The Unwinding of Medicaid Continuous Enrollment: Knowledge and Experiences of Enrollees
Findings
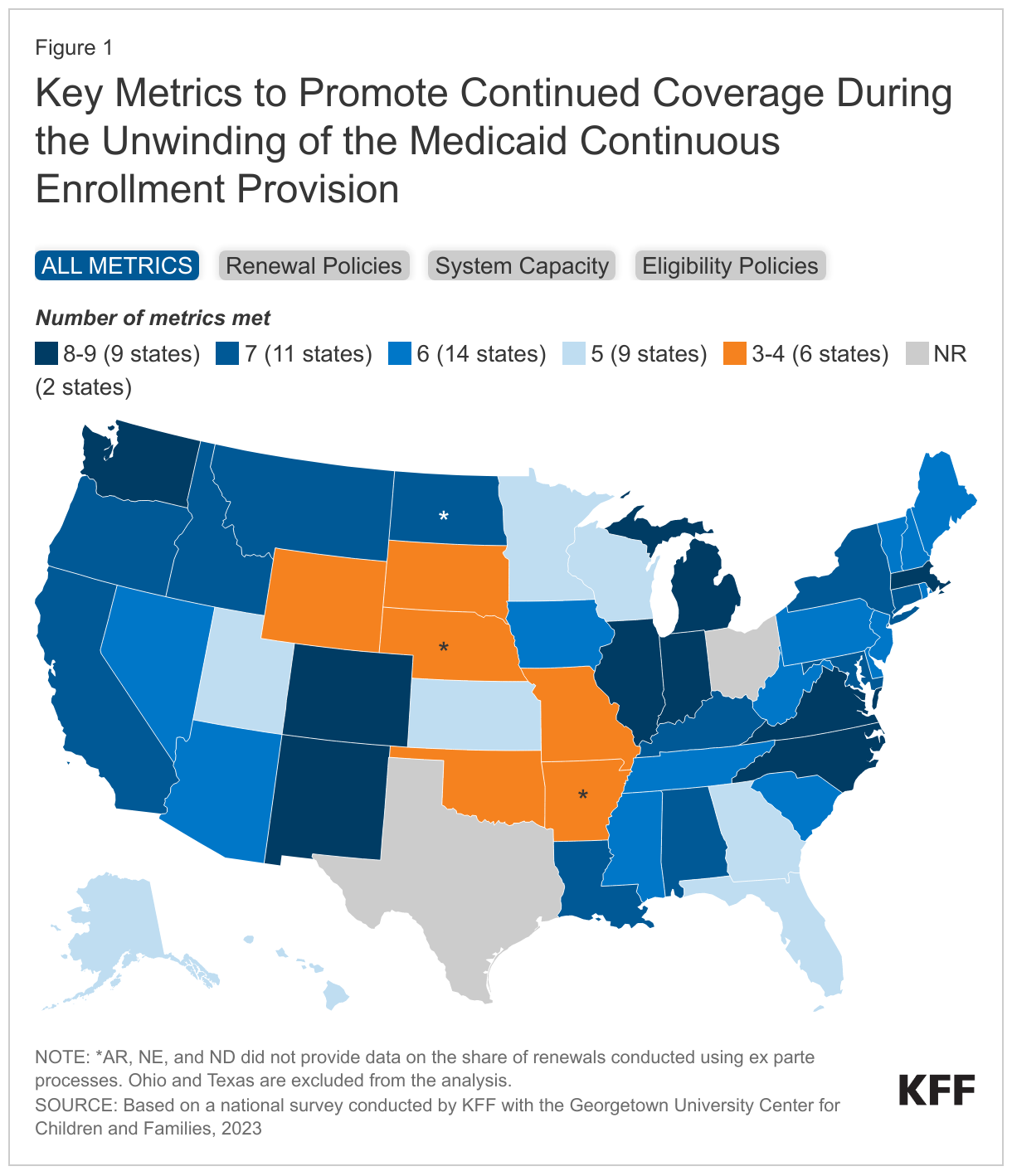
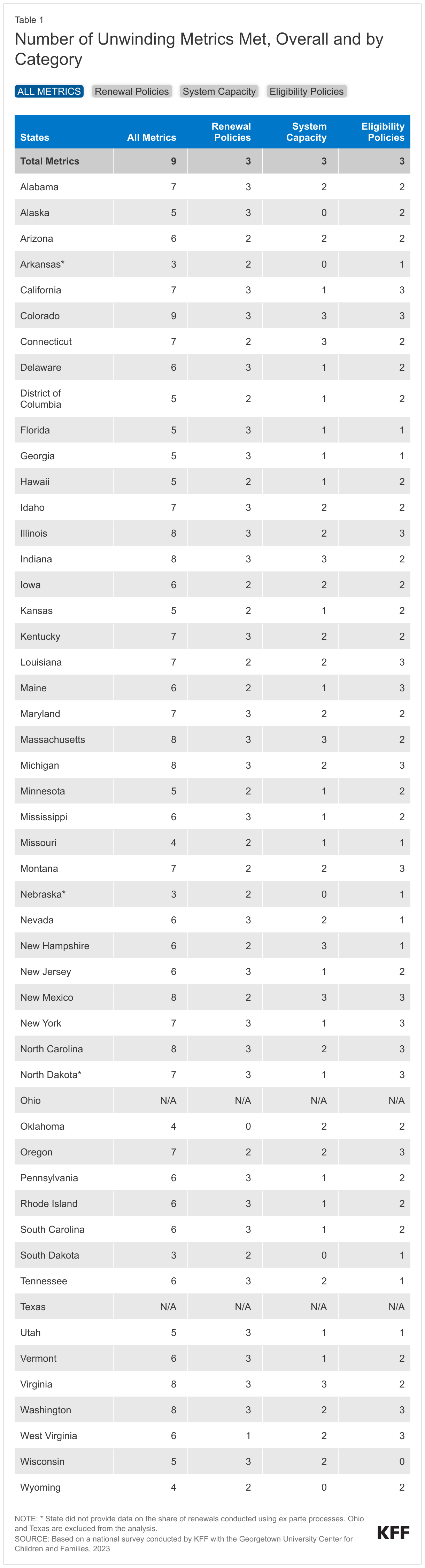
During the COVID-19 pandemic, states kept people continuously enrolled in Medicaid in exchange for enhanced federal funding. Continuous enrollment in Medicaid ended on March 31, 2023, and over the coming months, states will redetermine eligibility for people enrolled in Medicaid and will disenroll those who are either no longer eligible or who are unable to complete the renewal process. This brief gauges Medicaid enrollees’ knowledge of and preparedness for the Medicaid renewal process and possible disenrollment from the program, based on early findings from KFF’s new Survey of Health Insurance Consumers, fielded February 21 through March 14, 2023.
Key Findings
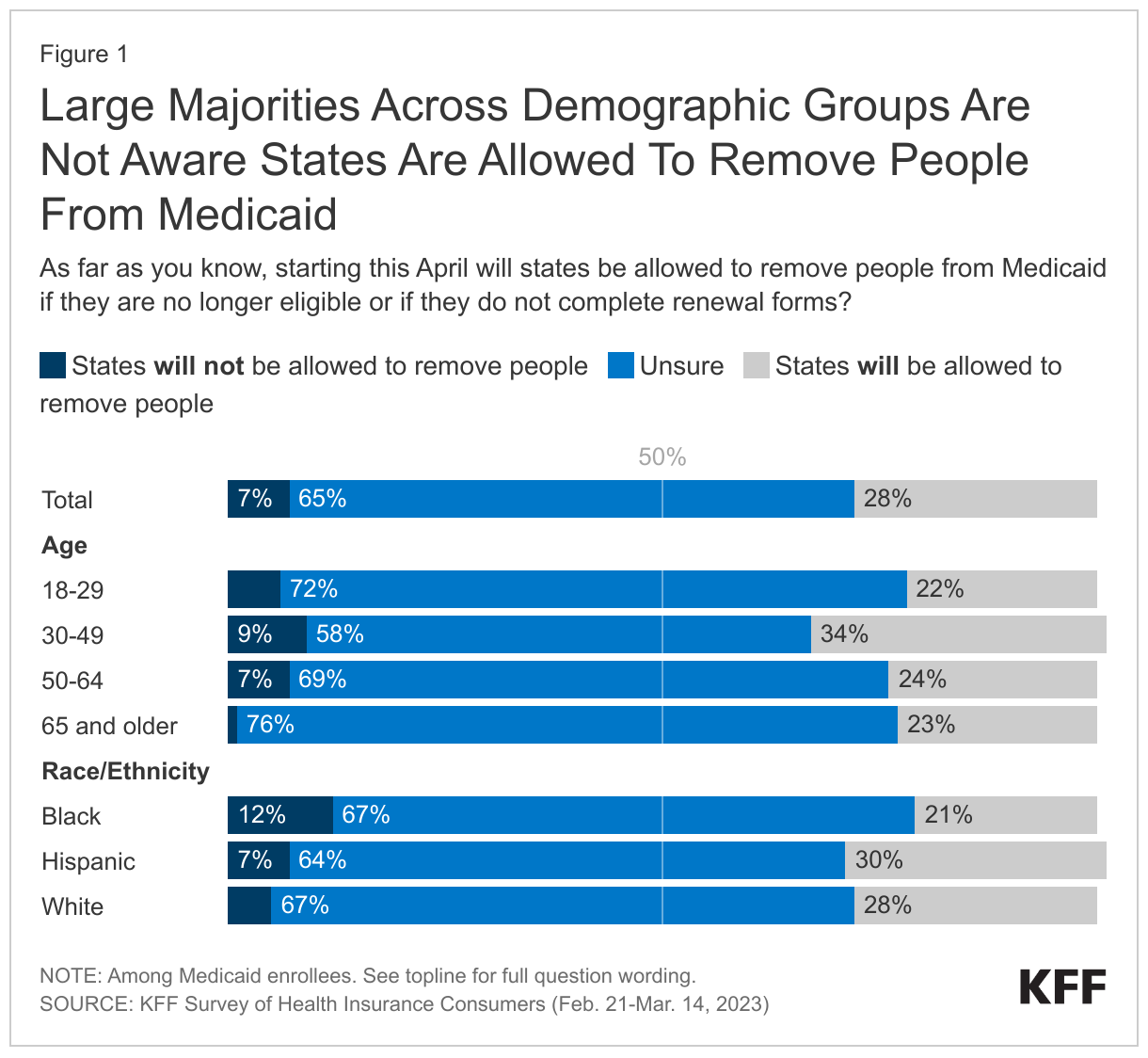
Most Medicaid enrollees were not aware that states are now permitted to resume disenrolling people from the Medicaid program. Roughly two-thirds (65%) of all Medicaid enrollees say they are “not sure” if states are now allowed to remove people from Medicaid if they no longer meet the eligibility requirements or don’t complete the renewal process, with an additional 7% incorrectly saying states will not be allowed to do this. Three in four adults 65 and older say they are unsure if states are allowed to remove people from Medicaid, and Black adults are more likely than White adults to incorrectly say that states will not be allowed to do this. Just under three in ten (28%) overall are aware states are now allowed to remove people from Medicaid.
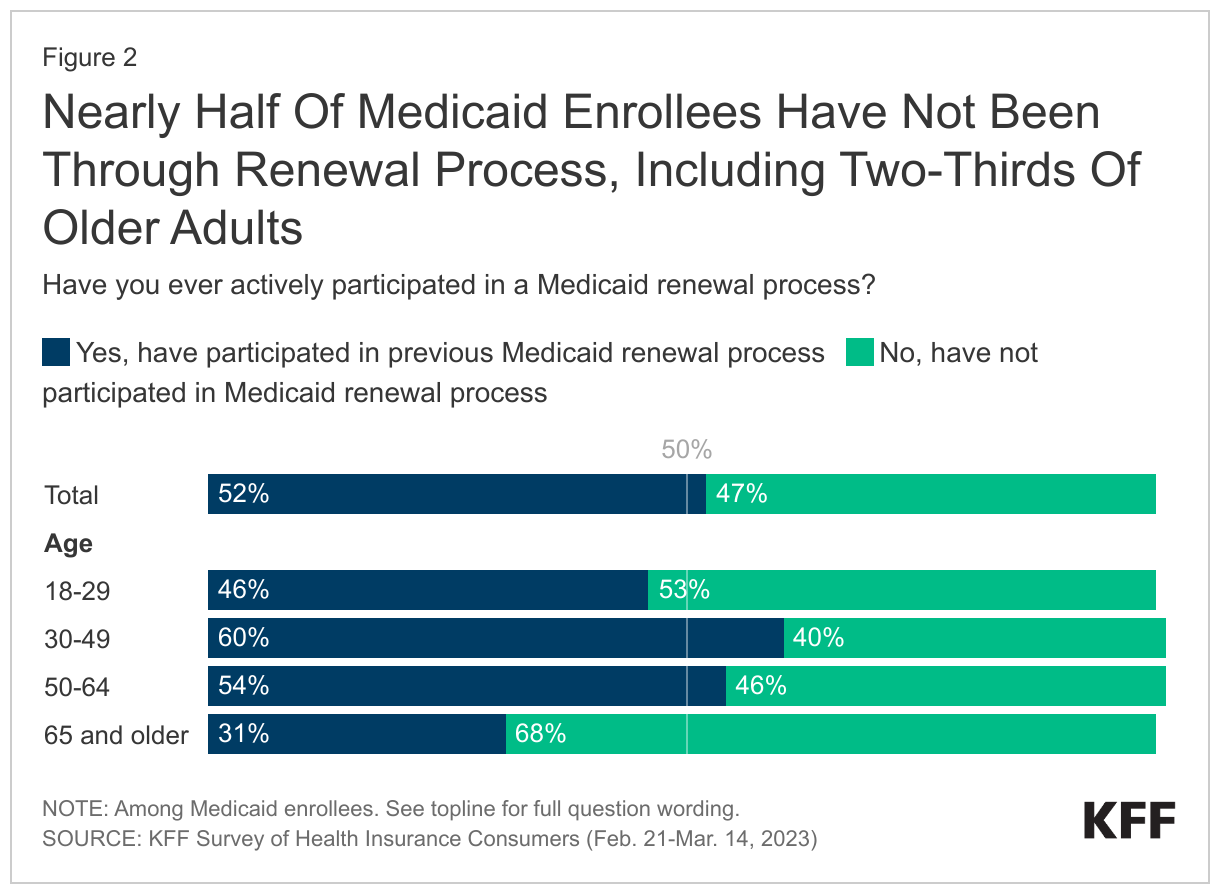
Nearly half of Medicaid enrollees say they have not previously been through the Medicaid renewal process. This includes two-thirds (68%) of Medicaid enrollees who are 65 and older and more than half of Medicaid enrollees who are between the ages of 18 and 29 (53%). Prior to the pandemic, Medicaid enrollees had their Medicaid coverage redetermined at least annually, and many lost coverage at renewal even though they remained eligible because they faced administrative barriers to completing the process. Some Medicaid enrollees may not be aware that their Medicaid coverage was renewed because the state was able to complete the process using available data sources, and therefore did not require the enrollee to take any action to maintain coverage. Having past experience with actively renewing Medicaid coverage can help enrollees prepare for what to expect when their eligibility is redetermined in the coming months and improve their ability to navigate and complete the renewal process.
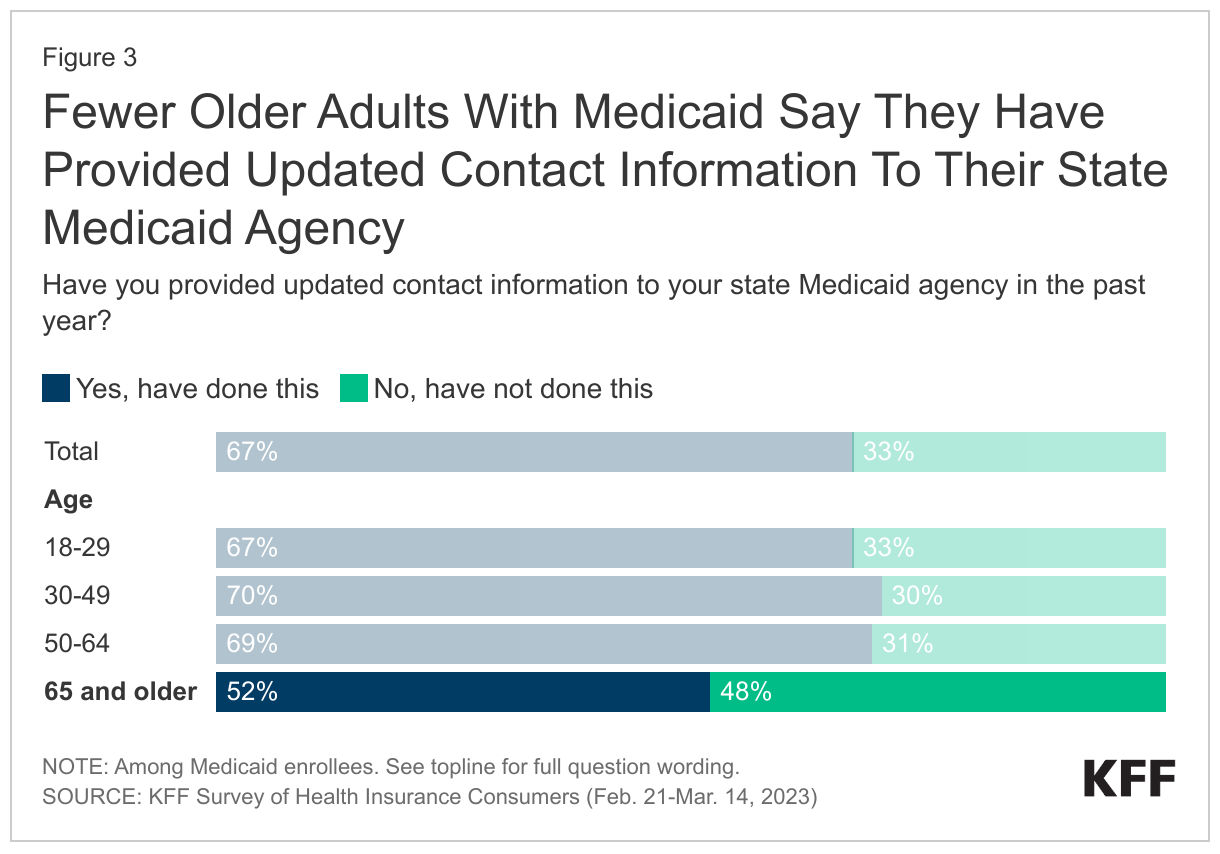
One-third of Medicaid enrollees say they have not provided updated contact information to their state Medicaid agency in the past year. States have taken several steps in the past year to encourage Medicaid enrollees to update their contact information to increase the likelihood that they receive renewal and other notices sent by the state. Two-thirds of Medicaid enrollees overall say they provided updated contact information to their state. Older adults are more likely than younger age groups to say they have not provided updated contact information to their state with about half (48%) of those 65 and older saying they have not done this, although older adults may have more stable contact information and consequently less need to report a change than other Medicaid enrollees. Older adults with Medicaid are also less likely to have either actively participated in a renewal process previously or provided updated contact information to their state Medicaid agencies. While one in five Medicaid enrollees overall haven’t done either of these things, the share increases to more than one-third (39%) of those 65 and older.
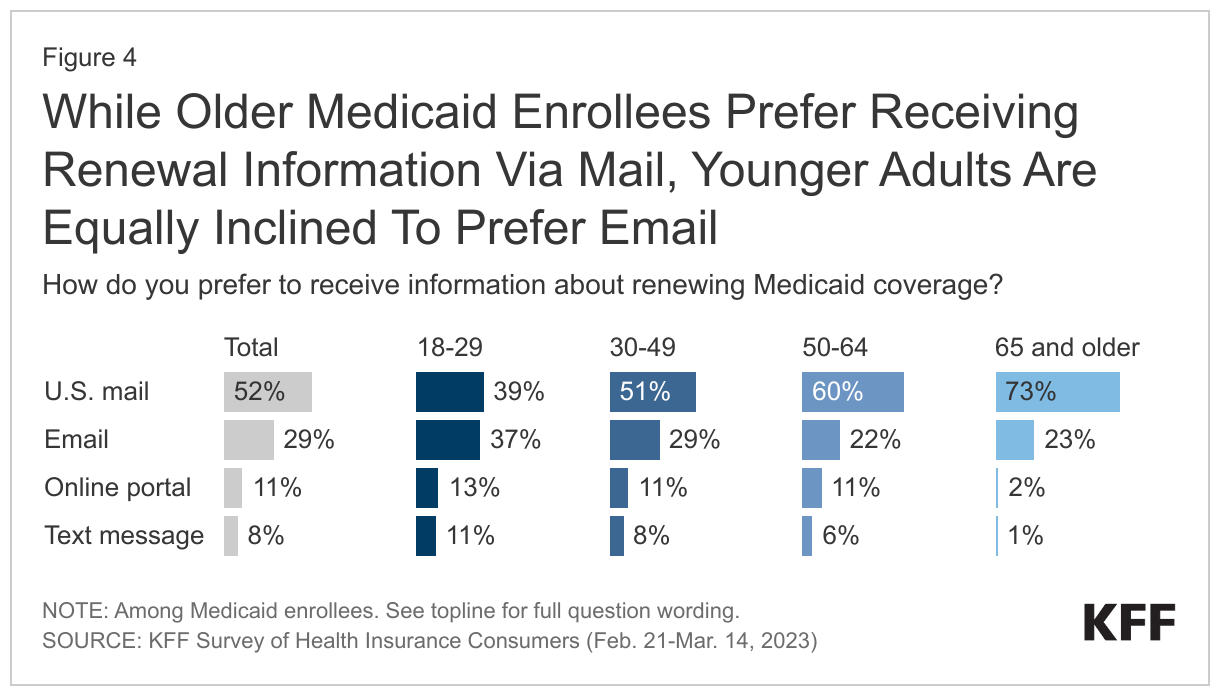
About half of Medicaid enrollees prefer to receive renewal information through modes other than the U.S. mail, such as email or via an online portal. While most state Medicaid agencies use the U.S. mail service as their primary method of communicating with Medicaid enrollees, many have taken steps to expand the ways in which they communicate with enrollees to include email and through online accounts. The survey finds that providing information to Medicaid enrollees through multiple methods can increase the chances that they receive the information. The U.S. mail is how about half (52%) of Medicaid enrollees say they would prefer to receive information about renewing Medicaid coverage, while three in ten (29%) say they prefer to receive information via email, and about one in ten say they prefer to get information through an online portal (11%) or via text message (8%). Three-fourths of older adults say they prefer to receive renewal information through the mail, but younger adults are equally likely to prefer receiving information through the U.S. mail (39%) as through email (37%). Even among younger enrollees, text is not a preferred communication method.
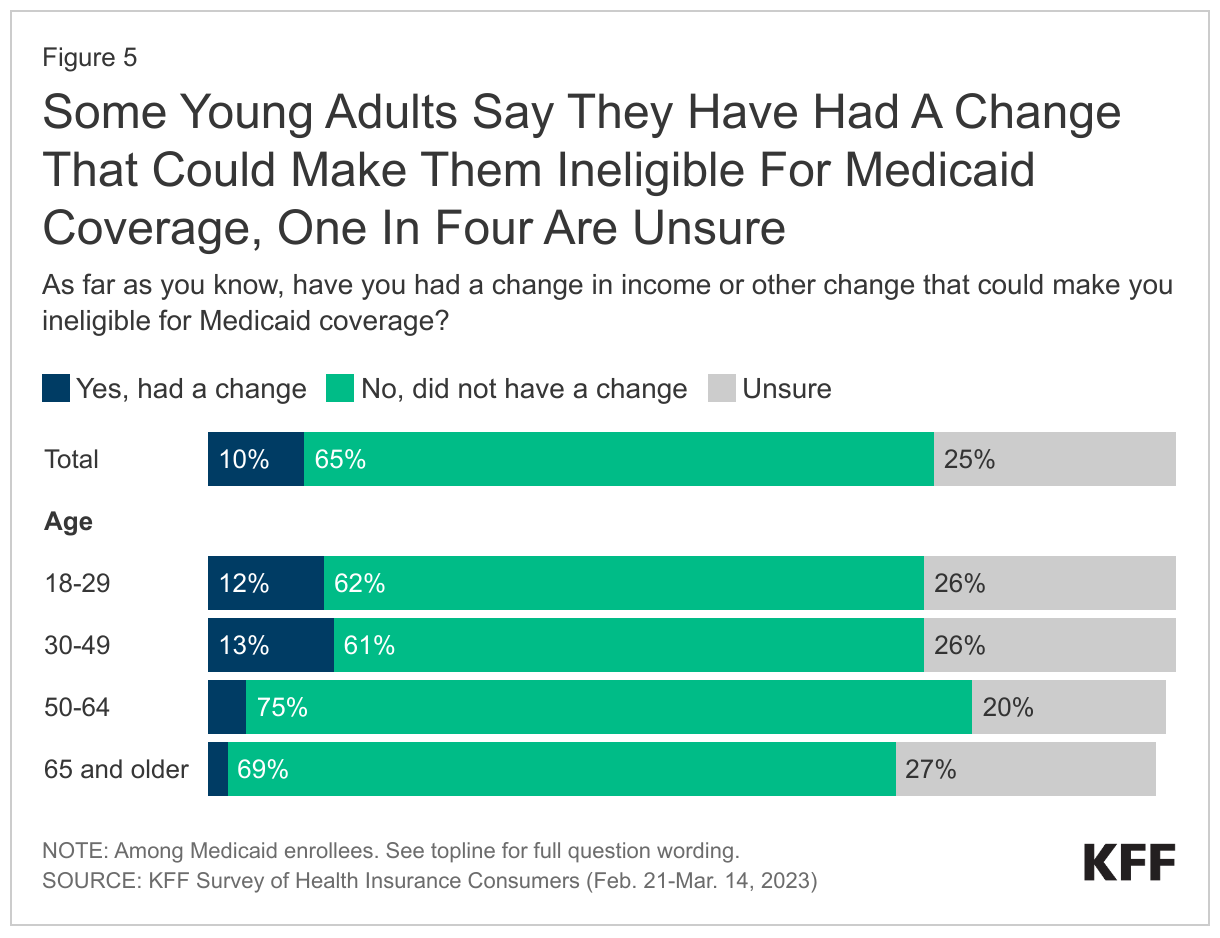
About one-third of Medicaid enrollees (35%) say they have had a change in income or other change that could now make them ineligible for Medicaid or are unsure if they have had such a change, but most enrollees say their circumstances have not changed, suggesting they are still eligible. Increases in income or another change in circumstance, such as a pregnant woman who completes her postpartum coverage period and no longer qualifies on the basis of pregnancy, can make people ineligible for Medicaid. If these types of changes occurred while Medicaid coverage was protected, individuals may no longer qualify when the state redetermines their eligibility in the coming months. One in ten Medicaid enrollees say they may have had such a change, and another 25% are not sure. However, enrollees who have not experienced a change that would make them ineligible may still be at risk of losing coverage if they are unable to complete the renewal process. Younger adults are more likely than their older counterparts to say they think they have had a change that would make them ineligible. About one in eight of 18–29-year-olds (12%) and 30-49-year-olds (13%) say they think they have had such a change, compared to very small shares of older adults (4% of those ages 50-64 and 2% of those ages 65 and older).
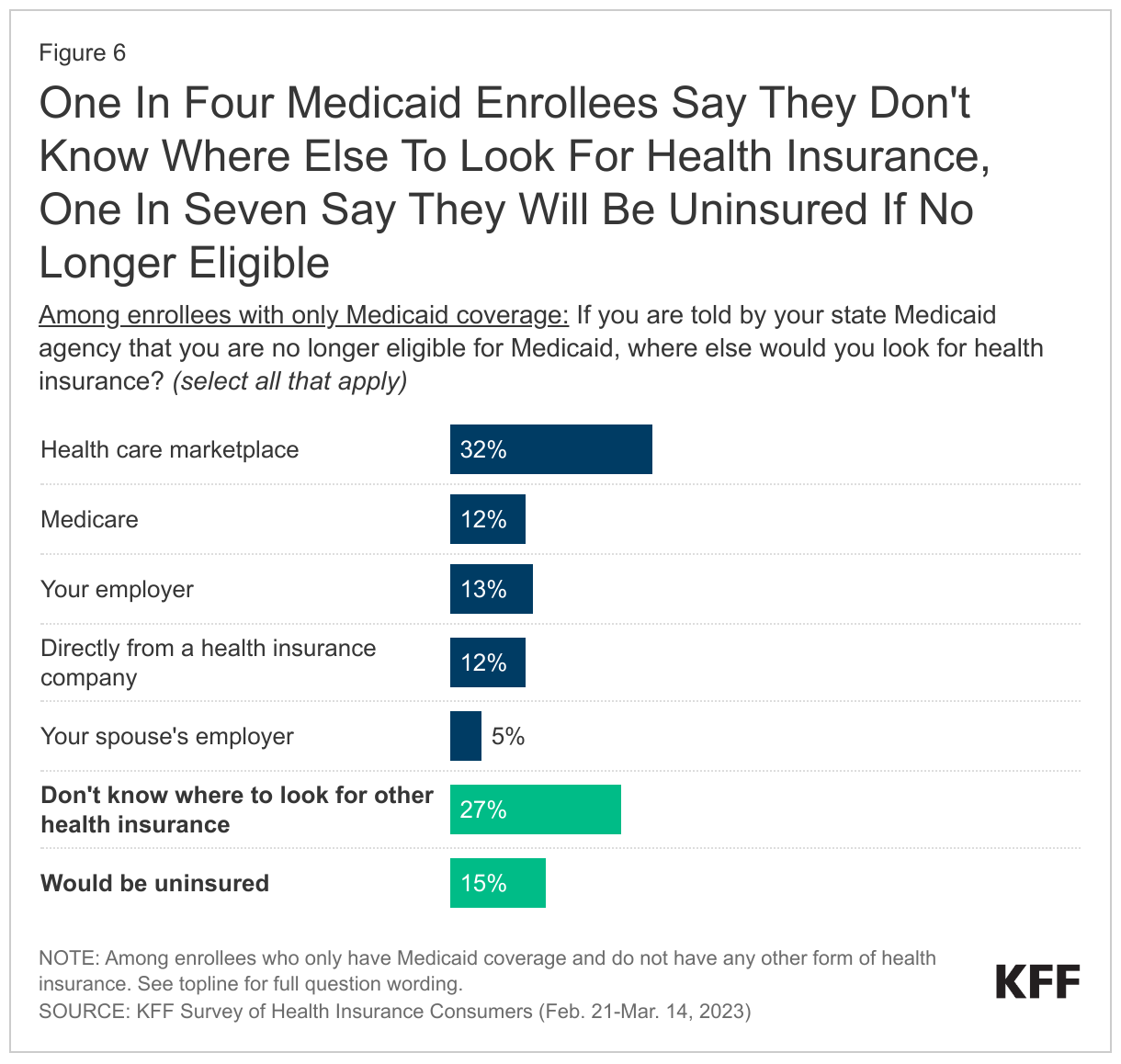
While about six in ten of those with Medicaid as their only source of coverage would look for coverage from other sources if they were told they were no longer eligible, over four in ten say they wouldn’t know where to look for other coverage or would be uninsured. Asked what they would do if informed by their state that they are no longer are eligible for Medicaid, about six in ten of those with Medicaid as their only source of coverage say they would look for coverage somewhere else including one-third (32%) who say they would look for coverage on the marketplaces, and one in eight who say they would look for coverage through their employer (13%), Medicare (12%), or directly from an insurance company (12%). About one in four adults (27%) with Medicaid as their only source of coverage say they wouldn’t know where to look for coverage if they were no longer eligible for Medicaid and an additional 15% say they would be uninsured.
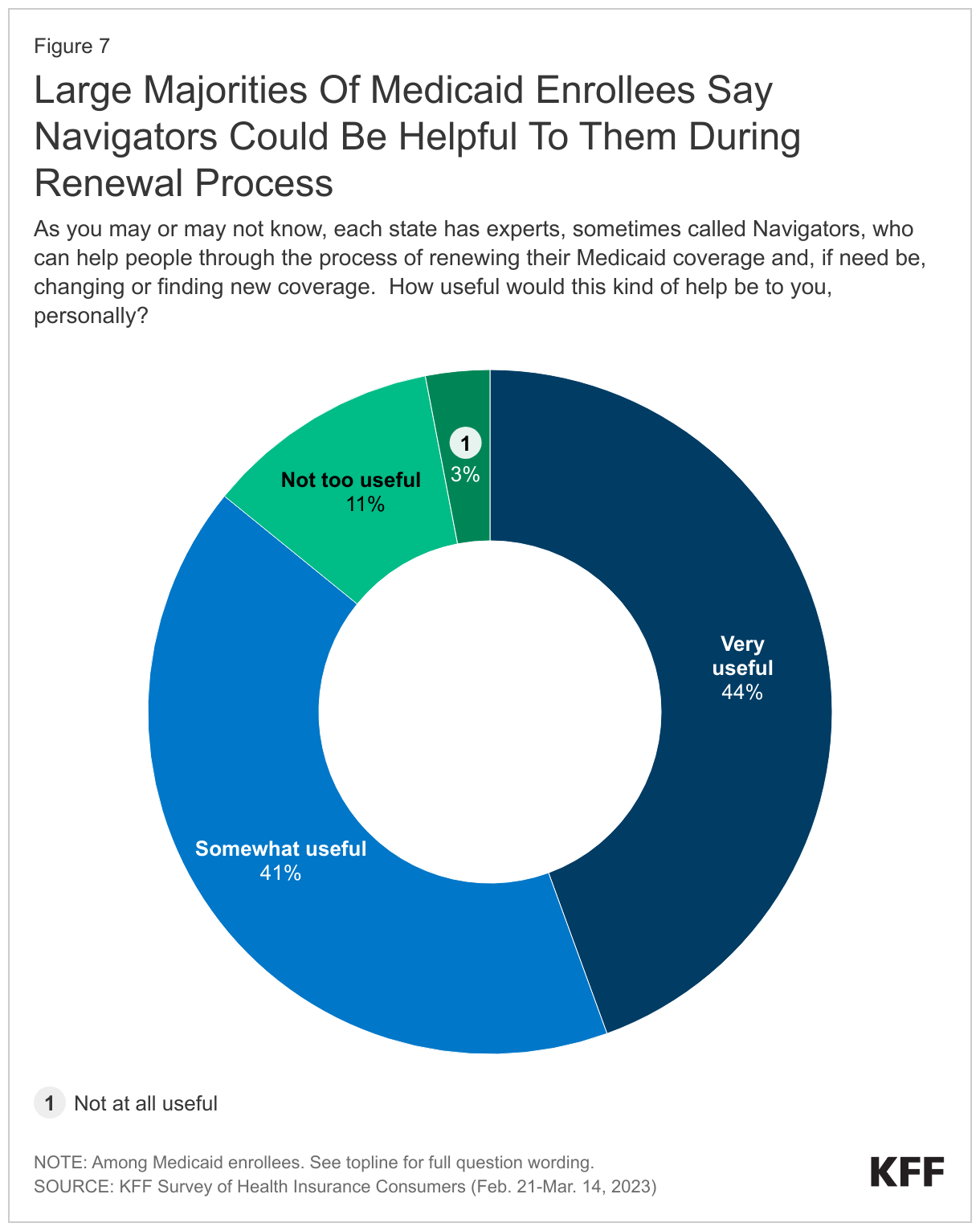
The large majority of Medicaid enrollees say having an expert help with the renewal process would be useful. As Medicaid enrollees begin the renewal process, nearly nine in ten say having a state expert to help them navigate the process of renewing their Medicaid coverage and looking for other coverage, if needed, would be at least “somewhat useful.” About four in ten (44%) Medicaid enrollees say having a navigator would be “very useful” in helping them with the renewal process with an additional four in ten (41%) saying it would be “somewhat useful.” About one in six either say it would be “not too useful” (11%) or “not at all useful” (3%).
Implications
As states resume disenrollments following the end of the Medicaid continuous enrollment provision, many Medicaid enrollees have been unaware of and may not be prepared for the coming changes, particularly older enrollees and enrollees ages 18-29. About half of enrollees say they have not completed a renewal process previously, so may not be on the lookout for renewal notices and may not be familiar with the steps they need to take to complete the process and maintain coverage if they remain eligible. While about half of Medicaid enrollees prefer to receive communications through modes other than the U.S. mail, some states continue to use the U.S. mail as the only method for sending notices. And, while only one in ten Medicaid enrollees say they have had a change that would likely make them ineligible for Medicaid, some are unsure, and many people are expected to fall through the cracks and lose coverage during the unwinding period even though they are still eligible. Engaging key stakeholders, including Medicaid managed care organizations (MCOs), Medicaid providers, and community-based organizations, in providing outreach to Medicaid enrollees, including targeted outreach to older adults, can raise awareness about the need to complete the renewal process. In addition, connecting people on Medicaid with Navigators and other organizations who can assist them with the renewal process can help increase the number of people who complete their renewals and retain coverage if they remain eligible or know where to look for and enroll in other coverage if they are determined to no longer be eligible.
Methodology
This KFF Survey of Health Insurance Consumers was designed and analyzed by public opinion researchers at KFF. The survey was designed to reach a representative sample of insured adults in the U.S. The survey was conducted February 21 – March 14, 2023, online and by telephone among a nationally representative sample of 3,605 U.S. adults who have employer sponsored insurance plans (978), Medicaid (815), Medicare (885), Marketplace plans (880), or a Military plan (47).
The sample includes 2,595 insured adults reached through the SSRS Opinion Panel either online or over the phone (n=75 in Spanish). The SSRS Opinion Panel is a nationally representative probability-based panel where panel members are recruited randomly in one of two ways: (a) Through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Groups (MSG) through the U.S. Postal Service’s Computerized Delivery Sequence (CDS); (b) from a dual-frame random digit dial (RDD) sample provided by MSG. For the online panel component, invitations were sent to panel members by email followed by up to three reminder emails. 2,500 panel members completed the survey online and panel members who do not use the internet were reached by phone (95). Another 504 respondents were reached online through the Ipsos Knowledge Panel This panel is recruited using ABS, based on a stratified sample from the CDS.
Another 289 (n=10 in Spanish) interviews were conducted from a random digit dial (RDD) of prepaid cell phone numbers (n=190) and landline telephone numbers (n=99). Phone numbers used for the prepaid cell phone component were randomly generated from a cell phone sampling frame with disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification for the prepaid cell phone sample was based on incidence of the race/ethnicity groups within each frame. Phone numbers for the landline component were randomly generated from a landline sampling frame utilizing MSG’s listed household sampling frame to identify households with an adult age 65 or older and therefore more likely to have Medicare. This landline sample was also disproportionately stratified to reach African American and Hispanic respondents. An additional 217 respondents were reached by calling back respondents who said they were insured in previous KFF probability-based polls. Respondents in the phone samples received a $10 incentive via a check received by mail. SSRS web respondents received a $5 electronic gift card incentive (some harder-to-reach groups received a $10 electronic gift card). Ipsos Knowledge Panel respondents were included in raffles and sweepstakes for cash prizes as appreciation for their participation.
Respondents with Employer-sponsored plans, Medicaid, Medicare, and Marketplace plans from the combined phone and panel samples were weighted separately to match each group’s demographics using data from the 2021 American Community Survey (ACS). Weighting parameters included gender, age, education, race/ethnicity, and region. The weights take into account differences in the probability of selection for each sample type (cellphone sample, landline sample, callback phone sample, and panel). This includes adjustment for the sample design, within household probability of selection, and the design of the panel-recruitment procedure. The total sample of insured adults was also weighted to match demographics of insured adults using data from the 2021 American Community Survey (ACS).
The margin of sampling error including the design effect for the full sample is plus or minus 2 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. KFF public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
This work was supported in part by the Robert Wood Johnson Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
| Group | N (unweighted) | M.O.S.E. |
| Total insured adults | 3,605 | ± 2 percentage points |
| Insured adults with Medicaid coverage | 1,212 | ± 4 percentage points |