KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
On July 24, 2020, President Trump signed four executive orders related to prescription drug costs. All four orders will require regulatory action by the Administration before they can be implemented. Three of the four executive orders were released publicly – one pertaining to prescription drug importation, one pertaining to Medicare Part D drug rebates, and one pertaining to the cost of insulin and injectable epinephrine in federally qualified health centers. The fourth executive order, referred to by the President as the “most favored nation” proposal, that uses international reference prices to lower drug costs in the U.S., was not released with the others. Instead, the President announced he would give pharmaceutical companies 30 days to come up with an alternative approach before that order would take effect.
Those 30 days have now passed, and the executive order has still not been released. According to press reports, the pharmaceutical industry has put together an alternative proposal, but it is not known whether the proposal has been presented to the White House, nor whether the President will accept the industry’s proposal and drop the “most favored nation” proposal. The President has continued to tweet and talk about this proposal, including at some length on the opening day of the Republican National Convention. According to the President’s statement at the signing ceremony, the executive order would ensure that the U.S. pays no more for pharmaceuticals than other countries.
While the content of this executive order has not been released to the public, a portion of the textthat was captured by a photographer during the President’s signing ceremony indicates that it may be similar to a proposal announced by the Administration in October of 2018 in an advance notice of proposed rulemaking (ANPRM). Under the 2018 proposal, Medicare would test a model that uses lower drug prices from several foreign countries to set payments for drugs that are covered under Medicare Part B, with the aim of paying 126% of what other countries pay, down from 180% currently. Medicare Part B covers a limited set of prescription drugs that are administered in outpatient settings, such as physician offices and hospital outpatient departments, mainly high-cost drugs used to treat serious illnesses such as cancer or rheumatoid arthritis. As proposed, the model would have no direct impact on the price of drugs covered under Medicare Part D or private insurance.
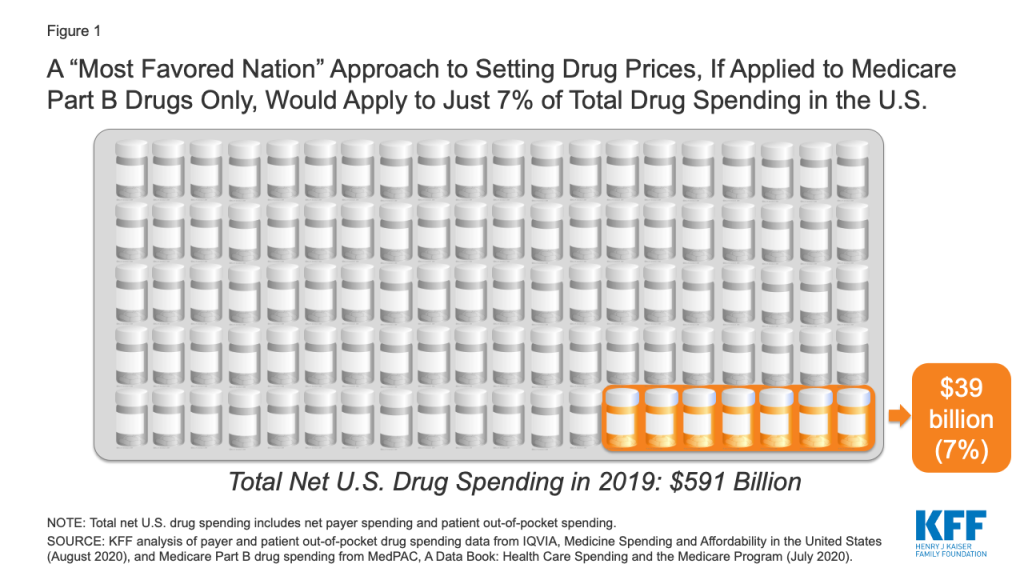
If the new executive order is similar to the 2018 proposal, and applies only to Medicare Part B drug spending, it would apply to just 7% of total national spending on prescription drugs, according to our analysis (Figure 1).
Figure 1: A “Most Favored Nation” Approach to Setting Drug Prices, If Applied to Medicare Part B Drugs Only, Would Apply to Just 7% of Total Drug Spending in the U.S.
If a “most favored nation” approach was limited to setting prices for prescription drugs covered by Medicare Part B only, it could lower drug costs for approximately 4 million Medicare beneficiaries, based on the number of people who used Part B drugs in 2018 (just 7% of all 60 million beneficiaries covered by Medicare). However, it would have no direct impact on the lion’s share of drug spending under Medicare for prescriptions filled by the 45 million beneficiaries covered under Medicare Part D, nor would it lower drug costs for the 157 million people with employer coverage or for millions more with other insurance coverage or no coverage whatsoever.
Methods
To calculate the share of total drug spending accounted for by Medicare Part B drug spending, we used data from IQVIA, Medicine Spending and Affordability in the United States: Understanding Patients’ Costs for Medicines (August 2020) and MedPAC, A Data Book: Health Care Spending and the Medicare Program (July 2020). According to IQVIA, total net payer spending on prescription drugs in 2019, including both retail and non-retail settings, was $509 billion, and patient out-of-pocket spending on drugs, both retail and non-retail, was an additional $82 billion, for a total of $591 billion in total net payer and patient drug spending in 2019. According to MedPAC, Medicare Part B drug spending was $35 billion in 2018. We trended this 2018 estimate forward to 2019 using the 11% average annual growth rate in Part B spending between 2009 and 2018, as reported by MedPAC, to derive an estimated Part B drug spending amount for 2019 of $39 billion. This $39 billion estimate formed the numerator and the $591 billion IQVIA estimate formed the denominator for our calculation of total drug spending accounted for by Medicare Part B drug spending in 2019.
States have taken a number of Medicaid policy actions to address the impact of COVID-19 on seniors and people with disabilities, many of whom rely on long-term services and supports (LTSS) to meet daily needs and are at increased risk of adverse health outcomes if infected with coronavirus. Medicaid is the primary source of coverage for LTSS, financing over half of these services in 2018. Collectively these actions could expand access to coverage (by enhancing financial and functional eligibility criteria and streamlining enrollment), expand access to long-term care services (by adding new benefits and increasing utilization limits), and bolster providers (through increased reimbursement or retainer payments). Increased funding may be required to extend community-based care more broadly and additional enrollee protections and oversight could be achieved through strengthened reporting requirements. This issue brief identifies state actions taken as of August 21, 2020 and implications for future consideration.
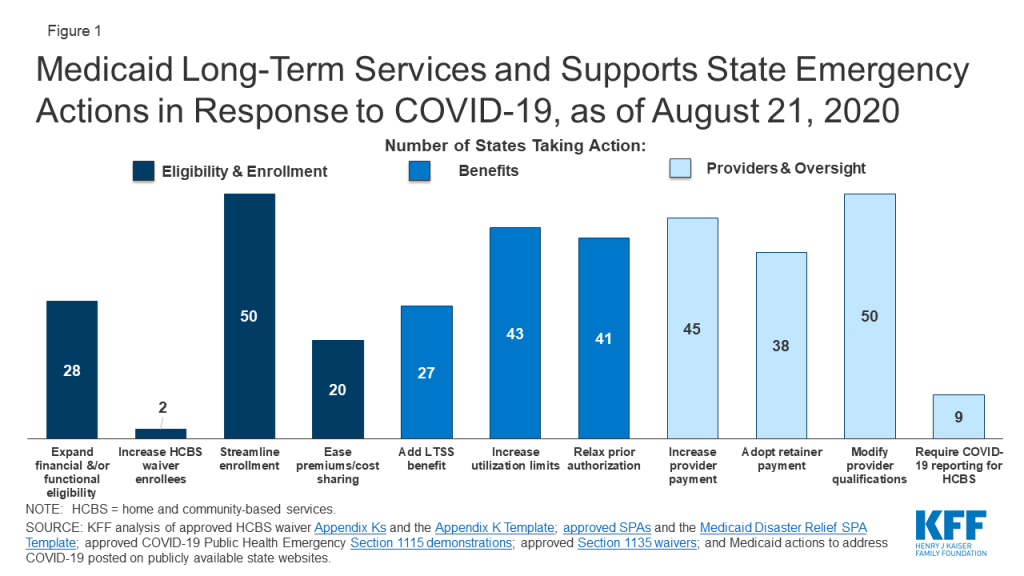
States have taken a number of emergency LTSS actions related to Medicaid eligibility, benefits and providers (Figure 1). Over half of states have expanded eligibility criteria for seniors and people with disabilities, while few states have increased the total number of HCBS waiver enrollees served. Nearly all states have streamlined enrollment processes, and over one-third of states have eased premium and/or cost-sharing requirements for seniors and people with disabilities. Just over half of states have added a new LTSS benefit to meet enrollee needs during the emergency; most benefit expansions are home and community-based services (HCBS). Most states have increased service utilization limits and relaxed prior authorization requirements. Nearly all states have increased provider payment rates for at least one LTSS and modified provider qualifications, and many have adopted retainer payments. Among states with provider payment rate increases, just over half have increased institutional rates, while about two-thirds have increased rates for at least some HCBS. Few states have required reporting on COVID-19 cases and deaths for HCBS enrollees and/or settings. CMS has adopted separate COVID-19 reporting requirements for nursing facilities.
Figure 1: Medicaid Long-Term Services and Supports State Emergency Actions in Response to COVID-19, as of August 21, 2020
The duration of the public health emergency has implications for policy actions adopted under Medicaid emergency authorities as well as the availability of enhanced federal funding provided through the matching rate increase. Many state policy changes have been adopted through temporary authorities that will expire after the public health emergency declaration ends, which will lead policymakers to assess whether any policies can or should be retained and transitioned to other authorities. In addition, some policy changes in response to the pandemic may be difficult for states to sustain without additional federal financial support beyond the 6.2 percentage point increase in federal Medicaid matching funds authorized by Congress during the public health emergency, as states are facing revenue declines and budget shortfalls.
A great deal of attention has been focused on the impact of COVID-19 in nursing homes, given the disproportionate number of cases and deaths among residents and staff nationally, with less attention on community-based residential settings. The Trump Administration has issued guidance about how nursing homes should respond to the pandemic, announced the formation of an independent commission to assess nursing home response, and adopted new reporting requirements for COVID-19 cases and deaths in nursing homes. To date, less attention to COVID-19 cases and deaths generally has been paid to community-based residential settings, such as group homes, where the pandemic presents similar risks to Medicaid enrollees and providers due to the highly transmissible nature of the coronavirus, the congregate nature of the settings, and the close contact that many workers have with residents. Data about COVID-19 cases and deaths in both institutional and community-based congregate settings may allow policymakers to more fully assess the impact across populations at increased risk of adverse health outcomes. The pandemic also may exacerbate the need for HCBS waiver services, which already are subject to waiting lists in a number of states. For example, elderly parents sickened by COVID-19 may no longer be able to provide care for their adult children with disabilities. Beyond the pandemic, the coming age wave makes LTSS and Medicaid’s role as the primary payer likely to be policy issues faced by the next Administration, in addition to the continuing effects of the pandemic and economic crisis.
Introduction
As the COVID-19 pandemic continues, states have taken a number of Medicaid policy actions to address the impact on seniors and people with disabilities, many of whom rely on long-term services and supports (LTSS) to meet daily needs and are at increased risk of adverse health outcomes if infected with coronavirus. Medicaid covers nearly 7.4 million seniors and almost 11.1 million people who are eligible based on a disability as of 2014. These enrollees may be at increased risk for adverse health outcomes if infected with coronavirus due to their older age, underlying health conditions, and/or residence in congregate settings, such as nursing homes, intermediate care facilities for people with intellectual or developmental disabilities (I/DD), or group homes. In addition, many seniors and people with disabilities rely on Medicaid LTSS to meet daily self-care and independent living needs, which makes it important for their coverage and access to care to continue uninterrupted during the pandemic.
Many state policy changes related to Medicaid LTSS have been adopted through temporary authorities that, according to CMS guidance, will expire when the Health and Human Services Secretary’s COVID-19 public health emergency declaration ends. This will lead policymakers to assess whether any changes can or should be retained and transitioned to other authorities. The public health emergency declaration currently is set to expire on October 23, 2020. While some state actions have been supported by the 6.2 percentage point increase in federal Medicaid matching funds authorized by Congress during the public health emergency, policy changes may be difficult for states to sustain without additional federal financial support, given the severity and expected longevity of the economic crisis resulting from the pandemic. The amount of fiscal relief to states from the increase in federal matching funds depends on the duration of the public health emergency, while the economic consequences of the pandemic are likely to persist beyond the public health emergency period. The current increase in federal matching funds could offset or reduce state spending but is unlikely to fully offset state revenue declines and address budget shortfalls.
The election will have implications for LTSS issues, and Medicaid’s role as its primary payer, given the effects of the pandemic, the resulting economic crisis, and the coming age wave. Democratic Presidential nominee Joe Biden recently released a plan to increase access to Medicaid home and community-based services (HCBS), while the Trump Administration has proposed a Medicaid program-wide federal financing cap in the President’s FY 2020 budget and is asking the Supreme Court to invalidate the entire Affordable Care Act, including provisions that allows states to expand Medicaid HCBS. This issue brief identifies trends in state policy actions related to Medicaid for seniors and people with disabilities and LTSS as of August 21, 2020. These include actions to expand eligibility and streamline enrollment, ease premium and/or cost-sharing requirements, enhance benefits, increase provider payment, modify provider qualifications, and alter reporting requirements.
Key Findings
States are adopting Medicaid policies targeted to seniors, people with disabilities, and LTSS in response to the pandemic through a variety of authorities that have different expiration dates. These authorities include Disaster-Relief State Plan Amendments (SPAs), traditional SPAs, other administrative authorities, HCBS waiver Appendix K, Section 1115 demonstration waivers, and Section 1135 waivers. The beginning and ending dates vary by authority (Appendix Table 1).
Eligibility and Enrollment
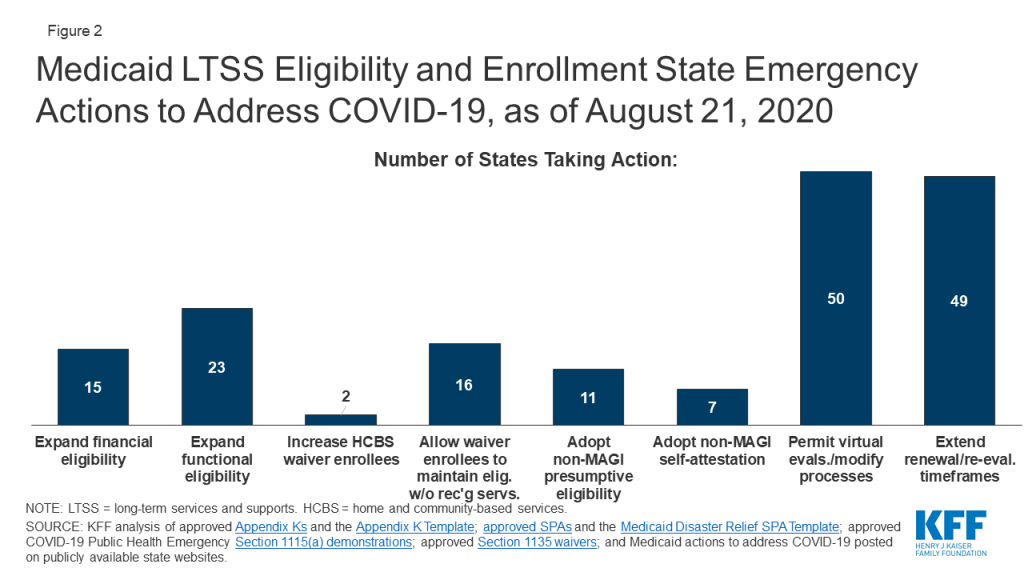
Fifteen states are expanding financial eligibility limits for seniors and people who qualify for Medicaid based on a disability to increase access to coverage during the public health emergency (Figure 2). Coverage groups where eligibility is based on old age or disability (known as “non-MAGI groups”) have income limits, and at state option, also may have asset limits. State actions to expand financial eligibility in these pathways include applying less restrictive income or asset methodologies and/or increasing HCBS waiver cost limits during the emergency period. For example, North Carolina is disregarding increases in assets for all non-MAGI groups until after the emergency period ends, and Massachusetts is allowing people with disabilities to obtain a temporary hardship waiver of the medically needy spend down requirement during the public health emergency. In addition, North Carolina and Washington are modifying financial eligibility criteria for some HCBS to cover beneficiaries who would otherwise not be eligible.
Figure 2: Medicaid LTSS Eligibility and Enrollment State Emergency Actions to Address COVID-19, as of August 21, 2020
Less than half of states (23) are expanding functional eligibility criteria to help more people qualify for coverage based on a disability during the emergency period (Figure 2). In addition to meeting financial eligibility criteria, coverage groups related to disability status require individuals to meet functional criteria, for example, based on the extent of their self-care needs. Missouri expanded coverage to adults who test positive for coronavirus by considering it a qualifying disability for its aged/blind/disabled pathway.1 Indiana is giving HCBS waiver enrollment priority to people with COVID-19 or who are presumed positive from its waiting lists for waivers that provide non-residential supports for people with I/DD, while other states are temporarily modifying HCBS waiver functional eligibility targeting criteria. In addition, 13 states are modifying HCBS waiver assessment requirements to allow individuals to begin receiving services before a functional eligibility evaluation is completed (no data shown).
Maryland and Utah are increasing the total number of individuals served in HCBS waivers during the emergency period (Figure 2). Maryland is increasing the number of individuals served in its waiver for children with autism spectrum disorder; Utah is increasing the number of individuals served by a waiver for people transitioning from institutions to the community. Unlike state plan coverage groups, states can limit the number of people who enroll in waivers, which can result in waiting lists when the number of people seeking services exceeds the number of waiver slots available. States acknowledged that the pandemic may exacerbate the need for HCBS waiver services; for example, Pennsylvania noted that many people on its waiver waiting list have aging caregivers who may not be able to continue providing care if they develop COVID-19. However, few states have been able to increase the number of waiver enrollees served in response to the pandemic. In addition, 16 states are allowing individuals to maintain HCBS waiver eligibility without receiving services, which can keep enrollees connected to coverage while services are interrupted due to provider shortages or restrictions due to state stay-at-home orders or while individuals are receiving inpatient treatment during the pandemic (Figure 2).
Nearly all states are taking at least one action to streamline eligibility determinations to expedite enrollment in coverage for seniors and people with disabilities during the emergency. Eleven states are allowing hospitals to make presumptive eligibility determinations for non-MAGI groups during the emergency, which can help connect people to coverage at the time they seek medical treatment (Figure 2). Seven states are allowing applicants in non-MAGI pathways to self-attest to financial and/or functional eligibility requirements in lieu of requiring documentation before determining eligibility (Figure 2). The most frequent action in this area is permitting virtual evaluations to determine HCBS waiver functional eligibility and/or otherwise modifying processes for HCBS waiver level of care evaluations and reevaluations to account for social distancing during the pandemic, adopted by 50 states (Figure 2).
Almost all states are extending eligibility renewal due dates during the pandemic to keep people connected to coverage and enable states to focus limited state agency staff time on responding to the emergency. Forty-nine states are extending reassessment and reevaluation due dates for one or more HCBS waivers (Figure 2). Pennsylvania is extending eligibility renewal deadlines for non-MAGI populations to every 12 months. As one of the conditions of receiving the enhanced federal matching funds under the Families First Coronavirus Response Act, states must provide continuous eligibility for individuals enrolled on or after March 18, 2020 through the end of the month in which the public health emergency ends.2
Premiums and Cost-Sharing
States are eliminating or easing premiums and cost-sharing requirements to help seniors and people with disabilities remain in coverage and facilitate access to services during the pandemic. More than one-third of states are eliminating or waiving premiums in Medicaid pathways that offer buy-in coverage for working people with disabilities, while a couple of states are easing cost-sharing requirements (Figure 1). Connecticut is suspending copayments for individuals who are dually eligible for Medicare and Medicaid. Rhode Island has adopted a policy that helps ensure that people with short-term nursing home stays will have a community-based residence to which they can return post-discharge by allowing enrollees to receive a home maintenance allowance throughout the public health emergency. This policy accounts for the financial cost of maintaining a home in the community by reducing the amount that these enrollees must pay out-of-pocket for institutional care and applies to individuals who were institutionalized for less than six months as of March 1, 2020, and unable to be discharged home due to COVID-19.
Benefits
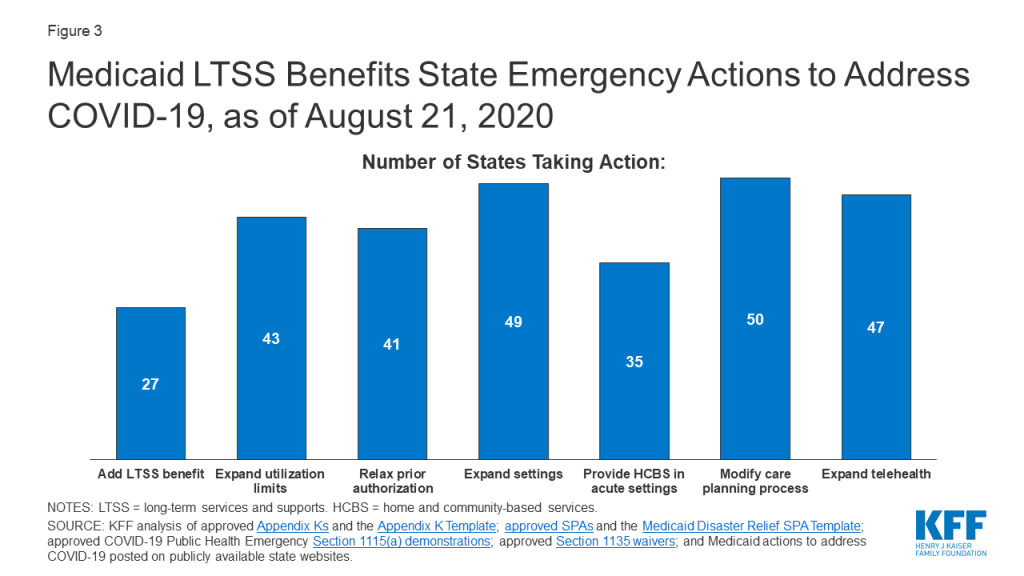
About half of states (27) are temporarily adding new services to their regular LTSS benefit packages to meet enrollee needs during the public health emergency (Figure 3). Nearly all state actions in this area relate to expanding the benefit packages available under HCBS waivers and/or Section 1915 (i) state plan HCBS. Frequently added services include home-delivered meals; medical supplies, equipment, and appliances; and assistive technology. Some states are adding other services to address the emergency. For example, Washington is adding wellness education to help HCBS waiver enrollees manage chronic conditions, avoid health risks and be informed about COVID-19. Indiana is adding rent and food reimbursement to help enrollees in an I/DD waiver offset the costs of room and board for an unrelated, live-in caregiver during the emergency. On the institutional LTSS side, Ohio has created a new benefit, Health Care Isolation Centers. These services are provided in specialized COVID-19 facilities to individuals who have been discharged from hospitals but continue to need medical and isolation care that cannot be provided in the community or their former congregate setting.
Figure 3: Medicaid LTSS Benefits State Emergency Actions to Address COVID-19, as of August 21, 2020
While the majority of benefits changes are expansions, one state is restricting benefits, and many are restricting visitors in HCBS settings in efforts to contain coronavirus spread (no data shown). Washington has authority to suspend specialized add-on nursing home services like habilitation during an emergency to protect the health of residents and staff. Similar to CMS guidance restricting visitors in nursing homes, 40 states are not allowing any visitors in at least some HCBS waiver residential settings to minimize the spread of infection.
Most states (43) are temporarily modifying utilization limits for covered services to ensure that enrollees can access services and address health and welfare issues during the emergency (Figure 3). Among these states, most are allowing utilization limits to be exceeded for HCBS waiver and/or state plan services. For example, Arkansas is removing its limit on physician visits in nursing homes, and Ohio is lifting hour and day limits on private duty nursing services post-discharge. In addition, 31 states are temporarily modifying the scope of HCBS waiver covered services to account for needs created by the pandemic (no data shown). For example, Tennessee is adding HCBS waiver services to support individuals with I/DD with shopping, hygiene, meal preparation and money management. By contrast, North Carolina, Rhode Island and Washington are restricting utilization of HCBS services (no data shown). All three states have Section 1115 waivers that allow them to vary the amount, duration, and scope of services based on population needs. In addition, North Carolina and Washington may target services on a less than statewide basis.
Most states (41) are suspending prior authorization requirements to ensure access to HCBS waiver and/or state plan services during the emergency (Figure 3). For example, Connecticut is waiving prior authorization for home health services, Maryland is suspending prior authorization for remote patient monitoring, and Nebraska is waiving prior authorization for transfers to post-acute long-term acute care hospitals, acute inpatient rehabilitation, or skilled nursing facility care. In addition, eight states are allowing other licensed providers to order home health services for state plan HCBS in addition to physicians (no data shown).
Nearly all states are expanding the settings where enrollees can receive HCBS to account for disruptions due to COVID-19 (Figure 3). Among these states, 49 are temporarily expanding the settings where HCBS waiver services can be provided during the public health emergency to include providing services in hotels, shelters, schools and churches, as needed. In addition, 35 states are allowing individuals in short-term inpatient settings to receive HCBS to provide communication and behavioral supports (Figure 3). Most states have adopted this policy for one or more HCBS waivers, and a couple are doing so for state plan HCBS: Alaska is allowing Community First Choice attendant care services to be provided in acute care hospitals, and Oregon is temporarily allowing payment for state plan HCBS, including home-based habilitation, behavioral habilitation, and psychosocial rehabilitation services, to individuals in an inpatient setting.
Nearly all states (50) are modifying care-planning processes to accommodate social distancing and facilitate access to services during the emergency (Figure 3). Examples of frequently adopted policy changes in this area include modifying the person-centered plan development process for HCBS waiver services, adjusting functional assessment requirements used to determine service levels, and adding electronic document signing. Other policy changes in this area include allowing verbal consent instead of a written signature for HCBS service plans and allowing the face-to-face encounter for home health services to take place up to one year after an individual begins receiving services. North Carolina and Washington are allowing for the provision of LTSS to individuals impacted by the emergency even if the services are not updated timely in the care plan. Michigan is extending service authorizations in person-centered service plans for state plan HCBS throughout the duration of the public health emergency.
Nearly all states have expanded the delivery of HCBS via telehealth (Figure 3). Forty-seven states are adding electronic service delivery methods to continue providing HCBS waiver and state plan in-home services remotely. Minnesota is allowing state plan group therapy and rehabilitative services to be provided via telehealth. Oregon is allowing adding telehealth delivery of state plan home-based habilitation, behavioral habilitation, and psychosocial rehabilitation services. Connecticut is allowing for telephonic check-ins in lieu of face-to-face assistance for certain mental health HCBS waiver enrollees. DC is also covering services provided remotely to state plan HCBS recipients, such as wellness checks and therapeutic activities.
Provider Payment
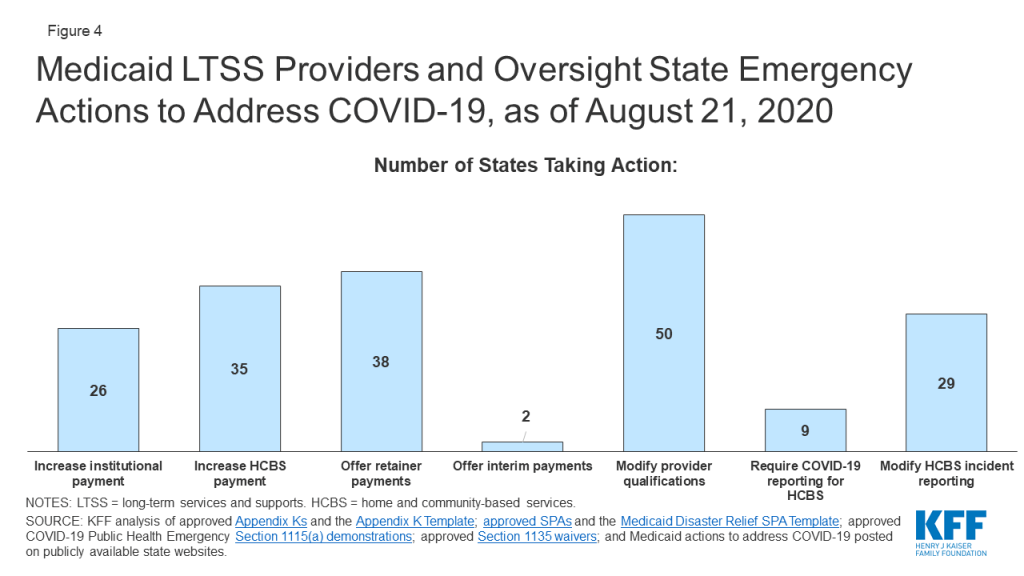
Just over half of states are increasing institutional LTSS payment rates (Figure 4). Among these 26 states, 24 have increased rates for nursing homes, which have been disproportionately affected by the COVID-19 pandemic, and five states are doing so for intermediate care facilities for people with intellectual or developmental disabilities or other institutional settings (no data shown). Most states are implementing per diem or percentage rate increases, while a few states are increasing the number of days for which facilities can receive bed hold payments to account for absences due to COVID-19 treatment. Alabama also is providing an additional add-on cleaning fee. Kentucky is temporarily pausing per diem rate sanctions to nursing facilities that are unable to meet medical record review thresholds to validate assignment of patients to reimbursement groups based on acuity during the public health emergency.
Figure 4: Medicaid LTSS Providers and Oversight State Emergency Actions to Address COVID-19, as of August 21, 2020
Some states limit the additional payments to facilities or patients with a COVID-19 diagnosis, while others apply them to all nursing facilities to account for increased costs related to staffing, equipment and cleaning as a result of the emergency (no data shown). For example, Michigan is providing a $5,000 per bed supplemental payment in the first month for COVID-19 regional hub nursing facilities to address immediate infrastructure and staffing needs and a $200 per diem rate increase in subsequent months to account for the higher costs of caring for COVID-19 patients.
A couple of states specifically have included pay increases for direct care workers in nursing homes and/or other institutional settings (no data shown). Arkansas adopted temporary supplemental payments that increase direct care workers’ weekly pay by a base supplemental payment according to number of hours worked and an additional tiered acuity payment for those working in facilities with COVID-19 positive patients. Texas’ nursing facility payment rates increase includes a pay increase for direct care workers and an increase for supply and dietary costs.
Just over two-thirds of states (35) are increasing provider payment rates for at least some HCBS state plan or waiver services during the public health emergency (Figure 4). For example, Alabama is increasing waiver payment rates for personal care, adult companion, respite, and skilled nursing care to account for overtime pay, staffing needs and infection control supplies. Louisiana has received approval to increase payments for all services provided under its Community Choices Waiver for elderly and disabled adults by up to 50% as needed to maintain staffing. States increasing payment rates for HCBS provided under state plan authority include targeted case management (AK), day habilitation (AR), skilled and/or private duty nursing (DC, OK), and home health and adult care homes (NC). Arkansas’s temporary supplemental payments for direct care workers in nursing facilities also apply to direct care workers in assisted living facilities and those providing home health and personal care services in the community. Michigan adopted a supplemental payment for providers of personal care and behavioral health treatment technician in-person services. Washington’s Section 1115 demonstration waiver allows the state to increase rates for Community First Choice attendant care services by up to 50 percent to maintain provider capacity during the public health emergency. In addition, Tennessee has adopted temporary payment rate increases for community-based residential, personal care, attendant care, personal assistance and intensive behavioral treatment stabilization and treatment services and a temporary per diem add-on to community-based residential and personal care payment rates to account for direct support staff hazard pay, overtime, and PPE costs using its existing directed payment authority; these services are provided under a Section 1115 HCBS waiver.
Among the states adopting LTSS provider payment increases, 18 states have increased rates for both institutional and community-based services (no data shown). Ten states have increased provider payments for only institutional services, while 17 states have increased rates for HCBS only.
About three-quarters of states are adopting retainer payments for HCBS providers (Figure 4). Thirty-eight states have adopted retainer payments for providers offering HCBS through waiver and/or state plan authorities. For example, Washington and New Hampshire have an approved Section 1115 waiver that authorizes retainer payments for personal care and habilitation services provided under state plan authority.
Two states are making interim payments to LTSS providers (Figure 4). Among these states, North Carolina allows any Medicaid-enrolled provider to request that their reimbursement be converted to an interim payment methodology, while Georgia is making interim payments to skilled nursing facilities.
Provider Qualifications
Nearly all states (50) are temporarily modifying HCBS state plan and/or waiver provider qualifications in response to potential staff shortages and increased demand due to COVID-19 (Figure 4). Frequently adopted policies in this area include temporarily permitting payment for HCBS waiver services rendered by family caregivers or other legally responsible relatives during the emergency (if not already permitted in the waiver), adopted by 38 states (no data shown). Twenty-three states are waiving conflict of interest rules and allowing case management entities to also be direct service providers for HCBS waiver enrollees during the emergency (no data shown). In addition, all states have adopted modified provider screening requirements through Section 1135 waiver authority, which may apply to LTSS providers as well as other providers.
Reporting and Oversight
Few states are adopting reporting requirements for COVID-19 cases and deaths among HCBS enrollees (Figure 4). CMS is requiring all nursing facilities to report COVID-19 cases and deaths as of May 8, 2020, but just nine states are requiring reporting of COVID-19 cases among HCBS waiver enrollees. HCBS waiver enrollees living in congregate settings such as group homes are likely to experience increased risk from coronavirus infection similar to individuals in nursing homes. In addition to the CMS nursing home reporting requirements, three states (AZ, CT, IN) have adopted their own reporting requirements related to COVID-19 cases and deaths for long-term care facilities. For example, Connecticut requires managed residential communities and nursing homes to provide daily COVID-19 status reports. Arizona also requires reporting on COVID-19 cases and deaths from group homes.
Twenty-nine states are temporarily modifying HCBS waiver incident reporting requirements and other participant safeguards during the public health emergency (Figure 4). This allows states to focus their administrative efforts on the COVID-19 response. However, there are potential risks for enrollees as incident reporting is a requirement for HCBS programs to protect enrollees from abuse, neglect and injury and to ensure their health and safety. Twenty-eight states are delaying submitting HCBS waiver enrollment and spending reports to CMS and/or are suspending data collection for performance measures other than health and welfare (no data shown). In addition, forty-seven states are suspending pre-admission screening and annual resident review requirements for nursing facilities (no data shown).
Looking Ahead
The duration of the public health emergency has implications for policy actions adopted under Medicaid emergency authorities as well as the availability of enhanced federal funding provided through the match rate increase. Many state policy changes have been adopted through temporary authorities that will expire after the public health emergency declaration ends, which will lead policymakers to assess whether any policies can or should be retained and transitioned to other authorities. In addition, some policy changes in response to the pandemic may be difficult for states to sustain without additional federal financial support beyond the 6.2 percentage point increase in federal Medicaid matching funds authorized by Congress during the public health emergency, as states are facing revenue declines and budget shortfalls.
A great deal of attention has been focused on the impact of COVID-19 in nursing homes, given the disproportionate number of cases and deaths among residents and staff nationally with less attention on community-based residential settings. The Trump Administration has issued guidance about how nursing homes should respond to the pandemic, announced the formation of an independent commission to assess nursing home response, and adopted new reporting requirements for COVID-19 cases and deaths in nursing homes. To date, less attention to COVID-19 cases and deaths generally has been paid to community-based residential settings, such as group homes, where the pandemic presents similar risks to Medicaid enrollees and providers due to the highly transmissible nature of the coronavirus, the congregate nature of the setting, and the close contact that many workers have with residents. Data about COVID-19 cases and deaths in both institutional and community-based congregate settings may allow policymakers to more fully assess the impact across populations at increased risk of adverse health outcomes. The pandemic also may exacerbate the need for HCBS waiver services, which already are subject to waiting lists in a number of states. For example, elderly parents sickened by COVID-19 may no longer be able to provide care for their adult children with disabilities. Beyond the pandemic, the coming age wave makes LTSS and Medicaid’s role as the primary payer likely to be policy issues faced by the next Administration, in addition to the continuing effects of the pandemic and economic crisis.
Appendix
Appendix Table 1: Medicaid Emergency Authorities
Authority
Description
Start Date
End Date
Disaster-Relief SPA
Allows states to make temporary changes to address eligibility, enrollment, premiums, cost-sharing, benefits, payments, and other policies differing from their approved state plan during the COVID-19 emergency. States may not make changes that restrict or limit payment, services, or eligibility or otherwise burden beneficiaries and providers.
1/1/20 (using Section 1135 waiver authority) or later date elected by state
End of public health emergency or earlier date elected by state
Traditional SPA
Allows states to amend their Medicaid state plans, which govern program elements such as coverage groups, covered services, provider reimbursement methodologies, and administrative activities.
1st day of quarter in which SPA is submitted to CMS or later date elected by state
Continues until subsequently amended or terminated
HCBS Waiver Appendix K
Allows state to amend Section 1915 (c) or Section 1115 HCBS waiver provisions related to eligibility, services, payment, provider qualifications, level of care evaluations, person-centered service plans, incident reporting, settings, and other policies to respond to emergency.
1/27/20 or later date elected by state and approved by CMS
1/26/21 or earlier date elected by state
Section 1115 Demonstration Waiver
Allows states operate to Medicaid programs without regard to specific statutory or regulatory provisions to furnish medical assistance in a manner intended to protect, to the greatest extent possible, the health, safety, and welfare of individuals and providers who may be affected by COVID-19.
3/1/20 or later date elected by state and approved by CMS
60 days after public health emergency ends or earlier date approved by CMS
Section 1135 Waiver
Allows states to operate Medicaid programs without regard to certain fee-for-service prior authorization, LTSS authorization and assessment, fair hearing procedural and timeline, provider enrollment, reporting and oversight, and other requirements, to ensure that sufficient health care items and services are available to meet enrollee needs and that providers are reimbursed.
3/1/20
End of public health emergency, per CMS guidance
SOURCE: KFF analysis of Medicaid emergency authorities and CMS guidance.
Endnotes
Missouri elects the Section 209 (b) option to apply Medicaid financial and/or functional eligibility rules to SSI beneficiaries that differ from federal SSI rules. KFF, Medicaid Financial Eligibility for Seniors and People with Disabilities: Findings from a 50-State Survey (June 2019), https://modern.kff.org/report-section/medicaid-financial-eligibility-for-seniors-and-people-with-disabilities-findings-from-a-50-state-survey-issue-brief/. In its COVID-19 Frequently Asked Questions, CMS notes that “[i]n making disability determinations, a state must generally use the same definition of disability as used for supplemental security income (SSI). A positive diagnosis for COVID-19 is not a per se disability under SSI criteria and therefore cannot be the sole basis of a determination of disability for purposes of Medicaid eligibility.” CMS, COVID-19 Frequently Asked Questions (FAQs) for State Medicaid and Children’s Health Insurance Program (CHIP) Agencies at II.C.2 (last updated June 30, 2020), https://www.medicaid.gov/state-resource-center/Downloads/covid-19-faqs.pdf. ↩︎
States generally must maintain Medicaid eligibility through the end of the month in which the public health emergency period ends for all individuals enrolled on or after March 18 2020, as a condition of receiving the 6.2 percentage point increase in federal matching funds. KFF, Key Questions About the New Increase in Federal Medical Matching Funds for COVID-19 (May 2020), https://modern.kff.org/coronavirus-covid-19/issue-brief/key-questions-about-the-new-increase-in-federal-medicaid-matching-funds-for-covid-19/. CMS has clarified that states are not prohibited from conducting regular eligibility renewals during this period, but as a condition of receiving the enhanced federal matching funds, states cannot terminate coverage for any Medicaid beneficiary enrolled on or after March 18 2020, unless the individual is no longer a state resident or requests voluntary termination. CMS, Families First Coronavirus Response Act – Increased FMAP FAQs, question B.11 (updated as of 4/13/2020), https://www.medicaid.gov/state-resource-center/downloads/covid-19-section-6008-faqs.pdf. ↩︎
Amid the coronavirus pandemic, half of Americans report that their mental health has been negatively impacted due to related stress and worry. Many are, or will be, struggling with mental health challenges due to anxiety, social isolation, loss of loved ones, and job losses – potentially leading to increased mental health care needs over the long term.
A new issue brief examines where President Trump and Democratic presidential nominee Joe Biden stand on key aspects of the nation’s mental health and substance use challenges. Key points include:
Opioid epidemic. President Trump declared a national public health emergency in 2017 and has renewed it repeatedly since then. His proposed 2021 budget would decrease total funding to the Substance Abuse and Mental Health Services Administration and to Medicaid, the nation’s largest payer for mental health services and main contributor for substance use disorder services. Vice President Biden’s campaign website features a five-point plan to address the opioid crisis that would increase access to services, curb unnecessary opioid prescriptions, and hold pharmaceutical companies accountable for their role in the crisis.
Suicide prevention. Both candidates’ suicide prevention plans focus on veterans, with President Trump creating a task force to tackle the issue and proposing to boost the Veterans Administration (VA) budget for suicide prevention. Vice President Biden proposes to expand and strengthen veterans’ mental health programs inside and outside the VA, as well as strengthen programs aimed at reducing suicide among LGBTQ teenagers.
Mental health parity. Vice President Biden’s campaign vows to redouble efforts to enforce existing mental health parity laws and expand funding for mental health, but has not offered specific plans. President Trump’s campaign website does not address mental health parity. His administration is seeking to overturn the Affordable Care Act, which would substantially limit the scope of parity rules.
Mental health workforce. Neither candidate specifically addresses mental health workforce shortages on their campaign websites. However, President Trump’s 2021 budget proposal includes a 24% increase for behavior health workforce development programs, and Vice President Biden’s education plan would double the number of psychologists, counselors and other mental health professionals in schools.
The brief draws on each candidates’ campaign website, news coverage, public statements and budget proposals. It is part of KFF’s ongoing efforts to provide useful information related to the health policy issues relevant for the 2020 elections, including policy analysis, polling, and journalism. Find more on our Election 2020 resource page.
KFF also has compiled state-specific data on mental health and substance use on more than 20 indicators, with mental health state fact sheets available profiling each state, as well as an updated look at how the COVID-19 pandemic is affecting Americans’ mental health.
Amid the COVID-19 pandemic, many Americans are struggling with mental health challenges. In a recent KFF poll, majority (53%) of adults in the United States reported that their mental health has been negatively impacted due to worry and stress over the virus. Additionally, more than one in three adults in the U.S. reported symptoms of anxiety or depressive disorder during the pandemic, up from roughly one in ten in 2019. As the virus continues to spread, the pandemic will likely lead to increased mental health care needs and significantly impact the well-being of people in the U.S. Under the Trump administration, the recently-passed Coronavirus Aid, Relief, and Economic Security Act (CARES Act) may address some of these needs.
Mental health was already a key public health issue. In recent years, growing numbers of Americans have reported being depressed, and deaths due to drug or alcohol abuse, or suicide have increased. In 2017-2018, nearly 17 million adults and an additional 3 million adolescents had a major depressive episode in the past year, and over 10 million adults with mental illness had serious thoughts of suicide in the past year. Nearly 14 million adults reported an unmet need for mental health or substance use treatment, with many citing cost as a barrier.
The 2020 presidential election could have a substantial effect on the United States’ response to growing mental health needs and long-term policy for addressing this public health challenge. This issue brief examines the presumptive 2020 presidential candidates’ positions on mental health and substance use disorders. Specifically, we analyzed candidate positions on suicide prevention, mental health workforce issues, mental health parity enforcement, and the opioid epidemic. We synthesize policy positions for President Donald Trump and the presumed Democratic nominee, Former Vice President Joe Biden.
We identified candidate positions first by gathering information directly from campaign platforms as stated on candidate websites. Where information was not available on former Vice President Biden’s website, we supplemented with information his campaign supplied in a survey conducted by Mental Health for US, a nonpartisan coalition of organizations working in mental health and addiction policy. President Trump did not participate in the survey as of this brief’s publication, so we also reviewed news coverage of his campaign from the last year and his proposed 2021 budget for mention of these mental health-related topics. While candidates may have made other statements about mental health and substance use disorders, we do not aim to capture all comments ever made but instead focus on the candidates’ stated platforms.
The candidate platforms differ in both the amount of attention paid to mental health and their approaches to addressing these issues. Election outcomes thus have potentially large implications for policy direction in these areas of mental health and substance use funding, service delivery, and access.
Rising Suicide Rates & Suicide Prevention
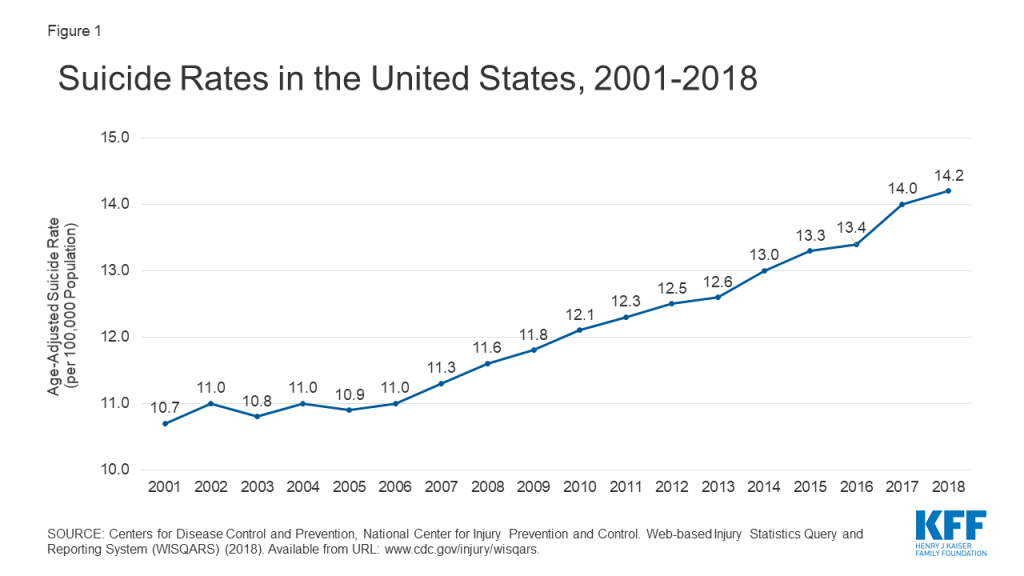
Due to necessary social distancing, many people are experiencing isolation, distress, and barriers to accessing mental health services. Historically, national crisis hotlines have seen a spike in calls during distressing nationals events, and as the pandemic continues, calls to hotlines are on the rise. There is particular concern about suicidal ideation during this time, as isolation is a risk factor for suicide. In 2018, over 48,000 Americans died by suicide1 , and in 2017-2018, over ten million American adults (4.3%) reported having serious thoughts of suicide in the past year. Suicide is one of the top ten causes of death in the U.S. and accounts for majority of firearm deaths. Moreover, the Centers for Disease Control and Prevention (CDC) documents a substantial increase in the national suicide rate over time, with the age-adjusted suicide rate rising from 10.7 per 100,000 people in 2001 to 14.2 per 100,000 people in 2018 (Figure 1). Among working-age Americans (ages 16-64 years), the suicide rate rose by 40% over the same period. Both presidential candidates have offered suicide prevention plans with particular attention paid towards veterans, one subgroup at higher risk of suicide than the general population.
Figure 1: Suicide Rates in the United States, 2001 – 2018
President Trump’s suicide prevention plan focuses on the veteran population. His campaign website spotlights his 2019 executive order creating a task force dedicated to preventing suicides among veterans, and his proposed 2021 budget for the Department of Veterans Affairs allocates roughly 30% more in funding for suicide prevention among veterans than the 2020 enacted budget. Separately, in President Trump’s proposed 2021 budget for SAMHSA, he includes a small increase in funding for specific grant-based suicide prevention programs.
Former Vice President Biden’s suicide prevention plan is primarily focused on the veteran population. His campaign website details several initiatives that he would implement within the Veterans Affairs health system, which would increase funding for mental health services, streamline the initiation of mental health treatment, and increase the number of mental health staff practicing in VA hospitals. Former Vice President Biden’s plan states that he would also establish a national center of excellence for reducing veteran suicide to develop and implement suicide prevention strategies outside of the VA health system, and that he would address risk factors for suicide such as PTSD and sexual assault among current and former service members, though details on possible approaches are not provided. Additionally, in the context of the youth LGBTQ community, former Vice President Biden states that he will strengthen suicide prevention programs for teens, but does not provide specific details.
Mental Health Workforce Shortages
The need for mental health care is expected to increase in light of the coronavirus pandemic. Due to ongoing, widespread efforts to slow the spread of the virus by means of social distancing, an increasing number of mental health providers are offering services through telehealth, but those with limited capacity to do so may be scaling back their practices. Meanwhile, many individuals seeking mental health care are already unable to access care in a timely manner due to provider shortages across the country. Nationwide, nearly 117 million people are in a mental health provider shortage area, and less than 30% of the need for psychiatrists is being met.2 Furthermore, HRSA projects there will be a nationwide shortfall of over 12,500 adult psychiatrists and over 11,500 addiction counselors by the year 2030. Access to pediatric providers is particularly problematic, with 70% of counties in the U.S. having no practicing child psychiatrist. Neither candidate has provided specific details on how they will increase the mental health workforce to address the lack of providers.
President Trump’s campaign website does not specifically address mental health workforce shortages. However, his 2021 budget proposal for HRSA indicates roughly a 24% increase in funding for behavioral health workforce development programs from 2019 to 2020, which would not change for 2021.
Former Vice President Biden’s campaign website does not specifically address mental health workforce shortages. However, in the context of his education plan, he states he will double the number of psychologists, guidance counselors, and other mental health professionals in schools. In a survey by Mental Health for US, former Vice President Biden states that he will increase funding for the National Health Service Corps and create partnerships between health centers, high schools, and community colleges in order to encourage youth to pursue health care jobs. He also adds that he will build on legislation such as the 21st Century Cures Act and the Opioid Workforce Act of 2019, which address the shortage of mental health and substance use disorder providers.
Mental Health Parity
There is a focus on addressing access barriers for services many people need in relation to the coronavirus pandemic, such as potentially high cost-sharing for testing and treatment. Access to mental health and substance use disorder services is also a key need to address, and has its own challenges due to lingering issues with mental health parity. The Mental Health Parity and Addiction Equity Act (MHPAEA) was passed in 2008, requiring insurer coverage of mental health and substance use disorder services in a way that is equivalent to coverage for medical and surgical services. The law prohibits most group health plans that offer coverage for mental health and substance use conditions from imposing treatment limitations and financial requirements on those benefits that are stricter than for medical and surgical benefits. The 2010 Affordable Care Act (ACA) expanded MHPAEA’s reach by requiring coverage of behavioral health services as an “essential health benefit” in many private health plans (a notable exception being large employer plans) and extending parity requirements to the small group, individual, and Medicaid managed care markets. Since the MHPAEA took effect, changes in the use of mental health services have been modest. Additionally, while research has documented an effect of parity on equalizing quantitative treatment limitations and cost sharing, it has been more difficult to measure and regulate the law’s effect on non-quantifiable treatment limitations, such as prior authorization and network adequacy, which are also supposed to be provided at parity. Questions remain as to how to improve parity enforcement; so far, both candidates have offered limited details.
President Trump’s campaign website does not address parity for mental health services. The Trump administration has joined Texas and several other states in Texas v. U.S. (known as California v. Texas by the Supreme Court, which recently agreed to hear the case), arguing that the ACA should be invalidated, an outcome that would substantially limit the scope of parity rules and eliminate the essential health benefit requirement. The Trump administration has also expanded the allowed duration of short-term health plans, which do not have to comply with ACA requirements, typically do not cover mental health services, and generally exclude people with pre-existing conditions such as serious mental illnesses.
Former Vice President Biden’s campaign website says that, as president, he would “redouble” efforts to enforce existing mental health parity laws and expand funding for mental health. He points to his previous role in implementing the MHPAEA but does not specify which actions his administration would take to further enforcement.
The Opioid Epidemic and Drug Overdoses
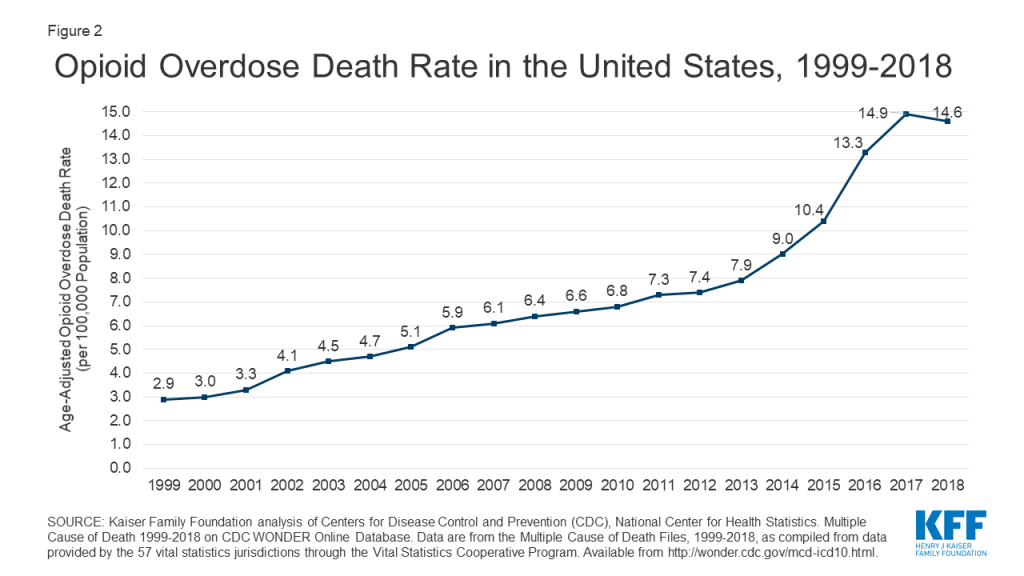
Preliminary data shows that deaths due to drug overdose are increasing during the coronavirus pandemic. This may be a result of necessary lockdowns, barriers to care, and the economic recession. Prior to the pandemic, deaths due to opioid overdose saw large increases, from 2.9 deaths per 100,000 people in 1999 to 14.6 deaths per 100,000 people in 2018 (Figure 2). In response to the growing opioid epidemic, the Department of Health and Human Services declared a public health emergency in 2017 and introduced five strategies: 1) improving access to treatment, 2) increasing use of drugs to reverse overdoses, 3) public health surveillance, 4) research on pain and addiction, and 5) identifying better practices to manage pain. In recent years, several indicators have shown some improvement in opioid misuse or overdose, but rising rates of use or misuse of illicit drugs—including methamphetamine, cocaine, and benzodiazepines—have broadened the scope of the addiction crisis. Each presidential candidate has proposed strategies to address the opioid epidemic and substance use disorder going forward, including details on making medication-assisted treatment3 more widely available.
Figure 2: Opioid Overdose Death Rate in the United States, 1999-2018
President Trump’s reelection campaign website states that addressing the opioid epidemic has been a priority for his administration, which declared the crisis a national public health emergency in late 2017 and has since renewed the declaration every 90 days. He also signed legislation approving additional grant funds to combat the opioid epidemic, including the SUPPORT for Patients and Community Act. However, President Trump’s proposed 2021 budget would continue to decrease total funding for both the Substance Abuse and Mental Health Services Administration (SAMHSA) and Medicaid – the U.S.’s largest payer for mental health services and a main contributor for substance use disorder services. Despite these overall cuts, the proposed budget for SAMHSA includes a small increase in state grants to address opioid use disorders, and the proposed budget for Medicaid includes increased funding over ten years for states to extend postpartum coverage for women with substance use disorders. The proposed budget for opioid response programs in rural areas under the Health Resources and Services Administration (HRSA) remains flat for 2020 and 2021, but down from 2019.
Former Vice President Biden’s campaign website outlines a detailed, five-point plan to address the opioid crisis. First, it states how he will monitor and hold pharmaceutical companies accountable for their role in the crisis, notably by banning pharmaceutical companies from financially incentivizing prescriptions and appointing an “Opioid Crisis Accountability Coordinator” to work with both federal and state-level efforts. Second, former Vice President Biden states that he will increase access to substance use disorder services through a $125 billion investment over a ten-year period. These investments will include making medication-assisted treatment universally accessible by 2025 by building on the 21st Century Cures Act; providing funding to underserved communities with high rates of substance use disorder; and increasing funding for the National Institutes of Health’s Helping to End Addiction Long-Term research initiative. His third point indicates several ways he intends to stop the unnecessary prescription of opioids, including having states require prescriber participation in prescription drug monitoring programs and supporting the use of alternative pain treatments and development of less addictive pain medications. The final two points of former Vice President Biden’s statement focus on reducing the amount of illicit drugs entering the U.S. and diverting incarceration based solely on drug use to drug courts and treatment services.
Discussion
As the novel coronavirus pandemic continues, it spotlights the importance of mental health issues in the lead-up to the 2020 election. The pandemic is expected to not only exacerbate the existing mental health issues and barriers to care that people face, but to also increase the need for already limited mental health services. President Trump and former Vice President Biden have taken stances on several mental health issues, including the opioid crisis, rising suicide rates, and – to a more limited extent – parity in coverage for mental health services and nationwide shortages in the mental health workforce.
Suicide Prevention: Both of the presumptive 2020 presidential candidates give special attention to veterans in their suicide prevention plans and plan to expand access to mental health services through the VA health system.
Mental Health Workforce: Former Vice President Biden supports increasing the mental health workforce, including expansion of national service organizations such as the National Health Service Corps.
Mental Health Parity: The candidates do not provide specific plans to enforce the mental health parity requirements of the MHPAEA and ACA, and President Trump, more broadly, is arguing in court that the ACA should be invalidated.
Opioids: Both President Trump and former Vice President Biden have presented plans to expand access to treatment services such as medication-assisted treatment programs. In addition to this, former Vice President Biden emphasizes holding pharmaceutical companies and drug manufacturers accountable and intends to stop the overprescribing of opioids.
Beyond the candidates’ specific plans, a number of major election issues have implications for mental health, including immigration, gun violence, and the future of the ACA.
The subjects of immigration and border security remain prominent in President Trump’s reelection campaign. Several mental health experts have weighed in on the Trump administration’s policy of separating families at the U.S.’s southern border, raising concerns that children separated from their parents and detained at border facilities may be at substantially elevated risk of developing mental health conditions. Former Vice President Biden has stated he would end current practices of long-term detention, separating families, and workplace immigration raids.
President Trump has responded to recent mass shootings by arguing that gun violence is best addressed as a mental health issue. The Trump administration has considered researching whether technological devices can be used to monitor people with mental illnesses in order to prevent them from committing violent acts. However, most scientific evidence does not support a direct link between mental illness and gun violence, and instead suggests that people with mental illness are more likely to be victims of violence than perpetrators. Former Vice President Biden supports stronger gun control, including universal background checks and an assault weapons ban.
The future of the ACA remains uncertain, as the Trump administration has joined Texas and several other states in pushing to invalidate the law in Texas v. U.S. Because the ACA’s provisions require insurers to cover mental health care and substance abuse treatment, a ruling against the law would likely reduce access to these services for many Americans. Particularly if the ACA is struck down, these actions may limit the federal administration’s capacity to reduce opioid overdose deaths and suicide rates, and would undermine efforts to achieve parity for mental health coverage. Former Vice President Biden has criticized efforts to have the ACA invalidated. In an open letter written to President Trump on the tenth anniversary of the ACA, the former vice president highlighted the ACA’s role as a safety net during the coronavirus pandemic and the potential impacts of dismantling it. Former Vice President Biden’s proposed health care plan includes public option programs that would preserve ACA marketplaces and increase subsidies for marketplace plans.
This work was supported in part by Well Being Trust. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
KFF analysis of Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) (2018). Accessed at: https://webappa.cdc.gov/sasweb/ncipc/mortrate.html↩︎
This refers to Health Professional Shortage Areas (HPSA), which are used to identify areas and population groups within the United States that are experiencing a shortage of health professionals. There are three categories of HPSA designation based on the health discipline that is experiencing a shortage: 1) primary medical; 2) dental; and 3) mental health. The primary factor used to determine a HPSA designation is the number of health professionals relative to the population with consideration of high need. Federal regulations stipulate that, in order to be considered as having a shortage of providers, an area must have a population-to-provider ratio of a certain threshold. For mental health, the population to provider ratio must be at least 30,000 to 1 (20,000 to 1 if there are unusually high needs in the community). More information is available here: https://data.hrsa.gov/topics/health-workforce/shortage-areas↩︎
Every Friday we recap the past week in the coronavirus pandemic from our tracking, policy analysis, polling, and journalism.
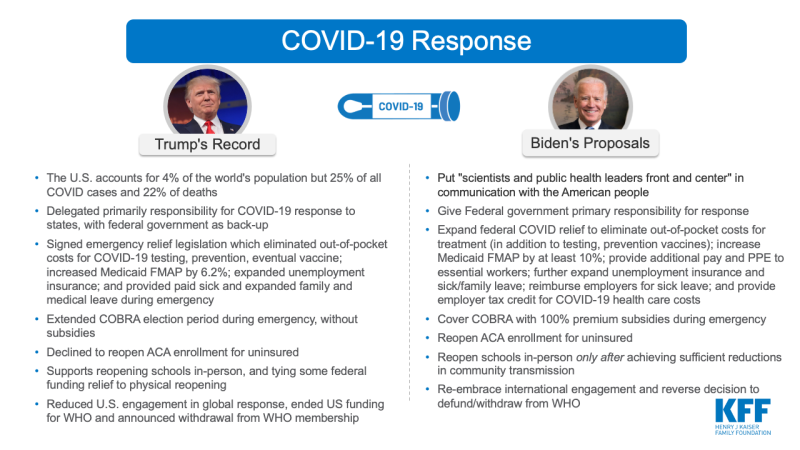
With the Democratic National Convention held this week and the Republican National Convention scheduled for next, the 2020 general election season is officially kicking off and brings an even greater focus on the country’s coronavirus pandemic response as a campaign issue. KFF’s survey research team wrote a Policy Watch post analyzing voters’ increasingly negative opinions of President Trump’s handling of the pandemic, with the caveat that the President continues to garner strong support among his base of Republican voters – even those living in areas disproportionately impacted by the virus.
KFF traditionally produces content on where the candidates stand on the key health policy issues facing the country. This election year is no different, but the global pandemic has overshadowed other key issues that may have had more attention. The new slideshow, Health Care and the 2020 Presidential Election, compares President Trump’s record and former Vice President Joe Biden’s proposals on several issues, including the slide below on the COVID-19 response.
Here are the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: Total cases worldwide surpassed 22 million this week – with an increase of approximately 1.8 million new confirmed cases in the past seven days. There were also approximately 43,500 new confirmed deaths worldwide, bringing the total to nearly 794,000 confirmed deaths.
U.S. Cases and Deaths: Total confirmed cases in the U.S. reached nearly 5.6 million this week. There was an approximate increase of 325,000 confirmed cases between August 14 and August 20. Over 7,000 confirmed deaths in the past week brought the total in the United States to over 174,000.
Race/Ethnicity Data: As of August 17, Black individuals made up a higher share of cases/deaths compared to their share of the population in 31 of 49 states reporting cases and 32 of 46 states reporting deaths. In 6 states (MI, MO, IL, WI, KS, and ME) the share of COVID-19 related deaths among Black people was at least two times higher than their share of the total population. Hispanic individuals made up a higher share of cases compared to their share of the total population in 36 of 46 states reporting cases. In 5 states (NE, WI, MN, NH and SD), Hispanic peoples’ share of cases was more than 3 times their share of the population. COVID-19 continues to have a sharp, disproportionate impact on American Indian/Alaska Native as well as Asian people in some states.
Face Mask Requirements– Enhanced requirements: CT, GA, MS• Social Distancing Measures– Extended: GA, HI, FL, MS, NV– Paused: No states– Rolled back: NY– New restrictions: IL, OR
The Affordable Care Act’s preventive care provisions eliminated out-of-pockets costs for contraception for many insured women, but some are still paying these out-of-pocket costs.
In an article for Contraception: X, KFF’s Brittni Frederiksen, Matthew Rae, and Alina Salganicoff examine large employer plans to identify which types and brands of oral contraceptive pills have the largest shares of oral contraceptive users with out-of-pocket spending and which oral contraceptives have the highest average annual out-of-pocket costs.
The authors found 10% of oral contraceptive users in large employer plans still had out-of-pocket costs in 2018.
Brand name oral contraceptives with generic alternatives had the largest share of users with annual out-of-pocket spending and the three drugs with highest average annual out-of-pocket spending were brand names without generic alternatives.
President Trump and Democratic nominee Joe Biden hold widely divergent views on health issues, with the president’s record and response to the coronavirus pandemic likely to play a central role in November’s elections.
A new KFF side-by-side comparison examines President Trump’s record and former Vice President Biden’s positions across a wide range of key health issues, including the response to the pandemic, the Affordable Care Act marketplace, Medicaid, Medicare, drug prices, reproductive health, HIV, mental health and opioids, immigration and health coverage, and health costs.
The resource provides a concise overview of the candidates’ positions on a range of health policy issues. While the Biden campaign has put forward many specific proposals, the Trump campaign has offered few new proposals for addressing health care in a second term and is instead running on his record in office.
It is part of KFF’s ongoing efforts to provide useful information related to the health policy issues relevant for the 2020 elections, including policy analysis, polling, and journalism. Find more on our Election 2020 resource page.
Analysis Finds 14 Million Medicare Part D and Large Employer Plan Enrollees Used Mail-Order Pharmacies Pre-Pandemic, Top Drugs Filled Were to Treat Chronic Conditions
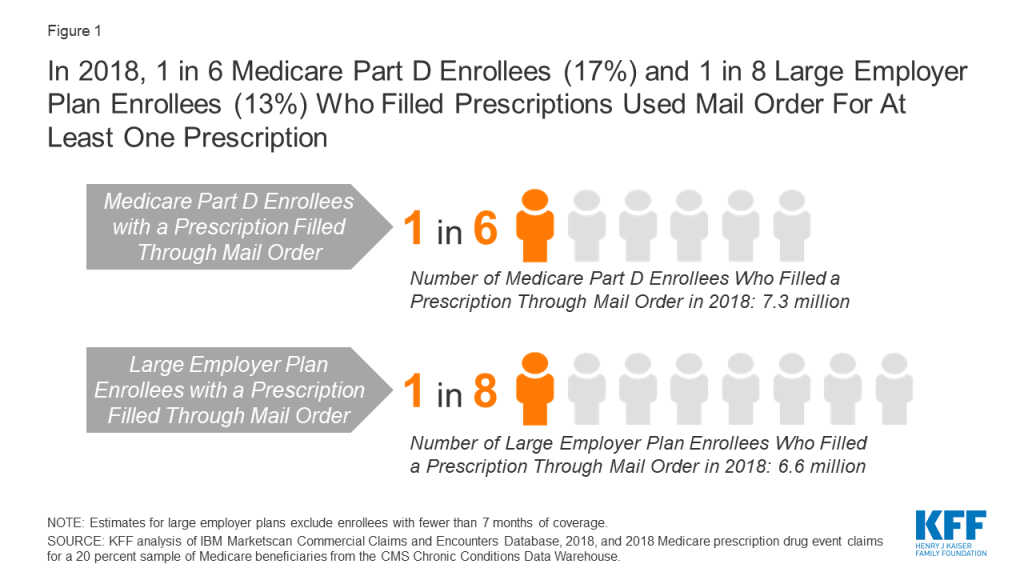
With questions being raised about potential delays in U.S. Postal Service delivery, a new KFF data note estimates 14 million enrollees in Medicare Part D and large employer plans relied on mail-order pharmacies for at least one prescription in 2018, with a total of over 170 million prescriptions fulfilled.
The use of mail-order pharmacies has been rising in recent years as patients have often been incentivized or mandated to use mail service for convenience and potential cost savings. This year’s COVID-19 pandemic has further boosted the use of mail-order pharmacies as government officials imposed stay-at-home orders and people stocked up on prescriptions.
The analysis finds that drugs for cardiovascular conditions made up half of the top ten drugs fulfilled by mail order for both Medicare Part D and large employer plan enrollees. More generally, drugs to treat chronic physical conditions and depression were among the most filled mail order prescriptions in both types of markets analyzed. Among large employer enrollees, 10% of all oral contraceptive prescriptions were filled via mail-order pharmacy, placing them in the top ten.
In July, the new Postmaster General instituted changes in the operation of the U.S. Postal Service that could result in delays in mail delivery. More recently, the post office has suspended these changes until after the November election. Prior to the announcement that he was postponing these changes, the Postmaster General had warned states of the possibility that mail-in ballots requested close to state deadlines would not be received in time to be counted in November’s election. Changes to the Postal Service’s delivery standards have potential implications that extend beyond those for the election.
Potential mail service delays could also be a concern for people who receive prescription drugs from mail-order pharmacies. In 2019, sales of mail-order prescriptions in the U.S. totaled nearly $145 billion (excluding rebates), with residents of some states more likely than others to use mail-order pharmacies. Mail service delays could affect a relatively large number of people in the midst of the COVID-19 pandemic. Data from the first seven months of 2020 shows that use of mail order increased by up to 20% over 2019 levels in the early weeks of the pandemic as patients stocked up on prescriptions and avoided retail settings, but as of late July, mail-order use is up only slightly compared to the same period last year. Getting prescriptions through mail-order pharmacies can offer convenience and cost savings to patients. Many large group plan enrollees choose to fill prescriptions at reduced cost through the mail, while others are only able to fill scripts at a mail-order pharmacy.
To understand who may be most affected by delays in the delivery of prescription drugs, we analyzed use of mail order in Medicare Part D and large group employer plans, and identified the therapeutic classes and specific drugs with the highest volume of fills by mail-order pharmacies in each market.
Based on 2018 data that predates the pandemic, 17% of Medicare Part D beneficiaries (7.3 million) and 13% of large employer plan enrollees (6.6 million) with prescription use had at least one prescription delivered from a mail-order pharmacy (Figure 1). Of the 157 million people who had employer coverage in 2018, 82 million were covered by an employer with 1,000 or more employees. In total, Medicare Part D beneficiaries and enrollees in large group employer plans filled 8% and 9% of prescriptions by mail order, accounting for 115 million and 58 million prescription fills respectively (Table 1). These estimates do not take into account mail-order use by people with other sources of coverage, including Medicaid, Marketplace plans, small-group enrollees, or the Veterans Administration.
Figure 1: In 2018, 1 in 6 Medicare Part D Enrollees (17%) and 1 in 8 Large Employer Plan Enrollees (13%) Who Filled Prescriptions Used Mail Order For At Least One Prescription
Across both Medicare Part D and large group employer plans, cardiovascular agents made up five of the top 10 therapeutic classes in terms of mail-order prescription fills in 2018 (Table 1). In each population, antihyperlipidemic drugs to aid in lowering cholesterol had the largest number of prescriptions filled by a mail-order pharmacy. Among Medicare Part D beneficiaries, 14% of antihyperlipidemic drugs were filled by mail (16.5 million prescriptions), while 20% of drugs in this class were filled by mail by large employer plan enrollees (6.7 million prescriptions).
Among large employer enrollees, oral contraceptives were among the top 10 therapeutic classes with prescriptions filled by mail order. In 2018, 10% percent of oral contraceptive prescriptions (2.4 million) filled by enrollees in a large group plan were filled by a mail-order pharmacy. Other classes that rank in the top 10 for mail-order prescriptions include certain diabetes medications, with 15% of prescriptions (2.5 million) for large employer enrollees and 11% of prescriptions (4.7 million) for Medicare Part D enrollees filled by mail order in 2018, and antidepressants, with 10% of prescriptions (5.7 million) for large employer enrollees and 7% of prescriptions (6.5 million) for Medicare Part D enrollees filled by mail order in 2018.
The top 10 drugs by volume of prescriptions filled by mail order in 2018 were the same for Medicare Part D and large employer plans, though the rankings vary slightly, and include several medications to treat high cholesterol and hypertension (Table 2). Among Medicare Part D enrollees, atorvastatin, which is used to treat high cholesterol, had the highest volume of mail-order fills (6.6 million, or 13% of all prescriptions for this product in 2018); among enrollees in large employer plans, levothyroxine sodium, which treats hypothyroidism, had the highest volume of mail-order fills (3.1 million, 16%).
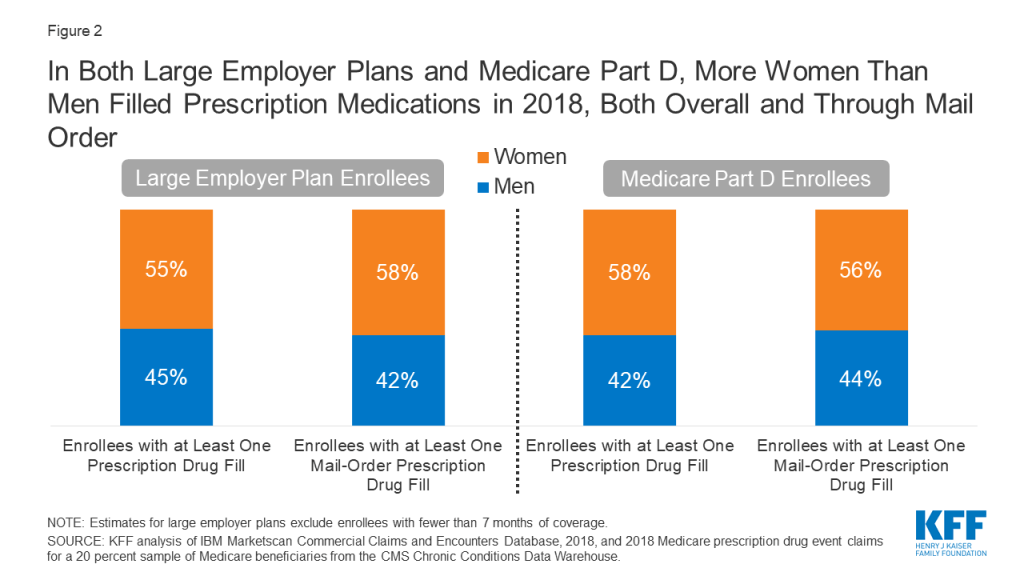
More women than men in both large employer plans and Medicare Part D filled prescription drugs and received at least one mail-order prescription drug in 2018 (Figure 2). Stratifying by age among individuals in large employer plans, among reproductive age individuals (ages 15 to 43) in large employer plans, a higher share of women than men had at least one mail-order prescription drug claim (11% for women in this age group versus 7% for men), which is partially driven by mail-order use for contraception. There were no differences by gender in the percentage of those who have at least one mail-order prescription among children ages 0-14 or individuals ages 44 to 64 (3% and 22% respectively).
Figure 2: In Both Large Employer Plans and Medicare Part D, More Women Than Men Filled Prescription Medications in 2018, Both Overall and Through Mail Order
Drugs used to treat chronic conditions, including hypothyroidism, high cholesterol, hypertension, and type 2 diabetes, are among the prescriptions most commonly filled by mail order for Medicare Part D enrollees and large employer plan enrollees, whether measured by therapeutic class or product. Therefore, delays in delivery due to changes to the operations of the U.S. Postal Service could lead to negative health consequences if it compromises patients’ ability to adhere to their medication regimens.
Tables
Table 1: Top 10 Therapeutic Classes Filled by Mail Order in Medicare Part D and Large Employer Plans,by Volume of Prescriptions, 2018
Therapeutic class
Therapeutic group
Number of prescriptions filled by mail order
Number of enrollees with mail-order prescription
Among all prescriptions filled within therapeutic class, share filled by mail order
Medicare Part D
TOTAL, all classes
114,888,200
7,293,635
7.8%
Antihyperlipidemic Drugs, NEC
Cardiovascular Agents
16,517,565
4,449,520
14.1%
Cardiac, Beta Blockers
Cardiovascular Agents
8,923,545
2,552,120
11.6%
Cardiac, ACE Inhibitors
Cardiovascular Agents
6,934,975
1,974,120
12.8%
Psychotherapeutics, Antidepressants
Central Nervous System
6,534,395
1,659,345
6.9%
Cardiac, Calcium Channel
Cardiovascular Agents
6,453,380
1,873,325
11.3%
Cardiac Drugs, NEC
Cardiovascular Agents
6,021,195
1,717,620
13.2%
Thyroit/Antithyroid, Thyroid/Hormones
Hormones & Synthetic Substitutes
5,803,410
1,561,605
12.4%
Gastrointestinal Drug Misc, NEC
Gastrointestinal Drugs
5,642,420
1,700,580
9.7%
Antidiabetic Agents, Misc
Hormones & Synthetic Substitutes
4,693,630
1,280,355
10.8%
Misc Therapeutic Agents, NEC*
Misc Therapeutic Agents
2,984,960
741,870
11.7%
Large Employer Plans
TOTAL, all classes
58,076,511
6,552,568
9.1%
Antihyperlipidemic Drugs, NEC
Cardiovascular Agents
6,743,934
1,807,415
20.1%
Psychotherapeutics, Antidepressants
Central Nervous System
5,723,719
1,466,376
10.3%
Thyroid/Antithyroid, Thyroid Hormones
Hormones & Synthetic Substitutes
3,409,575
897,768
15.9%
Cardiac, ACE Inhibitors
Cardiovascular Agents
3,185,892
922,549
15.6%
Cardiac, Beta Blockers
Cardiovascular Agents
2,680,792
780,268
15.5%
Cardiac Drugs. NEC
Cardiovascular Agents
2,574,019
747,708
16.1%
Antidiabetic Agents, Misc
Hormones & Synthetic Substitutes
2,512,233
665,014
15.0%
Contraceptive, Oral Comb, NEC
Hormones & Synthetic Substitutes
2,411,000
683,445
10.3%
Gastrointestinal Drugs Misc, NEC
Gastrointestinal Drugs
2,335,366
711,485
13.1%
Cardiac, Calcium Channel
Cardiovascular Agents
2,043,871
604,578
14.5%
NOTE: NEC is not elsewhere classified. Estimates for large employer plans exclude enrollees with fewer than 7 months of coverage. *Less than 1% of prescriptions in the “Misc Therapeutic Agents, NEC” class are categorized in the “Respiratory Tract Agents” therapeutic group.SOURCE: KFF analysis of IBM Marketscan Commercial Claims and Encounters Database, 2018, and 2018 Medicare prescription drug event claims for a 20 percent sample of Medicare beneficiaries from the CMS Chronic Conditions Data Warehouse.
Table 2: Top 10 Drug Products Filled by Mail Order in Medicare Part D and Large Employer Plans, by Volume of Prescriptions, 2018
Drug product
Number of prescriptions filled by mail order
Number of enrollees with mail-order prescription
Among all prescriptions filled for drug product, share filled by mail order
Indication
Common brand names
Medicare Part D
Atorvastatin calcium
6,636,765
1,967,555
13.0%
high cholesterol
Lipitor
Levothyroxine sodium
5,698,630
1,548,500
12.5%
hypothyroidism
Levothroid, Levoxyl, Synthroid, Unithroid
Amlodipine besylate
4,581,675
1,350,760
11.2%
hypertension
Katerzia, Norvasc
Lisinopril
4,353,865
1,265,540
11.7%
hypertension
Prinivil, Zestril
Simvastatin
3,776,125
1,089,485
16.1%
high cholesterol
Zocor
Metformin HCL
3,696,385
1,104,535
12.2%
type 2 diabetes
Glucophage
Omeprazole
3,264,810
1,004,740
11.3%
acid reflux, ulcers, heart burn
Prilosec
Losartan potassium
3,120,395
949,995
12.6%
hypertension
Cozaar
Metoprolol succinate
2,992,240
880,120
12.8%
hypertension, angina, heart failure
Kapspargo Sprinkle, Toprol XL
Hydrochlorothiazide
2,288,360
690,805
13.4%
hypertension
Microzide
Large Employer Plans
Levothyroxine sodium
3,072,413
837,581
16.3%
hypothyroidism
Levothroid, Levoxyl, Synthroid, Unithroid
Atorvastatin calcium
2,858,703
864,833
18.9%
high cholesterol
Lipitor
Lisinopril
2,067,537
608,625
15.2%
hypertension
Prinivil, Zestril
Metformin HCL
1,762,022
544,089
15.5%
type 2 diabetes
Glucophage
Amlodipine besylate
1,349,224
407,717
13.6%
hypertension
Katerzia, Norvasc
Simvastatin
1,196,826
348,014
23.1%
high cholesterol
Zocor
Losartan potassium
1,117,641
348,870
15.3%
hypertension
Cozaar
Omeprazole
1,077,168
339,343
13.4%
acid reflux, ulcers, heart burn
Prilosec
Metoprolol succinate
965,373
281,249
16.2%
hypertension, angina, heart failure
Kapspargo Sprinkle, Toprol XL
Hydrochlorothiazide
939,555
287,646
14.6%
hypertension
Microzide
NOTE: Estimates for large employer plans exclude enrollees with fewer than 7 months of coverage. Includes all prescriptions for products containing the specified generic name. Does not reflect combination products that include the active ingredient. Each of the top 10 drugs are available generically. The “common brand names” field is provided as an example of branded versions, though these do not account for all of the mail-order fills for any of these top 10 drug products.SOURCE: KFF analysis of IBM Marketscan Commercial Claims and Encounters Database, 2018, and 2018 Medicare prescription drug event claims for a 20 percent sample of Medicare beneficiaries from the CMS Chronic Conditions Data Warehouse.
Methods
For the analysis of large employer plans, we analyzed a sample of medical claims obtained from the 2018 IBM Health Analytics MarketScan Commercial Claims and Encounters Database, which contains claims information provided by large employer plans. We only included claims for people under the age of 65, as people over the age of 65 are typically on Medicare. This analysis used claims for almost 18 million people representing about 22% of the 82 million people in the large group market in 2018. Seventy percent of larger group enrollees who were enrolled for more than six months had at least one prescription drug claim in the year. Weights were applied to match counts in the Current Population Survey for enrollees at firms of 1,000 or more workers by sex, age and state. Weights were trimmed at eight times the interquartile range.
For the analysis of Medicare Part D, we used the 2018 Medicare Part D prescription drug event (PDE) claims data from the Centers for Medicare & Medicaid Services (CMS) Chronic Conditions Data Warehouse (CCW) for a 20 percent sample of Medicare beneficiaries. The analysis was limited to enrollees who filled a prescription in 2018, which equaled 42.9 million enrollees out of 46.1 million total (93.1%).
For both datasets, MarketScan’s Red Book was used to classify drugs by generic id and the therapeutic/pharmacologic category of the drug product. Drug spending paid for by someone other than an enrollee’s insurer, drugs administered in an inpatient setting, or not classified under the controlled substance act were excluded. Each prescription drug claim was counted as a single prescription regardless of the quantity or strength of that prescription. Drugs were grouped by the generic drug name, which may include multiple brands, but treats combination products separately.
To identify prescriptions filled by a mail-order pharmacy, we used the field indicating the type of pharmacy that filled the prescription. It is not possible to determine the method by which the prescription was subsequently mailed, and thus the totals here reflect prescriptions delivered via the U.S. Postal Service, as well as those delivered by other services, such as FedEx or UPS. In the Part D claims, specialty pharmacy claims are reported separately from mail-order pharmacy claims, although in some cases, specialty pharmacies may ship directly to patients; our analysis does not count these prescriptions as mail order because we are unable to identify them as such.