KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
There are an estimated 20 million new sexually transmitted infections (STIs) every year in the United States with rates of reported STIs continuing to rise, reaching record-breaking levels in 2018. This poll provides new data on the public’s knowledge and attitudes about STIs.
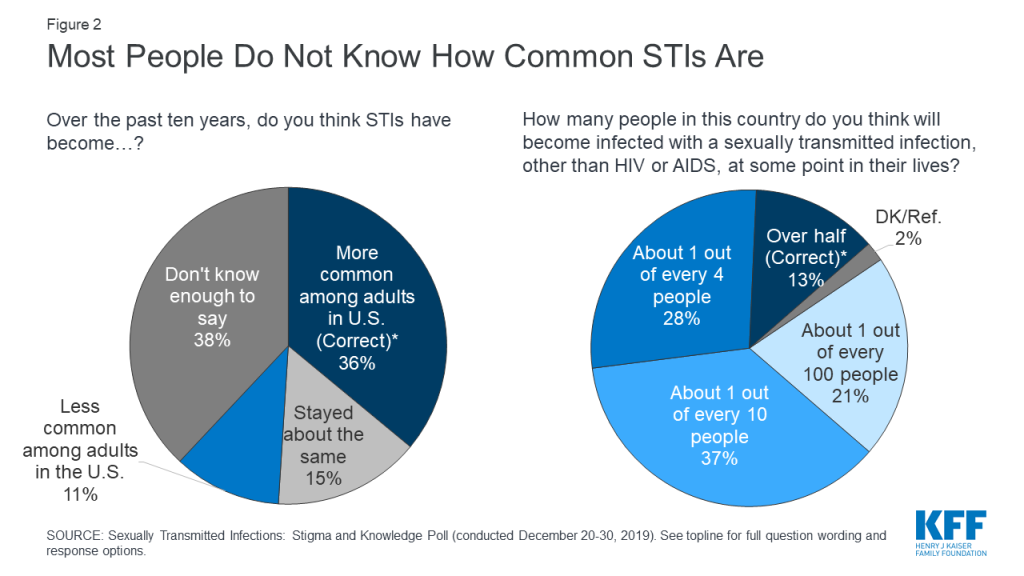
Large majorities of the public are unaware of how common STIs are among adults in the U.S. About one-third (36%) are aware that STIs have become more common over the past decade and few (13%) know that over half of people in the U.S. will get an STI sometime during the lifetime.
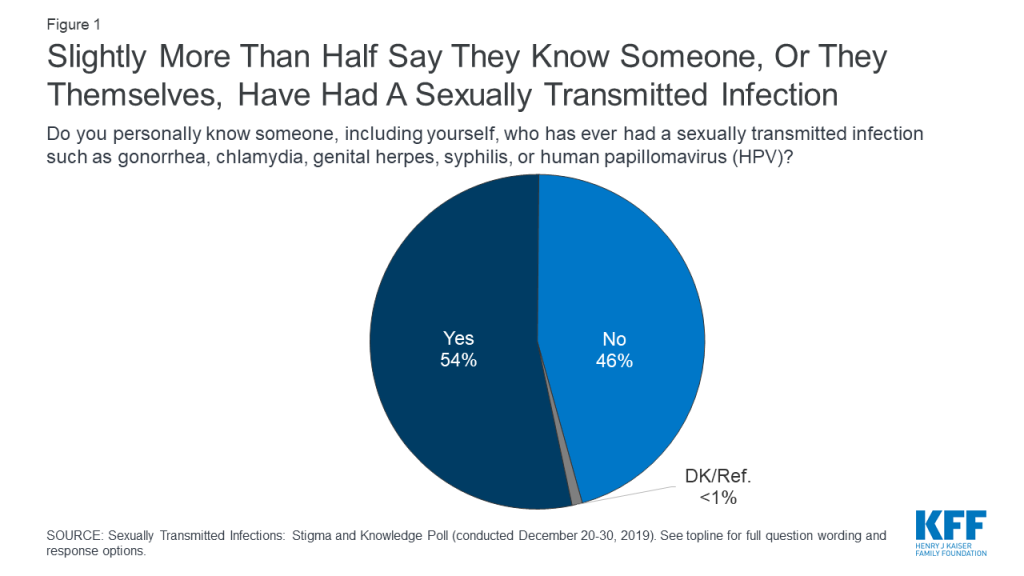
Slightly more than half (54%) say they know someone who has had an STI, including those who say they have personally had an STI. There are some differences by key demographic groups with larger shares of women and younger adults saying they personally know someone who has had an STI.
Small shares of the public (8%) are worried about contracting an STI in the next year, with larger shares of younger people, ages 18-29, expressing concern (20%). About one in ten Black adults (13%) and Hispanic adults (13%) and 5% of White adults say they are worried they may personally contract an STI in the next year.
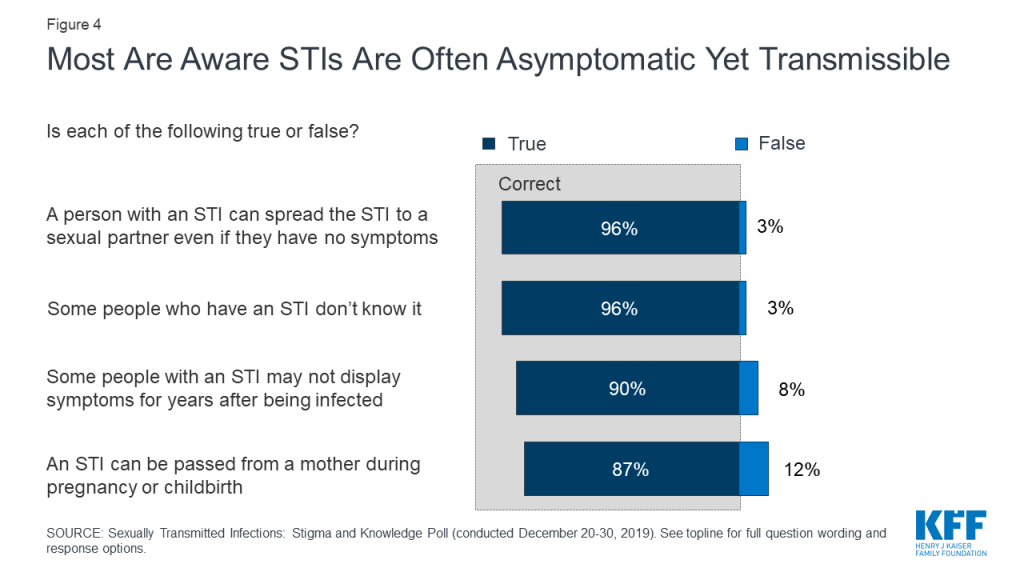
Overall, the public is aware that STIs are often asymptomatic, yet transmissible. Large majorities know that STIs can be transmitted even when that person is not showing any symptoms (96%) as well as during pregnancy and childbirth (87%). Equally large shares are aware some people who have an STI might not even know it (96%) and symptoms may not display in some people with an STI for years (90%).
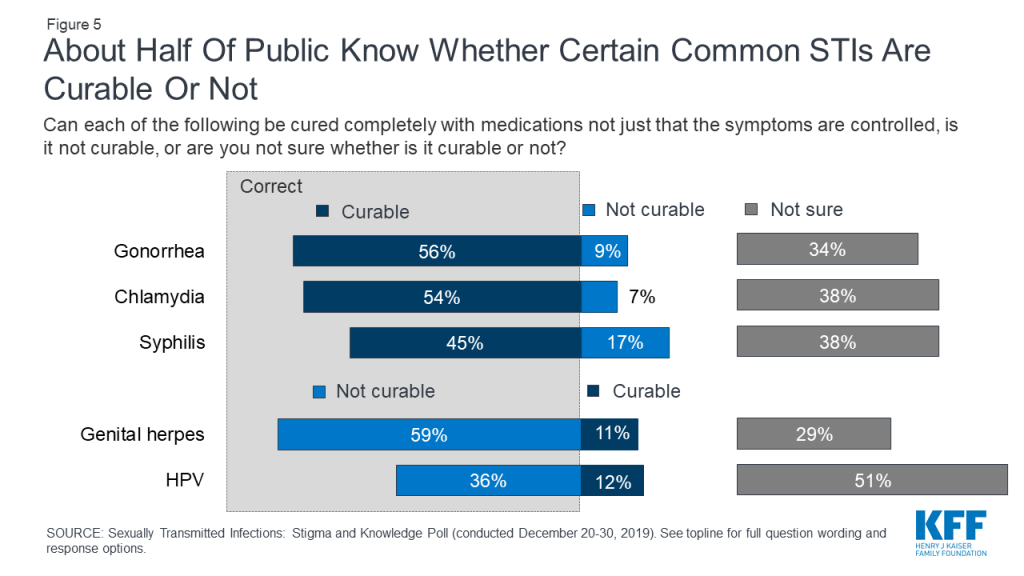
About half know chlamydia (54%), gonorrhea (56%), and syphilis (45%) are curable. More than half (59%) know that genital herpes is not curable.
Sexually Transmitted Infections
Slightly more than half (54%) of adults say they personally know someone, including themselves, who has had an STI such as gonorrhea, chlamydia, genital herpes, syphilis, or human papillomavirus (HPV). Nearly six in ten women (58%) say they know someone who has ever had an STI, as do half of men. Older adults are less likely to know someone compared to younger age groups (18-29 year olds: 54%; 30-49 year olds: 63%; 50-64 year olds: 57%; 65 and older: 36%).
Figure 1: Slightly More Than Half Say They Know Someone, Or They Themselves, Have Had a Sexually Transmitted Infection
Despite this, few know how common STIs are in the U.S. today and that STIs are on the rise. One-third of adults (36%) are aware that STIs have become “more common” over the past ten years, but this is similar to the share who say they “don’t know enough to say” (38%) and only ten percentage points higher than the share (26%) who either say STIs have become “less common” or “stayed about the same.” About one-third of men (32%) are aware that STIs have become more common over the past decade and about four in ten women are aware (39%). Awareness is also higher among Black adults (48%) compared to White adults (33%). Four in ten Hispanic adults are also aware STIs have become more common.
Additionally, a small percentage (13%) know that “over half of the people in the U.S.” will have an STI, other than HIV, at some point in their lifetime.
Figure 2: Most People Do Not Know How Common STIs Are
How Common Are Sexually Transmitted Infections?
Sexually transmitted infections (STIs) are very common, and over half of people in the U.S. will have an STI in their lifetime. In fact, the CDC estimates there are over 110 million sexually transmitted infections among men and women in the U.S., with 20 million new cases each year.
HPV is the most common STI (79 million cases), followed by genital herpes (24 million), trichomoniasis (3.7 million) and chlamydia (1.6 million). Gonorrhea, syphilis, hepatitis B and HIV are less common, although rates of syphilis, gonorrhea and chlamydia are rising, up 71%, 63% and 19% respectively from 2014 to 2018.
About one in ten (8%) are worried that they personally will contract a new STI over the next year, yet there are some groups who worry more about contracting an STI. Larger shares (20%) of younger adults (18-29) report being worried which is consistent with data from the CDC which states that this age group is the group at the highest risk for STIs. Additionally, STI rates are higher among Black adults and Hispanic adults compared to White adults. At least one in ten Hispanic adults (13%) and Black adults (13%) say they were worried about contracting an STI, compared to 5% of White adults.
Table 1: Share of U.S. Adults Who Are Worried They Will Contract A New STI Over The Next Year
Percent who say they are either “very worried” or “somewhat worried”:
Total adults
8%
Men
10
Women
6
18-29 years old
20
30-49 years old
9
50-64 years old
4
65 and older
1
White, Non-Hispanic
5
Black, Non-Hispanic
13
Hispanic
13
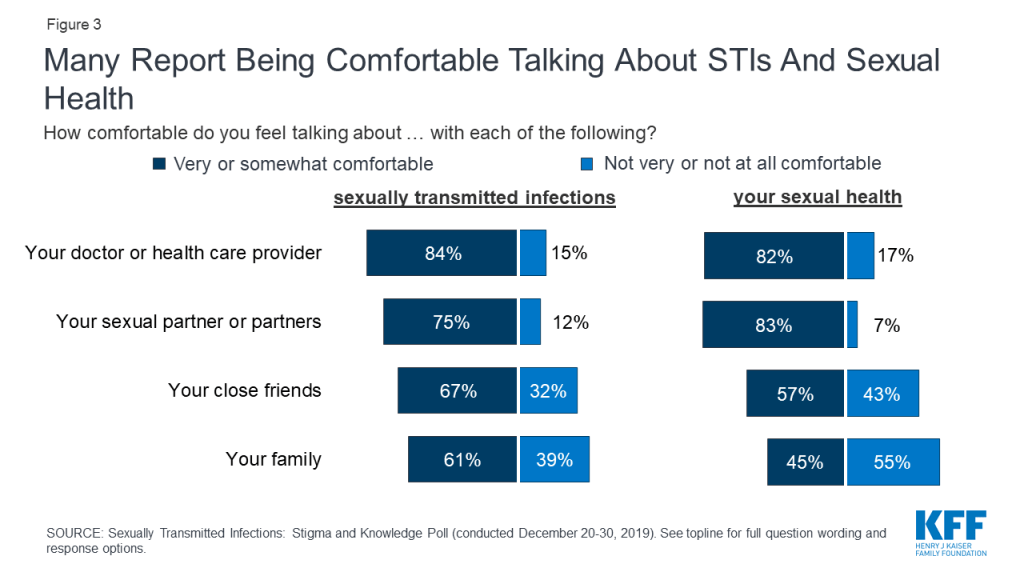
About one in eight say they are uncomfortable discussing STIs with a sexual partner (12%) and one in seven (15%) are uncomfortable talking about STIs with a doctor. In fact, large majorities of the public say they are “very comfortable” or “somewhat comfortable” talking about STIs with their doctor or health care provider (84%) or sexual partners (75%). Smaller majorities are comfortable talking about STIs with their close friends (67%) or family (61%). Similar shares also report feeling comfortable talking about their sexual health with these different groups. In a survey conducted more than two decades ago, KFF found that more than one-third of the public were uncomfortable discussing STIs with a sexual partner (37%) and three in ten (31%) were uncomfortable talking with a doctor about getting an STI test (compared to 12% and 15% in the most recent survey).
Figure 3: Many Report Being Comfortable Talking About STIs And Sexual Health
There are some differences by age and gender in how comfortable people are talking about the topic. A higher share of women than men said they were comfortable talking with their close friends about STIs (71% vs. 61%, respectively) and their sexual health (62% vs. 52%).
While most new STIs are among young adults, older adults are also at risk. A smaller share of those 65 and older say they are comfortable talking about STIs and their sexual health with a variety of audiences, compared to younger adults.
Table 2: Comfort Level Talking About STIs and Sexual Health, by Age
Share who feel very or somewhat comfortable talking about:
Adultsages 18-29
Adultsages 30-49
Adultsages 50-64
Adultsages 65+
Sexually transmitted infections with their…
Doctor or health care provider
83%
87%
88%
77%
Sexual partner(s)
79
85
75
60
Close friends
69
71
68
57
Family
51
59
71
60
Sexual health with their…
Doctor or health care provider
80
80
86
81
Sexual partner(s)
84
90
84
69
Close friends
66
68
51
38
Family
38
52
52
33
NOTE. Grey box indicates statistical significance at p<.05 compared to all other age groups.
Understanding of STI Transmission and Treatment Options
The vast majority of adults are aware that STIs are often asymptomatic, yet transmissible. More than nine in ten adults are aware that a person with an STI can spread it to a sexual partner even if they do not have any symptoms (96%) as well as during pregnancy and childbirth (87%). Equally large shares are aware some people who have an STI might not even know it (96%) and that some people with an STI may not display symptoms for years after contracting the STI (90%).
Figure 4: Most Are Aware STIs Are Often Asymptomatic Yet Transmissible
Large shares of the public are unsure about whether many STIs are curable with medication or not. Slightly more than half of adults know gonorrhea and chlamydia are curable with medication (56% and 54%, respectively), and genital herpes is not curable with medication (59%). Fewer are aware that syphilis is curable with medication (45%). About half (51%) of the public say they are unsure if HPV is curable with medication or not. HPV is a common STI that has more than 150 different strains (including some associated with cervical and other cancers and others that cause genital warts). There is no medical treatment for HPV, however, most people who acquire HPV (specifically those not associated with cancer or warts) will clear the infection on their own and without health problems. There is a vaccine available to protect against some of the more serious types of HPV.
In 1998, less than half of the public knew gonorrhea and chlamydia could be cured with medications (48% and 32%, respectively), while now more than half are aware of this (56% and 54%, respectively). Awareness that both genital herpes and HPV are not curable with medications has not changed over the past two decades.
Figure 5: About Half Of Public Know Whether Certain Common STIs Are Curable Or Not
Lifelong infection, but symptoms can be treated with antiviral medication
Human Papillomavirus (HPV)
Most people who acquire HPV will clear the infection on their own and without associated health problems. There is a vaccine for some types of HPV associated with cervical cancer that is recommended beginning at age nine.
Knowledge around treatment of STIs is generally higher among those who are under the age of 65. Majorities of younger adults are aware that chlamydia and gonorrhea are curable and that genital herpes is not curable with medication, compared to less than half of adults 65 and older who are aware of this. For each STI assessed, individuals aged 65+ were significantly less likely to correctly identify whether they are curable or not, compared to adults younger than 65 years old.
Table 3: Awareness of STI Treatment and Management, by Age
Percent who correctly know the following:
Adults ages 18-29
Adults ages 30-49
Adults ages 50-64
Adults ages 65+
Chlamydia is curable
57%
66%
55%
34%
Gonorrhea is curable
56
60
61
46
Syphilis is curable
34
49
53
39
Genital herpes is not curable
57
68
66
41
HPV is not curable
46
49
30
15
NOTE. Grey box indicates statistical significance at p<.05 compared to all other age groups.
There were also some differences by gender and race. A larger share of women than men correctly reported that chlamydia is curable and that HPV is not curable (even though most people who acquire HPV will clear the infection on their own and there is a vaccine for HPV prevention), while awareness about other infections was similar between women and men. A higher share of Black adults know that chlamydia, gonorrhea and syphilis are curable, compared to other races. A previous 2017 KFF survey showed a higher share of Black and Latina women compared to White women said their physician discussed STIs with them.
Table 4: Awareness About STI Treatment and Management, by Gender and Race/Ethnicity
Percent who correctly know the following:
Gender
Race/Ethnicity
Women
Men
Black
White
Hispanic
Chlamydia is curable
61%
47%
74%
51%
49%
Gonorrhea is curable
56
57
75
55
48
Syphilis is curable
44
46
54
44
39
Genital herpes is not curable
62
56
64
62
53
HPV is not curable
40
33
32
39
35
NOTE. Grey box indicates statistical significance at p<.05 compared to all other groups in demographic category.
Sexually transmitted infections encompass many different types of viral and bacterial infections. Every year, an estimated 20 million new sexually transmitted infections (STIs) are reported to the Centers for Disease Control and Prevention (CDC) in the United States. The rates of reported STIs reached record-breaking levels in 2018, continuing their recent rise. Despite these high rates, a 2019 KFF poll found that a large share of the public is unaware of how common STIs are, with less than half (36%) aware that STIs rates are increasing.
While all sexually active individuals are potentially at risk, rates are highest among 15-24 year olds, as well as gay and bisexual men. Black and Hispanic populations are also disproportionately affected relative to non-Hispanic White populations. Increasing rates of STIs highlight the importance of prevention, testing, treatment, as well as information and education, in curbing the transmission of these infections. This fact sheet examines trends and disparities in STI prevalence, reviews the STI screening and preventive care coverage policies for private insurance and public programs (including coverage gaps), and describes confidentiality in the provision of these services.
What are Sexually Transmitted Infections?
STIs are generally defined to include chlamydia, genital herpes, gonorrhea, hepatitis B, HIV, Human Papillomavirus (HPV), syphilis, and trichomoniasis . All STIs, including HIV, are preventable, and there are treatments to cure many, though not all, of them. Because some STIs often show no symptoms, at least initially, some people with an STI may not find out until more serious health concerns present. For this reason, preventive measures and routine screenings are important for the early identification of these infections in order to engage in treatment and to prevent further transmission and more serious complications.
Untreated STIs, particularly chlamydia and gonorrhea, can result in pelvic inflammatory disease (PID) in women and infertility. It is estimated that HPV, the most common STI in the United States, will be contracted at some point during the lifespan of nearly every sexually active individual. Most cases of HPV resolve on their own, but certain strains of HPV are linked to cervical, throat, penile, and anal cancers. The HPV vaccine protects against nine strains of this virus, including several that are associated with cancer.
Pregnant women with an untreated STI face increased risk of complications as do their infants. Exposure to an STI during pregnancy can result in preterm labor, low birth weight, premature rupture of membranes, and transmission to the infant during delivery. HIV and syphilis are particularly serious if transmitted to newborn infants. So long as a mother with HIV is engaged in consistent antiretroviral (ARV) treatment, it would be highly unlikely to transmit HIV to a baby. Up to 40% of babies born to women with untreated syphilis may be stillborn or die from the infection. Late or limited prenatal care has been associated with congenital syphilis (when the infection is present in utero or childbirth). Congenital syphilis is preventable in most cases, if women are screened for syphilis and treated early during prenatal care.
Prevalence of Sexually Transmitted Infections
While women still account for the highest reported cases of STIs (driven mainly by high numbers of chlamydia in women), men, in particular gay and bisexual men, saw greater increases in rates of syphilis, chlamydia, and gonorrhea in recent years. Syphilis infection rates nearly doubled among men from 2014 to 2018 (Figure 1).
Table 1: Sexually Transmitted Infection Rates of Reported Cases, by Selected Characteristics, 2018Rate per 100,00 population
Gonorrhea
Chlamydia
Syphilis (primary and secondary stages)
Congenital Syphilis
HIV
U.S. Total
179.1
539.9
10.8
33.1
11.4
Sex
Men
212.8
380.6
18.7
NR
22.5
Women
145.8
692.7
3
NR
5.1
Race
White
71.1
212.1
6
13.5
4.9
Black
548.9
1192.5
28.1
86.6
39.3
Hispanic
115.9
392.6
13
44.7
16.2
Asian/Pacific Islanders
35.1
132.1
4.6
9.2
NA
American Indian/Alaska Native
329.5
784.8
15.5
79.2
7.8
Age
15-19
432.4
2110.6
7.7
NR
8
20-24
713
2899.2
27.8
NR
27.6
25-29
553.6
1427.3
33
NR
32.5
30-34
366.4
701.5
26.9
NR
25.6
Region
Northeast
138.4
492.1
8.7
8.5
10
South
194.4
565.2
11.1
12.4
15.7
Midwest
184.5
524
7.1
44.7
7.2
West
179.7
548.5
15
48.5
9.3
NOTES: NR is Not Reported. Primary and secondary syphilis stages are the earliest stages of infection, reflect symptomatic disease, and are indicators of incident infection.SOURCE: Centers for Disease Control and Prevention (CDC), Sexually Transmitted Disease Surveillance 2018; CDC, Diagnoses of HIV Infection in the United States and Dependent Areas, 2018.
Figure 1: Rates of sexually transmitted infections by sex from 2014 to 2018
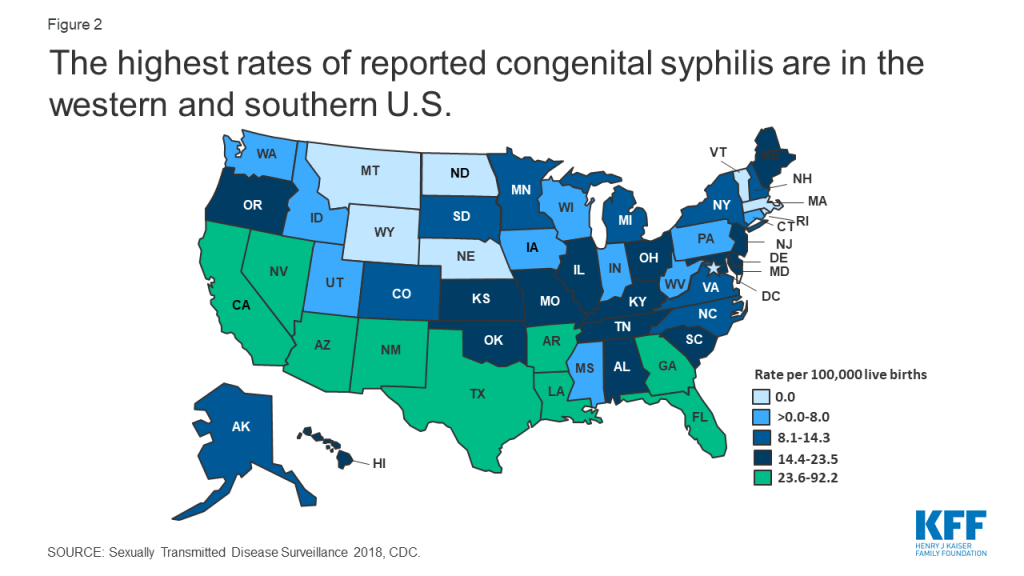
Congenital syphilis rates increased 173% between 2014 and 2018, with the number of cases the highest they have been since 1995. The highest rates of congenital syphilis were in the South, West, and Southwest (Figure 2).
Figure 2: The highest rates of reported congenital syphilis are in the western and southern U.S.
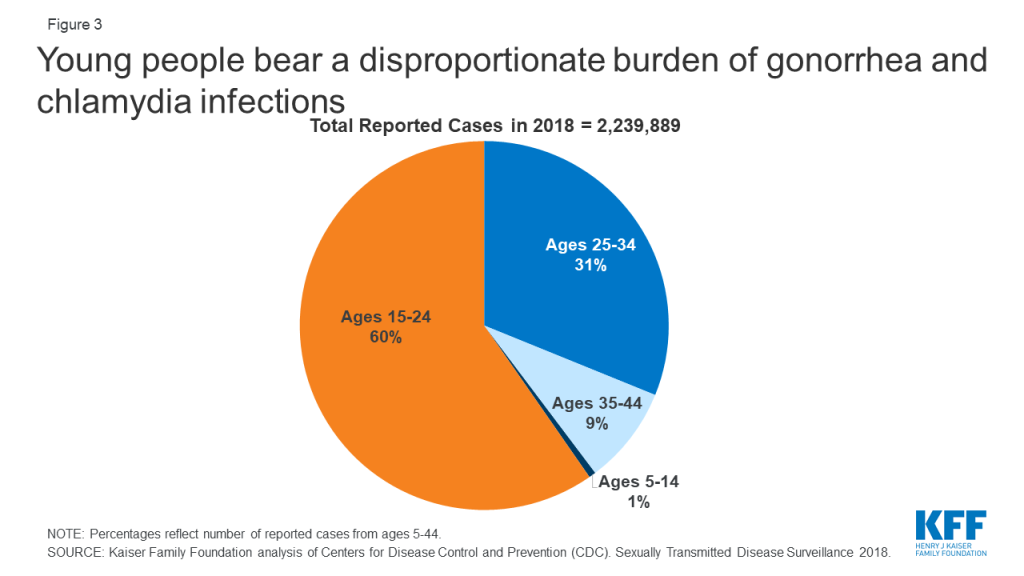
STIs also have a disproportionate impact on young people, ages 15-24, who acquire half of all new STIs, despite only representing 25% of the sexually active population (Figure 3). Young people, ages 15-24, account for 60% of all reported cases of gonorrhea and chlamydia.
Figure 3: Young people bear a disproportionate burden of gonorrhea and chlamydia infections
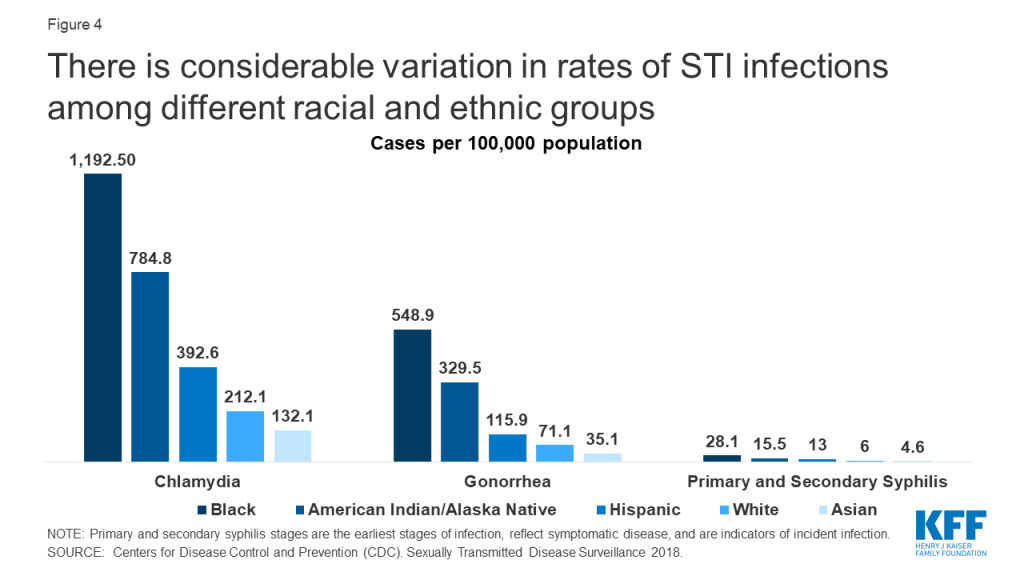
Due to a combination of social, structural, and economic inequities, HIV and other STIs disproportionately affect certain groups (Figure 4). In 2018, Blacks accounted for 38% of reported gonorrhea cases and 33% of primary and secondary syphilis cases, despite comprising just 13% of the population. Blacks also accounted for 42% of new HIV diagnoses in the U.S in 2018. Hispanics are also disproportionately affected, accounting for 27% of persons newly diagnosed with HIV and representing 18% of the population in 2018.
Figure 4: There is considerable variation in rates of STI infections among different racial and ethnic groups
Gay and bisexual men of all races have also been disproportionately affected since the start of the HIV/AIDS epidemic. In 2018, men who have sex with men (MSM) accounted for more than two thirds (69%) of all HIV diagnoses in the U.S., representing 86% of cases among males. MSM also accounted for 78% of male primary and secondary syphilis cases in 2018.
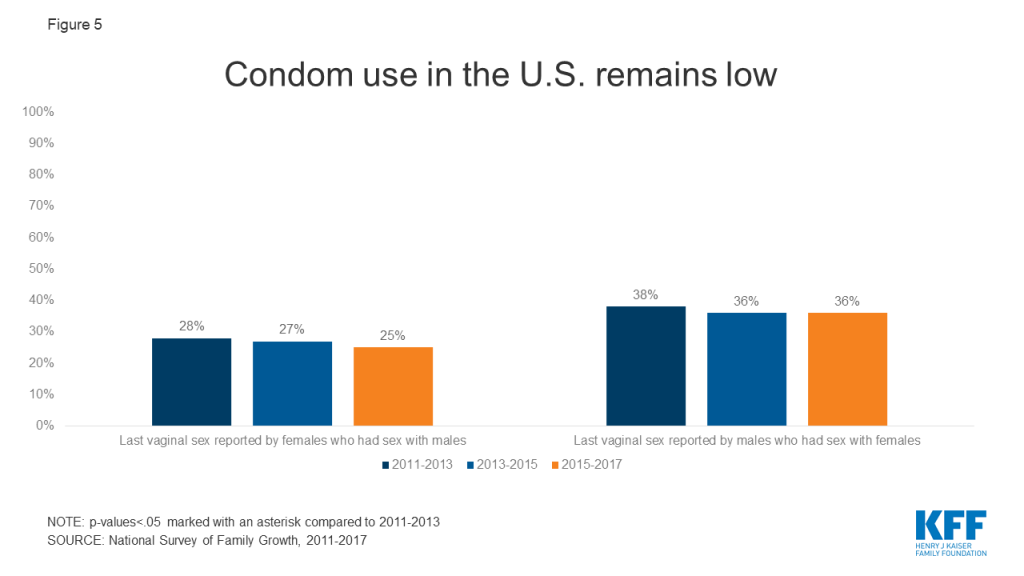
The higher prevalence of HIV and other STIs in certain communities can mean risk of exposure is also greater in these communities, particularly when sexual networks are close-knit. When used correctly, condoms are effective at preventing the transmission of HIV and other STIs. However, condom use in the U.S. remains low (Figure 5. Pre-exposure prophylaxis (PrEP), a daily pill approved by the FDA in 2012, reduces the risk of sexually contracting HIV by up to 99% among people at high risk.
Figure 5: Condom use in the U.S. remains low
Expedited Partner Therapy
Many states have laws allowing expedited partner therapy (EPT), which permits the treatment of partners of patients diagnosed with an STI without examination. The CDC has recommended this practice since 2006 in certain circumstances due to its success in reducing gonorrhea reinfection rates. Currently 39 states and DC allow physicians to provide at least some treatment to the partner of a patient diagnosed with a STI. Among publicly funded clinics, 79% provided expedited therapy for the patient’s partner at the same visit in 2015. However, even in states where EPT has been legalized, many do not allow the patient’s insurance coverage to be billed for the partner’s treatment, which can create a financial barrier to care.
Paying for STI Prevention and Treatment Services
Access to prevention, screening, testing and treatment services for STIs is facilitated by private insurance, public coverage such as Medicaid and Medicare, as well as publicly-supported health programs. The CDC estimates that in 2008 (the most recent estimate available), the annual direct medical costs in the US associated with STIs (including HIV) were nearly $16 billion.
Private Insurance
The Affordable Care Act (ACA) requires most private health insurance plans to cover recommended preventive services, including HIV and other STI screening, with no cost sharing. For adults, this includes US Preventive Services Taskforce (USPSTF) recommendations receiving an A or B grade, which include vaccines recommended by the CDC’s Advisory Committee for Immunization Practices, and services for women recommended by the Health Resources and Services Administration (HRSA). STI-related services that must be covered without cost-sharing by most plans are presented in Table 2.
In June 2019, the USPSTF Task Force added an A grade recommendation for PrEP for the prevention of HIV in high-risk populations, which means that most insurance plans must begin covering the full cost of the drug in the plan year that starts after June 2020. CDC guidelines on PrEP advise that individuals on PrEP have follow up visits and lab work, including being re-tested for HIV four times a year, but it is unclear whether these follow-up visits and lab work must be covered without cost-sharing by most insurance plans.
Plans are also required to cover prescription contraceptives for women, so coverage for female condoms would be required if an enrollee has a prescription but not when purchased over the counter. Twelve states (CA, CT, DE, IL, MD, MA, NJ (will apply to insurance plans in April 2020), NM, NV, NY, OR, WA) and DC currently require insurance coverage for over-the-counter contraceptive methods – of these however– 8 states (CA, DE, IL, MD, MA, NJ, NV, OR) exclude male condoms.
Medicaid
Medicaid, the national health coverage program for low-income individuals, is financed and operated jointly by the federal and state governments. For the 37 states and DC that have expanded Medicaid, STI counseling, screenings, preventive vaccinations, and PrEP must be covered at no cost for the newly eligible populations under the ACA just as they are for enrollees in private insurance plans (Table 2). However, this requirement does not apply to populations covered by Medicaid through other pathways, where coverage for specific STI screenings and treatments is determined by the state.
Some states extend access to STI services through limited-scope Medicaid family planning programs that provide Medicaid coverage solely for family planning services to women and men who do not qualify for full Medicaid benefits. Most of these programs cover STI screenings, but not all cover treatment if diagnosed. While all state Medicaid programs must cover medically necessary HIV testing, state coverage of routine HIV screening varies because it is an optional benefit under Medicaid. While several states cover condoms, they require prescriptions for this over-the-counter product. Medicaid is the largest public funder of HIV treatment and care, and all state Medicaid programs should cover PrEP.
Table 2: STI-related Preventive Care Benefits that Plans Must Cover without Cost-Sharing
Men who are sexually active or at higher risk
Women who are sexually active or at increased risk
Pregnant women
Young people
Gonorrhea screening
X – sexually active women <24 years, and older women at increased risk
X (for those at increased risk
Chlamydia screening
X – sexually active women <24 years, and older women at increased risk
X – under 25
Syphilis screening
X
X
X
HPV DNA Testing
X – 30 years and older
HPV vaccine
X – 11 to 26 years
X – 11 to 26 years
X – 11 to 26 years
Hepatitis B screening
X
X
X – at first prenatal visit
X
Hepatitis B vaccine
X
X
X – children under 18 years
STI prevention counseling
X
X
X – if sexually active
HIV screening and counseling
X – all aged 15 to 65 years, all others at higher risk
X – all aged 15 to 65 years, all others at higher risk
X
X
PrEP
X – all at high risk of HIV acquisition
X – all at high risk of HIV acquisition
X – all at high risk of HIV acquisition
X – all at high risk of HIV acquisition
Pap Test (cervical cancer screening)
X – All women ages 21 to 65
NOTES: Population covered and definition of high risk vary by condition. Coverage without cost sharing required in new private plans and Medicaid expansion groups.SOURCE: Kaiser Family Foundation, Preventive Services Tracker, October 2019.
Medicare
Medicare plays a key role in providing health coverage to 60 million people 65 and older as well as younger people with long-term disabilities. The ACA also requires Medicare to cover preventive services that are rated “A” or “B” by the USPSTF without cost-sharing. Medicare Part B (Medical Insurance) covers STI screenings for chlamydia, gonorrhea, syphilis, and/or Hepatitis B once every 12 months for individuals at increased risk for an STI or at certain times during pregnancy for pregnant individuals. Medicare also covers up to two individual 20-30 minute, face-to-face, high-intensity behavioral counseling sessions once each year for sexually active individuals at increased risk for STIs. Additionally, Medicare covers an HIV screening once per year for individuals age 15-65 without regard to perceived risk or for individuals outside of this age range who are at an increased risk for HIV. Medicare Part D is required to cover all approved antiretrovirals (one of “six protected” drug classes), which includes PrEP, but unlike most preventive services covered under Part B, plans are allowed to charge cost sharing for these drugs.
Services and Programs for Uninsured Individuals
Roughly 28 million people, 9% of the population, were uninsured in 2018. A patchwork of public-supported clinics and program make STI services available to uninsured individuals. STI programs funded by federal, state, and local governments, such as those that receive funding from various federal agencies such as HRSA, the CDC, or the Office of Population Affairs (OPA), are important sites of care for STI prevention and treatment, especially, those who are under- or uninsured. As part of the safety-net healthcare network, health centers and health departments provide low-income individuals with free or low-cost care, including counseling, testing, diagnosis and treatment. Research suggests that clinicians at these clinics are also more likely to provide routine STI care and discuss the use of condoms with patients than private providers.
The federal Title X family planning grant program, administered by OPA, also provides support to clinics to serve low-income and uninsured individuals in need of STI screening and treatment. In the past year, however, the network of clinics participating in the program has shrunk significantly. About one in four Title X funded sites have withdrawn from the program in response to the Trump Administration’s new regulations that block Title X support to clinics that provide abortion services and referrals in addition to family planning and STI services. The organizations that no longer participate in the program have not only lost funding available to provide low-income individuals with contraceptive services, but also may have had an impact on the availability of STI testing and treatment services in many communities.
For people living with HIV, the Ryan White HIV/AIDS Program works with health departments and local community-based organizations to provide HIV medical care and other support services for people living with HIV who have no insurance or are underinsured.
The AIDS Drug Assistance Program or ADAP is part of the Ryan White HIV/AIDS Program. It helps covers the cost of HIV-related prescription medications for low- to moderate- income people who have limited or no prescription drug coverage. Each state operates its own ADAP, so eligibility and program elements can vary state to state.
Gilead, the manufacturer of Truvada and Descivy, the PrEP medications, offers a Medication Assistance Program for PrEP that may provide the medication at no cost based on income, but does not cover the cost of the medical visits or the recommended lab testing. The program may also be available to those on Medicare who do not have Part D prescription drug coverage. In addition, some city and state health departments, and foundations offer navigation and other support services, as well as financial assistance to make PrEP free or low cost. In December 2019, the U.S. Department of Health and Human Services launched the Ready, Set, PrEP program, which makes PrEP prescriptions available at no cost to 200,000 at-risk, uninsured individuals each year for up to 11 years. The program does not support required labs and medical services, which can be expensive. This new program is still in early implementation stages.
Confidentiality
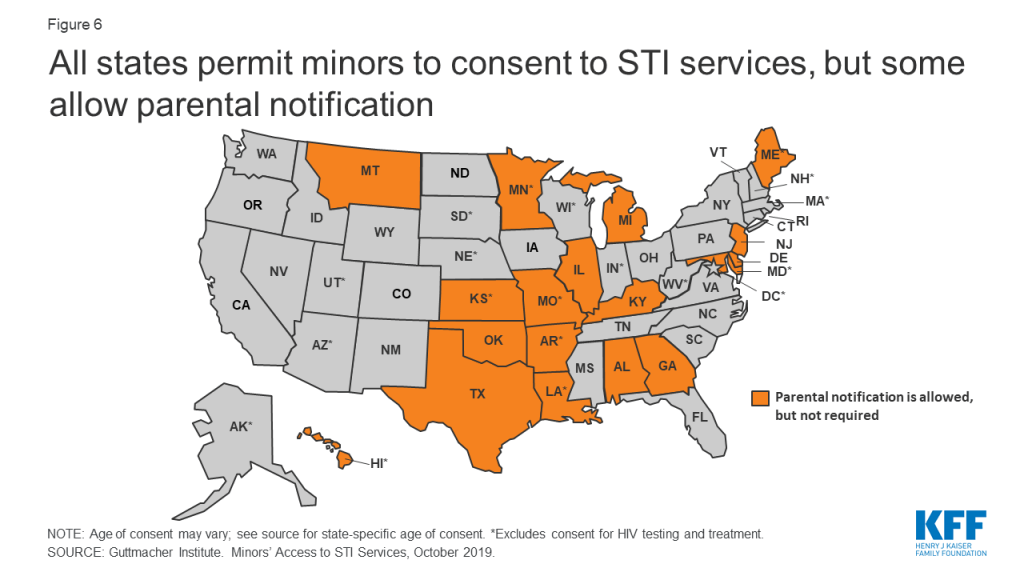
Confidentiality is a crucial factor in the provision of STI screening and treatment services. For minors in particular, it can be a challenge. Although all 50 states and DC allow minors to consent to STI services, 18 states allow physicians to inform a parent or guardian that the minor is seeking these services (Figure 6).
Figure 6: All states permit minors to consent to STI services, but some allow parental notification
Confidentiality has long been a fundamental principle of the Federal Title X family planning program; however, the Trump Administration’s new final regulations for the Title X program also have broadened its requirements to encourage family participation, require documentation of the specific actions taken to encourage family participation (or the specific reason why family participation was not encouraged) in minor’s records, and to document the age of the minor’s sexual partner. While the impact of this regulation on minors’ willingness to seek care at a Title X clinic has not yet been evaluated, there is concern that this new requirement will deter minors from seeking services because of their concerns about confidentiality.
Another confidentiality concern resulted from the ACA provision that allows dependents to remain covered under their parent’s plan up to the age of 26. In 2018, approximately 11.1 million young adults aged 19-25 were covered as dependents in an employer-sponsored insurance policy.1 Although this policy has expanded coverage for young adults, it has raised concerns about privacy and confidentiality in the use of sensitive health services such as STI screening and treatment for young adults covered as dependents. According to a 2013 Kaiser Family Foundation survey, 71% of women ages 18 to 25 rated confidentiality as important to them, but only 37% understood that an Explanation of Benefits (EOB) summary is sent to the primary policyholder (typically the parent) when health services are used.
However, seven states (CA, CO, HI, MD, ME, OR, and WA) have implemented broad laws to ensure confidentiality for minors seeking sensitive services such as STI screenings. Some states (CA, MD, and OR) require insurers to provide confidential communications upon the written request of the covered dependent, including minors. Other states (HI and ME) offer broader protections from disclosure of health information without the consent of the minor. Some states (CT, DE, and FL) have laws focusing specifically on the disclosure of STI treatment without a minor’s consent, including in the billing process.
Conclusion
High rates of STIs continue to be a public health concern. Women, people of color, and youth experience the highest rates of reported infections. Gay and bisexual men account for the majority of the increase between 2000 and 2018. The general public, however, appears to be unaware of the how commonly STIs occur and that their incidence is on the rise.
Publicly funded clinics, many funded by the CDC, OPA’s Title X program, and HRSA’s Ryan White program, including health centers, state and local health departments, STI clinics, and Planned Parenthood clinics, provide confidential STI and HIV care to at-risk and uninsured populations. With the passage of the ACA, most private health insurance plans and Medicaid expansion programs are now required to cover HIV and STI counseling and screening without cost sharing. In addition to coverage, access to and the availability of STI/HIV care will likely depend on a number of factors, including public funding for safety-net providers, adoption of practices aimed at the reduction of transmission such as patient education, expedited partner therapy, consistent routine screenings and treatment, as well as proximity to providers.
AppendixTable 1: Number of Reported Sexually Transmitted Infections, 2018
State
Chlamydia Cases
Gonorrhea Cases
Syphilis(Primary and Secondary) Cases
Congenital Syphilis Cases
HIV Prevalence (2017)
HIV Diagnoses
Alabama
28,437
12,742
477
7
13,124
572
Alaska
6,159
2,247
55
1
720
20
Arizona
40,807
12,870
1,047
61
16,062
806
Arkansas
17,663
7,300
288
25
5,634
281
California
231,415
79,192
7,607
332
128,153
4,398
Colorado
29,124
8,894
337
7
12,352
409
Connecticut
16,732
4,959
91
2
10,328
250
Delaware
6,038
1,691
30
0
3,285
91
DC
9,014
4,240
279
0
14,316
208
Florida
104,758
32,644
2,880
108
110,034
4,683
Georgia
65,936
20,867
1,607
31
52,528
2,552
Hawaii
7,735
1,495
92
4
2,524
66
Idaho
6,572
1,134
46
1
1,145
37
Illinois
77,325
25,422
1,408
29
35,076
1,352
Indiana
34,926
12,193
367
1
11,218
510
Iowa
14,682
4,839
86
3
2,671
116
Kansas
14,231
5,256
152
8
2,997
154
Kentucky
19,440
7,470
366
9
7,108
360
Louisiana
36,293
12,043
669
46
20,424
986
Maine
4,345
710
74
0
1,576
28
Maryland
35,482
10,305
737
29
32,436
979
Massachusetts
30,460
8,076
552
0
20,374
654
Michigan
50,592
16,688
649
13
15,667
718
Minnesota
23,569
7,542
292
10
8,304
283
Mississippi
22,086
9,749
464
3
9,399
479
Missouri
34,728
15,090
806
17
12,308
446
Montana
4,917
1,181
45
0
625
23
Nebraska
8,026
2,696
119
0
2,136
79
Nevada
17,508
6,475
682
31
9,609
508
New Hampshire
3,734
594
64
1
1,189
36
New Jersey
36,514
9,067
570
13
34,891
1,044
New Mexico
14,000
5,268
304
10
3,428
121
New York
119,571
37,262
2,654
28
126,495
2,470
North Carolina
66,553
23,725
1,098
17
30,953
1,200
North Dakota
3,525
1,369
41
0
407
36
Ohio
63,220
25,146
740
20
21,899
984
Oklahoma
21,974
8,998
531
12
6,084
234
Oregon
19,224
5,913
424
10
6,879
230
Pennsylvania
59,340
15,887
797
9
35,520
1,002
Rhode Island
5,487
1,336
96
0
2,547
76
South Carolina
33,910
13,801
384
9
16,858
719
South Dakota
4,432
1,689
41
1
568
28
Tennessee
38,212
14,627
553
12
16,612
759
Texas
146,510
47,231
2,538
367
88,099
4,483
Utah
10,541
2,895
169
1
2,757
121
Vermont
1,712
268
11
0
693
18
Virginia
42,965
11,776
702
9
22,149
867
Washington
34,449
11,207
802
7
13,205
503
West Virginia
3,599
1,143
65
1
1,810
85
Wisconsin
28,027
7,882
152
1
6,216
210
Wyoming
2,169
311
23
0
326
12
Sources: Centers for Disease Control and Prevention (CDC). 2018 Sexually Transmitted Diseases Surveillance. Atlanta: U.S. Department of Health and Human Services, October, 2019. CDC, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention (HCHHSTP) AtlasPlus, accessed February 2019.
Kaiser Family Foundation estimates based on the Census Bureau’s American Community Survey, 2018. ↩︎
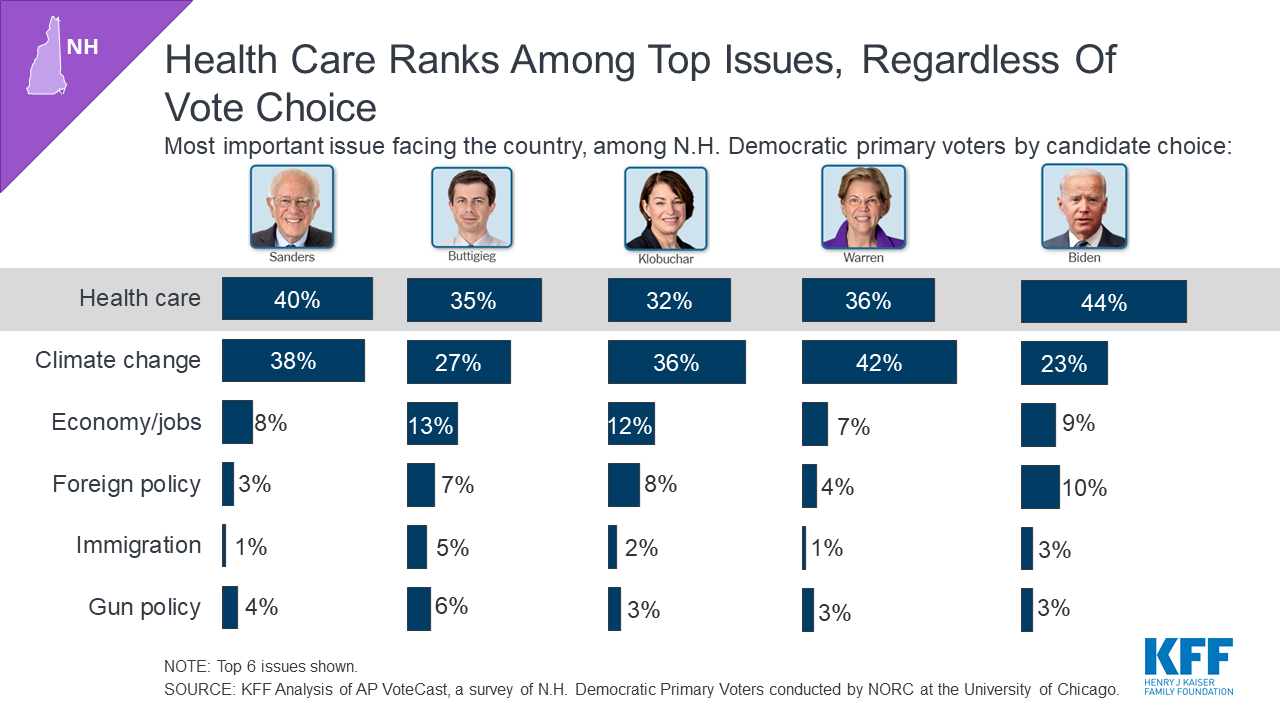
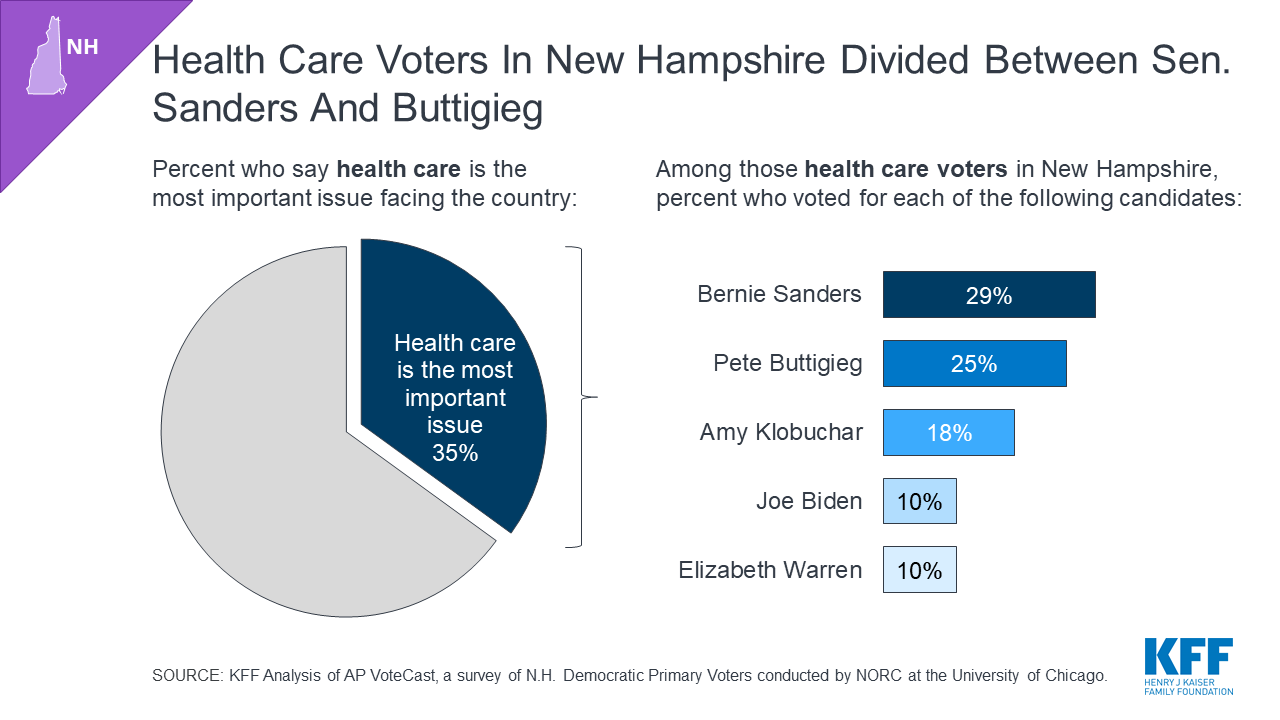
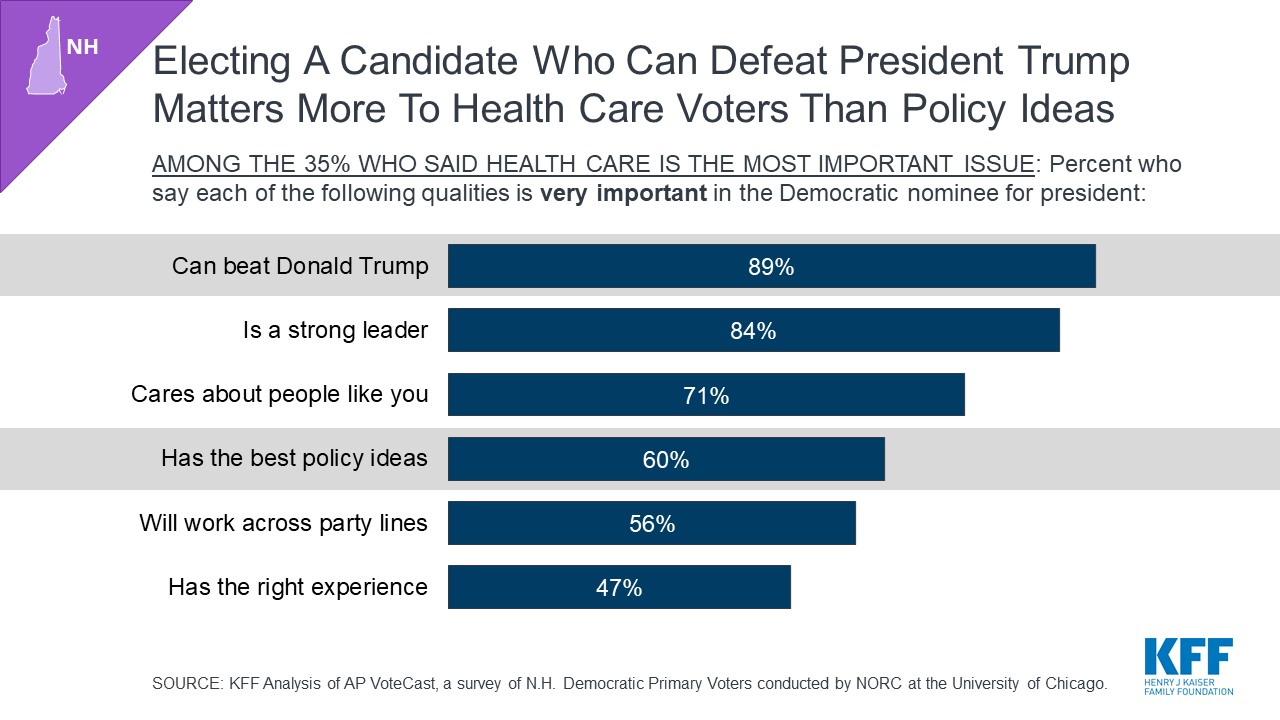
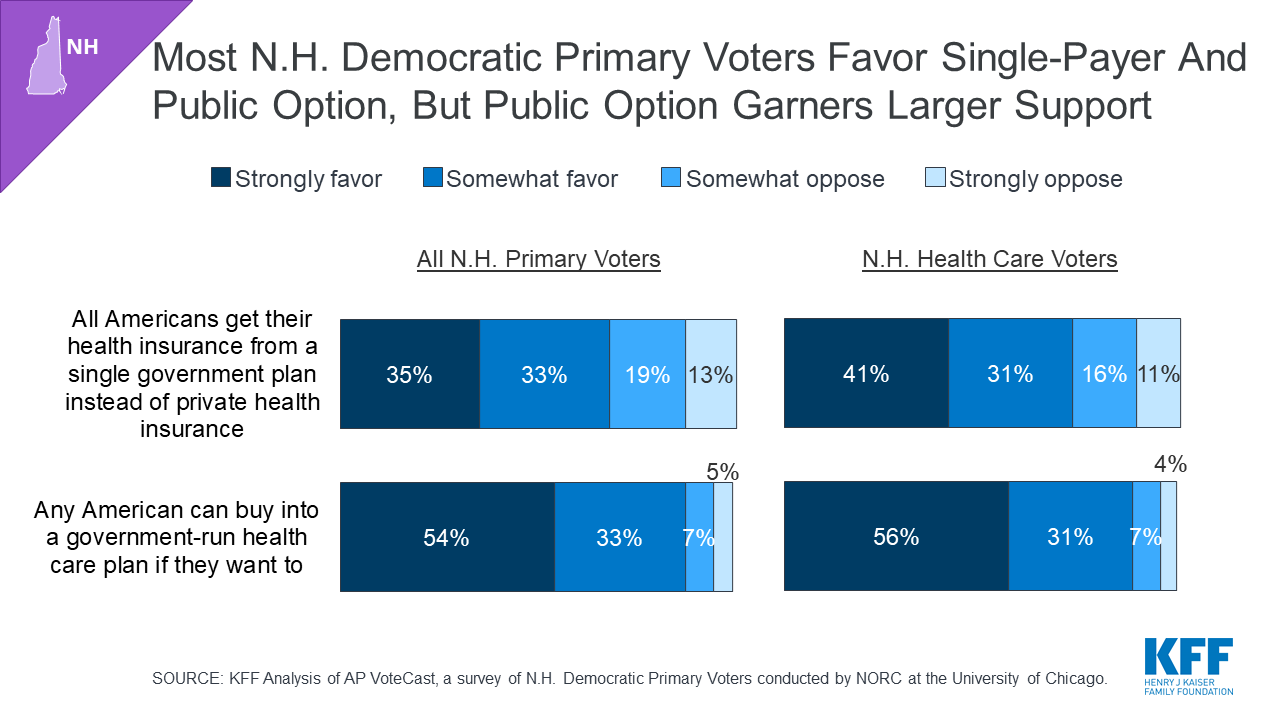
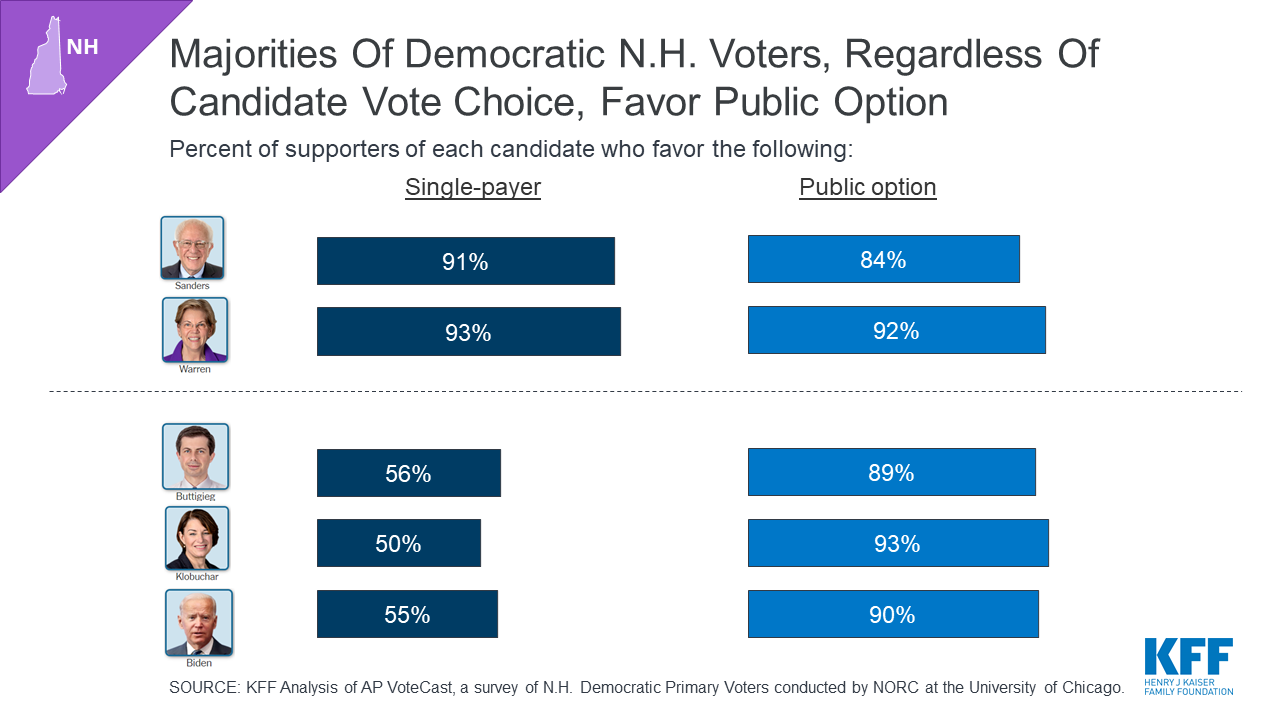
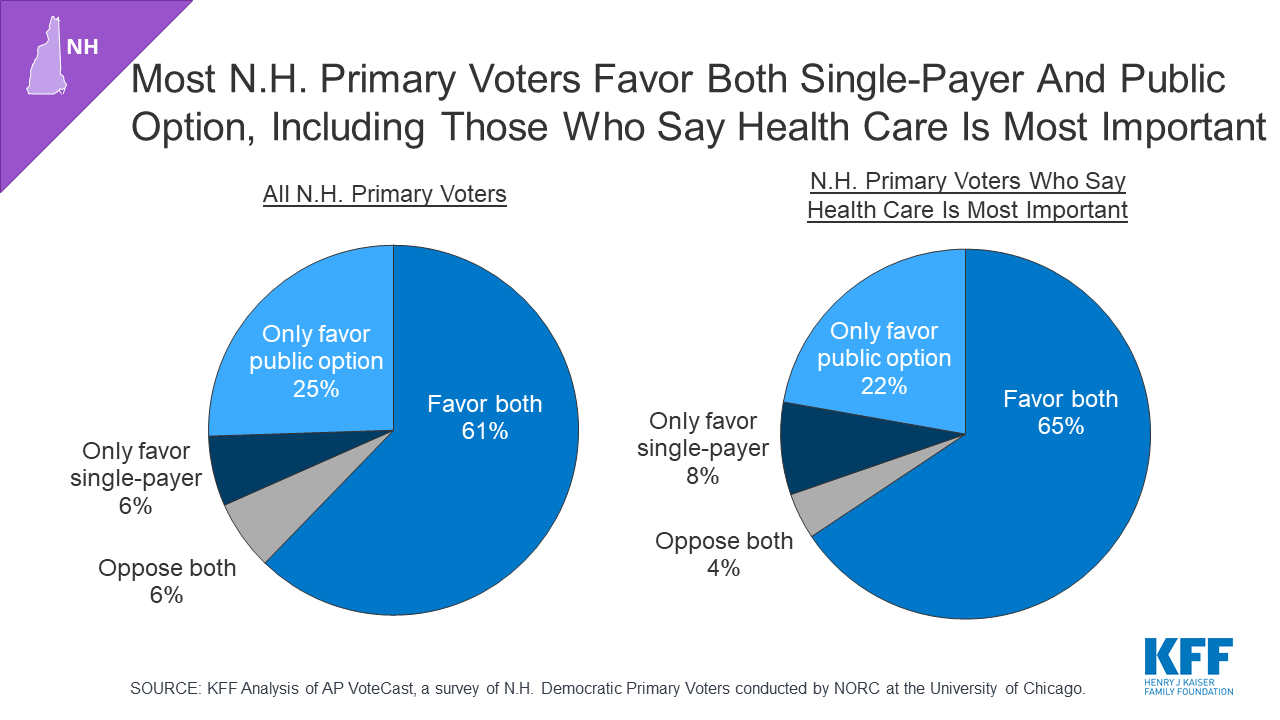
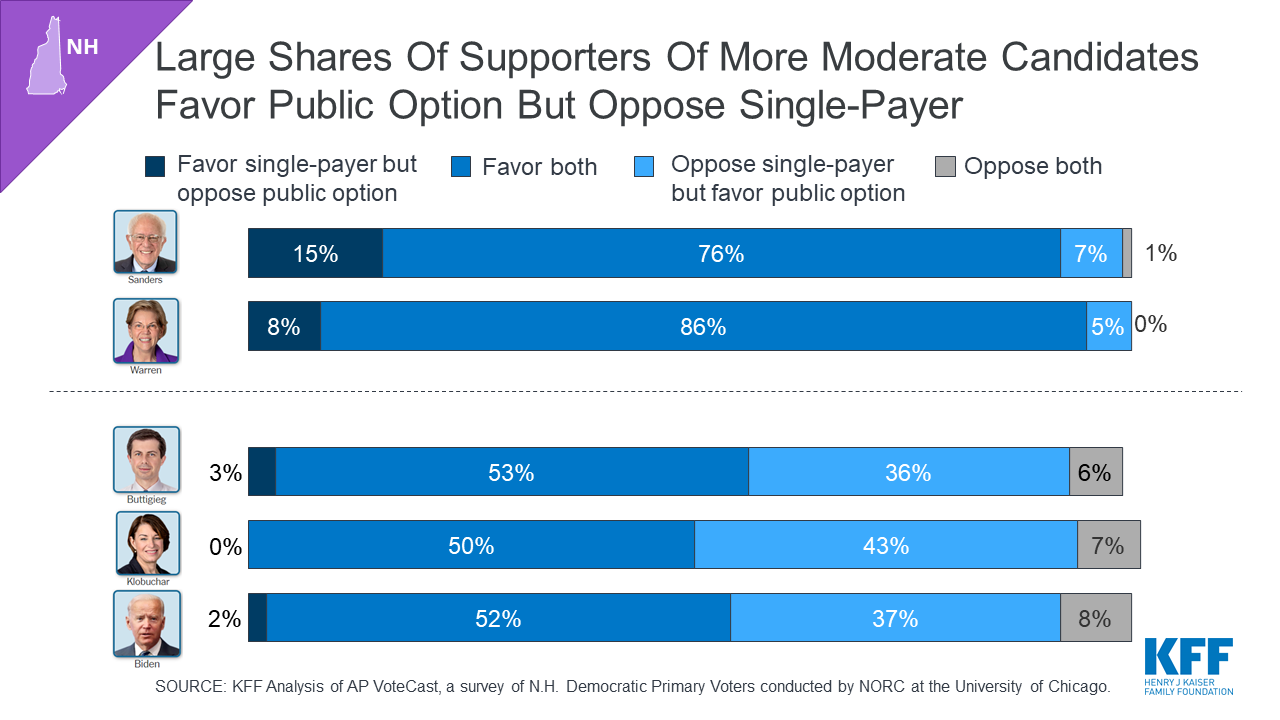
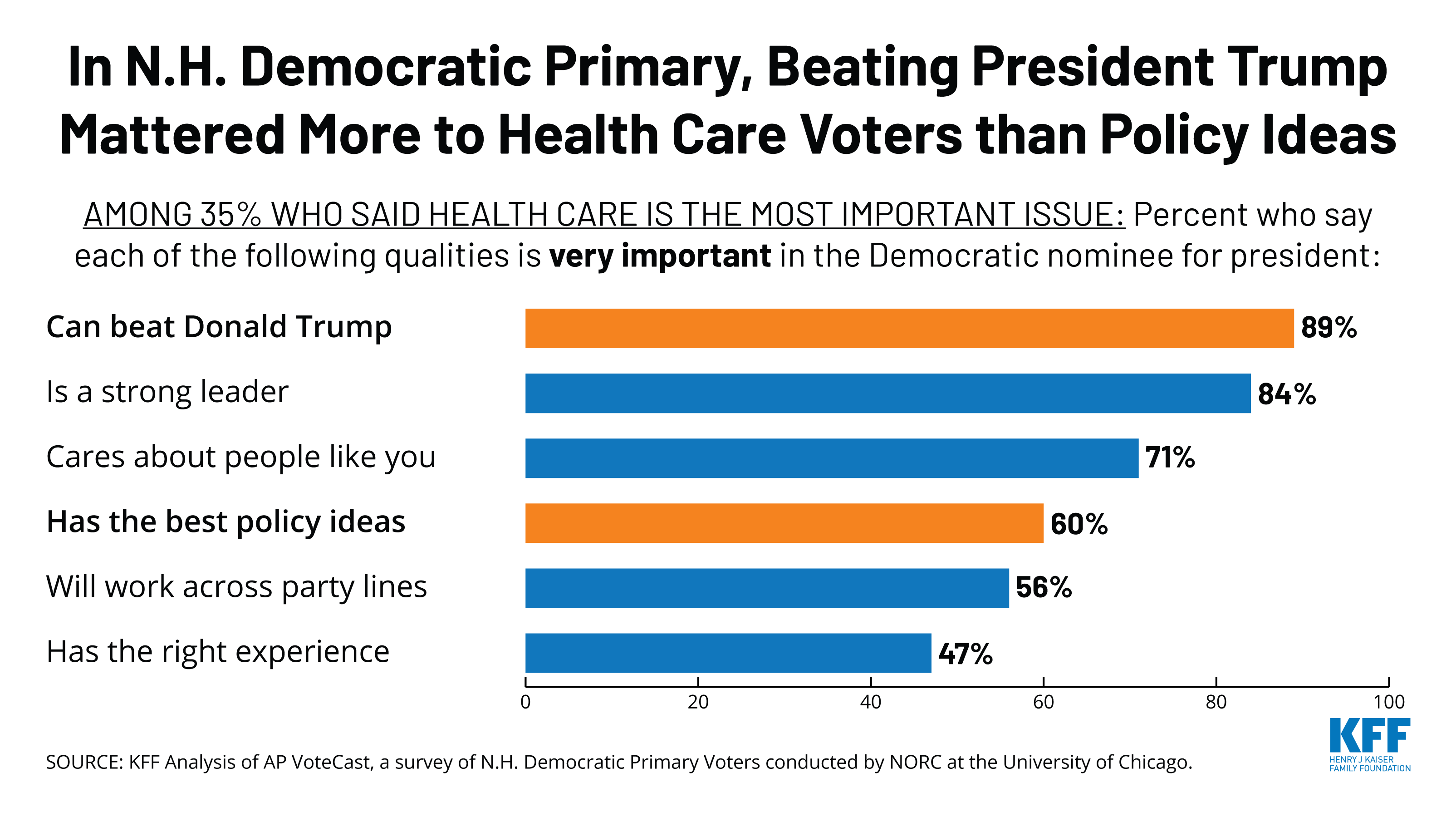
This slideshow examines the role of health care as an issue in the 2020 New Hampshire Democratic primary and is based on KFF analysis of AP VoteCast, a survey of New Hampshire primary voters conducted for the Associated Press by NORC at the University of Chicago.
The survey was conducted for seven days, concluding as polls closed, and is based on interviews conducted in English and Spanish with a random sample of 3,111 registered voters drawn from the state voter file. The margin of sampling error for results based on the full sample is plus or minus 3 percentage points. Find more details about AP VoteCast’s methodology here.
The White House released its FY 2021 budget request to Congress on February 10, 2020, which includes significant cuts to global health programs compared to the FY 2020 enacted levels. In addition, in some cases, these cuts are steeper than those proposed by the Administration in last year’s request. The FY 2021 budget request includes funding for U.S. global health programs at the State Department, the U.S. Agency for International Development (USAID), the Centers for Disease Control and Prevention (CDC), and the National Institutes of Health (NIH). Key highlights are as follows (see table for additional detail):
State Department & USAID:
Funding for global health programs through the Global Health Programs (GHP) account, which represents the bulk of global health assistance, totaled $5,998 million, a decrease of $3,095 million (34%) from the FY 2020 enacted level, and $346 million below the President’s FY 2020 request. Almost all program areas in the FY21 request declined compared to FY20 enacted levels.
Bilateral HIV funding through the President’s Emergency Plan for AIDS Relief (PEPFAR) is $3,180 million, $1,520 million below the FY20 enacted level, and $170 million below the FY20 Request ($3,350 million).
The request includes $658 million for the U.S. contribution to the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), a decrease of $902 million below the FY20 enacted level ($1,560 million) and $301 million below the FY20 Request ($958 million). The administration states that the U.S. will match $1 for every $3 contributed by other donors and that, when combined with already appropriated funding, this will keep the U.S. on track to meet its $3.3 billion pledge for the Global Fund’s sixth replenishment.
Funding for tuberculosis (TB) totals $275 million, $35 million below the FY20 enacted level ($310 million), and $14 million below the FY20 Request ($261 million).
Funding for malaria totals $709 million, $62 million below the FY20 enacted level ($770 million), and $35 million below the FY20 Request ($674 million).
The request includes $660 million for maternal and child health (MCH), a decrease of $191 million below the FY20 enacted level ($851 million), and $40 million below the FY20 Request ($620 million). This decrease is to bilateral MCH funding. Gavi, the Vaccine Alliance, which is included under MCH funding, is the only program area that did not decline compared to the FY20 enacted level; funding totals $290 million, matching the FY20 enacted level, and $40 million above the FY20 Request ($250 million).
Funding for nutrition totals $90 million, $60 million below the FY20 enacted level ($150 million), and $12 million below the FY20 Request ($79 million).
Bilateral family planning and reproductive health (FP/RH) funding totals $237 million, $287 million below the FY20 enacted level ($524 million), and the same level as requested in FY20 ($237 million). The FY21 Request proposed eliminating funding for the United Nations Population Fund (UNFPA). In FY20, Congress provided $32.5 million for the U.S. contribution to UNFPA. However, it is anticipated that the Trump Administration will invoke the Kemp-Kasten amendment to withhold this funding again (learn more about the Kemp Kasten amendment here).
The FY21 Request proposed eliminating funding for the vulnerable children program, which was funded at $25 million in FY20.
Funding for neglected tropical diseases (NTDs) totals $75 million, $28 million below the FY20 enacted level ($103 million), and matching the FY20 Request ($75 million).
Funding for global health security totals $90 million, a decrease of $10 million below the FY20 enacted level ($100 million) and matching the FY20 Request.
Funding to replenish the Emergency Reserve Fund, which is used to “quickly and effectively respond to emerging disease outbreaks,” totals $25 million; in FY20, Congress provided the authority to transfer $10 million in funding from other areas to the Emergency Reserve Fund if needed.
Funding for the World Health Organization (WHO) totaled $58 million, a $65 million decrease compared to the FY20 enacted level ($123 million) and flat compared to the FY20 Request.
Funding for the Pan American Health Organization (PAHO) totaled $16 million, a $50 million decrease compared to the FY20 enacted level ($66 million) and a $17 million decrease compared to the FY20 Request ($33 million).
Centers for Disease Control and Prevention (CDC): Funding for global health provided to the CDC totals $532 million, a decrease of $39 million compared to the FY20 enacted level ($571 million) and $75 million above the FY20 Request ($457 million). The entire increase in CDC funding is to support global health security activities; all other areas declined except global tuberculosis funding which remained flat. For example, funding for global HIV activities in the request declined by $59 million and funding for global immunization activities declined by $20 million.
Fogarty International Center (FIC): Funding for the Fogarty International Center (FIC) at the National Institutes of Health (NIH) totaled $74 million, $7 million below the FY 2020 enacted level ($81 million) and $7 million above the FY20 Request ($67 million).
The table (.xls) below compares global health funding in the FY 2021 request to the FY 2020 enacted funding amounts as outlined in the “Consolidated Appropriations Act, 2020” (P.L. 116-94; KFF summary here) and the FY 2020 request (KFF summary here). Note that total funding for global health is not currently available as some funding provided through USAID, Health and Human Services (HHS), and the Department of Defense (DoD) is not yet available.
Table: KFF Analysis of FY21 Budget Request for Global Health
Department / Agency / Area
FY20 Requesti(millions)
FY20 Enacted(millions)
FY21Requesti(millions)
Difference(millions)
FY21 Request – FY20 Request
FY21 Request – FY20 Enacted
SFOPs – Global Health
HIV/AIDS
$3,350.0
$4,700.0
$3,180.3
$-169.7 (-5%)
$-1,519.7 (-32%)
State Department
$3,350.0
$4,370.0
$3,180.3
$-169.7(-5%)
$-1,189.7(-27%)
USAID
$0.0
$330.0
$0.0
$0(NA)
$-330.0(-100%)
of which Microbicides
$0.0
$45.0
$0.0
$0(NA)
$-45.0(-100%)
Global Fund
$958.4
$1,560.0
$657.6
$-300.8 (-31%)
$-902.4 (-58%)
Tuberculosisii
$262.0
–
–
–
–
Global Health Programs (GHP) account
$261.0
$310.0
$275.0
$14(5%)
$-35(-11%)
Economic Support Fund (ESF) account
$1.0
Not available
Not available
–
–
Malaria
$674.0
$770.0
$708.5
$34.5 (5%)
$-61.5 (-8%)
Maternal & Child Health (MCH)iii
iv
–
–
–
–
GHP accountv
$619.6
$851.0
$659.6
$40(6%)
$-191.4(-22%)
of which Gavi
$250.0
$290.0
$290.0
$40(16%)
$0(0%)
of which Poliov
$16.0
$61.0
Not available
–
–
UNICEFvi
Not available
$139.0
Not available
–
–
ESF account
$75.5
Not available
Not available
–
–
of which Poliov
$7.0
v
Not available
–
–
Nutritionvii
$89.7
–
–
–
–
GHP account
$78.5
$150.0
$90.0
$11.5(15%)
$-60(-40%)
ESF account
$11.2
Not available
Not available
–
–
Family Planning & Reproductive Health (FP/RH)
$259.0
$607.5
–
–
–
Bilateral FPRH
$259.0
$575.0
–
–
–
GHP account
$237.0
$524.0
$237.0
$0(0%)
$-287(-55%)
ESF account
$22.0
$51.1
Not available
–
–
UNFPA
$0.0
$32.5
$0.0
$0(NA)
$-32.5(-100%)
Vulnerable Children
$0.0
$25.0
$0.0
$0(NA)
$-25.0(-100%)
Neglected Tropical Diseases (NTDs)
$75.0
$102.5
$75.0
$0 (0%)
$-27.5 (-27%)
Global Health Security
$90.0
$100.0
$90.0
$0 (0%)
$-10 (-10%)
GHP account
$90.0
$100.0
$90.0
$0(0%)
$-10(-10%)
Emergency Reserve Fund
$0.0
viii
$25.0
$25.0(NA)
–
Other (Non-GHP account)
$90.8
$188.4
$74.2
$-16.6(-18%)
$-114.2(-61%)
World Health Organization (WHO)ix
$57.9
$122.7
$57.9
$0(0%)
$-64.7(-53%)
Pan American Health Organization (PAHO)ix
$32.9
$65.8
$16.3
$-16.6(-50%)
$-49.5(-75%)
SFOPs Total (GHP account only)
$6,343.5
$9,092.5
$5,998.0
$-345.5(-5%)
$-3,094.5(-34%)
Health & Human Services (HHS)
Centers for Disease Control & Prevention (CDC) – Total Global Health
$457.0
$570.8
$532.2
$75.2 (16%)
$-38.6 (-7%)
Global HIV/AIDS
$69.5
$128.4
$69.5
$0(0%)
$-58.9(-46%)
Global Tuberculosisx
$7.2
$7.2
$7.2
$0(0%)
$0(0%)
Global Immunization
$206.0
$226.0
$206.0
$0(0%)
$-20(-9%)
Polio
Not available
$176.0
$165.0
–
$-11(-6%)
Other Global Vaccines/Measles
Not available
$50.0
$41.0
–
$-9(-18%)
Parasitic Diseases
$24.5
$26.0
$24.5
$0(0%)
$-1.5(-6%)
Global Public Health Protectionxi
$149.8
$183.2
$225.0
$75.2(50%)
$41.8(23%)
Global Disease Detection and Emergency Response
Not available
$173.4
Not available
–
–
of which Global Health Security (GHS)
$99.8
$125.0
$175.0
$75.2(75%)
$50(40%)
Global Public Health Capacity Development
Not available
$9.8
Not available
–
–
National Institutes of Health (NIH) – Total Global Health
$760.1
Not available
Not available
–
–
HIV/AIDS
$511.1
Not available
Not available
–
–
Malaria
$182.0
Not available
Not available
–
–
Fogarty International Center (FIC)
$67.0
$80.8
$73.5
$6.5(10%)
$-7.2(-9%)
Notes:
i – In the FY20 and FY21 Request, the administration proposed to consolidate the Development Assistance (DA), Economic Support Fund (ESF), the Assistance for Europe, Eurasia, and Central Asia (AEECA), and the Democracy Fund (DF) accounts in to one new account — the Economic Support and Development Fund (ESDF). ESF funding for the FY20 Request reflects the amounts requested by the administration for ESDF.
ii – Some tuberculosis funding is provided under the ESF account, which is not earmarked by Congress in the annual appropriations bills and determined at the agency level (e.g. in FY18, TB funding under the ESF account totaled $4 million).
iii – Some MCH funding is provided under the ESF account, which is not earmarked by Congress in the annual appropriations bills and determined at the agency level (e.g. in FY18, MCH funding under the ESF account totaled $15.5 million).
iv – It is not possible to calculate total MCH funding in the FY20 and FY21 request because UNICEF, which has historically received funding through the International Organizations and Programs (IO&P) account, was not specified in the FY20 and FY21 request.
v – The minority summary of the FY20 conference agreement states that part of the increase in MCH funding is “due to a shift of $7.5 million for polio prevention programs from the Economic Support Fund account to the Global Health Programs account.”
vi – UNICEF funding in the FY20 Conference Agreement includes an earmark of $5 million for programs addressing female genital mutilation.
vii – Some nutrition funding is provided under the ESF account, which is not earmarked by Congress in the annual appropriations bills and determined at the agency level. (e.g. in FY17, nutrition funding under the ESF account totaled $21 million).
viii – The explanatory statement accompanying the FY20 Conference Agreement states that the “agreement includes authority to reprogram $10,000,000 of Global Health Program funds to the Emergency Reserve Fund if necessary to replenish amounts used during fiscal year 2020 to respond to emerging health threats.”
ix – The FY20 enacted WHO and PAHO amounts are estimates.
x – In FY20, the administration proposed to formally transfer $7.2 million from the “HIV/AIDS, Viral Hepatitis, STI and TB Prevention” account to “Global Tuberculosis” activities under “Global Health Programs” at CDC. The FY20 conference agreement formalizes this transfer.
xi – In the CDC FY20 congressional justification, this funding line is titled “Global Disease Detection and Other Programs”.
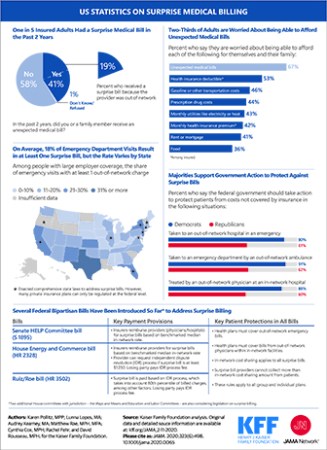
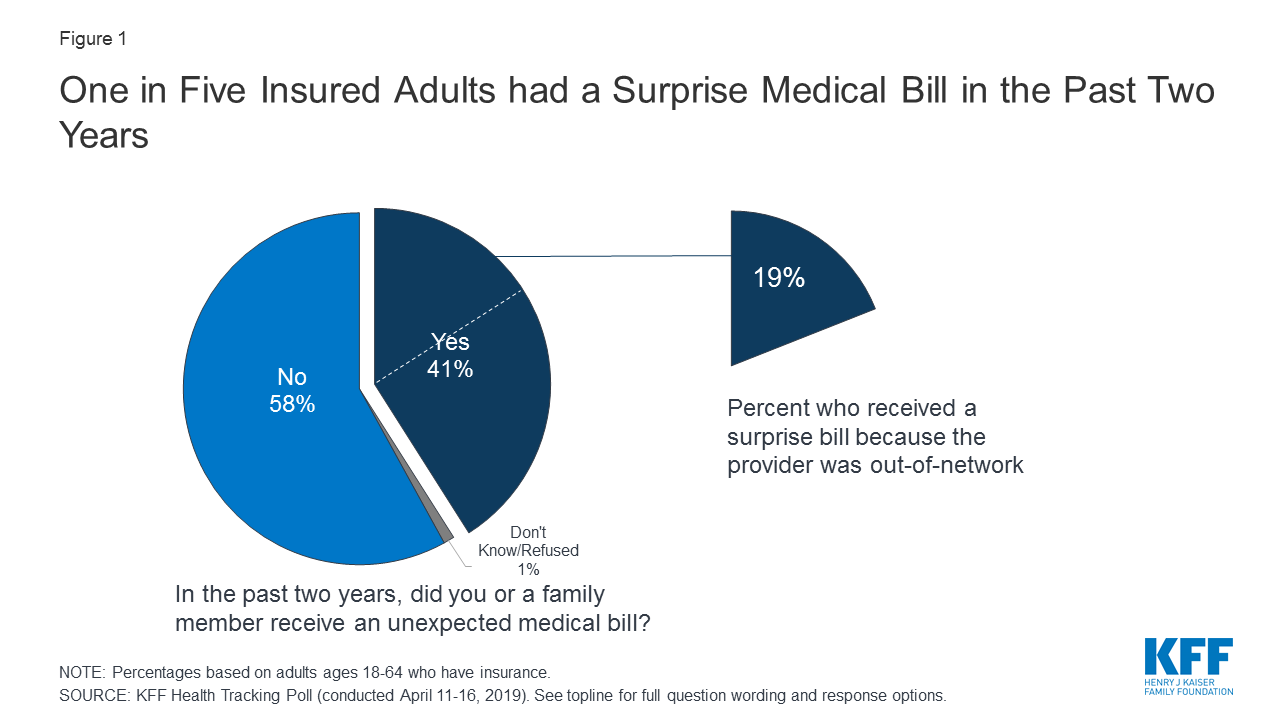
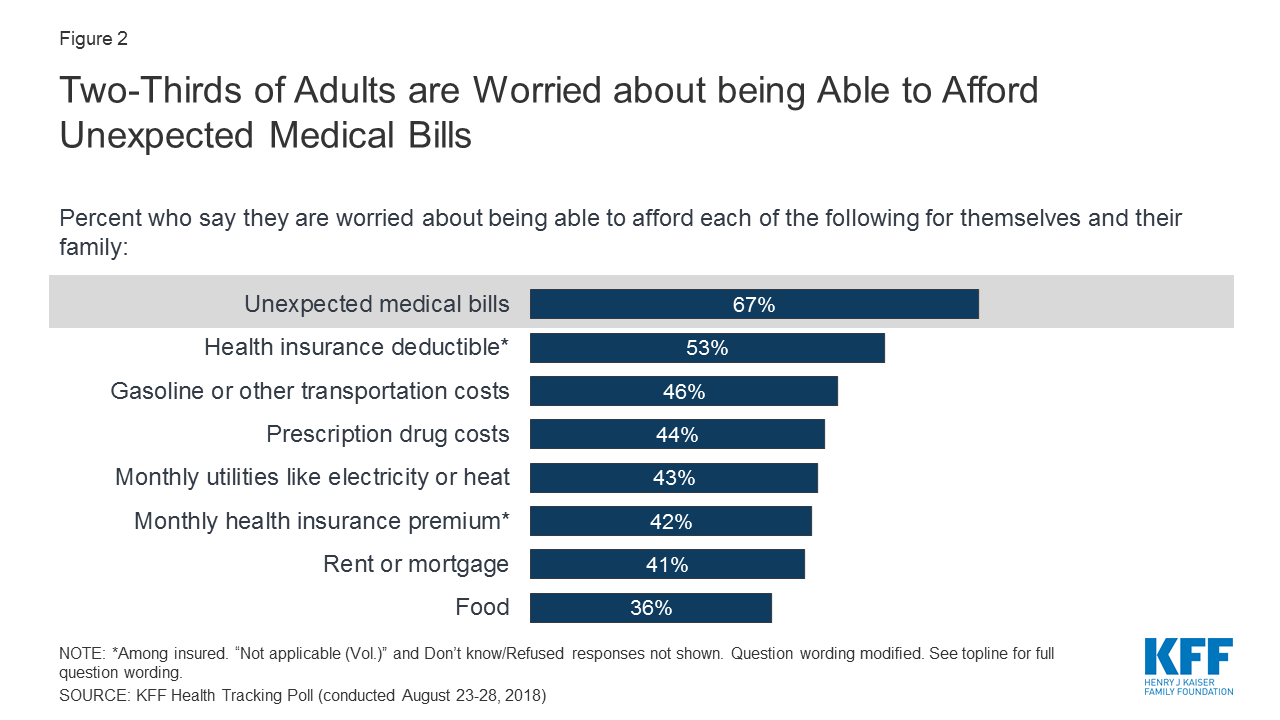
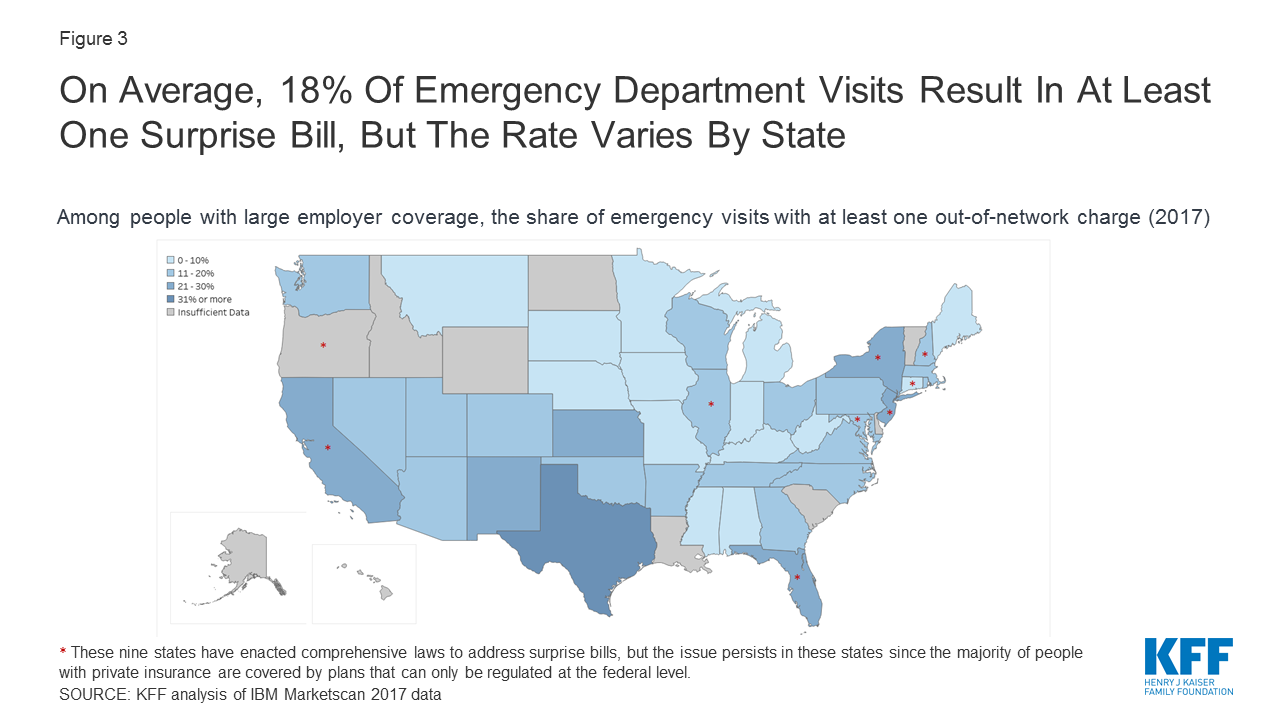
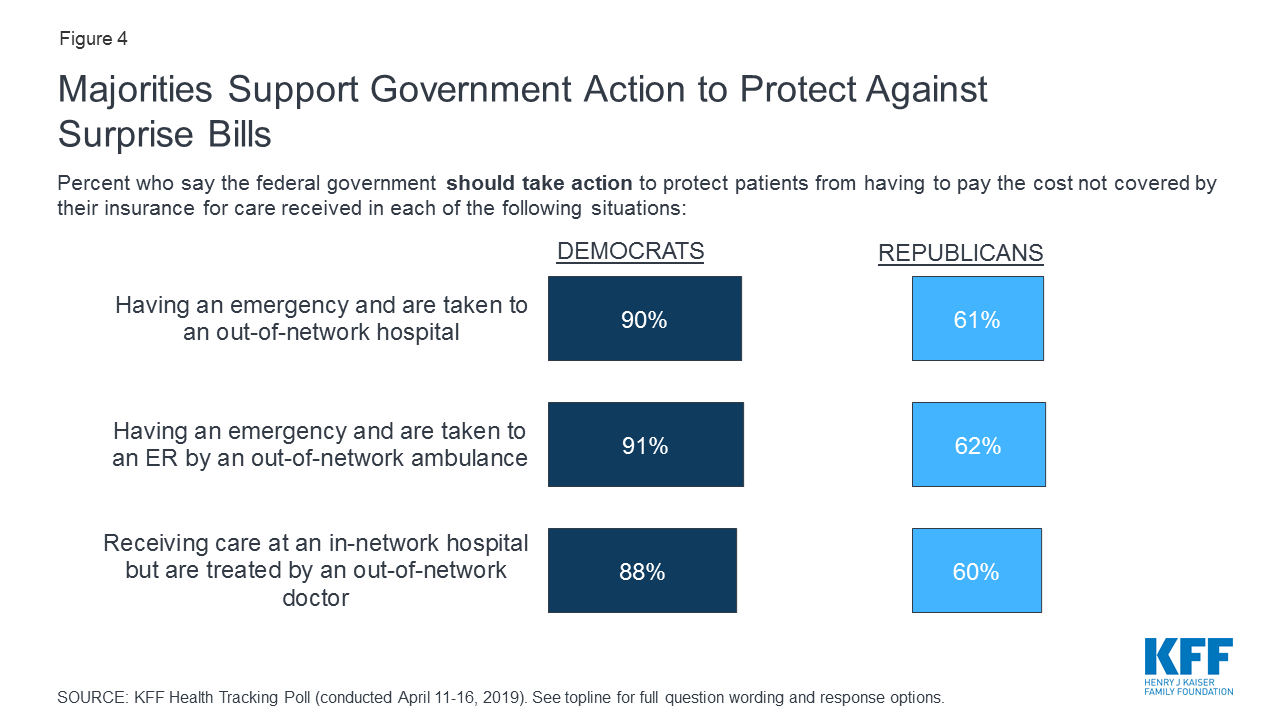
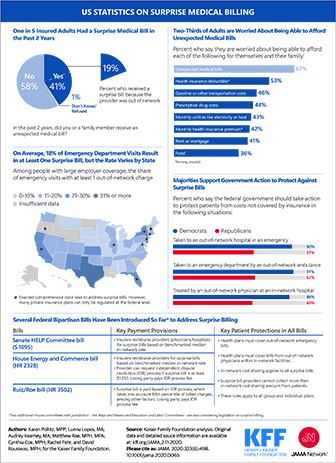
This Visualizing Health Policy infographic looks at the experience of unexpected or “surprise” medical bills in the United States. Out-of-network charges typically expose individuals to higher cost-sharing when they use services, and may lead to balance billing – in which providers bill patients directly, and often unexpectedly, at a higher rate. In the past two years, one in five insured adults had an unexpected medical bill from an out-of-network provider. Overall, two-thirds of adults are worried about affording these bills for themselves and their family. In emergency rooms across the country, 18 percent of visits result in at least one surprise bill, but rates vary by state. Politically, majorities of Democrats and Republicans support government action to protect patients against these unexpected bills. This infographic sources analysis and polling from KFF as well as the Peterson-KFF Health System Tracker.
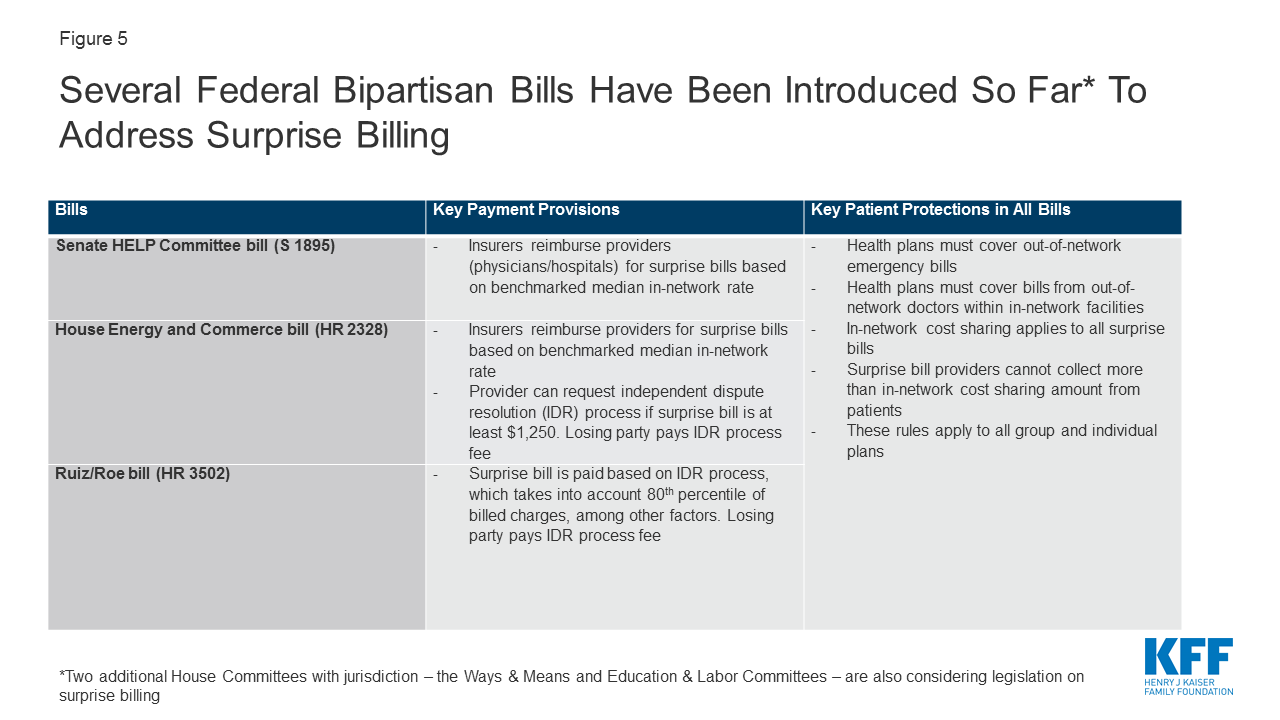
Visualizing Health Policy is an infographic series produced in partnership with the Journal of the American Medical Association (JAMA). The full-size infographic is freely available on JAMA’s website and is published in the print edition of the journal. The most recent developments on surprise billing legislation are tracked here.
The source slides for this infographic can be viewed below or downloaded here.
This Visualizing Health Policy infographic looks at the experience of unexpected or “surprise” medical bills in the United States. Out-of-network charges typically expose individuals to higher cost-sharing when they use services, and may lead to balance billing – in which providers bill patients directly, and often unexpectedly, at a higher rate. In the past two years, one in five insured adults had an unexpected medical bill from an out-of-network provider. Overall, two-thirds of adults are worried about affording these bills for themselves and their family. In emergency rooms across the country, 18 percent of visits result in at least one surprise bill, but rates vary by state. Politically, majorities of Democrats and Republicans support government action to protect patients against these unexpected bills. This infographic sources analysis and polling from KFF as well as the Peterson-KFF Health System Tracker.
With health care a top issue in the 2020 election, test your knowledge about health facts, policy issues and proposals that are emerging among the presidential candidates.
Take the quiz, share a link to the quiz with your colleagues and friends, and post your score on Twitter.
While every Democratic debate so far featured a slugfest among the candidates over the question of building on the Affordable Care Act by adding a public option or scrapping the current system in favor of Medicare-for-all, there hasn’t been nearly as much discussion of bringing down prescription drug prices.
In this February 2020 post for The JAMA Forum, Larry Levitt examines both the Democratic candidates’ proposals and the Trump administration’s record on lowering drug prices, which remains a top issue for the public with bi-partisan support.
Other contributions to The JAMA Forum are also available.