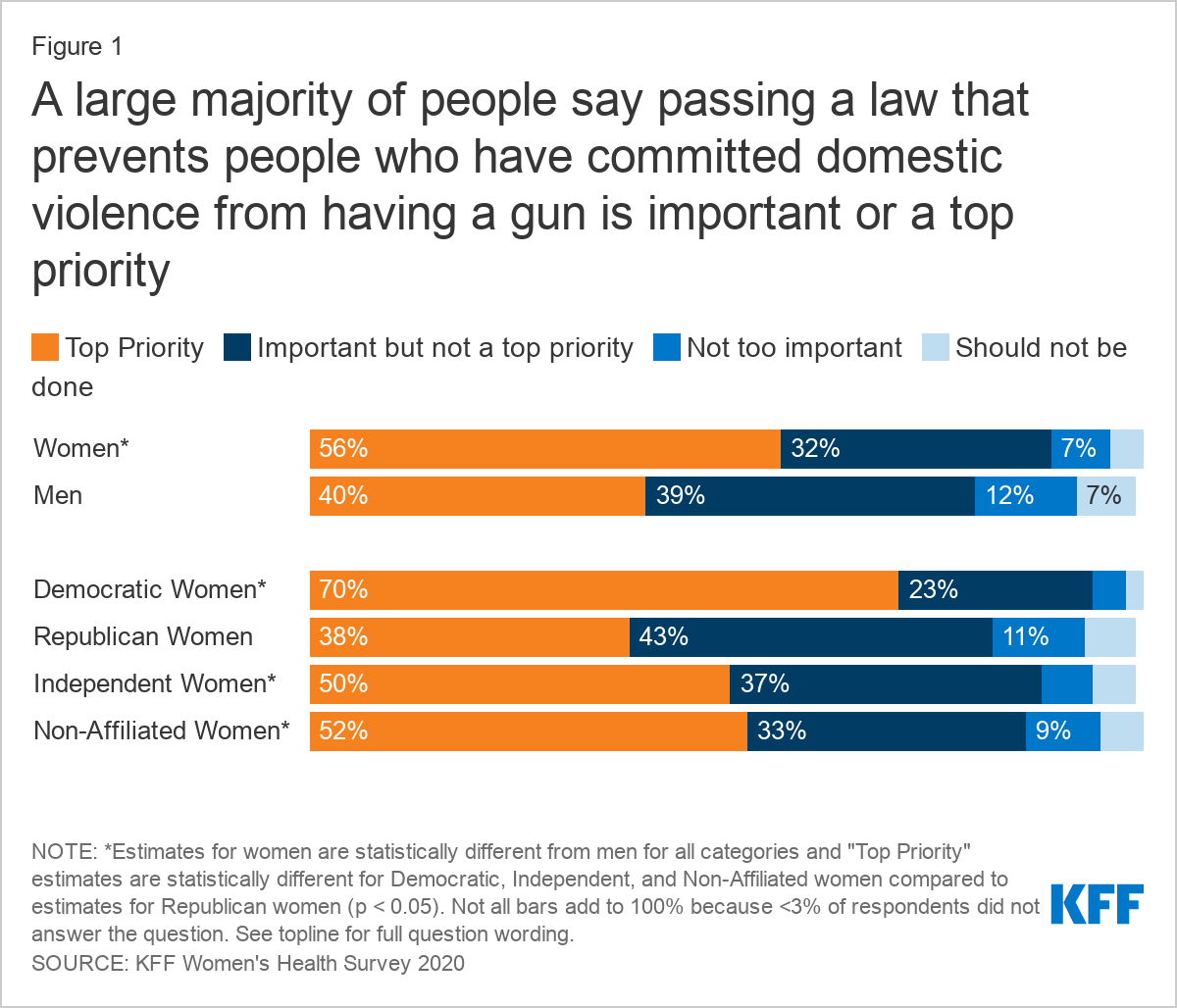
- Of the seven policy issues we asked about, passing a law that prevents people who have committed domestic violence from having a gun is a top priority for the largest share of women (56%) and men (40%), and women across party lines.
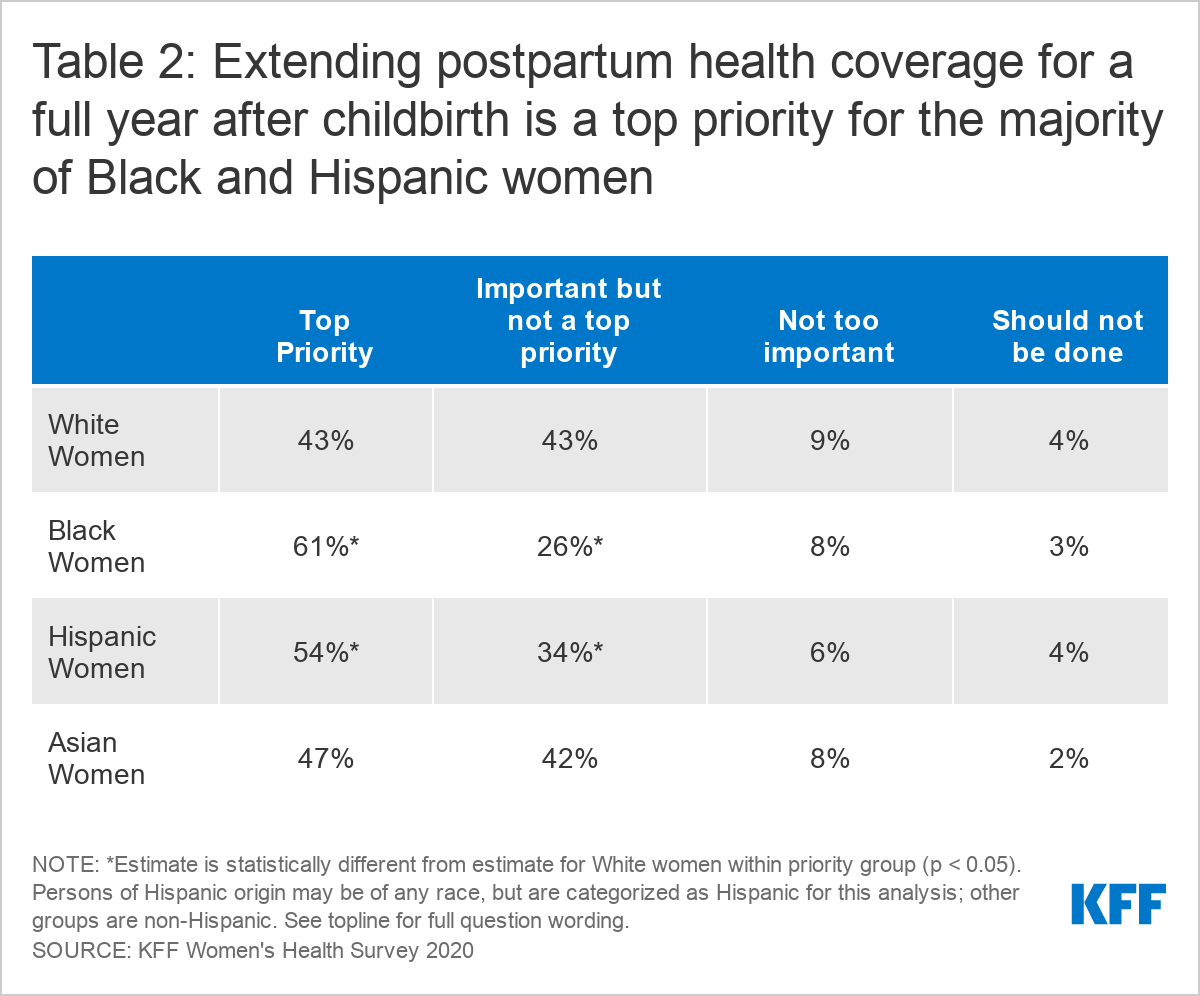
- The most important policy issue to Black women (61% said top priority), among those we asked about, is requiring that states allow women enrolled in public programs like Medicaid to keep their health coverage for a full year after childbirth.
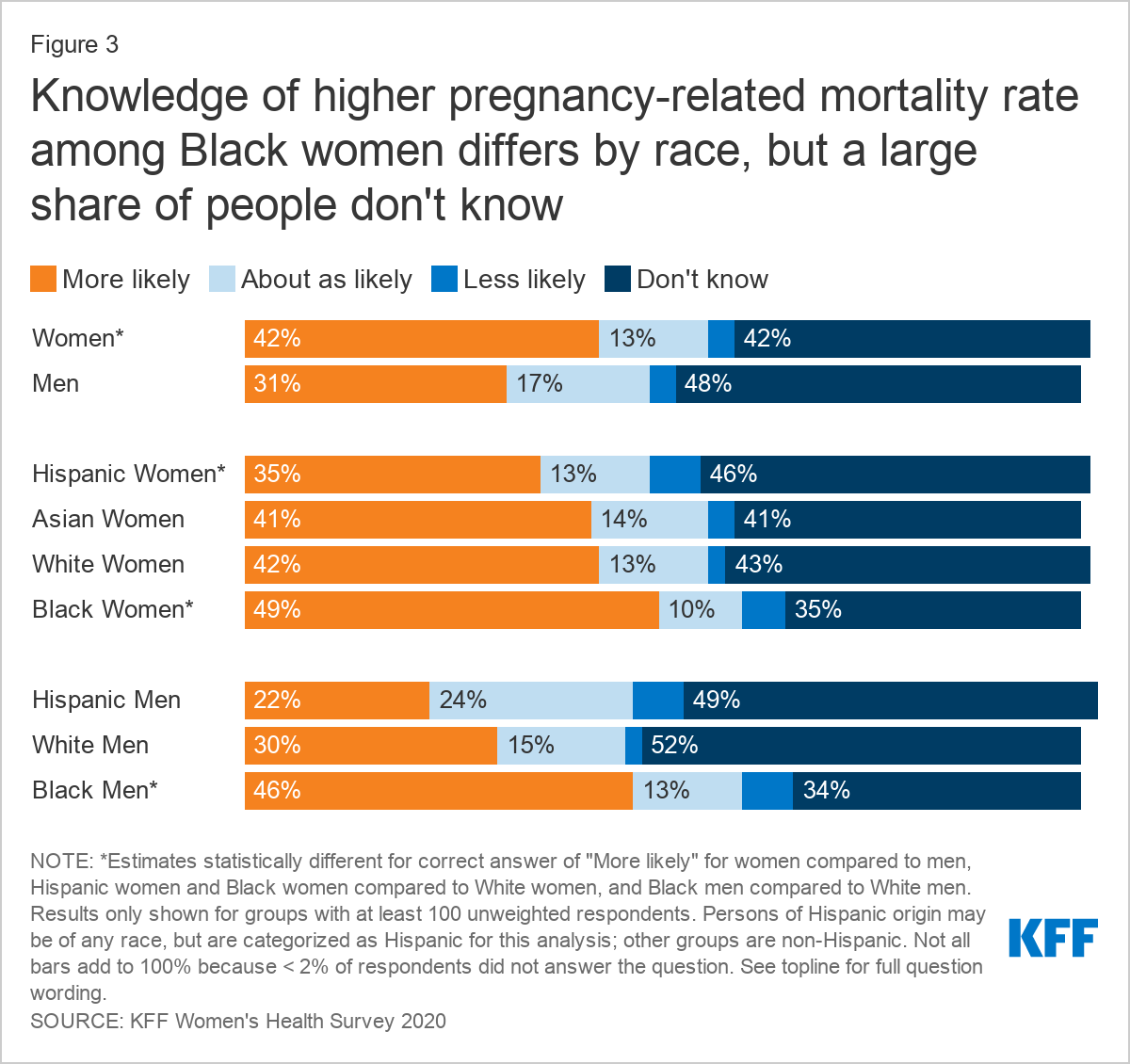
- Most people are unaware that Black women are more likely to die from pregnancy or childbirth than White women.
- One of the policy issues with the biggest gender differences in the top priority ranking is passing a national law that all workers be offered paid time off from work following the birth or adoption of a child (46% of women say it should be a top priority compared to 29% of men). Only three in ten women (29%) and men (31%) know that the U.S. does not have a national policy where workers can take paid time off from work for the birth or adoption of a child.
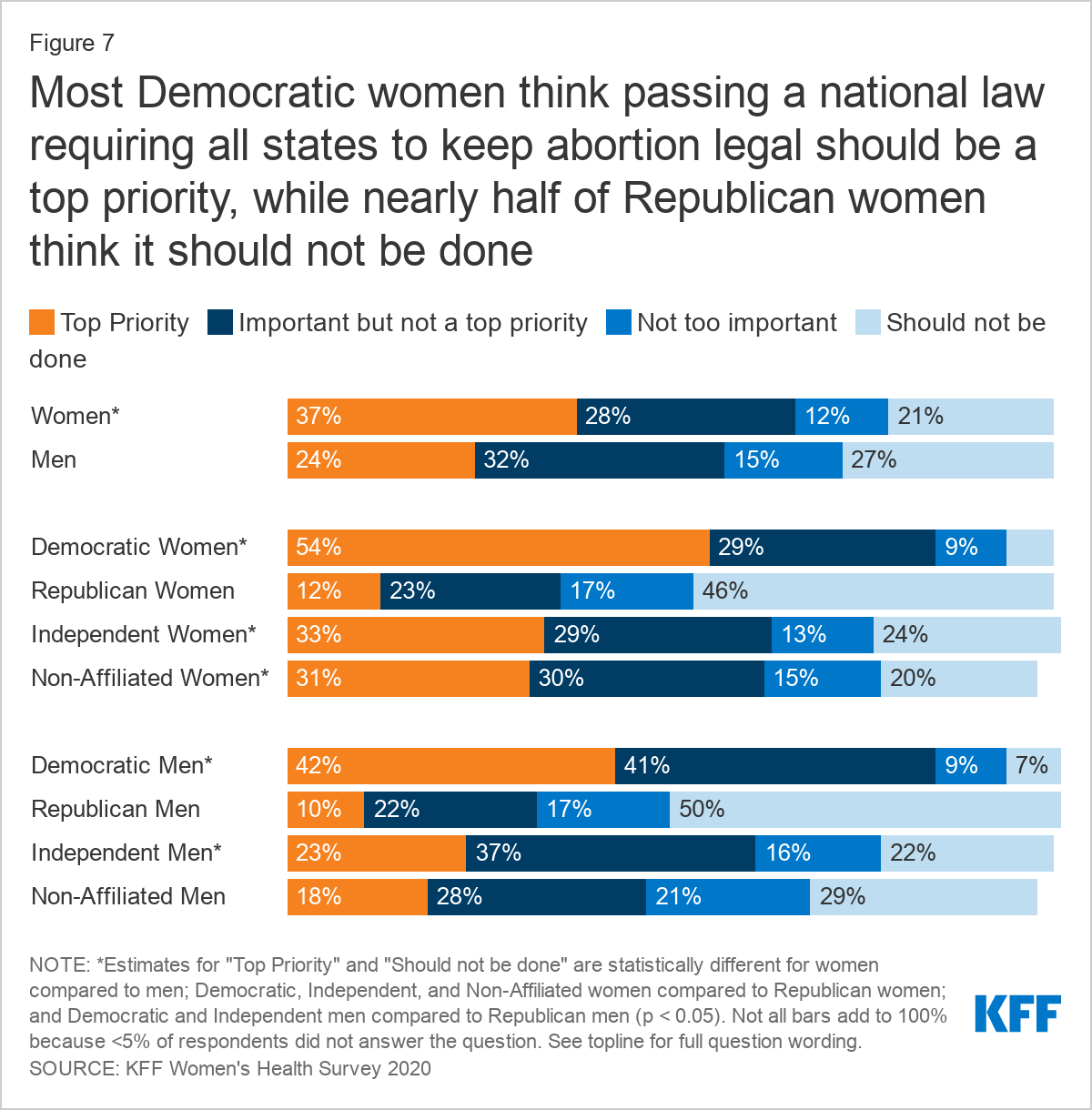
- Not surprisingly, attitudes toward passing a national law requiring states to keep abortion legal split along partisan lines with more than half of Republican women (63%) saying it is not too important or should not be done, in contrast to 54% of Democratic women who rank it as a top priority.
Introduction
The Biden-Harris Administration and new Congress, with Democratic majorities in the House and (effectively) the Senate, are expected to place a higher priority on certain women’s health issues than the previous administration. President Joe Biden and Vice President Kamala Harris prioritized many women’s health issues during their campaign, including reversing the Trump Administration’s Title X regulations, codifying Roe v. Wade, addressing the U.S.’s high maternal mortality rate, creating a national paid family and medical leave program, and reauthorizing the Violence Against Women Act.
KFF’s latest Women’s Health Survey surveyed 3,661 women and 1,144 men ages 18-64 (Methodology) between November 19 and December 17, 2020. Among several topics, we asked respondents how much of a priority seven key women’s health policies should be for the President and Congress – top priority, important but not a top priority, not too important, or should not be done. This issue brief examines attitudes toward those policy priorities and differences by gender, political party affiliation, and demographic factors.
Top Policy Priorities
We asked survey respondents about seven policy priorities around maternal health, paid leave, and sexual and reproductive health that are likely to be discussed with the change in control of the White House and the Senate. Women are more likely than men to say all these issues were a top priority. President Biden campaigned on many of these policy priorities, and indeed, there is variation in support of these policies by political affiliation. Across the board, women who identified as Democrats are more likely to say each of these were top priorities compared to Republican women or women who identify as political independents (Table 1).
Domestic Violence
As Senator, President Biden introduced the Violence Against Women Act (VAWA) that was signed into law in 1994 by President Bill Clinton. VAWA, which expired in 2018, helped establish many violence prevention efforts, including funding for rape crisis centers, shelters, and other supports for people who have experienced domestic violence. The House of Representatives passed the VAWA Reauthorization Act of 2019, but it stalled in the Senate due to Republican objections to a new provision that would prohibit perpetrators of domestic violence from purchasing or possessing a firearm. President Biden has said he will make VAWA reauthorization one of his top first 100-day priorities.
Of the seven policy issues we asked about, passing a law that prevents people who have committed domestic violence from having a gun is a top priority for the largest share of women (56%) and men (40%), and women of all political affiliations, though more Democratic (70%), independent (50%), and non-affiliated (52%) women than Republican women (38%) rank it a top priority (Figure 1).
Passing a law that prevents people who have committed domestic violence from having a gun is the most important issue to Asian women, with 73% saying this issue should be a top priority for the President and Congress. It is also the issue that the largest shares of White women (52%) and Hispanic women (58%) say should be a top priority.1
Discrimination
Section 1557 of the Affordable Care Act (ACA) prohibits discrimination based on race, color, national origin, sex, age, and disability in health care, but the Trump Administration revised the law’s regulations and eliminated some of the protections from discrimination based on gender identity, sex-stereotyping, and sexual orientation. During his campaign, President Biden pledged to revise those regulations to again prohibit this type of discrimination in health care, and on his first day as President, he issued an Executive Order to that effect.
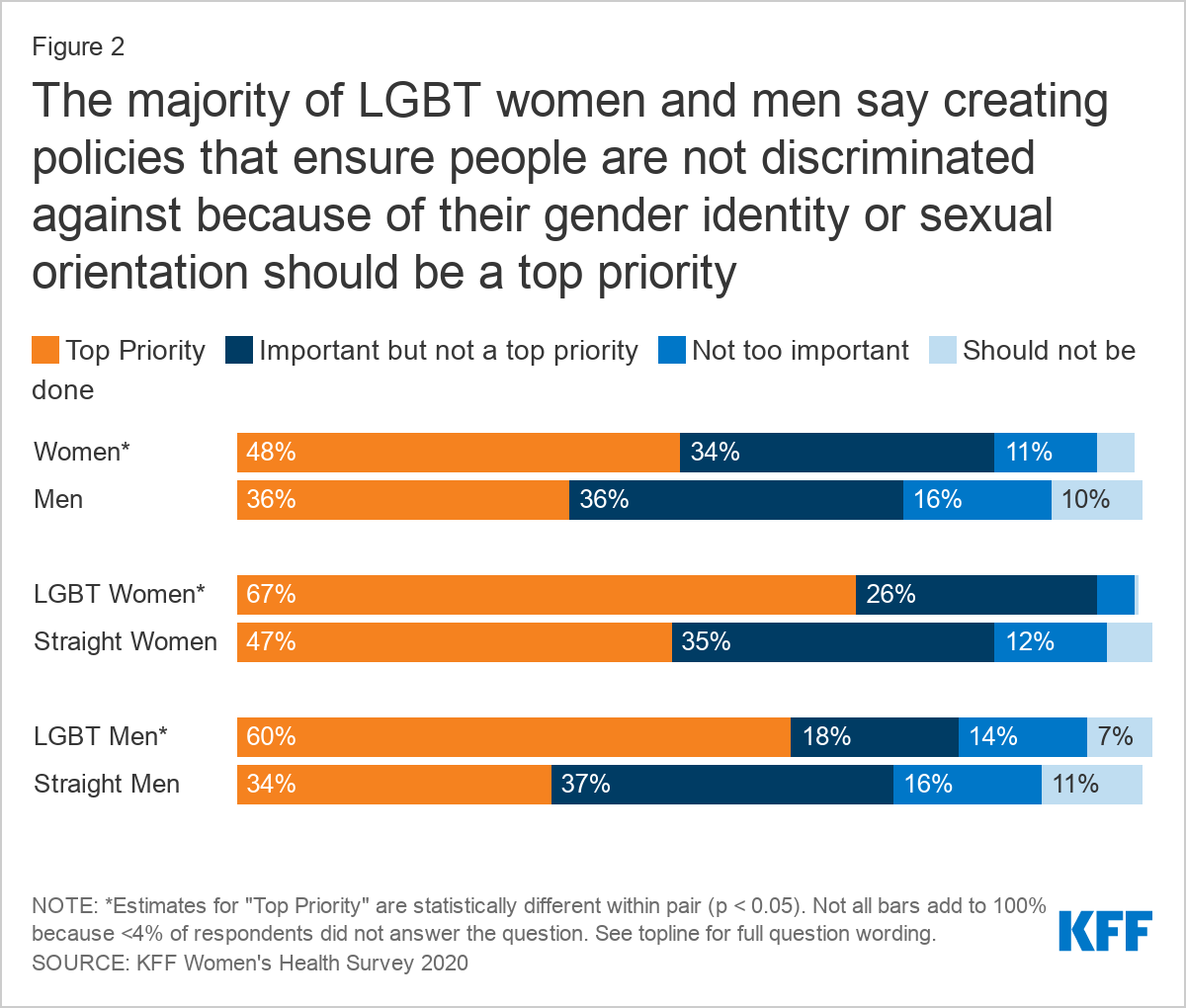
Creating policies that ensure people are not discriminated against because of their gender identity or sexual orientation is the next policy issue that has the next largest shares of both men (36%) and women (48%) who say it should be a top priority. Two-thirds of Democratic (66%) and nearly half of independent women (46%) also believe it should be a top priority. Two-thirds (67%) of LGBT women and 60% of LGBT men cite this issue as a top priority, compared to 47% of straight women and 34% of straight men (Figure 2).
Maternal Health
The Medicaid program finances more than four in ten births in the U.S.; coverage for pregnant enrollees ends 60 days after delivery. In the 39 states (including D.C.) that have expanded Medicaid under the ACA, postpartum women have a pathway to affordable coverage after those 60 days if their incomes remain modest. In the states that have not expanded Medicaid, many women who have Medicaid coverage for their pregnancy are left without a pathway to coverage and become uninsured two months after giving birth. This happens because the income eligibility limits for traditional Medicaid are lower than they are for pregnancy-related Medicaid in those states.2 CDC data show roughly one-third of all pregnancy-related deaths occur one week to one year after a pregnancy ends. Black women are significantly more likely than women of other races to have a severe maternal morbidity event at the time of delivery that could lead to death or require long-term care.
In the campaign, President Biden supported efforts to develop policy responses to address the high rate of maternal deaths among Black women. One policy proposal that has gained some traction is extending Medicaid’s coverage for pregnancy from 60 days postpartum to 12 months postpartum. Also, the Biden Administration could approve pending state waivers to extend postpartum Medicaid coverage.
Nearly half (48%) of women say that requiring states to allow women enrolled in public insurance like Medicaid to keep their health coverage for a full year after childbirth should be a top priority. Among the policy issues we asked about, this is the most important issue to Black women (61% said top priority) (Table 2), women with incomes below 200% of the federal poverty level (FPL) (50%),3 and women enrolled in Medicaid (56%).
Black women are 3.2 times more likely to die from a pregnancy-related complication than White women, but awareness of this substantial difference is not widely known. Among women with a college education or higher, Black women are 5.2 times more likely to die from a pregnancy-related complication than White women. When asked if Black women are more or less likely to die from pregnancy or childbirth than White women, one third of men (31%) and 42% of women know that Black women are more likely to die. About half of Black women (49%) and men (46%) are aware of the disparity (Figure 3).
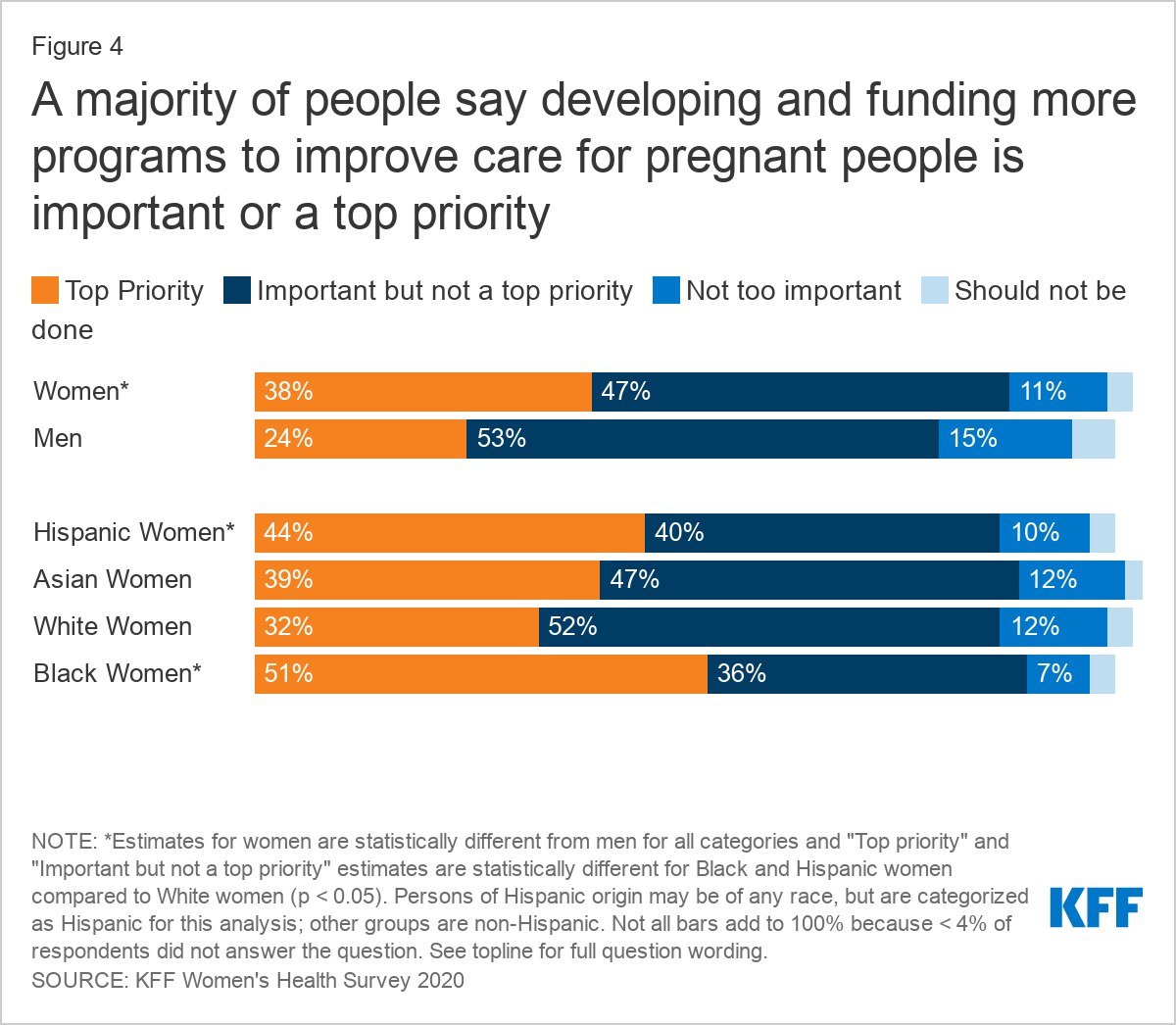
A majority also say developing and funding more programs to improve care for pregnant people should be a top priority or an important priority (Figure 4). About half of Black women (51%) and Democratic women (48%) say this should be a top priority. However, one-quarter of Republican women (25%) and one in five men (20%) say it is not too important or should not be done. To help improve care for pregnant people and improve maternal and infant outcomes, Congress took up several bills in the last session, including one sponsored by then-Senator Kamala Harris, that include, among others, proposals to improve data collection on maternity care; fund and require clinical training on health equity and implicit bias; use evidence-based quality improvement methods; diversify the perinatal workforce; and develop broader maternity care provider networks in rural areas.
Paid Parental Leave
The U.S. does not have a national paid parental leave policy. Federal employees were recently granted 12 weeks of paid parental leave following the birth or adoption of a child, but the 2019 KFF Employer Health Benefits Survey found that only 35% of non-federal workers are employed at a firm that offers paid parental leave for the birth or adoption of a child (voluntarily or required by states or local law), with substantial variation by firm characteristics.
Our survey finds that about three in ten women (29%) and men (31%) know that the U.S. does not have a national paid leave policy. The largest share of respondents to this question say they do not know. One-third of working mothers (32%) know that the U.S. does not have a national paid leave policy, slightly higher than non-working mothers (26%).
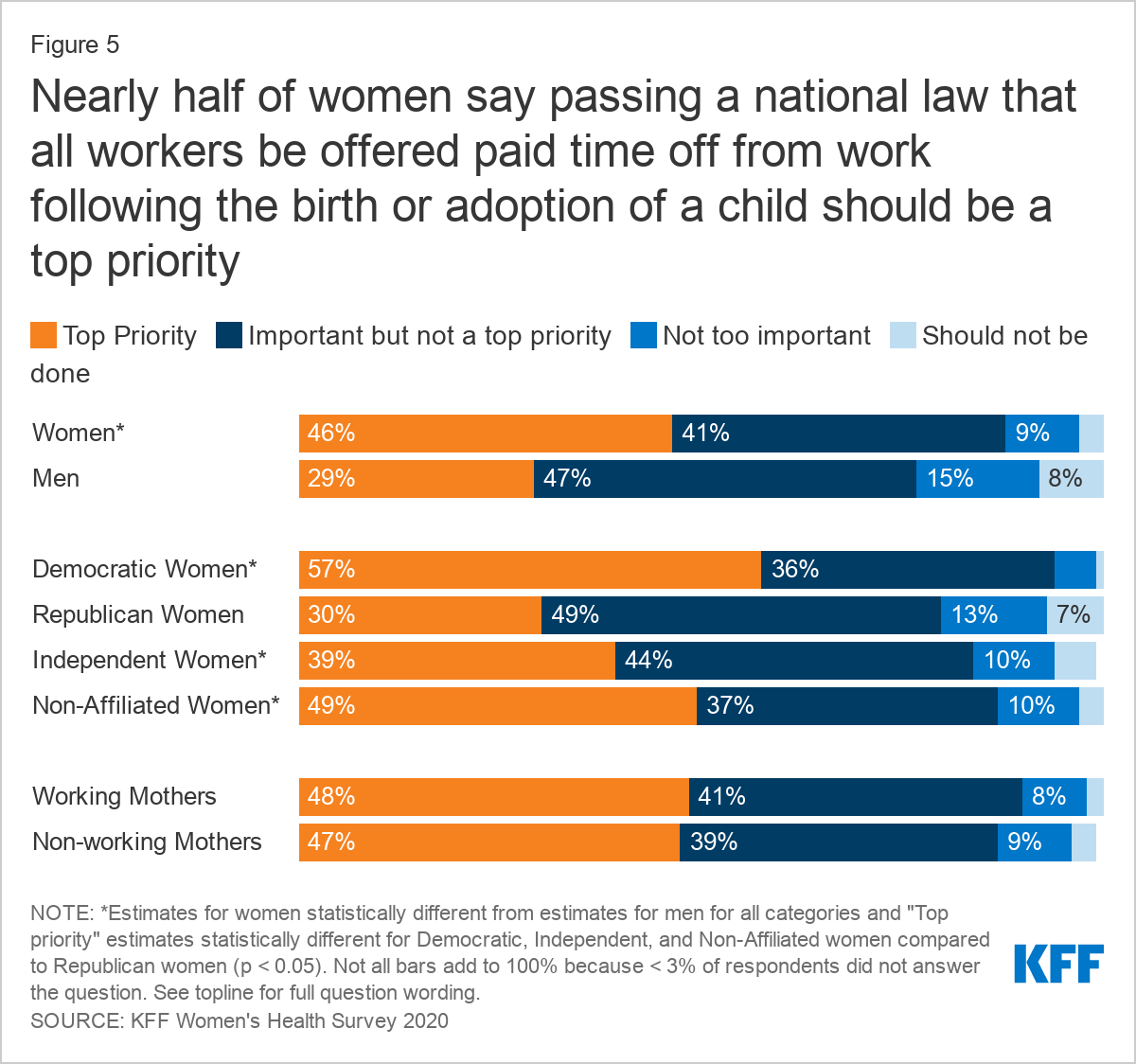
Among the policy priorities asked about, support for passing a national law that all workers be offered paid time off work following the birth or adoption of a child has the largest gender and age differences, with 34% of men and 50% of women ages 18-49 ranking it a top priority compared to 18% of men and 37% of women ages 50-64. A majority of women across party lines and race/ethnicity groups say that this issue is either important or a top priority, with larger shares of Democratic women (57%) and Black women (56%) than Republican women (30%) and White women (40%) saying it should be a top priority (Figure 5).
Family Planning
Though restricted under the Trump Administration, the Title X family planning program provides low- or no-cost family planning services and birth control to millions of low-income women and men. The services provided by Title X clinics help women avoid unintended, mistimed, or unwanted pregnancies and provide access to preventive care and STI screening and treatment. Annual funding for the Title X program has not increased for the past 10 years, though research suggests that the program would need more than twice that amount to adequately meet the need for publicly-funded family planning.
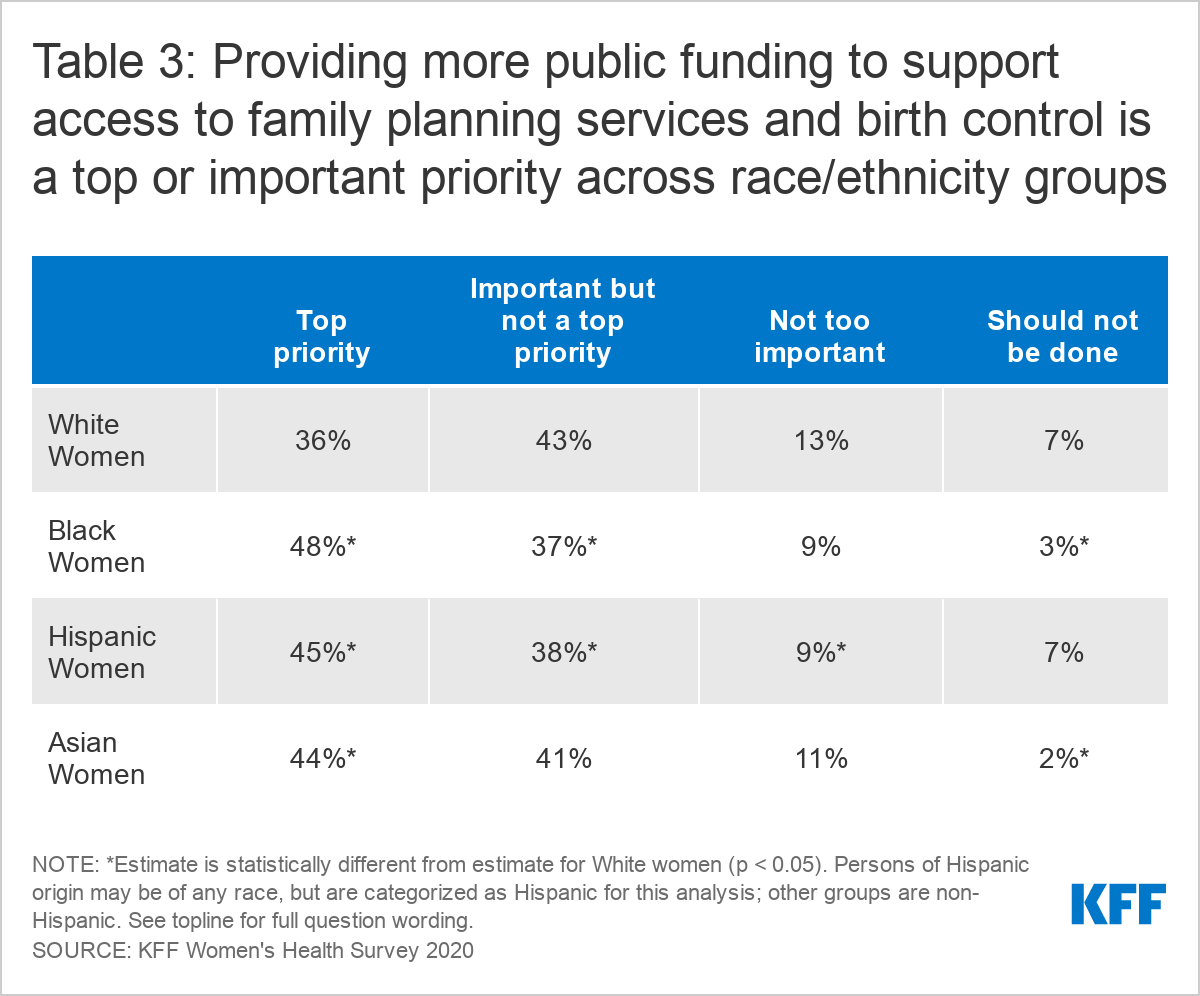
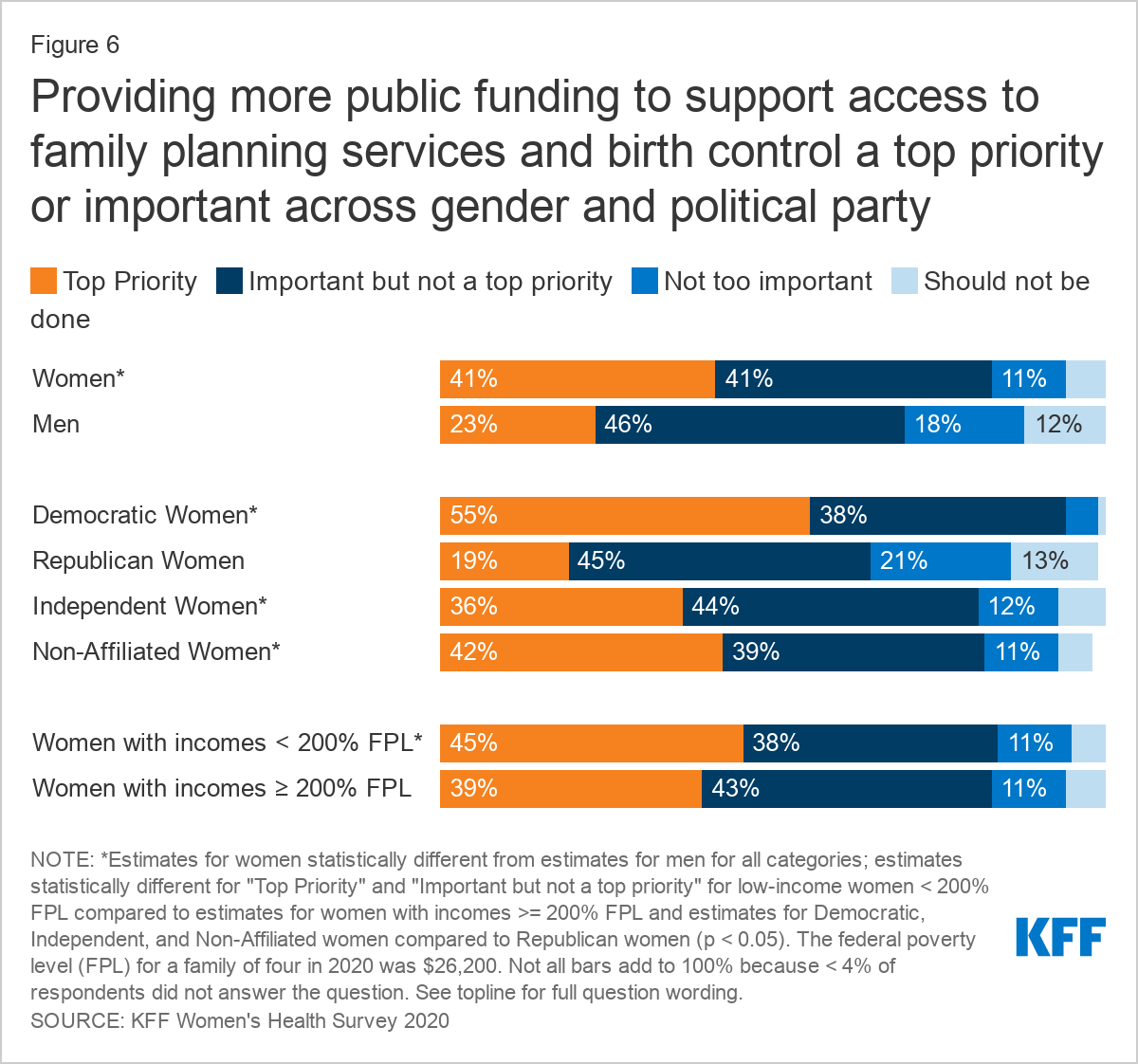
The majority of survey respondents say that providing more public funding to support access to family planning services and birth control should be a top or important priority (Table 3). This policy priority was rated a top priority for a larger share of Black women (48%), Hispanic women (45%), and Asian women (44%) compared to White women (36%). Larger shares of Democratic (93%), independent (80%), and non-affiliated (81%) women say this should be a top priority or important compared to Republican (64%) women. A larger share of women with incomes below 200% FPL (45%) say this should be a top priority compared to women with incomes ≥ 200% FPL (39%) (Figure 6). Three in ten men (30%) and about one-third of Republican women (34%) say this is “not too important” or “should not be done.”
Abortion Rights
It is widely expected that in the coming years, the U.S. Supreme Court will hear a challenge to the right to abortion established in Roe v. Wade. Ten states have laws that would ban all or nearly all abortions if Roe v. Wade were overturned. Seven states have laws that express the intent to restrict the right to legal abortion to the maximum extent permitted by the Supreme Court in the absence of Roe v. Wade. Passing a national law that would require all states to keep abortion legal, or codifying Roe v. Wade into law, would provide a federal right to abortion if Roe v. Wade were overturned by the Supreme Court. President Biden has pledged support for legislation codifying Roe v. Wade and the right to abortion in all states, though this extremely partisan issue would likely be met with resistance.
More than one-third (37%) of women say passing a national law that would require states to keep abortion legal should be a top priority, compared to about one-quarter (24%) of men. More than half (54%) of Democratic women say it should be a top priority, in contrast to 12% of Republican women. A larger share of respondents opposes this policy compared to other health and family policy issues tested in the survey, with 21% of women and 27% of men saying this “should not be done,” with a wide partisan split. Almost half of Republican women (46%) say that passing a national law requiring states to keep abortion legal should not be done, in contrast to 6% of Democratic women (Figure 7). A larger share of White women (25%) says passing a national law requiring all states to keep abortion legal should not be done, compared to Hispanic (19%), Asian (10%), and Black women (11%).
Conclusion
The KFF Women’s Health Survey outlines the level of support for many women’s health policy issues raised during the 2020 presidential campaign that may be priorities for the new presidential administration and Congress. The Biden-Harris Administration and new Congress may emphasize many women’s health issues in the coming years, but with a closely divided House and Senate it will be challenging to enact these policies, despite sizable public support for many of these them.
For an interactive tool to view cross-tabs by gender, party ID, and race/ethnicity, click on tab for cross-tabs.