Are Health Centers Facilitating Equitable Access to COVID-19 Vaccinations? A June 2021 Update.
Key Takeaways
Community health centers are a national network of safety net primary care providers and are a primary source of care for many low-income populations and communities of color. This updated analysis examines the extent to which COVID-19 vaccination efforts through community health centers are reaching people of color using data from the federal government’s weekly Health Center COVID-19 Survey for the weeks of January 8 through May 21, 2021 (the latest data available). Key findings include:
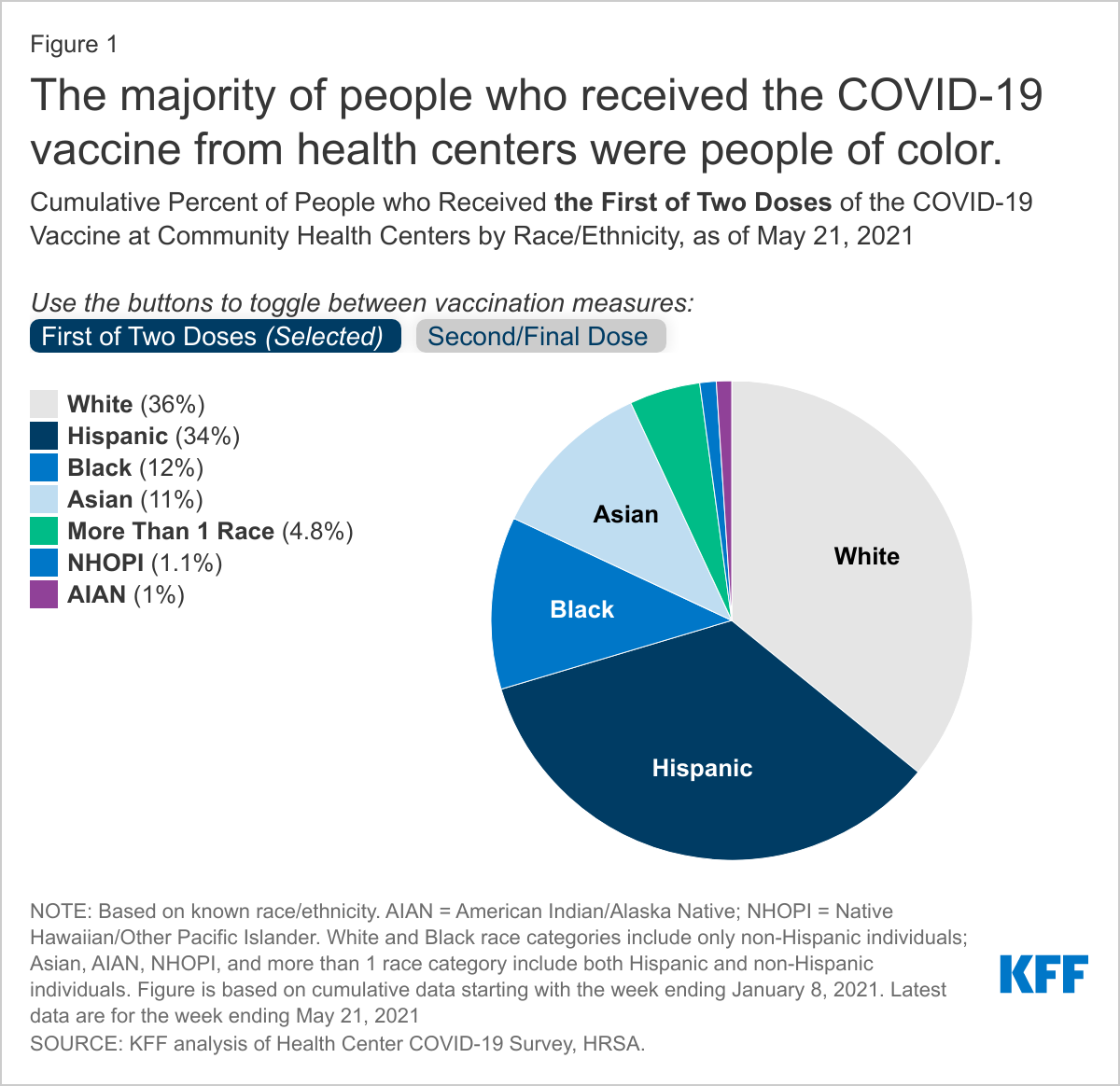
- Over the period of January 8 through May 21, 2021, people of color made up nearly two-thirds (64%) of people receiving the first dose and 61% of people receiving the second/final dose of the vaccine at health centers.
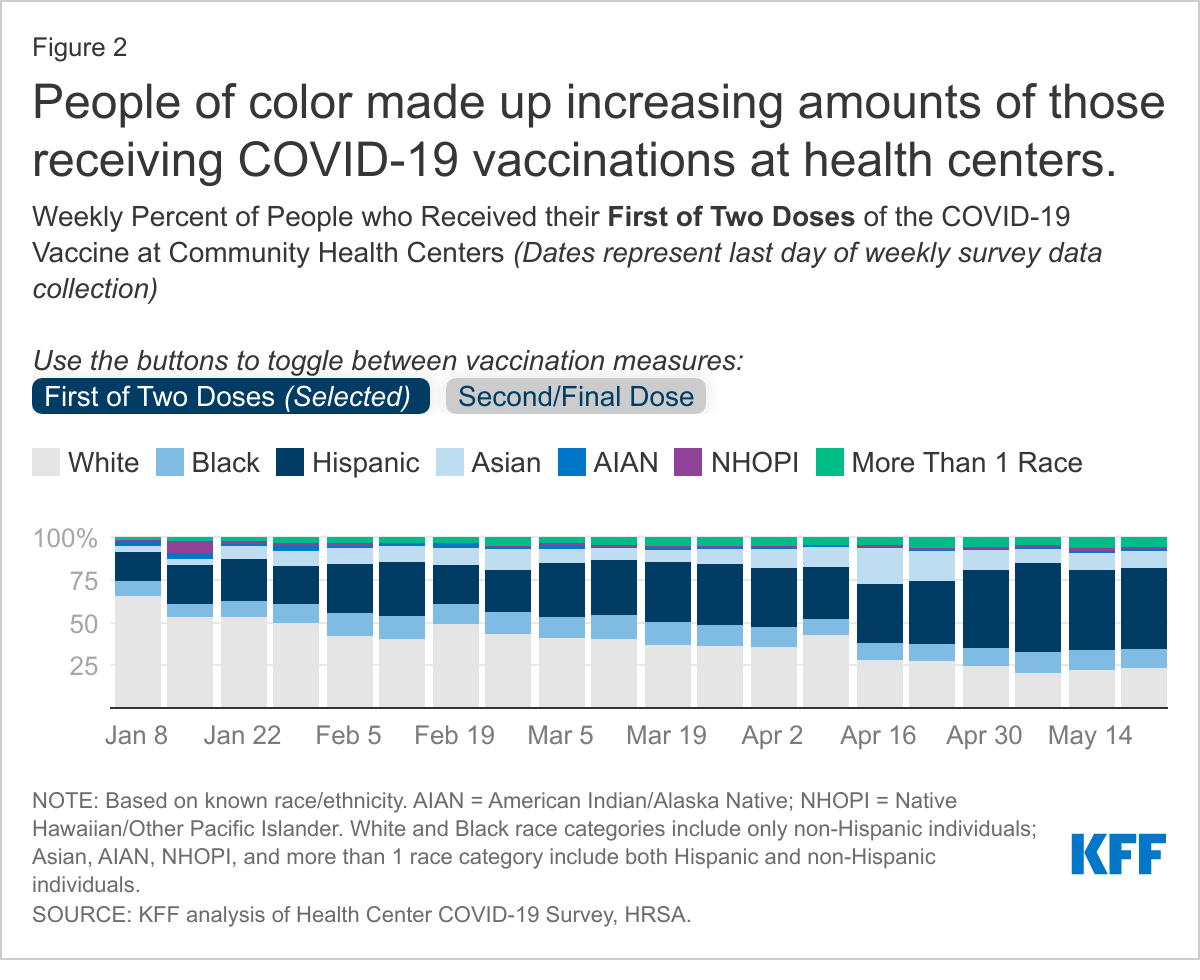
- Weekly data show that the share of first doses administered to people color at health centers has grown from 34% in early January to 77% in the week ending May 21. Growth was especially rapid among Hispanic people who made up 17% of first doses administered in the first week of January, growing to a high of 52% in the week of May 7.
- People of color represent greater shares of vaccinations at health centers compared to their shares of vaccinations nationally based on data reported by the CDC, especially for Hispanic people. To date, 34% of total first doses administered at health centers have gone to Hispanic people, over two times higher than their share of people who have received one or more doses nationally (14%).
- Health centers appear to be vaccinating people of color at similar or higher rates than their shares of the U.S. population, but data suggest there remain opportunities for health centers to reach more Black patients. The shares of people vaccinated at health centers who were Black, Hispanic, and Asian matched or exceeded their shares of the U.S. population. However, Black peoples’ share of health center vaccinations was lower than their share of the health center patient population for both first and second/final doses administered.
Introduction
Current data suggest significant racial disparities in COVID-19 vaccinations, with higher vaccination rates among White people compared to Hispanic and Black people as of late May, based on available state-reported data. The Biden administration has identified equity as a key priority in its national COVID-19 response strategy. One action the administration is pursuing to advance equity in vaccinations is to increase distribution through community health centers. Health centers are a primary source of care for low-income populations and people of color and served nearly 30 million patients in 2019. Given health centers’ focus on underserved communities and their long-standing role in encouraging and providing immunizations, health centers are generally seen as trusted providers in their communities, especially among people of color.
The Health Center COVID-19 Vaccine Program began allocating vaccines directly to an initial group of 250 health centers in mid-February. The early participants in the program serve large volumes of specific high-need populations that may require more resource-intensive vaccination efforts, such as agricultural workers, people living in or near public housing, individuals with limited English proficiency, and people experiencing homelessness. By April 7, 2021, the program expanded to include all health centers nationwide (roughly 1,400 health center organizations), with participation phasing in over several weeks. Although roughly 800 health centers were participating as of May 24, the majority of vaccinations administered by health centers so far have been supplied by states and local jurisdictions, which are also working with health centers to speed up equitable distribution of the vaccine. Between the doses supplied through the Health Center COVID-19 Vaccination Program and through state and local partnerships, health centers had administered more than 10 million doses of the COVID-19 vaccine by May 2021.
This analysis examines the extent to which vaccination efforts through community health centers are reaching people of color based on data from weekly surveys of health centers administered by the Health Resources and Services Administration (HRSA). We use cumulative weekly data starting January 8, 2021 (when health centers began reporting vaccinations in the survey) and ending May 21 (the most recent data available). We also provide information on first doses administered and second/final doses administered. Notably, the Johnson & Johnson vaccine is only reported as the second/final dose administered in the weekly survey, as it is completed in a single dose. Additionally, this analysis compares community health center survey data to national vaccination data reported by the CDC, total population data, and total community health center patient population data. (See the methods section for more information about the data underlying this analysis.)
Key Findings
Among those with known race/ethnicity information, people of color made up the majority of people who received vaccinations at community health centers between January 8 and May 21, including 64% of people receiving the first dose and 61% of people receiving the second/final dose of the vaccine. Hispanic people made up 34% of first doses and 32% of second/final doses administered by health centers, followed by Black people (12% and 11% of first and second/final doses, respectively), and Asian people (11% for both first and second/final doses). People identifying with more than one race, as well as American Indian and Alaska Native (AIAN) and Native Hawaiian and Other Pacific Islander (NHOPI) people each made up 5% or less of those receiving first and second/final doses (Figure 1). Race/ethnicity was unknown or not reported for about 16% of both first doses administered and second/final doses administered, resulting in gaps in the data. However, health center vaccination data are considerably more complete than national vaccinations reported by the CDC, which are missing race/ethnicity information for 43% of people receiving 1 or more vaccinations and 39% of people who are fully vaccinated as of May 25, 2021.
Weekly data show that the share of first doses administered to people of color at health centers has grown from 34% in early January to 77% in the week ending May 21 (Figure 2). Growth in the share of people receiving the first dose who were Hispanic was especially rapid, growing from 17% of vaccinations to as much as 52% in the week ending May 7 (then declining slightly to 48% in mid-May). Asian people have also accounted for a growing share of the first doses administered, growing from 3% in early January to 10% in the week of May 21. Black people have experienced a modest increase in their share of first doses, growing from 9% in early January to 11% in the week of May 21. Additionally, the number of vaccinations at health centers reported through the survey has increased since January, although vaccinations appear to have reached their peak in April and has since declined, similar to national trends. The number of vaccinations administered per health center responding to the survey has grown from 60 total doses per responding health center during the week of January 8 to peak at 980 during the week ending April 9. Data for most recent week ending May 21 shows 554 total doses per health center responding to the survey. While the rate of overall vaccinations at health centers has slowed since the peak in April, health centers appear to be focusing greater shares of vaccinations on communities color.
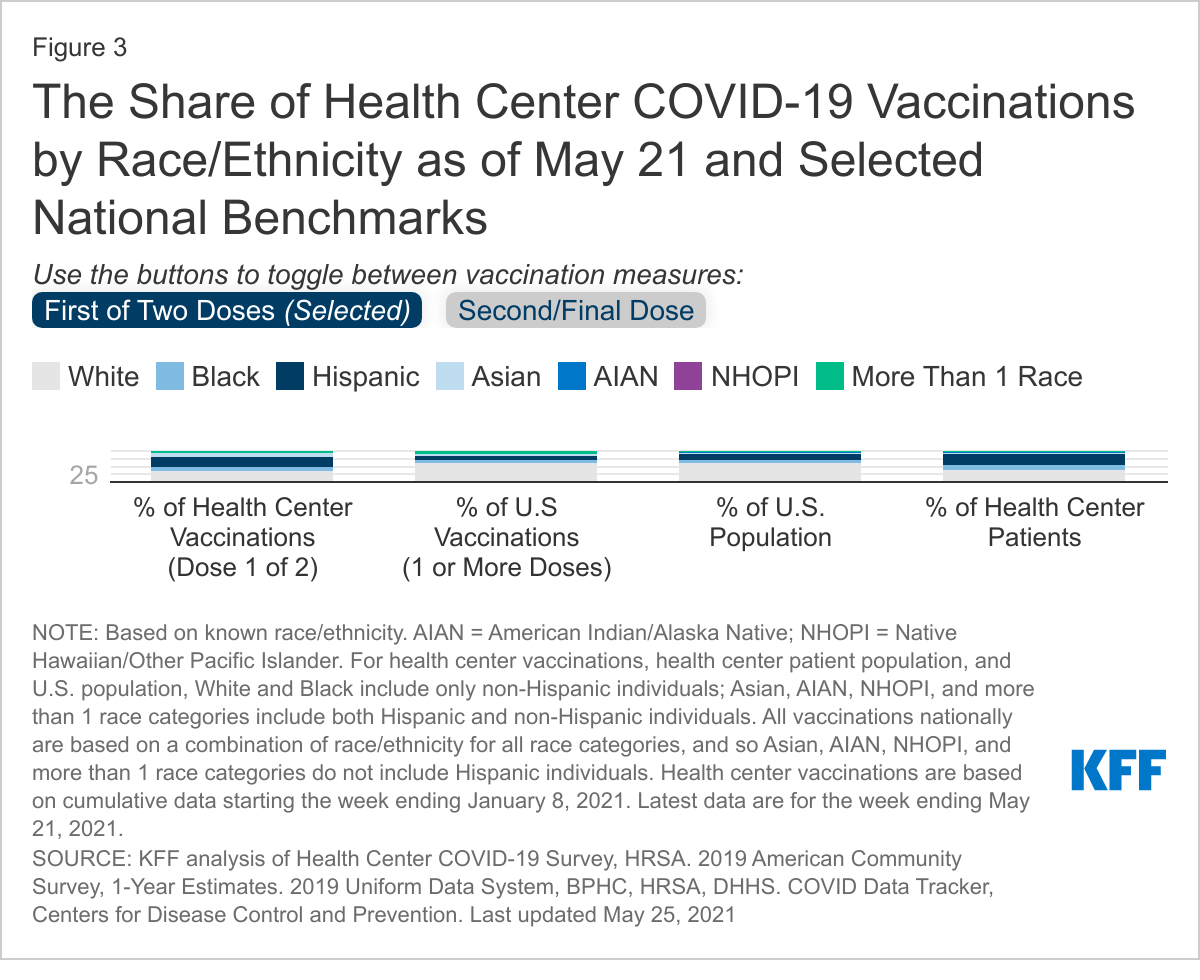
The data suggest that people of color represent greater shares of vaccinations at health centers compared to their shares of vaccinations nationally based on data reported by the CDC (Figure 3). For example, Hispanic people accounted for 34% of those who have received their first dose through a health center as of May 21, while they made up 14% of people who received 1 or more doses administered nationally as of May 25. Similarly, 12% of people who received their first dose through health centers were Black, while Black people made up 9% of those who received 1 or more doses nationally. Asian people also appear to be receiving vaccinations in greater shares at health centers compared to their share nationally, making up 11% of first doses administered at health centers vs 6% nationally. Overall findings were similar for second/final doses administered at health centers. However, the ability to draw strong conclusions from these comparisons is limited by differences between the data as well as gaps in the CDC data, including the high share of vaccinations with unknown race/ethnicity and a relatively high share of people reporting multiple or other race.
Health centers appear to be vaccinating people of color at similar or higher rates than their shares of the total population, but data suggest there remain opportunities for health centers to reach more Black patients (Figure 3). Health centers reached particularly large shares of Hispanic and Asian people relative to their shares of the total population, while the share of vaccinations that went to Black people was comparable to their share of the population. These vaccination patterns largely mirror health centers’ larger role serving patients of color, who made up 63% of patients in 2019. Although Hispanic and Asian peoples’ shares of vaccinations were generally similar to or greater than their shares of the health center patient population, the shares of first and second doses administered to Black people through health centers (12% and 11%, respectively) were lower than their shares of the patient population (19%), suggesting remaining opportunities for them to reach greater shares of Black people.
Looking Ahead
Health centers’ role in vaccine distribution is a major part of ongoing efforts to address the racial disparities in COVID-19 vaccinations that have emerged, especially for Hispanic people. The KFF COVID-19 Vaccine Monitor from April 2021 shows that 22% of vaccinated Hispanic adults and 10% of vaccinated Black adults reported getting their vaccine at a community health center. Reflecting their larger role serving and established trusted relationships with communities of color, evidence to date indicates that health centers are vaccinating larger shares of people of color compared to overall vaccination efforts. Health centers are also administering the vaccine to larger shares of people of color than their shares of the population, and there has been a substantial uptick in the share of people of color vaccinated at health centers over time. While people of color make up the majority of health center vaccinations, data suggest that there are further opportunities for health centers to reach more Black people, as the share of Black people vaccinated through health centers is still lower than their share of the health center patient population.
The growth in the share of people vaccinated in health centers who are people of color likely reflects several factors, including improvements in community outreach, logistics, and efforts to address access barriers faced by many people of color, as well as continued increases in people’s willingness to receive the vaccine over time. The Health Center COVID-19 Vaccine Program has increased the share of vaccinations distributed to people of color as well, although data are relatively limited on the program. According to federal officials, approximately 70% of the allocated doses have been administered to people of color.
Although health centers appear to be advancing equitable access to vaccinations, the number of vaccinations administered by health centers remains relatively small when scaled to the national total reported by the CDC. As of May 21, 2021, health centers had reported a cumulative 11.5 million doses (6.2 million first doses and 5.3 million second/final doses) administered in weekly surveys. However, this is likely an undercount, as between 56% and 81% of health centers have responded to weekly surveys, and those that do not respond are not included in the total vaccination counts for the week. Despite a likely undercount, health center vaccinations represent a fraction of the 288 million doses administered nationally as of May 21 and in comparison to the nearly 30 million health center patients in 2019. Still, health centers have focused the majority of their vaccinations within communities of color, especially in recent weeks, even as the number of vaccinations nationally have begun to slow since April 2021. Health centers’ continued involvement in vaccination and outreach efforts at the federal, state, and local levels will likely be a meaningful step in reaching people of color in greater numbers and advancing equity over the long term.
Methodology
This analysis primarily draws from the weekly Health Center COVID-19 Survey, administered by the Health Resources and Service Administration (HRSA). We rely on weekly data on the number of vaccinations per week by race/ethnicity starting with the January 8, 2021 survey through the May 21, 2021 survey. The National Association of Community Health Centers provided us with national totals of vaccinations by race/ethnicity for the week of January 22, which we were unable to access. We sum all weekly data over the period analyzed to represent cumulative totals.
Health center vaccinations are reported separately for first dose and second/final doses in this analysis. To report first doses administered, health centers are asked, “By race and ethnicity, how many patients have initiated (1st of 2 doses received) their COVID-19 immunization series in the last week?” For second/final doses administered, health centers are asked, “By race and ethnicity, how many patients have completed (2nd, or only, dose received) their COVID-19 immunization series in the last week?” In separate guidance, HRSA specified that health centers should report patients receiving doses administered as a one-dose vaccine series (i.e., the Johnson & Johnson vaccine) to be reported as the second/final dose. In the same guidance, HRSA also specified that health centers should include vaccinations at the health center, as well as among established patients receiving the vaccination elsewhere, if the health center has records of the immunization. When comparing changes in first and second/final doses over a period of weeks (e.g., Figure 2), the baseline week for second/final doses began later than that for first doses (the week of February 5 vs. the week of January 8) due to low numbers of second/final doses administered in January.
All findings reported are based on known race/ethnicity. For our calculations, both the “Unreported/Refused to Report Race and Ethnicity” as well as “Non-Hispanic/Latino Ethnicity Patients (Unreported/Refused to Report Race)” were defined as unknown race/ethnicity. “Hispanic/Latino Ethnicity Patients (Unreported/Refused to Report Race)” were categorized as ‘Hispanic’ individuals for our analysis.
The Health Center COVID-19 Survey reports race/ethnicity differently from most other data sources. White and Black categories only include non-Hispanic individuals, while Asian, AIAN, NHOPI, and more than one race include Hispanic and non-Hispanic individuals. When comparing to population estimates from the 2019 American Community Survey and the Uniform Data System, we adjusted race categories to match the Health Center COVID-19 Survey’s race/ethnicity categories. We did not adjust national vaccination tabulations by race/ethnicity from the CDC’s COVID Data Tracker.
Vaccination data by race/ethnicity from the CDC are based on administrative data reported to the CDC. However, the health center data are based on vaccinations from weekly surveys beginning in January 2021 with varying response rates. In addition to different data collection methods, it is possible that the health center survey data may also exclude some vaccinations in December 2020. Additionally, the CDC reports data for 1 or more vaccinations administered, while the health center data report first and second/final doses separately. Additionally, the health center first dose data do not include the Johnson & Johnson vaccine, which is reported as second/final dose.