KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
The Build Back Better Act, originally introduced in Congress on September 27, 2021, is a broad funding and programmatic package supported by President Biden. The bill, as first introduced by the House, was estimated to total $3.5 trillion. A more recent version now under consideration in the House is estimated to total significantly less, at $1.75 trillion, due to pressures to reduce the bill’s cost.
Among the provisions in the bill are several designed to strengthen the public health infrastructure, including the workforce, and to support pandemic preparedness. While the original version of the bill provided $51.8 billion for these purposes (with $36 billion directed toward improving the public health infrastructure and $15.8 billion toward pandemic preparedness), the new version of the bill provides 63% less, or $19.2 billion, including $16.2 billion for public health infrastructure and $3 billion for pandemic preparedness. Almost all public health and preparedness areas in the original bill saw reductions, and several were eliminated.
The following table identifies the provisions of the bill related to public health infrastructure and pandemic preparedness, their specific funding amounts, and activities supported.1 Unless otherwise specified, all funding would be made available until expended, and, if ultimately enacted, would build on funding provided in previous emergency spending bills passed by Congress to respond to the COVID-19 pandemic.
Area/Provision
Amount
Activities
HEALTH CARE INFRASTRUCTURE AND WORKFORCE
$16,160,000,000
SEC. 31001. FUNDING TO SUPPORT CORE PUBLIC HEALTH INFRASTRUCTURE FOR STATE, TERRITORIAL, LOCAL, AND TRIBAL HEALTH DEPARTMENTS AT THE CENTERS FOR DISEASE CONTROL AND PREVENTION
$7,000,000,000 (provided between 2022-2026)
Funding to support core public health infrastructure activities to strengthen the public health system and expand and improve activities of the Centers for Disease Control and Prevention (CDC). Activities include: health equity activities; workforce capacity and competency; all hazards public health and preparedness; testing capacity, including test platforms, mobile testing units, and personnel; health information, health information systems, and health information analysis (including data analytics); epidemiology and disease surveillance; contact tracing; policy and communications; financing; community partnership development; and relevant components of organizational capacity.
Funding Allocation: To support core public health infrastructure activities throughout the U.S.
Population-Based Grants: $3,500,000,000 provided to each State or territorial health department, and to local health departments that serve counties with a population of at least 2,000,000 or cities with a population of at least 400,000 people. Formula must consider population size and the Social Vulnerability Index.
Competitive Grants: $1,750,000,000 provided through competitive grants to State, territorial, local, or Tribal health departments.
NOTE: Of the grant funding provided to State health departments through formula and competitive awards, at least 25% must be reallocated to local health departments.
CDC: $1,750,000,000 to expand and improve core public health infrastructure and activities at the CDC.
SEC. 31002. FUNDING FOR HEALTH CENTER CAPITAL GRANTS
$2,000,000,000
Funding to be awarded through grants and cooperative agreements to support community health centers for capital improvement projects.
SEC. 31003. FUNDING FOR TEACHING HEALTH CENTER GRADUATE MEDICAL EDUCATION
$3,370,000,000
Funding for direct payments and awards to support the establishment of new as well as the maintenance and expansion of existing graduate medical residency training programs.
SEC. 31004. FUNDING FOR CHILDREN’S HOSPITALS THAT OPERATE GRADUATE MEDICAL EDUCATION PROGRAMS
$200,000,000
Funding to support children’s hospitals that operate graduate medical education programs.
SEC. 31005. FUNDING FOR NATIONAL HEALTH SERVICE CORPS
$2,000,000,000
Funding to support the National Health Service Corps.
SEC. 31006. FUNDING FOR THE NURSE CORPS
$500,000,000
Funding to support the Nurse Corps.
SEC. 31007. FUNDING FOR SCHOOLS OF MEDICINE IN UNDERSERVED AREAS
$500,000,000
Funding to be awarded to support the establishment, improvement, or expansion of an allopathic or osteopathic school of medicine, with priority given to minority-serving institutions, and taking into consideration equitable distribution of awards among the geographical regions of the United States (including rural populations) in order to reach disadvantaged, rural, underserved, underrepresented, and low-income individuals.
Among other things, supported activities include: recruiting, enrolling, and retaining students; curricula development, implementation, expansion, and modernization; facilities construction, modernization, or expansion; accreditation; and the hiring of faculty and staff.
SEC. 31008. FUNDING FOR SCHOOLS OF NURSING IN UNDERSERVED AREAS
$500,000,000
Funding to be awarded to support schools of nursing to enhance and modernize nursing education programs and increase the number of faculty and students at such schools, taking into consideration equitable distribution of awards among the geographical regions of the United States, the capacity of a school of nursing to provide care in underserved areas, and with priority to reach disadvantaged, rural, underserved, underrepresented, and low-income individuals.
Among other things, supported activities include: recruiting, enrolling, and retaining students; creating, modernizing, enhancing, or expanding curricula and programs; hiring and retention of faculty; modernizing school infrastructure; and establishing partnerships with healthcare providers as well as interdisciplinary programs to further educational opportunities.
SEC. 31009. FUNDING FOR PALLIATIVE CARE AND HOSPICE EDUCATION AND TRAINING
$25,000,000
Funding to be awarded through grants and contracts to support the training of health professionals in palliative and hospice care as well as foster patient and family engagement, integration of palliative and hospice care with primary care and other appropriate specialties, and collaboration with community partners to address gaps in health care for individuals in need of palliative or hospice care with priority given to rural, medically underserved populations and communities, Indian Tribes or Tribal Organizations, or Urban Indian organizations.
SEC. 31010. FUNDING FOR PALLIATIVE MEDICINE PHYSICIAN TRAINING
$20,000,000
Funding to be awarded through grants and contracts to accredited schools of medicine, schools of osteopathic medicine, teaching hospitals, and graduate medical education programs for the purpose of providing support for projects that fund the training of physicians or specialists who plan to teach or practice palliative medicine.
SEC. 31011. FUNDING FOR PALLIATIVE CARE AND HOSPICE ACADEMIC CAREER AWARDS
$20,000,000
Funding to be awarded to accredited schools of medicine, osteopathic medicine, nursing, social work, psychology, allied health, dentistry, or chaplaincy applying on behalf of board-certified or board-eligible individuals to promote the academic career development as hospice and palliative care specialists.
SEC. 31012. FUNDING FOR HOSPICE AND PALLIATIVE NURSING
$20,000,000
Funding to be awarded as grants and contracts to accredited schools of nursing, health care facilities, programs leading to certification as a certified nurse assistant, or partnerships of such schools and facilities to develop and implement programs and initiatives to train and educate individuals in providing interprofessional, interdisciplinary, team-based palliative care in health-related educational, hospital, hospice, home, or long-term care settings.
SEC. 31013. FUNDING FOR DISSEMINATION OF PALLIATIVE CARE INFORMATION
$5,000,000
Funding to be provided through the award of grants or contracts to public and nonprofit private entities to disseminate information to inform patients, families, caregivers, direct care workers, and health professionals about the benefits of palliative care throughout the continuum of care for patients with serious or life-threatening illness.
PANDEMIC PREPAREDNESS
$3,000,000,000
SEC. 31021. FUNDING FOR LABORATORY ACTIVITIES AT THE CENTERS FOR DISEASE CONTROL AND PREVENTION
$1,400,000,000
Acting through the Director of the Centers for Disease Control and Prevention, funding shall be used to renovate, improve, expand, and modernize State and local public health laboratory infrastructure as well as CDC laboratories. Activities supported include improving and enhancing: testing and response capacity; the Laboratory Response Network for rapid outbreak detection; genomic sequencing capabilities to detect emerging diseases and variant strains; and biosafety and biosecurity capacity.
Funding may also be used to enhance the ability of the Centers for Disease Control and Prevention to monitor and exercise oversight over biosafety and biosecurity of State and local public health laboratories.
SEC. 31022. FUNDING FOR PUBLIC HEALTH AND PREPAREDNESS RESEARCH, DEVELOPMENT, AND COUNTERMEASURE CAPACITY
$1,300,000,000
Acting through the Assistant Secretary for Preparedness and Response Activities, funding shall be used to support:
Surge capacity, including through construction, expansion, or modernization of facilities, to respond to a public health emergency, for procurement and domestic manufacture of drugs, active pharmaceutical ingredients, vaccines and other biological products, diagnostic technologies and products, personal protective equipment, medical devices, vials, syringes, needles, and other components or supplies for the Strategic National Stockpile
Expanded global and domestic vaccine production capacity, including by developing or acquiring new technology and expanding manufacturing capacity through construction, expansion, or modernization of facilities
Activities to mitigate supply chain risks and enhance supply chain elasticity and resilience for critical drugs, active pharmaceutical ingredients, and supplies (including essential medicines, medical countermeasures, and supplies in shortage or at risk of shortage), drug and vaccine raw materials, and other supplies through the construction, expansion, or modernization of facilities, adoption of advanced manufacturing processes, and other activities to support domestic manufacturing of such supplies
Activities conducted by the Biomedical Advanced Research and Development Authority for advanced research, standards development, and domestic manufacturing capacity for drugs, including essential medicines, diagnostics, vaccines, therapeutics, and personal protective equipment
Increased biosafety and biosecurity in research on infectious diseases, including by modernization or improvement of facilities.
SEC. 31023. FUNDING FOR INFRASTRUCTURE MODERNIZATION AND INNOVATION AT THE FOOD AND DRUG ADMINISTRATION
$300,000,000
Funding provided to improve and modernize infrastructure at the Food and Drug Administration and to enhance food and medical product safety as follows:
$150,000,000 for improving technological infrastructure, including through developing integrated systems, and improving the interoperability of information technology systems.
$150,000,000 for modernizing laboratory infrastructure of, or used by, the Food and Drug Administration, including modernization of facilities related to, and supporting, such laboratory infrastructure, including through planning for, and the construction, repair, improvement, extension, alteration, demolition, and purchase of, fixed equipment or facilities.
Only funding amounts listed under “Subtitle I – Public Health” in the “Build Back Better Act” (H.R. 5376) are included. Funding that may support public health activities provided under other subtitles is not included. ↩︎
COVID-19 Misinformation is Ubiquitous: 78% of the Public Believes or is Unsure About At Least One False Statement, and Nearly a Third Believe At Least Four of Eight False Statements Tested
Belief in Misinformation Much More Common among Unvaccinated Adults and Republicans
Most People Who Trust Network and Local Television, CNN, MSNBC and NPR on COVID-19 Believe Little or No Misinformation; Larger Shares Who Trust Newsmax, One American News, and Fox News Hold Many Misconceptions
More than three quarters (78%) of U.S. adults either believe or aren’t sure about at least one of eight false statements about the COVID-19 pandemic or COVID-19 vaccines, with unvaccinated adults and Republicans among those most likely to hold misconceptions, a new KFF COVID-19 Vaccine Monitor report shows.
Nearly two-thirds (64%) of unvaccinated adults believe or are unsure about at least half of the eight false statements – more than three times the share of vaccinated adults (19%). Nearly half (46%) of Republicans believe or are unsure about at least half the statements, three times the share of Democrats (14%).
The findings highlight a major challenge for efforts to accurately communicate the rapidly evolving science about the pandemic when false and ambiguous information can spread quickly, whether inadvertently or deliberately, through social media, polarized news sources and other outlets.
The new report assesses the public’s awareness of, and belief in, a range of “myths” about the disease and the vaccines to prevent it. The most common misconceptions include:
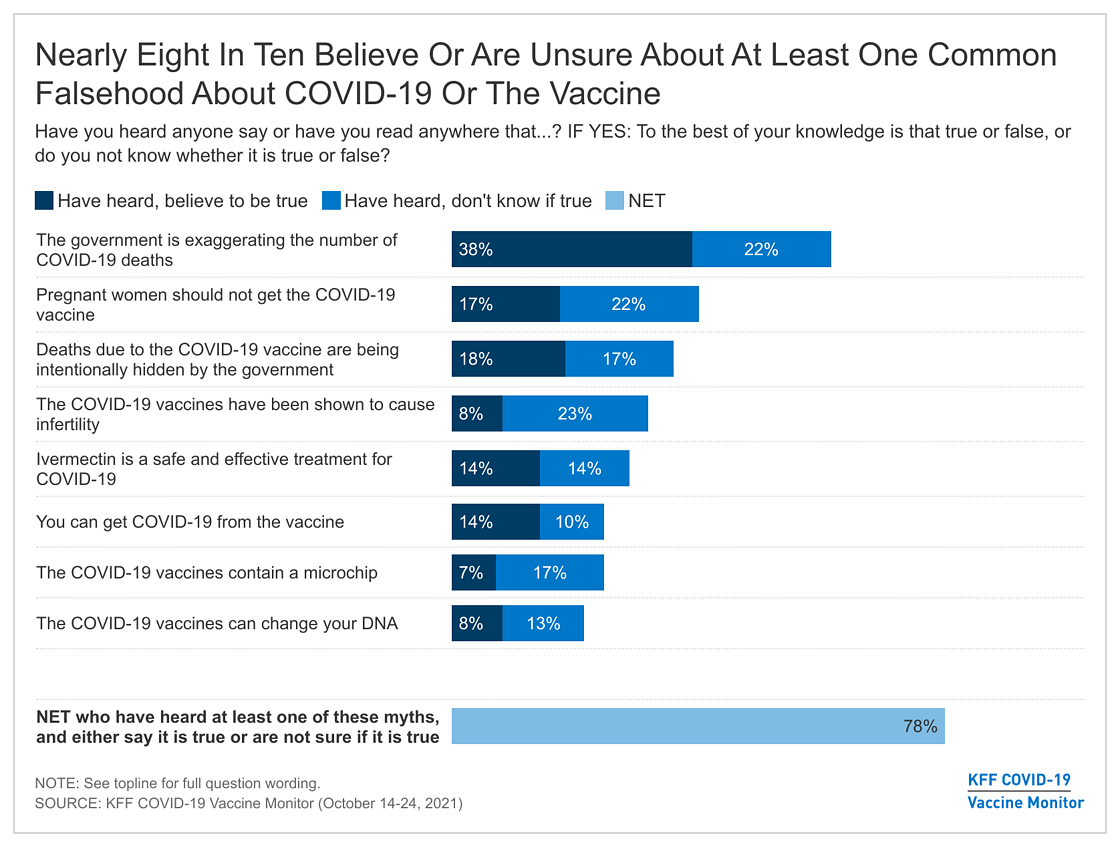
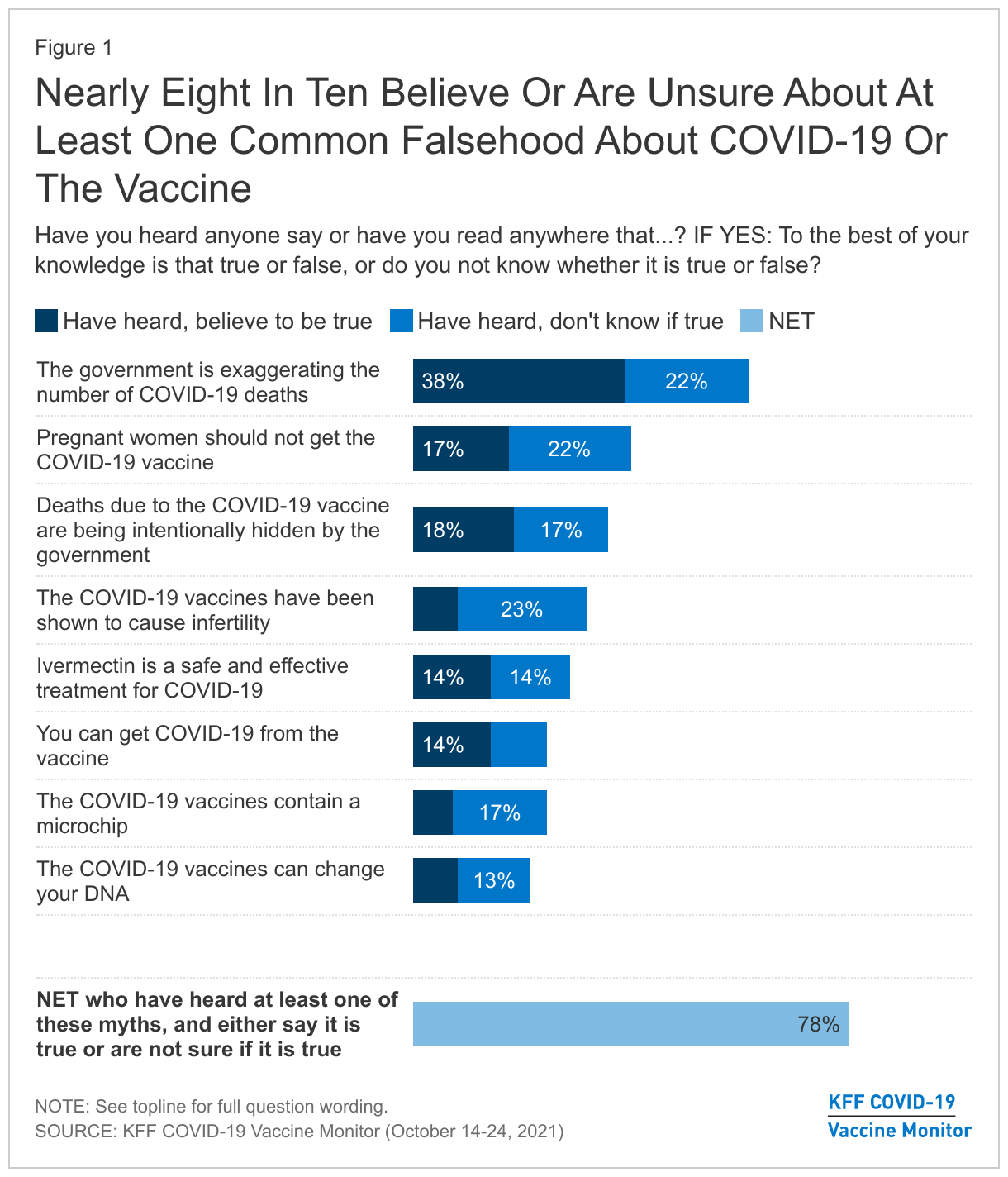
• Most (60%) adults say they’ve heard that the government is exaggerating the number of COVID-19 deaths by counting deaths due to other factors and either believe it to be true (38%) or aren’t sure if it is true or false (22%).
• Four in 10 (39%) say they’ve heard pregnant women should not get the COVID-19 vaccine and believe it to be true (17%) or aren’t sure (22%).
• Three in 10 (31%) say they’ve heard that the vaccine has been shown to cause infertility and either believe it (8%) or aren’t sure if it’s true (23%).
Many people believe or are unsure about several of the eight false statements, including about a third (32%) who believe or are unsure about at least half of them.
How Does Trust in News Sources Line Up with Misconceptions?
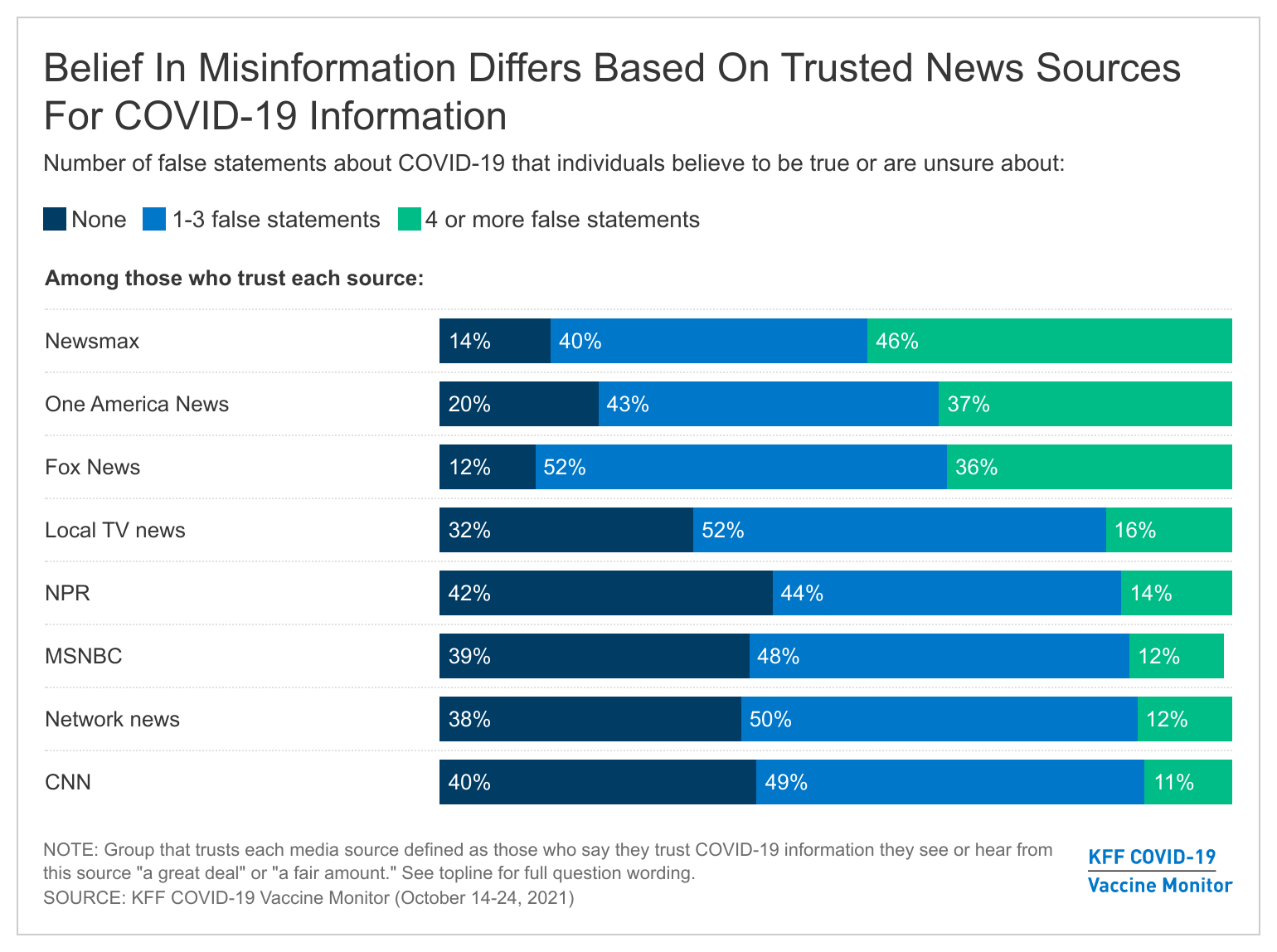
People’s trusted news sources are correlated with their belief in COVID-19 misinformation. At least a third of those who trust information from CNN, MSNBC, network news, NPR, and local television news do not believe any of the eight false statements, while small shares (between 11% and 16%) believe or are unsure about at least four of the eight false statements.
Larger shares of those who trust COVID-19 information from leading conservative news sources believe misinformation, with nearly 4 in 10 of those who trust Fox News (36%) and One America News (37%), and nearly half (46%) of those who trust Newsmax, saying they believe or are unsure about at least half of the eight false statements.
Whether this is because people are exposed to misinformation from those news sources, or whether the types of people who choose those news sources are the same ones who are pre-disposed to believe certain types of misinformation for other reasons, is beyond the scope of the analysis.
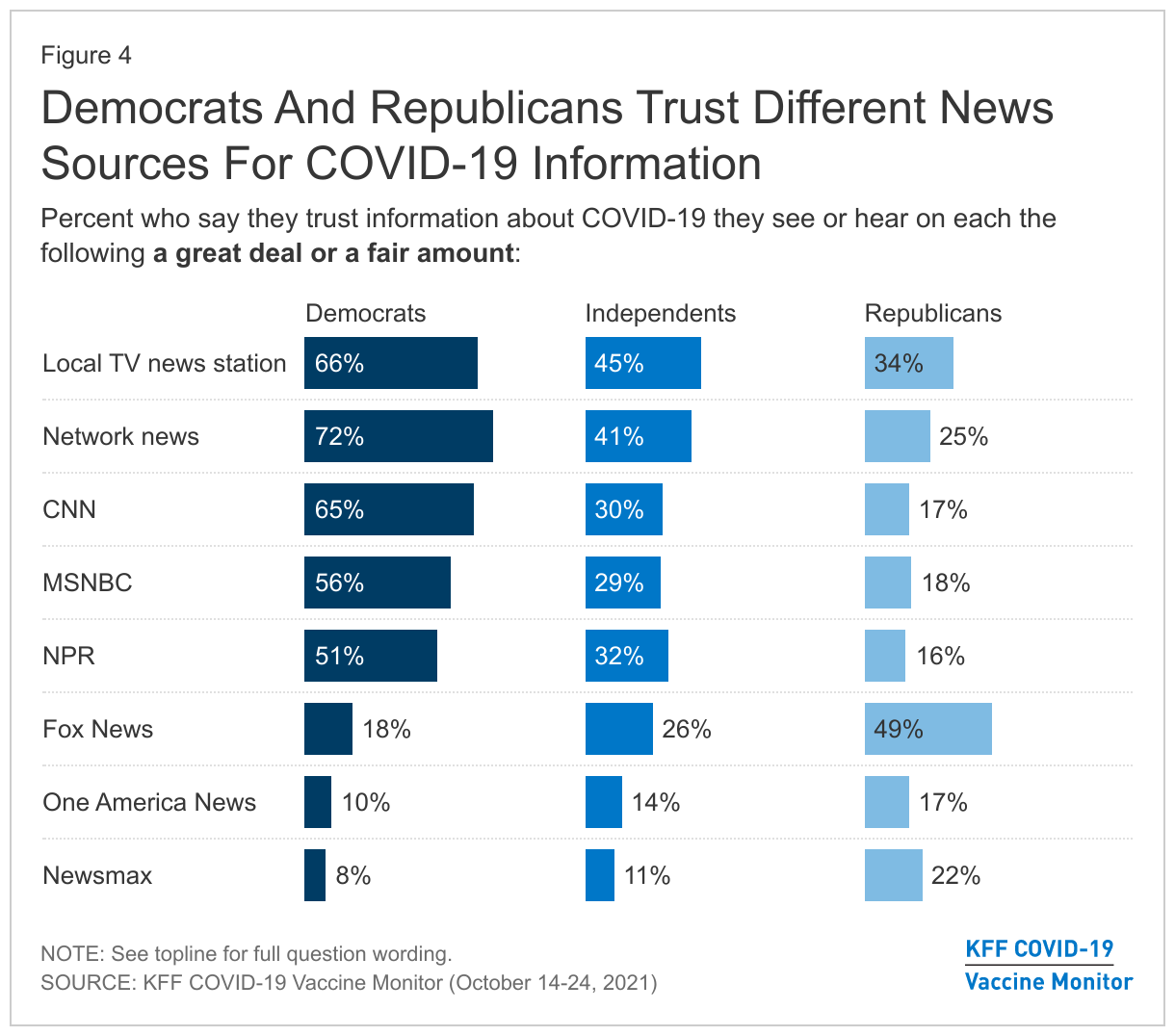
Underscoring the self-selection that now occurs in the news sources people trust, Democrats trust COVID-19 information from network (72%) and local (66%) television, CNN (65%), MSNBC (56%) and NPR (51%). Republicans’ most trusted news sources for COVID-19 information are Fox News (49%), local (34%) and network (25%) news, and Newsmax (22%).
Few adults say they trust social-media sources for information about COVID-19 such as YouTube (13%), Facebook (9%), Twitter (6%), and Instagram (5%). The group that is influenced by information they see on these platforms may be larger than the share that says they trust information they see there, as KFF surveys have previously found the share of adults who get information about COVID-19 vaccines from social media is nearly as large as the share who get information from cable, network, and local TV news.
Designed and analyzed by public opinion researchers at KFF, the KFF Vaccine Monitor survey was conducted from October 14-24 among a nationally representative random digit dial telephone sample of 1,519 adults. Interviews were conducted in English and Spanish by landline (168) and cell phone (1,351). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and acceptance, information needs, trusted messengers and messages, as well as the public’s experiences with vaccination.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and acceptance, information needs, trusted messengers and messages, as well as the public’s experiences with vaccination.
Key Findings
Misinformation about health care topics is nothing new, but social media, the polarization of news sources, and the pace of scientific development on COVID-19 have all contributed to an environment that makes it easier than ever for ambiguous information, misinterpretation, and deliberate disinformation to spread.1 We find in the latest Vaccine Monitor that belief in pandemic-related misinformation is widespread, with 78% of adults saying they have heard at least one of eight different false statements about COVID-19 and that they believe it to be true or are unsure if it is true or false. One-third (32%) of all adults believe or are uncertain about at least four false statements. Belief in COVID-19 misinformation is correlated with both vaccination status and partisanship, with unvaccinated adults and Republicans much more likely to believe or be unsure about false statements compared to vaccinated adults and Democrats.
With the public’s trust in news media declining over many years, we find that no news media source garners the trust of a majority of the public when it comes to COVID-19 information. While nearly half trust information about COVID-19 that they see on network and local television news, trust is lower for other news outlets and diverges in expected ways along partisan lines. Unvaccinated adults are far less likely than vaccinated adults to trust most of the news sources included in the survey for information on COVID-19, with the exception of conservative news sources.
People’s trusted news sources are correlated with their belief in COVID-19 misinformation. The share who hold at least four misconceptions is small (between 11-16%) among those who say they trust COVID-19 information from network news, local TV news, CNN, MSNBC, and NPR. This share rises to nearly four in ten among those who trust COVID-19 information from One America News (37%) and Fox News (36%), and to nearly half (46%) among those who trust information from Newsmax. One thing this study cannot disentangle is whether this is because people are exposed to misinformation from those news sources, or whether the types of people who choose those news sources are the same ones who are pre-disposed to believe certain types of misinformation for other reasons.
These findings suggest a challenge for reaching people with accurate information about COVID-19. While that challenge is particularly acute when it comes to reaching those who remain unvaccinated, the partisan divisions in misinformation and trusted news sources also have implications for those who are vaccinated, as we have reported a growing partisan divide in intention to get COVID-19 booster shots, even among the fully vaccinated.
Belief In COVID-19 Misinformation
Numerous studies have documented the prevalence of misinformation and disinformation about COVID-19, often fueled by social media2 . The latest KFF COVID-19 Vaccine Monitor sheds light on how common it is for people to hear and believe certain “myths” about the disease and the vaccine, and how these beliefs correlate with individuals’ trusted media sources.
Belief or uncertainty about COVID-19 misinformation is widespread, with nearly eight in ten adults saying they have heard at least one of eight different pieces of misinformation and either believe them to be true or are not sure whether they are true or false. Most commonly, six in ten adults have heard that the government is exaggerating the number of COVID-19 deaths by counting deaths due to other factors as coronavirus deaths and either believe this to be true (38%) or aren’t sure if it’s true or false (22%).3 About four in ten have heard that pregnant women should not get the COVID-19 vaccine and think this is true (17%) or aren’t sure (22%). Among women ages 18-44, 18% believe this to be true and 29% are uncertain.
Among other common myths, one-third believe or are unsure whether deaths due to the COVID-19 vaccine are being intentionally hidden by the government (35%), and about three in ten each believe or are unsure whether COVID-19 vaccines have been shown to cause infertility (31%) or whether Ivermectin is a safe and effective treatment for COVID-19 (28%). In addition, between a fifth and a quarter of the public believe or are unsure whether the vaccines can give you COVID-19 (25%), contain a microchip (24%), or can change your DNA (21%).
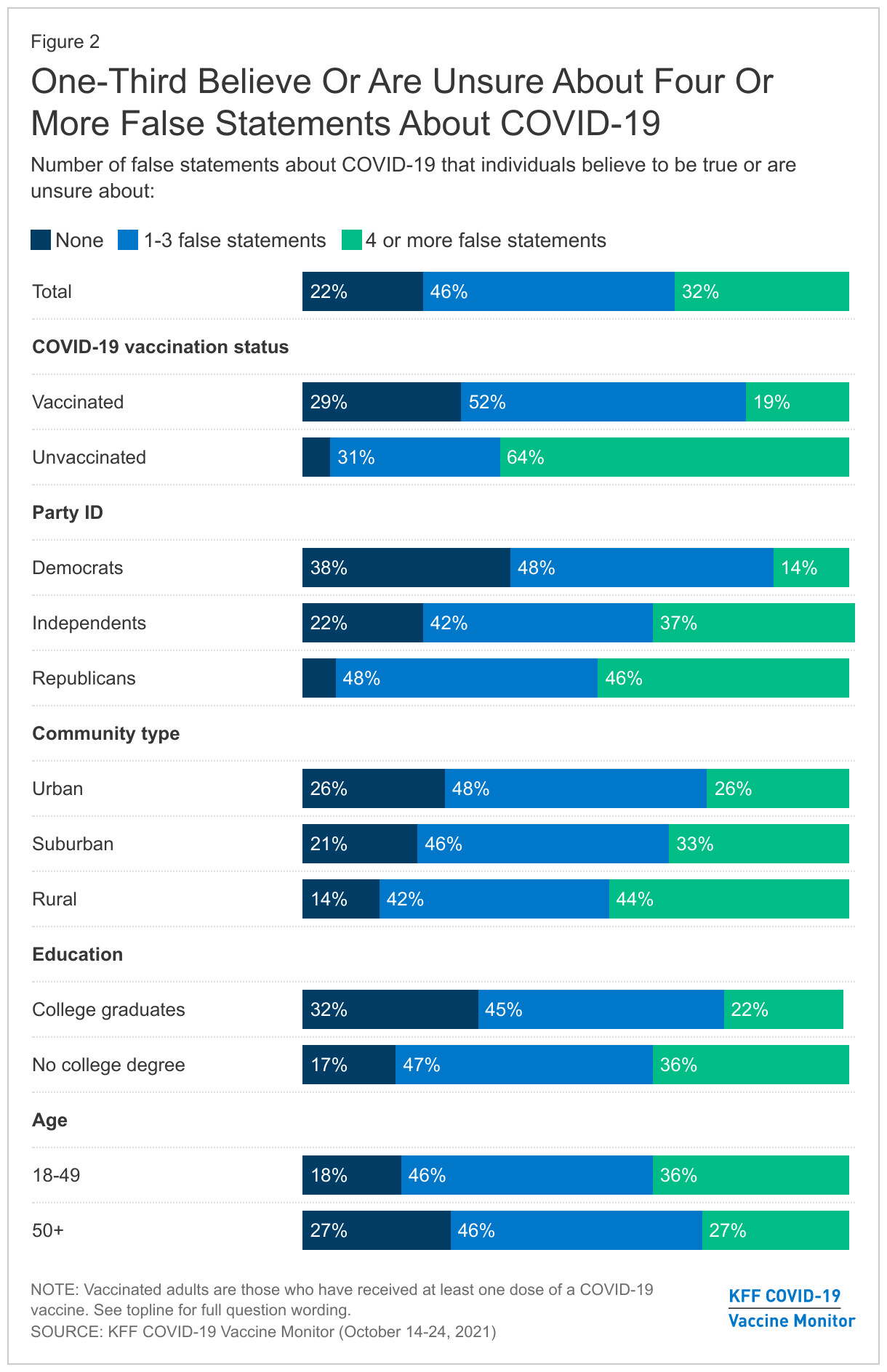
Overall, about one in five adults (22%) do not believe any of the eight pieces of information tested in the survey, while nearly half (46%) believe or are unsure about between one and three false statements. One-third of adults (32%) say they have heard at least four of these statements and believe them to be true or are uncertain if they’re true or false. There are notable differences in misinformation belief by vaccination status and partisan identity and smaller differences by community type and education level.
Among adults who have not gotten a COVID-19 vaccine, nearly two-thirds (64%) believe or are uncertain about four or more false statements about the virus. Among vaccinated adults, most believe or are unsure about at least one false statement, but just 19% say this about four or more statements. Unvaccinated adults are at least 20 percentage points more likely than vaccinated adults to lack knowledge about each piece of misinformation tested, with the largest gap on the statement that “Deaths due to the COVID-19 vaccine are being intentionally hidden by the government” (61% of unvaccinated adults believe or are unsure if this is true compared to 25% of vaccinated adults).
Nearly half (46%) of Republicans compared to just 14% of Democrats believe or are unsure about four or more misstatements about COVID-19. Strikingly, 84% of Republicans believe or are unsure whether the government is exaggerating the number of COVID-19 deaths by including deaths due to other causes, compared to just one third of Democrats. In addition, there are large gaps between Republicans and Democrats in the shares who believe or are unsure whether pregnant women should not get the vaccine (52% vs. 28%), whether the vaccines have been shown to cause infertility (43% vs. 15%), and whether Ivermectin is a safe and effective treatment for COVID-19 (44% vs. 10%).
In addition to these differences by partisanship and vaccination status, believing or having doubts about four or more pieces of COVID-19 misinformation is also more prevalent among rural residents compared to those living in urban and suburban areas, among those without a college degree compared to college graduates, and among those ages 18-49 compared to those ages 50 and over.
Trusted News Media Sources For COVID-19 Information
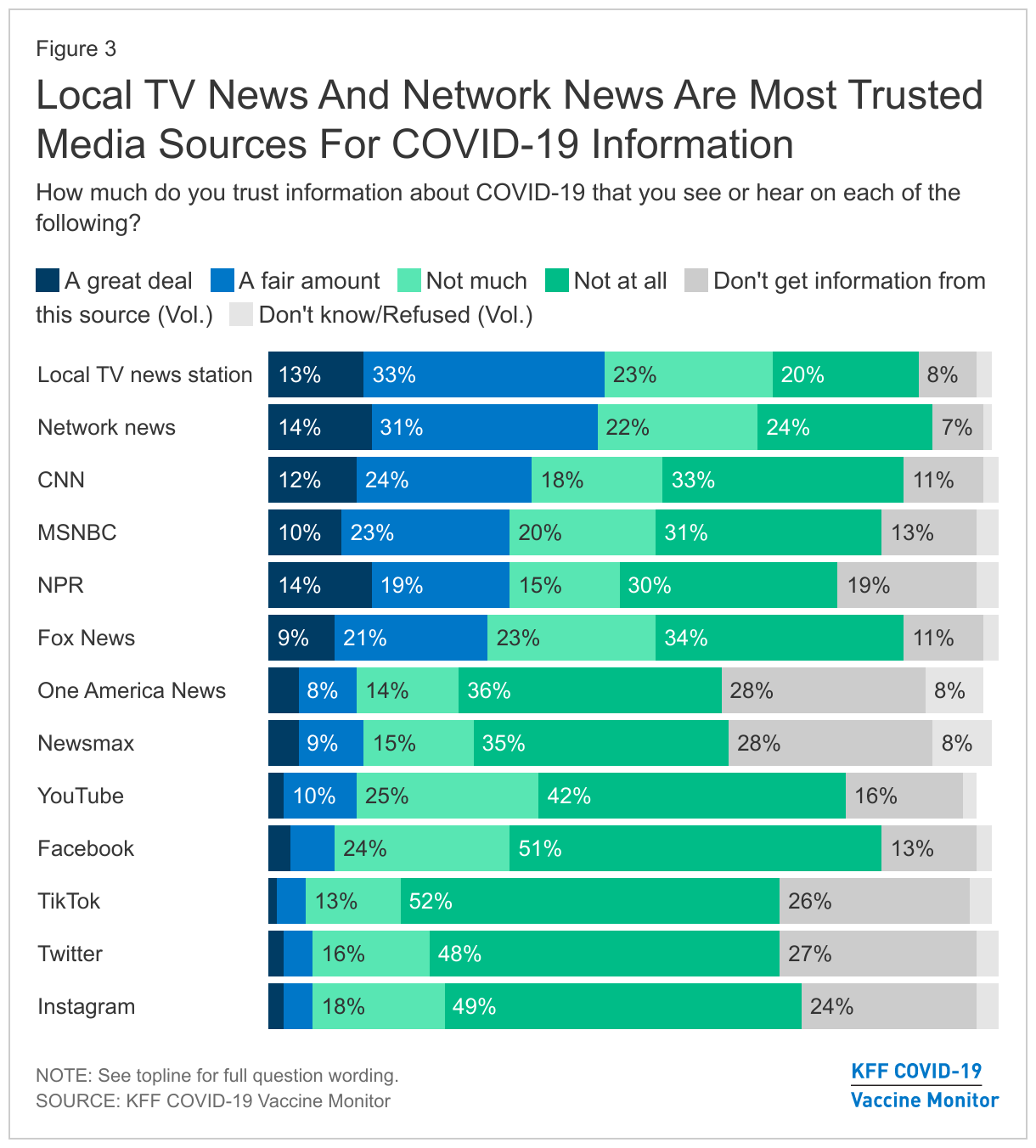
Overall, there is no news source that garners trust from a majority of the public on the topic of COVID-19. At the top of the list, nearly half say they have “a great deal” or “a fair amount” of trust in COVID-19 information that they see or hear on their local TV news station (47%) and on network news like ABC, NBC, and CBS (45%). About a third put a similar level of trust in information they see on CNN (36%), MSNBC (33%), and NPR (32%) while three in ten say the same about Fox News (29%). A smaller share put at least a fair amount of trust in COVID-19 information from One America News and Newsmax (13% each).
Overall, far fewer people say they trust information about COVID-19 that they see on social media compared to traditional news platforms (13% say they trust information they see on YouTube, 9% on Facebook, 6% each on Twitter and TikTok, and 5% on Instagram). The group that is influenced by information they see on these platforms may be larger than the share that says they trust information they see there, as we previously found in January that 31% of adults got information about COVID-19 vaccines from social media over a two-week period, nearly as large as the share who got information from cable, network, and local TV news.
As has been well documented (in particular by the Pew Research Center), the U.S. media environment has become increasingly polarized in recent years, with Democrats and Republicans placing trust in completely different news sources. This is true when it comes to trust in COVID-19 information as well. Majorities of Democrats say they trust information about COVID-19 from network news (72%), local TV news (66%), CNN (65%), MSNBC (56%), and NPR (51%), while none of these sources is trusted by a majority of independents or Republicans. Republicans’ most trusted sources of COVID-19 information is Fox News (49%) followed by smaller shares who trust local TV news (34%), network news (25%), and Newsmax (22%).
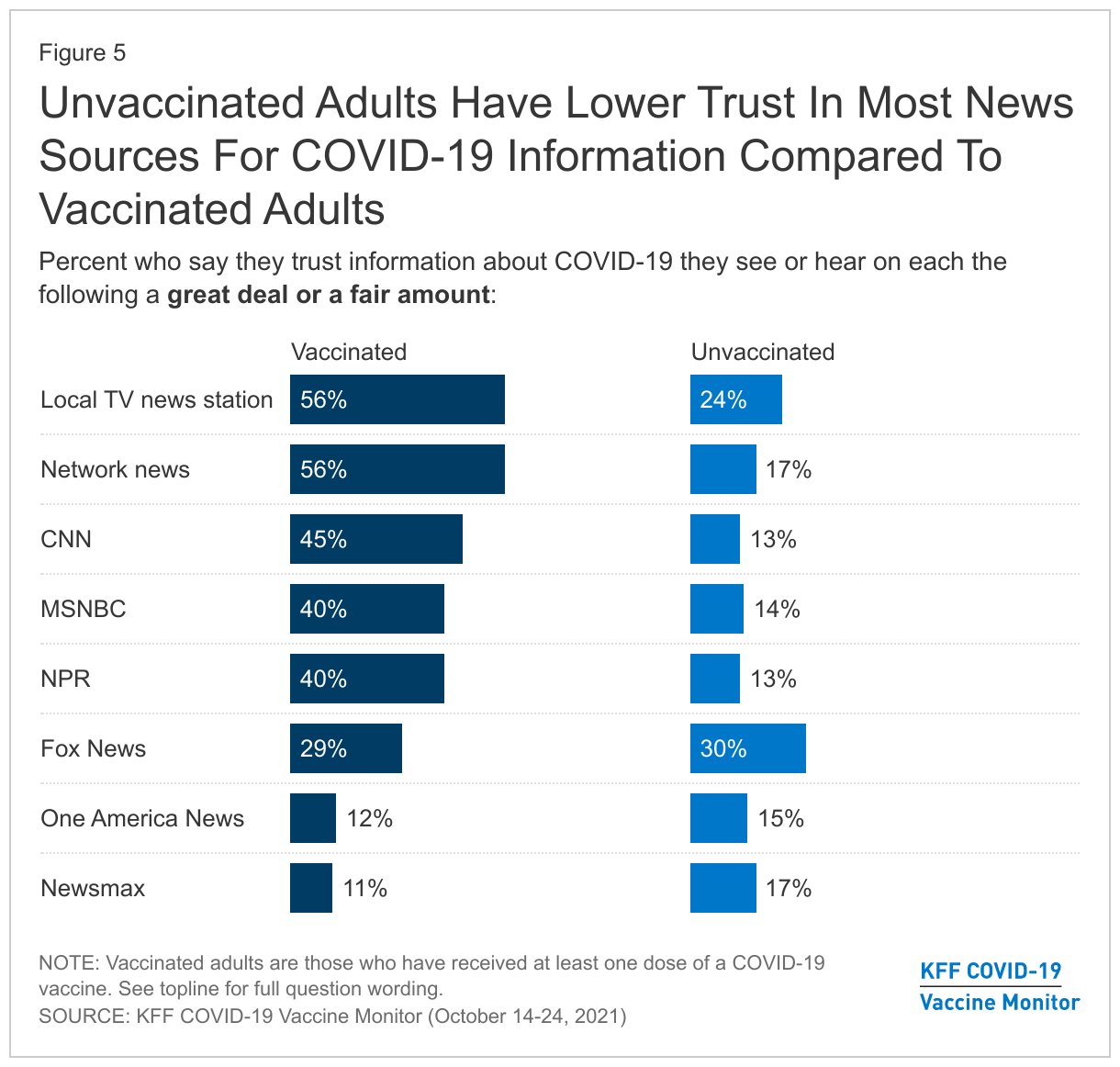
Trusted news sources for COVID-19 information differ by vaccination status in addition to partisanship. Among mainstream news sources, vaccinated adults are at least twice as likely as unvaccinated adults to say they trust COVID-19 information from their local TV news station, network news, CNN, MSNBC, and NPR. Similar shares of vaccinated and unvaccinated adults say they trust COVID-19 information they see on Fox News (29% and 30%, respectively). The one news source that is trusted by a larger share of unvaccinated adults compared to vaccinated adults is Newsmax (17% vs. 11%), though the shares who trust Newsmax are relatively small for both groups.
Relationship Between Trusted News Sources and Belief In COVID-19 Misinformation
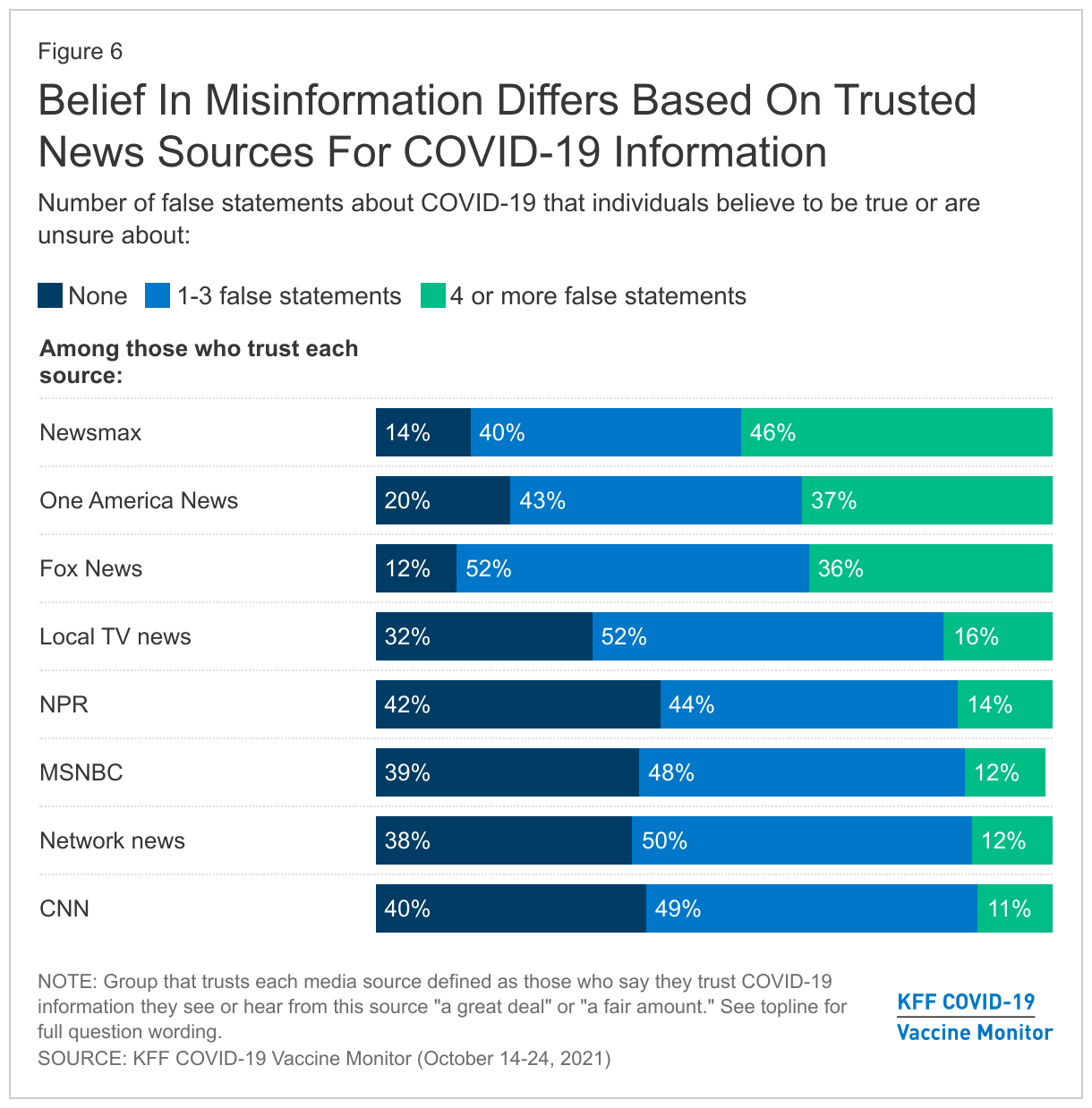
People’s trusted news sources are correlated with their belief in COVID-19 misinformation. Among those who say they trust COVID-19 information from CNN, MSNBC, network news, NPR, and local TV news, between three in ten and four in ten do not believe any of the eight pieces of misinformation tested in the survey, while small shares (between 11%-16%) believe or are unsure about at least four falsehoods.
Belief in misinformation is higher among those who say they trust COVID-19 information from conservative news sources, with nearly four in ten of those who trust Fox News (36%) and One America News (37%) and nearly half (46%) of those who trust Newsmax for such information saying they have heard at least four of the falsehoods tested in the survey and either believe them to be true or are unsure if they’re true or false. One thing this study cannot disentangle is whether this is because people are exposed to misinformation from those news sources, or whether the types of people who choose those news sources are the same ones who are pre-disposed to believe certain types of misinformation for other reasons.
Methodology
This KFF COVID-19 Vaccine Monitor was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted October 14-24, 2021, among a nationally representative random digit dial telephone sample of 1,519 adults ages 18 and older (including interviews from 309 Hispanic adults and 305 non-Hispanic Black adults), living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). Phone numbers used for this study were randomly generated from cell phone and landline sampling frames, with an overlapping frame design, and disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents as well as those living in areas with high rates of COVID-19 vaccine hesitancy. Stratification was based on incidence of the race/ethnicity subgroups and vaccine hesitancy within each frame. High hesitancy was defined as living in the top 25% of counties as far as the share of the population not intending to get vaccinated based on the U.S. Census Bureau’s Household Pulse Survey. The sample also included 87 respondents reached by calling back respondents that had previously completed an interview on the KFF Tracking poll at least nine months ago. Another 46 interviews were completed with respondents who had previously completed an interview on the SSRS Omnibus poll (and other RDD polls) and identified as Hispanic (including 23 in Spanish) or non-Hispanic Black (n=62). Computer-assisted telephone interviews conducted by landline (168) and cell phone (1,351, including 1,038 who had no landline telephone) were carried out in English and Spanish by SSRS of Glen Mills, PA. To efficiently obtain a sample of lower-income and non-White respondents, the sample also included an oversample of prepaid (pay-as-you-go) telephone numbers (25% of the cell phone sample consisted of prepaid numbers) Both the random digit dial landline and cell phone samples were provided by Marketing Systems Group (MSG). For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s 2019 U.S. American Community Survey (ACS), on gender, age, education, race, Hispanic origin, and region, within race-groups, along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the July-December 2020 National Health Interview Survey The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample, and design modifications, namely, the oversampling of potentially undocumented respondents and of prepaid cell phone numbers, as well as the likelihood of non-response for the re-contacted sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
This work was supported in part by grants from the Chan Zuckerberg Initiative DAF (an advised fund of Silicon Valley Community Foundation), the Ford Foundation, and the Molina Family Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Group
N (unweighted)
M.O.S.E.
Total
1,519
± 3 percentage points
COVID-19 Vaccination Status
Have gotten at least one dose of the COVID-19 vaccine
1,090
± 4 percentage points
Have not gotten the COVID-19 vaccine
406
± 6 percentage points
Race/Ethnicity
White, non-Hispanic
794
± 4 percentage points
Black, non-Hispanic
305
± 7 percentage points
Hispanic
309
± 7 percentage points
Party Identification
Democrats
460
± 6 percentage points
Republicans
341
± 7 percentage points
Independents
475
± 6 percentage points
Child Age Groups
Parents or guardians of children under 18
393
± 6 percentage points
Parents or guardians of children ages 12-17
202
± 9 percentage points
Parents or guardians of children ages 5-11
219
± 9 percentage points
Endnotes
For more information, see Sarah E. Gollust, Rebekah H. Nagler, Erika Franklin Fowler; The Emergence of COVID-19 in the US: A Public Health and Political Communication Crisis. J Health Polit Policy Law 1 December 2020; 45 (6): 967–981. doi: https://doi.org/10.1215/03616878-8641506↩︎
As of October 21, 2021, the Centers for Disease Control and Prevention (CDC) recommended that people who received the Pfizer-BioNtech or Moderna COVID-19 vaccine receive a booster shot if they are age 65 years and older, have underlying medical conditions that put them at higher risk for severe illness, or are in high-risk occupational and institutional settings. For people who got the Johnson and Johnson COVID-19 vaccine, the CDC recommends they get a booster if they are age 18 and older and were vaccinated two or more months ago. Data from CDC indicate that as of November 2, 19.8 million fully vaccinated people have received booster shots of the COVID-19 vaccine. However, data currently are limited to understand whether there are racial disparities in booster shot uptake. Increasing the availability of data to understand who is receiving booster doses is important for identifying and addressing potential disparities in COVID-19 booster shot uptake. This data note reviews data currently available at the federal and state level on race/ethnicity of booster shot recipients.
Federal COVID-19 Booster Dose Vaccination Data
The CDC is not reporting race/ethnicity of booster dose recipients at this time, although may begin reporting these data in the future. As of November 2, 2021 CDC reports the total number of booster shots administered and share of fully vaccinated people who have received a booster dose for the total population, adults 18 years of age and older, adults 50 years of age and older, and adults 65 years of age and older. These data show that as of November 2, 2021, about 10% of fully vaccinated people had received a booster dose, including over 25% of fully vaccinated people age 65 and older.
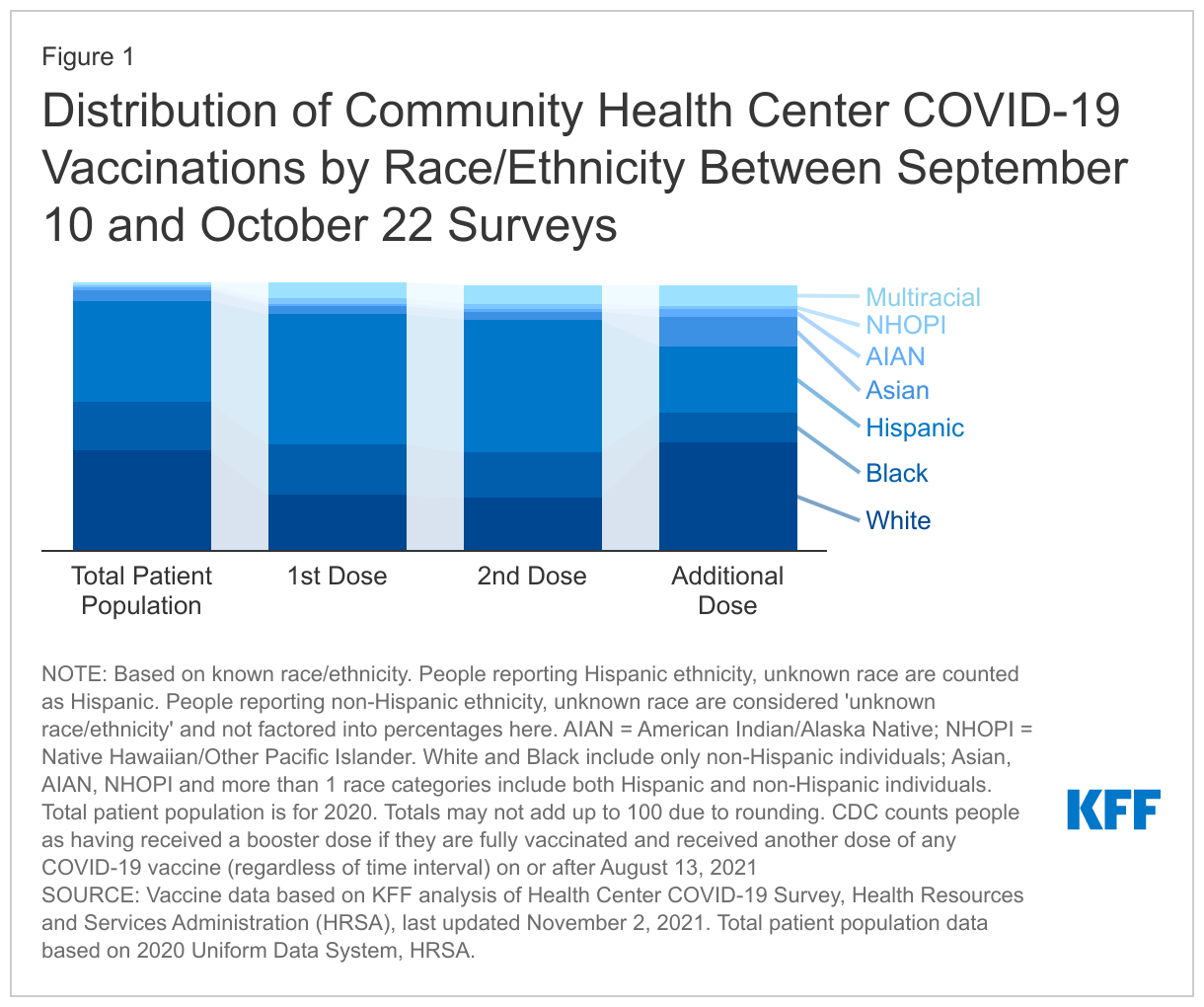
Separately, the Health Resources and Services Administration (HRSA) reports data on booster shot recipients for individuals who received them at a community health center. These data are based on the bi-weekly Health Center COVID-19 Survey and include race/ethnicity of booster dose recipients at the federal and state level. Community health centers are a primary source of care for low-income populations and people of color and have been a key federal partner in facilitating equitable access to vaccines.
Community health centers are providing first and second doses of the vaccine to people of color at rates higher than their share of the overall patient population, but the share of booster dose recipients who are people of color is similar to the share of the total patient population. In 2020, 62% of community health center patients were people of color. In contrast, between the September 10 and October 22 surveys, 80% of first and second dose vaccine recipients with known race/ethnicity were people of color. Only 59% of booster dose recipients at community health centers surveyed during the same period were people of color. White, Asian, American Indian and Alaska Native (AIAN) and multiracial people received similar or larger shares of booster doses compared to their representation in the overall patient population between the September 10 and October 22 surveys, while Hispanic, Black, and Native Hawaiian and Other Pacific Islander (NHOPI) people received smaller shares of booster shots. A larger share of booster doses also had unknown or missing race/ethnicity data (18%) compared to initial (14%) and second (13%) doses.
State COVID-19 Booster Dose Vaccination Data
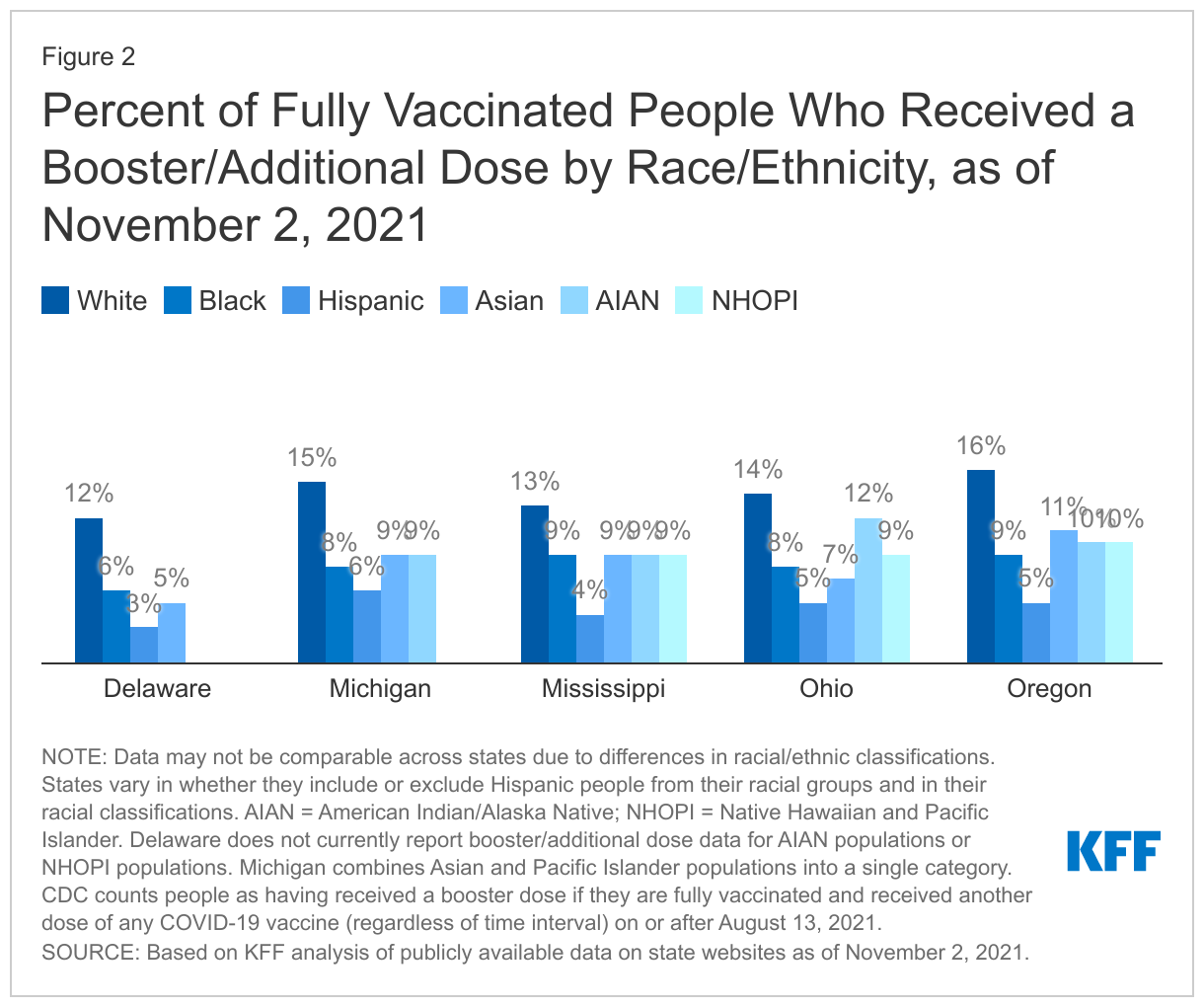
As of October 28, 2021, 27 states and Washington, DC were publicly reporting the total number of individuals who received booster or additional doses of the COVID-19 vaccine, but only 7 of these states (Colorado, Delaware, Michigan, Mississippi, New Jersey, Ohio, and Oregon) reported the race and ethnicity of booster dose recipients. As with state reporting of data for first and second doses, states vary in how they report booster dose data by race and ethnicity and in the completeness of their data. Delaware and New Jersey do not report data for AIAN or NHOPI people; Michigan combines Asian and Pacific Islander people into a single category, and the states vary in whether they report Hispanic ethnicity separately from race.
The limited data on booster shots by race/ethnicity available to date show that fully vaccinated White people are more likely to have received a booster dose compared to other groups as of November 2, 2021. Across the five states where we were able to calculate the share of fully vaccinated people who have received a booster dose by race/ethnicity, the share of fully vaccinated White people who had received a dose was higher compared to other racial/ethnic groups. These differences were largest compared to Hispanic people in all five of the states.
Discussion
In sum, to date, there is limited data on race/ethnicity of COVID-19 booster shot recipients. The limited data available to date suggest that fully vaccinated White people are more likely to have received a booster shot compared to other racial/ethnic groups. White people account for a larger share of booster shot recipients at community health centers compared to first and second dose recipients. Moreover, in the few states reporting data, a higher share of fully vaccinated White people received a booster dose compared to other racial/ethnic groups.
These patterns, in part, may reflect differences in the age distribution of racial/ethnic groups. CDC has recommended that people age 65 and older receive booster shots if they received a Pfizer or Moderna COVID-19 vaccine, and White people are more likely than people of color to be age 65 or older (21% vs. 10%).1 However, CDC guidance also notes that adults between ages 18-64 who have underlying health conditions and those who are at increased risk for COVID-19 exposure and transmission because of occupational or institutional setting may obtain a booster. Previous analysis has shown that people of color are more likely to have underlying health conditions that put them at increased risk for serious illness if infected with COVID-19 and to work in frontline essential jobs that increase risk of potential exposure to the virus. Further, it remains difficult to interpret the booster shot data because data are not available on who is eligible for a booster shot by race/ethnicity. For example, booster shot recommendations vary by type of vaccine received, with all adults who received the Johnson and Johnson vaccine recommended to get a booster shot two months or more after their initial dose. However, racial/ethnic data are not available for vaccine recipients by vaccine type. Going forward, comprehensive, consistent, and complete racial and ethnic data will be key for identifying potential disparities in uptake of the booster shots and directing efforts to address those disparities.
KFF analysis of 2019 American Community Survey data. ↩︎
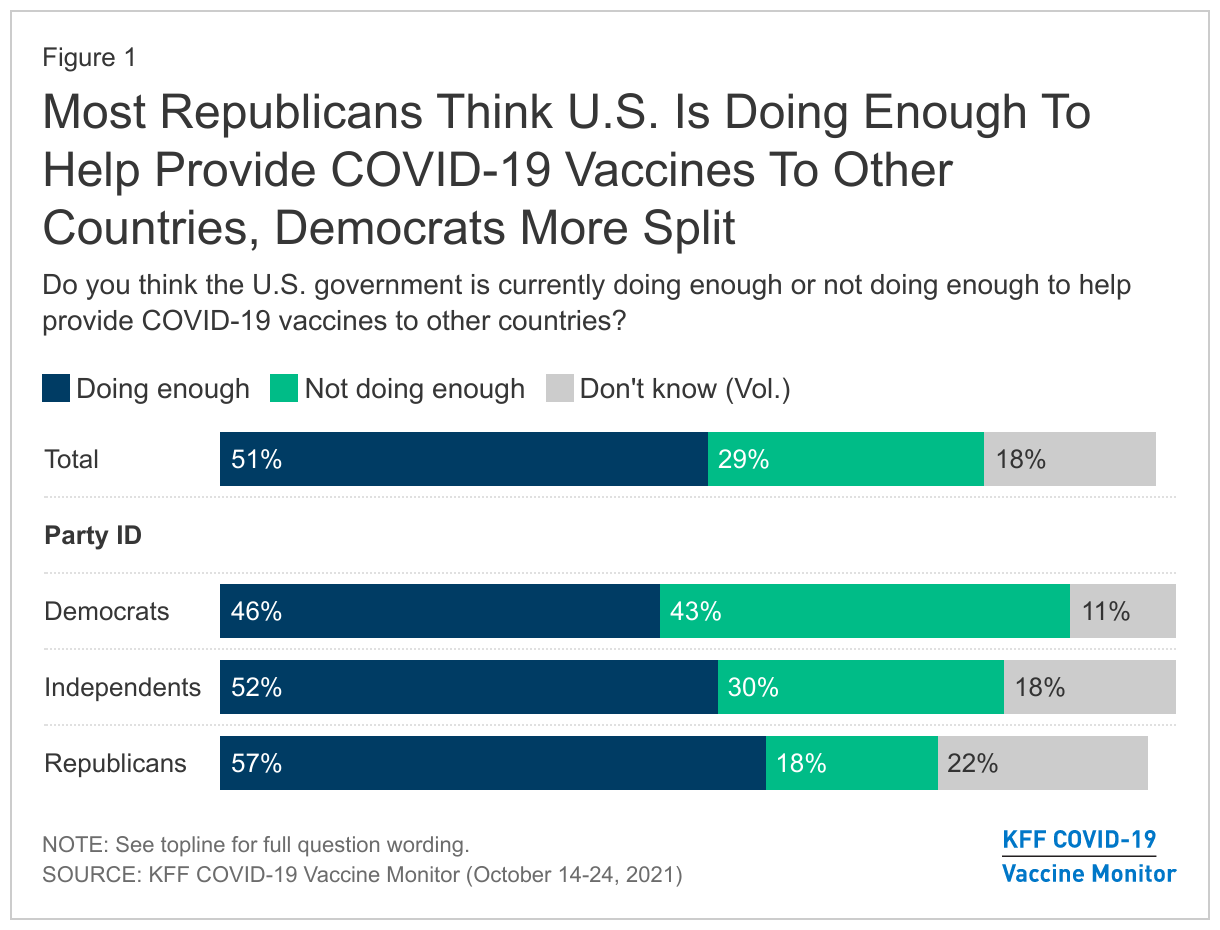
The Biden administration has stated its intention to help combat the COVID-19 pandemic around the world and recently convened a global summit to set global targets and announce new commitments. The U.S. has pledged more COVID-19 vaccine doses and funding than any other country. In the latest KFF COVID-19 Vaccine Monitor, we find that the public is generally supportive of this work, though more likely to prefer the U.S. playing a major role versus a leading one, and there are partisan differences. When informed that the U.S. has enough of its own vaccine supply, public support for the U.S. taking a major role in global vaccine distribution rises.
Survey Findings
About half of the public (51%) say that the U.S. government is doing enough to help provide COVID-19 vaccines to other countries, while around three in ten adults (29%) don’t think the U.S. is doing enough and another one in five aren’t sure. Across partisans, a majority of Republicans say the U.S. is doing enough to help provide vaccines to other countries (57%) whereas Democrats are more divided (46% say the U.S. is doing enough vs. 43% who say it is not).
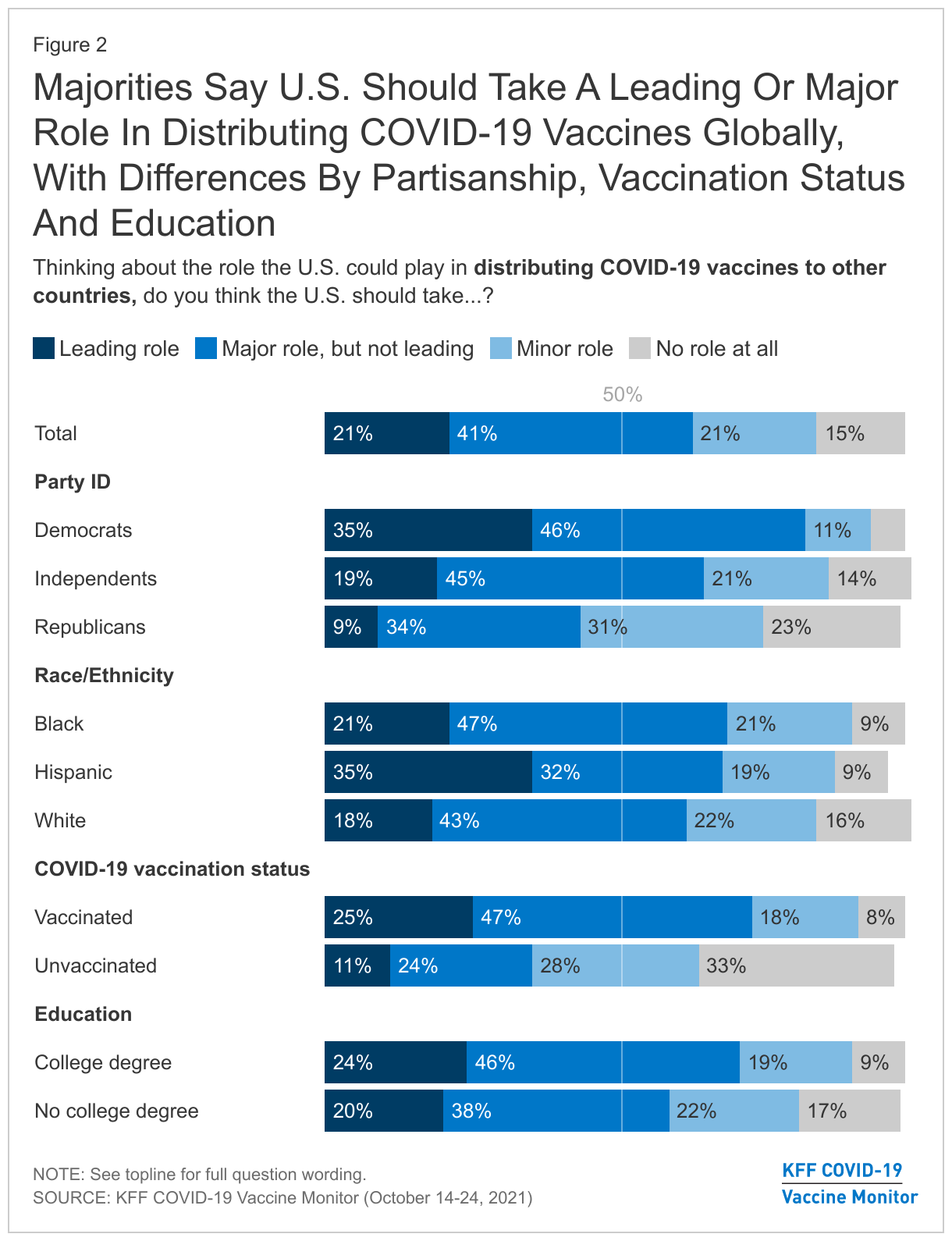
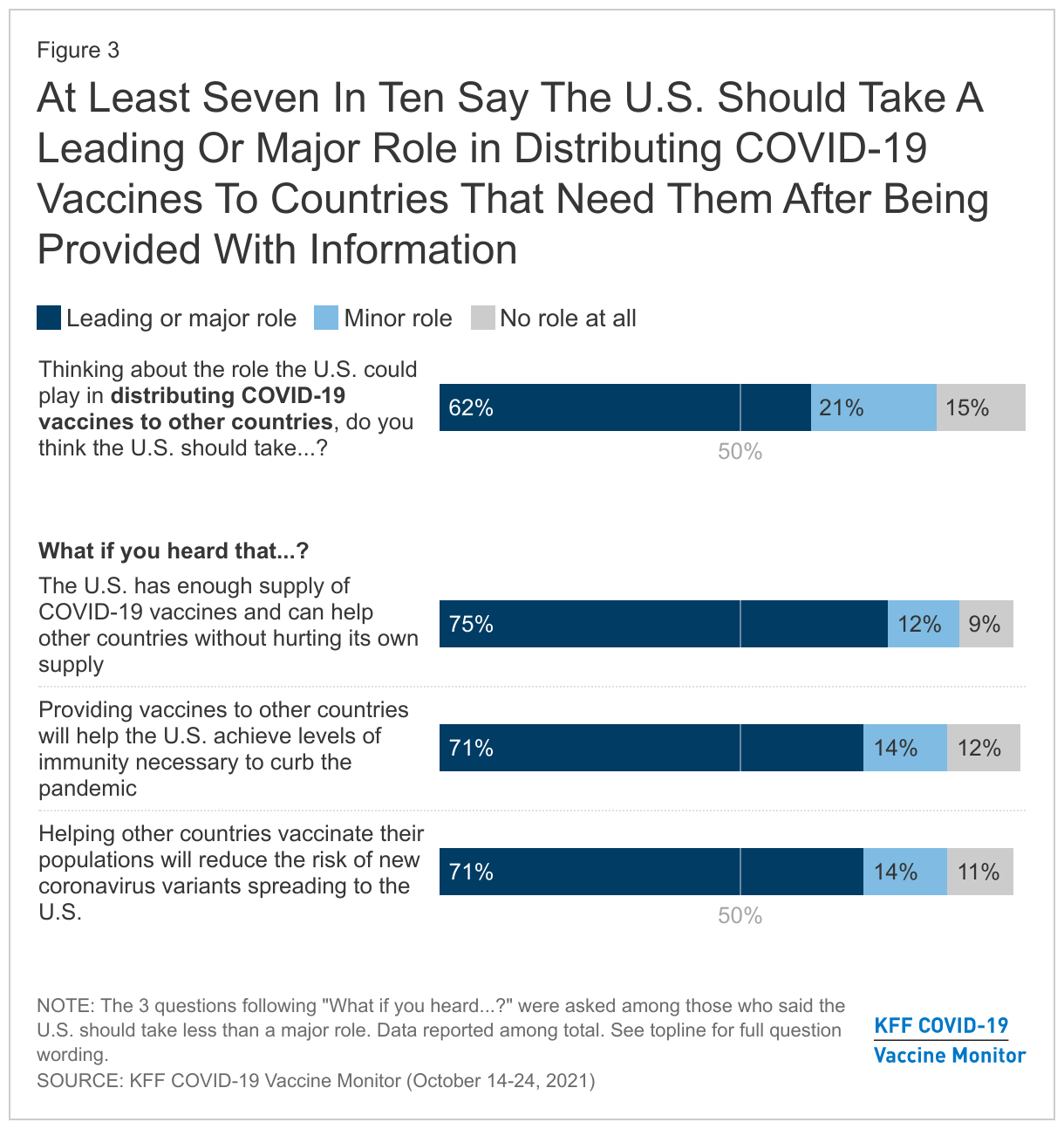
When it comes to how much of a role the U.S. should play, 62% of Americans say the U.S. should take a leading or major role in helping provide vaccines to other countries that need them, including 21% who think the U.S. should take a leading role in distribution (a slight decline from 27% in May).
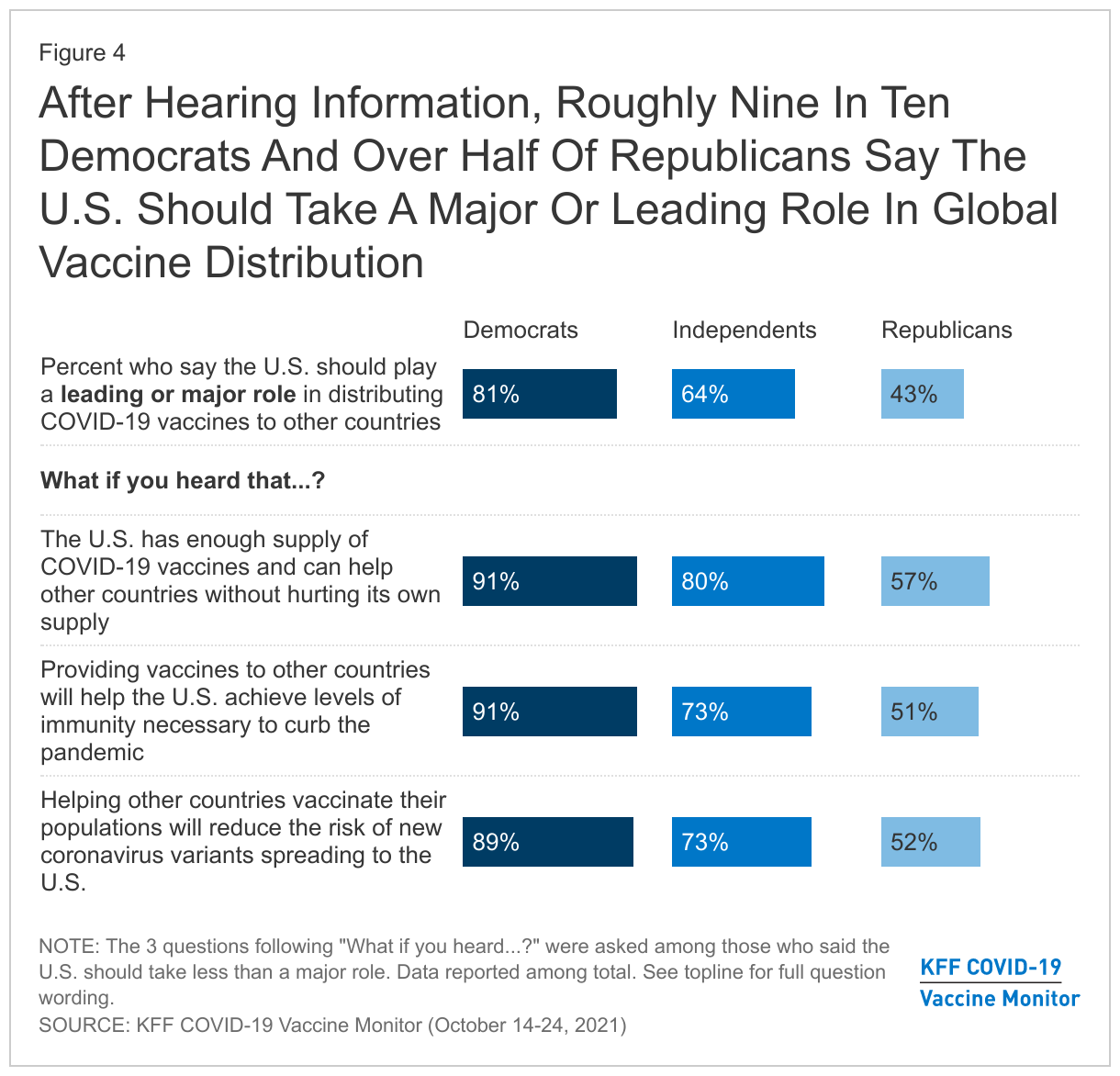
Partisans are divided on the role the U.S. should take in efforts to distribute the vaccine globally with eight in ten Democrats (81%) saying the U.S. should take a leading or major role in assisting with global distribution compared to less than half of Republicans (43%) who say the same. In addition, about seven in ten vaccinated adults (73%), those with college degrees (70%), Black adults (68%), and Hispanic adults (67%) think the U.S. should take a leading or major role.
The share of adults saying the U.S. should play a major or leading role in international vaccine distribution rose across partisans when presented with each piece of information tested in the survey. After hearing each piece of information, roughly nine in ten Democrats, more than seven in ten independents, and at least half of Republicans said the U.S. should play a major or leading role.
Methodology
This KFF COVID-19 Vaccine Monitor was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted October 14-24, 2021, among a nationally representative random digit dial telephone sample of 1,519 adults ages 18 and older (including interviews from 309 Hispanic adults and 305 non-Hispanic Black adults), living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). Phone numbers used for this study were randomly generated from cell phone and landline sampling frames, with an overlapping frame design, and disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents as well as those living in areas with high rates of COVID-19 vaccine hesitancy. Stratification was based on incidence of the race/ethnicity subgroups and vaccine hesitancy within each frame. High hesitancy was defined as living in the top 25% of counties as far as the share of the population not intending to get vaccinated based on the U.S. Census Bureau’s Household Pulse Survey. The sample also included 87 respondents reached by calling back respondents that had previously completed an interview on the KFF Tracking poll at least nine months ago. Another 46 interviews were completed with respondents who had previously completed an interview on the SSRS Omnibus poll (and other RDD polls) and identified as Hispanic (including 23 in Spanish) or non-Hispanic Black (n=62). Computer-assisted telephone interviews conducted by landline (168) and cell phone (1,351, including 1,038 who had no landline telephone) were carried out in English and Spanish by SSRS of Glen Mills, PA. To efficiently obtain a sample of lower-income and non-White respondents, the sample also included an oversample of prepaid (pay-as-you-go) telephone numbers (25% of the cell phone sample consisted of prepaid numbers) Both the random digit dial landline and cell phone samples were provided by Marketing Systems Group (MSG). For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s 2019 U.S. American Community Survey (ACS), on gender, age, education, race, Hispanic origin, and region, within race-groups, along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the July-December 2020 National Health Interview Survey The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample, and design modifications, namely, the oversampling of potentially undocumented respondents and of prepaid cell phone numbers, as well as the likelihood of non-response for the re-contacted sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
This work was supported in part by grants from the Chan Zuckerberg Initiative DAF (an advised fund of Silicon Valley Community Foundation), the Ford Foundation, and the Molina Family Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Group
N (unweighted)
M.O.S.E.
Total
1,519
± 3 percentage points
COVID-19 Vaccination Status
Have gotten at least one dose of the COVID-19 vaccine
As the ninth open enrollment period for the Health Insurance Marketplaces begins, enhanced Marketplace premium help along with increased funding for outreach and enrollment assistance mean there are more affordable coverage options for the millions of people who remain uninsured and more help available to connect those individuals to coverage. During the open enrollment period, which runs from November 1 through January 15 in the federal Marketplace (in states that operate their own Marketplaces, 9 have the same dates, 7 extend open enrollment to January 23 or 31, and 2 shorten it to December 15), advertising and outreach campaigns encourage new consumers to apply for Marketplace coverage and existing consumers to renew their coverage. Importantly, efforts to facilitate enrollment in the ACA Marketplaces will also identify low-income individuals who are eligible for Medicaid. In 2020, there were 27 million non-elderly uninsured people, and a majority were eligible for financial assistance through the ACA Marketplaces or Medicaid.
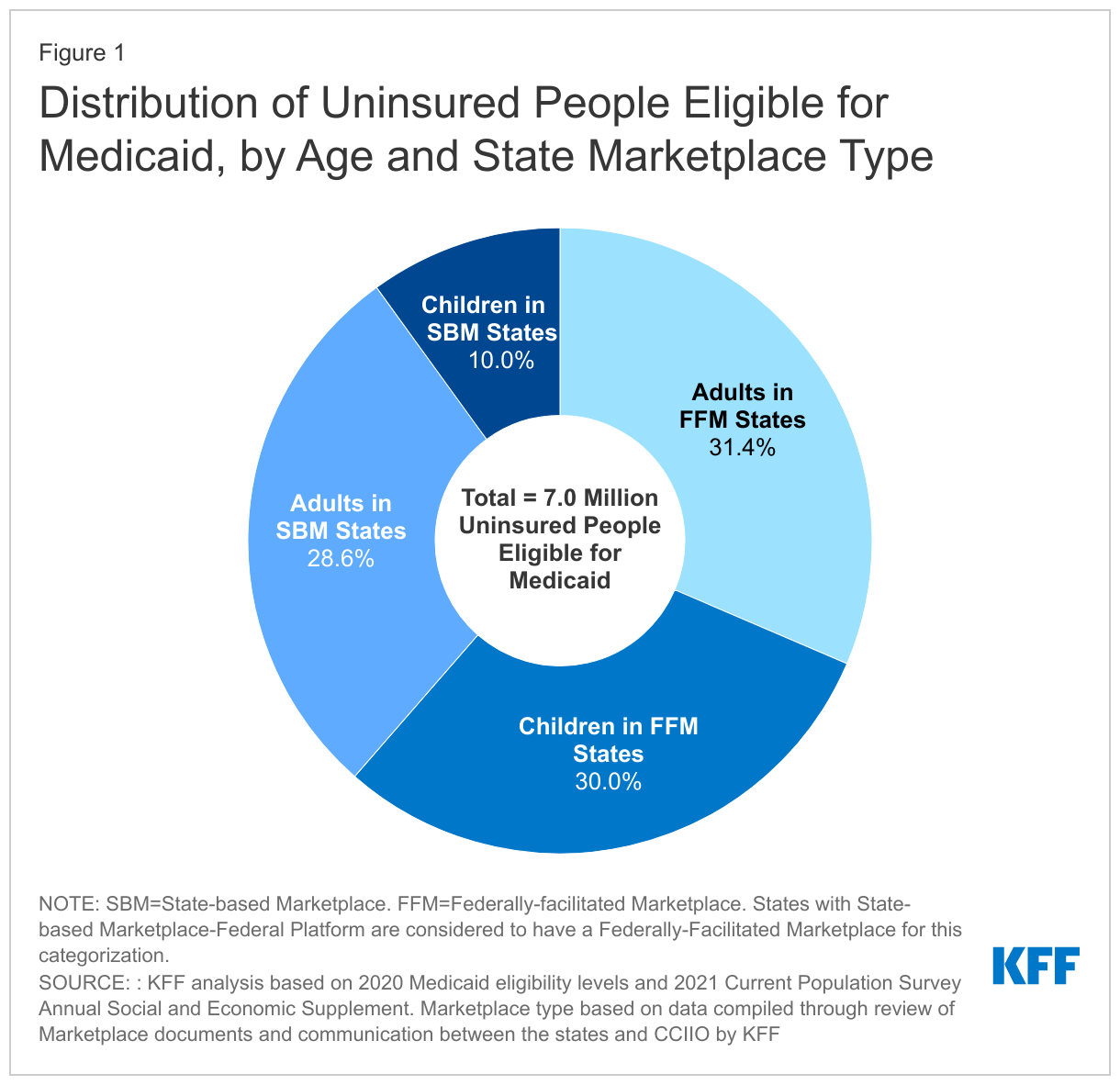
In 2020, 7.0 million uninsured people were eligible for Medicaid. Over six in ten of these people are adults (31%, or 2.2 million) or children (30%, or 2.1 million) living in the 33 states in which the ACA Marketplace is federally-operated (FFM) or state-operated but the state uses the federal Healthcare.gov platform (SBM-FP). Another 29% (2.0 million) are adults in states that fully operate their own marketplaces (SBM), while only 10% (0.7 million) are children in SBM states (Figure 1).
Under enrollment simplification processes established by the ACA, states must provide a singleapplication for Medicaid, CHIP, and Marketplace coverage, thereby establishing a “no wrong door” application process for ACA coverage. This process means that the Marketplaces will screen or assess individuals’ eligibility for all health coverage programs, including Medicaid and CHIP, and individuals will be enrolled in or referred to the program for which they are eligible regardless of how they apply. Most states utilizing the FFM do not authorize the FFM to make final Medicaid eligibility determinations for most groups, but instead conduct full eligibility determinations for individuals after the FFM assesses them as eligible for Medicaid. The states that operate SBMs typically have a single integrated system through which individuals can apply for and renew Medicaid, CHIP and Marketplace coverage.
During the Marketplace special enrollment period (SEP) that ran from February 15 to August 15, 2021, over half a million people applying for marketplace coverage in FFM states, or 13% of all applicants, were assessed or determined eligible for Medicaid. That share is up from the 8% of applicants (or836,451 people) who were assessed or determined eligible for Medicaid in FFM states during the 2020 Marketplace open enrollment period (which closed in December 2019). Increased advertising and outreach during the SEP coupled with the availability of zero-premium silver plans plans for those with incomes up to 150% of the federal poverty level (FPL) may have contributed to a larger share of lower income people applying for Marketplace coverage, including those who appeared to qualify for Medicaid in their states. The report did not include data from SBM states; the number of people determined eligible for Medicaid during the SEP would no doubt have been larger if it had.
Enhanced funding for outreach, advertising, and in-person assistance during the Marketplace open enrollment period can also raise awareness of Medicaid and promote Medicaid enrollment. For the 2022 open enrollment period, the Biden administration has launched expansive advertising and outreach campaigns to educate consumers on the availability of both Marketplace and Medicaid coverage. It has also increased funding for Navigators in the federal Marketplace seven-fold from $10 million in 2020 to $80 million in 2021. The enhanced Navigator funding will mean more staff to assist both Marketplace and Medicaid applicants.
The Build Back Better Act currently under consideration in Congress would provide a coverage pathway for the over 2 million people in the Medicaid coverage gapin the dozen states that have not expanded Medicaid under the ACA, allowing them to purchase subsidized coverage in the Marketplaces beginning in 2022. Unlike their counterparts in Medicaid expansion states, individuals currently in the coverage gap will not be eligible for Medicaid; however, funding in the legislation for targeted outreach to these newly eligible individuals may also reach those who are currently eligible for Medicaid but not enrolled, leading to overall gains in Medicaid enrollment.
While rapid home COVID-19 tests have been identified as an important component of controlling the spread of SARS-CoV-2, the virus that causes COVID-19, there have been ongoing supply challenges in the U.S. Challenges in accessing rapid home tests became more acute as the Delta variant took hold, vaccination rates stagnated, and cases, hospitalizations, and deaths surged. In addition, some workplaces began reopening, millions of school age children returned to in-person school and colleges and universities began the fall semester. Home test supply and access challenges in the U.S. contrast with the experience in several peer countries which have made rapid home tests widely available and at little or no cost. The Biden administration has taken recent steps to address these challenges, including a new announcement that it would work to identify manufacturers of high quality tests to encourage them to bring them to the U.S. market and to streamline the regulatory review pathway for authorization of over-the-counter at-home tests, though it is unclear if or how quickly these measures will fully resolve the issues.
In this brief, we examine the various interrelated factors that have contributed to rapid home test scarcity in the U.S. The five factors we identify include:
The regulatory framework: The FDA regulatory framework and process are central to the availability of COVID-19 testing, including for home testing. However, some argued the framework for evaluating rapid home tests was initially too stringent, creating challenges for manufacturers seeking authorization and hampering test availability. While the FDA took steps to modify the process, some suggested that the regulatory environment was still too strict. The new announcement that the FDA aims to further streamline the process is likely to address some of these issues.
Supply chain and the unpredictability of demand: The COVID-19 pandemic has led to supply chain disruptions worldwide, including for tests and their components, negatively impacting test supply. This, coupled with the unpredictability of the pandemic, have made it difficult for manufacturers to gauge demand and at times limited their willingness to scale up production due to perceived business risk, again impacting test availability. Recent steps taken by the administration are designed to increase supply.
Federal investment: While this may be beginning to shift, the lack of up-front federal investment in testing, including pre-purchasing of tests, is another factor that appears to have impacted testing availability and affordability, and contrasts with the federal government’s approach to vaccines.
Federal messaging and guidance: Evolving federal messaging and guidance related to the role of testing over the course of the pandemic and limited messaging about home testing may have led to confusion about its importance and impacted public understanding of home testing specifically.
Cost and coverage: While COVID-19 tests are generally covered by insurance, as required by emergency COVID-19 legislation passed by Congress, and are also available free of charge at many locations in the U.S., this is not the case for over-the-counter rapid home tests. Instead, consumers must pay out of pocket for these tests which can be costly, limiting access and potentially contributing to existing pandemic disparities. Recently, the federal government accelerated purchasing of rapid tests for use in certain community-based settings and negotiating with retailers to lower store prices, albeit for a time-limited period.
Taken together, we identify a number of barriers that have contributed to the scarcity of rapid home COVID-19 tests in the U.S. Recent actions taken by the Biden administration, including steps expected to result in an increase in home test production and to further streamline the authorization process, may alleviate some of these barriers, but others may persist.
Issue Brief
Introduction
While diagnostic testing is an important tool for helping to reduce the spread of COVID-19, there have been challenges in scaling up testing in the U.S. throughout the pandemic, and these have been particularly acute in the case of rapid home tests. Rapid home tests, some of which can provide results in as little as 15 minutes, have been identified as an important public health intervention for controlling COVID-19 transmission because of their ability to be used at home by an individual, provide results quickly, and to identify infection when someone is “likely to be most contagious.” Challenges in accessing rapid home tests became more acute as the Delta variant took hold, vaccination rates stagnated, and cases, hospitalizations, and deaths surged. In addition, some workplaces began reopening, millions of school age children returned to in-person school, and colleges and universities began the fall semester. These challenges contrast with the experiences of several other peer countries which have made rapid home tests widely available and at little or no cost. The UK government, for example, provides up to seven tests per day to those who cannot get tests from work or school and recommends each individual screen themselves twice weekly. Providing up to 7 tests per person allow one individual to collect tests for a whole household. Germany, until recently, made rapid antigen tests freely available as well (and tests can still be purchased for a few dollars in grocery stores).
President Biden announced early support for rapid tests. The Biden campaign said that if elected it would “Invest in next-generation testing, including at home tests and instant tests, so we can scale up our testing capacity by orders of magnitude.” The White House National Strategy for COVID-19, released on January 22, 2021, underscored the importance of rapid testing particularly to help “Safely reopen schools, businesses, and travel, while protecting workers” and funding was awarded in February to increase production of at-home tests. But ongoing supply shortages, particularly in the context of Delta, prompted more recent actions. On September 9, the President released a COVID-19 action plan that included, among other elements, the intent to use the Defense Production Act to increase the production of rapid tests; an investment of $2 billion to purchase 280 million rapid point-of-care and OTC at-home COVID-19 tests to be made available in a variety of community settings and long-term care facilities; and an agreement with several top retailers to sell rapid home tests at cost for a three month period. An additional $1 billion investment was announced on October 6 to further mobilize testing production, as well as agreements from some manufacturers to increase production. As a result, the administration expects to double rapid test capacity by the end of the year, from 100 million tests per month to 200 million, rising to 300 million by February 2022. As part of this effort, in late October, the administration announced additional measures, including a new program which aims to identify manufacturers of high quality tests to encourage them to bring them to the U.S. market, as well as a streamlining of the FDA regulatory pathway. It is not yet clear, however, if these recent actions will fully resolve rapid home test supply and access issues, particularly if there is another surge in cases at some point.
In this brief, we examine the various interrelated factors that have contributed to rapid home test scarcity in the U.S.
Background
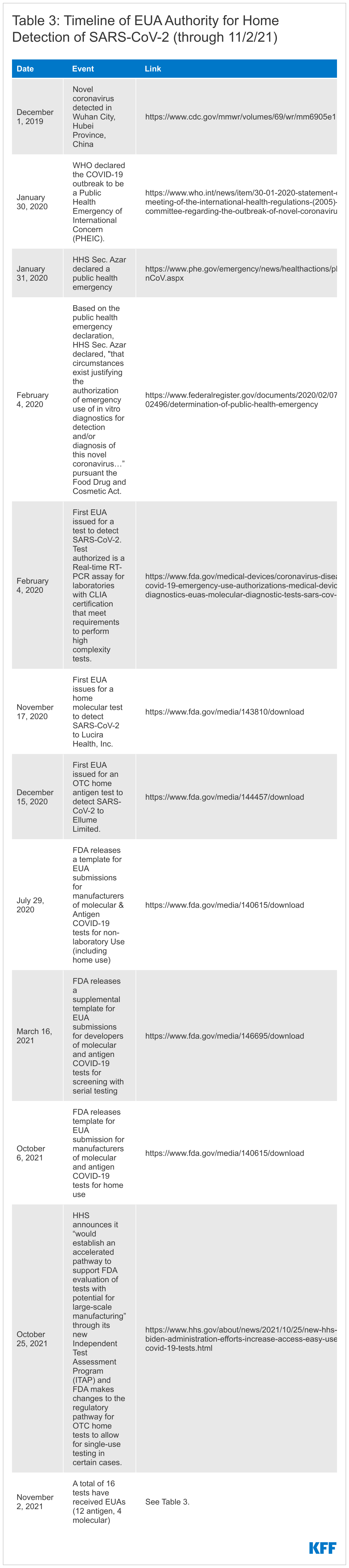
The declaration of a public health emergency due to COVID-19, first on January 20, 2020 and renewed every three months since (six times as of October 11, 2021), paved the way for the Food and Drug Administration (FDA) to exercise its expedited emergency use authorization (EUA) process for medical devices, including COVID-19 diagnostics.
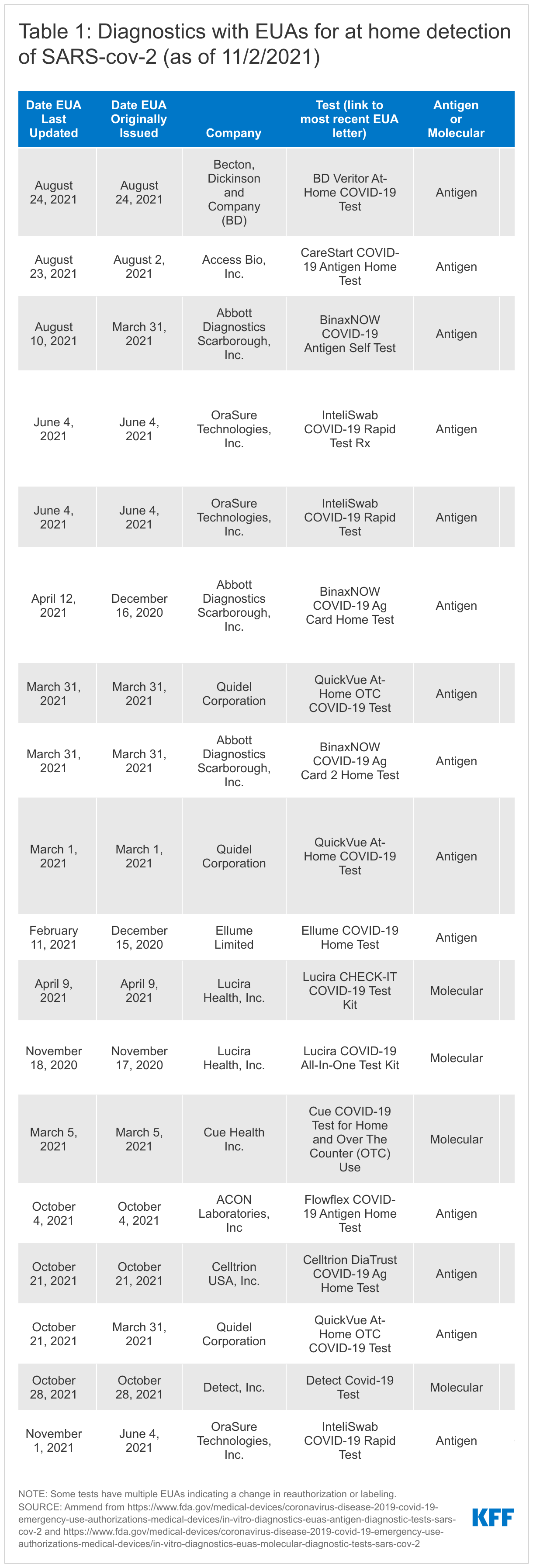
To date, the FDA has authorized 16 home tests (several receiving revised EUAs over time) to 11 companies (see Table1). In several cases, one manufacturer has received multiple EUAs for essentially the same product but has different indications in terms of prescription vs. over-the-counter use or with revisions to labeling. Of the 16 tests with EUAs, 12 are OTC while four require a prescription.
The 16 authorized home diagnostics include two types of tests: antigen tests (12 of the 16) and molecular tests (4 of the 16). Antigen tests detect specific viral antigens indicative of SARS-CoV-2, the virus that causes COVID-19. Molecular tests, including polymerase chain reaction (PCR) tests, detect the virus' genetic material (see Table 2). Antigen tests tend to be highly specific (the ability to accurately diagnose negative cases) but are typically less sensitive (the ability to accurately diagnose positive cases) compared with molecular tests. However, antigen tests demonstrate “comparable performance to” molecular tests in “symptomatic persons and/or if culturable virus present, when the person is presumed to be infectious.” They have advantages as well; they have a more simple design and are less expensive than molecular tests, potentially reducing both manufacturing and access barriers, and are available at the point-of-care, including in the home. Of the 12 authorized antigen tests, 9 appear to have been marketed directly to consumers, while none of the molecular tests have.
Table 2. Differences in Home COVID-19 Testing Options
Test Type
Antigen – Antigen tests detect specific viral antigens indicative of SARS-CoV-2, the infection that causes COVID-19. Antigen tests tend to be highly specific but are typically less sensitive than molecular tests.
Molecular or Nucleic acid amplification tests (NAAT) - Detects the virus' genetic material (RNA), highly sensitive and highly specific. Polymerase chain reaction (RT-PCR or PCR) is one type of NAAT.
Prescription or Over-the-counter
Prescription - Some home tests with an EUA require a prescription from a medical provider. In certain cases, tests can be prescribed and ordered online (e.g. http://www.emed.com)
Over-the-counter (OTC) - Some tests have been authorized for OTC use, meaning they can be purchased in a store or online without a prescription.
Collection, Results, and Reporting
Home - The test is conducted at home and the results are returned to the user within a short window, often 15 minutes. The individual is responsible for reporting results to a public health authority/provider or an app is used during the home test process and the app/manufacturer reports results to the appropriate public health authority.
Self-collection - The user collects a sample and places it into a home collection kit which is the sent to a lab for results interpretation. The lab reports results to appropriate public health authorities.
The first EUA for a COVID-19 diagnostic test, a laboratory-based PCR, was issued on February 4, 2020. Nine months later, on November 17, 2020, the first EUA for a home COVID-19 test, in this case a molecular test, was issued and the first EUA for a home antigen test was issued December 15, 2020. (See Table 3 for a more detailed timeline of authorization events).
Factors impacting availability of home COVID-19 tests
There are several interrelated factors that impact the availability of rapid home COVID-19 tests. These range from the regulatory environment to the supply chain to federal investment and messaging to affordability. Each is explored below.
The Regulatory Framework
The FDA regulatory framework and process are central to the availability of COVID-19 testing, be that in the home, community, clinic, or laboratory. All tests for COVID-19, including home tests, must go through regulatory review. Recognizing the importance of making safe and effective COVID-19 tests available and to facilitate and streamline the EUA process, the FDA provides manufactures with application templates. Though manufacturers are not required to use these templates, they can expedite the process and they provide agency recommendations for test performance and other elements.
There have been several templates and updates released since the beginning of the pandemic, targeting different types of tests, settings, and strategies. The first template was released in January 2020 for laboratory-based tests, with a template for non-laboratory-based tests, including for home use, coming in July 2020, and one for screening with serial testing (e.g. testing multiple times in a short window to improve chances of detecting infection) in March 2021. Most recently, the first template specifically for home tests was released in early October and then revised at the end of the month in 2021. (See Table 2 for a more detailed timeline.)
The recommendations for test performance continue to evolve over time. Earlier templates for use for rapid home tests set a high bar for efficacy, with FDA generally recommending efficacy quite similar to an “authorized high sensitivity molecular test.” Over time, FDA has changed its recommended benchmarks or created new pathways (e.g. for serial testing for use with asymptomatic individuals) and these changes have coincided with increased home test approval.
Despite these changes in the regulatory framework, however, some have argued that the comparison of antigen test performance to PCR test performance still sets the benchmark too high, making it overly difficult for developers to meet. One rationale behind this critique is that the focus on antigen test efficacy should be on its ability to detect infectious individuals to quickly interrupt onward transmission. Others disagree and suggest that while antigen tests perform well at detecting infectious individuals, they should not be used for assessing infectiousness on their own. CDC has found that Abbott’s antigen, “BinaxNow [test] performs better at identifying rRT-PCR–positive specimens with lower Ct (suggestive of higher viral loads) and positive viral cultures” but it warns “these factors are not precise proxies for infectiousness.”
Indeed, the U.S. recommendations are higher compared to standards in some peer countries, such as the UK. To the extent that FDA regulatory requirements are a barrier for companies to submit requests for EUAs, fewer tests with authorization could lead to decreased competition in the marketplace, potentially impacting both cost and availability. On the other hand, whether a lower standard would negatively impact test quality, and by association the ability to control the pandemic, is unknown.
While the FDA has not suggested it will lower the recommended threshold for tests, on October 25, 2021, HHS announced that the NIH “would establish an accelerated pathway to support FDA evaluation of tests with potential for large-scale manufacturing” through its new Independent Test Assessment Program (ITAP), an extension of its Rapid Acceleration of Diagnostics (RADx) initiative. HHS states the program, which will be a collaboration of NIH, FDA, and CDC and other HHS experts will “identify manufacturers of high quality tests and encourage them to bring those tests to the U.S. market, increasing options for people and overall supply and potentially lowering costs.” Companies will receive support to “help ensure they are providing the best submissions possible for FDA’s regulatory review” and scalable OTC tests will be prioritized. In addition, FDA made changes to the regulatory pathway for OTC home tests currently authorized only for serial testing by revising recommendations to allow for single-use testing for symptomatic individuals. This reduces the amount of data developers would need to submit and allows them to sell certain tests currently sold as two-packs as singles, potentially leading to more individual tests being available for sale at a lower price.
Finally, just because a test has an EUA does not mean that it will circulate widely in the consumer market, as we have seen with some of the antigen and all of the molecular tests with EUAs for home use, suggesting that regulatory issues alone are not the only factors in test availability.
Supply Chain and the Unpredictability of Demand
The COVID-19 pandemic has led to supply chain disruptions across the world, and this has, in some cases, included the raw materials needed to manufacture COVID-19 diagnostics. Certainly that both the Trump and Biden Administrations have leveraged the Defense Production Act (DPA) to support testing, including Biden’s use of the DPA for home tests, and address other supply shortages, such as for personal protective equipment, is suggestive of challenges in the production and availability of these essential goods.
Additionally, a review of testing manufacturer Securities and Exchange Commission (SEC) filings reveals concerns about supply chain with respect to raw materials and diagnostic components:
“As a result of the COVID-19 pandemic, we have seen delays in receipts for certain raw materials and components for our products. Such delays can result in disruption to our business operations….We cannot currently predict the frequency, duration or scope of these government actions and any supply disruptions, and the availability of various products is dependent on our suppliers, their location and the extent to which they are impacted by the COVID-19 pandemic, among other factors. …Our inventory levels may fluctuate due to supply chain variability in conjunction with larger and more frequent customer orders.” - Quidel Q2 2021 10-Q SEC filing
“Due to the significant uncertainty that exists relative to the duration and overall impact of the COVID-19 pandemic, our future operating performance, particularly in the short-term, may be subject to volatility. In this regard, we continue to see challenges posed by the pandemic to global transportation channels and other aspects of our supply chain, including the cost and availability of raw materials. As noted above, the pandemic continues to impact demand for certain of our products. The U.S. and other governments may enact or use laws and regulations, such as the Defense Production Act or export restrictions, to ensure availability of needed COVID-19 testing and vaccination delivery devices. Any such action may impact our global supply chain network.” - Becton, Dickinson and Company (BD) Q2 2021 10-Q SEC filing
Further, as manufacturers began securing EUAs for their at-home diagnostics, the pandemic appeared to be shifting, at least domestically. Vaccines were becoming more widely available, soon places of business and entertainment would start opening up, and the Delta variant had not yet taken hold in the United States. However, the landscape quickly reversed as vaccination rates stagnated and the more infectious Delta variant become the dominant strain in the U.S., resulting in increased cases, hospitalizations, and deaths. Investor calls and SEC filings by manufactures regarding testing overall, as well as home testing specifically, discussed this uncertainty, noting how an inability to predict the arc of the pandemic made assessing future testing demand difficult.
“Our financial performance and results of operations will depend on future developments and other factors that are highly uncertain, continuously evolving and cannot be predicted, including the duration of the COVID-19 outbreak, the severity and continuation of outbreak surges, actions to contain the spread of the virus such as mask wearing, social distancing and vaccination efforts globally, and the impact of these and other factors on testing demand.” – Quidel Q2 2021 10-Q SEC filing
“The real… factor here becomes COVID testing...that’s really the question here. How will testing play itself out in the second half here whether its variants, whether its vaccination rates, etc so that’s just something we are paying attention to…that’s why our guidance rage was pretty wide, to really account for that.” – Abbott Q2 2021 earning call
Indeed, Abbott’s decision to pull back on COVID-19 test production leading into the summer has been widely publicized and SEC filings indicate that this was related, at least in part, to a belief that the course of the pandemic had shifted and there was a reduced need for tests.
“On May 27, 2021, Abbott management approved a restructuring plan related to its Diagnostic Products segment to align its manufacturing network for COVID-19 diagnostic tests with changes in projected testing demand driven by several factors, including significant reductions in cases in the U.S. and other major developed countries, the accelerated rollout of COVID-19 vaccines globally and the U.S. health authority’s updated guidance on testing for fully vaccinated individuals.” - Abbott Q2 2021 10-Q SEC filing
As a result, by the time the demand for rapid home tests began to increase, due to rising cases, hospitalizations and deaths, re-opening workplaces, and the return to in-person schooling for millions of elementary school students, the supply was not there. The new federal ITAP effort is designed to help increase supply by seeking additional manufacturers to bring tests to the U.S, market and could help to address some of these barriers.
Federal Investment
The lack of up-front federal investment in testing, including advance purchasing of tests, is another factor that appears to have impacted testing availability and affordability. Whereas the federal government channeled billions of dollars into accelerating vaccine development and advance purchasing of millions of doses, which helped to mitigate manufacturer risk and allowed for vaccines to be provided at no cost to all in the United States, no similar strategy was undertaken for testing. Without such up-front investment, the risk and cost of scale up was largely placed on manufacturers, who might be reticent to do so in the face of uncertainty given their fiduciary responsibility to shareholders. As noted, this differs from the experience in the UK and Germany where governments simultaneously supported vaccination and home testing efforts.
The Biden Administration’s use of the DPA in September to spur more domestic production of rapid tests and its procurement of additional rapid tests injected new investments in this area. Since then, HHS announced contracts with Abbott, Celltrion, OraSure, Quidel, and Acon Laboratories. And, on October 6, 2021, the White House committed another $1 billion towards rapid tests to “further mobilize testing manufacturers…to expand production of tests…based on the United States government’s commitment to procure an additional 180 million rapid tests over the course of the next year.” Much of these new procurements will provide free and increased rapid testing to community sites and long-term care facilities, designed to reach high needs populations in specific settings, but not necessarily increase supply for consumers.
As mentioned above, this additional investment is expected to result in a supply of 200 million rapid antigen tests per month by December, and 300 million by February 2022. Some experts recommend, however, that rapid antigen testing be conducted once twice or even three times per week to optimally help to identify those who are infectious and interrupt onward transmission. In response to a recent study, an NIH official stated that “Rapid antigen testing at home, two to three times per week, is a powerful and convenient way for individuals to screen for COVID-19 infection,” further noting that “With schools and businesses reopening, an individual’s risk of infection can change from day to day. Serial antigen testing can help people manage this risk and quickly take action to prevent spread of the virus.” Indeed, many colleges and universities have adopted this approach to curb spread. Yet, the new U.S. investment, even if resulting in 300 million rapid tests per month, would be less than one test per month per person in the U.S. For two times per week testing, it would cover less than 40 million individuals. If everyone older than 11 were tested twice per week per the UK’s recommendation, we would need 2.3 billion tests per month. If just half the U.S. population tested weekly, that would translate to a need for more than 150 million tests per week, around 600 million per month. The recent announcement of the new federal ITAP effort invests an additional $70 million and could help to increase supply in the U.S. market, though how quickly is uncertain.
Federal Guidance and Messaging
One other challenge has been federal messaging and changing guidance related to the role of testing as part of the U.S. COVID-19 response over the course of the pandemic. This included mixed messages and changing recommendations during the Trump administration, including down-playing of the importance of testing and shifting guidance from the CDC during vaccine roll-out.
Before vaccine roll-out, in late 2020 CDC’s testing guidance was that “people who have had close contact (within 6 feet for a total of 15 minutes or more) with someone with confirmed COVID-19” should get tested. Then, as of March 17th 2021, when vaccines were starting to become more widely available to all adults in the United States, case rates were down, and Delta had not yet taken hold, CDC stated that “fully vaccinated people with no COVID-19 symptoms do not need to be tested following an exposure to someone with COVID-19.” Just a few months later, however, in early August 2021, the CDC again changed its guidance to recommend testing for fully vaccinated people following exposure: “fully vaccinated people should be tested 3-5 days following a known exposure to someone with suspected or confirmed COVID-19.” While this shift in messaging was responding to a rapidly changing pandemic and new evidence on an emerging and evolving disease, industry communications indicate that it had an impact on manufacturing:
“While we expect to close more accounts with employers and have several promising partnerships in the pipeline, they involve a good deal of blocking and tackling and are very hard to predict or value especially when guidance from CDC and the landscape of COVID testing seem to evolve daily. Recently the warning from public health officials that vaccinated people can become infected and spread the highly contagious delta variant of COVID-19 appears to be a near term driver for more masking and testing especially as schools and office look to reopen in the fall.” – Quidel Q2 2021 investor call
And as noted above:
“…changes in projected testing demand [are] driven by several factors, including significant reductions in cases in the U.S. and other major developed countries, the accelerated rollout of COVID-19 vaccines globally and the U.S. health authority’s updated guidance on testing for fully vaccinated individuals.” - Abbott Q2 2021 10-Q SEC filing
Beyond impact on industry, shifting messaging could have affected public understanding of testing and confidence in agency recommendations. More broadly, the CDC has provided limited guidance on the role of home or routine testing, as a public health tool in addressing the pandemic and how it may differ from testing in other settings. Guidance on preventing COVID-19 has focused on vaccination and the CDC page on COVID-19 testing is aimed at those who are at risk for infection, symptomatic or are traveling with no information on testing routinely or as a public health practice. In the How to Protect Yourself and Others factsheet (last updated in August 2021), there is no mention of how testing may be a tool in the pandemic response. Similarly, the home testing page focuses on testing among those who may be at risk for having COVID-19, and suggests that home testing may be something to pursue if you cannot get tested by a provider: “If you need to be tested for COVID-19 and can’t get tested by a healthcare provider, you can consider using either a self-collection kit or a self-test that can be performed at home or anywhere else.” CDC guidance on testing in schools and workplaces is more comprehensive in its discussion of tests as a public health or screening tools but is limited to those settings. The limited information on home tests and little explanation of their role as a public health tool for home use may impact public understanding of home testing and willingness to use rapid test kits. However, a recent FDA press release for a newly authorized home antigen test states that the agency “considers at-home COVID-19 diagnostic tests to be a high priority and we have continued to prioritize their review given their public health importance.”
Cost and Insurance Coverage Considerations
Cost may also be a barrier to accessing OTC rapid home tests. Domestically available OTC tests typically range from $14 for two tests, or $7 per test, to $38.99 per test.1 If a consumer wanted to test regularly, even the least expensive test ($14 for two tests) used twice a week would amount to $728 per year, assuming they could get tests in this quantity. The more typical (non-discounted) price would cost an individual more than $1,000 per year, and the most expensive test used twice a week would amount to over $4,000 per year. Elsewhere, outside the U.S., home tests are about a dollar and in some cases, like in the UK, Israel, and Singapore, free to all or many people.
While federal COVID-19 legislation ensures that a range of tests are available free of charge through insurance, federal guidance indicates that home tests are only required to be covered if “ordered by an attending health care provider who has determined that the test is medically appropriate for the individual based on current accepted standards of medical practice and the test otherwise meets the statutory criteria.” Further, if OTC home tests were covered by commercial insurance, it could be logistically cumbersome for an individual testing regularly to seek reimbursement each time.
The new ITAP aims to bring more tests to market which could increase competition and decrease costs. In addition, the revisions to the FDA pathway to allow for the sale of certain single use, rather than serial, tests could decrease the purchase price for some consumers. However, the real impact of these changes is yet to be realized.
Finally, even if supply problems are solved, cost could remain a barrier for some. Unless there is widespread scale up with multiple access points and free or truly inexpensive tests, disparities in terms of diagnosis and community transmission that already exist could be exacerbated. Some of these issues may be alleviated by recent federal investments to provide free rapid testing to certain community sites but that has yet to be proven.
Looking Ahead
Taken together, there are multiple interrelated factors that have contributed to the lack of availability of rapid home tests in the U.S., including the regulatory framework, supply chain and demand issues, federal investment, federal messaging, and affordability. Recent actions by the Biden administration are likely to help alleviate some of these challenges though it is not yet clear if they can fully resolve the issues. Even if scale-up hits the projected increase in supply to 300 million rapid tests per month by early next year, this would translate into less than one test per individual per month, not enough to test most people weekly as some recommend. Additionally, even with scale up and more widespread retail availability, cost will likely persist as a barrier for many people, and could run the risk of exacerbating existing inequities in the pandemic. It will also be important to monitor whether the growing vaccination or testing requirements from employers and other places of business/entertainment will generate more demand for tests and stress the already limited supply. As has been the case since the early days of the pandemic, the future of COVID-19 in the United States, from case load to vaccination to testing is hard to predict. More widespread use of testing, and home testing in particular, could help to address the pandemic in the face of ongoing uncertainty.
Endnotes
Prices come from searches for OTC COVID tests conducted twice a day over a week period (between September 21 and 27, 2021) on Amazon, Walgreens, CVS, Kroger, Target, and Walmart websites. ↩︎
Preventable rehospitalization of the nation’s older adults has proved a persistent health and financial challenge for the U.S., costing Medicare hundreds of millions of dollars each year. Various analyses have found many readmissions within a month of discharge might have been avoided through better care and more attention paid to the patients after they left the hospital. The federal government’s campaign to reduce the frequency of these readmissions by applying financial disincentives has entered its 10th year with Medicare’s decision to lower payments to 2,499 hospitals throughout the current fiscal year, which began last month and runs through September 2022.
The Hospital Readmissions Reductions Program (HRRP), created as part of the Affordable Care Act, punishes general acute-care hospitals when more Medicare patients return for a new admission within 30 days of discharge than the government decides is appropriate. The average penalty this fiscal year is 0.64%, with 39 hospitals losing the maximum of 3% of reimbursements.
Over the lifetime of the program, 2,920 hospitals have been penalized at least once. That’s 93% of the 3,139 general acute hospitals subject to HRRP evaluation, and 55% of all hospitals. Moreover, 1,288 have been punished in all 10 years. Only 219 eligible hospitals have avoided any payment reductions since the program’s start in 2013, though more than 2,000 hospitals are automatically exempt from penalties because they have specialized functions: those that focus on children, psychiatric patients, veterans, rehabilitation and long-term care or those that serve as the only hospital in an area.
Hospital readmissions have become less frequent since before the ACA was enacted, and most experts attribute that partly to the financial threat of the penalties, though other factors likely contributed to the improvements. Less debatable is that the penalties have saved the government billions of dollars since their inception. The Centers for Medicare & Medicaid Services estimates that because of the HRRP, Medicare will keep an extra $521 million this fiscal year. You can look up individual hospital penalties using KHN’s interactive tool.
Recent policy attention has focused on closing the coverage gap for roughly 2.2 million individuals living in the 12 states that have not adopted Medicaid expansion included in the Affordable Care Act (ACA). These individuals do not qualify for Medicaid and have incomes below poverty, making them ineligible for premium subsidies in the ACA Marketplace. Pending federal legislation may temporarily provide coverage to individuals in the coverage gap, but providing a permanent pathway to coverage may fall back to the states in the long-term.
The Build Back Better Act currently pending in Congress includes a provision to close the Medicaid coverage gap for three years. From January 1, 2022 through December 31, 2025, individuals in the coverage gap residing in nonexpansion states would become eligible for subsidies for coverage in the Marketplace. They would qualify for a full premium subsidy for a benchmark plan and for a cost-sharing reduction that gives them access to plans with an actuarial value of 99% (which means the cost-sharing paid by patients would average just 1% of expenses). The legislation would also increase the federal matching assistance percentage (FMAP) from 90% to 93% for the expansion population from 2023 through 2025 to help ensure that states that have already implemented expansion maintain coverage. In addition, the legislation includes provisions to phase out the current continuous coverage requirements under the public health emergency, but includes a 3.1 percentage point reduction in a states’ FMAP if a state restricts eligibility (including but not limited to expansion coverage) through December 2025.
Although the Build Back Better Act would expire after 2025, states that newly implement Medicaid expansion will have the option to receive a temporary fiscal incentive under the American Rescue Plan Act (ARPA). Under the ACA, the federal government pays for 90% of the costs for the expansion group. However, under ARPA which was enacted in March 2021, new expansion states would be eligible for an additional 5 percentage point increase in the state’s traditional match rate for two years if they implement the expansion at any time. The traditional FMAP applies to most services for non-expansion groups. Since this group is much larger than a state’s expansion population, states would benefit from additional funds for a large share of their Medicaid program. A KFF analysis also shows that all non-expansion states would see a net fiscal benefit for two years by newly expanding.
The ARPA federal incentive reignited discussion around Medicaid expansion in a few non-expansion states during the last state legislative session. While no state newly adopted expansion after the ARPA incentive was enacted, a number of states debated expansion and could come back to these debates when the federal coverage for those in the gap expires or at any time before that. Such action could depend on state politics (who is governor and what party controls the state legislature) as well as thoughts about tradeoffs with a short term federal fix versus an expansion program that is designated by the state. Recent activity around Medicaid expansion included activity in the following states:
In March 2021, Wyoming legislators introduced a Medicaid expansion bill recognizing the ARPA incentive. The bill passed the House but subsequently failed in a Senate committee by a slim margin – the furthest advance of Medicaid expansion legislation in the state.
Three states – Wisconsin, Kansas, and North Carolina– have Democratic governors that reintroduced Medicaid expansion proposals this year after failed attempts in prior years. Efforts did not advance in Republican-controlled legislatures, although as of November 1, 2021 the budget and the issue of Medicaid expansion are in flux in North Carolina.
Lawmakers in Texas introduced (but did not advance) Medicaid expansion proposals in the 2021 legislative session, with some bipartisan support. For example, there was legislation to place Medicaid expansion on the ballot as a constitutional amendment and other legislation to implement Medicaid expansion via Section 1115 authority, with premium requirements and healthy behaviors incentives.
Prior to ARPA, advocates in several states have considered expanding Medicaid through a voter-driven ballot initiative process. Efforts are on-going in South Dakota, but efforts in Mississippi were suspended and an initiative in Florida was delayed. Both Oklahoma and Missouri adopted expansion via ballot initiative last summer. Oklahoma implemented expansion on July 1, 2021. In Missouri, the path to implementation faced roadblocks but ultimately the state began processing Medicaid expansion applications on October 1.
For now, it seems like action to fully address the coverage gap will likely depend on federal action, but longer-term coverage may fall back to the states. If enacted, the Build Back Better legislation would provide a coverage option for the 2.2 million living in nonexpansion states who fall into the coverage gap. The plan would expand health coverage and promote racial equity. As the plan would only be available through 2025, the decision may fall into the hands of states again where they can choose to implement expansion and receive the temporary fiscal incentive under ARPA, or to Congress where they can choose to renew the federal proposal.
On October 4, 2021, the Biden Administration released new final regulations for the federal Title X family planning program. The new regulations replace those issued by the Trump Administration in 2019, which made significant and well documented changes to the Title X program leading to a significant reduction in the size of the Title X network and the number of low-income and uninsured clients served by the program. This brief presents new state-level data on the status of the Title X network on the eve of the implementation of the new regulations and summarizes the impact of Trump era regulations on the number of clients served and status of participation by clinics across the country.
The Impact of the 2019 Trump Regulations
The 2019 Trump Administration regulations substantially diminished the Title X family planning network by disqualifying family planning clinics with co-located abortion services and disallowing the provision of abortion referrals to clients that wanted them. In its 2020 Family Planning Annual Report, the federal Office of Population Affairs (OPA) documented the impact of both the Trump Administration’s regulations and the pandemic on the number of clients they served, as well as the change in the number of grantees and clinic sites from 2018 to 2020 (Table 1). In this two-year period, the number of clients served fell from 3.9 million to 1.5 million people. The report estimated that the Trump Administration’s final rule accounted for nearly two-thirds (63%) of the precipitous reduction in the number of family planning clients served while the COVID-19 pandemic accounted for one third of the falloff (Figure 1).
Table 1: Changes in the Title X Network from 2018 to 2020
2018
2019
2020
Clients served
3.9 million
3.1 million
1.5 million
Family planning visits
6.5 million
4.7 million
2.7 million
Grantees (receive funding from HHS OPA)
99
100
75
Sub-recipients (receive funding from grantees and can distribute to clinic sites or provide services themselves)
1,128
1,060
867
Clinic sites (receive funding from grantees or sub-recipients)
With the large exodus of clinics from the Title X program in summer of 2019, there are still five states without any Title X funded clinic sites: Oregon, Washington, Vermont, Maine, and Hawaii, while New York currently has only two sub-recipient sites (Table 2). Another seven states, including New York, have Title X clinic networks that are currently operating at less than 25% of their original capacity. Based on our analysis of OPA’s Title X Family Planning Directories, 36 states have experienced a decrease in participating Title X clinics from June 2019 to August 2021, while OPA’s Family Planning Annual Reports between 2018 and 2020 show 49 states and DC have seen a reduction in clients ranging from 2%-100%, with a median reduction in clients of 52%.
A small number of entities have rejoined the Title X network in the past year. One of Utah’s two grantees, Utah Navajo Health System, rejoined the Title X program in July 2020 as a sub-recipient under Arizona’s grantee, Arizona Family Health Partnership. Maryland Department of Health rejoined the program in October 2020 after the State of Maryland was granted a permanent injunction against enforcing the 2019 Title X Final Rule. Most of the Planned Parenthood clinics left the Title X Program after the Trump Administration’s Rule became final though few are now in the program, including those in Maryland, Washington D.C., and Missouri.
The Trump Administration Final Rule allowed “non-traditional” Title X grantees to join the network and some of these grantees are no longer part of the program under the Biden Administration. The Trump Administration regulations extended federal family planning funds to organizations that only offered their clients fertility awareness or abstinence options. The new regulations do not qualify them to participate as grantees if they do not offer a broader range of contraception methods to their clients. Notably, the Obria Group, Inc., a Christian organization based in Southern California that did not provide contraceptive services based on religious objections to hormonal contraception, left the Title X program in April 2021. Another Christian-based organization, Beacon Christian Community Health Center, which joined the Title X network as a New York grantee in October 2018, left the Title X program in April 2021 as well. Two of the three new Title X grantees that joined the Title X program under the Trump Administration that are not religiously based, City of El Paso in Texas and Osceola Community Health Services in Florida, remain in the program.
Key Aspects of the Final Biden Administration’s Title X Regulations
The new Biden regulations restore many aspects of the program that were removed through the Trump Administration regulations, including:
Allowing co-located abortion services and abortion referrals
Requiring clinics that are not able to provide clients with a broad range of family planning methods to provide a prescription or referral to the client if requested
Added confidentiality protections for adolescents— clinics may not require consent of a parent or guardian for the provision of services and cannot notify a parent or guardian before or after provision of any services
The regulations have also added new provisions to the program, including:
Adding telehealth as an option for providing medical services in addition to in-person care
Requiring family planning projects to provide services in a matter that is client-centered, culturally and linguistically appropriate, inclusive, and trauma-informed; protects the dignity of the individual; and ensure equitable and quality service delivery consistent with a nationally recognized standard of care
Adding a new funding criterion - the ability of the applicant to advance health equity
The final rules will be effective November 8, 2021, and clinics will once again be able to provide their clients with the care that meets the quality standards established by the CDC and OPA, including providing non-directive pregnancy options counseling with referrals for prenatal care, adoption services, or abortion services and confidential services for adolescents, but it will take time to restore the network of providers. On October 25, 2021, the state of Ohio, joined by 11 other states (AL, AZ, AK, FL, KS, KY, MO, NE, OK, SC, WV), filed a lawsuit in the US District Court for the Southern District of Ohio against HHS to block the implementation of the Biden Administration’s regulations. These states claim the final regulations violate Section 1008 of the Public Health Service Act that says none of the funds appropriated under Title X can be used in programs where abortion is a method of family planning. The litigants claim that by reinstating the regulations that allow co-located abortion services and require participating providers to offer referrals for abortions to clients who seek them, that HHS is not in compliance with the intent of the law. The States are requesting a ruling as soon as practicable and no later than December 31, 2021. If the Court does not rule before November 8th, the Biden regulations will become effective.
If the final regulations remain in effect, additional funding that can be extended to grantees that left the network is not anticipated until Spring of 2022 after the grant applications due January 11, 2022 are reviewed and approved. Funding will likely be awarded by April 1, 2022. Grantees that are still part of the Title X program can bring clinics back into their network if they have current funding available. Current grantees’ three-year grant cycle ends March 31, 2022.
In response to Texas’ S.B. 8 law banning most abortions, HHS will award additional funding to Texas’ largest Title X grantee to meet an increased demand for emergency contraception and family planning services. OPA is also planning to award an additional $10 million through a new funding opportunity entitled “Funding to Address Dire Need for Family Planning Services” that will provide grants to Title X entities that can demonstrate a need for additional funding for family planning services due to either an influx of clients as a result of Texas’ S.B. 8 abortion ban or some other reason. A second funding opportunity that OPA is planning on releasing will provide $45 million in Spring 2022 to Title X grantees to expand and enhance their telehealth infrastructure and capacity, which will be particularly important given the ongoing COVID-19 pandemic and increased demand for telehealth services.
Looking Forward
The final Biden Administration Title X regulations will make significant changes to sites across the nation and allow clinics like Planned Parenthood, which were formerly disqualified because they have co-located abortion services or provide abortion referrals for individuals who want them, to once again apply for federal support to provide family planning services to low-income and uninsured individuals. These regulations are being challenged by several states by litigation that could take years to resolve. If fully implemented, however, the real impact of the revised regulations will be when federal funds become available to grantees and clinics to rejoin the program and allow more low-income people to receive health services from Title X sites. While many grantees and clinics that left the network are anticipated to resume participation in the safety net program, it remains to be seen whether all those grantees and providers that left the program will apply to return. Some were able to obtain state-level funding to bridge the loss of federal support. These decisions will likely depend on whether states will continue to subsidize their family planning providers or whether additional federal funds will be needed to maintain and strengthen state family planning networks and services in communities that have historically been served by these providers.