HHS Public Health Policy Actions Under the Trump Administration 2025-2026
Note: Originally published on Nov. 12, 2025, this resource is updated as needed, most recently on March 19, 2026, to reflect additional developments.
Since assuming office for a second term, President Trump and officials in his administration have instituted numerous policy actions through the Department of Health and Human Services (HHS) affecting public health in the U.S. This resource lists and briefly describes key actions in the order in which they were first issued, reported or announced, with subsequent linked actions and related outcomes also included with each entry. As new policy changes occur, they will be added.
This resource is not meant to be exhaustive of all administration actions related to public health, as many other federal policy changes – including outside of HHS – have public health implications but are not captured here.
Additional KFF resources on administrative actions related to global health, LGBTQ+ health, and mental health and substance abuse are also available.
Date | | Action/Description |
|---|---|
| January 20, 2025 | Presidential Executive Orders precipitate removal of some HHS websites and health data. – In the first days of his second term President Trump issued a number of Executive Orders (EOs), including EOs that revoked many Biden administration orders and programs, and instituted new federal guidance related to “gender ideology,” “diversity, equity, and inclusion (DEI),” and “merit-based opportunities.” These EOs have implications for public health, particularly related to the collection and presentation of data and websites by the federal government. For example, in response to the EOs, HHS began to remove thousands of websites and numerous federal databases with public health information deemed to be related to DEI, LGBTQ, reproductive health, HIV/AIDS research, health disparities, and more, and limited some data collection and analysis in these areas. A lawsuit was filed to reverse these removals, and some information has been restored over time. In September, the administration agreed to restore all previously removed health-focused websites and data to versions that had existed on January 29, 2025. |
| February 7, 2025 | NIH announces change to indirect cost rate guidance. – As part of grants for health research, the National Institutes of Health (NIH) provides “indirect cost” funding to grant recipients, which supports administration and facilities costs at grantee institutions. On February 7, NIH announced it would apply a new 15% “standard indirect cost rate” on all grants, which would apply to any new grants and to existing grants for expenses as of February 10, 2025. This was challenged in federal court and federal judges placed holds on the policy, first through a temporary restraining order affecting 22 states on February 10, a nationwide preliminary injunction on March 5, and a permanent injunction on April 4; prior rates still apply for the time being. The administration appealed the ruling and legal proceedings continue. If implemented, a 15% indirect cost rate would be a much lower rate compared to historical NIH rates and would amount to a significant cut in funding for institutions performing NIH-sponsored health research. |
| February 13, 2025 | Robert F. Kennedy, Jr. confirmed as HHS Secretary under President Trump. – The Senate voted 52-48, along party lines, to confirm Robert F. Kennedy, Jr. as the Secretary of Health and Human Services. |
| February 13, 2025 | President Trump issues Executive Order (EO) establishing MAHA policy agenda and MAHA Commission. – The EO outlines the purpose and objectives of the Trump administration’s Make American Healthy Again (MAHA) efforts. Stating that the U.S. must “re-direct our national focus…toward understanding and drastically lowering chronic disease rates and ending childhood chronic disease,” it directs federal agencies to “aggressively combat” mental health disorders, obesity, diabetes, and other conditions. It also establishes the MAHA Commission to advise the President, naming Secretary Kennedy as Chair. The EO directs the Commission to submit an assessment on how to combat the “childhood chronic disease crisis” within 100 days, and a strategy to address the crisis within 180 days, setting in motion processes to develop further public health strategies and plans (discussed in other entries below). |
| February 14, 2025 | White House, DOGE initiate “reduction in force (RIF)”, including for HHS personnel. – The EO outlines the purpose and objectives of the Trump administration’s Make American Healthy Again (MAHA) efforts. Stating that the U.S. must “re-direct our national focus…toward understanding and drastically lowering chronic disease rates and ending childhood chronic disease,” it directs federal agencies to “aggressively combat” mental health disorders, obesity, diabetes, and other conditions. It also establishes the MAHA Commission to advise the President, naming Secretary Kennedy as Chair. The EO directs the Commission to submit an assessment on how to combat the “childhood chronic disease crisis” within 100 days, and a strategy to address the crisis within 180 days, setting in motion processes to develop further public health strategies and plans (discussed in other entries below). |
| February 14, 2025 | President Trump issues Executive Order prohibiting federal funding to schools and universities with COVID-19 vaccine requirements. – The EO requires HHS to work with the Department of Education to prohibit COVID-19 mandates in schools, by issuing guidelines for compliance and barring federal funds from going to any educational agency, K-12 school, or institution of higher education that requires COVID-19 vaccination to attend in-person education programs (educational vaccine mandates are set at the state level). Educational vaccine requirements are set at the state and local levels. At the time the EO was released in February, no state required K-12 students to be vaccinated against COVID-19 while 15 colleges required Covid vaccines for students. However, by March 14, 2025 all of those colleges had ended their COVID-19 vaccine requirements for students. |
| February 18, 2025 | Secretary Kennedy announces public health policy priorities during HHS welcome ceremony. – In his first remarks to HHS staff, Secretary Kennedy announces the public health priorities for his tenure. This include investigating the childhood vaccine schedule, tackling corruption and promoting transparency, and addressing a “chronic disease epidemic” especially in children, which he says may be linked to pesticides, food additives, antidepressants, microplastics, cellphone emissions, and other factors. |
| February 28, 2025 | Secretary Kennedy issues new rule ending public comment requirement for HHS grants and contracts. – The new rule rescinds a prior HHS policy on “Public Participation in Rule Making” (the “Richardson Waiver,” dating back to 1971) and “re-aligns the Department’s rule-making procedures with the Administrative Procedure Act.” As a result, “matters relating to agency management or personnel or to public property, loans, grants, benefits, or contracts” are exempt from the notice and comment procedures. This removes what had been a key step in the rulemaking process requiring public notification and a comment period. For example, changes to HHS policies related to work requirements for Medicaid and NIH funding would no longer require public comments under the new rule. This could streamline implementation of HHS policy, but also reduce public visibility on changes before they take effect. Some lawmakers and public health focused groups have asked HHS to return to the prior requirements under the Richardson Waiver. |
| March 7, 2025 | HHS announces that CDC will conduct a study of factors contributing to the rise in autism in the U.S. – In statements to the press, HHS officials indicate CDC will initiate a study looking at the factors that are contributing to the rise in autism diagnoses in the U.S.. To date, no new CDC study results on this topic have been released though in a related development, in September 2025 President Trump and HHS leadership announced at a press conference and through a White House Fact Sheet that they believe there is a link between acetaminophen (e.g., Tylenol) use in pregnancy to autism (further details provided below). President Trump and Secretary Kennedy both have a history of linking vaccines and autism, even though there is no evidence of such a link. |
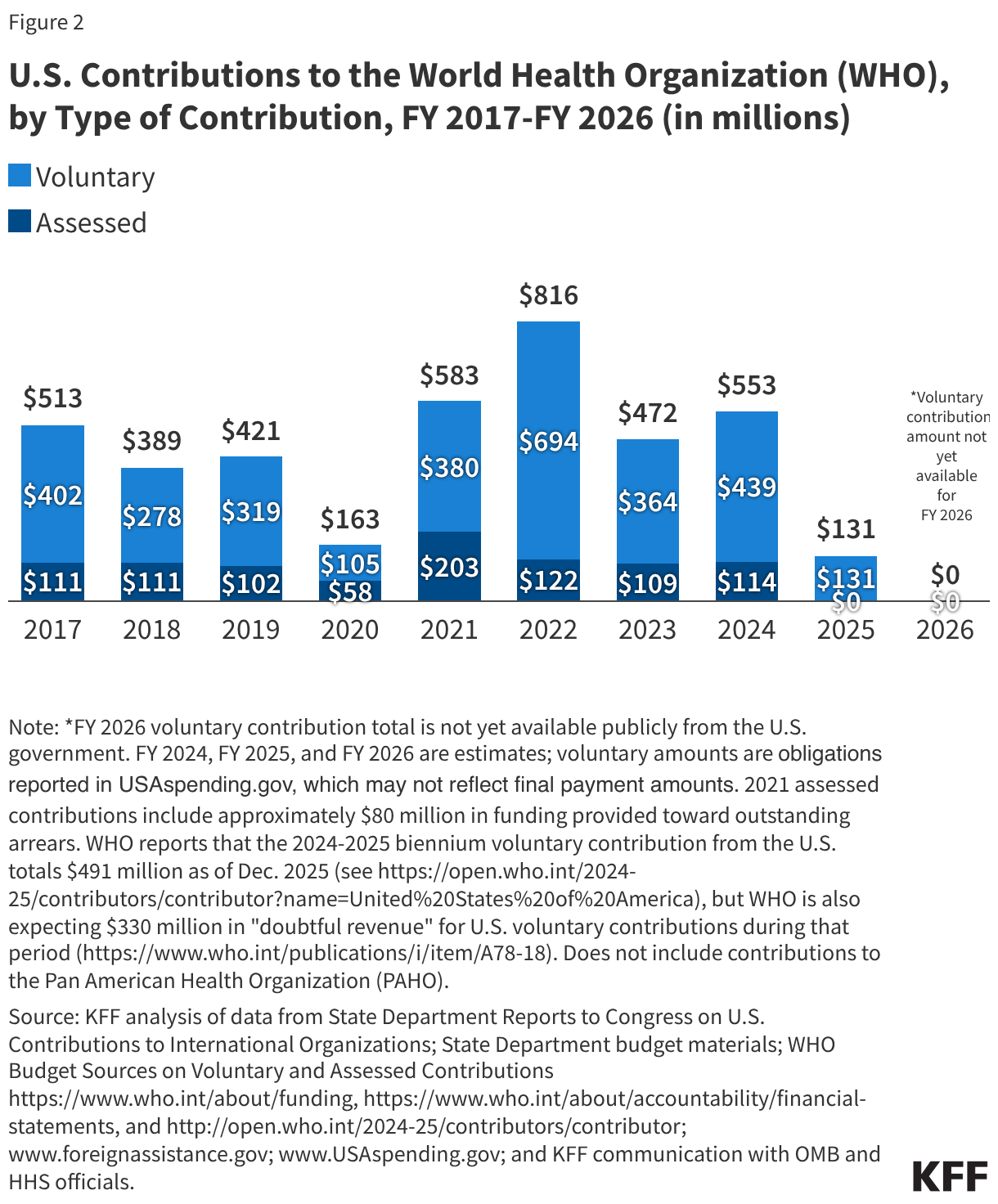
| March 13, 2025 | Food and Drug Administration (FDA) releases guidance on 2025-2026 influenza vaccine composition. – The FDA guidance identifies which influenza virus strains manufacturers should use as components of 2025-2026 influenza vaccines. To develop these recommendations, FDA convened meetings of federal scientific and public health experts, including from FDA, CDC, and Department of Defense, but did not consult with the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) or other professional groups outside the government. FDA had canceled the scheduled VRBPAC meeting on this topic, and the lack of input from outside experts was a break from past years’ practices. In addition, in past years there was active participation and coordination between U.S. federal experts and global technical experts working under the auspices of the World Health Organization (WHO), but official communications with WHO-linked experts has been curtailed since the Trump administration announced in January 2025 that the U.S. was withdrawing its membership from the UN agency. |
| March 17, 2025 | NIH initiates termination of numerous grants for HIV prevention and treatment programs. – The canceled NIH grants include support for researchers investigating use of PrEP, medication used pre-exposure to prevent HIV infections, and programs focused on HIV/AIDS in adolescents and young adults. Even as the first Trump administration supported HIV/AIDS prevention and treatment efforts, including through a highly visible federal effort to “end the HIV epidemic” in the U.S. by 2030, these same programs have now been targeted for cuts (further details below). |
| March 17, 2025 | HHS removes Surgeon General warning declaring gun violence a public health crisis. – The HHS website was changed, removing a 2024 advisory from the Surgeon General on the public health impacts of gun violence. In addition to removing the Surgeon General’s warning, the administration has rolled back a number of gun safety policies in place during the Biden administration. The White House Office of Gun Violence Prevention, established during the Biden administration was shut down in early 2025. Further, significant numbers of staff at CDC’s Injury Center, which collects data on violent deaths and injuries, and CDC’s Division of Violence Prevention have been let go as part of the Trump administration’s reduction in force efforts. |
| March 25, 2025 | HHS and CDC seek to pull back $11 billion in supplemental COVID-19 and public health funding from state and local health departments. – In a statement, HHS says it intends to pull back $11.4 billion in supplemental funding that had been provided by Congress for state and local public health departments through CDC for pandemic response activities. Following the announcement, on April 1, a group of 23 mostly Democratic-led states sued the Trump administration over the attempt to pull back this funding. On April 3, a federal judge placed a temporary block on the administration’s actions, and on May 16, another federal judge indefinitely blocked the administration from enacting its funding pull back for the states that are part of the lawsuit. As of late August 2025, almost 80% of the funds initially targeted for cuts by the Trump administration had been restored for the 23 states that won in court. However, funding has not been restored to the remaining states, the majority of which are Republican-led. |
| March 27, 2025 | HHS announces a major re-organization and job cuts plan. – HHS announces plans for a major restructuring of the department, in accordance with President Trump’s February 26 EO on “Implementing the President’s ‘Department of Government Efficiency’ Workforce Optimization Initiative.” The announcement says HHS will create an Administration for a Healthy America (AHA), which would combine several existing HHS offices including the Office of the Assistant Secretary of Health (OASH, which contains the Surgeon General’s Office), the Health Research and Services Administration (HRSA), the Substance Abuse and Mental Health Services Administration (SAMSHA), the Agency for Toxic Substance and Disease Registry (ATSDR), and the National Institute for Occupational Safety and Health (NIOSH). In addition, the Administration for Strategic Preparedness and Response (ASPR) at HHS would be moved under CDC. The announcement also says HHS will reduce its workforce by eliminating 10,000 full-time positions. Combined with other reduction in force efforts, a total of 20,000 HHS workers are expected to lose their jobs. On May 5, a coalition of 19 Democratic-led states and the District of Columbia filed a lawsuit against the mass firing of federal health workers and re-organization of HHS. On May 10, a court ordered a temporary pause on sweeping federal firings at HHS and other agencies. On July 1, a federal judge blocked mass firings at HHS, saying they are likely unlawful. However, on July 8 the Supreme Court overturned the lower court decisions, allowing the Trump administration to proceed with job cuts. As of August it is estimated that over 20,000 jobs at HHS have already been cut, meaning the administration already met its initial workforce reduction goal. Regarding re-organization, some organizational changes have been implemented at HHS, with major cuts or closures to public health related offices such as the HHS Office of Infectious Diseases & HIV Policy, the HHS Office of Minority Health, and HRSA’s Bureau of Primary Health Care. However, other proposals such as the formation of an Administration for a Healthy America (AHA), have not yet been implemented. Implementing AHA to the extent proposed is likely to require approval from Congress, though so far Congress has not acted on legislation codifying these proposals. |
| March 31, 2025 | HHS withholds portion of Title X family planning service grants. – HHS notifies one in five current grantees of the federal Title X family planning program that a portion of their funding would be temporarily withheld. This funding freeze affects all nine Planned Parenthood grantees, in addition to 7 other nonprofit grantees, and it is estimated that a total of 879 clinics (24% of all Title X clinics) in 23 states are affected. After several months, funds were reinstated to some organizations, but the Planned Parenthood grantees have still not had their funding reinstated. |
| April 1, 2025 | HHS ends federal support for the “Safe to Sleep” program, which focuses on prevention of infant deaths during sleep. – The Trump Administration ends federal participation in Safe to Sleep, a national campaign that focused on educating parents of newborns about safer sleeping practices for infants that can prevent death. The program, supported through the NIH’s National Institute of Child Health and Human Development (NICHD) Office of Communications in recent years, had been in existence for over 30 years and had contributed to a major decline in sudden infant deaths. The NICHD office was eliminated on April 1, along with federal support for “Safe to Sleep.” |
| April 2, 2025 | HHS requires CDC to reduce contract spending by $2.9 billion as part of DOGE cost reduction efforts. – According to reports, HHS orders CDC to reduce its contract spending by $2.9 billion by April 18.CDC contract funding has been used to support several services at the agency including security, cleaning, and computers/technology. The sudden requirement to cut this spending by approximately 35% affects CDC operations. |
| April 7, 2025 | HHS Secretary Kennedy announces changes to fluoride policies. – Secretary Kennedy announces a plan to implement a number of changes to federal policy related to water fluoridation, including stating that CDC will stop recommending water fluoridation as a public health intervention (though to date, HHS and CDC still recommend community water fluoridation). In addition, Kennedy says the defunct Community Preventive Services Task will be revived and reconvened, with a goal of studying and making recommendations about water fluoridation. Kennedy also called on states to ban fluoride in their drinking water. Already this year Utah and Florida have banned community water fluoridation, the first states ever to do so. |
| April 17, 2025 | FDA informs Pfizer/Moderna that mRNA COVID vaccines will require an expanded warning label about myocarditis. – In letters sent April 17, the FDA informs Pfizer and Moderna they must alter the warning labels for their COVID-19 mRNA vaccines to include expanded risks for myocarditis and pericarditis. Previously, the warning labels for these vaccines noted risks for these conditions for those aged 18 to 24 years (Moderna) and 12 to 17 years (Pfizer). However, updated labels are required to include new language saying “the observed risk of myocarditis and pericarditis following vaccination with mRNA COVID-19 vaccines has been highest in males 12 through 24 years of age” and that “persistence of abnormal cardiac magnetic resonance imaging (CMR) findings that are a marker for myocardial injury was common.” According to FDA, the labels must also include more information about these conditions and their health risks. Since the letters were sent, the companies have complied with the new FDA requirements. FDA approved the updated label language on June 25. |
| April 22, 2025 | FDA and HHS announce measures to phase out use of petroleum-based food dyes. – FDA and HHS announce a series of steps the federal government will take to remove petroleum-based synthetic dyes from the U.S. food supply. These actions include initiating a process to revoke federal authorization for two such dyes and planning phase-outs by the food industry for others. In addition, the government will support research on food additives and children’s health and authorize natural alternative coloring options. Under the current plan, the phase-outs will occur through voluntary action taken by food companies. |
| May 1, 2025 | HHS announces a $500 million investment in a “next generation universal vaccine platform.” – HHS and NIH announce that $500 million in funding will be directed to a new effort to develop a “universal vaccine platform for pandemic-prone viruses.” The platform uses inactivated whole viruses, and is part of a broader federal effort to develop universal vaccines called “Generation Gold Standard.” The funds for this new investment appear to be re-purposed vaccine development funds from the Biden Administration’s NextGen initiative to develop next generation COVID-19 vaccines. |
| May 2, 2025 | White House Releases FY 2026 President’s Budget Request calling for major fundings cuts at HHS. – The White House released an outline of the administration’s budget request for FY2026 and on May 30, the White House submitted the full Budget Request for FY2026 to Congress. The request proposes steep cuts to the HHS budget, including cuts for CDC, HRSA, SAMHSA, NIH, eliminating the Hospital Preparedness Program at ASPR, and reducing funding and cutting some programs focused on HIV/AIDS research and response. The budget request also asks Congress for $500 million to support a new “Administration for a Healthy America (AHA)” and MAHA-related priorities. The President’s Budget Request is only a proposal, as it is Congress that ultimately decides how much money the federal government appropriates. So far, Congressional spending bills for FY2026 have not included cuts to HHS of the magnitude requested by the President, and Congress has not provided the requested $500 million for AHA though budget negotiations continue. |
| May 5, 2025 | White House Executive Order restricts funding and increases oversight for “gain of function” research at HHS. – In an EO titled “Improving the Safety and Security of Biological Research” the White House cites concerns with federally funded “gain-of-function” (GOF) research on biological agents and states the Biden administration allowed dangerous GOF research to occur without sufficient oversight. The EO directs the Secretary of HHS to coordinate with other relevant Executive branch offices to establish guidance to end federal funding of “foreign entities” where GOF is being undertaken or in countries lacking oversight of GOF research. The EO requires the relevant Executive offices to submit updated policies and guidance for all federally supported GOF-related research, and to develop a strategy for managing risks of non- federally funded GOF research. The full implications of the EO are not yet clear, as the Executive branch offices must develop and implement specific guidance and regulations. According to outside experts, potential benefits of the EO include more transparency and stricter enforcement of dangerous research, while potential risks include hindering beneficial research that is not GOF and researchers choosing to curtail beneficial research to avoid potential repercussions under evolving federal restrictions. |
| May 20, 2025 | FDA leaders announce clinical trials will be needed for approval of certain new COVID vaccine formulations. – In a medical journal article, FDA leaders indicate that going forward, for federal approval of new or updated COVID-19 vaccines (“boosters”) for use in individuals who are not considered at higher risk (defined as persons 65 or older or those with certain health conditions), will require vaccine makers to present evidence from randomized, placebo-controlled trials that demonstrate safety and efficacy. The announced policy is a departure from prior years when FDA did not require new trial data to authorize or approve boosters, but instead allowed approvals based on immune response evidence. The new policy could hinder investments by pharmaceutical companies in developing new COVID vaccine formulations, given the greater expense and time required to conduct new, full clinical trials. |
| May 22, 2025 | MAHA Commission Report on childhood chronic disease published. – The first official report from the MAHA Commission (established by the February 13 EO discussed above) discusses factors contributing to a “chronic disease crisis” for U.S. children and provides a “call to action”. The report highlights four main drivers of the crisis: poor diet (primarily due to consumption of ultra-processed foods), exposure to chemicals, lack of physical activity and chronic stress, and “overmedicalization (excessive use of prescription drugs, such as antidepressants). The report calls for federal agencies to “close critical research gaps and guide efforts to better combat” these issues. It also says the MAHA Commission will develop and release a strategy in August (discussed below). The report expanded on the ideas initially outlined in the February EO and provided more details on Secretary Kennedy’s priorities to address chronic disease in children. There was some criticism of the report after its publication, with experts questioning some of the evidence and conclusions and pointing out significant errors and studies cited that did not exist, which indicated that artificial intelligence was likely used to help write the report. |
| May 23, 2025 | Administration ends NIH funding for several HIV vaccine research projects. – NIH notifies two grant recipients working on broadly neutralizing antibody research for HIV vaccines of the cancelation of their funding. The canceled grants supported early-stage vaccine development research that uses a different approach than other HIV vaccine candidates. Some other HIV vaccine candidates remain in the development pipeline and clinical trials continue, but the absence of this early-stage research could jeopardize the development of additional candidates going forward. |
| May 27, 2025 | HHS Secretary Kennedy announces CDC will no longer recommend COVID vaccines for healthy pregnant women and children. – In a video post on X, Secretary Kennedy announces “the COVID vaccine for healthy children and healthy pregnant women has been removed from the CDC recommended immunization schedule.” The announcement was a departure from the typical process for changing vaccine recommendations, which includes review and input from the Advisory Committee on Immunization Practices (ACIP) and a notification from the CDC Director. Initially, the implications of changing CDC guidance without ACIP input were unclear given that no-cost insurance coverage for vaccination is linked to ACIP and CDC recommendations. On May 30, CDC changed the language on its website for COVID-19 vaccines, removing its prior recommendation for pregnant women to be routinely vaccinated and stating that healthy children 6 months to 17 years old could be vaccinated in consultation with health care providers/parents – a recommendation known as “shared decision-making,” which would mean insurance would still have to cover such vaccinations. On July 7, a coalition of professional medical organizations filed a lawsuit against HHS over the new COVID-19 vaccine recommendations, saying the department did not follow federal procedures in making the change and also mislead the public on the issue (on January 6, 2026, a federal court confirmed these plaintiffs have standing to challenge HHS’s actions on the COVID-19 vaccine recommendations, allowing the case to proceed to arguments). On August 19, independent expert groups, including the AAP, issued their own recommendations for COVID vaccines in infants and young children in contrast with CDC’s new recommendations. On Aug 22, ACOG issued their own recommendations for pregnant patients. |
| June 9, 2025 | HHS Secretary Kennedy announces removal of all sitting members of ACIP. – In a post on X and a subsequent HHS press notice, Secretary Kennedy announces that all 17 sitting members of the CDC’s Advisory Committee on Immunization Practices (ACIP) are dismissed, to be replaced with new members selected by the Secretary. Kennedy says the move is “prioritizing the restoration of public trust above any specific pro- or anti-vaccine agenda.” The HHS Secretary does have the discretion to remove and nominate ACIP members, though no previous Secretary has dismissed all ACIP members at once. In a subsequent X post on June 11, Kennedy announces the nomination of eight new members to ACIP, several of whom have been critical of COVID-19 vaccines and have expressed concerns about harms caused by vaccinations more generally. In a later press release from September 15, HHS announces five more members to be appointed to ACIP, including several with a history of criticism of COVID-19 vaccine policies. |
| June 17, 2025 | FDA announces National Priority Vouchers for expedited regulatory review of new drugs that support “U.S. national interest.” – FDA announces a Commissioner’s National Priority Voucher (CNPV) program, which can be “redeemed by drug developers to participate in a novel priority program” that shortens regulatory review time from 10-12 months to 1-2 months. FDA says it will determine the availability of vouchers for companies that are aligned with the “national health priorities” of: addressing a health crisis in the U.S.; delivering more innovative cures for the American people; addressing unmet public health needs; and, increasing domestic drug manufacturing as a national security issue. On October 16, FDA announced the first nine CNPV recipients, and on November 6, announced six more recipients. The impact of this new priority voucher program on speeding drug approvals and onshoring drug manufacturing capacity is as yet unclear. In addition, there are several other existing priority review processes at FDA so adding another could strain FDA staff capacity at the same time there has been significant reductions in FDA’s staff and budget. These strains have already slowed FDA review times in general. |
| June 18, 2025 | FDA approves lenacapavir – a new HIV prevention drug. – FDA approves Gilead Sciences’ lenacapavir, a new injectable PrEP drug that has been shown to be highly effective at preventing HIV infection, and which requires just one dose every 6 months, making it the first ever twice-a-year drug option for HIV prevention. In September, CDC issued clinical guidance for use of injectable lenacapavir as PrEP, though that guidance did not include reference to transgender people, a group intentionally included in the clinical trials and at increased risk of HIV. FDA’s approval also precipitated a review by the World Health Organization (WHO) and on October 6, WHO pre-qualified lenacapavir for prevention of HIV. WHO pre-qualification can speed regulatory approval for the drug in many low- and middle-income countries with a high burden of HIV/AIDS and can also allow for global health mechanisms like the Global Fund to Fight AIDS, Tuberculosis and Malaria to procure the drug. |
| June 25-26, 2025 | The newly reconstituted ACIP makes recommendations and policy changes related to RSV and influenza vaccines, and designates new workgroups on hepatitis B, MMRV, and the childhood immunization schedule. – ACIP votes to recommend respiratory syncytial virus (RSV) injections for babies and RSV vaccine for people 50 and older, and a ban on the use of thimerosal in multi-dose influenza vaccine vials. ACIP also agrees to stand up three new workgroups that will review the U.S. childhood vaccination schedule, hepatitis B guidance, and combination MMRV vaccine. Subsequently, on July 3, CDC issued new RSV guidance that mirrored ACIP recommendations. On July 23, Secretary Kennedy enacted ACIP’s recommendation on thimerosal, rescinding federal recommendations for any influenza vaccines containing thimerosal (a change that only affects a very small percentage of the overall influenza vaccine market that is comprised of multidose vials). |
| July 1, 2025 | HHS alters program requirements and withholds funding from sex education and teen pregnancy prevention programs. – HHS notifies all Teen Pregnancy Prevention (TPP) program grantees and Personal Responsibility Education Program (PREP) grantees in 46 states and territories that their material must align with President Trump’s executive orders, including those that ban the promotion of gender inclusivity, risk losing federal funding. TPP is a national grant program that funds grantees to replicate, develop, test, and evaluate evidence-based approaches to prevent teen pregnancy, while PREP awards grants to state agencies to use evidence-based models in educating adolescents on both abstinence and contraception. In August, the Trump administration cancelled a $12.3 million PREP grant to California after state officials refused to revise curricula in compliance with the EOs. In September 2025, 16 states and D.C. sued HHS alleging that the new PREP grant conditions are unlawful, unconstitutional, and harmful to gender diverse youth. Similarly, a federal judge blocked the HHS policy changes for TPP in October 2025. |
| July 2, 2025 | CDC deactivates its emergency response for H5N1 influenza (bird flu) and limits tracking and reporting of data on bird flu infections in humans and animals. – CDC ends its emergency response for H5N1 bird flu in the U.S., which had been active since April 4, 2024. CDC reports the change is due to a decline in animal infections and no reports of human cases since February 2025. CDC also says data on the number of people tested for H5N1 will be reported only monthly, and no further data on infection rates in animals will be reported on the CDC website. Even so, reporting from states showed the number of H5N1 cases in birds, which had declined over the summer, began to increase again in fall 2025. However, much of the federal research and response efforts for H5N1 have been closed down or significantly limited following funding and staff cuts and a prolonged government shutdown. The limited federal tracking and reporting of H5N1 infections can slow identification of outbreaks and potentially slow response times. |
| July 9, 2025 | HHS Secretary Kennedy cancels a scheduled meeting of the U.S. Preventive Services Task Force (USPSTF). – Secretary Kennedy cancels a meeting of the USPSTF several days before it was scheduled to take place, with no reason given and no re-scheduled meeting date provided. Typically, the task force meets three times a year, though no meeting has yet occurred under Secretary Kennedy. USPSTF is responsible for reviewing and recommending preventive health services. USPSTF recommendations have implications for what services insurers must cover with no cost-sharing, under the Affordable Care Act (ACA). Such services can include screening tests, behavioral counseling, and medications that can prevent diseases and illness (other than vaccines, which are tied to ACIP recommendations). However, along with other parts of the ACA, USPSTF has faced court challenges. On June 27 (prior to Kennedy’s cancelation of the meeting), while the Supreme Court ruled the ACA requirement that insurers cover USPSTF-recommended services is indeed constitutional, it also found that the HHS Secretary has the power to add and remove USPSTF members at will, which underscores the possibility that Secretary Kennedy may choose to dismiss some or all of the existing USPSTF members and appoint new members (as Kennedy has done with ACIP), or simply not name any new members, and has the power to choose not to adopt USPSTF recommendations. In light of Kennedy’s cancellation and the Supreme Court ruling, 104 public health focused organizations called on Congress to “protect the integrity of the USPSTF” through legislative action. The subsequent USPSTF meeting was scheduled to occur in November but that was also canceled, with HHS citing the government shutdown as the reason. |
| July 31, 2025 | FDA announces new safety label requirement for opioid pain medications. – The FDA says will require safety labels on opioid medications so that users can better understand that risks of long-term opioid use. The updated labels should include a summary on the risk of addiction, misuse, and overdose, treatment guidance and the risk of higher doses, how to safely discontinue opioid use, drug interactions, digestive complications, and overdose reversal medications. Drug companies received notification letters and have 30 days to submit updated labels for review. |
| July 31, 2025 | HHS Secretary Kennedy swears in Susan Monarez as CDC Director. – In a statement welcoming the newly Senate-confirmed CDC Director, Secretary Kennedy says Monarez has “unimpeachable scientific credentials” and he has “full confidence in her ability to restore the CDC’s role as the most trusted authority in public health.” However, 28 days later (on August 27) the White House removed Monarez from her position at CDC. According to Kennedy, she was removed because he lost trust in her ability to serve as CDC Director and to implement the policies of the Trump Administration. According to Monarez, she was removed because she would not provide “blanket approval” for vaccine policy changes in advance and would not fire, as requested by Kennedy, CDC employees without cause. On August 28, Secretary Kennedy announced in a letter to CDC staff that Deputy Health and Human Services Secretary Jim O’Neill would serve as acting CDC Director. |
| August 1, 2025 | Newly announced CDC policy prevents outside professional medical and public health organizations from participating in working group meetings of ACIP. – Officials at HHS notify professional medical organizations such as the American Academy of Pediatrics (AAP), the American Medical Association (AMA), the American College of Obstetricians and Gynecologists (ACOG), and others that they will be excluded from joining ACIP working group discussions going forward. Professional groups representing medical doctors and other stakeholders in vaccine policies have long participated as non-voting members, including in ACIP working groups. Working groups are typically responsible for helping review available data about topics prior to ACIP meetings, and helping develop recommendation language for ACIP to vote on, as well as other activities in support of ACIP. While the outside groups can be present and can participate in full ACIP meetings, the new policy removes them from providing any input through working groups. |
| August 5, 2025 | HHS announces a “coordinated wind down” of $500 million in federal funding for mRNA vaccine research. – HHS announces that it will cancel and begin to wind down mRNA vaccine development activities funded through the Biomedical Advanced Research and Development Authority (BARDA). In total, HHS reports it is canceling 22 projects worth nearly $500 million because “these vaccines fail to protect effectively against upper respiratory infections like COVID and flu…Going forward, BARDA will focus on platforms with stronger safety records and transparent clinical and manufacturing data practices.” mRNA COVID-19 vaccines are effective in preventing severe illness and death from the disease, and mRNA vaccine technology has potential applications for other infectious diseases, as well as chronic diseases like cancer. The cancellation removes the bulk of U.S. federal funding for mRNA research, leaving questions about future progress by the U.S. in this area of vaccine technology. |
| August 15, 2025 | HHS reinstates the defunct Task Force on Safer Childhood Vaccines. – The original Task Force on Safer Childhood Vaccines, a federal panel created by Congress in 1986 “to improve the safety, quality, and oversight of vaccines” was disbanded in 1998, but HHS announces that the group will be re-instated at NIH with participation from officials at FDA, CDC, and other government agencies. The goal of the reconstituted Task Force will be “the development, promotion, and refinement of childhood vaccines that result in fewer and less serious adverse reactions than those vaccines currently on the market, and improvements in vaccine development, production, distribution, and adverse reaction reporting” to help increase federal oversight and investigation of vaccine injuries. The Task Force will come together to develop recommendations to be submitted to Congress within two years, with updates every two years after. Reinstatement of this panel has been a goal of anti-vaccine advocates for years, including the Children’s Health Defense, the anti-vaccine organization Secretary Kennedy founded, which supported a lawsuit earlier in 2025 against Kennedy that sought to require him to reconvene the Task Force. |
| August 27, 2025 | FDA approves COVID-19 vaccines for 2025-2026, while limiting scope of approval to certain ages and risk profiles. – FDA approves updated COVID-19 vaccines for 2025-2026, but also limited the approval to persons 65 and older and those between 18 and 64 with a health condition that puts them at higher risk for severe disease. Previously, the FDA had approved the use of vaccines for all ages (over 6 months) regardless of risk profile. |
| September 9, 2025 | MAHA Commission releases strategy to address childhood chronic disease. – A new MAHA Commission strategy document outlines actions the federal government is taking or plans to take to address childhood chronic disease in the U.S. These include “more than 120 initiatives” that together represent “the most ambitious national effort ever to confront childhood chronic disease,” and which outline a “blueprint for the entire government” to address chronic disease. Elements of the strategy include: changing federal science and research priorities, reforming dietary guidelines, changing nutrition and food regulations through reducing additives and ultra-processed foods, and improving effort to raise public awareness about chronic disease. The strategy highlights the risks of vaccine injuries, fluoride in drinking water, among many other areas. |
| September 18, 2025 | Secretary Kennedy renews the declaration of the national opioid crisis as a public health emergency. – In a declaration on an HHS website, Secretary Kennedy renews the declaration of the opioid crisis as a national public health emergency (PHE). The opioid crisis was initially declared a public health emergency in 2017; renewal is required every 90 days to continue the PHE. |
| September 19, 2025 | Secretary Kennedy announces that the FDA will launch a new review of mifepristone. – Secretary Kennedy announced that the FDA will undergo a review of the current Risk Evaluation and Mitigation Strategy (REMS) for mifepristone, due to new evidence including an April 2025 report from the Ethics and Public Policy Center (EPPC) which claims that mifepristone has a higher rate of adverse events than previously reported. This report has drawn criticism due to methodological flaws and lack of transparency regarding its data sources. |
| September 19, 2025 | ACIP makes several new recommendations related to MMRV and COVID-19 vaccines. – In its September 18-19 meeting, ACIP members vote on several new recommendations including to no longer recommend the combination MMRV (measles, mumps, rubella, and varicella) vaccine for children under the age of 4 and instead to recommend that children in this age group receive measles, mumps, and rubella (MMR) vaccine separately from the varicella vaccine (V). In addition, ACIP members vote to change what had been a universal COVID-19 vaccine recommendation (except for HHS’ recent change for healthy children and pregnant women) to “shared clinical decision-making”, including for those 65 and older, along with a recommendation for new language on risk-benefit for COVID-19 vaccinations. ACIP’s recommendations were adopted by CDC on October 6. While the separate MMR+V vaccines had been recommended as preferred by the CDC for many years, the combination MMRV provided an option for parents to reduce the number of injections their children receive. Now, insurers will no longer be required to cover this vaccine at no-cost. The new COVID-19 vaccine recommendations mean people of all age groups are now recommended to have an interaction with a health care provider (which could include a doctor, nurse, or pharmacist) to determine whether getting a COVID-19 vaccination is recommended for them. If that determination is made, insurers must cover the vaccine at no-cost, although it is possible that some consumers may face challenges in accessing providers in the first place or demonstrating that they have consulted with a medical provider seeking vaccination in some cases. |
| September 22, 2025 | President Trump and Secretary Kennedy announce new actions to address autism spectrum disorder in the U.S. – In a press conference and via an HHS press statement and Fact Sheet, President Trump and HHS Secretary announce several actions to address the issue of autism spectrum disorder (ASD) in the U.S. This includes FDA authorization for leucovorin, a treatment option for some children with autism, a regulatory change that will allow state Medicaid programs to newly cover leucovorin for the indication of ASD. President Trump and Secretary Kennedy also highlight what they say are risks of acetaminophen use during pregnancy and association with autism. The press release notes “HHS wants to encourage clinicians to exercise their best judgment in use of acetaminophen for fevers and pain in pregnancy by prescribing the lowest effective dose for the shortest duration when treatment is required.” In his remarks, President Trump also implicated childhood vaccines as a potential risk factor for autism, though no new evidence was presented and that link has already been repeatedly and conclusively ruled out. In a subsequent press statement on September 22, HHS announced FDA was initiating a labeling change for leucovorin, and a safety label change for acetaminophen to include information about the “potential risks of acetaminophen so patients can make a more informed decision.” Public health groups and experts criticized the conclusions linking acetaminophen use in pregnancy and autism, and expressed doubts about leucovorin as a treatment for autism. President Trump’s remarks also precipitated a lawsuit filed on October 28 in Texas against the maker of Tylenol. |
| September 30, 2025 | FDA approves a new generic mifepristone product. – The FDA approved Evita’s Solutions application for a generic version of mifepristone. The approval included a reminder that the generic mifepristone is subject to the same Risk Evaluation and Mitigation Strategy (REMS) as the brand-name. |
| September 30, 2025 | HHS awards $60 million in grants to support prevention of falls and related programs for older adults and those with disabilities. – Secretary Kennedy announced 59 new grants totaling $60 million is being awarded to states, territories, tribes, and local organizations supporting older adults and Americans with disabilities, including programs for “preventing falls among seniors, managing chronic conditions…and funding dementia-capable programs.” |
| October 10, 2025 | Trump Administration fires thousands of HHS employees, including hundreds at CDC, during federal government shutdown. – In the midst of a government shutdown and an ongoing federal funding impasse in Congress, the White House Office of Personnel and Management says over 4,000 federal workers are to be fired. At HHS, over a thousand workers are notified that they have lost their jobs, with most of those losses concentrated at CDC. Some of those job losses were reversed over the next few days, with HHS officials stating some notices were sent in error. Even so, as of October 14 it is estimated that about 600 CDC employees remain fired, including staff in areas such as injury prevention, health statistics, and Congressional relations. There is a question about whether such firings during a government shutdown are legal, and groups representing federal workers have filed lawsuits to halt these mass layoffs. |
| October 31, 2025 | FDA announces new restrictions on ingestible fluoride products for children. – FDA announces new enforcement actions “to restrict the sale of unapproved ingestible fluoride products for children” and sends letters to health care professionals warning about the risks associated with these products. The actions come after FDA conducted a review and published a scientific evaluation of these products. In the announcement. FDA says it will be developing a “fluoride research agenda” and “the first national oral health strategy” for the U.S. in partnership with NIH and other HHS agencies. |
| November 10, 2025 | FDA announces a warning label change on hormone replacement therapy (HRT) products for addressing symptoms of menopause. – In a press release, a fact sheet, and a live press event, FDA leaders announce that they will initiate the removal of broad “black box” warnings from HRT products for menopause. The FDA also announces approvals for two new drugs for menopausal symptoms. According to the FDA, women have been “under-utilizing approved therapies” since the “black box” warnings about risks associated with the drugs were placed on these products over 20 years ago. Labels will be rewritten with guidance saying that there are long-term health benefits if HRT is begun within 10 years of the onset of menopause. |
| November 19, 2025 | CDC changes language on its website to say a link between vaccines and autism cannot be ruled out. – A CDC website providing information to the public on Autism and Vaccines, is changed to include language saying “studies have not ruled out the possibility that infant vaccines cause autism.” The new site also discusses the “state of the evidence” on common childhood vaccines and supposed links to autism. The new language is a reversal from previous CDC statements saying “vaccines do not cause autism,” and contradicts the long established scientific consensus that there is no link between vaccines and autism. The new CDC webpage language has been criticized by professional medical organizations such as the American Medical Association and the American Academy of Pediatrics, as well as autism organizations such as Autism Speaks and the Autism Science Foundation. |
| November 21, 2025 | CDC staff ordered to end all monkey research programs, potentially affecting development of prevention tools for HIV and other infectious diseases. – According to reports, CDC staff are ordered to halt its monkey research program by the end of 2025. This program has helped develop HIV prevention tools such as pre-exposure prophylaxis (PrEP) and microbicides, as well supported prevention research for other infectious diseases. |
| November 28, 2025 | Internal FDA communication proposes stricter federal requirements for testing and approving vaccines. – According to reports, the head of FDA’s Center for Biologics Evaluation and Research (CBER), which is responsible for regulating vaccines, issues an email to staff proposing new, stricter federal requirements for vaccine testing, evidence, and approval. The email states that in the future FDA will “demand pre-market randomized trials assessing clinical endpoints for most new products” and that FDA “will not be granting marketing authorization to vaccines in pregnant women” without this kind of evidence. Newly developed pneumonia, influenza, and COVID-19 vaccines are specifically mentioned as vaccines that would be subject to these new requirements. The rationale given for this policy change is a new analysis of vaccine safety data indicating “COVID-19 vaccines have killed American children,” though no evidence to support that statement is provided in the email. |
| December 5, 2025 | ACIP votes to end recommendation that all newborns receive hepatitis B vaccine dose at birth On the second day of the Advisory Committee on Immunization Practices’ (ACIP) December 4-5 meeting, members vote to end a long-standing recommendation that all newborns in the U.S. receive a dose of hepatitis B vaccine. The committee now recommends parents of infants born to mothers who test negative for hepatitis B consult with their provider to help decide if and when their child should receive the first hepatitis B dose. ACIP continues to recommend that infants born to mothers who test positive for hepatitis B, or whose hepatitis B test status is unknown, receive the first hepatitis B vaccine dose at birth. A recommendation from ACIP becomes part of the official CDC immunization schedule once it is adopted by the CDC director. |
| December 30, 2025 | HHS ends certain requirements for state reporting of immunization data to the Centers for Medicare and Medicaid Services (CMS). A December 30 letter from the Centers for Medicare and Medicaid Services (CMS) informs state health officials that starting in 2026, states will no longer be required to report several measures related to immunization status to CMS. Specifically, CMS removes the following from its “Child and Adult Core Sets”: “Childhood Immunization Status”, “Immunizations for Adolescents”, “Prenatal Immunization Status: Under Age 21”; and “Prenatal Immunization Status: Age 21 and Older.” In addition, in its letter CMS informs state health officials it will “explore options to facilitate the development of new vaccine measures that capture information about whether parents and families were informed about vaccine choices, vaccine safety and side effects, and alternative vaccine schedules” and “how religious exemptions for vaccinations can be accounted for.” Data reported by states and included in the Child and Adult Core Sets are used by Medicaid and CHIP to monitor access to and quality of health care for their beneficiaries, so an absence of this data could make monitoring immunization coverage in this population more challenging. |
| January 5, 2026 | HHS announces changes to the federal childhood vaccination schedule that reduce the number of routinely recommended vaccines Health and Human Services (HHS) issues a memo implementing major changes to the government’s recommended vaccination schedule for children. Under the new guidelines, there are vaccines for 11 diseases recommended for all children, down from 17 diseases a year ago. In addition to COVID-19 (which HHS stopped recommending for all children back in October 2025), the new schedule no longer recommends routine vaccinations for five other diseases: rotavirus, COVID-19, influenza, hepatitis A, hepatitis B, and meningococcal. These vaccines have been moved from routine recommendation to “shared clinical decision making,” a process that is “individually based and informed by a decision process between the health care provider and the patient or parent/guardian.” The HPV vaccine remains recommended for routine vaccinations, though under the new guidelines HHS reduces the number of recommended doses of HPV drops from two or three (depending on age of initial vaccination) to one. Coverage for all of these immunizations should remain the same through public and private insurance mechanisms. On March 16, 2026, a federal judge issued a ruling that stayed changes to the vaccine schedule from being implemented, as the government did not follow required procedures. On April 29, HHS appealed the judge’s stay and court review continues. |
| February 3, 2026 | BARDA opens solicitations for a $100 million prize program for development of novel antivirals targeting dengue, West Nile, and other viruses. In a news release, HHS’ Biomedical Advanced Research and Development Authority (BARDA) announces it is opening solicitations for a share of a new $100 million SMART Antiviral prize intended to speed the development of “broad-spectrum, small-molecule antiviral therapies” targeting families of viruses that include dengue, Zika, West Nile, and Chikungunya. This first stage is designed to receive solicitations at the concept stage, with solicitations for further development stages anticipated in the future. |
| February 4, 2026 | Trump Administration instructs CDC to rescind $600 million in public health funds going to four Democratic-led states According to reports, the Office of Management and Budget ordered CDC to cut $600 million in funding that had been earmarked for state and local public health programs in California, Colorado, Illinois, and Minnesota. Most of the funding cuts affect programs focused on HIV and STD prevention, are are to be terminated because they “do not reflect agency priorities” according to an HHS spokesperson. On February 11, affected states filed a lawsuit in federal court against these cuts, and on February 12 a federal judge issued a temporary restraining order blocking the cuts from taking effect. |
| February 10, 2026 | FDA refuses to review Moderna’s license application for its investigational mRNA-based influenza vaccine Moderna announces it received a “Refusal to File” letter from FDA stating that the agency will not initiate a review of the company’s biological license application for its investigational mRNA-based seasonal influenza vaccine. According to FDA, the refusal is due to the company’s use of an inadequate comparison arm in its study. Moderna states the letter is “inconsistent with previous written communications” with FDA staff. On February 18, Moderna announced that FDA had reversed its decision, and will now review the application, following further discussions with the company. |
| February 18, 2026 | FDA to allow drug approvals with evidence from one clinical trial rather than two In an opinion article published in the New England Journal of Medicine, FDA leaders announce a new FDA policy that will make the default requirement for FDA approvals to be results from one clinical trial instead of the prior requirement of two clinical trials. The stated goal of the change is to accelerate the approval and availability of new medicines. |
| February 19, 2026 | CDC delays February ACIP meeting HHS/CDC announces the ACIP meeting previously scheduled for February 25-27 will be postponed. The postponement occurs amid an ongoing federal lawsuit filed by the American Academy of Pediatrics (AAP) and other medical groups that argues the recent revisions made by HHS to the federal child immunization schedule were arbitrary and violated administrative procedures and seeks to have the ACIP panel appointed by HHS Secretary Kennedy removed and replaced and its decisions overturned. On February 26, CDC announced the ACIP meeting had been rescheduled for March 18-19. On March 16, 2025, the judge ruled that 13 of 15 ACIP member appointments did in fact violate administrative procedures and their appointments are stayed along with any ACIP votes since the appointments were made. As a result, the planned March 18-19 ACIP meeting has been canceled. |
| February 23, 2026 | FDA launches new framework for speeding development and approval of therapies for rare diseases FDA announces draft guidance for drug developers that seek approval for targeted, individualized therapies. The new framework outlines new approaches to regulatory review and evidence requirements on the safety and efficacy for rare diseases, given that traditional randomized clinical trials may not be feasible for these conditions. |
| March 4, 2026 | HHS Postpones Third Straight Meeting of US Preventive Services Task Force (USPTF) USPTF, which makes recommendations on preventive health care services, has not met since March of 2026. Five of the 16 USPTF members’ terms have ended as of January 1 and have not been replaced. |