COVID-19 Cases, Deaths, and Vaccinations by Race/Ethnicity as of Winter 2022
As we pass the three-year mark since the World Health Organization characterized the COVID-19 pandemic on March 11, 2020, data from the U.S. show that cases and deaths have remained relatively low through the second half of 2022, over 8 in 10 people (81%) had received at least one COVID-19 vaccination dose as of February 23, 2023, while only 17% of people ages five and older had received an updated bivalent booster dose. Over the course of the pandemic, racial disparities in cases and deaths have widened during variant surges and narrowed when cases and deaths fall. However, overall, Black, Hispanic, and American Indian and Alaska Native (AIAN) people have borne the heaviest health impacts of the pandemic, particularly when adjusting data to account for differences in age by race and ethnicity. While Black and Hispanic people were less likely than their White counterparts to receive a vaccine during the initial phases of the vaccination rollout, the disparities in the share that have received at least one COVID-19 vaccination dose have narrowed over time and reversed for Hispanic people. Despite this progress, a vaccination gap persists for Black people and Black and Hispanic people are about half as likely as their White counterparts to have received an updated bivalent booster dose.
This data note presents an update on the status of COVID-19 cases and deaths by race and ethnicity as of December 2022 and vaccinations by race/ethnicity as of February 2023, based on federal data reported by the Centers for Disease Control and Prevention (CDC).
What is the status of COVID-19 cases and deaths by race/ethnicity?
Racial disparities in COVID-19 cases and deaths have widened and narrowed over the course of the pandemic, but when data are adjusted to account for differences in age by race/ethnicity, they show that AIAN, Black, and Hispanic people have had higher rates of infection and death than White people over most of the course of the pandemic.
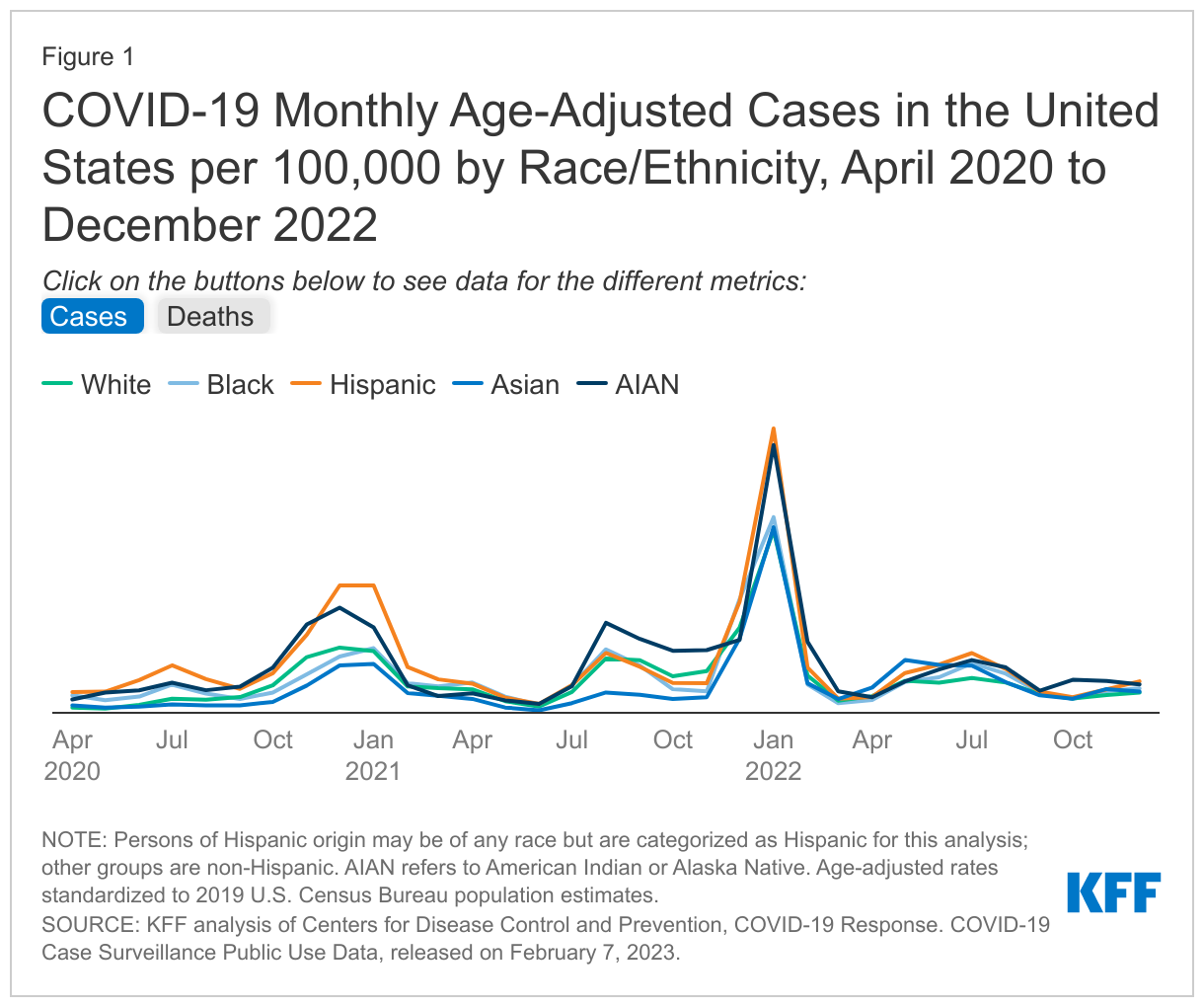
Early in the pandemic, there were large racial disparities in COVID-19 cases. Disparities narrowed when overall infection rates fell. However, during the surge associated with the Omicron variant in Winter 2022, disparities in cases once again widened with Hispanic (4,404.9 per 100,000), AIAN (4,148.6 per 100,000), Black (3,029.4 per 100,000) people having higher age-adjusted infection rates than Asian (2,873.4 per 100,000) and White people (2,826.4 per 100,000) as of January 2022 (Figure 1). Following that surge, infection rates fell in Spring 2022 and disparities once again narrowed. During Summer 2022, there was a slight rise in infection rates with higher age-adjusted infection rates for Hispanic, AIAN, Black, and Asian people compared to White people. Between Fall/Winter 2022, infection rates fell across groups, but as of December 2022, the age-adjusted COVID-19 infection rates were highest for Hispanic people (488 per 100,000) and AIAN people (440 per 100,000). White and Asian people had the lowest infection rates at 313 per 100,000 and 329 per 100,000, respectively.
While death rates for most groups of color were substantially higher compared with White people early in the pandemic, since late Summer 2020, there have been some periods when death rates for White people have been higher than or similar to some groups of color. However, age-adjusted data show that AIAN, Black, and Hispanic people have had higher rates of death compared with White people over most of the pandemic and particularly during surges. For example, as of January 2022, amid the Omicron surge, age-adjusted death rates were higher for Black (37.6 per 100,000), AIAN (34.8 per 100,000), and Hispanic people (30.0 per 100,000) compared with White people (23.5 per 100,000) (Figure 1). Following that surge, disparities narrowed when death rates fell. As of December 2022, age-adjusted death rates were similar across groups at 4.4 per 100,00 for White people, 3.8 per 100,000 for AIAN people, 3.7 per 100,000 for Black people, 3.5 per 100,000 for Hispanic people, and 3.2 per 100,000 for Asian.
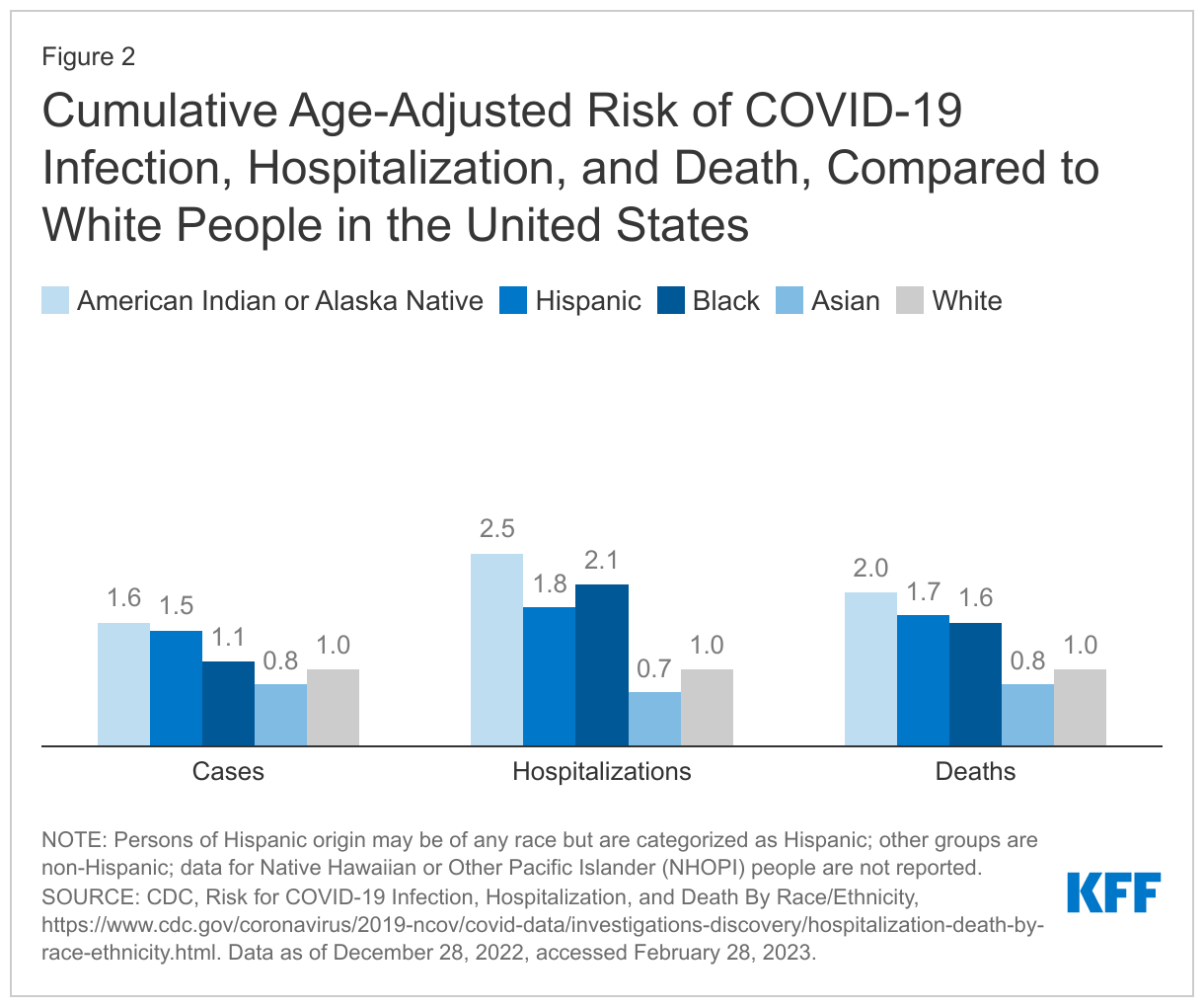
Despite these fluctuations in patterns of cases and deaths by race and ethnicity over time, total cumulative age-adjusted data show that AIAN and Hispanic people have had higher risk for COVID-19 infection and AIAN, Hispanic, and Black people have had higher risk for COVID-19 deaths compared with White people. As of December 28, 2022, cumulative age-adjusted data showed that AIAN and Hispanic people were about 1.5 times as likely to be infected with COVID-19 compared with White people (Figure 2). AIAN people were twice as likely as White people to die from COVID-19, and death rates for Hispanic and Black people were 1.7. and 1.6 times higher than White people, respectively. AIAN, Black, and Hispanic people also have had increased risk of hospitalization due to COVID-19 compared with White people.
What are COVID-19 vaccination and booster patterns by race/ethnicity?
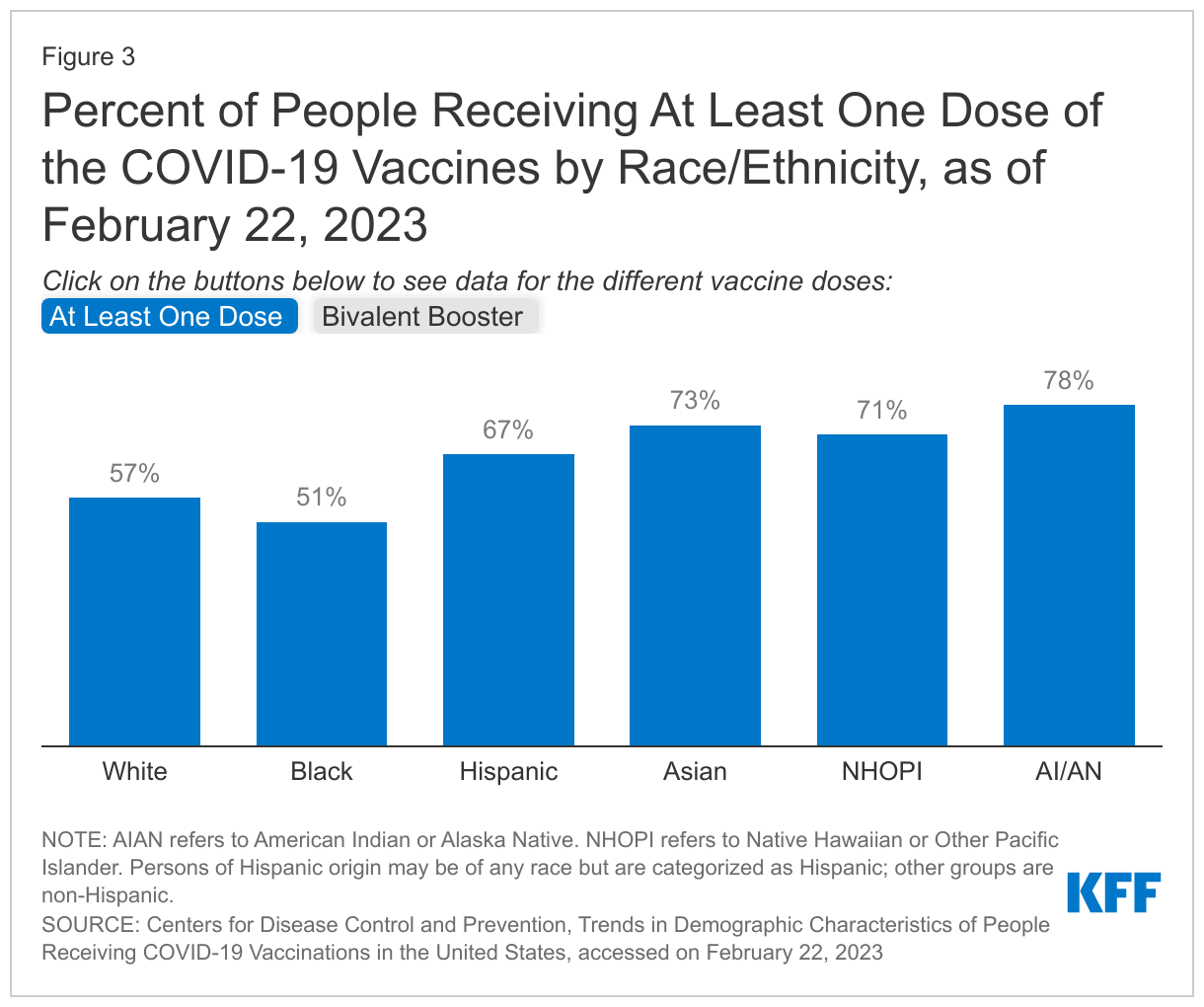
While disparities in the uptake of at least one COVID-19 vaccination dose have narrowed over time and have been reversed for Hispanic people, they persist for Black people. KFF analysis shows that at both the federal and state level, there were large gaps in vaccination for Black and Hispanic people in the initial phases of the vaccination rollout, which narrowed over time and eventually reversed for Hispanic people. Despite this progress, a vaccination gap persists for Black people. According to the CDC, over 8 in 10 people (81%) had received at least one COVID-19 vaccination dose as of February 23, 2023, and race/ethnicity was known for 76% of people who had received at least one dose. Based on those with known race/ethnicity, about half (51%) of Black people had received at least one dose compared with 57% of White people, roughly two-thirds (67%) of Hispanic people, and over seven in ten Native Hawaiian and other Pacific Islander (NHOPI) (71%), Asian (73%), and AIAN (78%) people (Figure 3).
Overall, few people have received the updated bivalent booster vaccine dose, and Black and Hispanic people are about half as likely as White people to have received this booster so far. The updated bivalent boosters protect against both the original virus that causes COVID-19 and the BA.4 and BA.5 Omicron variants. These boosters became available for people ages 12 years and older on September 2, 2022, and for people ages 5-11 years old on October 12, 2022. The CDC recommends that people ages 5 years and older receive one bivalent booster at least 2 months after their last COVID-19 vaccine dose. The CDC reports that, overall, 17% of people over age five have received the updated bivalent booster vaccine dose as of February 23, 2023, with race/ethnicity data available for 90% of recipients. Based on those with known race/ethnicity, 21% of eligible Asian people had received a bivalent booster dose, higher than the rate for White people (16%). Rates were slightly lower for eligible AIAN (14%) and NHOPI (11%) people, while eligible Black (9%) and Hispanic 8%) people were about half as likely as their White counterparts to have received the bivalent booster dose (Figure 3).
Discussion
While disparities in cases and deaths have widened and narrowed over the course of the pandemic, age-adjusted data show that AIAN, Black, and Hispanic people have had higher rates of cases and death compared with White people over most of the course of the pandemic and that they have experienced overall higher rates of infection, hospitalization, and death.
Data point to significantly increased risks of COVID-19 illness and death for people who remain unvaccinated or have not received an updated bivalent booster dose. During the initial vaccine rollout, Black and Hispanic people were less likely to receive vaccines than their White counterparts. However, disparities in the uptake of at least one COVID-19 vaccination dose have narrowed over time and reversed for Hispanic people, though they persist for Black people. Despite this progress in initial vaccination uptake, overall uptake of the updated bivalent booster dose has been slow so far, and eligible Black and Hispanic people have been about half as likely to have received an updated booster than their White counterparts.
Overall, these data show that although the pandemic has contributed to growing awareness and focus on addressing racial disparities, they persist, reflecting the underlying structural inequities that drive them. The findings highlight the importance of a continued focus on equity and efforts to address inequities that leave people of color at increased risk for exposure, illness, and death as well as to close gaps in access to health care, as COVID-19 recovery continues.