Text and figures 1 and 5 were updated on July 23, 2024 to reflect policy updates in Maryland & Michigan.
Key Takeaways
- Abortions at or after 21 weeks are uncommon and represent 1% of all abortions in the U.S. The procedures are expensive and often require travel and lost wages. They normally require treatment over multiple days and are only performed by a subset of all abortion providers.
- Claims of abortions occurring “moments before birth” or even “after birth” are false. These scenarios do not occur, nor are they legal in the United States.
- Reasons individuals seek abortions later in pregnancy include medical concerns such as fetal anomalies or maternal life endangerment, as well as barriers to care that cause delays in obtaining an abortion.
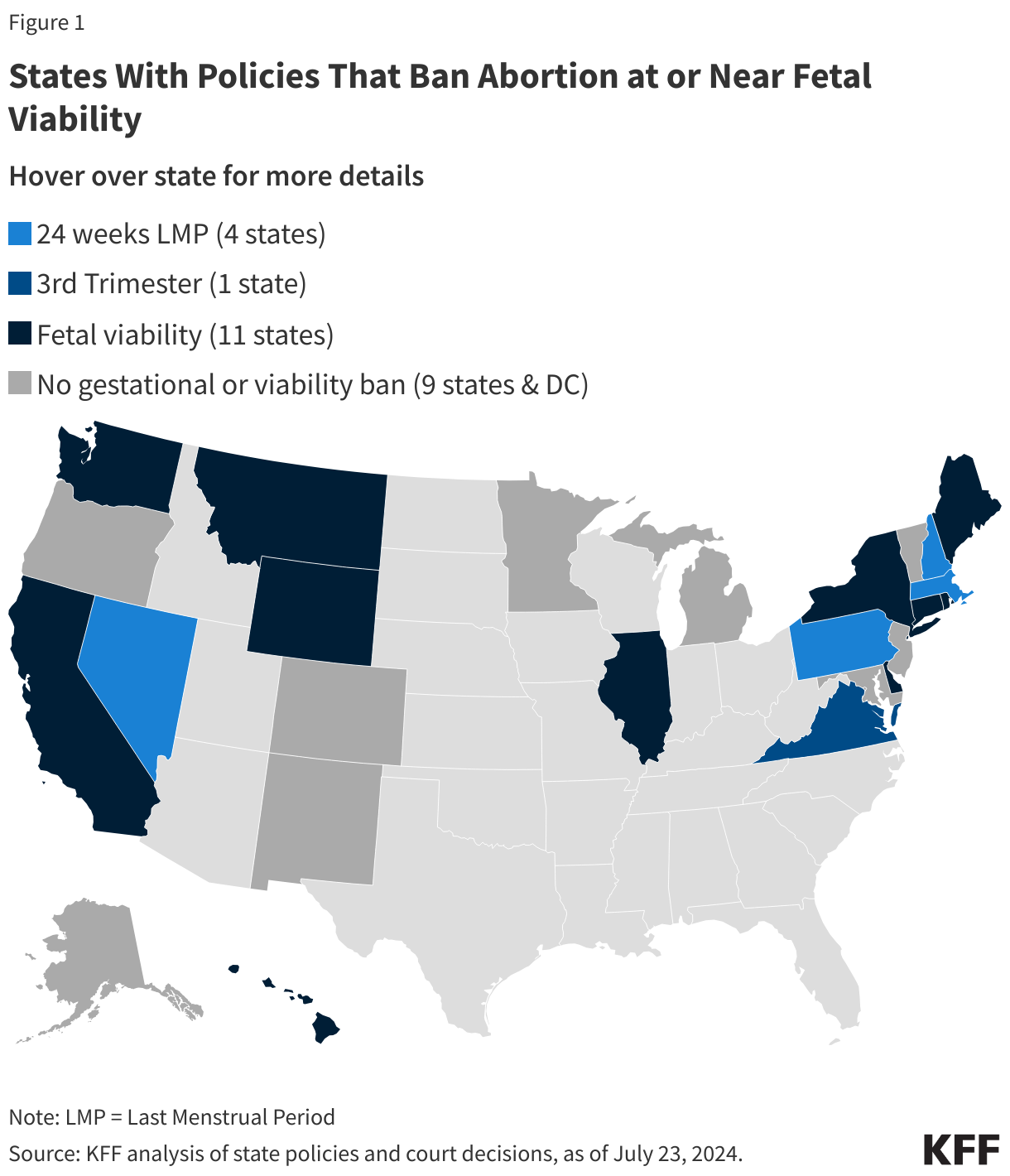
- Fourteen states currently ban abortion and 11 have gestational bans that restrict abortion at a certain point in pregnancy. An additional 16 states ban abortion at or near “viability”, the point where a fetus can survive outside the womb.
- Access to abortions later in pregnancy has always been limited; there are few providers that offer the services and the costs are often prohibitive. Changes in the landscape of abortion access in the U.S. post-Dobbs has led to an increase in out of state travel for abortion services as well as an increase in delays. It is still unknown whether this has led to an increase in the share of abortions that are performed later in pregnancy.
Introduction
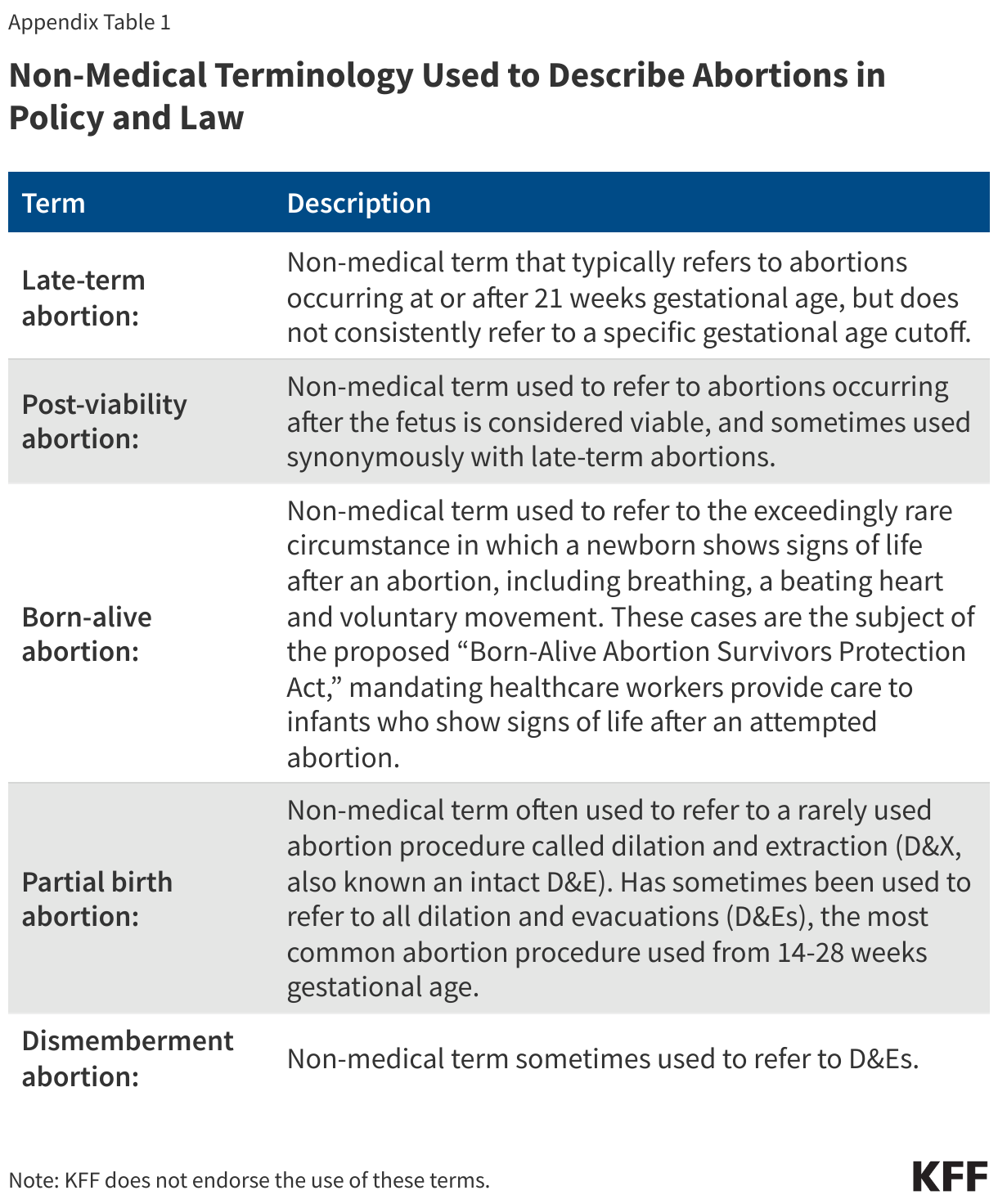
Abortions occurring at or after 21 weeks gestational age are rare. They are often difficult to obtain, as they are only available in a handful of states, performed by a small subset of abortion providers and are typically costly and time-intensive. Yet, these abortions receive a disproportionate share of attention in the news, policy and the law. Discussions on this topic are often fraught with misinformation; for example, intense public discussions have been sparked after several presidential candidates claimed there were abortions occurring “moments before birth” or even “after birth.” In reality, these scenarios do not occur, nor are they legal, in the United States. Discussion of this topic is distorted and inflamed by the terminology that is sometimes used to describe abortions later in pregnancy— including “late-term,” “post-viability,” “partial birth,” “dismemberment” and “born-alive” abortions. There have been some news reports of former President and current Republican presidential candidate Donald Trump’s support of a national 16-week abortion ban that would eliminate access to abortions later in pregnancy except when the life of the pregnant person is in danger or the pregnancy is a result of rape/incest. This brief explains why individuals may seek abortions later in pregnancy, how often these procedures occur, and the various laws which regulate access to abortions later in pregnancy across the country.
Clarifying Pregnancy Dating: pregnancies are measured using gestational age (GA), calculated in days and weeks since the first day of the last menstrual period (LMP). Since some people do not know the date of their LMP, ultrasound can also be used to calculate GA. Post-fertilization or fertilization age refers to the time since the egg and sperm fused to create a fertilized egg. Fertilization occurs approximately 2 weeks after menses, thus gestational age by LMP predates fertilization age by ~2 weeks. By convention, gestational age is used to discuss pregnancy dating as most pregnant individuals know their LMP, however certain abortion regulations reference fertilization age instead.
What is a so-called “late-term” abortion?
“Late term” abortion typically refers to abortions obtained at or after 21 weeks, however it is not an accepted medical term, nor is there a consensus around to which gestational ages it refers. Members of the medical community have criticized the term “late-term” abortion, as it implies abortions are taking place after a pregnancy has reached “term” (37 weeks) or “late term” (>41 weeks) which is false. In fact, the American College of Obstetricians and Gynecologists (ACOG) has written that “late-term abortion” has no medical meaning. As such, this brief discusses abortions occurring at ≥21 weeks gestation as abortions later in pregnancy, but it should be noted that 21 weeks is a largely arbitrary cutoff based on how the CDC collects data on abortions. Abortions at this stage in pregnancy are sometimes referred to as “later abortions” by the medical community as well.
How do states restrict or regulate abortions later in pregnancy?
On June 24, 2022, in Dobbs v. Jackson Women’s Health, the Supreme Court overturned Roe and eliminated the federal constitutional standard that had protected the right to abortion. Without any federal standards, states can now set their own policies banning or protecting abortion at any point in pregnancy. This has drastically changed the landscape of abortion in the United States, as 14 states have now banned abortion at any stage of pregnancy and 11 others have gestational limits banning abortion after a certain point in pregnancy, such as before cardiac activity is detected in the fetus or up to a certain number of weeks of pregnancy.
However, in states without abortion bans or gestational bans before 22 weeks LMP, access to abortions later in pregnancy is often limited for many reasons, including viability bans, bans on certain abortion procedures, and a limited number of abortion providers who are trained or willing to provide abortions later in pregnancy. While viability, the point when a fetus can survive outside the womb, is no longer the federal standard that defines the legality of abortion in the U.S., 16 states that still allow abortions currently have laws restricting abortion at “viability” or at 24 weeks LMP / 3rd trimester, when viability is presumed to occur (Figure 1). These states have abortion exemptions similar to the exemptions in abortion bans (such as to preserve the health or life of the pregnant person) and gestational limits, defining when an abortion is allowed to be performed after viability. Most of the 11 states that restrict abortions at “viability” define it as the point where a physician or other healthcare provider determines whether a fetus can survive outside the womb. Four of these states include language in their abortion policies defining viability as the point where there is a likelihood that the fetus could survive without the “application of extraordinary measures” and another three states have language clarifying the fetus could survive with or without extraordinary measures.
Box 1: What is viability?
Prior to the Dobbs decision, viability was the delineating factor in the abortion debate established by Roe v Wade and subsequent Supreme Court decisions. However, viability has never been properly defined by the courts and in reality, depends on the individual pregnancy and on various factors, including gestational age, fetal weight and sex, and medical interventions available. While viability does not refer to a specific gestational age, it is often presumed at 24 weeks gestation, with “periviability” referring to the time around viability (20 to 26 weeks gestation). The hospital at which the infant is delivered can greatly affect viability. Preterm infants born in resource-rich settings have a higher likelihood of survival than those born in resource-poor settings, thus their point of viability can be earlier than in other setting with fewer resources or trained clinicians. This is in part due to access to neonatologists and maternal-fetal-medicine doctors, but also due to hospital-specific policies; in a study of 24 academic hospitals, active treatment for infants born at 22 weeks ranged from 0% to 100% depending on the hospital, showing that the criteria used to determine viability at one hospital may not be the same at another.
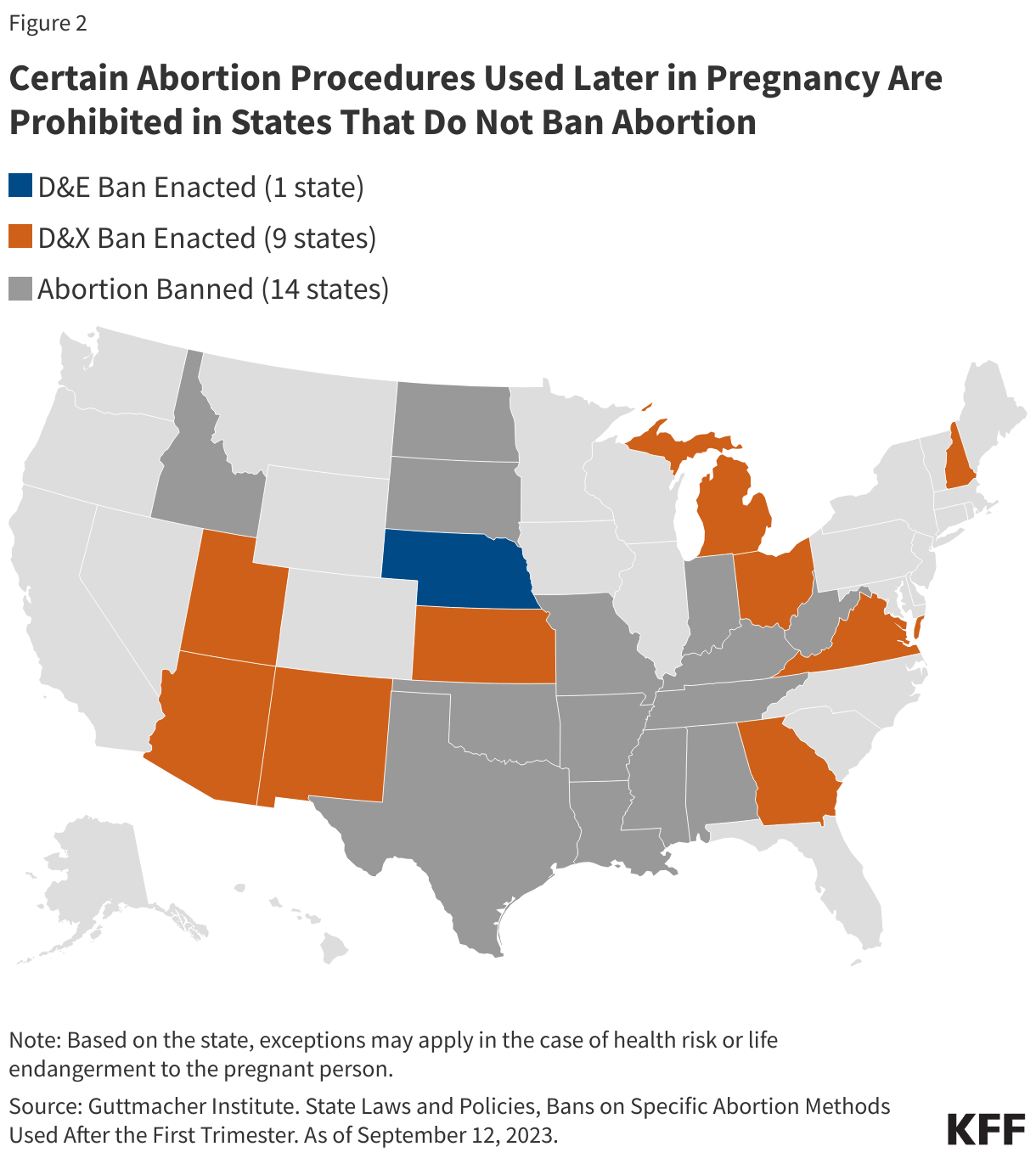
Some states have also passed laws banning clinicians from performing certain abortion procedures that are commonly used in later abortions (Figure 2). Almost all abortions performed at or after 21 weeks are performed by a dilation and evacuation (D&E) procedure (93–95% per CDC data). This involves dilating the cervix and evacuating the pregnancy tissue using forceps, with or without suction. D&Es can be performed safely up to at least 28 weeks gestational age, and when compared to their alternative of labor induction, have been found to be quicker and result in fewer complications; further, many individuals may prefer surgical management as they will be sedated and do not have to undergo labor and delivery of the fetus.
Nebraska has enacted a D&E ban, although the state also has a 12-week gestational ban. Nine states ban dilation and extractions (D&Xs), a rarely used abortion procedure also referred to as an intact D&E or a “partial birth abortion” by policymakers (Appendix Table 1).
In addition to gestational age limits and method bans used for abortions later in pregnancy, abortions later in pregnancy are subject to the same regulations that apply to abortions earlier in pregnancy, including mandatory waiting periods and physician and hospital requirements.
How common are abortions later in pregnancy?
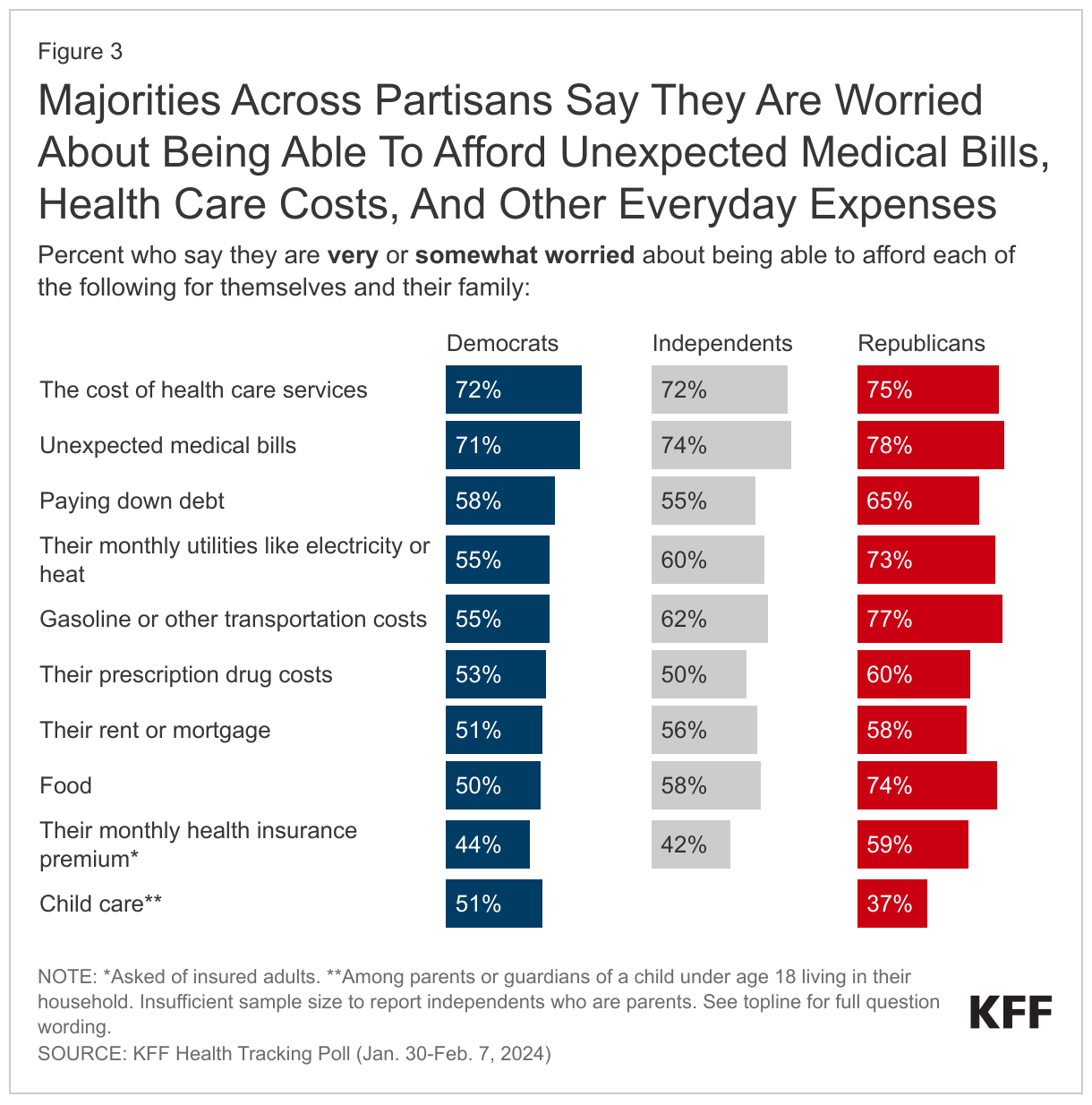
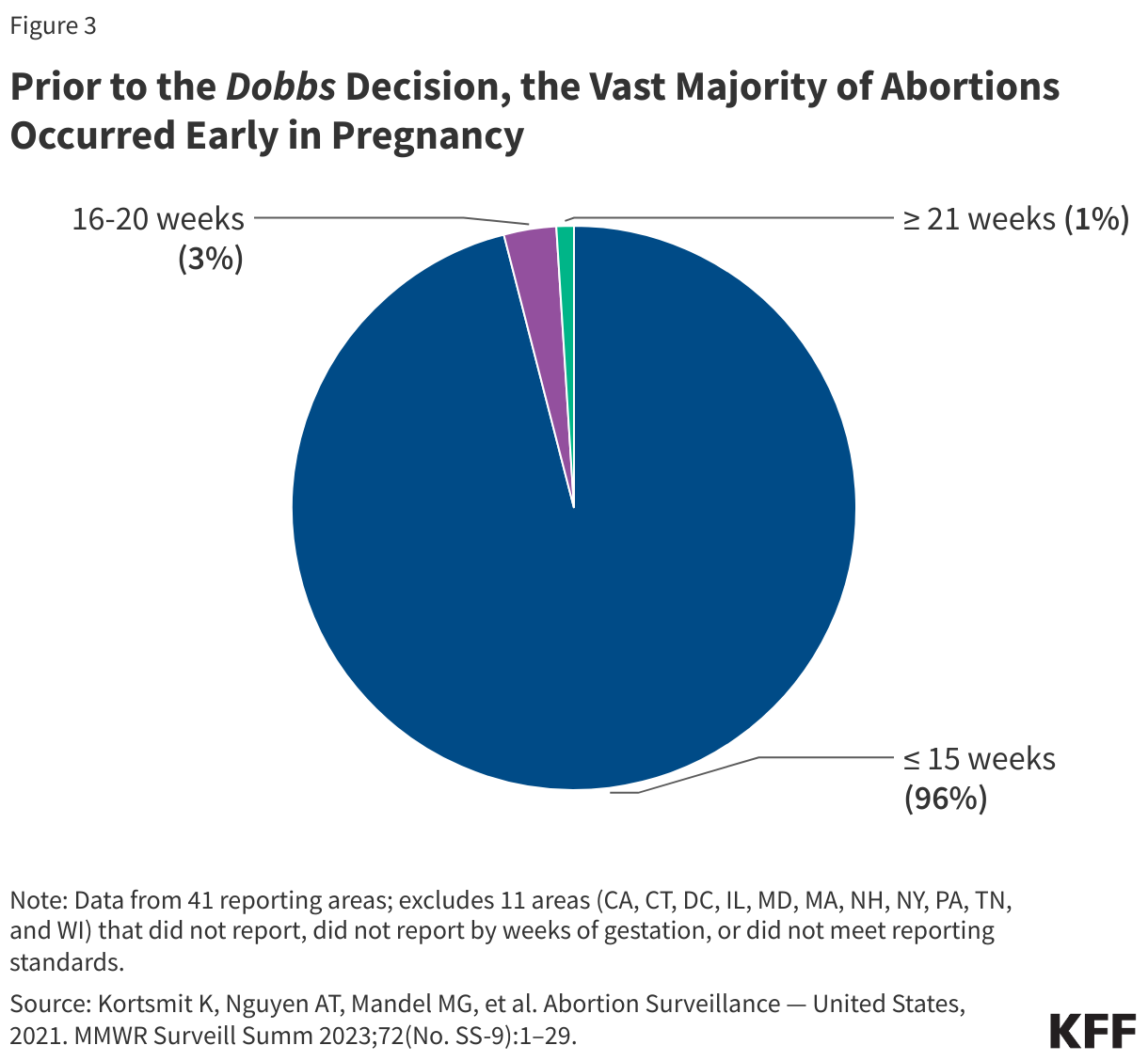
Abortions occurring at or after 21 weeks gestation are rare. According to the CDC’s Abortion Surveillance Data for 2021, prior to the Dobbs decision, the vast number of abortions (96%) occurred at or before 15 weeks gestation, while 3% occurred from 16 to 20 weeks gestation, and just 1% of abortions were performed at or after 21 weeks (Figure 3). This amounts to approximately 4,100 abortions per year occurring at or after 21 weeks. However, this estimate only includes the 41 reporting areas that report abortions to the CDC by gestational age and excludes major states such as California and New York. The percentage of abortions occurring at or before 13 weeks gestation has remained stable over the last few decades at 91-92%, however within this timeframe, more abortions are occurring earlier in pregnancy, at or before 9 weeks. This is likely in part due to the greater availability of medication abortions over the last two decades.
The CDC does not elaborate on the breakdown by gestational age for abortions occurring past 21 weeks, but it is likely that the vast majority occur soon after 21 weeks rather than much later in the pregnancy. While very limited contemporary data exists on this issue, a study from 1992 estimated 0.02% of all abortions occurred after 26 weeks gestation (320 to 600 cases per year).
Preliminary findings from a study on abortion provision since the Dobbs decision has found that patients living in states where abortion is banned or restricted have experienced increased delays in obtaining abortion care, in part due to arranging out-of-state travel to states where abortion is legal and limited appointment availability in abortion clinics in states where abortion is legal. Out-of-state travel for abortion services doubled in the first half of 2023 compared to the first half of 2020, likely driven by the overturning of Roe. Delays in accessing abortion services push people who want an abortion further along in their pregnancies, which could lead to an increase in the share of people who need abortions later in pregnancy.
In addition, even if patients can travel to a different state to access later abortion services, there are a few clinicians who provide abortions later in pregnancy. This was the case even before the Dobbs decision. Researchers from Advancing New Standards in Reproductive Health (ANSIRH) found that in 2023, 60 clinics provided abortions at or after 24 weeks and five clinics provided services at or after 28 weeks, meaning that most individuals in need of abortions later in pregnancy often have to travel significant distances to find an available and trained provider.1 A University of California San Francisco study found that compared to before Dobbs there was a slight increase in the number of abortion clinics that provide abortions after 24 weeks after the Dobbs ruling. Abortions at this stage also typically require two days to complete with inpatient care, as opposed to outpatient or at-home management that is possible earlier in pregnancy. Some facilities in the U.S. perform abortions later in pregnancy as outpatient procedures (up to certain gestational ages), but it is less common than offering inpatient care for these cases.
Why do people have abortions later in pregnancy?
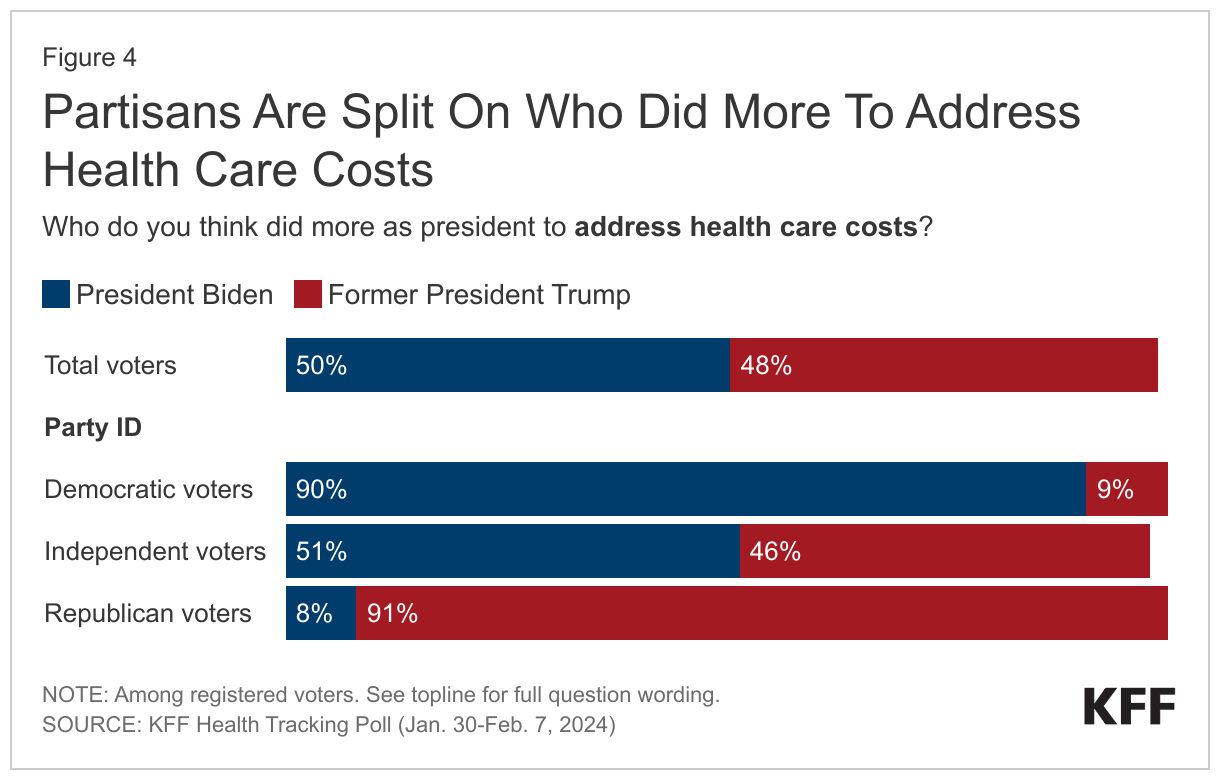
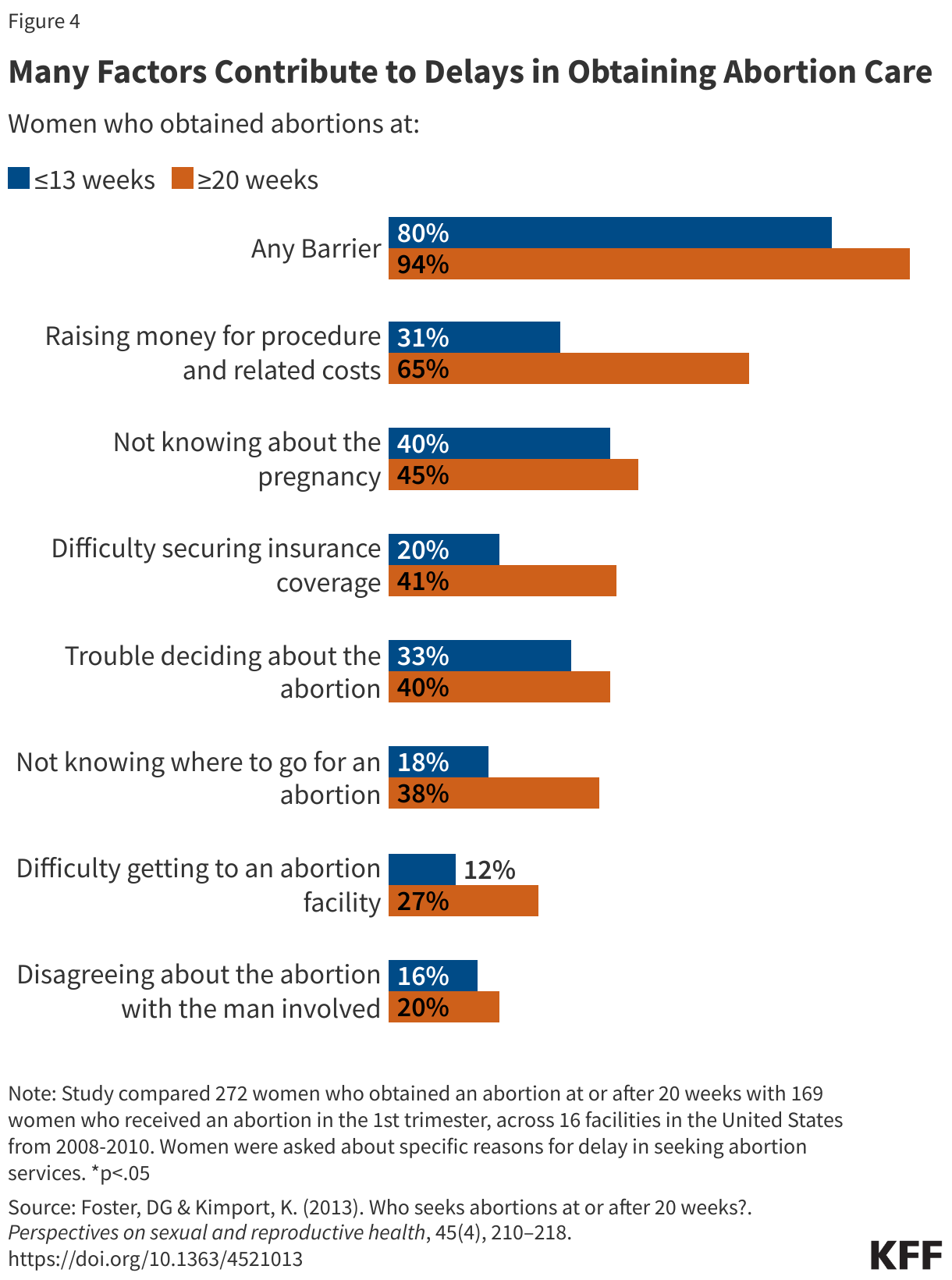
Individuals seek abortions later in pregnancy for a number of reasons. As part of the Turnaway study out of the University of California San Francisco, from 2008-2010 over 440 women were asked about why they experienced delays in obtaining abortion care, if any (Figure 4). Almost half of individuals who obtained an abortion after 20 weeks did not suspect they were pregnant until later in pregnancy, and other barriers to care included lack of information about where to access an abortion, transportation difficulties, lack of insurance coverage and inability to pay for the procedure. A 2022 study of patients seeking abortions later in pregnancy found that they fell into two categories: either they had learned new information about their pregnancies that made them no longer desirable, such as not finding out they were pregnant until very late in the pregnancy or the emergence of serious fetal or their own health issue; or experiencing barriers to abortion services earlier in the pregnancy that force them to delay the abortion until the third trimester.
Delays Stemming from Financial Barriers to Abortion Access: Abortions can be cost-prohibitive for many; a study examining abortion costs in 2021 found that the median out-of-pocket self-pay costs for medication abortion services was $568, $625 for first trimester procedural abortions, and $775 for second trimester procedural abortions (range $465 to $2,885). These costs do not account for lodging and transportation costs, loss of work or childcare costs, which can drive the price higher. Third trimester abortion costs can range from a couple thousand dollars to over $25,000, depending on how far along the pregnancy is and how clinically complex it is. The Federal Reserve Board found 32% of U.S. adults do not have enough in savings to pay for a $400 emergency expense, meaning many individuals may need to delay having an abortion until they can raise the necessary funds.
Fetal Anomalies: Individuals also seek abortions later in pregnancy due to medical reasons. With medical advances, many genetic fetal anomalies can be detected early in pregnancy; for example, chorionic villus sampling can diagnose Down Syndrome or cystic fibrosis as earlier as 10 weeks gestation. Structural fetal anomalies, however, are often detected much later in pregnancy. As part of routine care, a fetal anatomy scan is performed around 20 weeks, which entails ultrasound imaging of all the developing organs. Many structural anomalies are discovered at this time that would not have been apparent previously. A proportion of these are lethal fetal anomalies, meaning that the fetus will almost certainly die before or shortly after birth, meaning the fetus may be nonviable (consensus does not always exist as to which anomalies are fatal, and thus nonviable). In these cases, many individuals wish to terminate their pregnancies, rather than risk carrying the pregnancy until the fetus or newborn passes away. Very often these pregnancies are desired, making this decision exceedingly difficult for parents. Inadequate data exist to know how many abortions later in pregnancy occur due to fetal anomalies, but a study by Washington University Hospital showed almost all women whose fetuses had lethal fetal anomalies chose to terminate their pregnancies. Three (Alabama, Indiana and West Virginia) of the fourteen states with abortion bans and five states with early gestational bans (Florida, Georgia, North Carolina, South Carolina, and Utah) currently have exceptions for pregnancies with lethal fetal anomalies, but it is unknown whether any abortions under these exemptions have occurred. Among the states with viability or near viability bans, Delaware, Maryland, Massachusetts and New Hampshire have exemptions for fetal anomalies. Pregnant people who reside in states where abortion is banned and with no fetal anomaly exceptions who are unable to travel out of state can be forced to carry their pregnancies to term and deliver infants who are stillborn or die shortly after birth.
A 2011 survey of maternal fetal medicine (MFM) doctors—specialists who manage pregnancies with fetal anomalies— found most agreed that termination of pregnancy due to a lethal fetal anomaly should be allowed in all circumstances (76%). The majority (75%) discuss abortion as a management option soon after diagnosing a lethal fetal anomaly, but services for terminating pregnancies in these scenarios are limited. Even over decade before the Dobbs decision, only 40% of MFM doctors worked at healthcare centers offering abortions past 24 weeks for lethal fetal anomalies. An additional 12% knew of available services <50 miles away.
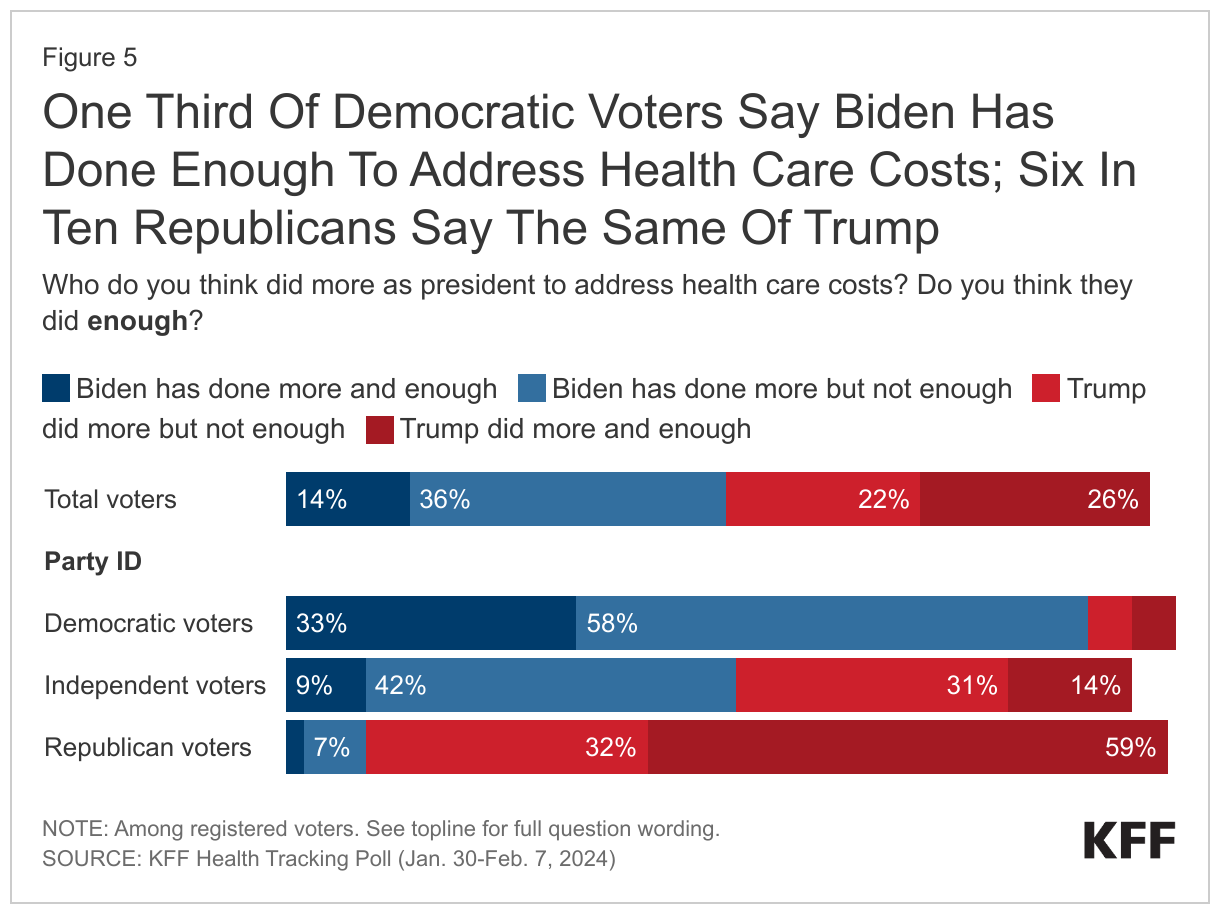
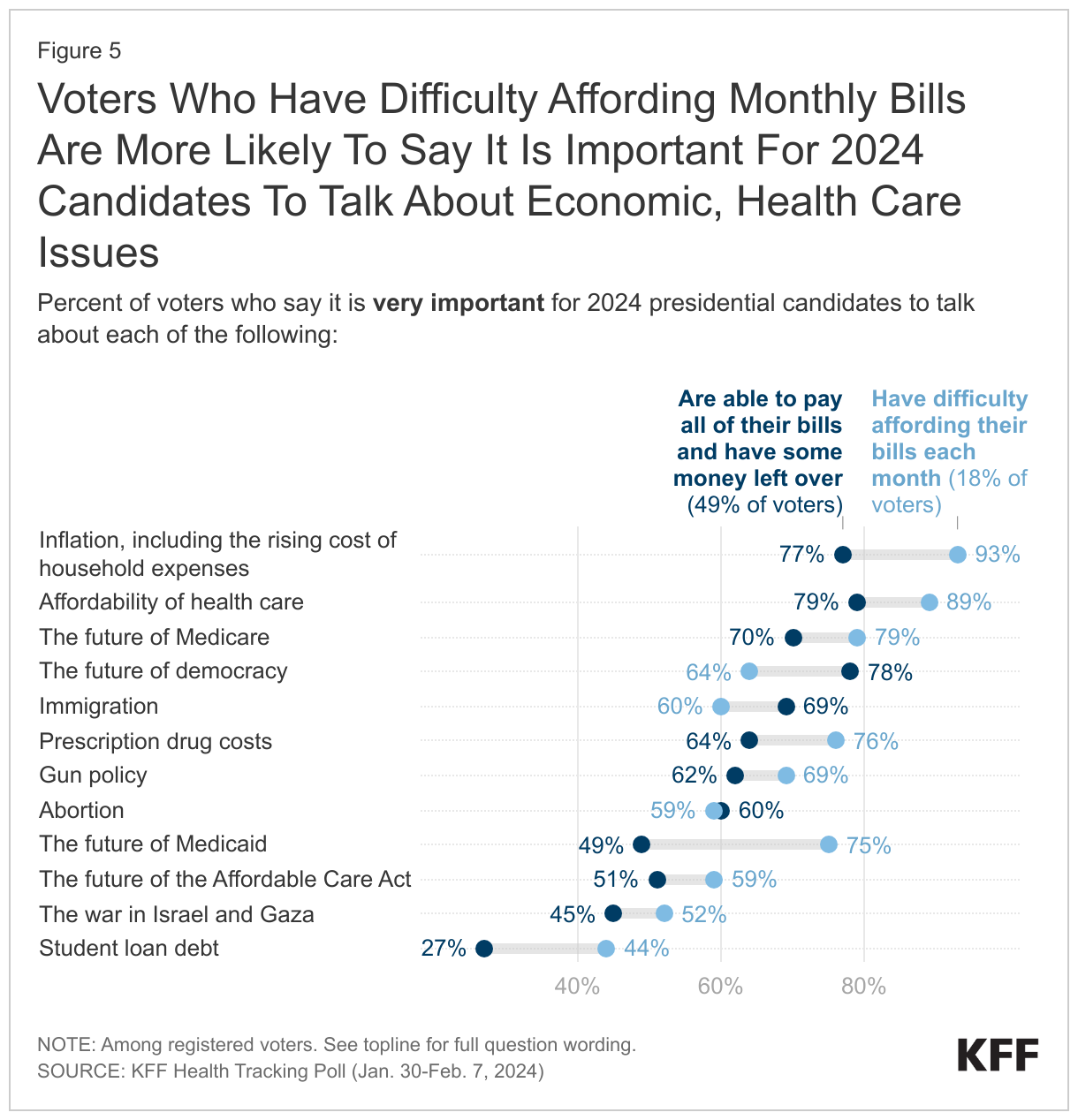
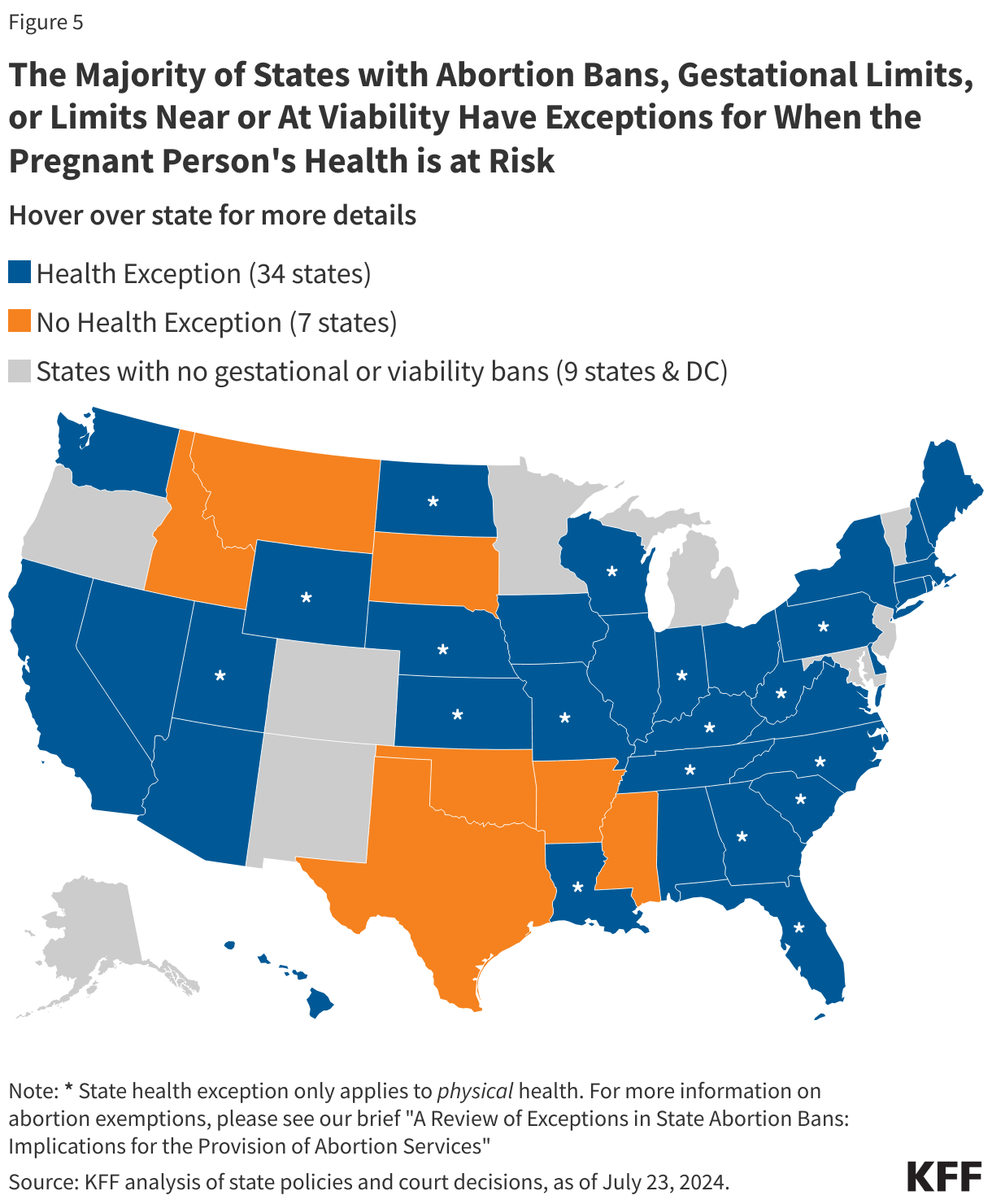
Health Risk to the Pregnant Person: Life threatening conditions may also develop later in pregnancy. These include conditions like early severe preeclampsia, newly diagnosed cancer requiring prompt treatment, and intrauterine infection (chorioamnionitis) often in conjunction with premature rupture of the amniotic sac (PPROM). If these conditions occur in a state where abortion is legal, the pregnant individual may pursue termination of pregnancy to preserve their own health. All states that ban abortion, have gestational bans, or limit abortion at or near viability, have exceptions allowing for abortions to occur when the life of the pregnant person is in danger, and 34 states have exceptions for when the health of the pregnant person is at risk (Figure 5). Former President Donald Trump reportedly supports a 16-week national abortion ban with exceptions for when the life of the pregnant person is in danger and in cases for rape or incest, but the 16-week national ban would not have an exception for when the health of the pregnant person is at risk. It is likely that a ban such as this would be structured so that it would limit abortions in states that currently permit abortions later in pregnancy, but allow states with abortion bans or gestational restrictions to keep their laws in effect.
The legal standards states use to determine when a pregnant person qualifies for a life or health exception can be ambiguous, with some standards leaving physicians in a legally vulnerable position that allow a prosecutor to bring an expert witness to contradict the physician’s medical judgment. In a recent case out of Texas, Kate Cox, a pregnant women seeking an abortion, sought a court order that would have allowed her to have an abortion under the exceptions to the Texas abortion ban. Fearing prosecution for providing abortion care that she believed it fit under the abortion ban’s exception based upon her good faith medical judgement, Ms. Cox’s physician asked a Texas District Court to determine that providing the abortion was not a violation of the state’s ban. While the District Court agreed with the plaintiffs that the case qualified for an exception, the Texas state Attorney General wrote a letter to the hospital stating that his office would still enforce the state abortion ban if abortion care was provided. Consequently, the Texas Supreme Court overruled the lower district court, finding that the physician’s “good faith belief” was insufficient to qualify for the exception, and only abortions that are certified to be necessary under the “reasonable medical judgement” standard are allowable under Texas law.
In states where abortion is banned, there have been questions and confusion about how ill a pregnant person must be for an abortion under a health exception to be performed. There are reports of patients having health complications that are not life threatening at the moment they are seeking care, and being sent home and subsequently developing serious complications that do threaten their lives as a result. In Idaho, Indiana, Tennessee, and Texas, physicians and people who were denied abortion care despite facing pregnancy complications that jeopardized their health have filed lawsuits regarding harms experienced as a result of the lack of health exceptions in their respective state abortion bans. They are asking for courts to clarify the scope of the state bans’ health exceptions and for physician judgment in making determinations about abortion as a medical treatment for emergent conditions to be granted greater deference.
In July 2022, the Department of Health and Human Services (HHS) issued guidance regarding the enforcement of EMTALA (Emergency Medical Treatment and Active Labor Act), the law that requires hospitals that take Medicare enrolled patients to perform appropriate medical screening examination to any patient who presents at the emergency department and to provide stabilizing care to patients identified as having an emergency medical condition. The 2022 guidance clarifies that hospitals and physicians have obligations to provide stabilizing care, including abortion in medically appropriate circumstances, when a patient presenting at an emergency department is experiencing an emergency medical condition. Since the guidance was issued, HHS has sued the state of Idaho for their abortion ban, which did not contain exceptions for health, and the state of Texas has sued to block enforcement of the guidance in Texas. The two federal district courts that have considered this issue have reached opposite decisions. In Texas, a federal district court blocked HHS from enforcing the EMTALA guidance in Texas and the Biden administration has appealed this decision to the 5th Circuit Court of Appeals. In Idaho, a federal district court issued a temporary stay blocking part of the Idaho ban, which was also stayed by the 9th Circuit Court of Appeals. However, in January 2024, the Supreme Court of the United States agreed to hear the Biden Administration’s challenge to the Idaho abortion ban and allowed Idaho’s ban to be fully in effect while the litigation is ongoing.
Have states taken action to expand access to abortions later in pregnancy?
Recognizing that access to abortions later in pregnancy can be a health preserving or life-saving medical service to a small group of pregnant people, yet very difficult to access, a few states have sought to expand access to abortions later in pregnancy. The New York Reproductive Health Act enacted in January 2019 expanded protections for abortion providers and pregnant individuals who have abortions after 24 weeks in cases of health or life endangerment or lethal fetal anomalies. In May 2023, Minnesota repealed its viability ban and in July 2023, Maine enacted L.D. 1619, allowing abortions after viability anytime a doctor deemed them medically necessary. Previously the law only allowed abortions after viability if the pregnant person’s life was in danger.
The authors would like acknowledge Gabriela Weigel, MD, former KFF-UCSF Fellow, who co-authored the 2019 version of this brief.
The authors would like to acknowledge Jennifer Karlin, MD, PhD (University of California, San Francisco) for her review of an earlier version of this brief.
Appendix