KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
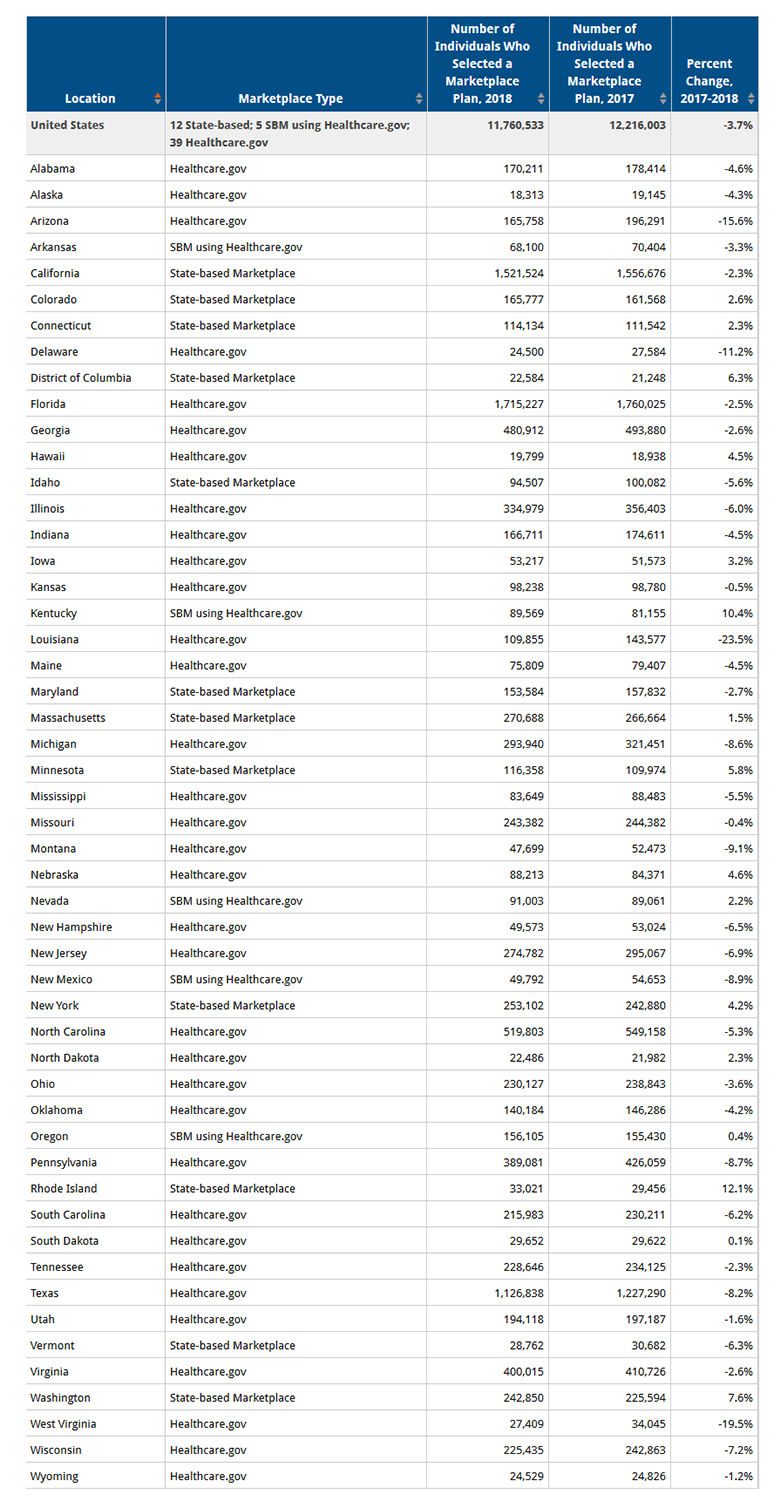
Overall ACA marketplace signups for 2018 dropped by 3.7 percent compared to last year’s enrollment period, a new analysis from the Kaiser Family Foundation finds.
11,760,533 people signed up for 2018 health insurance coverage on the ACA individual marketplaces, amid steep reductions in federal funding for outreach and navigators, an enrollment period half as long, and a climate of political uncertainty surrounding the law. The federal government also terminated cost-sharing subsidy payments to insurers in advance of the open enrollment period, leading to increases in premiums but also increased premium subsidies for many consumers that in some cases led to reductions in what they had to pay for coverage.
As a group, the 15 states plus the District of Columbia with state-based marketplaces, including those using the Healthcare.gov enrollment platform, exceeded last year’s totals this year by .2 percent, while the 34 states that relied on the federal healthcare.gov marketplace saw total signups drop by about 5.3 percent. State-based marketplaces control their own funding for outreach and consumer assistance.
Fifteen states and the District of Columbia exceeded 2017 signups in 2018 – eight of these were state-based marketplaces, three were state-based marketplaces using the Healthcare.gov enrollment platform (KY, NV, and OR), and five were federal Healthcare.gov marketplaces.
Rhode Island (12.1%), Kentucky (10.4%), and Washington State (7.6%) saw the largest share increases in signups, while Louisiana (-23.5%), West Virginia (-19.5%), and Arizona (-15.6%) had the largest drop in shares of signups.
Health centers play an important role in our health care system, providing comprehensive primary care services as well as dental, mental health, and addiction treatment services to over 25 million patients in medically underserved rural and urban areas throughout the country. Health care anchors in their communities and on the front lines of health care crises, including the opioid epidemic and the current flu outbreak, health centers rely on federal grant funds to support the care they provide, particularly to patients who lack insurance coverage. However, the Community Health Center Fund (CHCF), a key source of funding for community health centers, expired on September 30, 2017, and has since been extended through only March 31, 2018. The CHCF provides 70% of grant funding to health centers. With these funds at risk, health centers have taken or are considering taking a number of actions that will affect their capacity to provide care to their patients. This fact sheet presents preliminary findings on how health centers are responding to the funding uncertainty.
A key source of federal funding for #communityhealthcenters expired on September 30, 2017 and has not been renewed for the long term. How are centers responding to the funding delay?
What Funding Is at Stake for Health Centers
The Community Health Center Fund represents 70% of federal grant funding for health centers. Established by the Affordable Care Act, the CHCF increased federal grant fund support for health centers, growing from $1 billion in 2011 to $3.6 billion in 2017.1 Authorized for five years beginning in 2010, and extended for two years through September 2017, the CHCF also provided a more stable source of grant funding for health centers that was separate from the annual appropriations process. Prior to the CHCF, federal 330 grant funds were appropriated annually. In fiscal year 2017, federal section 330 grant funding totaled $5.1 billion, $3.6 billion from the CHCF and $1.5 billion from the annual appropriation.
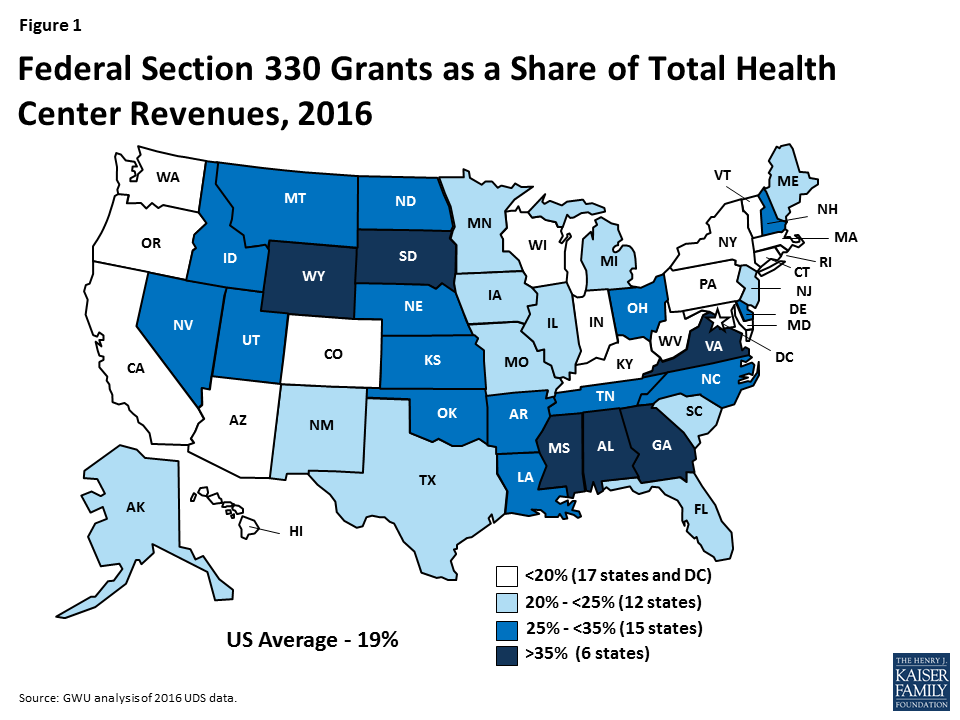
Federal health center grants represent nearly one-fifth of health center revenues. Federal Section 330 grant funds are the second largest source of revenues for health centers behind revenues from Medicaid. Overall, 19% of health center revenues (including US territories) come from federal grants; however, reliance on 330 grant funds varies across health centers. Federal grant funds are especially important for health centers in southern and rural non-expansion states where Medicaid accounts for a smaller share of revenue (Figure 1).2 These funds finance care for uninsured patients and support vital services, such as transportation and case management, that are not typically covered by insurance
Figure 1: Federal Section 330 Grants as a Share of Total Health Center Revenues, 2016
How Are Health Centers Responding to the Loss of Federal Funds?
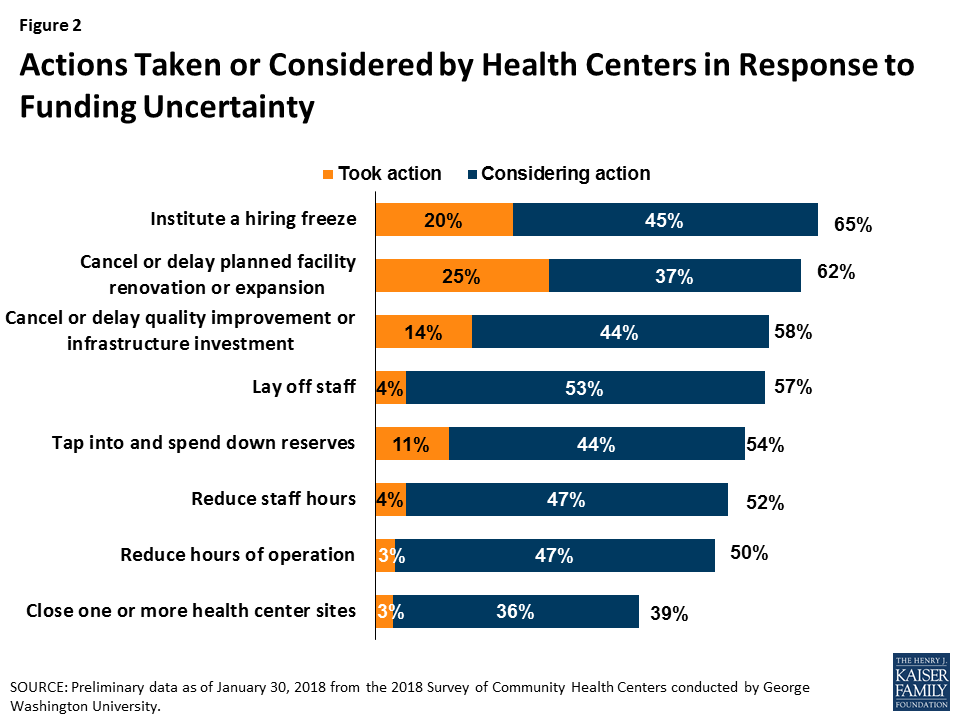
Health centers have taken or are considering taking a number of actions that will affect their ability to serve their patients. Overall, seven in ten responding health centers indicated they had taken or planned to take action to put off large expenditures or curtail expenses in face of reduced revenue. Some of these actions involve delaying or canceling capital projects and other investments or tapping into reserve funds. Other actions, however, have or will reduce the number of staff or the hours they work, which may in turn, affect the availability of services. Already 20% of health centers reported instituting a hiring freeze and 4% have laid off staff. Another 45% are considering a hiring freeze and 53% said they might lay off staff. While health centers seemed to focus on shorter-term actions that could easily be reversed were funding to be restored, 3% of responding health centers had already taken steps to close one or more sites and an additional 36% indicated they are considering doing so (Figure 2).
Figure 2: Actions Taken or Considered by Health Centers in Response to Funding Uncertainty
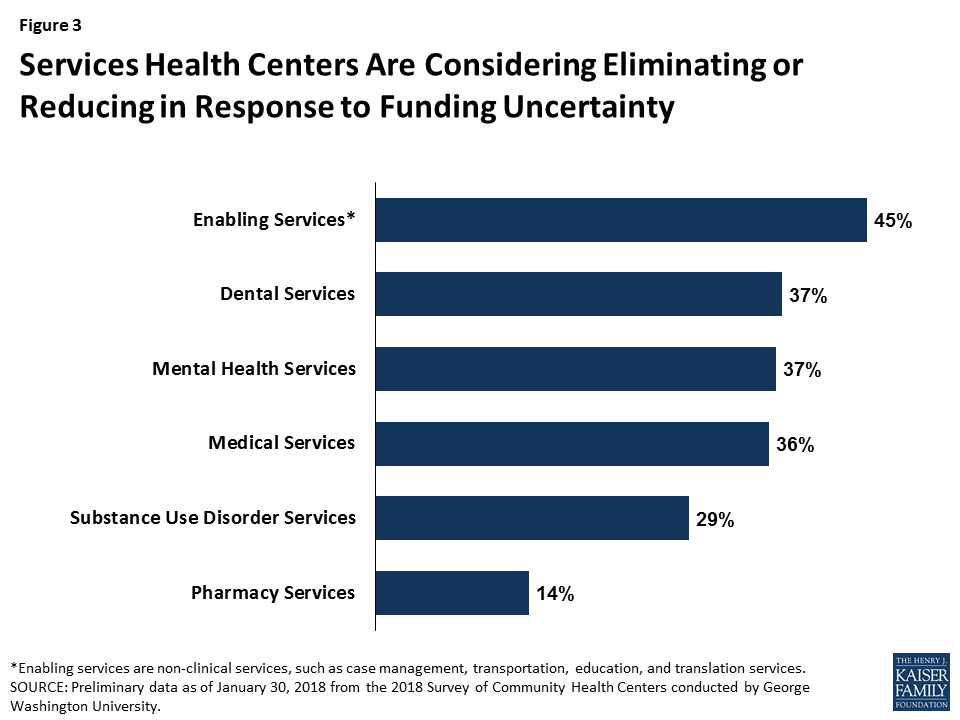
Health centers are considering cuts to patient services. While most health centers have not yet taken steps to cut or reduce patient care services, many reported they are weighing such actions if funding is not restored (Figure 3). Over four in ten indicated they might eliminate or reduce some enabling services, such as case management, translation, or transportation services. Additionally, over a third of reporting health centers indicated they might have to reduce the dental, medical, and/or mental health services they provide while 29% said cuts to addiction treatment services are being contemplated. Fewer health centers reported that cuts to pharmacy services might be made.
Figure 3: Services Health Centers Are Considering Eliminating or Reducing in Response to Funding Uncertainty
What Are the Implications of the Funding Delay?
Continued delays in restoring funding will likely lead to cuts in health center services and staff. To date, health centers have tried to mitigate the effects of the funding delay by forgoing major investments or dipping into reserve funds. However, the longer the funding delay continues, the greater the likelihood health centers will be compelled to cut services and staff, actions they are currently considering but have not yet adopted in large numbers. These cuts could reverse gains health centers have made in recent years in increasing patient care capacity and expanding the range of services they provide, particularly in the areas of mental health and addiction treatment. Health centers play a particularly important role in rural and medically underserved areas. The failure to reauthorize the CHCF and restore health center funding could jeopardize access to care for millions of vulnerable patients.
This analysis is based on preliminary data from the 2018 Survey of Community Health Centers designed by George Washington University’s Geiger Gibson/RCHN Community Health Foundation Research Collaborative and the Kaiser Family Foundation.
Appendix Table 1: Health Center Delivery Sites, Patients, and Revenues, by State, 2016
State
Number of Health Centers
Number of Delivery Sites
Total Patients
Total Patient Visits
Total Revenues
Federal BHPC Funding as Share of Total Revenues
Alabama
14
128
347,694
1,084,685
$173,627,218
44%
Alaska*
28
183
113,027
545,430
$316,966,135
20%
Arizona*
21
159
548,487
2,080,644
$506,266,156
16%
Arkansas*
12
120
195,397
721,288
$157,423,550
30%
California*
176
1,529
4,438,827
20,078,878
$4,922,877,855
12%
Colorado*
20
202
594,959
2,446,065
$571,663,876
17%
Connecticut*
16
250
373,182
1,943,325
$376,031,580
14%
Delaware*
3
15
49,900
171,842
$37,114,507
35%
District of Columbia*
8
60
178,324
874,310
$239,842,150
10%
Florida
48
535
1,397,966
5,276,142
$1,033,408,471
21%
Georgia
35
225
457,644
1,437,176
$294,596,676
37%
Hawaii*
14
75
152,155
715,612
$181,561,177
15%
Idaho
14
87
171,126
658,290
$174,323,258
26%
Illinois*
45
402
1,265,889
4,665,853
$897,271,451
21%
Indiana*
25
183
473,237
1,675,508
$343,283,730
20%
Iowa*
14
72
188,969
680,595
$163,280,598
25%
Kansas
18
61
193,843
582,658
$123,037,617
29%
Kentucky*
23
232
423,515
1,609,691
$344,167,330
20%
Louisiana*
34
229
384,893
1,409,006
$288,753,388
31%
Maine
18
130
186,039
818,065
$179,110,303
23%
Maryland*
17
126
313,411
1,478,011
$370,440,582
14%
Massachusetts*
39
288
751,918
3,839,821
$1,044,753,296
11%
Michigan*
39
262
672,753
2,554,782
$580,783,107
21%
Minnesota*
16
77
174,811
675,680
$171,499,152
22%
Mississippi
21
203
295,052
887,060
$177,107,230
41%
Missouri
28
228
527,054
1,925,230
$431,807,263
23%
Montana*
17
79
106,342
407,084
$104,950,776
34%
Nebraska
7
48
84,556
296,136
$72,574,862
26%
Nevada*
5
35
88,962
275,210
$73,240,156
25%
New Hampshire*
11
42
89,280
380,772
$89,972,159
25%
New Jersey*
23
144
511,947
1,892,603
$330,427,532
24%
New Mexico*
17
195
320,163
1,482,714
$298,922,222
23%
New York*
65
654
2,038,538
9,468,465
$2,023,496,947
12%
North Carolina
38
229
508,599
1,771,333
$370,692,573
33%
North Dakota*
4
22
40,331
133,261
$35,312,258
29%
Ohio*
45
271
667,007
2,326,809
$465,135,801
29%
Oklahoma
20
98
200,937
699,203
$155,357,831
34%
Oregon*
31
212
383,691
1,723,557
$570,120,560
15%
Pennsylvania*
44
264
774,921
2,660,676
$588,427,739
19%
Rhode Island*
8
55
164,057
683,021
$162,316,505
16%
South Carolina
22
176
374,257
1,386,551
$349,309,120
23%
South Dakota
5
48
69,137
239,716
$55,349,502
35%
Tennessee
29
182
396,877
1,413,029
$244,800,059
32%
Texas
73
466
1,309,020
4,918,538
$1,100,636,445
22%
Utah
13
56
151,250
496,233
$125,521,294
28%
Vermont*
11
66
171,828
677,293
$147,117,961
14%
Virginia
26
145
304,756
1,093,227
$217,530,129
38%
Washington*
27
306
1,035,629
4,188,973
$1,084,448,992
12%
West Virginia*
27
301
430,084
1,682,705
$338,912,992
19%
Wisconsin
17
115
303,266
1,147,896
$296,292,458
14%
Wyoming
6
10
17,582
53,786
$17,277,753
44%
US Total
1,337
10,280
25,413,089
102,334,438
$23,419,142,282
18%1
NOTES: * Medicaid expansion state. 1 US Total excludes territories. SOURCE: GWU analysis of 2016 UDS data
C. Stephen Redhead et al., Discretionary Spending Under the Affordable Care Act, (Congressional Research Services, 2017), available at https://fas.org/sgp/crs/misc/R41390.pdf (Accessed online January 230, 2018) ↩︎
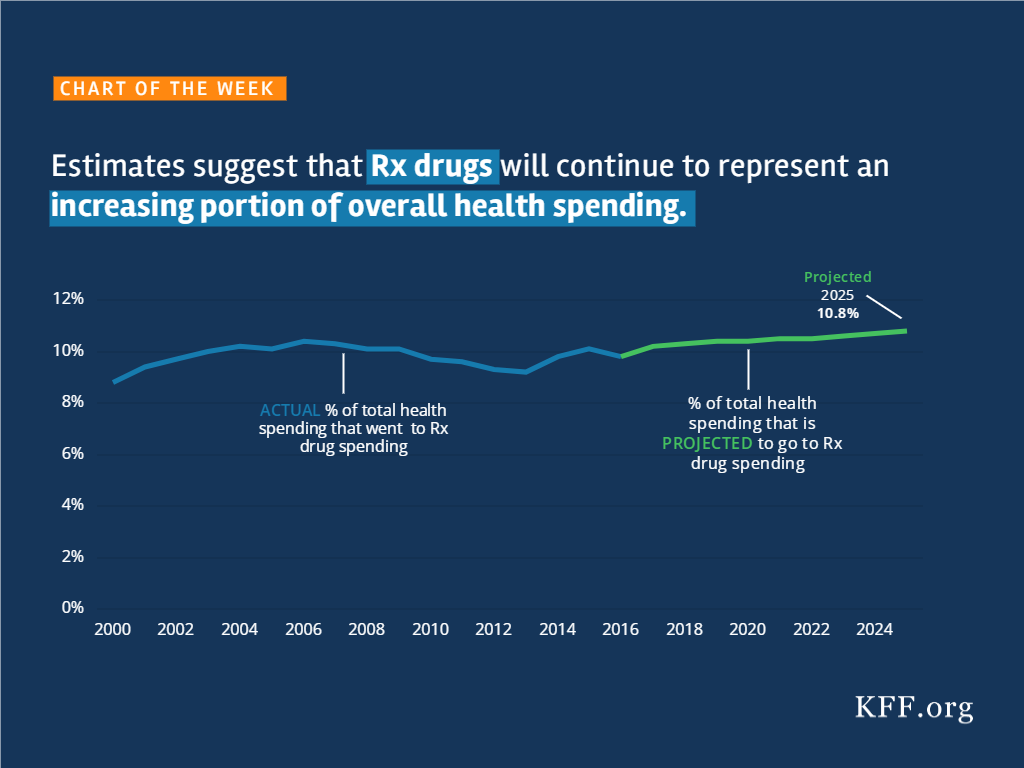
Source: Kaiser Family Foundation analysis of National Health Expenditure (NHE) Historical (1960-2016) and Projected (2016-2025) data from Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group (Accessed on December 13, 2017)
Note: the DC federal district court issued a decision in Stewart v. Azar on June 29, 2018. See our explainer.
On January 11, 2018, the Centers for Medicare and Medicaid Services (CMS) issued a State Medicaid Director letter announcing a new policy that, for the 1st time, allows states to condition Medicaid on participation in a work or “community engagement” program. The next day, CMS approved a new Medicaid waiver in Kentucky. The waiver includes a program called Kentucky HEALTH, which encompasses a work requirement as well as coverage lockouts of up to 6 months for failure to pay monthly premiums (up to 4% of income), timely renew eligibility, or timely report a change in circumstances, among other provisions. Kentucky HEALTH applies to most nonelderly adults, including low-income parents and expansion adults. The state plans to implement Kentucky HEALTH by July, 2018. On January 24, 2018, 15 Kentucky Medicaid enrollees filed a lawsuit in the U.S. District Court for the District of Columbia challenging CMS’s authority to issue the work requirement policy and approve the Kentucky waiver. This issue brief answers 5 key questions about the case.1
A guide to the lawsuit challenging CMS’s approval of the #Kentucky HEALTH #Medicaid #waiver and its #workrequirements.
Key Questions
1. Who are the Parties In the Lawsuit?
The complaint describes the 15 plaintiffs as “housekeepers and custodians, ministers and morticians, car repairmen, retired workers, students, church administrators, bank tellers, caregivers, and musicians.” They range in age from 20 to 62, and rely on Medicaid for services such as check-ups, treatment for chronic conditions such as diabetes and high blood pressure, mental health and substance use disorder counseling, prescription drugs, and vision and dental care. For example,
Ronnie Maurice Stewart is retired at 62 because he is no longer able to be on his feet all day. He receives $841 per month in Social Security benefits. Medicaid covers his treatment for chronic conditions, including diabetes, arthritis, high blood pressure, and cataracts. Before receiving Medicaid in 2014, he was unable to afford insurance.
Michael “Popjaw” Woods is 52 and owns a car repair center. His wife, Sara, 40, cleans houses and cares for their infant granddaughter and a neighbor’s child. Their income varies weekly. Both were uninsured prior to enrolling in Medicaid in 2014. With Medicaid, Mr. Woods has been able to get care for his blood pressure, which had been untreated. Mrs. Woods has received treatment for debilitating migraines and has been sober for nearly 3 years after receiving substance abuse treatment and suboxone covered by Medicaid.
Shawna Nicole McComas is 34 and married with 4 children. She works full-time in housekeeping, where her hours vary weekly, depending on overtime. She has chronic pain from osteoarthritis and a congenital hip condition and sees multiple specialists. She takes the bus 90 minutes each way to doctor appointments because the family does not have a car.
David Roode is 39 years old and married without children. He is a self-employed classical musician, and his hours and income fluctuate monthly. He relies on Medicaid for regular preventive health care.
The defendants are the U.S. Department of Health and Human Services (HHS), CMS, and their principal officials, including the HHS Acting Secretary, the CMS Administrator and Principal Deputy Administrator, and the Director of the CMS Center for Medicaid and CHIP Services.
2. What are the Plaintiffs Asking the Court to do?
The plaintiffs are asking the court to declare that the work requirement policy and Kentucky’s waiver are illegal and cannot be implemented because they violate the Administrative Procedures Act (APA), the Medicaid provisions of the Social Security Act, and the President’s Constitutional duty to take care that laws are faithfully executed. The plaintiffs argue that HHS “bypass[ed] the legislative process and act[ed] unilaterally to ‘comprehensively transform’ Medicaid” using a “narrow statutory waiver authority” that has “effectively rewritten the statute.” The plaintiffs argue that the Kentucky waiver puts them at risk of losing Medicaid by creating new eligibility criteria that they contend are beyond HHS’s authority, such as the work requirement and the highest premiums ever permitted in Medicaid. In support, they cite Kentucky’s waiver application, which projects 95,000 fewer enrollees and $2.5 billion less in spending over five years.
The lawsuit challenges the Kentucky HEALTH program as a whole and several individual provisions, including the work requirement; premiums and associated coverage delays, penalties and lockout; increased cost-sharing for non-emergency use of the emergency room; coverage lockouts for failure to timely renew eligibility or report a change in circumstances; and elimination of retroactive coverage and non-emergency medical transportation. It also points out that the work requirement policy, on which the Kentucky waiver is based, was issued after the public comment period for the waiver closed.
3. What Has CMS Said About Its Authority to Issue the New Policy and Approve the Kentucky Waiver?
CMS’s new policy explains that it is allowing waivers to test whether “requiring work or community engagement. . . will result in more beneficiaries being employed or engaging in other productive community engagement, thus producing improved health and well-being.” CMS has determined that programs “designed to promote better mental, physical, and emotional health” or, separately, “to help individuals and families rise out of poverty and attain independence” will further program objectives. CMS explains that there are other determinants of health in addition to high-quality health care and cites “a growing body of evidence suggest[ing] that targeting certain health determinants, including productive work and community engagement, may improve health outcomes.” The guidance acknowledges that “[t]his is a shift from prior agency policy” but maintains that “it is anchored in historic CMS principles that emphasize work to promote health and well-being.” For example, CMS cites the Medicaid buy-in option, which expands financial eligibility to enable working people with disabilities to maintain coverage, and the option to provide supported employment services to people with disabilities, although “receipt of these supports is not a condition of eligibility or coverage.”
In a letter accompanying the Kentucky waiver, CMS explains that the waiver is “likely to assist in improving health outcomes;. . . address behavioral and social factors that influence health outcomes;. . . incentivize beneficiaries to engage in their own health care and achieve better health outcomes; and. . . familiarize beneficiaries with a benefit design that is typical of what they may encounter in the commercial market and thereby facilitate smoother beneficiary transition to commercial coverage.”
4. What are the Legal Questions for the Court?
HHS relied on its authority under Section 1115 of the Social Security Act to issue the work requirement policy and the Kentucky waiver. Section 1115 permits the HHS Secretary to waive certain provisions of federal Medicaid law to allow states to undertake experimental, pilot or demonstration projects that the Secretary determines will further program objectives. Under the APA, the court will review the administrative record to determine if HHS acted lawfully. The court can set aside agency action that is “arbitrary, capricious, an abuse of discretion, or otherwise not in accordance with law,” contrary to the Constitution, outside the scope of the agency’s statutory authority, issued without required procedures, unsupported by substantial evidence, or unwarranted by the facts.2 The court might consider whether the work policy and the Kentucky waiver qualify as an experiment; whether the Secretary exceeded his authority when determining that the new policies further Medicaid objectives; whether the new policies are supported by evidence in the administrative record; and whether the work policy should have been issued using formal notice and comment rule-making.
5. What are the Next Steps?
The defendants have 60 days to respond to the complaint. They also need to file with the court the administrative record that forms the basis of the agency’s decisions. The plaintiffs are seeking to have the case certified as a class action on behalf of all Kentucky residents enrolled in Medicaid on or after January 12, 2018, a group that they anticipate numbers in the hundreds of thousands. The plaintiffs also are asking the court for a preliminary injunction, which would prevent implementation of the work policy and the Kentucky waiver until a final decision in the case.
Looking Ahead
While the Kentucky lawsuit proceeds, there are currently 9 other states (AR, AZ, IN, KS, ME, MS, NH, UT, & WI) with pending waiver applications seeking work requirements for expansion adults and/or low-income parents. Policymakers and other stakeholders in these states will be watching the Kentucky case to see how CMS responds to the complaint and what the court decides and waiting to see whether CMS approves more waivers with work requirements, on what terms, and whether litigation follows in other states.
Endnotes
No. 1:18-cv-00152. The case is currently known as Stewart v. Hargan but is likely to change to Stewart v. Azar with the confirmation of the new HHS Secretary. ↩︎
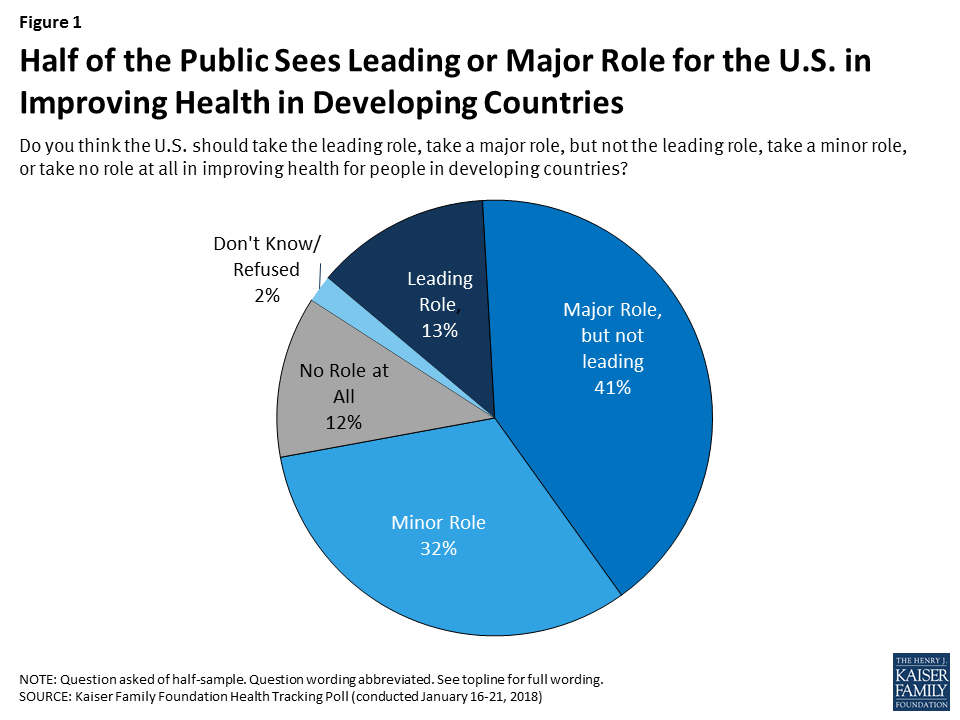
A new Kaiser Family Foundation issue brief assessing global health policy one year after President Trump took office finds half of Americans (54%) say they want the U.S. to play a major or leading role in improving health for people in developing countries, though support for such engagement is strongest among Democrats (73%) and lower among independents (47%) and Republicans (49%). The brief identifies a mix of challenges to U.S. global health policy, some of which pre-dated President Trump and some of which are the result of decisions and actions of the Administration.
Overall public support fell slightly from the last time the Foundation polled on this issue in 2016, when 61 percent said they think the U.S. should take a leading or major role.
Most of the public (59%) believes the U.S. is spending the right amount or too little on global health programs, but one-third (33%) believe the U.S. is spending too much – a significant increase from the 18 percent saying the U.S. was spending too much in 2016. Fifty-three percent say the Trump Administration has made global health a lower priority than previous administrations.
Against this backdrop of broad public support, the Trump Administration has instituted a number of notable changes in broader U.S. foreign policy that emphasize U.S. interests and affect global health, and in the area of global health specifically, proposed steep budget cuts and implemented policy changes, including the reinstatement and expansion of the Mexico City Policy. However, U.S. global health funding has so far been buoyed by strong bipartisan support from Congress and key stakeholders.
Looking ahead, the U.S. global health policy issues to watch for in 2018 and beyond include the soon-to-be released White House budget request for FY 2019, amidst ongoing budget pressures and concerns about the U.S. deficit; continuing implementation of the Mexico City Policy; decisions around the next phase of the President’s Emergency Plan for AIDS Relief; and the future of the Global Health Security Agenda, among others.
This month marks one year since Donald Trump became the 45th President of the United States after winning the election on a populist, “America-First”, platform. Since then, there have been many questions raised about what a Trump Presidency would mean for U.S. global health policy in light of statements on scaling back foreign aid and a skepticism of the value of multilateral institutions and key international agreements. Historically, global health has enjoyed bipartisan support and been highlighted as a major area of success for the United States. Funding for global health rose significantly in the last decade and, although it has leveled off, it still represents the largest component of U.S. foreign assistance (an estimated 24% in FY 2017).
In this brief, we take stock of the U.S. global health response on the occasion of one year of the Trump Presidency and look ahead to the global health policy issues that are likely to be front and center in the coming months and years. Overall, there are a mix of challenges facing the U.S. global health response, some of which pre-dated Trump and others that are the result of decisions and actions of the administration, including proposals to significantly scale back funding. At the same time, global health programs still enjoy strong bipartisan support in Congress and, according to our just-released poll, about half of the public still wants the U.S. to play a major or leading role in improving health in developing countries (see Figure 1 and Appendix).
Figure 1: Half of the Public Sees Leading or Major Role for the U.S. in Improving Health in Developing Countries
DIAGNOSIS
Administration Actions Have Led to Foreign Policy Upheaval
In keeping with the “America First” campaign and promises to re-examine the U.S. role in world affairs, the Trump Administration has made a number of notable changes in broader U.S. foreign policy that affect global health. These include the administration’s decision to withdraw from the Paris Climate Accord, its criticism of and new demands for U.S. engagement in the context of international trade agreements such as the Trans-Pacific Partnership (TPP) and North American Free Trade Agreement (NAFTA), and skepticism of, and intent to reduce U.S. support for the United Nations and potentially other multilateral organizations. More recently, the administration has proposed to cut foreign aid to countries that voted counter to U.S. government wishes at the UN. While this threat is not without precedent, it is a departure from U.S. policy over the prior two decades, and underscores the administration’s theme of emphasizing U.S. interests over other considerations.
The Trump Administration has also sought to make its mark on the agencies that carry out U.S. foreign policy, including the State Department and the U.S. Agency for International Development (USAID). Following a March 2017 White House Executive Order on reorganizing the executive branch, Secretary of State Rex Tillerson has attempted to re-organize and reform these agencies. One potential move that was feared by many was the idea of “merging” USAID and the State Department – the two currently exist as quasi-independent – but to date there is no evidence of such a change being actively pursued. At the same time, budget requests from the White House have demonstrated the administration’s desire to make significant cuts to these agencies’ budgets, and their day-to-day management has been criticized by current and formeremployees. In addition, there has been decidedly slow progress in nominating and appointing staff for key foreign policy leadership posts, along with a notable exodus of experienced staff over the last year. For example, as of this writing, President Trump had nominated far fewer candidates at the State Department (89) compared to Presidents Obama (137) and George W Bush (153) at the same point in their first terms.
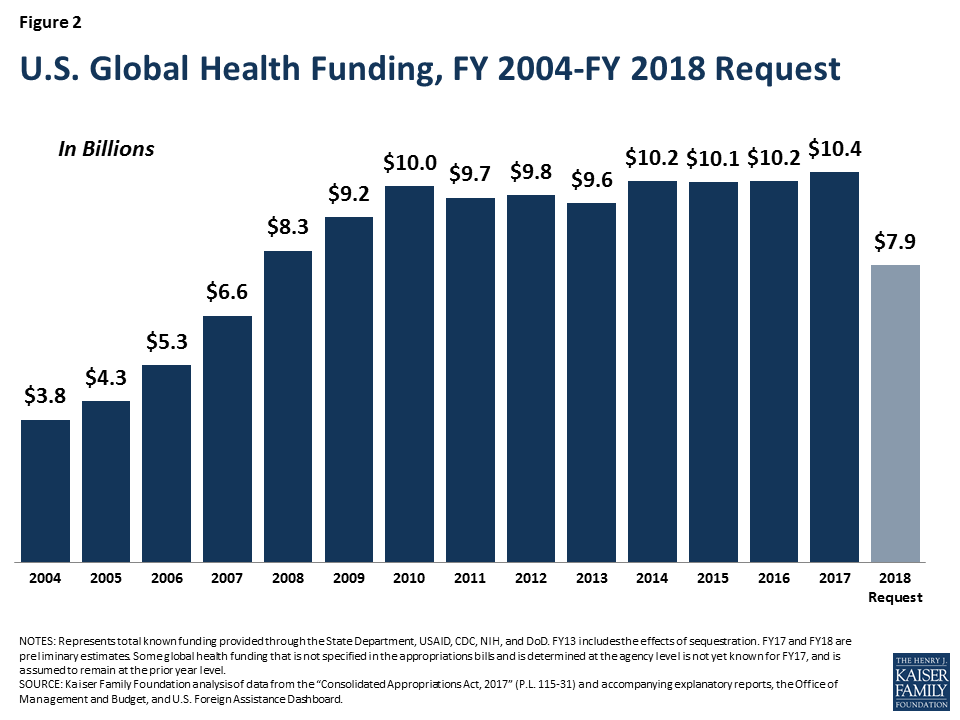
A lack of ambassadors in some countries, needed staff appointments in some positions, a shifting stance on human rights, and a shrinking foreign policy workforce have concerning implications for planning and carrying out U.S. global health programs. Such difficulties for global health have been compounded by certain policy decisions, including proposals to significantly cut U.S. global health funding (see Figure 2).
Figure 2: U.S. Global Health Funding, FY 2004-FY 2018 Request
The most concrete global health policy change of the administration to date came on the first Monday of President Trump’s term, in the form of a re-instatement and expansion of the Mexico City Policy. The Policy, which was in effect and applied to family planning assistance in previous Republican administrations, was not only re-instated but also expanded to encompass almostall global health assistance, increasing the number of organizations and the amount of funding affected by the policy. We found the expanded policy applies to more than $7 billion in funding and likely affects more than one thousand foreign NGOs. In addition, on March 30 the administration invoked the “Kemp-Kasten amendment” to withhold funding for the United Nations Population Fund (UNFPA), the lead U.N. agency focused on global population and reproductive health, as has been done in previous Republican administrations.
The administration’s request to significantly cut global health funding is unprecedented. For FY2018 the White House proposed cuts of over $2B to global health, representing a 23% overall reduction compared to FY2017; these included a proposed reduction to PEPFAR of more than $1 billion and a zeroing out of the family planning budget, among others. Multiple analyses of the potential impacts of such cuts conclude that serious negative health consequences would result, including many more infections and deaths from HIV and TB, and an increase in the number of abortions along with greater maternal mortality. None of these requested cuts have been enacted but this is the first time cuts of this magnitude have been proposed, and they mark a significant shift from the direction and emphasis of prior administrations.
Even as they have implemented more restrictive policies and proposed cuts, Trump Administration officials have publicly stated support for select U.S. global health priorities. In his first major speech to the United Nations in September, for example, President Trump highlighted three major U.S. global health areas of success: PEPFAR, the President’s Malaria Initiative, and the Global Health Security Agenda (GHSA). Secretary of State Tillerson has also spoken about the importance of PEPFAR and the GHSA; the U.S. has signaled its intention to remain engaged in the larger GHSA effort, and has even highlighted the importance of global health security in the newly revised U.S. National Security Strategy, and is expected to do the same in a forthcoming national biodefense strategy. Despite the foreign policy vacancies noted above, some global health and development leaders have remained in their roles since the Obama Administration, including the U.S. Global AIDS Coordinator and the Director of the National Institutes of Health, while other key positions have been filled by President Trump, including the new USAID Administrator who has a strong record in global health, the Director of the Centers for Disease Control and Prevention, and leadership on global health within the White House National Security Council.
Congress Pushes Back
Congress has also continued to play a significant role in global health, including bipartisan and bicameral push back against proposed funding cuts. Funding for global health was kept at FY 2017 levels and, while not yet final, will likely be level in FY2018 as well. Moreover, Congress has asserted its role in directing global health efforts by including, for the first time, language in the FY 2017 budget legislation that prevents the administration from changing global health program funding levels. Congress also included language requiring a report before any reorganization of State and USAID could occur. Many stakeholders, including current and former U.S officials, the faith community, and members of the military, have also pushed back on the administration’s proposed cuts to global health and development.
U.S. Public Support for Global Health Continues, Though with Some Declines & Partisan Divisions
Our latest (January 2018) tracking poll assessed public support for U.S. engagement in global health in the Trump era. The public perceives the Trump Administration as less supportive of global health, with half (53%) saying the Trump Administration has made global health a lower priority than previous administrations.
As mentioned above, about half of the public (54%) say they want the U.S. to play a leading or major role in improving health for people in developing countries. Support for such engagement is strongest among Democrats (73%), who also are more likely to support the U.S. playing “a leading role” (20%), and lower among independents (47%) and Republicans (49%), see Figure 3; Trump supporters are not interested in the U.S. playing a leading role (just 4% say they believe this). However, overall support fell slightly from 2016, when 61% said they think the U.S. should take a leading or major role.
Figure 3: Support for U.S. Role in Improving Health in Developing Countries by Party Identification
Most of the public (59%) believe the U.S. is spending the right amount or not enough on global health programs, but one-third (33%) believe the U.S. is spending too much – a significant jump from the 18% saying we were spending too much in 2016.
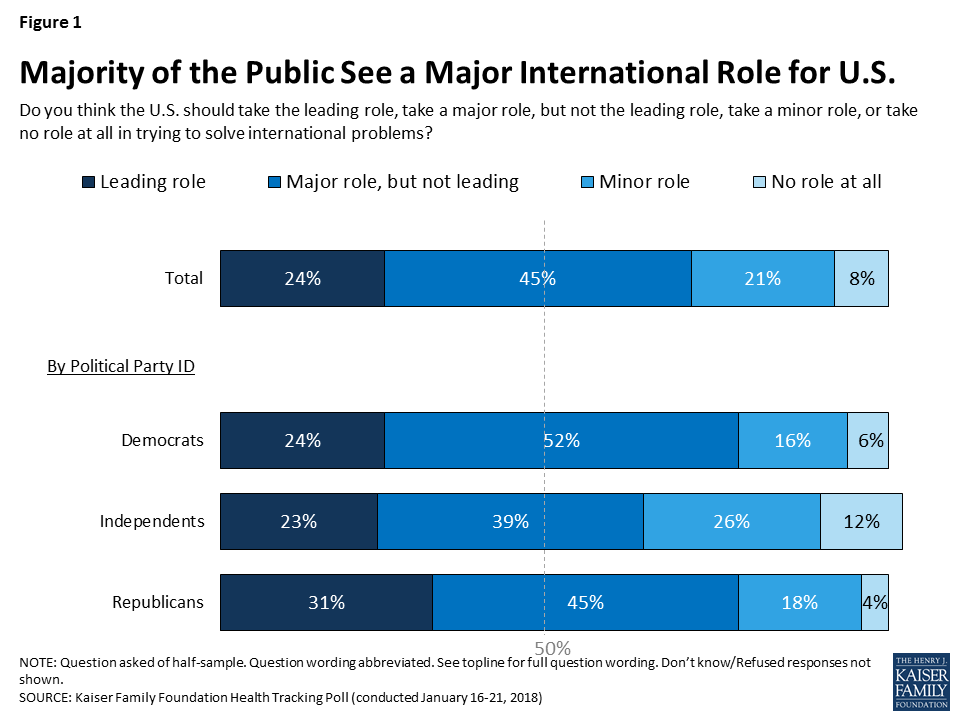
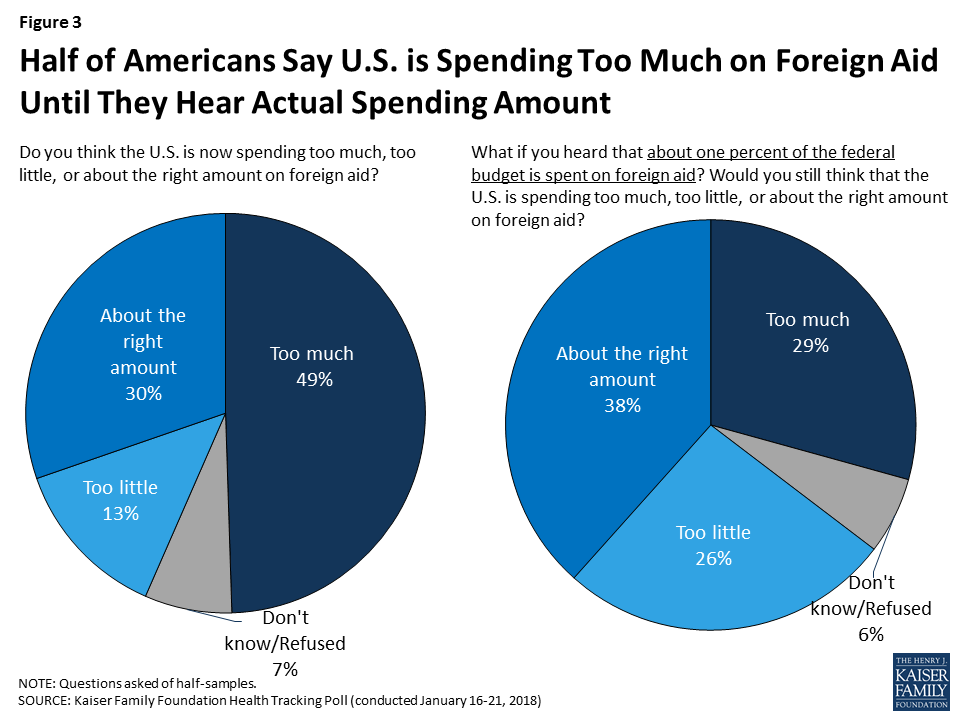
For overall global engagement, the poll numbers indicate a greater proportion of the U.S. public (69%) now believes the U.S. should take at least a major role in solving the world’s problems than in 2016 (57%). The share of Republicans agreeing with this statement grew from 20% in 2016 to 31% in 2018. However, confusion about the amount spent on U.S. foreign aid persists, with half (49%) saying too much is spent in this area but when presented with the actual amount – about 1% of the federal budget goes to foreign aid – people are much less likely (29%) to view that as too much spending (as found in previous polls). See Appendix and poll results for more detailed information.
PROGNOSIS
The push and pull in global health policy will likely continue in 2018 and potentially intensify. On the one hand, actions taken by the administration signal a reduced U.S. engagement in the world and intention to step back further in global health. On the other, U.S. global health programs have so far demonstrated resilience, buoyed by strong support from Congress and key stakeholders.
The tension will likely be tested again in the near term with the soon-to-be released FY 19 White House budget request, which many expect to propose at least the same level of deep cuts to global health. Negotiations will take place within the broader context of greater budget pressures and concerns about the deficit, particularly in wake of recently enacted tax legislation that could tighten discretionary spending, including for foreign assistance, even more.
Beyond that, there will be a number of other issues to watch, including:
Mexico City Policy: The expanded Mexico City Policy, which has only begun to be implemented, will likely be felt in a much more pronounced way in these next months and years including potential gaps in services in the field;
PEPFAR: The administration, Congress, and other stakeholders are beginning to assess whether they want to move forward to reauthorize PEPFAR – the program’s current authorization expires at the end of FY 2018 (though the program will not end and a new reauthorization is not needed to keep it funded). In addition, PEPFAR’s recently launched new strategy, which aims to focus most efforts on 13 priority countries, raises questions about the larger U.S. global AIDS response in the context of potential budget decreases;
Global Health Security Agenda: Key decisions about the next phase of the GHSA, including what to do regarding an impending fiscal cliff as supplemental Ebola funds expire in FY2019, will soon be coming down the pike and the U.S., as a founding and leading member of the partnership, will figure prominently in its future direction; and
Replenishment: Two major global health multilateral partners of the U.S. – the Global Fund and GAVI – will soon begin processes for launching their next replenishment conferences, marking an important moment for gauging future U.S. support.
The key question going forward, then, may very well be which vision of global health will end up holding sway in the political back-and-forth in Washington – that of the White House or Congress? Ultimately, the winners, or losers, of this “battle” will be the people that benefit from U.S. investments around the world.
Appendix
The January 2018 Kaiser Health Tracking Poll examines the public’s perceptions and attitudes about the role of the United States in efforts to improve health for people in developing countries.
#1: Majority of Americans Say the U.S. Should Play a Leading or Major Role in International Affairs
The survey finds that a majority of the public (69 percent), including most Democrats (76 percent), Republicans (76 percent), and independents (62 percent), think the U.S. should take a major or leading role in solving international problems.
Figure 1: Majority of the Public See a Major International Role for U.S.
#2: Smaller Shares – But Still About Half – Say the U.S. Should Play a Leading or Major Role in Improving Health for People in Developing Countries
About half the public (54 percent), including 73 percent of Democrats and around half of independents (47 percent) and Republicans (49 percent), say the U.S. should take a leading or major role in improving health for people in developing countries. About four in ten (41 percent) Trump supporters say the U.S. should take a leading or major role in improving health in developing countries, compared to two-thirds of those who do not approve of President Trump’s job performance.
Figure 2: About Half See a Major Role for U.S. in Improving Health in Developing Countries, Including Most Democrats
#3 Half of Americans Say U.S. Spends Too Much on Foreign Aid, Until They Hear Actual Spending Amount
The poll finds half of the public (49 percent) say that the U.S. is now spending “too much” on foreign aid, while 13 percent say the U.S. is spending “too little” and three in ten say the U.S. is spending “about the right amount.” Yet, after hearing that foreign aid spending is actually about one percent of the federal budget, the share of the public who say spending is “too much” decreases from 49 percent to 29 percent.
Figure 3: Half of Americans Say U.S. is Spending Too Much on Foreign Aid Until They Hear Actual Spending Amount
#4: More Now Say the U.S. Is Spending Too Much on Efforts to Improve Health for People in Developing Countries Compared to Previous Years
Most of the public (59 percent) believes the U.S. is spending “about the right amount” or “too little” on global health programs, but one-third (33%) believe the U.S. is spending “too much” – a significant increase from the 18 percent saying the U.S. was spending “too much” in 2016, the last year the Foundation polled on this issue, but more similar to previous years’ polling.
Figure 4: One-Third Say U.S. Is Spending Too Much on Improving Health for People in Developing Countries
#5: About Half Think Improving Global Health Is a Lower Priority For President Trump and his Administration
About half of the public (53 percent) believe President Trump and his administration have made improving health for people in developing countries a “lower priority” compared to previous administrations, and about one-third (36 percent) say the priority level has been “about the same.” Few (5 percent) say the Trump administration has made it a “higher priority.” When asked how they would like to see President Trump and his administration prioritize improving health for people in developing countries, four in ten Americans (43 percent) say President Trump’s current priority level is “about right.”
Figure 5: About Half Say Global Health Is a Lower Priority in Trump Administration; Four in Ten Think Current Level Is About Right
Health care costs are a substantial and growing burden for many people on Medicare and are projected to consume a larger share of total income over time, according to a new analysis from the Kaiser Family Foundation.
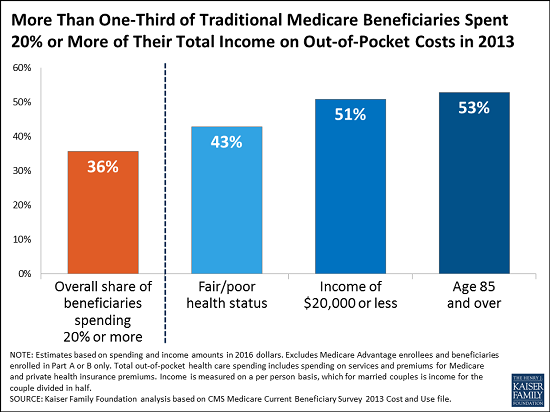
The study, Medicare Beneficiaries’ Out-of-Pocket Health Care Spending as a Share of Income Now and Projections for the Future, finds that more one-third of people with traditional Medicare spent at least 20 percent of their total income on out-of-pocket health care costs in 2013. That included premiums, deductibles and cost sharing for Medicare-covered services, as well as spending on services not covered by Medicare, such as dental and long-term care. The analysis of spending as a share of total income does not include enrollees in Medicare Advantage plans, who account for 19 million of the 59 million people with Medicare. Income is measured on a per person basis, which for married couples is income for the couple divided in half.
While some people with Medicare face relatively low out-of-pocket costs, the financial burden can be especially large for beneficiaries with modest incomes and significant medical needs. For instance, among beneficiaries in traditional Medicare, just over half with incomes below $20,000 and those ages 85 and over spent at least 20 percent of their total income on health expenditures in 2013, along with more than 4 in 10 beneficiaries in fair or poor health status.
Among all Medicare beneficiaries, out-of-pocket costs consumed 41 percent of beneficiaries’ per person Social Security income in 2013, on average. Older women and beneficiaries ages 85 and older tended to have higher average out-of-pocket spending as a share of average Social Security income than others, according to the analysis.
The analysis projects that the health care spending burden among Medicare beneficiaries will rise over time. By 2030, the study projects that under current policies 42 percent of people with traditional Medicare will spend 20 percent of their total income or more on health care costs. Among all people with Medicare, out-of-pocket costs are projected to consume half of the average per person Social Security benefit by 2030.
With rising health care costs representing a growing challenge to the financial security of older adults, these findings have implications for policies that could shift costs on to beneficiaries as part of a broader effort to reduce federal spending on Medicare, Medicaid or Social Security.
Medicaid provides health insurance for over 80 million Americans, including pregnant women, low-income parents, children, seniors, and people with disabilities, while Supplemental Security Income (SSI) is a monthly cash payment to help low-income people with disabilities pay for housing, food, and other basic needs. SSI does not include health insurance, but people who receive SSI generally automatically qualify for Medicaid. SSI enrollees are a subset of all Medicaid enrollees with disabilities. People who receive SSI cash assistance must meet stringent income, asset, and medical eligibility criteria. Many people with disabilities do not receive cash assistance from SSI but still qualify for health insurance from Medicaid through other eligibility pathways.
Proponents of Medicaid work requirements often describe these policies as applying to “able-bodied” adults. Recent guidance from the Centers for Medicare and Medicaid Services (CMS), allowing states for the first time to condition Medicaid eligibility on meeting a work requirement, permits states to target only people who are “eligible on a basis other than disability.” Kentucky’s waiver, the first to include a work requirement (referred to as community engagement),1 applies to Medicaid expansion adults and traditional adults, including low-income parents. As of mid-January, 2018, nine other states have submitted waiver proposals to CMS seeking work requirements (AR, AZ, IN, KS, ME, MS, NH, UT, and WI).
Although the CMS work guidance excludes people who are eligible for Medicaid based on a disability, many adults with disabilities will face Medicaid work requirements because they are eligible for Medicaid on another basis. While Medicaid work requirements could apply to all expansion adults and/or low-income parents, this issue brief focuses on the subset of those with disabilities because they may have difficulty meeting the work requirement or obtaining an exemption due to their health needs. We examine the implications of work requirements for nonelderly Medicaid adults with disabilities who do not receive SSI (referred to as non-SSI adults with disabilities) and compare their work status and functional limitations to those who do receive SSI. The Appendix contains 50-state data.
Key Findings
How Many Medicaid Adults Have a Disability?
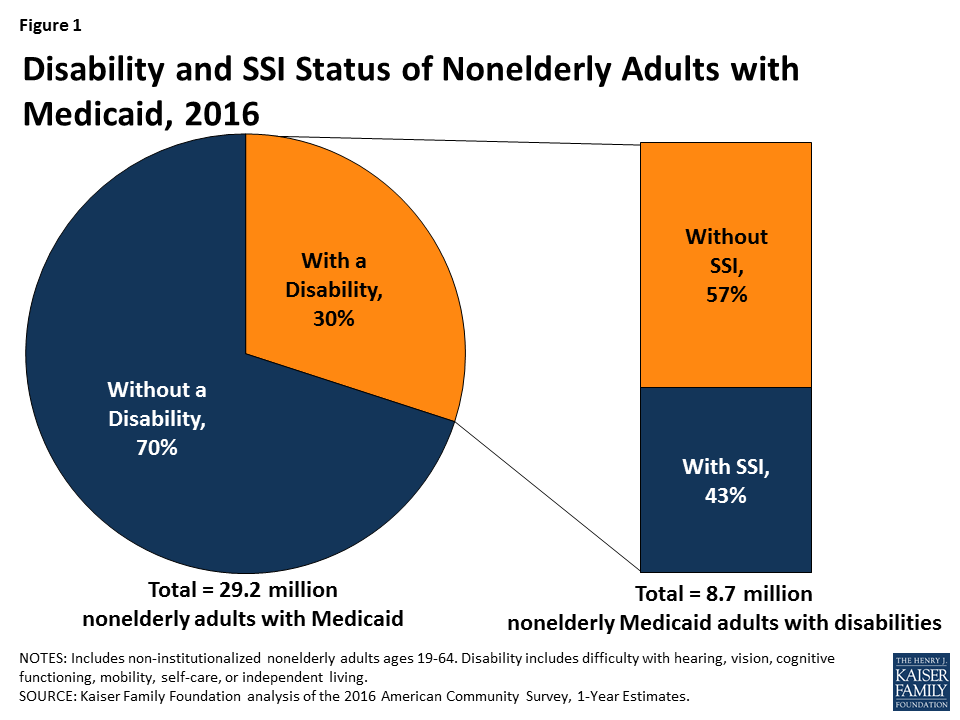
Three in 10 nonelderly adults with Medicaid report having a disability, according to data from the American Community Survey (ACS) (Figure 1). The ACS classifies a person as having a disability if the person reports serious difficulty with hearing, vision, cognitive functioning (concentrating, remembering, or making decisions), mobility (walking or climbing stairs), self-care (dressing or bathing), or independent living (doing errands, such as visiting a doctor’s office or shopping, alone).2 The ACS definition of disability is intended to capture whether a person has a functional limitation that results in a participation limitation and is similar to measures used in other federal surveys, such as the National Health Interview Survey.
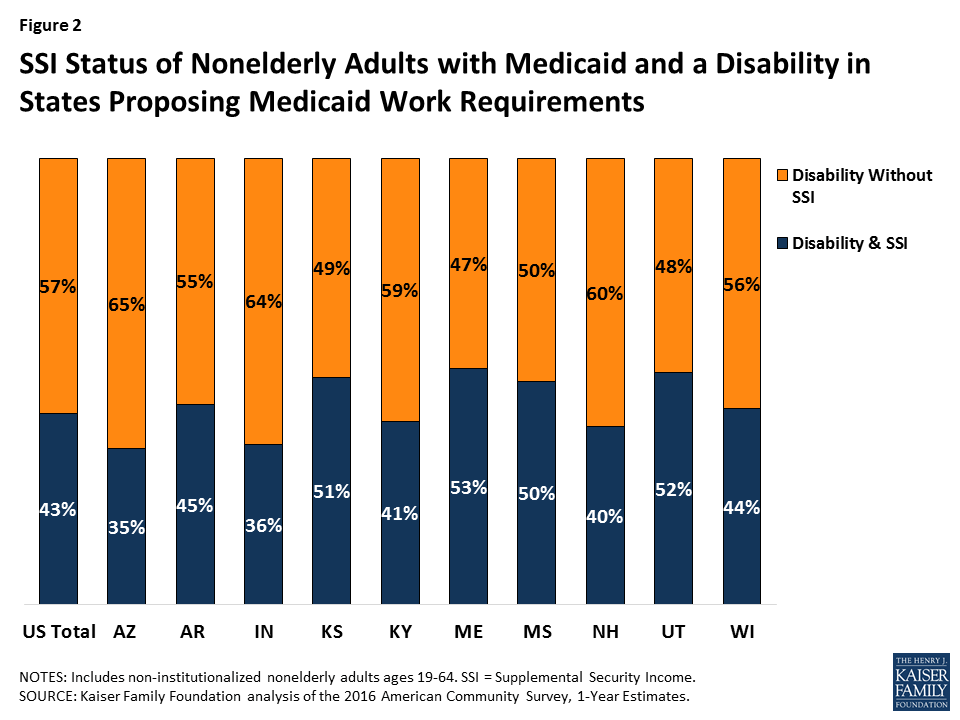
Figure 1: Disability and SSI Status of Nonelderly Adults with Medicaid, 2016Figure 2: SSI Status of Nonelderly Adults with Medicaid and a Disability in States Proposing Medicaid Work Requirements
Despite reporting serious difficulty in at least one ACS functional area, nearly six in 10 (57%) nonelderly Medicaid adults have a disability but do not receive SSI cash assistance (Figure 1). Box 1 below provides an overview of SSI eligibility criteria and the various Medicaid eligibility pathways available to people with disabilities. Many of the nonelderly Medicaid adults with disabilities in Kentucky and the nine states with work requirement proposals do not receive SSI (Figure 2 and Appendix Table 1). The share of nonelderly Medicaid adults with a disability who do not receive SSI in these states ranges from 47 percent in Maine to 65 percent in Arkansas.
Box 1: SSI vs. Medicaid Eligibility Criteria for People with Disabilities
In order to qualify for SSI, individuals must have low incomes, limited assets, and an impaired ability to work at a substantial gainful level as a result of old age or significant disability. The SSI disability standard is more stringent than the ACS definition of disability, which requires serious difficulty in at least one of the six functional areas described above. In addition, SSI income and asset limits are more restrictive than those required for Medicaid expansion adults and many optional disability-related Medicaid coverage pathways.3 People who meet the ACS definition of disability but do not receive SSI can be eligible for Medicaid as expansion adults or Section 1931 parents (based solely on their low income). They also may be eligible for Medicaid through an optional disability-related pathway (such as the state option to cover people with disabilities up to the federal poverty level or a home and community-based services waiver).4
How Many Medicaid Adults with Disabilities are Working?
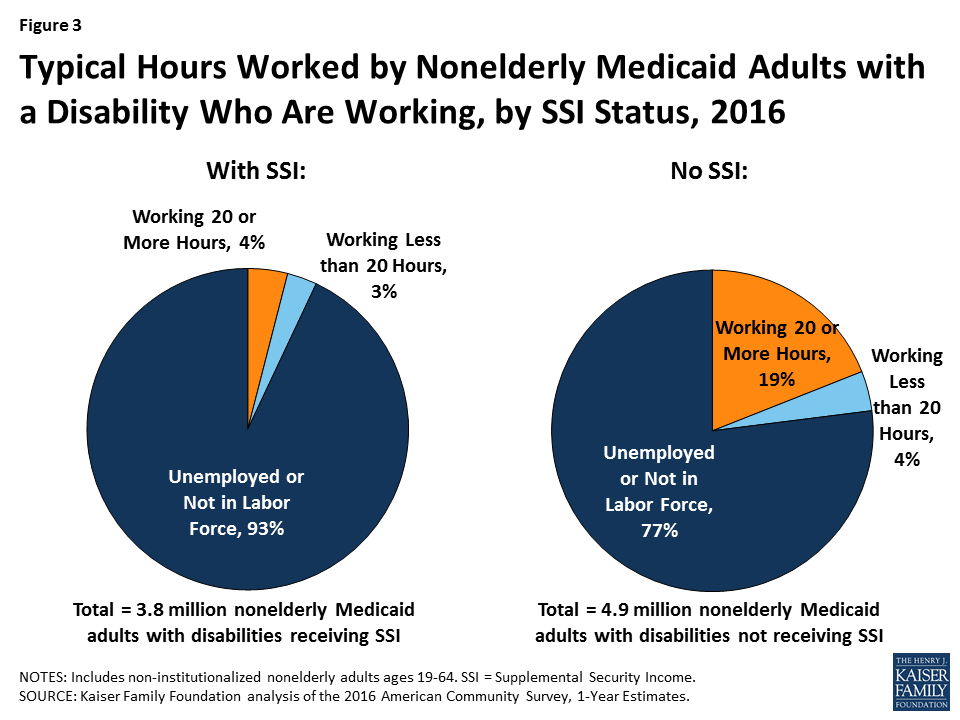
Despite reporting functional limitations, non-SSI adults with disabilities are more than three times as likely to be in the workforce than adults with disabilities who receive SSI (Figure 3). Less than one-quarter (23%) of non-SSI adults with disabilities work, compared to about seven percent of adults with disabilities who receive SSI (Figure 3). About one in five (19%) non-SSI adults with disabilities usually work 20 or more hours per week in the weeks they work, and another four percent usually work less than 20 hours per week (Figure 3). For comparison, Kentucky’s waiver requires non-exempt enrollees to work 80 hours per month (equivalent to 20 hours per week). Appendix Table 2 contains state-level data on the work status and usual hours worked for non-SSI adults with disabilities.
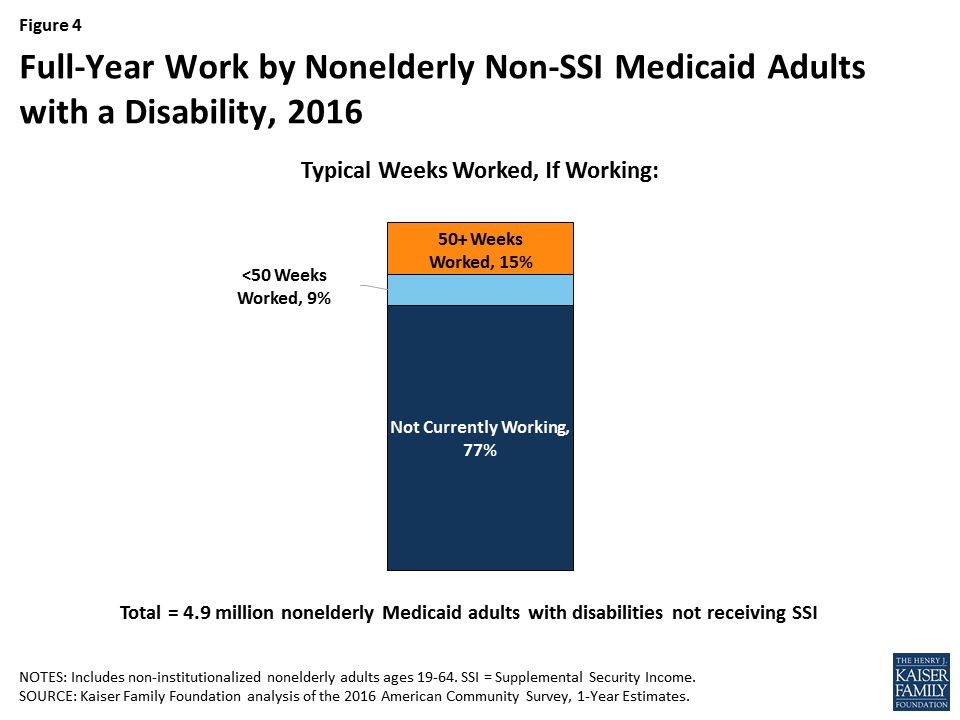
Figure 3: Typical Hours Worked by Nonelderly Medicaid Adults with a Disability Who Are Working, by SSI Status, 2016Figure 4: Full-Year Work by Nonelderly Non-SSI Medicaid Adults with a Disability, 2016
Over three-quarters (77%) of non-SSI adults with disabilities are not in the workforce (77%) (not working or unemployed but looking for work) (Figure 3). Their absence from the workforce is likely at least in part due to the serious functional difficulties they report in areas such as cognitive functioning, mobility, self-care, and independent living, as described above.
Among those who are working, 15 percent of non-SSI adults with disabilities typically are working for the full year (50 or more weeks) (Figure 4). Another nine percent are working, but typically for less than the entire year. People with disabilities may experience health issues related to their disability that prevent them from working consistently over time or from working every week.
What are the Characteristics of Medicaid Adults with Disabilities?
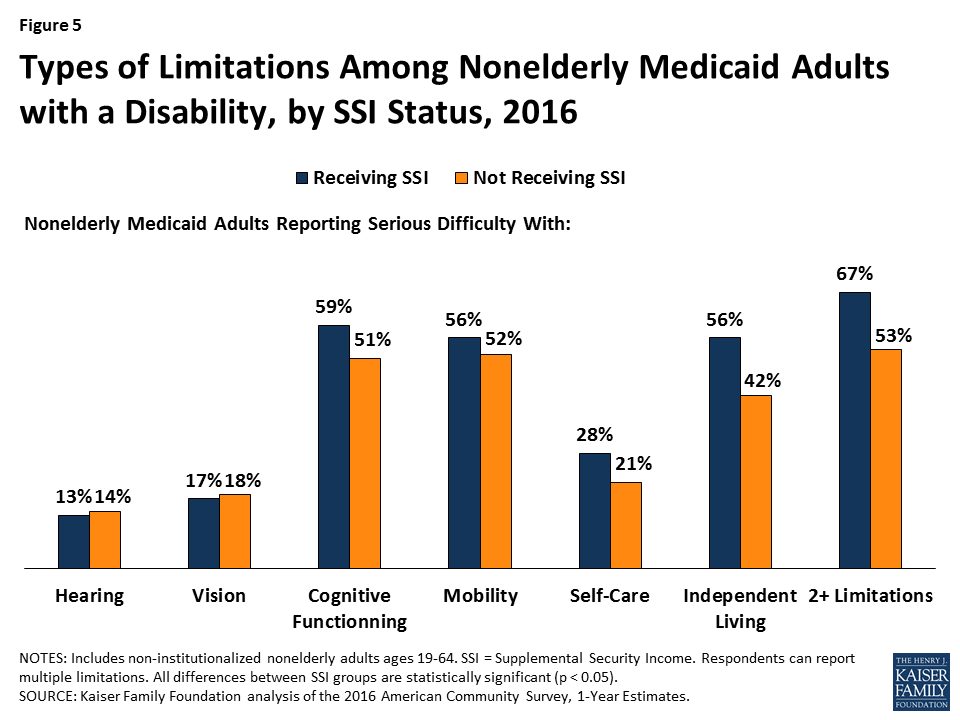
Nonelderly Medicaid adults with a disability may have health problems that limit their ability to work, or to work full-time, even though their needs do not rise to the stringent SSI level. Over half of non-SSI adults with disabilities report serious difficulty with mobility (52%), and a majority (51%) report serious difficulty with cognitive functioning (Figure 5). Over two in five (42%) non-SSI adults with disabilities report serious difficulty with independent living tasks, such as visiting a doctor’s office or shopping alone. Over one in five (21%) non-SSI adults with disabilities report serious difficulty with self-care tasks, such as dressing or bathing. Smaller shares report serious difficulty with vision (18%) and hearing (14%), compared to the other limitations that make up the ACS disability definition.
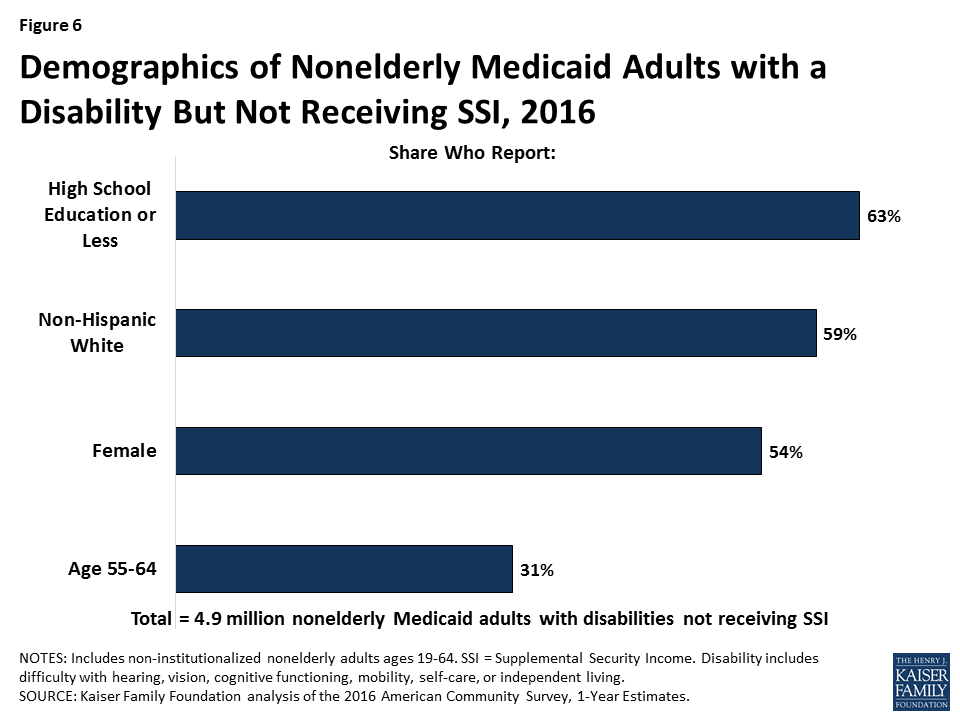
Figure 5: Types of Limitations Among Nonelderly Medicaid Adults with a Disability, by SSI Status, 2016Figure 6: Demographics of Nonelderly Medicaid Adults with a Disability But Not Receiving SSI, 2016
Most nonelderly Medicaid adults with a disability have multiple functional limitations. Over half (53%) of those without SSI have two or more of the six ACS functional limitations, compared to two-thirds (67%) of those with SSI (Figure 5).
Over six in 10 (63%) non-SSI adults with disabilities have a high school education or less, a factor that could create additional barriers to meeting a work requirement (Figure 6). About six in 10 (59%) non-SSI adults are non-Hispanic white, 54 percent are female, and more than three in 10 (31%) are ages 55 to 64 (Figure 6).
Looking Ahead
If they are not exempted, waivers that condition Medicaid eligibility on meeting a work requirement could adversely impact people with disabilities who have limitations that interfere with their ability to work but do not rise to the stringent SSI level of disability. While Kentucky’s waiver does not apply to people who receive SSI or other people who are eligible for Medicaid “based on a disability,” 59 percent of nonelderly Medicaid adults with disabilities in Kentucky do not receive SSI; this share is 57 percent nationally and ranges from 47 percent to 65 percent in the nine states with pending work requirement waivers.
Kentucky’s waiver requires people who are determined to be “medically frail” to be exempt from the work requirement, but there is no detail about how that process will be administered or whether all people with serious functional difficulties that impede their ability to work will qualify for an exemption. People who are classified as “medically frail” also will be exempt from other waiver provisions that can result in the loss of coverage, including the six-month coverage lockouts for failure to pay premiums (for those above 100% FPL), failure to timely renew eligibility, and failure to timely report a change in circumstances that affects eligibility.5 Kentucky’s waiver also requires the state to provide exemptions or reasonable modifications to the work requirement and other program rules under the Americans with Disabilities Act (ADA), Section 504 of the Rehabilitation Act, and Section 1557 of the ACA to assist people with disabilities and prevent eligible people from losing coverage.
Experience in TANF shows that work requirements can result in people with disabilities losing benefits for which they are eligible. Key issues to watch to determine the impact of Medicaid work requirement waivers on people with disabilities include whether states will have adequate staff, money, and administrative capacity to implement complex program rules; whether the medical frailty process will correctly identify and exempt all people who cannot comply with a work requirement because of a disability; what types of reasonable modifications and support services the state will provide under the ADA to enable people with disabilities to comply; how many people with disabilities will lose coverage for which they remain eligible; and whether they are able to successfully use the appeals process to regain or prevent lapses in coverage.
Appendix
Appendix Table 1: Nonelderly Medicaid Adults by Disability and SSI Status, 2016
Total Nonelderly Medicaid Adults
Nonelderly Medicaid Adults with a Disability
Nonelderly Medicaid Adults with a Disability but Not SSI
Number
Share of Total Nonelderly Medicaid Adults
Number
Share of Nonelderly Medicaid Adults with a Disability
United States Total
29,177,700
8,661,500
30%
4,900,400
57%
Alabama
326,800
143,900
44%
64,300
45%
Alaska
57,900
18,600
32%
10,500
56%
Arizona
765,900
200,300
26%
130,100
65%
Arkansas
324,300
117,000
36%
63,900
55%
California
5,187,300
1,018,900
20%
612,500
60%
Colorado
511,300
124,500
24%
81,800
66%
Connecticut
363,800
83,100
23%
56,500
68%
Delaware
88,500
24,700
28%
14,000
57%
DC
105,300
28,500
27%
19,100
67%
Florida
1,410,100
480,400
34%
234,600
49%
Georgia
563,900
227,900
40%
99,200
44%
Hawaii
112,200
22,700
20%
13,300
58%
Idaho
85,200
38,500
45%
15,200
39%
Illinois
1,186,200
299,800
25%
191,400
64%
Indiana
499,200
184,500
37%
118,400
64%
Iowa
272,300
82,200
30%
49,500
60%
Kansas
123,800
56,400
46%
27,500
49%
Kentucky
615,200
217,800
35%
129,300
59%
Louisiana
461,400
176,300
38%
90,300
51%
Maine
120,400
55,500
46%
26,300
47%
Maryland
493,900
140,500
28%
82,100
58%
Massachusetts
902,000
218,600
24%
128,100
59%
Michigan
1,144,800
381,800
33%
220,700
58%
Minnesota
491,200
127,200
26%
82,200
65%
Mississippi
246,200
108,200
44%
53,800
50%
Missouri
311,400
146,800
47%
88,100
60%
Montana
90,100
35,700
40%
21,600
60%
Nebraska
71,100
32,000
45%
15,000
47%
Nevada
256,300
73,500
29%
46,200
63%
New Hampshire
80,300
26,100
33%
15,800
60%
New Jersey
694,600
171,900
25%
90,100
52%
New Mexico
325,300
84,800
26%
49,900
59%
New York
2,721,500
592,900
22%
342,900
58%
North Carolina
642,300
245,300
38%
126,700
52%
North Dakota
35,600
14,900
42%
9,900
66%
Ohio
1,224,600
373,800
31%
241,400
65%
Oklahoma
201,600
92,300
46%
52,300
57%
Oregon
498,000
144,100
29%
92,900
64%
Pennsylvania
1,185,100
439,700
37%
259,500
59%
Rhode Island
120,600
42,200
35%
18,800
45%
South Carolina
354,000
137,700
39%
69,000
50%
South Dakota
37,300
15,300
41%
7,800
51%
Tennessee
592,400
228,200
39%
117,700
52%
Texas
1,247,200
513,700
41%
231,200
45%
Utah
128,600
46,800
36%
22,300
48%
Vermont
85,600
24,300
28%
12,900
53%
Virginia
330,000
130,300
39%
72,400
56%
Washington
727,400
219,000
30%
136,600
62%
West Virginia
277,000
98,100
35%
60,800
62%
Wisconsin
452,600
142,500
31%
79,500
56%
Wyoming
28,200
11,600
41%
4,800
41%
NOTES: Includes non-institutionalized nonelderly adults ages 19-64. SSI = Supplemental Security Income. Disability includes serious difficulty with hearing, vision, cognitive functioning, mobility, self-care, or independent living.SOURCE: Kaiser Family Foundation analysis based on the 2016 American Community Survey, 1-Year Estimates.
Appendix Table 2: Work Status of Nonelderly Medicaid Adults with a Disability but Not SSI, 2016
Total Non-SSI Medicaid Adults with Disabilities
Total Working
Share Working
Share Working 20+ Hours/Week
Share Working <20 Hours/Week
Share Unemployed or Not in Labor Force
United States Total
4,900,400
1,150,800
23%
19%
4%
77%
Alabama
64,300
6,700
10%
9%
2%
90%
Alaska
10,500
2,700
26%
21%
*
74%
Arizona
130,100
30,500
23%
19%
4%
77%
Arkansas
63,900
14,000
22%
19%
3%
78%
California
612,500
156,200
26%
22%
4%
74%
Colorado
81,800
22,600
28%
22%
5%
72%
Connecticut
56,500
12,600
22%
19%
3%
78%
Delaware
14,000
3,800
27%
19%
*
73%
DC
19,100
4,100
21%
20%
*
79%
Florida
234,600
42,400
18%
16%
2%
82%
Georgia
99,200
17,100
17%
15%
3%
83%
Hawaii
13,300
2,600
20%
16%
*
80%
Idaho
15,200
3,600
24%
17%
*
76%
Illinois
191,400
41,700
22%
18%
4%
78%
Indiana
118,400
26,700
23%
19%
4%
77%
Iowa
49,500
17,100
34%
25%
9%
66%
Kansas
27,500
7,600
28%
22%
*
72%
Kentucky
129,300
31,100
24%
22%
2%
76%
Louisiana
90,300
17,200
19%
16%
3%
81%
Maine
26,300
4,200
16%
12%
*
84%
Maryland
82,100
23,500
29%
25%
4%
71%
Massachusetts
128,100
37,700
29%
24%
5%
71%
Michigan
220,700
55,400
25%
20%
5%
75%
Minnesota
82,200
30,900
38%
28%
9%
62%
Mississippi
53,800
7,000
13%
11%
*
87%
Missouri
88,100
12,800
15%
12%
3%
85%
Montana
21,600
6,400
30%
22%
*
70%
Nebraska
15,000
4,400
29%
25%
*
71%
Nevada
46,200
9,500
20%
17%
4%
80%
New Hampshire
15,800
3,500
23%
20%
*
77%
New Jersey
90,100
21,200
24%
19%
5%
76%
New Mexico
49,900
12,000
24%
21%
*
76%
New York
342,900
90,800
26%
22%
4%
74%
North Carolina
126,700
22,500
18%
14%
4%
82%
North Dakota
9,900
*
38%
*
*
62%
Ohio
241,400
62,500
26%
21%
5%
74%
Oklahoma
52,300
8,800
17%
15%
*
83%
Oregon
92,900
29,200
31%
26%
6%
69%
Pennsylvania
259,500
62,200
24%
19%
5%
76%
Rhode Island
18,800
5,900
31%
27%
*
69%
South Carolina
69,000
12,100
17%
15%
*
83%
South Dakota
7,800
3,400
44%
30%
*
56%
Tennessee
117,700
23,500
20%
18%
2%
80%
Texas
231,200
49,100
21%
17%
4%
79%
Utah
22,300
6,500
29%
25%
*
71%
Vermont
12,900
4,100
32%
28%
*
68%
Virginia
72,400
13,600
19%
16%
*
81%
Washington
136,600
31,800
23%
18%
6%
77%
West Virginia
60,800
11,900
20%
16%
3%
80%
Wisconsin
79,500
19,400
24%
20%
5%
76%
Wyoming
4,800
1,200
24%
19%
*
76%
NOTES: Includes non-institutionalized nonelderly adults ages 19-64. SSI = Supplemental Security Income. Disability = serious difficulty with hearing, vision, cognitive functioning, mobility, self-care, or independent living.* indicates data do not meet standards of statistical reliability to report.SOURCE: Kaiser Family Foundation analysis based on the 2016 American Community Survey, 1-Year Estimates.
Endnotes
In addition to the work requirement, Kentucky’s waiver includes coverage lockouts for failing to pay premiums, timely renew eligibility, and timely report changes affecting eligibility, among other provisions. ↩︎
The ACS questions used to classify an individual as having a disability include: (1) Is this person deaf, or does he/she have serious difficulty hearing? (2) Is this person blind, or does he/she have serious difficulty seeing, even when wearing glasses? (3) Because of a physical, mental, or emotional condition, does this person have serious difficulty concentrating, remembering, or making decisions? (4) Does this person have serious difficulty walking or climbing stairs? (5) Does this person have difficulty dressing or bathing? (6) Because of a physical, mental, or emotional condition, does this person have difficulty doing errands alone, such as visiting a doctor’s office or shopping? U.S. Census Bureau, How Disability Data are Collected from the American Community Survey, (Oct. 17, 2017), https://www.census.gov/topics/health/disability/guidance/data-collection-acs.html. ↩︎
The maximum SSI benefit is about 74 percent of the federal poverty level (FPL, $9,000/year for an individual in 2018), and the asset limit is $2,000. The ACA Medicaid expansion covers individuals up to 138% FPL ($16,735/year for an individual in 2018) without an asset test. States have the option to extend financial eligibility for many disability-related Medicaid coverage pathways up to 300% of SSI ($27,000/year in 2018). ↩︎
People who qualify for Medicaid both as an expansion adult and based on a disability can choose the group through which they enroll in coverage; benefit packages may differ by coverage group. 42 C.F.R. § 435.911 (c) (2), (d). ↩︎
In addition, people who are medically frail will be exempt from the six-month healthy behavior incentive account suspension and account point deduction (for those at or below 100% FPL who choose to pay premiums but stop paying) and will not have to wait for the 60-day premium payment period to expire before coverage begins (for those who do not pay premiums). ↩︎
Health care is at the top of a group of issues that voters want 2018 midterm candidates to talk about, but it’s a much higher priority for Democratic voters (39 percent) and independent voters (32 percent) than Republican voters (13 percent); and a lower priority than other issues among voters living in areas where there are competitive 2018 House, Senate, or Governor races.
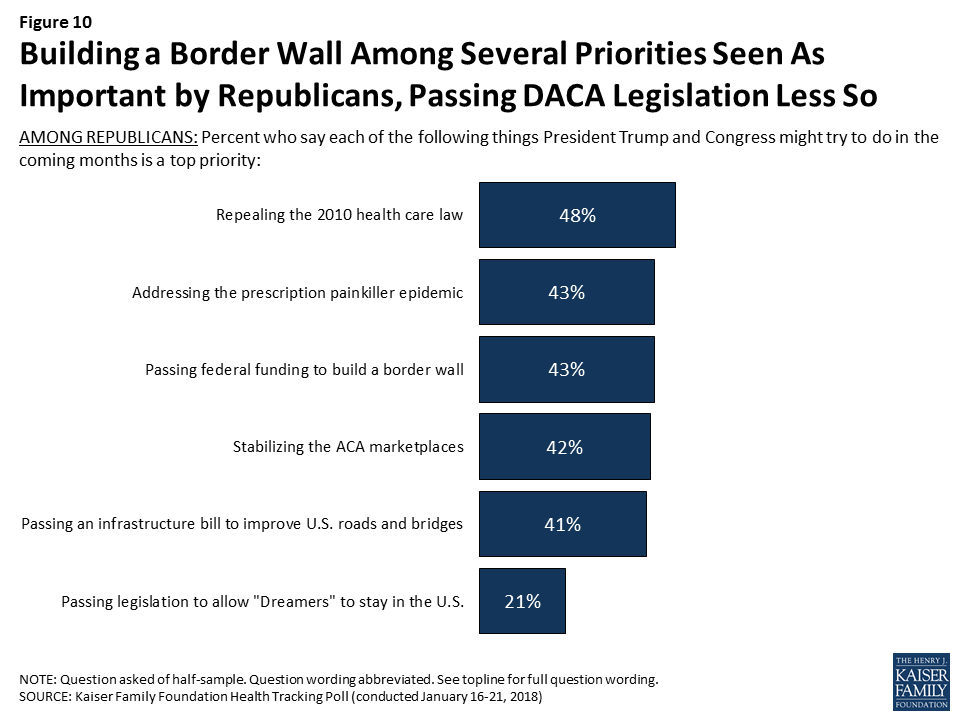
The current debate in Congress is about passing a budget to keep the government funded beyond February 8, 2018, in return for a deal on immigration policy and the Deferred Action for Childhood Arrivals (DACA). Providing federal funding for President Trump’s plan to build a border wall between the U.S. and Mexico ranks the lowest (21 percent) among the public’s priorities for the president and Congress, well behind other health-related priorities as well as passing DACA legislation. Passing federal funding for a border wall is tied for fourth (of eight priorities) among Republicans (43 percent).
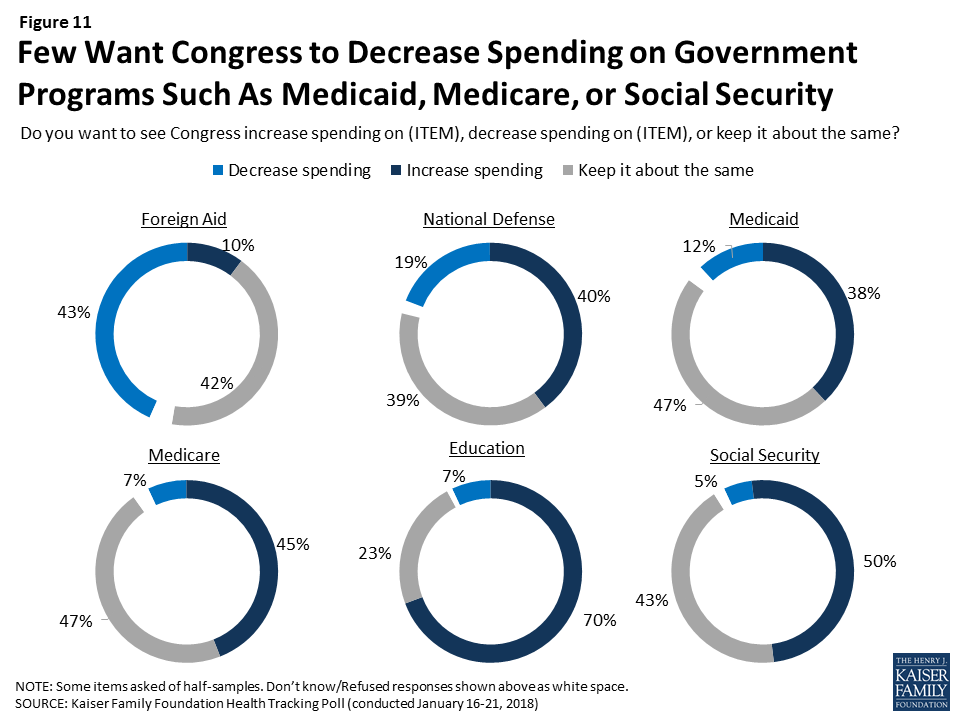
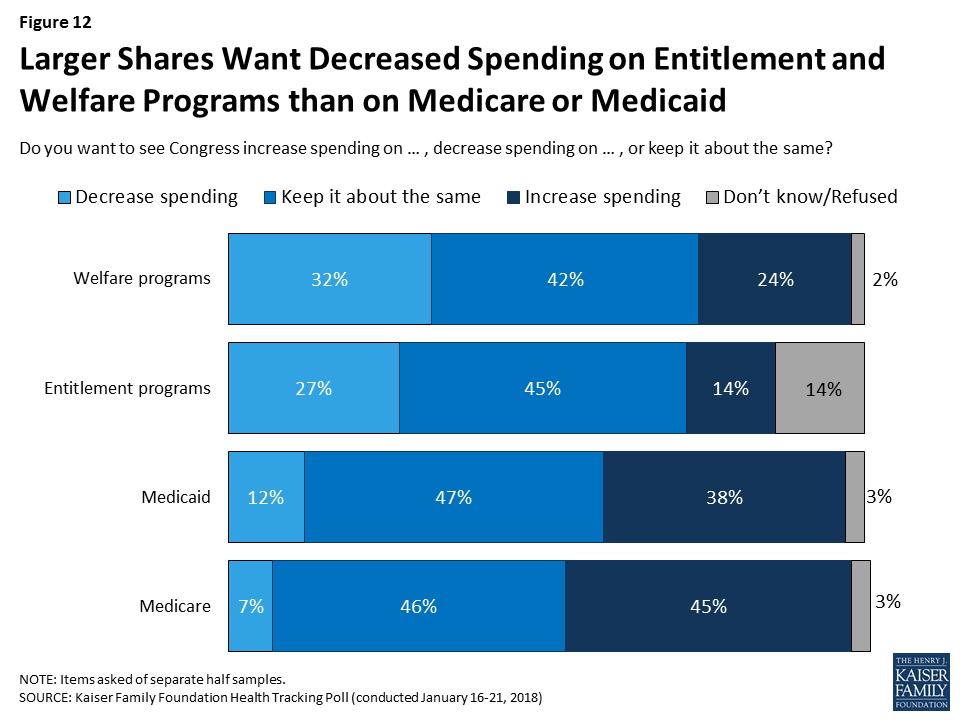
As Congress continues to work on a federal budget, some lawmakers have suggested making cuts to government programs such as Medicare and Medicaid. This poll finds that language can matter in framing questions about government spending on such programs. About one in ten say they want to see Congress decrease spending on Medicare (7 percent) and Medicaid (12 percent). When the public is asked about government spending using broader terminology like “welfare programs” or “entitlement programs” rather than a specific name, larger shares of the public say they want to see spending decrease (32 percent and 27 percent, respectively).
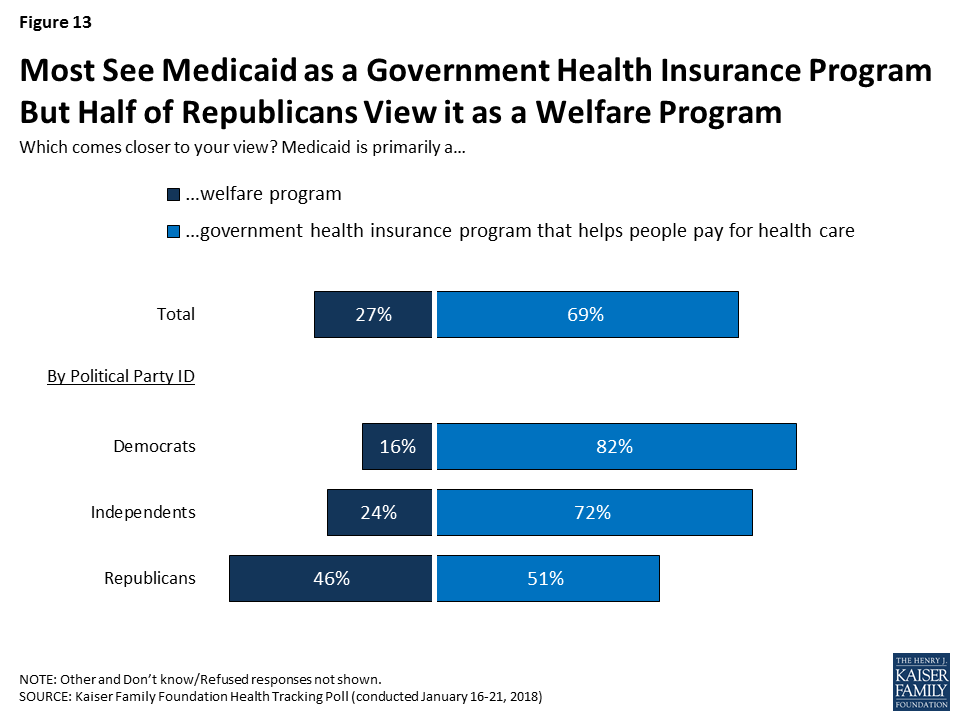
Most believe Medicaid is primarily a government health insurance program that helps people pay for health care while one-fourth (27 percent) believe it is primarily a welfare program. There are partisan differences; overwhelming majorities of Democrats (82 percent) and independents (72 percent) say it is a government health insurance program, while Republicans are divided with about half (51 percent) saying it is a government health insurance program and about half (46 percent) saying Medicaid is primarily a welfare program.
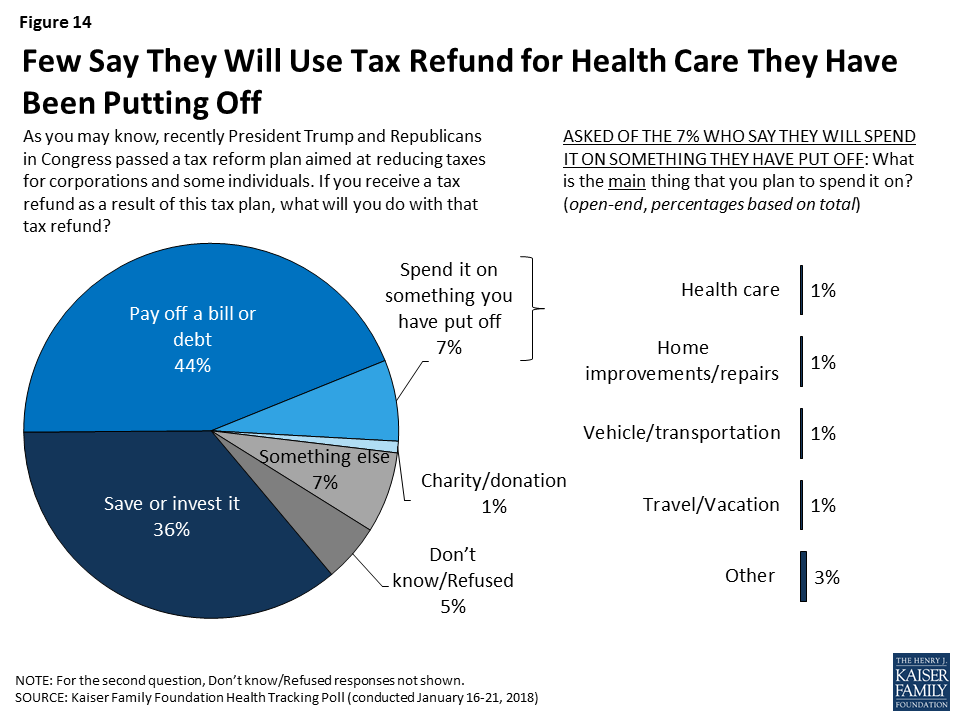
In light of the recent tax reform legislation passed by President Trump and Congress, the January Kaiser Health Tracking Poll asks the public what they would do with a tax refund. Four in ten (44 percent) say they would use their tax refund to pay off a bill or debt and about one-third say they would save or invest it. Fewer – 7 percent – say they would spend it on something they have put off, including 1 percent who say they would use it on health care they have been putting off.
2018 Midterm Elections
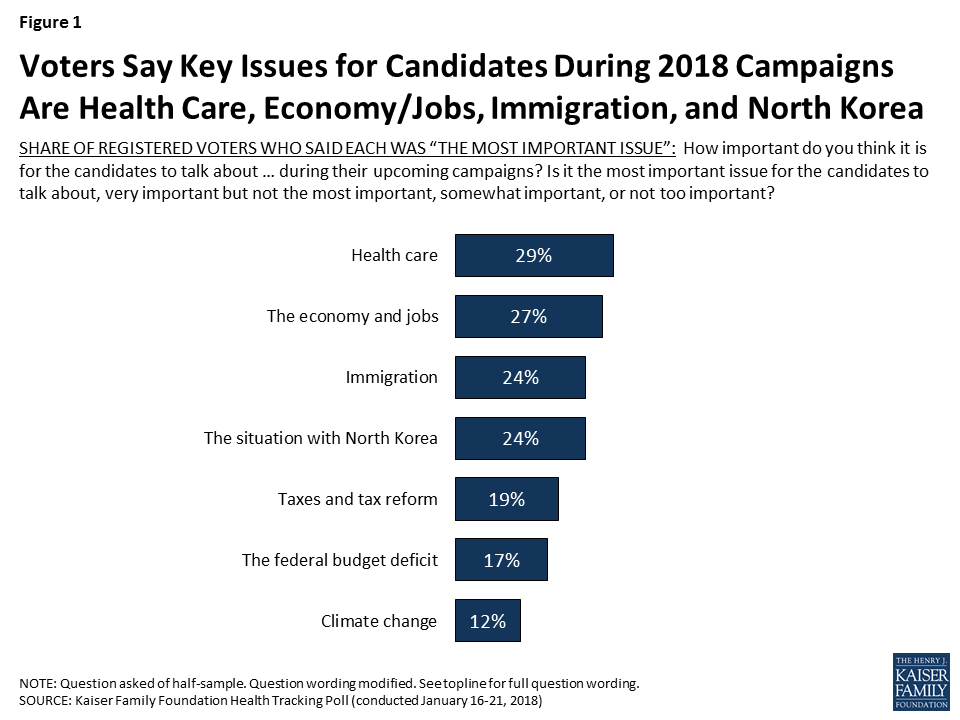
With the 2018 midterm elections still about ten months away, the January Kaiser Health Tracking Poll finds health care among the top issues American voters want 2018 candidates to talk about during their upcoming campaigns. When asked how important a series of major national issues are for 2018 congressional candidates to talk about, similar shares of registered voters say health care (29 percent) and the economy and jobs (27 percent) are “the most important issue.” This is closely followed by immigration (24 percent) and the situation in North Korea (24 percent). Fewer registered voters say “the most important issue” for congressional candidates to discuss are taxes and tax reform (19 percent), the federal budget deficit (17 percent), and climate change (12 percent).
Figure 1: Voters Say Key Issues for Candidates During 2018 Campaigns Are Health Care, Economy/Jobs, Immigration, and North Korea
Democratic voters are more focused on health care (39 percent) than Republican voters (13 percent), while one-third of independent voters (32 percent) say health care is the “most important issue” for congressional candidates to talk about during their campaigns. For Republican voters, the top issue they want to hear congressional candidates talk about is the situation with North Korea (31 percent), followed by immigration (27 percent) and the economy and jobs (25 percent).
Table 1: Views of Top Issues for 2018 Candidates by Party Identification
Percent who say each of the following is the most important issue for congressional candidates to talk about in their upcoming campaigns:
All Voters
Party ID
Democratic Voters
Independent Voters
Republican Voters
Health care
29%
39%
32%
13%
The economy and jobs
27
30
26
25
The situation with North Korea
24
23
20
31
Immigration
24
22
24
27
Taxes and tax reform
19
22
14
16
The federal budget deficit
17
17
16
14
Climate change
12
19
11
1
Voters in Battleground Elections
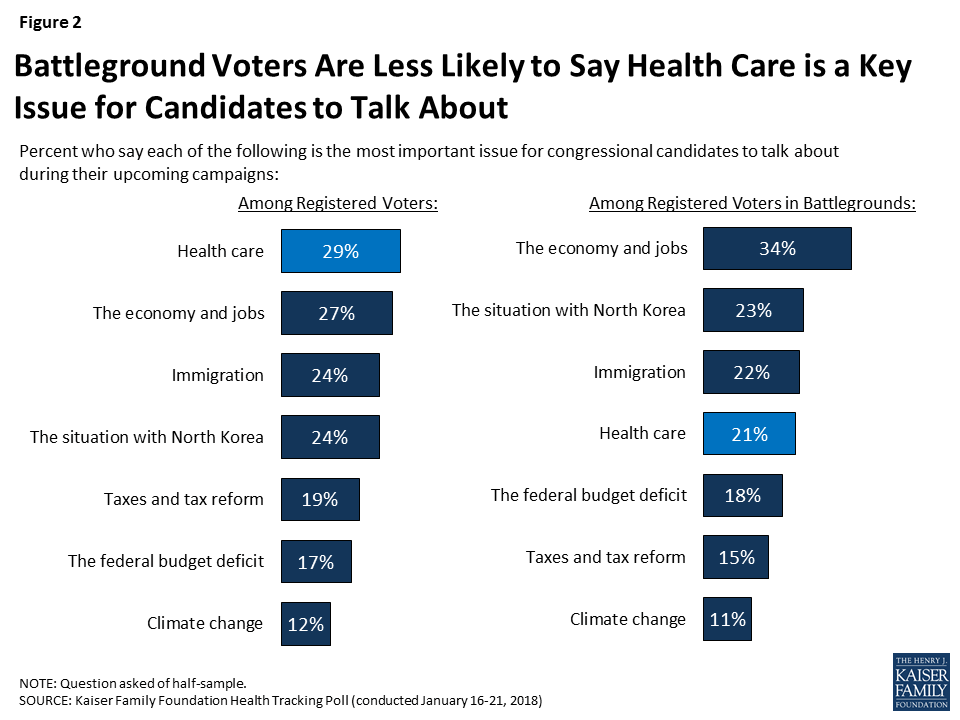
While health care is among the top issues for voters nationwide, it ranks lower among voters living in areas where there are competitive House, Senate, or Governor races. Voters in areas with competitive elections are more likely to prioritize candidates talking about the economy and jobs (34 percent) than other issues. One in five say the situation with North Korea (23 percent), immigration (22 percent), and health care (21 percent) are the most important issues for candidates to discuss.
Figure 2: Battleground Voters Are Less Likely to Say Health Care is a Key Issue for Candidates to Talk About
2018 Midterm Election Analysis
As part of Kaiser Family Foundation’s effort to examine the role of health care in the 2018 midterm elections, throughout the year we will be tracking the views of voters – paying special attention to those living in states or congressional districts in which both parties have a viable path to win the election. This group, referred to in our analysis as “voters in battlegrounds” is defined by the 2018 Senate, House, and Governor ratings provided by The Cook Political Report. Congressional and Governor races categorized as “toss-up” were included in this group. A complete list of the states and congressional districts included in the comparison group is available in Appendix A.
The Affordable Care Act
This month’s Kaiser Health Tracking Poll examines awareness of the recent repeal of the Affordable Care Act’s (ACA) individual mandate and the most recent open enrollment period, as well as views of who is most responsible for the 2010 health care law moving forward.
Public Awareness of the Repeal of the ACA’s Individual Mandate
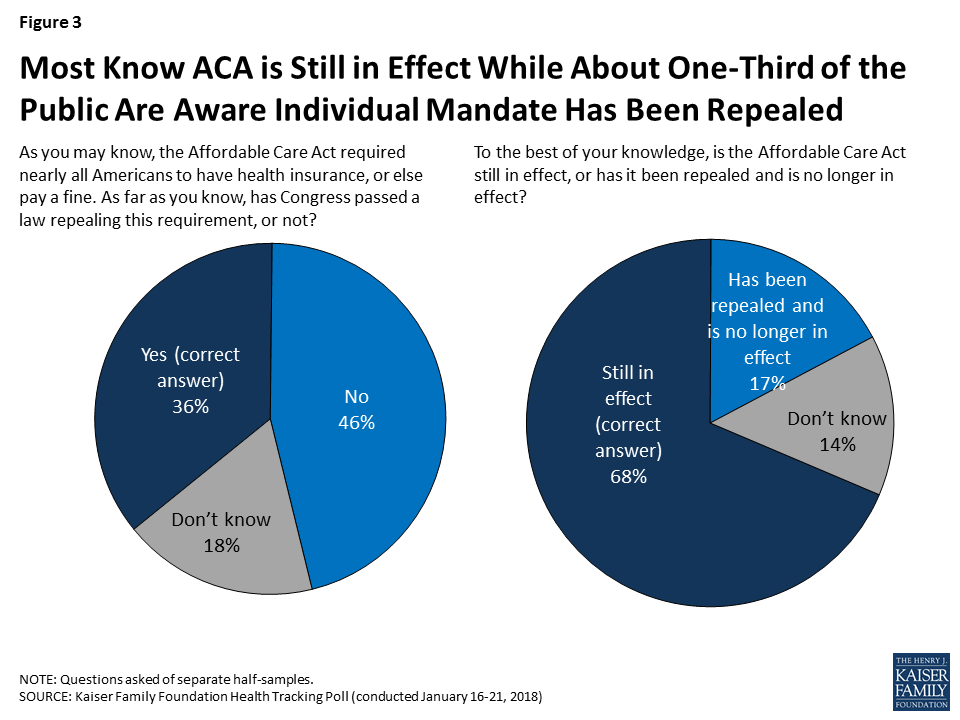
As part of the Republican tax reform plan signed into law at the the end of 2017, lawmakers eliminated the ACA’s requirement that nearly all individuals have health insurance or else pay a fine, known commonly as the individual mandate. The tax plan reduced the individual penalty for not having health insurance to zero beginning in 2019, effectively repealing the least favorable provision of the ACA (according to polling conducted by Kaiser Family Foundation). This month’s Kaiser Health Tracking Poll finds that one-third of the public (36 percent) are aware that Congress has a passed a law repealing this requirement while about half (46 percent) incorrectly say that the requirement has not been repealed. Another one in five (18 percent) are unsure of whether the individual mandate has been repealed or not. The results are similar when we look at those who are more likely to be impacted by this legislative change – the uninsured and those who buy their insurance through the individual market under the age of 65. Among this group, about four in ten (37 percent) are aware the individual mandate has been repealed, while 44 percent say it has not been repealed and 19 percent are unsure.
On the other hand, a majority of the public (68 percent) are aware that the ACA is still in effect, while one in five (17 percent) say it has been repealed and is no longer in effect and 14 percent are unsure.
Figure 3: Most Know ACA is Still in Effect While About One-Third of the Public Are Aware Individual Mandate Has Been Repealed
The ACA’s Fifth Open Enrollment Period and Individual Marketplaces
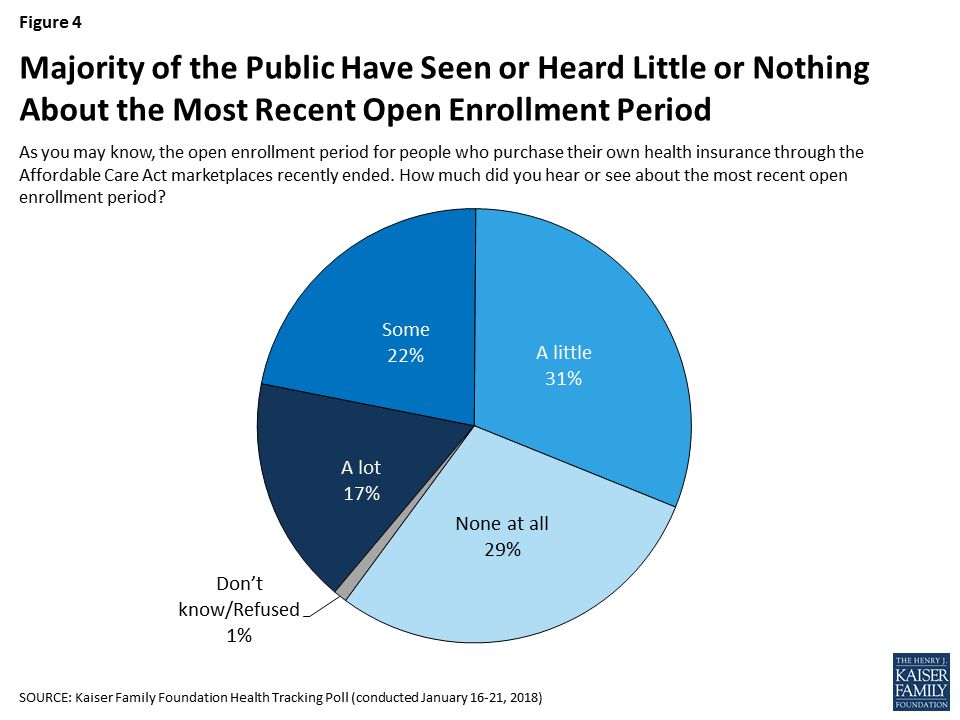
The ACA’s fifth open enrollment period, the time period that individuals who purchase health plans on their own can shop for insurance, ended for most people on December 15, 2017. About four in ten (39 percent) say they heard or read at least some about the open enrollment period, while six in ten say they heard or read either “a little” (31 percent) or “none at all” (29 percent).
Figure 4: Majority of the Public Have Seen or Heard Little or Nothing About the Most Recent Open Enrollment Period
According to the Centers for Medicare and Medicaid Services, nearly nine million people have signed up for insurance through the federal marketplace,1 which is 400,000 fewer than the number of people that signed up during the previous enrollment period.2 The public is divided in its perception of whether more or fewer people signed up for health insurance during the most recent open enrollmend period. About one-third (36 percent) say more people signed up (including about one in five who said “a lot more”) during open enrollment, while a similar share (31 percent) say fewer signed up (including 13 percent who said “a lot fewer”).
Figure 5: Public Divided in Whether More or Fewer People Signed Up for Health Insurance During the Most Recent ACA Open Enrollment
Perceptions of how the most recent open enrollment period went are largely driven by party identification. Democrats and independents are more likely to say more (either “a lot” or “a little”) people signed up this year than in previous years (43 percent and 37 percent, respectively) compared to Republicans (24 percent).
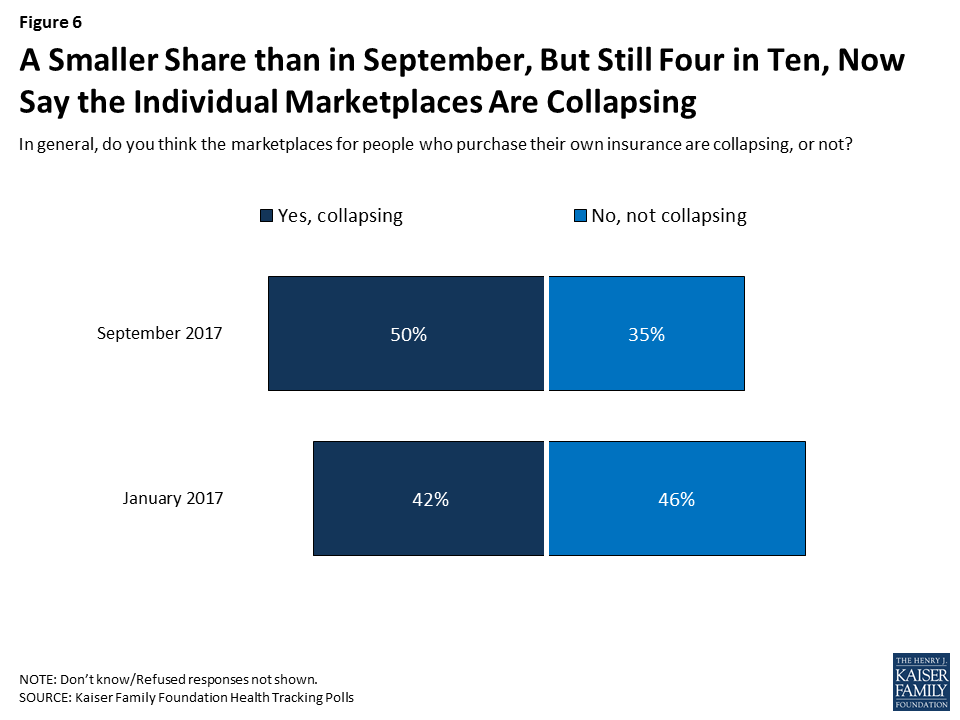
Overall, the share of the public who think the individual marketplaces are collapsing has decreased from September 2017 (down to 42 percent from 50 percent).
Figure 6: A Smaller Share than in September, But Still Four in Ten, Now Say the Individual Marketplaces Are Collapsing
The Future of the Affordable Care Act
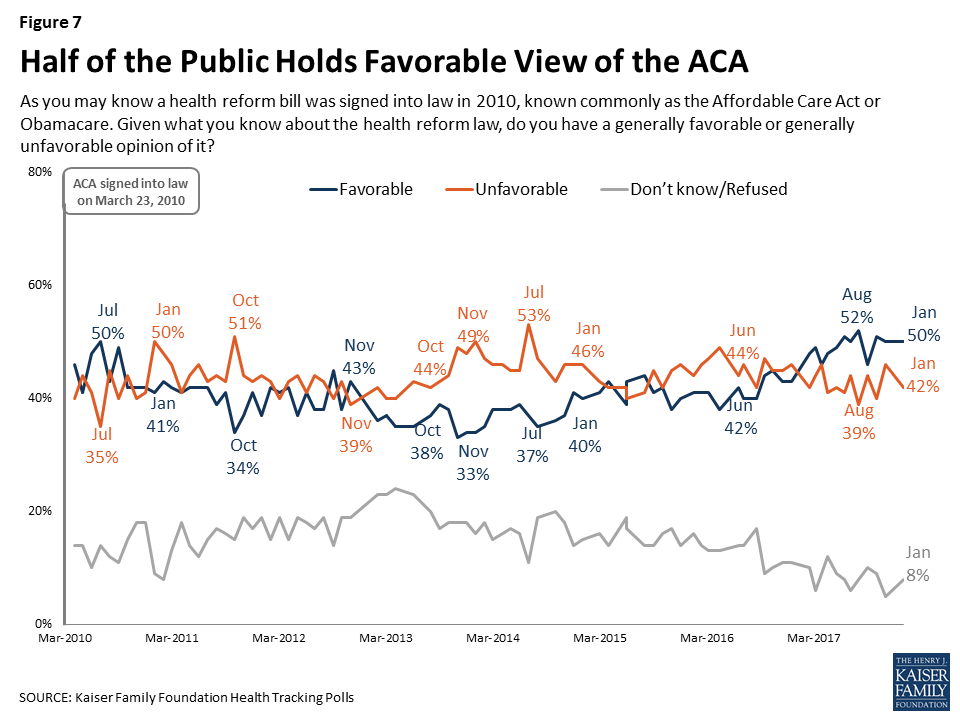
At the start of 2018, the public is more favorable in their views of the ACA, with 50 percent saying they have a favorable view and 42 percent saying they have an unfavorable view. This continues the trend of a larger share of the public holding favorable views rather than unfavorable ones first measured during the Republican efforts to repeal the ACA during 2017.
Figure 7: Half of the Public Holds Favorable View of the ACA
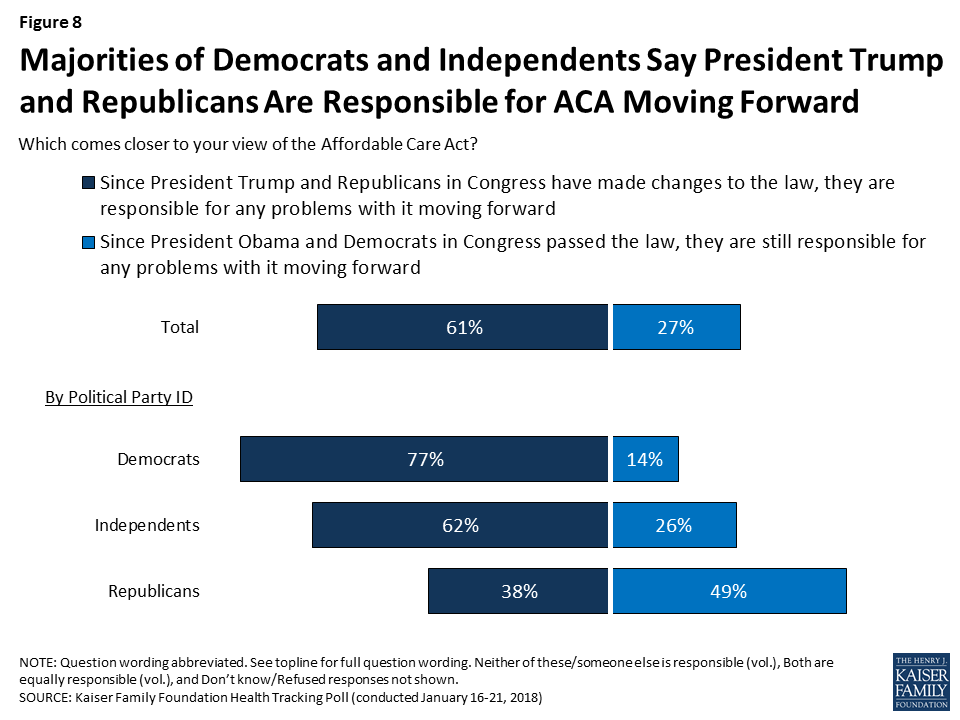
The majority of the public (61 percent) say since President Trump and Republicans in Congress have made changes to the ACA, they are responsible for any problems with it moving forward, compared to about three in ten (27 percent) who say that because President Obama and Democrats in Congress passed the law, they are responsible for any problems with it. Partisan differences continue, with majorities of Democrats and independents saying President Trump and Republicans are responsible for any problems with it moving forward while a larger share of Republicans say President Obama and Democrats are responsible for the law moving forward.
Figure 8: Majorities of Democrats and Independents Say President Trump and Republicans Are Responsible for ACA Moving Forward
Current Priorities for President Trump and Congress
In terms of how the public views the legislative priorities for President Trump and Republicans in Congress, passing federal funding for President Trump’s plan to build a border wall between the U.S. and Mexico ranks the lowest among the public (21 percent) – considerably lower than passing a federal budget to prevent a government shutdown (57 percent), stabilizing the ACA marketplaces where people who don’t get health insurance through their employer can buy coverage (51 percent), addressing the prescription painkiller addiction epidemic (48 percent), and passing legislation to allow Dreamers to stay in the U.S. (45 percent). Despite the recent attention given to Republican efforts to repeal the 2010 Affordable Care Act (ACA), about three in ten (28 percent) say this should be a top priority for President Trump and Congress in the coming months.
Across all Kaiser Family Foundation polling during the fall 2017 renewing funding for the Children’s Health Insurance Program (CHIP) consistently ranked at the top of the public’s priorities, including in this month’s Kaiser Health Tracking Poll (68 percent say it should be a “top priority”). Congress agreed to a six-year extension of the CHIP program as part of the continuing resolution passed on January 22, 2018.
Figure 9: Renewing CHIP Funding Is Public’s Top Priority For President Trump and Congress
Partisans Hold Differing Views on Top Priorities
Besides all partisans prioritizing passing legislation to prevent a government shutdown, views of what should be the top priorities for the President and Congress vary sharply across partisans. A majority of Democrats want President Trump and Congress to focus on passing legislation to allow Dreamers to legally stay in the U.S. (66 percent), stabilizing the ACA marketplaces (61 percent), and addressing the prescription painkiller addiction epidemic (54 percent).
Table 2: Views of Top Priorities by Party Identification
Percent who say each of the following should be a top priority for President Trump and Congress:
Total
Party ID
Democrats
Independents
Republicans
Renewing funding for the Children’s Health Insurance Program (CHIP)
68%
84%
69%
48%
Passing a federal budget to prevent a government shutdown
57
55
57
61
Stabilizing the ACA marketplaces
51
61
48
42
Addressing the prescription painkiller addiction epidemic
48
54
50
43
Passing legislation to allow “Dreamers” to legally stay in the U.S.
45
66
40
21
Passing an infrastructure bill to improve U.S. roads and bridges
40
39
40
41
Repealing the 2010 health care law
28
17
25
48
Passing federal funding to build a border wall
21
5
19
43
On the other hand, Republicans are more likely to prioritize repealing the ACA (48 percent), addressing the prescripton painkiller epidemic (43 percent), passing federal funding to build a border wall (43 percent), stabilizing the ACA marketplaces (42 percent), and passing an infrastructure bill (41 percent) than they are to prioritize legislation to allow Dreamers to stay in the U.S. (21 percent).
Figure 10: Building a Border Wall Among Several Priorities Seen As Important by Republicans, Passing DACA Legislation Less So
Few Support Reducing Federal Funding for Government Programs
As Congress continues to work on a federal budget, some lawmakers have suggested making cuts to government programs such as Medicare and Medicaid. Few Americans – regardless of party identification – want to see Congress decrease spending on Social Security (5 percent), Medicare (7 percent), or Medicaid (12 percent). This is similar to the share who want to see Congress decrease spending on education (7 percent) and smaller than the share who want to see Congress decrease spending on national defense (19 percent) or foreign aid (43 percent). Large shares want to see spending on all of these government programs say about the same.
Figure 11: Few Want Congress to Decrease Spending on Government Programs Such As Medicaid, Medicare, or Social Security
Support for Government Program Spending Can Change Depending on What You call It
This month’s Kaiser Health Tracking Poll finds that language can matter in framing questions about government spending on programs like Medicare and Medicaid. As noted above, four in ten say they want to see Congress increase spending on Medicare (45 percent) and Medicaid (38 percent), while about one in ten want to see Congress decrease spending on these programs (7 percent and 12 percent, respectively). When the public is asked about government spending using broader terminology like “welfare programs” or “entitlement programs” rather than a specific name, larger shares of the public say they want to see spending decrease (32 percent and 27 percent, respectively).
Figure 12: Larger Shares Want Decreased Spending on Entitlement and Welfare Programs than on Medicare or Medicaid
A larger share of Republicans say they would like Congress to decrease spending on welfare programs (58 percent) and entitlement programs (51 percent) than either independents (30 percent and 25 percent, respecitvely) or Democrats (11 percent for both).
Overall, the majority of the public (69 percent) believe Medicaid is primarily a government health insurance program that helps people pay for health care while one-fourth (27 percent) believe it is primarily a welfare program. There are partisan differences with overwhelming majorities of Democrats (82 percent) and independents (72 percent) saying it is a government health insurance program, while Republicans are divided with half (51 percent) saying it is a government health insurance program and about half (46 percent) saying Medicaid is primarily a welfare program.
Figure 13: Most See Medicaid as a Government Health Insurance Program But Half of Republicans View it as a Welfare Program
Few Americans Say They Would Use A Tax Refund On Health Care They Have Been Putting Off
In light of the recent tax reform legislation passed by President Trump and Congress, the January Kaiser Health Tracking Poll asks the public what they would do with a tax refund. Four in ten (44 percent) say they would use their tax refund to pay off a bill or debt and about one-third (36 percent) say they would save or invest it. Fewer – 7 percent – say they would spend it on something they have put off, including 1 percent who say they would use it on health care they have been putting off.
Figure 14: Few Say They Will Use Tax Refund for Health Care They Have Been Putting Off
Methodology
This Kaiser Health Tracking Poll was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted January 16-21 2018, among a nationally representative random digit dial telephone sample of 1,215 adults ages 18 and older, living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). Computer-assisted telephone interviews conducted by landline (433) and cell phone (782, including 497 who had no landline telephone) were carried out in English and Spanish by SSRS of Glen Mills, PA. Both the random digit dial landline and cell phone samples were provided by Marketing Systems Group (MSG). For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s 2016 American Community Survey (ACS) on sex, age, education, race, Hispanic origin, and region along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the January-June 2017 National Health Interview Survey. The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Health Care Ranks Among Voters’ Top Issues for the 2018 Midterm Elections, But It’s a Lower Priority Among Voters in Battleground States and Districts
Republicans View the Border Wall, the Opioids Epidemic and Stabilizing the ACA’s Marketplaces as Equal Priorities for Washington; Democrats Rank Protecting the Dreamers Above Any of Those Issues
Only One in Three Know the Tax Reform Law Repeals the ACA’s Unpopular Individual Mandate
Health care and the economy and jobs top voters’ list as “the most important issue” for Congressional candidates to talk about ahead of November’s midterm elections, but the lineup shifts among voters in states and districts with competitive elections, the January Kaiser Health Tracking Poll finds.
When asked how important a series of major national issues are, similar shares say health care (29%) and the economy and jobs (27%) is “the most important issue.” These are closely followed by immigration (24%) and the situation in North Korea (24%).
But a third (34%) of voters who live in states or Congressional districts expected to have highly competitive 2018 midterm races (based on The Cook Political Report’s ratings) cite the economy as “the most important issue.” Fewer voters in these battleground areas cite North Korea (23%), immigration (22%), or health care (21%) as the top issue.
Border Wall Ranks at Bottom of Public’s Priorities for Washington, But Higher for Republicans
The poll also weighs the public’s priorities for Washington as Congress continues to work on a budget deal to keep the federal government running past Feb. 8 and address immigration and border security, including the status of the “Dreamers,” who are immigrants brought to the U.S. illegally as children but allowed to stay under the Obama Administration’s Deferred Action for Childhood Arrivals (DACA) program.
Providing federal funding for a wall along the U.S.-Mexico border ranks the lowest among eight priorities for President Trump and Congress, with one in five (21%) people naming it as a “top priority.” Several health care priorities rank higher, including renewing the Children’s Health Insurance Program (68%), which Congress did Monday as part of a short-term budget deal to reopen government; stabilizing the Affordable Care Act’s marketplaces (51%); and addressing the prescription painkiller epidemic (48%). Nearly half (45%) of the public say passing legislation to allow the Dreamers to stay in the U.S. should be a top priority.
There are wide partisan differences in these priorities. Two thirds of Democrats cite the Dreamers as a top priority, ahead of health care issues including ACA stabilization (61%) and the opioids epidemic (54%). Republicans are about as likely to consider the border wall as a top priority (43%) as they are to consider repealing the ACA (48%), the opioids epidemic (43%), stabilizing the ACA marketplaces (42%), and passing an infrastructure bill (41%). Passing a federal budget to prevent a government shutdown ranks higher (61%).
Few Support Cuts to Medicare and Medicaid Spending, but Framing Language Matters
As Congress continues to work on a federal budget, few Americans – regardless of party identification – want to see reduced spending on Medicare (7%) or Medicaid (12%). However, the poll also finds that the way spending on such programs is framed can affect the public’s views. When asked about government spending using more loaded terms like “entitlement programs” or “welfare programs,” larger shares say they want to see spending decrease (32% for welfare programs, 27% for entitlement programs).
A clear majority of the public (69%) view Medicaid primarily as a government health insurance program that helps people pay for health care, compared to one-fourth (27%) view it primarily as a welfare program. There are partisan differences, with overwhelming majorities of Democrats (82%) and independents (72%) viewing it as insurance, and Republicans divided with a narrow majority (51%) saying it is insurance and nearly half (46%) saying it is welfare.
Relatively Few Know the Tax Reform Law Repeals the ACA’s Unpopular Individual Mandate
The poll also assesses the public’s awareness about the repeal of the law’s individual mandate provision effective in 2019 through the tax reform law enacted in December. The mandate, which requires most Americans to have health coverage or pay a tax penalty, has consistently polled as the ACA’s least popular provisions.
About one third (36%) of the public are aware that Congress repealed this requirement, while nearly half (46%) incorrectly say that the requirement has not been repealed. The rest (18%) are unsure if it was repealed or not. The results are similar among those who are most likely to be affected by the change – those who are either uninsured or buy their insurance through the individual market.
The poll also finds that most Americans do not plan to spend their tax refund on health care they have been putting off. When asked what they would do with a tax refund, four in ten (44%) say they would use a tax refund to pay off a bill or debt, while a third (36%) say they would save or invest it. Few (7%) say they would spend it on something they have put off, including just 1 percent who say they would use it for health care that they put off.
Designed and analyzed by public opinion researchers at the Kaiser Family Foundation, the poll was conducted from January 16 – 21, 2018 among a nationally representative random digit dial telephone sample of 1,215 adults. Interviews were conducted in English and Spanish by landline (433) and cell phone (782). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.