KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
This Visualizing Health Policy infographic examines state policies related to abortion and their intersection with clinical practice. Nine of 10 reported abortions in the United States are in the first trimester. Between 2003 and 2012, the abortion rate decreased 18% among women aged 15 to 44 years. Twenty-five states have laws that restrict insurance coverage of abortion in private plans. Twenty-seven states require women seeking abortion to wait 18 hours or more before obtaining an abortion, and several require women to be counseled on topics unsupported by medical consensus or evidence, such as abortion raising the risk of breast cancer. Many states have specific requirements for clinics and physicians who provide medication abortions, with 37 mandating that only a licensed physician dispense the abortion pill. Twenty-three states have laws that impose a jail sentence on physicians if they perform abortions past certain state-established gestational limits.
This Visualizing Health Policy infographic examines state policies related to abortion and their intersection with clinical practice. Nine of 10 reported abortions in the United States are in the first trimester. Between 2003 and 2012, the abortion rate decreased 18% among women aged 15 to 44 years. Twenty-five states have laws that restrict insurance coverage of abortion in private plans. Twenty-seven states require women seeking abortion to wait 18 hours or more before obtaining an abortion, and several require women to be counseled on topics unsupported by medical consensus or evidence, such as abortion raising the risk of breast cancer. Many states have specific requirements for clinics and physicians who provide medication abortions, with 37 mandating that only a licensed physician dispense the abortion pill. Twenty-three states have laws that impose a jail sentence on physicians if they perform abortions past certain state-established gestational limits.
EpiPen is a brand-name epinephrine auto-injector product, used in the event of a severe allergic reaction. It is a reliable, easy-to-use medical device that delivers a life-saving drug. In 2007, Mylan acquired EpiPen from Merck. At the time, the product had a list price of $94. Since then, Mylan has steadily increased EpiPen’s price, listing the product at $608 in summer 2016.1 The price increases have led to public debate, particularly among people who pay the full or a sizeable share of the full list price. However, the effect of EpiPen’s high list price goes beyond individual consumers. Medicare spending before rebates on EpiPen has grown substantially over the 2007-2014 period outpacing the growth in the number of Part D EpiPen users.2
Covering over 70 million people, a large portion of which is children, Medicaid is also a major provider of EpiPen and has been impacted by its increasing price. In this Data Note, we examine utilization, spending before rebates, and spending per prescription of EpiPen and other epinephrine auto-injectors before rebates in the Medicaid program. This analysis does not take into account drug rebates, as that data is proprietary.
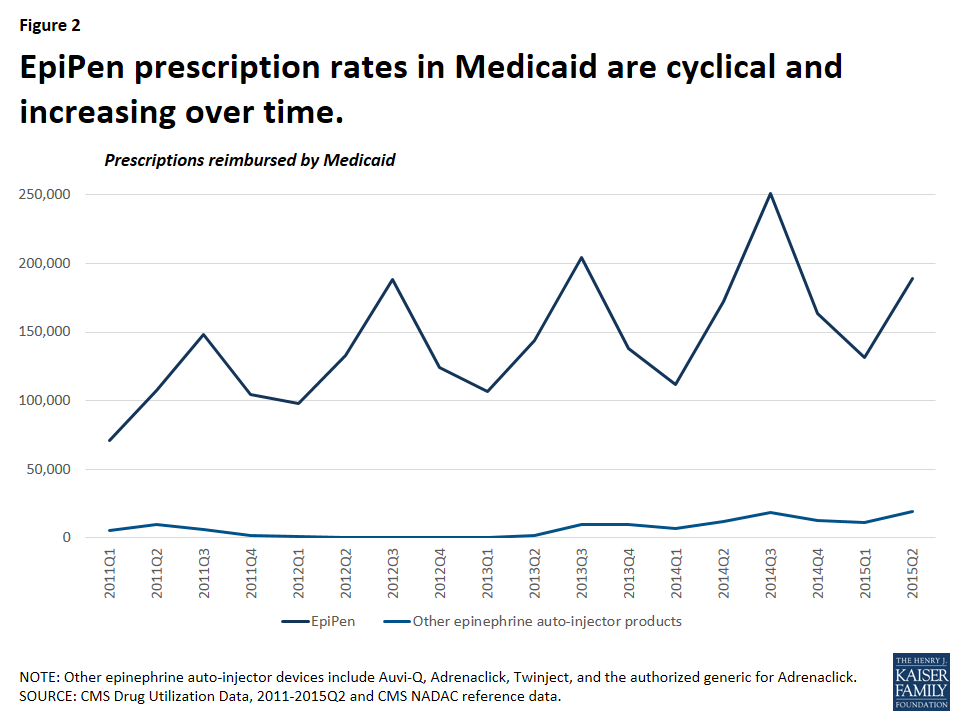
EpiPen dominated the Medicaid epinephrine auto-injector market.
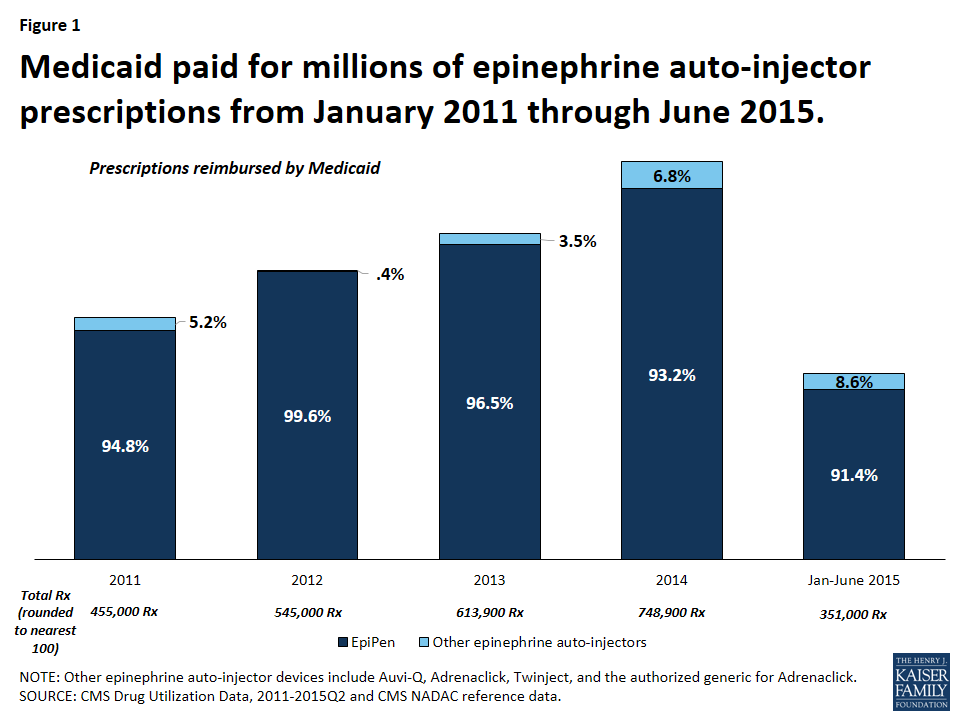
It is not surprising that Medicaid is a major provider of epinephrine auto-injector products, as the program covers over 30 million children.3 From January 2011 through June 2015, Medicaid reimbursed 2.7 million epinephrine auto-injector prescriptions, an average of nearly 600,000 per year.4 Mylan dominated the epinephrine auto-injector market over this period with 95 percent of these reimbursed prescriptions being for EpiPen (Figure 1). At this time, EpiPen’s only competitor in the epinephrine auto-injector market is Adrenaclick’s authorized generic.5 Adrenaclick and its authorized generic provide the same drug, epinephrine, at the same dosage as EpiPen, but through a different type of auto-injector device. A pharmacist cannot automatically substitute either Adrenaclick or the Adrenaclick authorized generic for a prescription for EpiPen.6 In 2013, Sanofi launched another epinephrine auto-injector, Auvi-Q, which is captured in this analysis. However, Sanofi voluntarily recalled the product in October 2015 after problems with the dosing of the drug. Between 2011 and 2015, prescriptions for EpiPen have grown. Within each year, EpiPen prescription rates are cyclical, peaking from July to September each year (Figure 2). Parents of children with severe allergies tend keep epinephrine auto-injectors both at home and at school. Additionally, EpiPen has a shelf life of 18 months, but is usually replaced annually.7 These two factors generate an increase of prescriptions at the start of the school year. Mylan has increased the list price of EpiPen in May or July each year since 2011, just before this annual spike in EpiPen prescriptions.8
Figure 1: Medicaid paid for millions of epinephrine auto-injector prescriptions from January 2011 through June 2015.Figure 2: EpiPen prescription rates in Medicaid are cyclical and increasing over time.
Medicaid spending before rebates per EpiPen prescription has increased over 200% in four years.
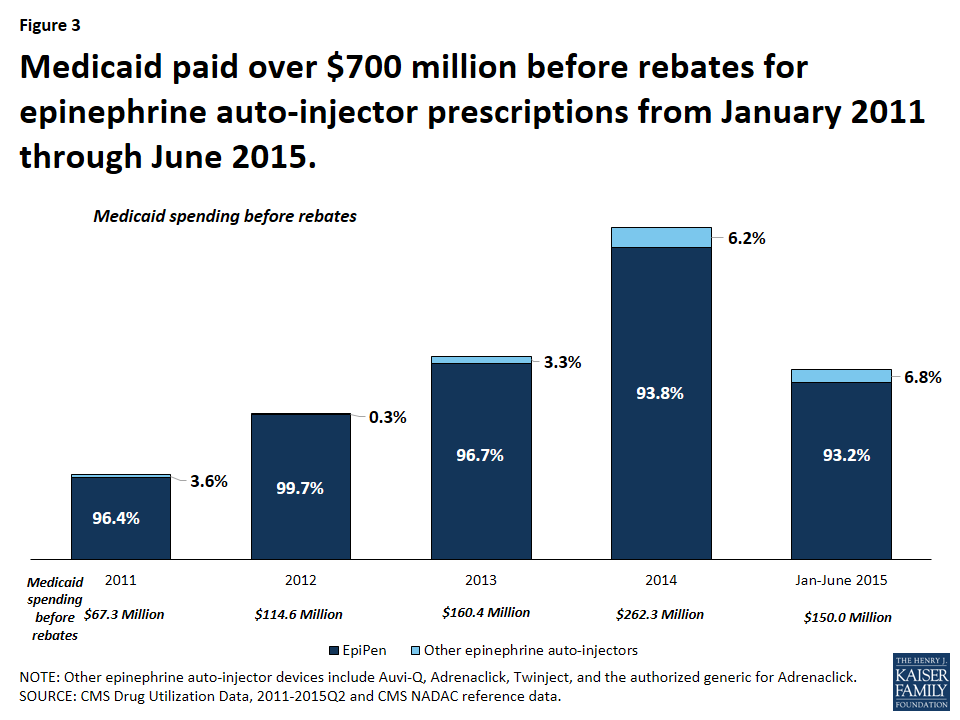
From January 2011 through June 2015, Medicaid paid over $720 million before rebates for EpiPen and nearly $754 million before rebates for all epinephrine auto-injectors (Figure 3). This accounts for 0.4% of all Medicaid outpatient drug spending over the period.9 From January through June of 2011, Medicaid paid $24.5 million before rebates for EpiPen prescriptions. Four years later, from January through June of 2015, Medicaid paid $139.7 million before rebates for EpiPen prescriptions, an increase of over 450%. In comparison, Medicaid outpatient drug spending over this period increased 38%.
Figure 3: Medicaid paid over $700 million before rebates for epinephrine auto-injector prescriptions from January 2011 through June 2015.
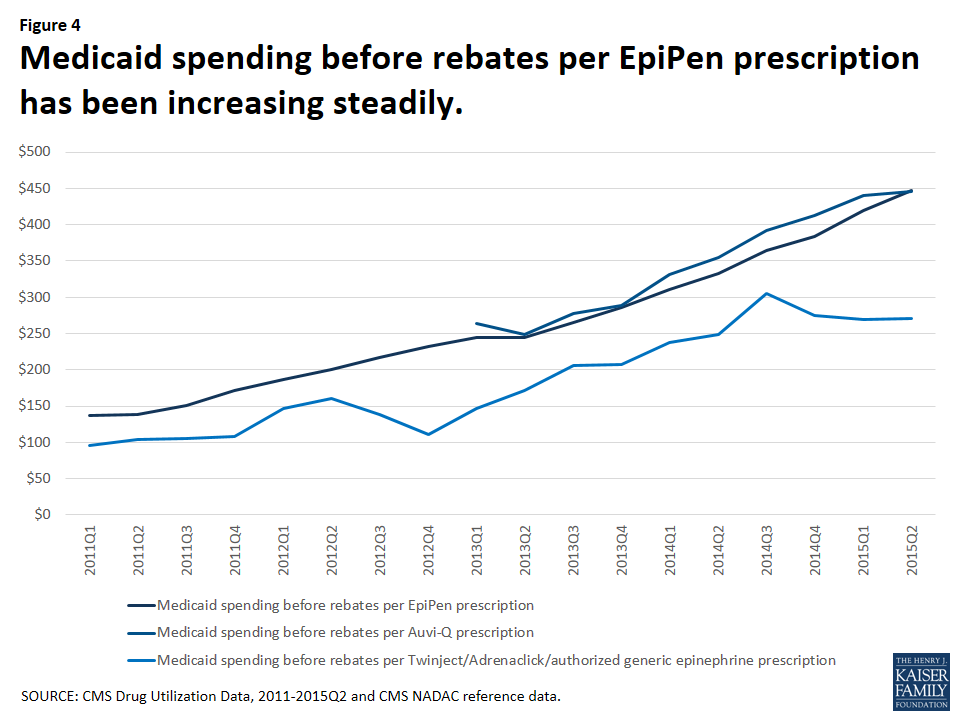
The increase in Medicaid’s spending on EpiPen reflects both the increased number of prescriptions as well as the increased amount Medicaid paid per prescription over this period. In the first quarter of 2011, Medicaid paid an average of $137 before rebates per EpiPen prescription. By the second quarter of 2015, the most recent period for which we have data, Medicaid paid an average of $447 before rebates per EpiPen prescription, reflecting an increase in spending per prescription of 227%.
Much attention is being given to the EpiPen price increases. However, over the January 2011 through June 2015 period, Medicaid spending before rebates on EpiPen prescriptions has not always been higher than other competitors in the field. In fact, from the second quarter of 2013 through the second quarter of 2015, Medicaid paid comparable amounts before rebates per prescription for Auvi-Q (Figure 4). Because rebates are proprietary, we are unable to account for their impact on overall Medicaid spending or on spending per prescription.
Figure 4: Medicaid spending before rebates per EpiPen prescription has been increasing steadily.
Reports have recently surfaced that Mylan has been paying rebates to the states as if EpiPen were a generic product and in an October 5th letter to Senator Ron Wyden, ranking member of the Senate Finance Committee, CMS confirmed this.10 All manufacturers are required to enter into a rebate agreement with the Secretary of HHS to secure Medicaid reimbursement. Rebates for brand drugs are larger than rebates for generic drugs. Additionally, rebates for brand drugs take into account when brand drug prices increase faster than inflation, but rebates for generic drugs do not.11 Thus, although we can see that Medicaid spending per prescription between Auvi-Q and EpiPen was comparable before rebates, we do not know how rebates have affected this.
Policy Implications
Medicaid provides coverage for a diverse population, a large share of whom are children, many of whom require epinephrine. However, as the number of prescriptions for the product, as well as the spending per prescription has been rising in recent years, overall spending on the product has been ballooning. To the extent that Medicaid can control its outpatient prescription drug spending, it is able to do so in large part through the Medicaid Drug Rebate Program. Additionally, state Medicaid programs are better able to acquire supplemental rebates when there is competition in the drug class.12 As policy makers discuss the effect of high EpiPen prices, this analysis shows that Medicaid is a major provider of the drug, and that the Medicaid program is bearing the high cost of the product.
Methodology
In this analysis, we used CMS State Utilization Data from 2011 through 2015 quarter 2, the most recent period for which data for all states are available. We downloaded this data from the CMS website in February 2016. In its letter to Senator Ron Wyden, CMS published annual spending and spending per prescription for EpiPen and other epinephrine auto-injector products from 2011 through the end of 2015. However, CMS has not yet made public all of the raw data files underlying these calculations in the second half of 2015. Our analysis largely aligns with the CMS analysis. We identified all epinephrine auto-injectors on the market by compiling a list from the final and draft NADAC weekly reference data and CMS Drug Product data. We estimated data by averaging the surrounding quarters in certain states for given quarters that through this and previous analysis13 we had determined unreliable.
Table 1: Medicaid Spending and Utilization of Epinephrine Auto-injector Products
NOTE: “N/A“ indicates that Auvi-Q was not on the market during this time. It was voluntarily removed from the market in October 2015, after the period of analysis.SOURCE: CMS State Drug Utilization Data 2011- 2015Q2, NADAC final and draft reference data and CMS Drug Product data used to identify epinephrine auto-injector NDCs.
Several health insurers, including United Healthcare and Aetna, are scaling back their participation in the Affordable Care Act (ACA) health insurance marketplaces, and in some cases exiting the broader individual market, due to substantial losses in these markets. A commonly cited reason for these losses is a sicker-than-expected risk pool, meaning that on average enrollees in this market may have been sicker or higher-cost than insurers expected or priced for. There are a number of related factors that could contribute to losses for insurers in the individual and exchange markets, including competition to offer a low-cost plan and lower-than-expected benchmark premiums, changes to risk corridors payments, and some insurers having less effective cost control than their competitors.
It is also possible that state policy decisions – in particular, on Medicaid expansion and allowing transitional (“grandmothered”) plans to continue for a period of time – have had an effect on the risk pool in the private individual market. A recent Health and Human Services Assistant Secretary for Planning and Evaluation (ASPE) brief finds that premiums were lower in states that expanded Medicaid, controlling for demographics and other factors. In states without Medicaid expansion, a sizable share of marketplace enrollees would have been enrolled in Medicaid had their state expanded the program, and it is possible these enrollees had greater health needs and higher costs than higher-income marketplace enrollees. In addition, a recent report from Milliman suggests that marketplace insurers in states that allowed transitional plans to continue in 2014 were less profitable than insurers in states that did not allow transitional plans to renew. In these states, transitional plan holders (generally expected to be healthier than the average enrollee because they were subject to medical underwriting by insurers prior to 2014) were not added to the individual risk pool, perhaps resulting in a sicker-than-expected individual market risk pool.
To gauge whether individual market risk pools are healthier in states that have expanded Medicaid and did not allow transitional plans, this data note compares average state risk scores using data from the Centers for Medicare & Medicaid Services Summary Report on Risk Adjustment for the 2015 benefit year. We find that states that expanded Medicaid and did not allow transitional plans had lower average risk scores, suggesting the risk pools in those state’s markets are healthier than in non-expansion states and in states that allowed transitional plans.
How Medicaid Expansion Could Affect the Risk Pool
Generally, marketplace subsidies are available to people with incomes between 100% and 400% of the federal poverty level (FPL), but actual subsidy eligibility varies depending on the state’s decision whether or not to expand Medicaid.
In states that opted to expand the program, Medicaid coverage is available to households with incomes up to 138% of poverty. In these states, marketplace subsidies are therefore available to people with household incomes between 138% and 400% of poverty. (In certain cases, such as legal immigrants who have been in the U.S. for less than five years and are therefore ineligible for Medicaid, some people with incomes below 138% of poverty may still receive marketplace subsidies in these states.)
As of July 2016, 19 states have decided not to expand Medicaid. Individuals living in non-expansion states must meet state eligibility requirements for Medicaid, which can be quite limited and many people fall into a “coverage gap,” meaning their incomes are too high for Medicaid yet too low for subsidies. In these states, marketplace subsidies are available to enrollees with incomes between 100% and 400% of poverty. Therefore, many people with household incomes between 100% and 138% of poverty are enrolled in the marketplace in non-expansion states, whereas they would be enrolled in Medicaid had their state expanded the program.
As a result, many more low-income individuals are in the private individual market risk pool in non-expansion states. A recent ASPE analysis estimates that individuals with incomes between 100% and 138% FPL make up close to 40% of the Marketplace population in non-expansion states, versus 6% in expansion states. Because low-income individuals, on average, report having worse health than those with higher incomes, this may lead to a sicker, and thus costlier, individual market risk pool in states that have not expanded Medicaid.
How Transitional Plans Could Affect the Risk Pool
Transitional coverage – also referred to as “grandmothered” coverage – includes plans that were purchased in the four years after the enactment of the ACA but before the beginning of the first open enrollment period in October 2013. Following controversy over these plans being cancelled because they did not comply with new insurance market rules taking effect in 2014 under the ACA, the Obama Administration issued guidance that ultimately permitted these plans to remain in effect until December 31, 2017. However, the federal rules granted discretion to states and individual insurers, so transitional plans were not allowed to continue in all cases. In 2015, 13 states did not allow transitional plans to continue. In the states that did allow transitional plans to continue, the ultimate decision was left to issuers whether to renew transitional policies. All transitional plans will be phased out by the end of 2017.
Transitional plans are non-ACA compliant and transitional policy holders are not considered a part of the individual risk pool under the ACA. In states that did not allow transitional plans to renew, transitional plan holders were obligated to switch to ACA-compliant plans. Because transitional plan holders may be healthier on average than the population in the ACA individual risk pool (because they were pre-screened by insurers before the ACA prohibited insurers from denying coverage based on pre-existing conditions), bringing these enrollees into the individual market could have resulted in a healthier, and less costly, individual market risk pool in states that did not allow transitional plans to continue.
Gauging the Effect of Medicaid Expansion and Transitional Policies on State Risk Scores
Under the ACA’s risk adjustment program, individualrisk scores – based on the individual’s age, sex, and diagnoses – are assigned to each enrollee in individual and small group market plans. Health plans with relatively low average risk scores (and thus “healthier” enrollees) make payments into the system, while plans with relatively high average risk scores (“sicker” enrollees) receive payments.
For this analysis, we compared states’ average individual market risk score for the 2015 benefit year based on state decisions to expand Medicaid and to allow transitional plans. The state average plan liability risk score (state risk score) is the weighted average risk score across all plans in the state’s individual marketplace. Higher state risk scores are associated with sicker state risk pools. The difference in risk scores between states likely translates as a difference in average premiums. In states with higher average risk scores (“sicker” enrollees), insurers will likely need to set higher premiums to account for higher expected health costs.
In our analysis, we compare the average state risk score across three groups (see Table 1):
Medicaid Expansion, Non-Transitional States: states that expanded Medicaid and did not allow transitional plans to continue in 2015 (11 states)
Medicaid Expansion, Transitional States: states that expanded Medicaid and allowed transitional plans to continue in 2015 (15 states)
Non-Expansion, Transitional States: states that did not expand Medicaid and allowed transitional plans to continue in 2015 (22 states)
Note: All states that did not expand Medicaid allowed transitional plans through 2015 –in other words, there were zero non-expansion, non-transitional states.
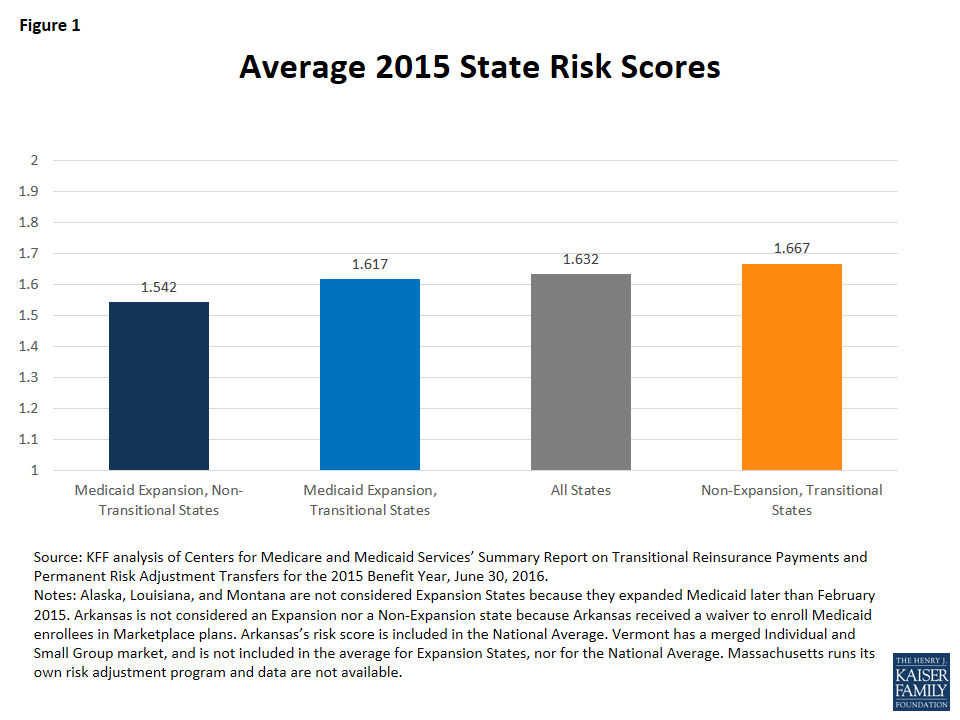
We find that in 2015 the average risk score across non-expansion, transitional states (1.667) was 3% higher than the average risk score across Medicaid expansion, transitional states (1.617) and 8% higher than Medicaid expansion, non-transitional states (1.542) (Figure 1). This trend was consistent in the 2014 benefit year as well. This suggests that, on average, non-expansion states have sicker risk pools than expansion states, and expansion states that allowed transitional plans have sicker risk pools than expansion states that did not allow transitional plans. This relationship is not necessarily causal, nor are states’ decisions on Medicaid expansion and transitional plans the only factors that could explain differences between these groups of states. For example, it is possible that non-expansion, transitional states have sicker-than-average populations overall, regardless of income. Risk scores can also be influenced by new enrollment (as new enrollees may not have a well-documented medical history, states with larger shares of new enrollees in 2015 may have lower risk scores) and similarly by new insurers (as new entrants with less experience may lack the ability to adequately code diagnoses, states with inexperienced plans may have lower average risk scores). However, it is possible that state policy decisions may have affected the insurance risk pool.
Figure 1: Average 2015 State Risk Scores
Risk scores in Medicaid expansion, non-transitional states ranged from a low of 1.344 in California to a high of 1.785 in Delaware. Meanwhile risk scores in Medicaid expansion, transitional states ranged from a low of 1.369 in Colorado to a high of 1.798 in Kentucky. In non-expansion, transitional states, state average risk scores range from lows of 1.416 in Montana and 1.455 in Utah to a high of 1.990 in Wisconsin in 2015 (Table 1). In states that allowed transitional plans to continue through 2015, the ultimate decision whether to renew transitional policies was left to issuers. In at least one transitional state (Montana), all individual market carriers ultimately decided to discontinue transitional policies in 2015 and switch to ACA-compliant plans. Montana’s state risk score is the lowest of the non-expansion states at 1.416, which is consistent with the general finding that states without transitional plans on average had lower risk scores. If we were to exclude Montana from our analysis, the average risk score for non-expansion, transitional states would increase from 1.667 to 1.693.
For the purpose of this analysis we do not include Arkansas as either a Medicaid expansion state or a non-expansion state because the state expanded Medicaid through a “private option” waiver, thereby enrolling all newly eligible Medicaid enrollees in marketplace plans. Arkansas also allowed transitional plans in 2015. Arkansas has the highest average risk score of all states at 2.08, which is consistent with the general finding that states that expanded Medicaid through traditional means (without a private option waiver) on average had lower risk scores.
Table 1: State Average Plan Liability Risk Scores for the 2015 benefit year
Medicaid Expansion States
Non-Expansion States
Private Option States
Transitional States
Colorado
1.369
Montana*
1.416
Arkansas*
2.075
North Dakota
1.395
Utah
1.455
New Hampshire
1.418
Nebraska
1.463
Oregon
1.445
Wyoming
1.515
Arizona
1.584
Maine
1.537
Iowa
1.587
Idaho
1.539
Illinois
1.603
Virginia
1.541
New Jersey
1.626
Alaska*
1.575
Michigan
1.674
Georgia
1.613
Indiana
1.728
South Dakota
1.616
Ohio
1.756
Texas
1.658
Hawaii
1.756
Kansas
1.681
West Virginia
1.760
Florida
1.699
Pennsylvania
1.762
Oklahoma
1.716
Kentucky
1.798
North Carolina
1.725
Average
1.617
Missouri
1.734
South Carolina
1.762
Mississippi
1.786
Louisiana*
1.816
Alabama
1.909
Tennessee
1.924
Wisconsin
1.990
Average
1.667
Non-Transitional States
California
1.344
District of Columbia
1.359
Minnesota
1.413
Washington
1.451
Connecticut
1.516
Maryland
1.547
New Mexico
1.559
Nevada
1.559
Rhode Island
1.702
New York
1.731
Delaware
1.785
Average
1.542
National Average: 1.632
SOURCE: KFF analysis of CMS Summary Report on Transitional Reinsurance Payments and Risk Adjustment Transfers for the 2015 Benefit Year, June 30, 2016.*NOTES: Alaska, Louisiana, and Montana are not considered Expansion States because they expanded Medicaid later than February 2015. Arkansas is not considered an Expansion State nor a Non-Expansion state because Arkansas received a waiver to enroll Medicaid enrollees in Marketplace plans. Arkansas’s risk score is included in the National Average. Vermont has a merged Individual and Small Group market, so we do not include the state’s risk score in our calculation of the average for Expansion States, nor for the National Average. Massachusetts runs its own risk adjustment program; data not available.
Discussion
There is some evidence that state decisions on Medicaid expansion and transitional plans have affected the state individual market risk pools. Namely, individual market risk pools may be “sicker” in states that have not expanded Medicaid and allowed transitional plans to continue. Transitional plans will be phased out in all states by the end of 2017, likely leading to some improvement in the individual market risk pool. States will continue to have discretion over whether to expand Medicaid. It is important to keep in mind that a number of demographic and policy factors, apart from Medicaid expansion and transitional policy, may explain why non-expansion states have sicker risk pools than expansion states on average. For example, it is possible that regardless of income non-expansion states have sicker average populations than states that did expand Medicaid. While this analysis does not attempt to control for any demographic factors, and does not prove a causal relationship between the state’s decisions and health of the state’s risk pool, it does suggest that state policy decisions may have had a noticeable effect on risk pools.
Methods
This analysis uses data from the Centers for Medicare and Medicaid Services’ Summary Report on Risk Adjustment for the 2015 benefit year. Appendix A of the report includes a state-by-state table of states’ average plan liability risk score (state risk score) for 2015. For the purpose of this analysis, we calculated the un-weighted average state risk score across three groups: 1) Medicaid expansion, non-transitional states (states that had expanded Medicaid by February 1, 2015 and did not allow transitional plans to continue into 2015); 2) Medicaid expansion, transitional states (states that had expanded Medicaid by February 1, 2015 and allowed transitional plans to continue in 2015), and 3) non-expansion, transitional states (states that had not expanded Medicaid by February 1, 2015 and allowed transitional plans to continue in 2015). All non-expansion states chose to allow transitional plans through 2015 – in other words, there were no non-expansion, non-transitional states. We calculated the simple average of state risk scores across these three groups of states. Since the focus of this analysis is on the effect of state decisions independent of the size of the state’s individual risk pool, we did not weight the group averages by billable member months. Compared to simple averages, weighted averages by billable member months show the same if not a stronger effect of state decisions on Medicaid expansion and transitional plans on the average state risk pool. Table 1 shows the state risk scores for the 2015 benefit year.
This analysis defines Medicaid expansion and non-expansion states using Kaiser Family Foundation’s report on the current status of state action on the Medicaid expansion decision. We consider states that expanded Medicaid before February 1, 2015 to be “expansion” states. For the purpose of this analysis we do not group Arkansas with expansion or non-expansion states because Arkansas expanded Medicaid through a “private option” waiver, thereby enrolling all newly eligible Medicaid enrollees in marketplace plans. Arkansas’s risk score is included in the national average. Two other states, New Hampshire and Iowa, received similar waivers, however, New Hampshire did not begin enrolling Medicaid expansion enrollees on exchange until 2016 and Iowa started phasing out this practice in 2014.
State decisions on whether to allow transitional plans were obtained from an Association of Health Insurance Plans (AHIP) map of state responses to administration policy on individual and small group coverage extensions. For the purpose of this analysis, we consider states that allowed transitional policies to continue in the individual marketplace through December 31, 2015 to be “transitional” states. In states that allowed transitional plans to continue through 2015, the ultimate decision whether to renew transitional policies was left to issuers. In at least one transitional state (Montana), all individual market carriers ultimately decided to discontinue transitional policies in 2015 and switch to ACA-compliant plans. Since the focus of this analysis is the effect of state policy decisions rather than carrier decisions, we consider Montana a transitional state.
This analysis excludes Vermont and Massachusetts. Vermont has a merged Individual and Small Group Market. Massachusetts ran its own state risk adjustment program in 2015 and data are not available.
While health care has not been central to the 2016 Presidential campaign, the election’s outcome will be a major determining factor in the country’s future health care policy. A number of issues have garnered media attention, including the future of the Affordable Care Act (ACA), rising prescription drug costs, and the opioid epidemic.
Hillary Clinton and Donald Trump have laid out different approaches to addressing these and other health care issues. Central among these is their position on the future of the ACA. Hillary Clinton would maintain the ACA, and many of her policy proposals would build on provisions already in place. Donald Trump, in contrast, would fully repeal the ACA, and although his policy proposals and positions do not offer a full replacement plan, they do reflect an approach based on free market principles.
See where the candidates stand on seven key health policy issues.
Health Insurance Coverage and Costs
The Affordable Care Act (ACA) set new standards for virtually all private health plans, including a prohibition on pre-existing condition exclusions and a requirement for private plans to extend dependent coverage to the age of 26. The law also established new marketplaces for the sale of nongroup insurance to all individuals except undocumented immigrants, and created new subsidies for nongroup coverage. New fees, taxes, and offsetting budget savings were adopted to finance ACA subsidies and reduce the deficit, including a so-called “Cadillac tax” on high-cost employer-sponsored plans. The Congressional Budget Office (CBO) estimated repeal of the ACA would increase the federal deficit by $137 – $353 billion over 10 years (2016-2025). Since enactment, the uninsured rate has fallen to 8.6% and an estimated 20 million Americans have gained coverage, while 27 million remain uninsured. Public opinion about the ACA remains divided, largely on partisan lines. Several issues have emerged in the 2016 campaign.
Key Issues
Affordability of premiums and cost sharing. Under ACA, refundable premium tax credits (APTCs) subsidize the cost of marketplace policies for people ineligible for affordable group coverage at work or public programs and who have income between 100% and 400% of the federal poverty level (FPL). These APTCs protect individuals from the full cost of coverage in the marketplaces; however, bigger premium increases proposed for 2017 are a concern. An estimated 6.1 million people are ineligible for APTCs because of the so-called “family glitch,” in which the definition of affordable group coverage takes into account the cost of self-only coverage even if adding dependents to the job-based plan is not affordable.
The ACA also offers cost sharing subsidies for marketplace participants with income between 100% and 250% FPL, and requires all new private plans to limit cost sharing for covered benefits to more than $7,150 for self-only coverage in 2017. Affordability of cost sharing pre-dates the ACA and continues to be a challenge. Under job-based group plans since 2010, annual deductibles have risen almost three time as fast as premiums and about seven times as fast as wages and inflation. One in five insured Americans struggle to pay medical bills. Health plan cost sharing is the leading factor contributing to medical debt among the insured. Out-of-network medical bills also contribute significantly; and 7 in 10 people who could not afford bills from out-of-network providers were unaware the provider was not in their plan network when they received care. Such bills are sometimes called surprise medical bills.
Enrollment in high-deductible plans continues to grow, a trend that predates the ACA. Enrollees in such plans can often open health savings accounts (HSAs) to defray cost sharing and could deduct HSA contributions. HSAs can transfer tax free to heirs who are spouses, but are otherwise subject to income tax upon the account holder’s death.
Marketplace enrollment. In March 2016, 11.1 million individuals were enrolled in marketplace plans representing 40% of the population estimated eligible to enroll in marketplace plans, though enrollment varies by state. If all states enrolled at the average rate of the top ten highest performing states (that together have enrolled 59% of eligible consumers) marketplace enrollment could be nearly 50% higher. Affordability continues to be the major reason that the uninsured lack coverage, but lack of awareness about the ACA is also a factor. Although Marketplaces are required to provide in-person consumer assistance, as the third open enrollment period ended, two-thirds of uninsured consumers polled were unaware the deadline was approaching and 80% said they had not been contacted by anyone about signing up for coverage.
Health plan choice and competition. The ACA requires all plans to provide standardized summaries of coverage to facilitate plan comparisons. Also to help consumers and regulators compare plan performance, the ACA requires all new private plans to disclose transparency data indicating how promptly claims are paid, how often they are denied, the availability and cost of in-network providers, and other measures. These transparency provisions have not yet been implemented.
Marketplaces were designed to encourage competition between health insurers. However, for 2017, some insurers have announced they will no longer offer plans on the marketplace, raising concerns about consumer access to a choice of plans and a reduction in competition, particularly in rural counties. Two-thirds of marketplace participants in urban counties will likely continue to have a choice of 3 or more insurance companies in 2017; by comparison, 41% of enrollees in rural counties will likely have a single insurer, up from 7% in 2016.
Where the Candidates Stand
Hillary Clinton. Hillary Clinton supports policies to maintain and build upon the ACA. She would increase premium subsidies in the marketplace so no participant is required to pay more than 8.5% of income for coverage. She would also fix the “family glitch” and allow people to buy coverage through the marketplace regardless of their immigration status. Hillary Clinton would make a public plan option available in every state and give people the option of buying into Medicare starting at age 55. She would invest $500 million annually in outreach and in-person assistance to enroll more uninsured in coverage, and she would enforce ACA transparency provisions. She would authorize the federal government to review and disapprove unreasonable health insurance premium increases in states that do not have such authority, and she would repeal the Cadillac tax. Hillary Clinton has also proposed new private plan standards to waive the annual deductible for at least three sick visits per year, limit monthly cost sharing for prescription drugs to $250, and protect against surprise medical bills when patients inadvertently receive care out of network. She has also proposed a new refundable tax credit of up to $5,000 to subsidize out-of-pocket health expenses (including premiums in marketplace plans) for all Americans with private insurance.
Donald Trump.
Donald Trump supports complete repeal of the ACA, including the individual mandate to have coverage. In lieu of requiring insurers to provide coverage to everyone regardless of health status, he would work with states to create high risk pools for individuals who have not maintained continuous coverage. In place of refundable premium tax credits, Donald Trump would provide a tax deduction for the purchase of individual health insurance. Donald Trump would promote competition between health plans by allowing insurers to sell plans across state lines; an insurer licensed under the rules of one state would be allowed to sell coverage in other states without regard to different state laws that might apply. Donald Trump would promote the use of Health Savings Accounts (HSA), and specifically would allow tax-free transfer of HSAs to all heirs. Donald Trump would also require price transparency from all hospitals, doctors, clinics and other providers so that consumers can see and shop for the best prices for health care procedures and other services.
Medicaid
Medicaid is the nation’s main public health insurance program for people with low incomes covering about 70 million Americans. Medicaid provides coverage for low income individuals and families with low or no out-of-pocket costs for care; assistance to low-income Medicare beneficiaries; coverage for long-term services and supports, and financing for safety-net hospitals, clinics and states. The two key Medicaid issues in the campaign focus around financing and the ACA Medicaid expansion.
Key Issues
ACA Medicaid Expansion. Effective January 1, 2014, ACA expanded Medicaid eligibility millions of non-elderly adults with income at or below 138% of the federal poverty level (FPL) – about $16,394 for an individual in 2016. The law also provided for 100% federal funding of the expansion through 2016, declining gradually to 90% in 2020 and future years. The Supreme Court ruling on the ACA in June 2012 effectively made the Medicaid expansion optional for states. As of September 2016, 32 states (including the District of Columbia) have implemented the ACA Medicaid expansion.
Financing. States administer their own Medicaid programs within federal requirements, and states and the federal government jointly finance the program. Under current law, federal Medicaid payments are guaranteed with no pre-set limit based on a formula set in statute that pays a larger share of program costs in poorer states. The financing structure allows states and the federal government to increase spending when there is increased demand or need (to respond to recessions, epidemics, emergencies or increases in medical or drug costs); however, it also makes federal financing more unpredictable and harder to control.
Where the Candidates Stand
Hillary Clinton. Hillary Clinton supports policies to maintain and strengthen the current Medicaid program and financing structure. Hillary Clinton would encourage and incentivize states to expand Medicaid by providing states with three years of full federal funding for newly eligible adults, whenever they choose to expand. Clinton would also continue to make enrollment easier and launch a campaign to enroll people who are eligible but not enrolled in coverage.
Donald Trump. Donald Trump supports a Medicaid block-grant and a repeal of the ACA (including the Medicaid expansion). He has said he would cover the low-income uninsured through Medicaid after repealing the ACA. The House Republican Plan, which is part of a larger package designed to replace the ACA and reduce federal spending for health care, would offer states a choice between a Medicaid per capita allotment or a block grant.
Medicare
Medicare is the nation’s health insurance program that provides coverage to 57 million seniors and younger adults with permanent disabilities. Four issues related to Medicare have emerged during the 2016 presidential campaign.
Key Issues
Premium support. Some have proposed changing the structure of Medicare to a system of premium supports under which Medicare would make a payment on behalf of each beneficiary which would be used toward the purchase of health insurance coverage — either traditional Medicare or a private plan. This proposal was frequently debated in the 2012 election, supported by Speaker Paul Ryan and included in the House Republican Plan.
Prescription drug costs.Rising drug costs, especially high-priced specialty drugs, have emerged as a significant issue for consumers, Medicare and other payers, leading to a number of proposals to slow cost increases.
Medicare buy-in for adults between the ages of 55 and 64. Allowing older adults to buy in to Medicare would provide another option for health insurance coverage, in addition to individual policies available to them in (or outside) the ACA Marketplaces.
Where the Candidates Stand
Hillary Clinton. Hillary Clinton supports maintaining the current structure of the Medicare program and opposes policies to transform Medicare into a system of premium supports. On the issue of prescription drug costs, Clinton supports allowing safe re-importation of drugs from other countries, allowing the federal government to negotiate drug prices in Medicare, especially for high-priced drugs with limited competition, and requiring drug manufacturers to provide rebates in the Medicare Part D low-income subsidy program equivalent to the rebates provided under Medicaid. Hillary Clinton does not support repealing the ACA or any of the Medicare provisions included in the law; rather, she supports expanding the law’s value-based delivery system reforms. On the issue of Medicare eligibility, Clinton has proposed to allow people ages 55 to 64 to buy into Medicare.
Donald Trump. Donald Trump has not stated his position on the issue of Medicare program restructuring or whether to allow older adults ages 55 to 64 to buy in to Medicare. Trump supports repealing the ACA, which would presumably mean repealing the law’s Medicare provisions. On the issue of prescription drug costs, Trump supports allowing safe re-importation of prescription drugs from other countries.
Prescription Drugs
Prescription drugs are the third largest area of U.S. health spending, and a main driver of growth. New drugs, which require significant research and development (R&D) investments, receive a period of patent protection and market exclusivity. Following this period, the Food and Drug Administration (FDA) may approve generic drugs, which perform the same as the brand name product, often at much lower costs. The Affordable Care Act (ACA) includes a provision to fast-track approval of “biosimilars,” which are drugs that perform similarly to an existing biologic drug (one derived from living organisms). Since 2010, more new specialty drugs have been approved than traditional drugs. Unlike traditional drugs, specialty drugs (which are often biologics) require special administration (such as injection) or close observation by a physician.
Out-of-pocket drug costs. Though most of the increase in drug spending was covered by insurance in 2014, out-of-pocket (OOP) spending on prescriptions also increased. In 2015, most people taking prescription drugs said they could afford their treatment, but about 1 in 4 people taking drugs have difficulty affording their medication.
Where the Candidates Stand
Hillary Clinton. To address drug prices, Hillary Clinton proposes to increase generic competition by prohibiting “pay-for-delay” deals whereby companies make payments to competitors for agreeing to delay market entry; increasing funding for the FDA Office of Generic Drugs to reduce their approval backlog; reducing the market exclusivity period for biologics; and directing the FDA to prioritize biosimilar drugs with few competitors. To address price increases for generic drugs, she proposes to establish consumer oversight in federal agencies; penalize drug companies for unjustified price increases; and allow importation of lower-cost drugs from countries with similar safety standards. She also supports eliminating tax deductions for direct-to-consumer advertising; requiring FDA approval of advertisements; tying federal support for drug companies to their investment in R&D; increasing transparency of the additional value new drugs have over existing treatments; and allowing Medicare to negotiate drug and biologic prices. To address OOP spending on prescriptions, Hillary Clinton proposes a $250 per month cap on cost sharing for covered drugs; and a rebate program for low-income Medicare beneficiaries that mirrors those in Medicaid.
Donald Trump. Donald Trump supports allowing importation of drugs from overseas that are safe and reliable but priced lower than in the U.S. He also supports greater price transparency from all health providers, especially for medical exams and procedures performed at doctors’ offices, clinics, and hospitals, but does not specify whether this policy would also apply to retail prescription drugs, which typically are not considered services or procedures.
The Opioid Epidemic
In recent years, the use of prescription painkillers for nonmedical purposes, as well as drugs derived from opium (such as heroin), has emerged as a major public health issue. In 2013, 1 in 20 nonelderly adults used opioids for nonmedical purposes. For one in five users (almost 2 million nonelderly adults), the nonmedical use of opioids increases to the level of opioid use disorder, often referred to as abuse, dependence, or addiction. Overdose deaths involving opioids have quadrupled since 1999, with over 14,000 individuals dying from opioid overdoses in 2014, leading to what many refer to as an “opioid epidemic.” The opioid epidemic creates an estimated $55 billion annually in societal costs, such as health care expenditures, workplace costs due to lost wages and utilization of sick days, and criminal justice costs. Proposed policy actions to address the opioid epidemic include efforts to change prescribing practices to curb utilization of opioids, improve access to treatment for individuals with opioid use disorder, and enforcing drug laws to combat access, sale and use of illicit drugs.
Where the Candidates Stand
Hillary Clinton. Hillary Clinton has released a $10 billion (over ten years) plan to fight drug addiction. The plan includes a federal-state partnership to support education and mentoring programs, development of treatment facilities and programs, efforts to change prescribing practices, funding to increase first responders’ access to naloxone, and criminal justice reform. Clinton’s plan also includes direct federal action to increase funding for inpatient and outpatient treatment options, change federal rules that prevent nurse practitioners and physician assistants from prescribing recovery medications, enforce federal parity standards, remove obstacles to Medicare and Medicaid payment for addiction services, and issue guidance on prioritizing treatment over incarceration for nonviolent and low-level federal drug offenders.
Donald Trump. Donald Trump has said he will stop of the flow of illegal drugs into the country by building a wall on the U.S.-Mexican border and closing shipping loopholes that allow dangerous drugs to be mailed into the U.S. Donald Trump would also enhance access to addiction services, end Medicaid policies that obstruct inpatient treatment, increase first responders’ access to naloxone, lift the cap on the number of patients that providers can treat with recovery medicines, and expand incentives for state and local governments to use drug courts and mandated treatment to respond to the addiction crisis.
Reproductive Health
Reproductive health is an essential element of women’s healthcare. The Affordable Care Act (ACA) greatly expanded coverage for these services for millions of women. Access and availability of abortion services and federal payments for contraceptive providers, however, have emerged as key issues in this year’s presidential election.
Key Issues
Preventive services. For women, a key provision of the ACA requires that all new private insurance plans and Medicaid expansion programs cover no-cost preventive services. The majority of these services are exclusively or primarily used by women, such as prescription contraception, STI counseling and testing, cancer screenings, a broad range of pregnancy-related screenings, and well-woman visits.
Publicly funded family planning. The Federal government has a long record of support for publicly funded family planning services through Medicaid and the Title X program. Planned Parenthood is a key participant in both of these programs. Recently, some states have attempted to remove Planned Parenthood from their Medicaid provider network. However, they have been blocked because the current federal law requires states to allow Medicaid beneficiaries to access family planning services from any participating provider of their choice.
Abortion. Starting with Roe v. Wade, the Supreme Court has defined a woman’s constitutional right to abortion. In 1980 the Court upheld the Hyde Amendment, which greatly restricts federal funding for abortion for millions of women enrolled in Medicaid as well as others covered by federal programs such as the military and Indian Health Service. In addition, many states have regulations that restrict access to abortion services. Most recently, the Supreme Court’s decision in Whole Women’s Health limited the state legislature’s ability to impose regulations on abortion clinics.
Where the Candidates Stand
Hillary Clinton. Hillary Clinton supports policies that protect and expand women’s access to reproductive healthcare, including affordable contraception and abortion. She defends the ACA’s policies, including no-cost preventive care and contraceptive coverage. She has promised to protect Planned Parenthood from attempts to defund it and would work to increase federal funds to the organization. She has also called for the repeal of the Hyde Amendment which she believes limits low-income women’s access to abortion care. She would appoint judges to the Supreme Court who support Roe v. Wade, ensuring a women’s right to choose an abortion.
Donald Trump. Donald Trump has called for defunding Planned Parenthood if they continue to provide abortion and would redirect their funding to community health centers. He states he is pro-life but with exceptions when the pregnancy is a result of rape, incest, and life endangerment. Trump has promised to appoint pro-life justices to the Supreme Court that seek to overturn Roe v. Wade. He would also work to make the Hyde Amendment permanent law and sign the Pain-Capable Child Protection Act, legislation that would sharply limit access to later term abortions. He would also repeal the ACA, which would eliminate minimum scope of benefits standards such as maternity care in individual plans and coverage of no-cost preventive services such as contraceptives in private plans.
Zika
Zika is a virus transmitted primarily by mosquitos; it can also be spread through sexual contact, from mother to child, and via blood transfusion. In 2015, Zika was reported for the first time in the Western Hemisphere. Zika infection during pregnancy has been linked to microcephaly and other serious birth defects. This link prompted the World Health Organization to declare a “public health emergency of international concern” earlier this year and the Centers for Disease Control and Prevention (CDC) to issue travel warnings to pregnant women and those seeking to become pregnant to avoid Zika-affected areas. The first cases of locally-transmitted Zika (from mosquito to human) in the U.S. were reported in Puerto Rico in December 2015. In July 2016, local transmission was reported in Miami, Florida.
Zika is the latest in a growing list of infectious disease outbreaks, joining HIV, SARS, H1N1, and Ebola, which have taken the world largely by surprise, raising challenging questions about how the U.S. and other countries can best anticipate and respond to these threats. With Zika, such questions have become political, particularly concerning funding as well as access to family planning and reproductive health services for women.
Key Issues
Funding for emerging disease threats. The U.S. currently has limited funding mechanisms available to respond to emerging disease threats and new Congressional appropriations are often needed or funding must be reallocated from other areas. Because of this, in February of this year, President Obama sent an emergency funding request to Congress for almost $1.9 billion to address Zika internationally and domestically (as it did with the Ebola outbreak in 2014). Congress has considered several bills to fund Zika, each of which provides significantly less funding than the President requested and includes other program and policy differences. To date, Congress has yet to approve any Zika funding, and the Administration is using funds from other areas, including Ebola, to address Zika.
Access to family planning and reproductive health services. Because the main public health concern related to Zika is the link between infection during pregnancy and birth defects, women’s access to family planning and reproductive health services is critically important and has become a contested issue in the Zika response. The Conference Agreement passed by the House placed a restriction on some of the funding for HHS, which some have argued would prevent funds from going to organizations that provide family planning and reproductive health services, and as a result, it has been opposed by Democrats in Congress.
Where the Candidates Stand
Hillary Clinton. Hillary Clinton supports emergency funding for Zika, and in March, called upon Congress to appropriate $1.8 billion in emergency funding. She supports the bipartisan Senate bill which passed in May and includes $1.1 billion in funding. She has stated that Congress should pass a bill “free of politics”. More broadly, Clinton has called for investment in public health preparedness including the creation of a Public Health Rapid Response Fund to address emerging disease threats like Zika.
Donald Trump. Donald Trump does not have a position on funding for Zika or on public health preparedness.
Election 2016: Side-by-side
Side-by-Side Comparison of the Candidates’ Health Care Positions
Hillary Clinton
Donald Trump
Position on the ACA
Maintain and build upon the ACA.
Repeal the ACA in its entirety. Repealing the law would rollback many changes to private health insurance, coverage through Medicaid and the marketplaces, preventive and women’s health services, and Medicare coverage and savings provisions.
Health Insurance Coverage and Costs
Insurance Premiums
Increase premium tax credits available through the Marketplaces so that individuals and families pay no more than 8.5% of their income on health insurance premiums.
Work with interested governors to establish a public option plan in their states using current flexibility under the ACA.
Create a fallback process that gives the Secretary of Health and Human Services the authority to modify or block unreasonable health insurance rate increases in states that do not have such authority.
Fix the “family glitch”.
Repeal the Cadillac tax.
Allow people to buy health insurance across state lines.
Work with states to establish high-risk pools for individuals who have not maintained continuous coverage.
Allow payments individuals make toward health care premiums to be tax deductible.
Out-of-Pocket Costs
Require plans to provide three sick visits per year that do not count towards deductibles.
Provide a new progressive refundable tax credit of up to $2,500 for an individual, $5,000 per family, for out-of-pocket costs (including marketplace premiums) in excess of 5% of income for insured individuals who are not eligible for Medicare or claiming existing deductions for medical costs.
Ensure consumers are required to pay no more than in-network cost-sharing for care received in a hospital in their plan’s network.
Enforce ACA transparency requirements; and require employers, providers, and insurers to provide more information about out-of-pocket costs, doctor networks, prescription drug costs, and other elements of health insurance so that consumers can make informed choices.
Allow people to enroll in tax-free Health Savings Accounts to pay for out-of-pocket costs, usable by all family members and inheritable without tax penalty.
Require price transparency from all health care providers to enable individuals to shop for the best prices on medical procedures.
Coverage for Immigrants
Allow families—regardless of immigration status—to buy insurance through the Health Insurance Marketplaces.
Outreach and Enrollment
Invest $500 million per year in a campaign to facilitate enrollment of eligible individuals into Marketplace coverage and Medicaid.
Medicaid
Medicaid Expansion
Encourage states to adopt the Medicaid expansion by allowing any state that expands Medicaid to receive a 100% federal match for the adult expansion population during the first three years, regardless of when the state chooses to expand.
Medicaid Financing
Maintain current Medicaid financing structure.
Transform Medicaid into a block-grant to states.
Medicare
Medicare Buy-in
Allow people age 55-64 to buy-in to Medicare.
Medicare Drug Prices
Allow Medicare to negotiate drug prices, especially for high-cost drugs with limited competition.
Require drug manufacturers to provide rebates in the Medicare low-income subsidy program that are equivalent to rebates in the Medicaid program.
Payment System Reform
Expand value-based delivery system reform in Medicare and Medicaid, and propose public-private efforts that incentivize employers and insurers to expand these payment models.
Opioids
Prevention
Focus on prevention by helping school districts implement age-specific drug abuse education programs and help communities develop peer and mentorship programs.
Treatment
Increase funding for the Substance Abuse Prevention and Treatment Block Grant by 15% to expand access to inpatient and outpatient treatment.
Create a state fund to help police, fire departments, and EMTs purchase naloxone, and ensure all first responders have access to it
Require licensed prescribers to meet training requirements and consult a prescription drug monitoring program before writing a prescription for controlled medications.
Direct the Department of Veterans Affairs and CMS to disseminate guidelines that identify treatments for pain management other than opioids.
Expand access to treatment slots.
Expand first responders’ and caregivers’ access to Narcan (naloxone).
Lift the cap on the number of patients that doctors can treat with recovery medications, provided they follow safe prescribing practices.
Insurance Coverage
Ensure enforcement of insurance parity laws between physical and behavioral health.
Reevaluate Medicare and Medicaid payment practices to remove obstacles to reimbursement and help integrate care for addiction into standard practice.
End Medicaid policies that obstruct inpatient addiction treatment.
Criminal Justice
Direct the Attorney General to issue guidance on prioritizing treatment over incarceration for nonviolent and low-level federal drug offenders.
Expand incentives for states and local governments to use drug courts and mandated treatment.
Prescription Drugs
Importation
Allow Americans to import drugs for personal use from foreign nations whose safety standards are as strong as those in the US.
Allow consumers access to imported, safe and dependable drugs from overseas.
Out-of-Pocket Drug Costs
Require health insurance plans to place a monthly limit of $250 on covered out-of-pocket prescription drug costs for individuals.
Generic Drugs and Biologics
Increase the availability of generic drugs by prohibiting “pay-for-delay” deals and by fully funding the FDA’s Office of Generic Drugs to clear out their generic drug approval backlog.
Lower the biologic exclusivity period from 12 to 7 years and direct FDA to give prioritized, expedited review to biosimilar applications with only one or two competitors in the marketplace.
Drug Prices
Eliminate corporate tax deductions for direct-to-consumer advertising; and require FDA approval of these advertisements.
Require pharmaceutical companies that benefit from federal support to invest a “sufficient amount” of revenue in research and development or pay rebates to support basic research.
Build on ACA provisions that use the results of private-sector analyses to hold drug companies accountable for justifying costs.
Women’s Reproductive Health
Reproductive Health
Protect a woman’s right to make personal health decisions and preserve access to affordable contraception, preventive care, and safe, legal abortions.
Oppose efforts to defund Planned Parenthood.
Repeal the Hyde Amendment.
Opposes abortion except to save the life of the woman or in the cases of rape or incest.
Supports laws that would limit access to later term abortions.
Defund Planned Parenthood.
Make Hyde Amendment permanent law.
Zika
Funding
Provide emergency funding for Zika.
Create a Public Health Rapid Response Fund to invest in public health preparedness and address emerging disease threats like Zika.
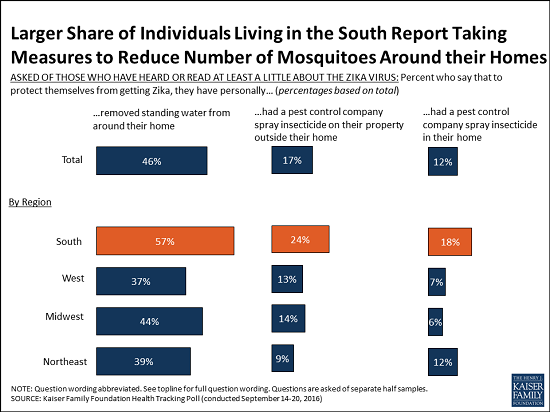
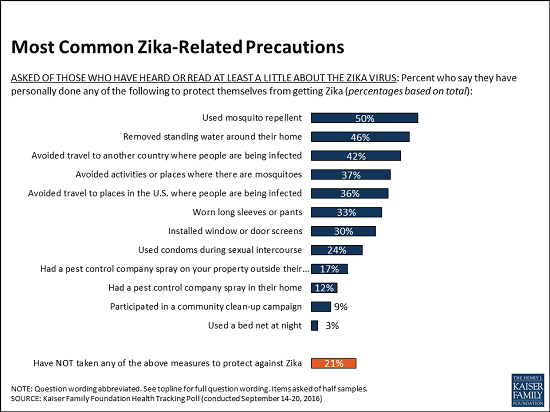
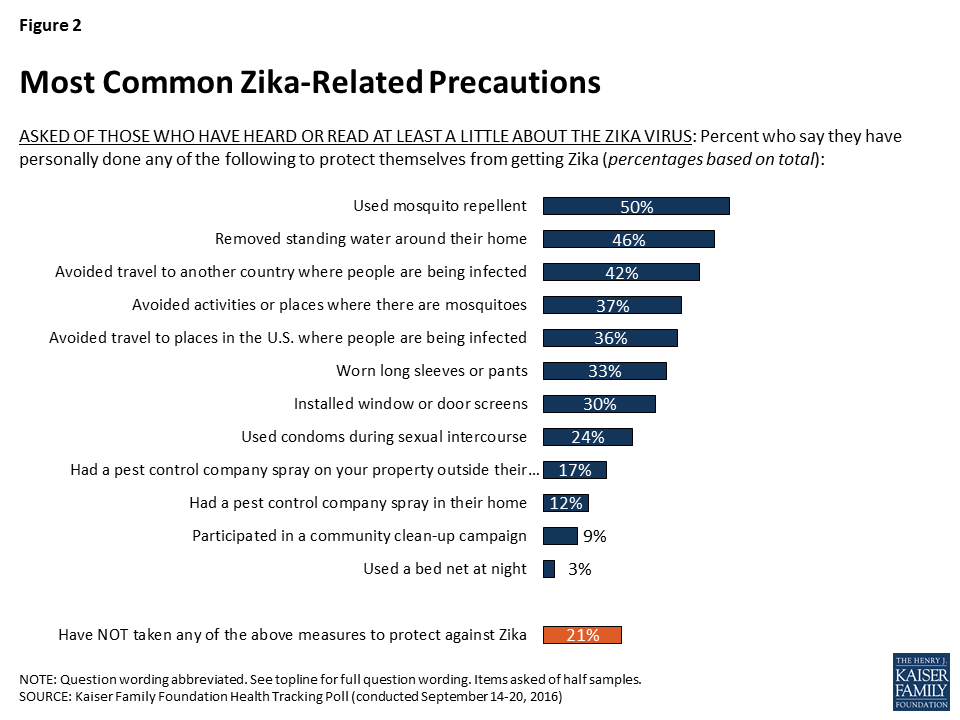
As part of the Kaiser Family Foundation’s ongoing efforts to track the public’s knowledge of the Zika virus outbreak and attitudes towards Zika-related issues, the September Kaiser Health Tracking Poll examines whether the public is taking precautions in order to protect themselves from getting Zika.
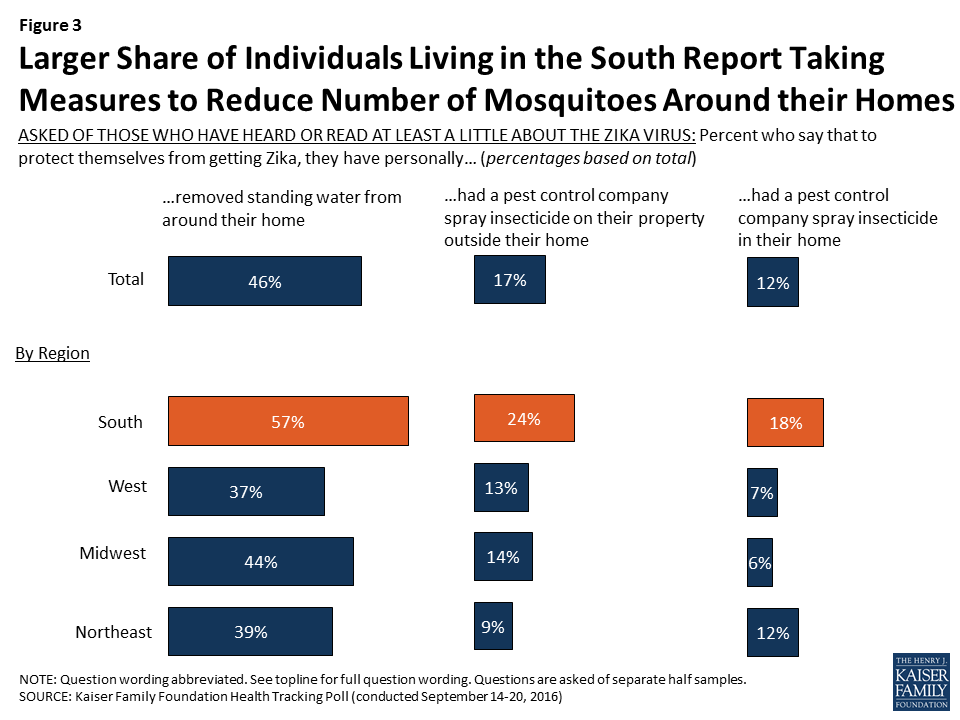
The poll finds people in the South are more likely to report taking action to reduce the number of mosquitoes in and around their homes. For example, a larger share of Southerners report that they removed standing water from around their home (57%) and that they had a pest control company spray outside their home (24%) than the share of residents in any other region of the country.
The survey finds that the most common precautions that Americans say they are taking are wearing mosquito repellent, removing standing water around their home, and avoiding travel to countries where people are being infected with the Zika virus by mosquitoes.
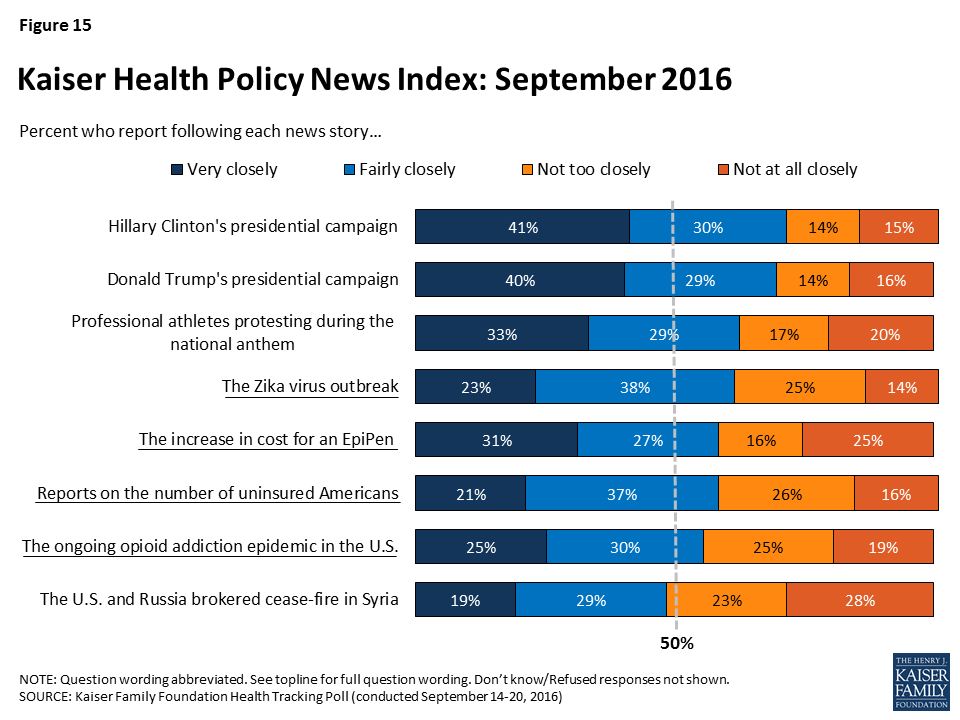
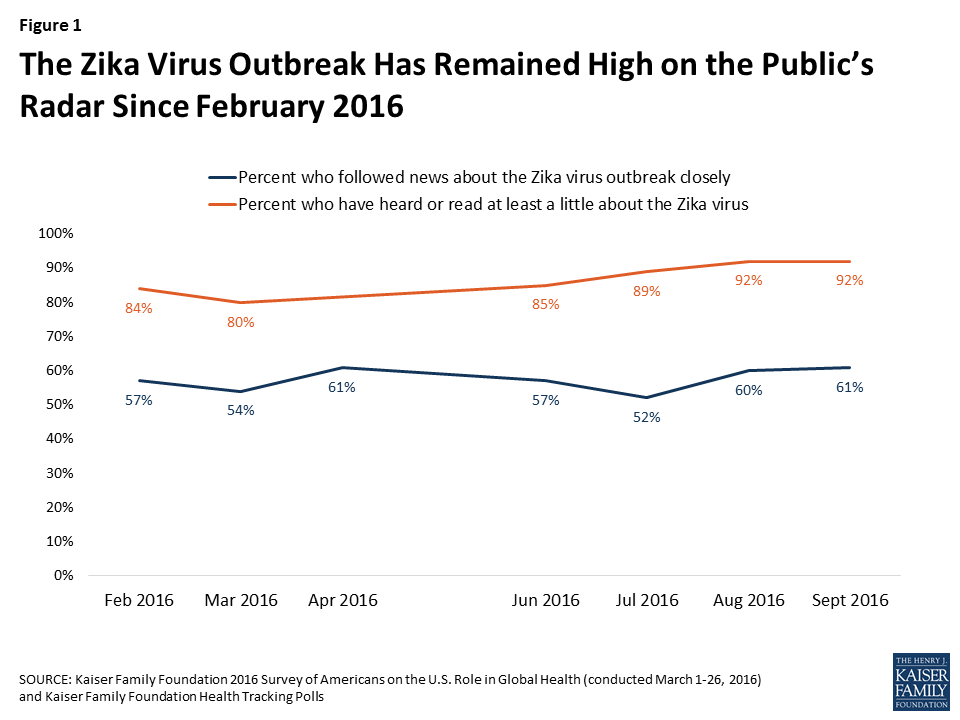
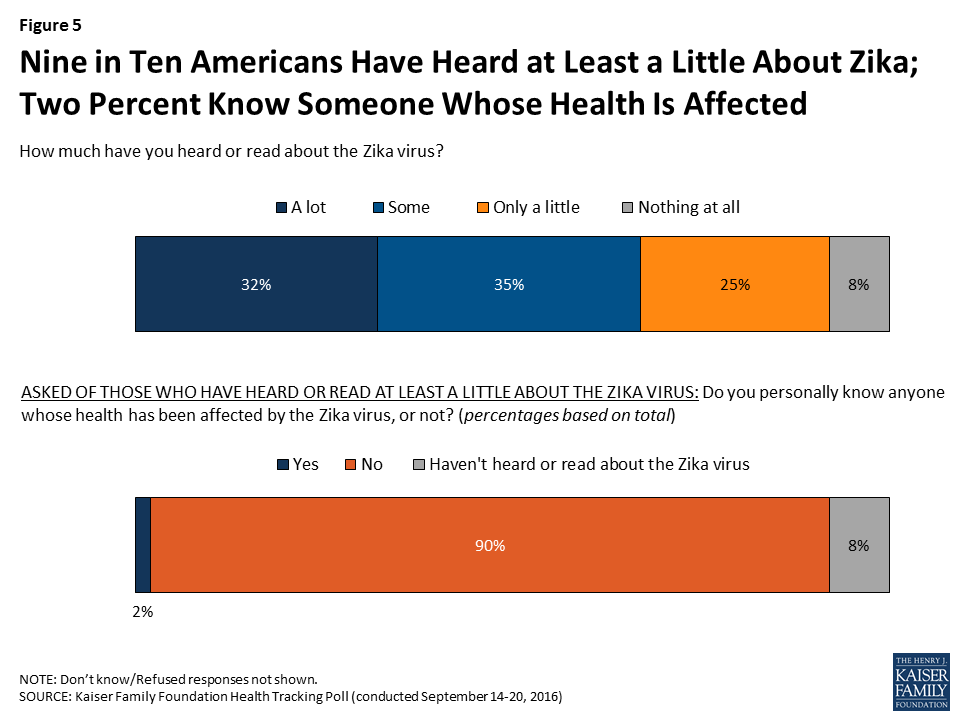
As in other recent months, the Zika virus outbreak is one of the top health policy news stories, with 61 percent of the public saying in September they were closely following news about it. While the vast majority of the public have heard or read at least a little about the virus, very few (2%) say they know anyone whose health has been affected by the virus, the poll finds.
Designed and analyzed by public opinion researchers at the Kaiser Family Foundation, the poll was conducted from September 14-20 among a nationally representative random digit dial telephone sample of 1,204 adults. Interviews were conducted in English and Spanish by landline (421) and cell phone (783). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
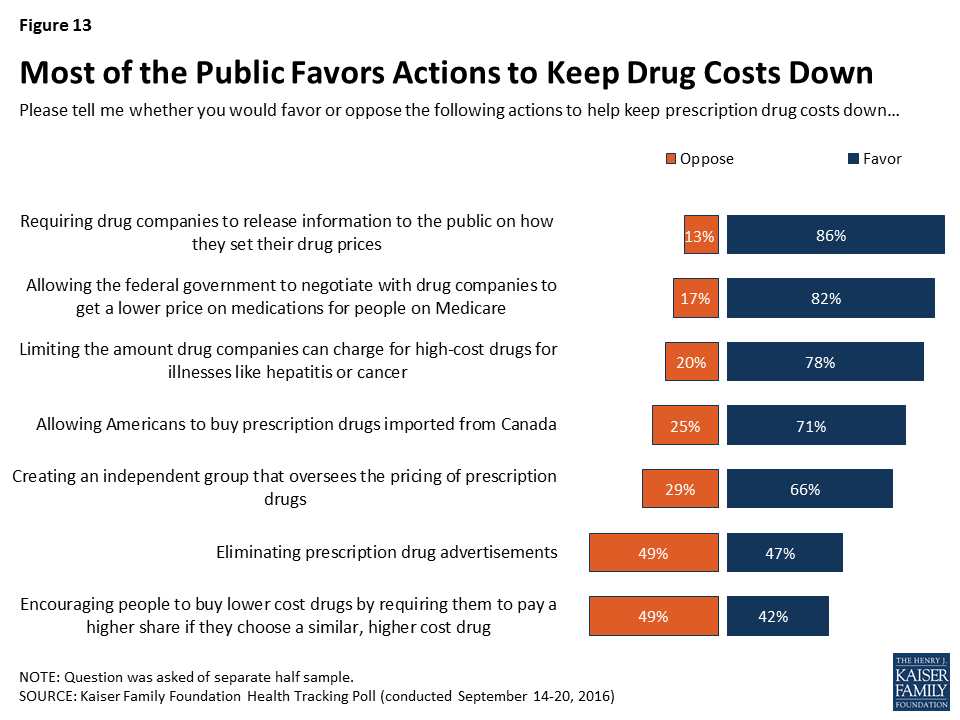
In the wake of the news about the increase in cost for the Epinephrine injection, the majority (77 percent) of Americans say prescription drug costs are unreasonable, up slightly from 72 percent a year ago. There is widespread support for a variety of actions in order to keep costs down including requiring drug companies to release information to the public on how they set their drug prices, allowing the federal government to negotiate with drug companies to get a lower price on medications for people on Medicare, limiting the amount drug companies can charge for high-cost drugs, allowing Americans to buy prescription drugs imported from Canada, and creating an independent group that oversees the pricing of prescription drugs.
In deciding which candidate to vote for in the 2016 presidential election, voters are slightly prioritizing the candidates’ personal characteristics over the candidates’ stances on specific issues or the candidates’ political party. While personal characteristics may drive much of the vote choice, when asked about the role that a variety of health care issues will play in the 2016 presidential election, many are salient to voters — including 58 percent of Clinton supporters who say the candidate’s plan to address prescription drug prices will be very important.
The September Kaiser Health Tracking Poll finds Americans’ opinion of the health care law is divided (44 percent have a favorable view while 47 percent have an unfavorable view).
The 2016 Presidential Election
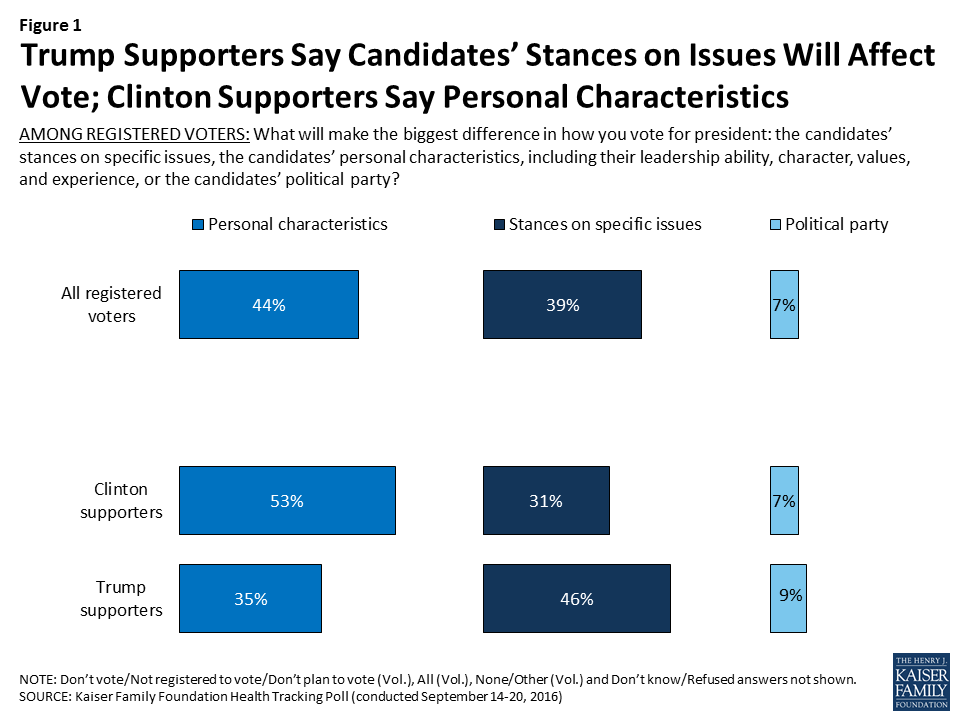
With less than six weeks before the general election, voters are balancing numerous considerations when deciding which candidate they will vote for in the 2016 presidential election. As polling conducted prior to the first presidential debate shows, a slightly larger share of voters (44 percent) say the candidates’ personal characteristics, including their leadership ability, character, values, and experience, will make the biggest difference in how they vote for president than say the candidates’ stances on specific issues (39 percent) or the candidates’ political party will make the biggest difference (7 percent).
When looking specifically at voters who say they currently plan on voting for Republican presidential nominee Donald Trump, about half (46 percent) say the candidates’ stances on specific issues will make the biggest difference in who they vote for compared to one-third (35 percent) that say the personal characteristics will make the biggest difference. Among voters who are currently supporting Democratic presidential nominee Hillary Clinton, the opposite is true — 53 percent say the candidates’ personal characteristics will make the biggest difference and three in ten (31 percent) say the candidates’ stances on specific issues will make the biggest difference in their vote.
Figure 1: Trump Supporters Say Candidates’ Stances on Issues Will Affect Vote; Clinton Supporters Say Personal Characteristics
Health Care Issues Are Important to Voters
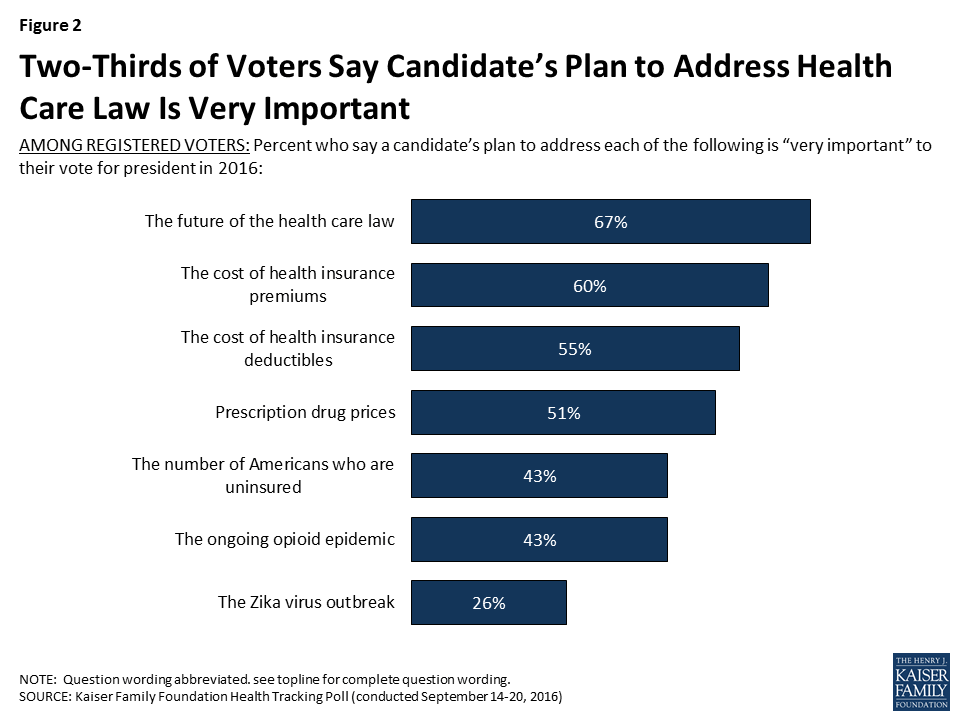
While personal characteristics may drive much of the vote choice, when asked about the role that a variety of health care issues will play in the 2016 presidential election, many are salient to voters. Two-thirds of voters say a candidate’s plan to address the future of the health care law is very important to their vote, six in ten say the same about a candidate’s plan to address the cost of health insurance premiums, 55 percent say the same about a candidate’s plan to address the cost of deductibles, and about half of voters (51 percent) say the same about a candidate’s plan to address prescription drug prices. Smaller shares of voters say a candidate’s plan to address the number of Americans who are uninsured (43 percent), the ongoing opioid epidemic (43 percent), or the Zika virus outbreak (26 percent) is very important to their vote for president.
Figure 2: Two-Thirds of Voters Say Candidate’s Plan to Address Health Care Law Is Very Important
Health Care Issues More Salient to Clinton Supporters Than Trump Supporters
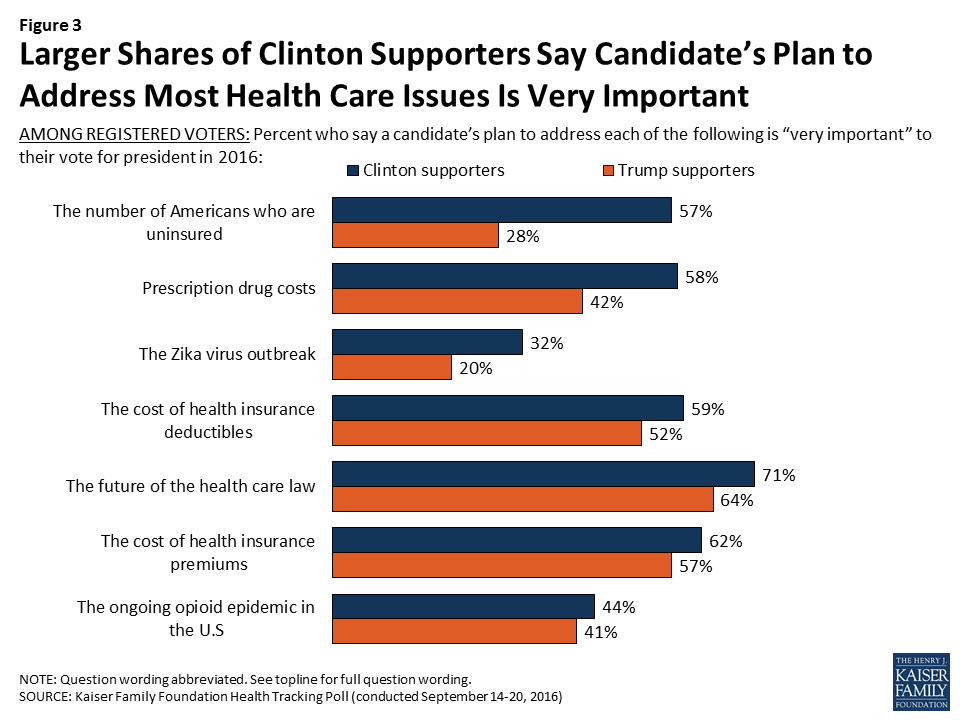
More Clinton supporters than Trump supporters say a candidate’s plan to address a series of health care issues is very important to their vote, including a candidate’s plan to address the number of Americans who are uninsured (57 percent vs. 28 percent), prescription drug costs, (58 percent vs. 42 percent), the Zika virus outbreak (32 percent vs. 20 percent). Slightly higher shares of Clinton supporters than Trump supporters say a candidate’s plan to address the cost of health insurance deductibles (59 percent vs. 52 percent) and the future of health care law (71 percent vs. 64 percent) is very important. While similar shares of Clinton supporters and Trump supporters say a candidate’s plan to address the cost of health insurance premiums and the ongoing opioid epidemic in the U.S. is very important to their vote for president. To see a side-by-side comparison of the two candidates’ proposed health care policies, please visit KFF’s Snapshot of where Hillary Clinton and Donald Trump Stand on Seven Health Care Issues.
Figure 3: Larger Shares of Clinton Supporters Say Candidate’s Plan to Address Most Health Care Issues Is Very Important
Americans’ Opinions of the Affordable Care Act
With two-thirds of voters saying a candidate’s plan to address the future of the health care law will be very important to their vote for president, the September Kaiser Health Tracking Poll finds Americans’ opinion of the health care law remains divided, with 44 percent saying they have a favorable view and 47 percent saying they have an unfavorable view. The share of individuals who said they “don’t know” whether they have a favorable or unfavorable opinion of the law or refused to answer the question decreased this month from 17 percent in August 2016 to 9 percent in September 2016.
Figure 4: Public Divided on View of the Health Care Law
While similar shares of Republicans (7 percent), Democrats (7 percent), and independents (11 percent) currently say they don’t know — or refuse to report — whether they have a favorable or unfavorable opinion of the law, the share of Democrats who don’t know or refuse the question is at its lowest level in four years.
The Number of Americans without Health Insurance
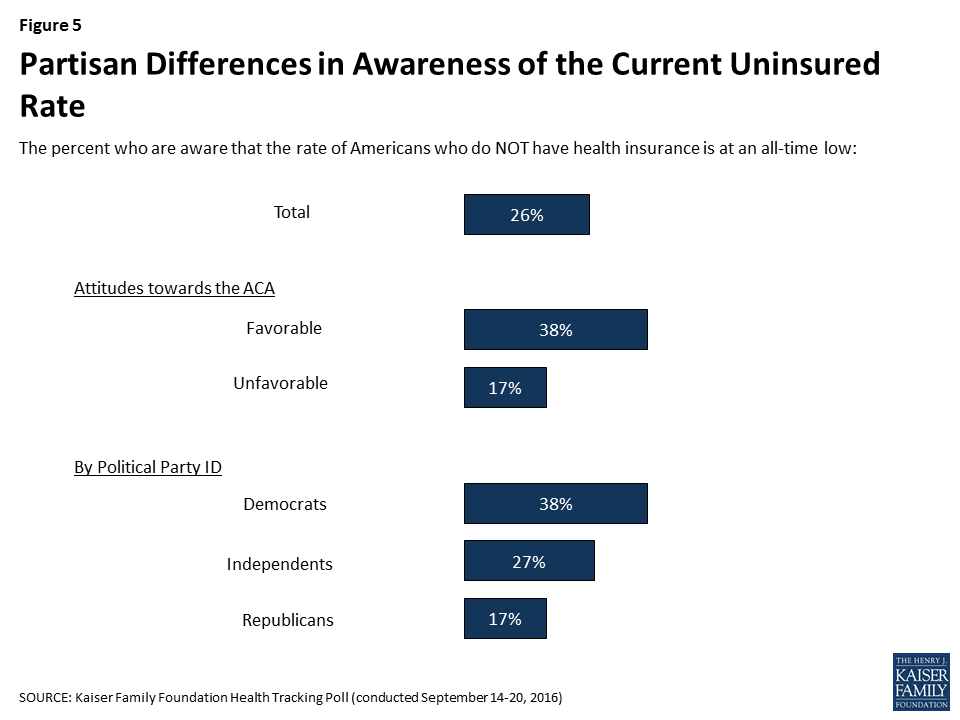
One of the key goals of the 2010 health care law was to reduce the number of Americans who did not have health insurance coverage. According to the U.S. Census, in 2015, 9 percent of Americans went without health insurance coverage — the lowest rate ever recorded.1 When asked whether the rate of Americans without health insurance is at an all-time high or an all-time low, about a quarter (26 percent) of Americans are aware that it is at an all-time low, while one-fifth (21 percent) say that it is at an all-time high and about half (46 percent) say it is about the same as it has been. Awareness of the uninsured rate is mainly viewed through a partisan lens, regardless of how closely Americans are following news about the issue. Four in ten (38 percent) individuals who have favorable attitudes toward the ACA are aware the rate is at an all-time low compared to 17 percent of those with an unfavorable opinion toward the ACA. In addition, 38 percent of Democrats, 27 percent of independents, and 17 percent of Republicans are aware the uninsured rate is at an all-time low. Among those who report they have been following news about this issue “very closely,” similar shares are aware the uninsured rate is at an all-time low (32 percent) as say it is at an all-time high (26 percent).
Figure 5: Partisan Differences in Awareness of the Current Uninsured Rate
Health Insurance Marketplaces
In August 2016, health insurer Aetna, Inc. announced it was withdrawing from the ACA exchanges — marketplaces where people who do not have employer-sponsored health insurance can buy coverage. This news was closely followed by about one-third (36 percent) of Americans according to the August Kaiser tracking poll. This month’s poll finds that half of Americans have heard at least some about health insurance marketplaces, which is considerably higher than the share of Americans who reported the same in December 2013 (36 percent).
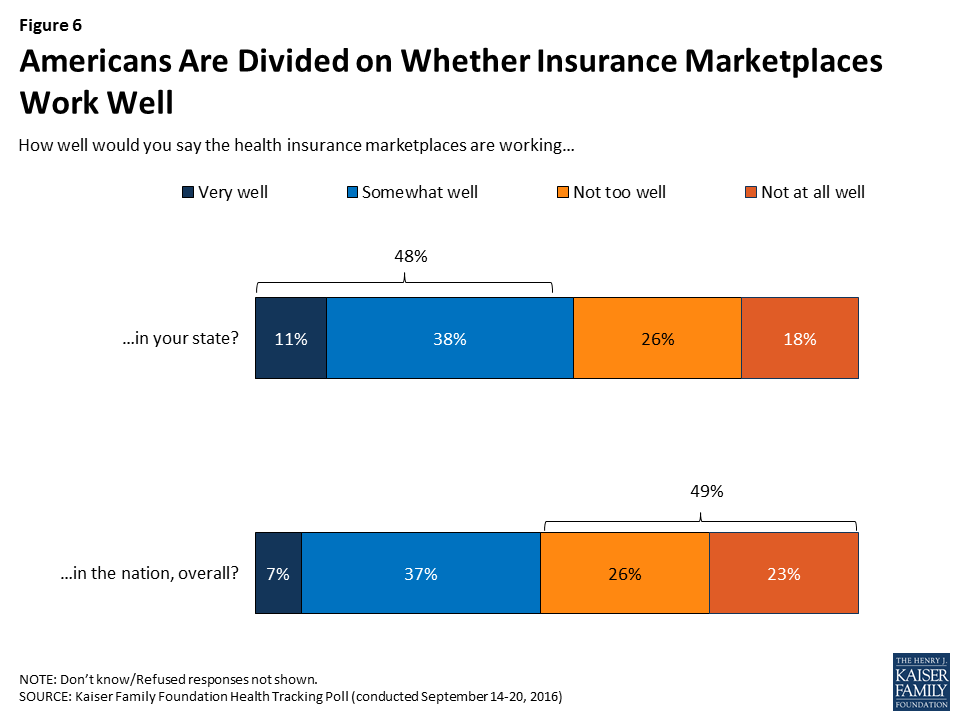
Americans are divided on how well they think the health insurance marketplaces are working in their own state and in the nation, overall. About half (48 percent) of individuals say the health insurance marketplaces in their own state are working well while 43 percent say they are working either not too well (26 percent) or not at all well (18 percent).
When asked how well they think the marketplaces are working in the nation overall, about half of Americans say they are not working well (26 percent say they are working “not too well” and 23 percent say they are working “not at all well”) while 44 percent say they are working either “very well” (7 percent) or “somewhat well” (37 percent).
Figure 6: Americans Are Divided on Whether Insurance Marketplaces Work Well
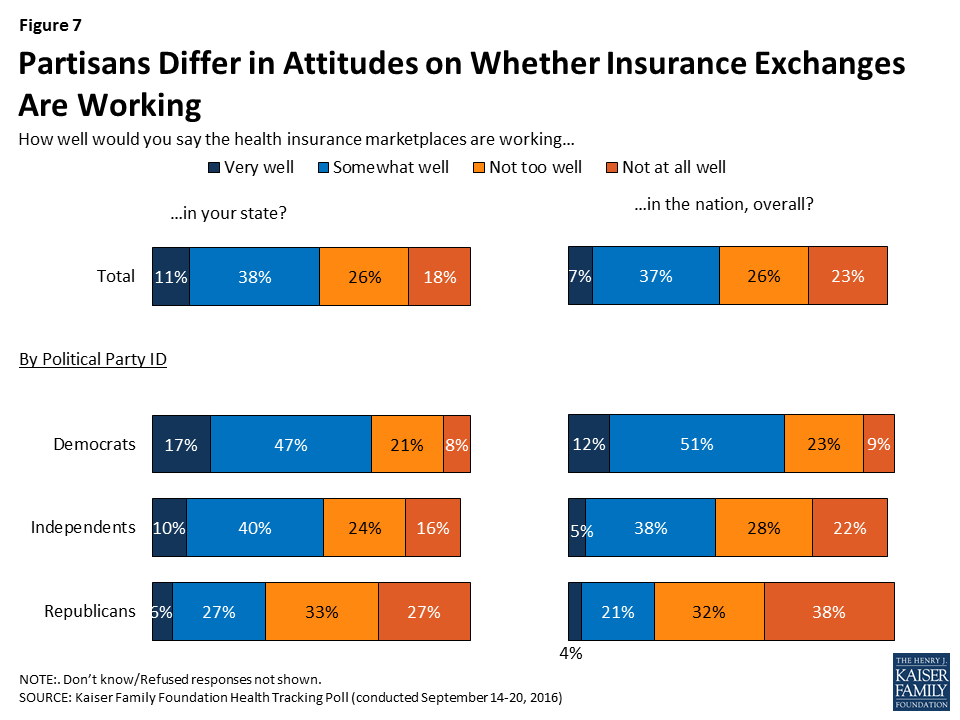
Similar to perceptions of the uninsured rate, attitudes towards the health insurance marketplaces also differ among partisans, regardless of how much they have heard about the health insurance marketplaces. Nearly two-thirds of Democrats say the marketplaces in their own state (64 percent) and in the nation overall (62 percent) are working well, while one-third of Republicans say the marketplaces in their own state are working well and 25 percent say the marketplaces in the nation overall are working well. Independents are more divided, with half saying the marketplaces in their own state are working well and 42 percent saying the marketplaces in the nation overall are working well.
Figure 7: Partisans Differ in Attitudes on Whether Insurance Exchanges Are Working
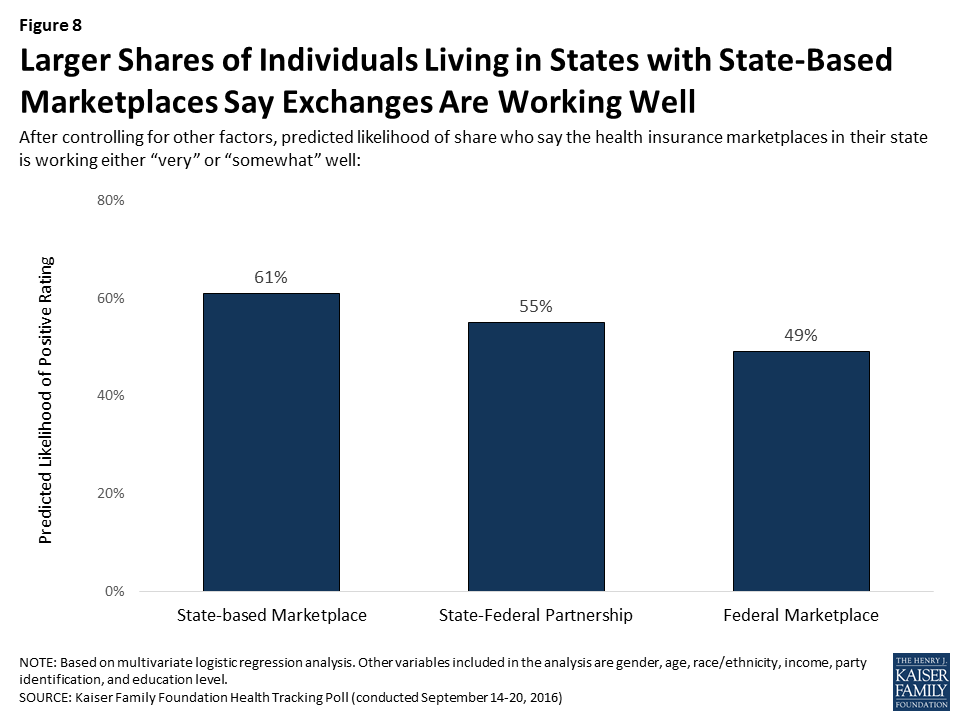
In addition, individuals living in states that have developed their own state-based marketplace are more likely to say the health insurance marketplace in their own state is working well — even when controlling for demographic factors that tend to predict support for the ACA (age, income, education level, party identification, gender, and race/ethnicity). Individuals living in states with state-based marketplaces are more positive in their evaluations with 61 percent saying the health insurance marketplace in their state is working either “very” or “somewhat” well. This is similar to the share of those living in states with a state-federal partnership (55 percent) but significantly more positive than those living in states that have not developed their own state-based marketplace and are using the federal marketplace (49 percent).
Figure 8: Larger Shares of Individuals Living in States with State-Based Marketplaces Say Exchanges Are Working Well
The Public’s Views On Prescription Drugs
In light of the news about the increase in the cost for the Epinephrine injection and many Clinton and Trump supporters (58 percent and 42 percent, respectively) saying a candidate’s plan to address prescription drug costs is very important to their vote, the September Kaiser Health Tracking Poll takes a look at the public’s attitudes on prescription drugs — in terms of overall benefits as well as methods aimed at curtailing costs.
To see more prescription drug-related poll findings, visit the prescription drug slideshow.
Large Share of Americans Say Prescription Drugs Have Made Lives Better, But Think Costs Are Unreasonable
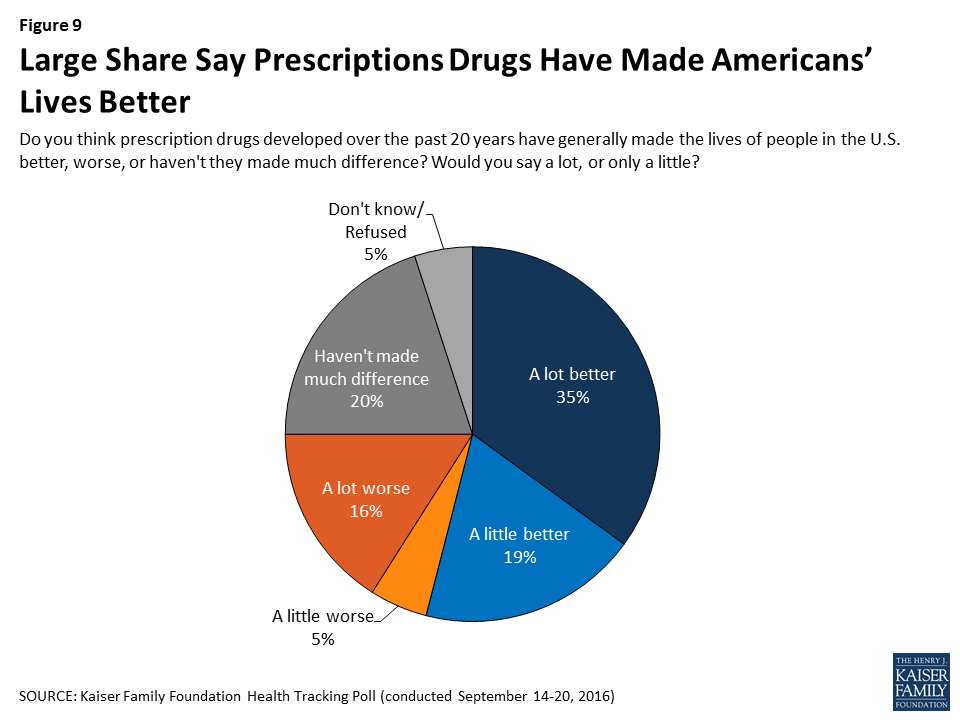
The majority of the public (56 percent) say prescription drugs developed over the past 20 years have generally made the lives of people in the U.S. better, including about one-third (35 percent) who say prescription drugs have made lives “a lot better.” This is compared to about one in five Americans who say prescription drugs have made the lives of people in the U.S either “a lot worse” (16 percent) or “a little worse” (5 percent), and 20 percent who say prescription drugs have generally not made a difference in people’s lives.
Figure 9: Large Share Say Prescriptions Drugs Have Made Americans’ Lives Better
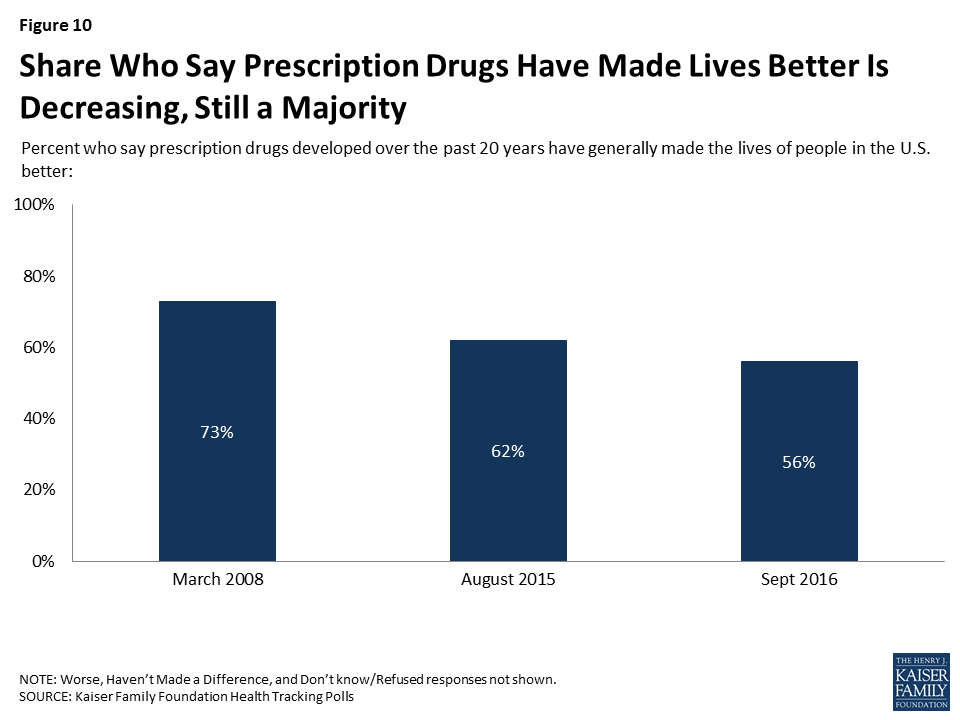
While the majority of Americans say prescription drugs have made lives better, there has been a decrease in the share who say this. In March 2008, 73 percent of Americans said that prescription drugs have made the lives of Americans better, including about half who said they had made lives “a lot better.” In addition, in August 2015, 62 percent of the public said prescription drugs have made the lives of Americans better.
Figure 10: Share Who Say Prescription Drugs Have Made Lives Better Is Decreasing, Still a Majority
Majority of Americans Say Prescription Drug Costs Are Unreasonable, But Few of Those Taking Prescription Medication Report Problems with Affordability
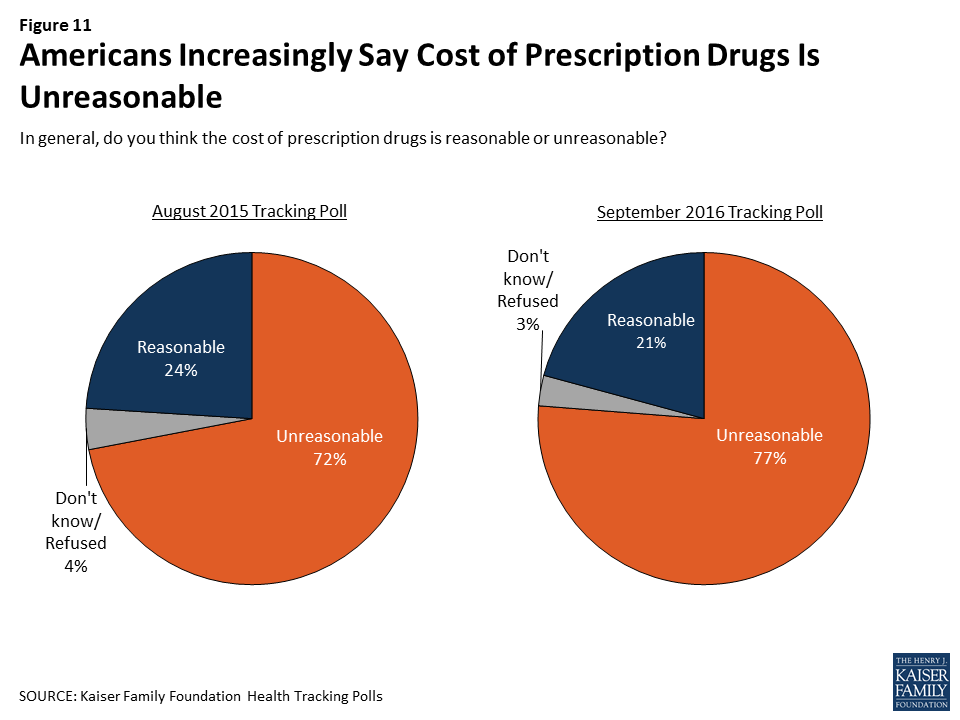
Costs could be one reason why the share of Americans who say prescription drugs have made the lives of people in the U.S. better is declining. A large majority (77 percent) perceive drug costs as unreasonable while less than a quarter (21 percent) say the costs are reasonable. The share of Americans who say prescription drug costs are unreasonable has increased somewhat over the past year, up from 72 percent in August 2015.
Figure 11: Americans Increasingly Say Cost of Prescription Drugs Is Unreasonable
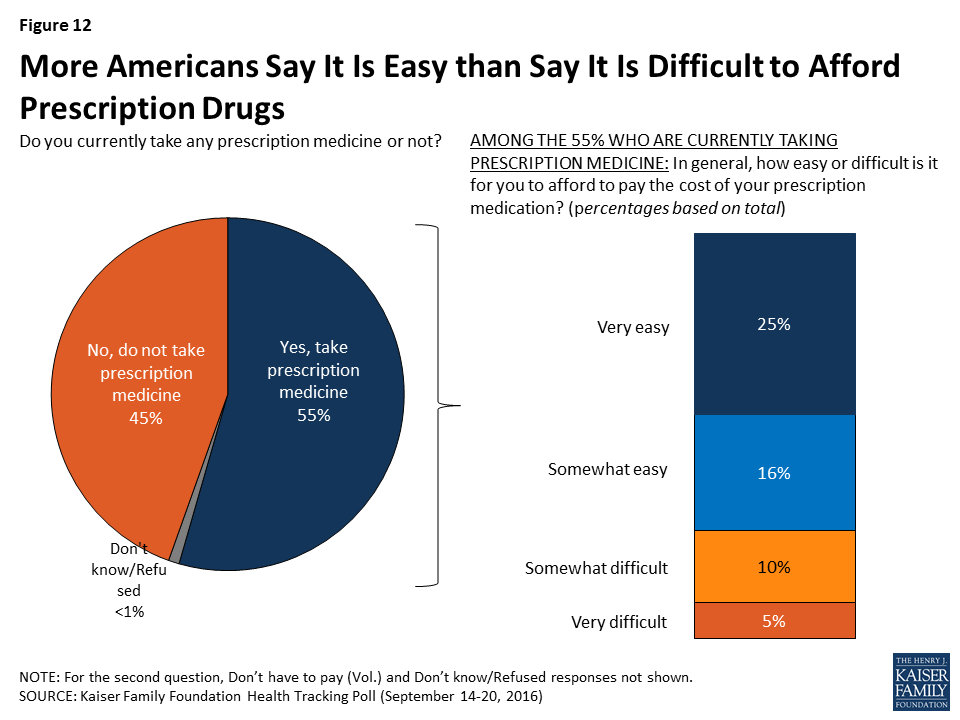
Yet despite the fact that most of the public says prescription drug costs are unreasonable, a large majority of Americans currently taking prescription drugs do not report any difficulty paying for the cost of their prescription medications. Of the 55 percent of Americans who currently take medications, the majority (73 percent) say that affording to pay for the cost of their prescription medicine is easy. Still, 26 percent report difficulty affording their medications (14 percent of the total population).
Figure 12: More Americans Say It Is Easy than Say It Is Difficult to Afford Prescription Drugs
The ability to afford prescription medication varies widely by reported health status and the number of prescription drugs an individual is taking. Among individuals currently taking prescription medications, a larger share of those who report being in “fair” or “poor” health report difficulty affording their medication (42 percent) than those who report being in “excellent,” “very good,” or “good” health (20 percent). In addition, four in ten individuals (37 percent) who are currently taking four or more medications report difficulty affording them compared to 19 percent of individuals taking prescription medications, but fewer than four.
Table 1: Those in Worse Health or Taking Four or More Drugs More Likely to Report Difficulty Affording Their Medicines
Health Status Among Those Taking Prescription Drugs
Prescription Drug Use
Excellent/Very Good/Good Health
Fair/Poor Health
Taking 1-3 Prescription Drugs
Taking 4 or More Prescription Drugs
Very easy
53%
21%
56%
30%
Somewhat easy
26
36
25
33
Somewhat difficult
15
24
14
22
Very difficult
5
18
5
14
NOTE: Don’t know/Refused responses not shown. “Don’t have to pay (Vol.)” responses not shown.
Views of Policy Options to Keep Prescription Drug Costs Down
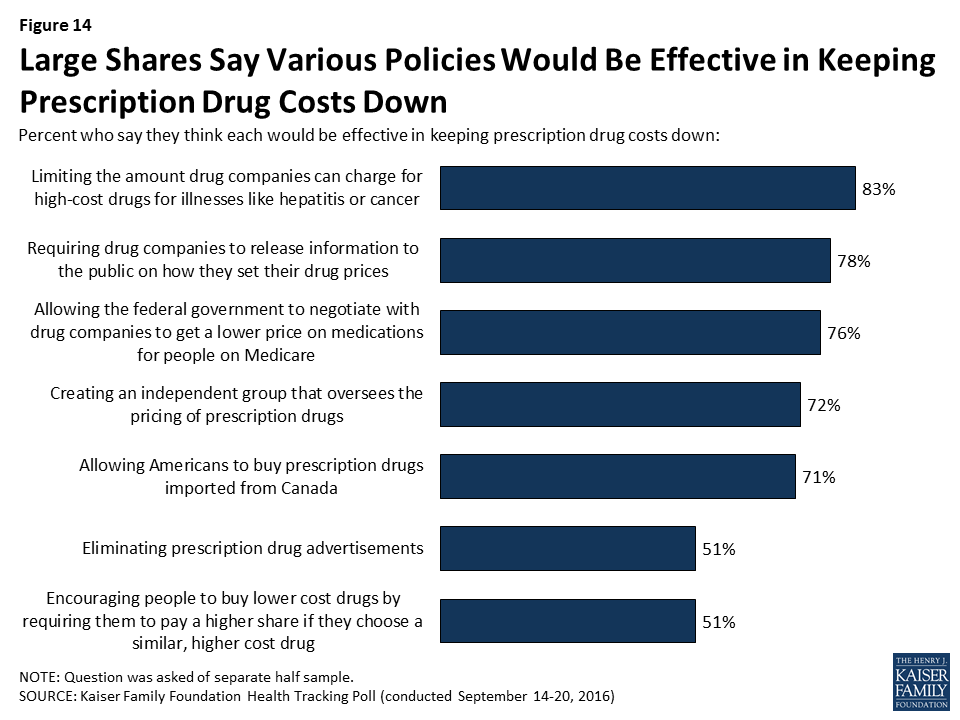
When presented with a list of policy options intended to help keep the cost of prescription drugs down, the majority of the public is in favor of most of the policy actions, and large shares also believe that the options would be effective in addressing rising drug costs.
The vast majority of Americans favor requiring drug companies to release information to the public on how they set drug prices (86 percent), and eight in ten favor allowing the federal government to negotiate with drug companies to get a lower price on medications for people on Medicare (82 percent) and limiting the amount drug companies can charge for high-cost drugs for illnesses like hepatitis or cancer (78 percent). In addition, 71 percent favor allowing Americans to buy prescription drugs imported from Canada and two-thirds (66 percent) favor creating an independent group that oversees the pricing of prescription drugs — a policy proposal put forth by Democratic presidential candidate Hillary Clinton in response to the EpiPen controversy.2 On the other hand, Americans are split on two potential policy actions: eliminating prescription drug advertisements and encouraging people to purchase lower cost drugs by requiring them to pay a higher share if they choose a similar, higher cost drug.
Figure 13: Most of the Public Favors Actions to Keep Drug Costs Down
In addition, a majority of Americans also believe most of the proposed policies would be effective in keeping prescription drug costs down. Somewhat fewer, but still half, say eliminating prescription drug advertisements (51 percent) and encouraging people to buy lower cost drugs by requiring them to pay a higher share if they choose a similar, higher cost drug (51 percent) would be effective.
Figure 14: Large Shares Say Various Policies Would Be Effective in Keeping Prescription Drug Costs Down
A majority of Republicans, Democrats, and independents both favor and think most of these policy actions would be effective in keeping prescription drug costs down, with the exception of two potential actions: eliminating prescription drug advertisements and encouraging people to buy lower cost drugs by requiring them to pay a higher share if they choose a similar, higher cost drug. Fewer partisans favor either of these policy actions.
Table 2: Views of Policy Actions to Keep Drug Costs Down by Party Identification
Percent who say they favor each of the following and percent who say they think each would be effective in keeping prescription drug costs down:
Party ID
Democrats
Independents
Republicans
Requiring drug companies to release information to the public on how they set their drug prices
Favorable
83%
88%
88%
Effective
82%
75%
78%
Allowing the federal government to negotiate with drug companies to get a lower price on medications for people on Medicare
Favorable
93%
85%
68%
Effective
87%
81%
65%
Limiting the amount drug companies can charge for high-cost drugs for illnesses like hepatitis or cancer
Favorable
79%
83%
73%
Effective
92%
81%
79%
Allowing Americans to buy prescription drugs imported from Canada
Favorable
66%
77%
70%
Effective
72%
76%
74%
Creating an independent group that oversees the pricing of prescription drugs
Favorable
72%
65%
60%
Effective
79%
72%
65%
Encouraging people to buy lower cost drugs by requiring them to pay a higher share if they choose a similar, higher cost drug
Favorable
39%
45%
37%
Effective
57%
52%
56%
Eliminating prescription drug advertisements
Favorable
44%
49%
44%
Effective
53%
51%
52%
NOTE: Questions were asked of separate half samples.
Kaiser Health Policy News Index: September 2016
The September Kaiser Health Tracking Poll finds the 2016 presidential campaign dominating the public’s attention, with the majority of Americans closely following stories about Hillary Clinton’s presidential campaign (70 percent) and Donald Trump’s presidential campaign (69 percent). About six in ten Americans report closely following several health policies news stories during the past month including the Zika virus outbreak (61 percent), the increase in cost for the Epinephrine injection, commonly known as the EpiPen (58 percent), and the reports on the number of uninsured Americans (58 percent). This is similar to the share who say they are following the stories about professional athletes, like NFL player Colin Kaepernick, protesting during the playing of the national anthem (62 percent). A majority of the public also say they are following news about the ongoing heroin and prescription painkiller addiction epidemic in the U.S. (56 percent). About half of the public (49 percent) say they are following news about the U.S. and Russia brokered cease-fire in Syria, which began on September 12th.3
Figure 15: Kaiser Health Policy News Index: September 2016
Zika
The Zika Virus Outbreak
As part of the Kaiser Family Foundation’s ongoing efforts to track the public’s knowledge of the Zika virus outbreak and attitudes towards Zika-related issues, the September Kaiser Health Tracking Poll examines whether the public has taken steps in order to protect themselves from getting Zika. To see all of our Zika-related poll findings, visit the Zika slideshow.
As seen in other recent Kaiser Health Tracking Polls, the Zika virus is one of the top health policy stories followed by the public, with nine in ten Americans (92 percent) saying they have heard or read at least a little about the Zika virus and 61 percent of the public reporting that they were closely following news about the Zika virus outbreak.
Figure 1: The Zika Virus Outbreak Has Remained High on the Public’s Radar Since February 2016
Many Americans Say They Are Taking Steps to Avoid Zika
The Centers for Disease Control and Prevention recommends that the public take steps to protect themselves and others from the Zika virus by preventing mosquito bites and, for those who may be at-risk for the virus, taking precautions while engaging in sexual intercourse. In addition, because there are outbreaks occurring in multiple countries and at least one U.S. city — Miami, Florida — the CDC recommends that pregnant couples, or partners who are planning a pregnancy, do not travel to those areas.4
In July, about half (51percent) of Americans said they thought the Zika virus posed a threat (either “major” or “minor”) to them, personally.5 The most recent Tracking Poll finds the most commonly reported precautions being taken by Americans to protect themselves from getting Zika are using mosquito repellent (50 percent), removing standing water from around their home (46 percent), and avoiding travel to another country (42 percent). Fewer Americans report taking other Zika-related precautions.
Figure 2: Most Common Zika-Related Precautions
Likelihood of Taking Steps to Avoid Zika Varies by Where you Live
When it comes to protecting yourself by reducing the number of mosquitoes in and around your home, more individuals living in the South report taking such precautions. Individuals living in the South are more likely to report having a pest control company spray outside their home to protect themselves than those living in other regions of the U.S. In addition, individuals living in the South (18 percent) are more likely to report having a pest control company spray insecticide inside their home than individuals in the West (7 percent) or Midwest (6 percent). Individuals living in the South are also more likely than people in other regions to report that they have removed standing water from around their home in order to protect themselves from catching Zika.
Figure 3: Larger Share of Individuals Living in the South Report Taking Measures to Reduce Number of Mosquitoes Around their Homes
Furthermore, individuals who report that there are a lot of mosquitoes where they live are more likely to say they have used mosquito repellent to protect themselves from getting the Zika virus than those who say there are not very many mosquitoes where they live (62 percent vs. 40 percent).
Those not taking Precautions do not Think They Are at Risk
One in five (21 percent) Americans report they have not taken any of these measures to protect themselves against the Zika virus outbreak. Among those who say they have not taken any of these precautions, two-thirds (68 percent) say it is because they do not think they are at risk, 11 percent say it is because they do not think it would be that serious if they caught the virus, and 3 percent say it is because they do not know how to protect themselves.
Figure 4: Most Who Aren’t Taking Precautions Don’t Think They Are at Risk
Few Americans Say They Have Been Personally Affected by the Zika Virus
When asked, very few (2 percent) Americans say they personally know someone whose health has been affected by the Zika virus.
Figure 5: Nine in Ten Americans Have Heard at Least a Little About Zika; Two Percent Know Someone Whose Health Is Affected
Methodology
This Kaiser Health Tracking Poll was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted September 14-20, 2016, among a nationally representative random digit dial telephone sample of 1,204 adults ages 18 and older, living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). Computer-assisted telephone interviews conducted by landline (421) and cell phone (783, including 468 who had no landline telephone) were carried out in English and Spanish by Princeton Data Source under the direction of Princeton Survey Research Associates International (PSRAI). Both the random digit dial landline and cell phone samples were provided by Survey Sampling International, LLC. For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s 2014 American Community Survey (ACS) on sex, age, education, race, Hispanic origin, and region along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the July-December 2015 National Health Interview Survey. The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Large Majorities Favor Wide Range of Policy Changes to Curb Prescription Drug Costs, Including Those That Give Government a Greater Role in Negotiating or Limiting Prices
Public Split on Whether ACA Marketplace in Their Own States Are Working Well; Just One in Four Aware the Nation’s Uninsured Rate Reached an All-Time Low
Amid news reports about increases in the price for EpiPen and other drugs, the vast majority of Americans – including majorities of Democrats, Republicans and independents – support several policy changes to control the cost of prescription drugs, including some that would expand government’s role in drug pricing, the latest Kaiser Family Foundation tracking poll finds.
About eight in 10 Americans say they favor allowing the federal government to negotiate with drug companies to get a lower price on medications for people on Medicare (82%) and limiting the amount drug companies can charge for high-cost drugs for illnesses like hepatitis or cancer (78%). In addition, two-thirds (66%) favor creating an independent group that oversees the pricing of prescription drugs, as Democratic presidential candidate Hillary Clinton recently proposed. Majorities also support requiring drug companies to release information to the public on how they set drug prices (86%) and allowing Americans to buy prescription drugs imported from Canada (71%).
A majority of Democrats, Republicans and independents support each of these five policy changes and also think each of them would be effective in keeping drug costs down.
Fewer overall and across parties favor two other potential policy changes: eliminating drug advertisements (47%) and encouraging consumers to buy lower-cost drugs by requiring them to pay more for similar but higher-cost ones (42%).
The survey probes the public’s views and experiences with prescription drugs more broadly. It finds a large majority (77%) perceive drug costs as unreasonable, while one in five (21%) say they are reasonable. The share who say drug costs are unreasonable is up somewhat from 72 percent a year ago in August 2015.
At the same time, relatively few Americans say they personally are having trouble paying for their medication. The survey finds about half (55%) of the public report currently taking prescription drugs, and the vast majority (73%) of them say paying for their medications is easy; far fewer (26% of those taking prescription drugs, or 14% of the total population) say it is difficult to pay for their drugs. Larger shares of those who report being in “fair” or “poor” health and those taking four or more medications say it is difficult to afford their prescriptions.
Views on the Affordable Care Act Remain Mixed with Large Partisan Divisions
The survey finds the public remains divided in its view of the Affordable Care Act (ACA), with 47 percent reporting an unfavorable view and 44 percent reporting a favorable one. As in the past, Democrats largely support the law, Republicans largely oppose it, and independents are in the middle, though leaning unfavorable. These divisions persist on other questions about views and facts related to the law’s impact.
For example, about half of the public (48%) say the marketplace in their own state is working well, while 43 percent say it is not working well. When asked how well they think the marketplaces are working in the nation overall, perceptions shift slightly with about half (49%) saying they are not working well and 44 percent say they are working well.
Majorities of Democrats perceive the marketplace in their state and marketplaces nationally as working well, while Republicans are more likely to say they are not working well. People living in states that have developed their own state-based marketplace are more likely to say the health insurance marketplace in their own state is working well — even when controlling for party identification and other demographic factors that tend to predict support for the ACA.
Also, a separate question gauges the public’s awareness of the nation’s uninsured rate, which stands at an all-time low. When asked whether the uninsured rate is at an all-time low or all-time high, a quarter (26%) are aware that it is at an all-time low, while a fifth (21%) say that it is at an all-time high. Democrats and those with a favorable view of the health reform law are more likely to be aware of this; Republicans and those with an unfavorable view are less likely to be aware.
Other findings include:
In polling completed before Monday’s first presidential debate, a larger share of voters (44%) say the candidates’ personal characteristics, including their leadership ability, character, values, and experience will make the biggest difference in how they vote for president than say the candidates’ stances on specific issues (39%) or the candidates’ political party (7%) will make the biggest difference.
At the same time, two thirds (67%) of voters say a candidate’s plan to address the future of the Affordable Care Act is very important to their vote, and smaller majorities say the same about a candidate’s plans to address the cost of health insurance premiums (60%), deductibles (55%) and prescription drug prices (51%).
Designed and analyzed by public opinion researchers at the Kaiser Family Foundation, the poll was conducted from September 14-20 among a nationally representative random digit dial telephone sample of 1,204 adults. Interviews were conducted in English and Spanish by landline (421) and cell phone (783). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
The Commonwealth of Puerto Rico has been in the news spotlight for over a year due to the debt crisis that has followed a decade’s long recession, and to the rapid spread of Zika cases on the island, exceeding 19,000 as of September 21, 2016, and counting.1 Nearly half of the population (46%) in Puerto Rico lives below the federal poverty line, and the unemployment rate is more than double that of the 50 states and D.C. (12% vs. 5%).2,3 For a snapshot of Puerto Rico’s demographic characteristics, key health indicators, and a broader discussion of Zika on the island, see our 8 questions and answers about Puerto Rico fact sheet.
Roughly one in two Puerto Ricans (49%) are enrolled in the island’s Medicaid program, a rate more than double that of the 50 states and D.C. (19%).4 Puerto Rico provides Medicaid coverage through an island-wide public health insurance program, known as Mi Salud, the umbrella program for Puerto Rico’s Medicaid, CHIP, some Medicare, and some Puerto-Rico only funded coverage. The Puerto Rico Department of Health has a cooperative agreement with the Puerto Rico Health Insurance Administration (PRHIA), also known as the Administracion de Seguros de Salud (ASES), to administer Mi Salud.5 Puerto Rico’s Medicaid financing structure differs from that of the 50 states and D.C. in two important ways. First, federal funding to the program is subject to a statutory cap, and second, the island’s FMAP is fixed at 55% rather than being determined annually based on its per capita income. Under the ACA, Puerto Rico’s Medicaid program received increased federal funding through a $6.4 billion allotment as well as a modest increase in its federal match rate.
This fact sheet provides an overview of the Medicaid program in Puerto Rico and emerging fiscal issues facing its health care system as Zika cases on the island continue to mount.
Medicaid and the ACA in Puerto Rico
Financing
Unlike the 50 states and D.C., annual federal funding for Puerto Rico’s Medicaid program is subject to a statutory cap. Federal matching funds for Medicaid in the 50 states and D.C. are not capped. However, federal Medicaid funding in Puerto Rico and the other territories are subject to a statutory cap, meaning that once federal funds are exhausted, the island no longer receives financial support for its Medicaid program during that fiscal year. In 2014, the allotment was capped at $321 million, and the island generally exhausts its capped allotment prior to the end of its fiscal year.6
In addition, Puerto Rico’s federal match rate is fixed in federal statute. States and the federal government jointly finance the Medicaid program according to an established formula that provides guaranteed matching funds. In the 50 states, the Federal Medical Assistance Percentage (FMAP) is determined by a formula set in statute that relies on states’ relative per capita income. For federal fiscal year 2017, the FMAP ranges from a floor of 50% to a high of 75% for Mississippi, the poorest state in the country.7 Puerto Rico and the other territories receive a match rate that is fixed in statute and unrelated to per capita income. Before 2011, Puerto Rico and the other territories received the statutory minimum FMAP of 50% despite the fact that per capita income in 2014 was nearly half what it was in Mississippi ($11,331 vs. $21,036).8
The ACA increased Puerto Rico’s traditional match rate from 50% to 55%. For 2014 and 2015, the island also received an additional 2.2 percentage point increase to its FMAP for its non-expansion population, bringing it to 57.2% during those two years.9 The ACA provided Puerto Rico with the expansion state match rate for non-disabled adults without children. The expansion state FMAP for Puerto Rico was 78% in 2014 (Table 1).10
Table 1: Changes to Puerto Rico FMAP under the ACA
Match Rate
Statutory Match Rate Pre-ACA
50%
Statutory Match Rate Post-ACA
55%
Special Match Rate for Non-Expansion Population in 2014-2015
57.2%
Match Rate for Childless Adults
Expansion State Match (78% in 2014)
The ACA also made additional funds available to Puerto Rico, totaling nearly $6.4 billion. The $6.4 billion consists of a $5.5 billion allotment available between July 2011 and September 2019 and another $925 million the island received in lieu of funds it would have received for creating its own Marketplace. These funds are also available through FY 2019 and can only be accessed after the first source of ACA funding has been depleted. In 2014, the ACA funds accounted for the majority of federal Medicaid funds expended (68%) (Figure 1).11
Puerto Rico’s Federal Medicaid Funding ($ in millions), FY 2014
Eligibility
Federal Medicaid eligibility and benefit rules are generally the same in Puerto Rico as in the 50 states and D.C. Medicaid requires Puerto Rico and the other territories to cover the same mandatory eligibility groups and benefits as the states, and allows them to cover the same optional eligibility groups and benefits. However, the island is not required to adhere to the federal poverty guidelines. Instead, the income-eligibility levels for Puerto Rico’s Medicaid program are based on a local poverty level that is established by the Commonwealth and approved by the Center for Medicare and Medicaid Services (CMS).12
Prior to the ACA, Puerto Rico offered coverage to those with incomes up to at least 100% of the local poverty level. Even prior to the ACA Medicaid expansions, Puerto Rico covered all eligible populations with incomes up to at least 100% of the local poverty level,13 including non-disabled adults without children, an optional eligibility group. As of January 2014, Puerto Rico expanded Medicaid eligibility up to at least 133% of the local poverty level for children, pregnant women, parents and other adults with incomes up to at least 133% of the local poverty level. Elderly beneficiaries and those with disabilities are covered at roughly the same eligibility level as in the states (73% FPL) (Figure 2).14
Figure 2: Medicaid and CHIP Income-Eligibility Levels, in Puerto Rico Local Poverty Level and FPL, 2015
Benefits and Delivery System
Despite being subject to the same mandatory benefit requirements as the 50 states and D.C., Puerto Rico does not currently cover all mandatory Medicaid benefits. There has not been a comprehensive analysis of the benefits covered under Puerto Rico’s Medicaid program; however, several sources point to some services that are not covered by the program. For example, Puerto Rico currently lacks the infrastructure and funds necessary to offer long-term care in nursing facilities and home health services,15,16 and does not cover hospice care or medical equipment and supplies.17 In addition, limited benefits are provided to children under the Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) benefit.18
Puerto Rico’s Medicaid program provides acute, primary, and specialty services through a mandatory managed care delivery model. In Puerto Rico, Medicaid is delivered exclusively through a managed care model for most populations. The island contracts with one managed care program, Triple S, a licensee of the Blue Cross Blue Shield Association, and offers that coverage island-wide. Behavioral health services are carved-out and provided island-wide through a separate behavioral health managed care organization. Dual eligibles have the option to participate in a Medicare Advantage plan, called Medicare Platino, which provides Medicare acute and primary care and Medicaid wraparound services, and which together offer coverage equivalent to Mi Salud. Medicare Platino is offered through seven managed care plans, including four local plans (First Medical/First Plus, MCS, MMM Healthcare, and PMC Medicare Choice) and three national plans (Humana and two Blue Cross/Blue Shield affiliates—American Health Medicare and Triple S).19
Puerto Rico’s safety net providers play an important role in delivering health care to the island’s most vulnerable populations. In 2014, Puerto Rico had 20 federally-funded community health centers, with 71 sites across the island. These sites serve nearly 340,000 patients (roughly 10% of the population), 12% of whom are uninsured.20 However, the distribution of available clinical resources and health care professionals is focused in large metropolitan areas across the island, while the outlying communities and rural areas have limited access to care and treatment.21 Notably, Puerto Rico and the other territories are ineligible for Medicaid Disproportionate Share Hospital (DSH) Subsidies, limiting the amount of resources available to the island’s safety net.22
Looking Ahead
ACA funding is estimated to be exhausted by the end of FY 2017. Puerto Rico has relied heavily on the nearly $6.5 billion in one-time ACA funds which were made available to the island in July 2011. While these funds are set to expire in September 2019, the island is expected to have exhausted them by the end of FY 2017.23 Absent reauthorization, up to 900,000 people (26% of the island’s population) could lose their health coverage.24
Inequities related to the island’s Medicaid finance structure, particularly the federal cap, have been acknowledged by various federal entities; however, no legislative action has been taken to date. The statutory cap on Puerto Rico’s Medicaid program combined with its low FMAP of 55% limits the island’s ability to offer certain mandatory Medicaid benefits and adds additional financial strain to its fragile economy. Acknowledging these difficulties, President Obama’s proposed budget for FY 2017 removed the cap and proposed gradually increasing the FMAP;25 however, this provision was not included in the final approved budget for FY 2017. Similarly, in August 2016, Treasury Secretary Lew and HHS Secretary Burwell sent a letter to the Congressional Task Force on Economic Growth in Puerto Rico urging Congress to remove the federal cap and increase the program’s FMAP. In the letter, the Secretaries stated that this proposed policy change, which has been analyzed for comparative effectiveness relative to other proposals, is one of the most powerful ways to support economic growth and long-term stability on the island.26 To date, no legislative action has been taken to reform the island’s Medicaid financing structure.
The number of Zika cases on the island continues to mount. In August 2016, the U.S. Department of Health and Human Services declared the Zika outbreak in Puerto Rico a public health emergency, signaling the significant threat the virus poses to pregnant women and children born to infected pregnant women on the island. The declaration allows the Commonwealth to apply for funds to control the spread of Zika and request the temporary reassignment of local public health departments and personnel to assist in Zika response.27 President Obama’s emergency Zika funding request in February 2016 included a temporary one-year increase of approximately $250 million to Puerto Rico’s federal Medicaid matching funds, but no emergency Zika package has been passed by Congress to date.28 Financial constraints have complicated the timely and comprehensive response required to respond to the outbreak.29 Given the critical role Medicaid plays for people with disabilities, the serious and costly health effects of Zika in Puerto Rico may place further demands on a program already facing steep funding shortfalls. According to the CDC, the dollar amount of caring for a single child with birth defects is estimated to be in the millions.30
The debt crisis has exacerbated many of the island’s health care issues. As a result of the debt crisis, the government has instituted strict austerity plans that have led to budget cuts to public programs and more severe poverty.31 Delayed payments by the government to Medicare and Medicaid managed care plans have caused a cascade of payment delays to medical providers and suppliers, and there have been reports of power and water shortages in hospitals, delays in the arrival of medical supplies, the laying off of hospital workers, and the closure of hospital floors and service areas.32,33 ,34 ,35 The debt crisis has also contributed to health provider shortages, as specialists and subspecialists leave the island for better opportunities on the U.S. mainland,36,37,38 resulting in longer waits for procedures and overcrowded emergency rooms.39 After several months of congressional debate, the Puerto Rico rescue bill known as PROMESA was signed into law on June 30, 2016. The law places Puerto Rico’s fiscal affairs under a federal oversight board, allows for the restructuring of some of Puerto Rico’s debts, and includes a temporary stay on bondholder lawsuits.40 While the law represents a first step toward economic recovery, it does not address the critical issues facing Puerto Rico’s health care system, including the impending expiration of ACA funding, the limits imposed by the capped Medicaid financing structure, or the mounting cases and future consequences of Zika on the island.
The Kaiser Family Foundation State Health Facts. “Cases of Zika Virus Disease in the United States.” Data Source: Centers for Disease Control and Prevention (CDC), Zika virus disease in the United States, 2015-2016, as of Sept. 14, 2016. ↩︎
Kaiser Family Foundation analysis of U.S. Census Bureau, 2014 American Community Survey, 1-Year estimates. ↩︎
Bureau of Labor Statistics, “Regional and State Employment and Unemployment,” March 2016. ↩︎
Kaiser Family Foundation estimates based on the Census Bureau’s 2014 American Community Survey, 1-year estimates. ↩︎
The District of Columbia is also subject to a statutorily set FMAP, which is 70%. The Kaiser Family Foundation State Health Facts. “Federal Medical Assistance Percentage (FMAP) for Medicaid and Multiplier, FY 2017,” Data Source: FY 2017: Federal Register, November 25, 2015 (Vol 80, No. 227), pp 73779-73782. Accessed September 21, 2016. ↩︎
Maria Portela and Benjamin D. Sommers, “On the Outskirts of National Health Reform: A Comparative Assessment of Health Insurance and Access to Care in Puerto Rico and the United States,” The Milbank Quarterly, 93 no. 3 (2015): 584-608, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4567854/. ↩︎
Puerto Rico provides CHIP coverage to children in families with incomes up to 266% of the Puerto Rico poverty level, or 100% FPL for a family of three. Annie Mach, Puerto Rico and Health Care Finance: FAQs, (Washington, D.C: Congressional Research Service, February 2016), https://www.fas.org/sgp/crs/row/R44275.pdf. ↩︎
“Puerto Rico, Information on How Statehood Would Potentially Affect Selected Federal Programs and Revenue Sources,” U.S. Government Accountability Office, Report to Congressional Requesters, March 2014, http://www.gao.gov/assets/670/661334.pdf. ↩︎