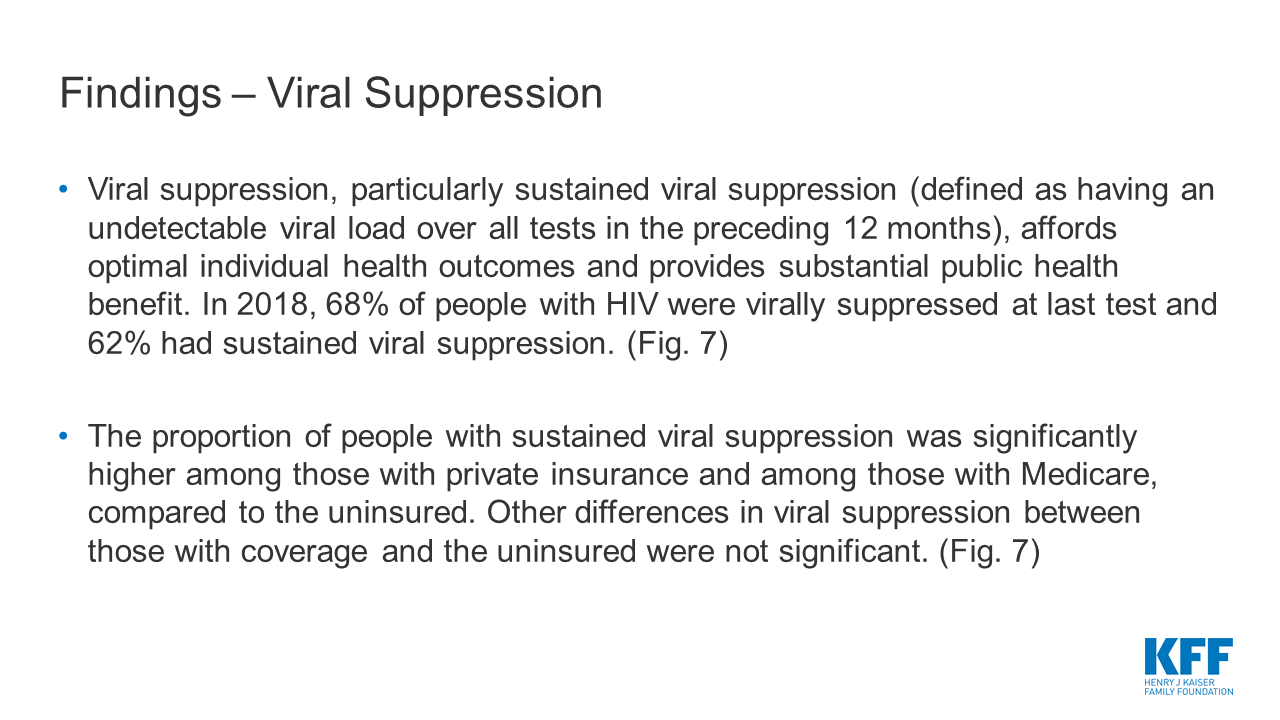
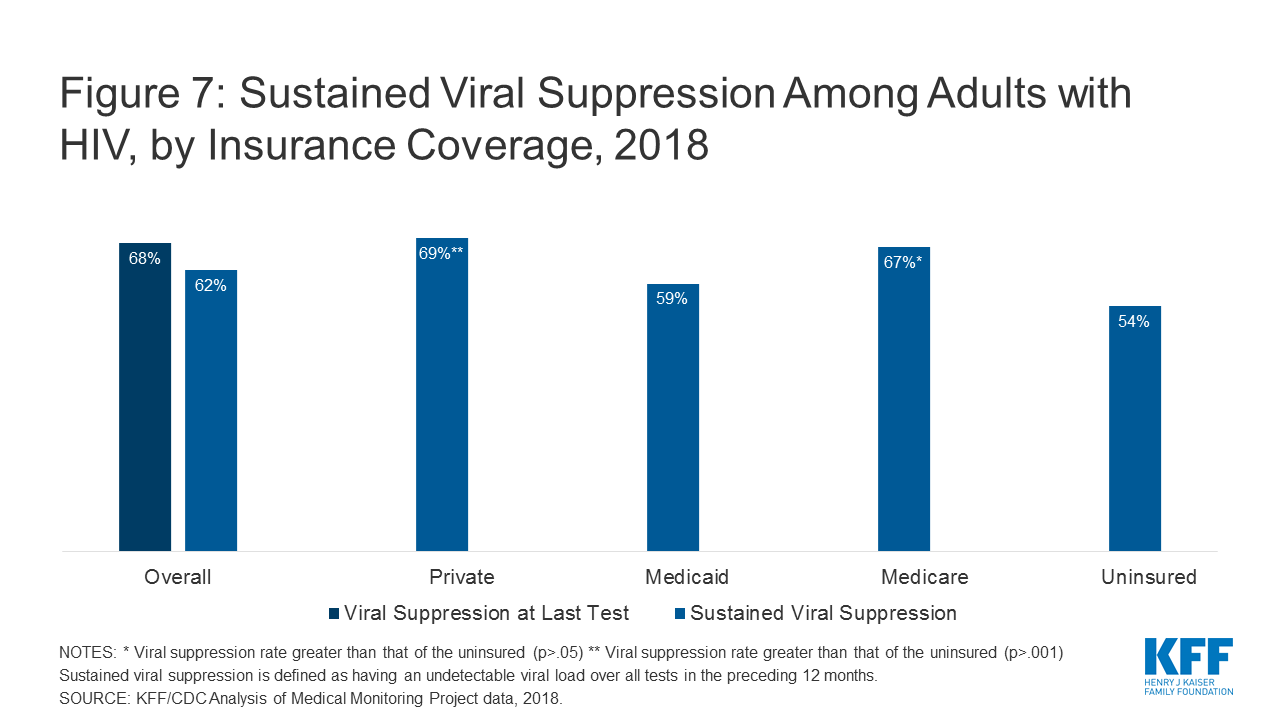
Supreme Court Decision June 29, 2020
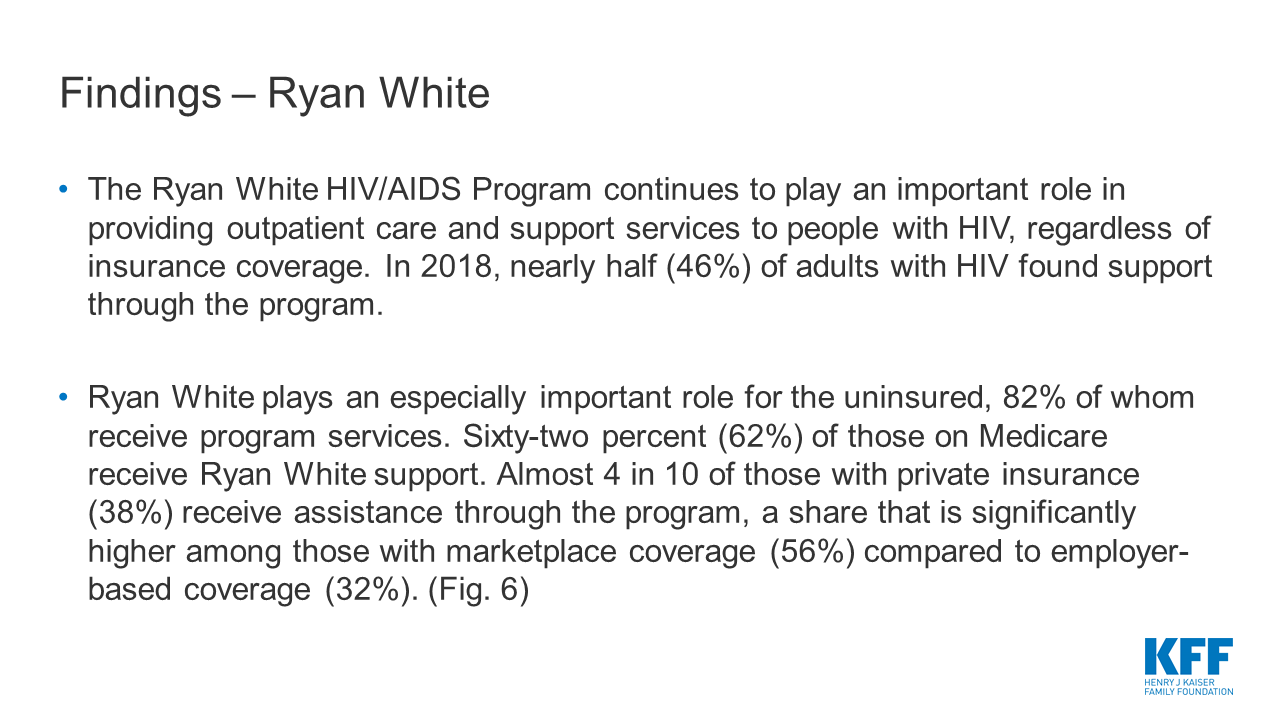
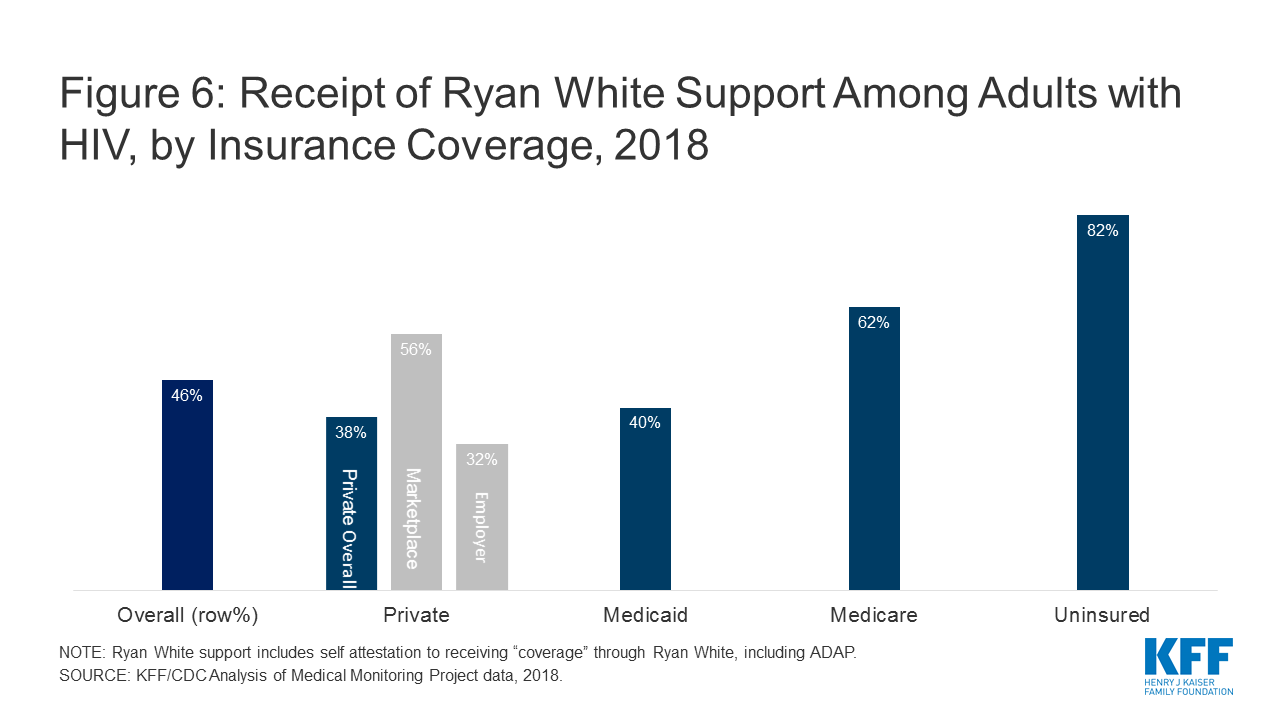
On June 29, 2020, the Supreme Court ruled that the Louisiana Act 620 is unconstitutional. Justice Breyer wrote the opinion of the court, which Justices Ginsburg, Kagan, and Sotomayor joined. Chief Justice Roberts wrote a concurring opinion, which reached the same conclusion that the Louisiana admitting privileges law places a “substantial obstacle” in the path of women seeking abortions, but he did not apply the balancing test used in Whole Woman’s Health. The Court will likely not apply the Whole Woman’s Health balancing test to future challenges to abortion restrictions, but will rather inquire whether the law poses a “substantial obstacle.” As a result, the Court may uphold some laws with little or no benefit.
Introduction
Since the Supreme Court’s 1973 landmark decision in Roe v. Wade, abortion has been squarely in the middle of political debates at the national and state levels. The Supreme Court last ruled on an abortion case, Whole Woman’s Health v. Hellerstedt, in June 2016, when President Obama was in office and there were eight justices on the Supreme Court, including Anthony Kennedy, the swing vote. On March 4, 2020, the Supreme Court will hear oral arguments in June Medical Services LLC v. Russo, a challenge to a Louisiana admitting privileges law that is nearly identical to the Texas law struck down by the Supreme Court in 2016. In Whole Woman’s Health, the Court ruled 5 to 3 in favor of the abortion providers, with Justice Kennedy siding with the majority.
Since that decision, the makeup of the Court has significantly changed. In 2018, Justice Kennedy retired. President Trump has nominated two new Justices: Justice Gorsuch to replace Justice Scalia and Justice Kavanaugh to replace Justice Kennedy. Emboldened by the new make-up of the Supreme Court, some states have passed new abortion restrictions with the goal of reaching the Court to re-consider Roe v. Wade. While the current case, June Medical Services LLC v. Russo, is unlikely to overturn Roe v Wade, the Court’s ruling could have significant implications for women’s access to abortion and could eliminate the right of abortion providers to bring legal challenges to state and federal laws and policies. This issue brief explains the legal and factual issues in dispute and the reviews the potential implications of different rulings.
What is the law in controversy?
The June Medical Services LLC v. Russo case is a challenge to a Louisiana law, Louisiana Unsafe Abortion Protection Act (“Act 620”), which requires physicians who perform abortions in the state to have “active admitting privileges” at a hospital within 30 miles of the facility where the doctor provides abortions. Doctors who perform an abortion without having admitting privileges, may be imprisoned or fined and the clinics that employ them can have their licenses revoked and may also be fined or face civil liability. According to the Louisiana Department of Health, approximately 10,000 women obtain abortions in Louisiana annually. Clinics and doctors have brought this litigation to the court, questioning the constitutionality of the Louisiana law, and the State of Louisiana has brought a counter challenge questioning the right of doctors and clinics to sue on behalf of their patients.
Louisiana’s then Governor, Bobby Jindal, signed the bill in June 2014, and it was scheduled to go into effect September 1, 2014. On August 22, 2014, June Medical Services LLC (doing business as Hope Clinic), two other clinics (Bossier Clinic and Choice), and two doctors who perform abortions at these clinics filed a legal complaint requesting a preliminary injunction to block the enforcement of the law. When the complaint was filed, there were a total of five licensed abortion clinics in Louisiana, and six doctors performing abortions in Louisiana. Since that time, one abortion provider retired, and two clinics (Bossier City Medical Suite and Causeway Medical Clinic in Metairie) closed. There are currently three licensed clinics and five doctors who perform abortions in Louisiana.
On August 31, 2014, the District Court issued a temporary restraining order until a hearing could be held to determine whether a preliminary injunction should be issued. Per this order, Plaintiffs were expected to continue seeking admitting privileges but the State was barred from penalizing doctors during this time for not having admitting privileges.
Do abortion providers have standing to challenge this law?
For the federal courts to be able to hear a case at all there must be a party with a real, concrete injury whose protection depends on an intervention by the court. Usually, a person can only challenge the constitutionality of a law if it infringes on their own rights, not broadly on the rights of others. However, “third-party standing” allows another person or organization to assert the rights of another individual when it is difficult for that person to assert their own rights, and the parties’ interests are closely aligned. In cases relating to the right to abortion, it is very hard for women themselves to serve as plaintiffs, and for 45 years the Court has permitted their doctors sue on behalf on women. The Supreme Court established third-party standing for abortion doctors on behalf of their patients in a 1976 decision, Singleton v. Wulff. That case was brought by two doctors challenging the exclusion of abortion in Missouri’s Medicaid program. Justice Blackmun wrote for the court, “Aside from the woman herself, the physician is uniquely qualified, by virtue of his confidential, professional relationship with her, to litigate the constitutionality of the State’s interference with, or discrimination against, the abortion decision. Singleton recognized that women are chilled from asserting their abortion rights out of concern for their privacy.
In this case, although Louisiana did not challenge the doctors’ and clinics’ third-party standing in any of the cases that had made their way through lower courts for the last five and half years, the State now maintains that the third-party standing is not appropriate. Louisiana contends the courts have incorrectly assumed that doctors always have third-party standing to assert their patients’ constitutional rights to abortion without reviewing the specific facts of each case.
The State argues that the doctors do not meet the standards for third-party standing which requires: (1) the party asserting the right [must have] a ‘close’ relationship with the person who possesses the right, and (2) there must be a “hindrance” to the possessor’s ability to protect his own interests. The State maintains that the doctors in this case do not have a close relationship with their patients, and there is an inherent conflict in clinics and doctors challenging a health and safety regulation intended to protect abortion patients. They maintain that women can and do assert their own alleged rights in litigation challenging abortion regulations. The State argues that there was no evidence in this case “that any particular Louisiana woman who has obtained or is considering an abortion would personally (1) prefer to obtain an abortion from a doctor without admitting privileges, (2) prefer to forgo the protections Act 620 was intended to provide, or (3) consider her decision to obtain an abortion to be burdened by Act 620.”
The Plaintiffs maintain that the State waived the right to object to the standing of the clinics and providers by not raising this issue in the lower courts. Louisiana did not dispute Plaintiffs’ third party standing and present any evidence in the courts below to support their challenge now to third-party standing. The Plaintiffs contend there is a long history of cases ruling that doctors have the right to challenge abortion regulations on behalf of their patients, and the Court should abide by this precedent.
If the Supreme Court rules in favor of the State of Louisiana and determines that the clinics and doctors do not have third-party standing, then the Court does not need to reach the question of constitutionality of the admitting privileges law. The admitting privileges requirement would be allowed to stand, and any new challenges would need to be brought by women impacted by the law. The district court found that abortion in Louisiana is accompanied by discrimination, hostility, and occasional violence. Women seeking abortions in Louisiana also must overcome numerous obstacles including financial limitations, and concerns for privacy and personal safety, that would likely make it difficult for them to assert their constitutional rights and challenge an abortion restriction.
This could have far-reaching implications for other cases where third-party standing has been recognized including physicians’ ability to challenge laws on behalf of their patients’ rights to privacy for contraception, and to obtain mental health services. Third- party standing has also been used for education rights, housing rights, and criminal justice cases.
What is the legal standard to evaluate whether an abortion regulation is unconstitutional?
Allowing courts to evaluate credible evidence to determine if an abortion regulation benefits women is essential to evaluating whether an abortion law is constitutional. While Louisiana is claiming that requiring abortion providers to have hospital admitting privileges will protect women, the Supreme Court found that a nearly identical provision in Texas was an unnecessary regulation that would not protect women’s health and that the burden that this regulation would put on women outweighed any benefit. The state of Louisiana is asking the Court to re-open this question in this case.
In Whole Woman’s Health, the Supreme Court clarified that abortion restrictions are only constitutional if they further a valid state interest and have benefits that outweigh the burdens placed on women seeking abortions. The benefits and burdens of the laws must be based on credible evidence. The Court emphasized that the previous standard established in Planned Parenthood of Southeastern Pa. v. Casey “[u]nnecessary health regulations that have the purpose or effect of presenting a substantial obstacle to a woman seeking an abortion impose an undue burden on the right.” The rule announced in Casey “requires that courts consider the burdens a law imposed on abortion access together with the benefits those laws confer.”
The Court concluded that the Texas law requiring doctors who perform abortions to have admitting privileges at nearby hospitals did not provide any benefit to women’s health and concluded each provision of the law “places a substantial obstacle in the path of women seeking a previability abortion, each constitutes an undue burden on abortion access.” Therefore, the burden the law placed on women’s access to abortion outweighed the benefit. The district court that held the Texas law was unconstitutional based the factual findings of the lack of benefits on peer- reviewed studies on abortion complications, and expert testimony.
How many women need to be burdened?
Abortion regulations have typically been challenged before they go into effect to avoid the irreparable harm that would be caused by clinics closing and women losing access to their constitutional right to abortion—the burden. The question of what constitutes a burden is also central to this case. In 1992, the Supreme Court’s ruling in Planned Parenthood of Southeastern PA v. Casey, explained that to meet the undue burden standard, a “substantial obstacle” must be present within “a large fraction of the cases in which [it] is relevant.” The Court reiterated this standard in Whole Woman’s Health: “the relevant denominator is ‘those [women] for whom [the provision] is an actual rather than an irrelevant restriction.’”
The parties do not agree on how to define the relevant group of women affected by the Act 620 or what percentage of that group is a “large fraction.” The State of Louisiana points to Justice Alito’s dissent in Whole Woman’s Health and is requesting the Supreme Court to revisit this legal standard and only invalidate a law that burdens all women of reproductive age in a state.
The parties in this case have made different calculations regarding the share of women burdened by law and have different interpretations of the standard for a substantial burden and it will be up to the Court to determine how to define the burden.
How have the lower courts ruled on the Louisiana law?
The law was initially challenged by a group of abortion clinics and physicians in the Federal Middle District Court of Louisiana, and then the ruling, in favor of the plaintiffs was appealed to the federal 5th Circuit Court of Appeals who ruled in favor of the State.
The Federal Middle District Court of Louisiana: Requiring Abortion Providers to Have Hospital Admitting Privileges Would “Cripple Women’s Ability to have an Abortion”Soon after the passage of Act 620, but before the scheduled effective date of September 1, 2014, abortion clinics and physicians filed a complaint to enjoin the law. (See Appendix 1 for the timeline of the case.) The federal district court issued a temporary restraining order on August 31, 2014, enjoining enforcement of Act 620, but requiring the Plaintiffs to continue seeking admitting privileges at the relevant hospitals. The district court held a six-day trial in June 2015.
In January 2016, the district court ruled that Act 620 is unconstitutional, finding, “The medical benefits which would flow from Act 620 are minimal and are outweighed by the burdens which would flow from this legislation.” The district court determined that only one physician and one clinic would be left in the State to continue to provide abortions if the admitting privileges requirement were to go into effect.
The Plaintiffs then appealed the decision to the 5th Circuit Court of Appeals. After the Supreme Court decided Whole Woman’s Health in June 2016, the 5th Circuit remanded the case back to the district court so that it could be re-considered in light of Whole Woman’s Health. The district court issued a final judgment April 26, 2017, permanently enjoining the Act, ruling the law does “little or nothing for women’s health” but would cripple women’s ability to have an abortion.” The court found that approximately 70% of the women in Louisiana seeking an abortion would be unable to get an abortion in the State. The court also found no relationship between ability to obtain admitting privileges and competency. For over one year, the doctors had attempted to get hospital privileges but were unable to obtain them for a variety of reasons. Louisiana does not have standards for hospitals admitting privileges, and there is no time period in which hospitals need to respond to an application. Some hospitals require doctors to have a record of inpatient services, something most abortion providers do not have (because there are such few complications resulting from abortions). The district court included a detailed evidentiary record of each doctor’s attempts to obtain hospital privileges and the challenges they faced.
Fifth Circuit Court of Appeals: “A minimal burden even on a large fraction of women does not undermine the right to abortion.” The Requirement for Admitting Privileges does not “Impose a Substantial Burden on a Large Fraction of Women.”On September 26, 2018, the 5th Circuit overruled the district court’s decision, finding the district court clearly erred with its factual findings, and did not apply the correct legal standard. Citing the legislative history of Act 620 and the intent to promote women’s health, the 5th Circuit found that that Act 620 has a minimal health benefit. In reviewing the burden, the Court found that Act 620 does not impose a substantial burden on a large fraction of women. It also found that several doctors failed to seek admitting privileges in good faith and some of the burden on women would be caused by the doctors’ actions not the Act. After setting aside the district’s court’s factual findings as clearly erroneous, the 5th Circuit ruled that the Plaintiffs did not demonstrate an undue burden on a large fraction of women; 30% of all women seeking an abortion is not a large fraction, and the women who would be affected would not be burdened substantially.
Who determines the benefit of the law: state legislatures or courts?
One of the important issues in this case is who decides whether a state law benefits or harms women. In Whole Woman’s Health, the Supreme Court stated, “the Court, when determining the constitutionality of laws regulating abortion procedures, has placed considerable weight upon evidence and argument presented in judicial proceedings.” The Court prioritized the evidence that was presented in the case and placed less emphasis on the purported purpose of the law when enacted by state legislators.
Louisiana maintains that when the legislature enacted Act 620, it held committee hearings with extensive testimony and that Act 620 improves credentialing of abortion providers, and conditioning abortion provider qualifications on hospital credentialing introduces verification of competency that would not otherwise exist. The State is requesting that the Supreme Court give deference to state legislatures to enact laws to protect the health and safety on their citizens. They conclude that the law in question is rational law to protect women seeking abortions in Louisiana.
| Constitutionality of the Louisiana Abortion Law: Facts and Legal Standards According to the Litigants |
| Litigants | Facts | Legal Standard for Review of Admitting Privileges | How Many Women Need to be Burdened? |
| Plaintiffs:June Medical Services LLCTwo doctors (Doe 1 and Doe 2) | Act 620 confers no health or safety benefit beyond the existing law. Act 620 would result in the closure of two Louisiana’s three remaining clinics leaving only one physician to provide abortion care in the whole state. 7,000 of the 10,000 women seeking abortion in Louisiana would not be able to obtain an abortion. | In Whole Woman’s Health, The Supreme Court found that conditioning outpatient abortion care on hospital admitting privileges disqualifies competent providers and burdens abortion access. The Court must weigh the benefit with the burden. When a law serves no health or safety benefit, any burden imposed by the law is by definition undue. | For those women actually restricted by Act 620, will that restriction amount to a substantial obstacle for a significant number of women. |
| Defendant:Stephen Russo, Interim Secretary, Louisiana Department of Health and Hospitals | Act 620 improves credentialing for abortion providers. Not all of the doctors made good faith efforts to obtain hospital admitting privileges. At most, the law would create a burden for 3,000 of the 10,000 women, but this burden would not be substantial | Regulations of abortion procedures that do not impose a substantial obstacle are examined under a rational basis standard. State legislatures and medical boards have primary authority to set health and safety regulations and courts must review their work with adequate deference to the core state role of protecting health and safety. Abortion regulations do not impose a substantial obstacle unless they make abortions nearly impossible to obtain for the relevant women (or all women, in a facial challenge), such that the abortion right exists in name only. | To be facially unconstitutional the Act would need to impose a substantial burden on a large fraction of women seeking an abortion. |
The Plaintiffs contend that the leader of an anti-abortion advocacy groups sent the legislative sponsor an article touting H.B.2’s “tremendous success in closing abortion clinics and restricting abortion access in Texas.” In hearings on the bill, witnesses reiterated to legislator that Act 620 would shutter facilities in Louisiana, just as H.B. 2 had done in Texas.
After a six-day trial, the district court found that the Act 620 does not advance health or safety or ensure that physicians are competent to provide abortion care. In contrast, the 5th Circuit Court of Appeals found some evidence of a minimal benefit stating that “the admitting-privileges requirement performs a real, and previously unaddressed, credentialing function that promotes the wellbeing of women seeking abortion.” The 5th Circuit cites to the legislative history of Act 620 as demonstrating an intent to promote women’s health.
Which court establishes the facts of the case?
Under most circumstances, the district court is responsible for hearing and reviewing evidence and determining the facts of the case. Only when the district court’s factual findings are clearly erroneous do the appeals courts set aside these facts and establish their own set of facts. In this case, however, the Appeals court has used their own set of facts and rejected the evidence used in the case heard by the lower federal court.
After a full trial with witnesses and evidence, the district court ruled that Act 620 would create a substantial burden for women seeking abortion services and would force two of Louisiana’s three abortion clinics to close, leaving only one physician in the state who could provide abortion services.
However, the 5th Circuit Court of Appeals rejected the district court’s findings, and ruled that only one doctor had put forth a good-faith effort to get admitting privileges. Based on its determination of the facts, the 5th Circuit found that Act 620 does not impose a substantial burden. Although the parties agree that a court of appeals should only substitute its factual findings for the district court’s factual findings when the findings are clearly erroneous, they disagree about whether that standard was met in this case.
Looking Ahead
The Supreme Court will likely release its decision in this case at the end of June 2020. With the election only months away, and party conventions in July, this case once again puts abortion right in the middle of the political debate. While the Court’s decision is unlikely to overturn Roe v. Wade, the implications could be far reaching. Here are some of the possible ways the Court could rule:
- Third-Party Standing: If the Court decides that doctors and clinics no longer have the right to challenge abortion regulations on behalf of their patients (third- party standing), abortion would remain a constitutional right, but many potentially unconstitutional abortion regulations may go unchallenged.
- Deference to Legislature on Benefit of Law: The Court could change the standard created in Whole Woman’s Health by not requiring courts to consider credible evidence but to defer to the stated reason given by the legislature for the law in its review, giving states that want to restrict abortion greater leeway.
- Standard for Substantial Burden: The Court could also alter the burden analysis by requiring a “large fraction” of all women of reproductive age to be “substantially burdened” not just the women affected by the law. This would raise the bar on the number or share of women who potentially would be harmed before a state law would be considered a “burden” to women.
No matter how the Court rules, the decision will have far reaching impact, affecting not only women in Louisiana, but potentially determining how far other states can go in limiting access to abortion services.