KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Updated Data on State Parental Consent Laws for COVID-19 Vaccination Available Here.
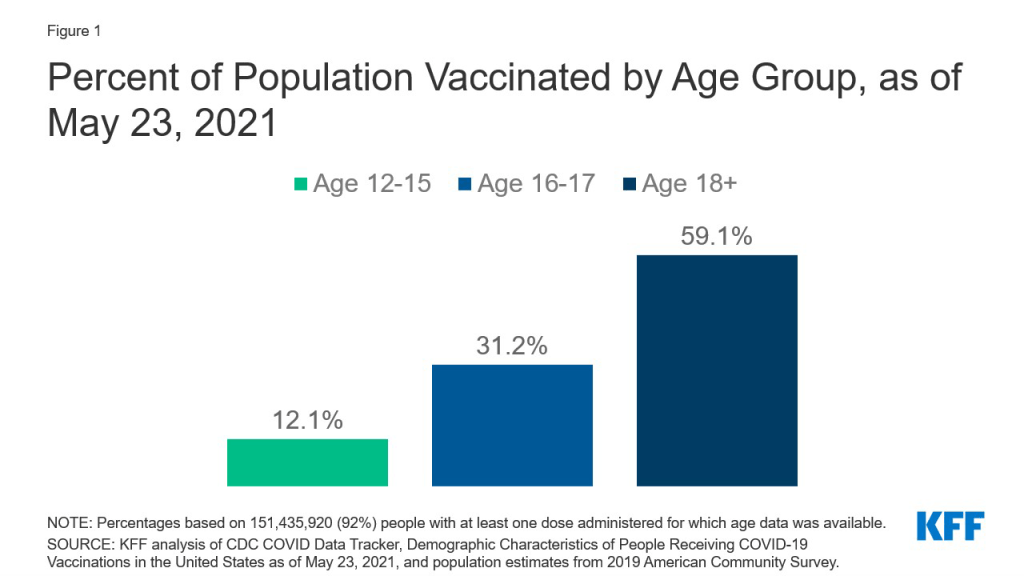
With the recent authorization of Pfizer’s COVID-19 vaccine for adolescents, ages 12-15, a group that totals almost 17 million, the next phase of the U.S. vaccination effort has begun. Authorization for even younger children is expected as early as the fall, and even before this point, Pfizer’s vaccine had been authorized for 16-17 year-olds. This has focused attention on the role of parents and parental consent for vaccination, especially since most parents are not yet ready to get their child vaccinated. In our most recent survey, fielded just before the FDA’s authorization for adolescents, 3 in 10 parents said they would do so right away, with most instead wanting to wait and see or saying they would not get their child vaccinated at all or would do so only if required for school. As of May 23, more than 2.0 million 12-15 year-olds and 2.5 million 16-17 year-olds had received at least one vaccine dose, approximately 12% and 31% of adolescents in each age group, respectively (Figure 1). To better understand the landscape of parental consent laws, we assessed which states have such laws, for what ages, and where exceptions for COVID-19 vaccination have been made.
Figure 1: Percent of Population Vaccinated by Age Group, as of May 23, 2021
Overall, we find that most states require parental consent at this point, though the landscape may be shifting slightly as more jurisdictions seek to encourage vaccination of young people. Specific findings are as follows:
Most states (41) require parental consent for vaccination of minors below the age of 18, although one of these states (NE) requires consent below age 19. There are some exceptions to these requirements:
Many allow for certain minors, such as those who are emancipated, homeless or living apart from their parent or guardian, or married, to self-consent.
Cities in two states (San Francisco in CA and Philadelphia in PA), have moved to allow minors, ages 12 and older, to self-consent for COVID-19 vaccination.
In one state (AZ), if a parent refuses to consent for COVID-19 vaccination, but if a child or a doctor requests it, a court order can be obtained to allow for vaccination.
In 5 states, a minor’s ability to self-consent is based on a specific age as follows:
Two states where a minor must be at least 16 (RI and SC)
One state where a minor must be at least 15 (OR)
One state where a minor must be at least 14 (AL)
One state where a minor must be at least 11 (DC; in DC, each healthcare provider may institute additional requirements which could include requiring a parent or guardian to be present).
The remaining 5 states apply the “mature minor doctrine”, meaning that there is no specific age cut-off but providers have discretion to decide if a minor possesses the maturity to consent for themselves (AR, ID, NC, TN, WA).
This means that parental consent has already been required for 16-17 year-olds in most states (41) since the initial authorization of the Pfizer vaccine on December 11, 2020. Two additional states require consent for some subset of 12-15 year-olds, bringing the count to 43 states where most minors in this age group would need parental consent. Once the next group of children is eligible for vaccination, those below age 12, this number will grow to 45.
As we find here, parents, and parental consent laws, will play a critical role in the COVID-19 vaccination effort to reach children in the U.S., particularly as authorization moves to even younger ages. Most states have already required parental consent for 16-17 year-olds, who have been eligible for vaccination since the nation’s vaccine effort began. There are only a handful of states where minors under the age of 16 can self-consent. As such, reaching parents with information about COVID-19 vaccination for children will be the driving factor for increasing vaccine coverage for young people. At the same time, the legal landscape may be shifting slightly. Similar to laws in a handful of states allowing minors to self-consent for certain other services (e.g., HIV and STI testing and treatment), some cities and states are moving to allow self-consent for minors for the COVID-19 vaccination specifically, in an effort to increase vaccinations among young people.
Mental Health and Substance Use Considerations Among Children During the COVID-19 Pandemic
During the COVID-19 pandemic, children have experienced major disruptions as a result of public health safety measures, including school closures, social isolation, financial hardships, and gaps in health care access. Many parents have reported poor mental health outcomes in their children throughout the pandemic – in May 2020, shortly after the pandemic began, 29% said their child’s mental or emotional health was already harmed; more recent research from October 2020 showed that 31% of parents said their child’s mental or emotional health was worse than before the pandemic. Some children have also exhibited increased irritability, clinginess, and fear, and have had issues with sleeping and poor appetite. As mental health issues become more pronounced among children, access to care issues may also be increasing. These access issues may exacerbate existing mental health issues among children.
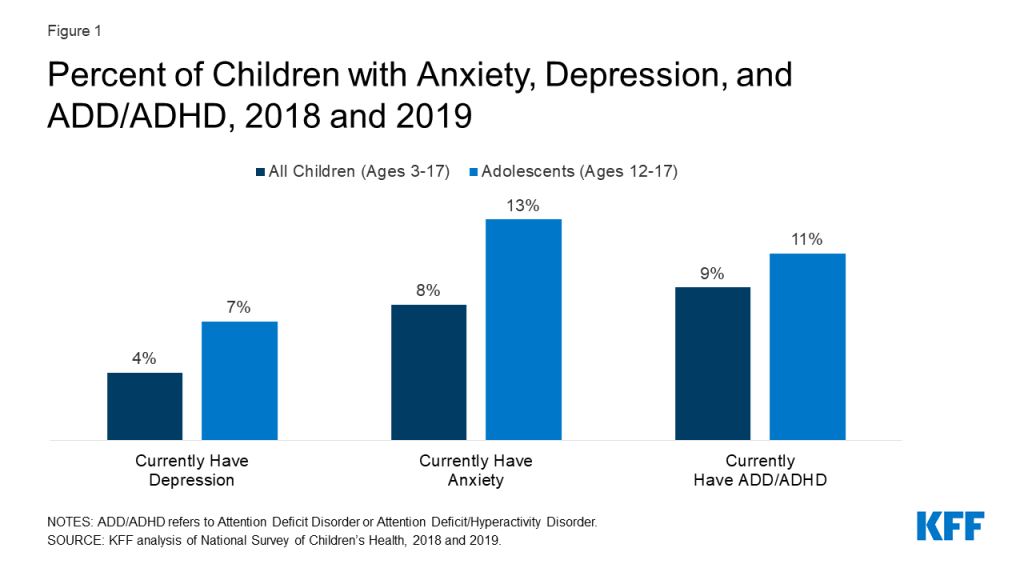
Even before the pandemic, many children in the United States were living with mental health disorders. On average, in the years 2018 and 2019, among children ages 3-17, 8% (5.2 million) had anxiety disorder, 4% (2.3 million) had depressive disorder, and 9% (5.3 million) had attention deficit disorder or attention deficit/hyperactivity disorder (ADD/ADHD) (Figure 1). Other mental health disorders among children and adolescents include obsessive-compulsive disorder (OCD), post-traumatic stress disorder (PTSD), and eating disorders. Adolescents in particular have seen increases in poor mental health outcomes in recent years, such as persistent feelings of sadness or hopelessness and suicidal thoughts. Many mental health conditions develop by adolescence and, if unaddressed, can persist into adulthood and limit quality of life.
Figure 1: Percent of Children with Anxiety, Depression, and ADD/ADHD, 2018 and 2019
This brief explores factors contributing to poor mental health and substance use outcomes among children during the pandemic, highlighting groups of children who are particularly at risk and barriers to accessing child and adolescent mental health care. Although data on child and adolescent mental health have historically been limited, where possible, we draw upon data from the National Survey of Children’s Health, the Youth Risk Behavior Surveillance System, and the National Survey on Drug Use and Health, in addition to surveys conducted during the pandemic. Key takeaways include:
Several pandemic-related factors may negatively impact children’s mental health. Social distancing and stay-at-home orders could lead to loneliness and isolation among children – known risk factors for poor mental health. Income insecurity and poor mental health experienced by parents during the pandemic may also adversely affect children’s mental health and may be associated with a possible rise in child abuse.
Adolescents, young children, LGBTQ youth, and children of color may be particularly vulnerable to negative mental health consequences of the pandemic. During the pandemic, more than 25% of high school students reported worsened emotional and cognitive health; and more than 20% of parents with children ages 5-12 reported their children experienced worsened mental or emotional health. A survey of LGBTQ youth found that many LGBTQ adolescent respondents (ages 13-17) reported symptoms of anxiety (73%) and depression (67%) and serious thoughts of suicide (48%) during the pandemic. Although data is limited on children of color, research suggests that even before the pandemic they had higher rates of mental illness, but were less likely to access care.
Prior to the pandemic, many children with mental health needs were not receiving care; and it is possible that access to mental health services has since worsened. Data shows that there have been large declines in pediatric mental health care utilization since the pandemic began. Access to mental health care via telehealth has increased, however, access via schools – a commonly utilized site of care for children and adolescents – may have decreased due to school closures.
Several bills that include funding related to children’s mental health have been introduced during the pandemic. The recently passed American Rescue Plan Act allocates funding for pediatric mental health care access and youth suicide prevention. The American Jobs Plan and American Families Plan propose additional funding for services to benefit children, including upgraded schools and nutrition programs.
Factors Contributing to Poor Mental Health Among Children During the Pandemic
Children’s mental health during the pandemic may be negatively affected by social distancing and stay-at-home orders, which could lead to loneliness and isolation – known risk factors for poor mental health outcomes. Nearly a quarter of high school students report feeling disconnected from their classmates during the pandemic. Research has broadly shown that loneliness is associated with anxiety and depression among children. Additionally, the duration of a child’s experience of loneliness is linked to mental health problems later in life. Pandemic-related isolation and quarantines may also lead to some children experiencing separation anxiety from their parents or caregivers and fear of themselves or family members becoming infected.
Many parents are experiencing stress and poor mental health during the pandemic. This may be due to a number of factors, including parents balancing both work and childcare, and parents facing income insecurity (49% of households with children reported a loss of employment income and 61% reported difficulty paying for usual household expenses in late March 2021). The poor mental health of parents may adversely affect children’s mental health. Additionally, children in low-income households are at greater risk for mental health issues and are less likely to have access to needed mental health care, compared to children in high-income households.
Mediareports suggest child abuse may have increased in light of the pandemic, although it is unclear based on available data. The pandemic’s negative impact on parents’ mental health and stress may be associated with the possible rise in child abuse. Child abuse can lead to immediate emotional and psychological problems and is also an adverse childhood experience (ACE) linked to possible mental illness and substance misuse later in life. Reports of child abuse have dropped since school closures began, and child abuse-related emergency department (ED) visits have decreased throughout the pandemic. However, the severity of injuries among these ED visits has increased and resulted in more hospitalizations; and it is possible that due to school closures and stay-at-home orders during the pandemic, many cases are going undetected, since educators play a primary role in identifying and reporting child abuse. Research has also found that cases of child abuse increased during the previous recession.
Special Mental Health Considerations for Adolescents and Children
Research during and leading up to the pandemic suggests that adolescents, young children, LGBTQ youth, and children of color may be particularly vulnerable to negative mental health consequences of the pandemic, including anxiety and depression.
Adolescents
Throughout the pandemic, data has shown that adolescents have experienced poor mental health outcomes. Shortly after the pandemic began, more than 25% of high school students reported worsened emotional and cognitive health. A more recent survey of high school students found that only one-third felt they were able to cope with their sources of stress, which include strained mental health and peer relationships. Private insurance data also shows that while all health care claims for adolescents ages 13-18 were down in 2020 compared to 2019, mental health-related claims for this age group increased sharply.1 The most frequently diagnosed mental health conditions in 2020 were depression, anxiety, and adjustment disorder. Even before the pandemic, 7% (1.8 million) of high school students had depression and 13% (3.1 million) had anxiety (Figure 1).
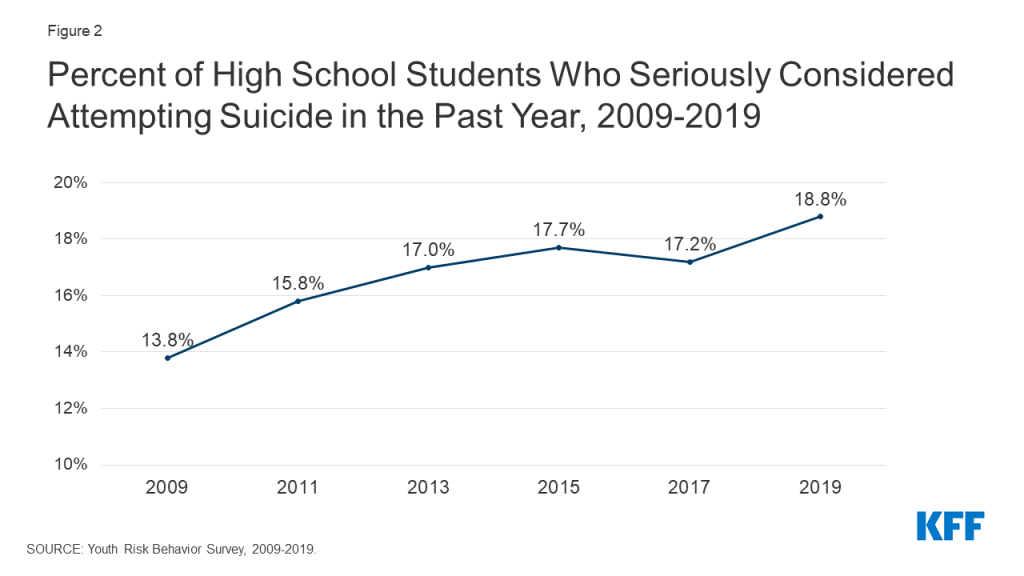
It is unclear whether suicidal ideation and suicides have increased among adolescents; however, mediareports and a study of a pediatric emergency department suggests they may have in light of the pandemic. Prior to the pandemic, serious thoughts of suicide were already on the rise among high school students (from 14% in 2009 to 19% in 2019, Figure 2). Suicide was also the second leading cause of death among adolescents (ages 12-17) in 2019, resulting in 1,580 deaths.2
Figure 2: Percent of High School Students Who Seriously Considered Attempting Suicide in the Past Year, 2009-2019
Some evidence also shows that substance use disorders and overdoses among adolescents are increasing during the pandemic. Solitary substance use, as opposed to social substance use, has increased among adolescents during the pandemic. An analysis of private insurance data found that, in general, claims for substance use disorders and overdoses increased as a share of all medical claims for adolescents ages 13 to 18 in 2020, compared to 2019.1 Prior to the pandemic, 1.1 million adolescents reported having a substance use disorder in the past year. When substance use begins at younger ages, it is more likely to persist into adulthood and increase the risk of addiction.
Young children
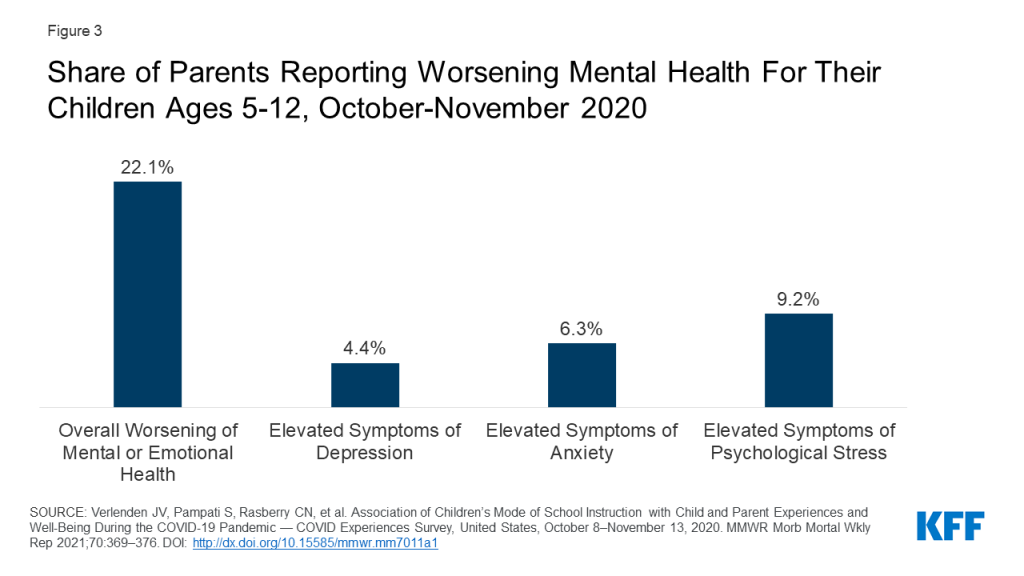
During the pandemic, parents have reported that young children experienced worsened mental health outcomes. Young children may be experiencing worsened mental health due to pandemic-related disruptions in their routine and caregiving or stressful home environments. Forty-seven percent of parents with children who are not yet school-age reported they are more worried about their children’s social development than they were before the pandemic. During the pandemic, parents with children ages 5-12 reported their children showed elevated symptoms of depression (4%), anxiety (6%), and psychological stress (9%); and experienced overall worsened mental or emotional health (22%) (Figure 3). Parents of children attending school virtually were more likely to report their children experienced overall worsened mental or emotional health than parents of children attending school in-person (25% vs. 16%, respectively).
Figure 3: Share of Parents Reporting Worsening Mental Health For Their Children Ages 5-12, October-November 2020
An analysis of private insurance data found that claims for OCD and tic disorders increased as a share of all medical claims for children ages 6 to 12 in 2020, compared to 2019.1 ADHD was the top mental health diagnosis for children ages 6 to 12 during 2020; however, claims for ADHD decreased as a share of all medical claims, compared to 2019. This decrease may be due to teachers being unable to observe possible signs of ADHD as they typically would during in-person instruction.
LGBTQ YOUTH
Research suggests that lesbian, gay, bisexual, transgender, and queer or questioning (LGBTQ) youth may be particularly vulnerable to negative mental health outcomes during the pandemic. A non-probability survey of LGBTQ youth conducted in Fall 2020 found that large shares of adolescent respondents (ages 13-17) reported symptoms of anxiety (73%) or depressive (67%) disorder in the past two weeks; and 48% seriously considered attempting suicide in the past year. Prior to the pandemic, LGBTQ youth were already at increased risk for depression, suicidal ideation, and substance use. In 2019, 66% of lesbian, gay, and bisexual high schools students reported persistent feelings of sadness and hopelessness (compared to 37% of all high school students) and 47% reported serious thoughts of suicide (compared to 19% of all high school students) (Figure 4). Larger than average shares of lesbian, gay, and bisexual youth also reported substance use before the pandemic.
Figure 4: Among High School Students Who Identify as Lesbian, Gay, or Bisexual, Share Reporting Mental Distress or Substance Use, 2019
Children of color
Poor mental health outcomes resulting from the pandemic may disproportionately affect children of color. Prior to the pandemic, children of color had higher rates of mental illness, but were less likely to receive care. They were also less likely than White children to have access to school health services, including mental health care. During the pandemic, these access issues may be further exacerbated as school services may have been suspended or limited. Asian children may also be uniquely at risk of adverse mental health outcomes due to anti-Asian racism that has emerged during the pandemic; prior to the pandemic, they were more likely to face barriers to accessing mental health services than White children. Structural racism has been associated with poor mental health outcomes. During the pandemic, Black and Latino adults have also experienced higher rates of illness and death from COVID-19, negative financial impacts, and poor mental health outcomes, which may have adverse mental health effects on children from these communities.
Suicide may also disproportionately affect children of color. Before the pandemic, Native American adolescent girls were three times more likely to die of suicide than White adolescent girls, and suicide rates have been increasing faster among Black children and teens than among non-Black children and teens.
Access to Children’s Mental Health Care During the Pandemic
Prior to the pandemic, many children with mental health needs were not receiving care for reasons including costs, lack of providers, and limited insurance coverage. In 2019, 11% of children ages 3-17 received mental health care in the past year. However, only one in five children with mental, emotional, or behavioral disorders were receiving mental health care from a specialized provider. It is possible that access to mental health care – like access to all health services – worsened during the pandemic. In an effort to slow the spread of the coronavirus, many health care providers changed the way they deliver services, sometimes suspending them or operating at limited capacity. Telehealth use has increased for many types of health services, but not necessarily by enough to offset the drop in in-person care.
A small share of parents also reported delaying mental health care (4%) or treatment for alcohol or drug use (2%) for their children in September 2020 in order to reduce exposure to COVID-19 or in light of limited provider services. However, other data suggests there have been large declines in pediatric mental health care utilization. Among Medicaid and Children’s Health Insurance Program (CHIP) beneficiaries under the age of 18, the number of children receiving mental health services dropped by 50% from February to October 2020 (Figure 5). While utilization rates of other services – including child screening and dental services – among Medicaid and CHIP beneficiaries under the age of 18 eventually began to rebound during this time period, mental health service utilization rates lagged in comparison. Nearly two out of five children under the age of 18 in the U.S. are Medicaid or CHIP beneficiaries. Private mental health care claims also decreased from 2019 to 2020.1 Despite a drop in the total number of mental health claims among privately insured patients, mental health care represented a larger share of total medical claims among these patients in 2020 than in 2019.
Figure 5: Mental Health Service Utilization Rates Per 1,000 Medicaid/CHIP Child Beneficiaries, February vs. October 2020
Throughout the pandemic, manyinsurers and mental health care providers have expanded telehealth services during the pandemic. Claims data from CMS show a significant increase in the utilization of outpatient mental health services via telehealth for Medicaid/CHIP child beneficiaries beginning in March 2020, with a peak in April. By July 2020 (the latest telehealth data for mental health services available at the time of this publication), the use of telehealth for mental health services decreased, but remained above pre-pandemic utilization levels. Analysis of pediatric private claims data has shown a similar trend.1 Additionally, a number of barriers may limit some children’s access to mental health care via telehealth during the pandemic, including lack of access to digital devices, internet, and privacy in speaking with a provider.
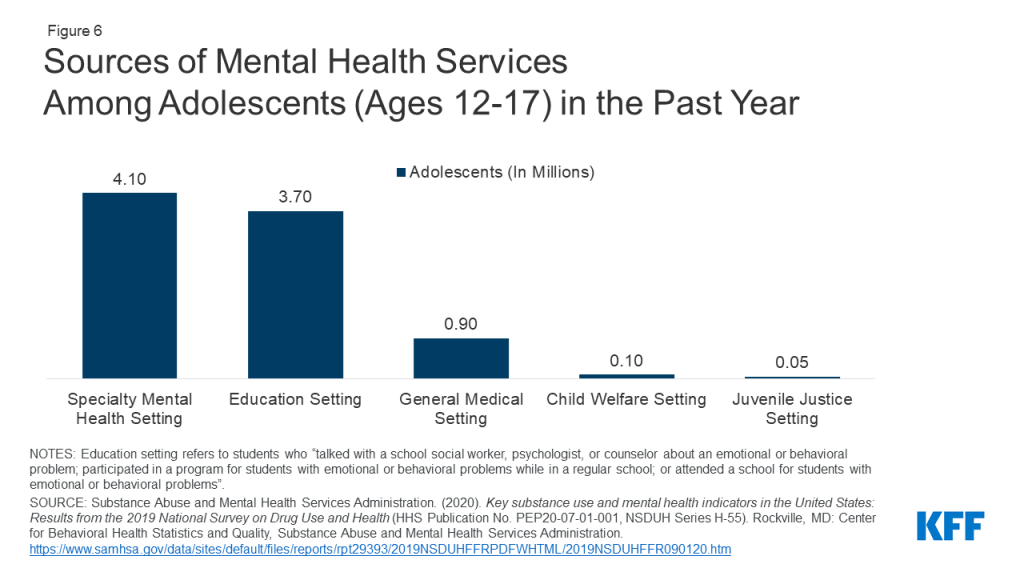
With pandemic-related school closures, children and adolescents may have faced limited or suspended health services they commonly access through school-based health centers (SBHCs), including mental health services. In focus groups conducted during the pandemic, many SBHC staff reported challenges delivering health care and heightened concerns around mental distress among students, including symptoms of anxiety and depression and suicidal ideation. Prior to the pandemic, many adolescents sought mental health care through schools (3.7 million adolescent visits in 2019, Figure 6).
Figure 6: Sources of Mental Health Services Among Adolescents (Ages 12-17) in the Past Year
Anecdotal evidence from numerousmediareports suggests that the availability of psychiatric beds in hospitals and mental health facilities has decreased during the pandemic, exacerbating an existing shortage of child and adolescent psychiatric beds, which are needed for individuals seeking emergency care during a mental health crisis. Surges of patients with severe COVID-19 have, at times, left hospitals at or above admissions capacity, and some have repurposed psychiatric beds for COVID-19 patients or have limited admissions in order to mitigate the spread of the coronavirus. Some financially hard-hit hospitals have closed inpatient psychiatric units entirely. It is possible that children in need of hospitalization for mental health disorders during the pandemic have challenges finding hospitals with enough capacity.
Policy Responses
Stimulus bills passed during the course of the pandemic have included direct financial support for families with children, as well as other provisions that may alleviate some of the mental health burdens children and adolescents face. The American Rescue Plan Act (ARPA), which was signed into law on March 12, 2021, builds on prior pandemic aid by providing financial support to many families with children. It also allocates funding for mental health and substance use disorder services, with a portion designated specifically for children’s mental health, including $80 million for pediatric mental health care access, $20 million for youth suicide prevention, and $10 million for the National Child Traumatic Stress Initiative. The ARPA also designates funding for school, child care, and nutrition programs that serve many children and adolescents; provides relief fund payments for rural Medicaid and CHIP providers; and newly offers federal support to states for community-based mobile crisis intervention services. The recently proposed American Jobs Plan and American Families Plan outline additional funding for services to benefit children, including free preschool, new and upgraded public schools and childcare facilities, and nutrition programs.
Bipartisan bills aimed at addressing mental health and substance use consequences from the pandemic were recently introduced. Several of these bills at both the national and state level specifically focus on children. The COVID-19 Mental Health Research Act proposes research on pandemic-related mental health impacts, including impacts on children and adolescents. In Colorado, the Rapid Mental Health Response For Colorado Youth bill would establish a temporary program allowing youth to access mental health and substance use disorder services for free or reduced costs.
Looking ahead, poor mental health outcomes and access to care issues among children and adolescents are likely to persist beyond the pandemic. The pandemic may also increase the risk of children having adverse childhood experiences, such as experiencing violence or being exposed to adult substance misuse, which can lead to long-term mental health and substance use issues. This brief highlights the need for policymakers, providers, educators, parents, and researchers to consider the ways the COVID-19 pandemic may impact children’s mental health for the long-term.
This work was supported in part by Well Being Trust. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
KFF analysis of Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) (2018). Accessed at: https://webappa.cdc.gov/sasweb/ncipc/leadcause.html↩︎
The pandemic has taken a heavy toll on the nation’s mental health, and a new issue brief shows that children are also facing worsening emotional and cognitive health. The brief examines factors contributing to worsening mental health and substance use outcomes among children and adolescents during the pandemic, looking closely at those who are at higher risk for negative mental health impacts, such as LGBTQ youth and children of color. A review of recent research finds:
More than 25% of high school students reported worsening emotional and cognitive health and over 20% of parents with children ages 5-12 reported similar worsening conditions for their children.
There has been a large decline in pediatric mental health care usage since the start of the pandemic. While access to mental health services via telehealth has increased, mental health services via schools likely decreased with closures. Among Medicaid and Children’s Health Insurance Program (CHIP) beneficiaries under the age of 18, the number of children receiving mental health services dropped by 50% from February to October 2020.
In addition to loneliness and isolation in light of public health safety measures, the poor mental health of parents could be a contributing factor in negative mental health outcomes for children.
The brief also notes several provisions of the recently passed American Rescue Plan Act that support pediatric mental health care services and other programs, as well as relevant provisions in other proposed legislation.
KFF also has state-specific data on mental health and substance use on more than 20 indicators, with mental health state fact sheets available profiling each state.
On May 17, 2021 President Biden announced that by the end of June, the U.S. would donate 80 million doses of COVID-19 vaccine for use internationally. Sixty million of these doses are expected to be U.S.-owned doses of the Oxford/AstraZeneca vaccine (enough to vaccinate 30 million people), which has yet to be authorized in the U.S. but is authorized in multiple countries. An additional 20 million U.S.-owned doses will be from a mix of Pfizer, Moderna, and Johnson and Johnson vaccines (while the exact combination of doses for each was not announced, this could amount to enough vaccines for an additional 10-20 million people).
Prior to this point, the U.S. had provided 4 million doses of AstraZeneca to Canada and Mexico (via a “loan”), so 80 million doses would represent a significant increase in U.S. vaccine donations and make the U.S. the largest single country donor of in-kind vaccine doses worldwide (see Figure). In addition, the U.S. has also appropriated $4 billion to COVAX, the international partnership for COVID-19 vaccine procurement and distribution overseen by the Gavi Alliance, CEPI, and the World Health Organization, making the U.S. the largest donor to this effort as well.* In addition, vaccine production and manufacturing continue to lag and a key supplier of global vaccines has announced it will not be exporting any additional doses until the end of this year, underscoring the importance of countries donating doses in the near term.
While some have praised the most recent U.S. donation announcement as an important development, others have said the U.S. could do much more, pointing to the large supply of doses the U.S. is building up and the slowing demand for vaccinations in the country. We sought to put the U.S. pledge of 80 million doses in further context, looking at what it represents relative to the current landscape:
Almost 3 times the number of doses pledged by the next largest country donor, France;**
56% of donated doses from all other governments combined;
115% of the total number of doses already delivered by COVAX through May 20;
Less than 2% of the number of doses needed to vaccinate all people in low- and middle-income countries (LMICs);
8-16% of the number of doses sufficient to vaccinate the highest risk groups in LMICs – health care workers and adults over 65;
29% of the total cumulative vaccine doses administered in the U.S. (as of May 18).
Figure: US pledge of 80 million doses vs. pledges from other donor governments
The world is still very unequal in terms of access to vaccines across regions and income groups, with estimates that some lower-income countries may not be able to vaccinate a majority of their adult populations for a year or more, even as many high-income countries approach or have already exceeded this milestone. Therefore, donated doses can help speed global vaccinations, provided the doses are distributed efficiently and administered effectively in the countries that need them. The U.S. has so far pledged to donate more doses than any other country and has provided the largest contribution to COVAX to date. Still, the U.S. effort represents only a fraction of what would be needed to vaccinate everyone, raising challenging questions about how access to COVID-19 vaccines will be scaled up and on what timeline, and what the role should of high income countries like the U.S. will be going forward.
Notes and Sources
*Information on the price of vaccine doses paid by COVAX to manufacturers is not available, so it is not known how many COVAX doses the U.S. contribution would support.
**Donors have pledged to provide COVID-19 doses over different time frames. For example, France has pledged to provide 30 million doses by the end of 2021, while the U.S. has pledged to provide 80 million doses by the end of June.
Data on COVID-19 vaccine dose donations were obtained from the UNICEF COVID-19 Vaccine Market Dashboard and other public news sources. Data include donations provided bilaterally as well as through COVAX. Data include donations with a confirmed delivery status and pledges.
COVAX delivery data were obtained from the UNICEF COVID-19 Vaccine Market Dashboard.
Population data for adults over 65 years in low- and middle-income countries, as defined by the World Bank, were obtained from the United Nations World Population Prospects using 2020 estimates. Health workforce data for low- and middle-income countries were obtained from World Health Organization National Health Workforce Accounts Data Portal, limiting data to the estimated number of physicians, nurses, and midwives under 65 years for the most recent year of data available.
U.S. vaccine administration data obtained from the Centers for Disease Control and Prevention’s COVID Data Tracker.
Much has been written about the multiple roles that women, particularly mothers have played in all stages of the pandemic – including as frontline workers, paid and informal caregivers, and ad hoc homeschool teachers just to name a few. Mothers will also play a pivotal role in the national efforts to get as many eligible children as possible vaccinated against COVID-19. Use of the COVID-19 vaccine from Pfizer has now been authorized for adolescents ages 12 – 15, and younger children may become eligible for vaccination later this year. While on average children have had less severe impact of COVID-19, cases of death, severe illness, and long-term consequences of COVID-19 have been documented among children. Even when they do not fall ill from COVID-19, asymptomatic children can be a source of spread of the disease.
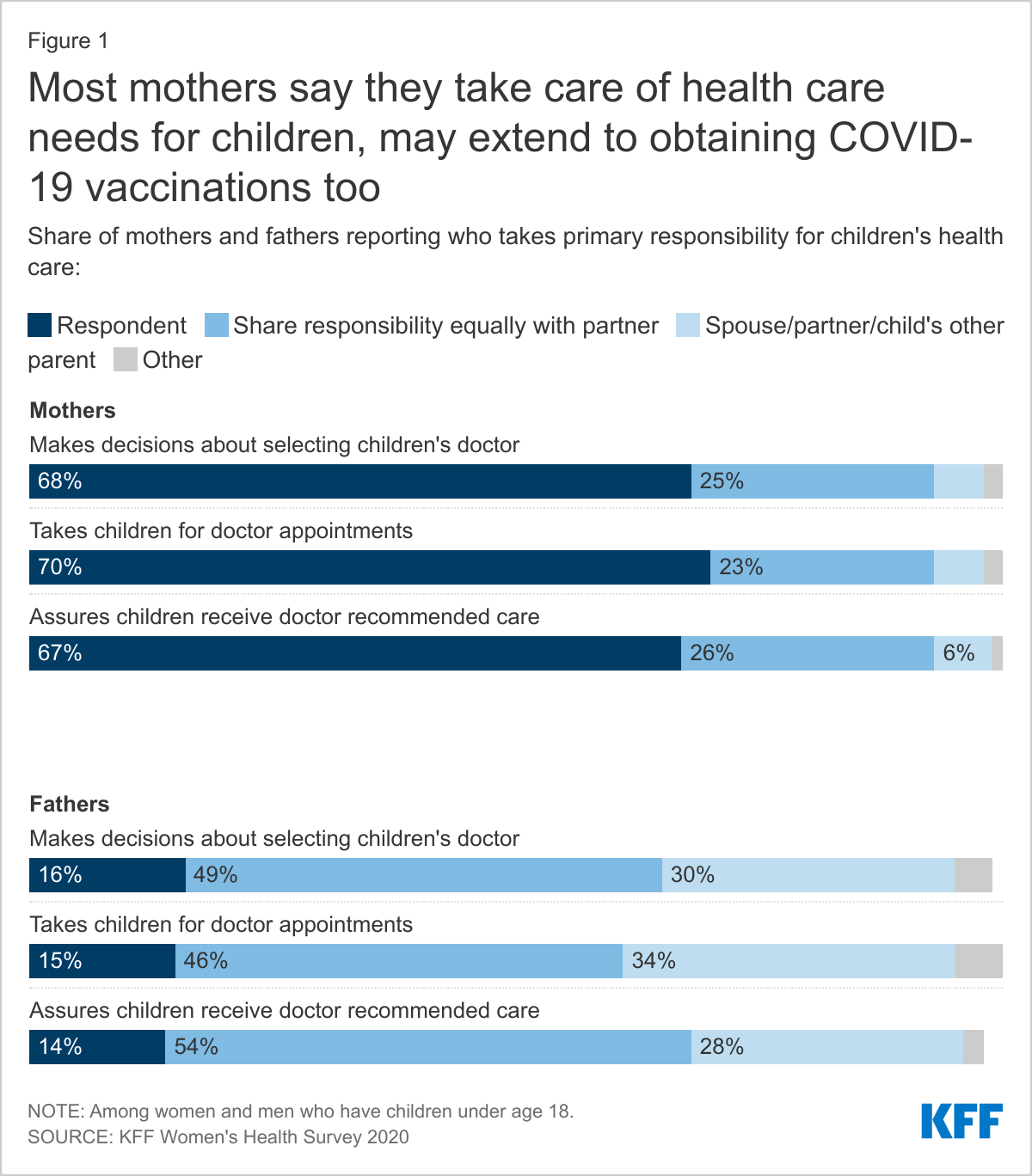
Who will ensure that kids receive vaccinations?
Parents will be the ones who determine whether children get their vaccines (Figure 1). In the 2020 Kaiser Women’s Health Survey, roughly seven in ten mothers of children under 18 say they are usually the ones who select their children’s doctor (68%), take children to medical appointments (70%) and follow up on recommended care (67%). Mothers and fathers differ somewhat on their assessment of involvement in children’s health care, but even among fathers, less than a fifth report they take care of these tasks and a substantial share say their partner takes care of them (Figure 1). However, about half of fathers say they share these responsibilities equally with a partner or other parent, compared to about a quarter of mothers.
While the majority of mothers in all groups say they are the ones who usually take care of kids’ health care needs, it is higher among Black and low-income mothers compared to those who are White and low-income, as we have previously reported. These differences are particularly important, given the disproportionate toll of the pandemic on communities of color and those who are low-income. More than one-third (36%) of children ages 12-15 are in low-income families. Not surprisingly, single mothers shoulder a higher share of children’s health care needs compared to those who are married/living with a partner.
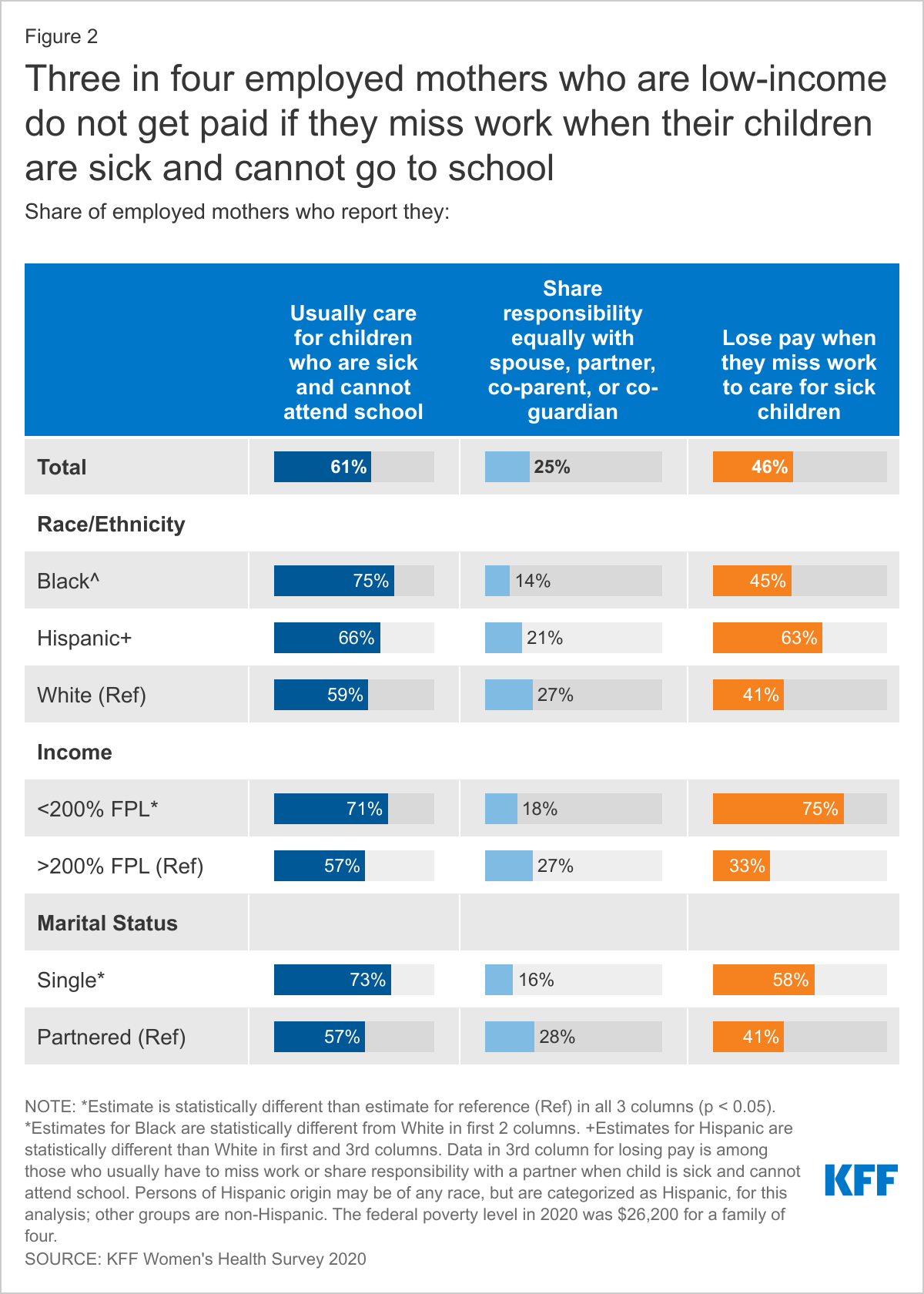
Another concern will be how mothers will find the time to take their children to get vaccinated and to deal with the potential side effects from the vaccine their children may experience and the impact on their pay. The Pfizer vaccine requires two shots and children may experience side effects that prevent them from attending school or other care. For employed parents, this may require taking time off from work and this responsibility has typically fallen on the shoulders of the mother. Six in ten (61%) employed mothers report that they are usually the ones who care for children when they are sick and cannot go to school, and nearly half (46%) of this group report that they are not paid for that time off. This gap is larger among some groups, particularly mothers who are Hispanic, low-income, or single, who also are more likely to have to care for children when they are sick and cannot attend school (Figure 2). In fact, less than half of employed low-income mothers (46%) report being offered paid sick leave compared to nearly three in four with higher incomes (72%).
What do we know about parents’ interest in vaccines?
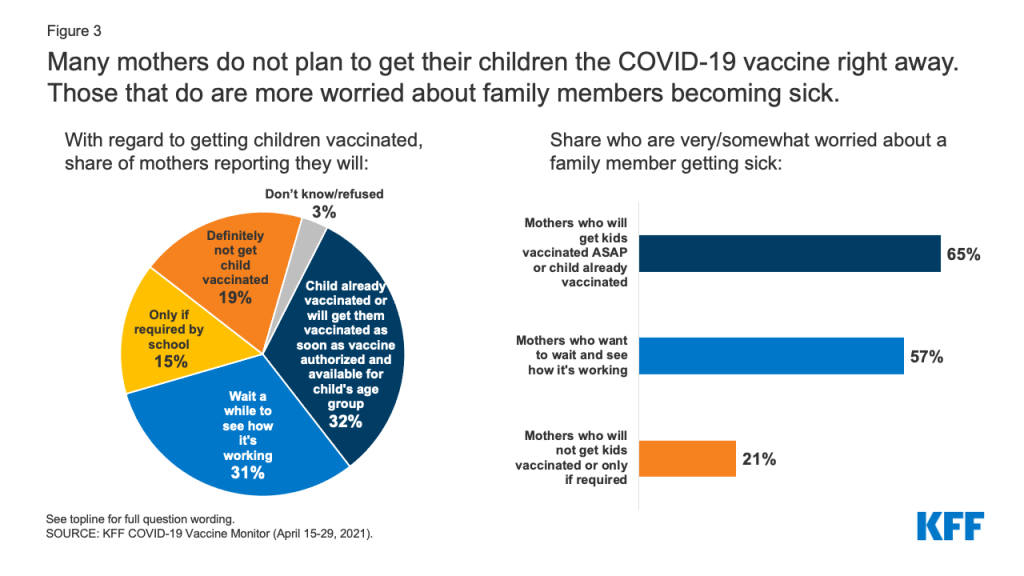
While mothers have traditionally played a leading role in managing their children’ health care, it is unclear how families are making decisions about whether their children should be vaccinated against COVID-19. Data from the latest KFF COVID-19 Vaccine Monitor find that as of mid-April (before the FDA authorized the vaccines for use in children ages 12-15), about a third of mothers (32%) of children under 18 said they would get their children vaccinated as soon as a vaccine was authorized for their child’s age group or have already gotten their child vaccinated (Figure 3). Nearly a third (31%) wanted to wait and see how the vaccine is working, 15% said they would only get it if required for school, and about a fifth (19%) said they would not get their children vaccinated. Rates among fathers are similar.
While the majority of mothers said they were not planning to get their children vaccinated right away, nearly half (48%) of mothers and 40% of fathers say they are worried (very or somewhat) about someone in their family getting sick from COVID-19. The share who are worried about someone in their family getting sick from COVID-19 rises to 65% among mothers whose kids are already vaccinated or want to get their kids vaccinated right away, 57% among mothers who want to wait and see before deciding on children’s vaccinations, but only 21% among mothers who do not want to get their children vaccinated or will only do so if required.
Figure 3: Many mothers do not plan to get their children the COVID-19 vaccine right away. Those that do are more worried about family members becoming sick.
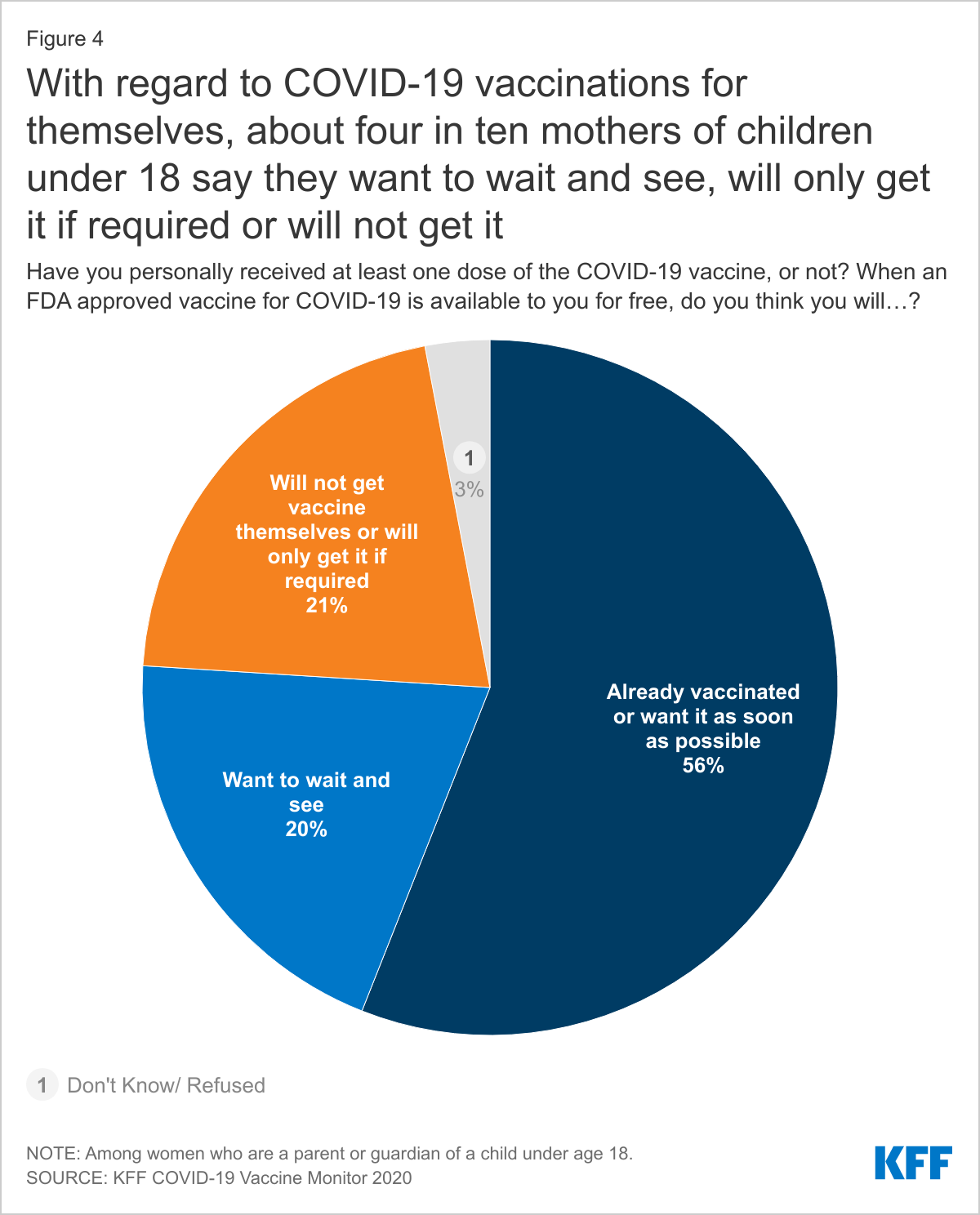
When it comes to adult vaccinations, more than half (56%) of mothers with children under 18 said they themselves have already been vaccinated or want to get vaccinated as soon as possible. A fifth of mothers said they want to wait and see about getting vaccinated themselves (20%) and about a fifth (21%) said they will not get vaccinated or will do it only if it is required (Figure 4). These percentages are similar among fathers.
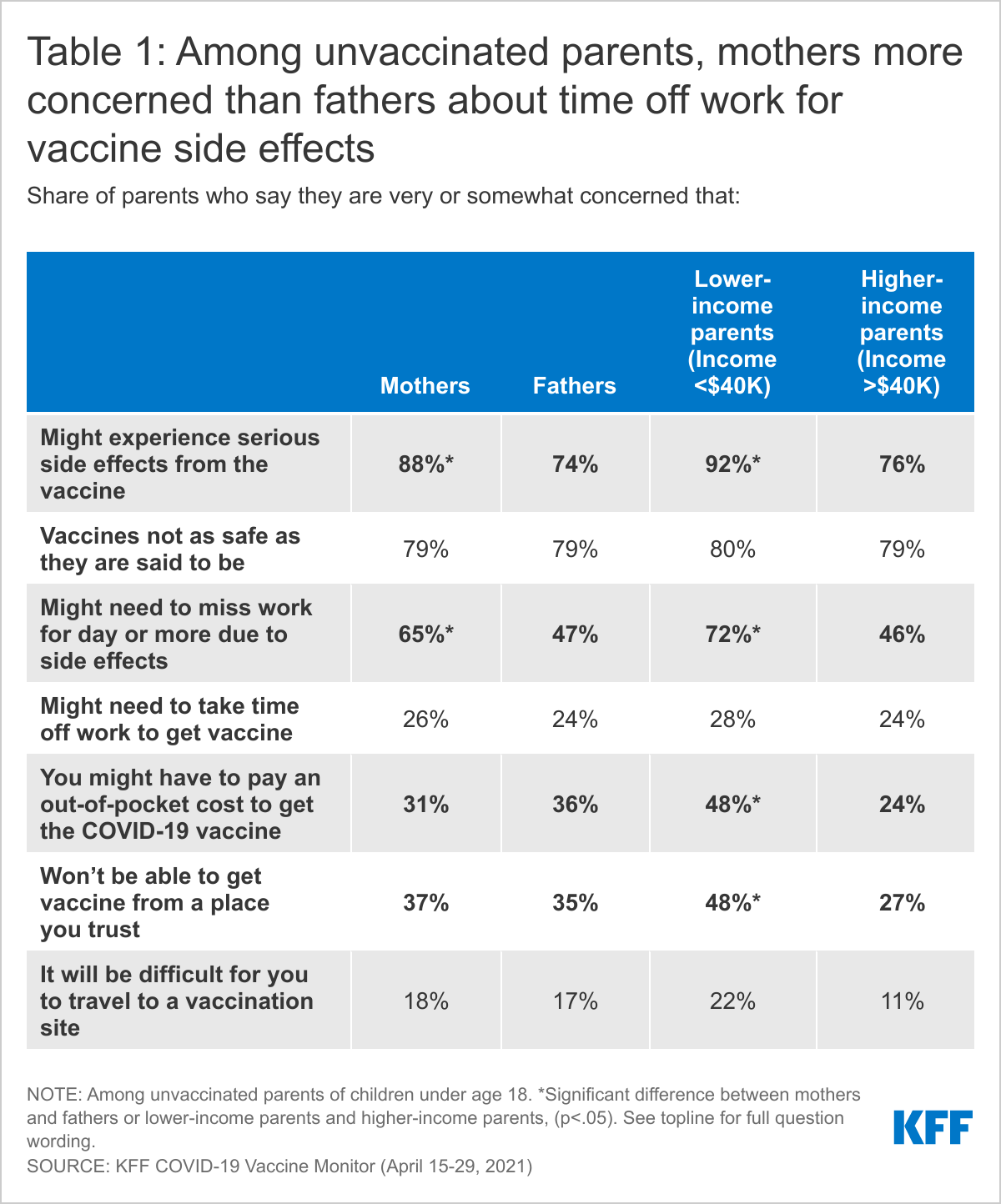
While we do not know the rationale for the lack of urgency some parents have so far regarding getting their children vaccinated, it can be informative to look at the reasons that parents state for not getting vaccinated yet themselves (Table 1). Among unvaccinated parents, the vast majority of mothers (88%) are concerned about experiencing serious side effects, higher than fathers (74%). Relatedly, nearly two-thirds of mothers (65%) also report concern about missing work if the side effects make them feel sick for a day or more, compared to less than half of fathers (47%). Many mothers and fathers also fear that the vaccines are not as safe as they are said to be.
Additionally, a larger share of unvaccinated parents with household incomes below $40,000 annually compared to those with higher incomes are also worried about experiencing serious side effects and having to miss work due to vaccine side effects. Parents may have these same concerns about their children experiencing side effects and needing to miss work to attend to them, particularly if they do not have paid sick leave benefits. Compared to higher income parents, a larger share of lower-income parents are also concerned about having to pay out-of-pocket costs for the vaccines (48% vs. 24%) and not being able to get the vaccine from a place they trust (48% vs. 27%).
Now that the FDA has authorized the Pfizer vaccine for adolescents, with younger children likely soon to follow, eyes have begun to shift to vaccine uptake among children. However, with less than a third of parents ready to get their children vaccinated right away, it will be important to provide accurate information to address their concerns. In addition, many parents, particularly mothers, report apprehension about side effects, and missing work with respect to their own vaccination decisions. Efforts to address these concerns such as paid sick leave or time off for children’s vaccinations could provide indirect avenues to allay potential fears regarding vaccinations for their children as well. Mothers have long played an outsize role in managing their children’s health, a role which could be central in determining how many children get vaccinated for COVID-19.
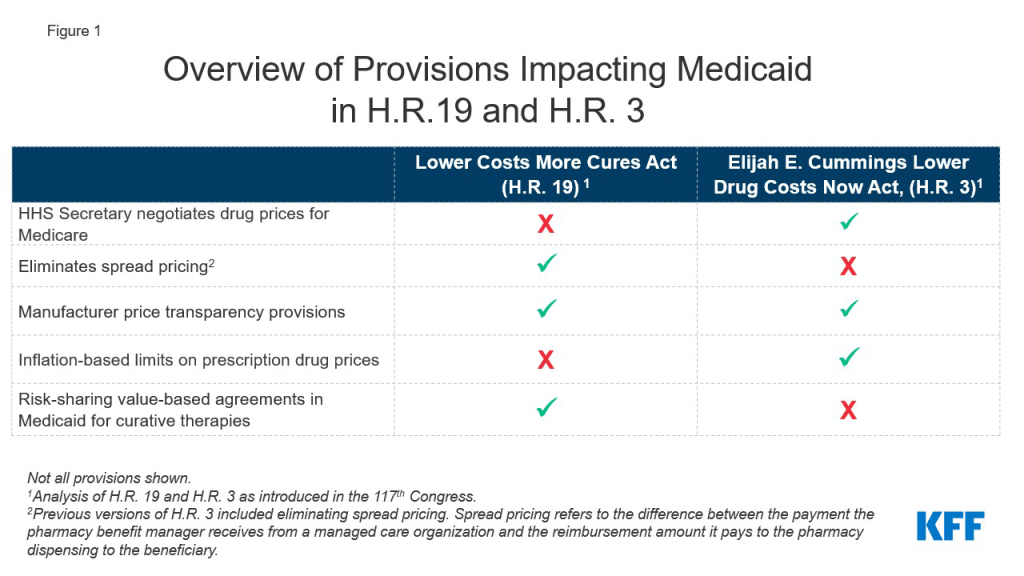
Prescription drug spending has again returned to the policy agenda, with Congress and the Administration developing proposals to target drug prices. Though attention in current federal actions is largely focused on Medicare and private insurance drug prices, federal legislation also has been recently introduced or enacted that would affect Medicaid prescription drug policy. In 2019, Medicaid gross drug spending was $66 billion and $37 billion was offset by rebates, resulting in $29 billion of net spending that is shared by states and the federal government. A separate analysis examines an array of leading federal and state policy drug pricing proposals and implications for Medicaid. A number of these proposals are included in two key bills that have been reintroduced in the 117th Congress: H.R. 3, The Elijah E. Cummings Lower Drug Costs Now Act, passed the house in 2019, it did not become law and has since been reintroduced in the 117th Congress. H.R. 19, The Lower Costs More Cures Act has also been reintroduced (Figure 1).
Figure 1: Overview of Provisions Impacting Medicaid in H.R. 19 and H.R. 3
Among the most notable provisions of H.R. 3 are allowing the government to negotiate drug prices for Medicare, which is not allowed under current law, and levying a penalty on drug prices that rise faster than inflation, both of which will likely affect Medicaid drug rebates. H.R. 3 would grant the Secretary of Health and Human Services (HHS) authority to negotiate prices for between 50 and 250 drugs without market competition, with an upper limit based on prices in a set of foreign countries. The negotiated price would apply to both Medicare and could also be used by commercial payers. There is also an additional penalty on Medicare drugs with prices rising faster than inflation. The Congressional Budget Office estimates that Medicaid direct spending would likely increase by about $2.5 billion due to lower rebate payments and higher launch prices due to the Medicare price negotiation and expanded inflation rebates, but federal spending overall would decrease significantly due to the large amount saved on Medicare drugs. Because Medicaid already receives inflationary rebates on drugs that have had large price increases over time, decreasing those prices may lead to lower rebates for the program. For brand drugs, inflation rebates account for about half of the total rebate Medicaid receives.
H.R. 19 includes provisions that would limit spread pricing bypharmacy benefit managers(PBMs) in Medicaid. Spread pricing refers to the difference between the payment the PBM receives from the state or MCO and the reimbursement amount it pays to the pharmacy. H.R. 19 would eliminate spread pricing in Medicaid by requiring pass-through pricing and only allow PBMs to collect an administrative fee. The version of H.R. 3 that passed the house in 2019 included a ban on spread pricing in Medicaid but the version reintroduced in 2021 does not. Eliminating spread pricing would generate savings for states and the federal government, through lower payments to MCOs or PBMs, approximately $929 million over ten years.
Both H.R. 3 and H.R. 19 would make information about list prices more accessible in an effort to curb drug costs. H.R. 19 includes a number of transparency provisions targeted both at Medicaid and at drug prices overall, including making National Average Drug Acquisition Cost (NADAC, a federal survey of pharmacies that helps states to determine pharmacy acquisition cost) mandatory, increasing oversight of manufacturer reporting for the MDRP, requiring manufacturers to provide notification and justification for certain price increases and for that information to be made available to the public. H.R. 3 would require the HHS Secretary to make the negotiated prices for drugs available to the public and would also require manufacturers to report to the Secretary of HHS to justify certain price increases. The impact of transparency on actual prices is uncertain, and may not produce savings for the Medicaid program unless transparency results in more accurate reimbursement to pharmacies or more accurate price reporting that increases rebates paid to states and the federal government.
H.R. 19 includes other provisions that have implications for Medicaid. H.R. 19 also includes other Medicaid-specific provisions, including collecting data on prescribing patterns and increased oversight of Medicaid pharmacy and therapeutic (P&T) committees. The bill would also create a state option for risk-sharing value-based agreements for curative drugs that would allow states to pay in installments over time.
Both H.R. 3 and H.R. 19 would make significant changes to the Medicare drug benefit and lower out of pocket costs for beneficiaries and people with private insurance, too. The proposals are expected to yield significant federal savings related to Medicare and private insurance, but there are implications for Medicaid as well. H.R. 3 and H.R. 19 have been introduced in the House and referred to committees, but a relatively narrow Democratic majority in the House and even narrower majority in the Senate could make legislative action difficult. However, if drug pricing proposals that offer significant savings, such as H.R. 3, do gain traction, the federal savings could be used as offsets for policies to advance other health care initiatives, such as lowering the age of Medicare eligibility and improving Medicare benefits or covering people in the Medicaid coverage gap.
A new KFF analysis shows that lowering the age of Medicare eligibility to 60 could improve the affordability of coverage for people who are already insured and expand coverage to over a million of the nation’s 30 million uninsured.
Such a policy could provide a path to Medicare coverage for up to 11.7 million people with employer-based insurance and 2.4 million with private, non-group coverage who are ages 60 to 64, although it is unclear how many would take up such coverage. Another 1.6 million people age 60-64 are uninsured and would be eligible for Medicare coverage under such a policy.
Lowering the age of Medicare eligibility could shift the cost of coverage largely from employers to the federal government and lower the cost of coverage for newly eligible people while increasing federal spending.
President Biden proposed lowering the age of Medicare eligibility to 60 during the presidential campaign and reiterated his support recently. Proposals to lower the age of Medicare, either to 60 or a younger age, may be considered by Congress.
The ultimate effect on coverage, access, and affordability of such a plan would depend on decisions individuals make and how the program is designed, including what type of premium and cost sharing assistance it provides to newly-eligible adults.
President Biden proposed lowering the age of Medicare eligibility to 60 during the presidential campaign and reiterated his support recently, with the goal of broadening coverage and making health coverage affordable for older adults. Proposals to lower the age of Medicare, either to 60 or a younger age, may be considered by Congress. One KFF analysis shows that lowering the age of Medicare eligibility to 60 could reduce costs for employer health plans by as much as 15 percent if all eligible employees shifted from employer plans to Medicare. In addition, another KFF analysis shows that 60- to 64-year-olds who move from employer plans to Medicare could be covered more cheaply because Medicare payments to hospitals, physicians and other health care providers are generally lower than what private insurance pays.
This data note looks at who might be affected by such policies and the implications for health coverage. Most people affected by a policy change to lower the age of Medicare already have private coverage, making the cost and affordability implications paramount. A relatively small share of people in this age range are currently uninsured, so the policy is likely to have a modest effect on increasing the number of people with health coverage.
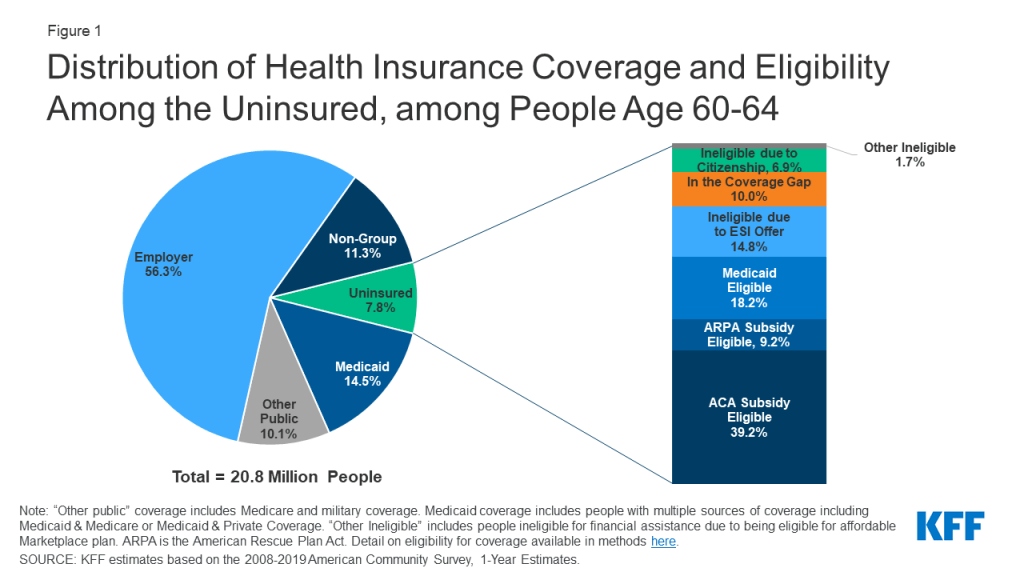
Two-thirds of adults age 60-64 have private coverage, either through an employer (56%) or though the non-group market, including those in the Affordable Care Act (ACA) marketplace (11%) (Figure 1). The policy to lower the age of Medicare eligibility could potentially shift 11.7 million people with employer coverage and 2.4 million with non-group coverage into Medicare. It is not clear how the policy would affect the 14.5% (3 million) who have Medicaid coverage, including the 4% within this group (just under 1 million) that are dually eligible for Medicare and Medicaid coverage (those who qualify on the basis of disability for both programs). About 8% of people age 60-64, or 1.6 million people, are uninsured and could newly gain Medicare coverage under this policy.
Among uninsured adults age 60-64, most (66%) are eligible for financial assistance for coverage through the ACA marketplace or Medicaid (Figure 1). Nearly half (48%) are eligible for marketplace premium help, including those eligible under temporary ARPA subsidies, and 18% are Medicaid-eligible. About 15% are estimated to have access to private coverage offered by an employer, which they may view as unaffordable. The remainder are in the coverage gap because they live in a state that has not expanded Medicaid (10%), are unauthorized immigrants (7%), or otherwise ineligible (2%).
Figure 1: Distribution of Health Insurance Coverage and Eligibility Among the Uninsured, among People Age 60-64
While a policy to lower the age of Medicare may have a small effect on covering the nearly 30 million uninsured people in the United States, it could improve access or affordability for millions. Policies to lower the age beyond 60—for example, to age 55 or even 50— could extend coverage to a larger number of uninsured adults (Table 1). Further, as otheranalysis shows, lowering the age of Medicare eligibility could shift the cost of coverage largely from employers to the federal government and lower the cost of coverage for this population while increasing federal spending. The ultimate effect on coverage, access, and affordability will depend on what type of premium and cost sharing assistance it provides to newly-eligible adults, as well as other structural factors.
Table 1: Health Insurance Coverage among Nonelderly Adults by Age, 2019
Just as the COVID-19 pandemic hit the United States (U.S.), the nation was ramping up efforts to address a different epidemic, HIV. Successful HIV outcomes require consistent access to care and medication, as does harnessing the preventive benefits of HIV treatment adherence. Similarly, key tools in HIV prevention are HIV testing and PrEP which necessitate access to health services. Yet, with options for medical care reduced, social distancing guidelines in place, and fears about COVID-19 exposure, COVID-19 threatened access to HIV care and prevention services and national efforts to address HIV. In addition, understanding the interplay of COVID-19 disease, vaccination, and HIV is important to the health of people with and at risk for HIV and curbing both epidemics. This analysis explores key questions around COVID-19 and HIV – what we know and what we are still learning.
Are people with HIV at higher risk for COVID-19?
NIH guidance states “whether people with HIV are at greater risk of acquiring SARS-CoV-2 infection is currently unknown.” While some researchers have proposed that people with HIV who are not virally suppressed or on treatment may be at increased risk of contracting SARS-CoV-2, the virus that causes COVID-19, because of a compromised immune system, others have found no such correlation. Most research and guidance to date has focused on whether people with HIV are more likely to experience severe outcomes from COVID-19 (e.g. severe illness, hospitalization, and death). Findings in this area were mixed for many months but a recent WHO report examining data from 24 countries and more than 15,500 people with HIV hospitalized for COVID-19 finds HIV is an independent risk factor for severe or critical COVID. Most previous research concludes that risk appears greatest for those who are immunocompromised or face other comorbid conditions. This study is particularly notable as it isolates HIV as a risk factor after controlling for disease severity and comorbidities along with a range of other factors. A significant limitation to the study, however, is that it lacked data on engagement with HIV treatment or viral suppression. Additional data on HIV and COVID risk includes:
Referring to severity of COVID-19 outcomes, the CDC states that while information is still somewhat limited, “we believe people with HIV who are on effective HIV treatment have the same risk for COVID-19 [disease] as people who do not have HIV.” Elsewhere CDC states that people “who have serious underlying medical conditions might be at increased risk for severe illness” and this may include “people who have weakened immune systems,” including people with HIV with a low CD4 cell count or not engaged in HIV treatment. As such CDC includes HIV in its list of conditions that “can” make someone more likely to get severely ill from COVID-19.
NIH guidance and a recent article by Dr. Anthony Fauci and others also finds the evidence as to whether people with HIV are at higher risk for COVID-19 or severe disease outcomes mixed. However, it concludes, “it is clear that the COVID-19 pandemic has had a great negative impact on persons with HIV” and that “the severity of COVID-19 disease in persons with HIV is related strongly to the presence of comorbidities that increase the risk of severe disease in COVID-19 patients in the absence of HIV.” Indeed, some of these comorbidities are more common in people with HIV than in those who are HIV negative.
Another review article finds that “the interaction between SARS-CoV-2 and HIV infection is still unclear and data are, at times, conflicting” but highlights larger more recent studies that find “that people living with HIV (particularly with low CD4 cell counts or untreated HIV infection) might have a more severe clinical course than those who are HIV-negative.”
Notably, many people with HIV in the U.S. could be considered at increased risk for severe COVID-19 illness based on the CDC definition due to uncontrolled HIV. An estimated 7% of people with HIV had a geometric mean CD4 count of less than 200 cells/µL (a marker of severely impaired immune system), another 11% had a CD4 count of less than 350 cells/µL. Further, just 60% of people with HIV report 100% antiretroviral therapy dose adherence in the preceding 30 days and over one-third (38%) do not have sustained viral suppression.
How do the social determinants of health, and their relationship to HIV, affect COVID-19 risk?
Apart from HIV, or comorbidities that heighten the risk for increased COVID-19 severity, people with HIV are overly represented in many of the demographic groups that that have been hardest hit by the COVID pandemic. Indeed, many are the very factors that place communities at risk for HIV. As such, people with HIV may be at higher risk for severe COVID-19 outcomes by virtue of their representation in these groups.
Race/Ethnicity
People of color have been disproportionately impacted by both COVID-19 and HIV, with overlapping risk factors. Compared to White people, people of color have been harder hit by COVID-19 in terms of cases, hospitalization, and deaths. This is true among Black, Hispanic, and especially American Indian or Alaskan Native people. American Indian or Alaskan Native people faced 1.6 times the case rate, 2.4 times the death rate, and 3.5 times the hospitalization rates compared to White people. Hispanic people also faced higher comparative rates at 2.0, 3.0, and 2.3 times that of White people, respectively (see figure 1). While case rates among Black people were similar to those among White people, rates of hospitalization and death were higher at 3.0 and 2.3 times the rate, respectively.
Notably, Black and Hispanic people, groups hard hit by COVID-19, are also hardest hit by HIV. While Black people represent just 12% of the U.S. population, they account for 41% of HIV cases; Hispanic people make up 19% of the US population but 23% of HIV cases (see figure 2). In addition, compared to White people with HIV, people of color with HIV have lower rates of viral suppression and engaging in HIV care, which could also make them more vulnerable to severe COVID-19 illness.
Age
Severe COVID-19 disease and deaths have been concentrated among older adults and on average, people with HIV are older compared to the general population. Nearly all (95%) COVID related deaths occurred among those 50 years and older; 81% have been among those 65 years and older. Those aged 64-74 have forty-times the risk of COVID-19 hospitalization compared to children aged 5-17 and the risk is ninety-five times greater among those 85 and older.
While national data on COVID-19 cases and outcomes by sexual orientation is not available, LGBT people have been hard hit by the pandemic in other ways, including with respect to job loss and negative mental health effects. Our recent survey found that a larger share of LGBT adults compared to non-LGBT adults report that they or someone in their household has experienced COVID-era job loss (56% v. 44%). In addition, three-fourths of LGBT people (74%) say that worry and stress from the pandemic has had a negative impact on their mental health, compared to 49% of those who are not LGBT, and LGBT people are more likely to say that the negative impact has been major (49% v 23%).
People with HIV are more likely to be LGBT than those in the general population and thus could be especially vulnerable to these negative effects of the pandemic. Over half (53%) of people with HIV identify as lesbian, gay, bisexual, or have a sexual identity other than heterosexual. Separately, two percent identify as transgender. This compared to 4.5% of people in the general population who identify as LGBT.
Income
People who live on lower incomes are thought to be at higher risk of exposure to SARS-CoV-2 and for serious illness if they become infected, compared to those who live on moderate to high incomes. Given that on average people with HIV live on substantially lower incomes than the general population, this too could put them in a higher risk group for COVID-19. Forty-three percent (43%) of adults with HIV live below the poverty level compared to 11% of U.S. adults overall.
Factors that contribute to these increased risks include socioeconomic and demographic circumstances and higher rates of certain comorbidities. People who live on lower incomes may be more likely to live in dense settings, work in essential jobs that did not allow for work remotely during the pandemic, or work in high-risk environments, such as in the service and healthcare industries. People on lower incomes may also be at higher risk due to increased rates of certain health conditions. For example, one KFF study found that non-elderly adults earning below $15,000 a year had double the risk of serious illness if they contracted COVID-19 compared to those earning $75,000 per year based on the presence of certain high-risk health conditions.
How likely is it that people with HIV live in COVID-19 hot spots?
People with HIV commonly live in counties hard hit by the COVID-19 pandemic. Three-quarters (75%) of the top 20 US counties by HIV prevalence are also among the top 20 counties by COVID case and/or death burden. These 15 counties are home to 32% of people with HIV (see figure 3). While some of the overlap might be accounted for by urbanicity, 20% (4 in 20) of the counties hardest hit by COVID and HIV were not among the nation’s 20 most populous counties. In addition, counties hard hit by the COVID-19 pandemic also face high levels of racial and ethnic, income, and other structural inequalities driven by deeply rooted discrimination.
What do we know about COVID-19 vaccines and HIV?
NIH clinical guidelines on COVID-19 and people with HIV state that “people with HIV should receive SARS-CoV-2 vaccines, regardless of CD4 or viral load, because the potential benefits outweigh potential risks” and also notes that people with HIV “who are well controlled on antiretroviral therapy (ART) typically respond well to licensed vaccines.” In addition, CDC states “people with moderately to severely compromised immune systems are especially vulnerable to COVID-19, and may not build the same level of immunity to 2-dose vaccine series compared to people who are not immunocompromised.” As such the agency “recommends that people with moderately to severely compromised immune systems receive an additional dose of mRNA COVID-19.” CDC includes people with “advanced or untreated HIV infection” in this group.
People with HIV were at first excluded from COVID-19 vaccine trials but were permitted to join midway through phase 3 clinical trials. Ultimately, all companies with vaccines authorized for use in the U.S. included people with HIV in their phase 3 trials. The largest group was in the Jansen (J&J) trial which enrolled 1,218 participants with HIV, representing 2.8% of the trial population, split evenly in the vaccine and placebo groups. In analysis the company provided to the FDA in February 2021, vaccine efficacy could not be observed specially among people with HIV based on limited data availability. However, data were not suggestive of any harm. Smaller numbers of people with HIV were enrolled in Moderna and Pfizer vaccine trials. In addition, AstraZenenca, Novavax, Sanofi/GlaxoSmithKline, which do not have authorization in the US, also recruited HIV positive participants. Overall, because participation to date has been relatively low, drawing conclusions about immune response among people with HIV is not yet possible.
Finally, CDC includes HIV among a list of conditions that can make someone more likely to get severely ill from COVID-19. In the past, the CDC list was divided into conditions known to have an increased risk for severe COVID-19 and conditions that might pose an increased risk. HIV was not included in the original list on its own, but “immunocompromised state,” defined to include immunocompromised due to HIV, was included in the second list. When making recommendations regarding prioritizing high-risk populations for COVID-19 vaccination, CDC referred to the main list which was also used by most states. States varied in how they incorporated the second list, including immunocompromised state, in their vaccine prioritization. Separately, some states elected to include HIV as a standalone priority condition. As a result, states varied on how early they prioritized people with HIV in their vaccine efforts.
The HIV Medical Association (HIVMA) and the Infectious Diseases Society of America (IDSA) provide a regularly updated frequently asked questions documents on HIV and COVID-19 vaccinations aimed at clinicians.
What role is the federal government playing in addressing COVID-19 among people with HIV?
Several federal agencies or programs have specifically responded to the impact of COVID-19 on people with and at risk for HIV, including, the Centers for Disease Control and Prevention (CDC), the Health Resources Service Administration’s (HRSA) Ryan White HIV/AIDS Program, the National Institute of Health (NIH), and Housing and Urban Development’s (HUD’s) Housing Opportunities for People with AIDS (HOPWA) program:
CDC: CDC provides general guidance on people with HIV and COVID-19, including an evolving statement on risk and, as noted above, includes HIV in a list of conditions that can make someone more likely to get severely ill from COVID-19. HIV was not included in an earlier version of this list..In addition to providing public health guidance on people with HIV and COVID-19, CDC has also modified some of its prevention activities in light of the pandemic. CDC released guidance related to home or self-HIV testing, recognizing that “HIV testing that requires face-to-face contact has been scaled back or suspended because of the COVID-19 pandemic response.” Similarly, the agency also released guidance around PrEP and COVID-19 for “when facility-based services and in-person patient-clinician contact is limited,” describing options for home STI specimen collection and self-testing for HIV.CDC HIV program staff are also contributing significantly to the nation’s COVID response which has, per the agency, caused disruptions to care and treatment activities as the National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. As of April 2021, nearly 700 CDC staff (with 1,125 cumulative deployments) from the National Center had been deployed to work on the COVID response since the epidemic began, in part, leveraging infectious disease expertise.1
NIH: NIH’s national HIV guidelines now include a section on “Interim Guidance for COVID-19 and Persons with HIV.” In addition, the NIH’s COVID-19 treatment guidelines include a “special population” section on “Special Considerations in People With Human Immunodeficiency Virus.” These sections review recommendations for ongoing HIV treatment during the pandemic (and in the case of COVID-19 infection) as well as COVID-19 prevention, treatment, and vaccination among people with HIV and are considered “living documents,” updated on a regular basis as more data become available.
The Ryan White Program (HRSA): Ryan White, the nation’s safety-net for HIV care and treatment, faced significant challenges in the wake of the Coronavirus pandemic. In our survey of Ryan White care providers conducted in late 2020, we found that operating challenges were common. Among those surveyed, 28% shut down all or most of their HIV prevention services in response to the pandemic at some point and others faced difficulty connecting with service partners or increased operating costs. Dealing with client and staff trauma and isolation was a significant challenge. However, in many cases, programs reported transforming to meet shifting client needs and to improve safety for staff and clients, including through offering telehealth, providing COVID-19 testing, and engaging in multi-month prescribing, among other activities..Recognizing the potential for increased need among people with HIV during the pandemic and, in order to “to prevent, prepare for, and respond to coronavirus,” Congress provided the Ryan White Program with $90 million in emergency funding in the CARES Act, the 3rd major COVID-relief package signed into law in March 2020. The Ryan White Program distributed the funding to 581 program grantees across the country, including to health departments, health clinics, community-based organizations and national training centers. In June 2021, The Program released a report examining grantees use of CARES Act funds for activities such as telehealth, COVID-19 testing, and other traditional program activities. It finds that, in December 2020, over 85,000 Ryan White clients received a service funded through the CARES Act grants. Grantees have used CARES Act funding to conduct and build out telehealth services including for ambulatory and mental health services, medical case management, and support services as well as to conduct COVID-19 testing, purchase protective equipment for staff and clients, fund client nutrition assistance programs, and support staff positions needed as part of pandemic response, and for other purposes. Between January 20, 2020 and December 31, 2020 CARES Act funded providers served nearly 19,000 clients with newly diagnosed COVID-19.In addition, the program has encouraged grantees to utilize existing flexibilities and waived certain requirements when possible, recognizing that business as usual has been challenged by the pandemic. In particular, the program has asked grantees to “reassess their organization’s eligibility and recertification policies and procedures and remove any procedures that may impede social distancing or other public health strategies necessary to minimize COVID-19 transmission, or that impose” unnecessary requirements. Historically, while some grantees have already simplified these processes, others have policies in place that can create barriers not required by the program. Certain penalties and requirements were waived for all grantees either automatically or by request, though some were only able to be extended to CARES Act funded activities. Waivers generally relate to penalties and how funds can be used.The program maintains an updated list of frequently ask questions about Ryan White and COVID-19. In addition, In January 2021, The Program issued a letter outlining how grant recipients can engage in vaccination efforts, noting that Ryan White grantees and subgrantees may “play an important role in COVID-19 vaccine administration” and that all play “a critical role in addressing COVID-19 vaccine hesitancy and distributing information about local access to vaccines.”
Housing Opportunities for People AIDS Program (HOPWA) (HUD): The CARES Act also provided $65 million for the HOPWA program to maintain operations, for rental assistance, supportive services, and other necessary actions, in order to prevent, prepare for, and respond to coronavirus. Grants were distributed to 140 formula grantees, 82 current HOPWA competitive renewal grantees, and existing technical assistance providers. The HOPWA program also provided grantees with clarity around waivers and flexibilities to improve services during the pandemic.
What do we know about HIV care, treatment, and prevention service use during the pandemic?
It appears that for some, HIV care and especially prevention access, in the U.S., has been impacted by the COVID-19 pandemic. While in some cases services and prescription fills have improved, it does not yet appear they have returned to the pre-pandemic baseline:
Care and Testing: As noted above, despite pivots to providing care in new ways that mitigated some of the impact, Ryan White providers reported that their ability to provide certain services declined during the pandemic, though there are some reports that it has picked up to a certain extent. While some patients were harder to reach through telemedicine, others thrived with the technology and some who had been out-of-care, were brought back in..CDC researchers found that HIV testing and viral load monitoring declined in the wake of the pandemic. While HIV testing and viral load monitoring has begun to pick back up, as of September 2020, it had not recovered to 2019 levels. In a separate analysis, CDC also found that ambulatory care visits and viral load testing declined while telemedicine visits increased in 2020. However, despite the increase in telemedicine, total visits did not fully rebound to pre-pandemic levels. Other research has echoed this with one analysis of 8 clinical sites finding that outpatient office visits for HIV care declined 78% between January and June 2020, even when accounting for telehealth visits.Researchers in Oregon found that public sector HIV and bacterial STI testing declined substantially in the state in the wake of COVID related distancing measures but once testing rebounded to a certain extent, primary and secondary syphilis diagnoses increased, “indicating ongoing sexual risk during physical distancing.”
ARVs (for treatment and prevention): Data from Gilead, the company supplying ARVs to the majority of people with HIV in the U.S., show that sales for HIV medications (presumably for both prevention and treatment) dropped initially in 2020 and picked up by the end of the year but had not fully recovered.One San Francisco clinic found that the share of patients with viral load suppression declined 30% during the pandemic, suggesting lack of access to or adherence with ARVs.A CDC analysis found that PrEP prescriptions in the U.S. declined 21%, and that there was a 28% drop in new PrEP starts, between March and September 2020, compared to what was expected. Decreases were sharpest for younger people, those paying with cash or using patient assistance programs, and those in certain states.
Analysis of prescription data from GoodRx point to declines in prescriptions for the medications used for PrEP during early months of the pandemic. While those drugs are also sometimes used for treatment, other non-PrEP treatment drugs saw a smaller, though still detectable decline. Prescriptions for the medications used for PrEP declined 18% compared to baseline while other drugs used for HIV treatment declined 5% compared to baseline.
In addition, for many with and at risk for HIV, meeting basic needs is a common struggle and for some, this was heighted during the pandemic. There have been reports that some people with HIV and HIV service organizations faced delays in access to food and financial assistance during the pandemic. Lack of basic security for key resources such as food, housing, and economic stability, can undermine people’s ability to access and engage in HIV care, treatment, and prevention.
This work was supported in part by the Elton John AIDS Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
CDC/HRSA Advisory Committee on HIV, Viral Hepatitis and STD Prevention and Treatment (CHAC). April 20, 2021. Presentation by Dr. Jonathan Mermin. ↩︎
New Campaign from THE CONVERSATION / LA CONVERSACIÓN Responds to Information Needs about COVID-19 Vaccines Among Latinos and Spanish-speaking People in U.S.
Latinx Doctors, Nurses and Promotoras Featured in Latest Installment of KFF’s Public Information Response to COVID-19, Presented with UnidosUS
May 20, 2021 – THE CONVERSATION / LA CONVERSACIÓN expands to address information needs about the COVID-19 vaccines in the Latinx community with new videos featuring doctors, nurses and promotoras (community health workers) in English and Spanish. This installment of the campaign is produced by KFF (Kaiser Family Foundation) under its Greater Than COVID public information response and presented with UnidosUS.
“THE CONVERSATION / LA CONVERSACIÓN campaign—and our efforts with the UnidosUS Esperanza Hope for All campaign—use trusted voices to send the message that the vaccines are our best chance at getting back to our lives. But we need more support to make sure everyone can get a vaccine as a new report from our friends at KFF shows. Unvaccinated Latinos want to get the vaccine but face obstacles such as not having access to paid leave, being asked by vaccine providers for sensitive information that increases barriers to getting more Americans vaccinated, or hard to access vaccination sites. We need to reaffirm that COVID-19 vaccines are free and available to ALL, regardless of immigration status or access to health insurance and we also urge that sites are put in places where Latinos are: schools, workplaces, and community centers across the country,” said UnidosUS President and CEO Janet Murguía.
Recent findings from the KFF COVID Vaccine Monitor shows strong interest from many Hispanic adults in getting vaccinated as soon as possible, indicating an opportunity for increased outreach and information. Health care providers, especially those representing the community, have consistently been shown to be the most trusted and preferred resources for information about the vaccines.
“Unvaccinated Hispanic adults are much more likely to want to get vaccinated than other adults and THE CONVERSATION/LA CONVERSACIÓN provides a platform for trusted messengers to build on interest in the Latino community in getting vaccinated,” said KFF President and CEO Drew Altman.
Eligibility and access issues, as well as questions about vaccine safety and efficacy, are among issues highlighted in more than 75 FAQ videos from Latinx healthcare workers, reflecting some of the most common concerns raised in KFF research.
In addition to providing accessible facts and dispelling misinformation, the health care workers also share their own experiences getting vaccinated, what it meant for them both personally and professionally, as well as their hopes for what it means for the community. “This is about returning to our roots, to our families, to being able to be safe and not live in fear,” says Susana Morales, MD, a primary care doctor in one of the videos included in the campaign. Dr. Morales, who is Vice Chair for Diversity in the Department of Medicine at Weill Cornell Medicine, is one of 10 Latinx health care workers featured in the new campaign.
YouTube provided funding to support development and distribution of the series and both YouTube and Google are providing high visibility promotion on their platforms. Facebook is supporting the campaign as part of a broader effort to amplify trusted voices in communities to help reach people most affected by COVID-19. Twitter and Pinterest are also helping to get out the messaging on their platforms.
UnidosUS, previously known as NCLR (National Council of La Raza), is the nation’s largest Hispanic civil rights and advocacy organization. Through its unique combination of expert research, advocacy, programs, and an Affiliate Network of nearly 300 community-based organizations across the United States and Puerto Rico, UnidosUS simultaneously challenges the social, economic, and political barriers that affect Latinos at the national and local levels. For more than 50 years, UnidosUS has united communities and different groups seeking common ground through collaboration, and that share a desire to make our country stronger. For more information on UnidosUS, visit www.unidosus.org or follow us on Facebook, Instagram, and Twitter.
Greater Than COVIDis a public information initiative from KFF to help individuals take charge of their health during the evolving COVID-19 public health crisis. Tailored media messages and community tools address information needs about the vaccines.