KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Several legislative proposals in Congress propose a $35 per month cap on what people with health insurance would have to pay out of pocket for insulin, a life-saving hormone taken regularly by many people with diabetes to maintain their health.
This analysis of insurance claims data finds that such a cap could provide financial relief to at least 1 out of 5 insulin users with different types of private health insurance.
Among people with private insurance who currently pay more than $35 per month for insulin on average, half would save at least $19 per month, and a quarter would save at least $42 per month. Savings are highest among people who buy their own insurance.
The report analyzes 2018 claims data from the Centers for Medicare and Medicaid Services EDGE data for the individual and small-group markets and the IBM Health Analytics MarketScan Commercial Claims and Encounters Database for the large-employer market. It is available through the KFF-Peterson Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.
Several legislative proposals in Congress propose a $35 per month cap on what people with health insurance would have to pay out of pocket for insulin, a life-saving hormone taken regularly by many people with diabetes to maintain their health.
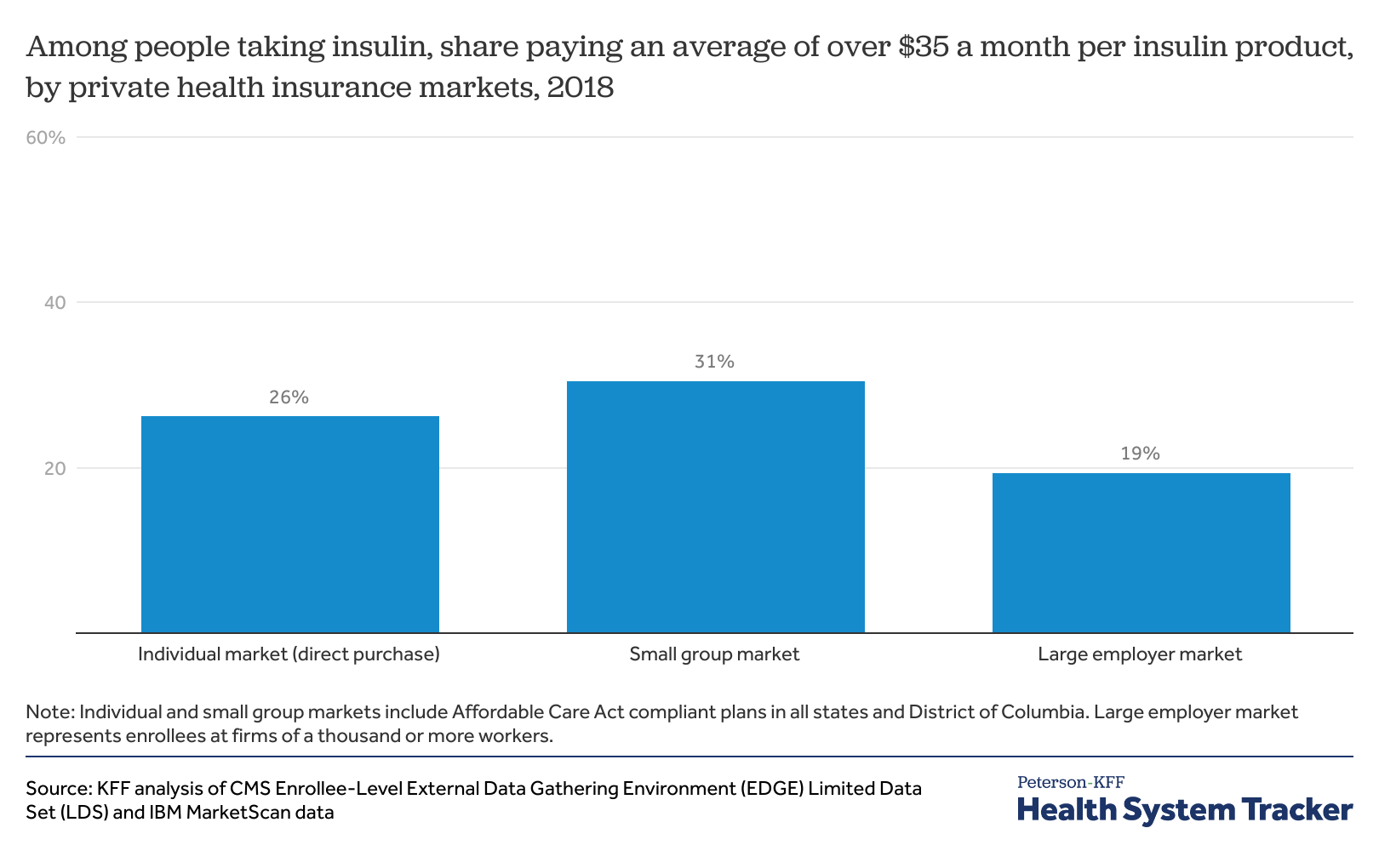
Such a cap could provide financial relief to at least 1 out of 5 insulin users with different types of private health insurance, a new KFF analysis of insurance claims data finds.
In the large employer market, 19% of people who take insulin spend an average of more than $35 per month ($420 annually) for insulin, the analysis shows. The shares are even higher for insulin users covered through the small group market (31%) and individual market (26%).
People in small group plans may face higher out-of-pocket costs for insulin because such coverage is generally less comprehensive than in large employer plans, and there is no reduced cost-sharing for low-income people as there is for individual market plans purchased through the Affordable Care Act’s marketplaces.
Among people with private insurance who currently pay more than $35 per month for insulin on average, half would save at least $19 per month, and a quarter would save at least $42 per month. Savings are highest among people who buy their own insurance.
The $35 per month cap on insulin out-of-pocket costs is the main provision in the Affordable Insulin Now Act, introduced in February 2022 by Sen. Raphael Warnock, and one of many drug-pricing provisions in the Build Back Better Act, which passed the House last year but stalled in the Senate.
The report analyzes 2018 claims data from the Centers for Medicare and Medicaid Services EDGE data for the individual and small-group markets and the IBM Health Analytics MarketScan Commercial Claims and Encounters Database for the large-employer market. It is available through the KFF-Peterson Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.
Medicaid managed care organizations (MCOs) deliver care to more than two-thirds of all Medicaid beneficiaries nationally. Medicaid MCOs (also referred to as managed care plans) may be in contact with enrollees as they provide care coordination and other member services (e.g., health education and promotion, call center support) and may conduct periodic outreach to promote appropriate use of care (e.g., to encourage prevention, wellness, and early intervention). Throughout the pandemic, states have worked with managed care plans to respond to changing public health conditions and new developments, including to promote the take-up of COVID-19 vaccinations.
Medicaid MCOs have seengrowth in their membership during the pandemic that tracksoverall Medicaid enrollment trends. Enrollment growth reflects downturns in the economy due to the pandemic and provisions in the Families First Coronavirus Response Act (FFCRA) that require states to ensure continuous enrollment for current Medicaid enrollees to access a temporary increase in the Medicaid match rate during the Public Health Emergency (PHE) period. It is expected that the PHE will be extended through at least mid-July 2022 since the Biden administration indicated it would give states 60 days-notice before the PHE is terminated or is allowed to expire (the current PHE is set to expire in mid-April). If the PHE ends in mid-July, the continuous enrollment requirement would expire at the beginning of August 2022.
Medicaid managed care plans can assist state Medicaid agencies in communicating with enrollees, conducting outreach and assistance, and ultimately, in improving coverage retention (including facilitating transitions to the Marketplace where appropriate). After the PHE ends, state Medicaid agencies will need to complete a large number of eligibility and enrollment tasks and actions, including processing renewals, redeterminations (based on changes in circumstance), and post-enrollment verifications. Current CMS guidance indicates states must initiate all renewals and other outstanding eligibility actions within 12 months after the PHE ends. Medicaid managed care plans have a financial interest in maintaining enrollment, which could also prevent disruptions in care for enrollees, including prescription drug benefits. Four for-profit parent firms that account for about 40% of Medicaid enrollment nationally (Anthem, Centene, Molina, and UnitedHealth Group) reported on Q4 2021 earnings calls that they expect modest enrollment declines in their Medicaid membership after the continuous enrollment requirement ends. However, these firms also indicated expecting to pick up/capture many individuals who transition from Medicaid through their other lines of business (i.e., the Affordable Care Act Marketplace and employer sponsored insurance (ESI)). Managed care plans have long cited lack of continuous eligibility, or churn, as a key challenge in ensuring access to care and for care continuity.
How can states engage MCOs to help individuals retain Medicaid coverage or transition to other coverage?
CMS released guidance for state Medicaid agencies on resuming normal operations including outlining strategies for working with managed care plans to promote continuity of coverage when the continuous enrollment requirement during the PHE ends. In the guidance, CMS notes that the federal Medicaid managed care marketing rules (42 CFR 438.104) do not prohibit plans from providing information and conducting general outreach on behalf of states. States must develop an “unwinding operational plan” to document their comprehensive plan to resume normal operations in their Medicaid and Children’s Health Insurance Program (CHIP) programs. CMS is encouraging states to gather input on their unwinding plans, including from managed care plans. Key strategies from the CMS guidance include:
Working with plans to obtain and update beneficiary contact information. States may direct MCOs to seek updated contact information from enrollees. Plans must confirm the accuracy of updates received from a third party (e.g., provider) with enrollees directly. MCOs may share this information with the state or may instruct or assist individuals in providing their updated contact information to the state. States may accept updated enrollee contact information from MCOs including mailing addresses, telephone numbers, and email addresses provided the state complies with certain beneficiary notice requirements (to confirm the accuracy of updated contact information) or the state receives a waiver of such requirements from CMS. While guidance expects plans to help in updating contact information, plans have historically cited difficulty reaching members and inaccurate member contact information as key barriers to engaging enrollees in care coordination activities. While state plans are evolving, as of January 2022, about half of states reported working with managed care plans to update beneficiary mailing addresses before the end of the PHE.
Sharing renewal files with MCOs to conduct outreach and provide support to individuals enrolled in Medicaid during their renewal period. States can provide monthly files to MCOs containing information about beneficiaries for whom the state is initiating the renewal process, or beneficiaries who have yet to submit renewal forms or other documentation and are at risk of losing coverage, to enable plans to conduct outreach and provide assistance with the renewal process. Prior to sharing information with managed care plans (e.g., renewal files), states may need to identify and address possible systems or operational challenges, including to ensure data accuracy.
Enabling MCOs to conduct outreach to individuals who have recently lost coverage for procedural reasons. States can provide MCOs monthly termination files to enable plans to conduct outreach to individuals terminated from Medicaid for procedural reasons (e.g., not returning renewal forms timely). CMS notes states may need to expedite review of plan outreach messaging or may want to consider developing standard language to be used by Medicaid managed care plans to ensure compliance with federal marketing requirements as well as any state-specific laws or contract requirements that may apply. Within two months or less after Medicaid coverage loss, managed care contracts must provide for automatic re-enrollment into an enrollee’s original plan. However, during the PHE unwinding period, CMS will approve state waivers to extend this automatic re-enrollment period up to 120 days.
Permitting plans to assist individuals to transition to and enroll in ACA Marketplace coverage if ineligible for Medicaid or CHIP. States may encourage MCOs that also offer a Qualified Health Plan (QHP) in the ACA Marketplace to share information with their own enrollees who have been determined ineligible for Medicaid to assist in the transfer of individuals to Marketplace coverage (which has higher income eligibility thresholds than Medicaid). To avoid gaps in coverage, managed care plans may reach out to individuals beforethey lose coverage to allow them to apply for Marketplace coverage in advance. CMS notes that federal Medicaid managed care marketing rules (and Exchange regulations) do not prohibit Medicaid managed care plans that offer a QHP from providing information about the QHP to enrollees who could potentially enroll in the QHP due to loss of eligibility; however, plans must comply with state-specific laws and/or contract requirements that may prohibit this activity.
In addition to strategies identified in the CMS guidance, Medicaid managed care plans may also consider adding staff to help manage the unwinding process. Additional staff could work proactively to identify members at-risk for disruptions in care and disenrollment (e.g., individuals with limited English proficiency, people with disabilities). Managed care plans can also work in partnership with providers (including community health centers) and community-based organizations to further bolster efforts to reach and assist members to ensure coverage retention or transitions to Marketplace coverage.
What to watch?
Understanding how managed care plans are involved in the development of state unwinding operational plans and what is included in the operational plans themselves will be key areas to watch. When continuous enrollment requirement ends, states will begin processing renewals and redeterminations and millions of people could lose coverage if they are no longer eligible or face administrative barriers during the process despite remaining eligible. The significant volume of work that states face will place a heavy burden on eligibility and enrollment staff and could contribute to coverage loss related to procedural errors. Medicaid managed care plans may be well positioned to assist states in conducting outreach and providing support to enrollees who will need to navigate the renewals or redeterminations.
As mid-April approaches, additional information about the timing of the end of the PHE may become available. The Biden administration indicated it would give states 60 days-notice before the PHE is terminated or is allowed to expire. The current PHE is set to expire in mid-April. On February 8, 2022, the Medicaid Health Plans of America (MHPA), a national trade association representing more than 130 MCOs, sent a letter to Congressional leaders asking Congress to provide at least 120-days lead time before the end of the continuous enrollment requirement. States are developing unwinding operational plans but it is not clear that these plans will be made publicly available. The policies adopted and the implementation of strategies to promote continuity of coverage will vary across states and plans and will have major implications for Medicaid and broader coverage as the PHE unwinds.
President Biden recently signed the reauthorization of the Violence Against Women Act (VAWA). The new VAWA includes changes that could help strengthen and expand the availability of health care services for victims, including better oversight of programs for survivors of sexual assault and a new public website with information about the availability of forensic nurse examiners.
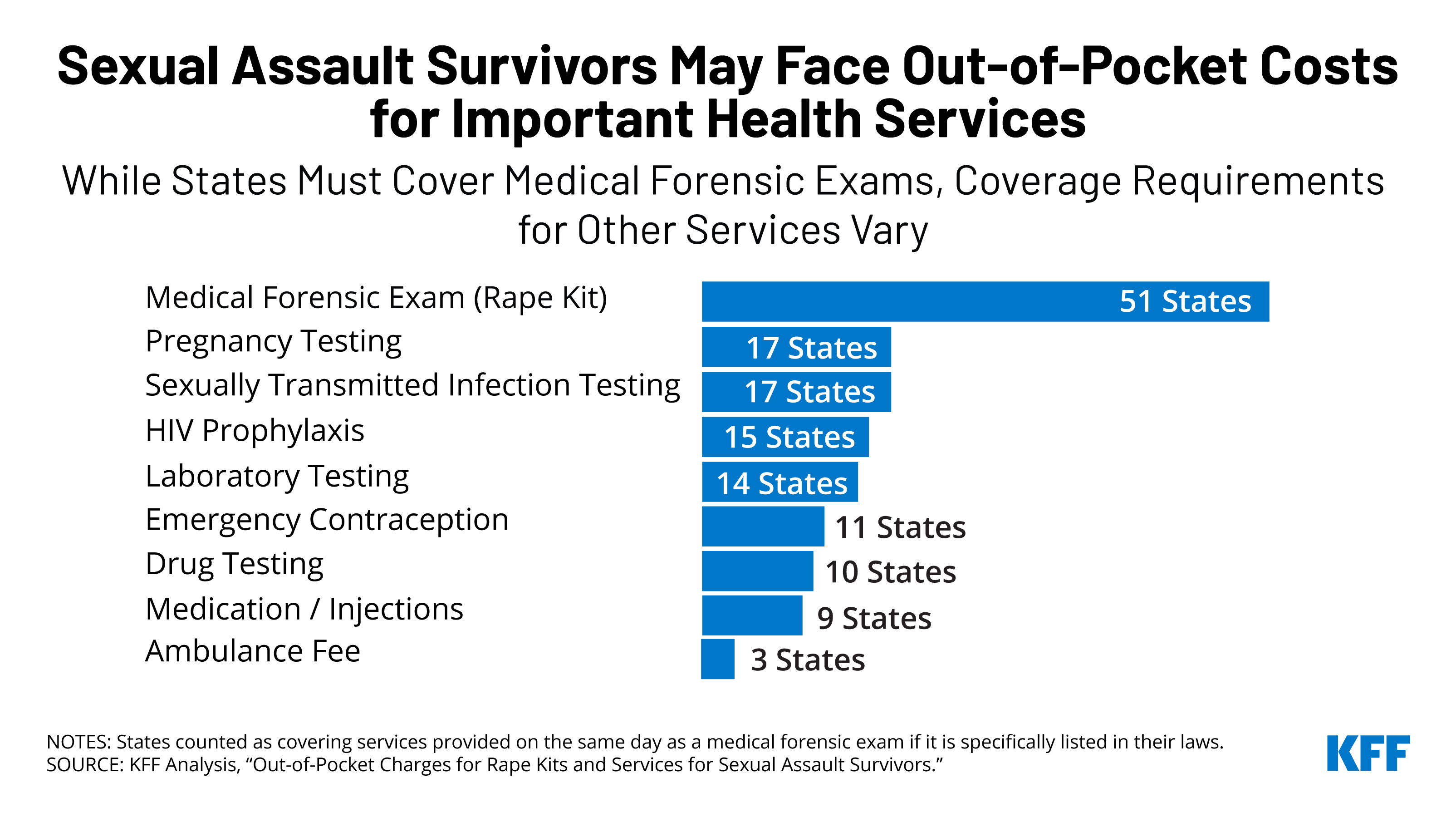
To qualify for federal grants to address violence against women, states are required to ensure that rape kits, or Medical Forensic Exams (MFE), are provided at no cost to survivors. However, there are often gaps in coverage for health care services that are outside of the MFE, like sexually transmitted infection testing, emergency contraception, or services for injuries incurred during sexual assault (such as stitches). Coverage policies for these services vary by state and are not necessarily guaranteed to be provided without cost-sharing. While the 2022 VAWA makes many changes, it does not specifically address out-of-pocket charges that many can face after a sexual assault.
In the United States, more than one in three women experience sexual violence in their lifetime. Despite the intent of Violence Against Women Act (VAWA) to protect survivors from out-of-pocket spending stemming from rape kit collection services also known as a medical forensic exam (MFE), many women face health care bills because they seek those critical services.
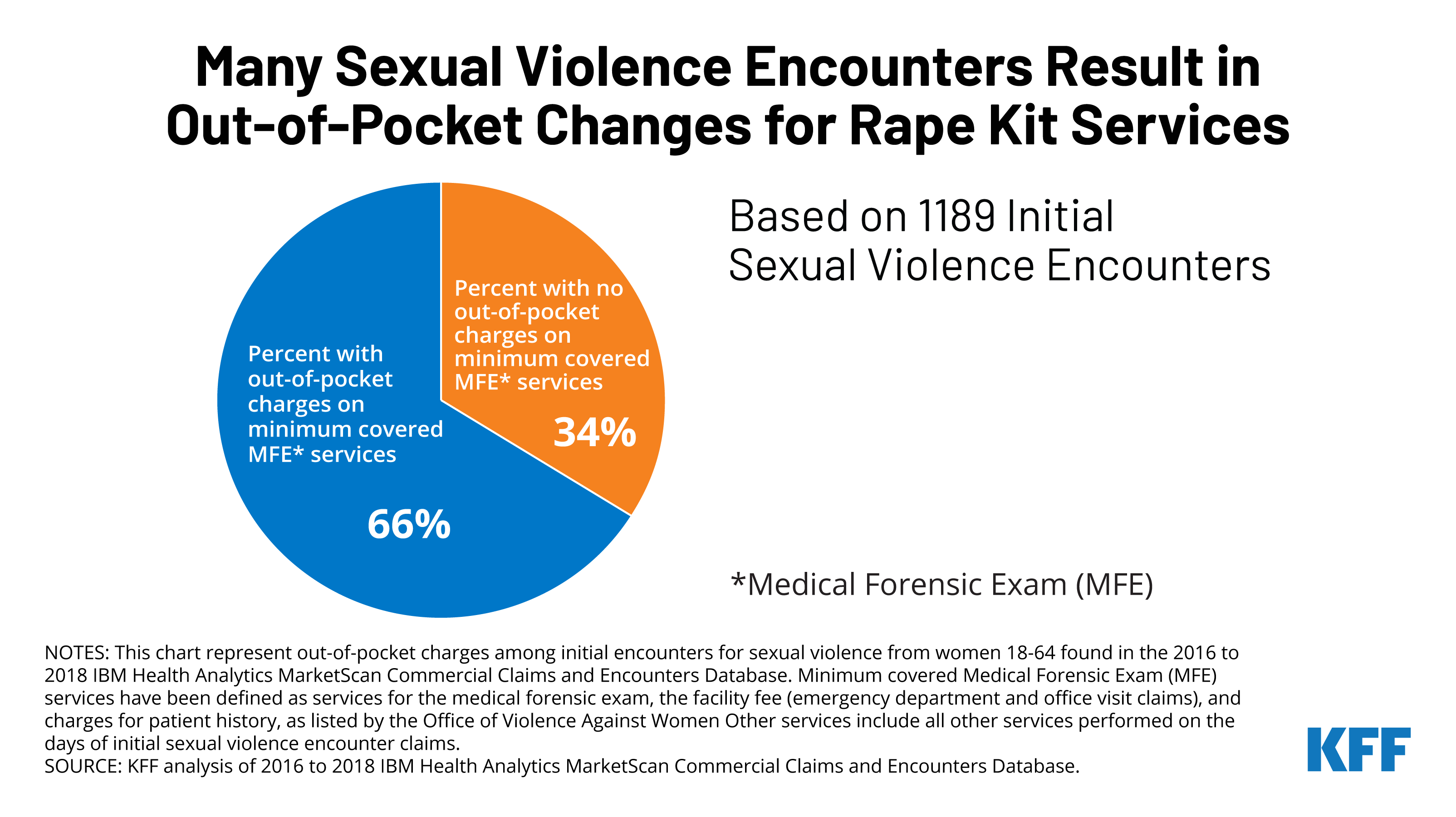
A new KFF analysis of a sample of private insurance claims from large employers finds that two-thirds (66%) of insured women who received a rape kit after a sexual assault faced out-of-pocket charges for these services, spending an average of $347 out of pocket.
This new analysis also reviews the federal and state policies that contribute to the gaps in coverage for these women, despite the intention of the VAWA to make no-cost rape kits accessible to all survivors.
President Biden recently signed the newly reauthorized VAWA, which does not specifically address the issue of out-of-pocket charges that many face for minimum covered services of the MFE. The reauthorization could help strengthen and expand the availability of health care services for victims, including better oversight and transparency regarding programming for survivors of sexual assault and a new public website with information about the availability of forensic nurse examiners.
Sexual violence is a public health concern that affects every community and often has lasting impacts on health and well-being.
While the intent of the Violence Against Women Act (VAWA) is to guarantee full coverage for rape kits or forensic exam services to survivors of sexual violence, some people are still charged for rape kit services. There are several reasons that that could be happening:
The exam is conducted by an individual who the state does not recognize as a provider of covered Medical Forensic Exams (MFEs). These are typically provided by Sexual Assault Nurse Examiners (SANEs).
Hospitals’ billing services may not know that the services should not be charged to the victim and send a bill to them for services provided.
Finding a place to get a rape kit from a provider specially trained in MFEs can be difficult in some places. Only a fraction of hospitals in the US have a trained forensic examiner such as a SANE. This makes it especially difficult to get an exam from a trained provider in rural communities. In addition, there is no government sanctioned national database of SANE providers making it difficult for victims who do not interact with law enforcement or a rape crisis center to know where to go.
The scope of services required to be performed along with the forensic exam and evidence collection vary by state. Many services that are considered to be the standard of care, outside of the forensic exam and evidence collection process and performed by a provider at the same time or on the same day as a forensic exam (such as medication, x-rays or MRIs), are not subject to the VAWA coverage requirement.
KFF analysis of a sample of private insurance claims from large employers found that two-thirds (66%) of privately-insured women who likely presented for a rape kit after a sexual assault were charged out-of-pocket costs for some services which are typically included in the minimum standard rape kit services as defined by the US Department of Justice. Women who were charged cost-sharing for services often included in the MFE spent an average of $347 dollars out of pocket.
Despite the intention of the VAWA to provide no-cost rape kits to all survivors of sexual violence, some survivors still face out-of-pocket charges for minimum standard rape kit services as well as other medical care that takes place following a sexual assault.
Introduction
Sexual violence impacts every community and affects people of all genders, sexual orientations, and ages, and often has lasting impacts on health and well-being. Sexual violence has been classified as a serious public health issue by the World Health Organization (WHO), and the Centers for Disease Control and Prevention (CDC). In the US, more than 1 in 3 women and 1 in 4 men experience sexual violence in their lifetimes. The Violence Against Women Act (VAWA) provides federal funding and guidance for programs to serve victims of sexual violence in the US. Despite the availability of federal and state funding and programs designed to support victims of sexual violence, many women face sizable out-of-pocket expenses for services they receive from a health care provider after a sexual assault.1 This brief examines the policies that impact coverage of health care services for survivors of sexual assault and identifies gaps in those programs and coverage for their care, particularly for women with private health insurance.
Overview of Federal and State Programs to Support Victims of Sexual Violence
The Violence Against Women Act (VAWA) is the major federal legislation that provides funding and guidance for programs that aid victims of sexual violence. VAWA’s scope is broad, covering domestic violence, sexual harassment, stalking, and sexual assault. VAWA provides grants to states, local governments, and other organizations to establish their own violence-related programs and protocols. While the focus of public policies on sexual assault tends to be prosecution of perpetrators and the collection of evidence, provisions in VAWA also address health care coverage and costs.
Violence Against Women Act (VAWA): First passed in 1994, VAWA authorizes federal funds to be used for services to aide individuals who are victims of sexual violence. VAWA requires states or another entity to provide no-cost rape kits and enforces and funds this requirement.
Services, Training, Officers, Prosecutors (STOP) grants in each state. These grants are VAWA formula grants which support state and territory efforts to develop and strengthen law enforcement and prosecution strategies to address violence against women and improve victim services, such as paying for rape kits (or Medical Forensic Exams). According to federal law, in order to qualify for these grants states must “incur the full out-of-pocket cost of forensic medical exams” by providing or arranging for MFEs free of charge to victims of assault.
Crime Victim’s Compensation Funds (CVCs): These state-level funds are established to reimburse victims for expenses related to crimes, which can include out-of-pocket expenses related to evidence collection and treatment. However, CVCs are typically the payer of last resort, and in most states, to be able to access the funds, the victim must report the crime to law enforcement within 72 hours of occurrence. These policies limit the availability of these funds to many victims of sexual violence.
What is a Rape Kit? It depends on where you live and where you go
Medical Forensic Exams (MFEs), Physical Evidence and Recovery Kits (PERKs), and Sexual Assault Forensic Exams (SAFEs) are all colloquially known as “rape kits.” In this brief, we use the terms MFE and rape kit interchangeably.
MFEs are used to collect evidence related to the sexual assault. The Office of Violence Against Women specifies that at a minimum, the standard medical forensic exam should include:
gathering information from the patient for the forensic medical history
head-to-toe examination of the patient
documentation of biological and physical findings
collection of evidence from the patient
use of the exam space, such as an emergency room
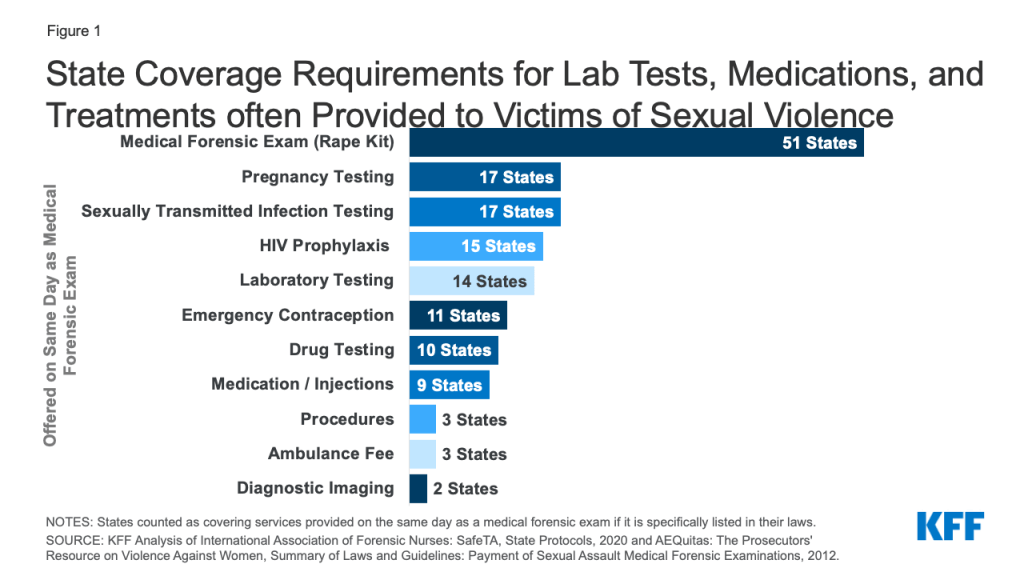
Beyond the minimum forensic exam, the Office of Violence Against Women states that “the inclusion of additional procedures (e.g., testing for sexually transmitted diseases) may be determined by the state in accordance with its current laws, policies, and practices.” Within these broad federal guidelines, states can define what is included in a rape kit which results in variation across the country. Although states are required to ensure that rape kits are provided at no-cost to survivors in order to qualify for STOP grants, there are often gaps in coverage for health care services that are outside of the MFE, like sexually transmitted infection (STI) testing, emergency contraception, or services for injuries incurred during sexual assault (such as stitches). Coverage policies for these services vary by state and are not necessarily guaranteed to be provided without cost-sharing.
The scope of coverage required by states is particularly unclear when it comes to lab testing, drug testing, pregnancy testing, and STI testing. For example, although MFEs typically include urinalysis, some states choose to specify that they cover these services as part of the kit, but many others do not. Because the services included in a rape kit are not explicitly defined in statute or by federal regulation, it is unclear whether states consider these services a part of the forensic exam (which they are required to cover in full per VAWA) or if they mandate them through separate state laws.
Furthermore, 17 states cap how much the state will spend on services per victim. For example, Georgia, Nevada, and Pennsylvania all limit spending to $1,000 per victim. Some states cap costs for the MFE, some states cap the costs paid to the provider but make clear that the patient will not have to pick up the extra costs, and some states specify ceilings for other services, such as medication or laboratory testing. Medical costs outside of the MFE may expose survivors to cost sharing following sexual assault in any state as VAWA does not explicitly mandate coverage for these services. Variation in state requirements contributes to differences in out-of-pocket costs between states.
Figure 1: State Coverage Requirements for Lab Tests, Medications, and Treatments often Provided to Victims of Sexual Violence
Access to Sexual Assault Nurse Examiners & Guaranteed No-Cost Rape Kits Varies by State and Exam Site
Sexual Assault Nurse Examiners (SANEs) or Sexual Assault Forensic Examiners (SAFEs), which are used interchangeably in this paper, are clinicians who are specially trained in provision of rape kits. Forensic exam nurses often get certified as SANEs after some time of providing rape kits — during this time, as they have already gone through the training, they would still be included under the VAWA coverage requirements. VAWA’s no-cost coverage only applies to rape exams that states confirm meet the criteria outlined in VAWA, effectively exams that are often conducted by SANEs. However, SANEs and other specially trained examiners are not available in every hospital and it is difficult to know where to find a hospital that staffs one of these examiners. The only national database of SANE nurse locations was created in December of 2020 and has identified between 800 and 900 SANE programs in the U.S., whereas there are more than 6,000 hospitals nationally. A Government Accountability Office (GAO) report found that access to SANE options and transportation varied across states. For example, the GAO found that survivors in some rural areas would need to travel two hours to find a hospital staffed by a SANE.
While some states, like Colorado and Massachusetts, publicly post a list of SANE locations, most states do not. As it stands, in order to find a trained examiner most survivors would need to call their local police department or a sexual assault service provider, like a hotline or local crisis center, or obtain access to the national database mentioned above. In some cases, the examiner may travel to the location of the patient to conduct the exam — in this case, it is the responsibility of the billing department to recognize the exam as covered, even if the location does not usually provide rape kits.
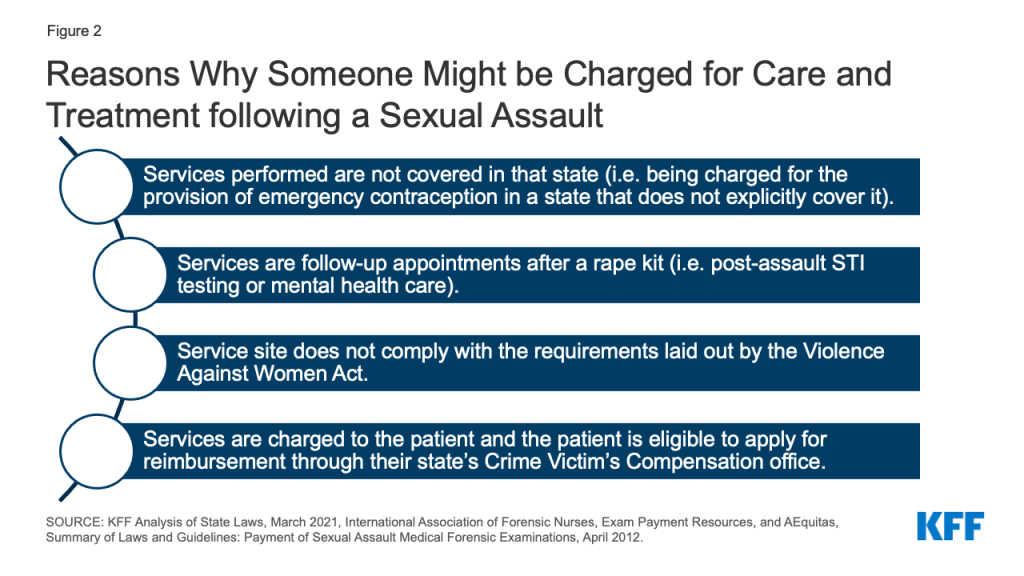
Although VAWA is widely believed to guarantee the provision of rape kits without cost-sharing for all, there are many gaps which may leave a survivor subject to out-of-pocket costs. These include a limited availability of rape kits, lack of clarity on coverage policies for non-SANE providers offering rape kits, as well as varying definitions of what services are included in rape kits between states, and unclear processes if a hospital or an insurer charges out of pocket costs (Figure 2).
Figure 2: Reasons Why Someone Might be Charged for Care and Treatment following a Sexual Assault
Out-of-Pocket Costs for Rape Kit Services Under Private Insurance
According to a Department of Justice guide on STOP grant funding, states can require or ask victims to submit charges for exams to their personal insurance providers, but they must ensure that victims are not billed any costs, such as co-payments or deductibles, for the services that constitute the MFE. We analyzed a sample of private insurance medical claims from the 2016 to 2018 IBM Health Analytics MarketScan Commercial Claims and Encounters Database, which contains claims information provided by large employer plans to examine out of pocket spending on typical rape kit services delivered in an outpatient hospital or emergency room setting. For more information see the Methods section.
Our analysis included identified episodes in which an adult women received a sexual violence diagnosis and either a STI test or exam procedure code typical of a rape kit (such as tissue examination or salvia swab), at an outpatient clinic, emergency room or urgent care clinic.
Eighty-three percent of women presenting under these circumstances and receiving an initial sexual violence diagnosis incurred out-of-pocket costs. On average, women facing out-of-pocket expenses in one of these cases faced $466 in cost-sharing, with half of women spending more than $226 dollars for all outpatient services.
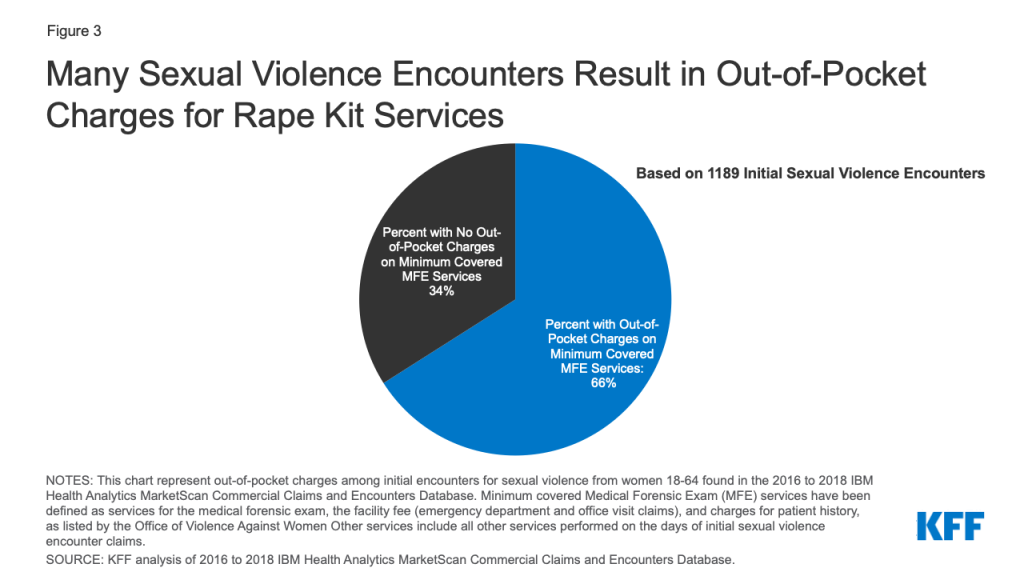
We then classified the different procedures that were billed as part of these encounters and identified a set of procedures that are often included as part of an MFEs: evaluation and management services or observation, patient history, swabs for DNA testing, and examinations of skin, hair, and nails. Two-thirds (66%) of survivors in this sample were charged out of pocket for at least one of these services (Figure 3). For example, among survivors who had a claim for emergency evaluation and management, roughly three quarters (74%) incurred out-of-pocket costs for these services. Among women facing cost-sharing for services often included in the MFE (an emergency room evaluation and management charge, an exam, patient history, pregnancy or STI test), victims with cost-sharing spent an average of $347 dollars, with half of women spending more than $200.
Figure 3: Many Sexual Violence Encounters Result in Out-of-Pocket Charges for Rape Kit Services
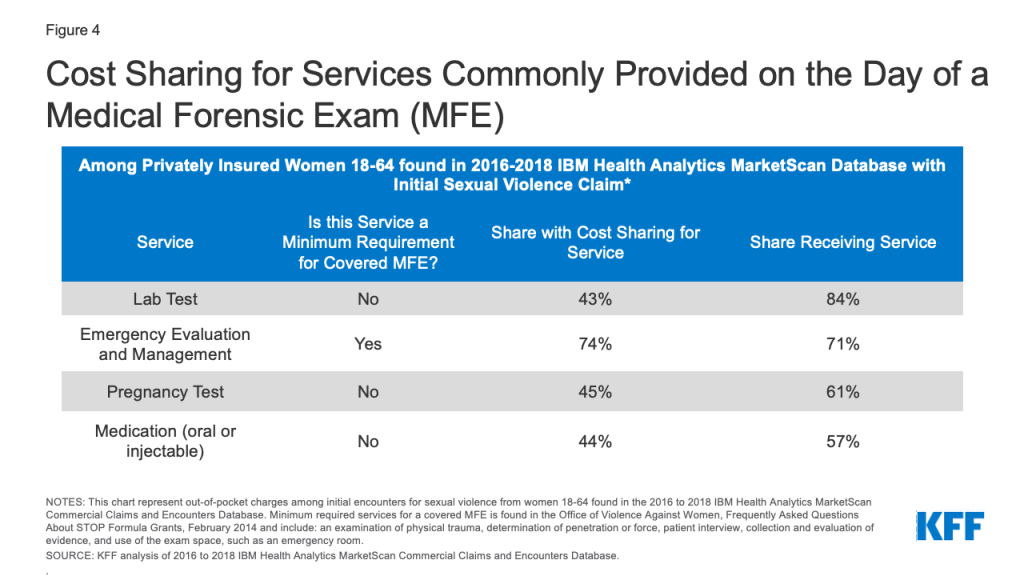
Many survivors also incurred cost sharing for a variety of services outside of the minimum covered services. While these services are not necessarily subject to the VAWA requirement for no-cost coverage of evidence collection, they are important components of care after a sexual assault for many survivors. For example, the majority of survivors had lab tests, pregnancy tests, and oral or injected medications such as antibiotics (Figure 4). Nearly half of all patients were charged out-of-pocket costs for these services. Other notable services, which were less frequently provided to survivors, also incurred out of pocket charges. This includes half (52%) of encounters that used an ambulance and almost half (47%) of those who had drug tests (data not shown). This analysis is consistent with previous research which also found that many patients were charged cost-sharing on days that they received rape kits.
Figure 4: Cost Sharing for Services Commonly Provided on the Day of a Medical Forensic Exam (MFE)
These data illustrate that many survivors of sexual violence are faced with charges for health services typically considered standard care after sexual violence but not necessarily directly relevant to obtaining evidence for law enforcement.
For uninsured survivors, the costs for the MFE would go directly to the state agency paying for the evidence collection, but survivors could still be charged for services that are outside of the MFE. Out-of-pocket charges for these services could, in theory, be submitted for reimbursement through the survivor’s state Crime Victim’s Compensation (CVC) office.
Looking Forward
Sexual violence survivors often face an array of short- and long-term health needs. Provisions in the VAWA were intended to eliminate cost barriers for victims of sexual assault to obtain forensic exams following an assault. This analysis on the immediate health charges experienced by people following an incident of sexual violence finds that in a large sample of medical claims among adult women who are insured and who are provided with a rape kit following a sexual assault, most faced out-of-pocket costs for this care. While provisions in VAWA were intended to prevent out-of-pocket charges for this care, many survivors are still faced with charges.
Victims of sexual assault in all states should not have to pay any out of pocket costs for MFE services. However, our analysis finds that some women are being charged for these services. Whether they are insured or uninsured, many survivors would likely not have or be able to get the information they need to navigate this complex system and obtain funds to cover their out-of-pocket medical and health costs following a sexual assault. They would also have to know that their MFE could be charged to their insurance first, that coverage of costs outside of evidence collection depends on their state’s policies, and that their state’s CVC might be required to cover their remaining costs.
Existing gaps in VAWA can result in survivors facing cost-sharing or barriers to access when victims seek services. These include the overall lack of SANEs and other trained providers in many hospitals, variation between states in what services they require to be covered in a rape kit, and variation in rules and processes for accessing CVCs.
The newly reauthorized VAWA, recently signed by President Biden, the original sponsor of VAWA in 1993, will likely address some of these gaps. For example, the law supports the creation of the first government-sanctioned database that would identify where SANEs are located to increase the likelihood that a victim of sexual violence obtains an exam and receives care that protects them from out-of-pocket charges. However, the new law will not necessarily prevent out-of-pocket charges for all health services needed following an assault.
Some have proposed other options to address these gaps outside of the VAWA legislative vehicle. The Survivor’s Access to Supportive Care Act (SASCA), reintroduced to Congress in 2021, aims to increase access to and availability of SANEs and would require the Office of the Inspector General to issue a report concerning hospital compliance about access to and reimbursements for MFEs.
Despite the protections and funding that VAWA offers to support victims of sexual violence, some people continue to incur out-of-pocket spending after a sexual assault, presenting another barrier to care for those who have just experienced trauma.
Appendix 1: State Requirements for Coverage of Services in Medical Forensic Exams
Appendix 2: Methods for analysis of out-of-pocket costs in claims from IBM Marketscan database
We analyzed a sample of medical claims obtained from the 2016 to 2018 IBM Health Analytics MarketScan Commercial Claims and Encounters Database, which contains claims information provided by large employer plans. We only included claims for women between the ages of 18 and 64.
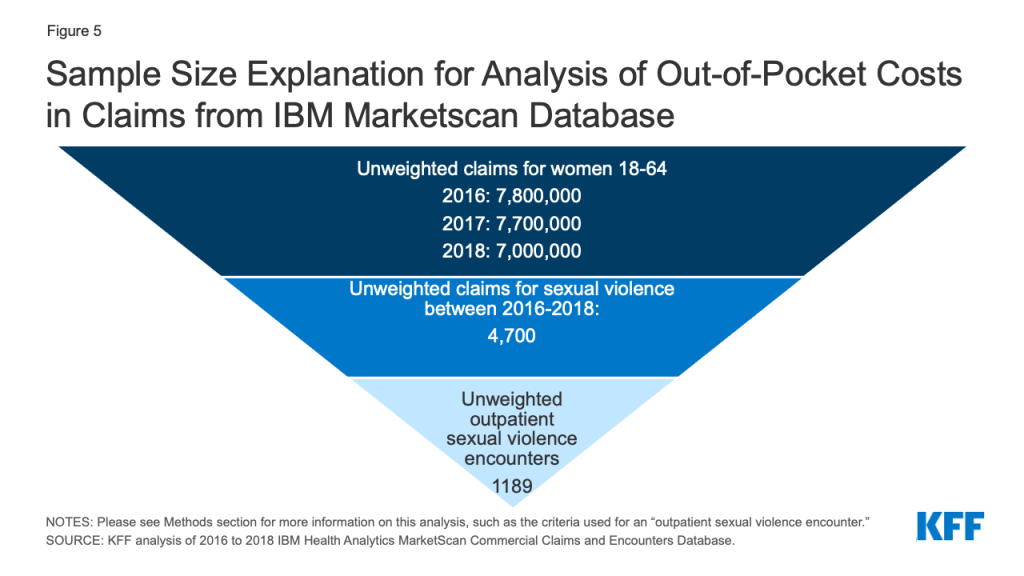
We further limited this analysis to women with claims for sexual violence (Figure 5). Sexual violence claims were defined as services in which an ICD-10 diagnosis code of T7421XA (Adult sexual abuse, confirmed, initial encounter), T7621XA (Adult sexual abuse, suspected, initial encounter) or Z0441 (Encounter for examination and observation following alleged adult rape) was assigned to the record. This method does not include services rendered to women who received a diagnosis of sexual exploitation, or received services to treat sexual violence after the initial encounter or in which another diagnosis was used on the claim. In total, over 4,700 unweighted enrollees had at least one claim of sexual violence over the three-year period.
Sexual Violence ICD-10 Diagnosis Codes
ICD-10 Diagnosis
Description
Z0441
Encounter for examination and observation following alleged adult rape
TZ421XA
Adult sexual abuse, confirmed, initial encounter
T7621XA
Adult sexual abuse, suspected, initial encounter
Of the 4,700 unweighted enrollees that had at least one claim of sexual violence over the three-year period, these claims were further limited to those submitted for outpatient care, meaning that inpatient services are not included or the cost of any retail prescription drugs they received after their visit. Claims were aggregated into an episode (‘outpatient days’), so that cost-sharing is considered spending that occurred on consecutive days in which a women has an sexual violence diagnosis and an STI or clinical exam.. We only considered cost-sharing that occurred during the initial encounter. Any cost-sharing on follow-up physician office visits were not included. We used a conservative denominator, including only days in which we expected a rape kit should have been administered: to do so we calculated days in which the survivor presented at an urgent care clinic or hospital (stdplac = 19, 22 or 23) and received both a sexual violence diagnosis and at least one STI test or exam. By doing so, we were attempting to exclude women who were receiving an initial sexual violence diagnosis weeks or years after the crime had been committed. We were unable to capture other locations where MFEs might be offered, like domestic violence safe houses or rape crisis centers.
In total there were 1189 unweighted sexual violence encounter outpatient days that met these criteria. Many of these outpatient days included claims with other diagnoses including depression screenings, treatments for physical violence or infection. In this analysis, we present cost-sharing for a limited set of services independent of these additional diagnoses. We looked at CPT codes related to pregnancy testing, STI testing, lab testing, drug testing, vaccines, medication (oral and injections), infusions, emergency department visits, patient history, office visits, diagnostic imaging, ambulance use, psychology use, contraception, pap smears, pregnancy care, procedures performed, physical therapy, and the MFE itself.
Figure 5: Sample Size Explanation for Analysis of Out-of-Pocket Costs in Claims from IBM Marketscan Database
Weights were applied to match counts in the Current Population Survey for enrollees at firms of a thousand or more workers by sex, age, and state. Weights were trimmed at eight times the interquartile range. On average 23% of women in large group plans are represented in the dataset.
This dataset does not include cases in which a person receives a rape kit but no claims are submitted to the insurer. Therefore, this data is not well suited for calculating prevalence of sexual violence, as spending is limited to women who received services, a diagnosis indicating sexual violence and the plan received the claim. This study attempts to discuss the cost-sharing faced by survivors presenting in a limited set of circumstances and not the financial burden of sexual violence overall. Cost-sharing includes the spending a woman faces from copays, coinsurances and deductibles.
The state policy tracking in shown in Appendix Table 1 was collected between June 2021 and December 2021. This data may change over time as fluctuations in state funds often impact what services states are able to cover.
The Department of Justice (DOJ) defines rape legally as the penetration, no matter how slight, of the vagina or anus with any body part or object, or oral penetration by a sex organ of another person, without the consent of the victim. Nearly 1 in 5 women in the United States have experienced attempted or completed rape during their lifetimes. In this paper, rape and sexual assault are used interchangeably, although sexual assault is an umbrella term that also includes attempted rape, unwanted sexual touching, and forcing the victim to perform sexual acts. The reason these terms are used interchangeably in this paper is that rape kits and associated services may be needed even in cases outside of the scope of the DOJ definition of rape.
↩︎
The Families First Coronavirus Response Act (FFCRA), enacted at the beginning of the coronavirus pandemic, requires states to provide continuous enrollment to Medicaid enrollees until the end of the month in which the public health emergency (PHE) ends in order to receive enhanced federal funding. During this time, states generally cannot disenroll people from Medicaid, which has prevented coverage loss and churn (moving off and then back on to coverage) among enrollees during pandemic. The PHE is currently in effect through mid-April 2022 and the Biden administration has said it will give states 60 days’ notice before the PHE ends. Since that notice was not issued in February 2022, it is expected the PHE will be extended again, although there is uncertainty over how long the extension will last.
Once states resume redeterminations and disenrollments at the end of the PHE, Medicaid enrollees who moved within a state during the pandemic but are still eligible for coverage are at increased risk of being disenrolled if their contact information is out of date. Many state Medicaid programs are heavily reliant on the mail for communicating with enrollees about renewals and redeterminations, including requests for information and documentation. States can disenroll individuals who fail to respond to these requests. We analyzed federal survey data for 2020 and found:
Roughly 1 in 10 Medicaid enrollees (9%) moved in-state in 2020. A much smaller share, just 1%, moved to a different state in the U.S. Individuals that move within the same state may continue to be eligible for Medicaid, while a move out of state would make them no longer eligible for Medicaid coverage in their previous state. Shares of Medicaid enrollees moving within a state has trended downward in recent years, but trends could have changed in 2021, as more people became vaccinated against COVID-19 and the national eviction moratorium was lifted in August 2021.
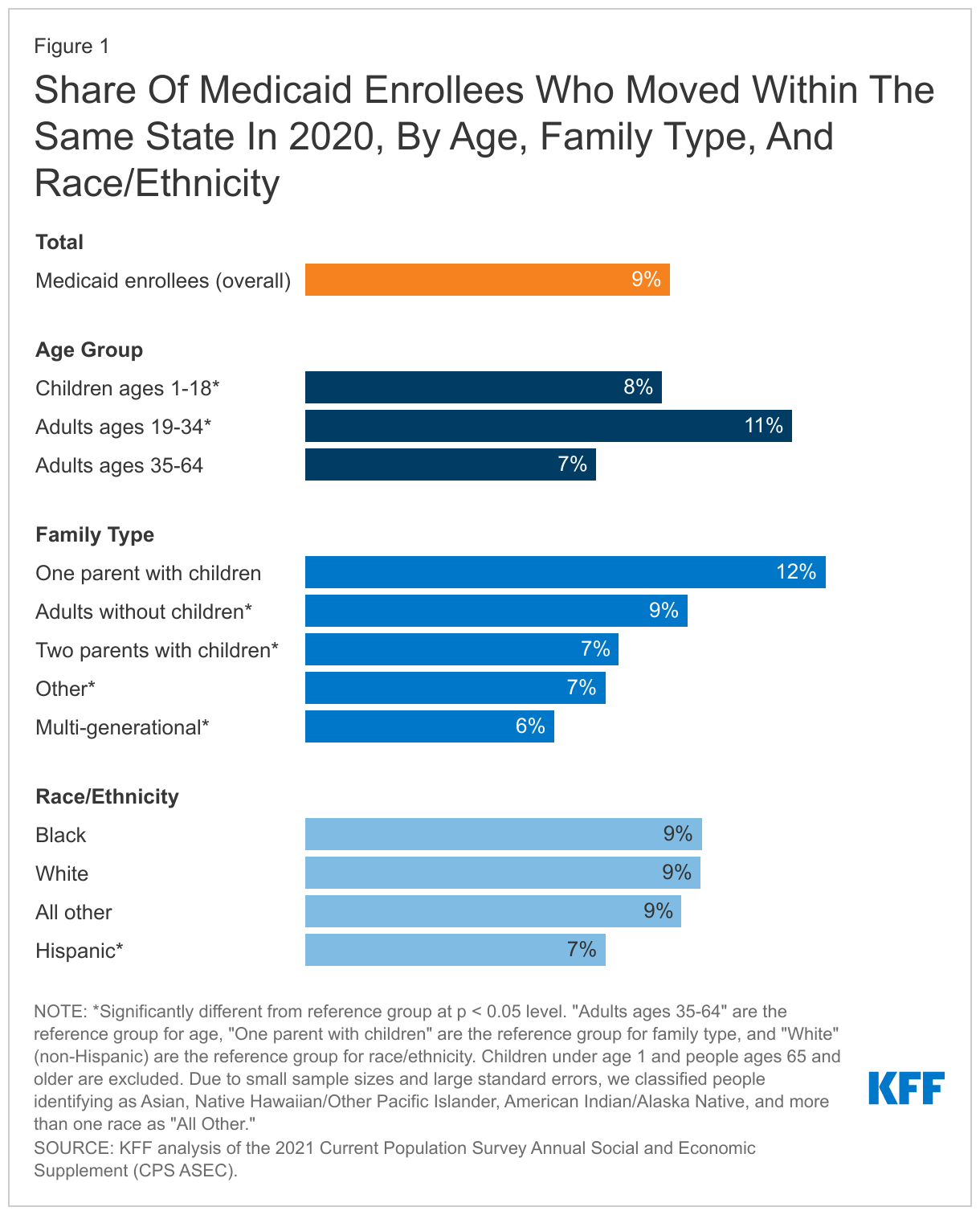
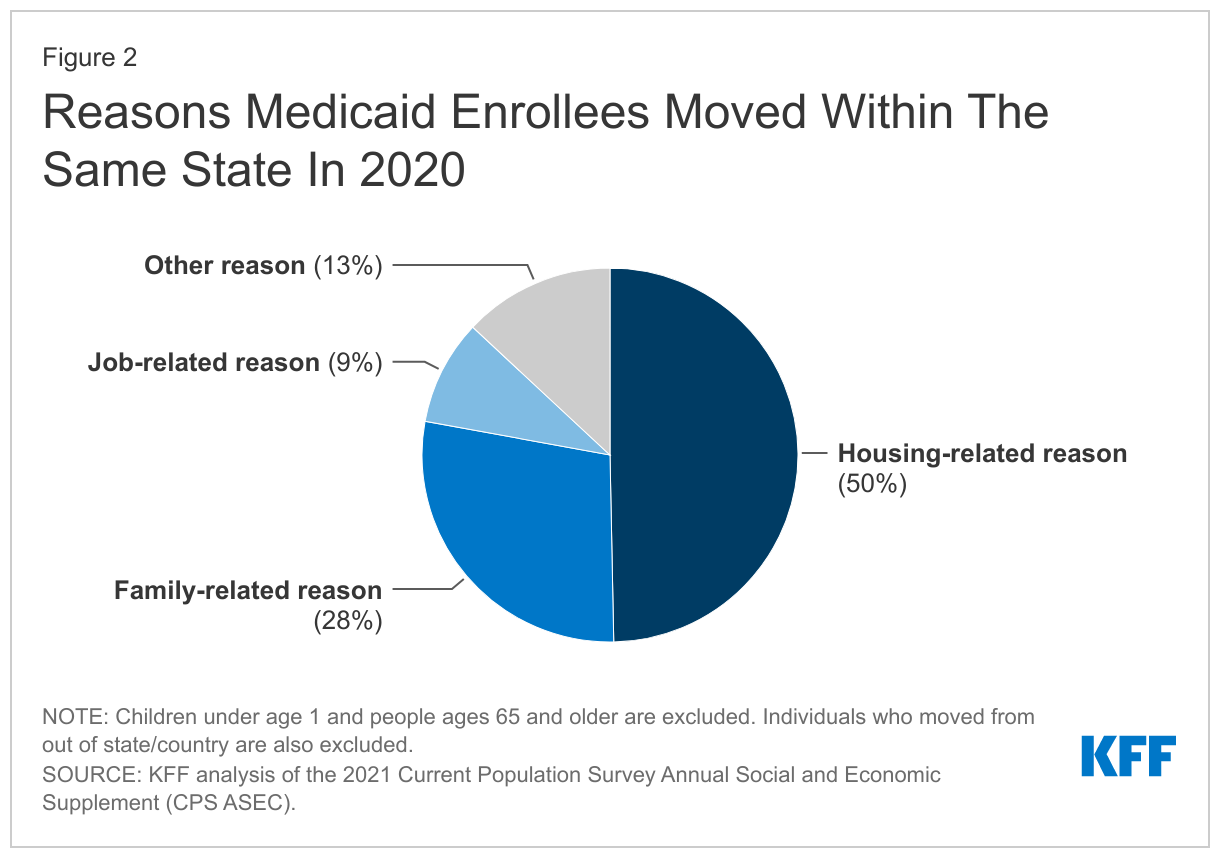
Among those covered by Medicaid, young adults and single-parent families with children were more likely to move within a state than other groups. Among Medicaid enrollees that moved within the same state in 2020, half (50%) moved for housing-related reasons and 28% moved for family-related reasons.
States can take a number of actions to update enrollees’ addresses and other contact information to minimize coverage gaps and losses for eligible individuals after the end of the PHE, particularly for individuals who may have moved within a state. These actions include conducting direct outreach to enrollees, partnering with managed care organizations and other stakeholders in outreach efforts, developing clear policies for returned mail, and checking available data sources for more up-to-date contact information. A recent survey of states found that most states (46) were taking proactive steps such as these to update contact information, although fewer (35) are following up on returned mail. Careful monitoring and oversight of state progress during the unwinding period could provide information to prevent erroneous terminations of coverage.
Introduction
To understand who may be at increased risk of losing Medicaid coverage because of out-of-date contact information, this brief analyzes data from the Current Population Survey’s (CPS) Annual Social and Economic Supplement (ASEC) from March 2021 to examine the share of Medicaid enrollees who moved within a state (and therefore are more likely to remain eligible for Medicaid in the same state) in 2020 and the demographic characteristics of those individuals. It also examines trends in residential mobility over time and discusses strategies states can adopt to minimize coverage losses among these individuals.
The data used in our analysis reflect mobility patterns during 2020 and were collected before important events, such as when the COVID-19 vaccine became widely available to all adults and the end of the national eviction moratorium, that may have affected the number of people who moved more recently. Additionally, our analysis focuses on non-elderly Medicaid enrollees (because enrollees ages 65 and older likely have Medicare as their primary source of coverage) and so we refer to non-elderly Medicaid enrollees simply as “enrollees” for the remainder of this brief. See the Methods box at the end of this brief for more details about the analysis and limitations.
What do we know about Medicaid enrollees who moved in-state in 2020?
Roughly 1 in 10 Medicaid enrollees (9%) moved in-state in 2020. A much smaller share, just 1%, moved to a different state in the U.S., which would make them no longer eligible for Medicaid coverage in their previous state. The share of enrollees moving within the same state was slightly higher compared to people who are not enrolled in Medicaid (8%), although the share was not significantly different for non-enrollees who moved to a different state in 2020 (2%). These estimates are based on CPS ASEC data, which asks survey respondents whether they lived in the same house one year ago. One limitation of this approach is that the CPS ASEC data do not identify people who have moved multiple times over the course of the year, reflecting more severe housing instability that is more common among low-income populations. Additionally, these data do not identify temporary (or seasonal) moves during the year, such as moving in with family or friends, which became more common in 2020 and early 2021 in response to the pandemic.
Among those covered by Medicaid, young adults and single-parent families with children were more likely to move within a state than other groups (Figure 1). In 2020, approximately 11% of young adults (ages 19-34) with Medicaid coverage moved in-state compared to 8% of children and 7% of adults ages 35-64 with Medicaid. Among the different family types analyzed, enrollees who live in single-parent families were the most likely to move in 2020 (12%), while enrollees living in multi-generational families were among the least likely to move (6%). When we compared residential mobility by race/ethnicity, a smaller share of Hispanic people enrolled in Medicaid moved within state in 2020 (7%) compared to White people (9%), while the shares of Black people (9%) and people of other races (9%) who moved were not different compared to White people.
Among enrollees that moved within the same state in 2020, half (50%) moved for housing-related reasons and 28% moved for family-related reasons (Figure 2). Housing-related reasons include wanting a better home and/or neighborhood, wanting cheaper housing, foreclosure or eviction, and other unspecified housing-related reasons. Family-related reasons include establishing one’s own household, changes in marital status, and other unspecified family reasons. Generally, Medicaid enrollees were more likely to move in-state for family-related reasons compared to people who were not enrolled in Medicaid (28% vs. 24%) and were less likely to move in-state for job-related reasons compared to people who were not enrolled (9% vs. 12%). Medicaid enrollees and non-enrollees both moved within the same state for housing-related or other reasons at about the same rate. When compared to the reason people moved in 2018 (the most recent measurement year before the pandemic), Medicaid enrollees’ reasons for moving have stayed relatively steady despite economic disruptions in 2020 related to the pandemic.
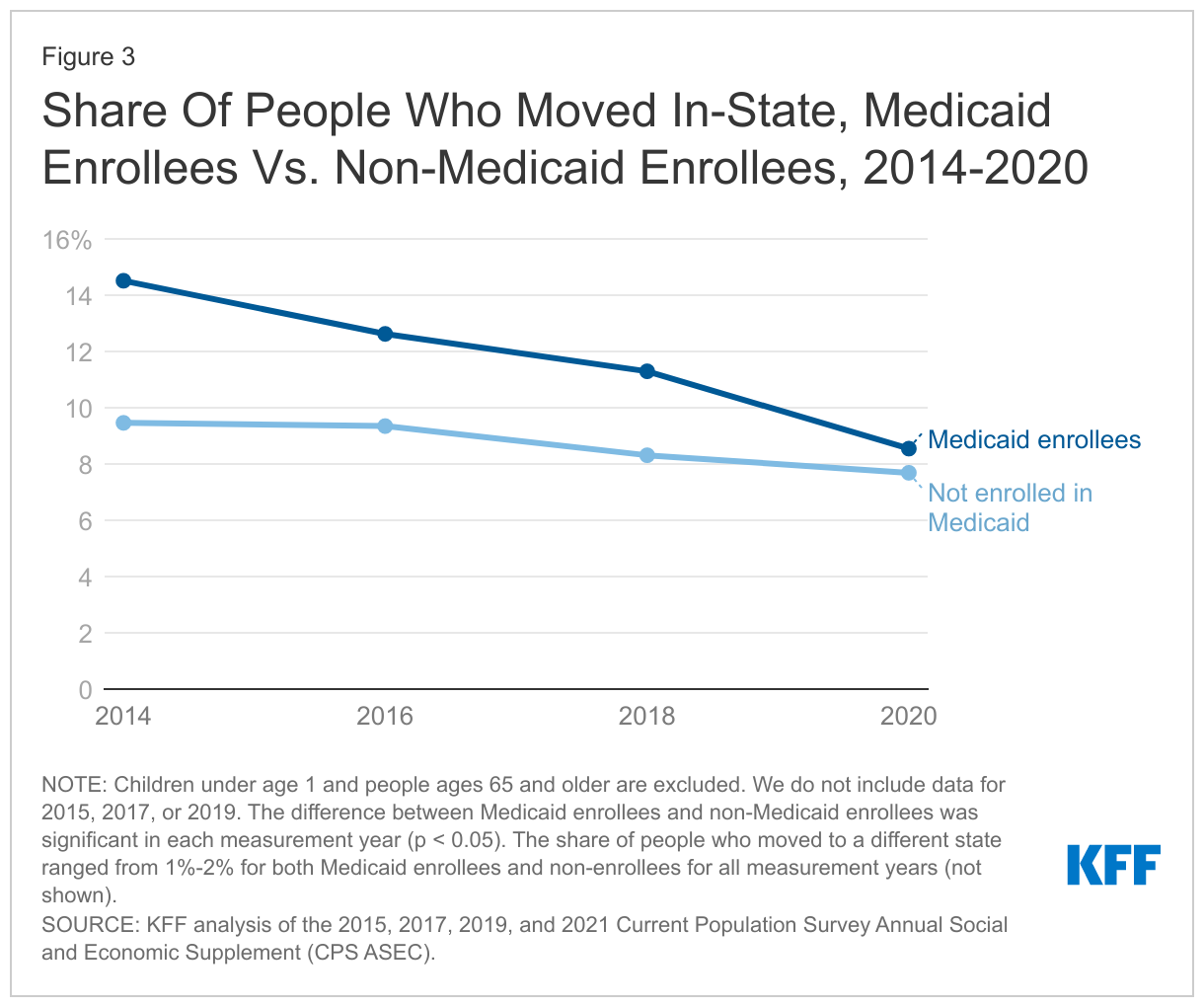
The share of Medicaid enrollees moving within the same state has declined slightly in recent years, from 15% in 2014 to 9% in 2020, although that trend could change in 2021 and 2022 (Figure 3). Declining shares of Medicaid enrollees moving within the same state since 2014 mirrors national trends of fewer people moving over time. However, the share of Medicaid enrollees moving has decreased faster compared to non-enrollees in recent years. While the pandemic has raised concerns about economic disruptions and housing instability among low-income populations, the data for 2020 indicate that residential mobility among both Medicaid enrollees and non-enrollees largely followed pre-pandemic trends. However, these trends could have changed in 2021, as more people became vaccinated against COVID-19 and the national eviction moratorium was lifted in August 2021.
How can states minimize coverage losses among eligible enrollees who move?
With the continuous enrollment requirement in place during the PHE and the prohibition on disenrolling individuals from Medicaid, states may not be communicating regularly with enrollees and, as a result, may have outdated contact information for those who have moved within the state during the past two years. When the PHE ends and states resume routine redeterminations and disenrollments, some enrollees may be at risk of losing coverage simply because they do not receive notices or renewal information. As states prepare to resume normal operations, they can take a number of actions to update enrollee addresses and other contact information to minimize coverage gaps and losses for eligible individuals. The Centers for Medicare and Medicaid Services (CMS) has developed a broad set of policy and operational strategies states can adopt to maintain continuous coverage for eligible individuals, including specific strategies for updating contact information and reducing returned mail:
Conduct communication campaigns through mail, text, and email to encourage enrollees to provide updated contact information. States can send periodic notices during the PHE to remind enrollees to update their contact information. To the extent states have alternative contact information, they can also reach out through automated phone calls, text messages and emails. And, to ensure that enrollees are reminded when they proactively reach out to the Medicaid or other social services agencies, states can update call center scripts to request updated contact information at the beginning of the call and can add alerts to Medicaid, CHIP, and social services websites.
Partner with managed care organizations (MCOs), community-based organizations, application assisters, and providers in outreach efforts. To expand the reach of outreach efforts, states can work with MCOs, community partners, and providers to reinforce messages and remind enrollees to provide updated information. Enrollees are used to receiving communication from MCOs and may be more likely to respond to reminders from them. Navigators and certified application assisters can also be effective partners because they regularly update contact information during interactions with clients. States can opt to accept updated information from these entities, or in the case of MCOs require that they share this information but should develop policies for verifying updated information with enrollees.
Develop clear policies for following up on returned mail that can include checking available data sources and contacting enrollees via phone, text, or email. When mail is returned and no forwarding address is provided, states are encouraged to check available data sources, including the United States Postal Service (USPS) National Change of Address Database, the Supplemental Nutrition Assistance Program (SNAP), Temporary Assistance for Needy Families (TANF) or other programs, and/or contact information from MCOs. They can also contact enrollees via phone, text, or email to obtain updated mailing addresses.
To prepare for the end of the PHE and continuous enrollment requirement, most states (46) are taking proactive steps to update enrollee addresses, although fewer (35) are following up on returned mail as of January 2022. Actions to update addresses include conducting outreach to enrollees, checking other programs for updated addresses, and working with managed care plans and providers to update address information. States that follow up on returned mail are most likely to call or email enrollees using information on file when they received returned mail from a notice sent to an enrollee.
Looking Ahead
As states resume redeterminations and disenrollments at the end of the PHE, evidence suggests that it is unlikely that large proportions of enrollees would be no longer eligible for Medicaid because they moved out of state. When asked to predict the primary reasons people will lose coverage after the continuous enrollment requirement is lifted, few states (3) identified moving as a key driver of disenrollments, and all cited other reasons, including increased income or other changes in circumstances, in addition to moving. While the number of Medicaid enrollees moving within the same state did not increase during the first year of the pandemic, the 9% of Medicaid who moved in-state in 2020 still amounts to a significant number of enrollees whose contact information is more likely to be out of date and who are at increased risk of losing coverage as states unwind the continuous enrollment requirement. It is also possible that, as the pandemic continued into 2021 and 2022, the cumulative number of Medicaid enrollees who moved has increased as well. States with relatively large numbers of disenrollments due to returned mail may indicate erroneous terminations, as returned mail alone does not necessarily indicate a change in economic circumstances that affects eligibility, especially when relatively few enrollees move out of state (approximately 1% of enrollees in 2020). Careful monitoring and oversight of state progress during the unwinding period could provide information to prevent erroneous terminations of coverage.
Methods
We analyzed data from Current Population Survey’s (CPS) Annual Social and Economic Supplement (ASEC) from March 2021, 2019, 2017, and 2015. These data provide information on who moved during the previous year (2020, 2018, 2016, and 2014, respectively). Our analysis focuses on people who had Medicaid coverage at some point during the year and who moved within the same state (moving out of state would mean that the enrollee no longer qualifies for Medicaid coverage in the previous state). We exclude enrollees ages 65 and older since nearly all would qualify for Medicare and are less likely to lose their primary source of coverage. Children under age 1 are also excluded because the CPS ASEC questions on moving as of March of the previous year are not applicable to respondents under age 1. Our analysis also focuses on individuals who moved within the US. While our analysis includes a small number of people who have moved from outside the U.S. (i.e., from a US territory or a foreign country), we do not include these individuals in our counts of people who moved in-state or to a different state. For the March 2021 CPS data (and not for previous years), we analyzed differences in selected demographic groups, including age group, family type, and race/ethnicity. We also analyzed the share of people moving within state by sex, urban/rural (using metropolitan statistical areas as a proxy), and foreign born, but we did not find significant differences between these groups and so are not shown in Figure 2. All differences reported in this brief are measures at the p < 0.05 level.
The analysis focuses on individuals and uses person weights, which is important for interpreting our findings on demographic groups. For example, although children will typically move with adults, the difference between child enrollees and older enrollees reflects situations where adults do not live with children or, in some cases, children (especially those aged 18) who do not live with adults. In other households, the children may be enrolled in Medicaid but their parents are not, or there could be more children enrolled in Medicaid than adults (or vice versa). In analyzing family type, we consider the type of family for each individual. For example, while we excluded enrollees ages 65 and older from our analysis, child enrollees who live with their parents and grandparents are considered to live in multi-generational households.
We conducted a robustness check of our findings by comparing the share of people moving in-state as identified in the CPS ASEC versus the American Community Survey (ACS). We compared findings for Medicaid enrollees and non-enrollees ages 1-64, using data collected in the March 2019 CPS ASEC sample and the 2019 ACS sample. Generally, the percent of people moving in-state over the past year were slightly lower in the March 2019 CPS ASEC sample (11% of enrollees and 8% of non-enrollees) compared to the 2019 ACS sample (13% of non-enrollees and 11% of non-enrollees). We would expect some differences due to different and data collection methods and timing between CPS and ACS, and so the difference of 2 or 3 percentage points seemed reasonably small.
Our findings have important limitations. First, the CPS ASEC sample does not tell us when a person moved. So, we do not know whether the person was enrolled in Medicaid before, during, or after the move. Additionally, we do not know how many times a person moved and, depending upon timing, temporary moves may not be captured. Second, the latest CPS data used here only provide data for 2020, but the economic impacts of the pandemic have lasted much longer, including when the federal government lifted the national eviction moratorium in August 2021.
The “California Advancing and Innovating Medi-Cal” (CalAIM) initiative was recently approved by the Centers for Medicare and Medicaid Services (CMS) and launched in January 2022. CalAIM seeks to improve health outcomes and advance health equity for “Medi-Cal” (Medicaid) beneficiaries and other low-income people in the state. As of September 2021, over 13 million people were enrolled in Medi-Cal in California – the largest Medicaid program in the nation. CalAIM will leverage Medicaid as a tool to help address complex challenges, including behavioral health access, the health needs of people experiencing homelessness, and the complex clinical needs of justice-involved populations. Central to the demonstration is a person-centered approach, first authorized as “Whole Person Care” (WPC) pilots implemented through a waiver approved by the federal government under section 1115 of the Medicaid statute (known as “Medi-Cal 2020”). The WPC pilot program aimed to coordinate and integrate physical health, behavioral health, and social services for Medicaid enrollees with complex needs. Under CalAIM, the state will incorporate and transition WPC pilot services statewide through the state’s Medicaid managed care system. The California initiatives are part of a growing movement to better meet behavioral health needs and improve equity and health by addressing underlying social determinants.
As CalAIM launches, it is useful to take a closer look at the WPC pilot program and what has been learned to date from its implementation. This brief draws heavily on findings from the interim evaluation, which assessed WPC infrastructure development and implementation and analyzed whether WPC led to “better care and better health” within the first three years. In this brief, we explore key questions involving the WPC pilots, which may provide insights for other states pursuing or contemplating similar strategies for identifying and addressing the medical and non-medical or social needs of high-risk, high-utilizing Medicaid enrollees.
What Were Whole Person Care Pilots (WPC)?
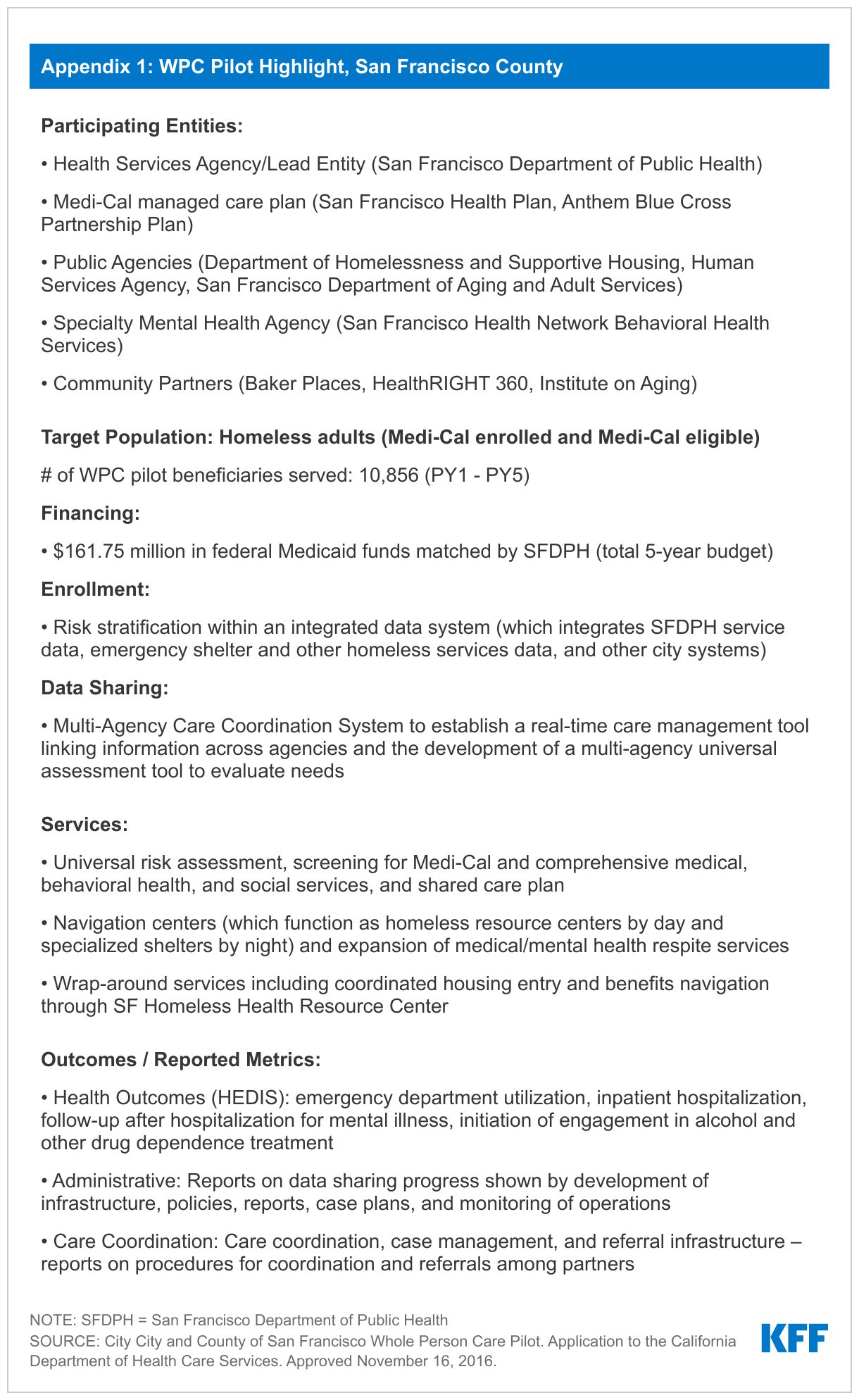
In 2016, California began its “Whole Person Care” (WPC) pilot program, which aimed to coordinate and integrate physical health, behavioral health, and social services for Medicaid enrollees with complex needs. The WPC pilot program also aimed to increase integration and data sharing among county agencies, health plans, and community-based organizations. The pilot was authorized under the state’s Section 1115 waiver. California’s Department of Health Care Services (DHCS) selected 25 WPC pilots (spanning 26 counties) to participate in the program across the state.1 (See Appendix for a spotlight on San Francisco County’s WPC pilot.) Each individual WPC pilot program defined its target population and interventions, within state guidelines. The WPC pilots were scheduled to end in December 2020 but were extended through December 2021 under the state’s Section 1115 waiver.
Each WPC pilot included a “lead entity” and key community partners (called “participating entities”). Lead entities coordinated the pilot, collaborated with local community partners, and served as the single point of contact for DHCS. Lead entities included county health and health services agencies, healthcare systems, behavioral health departments, and a city municipality.2 Each WPC pilot included key community partners, including Medi-Cal managed care plans, county health agencies, other public agencies (e.g., county alcohol and substance use disorder programs, human services agencies, public health departments, criminal justice/probation entities, and housing authorities), and community-based providers.3 In their applications, approved WPC pilots enumerated specific roles of each participating entity in service provision, data management, and implementation of WPC programs. In the initial program years, WPC pilots focused heavily on developing data and administrative infrastructure for data sharing, case management, outreach and enrollment, performance, and quality improvement efforts.
WPC pilots targeted a number of high-risk populations with complex needs. Primary WPC target populations included high utilizers of health care (e.g., those with avoidable use of the emergency room and/or hospital admission), individuals experiencing homelessness or at-risk of homelessness, individuals with multiple chronic conditions, individuals with severe mental illness or substance use disorders (SMI/SUD), and justice-involved individuals. Nearly half (46%) of all pilot enrollees were homeless across target populations, and most were men, 50-64 years old, White, English speaking, and enrolled in managed care. Pilots classified 10% of enrollees as at-risk of homelessness and 6% as justice-involved. Beneficiaries had high rates of hypertension, substance use disorders, and mental health conditions, as well as high rates of service use (particularly SUD services and emergency department visits). Participation in the pilot program was voluntary for eligible individuals. Many WPC pilots used street or shelter-based outreach to identify eligible enrollees.4 Other strategies used to identify pilot enrollees included referrals from health care facilities, health plan eligibility lists, and predictive modeling based on program criteria.
WPC pilot beneficiaries received care coordination and other services not covered by Medi-Cal to address medical, behavioral health, and social needs. All pilots were required to provide care coordination services, but pilots also offered a variety of other services tailored to local needs and available resources. Services offered by WPC pilots included housing-related services, employment assistance, short-term residential care for individuals experiencing homelessness (referred to as “medical respite”), and sobering centers. Given the high need for housing support, pilots commonly provided housing-related services, including housing navigation (to help identify and secure affordable housing), tenancy supports (e.g., security deposit and first month’s rent), as well as landlord incentives and coaching. Other WPC service examples included providing linkages to health, mental health, and substance use disorder services through medical respite, peer support specialists, mobile teams, or service integration teams.
The state’s Section 1115 waiver authorized up to $3 billion in federal and state Medicaid funds over five years for the WPC pilot. For each demonstration year, $300 million was made available in federal financial participation to fund the WPC pilots. The non-federal share was financed through local funds from participating government agencies (also referred to as “intergovernmental transfers” or IGTs). Each WPC pilot had an annual budget and could draw down funds for eligible activities including infrastructure development, data collection, and services/interventions as well as other outcome-based incentive payments. WPC pilots reimbursed for services on a fee-for-service (FFS) (i.e., per service or encounter) basis or using a per-member-per-month (PMPM) bundle.5 In the early stages, pilots were reimbursed for application submission and reporting baseline data, while subsequent years were oriented toward providing services, achieving proposed metrics, and providing incentive payments.
Pilots were required to submit mid-year and annual reports detailing spending and outcome metrics, including NCQA and HEDIS measures as well as county and population-specific measures. The state is also subject to independent evaluation requirements under its Section 1115 waiver. Findings from the state’s interim independent evaluation of the WPC program are discussed in more detail in the section that follows.
What Can We Learn from WPC?
A variety of strategies resulted in the enrollment of more than more than 108,000 unique individuals into WPC between January 2017 and December 2018 (PY 2 and PY 3).6 To identify and enroll eligible individuals, WPC pilots used administrative and electronic medical record data, referrals from partners (managed care plans, health care providers, and clinics), and warm hand-offs from social services agencies. To facilitate referrals into the program, some WPC pilots developed formal contracts with community partners. Pilots also used street- and shelter-based outreach to identify people eligible for but not enrolled in Medi-Cal. To identify the appropriate interventions for enrollees, some pilots developed universal risk assessment tools (used across partner agencies) to stratify client acuity (or level of need) across multiple domains (e.g., health and housing status). To address eligibility gaps in Medi-Cal (also referred to as “churn”), WPC pilots proactively monitored eligibility and renewal dates.7 Nearly all pilots identified low beneficiary engagement – or willingness to enroll and participate in services – as a barrier and stressed the importance of using a “relationship-based” approach to engage medically and socially complex prospective enrollees, as well as a variety of other strategies to foster engagement (e.g., connecting enrollees to immediate benefits, hiring WPC staff with shared lived experience to build trust).8
Data sharing presented challenges for the vast majority of WPC pilots, although capacity increased over time. The majority of pilots developed electronic platforms to facilitate and track care coordination activities (e.g., care plans, encounter notes, and service referrals). Multiple pilots reported participating in health information exchanges and reported increased utilization of real-time data platforms across lead entities and partner agencies over time. Challenges – including duplicative data entry and managing multiple disparate data systems across settings – persisted across most pilots. Other data sharing challenges included concerns around legal risks of data sharing and differing interpretations of laws and regulations involving patient privacy and confidentiality. To address data sharing concerns, some pilots developed universal consent forms to facilitate the release of information across WPC partner organizations, while others developed consent forms to allow for the targeted release of specific data, allowing enrollees to opt out of sharing certain information (e.g., mental health history and HIV test results).9
Pilots reported success with introducing new care coordination processes and using data systems/sharing to support care coordination activities. Care coordination services were frequently provided by non-clinical staff (under supervision of clinical staff) including community health workers (CHWs), and most pilots reported employing care coordinators with shared lived experience. Many pilots reported using a single dedicated care coordinator who followed enrollees across all WPC-participating care settings. Nearly all pilots reported the most common mode of communication between care coordinators and enrollees was in-person. All pilots reported using “active” referral strategies, including helping enrollees schedule appointments, accompanying enrollees to appointments, assisting with transportation, and following up with enrollees after appointments. Challenges common to care coordination included limited availability and/or accessibility of services for referrals. This was especially true for housing needs, where barriers included long wait times for permanent housing, limited housing options available, and poor housing quality.
Figure 1: Interim Outcomes and Learnings form WPC Pilots
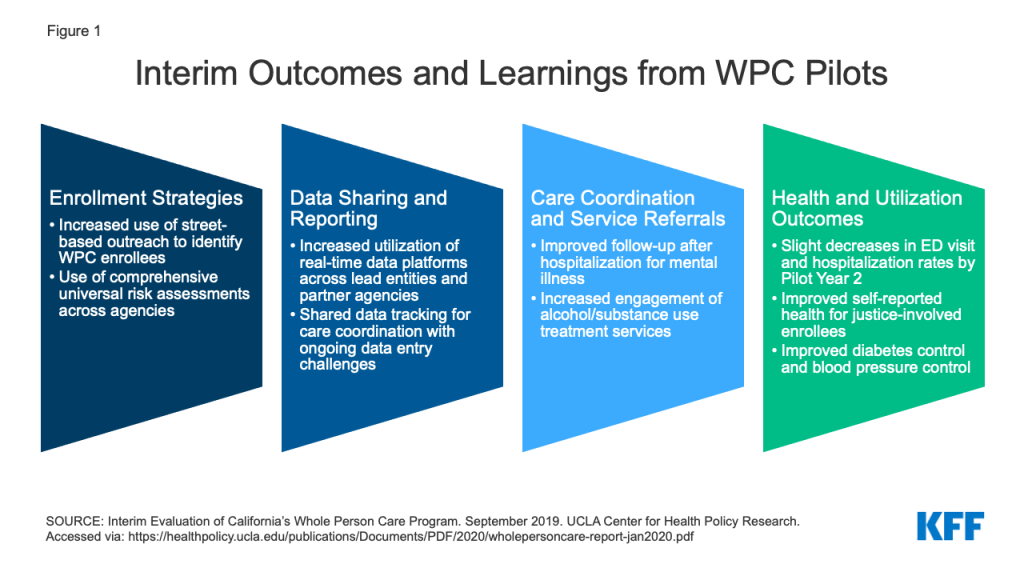
WPC pilots demonstrated improvements in select health utilization and outcomes, care coordination, and delivery of housing services. The interim evaluation used pilot-reported metrics and Medi-Cal data to determine whether WPC led to better care and better health in the first three years. Analyses included comparison of selected Medi-Cal metrics before and after WPC implementation for WPC enrollees and a control group of Medi-Cal enrollees with similar characteristics. Interim evaluation data showed WPC pilots improved rates of follow-up after hospitalization for mental illness, initiation and engagement in alcohol and drug dependence treatment, and timely provision of comprehensive care plans and suicide risk assessments. The interim evaluation found that emergency department (ED) visit rates from WPC Pilot Year 1 to Pilot Year 2 decreased by 19% for WPC enrollees and 8% for the control group, a significantly larger decrease for the WPC enrollees, although analysis of pre-WPC enrollment compared to post-enrollment ED visit rates found no difference for both groups.10 While adjusted trends of all-cause readmissions did not show a reduction in either group, rates of all-cause readmissions declined from year 1 to year 2 (this decline was greater among WPC enrollees compared to the control group). The interim evaluation also found improvement in health outcomes metrics, including self-reported overall and emotional health and diabetes and blood pressure control. Nearly half of all pilot enrollees were homeless across target populations. The interim evaluation showed success in delivery of housing services and in the receipt of supportive housing, but challenges related to adequate housing supply and direct funding to provide housing. Recent analyses found the COVID-19 pandemic impacted WPC pilots in a variety of ways, but pilots were able to capitalize on existing WPC infrastructure and leverage/coordinate with other COVID-19 response activities. The final evaluation will assess the role of WPC in reducing costs for pilot enrollees and the Medi-Cal program overall, whether care coordination and partnerships were sustained beyond the demonstration, and any differences in interventions/services by target population and pilot site to help identify which services may improve outcomes.
What is Next for WPC and CalAIM?
Under CalAIM, the state will move beyond county pilots to standardize and incorporate services offered by WPC statewide through Medi-Cal managed care plans. CalAIM, which launched in January 2022, seeks to take the state’s whole person care approach statewide, with a central focus on improving health and reducing health disparities and inequities.11 CalAIM adds new programs and reforms existing programs.12 The CalAIM demonstration and its various components are authorized under Section 1115, Section 1915(b), and through state plan amendments. The three stated goals of CalAIM13 are as follows:
Identify and manage member risk and need through whole person care approaches and addressing SDOH.
Improve quality outcomes, reduce health disparities, and drive delivery system transformation and innovation through value-based initiatives, modernization of systems, and payment reform.
Move Medi-Cal to a more consistent and seamless system by reducing complexity and increasing flexibility.
Under CalAIM, Medi-Cal managed care plans will provide Enhanced Care Management (ECM) and Community Supports to targeted high-need beneficiaries. These services will be provided through contracts with community-based providers including organizations that participated in WPC.14 With the launch of ECM and Community Supports, DHCS will sunset the WPC pilots and the Health Homes program.15 Although the state has indicated many WPC enrollees will automatically transition to receiving ECM and Community Supports (many of which the state says may be equivalent to services received under WPC), some WPC enrollees will not transition to receiving these services, and some individuals may lose access to certain services they received under WPC.16 ECM and Community Supports (described in detail in the box below) will only be available to Medicaid beneficiaries enrolled in managed care plans, and managed care plans will have discretion over which Community Supports to cover.
Key New Services Offered Under CalAIM
Enhanced Care Management Benefit: The new enhanced care management benefit includes care coordination and comprehensive care management services to address the clinical, behavioral, and social needs of Medi-Cal enrollees with complex needs. Managed care plans will contract with community-based entities (e.g., county agencies, FQHCs, PCPs, CMHCs) to provide care management services.17 DHCS has identified populations of focus for the new ECM benefit (e.g., individuals experiencing homelessness, high utilizers, and adults with serious mental illness or substance use disorders) while managed care plans will be able to add to this list.18 Every beneficiary enrolled in ECM will have a dedicated care manager.
Community Supports: Community Supports (also referred to as “in lieu-of services” (ILOS)) will address social drivers of health.19 These services build on and scale existing work from WPC pilots, Health Homes, and home and community-based services (HCBS) waivers. DHCS has identified 14 Community Supports.20 Services will be delivered through community providers and integrated with ECM. Examples include housing navigation services, recuperative care (medical respite), environmental accessibility adaptations, medically tailored meals, and sobering centers. These services will substitute for certain medical services (e.g., emergency department visits, inpatient hospital care, or nursey facility services) covered by Medi-Cal. The state is encouraging (but not requiring) managed care plans to offer as many of the 14 Community Supports as possible. Most of the Community Supports have been authorized as “ILOS” under Section 1915(b) waiver authority.21 Although “Special Terms and Conditions” (STCs) are not a typical feature of 1915(b) waiver approvals, CMS imposed extensive STCs in connection with the state’s 1915(b) approval. The STCs impose documentation and reporting requirements on both managed care plans and the state Medicaid agency as CMS aims to evaluate the effectiveness of the ILOS and their impact on Medicaid beneficiaries.
Under Section 1115, CMS authorized $1.44 billion in one-time funding to assist with transitioning the WPC pilots and Health Homes programs from Medi-Cal 2020 to CalAIM. “Providing Access and Transforming Health” (PATH) will provide transitional funding to support continuity of services and maintain and support provider and community-based organization capacity. One goal of PATH will be to help ensure Medi-Cal enrollees have continuous access to benefits and services provided previously through WPC pilots as these services and activities are integrated into managed care plans. The funding may not be used to initiate new services but is supposed to ensure continuity for services that correspond to Community Supports managed care plan choose to offer.22 A portion of PATH funds will be used to support justice-involved individuals by sustaining pre- and post-release services provided through WPC pilots and by supporting certain pre-release application planning and IT investments for justice-involved activities.
In addition to incorporating services offered by WPC pilots statewide, the state is planning to undertake a host of other behavioral health reforms under CalAIM. For example, the state plans to integrate the administration and financing of specialty mental health and SUD services under a single state/county contract. The goal is to improve outcomes for enrollees through more coordinated treatment and to allow providers to respond in a more patient-centered way. The state also plans to improve coordination of mental health care between Medi-Cal managed care plans (managing non-specialty mental health services) and county-operated mental health (managing specialty mental health services and SUD treatment). Distinct from these efforts, CalAIM also includes a plan to test the full integration of physical health, behavioral health, and oral health under one contracted managed care entity.
Looking Ahead
As mental illnesses and substance use disorder have worsened during the COVID-19 pandemic, many states are building on and developing initiatives to address behavioral health issues in Medicaid. States are expanding benefits such as community-based mobile crisis intervention services and screening, expanding the use of telehealth for behavioral health, and using managed care organizations to deliver services. In addition to California, Colorado, Massachusetts, Montana, and Washington are advancing broad behavioral health initiatives spanning many areas. Key lessons from California to date show that such initiatives require integrated data systems, adequate funding streams, and multi-sector provider partnerships to coordinate services. Going forward, California’s experience in trying to scale the WPC pilots statewide and use managed care authority to broadly deliver a range of additional services will be important to understand and learn from as other states work to improve behavioral health services and address social determinants to enhance health and equity.
Appendix
Two pilots (Small County and Solano County) discontinued their WPC programs as of 12/31/2020. ↩︎
Organizations eligible to apply as lead agencies as defined by the state included county or city agencies, certain designated public hospitals, federally recognized tribes or tribal health programs, or a consortium of these entities. ↩︎
For example, FFS payments might be made for discrete services including mobile clinic visits, housing transition services, medical respite, transportation, or care coordination. PMPM bundled payments might be made for one or more services and/or activities including comprehensive case management, housing support services, mobile outreach and engagement, or long-term care diversion. DHCS may allow pilots to rollover unspent funds from one year to the next. ↩︎
Chuang E, Pourat N, Haley LA, O'Masta B, Albertson E, and Lu C. Integrating Health And Human Services In California's Whole Person Care Medicaid 1115 Waiver Demonstration. Health Aff (Millwood). 2020 Apr;39(4):639-648. doi: 10.1377/hlthaff.2019.01617. PMID: 32250689. Accessed via: https://www.healthaffairs.org/doi/10.1377/hlthaff.2019.01617↩︎
The interim evaluation used difference-in-difference methodology to compare WPC enrollees to the Medi-Cal enrollee control group between a baseline period (pre-WPC enrollment) and an enrollment period (including data from one year after WPC Year 1 and two years after WPC enrollment). The analysis found no significant change for either group for adjusted trends in emergency department (ED) visit rates and a significant increase in hospitalizations for WPC enrollees compared to the control group. However, the analysis found a decrease in ED and hospitalization rates for both groups from the first to the second years of WPC enrollment. Emergency department (ED) visits, hospitalizations, and all-cause readmission for WPC enrollees were rising prior to WPC enrollment and continued to increase in the first year of pilot enrollment (reflecting successful enrollment of high utilizers into the pilot), before declining overall in the second program year. ↩︎
CalAIM builds on existing infrastructure for the 25 WPC pilots, and counties that did not already have WPC pilots in place were able to apply for additional funding in 2020 to initiate WPC-like pilot capacity. All of the 33 counties that applied for the $20 million one-time funding were approved. Accessed via: https://www.dhcs.ca.gov/services/Documents/MCQMD/WPC_Documents/20M-One-Time-Funding-10-18-19.pdf↩︎
In 2018, DHCS launched the Health Homes Program (HHP). The HHP serves eligible Medi-Cal managed care plan Members with complex medical needs and chronic conditions who may benefit from intensive care management and coordination. Health plans are required to automatically authorize all HHP Members for ECM and reassess within six months to determine if they still benefit from ECM-level care coordination. Health plans must also appropriately transition eligible HHP Members to applicable Community Supports that the health plan elects to offer. Accessed via: https://www.dhcs.ca.gov/Documents/MCQMD/WPC-and-HHP-Transition-Public-Webinar-9-21-21.pdf↩︎
“In-lieu-of” services are a substitute for covered services and may qualify as a covered service for the purposes of capitation rate setting, as long as the state determines in-lieu-of services are medically appropriate and cost effective. Enrollees are not required to use the alternative service or setting but may choose to do so. Approved in-lieu-of services are authorized and identified in MCO contracts. Costs associated with in-lieu-of services may be included in the numerator of the medical loss ratio (MLR) and are taken into account when developing capitation rates. ↩︎
The Section 1115 demonstration provides separate authority for short-term post hospitalization housing and recuperative care services (delivered by managed care plans). ↩︎
Funding will be available where there is a current commitment from the managed care plan that it will elect to offer the service by January 1, 2024. ↩︎
The COVID-19 pandemic has coincided with worsening mental health across the country, and California is no exception. For this data note, we analyzed data from the California Health Interview Survey (CHIS), which asks noninstitutionalized adults detailed questions on mental health and substance use, to further examine the impact of the pandemic on mental health in the state.
The pandemic comes on the heels of an already worsening mental health and substance use crisis in California. As shown in Figure 1, a growing share of nonelderly adults have reported past year serious psychological distress over time in California, up from 9% in 2016 to 15% in 2020. Substance use issues have also worsened – drug overdose deaths increased over 40% from 2019 to 2020 in California.
During the pandemic, serious psychological distress was more pronounced among some communities, including women and low-income adults in California. As shown in Figure 2, women in California (16%) were more likely than men (13%) to experience serious psychological distress in 2020. In general, women have more often reported poor mental health compared to their male counterparts both before and during the pandemic. In California, lower-income adults were more likely to experience serious psychological distress (19% for incomes between 0 and 138% FPL; 17% for incomes between 139 and 249% FPL; and 15% for incomes between 250 and 399% FPL) than high-income adults (11%) in 2020 (Figure 2). A recent survey of nonelderly adult Californians who saw a health care provider in the past year also found that low-income individuals were more likely than higher-income individuals to report worsening mental health during the pandemic.1 Separately, compared to White adults in California (15%), some communities of color – including Asian (12%) and Black (11%) adults – were less likely to report experiencing serious psychological distress in 2020 (Figure 2). Serious psychological distress among Hispanic adults (15%) was similar to White adults (Figure 2). Other KFF analyses found that, nationally, mental health and substance use concerns have been exacerbated among many people of color throughout the pandemic. Research has also shown that stigma – including stereotypes and discrimination – around mental health concerns is more pronounced among communities of color, perhaps affecting self-reporting of mental health and access to care. Additionally, a survey of adults in California found that among nonelderly individuals with mental health needs, people of color were less likely than White people to receive care.
In 2020, poor mental health outcomes among nonelderly adults varied greatly across counties in California. As shown in the map below, the share of nonelderly adults with past year serious psychological distress ranged from 9% to 28% across counties in 2020; highest in some Central Valley counties (Colusa/Glenn/Tehama, 28.3%; Butte, 26.9%; Merced, 24.2%) and lowest in Bay Area counties (San Francisco, 9.1%; Marin, 9.5%; Contra Costa, 9.6%). The share of nonelderly adults who ever had thoughts of suicide ranged from 8% to 34% across counties in 2020; highest in northern counties (Del Norte/Lassen/Modoc/Plumas/Sierra/Siskiyou, 34.3%; Butte, 29.7%; Mendocino, 29.2%) and lowest in some southern and eastern counties (El Dorado, 8.1%; Imperial, 8.8%; Placer, 9.3%).
Nearly nine in ten nonelderly adults in California have insurance coverage to help them access and cover the cost of health care, including mental health services. In recent years and in response to the pandemic, the state has introduced several policy measures to increase access to mental health and substance use services; many of these efforts leverage insurance coverage through Medi-Cal (the state’s Medicaid program), which covers 20% of nonelderly adults, or private coverage, which covers 67%.
Across insurance types, large shares of nonelderly adults reported poor mental health outcomes in 2020. Medi-Cal enrollees were significantly more likely than private insurance enrollees to experience past year serious psychological distress in 2020 (18% vs. 11%, respectively) (Figure 4), perhaps reflecting Medi-Cal coverage of many people with disabling health conditions including serious mental illness and/or many low-income individuals who may be more likely to report poor mental health. Many nonelderly adults also reported thoughts of suicide in 2020: 14% among Medi-Cal enrollees and 13% among private insurance enrollees (data was not statistically different).
Many insured adults in California reported barriers to care for mental health and substance use services in 2020. Twenty four percent of nonelderly adults in California reported needing help for mental health or substance use issues in the past year (Table 1).2 Among nonelderly adults with mental health or substance use needs, the share who received treatment in the past year was similar across plan type (60% of Medi-Cal enrollees and 55% of private insurance enrollees) (Table 1). Medi-Cal enrollees who received treatment reported a higher average number of visits to a professional in the past year compared to their privately insured counterparts (18 visits vs. 11 visits).
Many Medi-Cal (40%) and private insurance (45%) enrollees with mental health or substance use needs did not receive treatment. Large shares of insured adults who did not receive treatment cited concerns about costs (54% of Medi-Cal enrollees and 49% of private insurance enrollees) and difficulties scheduling an appointment (30% of Medi-Cal enrollees and 20% of private insurance enrollees) as barriers. With the pandemic and accompanying economic recession, many adults have faced financial hardship and have had difficulty paying for usual expenses. This may be linked to the high shares of adults citing concerns over costs as a barrier for accessing mental health or substance use treatment – even for Medi-Cal enrollees, who have very low or no out-of-pocket costs for these services. Scheduling difficulties as a barrier to accessing mental health or substance use services may reflect an insufficient availability of providers.
Table 1: Among Nonelderly Adults with Any Mental Health or Substance Use Needs, Access and Utilization of Services in the Past Year, by Insurance Type, 2020
All Nonelderly Adults
Medi-Cal Enrollees
Private Insurance Enrollees
Share of Nonelderly Adults with Mental Health or Substance Use Needs
24.3%
23.2%
23.8%
Share that Received Treatment
53.8%
59.6%
54.8%
Average Number of Visits to a Professional
13
18*
11*
Share that Did Not Receive Treatment
46.2%
40.4%
45.2%
Did Not Receive Care Due to Concerns About Costs^
57.2%
53.9%
49.1%
Did Not Receive Care Due to Difficulty Scheduling an Appointment^
23.0%
30.2%
19.9%
*Indicates statistically significant difference between Medi-Cal and private insurance enrollees.^Respondents were able to select from multiple reasons regarding not accessing needed mental health or substance use services.NOTES: Nonelderly adults refers to adults ages 18 to 64. Medi-Cal enrollees refers to enrollees with only Medi-Cal coverage for the past 12 months. Private insurance enrollees refers to enrollees with only private insurance (through employer plans or privately purchased) for the past 12 months.SOURCE: KFF analysis of California Health Interview Survey (CHIS) Adult Data Files, 2020.
The pandemic highlights issues with accessing mental health and substance use care across California. California continues to face shortages of mental health providers. In light of pandemic-related precautions and restrictions, accessing services for health care, including mental health or substance use care, has been challenging nationally. In response, measures, including the temporary public health emergency, have allowed many providers to offer care through telehealth. Across the state of California, access to mental health care can also vary greatly. Specifically, for Medi-Cal enrollees, access can vary widely from county to county and navigating care can be particularly challenging for enrollees with co-occurring serious mental health and physical health needs.
In response to mental health and substance use needs in California during the pandemic, several policy actions were taken to increase and standardize access to care.Senate Bill 855 addresses gaps in existing mental health parity laws by requiring insurers to expand coverage to a broader range of mental health and substance use disorders (apart from Medi-Cal). Assembly Bill 2265 will allow for funds from the Mental Health Services Act, typically reserved for mental health services only, to be used for substance use services as well among people with co-occurring mental health and substance use issues. Additionally, through Senate Bill 803, Medi-Cal mental health and substance use services will expand to include peer support specialists. In California’s recent state budget proposal, funds were allocated for dyadic care – allowing for behavioral health services for parents to be incorporated into pediatric health care visits among Medi-Cal beneficiaries. California’s renewal applications for Section 1115 and 1915(b) waivers, known as California Advancing and Innovating Medi-Cal (CalAIM), were also recently approved. CalAIM builds on the state’s Medi-Cal 2020 Whole Person Care pilot program to coordinate and integrate physical health, behavioral health, and social services for Medicaid enrollees with complex needs. In addition to transitioning these services to the state’s managed care system, CalAIM includes behavioral health initiatives to address the division of services between county-level mental health plans and managed care plans, and to standardize access to services for enrollees with serious mental health needs. Private insurers have also taken steps to address mental health and substance use care. Nationally, some plans expanded coverage to include mental health or substance use services accessed through telehealth and many employer sponsored plans made changes such as waiving or reducing cost-sharing and increasing coverage for out-of-network services. Separately, California has taken steps to fund the statewide launch of 988, a mental health crisis hotline.
Looking ahead, further research on access to care and utilization of mental health services will be informative as state policymakers, administrators, and health care providers continue to discuss how to address mental health and substance use needs among Californians.
This work was supported in part by Well Being Trust. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods
This analysis uses the 2020 California Health Interview Survey (CHIS) Adult Data Files, which surveys noninstitutionalized individuals. We narrowed our analysis to nonelderly adults, ages 18 to 64. In 2019, CHIS conducted a redesign of the survey. The redesign affected representation of different groups in the sample frame. Therefore, some demographic level data are not reported in this analysis; for example, demographic breakouts by type of insurance is excluded.
This survey from California Health Care Foundation used both a probability-based sample and nonprobability sample of nonelderly adults (age 18–64) in California. ↩︎
All respondents of the California Health Interview Survey were asked whether they felt they needed help for a mental or emotional or alcohol or drug problem in the past year. ↩︎