KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Few People Switch Medicare Advantage Plans Each Year, Raising Questions About Whether Seniors Have the Tools and Information They Need To Compare Plans
A small share of Medicare Advantage enrollees switch plans each year, but those who do tend to pick plans with lower premiums and out-of-pocket limits than the plans they left behind, according to a new analysis by the Kaiser Family Foundation.
Eleven percent of enrollees voluntarily switched from one Medicare Advantage plan to another between 2013 and 2014, the analysis finds, while another four percent were forced to change because their Medicare Advantage plan exited the marketplace. Looked at another way, roughly 8 in 10 enrollees stayed in the same plan from one year to the next – a share that has remained fairly steady since 2007.
The relatively small share of Medicare Advantage enrollees to change plans – what some policy experts call “stickiness” – mirrors earlier research about Medicare prescription drug plan enrollees. (In contrast, 43 percent of Affordable Care Act marketplace enrollees switched plans between 2015 and 2016.)
Medicare Advantage enrollees who switch plans reap some benefits by shifting to plans with lower average premiums ($17.51 per month lower, on average) and lower out-of-pocket limits ($401 lower, on average) than they would have paid had they remained in the same plan.
These findings and previous research underscore the importance of tools and support to help beneficiaries choose plans that are most likely to meet their individual needs. Efforts that aim to make it easier for Medicare beneficiaries to evaluate their options could possibly increase competition among plans and improve beneficiaries’ satisfaction with their coverage.
The latest example of high and rising prescription drug prices to attract significant media and public attention relates to the EpiPen, an auto-injector containing the drug epinephrine which is used to reverse the effects of severe allergic reactions. Since Mylan acquired the EpiPen from Merck in 2007, the company has increased the list price for a pack of two EpiPens nearly 550%, from $94 in January 2007 to $609 in May 2016.1 While the EpiPen can be a lifesaver for children with serious food allergies, it is also used to treat life-threatening allergic reactions experienced by the older adults and people with disabilities who are covered by Medicare. The EpiPen is covered under Medicare Part D, which provides outpatient prescription drug coverage to beneficiaries who enroll in private drug plans.
This data note examines the effects of rising EpiPen prices on Medicare and beneficiaries. Using data from a 5% sample of Medicare prescription drug event claims from the Centers for Medicare & Medicaid Services (CMS) Chronic Conditions Data Warehouse, we analyze EpiPen spending, in the aggregate and per user, in Medicare Part D between 2007 (the year after the drug benefit took effect, and the year Mylan acquired the product) and 2014 (the most recent year of data available). Our analysis is restricted to Medicare beneficiaries who had at least one month of Part D enrollment during the year and at least one prescription drug event with a brand name of EpiPen 2-pak, EpiPen Jr. 2-pak, EpiPen, or EpiPen Jr. during the year. The analysis is based on retail claims data that do not take into account manufacturer discounts (rebates) to plans, which ranged from an average of 9.6% of total Part D spending in 2007 to 14.3% in 2014, according to Medicare’s actuaries.2 Part D rebate information submitted to CMS is confidential3 ; therefore, no data on rebates for the EpiPen to Part D plans is publicly available.
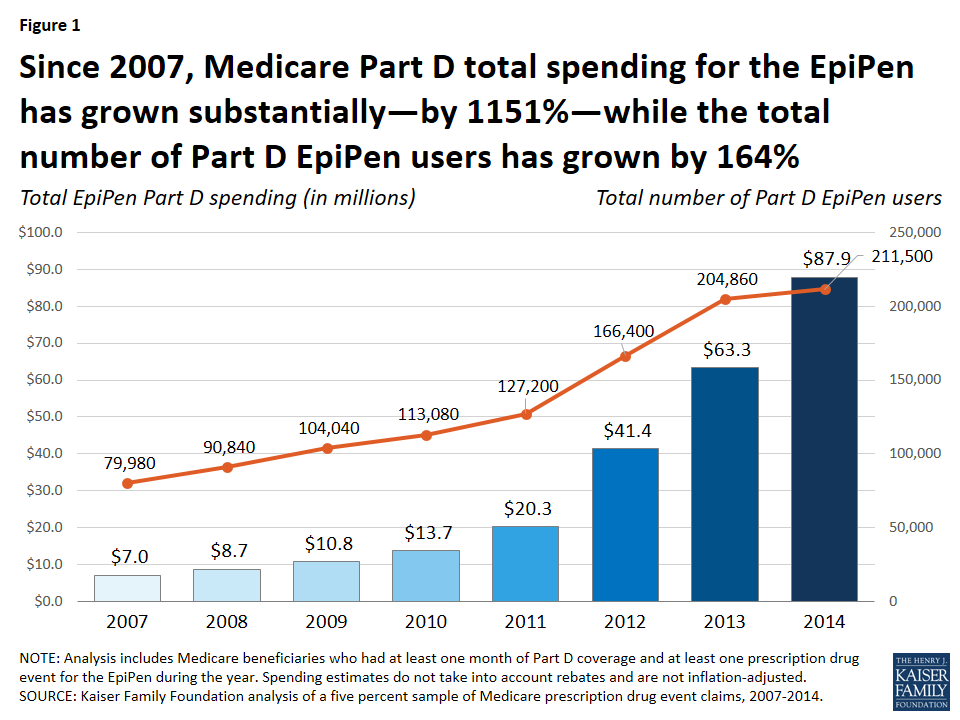
Total Medicare Part D spending on the EpiPen. According to our analysis, total Medicare Part D spending for the EpiPen increased from $7.0 million in 2007 to $87.9 million in 2014, an increase of 1151% (Figure 1).
Figure 1: Since 2007, Medicare Part D total spending for the EpiPen has grown substantially—by 1151%—while the total number of Part D EpiPen users has grown by 164%
While the total number of Part D enrollees using the EpiPen also increased over this time period—from nearly 80,000 users in 2007 to more than 211,000 in 2014—the increase was significantly lower in percentage terms (164%).
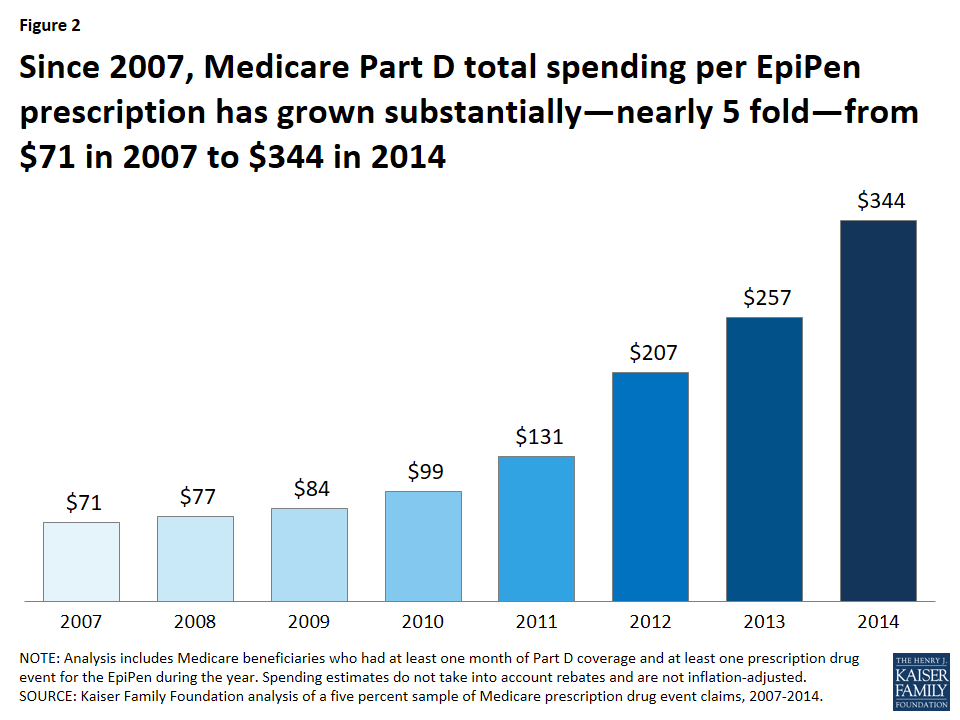
Over this same time period, average total Part D spending per EpiPen prescription increased nearly five-fold, from an average of $71 in 2007 to $344 in 2014 (a 383% increase) (Figure 2).
Figure 2: Since 2007, Medicare Part D total spending per EpiPen prescription has grown substantially—nearly 5 fold—from $71 in 2007 to $344 in 2014
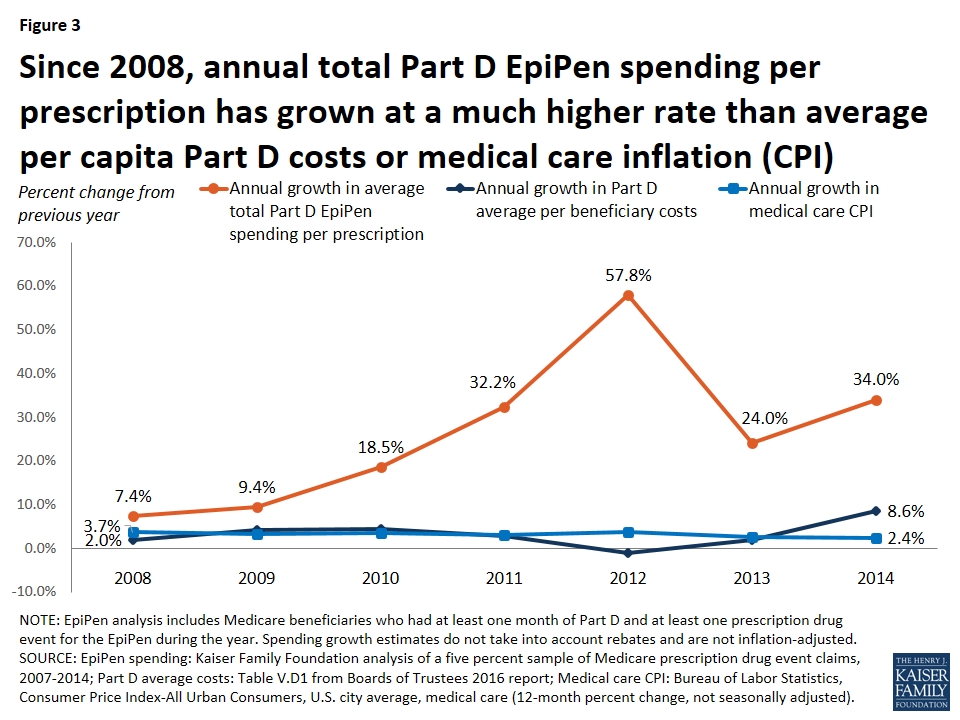
To put EpiPen spending increases in context, we compared annual growth in average total Part D spending per EpiPen prescription in each year from 2008 to 2014 to annual growth in average per capita costs for Part D overall and in medical price inflation (the Consumer Price Index, or CPI, for medical care). The annual rate of growth for total Part D EpiPen spending per prescription was significantly higher each year (Figure 3).
Figure 3: Since 2008, annual total Part D EpiPen spending per prescription has grown at a much higher rate than average per capita Part D costs or medical care inflation (CPI)
For example, in 2008, Part D spending per EpiPen prescription increased by 7.4%, more than 3.5 times greater than the increase in total Part D per capita spending (2.0%) and twice the rate of medical care price inflation (3.7%). In 2014, Part D spending per EpiPen prescription increased by 34.0%, four times the rate of increase in Part D per capita spending (8.6%) and 14 times larger than the 2.4% increase in medical care price inflation.
Out-of-pocket spending on the EpiPen by Medicare Part D enrollees. Since Medicare Part D plans cover a portion of enrollees’ total drug costs, beneficiaries in Part D plans pay less than the full retail cost of drugs covered by their plan, including the EpiPen. Still, average out-of-pocket spending by Part D enrollees for each EpiPen prescription nearly doubled between 2007 and 2014, from $30 to $56, among enrollees who do not receive Low-Income Subsidies (LIS) under Part D4(Table 1). In the aggregate, out-of-pocket spending by all Part D enrollees who used the EpiPen increased more than five-fold between 2007 and 2014, from $1.6 million to $8.5 million, reflecting both an increase in the number of users and price increases for the EpiPen.
Table 1: Medicare Part D Spending for the EpiPen, 2007-2014
Year
Number of EpiPen users
Number of EpiPen prescriptions1
Total EpiPen spending
Average total spending per EpiPen prescription
Total out-of-pocket spending on the EpiPen
Average out-of-pocket spending by non-LIS enrollees per EpiPen prescription 2
2007
79,980
98,579
$7,027,685
$71
$1,608,896
$30
2008
90,840
113,027
$8,653,183
$77
$1,979,054
$31
2009
104,040
128,624
$10,769,049
$84
$2,543,034
$36
2010
113,080
138,212
$13,713,744
$99
$3,000,749
$40
2011
127,200
154,460
$20,264,292
$131
$3,685,566
$42
2012
166,400
199,853
$41,379,681
$207
$5,831,017
$51
2013
204,860
246,725
$63,342,313
$257
$7,504,229
$51
2014
211,500
255,419
$87,892,967
$344
$8,481,497
$56
NOTE: LIS is Low-Income Subsidy. Analysis includes Medicare beneficiaries who had at least one month of Part D coverage and at least one prescription drug event for the EpiPen during the year. Total spending does not take into account rebates and is not inflation-adjusted. 1Standardized to a 30-day supply. 2Reflects out-of-pocket spending by Part D enrollees not receiving Low-Income Subsidies.SOURCE: Kaiser Family Foundation analysis of a 5% sample of Medicare prescription drug event claims, 2007-2014.
The impact of rising EpiPen prices since 2014. Because our analysis is based on data available only to 2014, our estimates do not reflect additional EpiPen price increases that have occurred since then. The list price of the EpiPen has increased (in nominal terms) from $349 in May 2014 to $609 in May 2016, a 74% increase. If total Part D spending per EpiPen prescription also increased by 74% between 2014 and 2016, Medicare Part D spending for the EpiPen would have increased from $344 per prescription in 2014 to $600 per prescription in 2016—more than an eight-fold increase since 2007.
Illustrating the potential effect of rebates. As noted above, Medicare does not disclose drug-specific rebates, and therefore we are unable to determine the extent to which our estimates of total Part D spending on the EpiPen might overstate actual plan costs for the EpiPen over this time period. To approximate the potential effect of rebates on total Part D spending, if we assume that all Part D plans had received for the EpiPen the average rebate reported by Medicare’s actuaries each year between 2007 and 2014, EpiPen spending would have increased from $6.4 million in 2007 (applying the 9.6% average rebate in 2007) to $75.3 million in 2014 (applying the 14.3% average rebate in 2014)—for an increase in total spending of nearly 1100%. This is similar to the 1151% increase based on total gross Medicare spending not accounting for rebates. In other words, even if total Part D spending for the EpiPen had been lower each year as a result of rebates, we might still expect to see a similar trend in the rate of Medicare Part D spending growth for the EpiPen, unless plans received significantly larger rebates over time. But it could also be the case that plans received relatively low rebates for the EpiPen, due to the lack of competition for this product—a situation that gives drug manufacturers less incentive to negotiate price discounts with insurers.
Implications. Although the total cost of the EpiPen to Medicare and beneficiaries may seem modest relative to the cost of more expensive specialty drugs and biologics, our analysis demonstrates that EpiPen price increases have translated into higher spending for Medicare Part D plans, enrollees, and the program overall. When drug manufacturers raise prices for their products and insurers’ costs increase as a result, these increases can translate into higher cost sharing and higher premiums for consumers. Rising prices for the EpiPen in recent years and the resulting significant increases in Medicare Part D spending illustrate why the cost of prescription drugs is an ongoing concern for consumers, public and private payers, and policy makers alike.
Juliette Cubanski and Tricia Neuman are with the Kaiser Family Foundation.Anthony Damico is an independent consultant.
Part D Low-Income Subsidies provide additional financial assistance for enrollees with low incomes and modest assets, by paying some or all of plan premiums and reducing prescription drug cost-sharing amounts. ↩︎
Each year, Medicare Advantage enrollees have the opportunity to change plans during an annual enrollment period. This opportunity is important because Medicare Advantage plans can make changes in their benefits, cost-sharing, provider networks, and premiums each year, and beneficiaries’ health needs may change from one year to the next. The open enrollment period allows enrollees to compare plans, stick with their current plan, switch to another plan, or shift to traditional Medicare. It is also the time when beneficiaries in traditional Medicare can switch to Medicare Advantage plans.
Little is known about the extent to which Medicare Advantage enrollees change plans during the annual open enrollment period. Prior research shows that roughly the same share of beneficiaries, 5 percent, shift between Medicare Advantage and traditional Medicare each year,1 that most enrollees tend to stay in a Medicare Advantage plan once in Medicare Advantage,2 and that switching rates from Medicare Advantage to traditional Medicare are higher among high-need, high-cost patients.3,4
This analysis focuses on enrollees in Medicare Advantage plans with prescription drug coverage (MA-PDs) who change plans when given the opportunity. It also analyzes the variation in the rate of plan switching by enrollee and plan characteristics and whether people who voluntarily switch plans tend to move to plans with lower premiums, lower out-of-pocket limits, or higher quality ratings. The analysis is based on a five percent sample of Medicare claims data merged with plan data from 2007 to 2014 (see Methods).
Issue Brief
Switching Rates
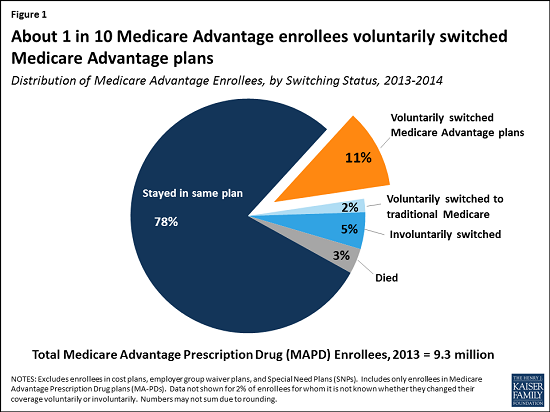
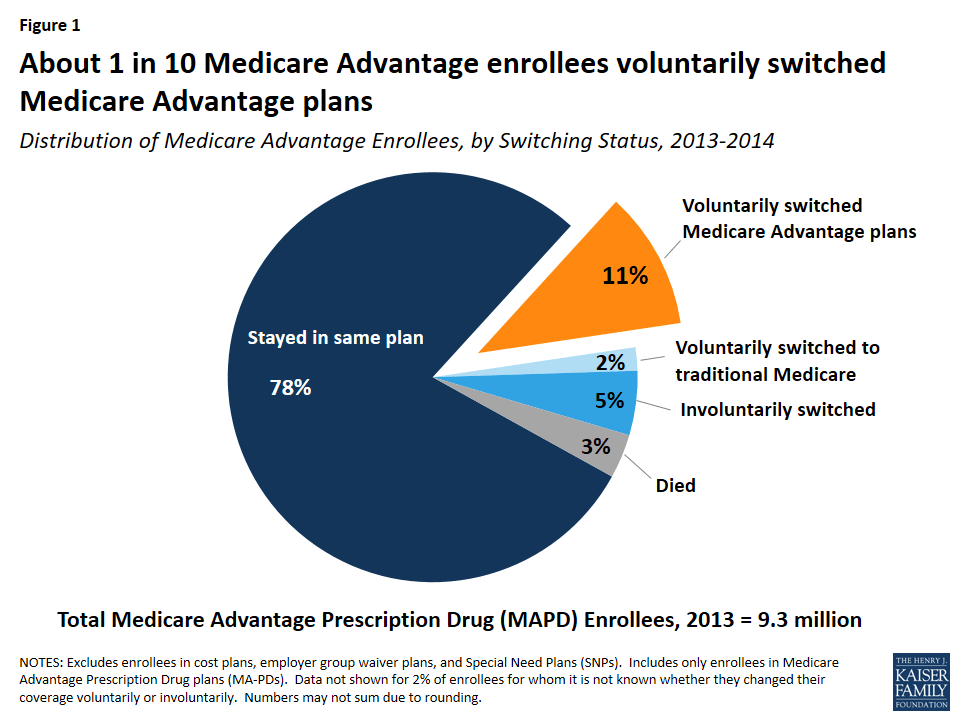
About one in ten Medicare Advantage plan enrollees (11 percent) in 2013 voluntarily switched to another plan in 2014 (Figure 1). Another two percent of enrollees voluntarily switched to traditional Medicare5 and another five percent were required to switch (involuntarily switched) plans because their plan exited the market.
Figure 1: About 1 in 10 Medicare Advantage enrollees voluntarily switched Medicare Advantage plans
Of the five percent of involuntary switchers, four percent switched to a different Medicare Advantage plan, and about one percent elected coverage under traditional Medicare. Another three percent of enrollees in 2013 died before the start of the 2014 calendar year. Overall, 78 percent of Medicare Advantage enrollees did not change their source of coverage between 2013 and 2014.
Switching Rates, by Year
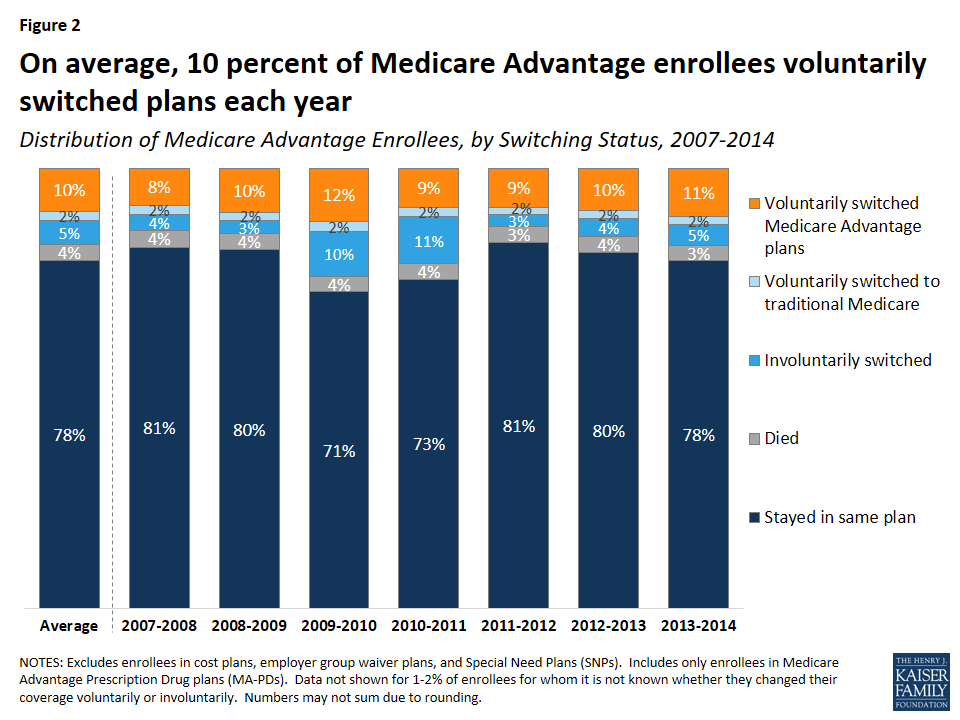
The share of Medicare Advantage enrollees switching plans has been virtually the same each year between 2007 and 2013, averaging 9 percent annually (Figure 2). The relatively constant rate of voluntary plan switching is noteworthy given the number of changes in Medicare Advantage policies and payments implemented during this time frame, including the establishment of new network requirements for private fee-for-service (PFFS) plans enacted as part of the Medicare Improvements for Patients and Providers Act (MIPPA) and implemented in 2011, as well as the reductions in federal payments to plans enacted as part of the Affordable Care Act of 2010.
Figure 2: On average, 10 percent of Medicare Advantage enrollees voluntarily switched plans each year
Voluntary switching rates were slightly higher between 2009 and 2010 and between 2013 and 2014 than in other years. The slight increase between 2009 and 2010 may have been due to PFFS plans encouraging their enrollees to switch to another plan offered by their firm in anticipation of terminating their PFFS plans in 2011 due to new provider network requirements for PFFS plans.6 Involuntary switching rates were also higher between 2009 and 2011.
Switching Rates, By Firm
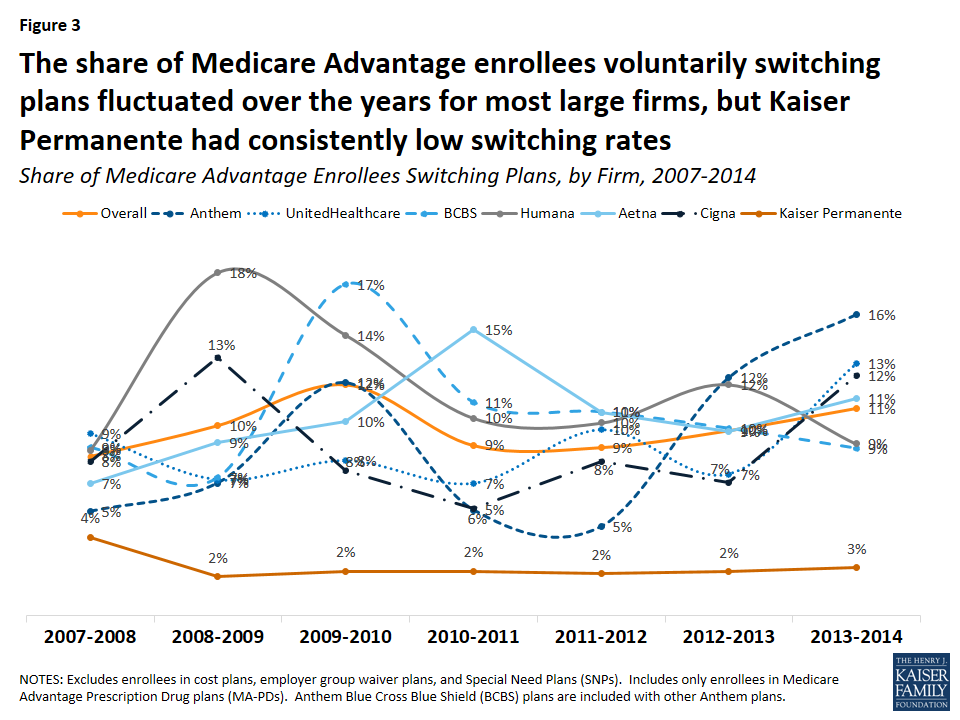
Switching rates among enrollees were not consistently higher or lower in one large firm compared to another, with the exception of plans offered by Kaiser Permanente, which had consistently low switching rates relative to all other firms (Figure 3). Switching rates by firm fluctuated over the years. Higher switching rates in some years may have been due to PFFS plans exiting markets, a larger share of people switching out of regional PPOs, or other firm-specific factors.
Figure 3: The share of Medicare Advantage enrollees voluntarily switching plans fluctuated over the years for most large firms, but Kaiser Permanente had consistently low switching rates
Between two percent and four percent of Kaiser Permanente enrollees switched Medicare Advantage plans between 2007 and 2014 – far lower than the overall average of ten percent. The low voluntary switching rate among enrollees in Kaiser Permanente plans could be partly due to its integrated delivery system, which would require enrollees to change doctors if they switched to a plan offered by another firm.
Comparison of Switching Rates Across Markets
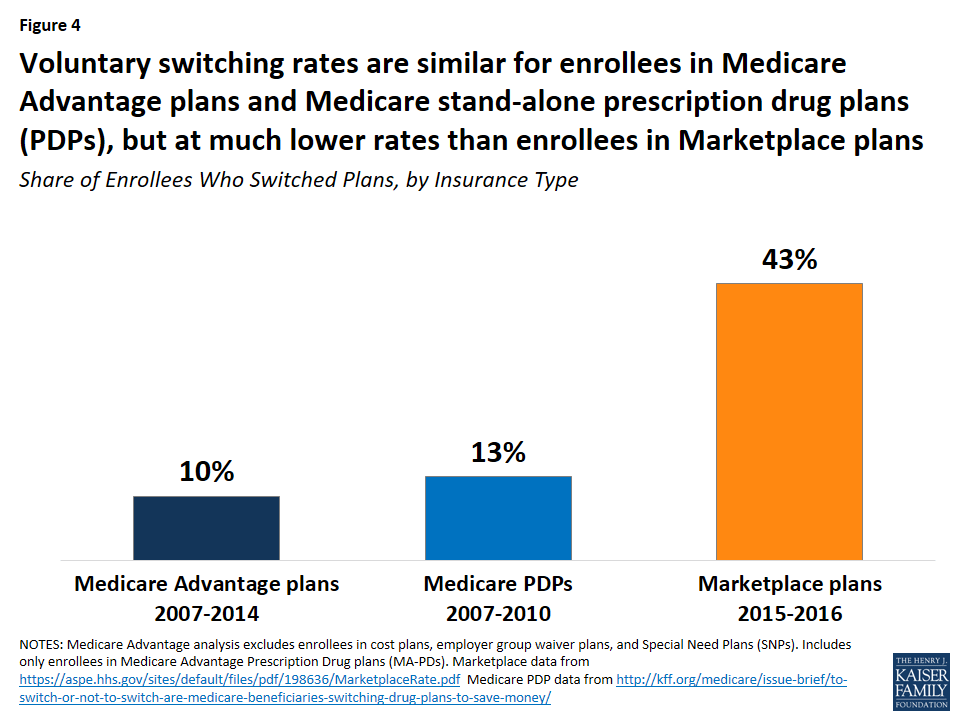
Medicare Advantage enrollees switch plans at similar rates as Medicare prescription drug plan (PDP) plan enrollees but at much lower rates than enrollees in ACA Marketplace plans (Figure 4). Between 2006 and 2010, 13 percent of Medicare PDP enrollees voluntarily switched plans (excluding enrollees receiving Low Income Subsidies),7 similar to the share of Medicare Advantage enrollees switching plans between 2007 and 2014. A much higher share of Marketplace enrollees – 43 percent – switched plans between 2015 and 2016.8 Even when all plan switchers, both voluntary and involuntary, are included, the rate (17 percent) is still much lower among Medicare Advantage than Marketplace enrollees.9
Figure 4: Voluntary switching rates are similar for enrollees in Medicare Advantage plans and Medicare stand-alone prescription drug plans (PDPs), but at much lower rates than enrollees in Marketplace plans
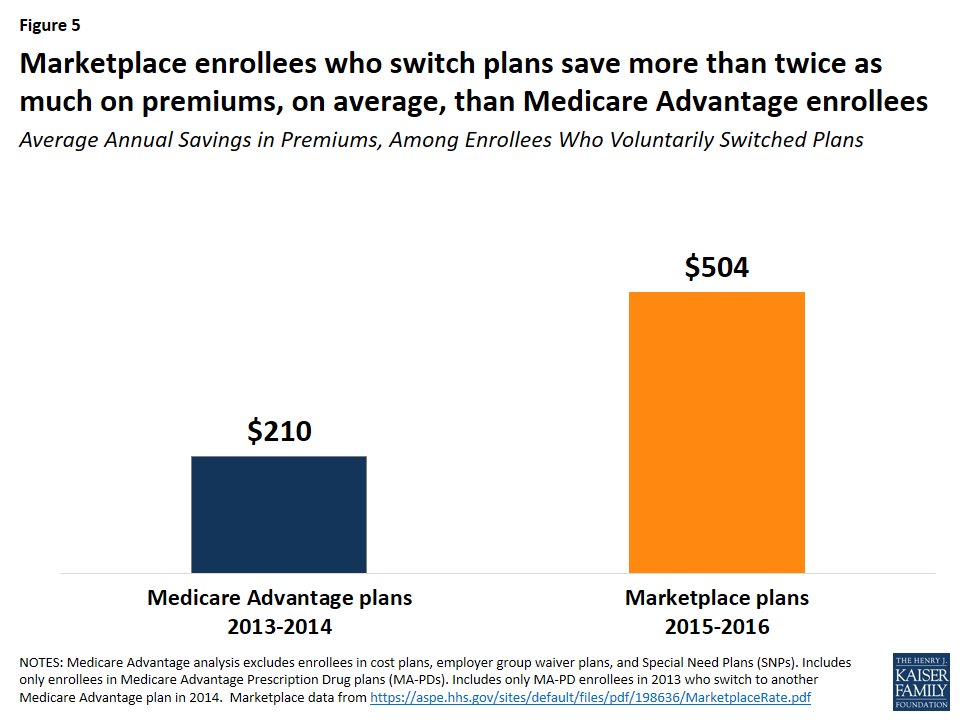
The lower switching rate among Medicare Advantage enrollees may be due to a number of factors. Marketplace enrollees save more in premiums when they switch plans than Medicare Advantage enrollees. Between 2015 and 2016, for example, Marketplace enrollees saved more than twice as much on annual premiums (saving $504 per year, on average) than Medicare Advantage enrollees saved by switching plans in 2014 (saving $210 per year, on average; Figure 5).10 Other factors influencing the difference in switching rates could include the anchoring of subsidies to the second lowest cost silver plan in the Marketplaces, more news coverage about the importance of switching Marketplace plans, greater volatility in premiums among the Marketplace plans, more technology savviness among younger Marketplace enrollees,11 and better tools available to help Marketplace enrollees shop for plans.
Figure 5: Marketplace enrollees who switch plans save more than twice as much on premiums, on average, than Medicare Advantage enrollees
Factors Associated with Voluntarily Switching Plans
Beneficiary Characteristics
Age
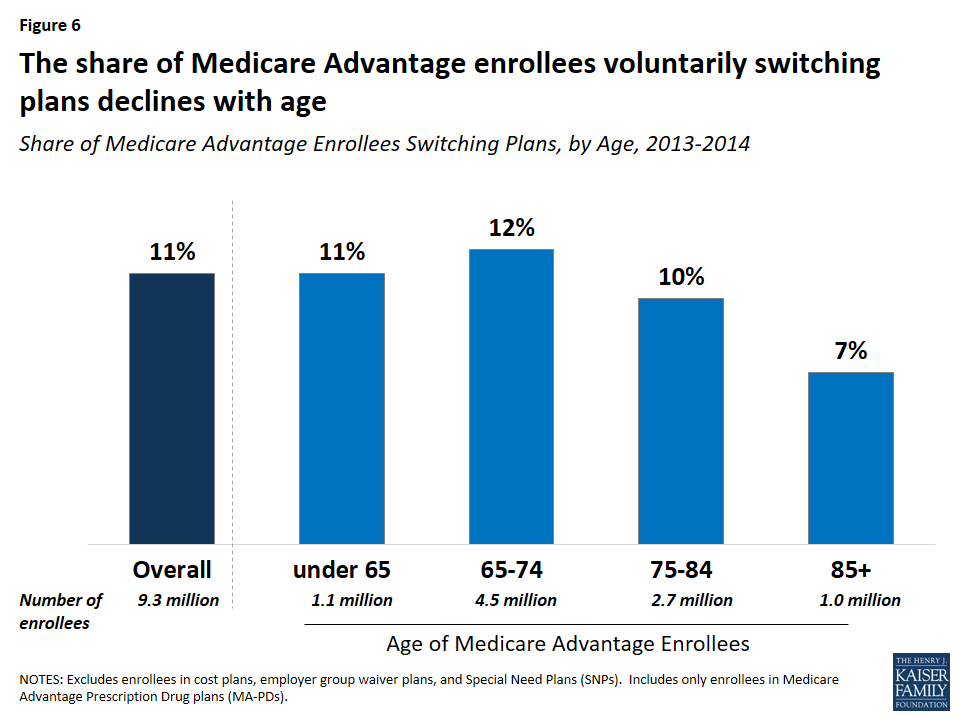
Switching rates among enrollees were somewhat higher among beneficiaries who were relatively young (ages 65 to 75). Plan switching declined with age, from 12 percent (ages 65-74) to 7 percent (ages 85 and older) between 2013 and 2014 (Figure 6).
Figure 6: The share of Medicare Advantage enrollees voluntarily switching plans declines with age
Dual Eligibles
A somewhat larger share of enrollees dually eligible for Medicare and Medicaid (13 percent) than other Medicare Advantage enrollees (10 percent) switched plans. One possible explanation for this is that dually eligible beneficiaries are permitted to switch plans at any time during the year, unlike other Medicare Advantage enrollees, while another possible explanation is that dually eligible beneficiaries feel their needs are not being met by their current plan. Other research has also noted that a larger share of dually eligible beneficiaries than other Medicare beneficiaries switch from Medicare Advantage to traditional Medicare.12
Switching rates were lower among dual eligibles in Medicare Advantage Special Needs Plans (SNPs), which are for beneficiaries who are either dually eligible for Medicare and Medicaid, require an institutional level of care, or have specific chronic conditions. Between 2013 and 2014, about nine percent of dually eligible beneficiaries in SNPs switched to another Medicare Advantage plan compared to 13 percent of dual eligibles in non-SNP Medicare Advantage plans and 11 percent of all dual eligibles in Medicare Advantage plans.13
Other Characteristics
Switching rates among Medicare Advantage enrollees did not vary by gender, nor were they consistently higher or lower than among enrollees in metropolitan or non-metropolitan areas.14 Due to data limitations, this analysis does not examine whether switching rates differed by enrollees’ health status, chronic conditions, or use of health care services.
Plan Characteristics
Premiums
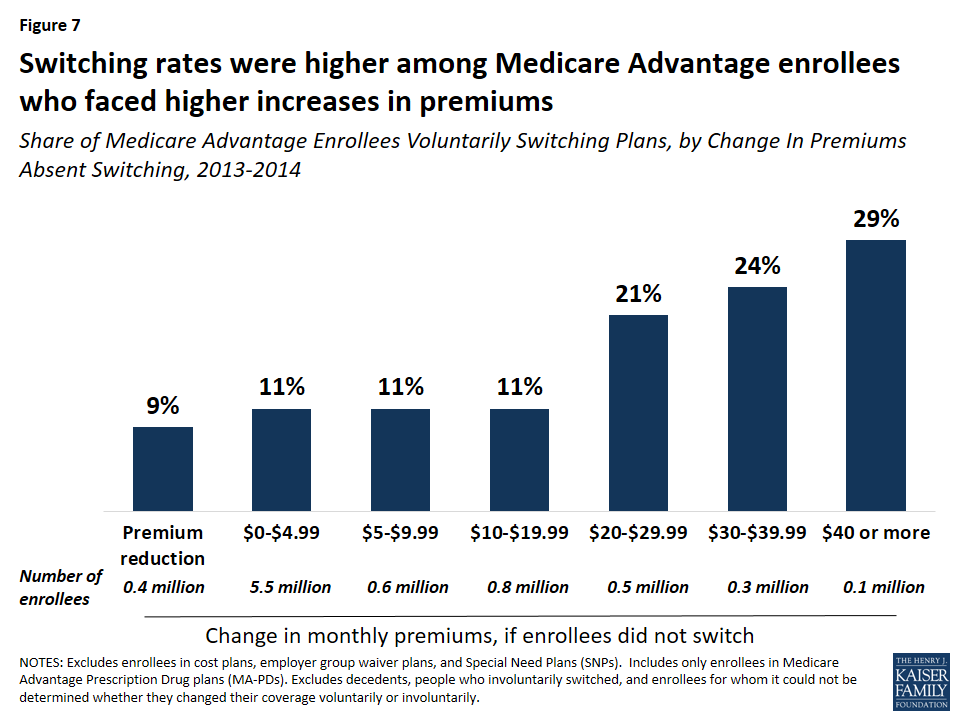
Switching rates were higher among Medicare Advantage enrollees who faced higher increases in premiums between 2013 and 2014. Among Medicare Advantage enrollees who faced a premium increase of less than $20, about 11 percent switched plans, but switching rates were much higher among enrollees who faced a premium increase of $20 or more and switching rates rose with premium increases (Figure 7). About one in five (21 percent) enrollees who faced a premium increase of $20 to $29 switched plans, one in four (24 percent)enrollees who faced a premium increase of $30 to $39 switched plans, and three in ten (29 percent) enrollees who faced a premium increase of $40 or more switched plans.15 Notably, nine percent of enrollees who faced a premium reduction switched plans – similar to the switching rates for enrollees with premium increases between $0 and $19.
Figure 7: Switching rates were higher among Medicare Advantage enrollees who faced higher increases in premiums
Most (79 percent) Medicare Advantage enrollees in 2013 faced premium increases of less than $10, which may have influenced their decision to stay in their plan. Conversely, 11 percent of Medicare Advantage enrollees faced premium increases of $20 or more, and more than 20 percent of these enrollees elected to change plans. As noted in more detail later, Medicare Advantage enrollees who switched plans tended to change to a plan with a lower premium, on average.
Quality Ratings
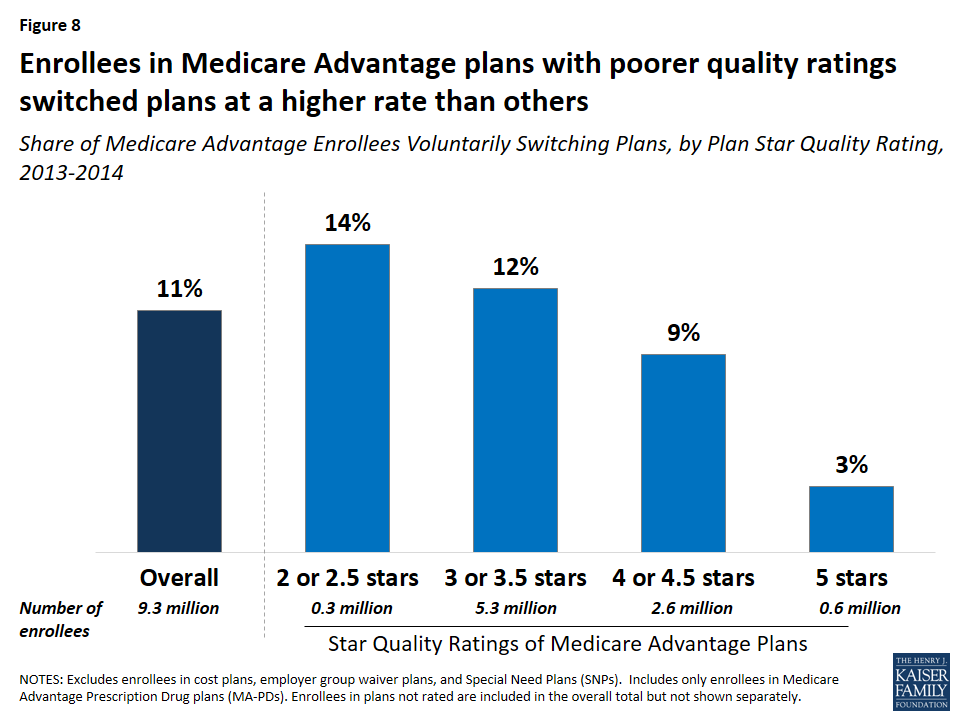
Medicare Advantage enrollees who voluntarily switched plans were disproportionately in plans with lower quality ratings. Between 2013 and 2014, one in seven (14 percent) enrollees in plans with 2 or 2.5 star quality ratings switched plans compared to one in ten (9 percent) enrollees in plans with 4 or 4.5 stars and only one in thirty (3 percent) enrollees in 5 star plans (Figure 8). These findings suggest that factors related to the star ratings may cause some beneficiaries to switch plans. However, as noted later, enrollees who switched plans ended up in a plan with only modestly higher quality ratings.
Figure 8: Enrollees in Medicare Advantage plans with poorer quality ratings switched plans at a higher rate than others
Plan Type
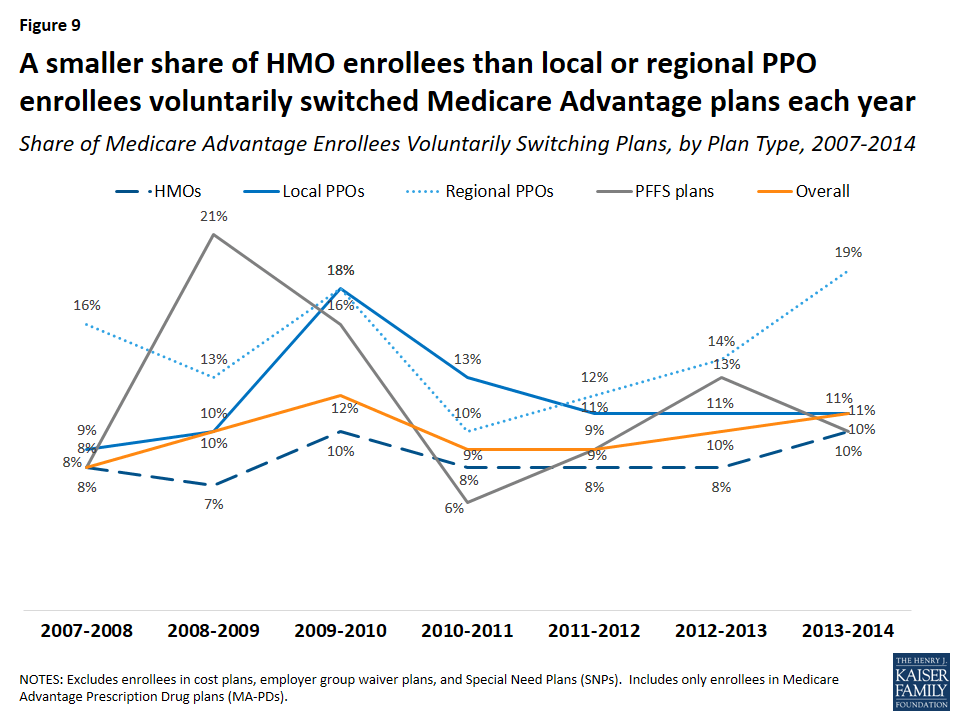
For most years between 2007 and 2014, a larger share of enrollees in regional PPOs than enrollees in other plan types voluntarily switched plans (Figure 9). In contrast, the switching rate was generally lowest among HMO enrollees.
Figure 9: A smaller share of HMO enrollees than local or regional PPO enrollees voluntarily switched Medicare Advantage plans each year
Age of Contract
Switching rates from enrollees in plans under relatively new contracts (beginning in 2006 or more recent) were higher than among enrollees in plans under older contracts. Between 2013 and 2014, nine percent of enrollees in contracts that began before 2000 switched plans compared to 15 percent of enrollees in contracts that began in 2006 or later. However, these differences are intertwined with the types of plans that were available in a given year. For example, regional PPOs, which have higher switching rates than other plan types, could not be offered prior to 2006. Similarly, most of the contracts prior to 2000 were for HMOs.
County Characteristics
Voluntary switching rates did not differ across the county characteristics that were examined, including the number of plans available or the Medicare Advantage payment quartile for the county.
Changes in Premiums, Out-of-Pocket Limits, Quality Ratings, Firms, and Plan Types
Premiums
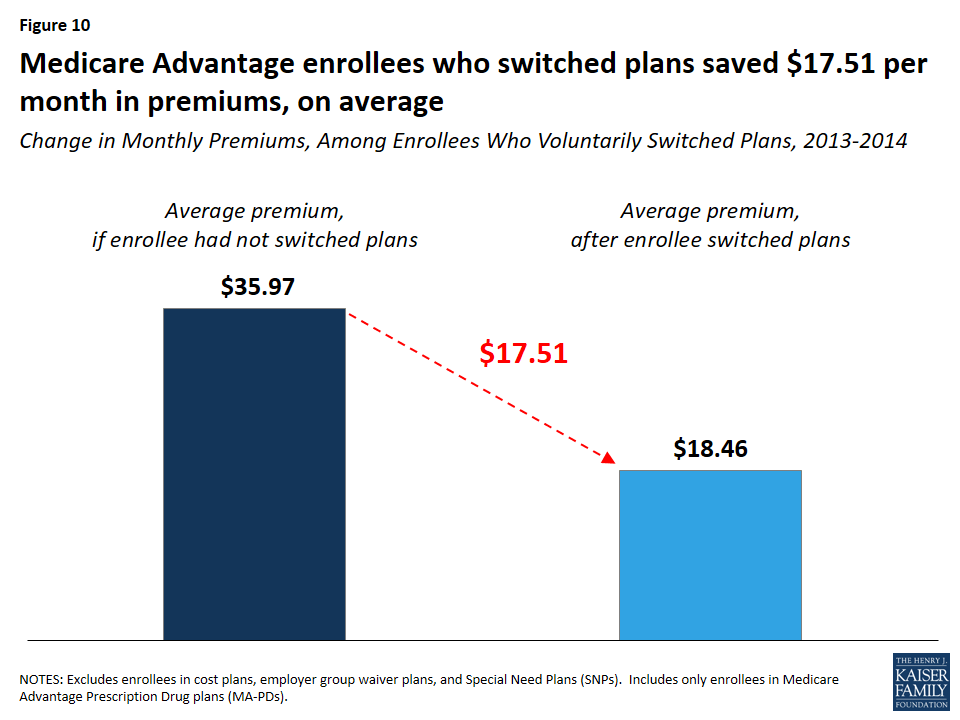
Enrollees who switched plans saved $15.87 per month in premiums, on average. Enrollees who switched plans would have paid $35.97 per month in premiums, on average, had they stayed in the same plan, but instead paid $18.46 per month, on average, after switching to another plan, saving $17.51 per month, on average (Figure 10). In contrast, enrollees who stayed in the same plan paid $4.26 more per month in premiums, on average. As noted earlier, switching rates were higher among Medicare Advantage enrollees who faced higher premium increases, particularly among enrollees with monthly premium increases of $20 or more.
Figure 10: Medicare Advantage enrollees who switched plans saved $17.51 per month in premiums, on average
Out-Of-Pocket Limits
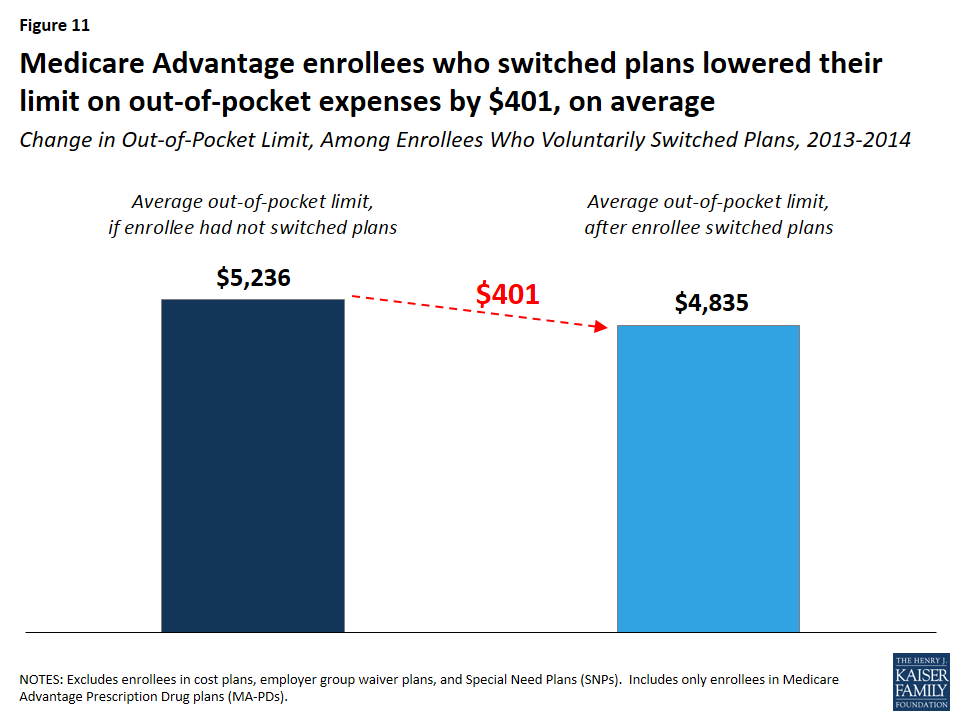
Enrollees who switched plans lowered their out-of-pocket limit by $401, on average (Figure 11). Medicare Advantage enrollees who switched plans between 2013 and 2014 would have seen their out-of-pocket spending limits rise by $728, from $4,508 to $5,236, on average, had they stayed in the same plan. By switching plans, enrollees got better catastrophic protection, with lower out-of-pocket spending limits ($4,835, on average), a difference of $401.
Figure 11: Medicare Advantage enrollees who switched plans lowered their limit on out-of-pocket expenses by $401, on average
Since 2011, all Medicare Advantage plans have been required to limit enrollees’ out-of-pocket expenses on Medicare Part A and B services to no more than $6,700 and are encouraged by the Centers for Medicare and Medicaid Services (CMS) to have limits of $3,400 or less.
Quality Ratings
Medicare Advantage enrollees who voluntarily switched plans changed to plans with slightly higher star ratings than their original plan, but the improvement was a modest 0.11 stars, on average. Between 2013 and 2014, Medicare Advantage enrollees who switched plans moved from a plan with 3.51 stars in 2014, on average, to a plan with 3.79 stars in 2014, on average –0.28 points higher than their prior plan. Had they stayed in the same plan, they would have seen their plan’s rating increase 0.17 points, on average, the same as the increase in quality ratings for enrollees who did not switch plans.
Firm and Plan Type
Among enrollees who voluntarily switched plans between 2013 and 2014, seven in 10 (71 percent) switched to a plan offered by a different firm (Table 1). Among enrollees who switched to a different firm, most chose a plan of the same type as their original plan. The fact that most people who switched plans moved to a plan offered by a different firm could be an indication that brand loyalty was not a strong factor in their plan choice.
Table 1: Share of Medicare Advantage Enrollees Switching Plans, by Differences in Firm and Plan Type
Same Firm
Different Firm
Total
Same Plan Type
18%
44%
62%
Different Plan Type
11%
27%
38%
Total
29%
71%
100%
Most (62 percent) Medicare Advantage enrollees who voluntarily switched plans changed to a plan of the same type as their original plan, even if from a different firm. Yet, most of the loyalty to plan type was among the HMO enrollees. The majority of HMO enrollees who switched plans shifted to another HMO (81 percent), while a majority of local PPO, regional PPO, and PFFS enrollees who switched plans changed to a different type of Medicare Advantage plan between 2013 and 2014.
Discussion
Relatively few Medicare Advantage enrollees, roughly one in ten, voluntarily switch from one MA-PD to another MA-PD each year, suggesting that plan switching among seniors is more the exception than norm. The takeaway from this analysis for beneficiaries is not entirely clear. On the one hand, our analysis shows some price sensitivity among Medicare Advantage enrollees: switching rates were higher among the minority of enrollees with relatively big premium increases. On the other hand, the findings confirm that the vast majority of enrollees do not change plans, and that plan “stickiness” may come at a cost, in terms of higher premiums and higher out-of-pocket spending limits.
Enrollees may be sticking with their plan for a number of reasons. They may be satisfied with their coverage. They may decide they would rather pay a bit more in premiums to avoid the hassle and time involved with making a change, particularly because most face a premium increase of less than $10 on average, in 2014. In focus groups, seniors have said that they appreciate the opportunity to change plans but often feel that the differences across plans are not important enough to warrant the time and effort it takes to compare and change plans.16 Some enrollees may place a higher value on other factors, such as having access to specific doctors or the comfort of sticking with a plan that is familiar. They may find that the information they need to compare plans is not readily available or that the process of comparing premiums, benefits, and provider networks across plans is too tedious.
For plans, the relatively high enrollee retention rate could strengthen incentives to keep their enrollees relatively healthy with low medical costs over the course of many years. However, it could also send a signal to plans that the risk of losing enrollees to a competitor is low as long as they do not drastically increase enrollees’ costs or disrupt their care arrangements.
For policymakers, these findings underscore the importance of tools and other support to help beneficiaries choose plans that are most likely to meet their individual needs. For instance, the Medicare Plan Finder could be improved to allow beneficiaries to more easily compare provider networks, cost-sharing, and benefits. Additionally, support could be strengthened for counselors and others who help Medicare beneficiaries with these increasingly complex decisions. Efforts that aim to make it easier for Medicare beneficiaries to evaluate their options could increase competition among plans and improve beneficiaries’ satisfaction with their coverage. The fact that most Medicare Advantage enrollees are not changing plans may not be cause for concern, but it does raise questions about whether the Medicare Advantage market is working as well as it could for consumers, especially those who are relatively old or with significant health care needs.
Methods
This analysis focuses on enrollees in Medicare Advantage Prescription Drug plans (MA-PDs) who switched plans when they had the option of remaining in the same plan (voluntary switchers) rather than Medicare Advantage enrollees who had no choice but to switch because their plan exited the market (involuntary switchers) or beneficiaries who switched from Medicare Advantage to traditional Medicare. The brief uses claims data from a 5 percent sample of Medicare beneficiaries from the Master Beneficiary Summary Files of CMS’s Chronic Conditions Data Warehouse for 2007 through 2014, the latest year of data available. The data was used in conjunction with the Medicare Advantage landscape file, Medicare Advantage crosswalk file, and Medicare Advantage enrollment file for each year. Some plans that were in the claims data and the Medicare Advantage landscape file were not in the Medicare Advantage crosswalk file, thus it could not be determined for a small share of Medicare Advantage enrollees (1-2 percent, depending on the year) whether they switched plans voluntarily or were forced to switch plans because their plan withdrew from the market (involuntary switching). The analysis excluded 4.96 million Medicare Advantage enrollees in 2013 because they were in plans that are not available for general enrollment (employer group waiver plans, Special Needs Plans, and demonstrations), in plans that are structured differently from Medicare Advantage plans (cost plans), or in plans that did not offer prescription drug coverage and are not marketed for general enrollment.
Gretchen Jacobson and Tricia Neuman are with the Kaiser Family Foundation. Anthony Damico is an independent consultant.
The authors appreciate the helpful review and comments that Marsha Gold provided on this paper.
Endnotes
Jacobson, Gretchen A., Patricia Neuman, and Anthony Damico, “At Least Half Of New Medicare Advantage Enrollees Had Switched From Traditional Medicare During 2006-11,” Health Affairs (Milwood), 34(1): 148-55, January 2015. ↩︎
Riley, Gerald F., “Impact of Continued Biased Disenrollment from the Medicare Advantage Program to Fee-for-Service” Medicare & Medicaid Research Review 2(4): E1-E16, 2012. Available at: https://www.cms.gov/mmrr/Downloads/MMRR2012_002_04_A08.pdf. ↩︎
McWilliams, J. Michael, John Hsu, and Joseph P. Newhouse. “New Risk-Adjustment System Was Associated with Reduced Favorable Selection in Medicare Advantage.” Health Affairs (Milwood) 31(12): 2630-2640, December 2012. Available at: http://content.healthaffairs.org/content/31/12/2630.full.pdf+html. ↩︎
Newhouse, Joseph P., Mary Price, Jie Huang, J. Michael McWilliams, and John Hsu. “Steps to Reduce Favorable Risk Selection in Medicare Advantage Largely Succeeded, Boding Well for Health Insurance Exchanges.” Health Affairs (Milwood), 31(12): 2618-2628, December 2012. Available at: http://content.healthaffairs.org/content/31/12/2618.full.pdf+html. ↩︎
A prior analysis found a higher rate of switching between Medicare Advantage and traditional Medicare. The rate is somewhat lower in this analysis because it excludes beneficiaries enrolled in Medicare Advantage plans that did not offer prescription drug coverage, employer group waiver plans, and Special Needs Plans (n=4.78 million beneficiaries in 2013). In total, 4.78 million beneficiaries who would have been included in the other analysis were excluded from this analysis for 2013. For the other analysis, see Jacobson, Gretchen A., Patricia Neuman, and Anthony Damico, “At Least Half Of New Medicare Advantage Enrollees Had Switched From Traditional Medicare During 2006-11,” Health Affairs (Milwood), 34(1): 148-55, January 2015. ↩︎
The rates of plan switching in the Federal Employees Health Benefits (FEHB) Program was 12 percent between 2000 and 2001. See Atherly, Adam, Curtis Florence, and Kenneth E. Thorpe. “Health Plan Switching Among Members of the Federal Employees Health Benefits Program.” Inquiry, 42: 255-265, Fall 2005. Available at: http://inq.sagepub.com/content/42/3/255.full.pdf. Approximately 6 percent of CalPERS members switched health plans between 2014 and 2015, which was higher than previous years. See CalPERS Pension and Health Benefits Committee. “Health Open Enrollment Results.” February 18, 2015. Available at: https://www.calpers.ca.gov/docs/board-agendas/201502/pension/item-10.pdf. ↩︎
Levine, David M., Stuart R. Lipsitz, and Jeffrey A. Linder. “Trends in Seniors’ Use of Digital Health Technology in the United States, 2011-2014.” JAMA, August 2016. Available at: http://jama.jamanetwork.com/article.aspx?articleid=2540389. ↩︎
Jacobson, Gretchen A., Patricia Neuman, and Anthony Damico, “At Least Half Of New Medicare Advantage Enrollees Had Switched From Traditional Medicare During 2006-11,” Health Affairs (Milwood), 34(1): 148-55, January 2015. ↩︎
While most SNP enrollees are dual eligibles, not all dually eligible beneficiaries who are enrolled in Medicare Advantage plans are in SNPs: about 1.2 million dual eligibles were enrolled in SNPs and about 1.1 million dual eligibles were enrolled in other Medicare Advantage plans in 2013. ↩︎
Notably, a larger share of enrollees in non-metropolitan areas (8 percent) than metropolitan areas (4 percent) were forced to switch plans (involuntary switching) because their plan exited the market between 2013 and 2014. This difference in involuntary switching rates was consistent across all years of this study. ↩︎
For another example and discussion of price elasticity in plan choice, see Buchmueller, Thomas C. and Paul J. Feldstein. “The Effect of Price on Switching Among Health Plans.” Journal of Health Economics, 16(2): 231-247, April 1997. ↩︎
The latest Kaiser Family Foundation/CNN partnership poll explores the views and experiences of white Americans without college degrees (a group defined in this survey as “working-class whites”), including how they feel about their own lives and the direction of the country, their attitudes towards government, their economic priorities, feelings about immigration and increasing racial and ethnic diversity, and personal experiences with employment and finances. It also compares this group’s attitudes and experiences with those of whites with college degrees, as well as those of blacks and Hispanics without college degrees (working-class blacks and Hispanics). Finally, the survey explores the views of different subgroups within the white working class, including variations by partisanship, age, income, region of the country, and religious identification.
A new Kaiser Family Foundation survey of states’ Medicaid family planning policies under fee-for-service finds wide coverage of most prescription contraceptives among 40 states and the District of Columbia (DC), but variable coverage of emergency contraceptives and other family planning-related services. It is the first published report on state coverage of family planning benefits since the passage of the Affordable Care Act (ACA).
The states surveyed all cover daily oral contraceptives, and most also cover other prescription contraceptive methods such as injectable contraceptives, the diaphragm, the patch, and vaginal ring. Coverage of long-acting reversible contraceptives such as intra-uterine devices and implants is widespread across states that participated in the survey, and few states put limits or restrictions on these devices or their removal. Furthermore, many states are experimenting with a variety of payment policies for long-acting reversible contraception provided immediately after labor and delivery.
Medicaid coverage of the over-the-counter emergency contraception product Plan B and other over-the-counter contraceptives is more limited than prescription methods. At least one form of emergency contraceptive pills is covered through traditional Medicaid programs in all but three surveyed states, but the over-the-counter product Plan B is covered in fewer states than ella, which is a prescription form of emergency contraception. Coverage for other over-the-counter contraceptives is more limited than prescription methods: ten states do not cover condoms, spermicide, and sponges.
While virtually all states surveyed covered family planning-related services like contraceptive counseling, well women visits, and cervical and breast cancer screenings, fewer (35 out of 41) reported coverage for screenings for intimate partner violence. Only one state, Nebraska, covered fertility treatments for either women or men and this coverage was limited to infertility caused by medical issues.
The report, prepared by Health Management Associates and the Kaiser Family Foundation, features detailed data for 40 states and DC and looks at family planning benefits across full scope traditional Medicaid programs and Medicaid expansion under the Affordable Care Act (ACA), as well as limited scope Medicaid family planning programs.
Since 2006, Medicare beneficiaries have had access to prescription drug coverage offered by private plans, either stand-alone prescription drug plans (PDPs) or Medicare Advantage drug plans (MA-PD plans). Medicare drug plans (also referred to as Part D plans) receive payments from the government to provide Medicare-subsidized drug coverage to enrolled beneficiaries, who pay a monthly premium that varies by plan. The law that established Part D defined a standard drug benefit, but nearly all Part D plan sponsors offer plans with alternative designs that are equal in value, and plans may also offer an enhanced benefit. Part D plans also must meet certain other requirements, but vary in terms of premiums, benefit design, gap coverage, formularies, and pharmacy networks.
This chart collection presents findings on the Medicare Part D marketplace in 2016 and trends since 2006:
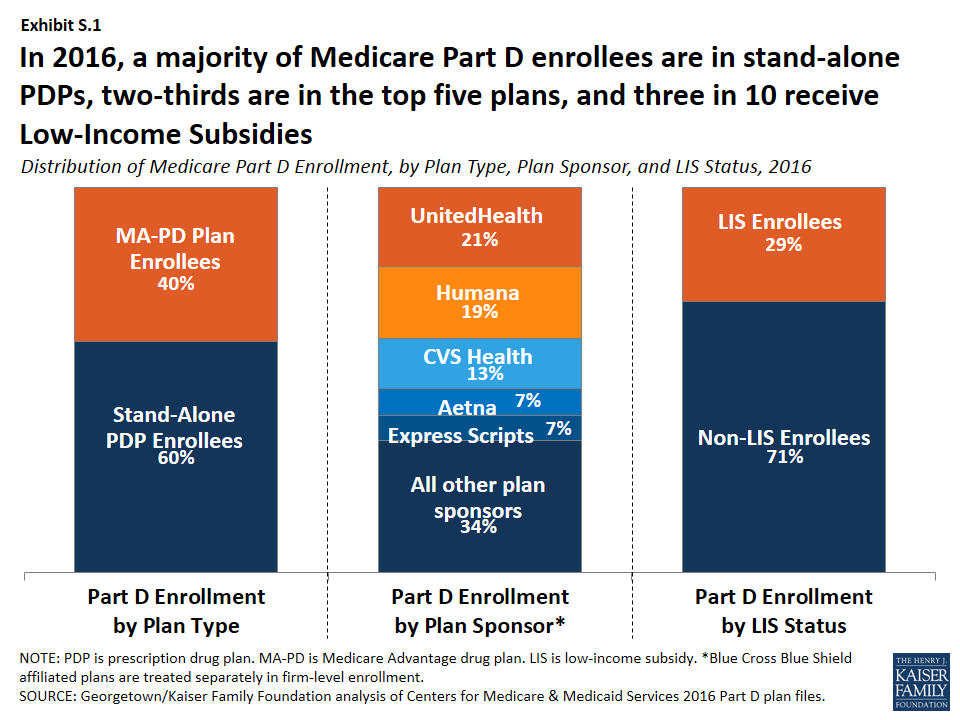
Nearly 41 million of the 57 million people on Medicare (71 percent) are enrolled in a Part D plan in 2016; most (60 percent) are in PDPs, but a rising share (40 percent in 2016, up from 28 percent in 2006) are in MA-PD plans (Exhibit S.1). More than half of Part D enrollees are in enhanced plans.
Exhibit S.1: Distribution of Medicare Part D Enrollment, by Plan Type, Plan Sponsor, and LIS Status, 2016
Nearly three in 10 Part D enrollees (29 percent, or about 12 million enrollees) are receiving extra help through the Part D Low-Income Subsidy (LIS) program that pays their drug plan premiums (if they enroll in a benchmark plan) and reduces their cost sharing.
Three firms—UnitedHealth, Humana, and CVS Health—account for over half (53 percent) of all Part D enrollment in 2016; if the Humana-Aetna merger goes through, the combined firm would account for 26 percent of Part D enrollment nationwide, without divestitures.
After several years of relatively low growth, average monthly PDP premiums increased by 6 percent in 2016 to $39.21 per month. However, monthly premiums for two of the most popular PDPs (AARP Rx Preferred and Humana Enhanced) increased by more than 20 percent in 2016. Premiums vary widely across regions and across plans, even among those of the same benefit type (basic or enhanced).
The average Medicare beneficiary has a choice of 26 PDPs and 16 MA-PD plans in 2016; by contrast, the average Part D enrollee receiving the LIS has a choice of seven premium-free benchmark PDPs, fewer than in any year since 2006.
One in eight Part D enrollees who receive the LIS—1.5 million beneficiaries—pay a monthly premium for Part D coverage, averaging $21 per month, even though premium-free PDPs are available in all regions; 45 percent of these 1.5 million enrollees pay $20 or more per month.
Almost all Part D enrollees are in plans with five cost-sharing tiers: two generic tiers, two brand tiers, and a specialty tier. PDPs typically charge coinsurance rather than copayments for brand-name drugs, and the use of tiered pharmacy networks is now the norm in PDPs. These trends have cost implications for beneficiaries, with greater unpredictably in out-of-pocket costs associated with coinsurance rates, but also the potential for savings if beneficiaries use drugs on preferred tiers or obtained from preferred cost-sharing pharmacies.
Key Findings: Section 1: Part D Enrollment And Plan Availability
Since 2006, the share of Medicare beneficiaries enrolled in a Part D plan has increased from 52 percent to 71 percent of all eligible Medicare beneficiaries.
Nearly 41 million Medicare beneficiaries, or 71 percent of all Medicare beneficiaries nationwide, are enrolled in Part D plans, including plans open to everyone and employer-only plans designed solely for retirees of a former employer 1. The percent of Medicare beneficiaries with Part D coverage in 2016 varies by state, from 56 percent in Alaska to 89 percent in North Dakota 2.
More than half (60 percent) of Part D enrollees are in PDPs, but enrollment in MA-PD plans has increased over time as a share of total Part D enrollment, from 28 percent in 2006 to 40 percent in 2016, roughly in line with overall growth in Medicare Advantage enrollment 3. In five states (Arizona, California, Florida, Hawaii, and Oregon), MA-PD plan enrollees account for over half of all Part D enrollees 4.
In 2016, 6.6 million Medicare beneficiaries are enrolled in employer-only Part D plans 5. This number has grown rapidly since a change in the tax status of the federal retiree drug subsidy (RDS), which is available to employers that provide drug benefits directly to their retirees, took effect in the 2013 tax year. Only 1.9 million beneficiaries (down from 7.2 million in 2006) have drug coverage from employers that receive the RDS.
In 2016, three Part D sponsors account for more than half of all Part D enrollees.
UnitedHealth, Humana, and CVS Health have enrolled half (52 percent) of all participants in Part D 6. This level of market concentration has increased modestly since 2006, but more so among PDPs. UnitedHealth and Humana have had large market shares since the program began, while enrollment in CVS Health has grown through acquisition of other plan sponsors 7.
If the acquisition of Humana by Aetna is approved, the combined firm would account for 26 percent of total Part D enrollment in 2016 nationwide, without divestitures. But in seven regions, the combined firm would have between 40 percent and 50 percent of total Part D enrollment. This acquisition, along with the proposed acquisition of Cigna by Anthem, would increase market concentration. Two thirds of all regions (23 of 34) would be considered highly concentrated, based on the Herfindahl index, with respect to PDP enrollees who are not receiving Low-Income Subsidies (LIS), up from 10 of 34 regions today 8. The market for LIS enrollment would also become highly concentrated in more regions (15 post-acquisitions versus four today).
The vast majority of PDP enrollees are in plans sponsored by firms participating in all or most all regions of the country 9. Firms offering plans in one or a few regions play a relatively small role in the program. MA-PD plans sponsored by local firms play a much larger role in that Part D market segment. Nationally, Blue Cross Blue Shield plans comprise 7 percent of PDP enrollment and 17 percent of MA-PD plan enrollment.
The ten largest sponsors of Part D plans account for 80 percent of all enrollment 10, and have varying shares of enrollees in PDPs versus MA-PD plans 11. UnitedHealth, by itself, has maintained the top position for all 10 years of the program, and in 2016 provides coverage to more than one in five PDP and MA-PD plan enrollees, but CVS Health has the most PDP enrollees for the first time in 2016. At the individual plan level, SilverScript Choice PDP has the most enrollees in 2016, a position previously held by AARP MedicareRx Preferred PDP 12. Since 2006, PDP enrollment has grown substantially in some of the largest plan sponsors; in others, enrollment growth has been relatively flat 13.
SilverScript Choice PDP has the most LIS PDP enrollees 14, while AARP MedicareRx Preferred PDP has the most non-LIS PDP enrollees 15.
The average Medicare beneficiary has a choice of 26 PDPs and 16 MA-PD plans in 2016.
The average number of PDPs available to people on Medicare has dropped from a high of 55 plans in 2007 to 26 plans in 2016, which are offered by 13 different firms 16. The number of MA-PD plans per beneficiary in 2016 increased slightly from 2015, from 15 to 16 plans. The total number of stand-alone PDPs available in 2016—886 PDPs—is lower than in any previous year 17.
Key Findings: Section 2: Part D Premiums
Average monthly PDP premiums rose in 2016 after being essentially flat since 2010; MA-PD plan premiums for Part D coverage only have risen modestly in the past few years.
PDP enrollees are in plans with an average monthly premium of $39.21 in 2016, up by 6 percent from 2015 1. MA-PD plan enrollees are in plans with an average monthly premium of $16.99 for Part D benefits, a lower amount due in part to the ability of firms offering MA-PD plans to use rebate dollars from Medicare payments for benefits covered under Parts A and B to lower their Part D premiums. The combined average Part D premium for PDP and MA-PD plan enrollees is $31.21 in 2016.
Premiums for enhanced PDPs grew more rapidly than premiums for basic plans from 2015 to 2016 (11 percent versus 4 percent) 2.
In 2016, just over half of MA-PD plan enrollees are in plans that charge no monthly premium for Part D coverage. Nearly half of PDP enrollees are in plans that charge less than $30 per month, but one in five are in plans charging at least $60 3.
Premiums for some of the most popular plans increased in 2016, while for others, premiums fell.
Monthly premiums for three of the six largest PDPs (AARP MedicareRx Preferred, AARP MedicareRx Saver Plus, and Humana Enhanced) increased premiums by at least 20 percent in 2016 over 2015 levels 4; 5. By contrast, SilverScript Choice lowered its premium by 3 percent. Some PDPs have entered the market and gained enrollment by charging low premiums, but increased premiums substantially in later years.
Premiums vary widely across plans, even among those offering an equivalent benefit type.
PDPs offering the basic Part D benefit have an average monthly premium of $29.30 in 2016, while PDPs offering enhanced benefits have a higher average monthly premium of $52.91. The portion of the premium for enhanced plans that is attributable to the basic benefit is about 40 percent higher than the average premium for basic plans, suggesting that some of the difference may be attributable to health differences of enrollees in enhanced plans not captured by risk adjusters 6.
Premiums vary widely for basic-benefit PDPs, ranging from $11.40 (SilverScript Choice in Arkansas) to $139.70 (Transamerica MedicareRx Classic in Illinois). Premiums for enhanced PDPs also vary widely, from $18.40 for the Humana Walmart Rx PDP, available in all 34 regions, to $174.40 for the BlueMedicare Rx-Option 2 PDP, only available in Florida. Even within any given region, stand-alone PDPs offering the same type of benefit—basic or enhanced—can have vastly different monthly premiums 7.
MA-PD plan monthly premiums for Part D benefits also vary considerably, although MA-PD plan enrollees typically see a total premium that combines the cost of their medical and drug benefits. About half of MA-PD plan enrollees are in plans with a $0 drug premium, but premiums range as high as $78.80 for a plan offering the basic benefit and $139.10 for a plan with an enhanced benefit. Weighted average Part D premiums for the firms with the most MA-PD plan enrollees range from about $5 per month (Aetna and Cigna) to about $20 per month (Anthem) 8.
Premiums vary widely across geographic regions.
The average monthly premium for PDPs offering the basic benefit is $17.05 in New Mexico, but it is more than twice that amount ($37.13) in New Jersey 9.
For the identical plan offered by the same sponsor, monthly premiums vary across regions by as much as nearly four-fold 10. For example, premiums for SilverScript Choice, the PDP with the most enrollees nationally, range from $11.40 in Arkansas to more than three times that amount ($39.90) in Alaska.
In most regions, the range of premiums for PDPs offering the basic benefit is substantial 11. In Illinois, for example, the highest basic PDP premium is $139.70, almost seven times higher than the lowest basic PDP premium of $20.50. These differences are exaggerated by high premiums for the Transamerica MedicareRx Classic PDPs, which has no more than 0.2 percent of enrollment in any of the 30 regions where it is offered.
Key Findings: Section 3: Part D Benefit Design And Cost Sharing
Stand-alone PDPs and MA-PD plans differ along several key characteristics related to benefit design.
The majority of PDP and MA-PD plan enrollees are in plans with five-tier formularies, tiered pharmacy networks, enhanced benefits, no additional gap coverage, and deductibles below the standard amount of $360. However, a much larger share of MA-PD plan enrollees are in enhanced plans with deductibles less than $360. More PDP enrollees are in plans with tiered pharmacy networks 1.
Over half of PDP enrollees are in PDPs offering the basic benefit in 2016.
In 2016, 58 percent of PDP enrollees—but only 14 percent of MA-PD plan enrollees—are in plans offering the basic (rather than enhanced) benefit, a sizeable reduction from 83 percent of PDP enrollees in basic-benefit plans in 2006 2.
In 2016, about half of all enrollees in PDPs or MA-PD plans are in plans that waive the Part D deductible.
About 48 percent of PDP enrollees are in plans charging the full standard deductible ($360) in 2016, and 3 percent of PDP enrollees are in plans with a deductible that is smaller than the standard amount 3. The shares among MA-PD plan enrollees are 14 percent and 37 percent, respectively 4.
In 2016, nearly all plans use five cost-sharing tiers: preferred and non-preferred generic drugs, preferred and non-preferred brand drugs, and specialty drugs.
The vast majority of all Part D enrollees (98 percent of PDP enrollees and 96 percent of MA-PD plan enrollees) are in plans that use five cost-sharing tiers for their formularies, a design that gained popularity starting in 2012 5; 6. In 2006, most enrollees were in plans with only three or four tiers.
Cost sharing for generic drugs is lower in 2016 than in 2006 for those drugs now placed on preferred generic tiers.
Median cost sharing for preferred generics is $1 for PDPs and $3 for MA-PD plans in 2016, down from $5 in 2006 7. For drugs on the non-preferred generic tier—a tier that became common in 2012—median cost sharing is $7 for PDPs and $12 for MA-PD plans. In 2016, 13 percent of PDP enrollees and 22 percent of MA-PD plan enrollees are in plans that charge $0 copayment for preferred generics 8.
Unlike Part D plans, most employer plans do not use two generic tiers. Median cost sharing in 2015 for employer plans was $10 for the single generic tier, well above median copayments for generics in Part D.
Cost sharing for PDP enrollees for brand-name drugs increasingly takes the form of coinsurance instead of copayments.
In 2016, many PDP enrollees are in plans that charge coinsurance instead of copayments: 31 percent of enrollees now face coinsurance for preferred brand drugs and 96 percent do so for non-preferred brand drugs 9. By contrast, nearly all PDPs and MA-PD plans charge copayments for generic tiers, and most MA-PD plans use copayments for all tiers except the specialty tier.
Cost sharing for brand-name drugs has been relatively stable in recent years, but is much higher in 2016 than in 2006.
Median cost sharing for preferred brands increased between 2006 and 2016 by about 46 percent ($28 to $41) for PDP enrollees and by nearly 70 percent ($27 to $45) for MA-PD plan enrollees. For PDP enrollees who face coinsurance for preferred brands, the median coinsurance rate is 20 percent. Copayments for brand-name drugs in Part D are higher than those typically charged by large employer plans.
Among PDP enrollees in plans that use copayments for preferred brands, a majority (70 percent) are in plans charging between $29 and $44, while most MA-PD plan enrollees (78 percent) are in plans charging at least $45 for preferred brands 10.
For non-preferred brands, most PDP enrollees are in plans charging coinsurance of 40 percent or more; most MA-PD plan enrollees are in plans charging copayments more than $90 11. For PDP enrollees, the median coinsurance rate for non-preferred brands is 40 percent, while for MA-PD plan enrollees, the median copayment amount is $95.
Nearly all Part D plans use specialty tiers for high-cost drugs and charge coinsurance of 25 percent to 33 percent during the benefit’s initial coverage period.
Nearly half of PDP enrollees (49 percent) and more than 4 in 10 MA-PD plan enrollees (43 percent) are in plans that charge the maximum 33 percent coinsurance rate for specialty drugs, defined by CMS as those that cost at least $600 per month 12. Between 2015 and 2016, the share of MA-PD plan enrollees facing 33 percent specialty tier coinsurance declined. Only those plans that waive some or all of the standard deductible are permitted to set specialty tier coinsurance above 25 percent.
The use of tiered pharmacy networks has grown rapidly in recent years and is now the norm in PDPs.
The share of stand-alone PDPs with tiered pharmacy networks grew from 7 percent in 2011 to 85 percent in 2016 13. These plans have 96 percent of PDP enrollees. By contrast, only 30 percent of MA-PD plans, with 21 percent of MA-PD plan enrollees, use tiered pharmacy networks 14.
Non-LIS enrollees in plans with tiered pharmacy networks pay lower cost sharing in pharmacies offering preferred cost sharing and higher cost sharing in other pharmacies 15. The largest differences are for preferred generic drugs: a median copayment of $1 at pharmacies offering preferred cost sharing versus $7 at other pharmacies ($7 versus $13 for non-preferred generic drugs). Differences are more modest for preferred brand drugs: $35 versus $45 for PDPs using copays and 25 percent versus 35 percent for PDPs using coinsurance.
Most Part D enrollees are in plans without additional gap coverage beyond what is provided in the standard benefit as the coverage gap is being phased out.
In 2016, 88 percent of PDP enrollees and 54 percent of MA-PD plans enrollees are in plans without additional gap coverage 16. Although CMS no longer reports on the share of formulary drugs for which additional gap coverage is provided, gap coverage typically applies only to generic drugs and at most a small share of brand drugs, based on data from earlier years.
Monthly premiums for PDPs that offer additional gap coverage are twice the premium amount for PDPs that lack additional coverage, despite the modest additional gap coverage offered in these PDPs 17.
Key Findings: Section 4: The Low-income Subsidy Program
Nearly three in 10 Part D enrollees receive additional financial subsidies for Part D coverage through the Low-Income Subsidy program.
About 12 million Part D enrollees (29 percent of all Part D enrollees) receive additional subsidies through the Low-Income Subsidy (LIS) program (also called “extra help”) 1. The LIS pays Part D premiums for eligible beneficiaries, as long as they enroll in PDPs designated as benchmark plans, and also reduces cost sharing.
About two-thirds of LIS enrollees (66 percent, or 8 million) are enrolled in stand-alone PDPs; others are in standard MA-PD plans, Special Needs Plans (SNPs), Medicare-Medicaid plans participating in financial alignment demonstrations, cost plans, or PACE plans 2. PDP LIS enrollment has been relatively constant since the program began, but MA-PD plan enrollment (including enrollment in SNPs) has more than tripled since 2006.
The percent of Part D enrollees receiving LIS is higher in some states than others, and tends to be higher in southern states than in other regions of the country 3.
In three states (Arizona, Florida, and Hawaii), more than half of LIS enrollees are in some type of MA-PD plan 4. In six states, more than 95 percent of LIS enrollees are in PDPs.
Fewer PDPs qualify as benchmark plans in 2016, compared to any previous year.
In 2016, 226 PDPs nationwide (about one-fourth of plans) qualify as benchmark plans; that is, plans that are available to beneficiaries receiving the LIS for no monthly premium 5. This represents a 20 percent reduction in benchmark plans since 2015. In 2016, the average LIS beneficiary has a choice of seven benchmark plans, fewer than any previous year. About one-fourth of benchmark PDPs in 2016 qualify through a policy that allows plans to waive a premium of up to $2 per month.
Benchmark plan availability ranges by region in 2016 6. LIS beneficiaries have a choice of 10 benchmark plans in three regions (Arizona, Idaho/Utah, and Pennsylvania/West Virginia), but just two benchmark plans in Hawaii and three in Florida.
Some LIS beneficiaries pay premiums, even though they are eligible for premium-free Part D coverage; of the 1.5 million LIS enrollees paying premiums, close to half pay $20 or more per month.
In 2016, about 13 percent of all LIS beneficiaries (1.5 million) pay a premium because they are not enrolled in benchmark plans 7. CMS reassigns some beneficiaries to a zero-premium PDP during open enrollment if their previous PDP loses benchmark status and charges a premium. But these LIS enrollees are not reassigned by CMS because they have actively selected the plan they are in, whether it is a PDP or an MA-PD plan.
The number of LIS beneficiaries paying premiums is currently lower than in 2009 and 2010, at least partly because of the policy that allows plans to waive premiums up to $2 per month.
In 2016, 71 percent of the 1.5 million LIS enrollees who pay a premium for Part D coverage pay $10 or more per month 8. Almost half (45 percent) of the 1.5 million LIS enrollees who pay a premium pay $20 or more a month for their Part D coverage.
On average, the 1.5 million LIS beneficiaries paying Part D premiums in 2016 pay $20.51 per month ($246 per year) 9. This amount is up 19 percent from 2015 and is more than double the amount in 2006.
Key Findings: Section 5: Part D Plan Performance Ratings
In 2016, a much larger share of MA-PD plan enrollees than PDP enrollees are in plans with 4 or more stars out of a possible 5 stars for the rating factors based on their Part D performance.
Less than one in five PDPs (18 percent) are rated with 4 or more stars in 2016; one-fourth of all PDP enrollees are in these plans 1. By contrast, 69 percent of MA-PD plans, with 83 percent of MA-PD plan enrollees, have 4 or more stars for the rating factors based on their Part D performance. Medicare Advantage plans receive higher payments if they receive at least 4 stars for their performance providing all Medicare-covered services, including Part D, where applicable. Stand-alone PDPs have no direct financial incentives connected to their star ratings.
In 2016, one in four PDPs (26 percent), with 7 percent of PDP enrollees, are rated 2.5 or fewer stars. By contrast, only 1 percent of MA-PD plans, with less than 1 percent of enrollees, have 2.5 or fewer stars for their Part D performance in 2016. Plans with ratings this low for three consecutive years are flagged by CMS as “low-performing plans” and are at risk for having their contracts canceled, though CMS has not yet exercised the option of canceling contracts.
About 20 percent of MA-PD plan enrollees are in 5-star drug plans in 2016, as measured by their Part D performance ratings alone. By contrast, only 2 PDPs with 21,000 enrollees, both offered by WPS Health Insurance in Wisconsin, are rated with 5 stars in 2016.
In terms of both national averages and the performance of the leading plan sponsors, ratings have fluctuated annually.
In the years between 2010 and 2016, plans offered by CVS Health have received as few as 1.5 stars and as many as 4 stars, while the ratings for Humana’s plans have ranged from 2.5 to 4 stars 2. Changes are made each year to star rating component measures and to the cut points on each measure; these factors may influence the year-to-year variability in ratings. This variability limits the value of ratings to CMS in assessing plan performance and to consumers in selecting plans.
The average PDP plan rating, weighted by enrollment, declined from 3.7 stars in 2015 to 3.3 stars in 2016, but is closer to the averages in 2013 (3.1 stars) and 2014 (3.0 stars) 3. The average PDP plan rating has fluctuated up and down since 2011, in contrast to the trend in the average MA-PD plan rating for the rating factors based on their Part D performance, even though both types of plans are scored on the same Part D performance factors.
Methodology
This chart collection presents an analysis of the Medicare Part D 2016 marketplace and trends since 2006, prepared by Jack Hoadley, Health Policy Institute, Georgetown University; and Juliette Cubanski and Tricia Neuman, Kaiser Family Foundation. Anthony Damico, an independent consultant, provided data analysis on the average number of Medicare Advantage drug plans per beneficiary.
Data on Part D plan availability, enrollment, and premiums were collected primarily from a set of data files released by the Centers for Medicare & Medicaid Services (CMS) on a regular basis:
Part D plan landscape files, released each fall prior to the annual enrollment period. These files include basic plan characteristics, such as plan names, premiums, deductibles, gap coverage, and benchmark plan status.
Part D plan premium files, released each fall. These files include more detail on plan characteristics, including premiums charged to LIS beneficiaries, the portions of the premiums allocated to the basic and enhanced benefits, and the separate drug premiums for MA-PD plans.
Part D plan crosswalk files, released each fall. These files identify which plans are matched up when a plan sponsor changes its plan offerings from one year to the next.
Part D enrollment files, released on a monthly basis. These files include total enrollment by plan. We use February 2016 enrollment counts for enrollment-based analysis in this report. Enrollment files suppress totals for plans with 10 or fewer enrollees. We impute a value of five enrollees for these plans.
Part D Low-Income Subsidy enrollment files, released each spring (in March for 2016). These files include total enrollment counts for LIS enrollees. There are small differences, most likely due to different dates and underlying files, between total enrollment counts in the LIS enrollment files and those in the general enrollment files. As with the other enrollment files, we impute a value of five enrollees for amounts suppressed for plans with 10 or fewer enrollees.
Medicare plan benefit package files, released each fall. These files supply detailed information on the benefits offered by plans, including cost-sharing amounts for each formulary tier, tier labels, and the different cost-sharing amounts for standard and preferred cost-sharing pharmacies, where applicable.
Medicare county-level enrollment files, released on a monthly basis. These files are used to create total counts at the state level. Because they are different than the plan-level enrollment files, national totals for these files are not identical to totals in other exhibits. We impute values of one beneficiary for all plan/county combination where values of 10 or fewer beneficiaries are suppressed.
Due to methodological differences, some numbers for MA-PD plans in this analysis differ from those in a May 2016 Kaiser Family Foundation report, Medicare Advantage 2016 Spotlight: Enrollment Market Update. Methodological differences include:
How Blue Cross Blue Shield (BCBS) affiliates are treated: this analysis treats BCBS-affiliated firms separately; the Medicare Advantage Spotlight combines BCBS-affiliated firms [excluding Anthem).
How plans in the territories are treated: this analysis does not include data for plans in the territories, including Puerto Rico; the Medicare Advantage Spotlight includes Puerto Rico but excludes other territories.
Which month is used for enrollment counts: this analysis uses February for Part D enrollment; the Medicare Advantage Spotlight uses March enrollment files.
How plans with small enrollment counts that are suppressed in CMS files are treated: this analysis imputes a value of five enrollees for total enrollment in such plans; the Medicare Advantage Spotlight excludes plans with small enrollment counts in estimates that are plan-enrollment weighted.
An updated version of this report was released on February 17, 2022 and can be found here.
Overview
Medicaid plays a major role financing family planning services for low-income women in the United States. Family planning services are “mandatory” benefits under Medicaid and must be provided to individuals of childbearing age free of cost-sharing. There is, however, no formal federal definition of “family planning,” which has given states considerable discretion to determine the specific services covered under this benefit. Furthermore, a state may establish different coverage requirements for Medicaid funded family planning services for different eligibility pathways. The Affordable Care Act (ACA) created a new Medicaid eligibility category which has federally-specified coverage requirements for aspects of family planning (contraceptives, screening services, and counseling), but these requirements do not apply to traditional Medicaid available prior to the ACA. This has magnified the potential for variations in coverage standards for different Medicaid eligibility pathways (e.g. traditional Medicaid available prior to the ACA, ACA Medicaid expansion, or Medicaid Family Planning Expansion program) within a state. The multiple pathways and coverage options make it difficult to assess coverage differences for family planning services both within and across states under fee-for-service.
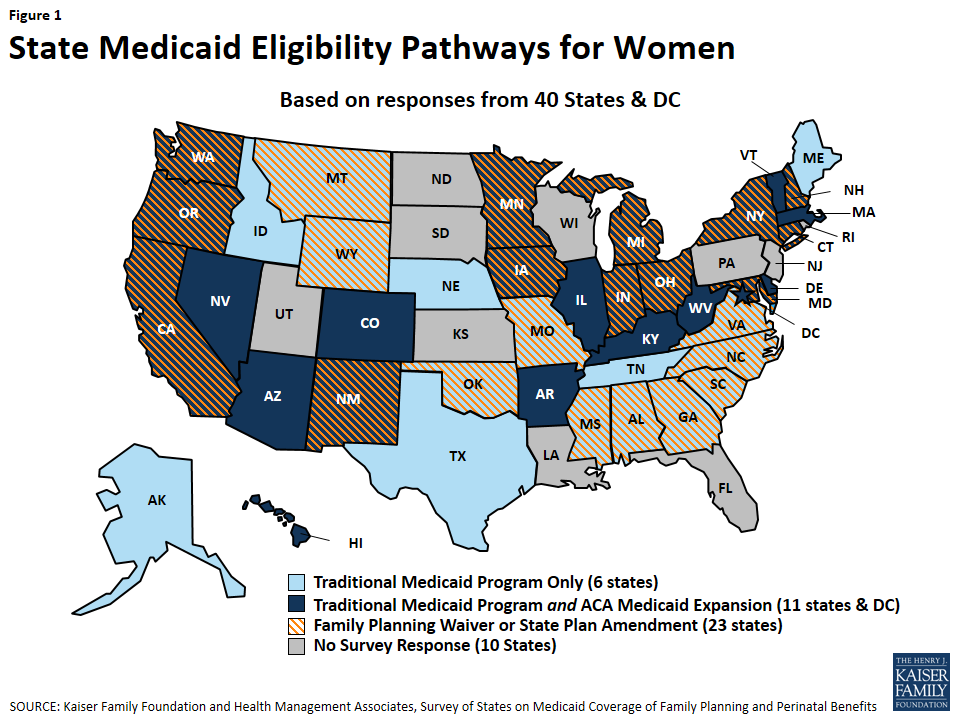
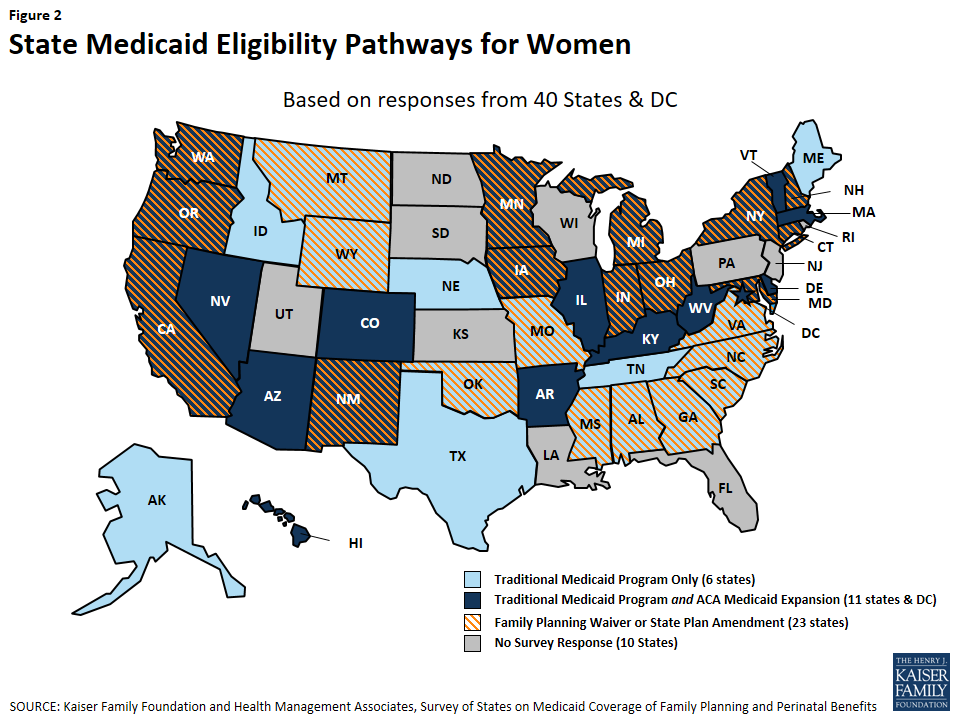
This report presents findings from a state-level survey on states’ family planning benefits under Medicaid, as of July 2015. The survey queried states about their coverage policies under fee-for-service for the following family planning services: reversible contraceptives, sterilization services, fertility diagnosis and treatment, services related to family planning and sexual health such as cancer treatment and partner violence, and managed care policies. The survey identifies differences between states as well as within states between Medicaid eligibility pathways: traditional Medicaid (available pre-ACA), Medicaid expansion under the ACA, and family planning-only coverage through a state Medicaid waiver or State Plan Amendment (SPA). All 50 states and the District of Columbia were invited to respond to the survey, but data are presented for 40 states and the District of Columbia that provided responses (Figure 1). Throughout the report, DC is counted as a state, totaling 41 respondents.
Figure 1: State Medicaid Eligibility Pathways for Women
Key Findings
Reversible Contraception
All responding states cover nearly all prescription contraceptive methods approved by the Food and Drug Administration under their fee-for-service programs, including IUDs and implants (Table 1).1 Coverage of over-the-counter contraceptives, particularly emergency contraception, showed more variation and utilization controls. Most states, but not all states, have aligned their coverage of prescription contraceptives across all of their Medicaid eligibility pathways.
Thirty-six out of 41 states covered all prescription methods in the survey under their traditional Medicaid pathway. Of the five states that did not cover all methods, two states did not cover one form of injectable and three of them did not cover ella, an emergency contraceptive pill.
While most contraceptives are covered, a number of states apply utilization controls such as quantity limits on oral contraceptives and injectables. Some states, however, have moved in the opposite direction, permitting clinics to dispense a 12-month supply of oral contraceptives.
Coverage of IUDs and implants is widespread and no states reported that they limited access to long-acting reversible contraceptives (LARCs) by requiring prior authorization, although some have utilization limits under fee-for-service, such as limiting coverage to certain brands.
States are considering and adopting a variety of payment policies to facilitate postpartum LARC While maternity services are typically paid for with a global fee that includes postpartum care, some states have developed a separate payment outside the global fee to compensate clinicians and hospitals for postpartum LARC insertions. Several states continue to include either the device or clinician fee in the maternity global fee, which can be a disincentive for providers to insert postpartum LARCs given the relatively higher costs of IUDs and lack of separate reimbursement for the insertion.
Table 1: Summary Findings on State Coverage of Contraceptive Methods in Traditional Medicaid Programs
Covers 20 forms of prescription contraceptives in Traditional Medicaid Program (36/41 states)
AK, AR, AZ, CO, CT, DC, DE, GA, HI, IA, IL, IN, KY, MA, MD, MI, MN, MO, MS, MT, NC, NE, NH, NM, NV, NY, OH, OK, OR, TN, TX, VA, VT, WA, WV, WY
5 states that do not cover all methods:
CA, ME cover all methods except Injectable- subcutaneous
AL, ID, SC cover all methods except ella emergency contraceptive
Cover 3 forms of LARC in Traditional Medicaid Program (41/41states)
AL, AK, AZ, AR, CA, CO, CT, DE, DC, GA, HI, ID, IL, IN, IA, KY, ME, MD, MA, MI, MN, MS, MO, MT, NE, NV, NH, NM, NY, NC, OH, OK, OR, SC, TN, TX, VT, VA, WA, WV, WY
Covers 2 forms of Emergency Contraception in Traditional Medicaid Program (35/41 states)
AK, AR, AZ, CA, CO, CT, DC, DE, GA, HI, IA, IL, MA, MD, ME, MI, MN, MO, MT, NC, NE, NH, NM, NV, NY, OH, OK, OR, TN, TX, VA, VT, WA, WV, WY
Covers 4 forms of OTC contraceptives Traditional Medicaid Program (22/41 states)
AK, AZ, CA, DC, HI, IA, IL, MA, MD, MI, MN, MT, NE, NH, NM, NV, NY, OH, OK, VA, WA, WY
NOTES: Prescription contraceptive methods in this survey are: Copper IUD, Hormonal IUD, Implant, Injectable- intra-muscular, Injectable- subcutaneous, Diaphragm, Contraceptive Patch, Vaginal Ring, Oral Contraceptive Pills Combined, Oral Contraceptive Pills- Progestin Only, Oral Contraceptive Pills-Extended Use, ella Emergency Contraceptive Pills, Tubal Ligation- General, Tubal Ligation- Post Partum, Sterilization Implant, and Vasectomy. LARC methods in this survey are: Copper IUD, Hormonal IUD, and Implant. OTC contraceptive methods in this survey are: Male condom, spermicide, sponges and levonorgestrel emergency contraceptive pills.
Coverage for emergency contraception (EC) pills, particularly the over-the-counter (OTC) product (levonorgestrel, also known as Plan B), is not as uniform as for the prescription method (ulipristal acetate, also known as ella). While at least one form of EC pills is covered in traditional Medicaid programs in most states, the OTC option is covered in fewer states and subject to greater utilization controls, sometimes requiring a prescription. Three states report that they do not cover either type of EC pills. All states reported that they cover the copper IUD, which can be used as an EC, in all of their pathways.
Variation in coverage across the states was most notable for over-the-counter (OTC) contraceptives, including condoms and Plan B emergency contraception. Coverage for OTC supplies also varied across state Medicaid eligibility pathways, and a number of states require prescriptions for coverage, which creates an access barrier for products the FDA has deemed to be safe and effective for over-the-counter use.
Sterilization and Fertility Services
Most states cover sterilization services in their FFS program, but few pay for fertility services. Federal law specifies that states must cover surgical and implant sterilization procedures for women under ACA Medicaid expansion, and all of the responding states reported that they cover these procedures in traditional Medicaid as well.
Medicaid family planning expansion program do not always pay for sterilization services for women.
While all states reported they cover vasectomies under traditional Medicaid, not all cover the procedure in their family planning expansion programs or under their full scope Medicaid expansion programs.
Very few states cover diagnostic testing related to fertility, including laparoscopy for women and semen analysis for men.
Only one state covers fertility treatments for either women or men, but this is restricted to individuals who have infertility as a symptom of separate medical problem.
Family Planning-Related Services
The definition of high quality family planning encompasses a broad array of services including screening and treatment for cervical and breast cancers, interpersonal violence screening and prevention, and sexual health counseling. These family planning-related services, however, are less consistently covered by family planning expansion programs than contraceptives.
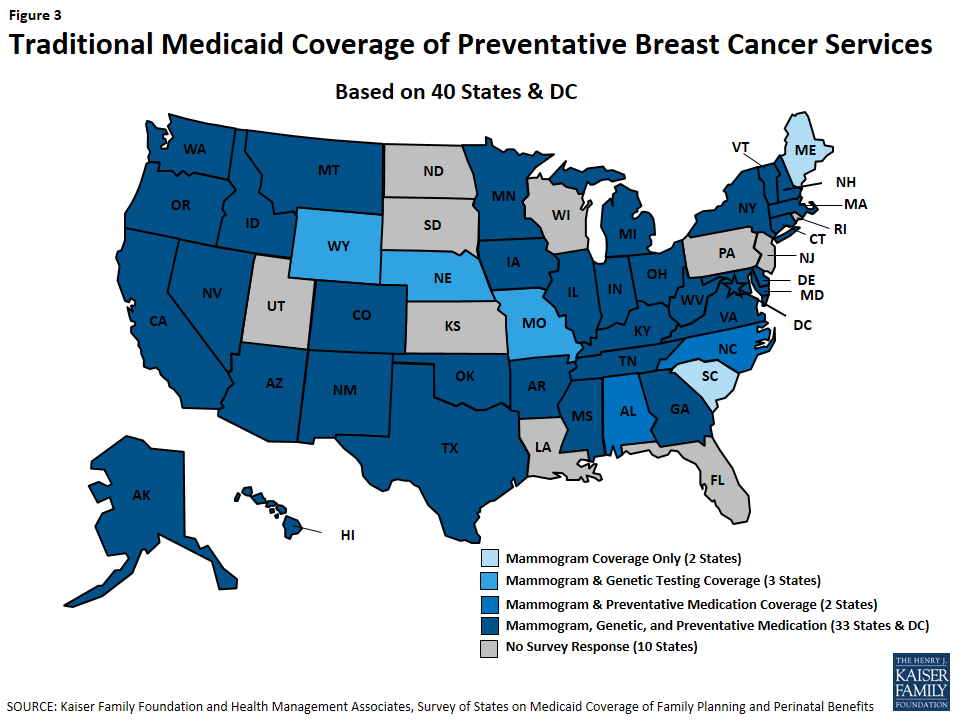
Although breast cancer screening is considered “optional” under traditional Medicaid, it is a required benefit in ACA Medicaid expansion programs. All responding states provided breast cancer screening services under these two full scope eligibility pathways. Few states, however, provide this benefit through their family planning waiver or SPA.
All states cover Pap screening for cervical cancer regardless of eligibility pathway, but follow-up tests for abnormal screening results are less likely to be covered in state family planning waivers or SPAs.
HPV vaccines for young adults are covered in all but one state, but the benefit is less likely to be covered through a family planning expansion program.
Contraceptive counseling and screening for intimate partner violence are covered by most states, but services are typically subject to restrictions and are not always covered for all eligibility pathways available within a state.
Managed Care Policies
The majority of states have capitated managed care contracts that include family planning services. Many of these states, however, do not address how utilization controls can be used in the context of family planning in their contracts. Some of the states noted that they contract with MCOs that include providers with religious objections to family planning in their networks, but not all of these states detailed referral processes to assure that women can get family planning care from other providers.
Most of the responding states have capitated contracts that include family planning in the capitation rate. Just over one-third of these states explicitly address potential utilization controls on family planning services in the contracts with managed care organizations.
A handful of states reported that they do not claim the enhanced 90% federal match for family planning services provided through managed care organizations.
California and New York, states with the most beneficiaries, also contract with faith-based plans that oppose some forms of contraception. While California reported that they have a process in place for referral for family planning services for the beneficiaries in these plans, New York did not report a referral practice.
Conclusion
The analysis of state responses to this survey found that overall most states cover a broad range of prescription contraceptive methods in their full scope, traditional Medicaid programs and their full scope ACA Medicaid expansions, but finds more variation in coverage through the family planning expansion programs. Thirty-six of 41 surveyed states report that they cover all prescription contraceptives for women through their full scope programs. While states are not required to cover all methods under all pathways, most do. However, there is more variation between and within states for coverage of over-the-counter contraceptives, including condoms and Plan B emergency contraception pills. In some states that provide coverage, it is only with a prescription which can limit access to these safe and effective methods. Furthermore, over the years the family planning field has evolved to encompass other services beyond contraception that help women and men maintain and control their reproductive and sexual health. Medicaid coverage for prevention and management of breast and cervical cancers and screening for interpersonal violence is available in most states, but not as consistently as for contraceptives. These preventive services must be covered by new private insurance plans as a result of the ACA, but there is no requirement that they be covered under traditional Medicaid or under the family planning expansion programs.
Access to the full range of contraceptive methods as well as related family planning services has become a standard of comprehensive health care for women and men in their reproductive years.2 As enrollment in the Medicaid program continues to grow as a result of the ACA and state decisions to expand coverage for family planning services, policy choices defining coverage of services under Medicaid family planning will continue to be a significant force shaping access to sexual and reproductive health services for low-income women and men in years to come.
Acknowledgements
The authors express appreciation for the assistance of several individuals who assisted with the preparation, testing, and refinement of the survey instrument, including Yali Bair of Ursa Consulting, Amy Moy from the California Family Health Council, Tasmeen Weik of the federal Office of Population Affairs, Melanie Reece of Colorado’s Department of Health Care Policy and Financing, and Lisa DiLernia of Michigan’s Department of Health and Human Services.
We thank the following colleagues from Health Management Associates: Joan Henneberry for guidance and subject matter expertise; Dennis Roberts for database development and management; and Nicole McMahon for assistance with compiling the state data tables.
We also thank the Medicaid directors and staff in the 40 states and the District of Columbia who completed the survey on which this report is based.
Introduction
Introduction
Overview
Medicaid is the primary funding source for family planning services for low-income women. While the federal and state governments jointly finance the program, states operate their programs and establish benefits, eligibility and coverage policies subject to broad federal guidelines. To understand variations in the scope of coverage for family planning and perinatal services and related state Medicaid policies across the nation, the staff of the Kaiser Family Foundation and Health Management Associates surveyed states about benefit policies in place as of July 1, 2015, for family planning and perinatal services.
The survey was conducted between October 2015 and February 2016. Forty states and the District of Columbia responded to the survey. Non-responding states are: Florida, Kansas, Louisiana, New Jersey, North Dakota, Pennsylvania, Rhode Island, South Dakota, Utah and Wisconsin. A majority of the states responding to the survey contract with managed care organizations (MCOs) under a capitated structure to deliver Medicaid services, including family planning. While the survey asked states to consider only state Medicaid policies under fee-for-service when responding to the questions, it is possible that MCOs provide additional family planning services to enrollees as added value benefits, unless they are contractually prohibited from doing so.
As illustrated in Figure 2, of the 41 responding states, as of July 1, 2015:
25 had adopted an ACA Medicaid expansion program 3
13 had both an ACA expansion program and a family planning-only waiver or SPA program
6 provide services through their traditional Medicaid program only, although one (Texas) also has an exclusively state-funded family planning program.
Figure 2: State Medicaid Eligibility Pathways for Women
This report presents the survey findings on 41 states’ Medicaid coverage of family planning services as of July 2015 (DC is referred to as a state throughout this report, for simplicity). Summary tables are presented throughout the report and more detailed, state-level tables are in Appendix A. A companion report summarizing state Medicaid coverage of perinatal services will be issued in the near future.
Background
The manner in which family planning services are financed and organized is unique within the Medicaid program. Federal law:
Classifies family planning services and supplies as a “mandatory” benefit category that states must cover, but states have some discretion as to which services they include in this category;
Prohibits copayments or any other form of patient cost sharing for family planning services;
Entitles beneficiaries to seek family planning services from any provider that participates in the Medicaid program, called freedom of choice; and
Provides a 90% federal matching rate for the costs of family planning services, a higher proportion than for other services. States pay the remaining 10% of costs.
In addition to long-standing coverage under traditional Medicaid programs, states have also applied to the federal government via “Section 1115 Medicaid waivers” establish programs that extend Medicaid coverage for family planning services only to women and men who are not otherwise eligible for full-scope Medicaid. Prior to the ACA, waivers were the only mechanism for states to establish these limited scope programs. The waivers must be approved by the Centers for Medicare and Medicaid Services (CMS), the federal agency that oversees the Medicaid program. Multiple studies have found that these programs prevent unintended pregnancies and abortions, thus improving women’s health and saving money for the federal and state governments.5
The ACA made many changes to Medicaid coverage that affected beneficiaries’ access to family planning services under the program. Beginning in 2014, states could expand Medicaid eligibility to most people with incomes below 138% FPL without regard to categorical eligibility. As of March 14, 2016, 31 states and the District of Columbia have chosen to adopt full scope Medicaid expansion programs.6 ACA also defined a minimum “Alternative Benefit Plan” (ABP) that states must provide to beneficiaries under this full scope Medicaid expansion option. The ACA specifies that the ABP must include ten “essential health benefits,” including preventive services, at no cost to the patient.7 The preventive services under this policy include several services related to family planning, such as all FDA-approved contraceptives with a prescription, testing for sexually transmitted infections, screening for cervical and breast cancers, the HPV vaccine, and screening for intimate partner violence. Traditional, pre-ACA Medicaid programs and waiver-specific programs, however, are not bound by the ABP requirements, which means that the benefits package can vary within states for different Medicaid populations based on their eligibility pathway (Appendix B).
The ACA also eased the process for states to establish limited scope family planning programs, enabling them to change their program by adopting “state plan amendments,” or SPAs, without requesting a federal waiver of Medicaid rules. States could continue to operate their family planning programs under the waivers as they had historically done, or they could establish the program under SPA authority.
Table 2: Medicaid Eligibility Pathways for Family Planning Services
Traditional Medicaid – Medicaid coverage available prior to the Affordable Care Act (ACA) was based on an individual having income below states’ very low thresholds as well as being in one of the program’s eligibility categories: pregnant, mothers of children 18 and younger, disabled, or over age 65
ACA Medicaid Expansion – The ACA allowed states to eliminate categorical requirements and extend Medicaid to most women and men with family income at or below 138 percent of the federal poverty level.
Family planning-only programs – Several states operate programs that provide Medicaid coverage just for family planning services to women who are not otherwise eligible for full Medicaid benefits. These programs are authorized either with waivers or State Plan Amendments (SPAs) that must be approved by CMS.
There is a minimum floor of family planning services that must be covered under ACA Medicaid expansion, but that is not the case for traditional Medicaid or family planning-only coverage (Table 2). This survey asked states about the scope of states’ coverage of family planning benefits under multiple eligibility pathways for Medicaid. Detailed findings from 40 states and DC on commonalities and differences between and within states are presented for reversible contraceptives, sterilization services, fertility diagnosis and treatment, related sexual health services such as cancer treatment and partner violence screening, and managed care policies.
Reversible Contraception
Key Finding: Prescription Contraceptives
All responding states provide coverage for most prescription contraceptive methods approved by the Food and Drug Administration (FDA). In addition, with few exceptions, most states aligned their coverage of prescription contraceptives across all of their Medicaid eligibility pathways.
While most contraceptives are covered, a number of states apply utilization controls such as quantity limits on oral contraceptives and injectables.
The survey examined state coverage policies for multiple types of contraceptive devices and methods including, prescription and non-prescription methods, as well as reversible methods and sterilization procedures for women and men. Reversible methods include a wide range such as long-acting reversible contraceptives (LARCs) – intra-uterine devices (IUDs) and implants; oral contraceptives; injectables, emergency contraceptives; and various other products and devices available by prescription or over-the-counter (OTC).
Long-Acting Reversible Contraceptives (LARCs)
Key Finding: LARC
Coverage of IUDs and implants is widespread and no states limited access to LARCs by requiring prior authorization or other utilization limits.
LARCs are highly effective for extended periods of time, ranging from three to 10 years depending on the specific type that a woman uses. In the United States, three types of LARCs are available: Hormonal and non-hormonal IUDs and implants. All states participating in the survey cover all LARC methods through all of their Medicaid programs offering family planning services (Table 3). The ACA requires coverage of these benefits in Medicaid expansion programs.
Table 3: State Coverage of LARCs
Contraceptive Device or Service
Traditional Medicaid(n = 41)
Family Planning Waiver or SPA(n = 23)
ACA Medicaid Expansion(n=25)
Apply Limitations or Restrictions
Copper IUD
41
23
Required
3
Hormonal IUD
41
23
Required
6
IUD Removal
41
23
Required
4*
Implant
41
23
Required
3
Implant Removal
41
23
Required
3*
* “Medical necessity” is included in the count of states with restriction or limitations for IUD and implant removal.
LARC Limitations or Restrictions
Only a few states noted utilization controls or restrictions for devices. Typically, restrictions apply to benefit frequency or for specific devices (Table 4). For device removal, “medical necessity” was treated as a limitation since it is not clear whether states consider the desire to become pregnant a medical necessity. This was the most common restriction noted for device removal.
For removal of an IUD, Alabama specified the following criteria: the recipient develops high blood pressure or other medical condition that would allow for a progestin only method; any nulliparous woman who has a spontaneous expulsion within six months of placement; Mirena IUD is removed to allow a pregnancy; surgical removal of an embedded IUD in an office or outpatient setting. Missouri noted that the specific CPT code for IUD removal is not covered, but providers are instructed to use an office visit code for reimbursement. In addition to limits on quantity, California noted that LARC devices are limited to clinic dispensing only.
Table 4: State Utilization Controls for LARCs
IUD Device
IUD Removal
Implant Device
Implant Removal
Quantity/frequency limits
AL, CA, MI, MO
CA, MI, MO
Brand/type restrictions
AL, ME, OK
Coverage subject to certain medical conditions or “medical necessity”
AL, NY, OK, TN
NY, OK, TN
Removal covered to allow pregnancy
AL
LARCs Provided Immediately Post Labor and Delivery
Key Finding: LARC Reimbursement
States are experimenting with a variety of payment policies to facilitate postpartum LARC insertion. Approaches include separate payments for LARC device as well as clinician fee outside of the global fee. Several states continue to include either the device or the clinical fee within the global fee that is used to typically pay for maternity care.
States were asked how they reimburse providers for LARCs provided immediately after labor and delivery. This has been the source of considerable research, public health education, and policy activity in recent years in part because data that suggests birth spacing is an important component of healthy pregnancies and optimal birth outcomes.8 LARCs are among the most effective forms of reversible contraception and research suggests that providing them during the postpartum period, either at the time of delivery or at the follow up visit can help lower the rate of unintended pregnancies.
Labor and delivery is typically reimbursed through a global fee that covers the costs of all maternity care, including labor and delivery services, and postpartum care. Many providers have reported that the global fee is not sufficient to cover the costs of providing a LARC postpartum at the time of delivery or at the follow up postpartum visit. The absence of a separate fee or an increase has been a disincentive for some providers. Among the 41 states responding to the survey, the reimbursement methodology for hospitals most frequently reported is a global fee for both the LARC device and insertion (17 states), followed by 10 states that include insertion in a global fee and reimburse hospitals separately for the device. Conversely, the most frequently reported methodology for reimbursing other providers was a separate fee for both the device and insertion (25 states). Table 5 illustrates summary data for reimbursement for LARC device and insertion post labor and delivery. AppendixTable A1 provides detail for each state response.
Three states indicated no specific hospital reimbursement for post labor/delivery LARCs. Arizona indicated that when the state implemented a hospital APR DRG9 payment methodology, the fee associated with the labor and delivery for the hospital did not consider the inclusion of LARC, but it will be considered in the future. The District of Columbia noted it does not reimburse for immediate post- partum LARC, but the managed care plans do, and the reimbursement methodology varies across the three contracted health plans. North Carolina reported that many hospitals and physician offices have chosen not to place LARCs in the immediate postpartum period.
Table 5: Reimbursement Structure for Post Labor & Delivery LARC Device and Services
Hospital(n=41)
Other Provider(n=40)*
Global Fee includes LARC Device and Insertion
17
6
Separate Fee for Both LARC Device and Insertion
7
25
Device included in Global Fee; Insertion Separate Reimbursement
4
4
Device Separate Reimbursement; Insertion included in Global Fee
10
1
Other
3
4*
*Maryland did not provide a response for reimbursing other providers; Delaware noted that other providers are reimbursed for insertion as part of a global fee, but did not provide a response for the device itself.
States were asked to identify and briefly describe any known policy or reimbursement barriers that inhibit the provision of LARCs immediately following labor and delivery. Several states that use a global fee to reimburse hospitals noted low utilization of postpartum LARC provision, whether the global fee was for the device, insertion or both. Several states reported plans to change their reimbursement methodology.
CMS Bulletin on Payment Approaches for LARCs
In April 2016, CMS issued a bulletin addressing reimbursement for LARC devices. CMS identifies some of the barriers that have impeded broader use of these devices, including low reimbursement levels, the absence of a separate payment from the typical global maternity fee, and administrative hurdles for providers to keeping devices on hand so that they can be provided upon request. The bulletin highlights recent state activity to address these barriers as well as potential strategies to encourage clinicians to provide LARCs postpartum and in the primary care setting, including:
Raising provider payment rates
Unbundling payment for LARC from other maternity services.
Reducing logistical barriers for supply management
Removing administrative barriers for provision of LARC
Colorado and Tennessee use the global maternity fee to reimburse hospitals for both the device and insertion. Colorado notes that postpartum LARCs are currently covered and available under normal labor and delivery reimbursement but also stated that the state is “looking to carve out payment from the global [labor and delivery] fee, but [are] still working on an appropriate process and CMS approval.” Tennessee plans to unbundle payments in 2016 to allow for separate reimbursement for postpartum LARCs “…in hopes of improving access for this contraceptive technology to Medicaid enrollees.”
Georgia reimburses hospitals for LARC insertion using a global fee and reimburses for the device separately, but notes that few LARCs have been purchased by hospitals to date for immediate postpartum insertion. The state intends to make system changes in 2016 that will allow separate reimbursement to hospitals for postpartum LARC insertion.
Texas included LARC device reimbursement within the hospital DRG but effective January 1, 2016 allows hospitals to receive reimbursement for the LARC device in addition to the DRG payment when the device is inserted immediately postpartum.
Other states reported issues with global payments for postpartum LARC procedures and devices: Massachusetts, which uses global payments, noted that providers would prefer a different reimbursement mechanism; Minnesota noted that they do not have a different DRG for LARC procedures/devices following a birth, as there is with sterilization procedures following a birth; Oregon reported that the DRG payment does not adequately cover the hospital cost so they are currently considering options to enhance the reimbursement amount; Washington changed its policy to allow separate reimbursement for a LARC device and enhanced reimbursement for LARC insertion added to the RVU-based fee.
Two states that use a global hospital reimbursement for both the device and LARC insertion, Michigan and Ohio, reported no barriers to utilization. Virginia, which also uses a global reimbursement methodology, described a four month pilot project implemented by one of its managed care plans that allowed for separate payment for the LARC device. However, there were no requests for immediate postpartum LARC insertions, so the pilot ended. The state noted “…it appears that a primary potential barrier of accessing this method of LARC is lack of provider and member education and training versus policy and reimbursement.”
Oral Contraceptives
Key Finding: Oral Contraceptives
All responding states cover daily use oral contraceptives (Combined, Progestin only, as well as Oral Extended and Continuous use) regardless of the eligibility pathway.
Few states allow a 12-month supply for oral contraceptives; supply limits are the most common method to control utilization.
Oral contraceptives are the most commonly used form of reversible contraception among women in the United States. All states surveyed cover all forms of oral contraceptives in their traditional Medicaid program and their family planning waiver or SPA as applicable. The ACA requires states to cover oral contraceptives for adults in their Medicaid expansion programs (Table 6). The survey also asked states whether they provide coverage for 12 months’ supply of oral contraceptives. Eleven of the responding states indicated that they allow a 12-month supply of oral contraceptives to be dispensed, but typically with some restrictions (7 states). For example, California10 and Virginia noted that 12-month dispensing is restricted to clinics and on-site dispensing by medical providers. Pharmacies may not dispense a 12-month supply, with the exception of California’s family planning expansion program.
Table 6: Oral Contraceptive Coverage
Benefit
Traditional Medicaid(n=41)
ACA Medicaid Expansion(n=25)
Family Planning Waiver or SPA(n=23)
Oral Contraceptives (specific)
– Combined Estrogen Progestin
41
Required
23
– Progestin Only
41
Required
23
– Oral Extended/Continuous Use
41
Required
23
Limitations and Restrictions
Supply limits are the most common restriction reported for oral contraceptives, and limits are most usually tied to the dispensing provider, or program (Table 7). Seven states reported they restrict their supply to three months. Vermont requires prior authorization for non-preferred brands, along with a trial of a preferred brand. Mississippi and Vermont include oral contraceptives on the state’s Preferred Drug List (PDL), which means that coverage for these drugs is not subject to prior authorization. Appendix Table A2 provides state response detail around 12 month supply dispensing and utilization controls for oral contraceptives.
Table 7: State Utilization Policies for Oral Contraceptives
Utilization Control
States Utilizing
Notes
Limited to 3 month/90 day supply (7)
CA, IL, MI, MN, MS, NH, WY
CA and MI limit applies to pharmacy dispensing
Limited to 6 month supply (1)
CO
Allow 12 month supply (11)
AL, CA, IN, MO, MS, NM, OR, SC, TX, VA, WA
AL, CA, MS, SC, TX, VA allowance applies to clinic dispensing only; OR applies only to family planning waiver service recipients
Quantity limit, unspecified (1)
AR
Pharmacy benefit only (2)
GA, CA
CA limit applies only to extended use oral contraceptives for family planning expansion program
Included on Preferred Drug List (2)
MS, VT
Prior Authorization (2)
CA, VT
CA limit applies to extended use oral contraceptives only; VT requires prior authorization for non-preferred brand with trial of preferred brand
Other Prescription Contraceptives – Injectable, Diaphragm, Patch, Ring
Almost all of the responding states covered the remaining prescription contraceptives included in the survey across all available eligibility pathways. These methods include injectable contraceptives, the diaphragm, contraceptive patch, and vaginal ring. California and Maine indicated they do not cover the subcutaneous injectable, but California was in the process of adding coverage for this method.
Limitations and Restrictions
The most common utilization control noted by states for these contraceptive methods is limits on quantity or dose (Table 8). States that identified quantity and/or dose limits for one or more of the methods include: Alabama, Arkansas, California, Illinois, Michigan, and Missouri. Other restrictions pertain to the type of provider that can provide or dispense the contraceptive. California allows only clinics to dispense injectable contraceptives, but restricts dispensing of diaphragms to pharmacies. The place of service – either pharmacy or clinic – for the contraceptive patch and vaginal ring depends on the type of product dispensed. Michigan allows up to two diaphragms per year, but they must be dispensed from the same billing provider. States also reported other policies and program integrity measures. For example, in Texas the claim for the product must be accompanied by a family planning diagnosis code.
Table 8: Coverage and Utilization Controls for Other Contraceptive Methods
Traditional Medicaid(n=41)
ACA Medicaid Expansion(n=25)
Family Planning Waiver or SPA(n=23)
Number of States with Utilization Controls
Injectable –intra-muscular
41
Required
23
Quantity/dose: 5Place of service: 1Other: 4
Injectable – subcutaneous
39
Required
22
Quantity/dose: 4Other: 4
Diaphragm
41*
Required
23
Quantity/dose: 4Place of Service: 2Other: 1
Contraceptive Patch
41
Required
23
Quantity/dose: 4Place of Service: 1Other: 3
Vaginal Ring
41*
Required
23
Quantity/dose: 3Place of Service: 1Other: 2
* North Carolina covers diaphragm fitting only; Georgia covers the Vaginal Ring as a component of a family planning visit.
Emergency Contraceptives
Key Finding: Emergency Contraception
At least one form of emergency contraceptive pills (levonorgestrel and ulipristal acetate) are covered in traditional Medicaid programs in all but three responding states. The over-the-counter option (levonorgestrel, also known as Plan B) is covered in fewer states and subject to greater utilization controls, including requiring a prescription. All states reported that they cover the copper IUD, which can be used as an emergency contraceptive, in all of their pathways.
In addition to coverage for Copper IUDs, which can be used as an emergency contraceptive, the survey asked states about their policies with respect to oral emergency contraceptives, including ella (ulipristal acetate) which is only available with a prescription, and Plan B products (levonorgestrel)11 which are available OTC without a prescription.
A few states provide unrestricted access to emergency contraception, or provide Plan B without a prescription: Maryland, Nebraska, Oregon, and Washington. Only three states reported that they do not cover either form of emergency contraceptive pills in any of their Medicaid programs – Alabama, Idaho, and SouthCarolina. Thirty-eight states cover ella, and 35 cover both Plan B products and ella emergency contraceptives in their traditional Medicaid programs. The ACA requires that Medicaid expansion programs cover emergency contraceptives, but only with a prescription under the ABP (Table 9). This means that these programs must always cover ella, but only are required to cover Plan B with a prescription.
For OTC Plan B emergency contraception, 21 of 25 states with an ACA Medicaid expansion population provide coverage through that pathway. Alabama, Idaho, Indiana, Kentucky, Mississippi, and South Carolina do not provide emergency OTC contraceptive coverage in any of the eligibility pathways available within the state. Minnesota does not provide the benefit in its ACA Medicaid expansion, but does provide it in the traditional Medicaid program and through the family planning SPA. Wyoming does not provide the benefit through its family planning waiver but does cover the benefit under traditional Medicaid.
Table 9 State Coverage of Emergency Contraceptives, by Type of Program
Traditional Medicaid(n=41)
ACA Medicaid Expansion(n=25)
Family Planning Waiver or SPA(n=23)
Number of States Noting Restrictions*
Ella
38
Required
20
7
Plan B
35
21
18
31
Both Ella and Plan B
35
21
17
Neither Ella nor Plan B
3
0
2
AL, ID, SC do not cover either ella or Plan B in traditional Medicaid; AL and SC do not cover in family planning waiver/SPA
* Requiring a prescription is not counted as a restriction for Ella, since a prescription is required in all states for this product. Requiring a prescription is counted as a restriction for Plan B products, which are available for purchase over the counter.
Utilization Controls and Restrictions for Emergency Contraceptives
In the case of ella, which requires a provider prescription, fewer states apply utilization controls across states compared to Plan B OTC products (Table 10). Only seven states note any kind of utilization control for ella, with quantity limits the most prevalent limitation. The most common utilization restriction imposed by states, other than requiring a prescription for OTC products is quantity control (6 states). Two states restrict the place of dispensing to pharmacies and Washington allows pharmacists to dispense OTC emergency contraceptives directly to the client without prescription. Appendix Tables A3 and A4 include more detail on state responses to survey questions concerning how states cover of emergency contraception.
Seven states cover Plan B products but do not cover other methods of OTC contraceptives (Georgia, Maine, Missouri, North Carolina, Tennessee, Vermont, and West Virginia). Of the 41 responding states, most require prescriptions for OTC products (29 states), including Plan B (27 states).
Table 10: State Utilization Controls for Emergency Contraceptives
Utilization Controls – Ella (Rx)
States with Utilization Control Policies
Quantity Limits (5)
AR, CA, IL, MN, NY,
Place of dispensing controls (1)
GA (pharmacy benefit only)
Gender controls (2)
AR, CA
On PDL (1)
MS
Utilization Controls – Plan B (OTC)
Requires Prescription (27)
AK, AR*, AZ, CA, CO, CT, DC, DE, HI, IA, MA, ME*, MI, MO*, MT, NC*, NH, NM, NV, OH, OK, TN*, TX, VA, VT*, WV*, WY
Quantity Limits (6)
AR, CA, IL, ME, MN, NY,
Place of dispensing controls (2)
GA, TX (pharmacy benefit only)
Gender Controls (2)
AR, CA
Prior Authorization (1)
VT*
Age Controls (1)
GA
* Arkansas requires a prescription within the ACA Medicaid expansion population only.Georgia, Maine, Missouri, North Carolina, Tennessee, Vermont, and West Virginia do not cover OTC contraceptives except for Plan B emergency contraception.Vermont requires prior authorization for Plan B brand only. Other products are covered with a prescription.
Over-the-Counter (OTC) Contraceptives
Key Findings: OTC Contraceptives
There is more variation in coverage for over-the-counter contraceptive methods compared to prescription methods. A number of states also require prescriptions for these methods to be covered by Medicaid.
In addition to emergency contraceptive options discussed above, states were asked about their Medicaid coverage policies for male condoms, spermicide and sponges which are available over the counter to the public. Under the ACA, full scope Medicaid expansion pathways must cover prescription methods, but the requirement does not apply to over the counter methods. The survey found more variability between states and between eligibility groups for over-the-counter methods, compared to prescription methods.
Fewer than half of responding states (20 states), cover all three types of OTCs in all eligibility pathways available within the state. Ten states do not cover any of the three OTC products in any Medicaid program: Alabama, Georgia, Idaho, Kentucky, Maine, Missouri, North Carolina, Tennessee, Vermont and West Virginia. As illustrated in Table 11, male condoms and spermicide are covered in 27 of the 41 responding states and the sponge in 26 states. All three types of contraceptives were covered for ACA Medicaid expansion groups in 18 states of the 25 states with that eligibility pathway. Most of the responding states with a family planning waiver or SPA cover male condoms, spermicide and sponges (18, 17, and 17 states respectively). Appendix Tables A5 and A6 provide additional detail on state coverage of OTCs and utilization controls applied and coverage of OTC contraceptives in each of the eligibility pathways.
Table 11: Medicaid Coverage of OTC Contraceptives
Traditional Medicaid(n=41)
ACA Medicaid Expansion(n=25)
Family Planning Waiver/SPA(n=23)
Not Covered in Any Program
Male Condoms
27
18
18
11
Spermicide
27
18
17
12
Sponges
26
18
17
13
Utilization Controls for Over-the-Counter Contraceptive Supplies
Only six states noted no restrictions for any of the three OTC supplies for which they provide coverage: Illinois, Indiana,12Maryland, Minnesota, Nebraska and Oregon (Table 12). Requiring a prescription is the most common utilization control for OTC contraceptive supplies. This is likely due, at least in part, to the established reimbursement mechanism to pharmacies for prescription drugs. Twenty-two states require a prescription or other form of documentation for OTCs. Michigan requires a prescription for spermicide and sponges purchased OTC, but does not require a prescription for condoms. Delaware also requires a prescription for both spermicide and sponge contraceptives, but does not cover male condoms.
Some states noted differences in coverage of OTCs based on whether the supply was obtained through a pharmacy benefit or through a clinic (point of service). For example, Virginia restricts access to all three OTC types to pharmacy dispensing only with a prescription. Connecticut does not cover spermicide under the retail pharmacy benefit (but does cover condoms that contain spermicide). Under the medical benefit, spermicide is covered when provided by an enrolled family planning clinic or from a medical/surgical supplier. Texas only allows reimbursement to family planning agencies for dispensing male condoms and spermicide. In Mississippi, condoms are only reimbursable through a medical claim for family planning waiver participants.
Table 12: Methods Used by States to Restrict Utilization of OTC Contraceptive Supplies
Male Condom
Spermicide
Sponges
No restrictions (6)
IL, IN, MD, MN, NE, OR
IL, IN, MD, MN, NE, OR
IL, IN, MD, MN, NE, OR
Quantity/Claim limits (3)
CA, MI, OH
CA, OH
CA
Point of service restriction (4)
MS, TX, VA
CT, TX, VA
VA
Prescription or other documentation required (22)
AK, AZ, AR, CA, CO, CT, DC, HI, IA, MA, MT, NV, NH, NM, NY, OH, OK, SC, VA, WA, WY
AK, AZ, AR, CA, CT, DE, DC, HI, IA, MA, MI, MT, NV, NH, NM, NY, OH, OK, SC, VA, WA, WY
AK, AZ, CA, CO, DE, DC, HI, IA, MA, MI, MT, NV, NH, NM, NY, OH, OK, SC, VA, WA, WY
Prior authorization (1)
OH
OH
* Ohio requires prior authorization to exceed quantity limits (36/month for condoms;1/month spermicide)
Sterilization Procedures
Key Finding: Sterilization
Coverage of sterilization services varied by eligibility pathway. States must cover surgical and implant sterilization procedures for women under ACA Medicaid expansion, and all of the responding states reported that they cover these procedures in Traditional Medicaid as well. However, not all family planning expansion programs cover these services.
This survey inquired about states coverage of sterilization procedures for women (tubal ligation and non-surgical essure) and men (vasectomy). As with FDA-approved reversible methods, the ACA requires coverage under the ACA Medicaid expansion to include surgical and non-surgical sterilization procedures for women. The requirement does not apply to vasectomy for men.
Federal Rules for Payment of Sterilization
Federal funds can only be used to pay for the sterilization of an individual when:
a) The individual is at least 21 years old at the time consent is obtained;
b) The individual is not a mentally incompetent individual;
c) The individual has voluntarily given informed consent in accordance with all the requirements prescribed in §§441.257 and 441.258; and
d) At least 30 days, but not more than 180 days, have passed between the date of informed consent and the date of the sterilization, except in the case of premature delivery or emergency abdominal surgery. An individual may consent to be sterilized at the time of a premature delivery or emergency abdominal surgery, if at least 72 hours have passed since he or she gave informed consent for the sterilization. In the case of premature delivery, the informed consent must have been given at least 30 days before the expected date of delivery.
Source: 42 CFR §441.253
The federal government requires states to cover sterilization procedures only when certain conditions are met. These requirements are intended to protect against coercive practices that had historically forced sterilizations upon marginalized groups, including low-income women, women with disabilities, women of color, and incarcerated women.13 Protections against these practices include requiring women to sign an informed consent form at least 30 days prior to a procedure as well as prohibition of federal matching funds for the sterilization of a mentally incompetent or institutionalized individual.
Most states with a Family Planning waiver or SPA also cover the procedures for women (Table 13), but there are exceptions. Ohio and Oregon do not cover tubal ligation (neither general nor post-partum) in their family planning programs. Connecticut, Georgia, Missouri, and Mississippi do not cover tubal ligation performed post-partum in their family planning programs, with Georgia noting that pregnant women are not enrolled in the state’s family planning waiver.
Although vasectomy is not a required benefit, all but two of the surveyed states covered this service for men. The District of Columbia and Hawaii, do not provide the benefit in their ACA Medicaid expansion programs. In Michigan, Missouri, Wyoming, Georgia and Maryland, only women are enrolled in their family planning waivers so they didn’t cover vasectomies. Ohio’s’ family planning SPA included men, but also did not cover vasectomies.
In the survey, three states noted utilization controls. North Carolina noted that only one procedure is allowed per lifetime. Kentucky requires prior authorization for vasectomies. Alabama will not pay for family planning services after a sterilization procedure has been conducted and also requires prior authorization for Essure.
Table 13: Number of States Covering Sterilization Procedures, by Type of Program
Procedure
Traditional Medicaid(n=41)
Family Planning Waiver/SPA(n=23)
ACA Medicaid Expansion(n=25)
Tubal Ligation Post-Partum
41
17
Required
Tubal Ligation General
41
21
Required
Essure: Non-surgical
41
19
Required
Vasectomy
41
17
23
Fertility Services
Key Finding: Fertility Services
No state covers fertility treatments for either women or men. Some states cover diagnostic testing related to fertility, although some restrict the test for medical reasons other than for fertility.
There are no federal requirements for state Medicaid programs to cover fertility testing or treatment such as medications, intrauterine insemination, or in-vitro fertilization for individuals enrolled in Medicaid. States may cover diagnostic services to detect the underlying medical reasons for infertility.
States were asked about diagnostic testing for both women (laparoscopy) and men (semen analysis). Nine of the 41 responding states cover fertility testing for women and men in their traditional Medicaid program as do 6 of the 25 responding ACA expansion states (Table 14). Just 3 of 23 states cover testing for women (Maryland, Minnesota, Oklahoma) and men (Alabama, Maryland, Minnesota) under a family planning waiver or SPA. Overall, five states provide the coverage for both genders in all of their eligibility pathways: Arkansas, Hawaii, Massachusetts, Maryland, and Nebraska. Notably, Nebraska is the only state that indicated it provides women with medication such as clomid and hCG, but only when infertility is a symptom of a separate medical problem. Appendix Tables A7 and A8 detail fertility testing policies for women and men.
Table 14: Fertility Testing and Services in State Medicaid Programs, by Type of Program
Traditional Medicaid(n=41)
ACA Medicaid Expansion(n=25)
Family Planning Waiver/SPA(n=23)
Diagnostic Testing for Women
9
6
3
Diagnostic Testing for Men
9
6
3
Medications for women (Clomid, hCG)
1
1
0
Intrauterine Insemination
0
0
0
In-vitro Fertilization
0
0
0
Family Planning Support Services
Key Finding: Family Planning Support Services
There is broad coverage for some family planning-related services such as counseling and well woman visits, but considerably fewer states reported they cover screenings for intimate partner violence.
Family planning services are an integral component of comprehensive primary, preventive, and sexual health care. The survey asked states about their coverage policies for family planning support services including contraceptive counseling, contraceptive follow-up and side effects management, well woman visits and check-ups, and intimate partner violence (IPV) screening. Nearly all states indicated that they cover support services, but this varied across eligibility pathways (coverage is required for ACA expansion programs), and some states indicated the service is not separately reimbursable, but is a component of some other type of office visit.
Coverage across Eligibility Pathways
Six states noted that contraceptive counseling is provided as a component of an office visit and is not separately reimbursable: Alaska, Alabama, Connecticut, Washington and West Virginia indicated the service is a component of a clinic or office visit and Georgia noted the service is a component of a family planning visit. In 2012, Illinois implemented a special initiative to pay an enhanced rate for family planning counseling services to select providers that have a family planning focus.
Coverage varied considerably across eligibility pathways for IPV screening (Table 15). Of the responding states with a family planning waiver or SPA, 16 out of 23 cover IPV screening. Nine states noted that intimate partner violence screening would be included in the context of other types of office visits or services. Maryland, Missouri, NewMexico, Virginia and Wyoming do not cover IPV screening in either their family planning waiver/SPA or in their traditional Medicaid program.
Limitations and Utilization Controls
A few states reported utilization controls for family planning support services. North Carolina allows one annual visit and six follow up exams for contraceptive counseling and follow up in its family planning waiver. Well woman visits are limited to one annual exam per year and IPV screening is left to the discretion of the provider. Alabama allows one initial visit, one annual visit and four periodic visits for contraceptive side effects management and for well woman visits. Contraceptive counseling is considered a component of these visits. The state also covers IPV screening for family planning waiver recipients receiving care coordination (not available under traditional Medicaid). Ohio provides one well woman or checkup visit per year.
Table 15: Coverage for Family Planning Services
Traditional Medicaid(n=41)
Family Planning Waiver/SPA(n=23)
Covered as a componentof an office visit or other service
Not Covered in Either Program
Contraceptive Counseling
40
22
6
MD
Follow-up Visit/Side Effects Management
41
22
1
Well Woman Visits/Check-ups
41
22
4
Intimate Partner Violence Screening
35
16
9*
MD, MO, NM, VA, WY
NOTES: *West Virginia’s Right from the Start program assesses each prenatal and infant client for partner or household violence. The state requires that the screening happen once, but the Designated Care Coordinator (DCC) is free to complete the assessment for partner violence at any time it is felt necessary. Service is billed under care coordination. The state also noted that screening is a component of a mental health assessment.Alabama provides screening under its care coordination benefit for family planning recipients.Oregon provides the service in its family planning waiver in the context of a contraceptive management visit. Connecticut, Illinois, Michigan, Montana, and Washington report that the service is provided with a clinic or routine office visit. Georgia noted the service is a component of a family planning visit.
Cervical And Breast Cancer Services
The survey asked states about their policies with respect to coverage of services for cervical and breast cancers under their traditional programs and family planning expansion programs. These include the HPV vaccine, pap smear and follow up testing after abnormal laboratory results, mammograms, genetic (BRCA) screening for high-risk women, and breast cancer preventive medication for high-risk women. These services are required coverage for the ACA expansion group as they are recommended by the US Preventive Services Task Force.
Cervical Cancer Services – PAP Test and Follow Up, HPV Vaccine
Key Finding: Cervical Cancer Services
All states cover Pap screening for cervical cancer regardless of eligibility pathway, but follow-up tests for abnormal screening results are less likely to be covered in state family planning waivers or SPAs. Of the states that do provide coverage, many indicate that the procedures or services are covered as part of a family planning visit under a family planning waiver or SPA, rather than as a specific benefit.
The survey inquired about coverage of pap and lab testing as well as additional screening procedures subsequent to an abnormal result from the pap test. These procedures include:
Colposcopy is a procedure to examine the cervix following abnormal pap smear results. The procedure may include extracting a small sample of tissue (biopsy) during the examination.
LEEP, Loop Electrosurgical Excision Procedure, is a treatment for abnormal cells on the cervix, using a thin wire loop that has an electric current to remove the abnormal tissue. LEEP may be performed after abnormal cells are discovered during a pap test, colposcopy or biopsy.
HPV DNA testing consists of using one of various biologic tests on a sample of tissue to detect the presence of DNA or RNA from the human papilloma virus.
Coverage across Eligibility Pathways
All of the states responding to the survey provide coverage for pap smear and lab in all three Medicaid pathways. All states participating in the survey cover the three follow-up screening methods in their traditional Medicaid and ACA Medicaid expansion programs, except North Carolina, which does not cover HPV DNA testing through any Medicaid pathway offered in the state. Coverage of the three follow-up screening methods varies more in state family planning programs (Table 16). Five states do not cover any of the three follow-up procedures in their family planning waiver or SPA: NorthCarolina, Oklahoma, Oregon, Virginia and Washington. Four states cover HPV DNA testing within their family planning waiver or SPA, but do not cover colposcopy or LEEP: Alabama, Michigan, SouthCarolina and Wyoming. Missouri covers colposcopy and HPV DNA testing, but does not cover LEEP.
All but one state (South Carolina) cover HPV vaccines for young adults in their traditional Medicaid programs, but only 14 of 23 states cover HPV vaccines in their family planning waiver or SPA despite the widespread coverage for pap screening. States must cover the vaccine for ACA expansion groups, as all vaccines recommended by the national Advisory Committee on Immunization Practices (ACIP) are included in the ACA’s preventive services coverage requirement.
Utilization Controls
Only two states noted utilization controls for cancer screening methods. California restricts utilization to women ages 21 through 65 regardless of sexual history. Colorado limits a pap smear and lab to one per year unless additional screens are determined to be medically necessary.
23: AL, CA, CT, GA, IA, IN, MD, MI, MN, MO, MS, MT, NC, NH, NM, NY, OH, OK, OR, SC, VA, WA, WY
CA, IA*, MO, OR*, VA
Follow- up Procedures with Abnormal Pap
Colposcopy
41
24
14: CA, CT, GA, IA, IN, MD, MN, MO, MS, MT, NH, NM, NY, OH
IA*, MO
LEEP
41
24
13: CA, CT, GA, IA, IN, MD, MN, MS, MT, NH, NM, NY, OH
HPV DNA Testing
40ǂ
Required
18: AL, CA, CT, GA, IA, IN, MD, MI, MN, MO, MS, MT, NH, NM, NY, OH, SC, WY
MO
Note: † Not covered in SC. ǂ Not covered in NC. *IA: sometimes considered family planning, depending on context of the visit. OR: Pap covered under state family planning waiver when provided in context of a contraceptive management visit.
Breast Cancer Services
Key Finding: Breast Cancer Services
Breast cancer screening is a required benefit in ACA Medicaid expansion programs, but it is considered “optional” under traditional Medicaid; however, all states covered this screening under these two programs.
Few states cover breast cancer screening and prevention services through their family planning waiver or SPA.
The USPSTF recommends three services for women related to detection and prevention of breast cancer: 1) biannual mammograms for women ages 50 to 74 to screen for breast cancer; 2) genetic testing for mutation of the BRCA1 and BRCA2 genes in some women with family members that have breast, ovarian, fallopian tube, or peritoneal cancer; 3) preventive medication for some women with elevated risk of breast cancer. Because these services are all recommended by the USPSTF, they must be covered in Medicaid ACA expansion programs but are not required in traditional or family planning pathways.
Minnesota, Montana, NewHampshire, and NewMexico cover all three services across all of their eligibility pathways. Thirty-three states and DC cover all of these services under traditional Medicaid (Figure 3). All states cover mammograms, and most cover genetic BRCA screening (37 of 41 states), and breast cancer preventive medication (36 of 41 states) for high-risk women under their traditional Medicaid program (Table 17). Maine and South Carolina do not cover BRCA Screening/Counseling nor breast cancer preventive medication in any of the pathways where coverage for these services is optional.
Figure 3: Traditional Medicaid Coverage of Preventative Breast Cancer Services
Coverage of breast cancer screening and prevention under state family planning waivers or SPAs is much less common, with seven of 23 of these programs covering mammograms (Maryland, Minnesota, Montana, NewHampshire, and NewMexico, Ohio, SouthCarolina) and six states covering BRCA screening and counseling (Minnesota, Montana, NewHampshire, and NewMexicoMaryland, Iowa) or preventive breast cancer medication (Minnesota, Montana, NewHampshire, and NewMexico, Ohio, Iowa).
Utilization Controls
No states noted utilization controls for mammograms. Five states have utilization controls applied to BRCA screening and counseling. Michigan, Texas, Vermont and Washington require prior authorization and in Nevada, genetic counseling must precede the testing. Michigan requires prior authorization for preventive medications. Appendix Table A9 provides detail for state responses on breast cancer services.
Table 17: Coverage for Breast Cancer Screening and Prevention
Traditional Medicaid(n=41)
ACA Medicaid Expansion(n=25)
Family Planning Waiver/SPA(n=23)
Mammogram
41
Required
7
Genetic (BRCA) Screening and Counseling for High-Risk Women
37
Required
6
Breast Cancer Preventive Medication for High-Risk Women
36
Required
6
Managed Care And Family Planning Services
Key Finding: Managed Care and Family Planning Services
Most of the responding states have capitated contracts that include family planning in the capitation rate. Just over one-third of these states explicitly address potential utilization controls on family planning services in the contracts.
Managed care is now the predominant delivery system for Medicaid in most states. Over three in four women of reproductive age covered by Medicaid are enrolled in managed care arrangements.14
For MCO enrollees, ensuring that federal family planning requirements are met can present special challenges. For example, while MCOs typically limit beneficiaries to a contracted network of providers, in the case of family planning this is not allowed under the federal “freedom of choice” policy. Beneficiaries are entitled to see any Medicaid provider for family planning care, but may not be aware of this right. Some providers have also reported difficulty receiving reimbursement if they are not part of an MCO network. In capitated arrangements, it can also be difficult to know whether the state is obtaining the higher 90% matching rate applicable to family planning services. This survey included questions that explore the role of capitated MCOs in providing family planning services to women enrolled in Medicaid.
Of the 41 states responding to this survey, 31 reported contracting with capitated MCOs and 29 of these states indicated that family planning supplies and services are always included within the MCO capitation rate (Table 18). Two additional states, New York and Texas, indicated that some or all family planning services are carved-out of MCO contracts only but for MCOs claiming a “conscience” or religious exemption from the requirement to provide family planning services.
Twenty-five of the 31 responding states with MCOs reported that they claimed the higher 90 percent federal matching rate (“FMAP”) for family planning services provided through the MCO while five states15 indicated that they did not.
Table 18: State Reporting on Capitated MCO Contracts
Yes
No
State has capitated MCO contracts? (N=41)
31
10
State include family planning within capitation rates? (N=31)
29 – Always2 – Sometimes
State claims 90% FMAP for family planning services provided through an MCO? (N=31)
25
6*
MCO states contract with MCO with religious exemption? (N= 31)
4
27
MCO contract addresses family planning utilization controls? (N=31)
11
20
* South Carolina was in the process of claiming 90% FMAP
In addition to New York and Texas, only two other states (California and Oregon) reported having contracts with MCOs having a conscience or religious exemption from the requirement to provide family planning services. Only California reported having a referral process for enrollees in these plans, requiring the MCO to arrange for the timely referral and coordination of family planning services and to demonstrate the ability to arrange, coordinate and ensure provision of services through referrals at no additional expense to the state. The MCO is also required to identify these services in its Member Services Guide.
Key Finding: Faith-Based Plans
California and New York, states with the most beneficiaries, also contract with faith-based plans that oppose some forms of contraception. While California reported that they have a process in place for referral for family planning services for the beneficiaries in these plans, New York did not report a referral practice.
States were also asked whether their contracts with MCOs explicitly address how MCOs can use prior authorization, step therapy or other medical management controls for contraceptives. Eleven of the 31 of the responding states with MCO contracts answered “Yes.” Of these, three states (Illinois, Massachusetts and Texas) indicated that their MCO contracts prohibit prior authorization requirements for contraceptives and Arizona reported that MCOs are “not allowed to create barriers to contraceptive utilization.” Conversely, Maryland indicated that prior authorization and quantity limitations are permitted and Delaware reported that MCOs are required to follow the state’s preferred drug list, which includes contraceptive agents. Three states (Illinois, Maryland and New Mexico) said that MCOs are required to cover all FDA-approved contraceptives. AppendixTable A10 provides additional detail for state managed care policies.
Conclusion
Conclusion
The analysis of state responses to this survey found that overall most states cover a broad range of prescription contraceptive methods in their full scope traditional Medicaid program, their full scope ACA Medicaid expansion, and the family planning expansion programs. Thirty-six of 41 surveyed states report that they cover all prescription contraceptives for women through their full scope programs. While states are not required to cover all methods under all pathways, most do. However, there is more variation between and within states for coverage of over-the-counter contraceptives, including condoms and Plan B emergency contraception pills. In some cases, when states provide coverage, it is only with a prescription which can limit access to these safe and effective methods.
Under traditional Medicaid, many screening and preventive services that are considered family planning “related services”, such as screening for partner violence and preventive therapies for breast cancer for women at elevated risk are optional. While coverage is provided for many women who qualify for the full scope pathways (traditional Medicaid or ACA expansion), coverage is less consistent for women who qualify for family planning expansions programs (SPA or Waiver). These are services that often allow providers to address underlying health and personal issues that affect sexual and reproductive health for women and men; limited reimbursement options mean that many will not get these services because providers do not have a way to charge for this care. This is not an issue that is unique to family planning and has long plagued the health care system for a broad array of preventive health care issues.16
The survey also finds that several states are actively working to promote access to LARC contraception methods. Most states provided coverage for the different types of IUDs that are available under all of their pathways and without utilization limits such as prior authorization or step therapy. Use of LARCs has increased significantly in recent years and the provider community has been encouraging greater use. Most recently, the American College of Obstetricians and Gynecologists endorsed broader provision of LARC methods postpartum.17
However, there are a number of financial and administrative disincentives that have made it challenging for clinicians to facilitate access to LARCs for women who want them. Policies including the integration of the cost of postpartum LARC insertion with the global maternity fee, low reimbursement levels, and administrative requirements can make it difficult for providers to retain a stock of IUDs. Given that Medicaid finances roughly half all birth in the US, state Medicaid policy on reimbursement of post-partum LARCs has the potential to broaden access to these effective methods for women who desire them. An April 2016 bulletin from CMS outlines a number of options for states to facilitate the use of post-partum LARC, including: increasing reimbursement, unbundling post-partum LARC insertion from the typical maternity care global fee, reducing administrative and logistical barriers to stocking IUDs, and providing them the same day a patient visits her provider.18 The survey finds that a number of states are providing payment separate from the maternity fee for postpartum LARCs, a change that has likely taken place in recent years as documented by other research.19
Medicaid enrollment has risen significantly since the ACA’s passage and could further increase if all states take up the ACA option to expand the program to all individuals living below 138% of the poverty level. Short of that, some of the states that have chosen not to expand full scope Medicaid have opted to establish family planning programs through Medicaid waivers or SPAs. These programs offer access to some family planning services, particularly contraceptives, but often not to the same degree as full scope Medicaid. Access to the full range of contraceptive methods as well as related family planning services has become a standard of comprehensive health care for women and men in their reproductive years.20 As enrollment in the Medicaid program continues to grow as a result of the ACA, coverage of family planning services under Medicaid will continue to be a significant force in shaping access to sexual and reproductive health services for low-income women and men in years to come.
Gold, RB. “Doing More for Less: Study Says State Medicaid Family Planning Expansions Are Cost-Effective.” Guttmacher Report on Public Policy, March 2004. ↩︎
Cooper, C., et al. Interpregnancy Intervals in the United States: Data From the Birth Certificate and the National Survey of Family Growth, National Vital Statistics Reports, April 16, 2015. ↩︎
All Patient Refined Diagnosis Related Group. Currently three major versions of the DRG in use include: basic DRGs, All Patient DRGs, and All Patient Refined DRGs. DRGs, used by Medicare, measure the typical resource use of an inpatient stay. AP-DRGs are similar to DRGs, but also include a more detailed DRG breakdown for non-Medicare patients such as newborns and children. The APR-DRG structure is similar to AP-DRG, but also measures severity of illness and risk of mortality in addition to resource utilization. See: Jason Shafrin; What is the Difference Between DRGs, AP-DRGs and APR-DRGs; Healthcare Economist; June 2012; accessed at: http://healthcare-economist.com/2012/06/19/what-is-the-difference-between-drgs-ap-drgs-and-apr-drgs/↩︎
This survey was conducted prior to California’s implementation of policy requiring Medicaid plans to cover 12 month supply of oral contraceptives. ↩︎
Plan B, progestin, brand names include Plan B One Step, Next Choice One Dose, My Way and Take Action. ↩︎
In Indiana, contraceptive drugs and supplies may be administered, dispensed, prescribed, or ordered. However, for a pharmacy provider to be reimbursed for over-the counter external contraceptive supplies, a Medicaid practitioner with prescriptive authority must prescribe them. IHCP Bulletin BT201301; January 8, 2013 accessed at: http://provider.indianamedicaid.com/ihcp/Bulletins/BT201301.pdf. ↩︎
Average Annual Workplace Family Health Premiums Rise Modest 3% to $18,142 in 2016; More Workers Enroll in High-Deductible Plans With Savings Option Over Past Two Years
Average Deductible Rises 12% to $1,478 Annually for Covered Workers Who Have Them; At Small Firms, Average Deductibles Now Top $2,000
Few Employers Report Changing Workers’ Hours Due to ACA’s Employer Requirements; Those That Do Are More Likely to Shift Workers to Full-Time Status
Menlo Park, Calif. – Annual family premiums for employer-sponsored health insurance rose an average of 3 percent to $18,142 this year, a modest increase at a time when workers’ wages (2.5%) and inflation (1.1%) also grew modestly, according to the benchmark Kaiser Family Foundation/Health Research & Educational Trust (HRET) 2016 Employer Health Benefits Survey released today. Workers on average contribute $5,277 annually toward their family premiums.
This year’s low family premium increase is similar to last year’s (4%) and reflects a significant slowdown over the past 15 years. Since 2011, average family premiums have increased 20 percent, more slowly than the previous five years (31% increase from 2006 and 2011) and more slowly than the five years before that (63% from 2001 to 2006).
“We’re seeing premiums rising at historically slow rates, which helps workers and employers alike, but it’s made possible in part by the more rapid rise in the deductibles workers must pay,” KFF President and CEO Drew Altman said.
The recent trend in part reflects covered workers moving into high-deductible plans compatible with Health Savings Accounts (HSAs) or tied to Health Reimbursement Arrangements (HRAs). These plans have lower average premiums than other plan types.
In 2016, 29 percent of all workers were in such plans, up from 20 percent in 2014, while a shrinking share of workers (48% in 2016, down from 58% in 2014) are enrolled in Preferred Provider Organization (PPO) plans, which have higher-than-average premiums. These shifts effectively reduced the average premium increase by half a percentage point in each of the past two years, the analysis shows.
Again, partly as a result of this trend, the survey finds average deductibles continuing to rise for covered workers. In 2016, 83 percent of covered workers face a deductible for single coverage, which averages $1,478. That’s up $159 or 12 percent from 2015, and $486 or 49 percent since 2011. The average deductible for workers who face one is higher for workers in small firms (three to 199 employers) than in large firms ($2,069 vs. $1,238).
For the first time, the survey also finds half (51%) of all covered workers face deductibles of at least $1,000 annually for single coverage. This includes two thirds (65%) of workers at small firms (three-199 workers), who typically face higher deductibles than workers at large firms (200 or more workers).
In some cases, employers make contributions to tax-preferred HSAs or HRAs, which workers can use to pay part or all of their deductible expenses, thereby reducing their effective deductible. Counting employer contributions this way would reduce the share of covered workers with deductibles of at least $1,000 to 38 percent.
The 18th annual Kaiser/HRET survey of more than 1,900 small and large employers provides a detailed picture of the status and trends in employer-sponsored health insurance, costs, and coverage. In addition to the full report and summary of findings released today, the journal Health Affairs is publishing a Web First article with select findings, and the Foundation is releasing an updated interactive graphic that charts the survey’s premium trends for different groups, including by firm size, region, and industry.
“The importance of this study is its ability to inform decision makers from all sectors as new or emerging strategies for health care coverage are being constructed. This is especially helpful for consumers as they understand health plan structures and what it means for them,” said Dr. Ken Anderson, HRET’s chief operating officer.
This year, the Affordable Care Act provision requiring employers with at least 50 full-time equivalent employees to offer health benefits to full-time workers or pay a penalty took full effect. The survey finds 93 percent of firms with at least 50 employees offer health benefits to at least some employees, and the vast majority say their coverage meets the ACA’s requirements for value and affordability.
The survey also finds little evidence that businesses are reducing workers’ hours to avoid the law’s requirements to offer coverage. In fact, more employers with 50 or more full-time equivalent workers who offer coverage say they shifted or plan to shift workers’ hours from part-time to full-time status to make them eligible for health benefits (7%) than say they shifted or plan to shift workers from full-time to part-time status to make them ineligible (2%).
Overall 56 percent of employers offer health benefits to at least some of their workers this year, statistically unchanged from 57 percent last year. Offer rates vary by firm size, with less than half (46%) of the smallest firms (three to nine workers) offering coverage and essentially all employers with at least 1,000 workers doing so. Since 2011, the share of firms with 10 to 49 workers who offer coverage has fallen from 74 percent to 66 percent.
This year’s survey finds that while most employers who provide health benefits offer coverage to workers’ spouses, some employers are using a number of strategies that can limit workers and their spouses from enrolling in coverage when other options are available. For example:
Among employers that offer spousal coverage, 13 percent of small firms and 5 percent of large ones do not allow a worker’s spouse to enroll in coverage if their spouse is offered coverage from another source. An additional 5 percent of small firms and 8 percent of large ones only allow enrollment under certain conditions. In addition, 12 percent of firms require spouses with other coverage options to pay higher premiums or cost-sharing than other spouses;
10 percent of all offering firms give additional compensation to workers who enroll in their spouse’s health plan instead of the company’s plan. This share is similar for large and small firms.
Among firms offering family coverage, 45 percent of small businesses and 18 percent of larger ones contribute the same dollar amount towards premiums for workers whether they enroll their dependents or not. This in effect requires workers to pay the full costs of enrolling their dependents.
“Particularly for workers at small firms, these limitations and incentives can create challenges for low-income workers to afford health coverage for their families,” said study lead author Gary Claxton, a Foundation vice president and director of the Health Care Marketplace Project.
Other findings from the survey include:
Single Premiums. Premiums for single coverage now average $6,435 annually, of which workers contribute $1,129 on average.
Cadillac tax. The survey provides an updated look at employers’ response to the Affordable Care Act’s excise tax on high-cost health plans, sometimes called the “Cadillac tax,” which is now scheduled to take effect in 2020. Nearly two thirds (64%) of large employers offering health benefits say that they conducted an analysis to determine if any of their plans would exceed the Cadillac tax thresholds, and a quarter (27%) of this group say their largest plan would do so. In addition, 15 percent say they have increased their plan’s cost-sharing to avoid reaching the excise tax thresholds, and 9 percent say they switched to a lower-cost health plan.
Health risk assessments. Most large firms offering health benefits (59%) offer to give workers a health risk assessment that asks questions about their medical history, health status, and lifestyle. Of those that do, most (54%) offer financial incentives to encourage workers to complete the assessment, such as reduced premiums or cost-sharing; eligibility for other wellness benefits; or cash, contributions to an HSA, or merchandise.
Biometric screenings. As with health risk assessments, most large firms offering health benefits (53%) offer workers biometric screenings, which are health examinations that measure such things as body weight, cholesterol, blood pressure, stress, and nutrition. Most (59%) of these firms offer financial incentives for undergoing the screenings, and some (14%) tie the incentives to meeting specific outcomes such as a targeted body mass index (BMI) or cholesterol level.
Methodology
The annual survey is a joint project of the Kaiser Family Foundation and the Health Research & Educational Trust. The survey was conducted between January and June of 2016 and included 3,110 randomly selected, non-federal public and private firms with three or more employees (including 1,933 that responded to the full survey and 1,177 others that responded to a single question about offering coverage). A research team at Kaiser, HRET and NORC at the University of Chicago, led by Kaiser vice president and long-time project director Gary Claxton, designed, conducted and analyzed the survey. For more information on the survey methodology, please visit the Survey Design and Methods Section.
Founded in 1944, the Health Research & Educational Trust (HRET) is a private, not-for-profit organization involved in research, education, and demonstration programs addressing health management and policy issues. An affiliate of the American Hospital Association (AHA), HRET collaborates with health care, government, academic, business, and community organizations across the United States to conduct research and disseminate findings that shape the future of health care. For more information about HRET, visit http://www.hret.org.
Health Affairs is the leading journal at the intersection of health, health care, and policy. Published by Project HOPE, the peer-reviewed journal appears each month in print, with frequent Web First studies and health policy briefs published at www.healthaffairs.org. The full text of each Health Affairs Web First paper is available free of charge to all website visitors for a one-week period following posting; it then switches to pay-per-view for nonsubscribers. You can also find the journal on Facebook and Twitter. Read daily perspectives on Health Affairs Blog. Download our podcasts, including monthly Narrative Matters essays, on iTunes. Tap into Health Affairs content with the iPad app.
The recent release of 2015 information from the Insurance Component of the Medical Expenditure Panel Survey (MEPS-IC) shows continuation of the fairly long-term decline in the share of private-sector workers in small firms that are offered coverage and that receive coverage at their job. This is part of a larger, long-term trend that shows a decline among all private-sector workers in the percentage who are covered by their own employer. While many of these workers are able to find coverage from other sources, such as coverage as a dependent through a spouse or through a public program, the decline is a concern because employer-based coverage is by far the largest source of coverage in the U.S., and its diminishing reliability puts more workers at risk of being left without a source of coverage. Workers who are not offered coverage at their job in general are more likely to be uninsured than workers who are. Among workers aged 18 to 64 at private industries, 28 percent of workers without an offer of employer sponsored insurance (ESI) were uninsured compared to only 4 percent of workers with an offer of ESI1 . Workers without an offer of ESI are natural beneficiaries of the new coverage options under the Affordable Care Act (ACA), and we find that the rate of uninsurance fell after 2013 among workers in smaller establishments not offered coverage at their job.
We use information from multiple years of the MEPS-IC to look at long-term trends in health insurance offer and enrollment rates in private sector establishments, broken out by size of firm. Although MEPS-IC surveys state and local government employers, we have limited this analysis to the private sector since a very large share of governments offer health benefits to their workers. It also is not possible to classify state and local government workers by “firm or establishment size” in the MEPS-IC with available public information. We also use the National Health Interview Survey (NHIS) to look at health insurance status over time. NHIS provides the most current coverage information and it permits us to differentiate workers based on whether or not they were offered coverage at their job. Beginning in 2001, NHIS contains information about the size of the establishment for workers (Generally, “establishment” refers to a business location, while “firm” refers to the whole enterprise and may include multiple locations. See Methods Box for difference between “firm” and “establishment”).
Overall, we find from the MEPS-IC that the percentage of workers in private-sector businesses who work in firms that offer health benefits and who are eligible for those benefits (“Share Offered”) has been falling for many years, as has the percentage of workers covered by health insurance in their own firm (“Share Covered”). These declines were particularly large for workers in firms with fewer than 50 employees. The NHIS shows that the uninsurance rate for workers in small establishments who are not offered health insurance at work has been consistent and high over many years, but fell when the new ACA coverage options were implemented in 2014. While an improvement in the insurance status for these workers, their rates of uninsurance remains considerably higher than those of workers in small establishments who are offered coverage at their job.
Offer and Coverage Rates and Trends
Of the almost 120 million private-sector employees in the U.S., not quite one-half (48%) are covered by health insurance offered by their employer in 2015, and this rate has been falling since MEPS-IC began collecting offer and coverage rates in 1996 (Table 1, Appendix). The share covered has two components: the share of workers in businesses that offer health insurance who enroll in that insurance, and the share of workers in businesses that do not offer health insurance to any of their workers. In 2015, about 84% of private-sector workers worked in a business that offered health insurance to at least some of the employees working at the firm, about three-quarters (76%) of those workers were eligible to enroll in the coverage, and of those eligible, three-quarters (75%) enrolled in the coverage. This means about 57% of private-sector workers in businesses offering coverage were covered at their job, and when combined with the 16% of workers in businesses not offering coverage to any workers, the overall coverage rate was about 48%. Most of these percentages have declined over time: between 2000 and 2015, the Share Offered fell from 71% to 64%, while the Share Covered fell from 57% to 48%. The Appendix table displays the complete annual trend in eligibility and enrollment for both all firms and small firms over the period from 1996 to 2015.
Table 1: Offer and Coverage Rates at All Private Employers
Year
Share of All Employees Who Work in Firms That Offer Health Insurance and Who are Eligible to Enroll
Share of All Employees Covered At Their Employer
2000
71%
57%
2005
68%
54%
2010
68%
52%
2015
64%
48%
SOURCE: Agency for Healthcare Research and Quality. Medical Expenditure Panel Survey Insurance Component Tables.
The declines have been more significant for workers in smaller firms (fewer than 50 employees at all locations). Between 2000 and 2015, the share of workers offered coverage fell from 53% to 38%, while the share covered by their own employer fell from 42% to 27% (Table 2, Appendix).
Table 2: Offer and Coverage Rates at Small Firms (Fewer than 50 Employees At All Locations)
Year
Share of All Employees Who Work in Firms That Offer Health Insurance and Who are Eligible to Enroll
Share of All Employees Covered At Their Employer
2000
53%
42%
2005
49%
37%
2010
45%
34%
2015
38%
27%
SOURCE: Agency for Healthcare Research and Quality. Medical Expenditure Panel Survey Insurance Component Tables.
As noted above, many workers who are not offered coverage at work are able to find alternate sources of coverage. We use the NHIS to look at the insurance status of these workers.
Effect of New Coverage Options
Employees not offered coverage at work have high rates of uninsurance; this is true for all workers and for workers in small establishments (Figure 1). Unfortunately, the NHIS statistics are reported for “establishments” of fewer than 50 workers, which is a more inclusive grouping than “firms of fewer than 50 workers” reported in MEPS-IC: a firm may have several smaller establishments (for example, a franchise with several small fast food restaurant locations). This means that the NHIS statistics include information for some workers in smaller establishments owned by larger firms as well as information about smaller firms. There are no alternative sources of data that would allow us to identify workers in smaller firms over the same period, so the establishment-size information in NHIS is the best approximation that we have. We excluded government workers from the analysis to more closely match the private-sector workers in the MEPS-IC statistics.
Figure 1: Among Private-Sector Workers Aged 18-64, Percent Uninsured by Health Insurance Offer Status and Establishment Size, 2001-2015
Figure 1 shows the rate of uninsurance among nongovernment workers age 18 to 64. For those not offered coverage at work, the uninsurance rate ranged between 43% and 51% between 2001 and 2013, before falling to 36% in 2014 and 28% in 2015. The uninsurance rate was much lower for those offered coverage at work, ranging between 6% and 8% between 2001 and 2013, before falling to 4% in 2015. The pattern is quite similar for workers in smaller establishments.
Not surprisingly, offers of health insurance are strongly tied to earnings: in 2015 workers offered coverage at work had average earnings of $53,960 while those without an offer had average earnings of just $23,245. The difference in 2010 (Pre-ACA) was $47,297 for workers offered coverage and $19,684 for those who were not. Looked at another way, only 42% of worker in the lowest earnings quartile (earnings below $23,400) in 2015 were offered coverage age work, compared with 92% of workers in the highest earnings quartile (earnings greater than $58,900).
We looked at the trends by type of coverage for workers not offered coverage at work to see how the new ACA coverage options were affecting this population (Figure 2). The ACA particularly benefits low and moderate income workers who are not offered employer-based coverage by providing income-related premium subsidies; it also expanded Medicaid coverage for low-income workers. After 2013, the uninsurance rate fell sharply for this group of workers, while coverage in both Medicaid and nongroup insurance increased. The same pattern holds for workers in smaller establishments not offered coverage at work (Figure 3). Even with these coverage improvements, however, workers not offered coverage at their job remain much more likely to be uninsured than those offered coverage at work.
Figure 2: Among Workers Not Offered Coverage at Work, Selected Health Insurance Coverage Types, 2001-2015Figure 3: Among Workers at Smaller Establishments Not Offered Coverage at Work, Selected Health Insurance Coverage Types, 2001-2015
Discussion
Private sector firms, particularly smaller firms, have been a diminishing source of coverage for their workers, with long-term decline in both the Share Offered and Shared Covered. Workers with lower earnings are particularly unlikely to be offered coverage at their job. While many workers who are not offered or covered at their job have other sources of coverage, such as dependent coverage through a spouse, the uninsurance rate for these workers has been high for many years. The new ACA coverage options have significantly improved coverage for this group, many of whom can benefit from the subsidized coverage made available in Marketplaces or Medicaid in states that have adopted the ACA coverage expansion. Despite these advances, however, the uninsurance rate for this group remains higher than the rate for workers offered coverage at work, suggesting that additional steps may need to be considered to improve the affordability of coverage for this population.
METHODS
This Insight relies on the Agency for Healthcare Research and Quality’s Medical Expenditure Panel Survey – Insurance Component (MEPS-IC) dataset for firm-level estimates of offers and take-up (enrollment) of ESI from the start of the survey in 1996 up until the most recent available estimates in 2015. Although MEPS-IC can be disaggregated by firm-level characteristics such as number of employees and private ownership, its publicly-available data do not include employee-level characteristics (such as worker age or non-ESI sources of health insurance coverage). In order to investigate the relationship between offers of ESI and workers’ uninsured rate, we used the Centers for Disease Control and Prevention (CDC)’s National Health Interview Survey (NHIS) microdata to examine coverage trends at the worker-level. Since nearly all Americans aged 65 or older are eligible for Medicare, we restricted our NHIS analyses of the uninsured rate to non-elderly workers at privately-held firms.
Between 2000 and 2001, NHIS altered the text of their workers’ place of employment size question from asking, ‘Thinking about this MAIN job or business, how many people are employed there full and part time, including employees at all locations?’ to instead asking the question ‘Thinking about {this MAIN job or business}, how many people work(ed) at this location? Note to FR: “People” includes both full- and part-time employees; “location” refers to the street address of the workplace.’ Starting in 2001, NHIS began collecting establishment size rather than firm size. For more detail about the difference between establishments and firms, see the US Census Bureau’s definition. Due to this change, we limited the NHIS component of our analysis to the period from 2001 to 2015.
Although this paper only presents NHIS statistics from establishments with fewer than fifty workers, we also examined the offer and take-up patterns of workers at establishments with fewer than twenty-five workers and found the trends to move in the same direction as workplaces with less than fifty employees.
NHIS has information about which member of a household is the policyholder for employer-sponsored coverage, and also asks workers that do not report employer-sponsored coverage whether or not they were offered coverage at work. We considered individuals who were working to have been offered coverage at their job if they were a policyholder of employer-sponsored coverage or if they said they were offered coverage at work but did not accept it.
The MEPS-IC tables provide information about the number of private sector employees, the percent of private sector employees in firms that offer health insurance, and the share of private sector employees in firms that offer health insurance who are eligible to enroll and who enroll. To derive the share of all private sector employees offered coverage, we multiply the number of employees in firms that offer health insurance by the share of employees at offering firms who are eligible to enroll themselves, and divide that number by the total number of employees. To derive the share of all private sector employees enrolled with their employer, we multiply the number of employees enrolled in firms that offer health insurance by the share of employees at offering firms who are eligible to enroll themselves and then divide that number by the total number of employees. We do this for all private sector employees and for employees in firms with fewer than 50 workers. By doing this, we do not have standard errors for the final statistics and cannot do statistical testing for the change over time.
We did test year-to-year changes in both the share of employees covered by firms that offer health benefits and also the share of employees that are eligible to enroll at firms that offer health benefits across the period from 1996-2015 for both all private firms and also firms with fewer than 50 employees. For all private sector workers and for private sector workers in firms with fewer than 50 workers, there were statistically significant declines for the 2000 to 2010 period and for the 2005 to 2015 period in (1) the percent of employees in establishments offering health insurance, (2) the percent of employees that are enrolled in health insurance among employees eligible for health insurance , and (3) the percent of employees that are enrolled in health insurance among employees of establishments offering health insurance.
Appendix
Appendix: Offer and Coverage Rates at Private Employers, 1996-2015
Year
Firms that Offer Health Insurance
All Firms
Small Firms (Fewer than 50 Employees At All Locations)
Percent of Employees Eligible for Health Insurance
Percent of Eligible Employees Enrolled in Health Insurance
Percent of Employees in Firms that Offer Health Insurance to Any Worker
Percent of Employees Eligible for Health Insurance
(“Share Offered”)
Percent of Employees Enrolled in Health Insurance
(“Share Covered”)
Percent of Employees in Firms that Offer Health Insurance to Any Worker
Percent of Employees Eligible for Health Insurance
(“Share Offered”)
Percent of Employees Enrolled in Health Insurance
(“Share Covered”)
1996
81%
86%
87%
70%
60%
62%
51%
42%
1997
79%
84%
86%
68%
57%
62%
50%
40%
1998
78%
85%
87%
68%
58%
65%
49%
39%
1999
79%
82%
89%
70%
58%
68%
53%
43%
2000
79%
81%
89%
71%
57%
68%
53%
42%
2001
78%
80%
89%
69%
55%
65%
50%
39%
2002
77%
81%
88%
68%
55%
64%
50%
39%
2003
79%
80%
87%
68%
55%
62%
48%
37%
2004
78%
80%
87%
68%
54%
61%
48%
38%
2005
79%
80%
87%
68%
54%
62%
49%
37%
2006
78%
78%
87%
67%
53%
61%
48%
37%
2008
78%
79%
88%
68%
54%
62%
48%
37%
2009
80%
77%
88%
70%
54%
60%
47%
36%
2010
78%
77%
87%
68%
52%
58%
45%
34%
2011
78%
76%
85%
67%
51%
55%
43%
32%
2012
78%
76%
85%
66%
50%
53%
41%
31%
2013
78%
75%
85%
66%
49%
53%
41%
30%
2014
75%
77%
83%
63%
48%
50%
39%
28%
2015
76%
75%
84%
64%
48%
48%
38%
27%
NOTES: 2007 data were not collected for the MEPS-ICSOURCE: Agency for Healthcare Research and Quality. Medical Expenditure Panel Survey Insurance Component Tables.
Endnotes
Kaiser Family Foundation Analysis of the National Health Interview Survey, 2015. ↩︎
This annual survey of employers provides a detailed look at trends in employer-sponsored health coverage including premiums, employee contributions, cost-sharing provisions, and employer opinions. The 2016 survey included more than 1,900 interviews with non-federal public and private firms. Annual premiums for employer-sponsored family health coverage reached $18,142 this year, up 3 percent from last year, with workers on average paying $5,277towards the cost of their coverage, according to the Kaiser Family Foundation/Health Research & Education Trust 2016 Employer Health Benefits Survey. The 2016 survey includes information on the use of incentives for employer wellness programs, plan cost-sharing as well as firm offer rate. Survey results are released here in a variety of ways, including a full report with downloadable tables on a variety of topics, summary of findings, and an article published in the journal Health Affairs.
NEWS RELEASE
A news release announcing the publication of the 2016 Employer Health Benefits Survey is available here.
SUMMARY OF FINDINGS
The Summary of Findings provides an overview of the 2016 survey results and is available under the Summary of Findingssection.
FULL REPORT
The complete Employer Health Benefits Survey Report includes over 200 exhibits and is available under the Report section. The Report section contains 14 separate sections. Users can view each section separately or download the section exhibits from the bottom of the respective section page.
On Wednesday, September 14, 2016, the Kaiser Family Foundation and the Health Research & Educational Trust (HRET) held a reporters-only web briefing to release the 2016 Employer Health Benefits Survey.
Over twenty overview slides from the 2016 Employer Health Benefits Survey are available as a slideshow or PDF.
ADDITIONAL RESOURCES
Standard errors for selected estimates are available in the Technical Supplement here.
Employer Health Benefits Surveys from 1998-2015 are available here. Please note that historic survey reports have not been revised with methodological changes.
Researchers may request for a public use dataset by going to Contact Us and choosing “TOPIC: Health Costs.”
Researchers at the Kaiser Family Foundation, NORC at the University of Chicago, and Health Research & Educational Trust designed and analyzed the survey.
Summary Of Findings
Employer-sponsored insurance covers over half of the non-elderly population; approximately 150 million nonelderly people in total.1 To provide current information about employer-sponsored health benefits, the Kaiser Family Foundation (Kaiser) and the Health Research & Educational Trust (HRET) conduct an annual survey of private and nonfederal public employers with three or more workers. This is the eighteenth Kaiser/HRET survey and reflects employer-sponsored health benefits in 2016.
HEALTH INSURANCE PREMIUMS AND WORKER CONTRIBUTIONS
In 2016, the average annual premiums for employer-sponsored health insurance are $6,435 for single coverage and $18,142 for family coverage. The average family premium rose 3% over the 2015 average premium while the increase in the premium for single coverage was not statistically significant. The average premium for family coverage is lower for covered workers in small firms (3-199 workers) than for workers in large firms (200 or more workers) ($17,546 vs. $18,395). Workers’ wages increased 2.5% and inflation increased 1.1% over the period.2 Premiums for family coverage have increased 20% since 2011 and 58% since 2006. Average premiums for high-deductible health plans with a savings option (HDHP/SOs) are considerably lower than the overall average for all plan types for both single and family coverage, at $5,762 and $16,737 respectively (Exhibit A). These premiums do not include any employer contributions to workers’ health savings accounts or health reimbursement arrangements. As discussed below, the share of covered workers with HDHP/SOs has grown eight percentage points over the last two years; this change in enrollment has reduced the growth in single and family premiums by roughly a half percentage point each of the last two years.3
Exhibit A: Average Annual Firm and Worker Premium Contributions and Total Premiums for Covered Workers for Single and Family Coverage, by Plan Type, 2016
Premiums vary significantly around the averages for both single and family coverage, reflecting differences in health care costs and compensation decisions across regions and industries. Seventeen percent of covered workers are in plans with an annual total premium for family coverage of at least $21,771 (120% or more of the average family premium), and 19% of covered workers are in plans where the family premium is less than $14,514 (less than 80% of the average family premium) (Exhibit B).
Exhibit B: Distribution of Annual Premiums for Single and Family Coverage Relative to the Average Annual Single or Family Premium, 2016
Most covered workers make a contribution towards the cost of the premium for their coverage. On average, covered workers contribute 18% of the premium for single coverage and 30% of the premium for family coverage, similar percentages to the recent past. Workers in small firms contribute a higher average percentage of the premium for family coverage (39% vs. 26%) than workers in large firms. Covered workers in firms with a relatively high percentage of lower-wage workers (at least 35% of workers earn $23,000 a year or less) contribute higher percentages of the premium for single (23% vs. 18%) and family (35% vs. 30%) coverage than workers in firms with a smaller share of lower-wage workers. As with total premiums, the share of the premium contributed by workers varies considerably. For single coverage, 12% of covered workers are in plans that do not require them to make a contribution, 62% are in plans which require a contribution of 25% or less of the total premium, and 2% are in plans that require a contribution of more than half of the premium. For family coverage, 3% of covered workers are in plans that do not require them to make a contribution, 45% are in a plan that requires a contribution of 25% or less of the total premium, and 15% are in plans that require more than half of the premium (Exhibit C). Covered workers in small firms are much more likely to be in a plan that requires the worker to contribute more than 50% of the total family premium than covered workers in larger firms (34% vs. 7%).
Exhibit C: Distribution of Percentage of Premium Paid by Covered Workers for Single and Family Coverage, by Firm Size, 2016
One reason for this variation is the different approaches that employers use to structure employee contributions, particularly for family coverage. Of firms that offer family coverage: 45% of small firms and 18% of large firms provide the same dollar contribution for single and family coverage, which means that employees must pay the full additional premium cost to enroll family members in their plan; 45% of small firms and 67% of large firms make a higher dollar contribution for family coverage than for single coverage, 3% of small firms and 6% of large firms vary their approach with the class of the employee; and the remaining 7% of small firms and 9% of large firms take some other approach. Fifteen percent of firms that offer health benefits require workers who use tobacco to contribute more towards the premium than those who do not use tobacco. Looking at the dollar amounts that workers contribute, the average annual premium contributions for 2016 are $1,129 for single coverage and $5,277 for family coverage. Covered workers’ average dollar contribution to family coverage has increased 78% since 2006 (Exhibit D) and 28% since 2011 (data not shown). Covered workers in small firms have lower average contributions for single coverage than workers in large firms ($1,021 vs. $1,176), but higher average contributions for family coverage ($6,597 vs. $4,719). Average contribution amounts for covered workers in HDHP/SOs are lower for single and family coverage than for covered workers in other plan types (Exhibit A).
Exhibit D: Average Annual Health Insurance Premiums and Worker Contributions for Family Coverage, 2006-2016
PLAN ENROLLMENT
PPOs continue to be the most common plan type in 2016, enrolling 48% of covered workers. Twenty-nine percent of covered workers are enrolled in a high-deductible plan with a savings option (HDHP/SO), 15% in an HMO, 9% in a POS plan, and less than 1% in a conventional (also known as an indemnity) plan. Over the last two years, enrollment in PPOs has fallen 10 percentage points while enrollment in HDHP/SOs has increased 8 percentage points (Exhibit E).4
Exhibit E: Percentage of Covered Workers Enrolled in an HDHP/HRA or HSA-Qualified HDHP, 2006-2016
Plan enrollment differs with firm size: 52% of covered workers in large firms are enrolled in PPOs, compared to 39% percent in small firms; 18% percent of covered workers in small firms are enrolled in POS plans, compared to 4% in large firms.
EMPLOYEE COST SHARING
Most covered workers must pay a share of the cost when they use health care services. Eighty-three percent of covered workers have a general annual deductible for single coverage that must be met before most services are paid for by the plan. Even workers without a general annual deductible often face other types of cost sharing when they use services, such as copayments or coinsurance for office visits and hospitalizations. Among covered workers with a general annual deductible, the average deductible amount for single coverage is $1,478, higher than the average deductible last year ($1,318). Among all covered workers, those enrolled at firms with a deductible and those without, the average deductible is $1,221, significantly more than $1,077 in 2015. The average deductible for covered workers is higher in small firms than in large firms ($2,069 vs. $1,238). Sixty-five percent of covered workers in small firms and 45% of covered workers in large firms are in a plan with a deductible of at least $1,000 for single coverage, similar to the percentages last year (Exhibit F); a similar pattern exists for those in plans with a deductible of at least $2,000 (41% for small firms vs. 16% for large firms).
Exhibit F: Percentage of Covered Workers Enrolled in a Plan with a General Annual Deductible of $1,000 or More for Single Coverage, By Firm Size, 2006-2016
Deductibles have increased in recent years due to higher deductible amounts within plan types (particularly PPO plans) and to higher enrollment in HDHP/SOs. While growing deductibles in PPOs and other plan types generally increases enrollee out-of-pocket liability, the shift in enrollment to HDHP/SOs does not necessarily do so because most HDHP/SO enrollees receive an account contribution from their employers, which in essence reduces the high cost sharing in these plans. Fourteen percent of covered workers in an HDHP with a Health Reimbursement Arrangement (HRA) and 7% of covered workers in a Health Savings Account (HSA)-qualified HDHP receive an account contribution for single coverage at least equal to their deductible, while another 47% of covered workers in an HDHP with an HRA and 28% of covered workers in an HSA-qualified HDHP receive account contributions that, if applied to their deductible, would reduce their deductible to less than $1,000. If we reduce the deductibles that workers face by employer account contributions, the percentage of covered workers with a deductible liability of $1,000 or more would be reduced from 51% to 38% (Exhibit G).
Exhibit G: Percentage of Covered Workers Enrolled in a Plan Where the Single Coverage Deductible and Out-of-Pocket Liability After HRA/HSA Contributions is $1,000 or More, 2009-2016
Whether they face a general annual deductible or not, a large share of covered workers also pay a portion of the cost when they visit a physician. For primary care, 67% of covered workers face a copayment (a fixed dollar amount) when they visit a doctor and 25% face coinsurance (a percentage of the covered amount). For specialty care, 66% face a copayment and 26% face coinsurance. The average in-network copayments are $24 for primary care and $38 for specialty care. The average in-network coinsurance is 18% for primary and 19% for specialty care. These amounts are similar to those in 2015. Most workers also face additional cost sharing for a hospital admission or an outpatient surgery episode. After any general annual deductible is met, 64% of covered workers have a coinsurance and 14% have a copayment for hospital admissions. Lower percentages have per day (per diem) payments (6%), a separate hospital deductible (1%), or both copayments and coinsurance (10%). The average coinsurance rate for hospital admissions is 19%. The average copayment is $282 per hospital admission, the average per diem charge is $281, and the average separate annual hospital deductible is $898. The cost sharing provisions for outpatient surgery follow a similar pattern to those for hospital admissions; most covered workers have either coinsurance (66%) or copayments (17%). For covered workers with cost sharing for outpatient surgery, the average coinsurance rate is 19% and the average copayment is $170. While almost all (98%) covered workers are in plans with a limit on in-network cost sharing (called an “out-of-pocket maximum”) for single coverage, there is considerable variation in the actual dollar limits. Fourteen percent of these workers are in a plan with an annual out-of-pocket maximum for single coverage of less than $2,000 while 18% are in a plan with an out-of-pocket maximum of $6,000 or more.
AVAILABILITY OF EMPLOYER-SPONSORED COVERAGE
Fifty-six percent of firms offer health benefits to at least some of their workers, similar overall to percentages in recent years (Exhibit H). The percentages of smaller firms (10 to 49 workers) offering coverage, however, has fallen since 2011 and years before. This trend precedes the ACA coverage expansions and is consistent with longer-term trends reported elsewhere.
Exhibit H: Percentage of Firms Offering Health Benefits, by Firm Size, 1999-2016
The likelihood of offering health benefits differs significantly by firm size, with only 46% of employers with 3 to 9 workers offering coverage while virtually all employers with 1,000 or more workers offer coverage. Eighty-nine percent of workers are in a firm that offers health benefits to at least some of its employees, similar to recent years. Even when firms do offer health benefits, not all of their workers are covered there. Some workers are not eligible to enroll (e.g., waiting periods or part-time or temporary work status) and others who are eligible choose not to enroll (e.g., they feel the coverage is too expensive or they are covered through another source). In firms that offer coverage, an average of 79% of workers are eligible for the health benefits offered by the firm, and of those eligible, 79% take up the firm’s offer, resulting in 62% of workers in offering firms having coverage through their employer. If we look across workers both in firms that offer and those that do not offer health benefits, 55% of workers are covered by health plans offered by their employer. All of these percentages are similar to 2015. Over the longer term, however, the percentage of workers in all firms covered by a health plan from their employer has fallen from 59% in 2006 and 58% in 2011 to 55% in 2016 (Exhibit I).
Exhibit I: Percentage of All Workers Covered by Their Employers’ Health Benefits, in Firms Both Offering and Not Offering Health Benefits, by Firm Size, 1999-2016
The Affordable Care Act (ACA) provision requiring employers with at least 50 full-time equivalent employees (FTEs) to offer health benefits that meet minimum standards for value and affordability to their full-time workers or pay a penalty took full effect in 2016. Ninety-seven percent of firms with at least 50 FTEs reported that they offer coverage to at least 95% of their employees who work on average 30 hours per week or more, and 96% responded that they offer at least one plan that met the ACA standards for affordability and minimum value. These firms were also asked about changes they planned to make or had made in the past year in response to the employer responsibility requirement. Two percent said they changed or planned to change the job classifications of some employees from full-time to part-time so that they would not be eligible for health benefits, while 7% said they changed or planned to change job classifications of some employees from part-time to full-time so that they would become eligible for health benefits. Other actions included 4% reducing or planning to reduce the number of full-time employees that they intended to hire because of the cost of providing health benefits to them, 2% increasing or planning to increase the waiting period before new employees become eligible for benefits, 12% extending or planning to extend eligibility for health benefits to workers who were not previously eligible, and 2% extending or planning to extend eligibility for more comprehensive benefits to employees previously eligible only for limited benefit plans. Coverage for Spouses and Unmarried Partners. Virtually all firms offering health benefits offer coverage for spouses, although 13% of small firms and 5% of large firms say that spouses are ineligible to enroll if a spouse is offered coverage from another source, and an additional 5% of small firms and 8% of large firms say that spouses offered coverage from other sources can enroll only under certain conditions. Twelve percent of firms offering coverage to spouses have a higher contribution or cost sharing for spouses who are eligible for coverage from another source, while 10% of firms offering coverage give additional compensation to employees who choose to enroll in their spouse’s plan. Two percent of firms offering coverage to spouses report that they made a significant reduction in the amount that they contributed for covering employees’ spouses during the last year. All of these percentages are similar for small and large firms. Among firms offering family coverage, 32% offer coverage to same-sex unmarried partners, with an additional 33% saying they do not know or have not encountered the situation. Large firms are more likely to offer coverage to same-sex unmarried partners than small firms (49% vs. 32%); small firms are much more likely to say they do not know or have not encountered the situation (34% vs. 5%). Twenty-seven percent of firms offering family coverage offer to unmarried opposite-sex partners, with an additional 28% saying that do know or have not encountered the situation. Large firms are more likely to offer coverage to unmarried opposite-sex partners than smaller firms (42% vs. 26%); small firms are more likely to report they do not know or have not encountered the situation (28% vs. 2%).
RETIREE COVERAGE
Of the large firms offering health benefits in 2016, 24% also offer health benefits to retirees, similar to the percentage in 2015 (23%). Among large firms that offer retiree health benefits, 92% offer health benefits to early retirees (workers retiring before age 65) and 72% offer health benefits to Medicare-age retirees. Six percent of large firms offering retiree benefits offer some retiree benefits through a corporate or private exchange, and 17% (down from 26% in 2015) report they are considering changing the way they offer retiree coverage because of the new health insurance exchanges established by the ACA.
WELLNESS, HEALTH RISK ASSESSMENTS AND BIOMETRIC SCREENINGS
Employers continue to show interest in programs that encourage employees to identify health issues and to take steps to improve their health (Exhibit J). A large share now offer health screening programs including health risk assessments, which are questionnaires asking employees about lifestyle, stress or physical health, and in-person examinations such as biometric screenings. Many employers have incentive programs that reward or penalize employees for completing assessments, participating in wellness programs, or meeting biometric outcomes. These survey questions on these topics were revised for 2016 and are asked only of firms offering health benefits. Because there was considerable uncertainty among small firms on some questions, particularly those related to incentives, findings are reported only for large firms in some instances.
Exhibit J: Among Large Firms (200 or more workers) Offering Health Benefits, Percentage of Firms Offering Incentives for Various Wellness and Health Promotion Activities, 2016
Health Risk Assessments. Among firms offering health benefits, 32% of small firms and 59% of large firms provide employees with an opportunity to complete a health risk assessment. A health risk assessment includes questions about a person’s medical history, health status, and lifestyle. Fifty-four percent of large firms with a health risk assessment program offer a financial incentive to encourage employees to complete the assessment. Among large firms with an incentive, the incentives include: lower premium contributions or cost sharing (51% of firms); requiring a completed health risk assessment to be eligible for other wellness incentives (44% of firms); and cash, contributions to health-related savings accounts, or merchandise (60% of firms). Biometric Screening. Twenty percent of small firms and 53% of large firms offering health benefits offer employees the opportunity to complete biometric screening. Biometric screening is a health examination that measures an employee’s risk factors such as body weight, cholesterol, blood pressure, stress, and nutrition. Fifty-nine percent of large firms with biometric screening programs offer employees an incentive to complete the screening. Among large firms with an incentive, the incentives include: lower premium contributions or cost sharing (52% of firms); requiring a completed biometric screening to be eligible for other wellness incentives (32% of firms); and cash, contributions to health-related savings accounts, or merchandise (56% of firms). In addition, 14% of large employers with biometric screening programs have financial incentives tied to whether or not employees met or were able to meet specified biometric outcomes, such as a targeted body mass index (BMI) or cholesterol level. Health and Wellness Promotion Programs. Many employers offer wellness or health promotion programs to help employees improve their health and avoid unhealthy behaviors. Forty-six percent of small firms and 83% of large firms offer a program in at least one of these areas: smoking cessation; weight management; behavioral or lifestyle coaching. Three percent of small firms and 16% of large firms report collecting health information from employees through wearable devices such as a Fitbit or Apple Watch. Forty-two percent of large firms with one of these health and wellness programs offer employees a financial incentive to participate in or complete the program. Among large firms with an incentive for completing wellness programs, incentives include: lower premium contributions or cost sharing (34% of firms); cash, contributions to health-related savings accounts, or merchandise (76% of firms); some other type of incentive (14% of firms). Some firms separate financial incentives for different programs and some others have incentives that require participation in more than one type of program (e.g., completing an assessment and participating in a health promotion activity). We asked firms that had any incentives for health risk assessments, biometric screening or the specified health and wellness promotion programs what the maximum financial incentive was for a worker for all of their programs combined. Among large firms with any type of incentive, 26% have a maximum financial incentive of less than $150, 35% have a maximum incentive between $150 and $500, 23% have a maximum incentive between $500 and $1,000, 9% have a maximum incentive between $1,000 and $2,000, and 7% have a maximum incentive of $2000 or more.
Sites of Care
Telemedicine. Thirty-nine percent of large firms that offer health benefits cover the provision of some health care services through telecommunication in their largest health plan. We revised our questions for 2016 to clarify that we were asking about payment for services and not just the electronic exchange of information. Among these firms, 33% reported that workers have a financial incentive to receive services through telemedicine as instead of visiting a physician’s office. Retail Health Clinics. Sixty percent of small firms and 73% of large firms cover services offering health benefits provided in retail health clinics, such as those found in pharmacies and supermarkets, in their largest health plan. Among large firms covering services in retail clinics, 10% reported that workers had a financial incentive to receive services in a retail clinic instead of visiting a traditional physician’s office. On-Site Health Clinics. Among firms with at least 50 employees offering health benefits, five percent provide health services to employees through an on-site health clinic in at least one of their major locations. Eighty-six percent of these firms provided some services for non-work-related illnesses through the on-site clinic. Firms with at least 1,000 workers were more likely to have an on-site health clinic than smaller firms (25% vs. 4%).
PROVIDER NETWORKS
High Performance or Tiered Networks. Fourteen percent of large firms offering health benefits have high performance or tiered networks in their largest health plan, down from 24% last year. These programs identify providers that are more efficient or have higher quality care, and may provide financial or other incentives for enrollees to use the selected providers. Narrow Networks. Seven percent of firms offering health benefits offer a health plan that they consider to have a narrow network (i.e., a network they would consider more restrictive than a standard HMO network), similar to the percentage reported last year. There is no difference between small and large firms on this measure. Six percent of firms reported that they or their insurer had eliminated a hospital or health system from any of their plans’ networks in order or reduce costs. There is no difference between small and large firms on this measure.
OTHER TOPICS
Self-Funding. Thirteen percent of covered workers in small firms and 82% in large firms are enrolled in plans that are either partially or completely self-funded, similar to last year. Overall, 61% of covered workers are enrolled in a plan that is either partially or completely self-funded. Private Exchanges. Four percent of firms offering health benefits with at least 50 employees offer health benefits through a private exchange. Private exchanges are arrangements, usually created by consultants, brokers or insurers, which allow employers to offer their employees a choice of different benefit options, often from different insurers. Among firms offering health benefits that do not currently offer through a private exchange, 18% with at least 50 workers, including 28% with at least 5,000 workers, say they have considered offering coverage through a private exchange. Professional Employment Organization. Some firms provide for health and other benefits by entering into a co-employment relationship with a Professional Employer Organization (PEO). Under this arrangement, the firm manages the day-to-day responsibilities of employees, but the PEO hires the employees and acts as the employer for insurance, benefits, and other administrative purposes. Four percent of small firms offering health benefits offer coverage through a PEO, similar to last year. Grandfathered Health Plans. The ACA exempts “grandfathered” health plans from a number of its provisions, such as the requirement to cover preventive benefits without cost sharing or the new rules for small employers’ premiums ratings and benefits. An employer-sponsored health plan can be grandfathered if it covered a worker when the ACA became law (March 23, 2010) and if the plan has not made significant changes that reduce benefits or increase employee costs.5 Twenty-three percent of firms offering health benefits offer at least one grandfathered health plan in 2016, down from 35% last year. Twenty-three percent of covered workers are enrolled in a grandfathered health plan, similar to the percentage in 2015.
EXCISE TAX ON HIGH-COST HEALTH PLANS
Under the ACA, employer health plans in 2020 will be subject to an excise tax of 40% on the amount by which their cost exceeds specified thresholds.6 The tax was scheduled to take effect in 2018, but its effective date was delayed two years. The tax is calculated with respect to each employee based on the combination of health benefits received by that employee, including the employer and employee share of health plan premiums and account contributions. Of firms offering health benefits, 15% of small firms and 64% of large firms say they have conducted an analysis to determine if they will exceed the thresholds, with 29% of the small firms and 27% of the large firms saying that their largest health plan would exceed the threshold in 2020. Some plans report planning or taking action in the last year in anticipation of the assessment: four percent of small firms and 15% of large firms increased cost sharing; three percent of small firms and nine percent of large firms switched to a lower cost plan or eliminated a plan option; three percent of small firms and eight percent of large firms moved benefit options to an account-based plan; and four percent of small firms and two percent of large firms selected a plan with a smaller network of providers.
CONCLUSION
This is the fifth straight year of relatively low premium growth (family coverage growing between 3 and 4 percentage points each year), but the stability for premiums belies some other changes that have occurred during the period. Deductibles continued to grow in 2016; over the last five years, the percentage of covered workers facing a general annual deductible has grown from 74% to 83%, while the average single deductible amount (among those facing a deductible) increased from $991 to $1,478. These higher deductibles likely contributed to the moderating premium increases over this period. The higher deductibles have resulted, in part, by growing enrollment in HDHP/SOs, where enrollment has gone from 17% of covered workers in 2011 to 29% in 2016. Just in the last two years, enrollment in HDHP/SOs has grown by eight percentage points while PPO enrollment has declined by ten. More enrollment in HDHP/SOs has several implications for costs: they have higher deductibles than other plan types, but many enrollees also receive contributions to their HSA or HRAs that offset some or all of the cost sharing; they have lower total premiums and worker contribution amounts, although contributions by employers toward enrollee HRAs and HSAs offset some of the impact of the lower premiums for employers. There has been a reduction in offering for firms with 10 to 49 workers over the period, decreasing from 74% in 2011 (and 76% in 2012) to 66% in 2016. This change precedes the introduction of public marketplaces and premium tax credits, and other sources show a longer term reduction in offer rates among small private firms. Across all workers (both in firms that offer and do not offer coverage) during the period, the percentage of workers with coverage from their own employer has fallen from 58% in 2011 to 55% in 2016. Employers, particularly larger ones who employ most workers, continue to show interest in programs to improve health and in new delivery options. Significant shares of small and large employers offer employees the opportunity to complete health risk assessments or biometric screening or to participate in lifestyle coaching or other health promotion programs; many large employers provide employees with financial incentives to complete assessments or participate in programs. Employers also are covering services through new venues, such as retail health clinics and telemedicine, sometimes providing financial incentives for employees to use these new options. Finally, the continuing implementation of the ACA does not appear to be causing major disruptions in employer market. The employer responsibility provision was fully implemented in 2016, with virtually all employers with 50 or more FTEs saying that they offer coverage to full-time employees that meets affordability and minimum value standards. Relatively few employers made changes to working hours or hiring as a result of the provision, with more taking actions that increased coverage offers than reducing them, similar to the results last year. Most large employers, but few small employers, have analyzed how the high cost plan tax will affect them when it takes effect in 2020, with about 12% of offering firms saying they have taken some action in response to the tax. Looking forward, there are several emerging issues to watch. One is growth of HDHO/SOs, which after a lull, have seen significant enrollment growth in the last two years. These plans have relatively high cost sharing, but as discussed above, some workers receive significant account contributions to offset some of these costs. Another issue is whether the share of smaller firms offering coverage continues to fall. These firms are not required to offer coverage under the ACA, and in some cases, their workers might have more affordable options in public marketplaces than through work, which could encourage employers to stop offering. And, while the high-cost plan excise tax has been delayed until 2020, a meaningful share of employers estimates that they will be subject to the assessment. Only small shares of firms have reacted so far, but this may accelerate over the next couple of years if the 2020 date remains in place.
METHODOLOGY
The Kaiser Family Foundation/Health Research & Educational Trust 2016 Annual Employer Health Benefits Survey (Kaiser/HRET) reports findings from a telephone survey of 1,933 randomly selected public and private employers with three or more workers. Researchers at the Health Research & Educational Trust, NORC at the University of Chicago, and the Kaiser Family Foundation designed and analyzed the survey. National Research, LLC conducted the fieldwork between January and June 2016. In 2016, the overall response rate is 40%, which includes firms that offer and do not offer health benefits. Among firms that offer health benefits, the survey’s response rate is also 40%. We asked all firms with which we made phone contact, even if the firm declined to participate in the survey: “Does your company offer a health insurance program as a benefit to any of your employees?” A total of 3,110 firms responded to this question (including the 1,933 who responded to the full survey and 1,177 who responded to this one question). Their responses are included in our estimates of the percentage of firms offering health benefits. The response rate for this question is 65%. Since firms are selected randomly, it is possible to extrapolate from the sample to national, regional, industry, and firm size estimates using statistical weights. In calculating weights, we first determine the basic weight, then apply a nonresponse adjustment, and finally apply a post-stratification adjustment. We use the U.S. Census Bureau’s Statistics of U.S. Businesses as the basis for the stratification and the post-stratification adjustment for firms in the private sector, and we use the Census of Governments as the basis for post-stratification for firms in the public sector. Some numbers in the report’s exhibits do not sum up to totals because of rounding effects, and, in a few cases, numbers from distribution exhibits referenced in the text may not add due to rounding effects. Unless otherwise noted, differences referred to in the text and exhibits use the 0.05 confidence level as the threshold for significance. For more information on the survey methodology, please visit the Methodology section at http://ehbs.kff.org/. The Kaiser Family Foundation, a leader in health policy analysis, health journalism and communication, is dedicated to filling the need for trusted, independent information on the major health issues facing our nation and its people. The Foundation is a non-profit private operating foundation based in Menlo Park, California. The Health Research & Educational Trust (HRET) Founded in 1944, the Health Research & Educational Trust (HRET) is the not-for-profit research and education affiliate of the American Hospital Association (AHA). HRET’s mission is to transform health care through research and education. HRET’s applied research seeks to create new knowledge, tools and assistance in improving the delivery of health care by providers and practitioners within the communities they serve.
Report: Section One: Cost Of Health Insurance
The average annual premiums in 2016 are $6,435 for single coverage and $18,142 for family coverage. The average family premiums increased approximately 3% since 2015. The average family premium has increased 58% since 2006 and 20% since 2011. The average family premium for covered workers in small firms (3-199 workers) ($17,546) is significantly lower than average family premiums for workers in large firms (200 or more workers) ($18,395).
Premium Costs for Single and Family Coverage
The average premium for single coverage in 2016 is $536 per month, or $6,435 per year. The average premium for family coverage is $1,512 per month or $18,142 per year 1.
The average annual premiums for covered workers in HDHP/SOs are lower for single ($5,762) and family coverage ($16,737) than the overall average premiums for covered workers. The average premiums for covered workers enrolled in PPO plans are higher for single ($6,800) and family coverage ($19,003) than the overall plan average 1.
The average annual premium for family coverage for covered workers in small firms ($17,546) is lower than the average premium for covered workers in large firms ($18,395) 2.
The average family premium for covered workers is lower in the South ($17,429) than the average premium for covered workers in all other regions 3.
The average single premium for covered workers employed in the retail industry ($5,807) is lower than the average premium for covered workers in all other industries. The average single premium for covered workers employed in the state/local government industry ($7,218) is higher than the average premium for covered workers in all other industries 4.
The average family premium for covered workers employed in the retail industry ($16,321) is lower than the average premium for covered workers in all other industries 4.
The average single premium for covered workers in firms with a larger share of younger workers (where 35% or more of the workers are age 26 or younger) is lower than the average premium for covered workers in firms with a lower share of younger workers ($6,047 vs. $6,472) 5.
The average family premium for covered workers in firms with some union workers ($18,906) is higher than the average premium for covered workers in firms without union workers ($17,748) 6.
The Distribution of Premiums
There is considerable variation in premiums for both single and family coverage.
Eighteen percent of covered workers are employed in a firms with a single premium at least 20% higher than the average single premium, while 19% of covered workers are in firms with a single premium less than 80% of the average single premium 7 and 8.
For family coverage, 17% of covered workers are employed in a firm with a family premium at least 20% higher than the average family premium, while 19% of covered workers are in firms with a family premium less than 80% of the average family premium7 and 8.
Seven percent of covered workers are in a firm with a premium of $9,000 a year or more for single coverage 9. Nine percent of covered workers are in a firm with a premium of $24,000 a year or more for family coverage 10.
Premium Changes Over Time
The 2016 average family coverage premiums are three percent higher than the 2015 average premiums 11.
The $18,142 average family premium in 2016 is 20% higher than the average family premium in 2011 and 58% higher than the average family premium in 2006 11 and 16. The 20% family premium growth in the last five years is smaller than the 31% growth between 2006 and 2011, or the 63% premium growth between 2001 and 2006 16.
The average family premiums for both small and large firms have seen a similar increase since 2011 (24% for small and 19% for large). For small firms (3 to 199 workers), the average family premium rose from $14,098 in 2011 to $17,546 in 2016. For large firms (200 or more workers), the average family premium rose from $15,520 in 2011 to $18,395 in 2016 13.
The rates of growth for the average family premiums in small firms and large firms since 2006 also have been similar. Since 2006, the average family premium for small firms increased 55% ($17,546 in 2016 vs. $11,306 in 2006), and the average family premium for large firms increased 59% ($18,395 in 2016 vs. $11,575 in 2006) 13.
For covered workers in large firms, the average family premium in firms that are fully insured has grown between 2011 to 2016 at a similar rate to premiums for workers in fully or partially self-funded firms (21% for fully insured plans and 18% for self-funded firms) 17.
Report: Section Two: Health Benefits Offer Rates
While nearly all large firms (200 or more workers) offer health benefits to at least some employees, small firms (3-199 workers) are significantly less likely to do so. The percentage of all firms offering health benefits in 2016 (56%) is similar to the percentages of firms offering health benefits in 2006 (61%) and 2011 (60%). The percentages of smaller firms (10 to 49 workers) offering coverage, however, has fallen since 2011 and years before. This trend precedes the ACA coverage expansions and is consistent with longer-term trends reported elsewhere.
Firms not offering health benefits continue to cite cost as the most important reason they do not do so. Almost all firms that offer coverage offer to dependents such as children and the spouses of eligible employees.
In 2016, 56% of firms offer health benefits, similar to the 57% who reported doing so in 2015 1.
Ninety-eight percent of large firms offer health benefits to at least some of their workers 3. In contrast, only 55% of small firms offer health benefits in 2016. The percentage of both small and large firms offering health benefits to at least some of their workers is similar to last year 2.
Since most firms in the country are small, variation in the overall offer rate is driven largely by changes in the percentages of the smallest firms (3-9 workers) offering health benefits. For more information on the distribution of firms in the country, see the Survey Design and Methods Section and Exhibit M1.7
Ninety-six percent of firms with 100 or more workers offer health benefits to at least some of their employees in 2016. Eighty-nine percent of firms with 50 to 99 workers offer benefits to at least some workers 4.
The percentages of smaller firms (10 to 49 workers) offering coverage has fallen since 2011 and years before.
The overall percentage of firms offering coverage in 2016 is similar to the percentage offering coverage in 2011 (60%) and 2006 (61%).
Offer rates vary across different types of firms.
Small firms are less likely to offer health insurance: 46% of firms with 3 to 9 workers offer coverage, compared 80% of firms with 25 to 49 workers, and 91% of firms with 50 to 199 employees 3.
Offer rates throughout different firm size categories in 2016 remain similar to those reported in 2015 2.
Part-Time and Temporary Workers
Among firms offering health benefits, relatively few offer benefits to their part-time and temporary workers.
The Affordable Care Act (ACA) defines part-time workers as those who on average work fewer than 30 hours per week. The employer shared responsibility provision of the ACA requires that large firms offer full-time employees a minimum standard of coverage or be assessed a penalty.8 Beginning in 2015, we modified the survey to explicitly ask employers whether they offered benefits to employees working fewer than 30 hours. Our previous question did not include a definition of “part-time”. For this reason, historical data on part-time offer rates are shown, but we did not test whether the differences between 2014 and 2015 were significant. Many employers may work with multiple definitions of part-time; one for their compliance with legal requirements and another for internal policies and programs.
In 2016, 16% of all firms that offer health benefits offer them to part-time workers 7. Large firms are more likely to offer health benefits to part-time employees than small firms (33% vs. 15%) 9.
A small percentage (4%) of firms offering health benefits offer them to temporary workers 8. More large firms offering health benefits elect to offer temporary workers coverage than small firms (17% vs. 3%) 10. The percentage of large firms offering health benefits to temporary workers is higher than the 11% reported in 2015.
Spouses, Dependents and Domestic Partner Benefits
The majority of firms offering health benefits offer to spouses and dependents, such as children. In 2016, 89% of small firms and 99% of large firms offering health benefits offer coverage to spouses 11. Fewer small firms offer coverage to spouses in 2016 than did in 2015 (98%). Eighty-eight percent of small firms and 100% of large firms offering health benefits cover other dependents, such as children, similar to last year. Eleven percent of small firms offering health benefits offer only single coverage to employees, higher than the 2% of small firms last year.
Employers were also asked whether same-sex or opposite-sex domestic partners were allowed to enroll in the firm’s coverage. While definitions may vary, employers often define domestic partners as an unmarried couple who has lived together for a specified period of time. Firms may define domestic partners separately from any legal requirements a state may have, and also, employers may have a different policy in different parts of the country.
In 2016, 27% of firms offering health benefits offer coverage to opposite-sex domestic partners, similar to the 28% who did so in 2015. Thirty-two percent of firms offering health benefits offer coverage to same-sex domestic partners, similar to the 42% who did so last year 13.
When we ask employers if they offer health benefits to opposite or same-sex domestic partners, many firms report that they have not encountered this issue. At many small firms, the firm may not have formal human resource policies on domestic partners simply because none of the firm’s employees have asked to cover a domestic partner. Regarding health benefits for opposite-sex domestic partners, 28% of firms report in 2016 that they have not encountered this request or that the question was not applicable 12. The vast majority of firms in the United States are small businesses; 61% of firms have between 3 and 9 employees and 98% have between 3 and 199 employees (Exhibit M.1). Therefore, statistics about the percentage of firms that offer domestic partner benefits are largely determined by small businesses. More small firms (28%) compared to large firms (2%) indicate that they have not encountered this request or that the question was not applicable 12. Regarding health benefits for same-sex domestic partners, 33% of firms report that they have not encountered the request or that the question was not applicable. More small firms (34%) than large firms (5%) report that they have not encountered the issue of offering benefits to same-sex domestic partners 12.
Virtually all firms offering family coverage offer coverage to spouses. Among firms offering health benefits to spouses, 13% do not allow an employee’s spouse to enroll in the firm’s plan if that spouse is offered coverage from another source, and an additional 5% allow the spouse to enroll subject to conditions 14. Among firms offering health benefits to spouses, 12% require an employee’s spouse to contribute more to the coverage if that spouse is offered coverage from another source. Very large firms (5,000 or more workers) are more likely than smaller firms to require higher spousal contributions when the spouse is offered coverage elsewhere (26% vs. 12%).
Among firms offering health benefits to spouses, 2% have made a significant reduction in the amount they contribute to cover an employee’s spouse in the last year, with no difference between small and large firms 15.
Among all firms that offer health benefits, 10% report providing additional compensation or benefits to employees if they enroll in a spouse’s plan, and 9% provide additional compensation or benefits to employees if they do not participate in the firm’s health benefits 16.
Firms Not Offering Health Benefits
The survey asks firms that do not offer health benefits if they have offered insurance or shopped for insurance in the recent past, and about their most important reasons for not offering coverage. Because such a small percentage of large firms report not offering health benefits, we present responses for small non-offering firms only.
The cost of health insurance remains the primary reason cited by firms for not offering health benefits. Among small firms not offering health benefits, 34% cite high cost as “the most important reason” for not doing so, followed by “employees are generally covered under another plan” (24%) 17. Relatively few small employers indicate that they do not offer because they believe that employees will get a better deal on the health insurance exchanges (1%).
Many non-offering small firms have either offered health insurance in the past five years, or shopped for health insurance in the past year. Nineteen percent of non-offering small firms have offered health benefits in the past five years, while 23% have shopped for coverage in the past year 18. The 19% of non-offering small firms that have offered coverage in the past five years is similar to the 25% reported last year.
Thirty percent of non-offering small firms report that they stopped offering coverage within the last year, similar to the percentage (38%) last year.
Among non-offering small firms, 11% report that they provide funds to their employees to purchase health insurance on their own in the individual market or through a health insurance exchange 19. The IRS has issued guidance limiting the circumstances in which employers can contribute to an employee’s non-group plan going forward.9
SHOP Exchanges
The Small Business Health Options Program (SHOP) is federal or state sponsored exchanges in which employers may offer and contribute to health insurance provided to their employees. Firms with 50 or fewer full-time equivalent workers (FTEs) are eligible to participate in a SHOP exchange. Beginning in 2016, states have the option to expand SHOP to include firms with up to 100 FTEs. Some employers are eligible for tax credits when purchasing coverage on the exchanges.
Eighteen percent of firms with 3 to 50 FTEs who do not offer health benefits said they looked at coverage on a SHOP exchange 20.
Thirteen percent of firms with 3 to 50 FTEs who offer health benefits said they looked at coverage on a SHOP exchange 20.
Among non-offering firms with 50 or fewer FTEs that looked at coverage but chose not to purchase on a SHOP exchange, 70% reported they did not do so because the plans were too expensive 21.
Among offering firms with 50 or fewer FTEs that looked at coverage but chose not to purchase on a SHOP exchange, their reasons included that they like their current insurer or broker (67%) and that they got a better deal elsewhere (64%) 22.
Report: Section Three: Employee Coverage, Eligibility, And Participation
Employers are the principal source of health insurance in the United States, providing health benefits for about 150 million non-elderly people in America.10 Most workers are offered health coverage at work, and the majority of workers who are offered coverage take it. Workers may not be covered by their own employer for several reasons: their employer may not offer coverage, they may be ineligible for the benefits offered by their firm, they may elect to receive coverage through their spouse’s employer, or they may refuse coverage from their firm. Before eligible employees may enroll, almost three-quarters (72%) of covered workers face a waiting period, although the average length waiting periods for covered workers with waiting periods has decreased since 2014 when an ACA provision prescribing a maximum waiting period of 90 days was implemented.
Among workers at firms offering health benefits, 62% percent of workers are covered by health benefits through their own employer 2.
Among workers in all firms, including those that offer and those that do not offer health benefits, 55% of workers are covered by health benefits offered by their employer, similar to the percentage (56%) last year. The coverage rate in 2016 is lower than the coverage rate in 2006 (59%) and in 2011 (58%) 1.
Eligibility
Not all employees are eligible for the health benefits offered by their firm, and not all eligible employees “take up” (i.e., elect to participate in) the offer of coverage. The share of workers covered in a firm is a product of both the percentage of workers who are eligible for the firm’s health insurance and the percentage that choose to take up the benefit. The percentage of workers eligible for health benefits at offering firms in 2016 is similar to last year for both small firms and large firms 6.
Seventy-nine percent of workers in firms offering health benefits are eligible for the coverage offered by their employer. The percentage of eligible workers is higher is small firms than in large firms (82% vs. 78%) 2.
Eligibility varies considerably by wage level. Employees in firms with a larger share of higher-wage workers (35% or more earn $59,000 or more annually) are more likely to be eligible for health benefits than employees in firms with a smaller share of higher-wage workers (86% vs. 73%) 3.
Eligibility also varies by the age of the workforce. Those in firms with a smaller share of younger workers (less than 35% of workers are age 26 or younger) are more likely to be eligible for health benefits than those in firms with a larger share of younger workers (81% vs. 64%) 3.
The average eligibility rate is particularly low (55%) in retail firms 2.
Take-up Rate
Employees who are offered health benefits generally elect to take up the coverage. In 2016, 79% of eligible workers take up coverage when it is offered to them, unchanged from last year 6.11
The likelihood of a worker accepting a firm’s offer of coverage also varies with the workforce’s wage level. Eligible employees in firms with a smaller share of lower-wage workers are more likely to take up coverage than eligible employees in firms with a larger share of lower-wage workers (35% or more of workers earn $23,000 or less annually) (80% vs. 61%). A similar pattern exists in firms with a larger share of higher-wage workers, with workers in these firms being more likely to take up coverage than those in firms with a smaller share of higher-wage workers (84% vs. 73%) 4.
The percentage of eligible workers taking up benefits in offering firms varies considerably by industry 2.
Coverage
The percentage of workers at firms offering health benefits that are covered by their firm’s health plan in 2016 is 62%. The coverage rate at firms offering health benefits is similar to last year for both small firms and large firms 6.
There is significant variation by industry in the coverage rate among workers in firms offering health benefits. For example, only 37% of workers in retail firms offering health benefits are covered by the health benefits offered by their firm, compared to 77% of workers in manufacturing, and 77% of workers in the state/local government industry category 2.
Among workers in firms offering health benefits, those in firms with a smaller share of lower-wage workers (less than 35% of workers earn $23,000 or less annually) are more likely to be covered by their own firm than workers in firms with a larger share of lower-wage workers (64% vs. 45%). A comparable pattern exists in firms with a larger share of higher-wage workers (35% or more earn $59,000 or more annually), with workers in these firms more likely to be covered by their employer’s health benefits than those in firms with a smaller share of higher-wage workers (72% vs. 54%) 5.
Among workers in firms offering health benefits, those in firms with a smaller share of younger workers (less than 35% of workers are age 26 or younger) are more likely to be covered by their own firm than those in firms with a larger share of younger workers (65% vs. 43%) 5.
Among workers in all firms, including those that offer and those that do not offer health benefits, 55% of workers are covered by health benefits offered by their employer, similar to the percentage (56%) last year. The coverage rate in 2016 is lower than the coverage rate in 2006 (59%) and in 2011 (58%),
Waiting Periods
Waiting periods are a specified length of time after beginning employment before employees are eligible to enroll in health benefits. With some exceptions, the Affordable Care Act requires that waiting periods cannot exceed 90 days.12 For example, employers are permitted to have orientation periods before the waiting period begins which, in effect, means an employee is not eligible for coverage 3 months after hire. If an employee is eligible to enroll on the 1st of the month after three months of employment, this survey rounds up and considers the firm’s waiting period four months. For these reasons, some employers still have waiting periods exceeding the 90-day maximum.
Seventy-two percent of covered workers face a waiting period before coverage is available, similar to last year 9. Covered workers in small firms (3-199 workers) are more likely than those in large firms to have a waiting period (78% vs. 70%) 7.
The average waiting period among covered workers who face a waiting period is 1.9 months 7. A small percentage (3%) of covered workers with a waiting period have a waiting period of more than 3 months.
Among firms with a waiting period of greater than 4 months, a majority of firms indicated that they have an employee measurement period. 13
Report: Section Four: Types Of Plans Offered
Most firms that offer health benefits offer only one type of health plan (83%) (see text box). Large firms (200 or more workers) are more likely to offer more than one type of health plan than small firms (3-199 workers). Employers are most likely to offer their workers a PPO plan and are least likely to offer a conventional plan (sometimes known as indemnity insurance).
Eighty-three percent of firms offering health benefits in 2016 offer only one type of health plan. Large firms are more likely to offer more than one plan type than small firms (53% vs. 16%) 1.
In addition to looking at the percentage of firms that offer multiple plan types, the percentage of covered workers at firms that offer multiple plan types can also be analyzed. Fifty-nine percent of covered workers are employed in a firm that offers more than one health plan type. Sixty-nine percent of covered workers in large firms are employed by a firm that offers more than one plan type, compared to 35% in small firms 2.
Nearly three quarters (74%) of covered workers in firms offering health benefits work in firms that offer one or more PPO plans; 56% work in firms that offer one or more HDHP/SO plans; 33% work in firms that offer one or more HMO plans; 13% work in firms that offer one or more POS plans; and 2% work in firms that offer one or more conventional plans 4.14
Among firms offering only one type of health plan, covered workers in large firms are more likely to be offered PPO plans than covered workers in small firms (62% vs. 39%), while covered workers in small firms are more likely to be offered HMO (12%) and POS (22%) plans than covered workers in large firms (3% and 4%, respectively) 5.
Among firms offering only one type of health plan, 29% of covered workers are in firms that only offer an HDHP/SO and 51% of covered workers are in firms that only offer a PPO 5.
The survey collects information on a firm’s plan with the largest enrollment in each of the plan types. While we know the number of plan types a firm has, we do not know the total number of plans a firm offers workers. In addition, firms may offer different types of plans to different workers. For example, some workers might be offered one type of plan at one location, while workers at another location are offered a different type of plan.
HMO is health maintenance organization.
PPO is preferred provider organization.
POS is point-of-service plan.
HDHP/SO is high-deductible health plan with a savings option such as an HRA or HSA.
Report: Section Five: Market Shares Of Health Plans
Enrollment remains highest in PPO plans, covering just under half of covered workers, followed by HDHP/SOs, HMO plans, POS plans, and conventional plans. Enrollment distribution varies by firm size: for example, PPOs are relatively more popular for covered workers at large firms (200 or more workers) than small firms (3-199 workers) (52% vs. 39%) and POS plans are relatively more popular among small firms than large firms (18% vs. 4%). Enrollment in HDHP/SOs has increased significantly over the past two years while enrollment in PPOs has fallen.
Forty-eight percent of covered workers are enrolled in PPOs, followed by HDHP/SOs (29%), HMOs (15%), POS plans (9%), and conventional plans (< 1%) 1. More covered workers are enrolled in HDHP/SO plans than in HMOs in both small firms and large firms 2.
The percentage of covered workers enrolled in HDHP/SOs in is similar to last year but has grown significantly since 2014 (29% vs. 20%).15 Since 2014, enrollment in PPOs has fallen significantly (48% vs. 58%) 1.
Plan enrollment patterns vary by firm size.
Covered workers in large firms are more likely than covered workers in small firms to enroll in PPOs (52% vs. 39%). Covered workers in small firms are more likely than covered workers in large firms to enroll in POS plans (18% vs. 4%) 2.
The share of covered workers in HDHP/SOs is similar for large firms and small firms 2.
Plan enrollment patterns also differ across regions.
HMO enrollment is significantly higher in the West (30%) and significantly lower in the South (10%) and Midwest (6%) 3.
Covered workers in the South (57%) are more likely to be enrolled in PPOs than workers in other regions; covered workers in the West (35%) and the Northeast (39%) are less likely to be enrolled in a PPO 3.
Enrollment in HDHP/SOs is similar across regions 3.
Plan enrollment patterns differ by industry as well.
Covered workers in the agriculture/mining/construction, (5%), manufacturing (8%) and finance (8%) are less likely to be enrolled in an HMO plan than covered workers in other industries. Covered workers in the service industry (20%) are more likely to be enrolled in an HMO than covered workers in other industries 3.
Covered workers in the state/local government (64%) are more likely to be enrolled in a PPO plan than covered workers in other industries. Covered workers in the finance industry (32%) are less likely to be enrolled in a PPO than covered workers in other industries 3.
Covered workers in the state/local government (19%) and agriculture/mining/construction industries (15%) are less likely to be enrolled in an HDHP/SO plan than covered workers in other industries. Covered workers in the finance industry (49%) are more likely to be enrolled in an HDHP/SO than covered workers in other industries
Report: Section Six: Worker And Employer Contributions For Premiums
In 2016, premium contributions by covered workers average 18% for single coverage and 30% for family coverage.16 The average monthly worker contributions are $94 for single coverage ($1,129 annually) and $440 for family coverage ($5,277 annually).17 Covered workers in small firms (3-199 workers) have a lower average contribution amount for single coverage ($1,021 vs. $1,176), but a higher average contribution amount for family coverage ($6,597 vs. $4,719) than covered workers in large firms (200 or more employees).
In 2016, covered workers on average contribute 18% of the premium for single coverage and 30% of the premium for family coverage 1. These contribution percentages have remained stable in recent years for both single and family coverage.
Covered workers in small firms contribute a higher percentage of the premium for family coverage (39% vs. 26%) than covered workers in large firms 23.
On average, workers with single coverage contribute $94 per month ($1,129 annually), and workers with family coverage contribute $440 per month ($5,277 annually) towards their health insurance premiums 2, 3, and 4.
The average worker contribution in HDHP/SOs is lower than the overall average worker contribution for single coverage ($943 vs. $1,129) and family coverage ($4,289 vs. $5,277) 5.
Worker contributions also differ by firm size. As in previous years, workers in small firms contribute a lower amount annually for single coverage than workers in large firms ($1,021 vs. $1,176). In contrast, workers in small firms with family coverage contribute significantly more annually than workers in large firms ($6,597 vs. $4,719) 6.
The average worker contributions for single coverage and family coverage are similar to last year for both small firms and large firms 8 and 9.
Variation in Worker Contributions to the Premium
The majority of covered workers are employed by a firm that contributes at least half of the premium for single and family coverage.
Twelve percent of covered workers are in plans where the employer pays the entire premium for single coverage; three percent of covered workers are in plans where the employer pays the entire premium for family coverage 17.
Covered workers in small firms are much more likely to work for a firm that pays 100% of the premium than workers in large firms. Thirty percent of covered workers in small firms have an employer that pays the full premium for single coverage, compared to five percent of covered workers in large firms 18. For family coverage, eight percent of covered workers in small firms have an employer that pays the full premium, compared to one percent of covered workers in large firms 19.
Fifteen percent of covered workers have a plan where they are required to contribute more than 50% of the cost of family coverage.
Three percent of covered workers in small firms and 1% of covered workers in large firms contribute more than 50% of the premium for single coverage 18. For family coverage, 34% of covered workers in small firms work in a firm where they must contribute more than 50% of the premium, compared to seven percent of covered workers in large firms 19.
There is considerable variation around the distribution of the average dollar contribution amounts. Note that we changed our methods beginning in 2016: previously, the percentages were calculated excluding workers who do not make a premium contribution; now all covered workers are included (with a zero dollar contribution value for those workers where the employer pays 100% of the premium).
For single coverage, 34% of covered workers contribute $1,355 or more annually (120% or more of the average worker contribution), while 41% of covered workers have an annual worker contribution of less than $903 (less than 80% of the average worker contribution) 16.
For family coverage, 27% of covered workers contribute $6,332 or more annually (120% or more of the average worker contribution), while 41% of covered workers have an annual worker contribution of less than $4,222 (less than 80% of the average worker contribution) 16.
Differences by Firm Characteristics
The percentage of the premium paid by covered workers varies by several firm characteristics.
Covered workers in firms with a larger share of lower-wage workers (35% or more earn $23,000 or less annually) contribute a greater percentage of the premium for single coverage (23% v. 18%) and family coverage (35% vs. 30%) than those in firms with a smaller share of lower-wage workers 21 and 22. Covered workers in firms with a larger share of higher-wage workers (35% or more earn $59,000 or more a year) contribute less on average for family coverage (27% vs. 33%) than those in firms with a smaller share of higher-wage workers.
Looking at dollar amounts, covered workers in firms with a larger share of lower-wage workers (35% or more earn $23,000 or less annually) on average contribute $1,322 for single coverage compared with $1,115 for covered workers in firms with a smaller share of lower-wage workers 15.
Covered workers in large firms that have at least some union workers have lower average contribution percentages for family coverage than those in firms without any unionized workers (22% vs. 29%). Covered workers at firms with some union workers have a lower average contribution amount for family coverage ($4,264 vs. $5,800) 15 and 22.
Covered workers in large firms that are partially or completely self-funded have a lower average percentage contribution for family coverage than workers in large firms that are fully insured (25% vs. 30%) 22.18
Covered workers in public organizations have lower average premium contributions for single and family coverage than workers in private for-profit firms 21 and 22.
Contribution approaches
Firms take different approaches for contributing towards family coverage. Among firms offering health benefits, 45% of small firms and 18% of large firms contribute the same dollar amount for single coverage as for family coverage, which means that the worker must pay the entire difference between the cost of single and family coverage if they wish to enroll their family members. Forty-five percent of small firms and 67% of large firms make a larger dollar contribution for family coverage than for single coverage 26.
Among firms offering health benefits, 15% require workers who use tobacco to contribute more towards the premium or cost-sharing than those who do not use tobacco 28.
Changes over Time
The average worker contributions for single and family coverage have increased 80% and 78%, respectively, over the last 10 years, and 23% and 28%, respectively, over the last five years.
The average premium contributions for covered workers with single and family coverage have grown at similar rates in small firms and large firms 8 and 9.
Report: Section Seven: Employee Cost Sharing
In addition to any required premium contributions, most covered workers face cost sharing for the medical services they use. Cost sharing for medical services can take a variety of forms, including deductibles (an amount that must be paid before most services are covered by the plan), copayments (fixed dollar amounts), and/or coinsurance (a percentage of the charge for services). The type and level of cost sharing often vary by the type of plan in which the worker is enrolled. Cost sharing may also vary by the type of service, such as office visits, hospitalizations, or prescription drugs.
The cost-sharing amounts reported here are for covered workers using services provided in-network by participating providers. Plan enrollees receiving services from providers that do not participate in plan networks often face higher cost sharing and may be responsible for charges that exceed plan allowable amounts. The framework of this survey does not allow us to capture all of the complex cost-sharing requirements in modern plans, particularly for ancillary services (such as durable medical equipment or physical therapy) or cost-sharing arrangements that vary across different settings (such as tiered networks). Therefore, we do not collect information on all plan provisions and limits that affect enrollee out-of-pocket liability.
General Annual Deductibles For Workers in Plans with Deductibles
A general annual deductible is an amount that must be paid by enrollees before most services are covered by their health plan. Non-grandfathered health plans are required to cover some services such as preventive care without cost sharing. Some plans require enrollees to meet a service-specific deductible such as on prescription drugs or hospital admissions in lieu of or in addition to a general deductible.
Eighty-three percent of covered workers are enrolled in a plan with a general annual deductible for single coverage, similar to 81% in 2015. Since 2011, the percentage of covered workers with a general annual deductible for single coverage has increased from 74% to 83% 2.
The percentage of covered workers enrolled in a plan with a general annual deductible for single coverage is similar for small firms (3-199 workers) and large firms (200 0r more workers) (82% and 83%) 1.
The likelihood of having a deductible varies by plan type. Covered workers in HMOs are less likely to have a general annual deductible for single coverage than workers in other plan types. Fifty-four percent of workers in HMOs do not have a general annual deductible for single coverage, compared to 24% of workers in POS plans and 16% of workers in PPOs 1. The percentage of covered workers in HMO plans with a general annual deductible for single coverage has increased from 29% in 2011 to 46% in 2016 2.
Covered workers in plans without a general annual deductible often have other forms of cost sharing when they are hospitalized or use other medical services. For covered workers in plans without a general annual deductible with single coverage, 82% in HMOs, 64% in PPOs, and 78% in POS plans are in plans that require some cost sharing for hospital admissions. The percentages are similar for family coverage 4.
For covered workers in a plan with a general annual deductible, the average annual deductible for single coverage is $1,478, an increase over the average deductible ($1,318) last year 7.
Average deductibles vary considerably by plan type. For covered workers in plans with a general annual deductible, the average deductibles for single coverage are $917 in HMOs, $1,028 in PPOs, $1,737 in POS plans, and $2,199 for HDHP/SOs 5.
Deductibles for single coverage are generally higher for covered workers in small firms than for covered workers in large firms across plan types. For example, for covered workers in PPOs with a general annual deductible, the average deductible amount for single coverage in small firms is more than twice as large as the average deductible amount in large firms ($1,662 vs. $814). Overall, for covered workers in plans with a general annual deductible, the average deductible amount for single coverage in small firms is higher than the average deductible amount in large firms ($2,069 vs. $1,238) 5.
The average general annual deductible for single coverage for covered workers in plans with a deductible has increased 49% over the last five years, from $991 in 2011 to $1,478 in 2016 7.
There is considerable variation in the dollar values of general annual deductibles for covered workers at different firms. For example, 25% of covered workers enrolled in a PPO plan with a general annual deductible for single coverage have a deductible of less than $500 while 14% have a deductible of $2,000 or more 16.
For family coverage, the majority of covered workers with general annual deductibles have an aggregate deductible, meaning all family members’ out-of-pocket expenses count toward meeting the deductible amount. Among those with a general annual deductible for family coverage, the percentages of covered workers with an average aggregate general annual deductible are 61% for workers in HMOs, 64% for workers in PPOs, and 77% for workers in POS plans 18.
The average deductible amounts for covered workers with an aggregate deductible for family coverage are $2,245 for HMOs, $2,147 for PPOs, $3,769 for POS plans, and $4,343 for HDHP/SOs 19. Deductible amounts for aggregate family deductibles are similar to last year for plan types other than POS plans 20.
The other type of family deductible, a separate per-person deductible, requires each family member to meet a separate per-person deductible amount before the plan covers expenses for that member. Many plans with separate per-person family deductibles (71%) consider the deductible met for all family members if a prescribed number of family members each reaches his or her separate deductible amounts 23. Plans may also require each family member to meet a separate per-person deductible until the family’s combined spending reaches a specified dollar amount.
For covered workers in health plans that have separate per-person general annual deductible amounts for family coverage, the average deductibles are $632 for HMOs, $1,052 for PPOs, $1,180 for POS plans, and $2,411 for HDHP/SOs 19.
Most covered workers in plans with a separate per-person general annual deductible for family coverage have a limit to the number of family members required to meet the separate deductible amounts 23.19 Among those covered workers in plans with a limit on the number of family members, the most frequent number of family members required to meet the separate deductible amounts is two (45%) 24.
The majority of covered workers with a general annual deductible are in plans where the deductible does not have to be met before certain services, such as physician office visits or prescription drugs, are covered.
Large majorities of covered workers (87% in HMOs, 72% in PPOs, and 60% in POS plans) with general annual deductibles are enrolled in plans where the deductible does not have to be met before physician office visits for primary care are covered 26.
Similarly, among workers with a general annual deductible, large shares of covered workers in HMOs (93%), PPOs (91%), and POS plans (89%) are enrolled in plans where the general annual deductible does not have to be met before prescription drugs are covered 26.
General Annual Deductibles Among All Covered Workers
As discussed above, the share of covered workers in plans with a general annual deductible has increased significantly over time: from 55% in 2006, to 74% in 2011, to 83% in 2016, as have the average deductible amounts for covered workers in plans with deductibles: from $584 in 2006, to $991 in 2011, to $1,478 in 2016. Neither trend by itself captures the full impact of changes in deductibles on covered workers. We can look at the average impact of both trends together on covered workers by assigning a zero deductible value to covered workers in plans with no deductible and looking at how the resulting averages change over time. These average deductible amounts are lower in any given year but the changes over time reflect both the higher deductibles in plans with deductibles and the fact that more workers face them.
Using this approach, the average general annual deductible for single coverage for all covered workers in 2016 is $1,221 9.
The 2016 value is 63% higher than the average general annual deductible of $747 in 2011 and 300% higher than the average general annual deductible of $303 in 2006 9.
Another way to look at deductibles is the percentage of all covered workers who are in a plan with a deductible that exceeds certain thresholds. Fifty-one percent of covered workers are in plans with a general annual deductible of $1,000 or more for single coverage, similar to the percentage in 2015 (46%) 10.
Over the last five years, the percentage of covered workers with a general annual deductible of $1,000 or more for single coverage has grown substantially, increasing from 31% to 51% 10.
Workers in small firms are more likely to have a general annual deductible of $1,000 or more for single coverage than workers in large firms (65%vs. 45%) 8.
Twenty-three percent of covered workers are enrolled in a plan with a deductible of $2,000 or more, similar to the percentage last year (19%) 12. Forty-one percent of covered workers at small firms have a general annual deductible of $2,000 or more, in contrast to 16% in large firms 8.
One of the reasons for the growth in deductible amounts has been the growth in enrollment in HDHP/SOs, which have higher deductibles than other plans. While growing deductibles in PPOs and other plan types generally increases enrollee out-of-pocket liability, the shift in enrollment to HDHP/SOs does not necessarily do so because most HDHP/SO enrollees receive an account contribution from their employers, which in essence reduces the high cost sharing in these plans.
Fourteen percent of covered workers in an HDHP with an HRA and 7% of covered workers in an HSA-qualified HDHP receive an account contribution for single coverage at least equal to their deductible, while another 47% of covered workers in an HDHP with an HRA and 28% of covered workers in an HSA-qualified HDHP receive account contributions that, if applied to their deductible, would reduce the deductible to $1,000 or less 14.
If we reduce the deductibles that workers face by employer account contributions, the percentage of covered workers with a deductible liability of $1,000 or more would be reduced from 51% to 38% 11.
Hospital and Outpatient Surgery Cost Sharing
Whether or not a worker has a general annual deductible, most workers face additional types of cost sharing (such as a copayment, coinsurance, or a per diem charge) when admitted to a hospital or having outpatient surgery. The distribution of workers with cost sharing for hospital and outpatient surgery does not equal 100% as workers may face a combination of types of cost sharing. In addition, the average copayment and coinsurance rates for hospital admissions include workers who may have a combination of these types of cost sharing.
For hospital admissions, 64% of covered workers have coinsurance and 14% have copayments. Lower percentages of workers have per day (per diem) payments (6%), a separate hospital deductible (1%), or both copayments and coinsurance (10%), while 16% have no additional cost sharing for hospital admissions after any general annual deductible has been met. For covered workers in HMO plans, copayments are more common (46%) and coinsurance (24%) is less common than in other plan types. Only 2% of covered workers in HDHP/SOs have a copayment for hospital admissions, lower than other plan types 27.
The percentage of covered workers in a plan that requires coinsurance for hospital admissions has increased from 55% in 2011 to 64% in 2015.
The average coinsurance rate for hospital admission is 19%; the average copayment is $282 per hospital admission; the average per diem charge is $281; and the average separate annual hospital deductible is $898 29.
The cost-sharing provisions for outpatient surgery are similar to those for hospital admissions, as most workers have coinsurance or copayments. Sixty-six percent of covered workers have coinsurance and 17% have copayments for an outpatient surgery episode. In addition, 1% has a separate annual deductible for outpatient surgery, and 4% have both copayments and coinsurance, while 17% have no additional cost sharing after any general annual deductible has been met 28.
For covered workers with cost sharing for outpatient surgery, the average coinsurance rate is 19% and the average copayment is $170 29.
Cost Sharing for Physician Office Visits
The majority of covered workers are enrolled in health plans that require cost sharing for an in-network physician office visit, in addition to any general annual deductible20 .
The most common form of physician office visit cost sharing for in-network services is copayments. Sixty-seven percent of covered workers have a copayment for a primary care physician office visit and 25% have coinsurance. For office visits with a specialty physician, 66% of covered workers have copayments and 26% have coinsurance. Workers in HMOs, PPOs, and POS plans are much more likely to have copayments than workers in HDHP/SOs for both primary care and specialty care physician office visits. For primary care physician office visits, 64% of covered workers in HDHP/SOs have coinsurance, 18% have no cost sharing after the general annual plan deductible is met, and 16% have copayments 30.
Among covered workers with a copayment for in-network physician office visits, the average copayment is $24 for primary care and $38 for specialty physician office visits 31, similar to the amounts last year 31.
Among workers with coinsurance for in-network physician office visits, the average coinsurance rates are 18% for a visit with a primary care physician and 19% for a visit with a specialist 31, the same rates as last year.
Out-Of-Pocket Maximum Amounts
Most covered workers are in a plan that partially or totally limits the cost sharing that a plan enrollee must pay in a year. These limits are generally referred to as out-of-pocket maximum amounts. The Affordable Care Act (ACA) requires that non-grandfathered health plans have an out-of-pocket maximum of $6,850 or less for single coverage and $13,700 for family coverage.21 Many plans have complex out-of-pocket structures, which makes it difficult to accurately collect information on this element of plan design.
In 2016, 98% percent of covered workers are in a plan with an out-of-pocket maximum for single coverage. This is a significant increase from 83% in 2011.
For covered workers in plans with out-of-pocket maximums for single coverage, there is wide variation in spending limits.
Fourteen percent of covered workers in plans with an out-of-pocket maximum for single coverage have an out-of-pocket maximum of less than $2,000, while 18% have an out-of-pocket maximum of $6,000 or more 36.
Report: Section Eight: High-deductible Health Plans With Savings Option
To help cover out-of-pocket expenses not covered by a health plan, some employers offer high deductible plans that are paired with an account that allows enrollees to use tax-preferred savings to pay plan cost sharing and other out-of-pocket medical expenses. The two most common are health reimbursement arrangements (HRAs) and health savings accounts (HSAs). HRAs and HSAs are financial accounts that workers or their family members can use to pay for health care services. These savings arrangements are often (or, in the case of HSAs, always) paired with health plans with high deductibles. The survey treats high-deductible plans paired with a savings option as a distinct plan type – High-Deductible Health Plan with Savings Option (HDHP/SO) – even if the plan would otherwise be considered a PPO, HMO, POS plan, or conventional health plan. Specifically for the survey, HDHP/SOs are defined as (1) health plans with a deductible of at least $1,000 for single coverage and $2,000 for family coverage22 offered with an HRA (referred to as HDHP/HRAs); or (2) high-deductible health plans that meet the federal legal requirements to permit an enrollee to establish and contribute to an HSA (referred to as HSA-qualified HDHPs).23
Percentage of Firms Offering HDHP/HRAs and HSA-Qualified HDHPs, and Enrollment
Twenty-eight percent of firms offering health benefits offer an HDHP/HRA, an HSA-qualified HDHP, or both. Among firms offering health benefits, 5% offer an HDHP/HRA and 24% offer an HSA-qualified HDHP 1. The percentage of firms offering an HDHP/SO is similar to last year but has increased since 2006 (7%).
Large firms (200 or more workers) are more likely than small firms (3-199 workers) to offer an HDHP/SO (51% vs. 27%). 2.
Health Reimbursement Arrangements (HRAs) are medical care reimbursement plans established by employers that can be used by employees to pay for health care. HRAs are funded solely by employers. Employers may commit to make a specified amount of money available in the HRA for premiums and medical expenses incurred by employees or their dependents. HRAs are accounting devices, and employers are not required to expend funds until an employee incurs expenses that would be covered by the HRA. Unspent funds in the HRA usually can be carried over to the next year (sometimes with a limit). Employees cannot take their HRA balances with them if they leave their job, although an employer can choose to make the remaining balance available to former employees to pay for health care.
HRAs often are offered along with a high-deductible health plan (HDHP). In such cases, the employee pays for health care first from his or her HRA and then out-of-pocket until the health plan deductible is met. Sometimes certain preventive services or other services such as prescription drugs are paid for by the plan before the employee meets the deductible.
Health Savings Accounts (HSAs) are savings accounts created by individuals to pay for health care. An individual may establish an HSA if he or she is covered by a “qualified health plan” –a plan with a high deductible (i.e., a deductible of at least $1,300 for single coverage and $2,600 for family coverage in 2016) that also meets other requirements.[1] Employers can encourage their employees to create HSAs by offering an HDHP that meets the federal requirements. Employers in some cases also may assist their employees by identifying HSA options, facilitating applications, or negotiating favorable fees from HSA vendors.
Both employers and employees can contribute to an HSA, up to the statutory cap of $3,350 for single coverage and $6,750 for family coverage in 2016. Employee contributions to the HSA are made on a pre-income tax basis, and some employers arrange for their employees to fund their HSAs through payroll deductions. Employers are not required to contribute to HSAs established by their employees but if they elect to do so, their contributions are not taxable to the employee. Interest and other earnings on amounts in an HSA are not taxable. Withdrawals from the HSA by the account owner to pay for qualified health care expenses are not taxed. The savings account is owned by the individual who creates the account, so employees retain their HSA balances if they leave their job.
Enrollment in HDHP/SO plans has increased over time from 17% of covered workers in 2011 to 29% in 2016.
Nine percent of covered workers are enrolled in HDHP/HRAs in 2016, similar to last year (9%). The percentage of covered workers enrolled in HSA-qualified HDHPs increased from 15% in 2015 to 19% in 2016 5.
A similar percentage of covered workers at small firms (3-199 workers) and large firms are enrolled in HDHP/SOs 5
Plan Deductibles
As expected, workers enrolled in HDHP/SOs have higher deductibles than workers enrolled in HMOs, PPOs, or POS plans.
The average general annual deductible for single coverage is $2,031 for HDHP/HRAs and $2,295 for HSA-qualified HDHPs 7. These averages are similar to the amounts reported in recent years. There is wide variation around these averages: 17% of covered workers enrolled in an HDHP/SO are in a plan with a deductible of $1,000 to $1,499 while 21% are in a plan with a deductible of $3,000 or more 9.
The survey asks employers whether the family deductible amount is (1) an aggregate amount (i.e., the out-of-pocket expenses of all family members are counted until the deductible is satisfied), or (2) a per-person amount that applies to each family member (typically with a limit on the number of family members that would be required to meet the deductible amount) (for more information see Section 7).
The average aggregate deductibles for workers with family coverage are $4,321 for HDHP/HRAs and $4,364 for HSA-qualified HDHPs 7. As with single coverage, there is wide variation around these averages for family coverage: 15% of covered workers enrolled in HDHP/SOs with an aggregate family deductible have a deductible of $2,000 to $2,999 while 19% have a deductible of $6,000 dollars or more 11.
Out-of-Pocket Maximum Amounts
HSA-qualified HDHPs are legally required to have a maximum annual out-of-pocket liability of no more than $6,550 for single coverage and $13,100 for family coverage in 2016. Non-grandfathered HDHP/HRA plans starting in 2016 are required to have out-of-pocket maximums of no more than $6,850 for single coverage and $13,700 for family coverage. Virtually all HDHP/HRA plans have an out of pocket maximum for single coverage in 2016.
The average annual out-of-pocket maximum for single coverage is $4,264 for HDHP/HRAs and $4,083 for HSA-qualified HDHPs 7.
Premiums
The average annual premiums in 2016 for covered workers in HDHP/HRAs are $5,860 for single coverage and $17,734 for family coverage. The average single premium for covered workers in HDHP/HRAs is lower than the average single premium for covered workers in non-HDHP/SO plans 8.
The average annual premium for workers in HSA-qualified HDHPs is $5,719 for single coverage and $16,246 for family coverage. These amounts are significantly less than the average single and family premium for covered workers in plans that are not HDHP/SOs 8.
The average single and family coverage premiums for HSA-qualified HDHPs are similar to the premiums for covered workers enrolled in HDHP/HRAs.
Worker Contributions to Premiums
The average annual worker contributions to premiums for workers enrolled in HDHP/HRAs are $1,143 for single coverage and $5,105 for family coverage 8.
The average annual worker contributions to premiums for workers in HSA-qualified HDHPs are $849 for single coverage and $3,930 for family coverage. The average contributions for single and family coverage for covered workers in HSA-qualified HDHPs are significantly less than the average premium contribution made by covered workers in plans that are not HDHP/SOs 8.
Employer Contributions to Premiums and Savings Options
Employers contribute to HDHP/SOs in two ways: through their contributions toward the premium for the health plan and through their contributions (if any, in the case of HSAs) to the savings account option (i.e., the HRAs or HSAs themselves).
Looking at only the annual employer contributions to premiums, covered workers in HDHP/HRAs on average receive employer contributions of $4,717 for single coverage and $12,628 for family coverage. The average employer contribution for covered workers in HDHP/HRAs for single coverage is lower than the average contribution for covered workers in plans that are not HDHP/SOs 8.
The average annual employer contributions to premiums for workers in HSA-qualified HDHPs are $4,870 for single coverage and $12,316 for family coverage. The average employer contribution for covered workers in HSA qualified HDHPs for single coverage is lower than the average contribution for covered workers in plans that are not HDHP/SOs 8.
When looking at employer contributions to the savings option, covered workers enrolled in HDHP/HRAs on average receive an annual employer contribution to their HRA of $1,059 for single coverage and $1,867 for family coverage 8.
HRAs are generally structured in such a way that employers may not actually spend the whole amount that they make available to their employees’ HRAs.24 Amounts committed to an employee’s HRA that are not used by the employee generally roll over and can be used in future years, but any balance may revert back to the employer if the employee leaves his or her job. Thus, the employer contribution amounts to HRAs that we capture in the survey may exceed the amount that employers will actually spend.
Covered workers enrolled in HSA-qualified HDHPs on average receive an annual employer contribution to their HSA of $686 for single coverage and $1,208 for family coverage 8. These amounts do not include the 1% of covered workers in HSA-qualified HDHPs whose employers say they vary account contributions based on certain factors, such as participation in a wellness program or job classification.
In many cases, employers that sponsor HSA-qualified HDHP/SOs do not make contributions to HSAs established by their employees. Fifty-two percent of employers offering single coverage and 55% offering family coverage through HSA-qualified HDHPs do not make contributions towards the HSAs that their workers establish. Twenty-five percent of workers with single coverage and 25% percent of workers with family coverage in an HSA-qualified HDHP do not receive an account contribution from their employer (see notes in 14 and 15.
The average HSA contributions reported above include the portion of covered workers whose employer contribution to the HSA is zero. When those firms that do not contribute to the HSA are excluded from the calculation, the average employer contribution for covered workers is $916 for single coverage and $1,617 for family coverage.
The percentage of covered workers enrolled in a plan where the employer makes no HSA contribution for single coverage (25%) is similar to the percentage in recent years.
Employer contributions to savings account options (i.e., the HRAs and HSAs themselves) for their employees can be added to their health plan premium contributions to calculate total employer contributions toward HDHP/SOs.–We note that HRAs are a promise by an employer to pay up to a specified amount and that many employees will not receive the full amount of their HRA in a year, so adding the employer premium contribution amount and the HRA contribution represents an upper bound for employer liability that overstates the amount that is actually expended. Since employer contributions to employee HSA accounts immediately transfer the full amount to the employee, adding employer premium and HSA contributions is a good way to look at their total liability under these plans.
For HDHP/HRAs, the average annual total employer contribution for covered workers is $5,776 for single coverage and $14,495 for family coverage. The average total employer contribution amounts for covered workers for family coverage in HDHP/HRAs are higher than the average amount that employers contribute towards family coverage in health plans that are not HDHP/SOs 8.
For HSA-qualified HDHPs, the average total annual firm contribution for covered workers is $5,561 for single coverage and $13,528 for workers with family coverage. The average total firm contribution amounts for single and family coverage in HSA-qualified HDHPs are similar to the average firm contributions towards single and family coverage in health plans that are not HDHP/SOs 8.
Variation in Employer Contributions to Savings Options
There is considerable variation in the amount that employers contribute to savings accounts.
Looking at how contributions vary around the average, 30% of covered workers in HDHP/HRAs have an HRA contribution for single coverage of less than $635 (60% of the average), while 21% have an account contribution of $1,482 (140% of the average) or more 16.
Thirty-eight percent of covered workers in HSA-qualified HDHPs have an annual HSA contribution for single coverage of less than $411 (60% of the average) while 29% have an account contribution of $960 (140% of the average) or more 17.
Cost Sharing for Office Visits, Outpatient Surgery and Hospital Surgery
The cost-sharing pattern for primary care office visits differs for workers enrolled in HDHP/SOs. Thirty-three percent of covered workers in HDHP/HRAs have a copayment for primary care physician office visits compared to 8% enrolled in an HSA-qualified HDHP 19. Workers in other plan types are much more likely to face copayments than coinsurance for physician office visits (see Section 7 for more information).
Report: Section Nine: Prescription Drug Benefits
Almost all covered workers have coverage for prescription drugs. For 2016, to reduce burden on respondents, we revised the survey to ask respondents about the attributes of prescription drug coverage only in their largest health plan; previously, we asked about prescription coverage in their largest plan for each of the plan types that they offered. In addition, we began asking employers about their cost sharing for tiers that cover specialty drugs exclusively. In cases in which a tier covers only specialty drugs, we report the plan attributes under the specialty banner, rather than as one of the four standard tiers. Therefore, the number of tiers a firm reports may not correspond with the number of tiers for which we have cost-sharing information. For more information, see the survey design and methods section. While this new approach produces estimates that are quite similar to those obtained by the prior method, we do not do statistical comparisons with 2016 estimates and those from prior years.25
Nearly all (more than 99%) covered workers work at a firm that provides prescription drug coverage in their largest health plan.
A large share of covered workers (89%) work at a firm whose largest health plan has a tiered cost-sharing formula for prescription drugs 1. Cost-sharing tiers generally refer to a health plan placing a drug on a formulary or preferred drug list that classifies drugs into categories that are subject to different cost sharing or management. It is common for there to be different tiers for generic, preferred and non-preferred drugs. In recent years, plans have created additional tiers which, for example, may be used for lifestyle drugs or expensive biologics. Some plans may have multiple tiers for different categories; for example, a plan may have preferred and non-preferred specialty tiers. The survey obtains information about the cost-sharing structure for up to five tiers.
Eighty-four percent of covered workers work at a firm that has three, four, or more tiers of cost sharing for prescription drugs in their largest health plan 1.
Covered workers at large firms (200 or more workers) whose largest health plan is an HDHP/SO have a different cost-sharing pattern for prescription drugs than covered workers with other plan types: they are more likely to be in a plan with the same cost sharing regardless of drug type (17% vs. 3%) or in a plan that has no cost sharing for prescriptions once the plan deductible is met (8% vs. <1%) 2.
Three or More Tiers
Thirty-two percent of covered workers work at a firm whose largest health plan has four or more tiers of cost sharing for prescription drugs 1.
For covered workers at firms whose largest plan has three or more tiers of cost sharing for prescription drugs, copayments are the most common form of cost sharing in the first three tiers and coinsurance is the next most common. Among those with a fourth tier, 46% have a coinsurance requirement and 41% have a copayment (difference not significant) 3.
Among covered workers at firms whose largest health plan has three or more tiers of cost sharing for prescription drugs, the average copayments are $11 for first-tier drugs, $33 second-tier drugs, $57 third-tier drugs, and $102 for fourth-tier drugs 4.
Among covered workers at firms whose largest health plan has three or more tiers of cost sharing for prescription drugs, the average coinsurance rates are 17% for first-tier drugs, 25% second-tier drugs, 37% third-tier drugs, and 29% for fourth-tier drugs 4.
Single and Two Tiers
Five percent of covered workers work at firms whose largest health plan has two tiers for prescription drug cost sharing 1. For these workers, copayments are more common than coinsurance for both first-tier and second-tier drugs. The average copayment for the first tier is $12 and the average copayment for the second tier is $29 7.
Seven percent of covered workers at firms whose largest health plan covers prescription drugs have the same cost sharing regardless of the type of drug 1.
Among these workers, 19% have copayments and 81% have coinsurance 8. The average coinsurance rate is 22% and the average copayment is $12 9.
Thirteen percent of these workers are at firms whose largest health plan limits coverage for prescriptions to generic drugs 10.
Limits on Coinsurance
Coinsurance rates for prescription drugs often have maximum and/or minimum dollar amounts associated with the coinsurance rate. Depending on the plan design, coinsurance maximums may significantly limit an enrollee’s out-of-pocket spending on higher cost drugs.
These coinsurance minimum and maximum amounts vary across the tiers. Among covered workers at firms whose largest health plan has coinsurance for the first cost-sharing tier, 20% have only a maximum dollar amount attached to the coinsurance rate, 4% have only a minimum dollar amount, 26% have both, and 50% have neither. For those with coinsurance for the fourth cost-sharing tier, 76% have a maximum dollar amount, 3% have a minimum dollar amount, and 21% have neither 12.
Specialty drugs
Specialty drugs such as biologics may be used to treat chronic conditions and often require special handling and administration. We revised the questions in the 2016 survey regarding specialty drugs, and are reporting results only among large firms because a large share of small firms were unsure whether their largest plan covered these drugs.
Ninety-eight percent of covered workers at large firms work for employers whose largest health plan provides coverage for specialty drugs 13. Among these workers, 43% work at firms whose largest plan has a cost-sharing tier just for specialty drugs 14.
Among covered workers at large firms whose largest plan has a separate tier for specialty drugs, 43% have a copayment for specialty drugs and 46% have a coinsurance requirement 15. The average copayment is $89 and the average coinsurance rate is 26% 16. Seventy-eight percent of those with a coinsurance requirement have a maximum dollar limit on the amount of coinsurance they must pay.
Specialty drugs are typically high cost; firms use a variety of strategies to contain these costs. Among covered workers at large firms whose largest health plan provides coverage for specialty drugs, 38% use a different pharmacy benefit manager for specialty drugs; 28% have a dispensing program with incentives to encourage enrollees to receive specialty drugs in an alternative setting; 68% use a step therapy approach where enrollees must try alternatives before specialty drugs are covered; 61% use tight limits on the number of units administered at a single time; 70% use utilization management programs to review discharges, care settings and effectiveness; 82% require prior authorization; and 89% have a mail order option for specialty drugs 17.26
Generic drugs: Drugs product that are no longer covered by patent protection and thus may be produced and/or distributed by multiple drug companies.
Preferred drugs: Drugs included on a formulary or preferred drug list; for example, a brand-name drug without a generic substitute.
Non-preferred drugs: Drugs not included on a formulary or preferred drug list; for example, a brand-name drug with a generic substitute.
Fourth-tier drugs: New types of cost-sharing arrangements that typically build additional layers of higher copayments or coinsurance for specifically identified types of drugs, such as lifestyle drugs or biologics.
Brand-name drugs: Generally, a drug product that is covered by a patent and is thus manufactured and sold exclusively by one firm. Cross-licensing occasionally occurs, allowing an additional firm to market the drug. After the patent expires, multiple firms can produce the drug product, but the brand name or trademark remains with the original manufacturer’s product.
Report: Section Ten: Plan Funding
Federal law (the Employee Retirement Income Security Act of 1974, or ERISA) exempts self-funded plans from most state insurance laws, including reserve requirements, mandated benefits, premium taxes, and consumer protection regulations. Sixty-one percent of covered workers are in a self-funded health plan. Self-funding is common among larger firms because they can spread the risk of costly claims over a large number of employees and dependents. Many self-funded plans use insurance, often called stoploss coverage, to limit the plan sponsor’s liability for very large claims or an unexpected level of expenses. Nearly three in five covered workers in fully or partially self-funded plans are in plans with stoploss protection.
Self-Funded Plan: An insurance arrangement in which the employer assumes direct financial responsibility for the costs of enrollees’ medical claims. Employers sponsoring self-funded plans typically contract with a third-party administrator or insurer to provide administrative services for the self-funded plan. In some cases, the employer may buy stoploss coverage from an insurer to protect the employer against very large claims.
Fully Insured Plan: An insurance arrangement in which the employer contracts with a health plan that assumes financial responsibility for the costs of enrollees’ medical claims.
Sixty-one percent of covered workers are in a plan that is completely or partially self-funded, similar to last year. The percentage of covered workers who are in a self-funded plan has increased over time from 49% in 2000 and 54% in 2005. In recent years, the percentage of covered workers enrolled in a self-funded plan has remained steady: 60% of covered workers were in such an arrangement in 2011; similar to 61% in 2016 1.
The percentage of covered workers enrolled in self-funded plans has been stable in recent years in both small firms (3-199 workers) and large firms (200 or more workers) 2.
The percentage of covered workers in self-funded plans differs by plan type: 69% of covered workers in PPOs, 67% in HDHP/SOs, 37% in HMOs, and 24% in POS plans are in a self-funded plan 3.
As expected, covered workers in large firms are significantly more likely to be in a self-funded plan than covered workers in small firms (82% vs. 13%). The percentage of covered workers in self-funded plans increases as the number of employees in a firm increases. Eighty-three percent of covered workers in firms with 1,000 to 4,999 workers and 94% of covered workers in firms with 5,000 or more workers are in self-funded plans in 2016 4.
Stoploss Coverage and Attachment Points
Fifty-seven percent of workers in self-funded health plans are in plans that have stoploss insurance 10. Stoploss coverage may limit the amount of claims that must be paid for each employee or may limit the total amount the plan sponsor must pay for all claims over the plan year.
The percentage of workers in self-funded health plans with stoploss insurance is unchanged from 2011, when the survey first asked about stoploss insurance (58% in 2011 and 57% in 2016).
Ninety-one percent of covered workers in self-funded plans that have stoploss protection are in plans where the stoploss insurance limits the amount that the plan must spend on each employee 11. This includes stoploss insurance plans that limit a firm’s per-employee spending and plans that limit both a firm’s overall spending and per-employee spending.
Firms with per-enrollee stoploss coverage were asked for the dollar amount where the stoploss coverage would start to pay for most or all of the claim (called an attachment point). The average attachment point in small firms is $160,000. For large firms with a per-person limit, the average attachment point is $330,000 11.
Among firms that purchase insurance underwritten by an insurer, 1% plan to self-insure because of ACA provisions 14.
Report: Section Eleven: Retiree Health Benefits
Retiree health benefits are an important consideration for older workers making decisions about their retirement. Health benefits for retirees provide an important supplement to Medicare for retirees age 65 or older. Over time, the percentage of firms offering retiree coverage has decreased.
Twenty-four percent of large firms (200 or more workers) that offer health benefits to their employees offer retiree coverage in 2016, similar to recent years. There has been a downward trend in the percentage of firms offering retirees coverage, from 34% in 2006 and 40% in 1999 1.
The offering of retiree health benefits varies considerably by firm characteristics.
Among large firms offering health benefits, the likelihood that a firm will offer retiree health benefits increases with size: from 21% of firms with 200-999 workers, to 36% of firms with 1,000-4,999 workers, to 46% of firms with 5,000 or more workers 2.
The share of large firms offering retiree health benefits varies considerably by industry. State and local governments (72%), firms in transportation/utilities/communication (55%) and firms in finance (46%) have particularly high rates of offer while retail firms (2%) have a particularly low rate 2.
Among large firms offering health benefits, those with a larger share of older workers (35% or more of workers are age 50 or older) are more likely to offer retiree health benefits than large firms with a smaller share of older workers (32% vs. 18%) 3.
Among large firms offering health benefits, those with a larger share of higher-wage workers (35% or more earn at least $59,000 per year) are more likely to offer retiree health benefits than those with a smaller share of higher-wage workers (30% vs. 20%) 3.
Among large firms offering health benefits, the share of public firms offering retiree benefits (58%) is higher than the shares of private for-profit firms (14%) or private not-for-profit firms (21%) offering retiree benefits 3.
Large firms with at least some union workers are more likely to offer retiree health benefits than large firms without any union workers (43% vs. 17%) 3.
Among all large firms offering retiree health benefits, most firms offer to early retirees under the age of 65 (92%). A lower percentage (72%) of large firms offering retiree health benefits offer to Medicare-age retirees. These percentages are similar to those in recent years 4.
Among all large firms offering retiree health benefits, 64% offer health benefits to both early and Medicare-age retirees.
Private Exchanges and Public Exchanges
Private exchanges have received considerable attention over the last several years. They are typically created by a consulting company, broker, or insurer, and are different than the public exchanges created under the Affordable Care Act (ACA). Private exchanges allow employees or retirees to choose from several health benefit options offered on the exchange. Six percent of large firms (200 or more workers) offering retiree health benefits report they offer benefits through a private exchange, similar to the percentage last year (7%) 7. For more information on the use of private exchanges for active employees, please see section 14.
Since 2014, households with an income between 100% and 400% of the federal poverty level and without an offer of employer coverage may be eligible for subsidized health insurance on federal and state exchanges. Some current retirees may be eligible for premium tax credits for coverage provided through these marketplaces.
Seventeen percent of large firms offering retiree health coverage report they are considering changes in the way they offer retiree health benefits because of the new marketplaces, lower than the percentage last year (26%) 9.
Report: Section Twelve: Health Risk Assessment, Biometrics Screening And Wellness Programs
Employers continue to show considerable interest in programs that help employees identify health issues and manage chronic conditions. Many employers believe that improving the health of their workers and their family members can improve morale, productivity and reduce health care costs.
In addition to offering wellness programs, a majority of large employers now offer health screening programs including health risk assessments, which are questionnaires asking employees about lifestyle, stress or physical health, and biometric screening, which we define as in-person health examinations conducted by a medical professional. Employers and insurers may use the health information collected during screenings to target wellness offerings or other health services to employees with risk conditions or behaviors that pose a risk for their health. Some employers have incentive programs that reward or penalize employees for different activities, including participating in wellness programs or completing health screenings.
In 2015 we revised the survey to better capture employers’ evolving approaches to wellness programs and health screening, including collecting information on employers’ use of incentive programs, so in most cases, statistics reported in 2015 and 2016 are not comparable to previous years’ findings because of these changes. Only firms offering health benefits were asked about their wellness and health promotion programs. Information about incentives is reported only for large firms (200 or more employees) because large shares of small firms (3-199 workers) did not know this information about their programs.
In 2016, of large firms offering health benefits, 59% offer employees the opportunity to complete health risk assessments, 53% offer employees the opportunity to complete biometric screening, and 83% offer employees wellness programs such as programs to help employees stop smoking, programs to help employees lose weight, or other lifestyle and behavioral coaching. Substantial shares of these large firms provide financial incentives for employees to participate in or complete the programs.
Health Risk Assessments
Some firms provide their employees the opportunity to complete a health risk assessment to identify potential health issues. Health risk assessments generally include questions about medical history, health status, and lifestyle.
Among firms offering health benefits, 32% of small firms and 59% of large firms provide employees the opportunity to complete a health risk assessment 1. Each of these is higher than the corresponding percentage for 2015 (18% for small firms and 50% for large firms) 2.
Seventy-four percent of firms offering health benefits with 5,000 or more employees provide employees the opportunity to complete a health risk assessment, similar to the percentage last year (72%) 1.
Some firms offer financial incentives to encourage employees to complete health risk assessments.
Among large firms that have a health risk assessment, 54% offer an incentive to employees to complete the assessment 4. Some firms offer more than one type of incentive to employees.
Among large firms offering incentives for employees to complete a health risk assessment, 51% lower premium contributions or reduce cost sharing; 60% offer cash, gift cards, merchandise or contributions to HSAs or HRAs; 44% require completion of a health risk assessment to be eligible for incentives under wellness or health promotion programs; and 5% offer additional paid time off 5.
Forty-one percent of covered workers in large firms providing the opportunity to complete a health risk assessment complete the assessment, similar to the percentage in 2015 (45%).
There is considerable variation in the percentage of workers who complete the assessment. Nineteen percent of large firms providing employees the opportunity to complete a health risk assessment report that more than 75% of their employees complete the assessment, while 41% report no more than 25% of employees complete the assessment 3.
Biometric Screening
Biometric screening is a health examination that measures an employee’s risk factors for certain medical issues such as cholesterol, blood pressure, stress, and nutrition. Biometric outcomes may include meeting a target body mass index (BMI) or cholesterol level. As defined by this survey, goals related to smoking are not included.
Among firms offering health benefits, 20% of small firms and 53% of large firms provide employees the opportunity to complete biometric screenings 7. These percentages are similar to last year (13% and 50%) 8.
Sixty-two percent of firms offering health benefits with 5,000 or more workers have biometric screening programs 7.
Firms that provide employees the opportunity to complete biometric screenings may include additional incentives for those employees who do so.
Among large firms with biometric screening programs, 59% offer an incentive for employees to complete the screening 10. Firms with 5,000 or more employees with biometric screening programs are more likely to have an incentive to complete the screening (70%) than firms in other size categories. Some firms report having more than one type of incentive.
Among large firms with an incentive for employees to complete biometric screening, 52% lower premium contributions or reduce cost sharing; 56% offer cash, gift cards, merchandise or contributions to HSAs or HRAs; 32% require completion of the screening to be eligible for incentives under wellness or health promotion programs; and 7% offer additional paid time off 11.
Among large firms with biometric screening programs, 14% have rewards or penalties for workers based on achieving specified biometric outcomes (e.g., meeting target BMI) 10.
There is considerable variation in the size of the incentives that employers offer for meeting biometric outcomes. Among large firms offering a reward or penalty for meeting biometric outcomes, the maximum reward is valued at a $150 dollars or less for 10% percent of firms and $1,000 or more for 21% of firms 13. Twenty-two percent of these firms combine the reward with incentives for other programs.
Wellness and Health Promotion Programs
Many employers and health plans offer programs to help employees engage in healthy lifestyles and reduce health risks. Wellness and health promotion programs may include exercise programs, health education classes, and stress-management counseling. These programs may be offered directly by the firm, an insurer, or a third-party contractor.
Among firms offering health benefits, 37% of small firms and 74% of large firms offer programs to help employees stop smoking, 33% of small firms and 68% of large firms offer programs to help employees lose weight, and 36% of small firms and 73% of large firms offer some other lifestyle or behavioral coaching program. Forty-six percent of small firms and 83% of large firms offering health benefits offer at least one of these three programs 15.
To encourage participation in wellness programs, firms may offer financial incentives to employees who participate in or complete wellness programs.
Forty-two percent of large firms offering one of these wellness or health promotion programs offer an incentive to encourage employees to participate in or complete the programs 16. Fifty-two percent of firms with more than 5,000 employees offering one of these wellness or health promotion programs offer an incentive to participate in or complete the programs.
Among large firms offering incentives to employees to participate in or complete wellness or health promotion programs, 34% lower premium contributions or reduce cost sharing; 76% offer cash, gift cards, merchandise or contributions to HSAs or HRAs; and 14% have some other type of incentive 17.
Firms with incentives for health risk assessment, biometric screening, or wellness or health promotion programs were asked to report the maximum reward or penalty an employee could earn for all of the firm’s health promotion activities combined. Some employers do not offer incentives for individual activities, but offer rewards to employees who complete a variety of activities. Among large firms offering incentives for any of these programs, the maximum value for all wellness-related incentives is $150 or less in 26% of firms and more than $1,000 in 16% of firms 18.
Firms with incentives for health risk assessment, biometric screening, or wellness or health promotion programs were also asked how effective they believed incentives were for encouraging participation. Thirty-one percent of large firms offering incentives for any one of these programs say the incentives are “very effective” at encouraging employees to participate, 56% say that the incentives are somewhat effect, while 10% say the incentives are not effective 19.
Among firms offering health benefits, 3% of small firms and 16% of large firms collect information from employees’ wearable devices, such as a Fitbit or Apple Watch, as part of their wellness or health promotion program 21.
Report: Section Thirteen: Grandfathered Health Plans
The Affordable Care Act (ACA) exempts certain health plans that were in effect when the law was passed, referred to as grandfathered plans, from some standards in the law, including the requirement to cover preventive benefits without cost sharing, have an external appeals process, or comply with the new benefit and rating provisions in the small group market. In 2016, 23% of firms offering health benefits offer at least one grandfathered health plan, and 23% of covered workers are enrolled in a grandfathered plan.
Grandfathered Plans: In the employer-sponsored market, health plans that were in place when the ACA was enacted (March 2010) can be grandfathered health plans. Department of Health and Human Services (HSS) rules stipulate that firms cannot significantly change cost sharing, benefits, employer contributions, or access to coverage in grandfathered plans. New employees can enroll in a grandfathered plan as long as the firm has maintained consecutive enrollment in the plan. Grandfathered plans are exempted from many, but not all, of the ACA’s consumer protection provisions.
In responding to the 2016 survey, some employers found it difficult to distinguish between the grandfathering provisions in the ACA and the guidance (sometimes called “grandmothering”) issued by HHS. We would note that smaller firms in particular appear to have some confusion about whether or not they are grandfathered. Many smaller firms, even those offering a health plan in effect in March 2010 (when the ACA was enacted), were unsure about whether their plan was grandfathered.
Twenty-three percent of offering firms report having at least one grandfathered plan in 2016, down from 35% in 2015 1.
Twenty-three percent of covered workers are enrolled in a grandfathered health plan in 2016 2.
The percentage of covered workers enrolled in a grandfathered plan is similar to 2015 (25%), but down from 36% in 2013, 48% in 2012, and 56% in 2011 4.
Covered workers in the south are more likely to be enrolled in a grandfathered plan and covered workers in the Midwest are less likely to be enrolled in a grandfathered plan than covered workers in other regions 2.
Report: Section Fourteen: Employer Opinions And Health Plan Practices
Employers play a significant role in health insurance coverage – so their opinions and experiences are important factors in health policy discussions. Employer practices continue to evolve, partially in response to Affordable Care Act provisions, including the employer shared responsibility provisions, which require large employers offer coverage or pay a fee, and the impending excise tax on high-cost plans.
Employers continue to innovate as to how they offer, structure, and deliver their benefits. A considerable number of employers have developed strategies to reduce costs or improve quality through changes to their plan’s provider networks.
Shopping for Health Coverage
Fifty-one percent of firms offering health benefits reported shopping for a new health plan or a new insurance carrier in the past year, similar to the percentages in recent years
Among firms that offer health benefits and who shopped for a new plan or carrier, 21% changed insurance carriers 2.
COBRA Premiums
Sixteen percent of small firms (3-199 workers) and 1% of large firms (200 or more workers) say they adjust the COBRA premium for former employees based on their age 24.
Networks and Delivery of Care
Many employers and health plans are delivering services through alternative sites of care.
Sixty-one percent of firms that offer health benefits cover services provided in retail health clinics, such as those found in pharmacies, supermarkets and retail stores 9. These percentages are similar to those reported in 2014 when this question was last asked.
Large firms are more likely to cover services provided through retail health clinics than small firms (73% vs. 60%) 9.
Six percent of firms that cover services provided in retail clinics have a financial incentive for enrollee to receive services in a clinic as compared to visiting a physician’s office 9. Large firms are more likely to have such a financial incentive than small firms (10% vs. 6%).
Thirty-nine percent of large firms offering health benefits cover the provision of some health care services through telecommunication in their largest health plan 7. The question in the survey were revised for 2016 to clarify that we were asking about payment for services and not just the electronic exchange of information.
Among these firms, 33% report that workers have a financial incentive to receive services through telemedicine rather than visiting a physician’s office 7.
Among firms with at least 50 employees offering health benefits, 5% provide health services to employees through an on-site health clinic at one of their major locations 11.
Eighty-six percent of these firms allow employees to receive treatment for non-work-related services through the on-site clinic 11.
Firms with at least 1,000 workers were more likely to have an on-site health clinic than smaller firms (25% vs. 4%).
A tiered or high-performance network groups providers in the network together based on quality, cost, and/or the efficiency of the care they deliver. These networks encourage patients to visit preferred doctors by either restricting networks to efficient providers, or by having different cost sharing requirements based on the provider’s tier.
Fourteen percent of large firms that offer health benefits include a high-performance or tiered provider network in their health plan with the largest enrollment, down from 24% in 2015. The largest firms (those with 1,000 or more employees) are more likely to incorporate a high-performance or tiered network into their largest plan 6.
Firms offering health benefits were asked whether they offered a plan that they considered to be a narrow network. Narrow networks are plans that limit the number of providers who can participate in order to reduce costs. Narrow network plans are generally more restrictive than standard HMO networks.
Six percent of offering firms with 50 or more employees indicated that they offer a plan they considered to be a narrow network plan, similar to the percentages reported in the last few years 4.
Six percent of firms offering health benefits said that either they or their insurer eliminated a hospital or health system from a provider network in order to reduce the plan’s cost
.
Private exchanges
There has been considerable interest in private exchanges recently. An exchange is a marketplace for health insurance. Private exchanges allow employees to choose from several health benefit options offered on the exchange. Private exchanges generally are created by consulting firms, insurers, or brokers, and are different than the public exchanges that have been created by states or the federal government. There is considerable variation in the types of exchanges currently offered; some exchanges allow workers to choose between multiple plans offered by the same carrier while in other cases multiple carriers participate. The exchange operator may establish strict standards for the plans offered or allow the insurers more flexibility in determining their plan offerings.
Four percent of firms offering health benefits with 50 or more employees offer coverage through a private exchange. Looking at worker enrollment, private exchanges cover 2% of covered workers at firms with 50 or more employees 15. These percentages are similar to those in 2015.
Firms offering health benefits with 50 or more employees and who do not already offer health benefits through a private exchange were asked whether they were considering private exchanges in the future. Eighteen percent of these firms are considering offering benefits through a private exchange, similar to the percentage last year 14.
Private exchanges may or may not include a defined contribution for premiums. A defined contribution is a set dollar amount offered to the employee by the employer. Employees may then select one of several plans, paying the difference between the defined contribution and the cost of their chosen health insurance plan. This permits an employer to offer a larger variety of health plans to employees and to structure contributions or other rules to encourage employees to choose more efficient plans.
Firms offering health benefits with 50 or more employees and who do not already offer health benefits through a private exchange were asked whether they were considering a defined contribution approach. Twenty-one percent of these firms were considering such an approach 14.
Employer shared responsibility
The Affordable Care Act (ACA) provision requiring employers with at least 50 full-time equivalent employees (FTEs) to offer health benefits that meet minimum standards for value and affordability to their full-time workers or pay a penalty took full effect in 2016.
Among firms offering health benefits with at least 50 FTEs, 97% report that they offer a health plan to at least 95% of their employees who worked on average 30 hours per week or more, and 96% report that they offer at least one health plan that meets the ACA standards for affordability and minimum value 22.
Firms made changes to their employment practices in response to the employer shared responsibility requirement:
Two percent of firms offering health benefits say they changed or planned to change the job classifications of some employees from full-time to part-time so that they would not be eligible for health benefits, while 7% said they changed or planned to change job classifications of some employees from part-time to full-time so that they would become eligible for health benefits 23.
Two percent of firms offering health benefit say they increased or were planning to increase the waiting period before new employees become eligible for benefits 23.
Twelve percent of firms offering health benefits say they extended or were planning to extend eligibility for health benefits to workers who were not previously eligible, and 2% reported extending or planning to extend eligibility for more comprehensive benefits to employees previously eligible only for limited benefits 23. Four percent of these firms reported that they reduced the number of employees they intended to hire because of the cost of providing health benefits 23.
Excise tax on high cost health plans
Under the ACA, employer health plans in 2020 will be subject to an excise tax of 40% on the amount by which their cost exceeds specified thresholds.27 The tax was scheduled to take effect in 2018, but its effective date was delayed two years. The tax is calculated with respect to each employee based on the combinations of health benefits received by that employee, including the employer and employee share of health plan premiums (or premium equivalents for self-funded plans), Flexible Spending Account (FSA) contributions, and employer contributions to health savings accounts and health reimbursement arrangement contributions. In anticipation of the high-cost plan tax (sometimes referred to as the “Cadillac plan tax”), some employers have begun making changes to their health benefits.
Among firms offering health benefits, 15% of small firms and 64% of large firms say that they have conducted an analysis to determine if one of their plans will be subject to the tax when it takes effect 19.
Among firms who have conducted an analysis, 29% report their plan with the largest enrollment will exceed the thresholds in 2020 20.
Some employers have already taken action to mitigate the anticipated impacts of the high-cost plan excise tax.
Three percent of small firms and 9% of large firms say they have switched to a lower cost plan or eliminated a plan option 19.
Four percent of small firms and 15% of large firms say they have increased cost sharing 19.
Four percent of small firms and 2% of large firms say they selected a plan with a smaller network of providers 19.
Three percent of small firms and 8% of large firms say they moved benefit options to an account-based plan such as an HRA or HSA 19.
Thirty-one percent of employers who conducted an analysis of the anticipated impact of the high-cost plan excise tax say that the delay in the implantation date from 2018 to 2020 caused them to reconsider or postpone changes that they had planned to make 21.
Survey Design And Methods
The Kaiser Family Foundation and the Health Research & Educational Trust (Kaiser/HRET) conduct this annual survey of employer-sponsored health benefits. HRET, a nonprofit research organization, is an affiliate of the American Hospital Association. The Kaiser Family Foundation designs, analyzes, and conducts this survey in partnership with HRET, and also funds the study. Kaiser contracts with researchers at NORC at the University of Chicago (NORC) to work with the Kaiser and HRET researchers in conducting the study. Kaiser/HRET retained National Research, LLC (NR), a Washington, D.C.-based survey research firm, to conduct telephone interviews with human resource and benefits managers using the Kaiser/HRET survey instrument. From January to June 2016, NR completed full interviews with 1,933 firms.
Survey Topics
Kaiser/HRET asks each participating firm as many as 400 questions about its largest health maintenance organization (HMO), preferred provider organization (PPO), point-of-service (POS) plan, and high-deductible health plan with a savings option (HDHP/SO).28 We treat exclusive provider organizations (EPOs) and HMOs as one plan type and report the information under the banner of “HMO”; if an employer sponsors both an HMO and an EPO, they are asked about the attributes of the plan with the larger enrollment. Similarly, starting in 2013, plan information for conventional (or indemnity) plans was collected within the PPO battery. Less than 1% of firms that completed the PPO section had more enrollment in a conventional plan than in a PPO plan.
The survey includes questions on the cost of health insurance, health benefit offer rates, coverage, eligibility, enrollment patterns, premium contributions,29 employee cost sharing, prescription drug benefits, retiree health benefits, and wellness benefits.
Firms are asked about the attributes of their current plans during the interview. While the survey’s fielding period begins in January, many respondents may have a plan whose 2016 plan year has not yet begun (Exhibit M.4). In some cases, plans may report the attributes of their 2015 plans and some plan attributes (such as HSA deductible limits) may not meet the calendar year regulatory requirements.
Exhibit M.4: Among Firms Offering Health Benefits, Month in Which Plan Year Begins, 2016
Response Rate
After determining the required sample from U.S. Census Bureau data, Kaiser/HRET drew its sample from a Survey Sampling Incorporated list (based on an original Dun and Bradstreet list) of the nation’s private employers and from the Census Bureau’s Census of Governments list of public employers with three or more workers. To increase precision, Kaiser/HRET stratified the sample by ten industry categories and six size categories. Kaiser/HRET attempted to repeat interviews with prior years’ survey respondents (with at least ten employees) who participated in either the 2014 or the 2015 survey, or both. Firms with 3-9 employees are not included in the panel to minimize the impact of panel effects on the offer rate statistic. As a result, 1,457 of the 1,933 firms that completed the full survey also participated in either the 2014 or 2015 surveys, or both.30 The overall response rate is 40%.31 To increase response rates, firms with 3–9 employees were offered an incentive of $75 in cash or as a donation to a charity of their choice to complete the full survey.
The vast majority of questions are asked only of firms that offer health benefits. A total of 1,687 of the 1,933 responding firms indicated they offered health benefits. The response rate for firms that offer health benefits is also 40%.
We asked one question of all firms in the study with which we made phone contact but where the firm declined to participate. The question was, “Does your company offer a health insurance program as a benefit to any of your employees?” A total of 3,110 firms responded to this question (including 1,933 who responded to the full survey and 1,177 who responded to this one question). These responses are included in our estimates of the percentage of firms offering health benefits.32 The response rate for this question is 65%. In 2012, the calculation of the response rates was adjusted to be slightly more conservative than previous years.
Beginning in 2014, we collected whether firms with a non-final disposition code (such as a firm that requested a callback at a later time or date) offered health benefits. By doing so we attempt to mitigate any potential non-response bias of firms either offering or not offering health benefits on the overall offer rate statistic. In 2016, 353 of the 1,173 firm responses that solely answered the offer question were obtained through this pathway.
Firm Size Categories and Key Definitions
Throughout the report, exhibits categorize data by size of firm, region, and industry. Firm size definitions are as follows: small firms: 3 to 199 workers; and large firms: 200 or more workers. (Exhibit M.1) shows selected characteristics of the survey sample. A firm’s primary industry classification is determined from Survey Sampling International’s (SSI) designation on the sampling frame and is based on the U.S. Census Bureau’s North American Industry Classification System (NAICS). A firm’s ownership category and other firm characteristics used in exhibits such as 3.3 and 6.21 are based on respondents’ answers. While there is considerable overlap in firms in the “State/Local Government” industry category and those in the “public” ownership category, they are not identical. For example, public school districts are included in the service industry even though they are publicly owned.
Exhibit M.1: Selected Characteristics of Firms in the Survey Sample, 2016
(Exhibit M.3) presents the breakdown of states into regions and is based on the U.S Census Bureau’s categorizations. State-level data are not reported both because the sample size is insufficient in many states and we only collect information on where a firm is headquartered rather than where workers are actually employed. Some mid- and large-size employers have employees in more than one state, so the location of the headquarters may not match the location of the plan for which we collected premium information.
Exhibit M.3: States by Region, 2016
(Exhibit M.2) displays the distribution of the nation’s firms, workers, and covered workers (employees receiving coverage from their employer). Among the over three million firms nationally, approximately 60.8% employ 3 to 9 workers; such firms employ 7.9% of workers, and 3.3% of workers covered by health insurance. In contrast, less than 1% of firms employ 5,000 or more workers; these firms employ 35.4% of workers and 38.9% of covered workers. Therefore, the smallest firms dominate any statistics weighted by the number of employers. For this reason, most statistics about firms are broken out by size categories. In contrast, firms with 1,000 or more workers are the most influential employer group in calculating statistics regarding covered workers, since they employ the largest percentage of the nation’s workforce.
Exhibit M.2: Distribution of Employers, Workers, and Workers Covered by Health Benefits, by Firm Size, 2016
Throughout this report, we use the term “in-network” to refer to services received from a preferred provider. Family coverage is defined as health coverage for a family of four.
The survey asks firms what percentage of their employees earn less than a specified amount in order to identify the portion of a firm’s workforce that has relatively low wages. This year, the income threshold is $23,000 per year for lower-wage workers and $59,000 for higher-wage workers. These thresholds are based on the 25th and 75th percentile of workers’ earnings as reported by the Bureau of Labor Statistics using data from the Occupational Employment Statistics (OES) (2015).33 The cutoffs were inflation-adjusted and rounded to the nearest thousand. Prior to 2013, wage cutoffs were calculated using the now-eliminated National Compensation Survey.
Rounding and Imputation
Some exhibits in the report do not sum to totals due to rounding. In a few cases, numbers from distribution exhibits may not add to the numbers referenced in the text due to rounding. Although overall totals and totals for size and industry are statistically valid, some breakdowns may not be available due to limited sample sizes or a high relative standard error. Where the unweighted sample size is fewer than 30 observations, exhibits include the notation “NSD” (Not Sufficient Data). Many breakouts by subsets may have a large standard error, meaning that even large differences are not statistically different.
To control for item nonresponse bias, Kaiser/HRET imputes values that are missing for most variables in the survey. On average, 6% of observations are imputed. All variables are imputed following a hotdeck approach. The hotdeck approach replaces missing information with observed values from a firm similar in size and industry to the firm for which data are missing. In 2016, there were 12 variables where the imputation rate exceeded 20%; most of these cases were for individual plan level statistics – when aggregate variables were constructed for all of the plans, the imputation rate is usually much lower. There are a few variables that Kaiser/HRET has decided not to impute; these are typically variables where “don’t know” is considered a valid response option (for example, firms’ opinions about the effectiveness of incentives to encourage worker participation in health and wellness programs). In addition, there are several variables in which missing data are calculated based on respondents’ answers to other questions (for example, employer contributions to premiums are calculated from the respondent’s premium and the worker contribution to premiums).
Starting in 2012, the method to calculate missing premiums and contributions was revised; if a firm provides a premium for single coverage or family coverage, or a worker contribution for single coverage or family coverage, that information is used in the imputation. For example, if a firm provided a worker contribution for family coverage but no premium information, a ratio between the family premium and family contribution was imputed and then the family premium was calculated. In addition, in cases where premiums or contributions for both family and single coverage were missing, the hotdeck procedure was revised to draw all four responses from a single firm. The change in the imputation method did not have a significant impact on the premium or contribution estimates.
Starting in 2014, we estimate separate single and family coverage premiums for firms that provide premium amounts as the average cost for all covered workers, instead of differentiating between single and family coverage. This method more accurately accounts for the portion that each type of coverage contributes to the total cost for the 0.4% of covered workers who are enrolled at firms affected by this adjustment.
Sample Design
We determined the sample requirements based on the universe of firms obtained from the U.S. Census Bureau. Prior to the 2010 survey, the sample requirements were based on the total counts provided by Survey Sampling Incorporated (SSI) (which obtains data from Dun and Bradstreet). Over the years, we found the Dun and Bradstreet frequency counts to be volatile due to duplicate listings of firms, or firms that are no longer in business. These inaccuracies vary by firm size and industry. In 2003, we began using the more consistent and accurate counts provided by the Census Bureau’s Statistics of U.S. Businesses and the Census of Governments as the basis for post-stratification, although the sample was still drawn from a Dun and Bradstreet list. In order to further address this concern at the time of sampling, starting in 2009, we use Census Bureau data to determine the number of firms to attempt to interview within each size and industry category.
Starting in 2010, we defined Education as a separate sampling category for the purposes of sampling, rather than as a subgroup of the Service category. In the past, Education firms were a disproportionately large share of Service firms. Education is controlled for during post-stratification, and adjusting the sampling frame to also control for Education allows for a more accurate representation of both the Education and Service industries.
In past years, both private and government firms were sampled from the Dun and Bradstreet database. Beginning in 2009, Government firms were sampled from the 2007 Census of Governments. This change was made to eliminate the overlap of state agencies that were frequently sampled from the Dun and Bradstreet database. The sample of private firms is screened for firms that are related to state/local governments, and if these firms are identified in the Census of Governments, they are reclassified as government firms and a private firm is randomly drawn to replace the reclassified firm. The federal government is not included in the sample frame.
Finally, the data used to determine the 2016 Employer Health Benefits Survey sample frame include the U.S. Census’ 2012 Statistics of U.S. Businesses and the 2012 Census of Governments. At the time of the sample design (December 2015), these data represented the most current information on the number of public and private firms nationwide with three or more workers. As in the past, the post-stratification is based on the most up-to-date Census data available (the 2013 update to the Census of U.S. Businesses was purchased during the survey fielding period).
Weighting and Statistical Significance
Because Kaiser/HRET selects firms randomly, it is possible through the use of statistical weights to extrapolate the results to national (as well as firm size, regional, and industry) averages. These weights allow us to present findings based on the number of workers covered by health plans, the number of total workers, and the number of firms. In general, findings in dollar amounts (such as premiums, worker contributions, and cost sharing) are weighted by covered workers. Other estimates, such as the offer rate, are weighted by firms. Specific weights were created to analyze the HDHP/SO plans that are offered with a Health Reimbursement Arrangement (HRA) or that are Health Savings Account (HSA)-qualified. These weights represent the proportion of employees enrolled in each of these arrangements.
Calculation of the weights follows a common approach. We trimmed the weights in order to reduce the influence of weight outliers. First, we grouped firms into size and offer categories of observations. Within each strata, we identified the median and the interquartile range of the weights and calculated the trimming cut point as the median plus six times the interquartile range (M + [6 * IQR]). Weight values larger than this cut point are trimmed to the cut point. In all instances, very few weight values were trimmed. Finally, we calibrated the weights to U.S. Census Bureau’s 2013 Statistics of U.S. Businesses for firms in the private sector, and the 2012 Census of Governments as the basis for calibration / post-stratification for public sector firms. Historic employer-weighted statistics were updated in 2011.
We conducted a follow-up survey of those firms with 3 to 49 workers that refused to participate in the full survey and conducted a McNemar test to verify that the results of the follow-up survey are comparable to the results from the original survey.
Between 2006 and 2012, only limited information was collected on conventional plans. Starting in 2013, information on conventional plans is collected under the PPO section and therefore, the covered worker weight is representative of all plan types for which the survey collects information.
The survey contains a few questions on employee cost sharing that are asked only of firms that indicate in a previous question that they have a certain cost-sharing provision. For example, copayment amounts for physician office visits are asked only of those that report they have copayments for such visits. Because the composite variables (using data from across all plan types) are reflective of only those plans with the provision, separate weights for the relevant variables were created in order to account for the fact that not all covered workers have such provisions.
To account for design effects, the statistical computing package R and the library package “survey” were used to calculate standard errors.34,35 All statistical tests are performed at the .05 confidence level, unless otherwise noted. For figures with multiple years, statistical tests are conducted for each year against the previous year shown, unless otherwise noted. No statistical tests are conducted for years prior to 1999. In 2012, the method to test the difference between distributions across years was changed to use a Wald test, which accounts for the complex survey design. In general, this method is more conservative than the approach used in prior years.
Statistical tests for a given subgroup (firms with 25-49 workers, for instance) are tested against all other firm sizes not included in that subgroup (all firm sizes NOT including firms with 25-49 workers, in this example). Tests are done similarly for region and industry; for example, Northeast is compared to all firms NOT in the Northeast (an aggregate of firms in the Midwest, South, and West). However, statistical tests for estimates compared across plan types (for example, average premiums in PPOs) are tested against the “All Plans” estimate. In some cases, we also test plan-specific estimates against similar estimates for other plan types (for example, single and family premiums for HDHP/SOs against single and family premiums for HMO, PPO, and POS plans); these are noted specifically in the text. The two types of statistical tests performed are the t-test and the Wald test. The small number of observations for some variables resulted in large variability around the point estimates. These observations sometimes carry large weights, primarily for small firms. The reader should be cautioned that these influential weights may result in large movements in point estimates from year to year; however, these movements are often not statistically significant.
2016 Survey
Between 2015 and 2016, we conducted a series of focus groups that led us to the conclusion that human resource and benefit managers at firms with between 20 and 49 employees think about health insurance premiums more similarly to benefit managers at smaller firms than larger firms. Therefore, starting in 2016, we altered the health insurance premium question pathway for firms with between 20-49 employees to match that of firms with 3-19 employees rather than firms with 50 or more employees. This change affected firms representing 8% of the total covered worker weight. We believe that these questions produce comparable responses and that this edit does not create a break in trend.
Firms with 50 or more workers were asked: “Does your firm offer health benefits for current employees through a private or corporate exchange?” Employers were still asked for plan information about their HMO, PPO, POS and HDHP/SO plan regardless of whether they purchased health benefits through a private exchange or not.
Starting in 2015, employers were asked how many full-time equivalent workers (FTEs) they employed. In cases in which the number of full-time equivalents was relevant to the question, interviewer skip patterns may have depended on the number of FTEs. In 2016, questions were added to ask firms to estimate the number of hours that a typical part-time worker averaged over the course of one week in order to more accurately determine which firms might be subject to the Employer Shared Responsibility Provision of the Affordable Care Act. In cases where a firm did not know how many FTEs it employed, we calculated the number based on the number of part-time hours the firm reported. In all cases, we assumed that firms with more than 250 full time employees had more than 50 FTES.
Starting in 2016, we made significant revisions to how the survey asks employers about their prescription drug coverage. In most cases, information reported in Prescription Drug Benefits (Section 9) is not comparable with previous years’ findings. First, in addition to the four standard tiers of drugs (generics, preferred, non-preferred, and lifestyle), we began asking firms about cost sharing for a drug tier that covers only specialty drugs. This new tier pathway in the questionnaire has an effect on the trend of the four standard tiers, since respondents to the 2015 survey might have previously categorized their specialty drug tier as one of the other four standard tiers. We did not modify the question about the number of tiers a firm’s cost-sharing structure has, but in cases in which the highest tier covered exclusively specialty drugs we reported it separately. For example, in Exhibits 9.3 and 9.4, a firm with three tiers may only have copays or coinsurances for two tiers because their third tier copay or coinsurance is being reported as a specialty tier. Furthermore, in order to reduce survey burden, firms were asked about the plan attributes of only their plan type with the most enrollment. Therefore, in most cases, we no longer make comparisons between plan types. Lastly, prior to 2016, we required firms’ cost sharing tiers to be sequential, meaning that the second tier copay was higher than the first tier, the third tier was higher than the second, and the fourth was higher than the third. As drug formularies have become more intricate, many firms have minimum and maximums attached to their copays and coinsurances, leading us to believe it was no longer appropriate to assume that a firm’s cost sharing followed this sequential logic.
In cases where a firm had multiple plans, they were asked about their strategies for containing the cost of specialty drugs for the plan type with the largest enrollment. Between 2015 and 2016, we modified the series of ‘Select All That Apply’ questions regarding cost containment strategies for specialty drugs. In 2016, we elected to impute firms’ responses to these questions. We removed the option “Separate cost sharing tier for specialty drugs” and added specialty drugs as their own drug tier questionnaire pathway. We added question options on mail order drugs and prior authorization.
We discovered that the HRA and HSA distribution cutoff thresholds presented in prior years’ High Deductible Health Plan Section (Section 8) were calculated using each firm’s covered worker weight rather than the HRA- or HSA-specific enrollment weights. Starting in 2016, the means and their subsequent distributions are now calculated using these plan-specific enrollment weights and therefore those thresholds are not directly comparable to prior-year statistics.
In our 2015 calculation of out-of-pocket (OOP) maximums, we mistakenly included plans in our calculations with $0 OOP maximums, representing 2.4% the total of covered worker weight, which pushed the distribution downward in 2015 Exhibit 7.31. In the same 2016 exhibit (7.36), firms with $0 OOP maximums have been excluded.
Twenty-five firms reported allowing flexible spending account (FSA) employee contributions above the legal limit of $2,550 in 2016. Although these firms were asked to confirm that their maximum contributions were above $2,550, we nonetheless recoded their responses to the legal ceiling of $2,550 and intend to provide additional clarification that we are interested in only a firm’s health FSA in the future.
In 2016, we modified our questions about telemedicine to clarify that we were interested in the provision of health care services, and not merely the exchange of information, through telecommunication. We also added dependent and spousal questions to our health risk assessment question pathway.
In 2016, we ceased publication of the slide “Percentage of Firms Offering Health Benefits, by Firm Characteristics” (Exhibit 2.4 in the 2015 EHBS report). Since firm characteristics are not collected from respondents that solely answer the offer question, this exhibit had been calculated using the employer weight derived from only firms that had completed the full survey.
Annual inflation estimates are usually calculated from April to April. The 12 month percentage change for May to May was 1%.36
Historical Data
Data in this report focus primarily on findings from surveys jointly authored by the Kaiser Family Foundation and the Health Research & Educational Trust, which have been conducted since 1999. Prior to 1999, the survey was conducted by the Health Insurance Association of America (HIAA) and KPMG using a similar survey instrument, but data are not available for all the intervening years. Following the survey’s introduction in 1987, the HIAA conducted the survey through 1990, but some data are not available for analysis. KPMG conducted the survey from 1991-1998. However, in 1991, 1992, 1994, and 1997, only larger firms were sampled. In 1993, 1995, 1996, and 1998, KPMG interviewed both large and small firms. In 1998, KPMG divested itself of its Compensation and Benefits Practice, and part of that divestiture included donating the annual survey of health benefits to HRET.
This report uses historical data from the 1993, 1996, and 1998 KPMG Surveys of Employer-Sponsored Health Benefits and the 1999-2015 Kaiser/HRET Survey of Employer-Sponsored Health Benefits. For a longer-term perspective, we also use the 1988 survey of the nation’s employers conducted by the HIAA, on which the KPMG and Kaiser/HRET surveys are based. The survey designs for the three surveys are similar.
Endnotes
Kaiser Commission on Medicaid and the Uninsured. The uninsured: A primer—key facts about health insurance and the uninsured in America [Internet]. Washington (DC): The Commission; 2015 Nov [cited 2016 Aug 1]. https://modern.kff.org/uninsured/report/the-uninsured-a-primer/. See supplemental tables – Table 1: 270.2 million non-elderly people, 55.5% of whom are covered by ESI. ↩︎
Kaiser/HRET surveys use the April-to-April time period, as do the sources in this and the following note. The inflation numbers are not seasonally adjusted. Bureau of Labor Statistics. Consumer Price Index – All Urban Consumers: Department of Labor; 2015. [cited 2016 July 28] http://data.bls.gov/timeseries/CUUR0000SA0?output_view=pct_1mth. Wage data are from the Bureau of Labor Statistics and based on the change in total average hourly earnings of production and nonsupervisory employees. Employment, hours, and earnings from the Current Employment Statistics survey: Department of Labor; 2016 [cited 2016 July 28]. http://data.bls.gov/timeseries/CES0500000008↩︎
The change in enrollment in HDHP/SO between 2014 (20%) and 2016 (29%) is 8% due to rounding. ↩︎
The change in enrollment in HDHP/SO between 2014 (20%) and 2016 (29%) is 8% due to rounding. ↩︎
Because surveys only collect information from a portion of the total number of firms in the country, there is uncertainty in any estimate. Since there are so many small firms, sometimes even seemingly large differences are not statistically different. For more information on the Employer Health Benefits Survey’s weighting and design please see the Survey Design and Methods section. ↩︎
Kaiser Commission on Medicaid and the Uninsured. The uninsured: A primer—key facts about health insurance and the uninsured in America [Internet]. Washington (DC): The Commission; 2015 Nov [cited 2016 Aug 1]. https://modern.kff.org/uninsured/report/the-uninsured-a-primer/. See supplemental tables – Table 1: 270.2 million non-elderly people, 55.5% of whom are covered by ESI. ↩︎
In 2009, Kaiser/HRET began weighting the percentage of workers that take up coverage by the number of workers eligible for coverage. The historical take up estimates have also been updated. See the Survey Design and Methods section for more information. ↩︎
Variable hour employees may have a measurement period of up to 12 months before it is determined if they are eligible for benefits. Employers may require a cumulative service requirement of up to 1,200 hours before an employee may enroll. Federal Register. Vol. 79, No. 36. Feb 12, 2014. https://www.gpo.gov/fdsys/pkg/FR-2014-02-24/pdf/2014-03809.pdf↩︎
Starting in 2010, we included firms that said they offer a plan type even if there are no covered workers enrolled in that plan type. ↩︎
The change in enrollment in HDHP/SO between 2014 (20%) and 2016 (29%) is 8% due to rounding. ↩︎
Estimates for premiums, worker contributions to premiums, and employer contributions to premiums presented in Section 6 do not include contributions made by the employer to Health Savings Accounts (HSAs) or Health Reimbursement Arrangements (HRAs). See Section 8 for estimates of employer contributions to HSAs and HRAs. ↩︎
The average percent contribution is calculated as a weighted average of all a firm’s plan types and may not necessarily equal the average worker contribution divided by the average premium. ↩︎
For definitions of Self-Funded and Fully-Insured plans, see the introduction to Section 10. ↩︎
Some workers with separate per-person deductibles or out-of-pocket maximums for family coverage do not have a specific number of family members that are required to meet the deductible amount and instead have another type of limit, such as a per-person amount with a total dollar amount limit. These responses are included in the averages and distributions for separate family deductibles and out-of-pocket maximums. ↩︎
Starting in 2010, the survey asked about the prevalence and cost of physician office visits separately for primary care and specialty care. Prior to the 2010 survey, if the respondent indicated the plan had a copayment for office visits, we assumed the plan had a copayment for both primary and specialty care visits. The survey did not allow for a respondent to report that a plan had a copayment for primary care visits and coinsurance for visits with a specialist physician. The changes made in 2010 allow for variations in the type of cost sharing for primary care and specialty care visits. The survey includes cost sharing for in-network services only. ↩︎
For those enrolled in an HDHP/HSA, the out-of-pocket maximum is $6,550 for an individual plan and $13,100 for a family plan. ↩︎
There is no legal requirement for the minimum deductible in a plan offered with an HRA. The survey defines a high-deductible HRA plan as a plan with a deductible of at least $1,000 for single coverage and $2,000 for family coverage. Federal law requires a deductible of at least $1,300 for single coverage and $2,600 for family coverage for HSA-qualified HDHPs in 2016. See the Text Box for more information on HDHP/HRAs and HSA-qualified HDHPs. ↩︎
The definitions of HDHP/SOs do not include other consumer-driven plan options, such as arrangements that combine an HRA with a lower-deductible health plan or arrangements in which an insurer (rather than the employer as in the case of HRAs or the enrollee as in the case of HSAs) establishes an account for each enrollee. Other arrangements may be included in future surveys as the market evolves. ↩︎
The survey asks “Up to what dollar amount does your firm promise to contribute each year to an employee’s HRA or health reimbursement arrangement for single coverage?” We refer to the amount that the employer commits to make available to an HRA as a contribution for ease of discussion. As discussed, HRAs are notional accounts, and employers are not required to actually transfer funds until an employee incurs expenses. Thus, employers may not expend the entire amount that they commit to make available to their employees through an HRA. Some employers may make their HRA contribution contingent on other factors, such as completing wellness programs. ↩︎
See the Methods Section for more information. In cases in which a firm indicated that one of their tiers was exclusively for specialty drugs, we reported the cost-sharing structure and any copay or coinsurance information under the specialty drug banner. Therefore, a firm that has three tiers of cost sharing may only have plan attributes for the generic and preferred tier. ↩︎
See the Methods Section for changes in these questions and responses as compared to 2015. ↩︎
HDHP/SO includes high-deductible health plans with a deductible of at least $1,000 for single coverage and $2,000 for family coverage and that offer either a Health Reimbursement Arrangement (HRA) or a Health Savings Account (HSA). Although HRAs can be offered along with a health plan that is not an HDHP, the survey collected information only on HRAs that are offered along with HDHPs. For specific definitions of HDHPs, HRAs, and HSAs, see the introduction to Section 8. ↩︎
HDHP/SO premium estimates do not include contributions made by the employer to Health Savings Accounts or Health Reimbursement Arrangements. ↩︎
In total, 124 firms participated in 2014, 269 firms participated in 2015, and 1,064 firms participated in both 2014 and 2015. ↩︎
Response rate estimates are calculated by dividing the number of completes over the number of refusals and the fraction of the firms with unknown eligibility to participate estimated to be eligible. Firms determined to be ineligible to complete the survey are not included in the response rate calculation. ↩︎
Estimates presented in Exhibits 2.1, 2.2, 2.3 and 2.5 are based on the sample of both firms that completed the entire survey and those that answered just one question about whether they offer health benefits. ↩︎
Analysis of the 2011 survey data using both R and SUDAAN (the statistical package used prior to 2012) produced the same estimates and standard errors. ↩︎
A supplement with standard errors for select estimates can be found online at Technical Supplement: Standard Error Tables for Selected Estimates, http://ehbs.kff.org↩︎