KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Ensuring racial and ethnic diversity in clinical trials for development of COVID-19 vaccines is particularly important since COVID-19 has taken a heavy disproportionate toll on people of color, and people of color, particularly Black adults, historically have had lower vaccination rates and express more concerns about getting a COVID-19 vaccine compared to their White counterparts. Diversity within clinical trials for a COVID-19 vaccine helps ensure safety and effectiveness across populations and may increase confidence in getting the vaccine among people of color. Historically, people of color have been underrepresented in clinical trials. There have been recent efforts to increase racial diversity within clinical trials and specific efforts to increase diversity within the trials associated with development of COVID-19 vaccines. With two COVID-19 vaccines now authorized in the U.S. (the Pfizer-BioNTech and Moderna vaccines), we review why racial diversity within COVID-19 vaccine clinical trials is important, discuss the barriers to participation in clinical trials among people of color, and examine the racial/ethnic composition of clinical trial participants for the Pfizer-BioNTech and Moderna vaccines.
Why is it important to have diversity within the COVID-19 vaccine trials?
Diverse racial/ethnic representation in COVID-19 vaccine trials is important because drugs and vaccines can differentially affect groups reflecting variation in underlying experiences and environmental exposure. Clinical trials are research studies that determine whether medical products like medicines, vaccines, or devices are safe and effective. It important for participants in clinical trials to represent the patients that will be using the medical products since responses may vary across patient groups. In general, to be representative, vaccine trials should enroll people of color in percentages similar to their representation in the population. However, since people of color have been disproportionately affected by COVID-19 pandemic, scientists, including Dr. Fauci, have indicated that the COVID-19 vaccine trials should overrepresent people of color compared to their population share.
Why are people of color underrepresented in clinical trials?
Access barriers, lack of information, and historic and ongoing racism and discrimination contribute to underrepresentation of people of color in clinical trials. People of color face an array of structural access-related barriers to participating in trials. For example, fewer clinical trials are available through under-resourced hospital systems where people of color are more likely to receive care, and people of color may be less likely to be eligible to participate in trials if being uninsured or having co-morbidities excludes individuals from participation. Other access challenges, such as prohibitive distance to trial sites for people with limited transportation options, limited flexibility in work and caregiving schedules, and lack of access to technology for monitoring that may be required as part of the trial also may increase barriers to participation among people of color. Beyond these challenges, lack of awareness and information may limit participation. For example, some research suggests that physicians are less likely to discuss clinical trials with patients of color. Further, enrollment efforts may not effectively reach people of color if they are not culturally appropriate and do not address differences in language and health literacy. Moreover, the medical system’s historic abuse and mistreatment of people of color, including but not limited to the infamous Tuskegee syphilis experiment, as well as ongoing racism and discrimination in health care today may contribute to less willingness among people of color to participate in clinical trials.
What steps are being taken to increase racial diversity within clinical trials?
There have been ongoing efforts to increase diversity in clinical trials broadly and specific to development of COVID-19 vaccines. The Federal Drug Administration (FDA) is engaged in a range of efforts to encourage greater diversity in clinical trials, including creating a public-facing education and outreach campaign and working with varied stakeholders. It also developed recommendations to industry and agency staff on how to collect race and ethnicity data in clinical trials. The National Institutes of Health (NIH) has longstanding guidelines on the inclusion of women and minorities as subjects in clinical research. In addition to these general guidelines, there have been specific efforts focused on COVID-19 vaccine trials. For example, in June 2020, the FDA offered nonbinding recommendations to the industry on development and licensure of COVID-19 vaccines that strongly encouraged the “enrollment of populations most affected by COVID-19, specifically racial and ethnic minorities.” Both Pfizer and Moderna have said they worked to ensure that people of color were included in their trials, with Moderna even slowing down enrollment to try to enroll more racial and ethnic minorities. There have also been efforts on the community side. For example, historically Black colleges and universities are participating in COVID-19 vaccine trials and encouraging participation among their communities.
How diverse are participants in COVID-19 vaccine trials?
Pfizer-BioNTech and Moderna have reported the racial/ethnic composition of the participants in the late-stage clinical trials for their COVID-19 vaccines. Pfizer-BioNTech and Moderna provided demographic data for participants in their late-stage clinical trials, including racial/ethnic composition, as part of their emergency use authorization (EUAs) applications to the FDA. These data show, that, overall, people of color are underrepresented in these trials relative to their share of the total U.S. population (Table 1), with the largest disparity among the Black population. While the trials have not included the overrepresentation of people of color that some had suggested, as noted above, these trials have achieved greater diversity than many previous trials for other drugs. In both COVID-19 trials, the demographics of the placebo and vaccine groups are similar, as are the characteristics between all participants and the safety populations (the group of individuals receiving the vaccine and followed for safety). In addition, similar vaccine efficacy results were observed across racial and ethnic groups in both the Pfizer and Moderna trials.
Table 1: Race/Ethnicity of Participants in Pfizer-BioNTech and Moderna COVID-19 Vaccine Clinical Trials
Total US Population Age 16+
Pfizer-BioNTech*
Moderna
Total
258 million
40,277
27,817
Race
White
73.6%
81.9%
79.4%
Black
12.3%
9.8%
9.7%
Asian
5.9%
4.4%
4.7%
American Indian/Alaska Native
0.8%
0.6%
0.8%
Native Hawaiian or Other Pacific Islander
0.2%
0.2%
0.2%
Ethnicity
Hispanic
17.6%
26.2%
20.0%
Non-Hispanic
82.4%
73.2%
79.1%
NOTES: *Pfizer-BioNTech data are for all participants globally; of which 76.7% are in the United States. Pfizer results provided for Phase 2/3 trial, Moderna results for Phase 3 trial. The Pfizer trial included those ages 16 and older. The Moderna trial included those ages 18 and older.SOURCES: Racial/ethnic distribution of total population age 16 or older based on KFF analysis of 2019 American Community Survey data; FDA, Briefing Document: Pfizer-BioNTech COVID-19 Vaccine, December 10, 2020; FDA, Briefing Document: Moderna COVID-19 Vaccine, December 17, 2020
What are implications of diversity in COVID-19 vaccine trials for vaccination efforts?
These data show that although people of color are underrepresented in the clinical trials for the two initial COVID-19 vaccines compared to their share of the population, the trials include people from diverse racial/ethnic backgrounds and are more diverse than some trials have historically been. The findings showing that vaccine safety and efficacy were similar for people of color and White participants could help increase confidence in willingness to get the vaccine, particularly among Black adults who are more likely than White adults to point to concerns about safety and side effects as major reasons for why they probably or definitely would not get the vaccine. As such, information on the diversity of participants in the clinical trials and the trials’ findings on safety and efficacy for people of color could be an important component of outreach and education campaigns and vaccination efforts that could help prevent disparities in vaccination.
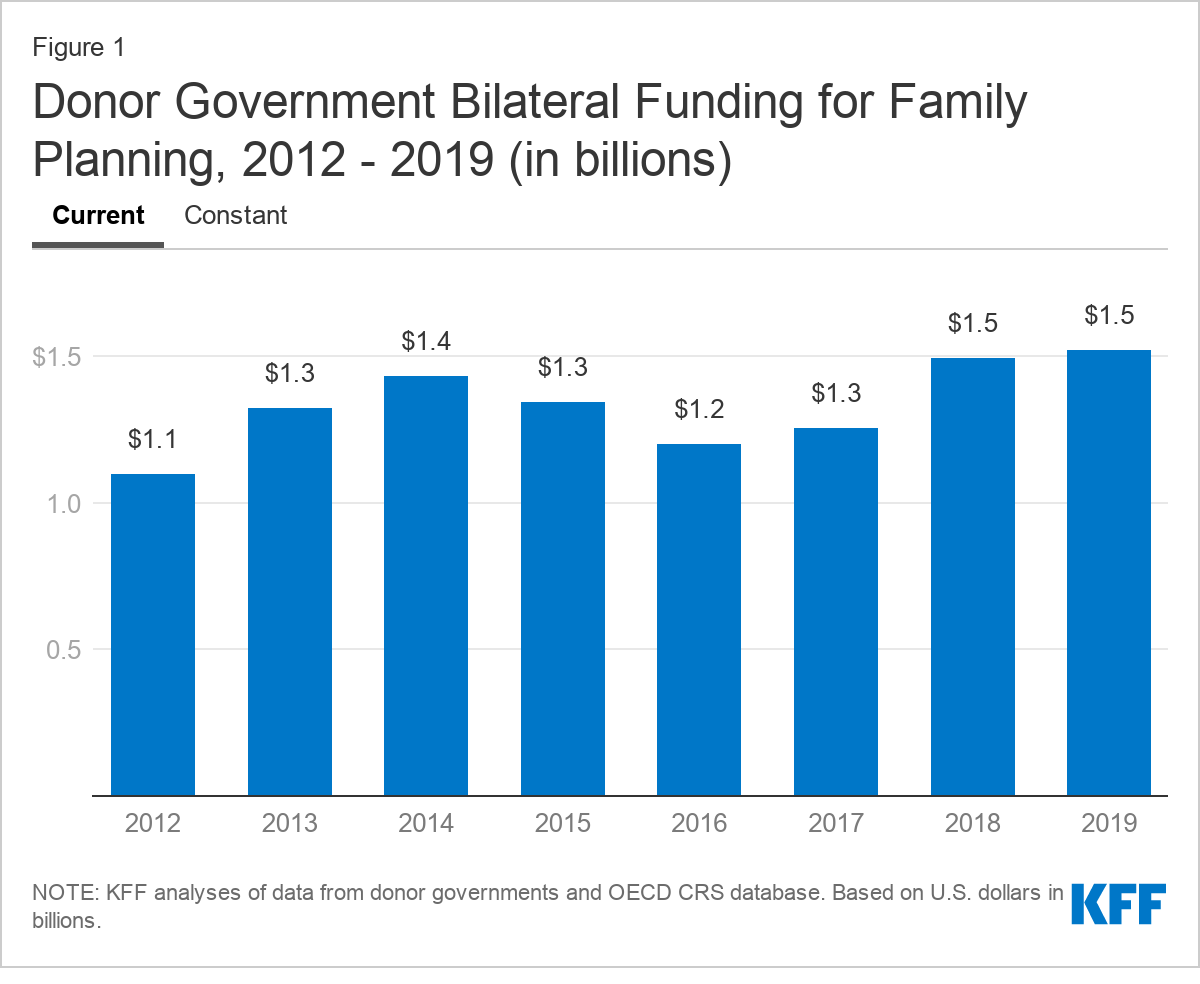
A new KFF analysis finds donor government support for global family planning efforts totaled US$1.5 billion in 2019, matching the previous year’s record level and well above the US$1.1 billion in 2012 since the London Summit on Family Planning that created an international goal of increasing family planning services.
The funding helps to support a range of activities including contraceptives, information, education and communication activities; and capacity building and training in low- and middle- income countries. It reflects donor nation’s funding decisions prior to the global COVID-19 pandemic and does not reflect any changes in priorities sparked by that crisis.
Key findings include:
Half of donors increased bilateral funding in 2019 (Australia, Canada, Norway, Sweden, and the U.K.) while the other half decreased funding (Denmark, France, Germany, the Netherlands, and the U.S.).
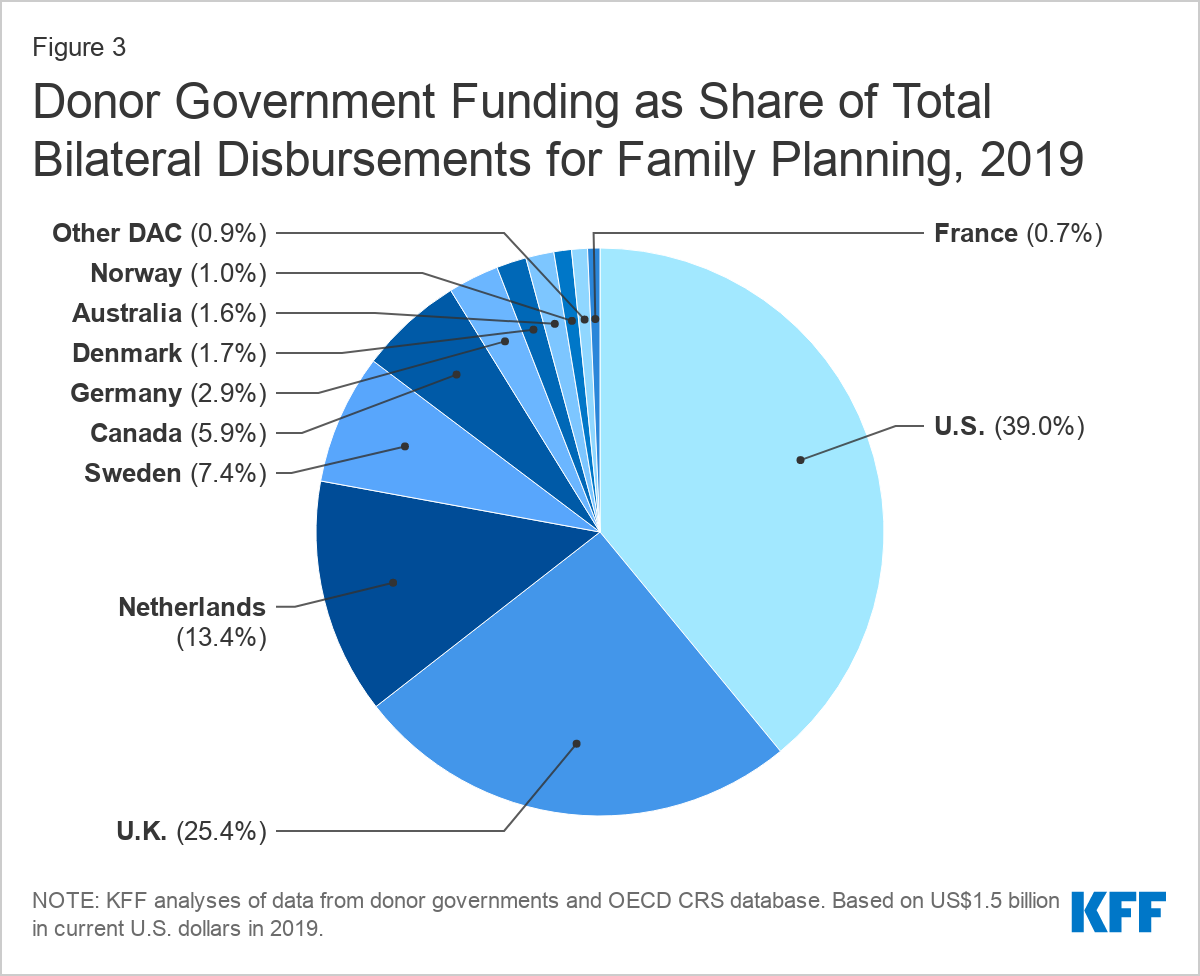
Despite a decline by the U.S., it remains the largest bilateral donor to family planning, providing US$592.5 million or 39% of total funding from donor governments. The decline is largely due to timing and does not reflect the actual U.S, appropriations by Congress, which have remained steady.
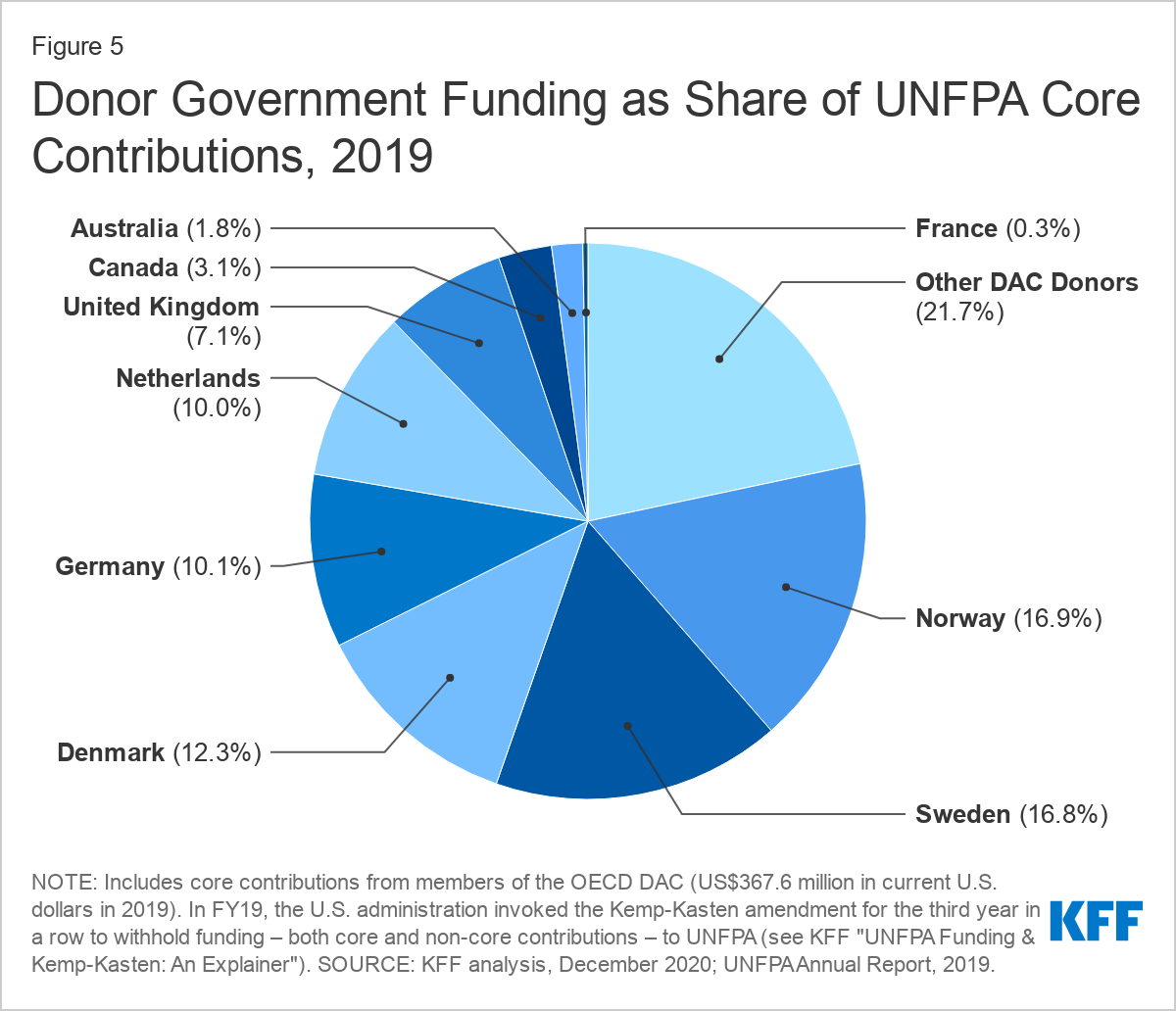
Funding for the multilateral United Nations Population Fund (UNFPA) remained steady in 2019, with Norway providing the largest contribution at US$62.0 million, followed by Sweden, Denmark, Germany, and the Netherland keeping the funding levels at US$367.6 million, similar to 2018 (US$374.1 million). The Trump administration withheld all U.S. support for UNFPA throughout its tenure.
Future funding levels for family planning could depend on the fallout from the COVID-19 pandemic and the changing U.S. administration priorities. The incoming Biden administration has expressed support for global family planning efforts and may seek additional funding, though any funding request would need to be approved by Congress.
Results of this analysis are also included in the annual progress report from FP2020, The Arc of Progress, a global partnership to monitor progress toward the 2012 London Summit on Family Planning goals to expand contraceptive access to an additional 120 million women and girls in low- and middle income countries by 2020.
This report provides an analysis of donor government funding to address family planning in low- and middle-income countries in 2019, the most recent year available, as well as trends over time. It is part of an effort by KFF (the Kaiser Family Foundation) to track such funding that began after the London Summit on Family Planning in 2012. Importantly, these findings reflect political funding decisions made before the COVID-19 pandemic and therefore precede possible effects on donor government spending for family planning. At the same time, data have already shown that family planning services have been disrupted by COVID-19, which could exacerbate unmet needs. Key findings include:
DONOR GOVERNMENT FUNDING FOR FAMILY PLANNING WAS ESSENTIALLY FLAT COMPARED TO THE PRIOR YEAR. In 2019, donor government funding for family planning totaled US$1.5 billion, on par with peak-level 2018 funding (US$1.5 billion).1
HALF OF DONORS INCREASED BILATERAL FUNDING FOR FAMILY PLANNING IN 2019. Among the 10 donor governments profiled, five increased bilateral funding (Australia, Canada, Norway, Sweden, and the U.K.) and five decreased (Denmark, France, Germany, the Netherlands, and the U.S.); these trends were the same after adjusting for inflation and exchange rate fluctuations, except for the Netherlands, which was level in currency of origin.
THE U.S. CONTINUES TO BE THE LARGEST DONOR TO FAMILY PLANNING. The U.S. was the largest bilateral donor to family planning in 2019 (even after a decline in funding compared to 2018), providing $592.5 million or 39% of total bilateral funding from governments.2 The U.K. (US$386.5 million, 25%) was the second largest donor, followed by the Netherlands (US$203.3 million, 13%), Sweden (US$113.1 million, 7%), and Canada (US$89.4 million, 6%).
DONOR FUNDING HAS GENERALLY INCREASED SINCE THE LONDON SUMMIT IN 2012, ALTHOUGH THERE HAVE BEEN FLUCTUATIONS OVER THE PERIOD. Funding from donor governments in 2019 was more than US$400 million above the 2012 level (US$1.1 billion). In addition, 2019 funding levels for seven of the ten donor governments profiled were higher than in 2012. Funding reached its highest level since the summit in 2018 and remained there in 2019.
FUNDING TO UNFPA REMAINED STEADY IN 2019, EVEN WITHOUT U.S. SUPPORT. In addition to bilateral funding for family planning, the donor governments profiled provided US$367.6 million in core contributions to UNFPA in 2019, similar to 2018 (US$374.1 million).3,4 Norway provided the largest core contribution (US$62.0 million), followed by Sweden (US$61.7 million), Denmark (US$45.3 million), Germany (US$37.0 million), and the Netherlands (US$36.7 million).The U.S. did not provide any funding to UNFPA in 2019. This was the third year in a row that the Trump administration invoked the Kemp-Kasten amendment to withhold funding from the organization.5
FUTURE FUNDING MAY DEPEND ON THE IMPACTS OF COVID-19 ON DONOR BUDGETS AND COUNTRY NEEDS, AND CHANGING U.S. ADMINISTRATION PRIORITIES. While donor government funding for family planning has generally increased since the London Summit, and more recently held steady, future levels could depend on the fall-out from the COVID-19 pandemic, including how significantly the pandemic affects donor budgets as well as needs on the ground. At the same time, the Biden Administration has expressed support for global family planning efforts and may seek additional funding for these efforts, though any funding request would need to be approved by Congress.
Report
Introduction
This report provides data on donor government funding for family planning activities in low- and middle-income countries in 2019, the most recent year available, as well as trends over time. It is part of an effort by KFF that began after the London Summit on Family Planning in 2012 and includes data from all 30 members of the Organisation for Economic Co-operation and Development (OECD)’s Development Assistance Committee (DAC), as well as non-DAC members where data are available.6 Data are collected directly from donors and supplemented with data from the DAC. Direct data collection was carried out for ten donor governments that account for 98% of total funding for family planning. Both bilateral assistance and core contributions to UNFPA are included. For more detail, see the below methodology.
Findings
Bilateral Funding
In 2019, donor governments provided US$1.5 billion in bilateral funding for family planning activities (see Figure 1, Table 1 & Appendix 2), on par with the 2018 level (US$1.5 billion), which was the highest level of funding since the London Summit in 2012.7 However, after adjusting for inflation and exchange rate fluctuations, funding in 2019 declined slightly compared to 2018.
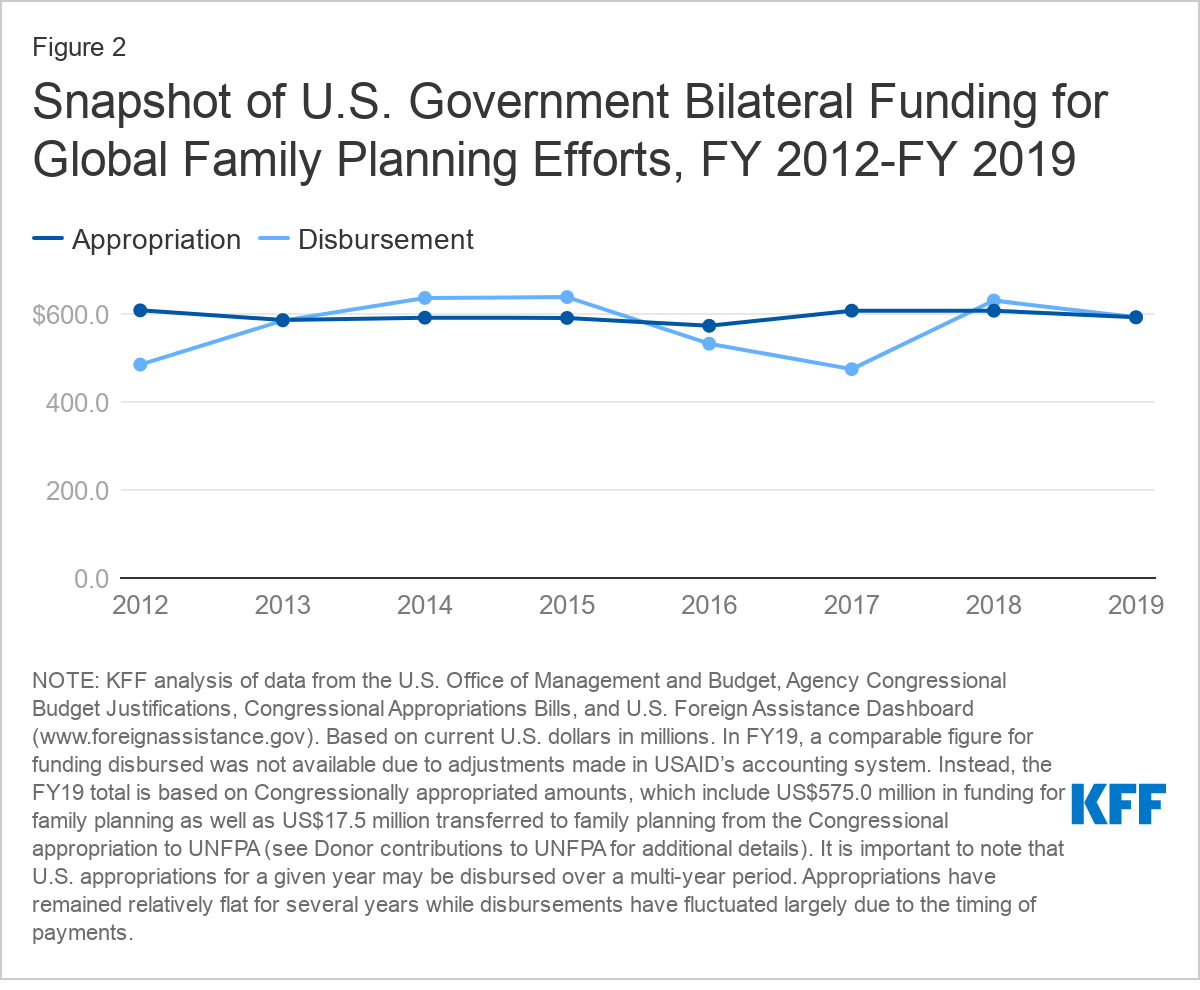
Among the ten donors for which direct data collection was conducted, half increased funding in 2019 (Australia, Canada, Norway, Sweden, and the U.K.) and half decreased (Denmark, France, Germany, the Netherlands, and the U.S.). These trends were the same after adjusting for inflation and exchange rate fluctuations, except for the Netherlands, which was flat in currency of origin. It is important to note that the U.S. decline was largely due to timing and does not reflect an actual decrease in U.S. appropriations, which are firm commitments that may be spent over a multi-year period. In fact, U.S. appropriations for family planning have remained steady in recent years (see Figure 2).8
Despite a decline in 2019, the U.S. remained the largest donor to family planning, accounting for 39% of donor government funding (see Figure 3).9 The U.K. (25%) was the second largest donor followed by the Netherlands (13%), Sweden (7%), and Canada (6%).
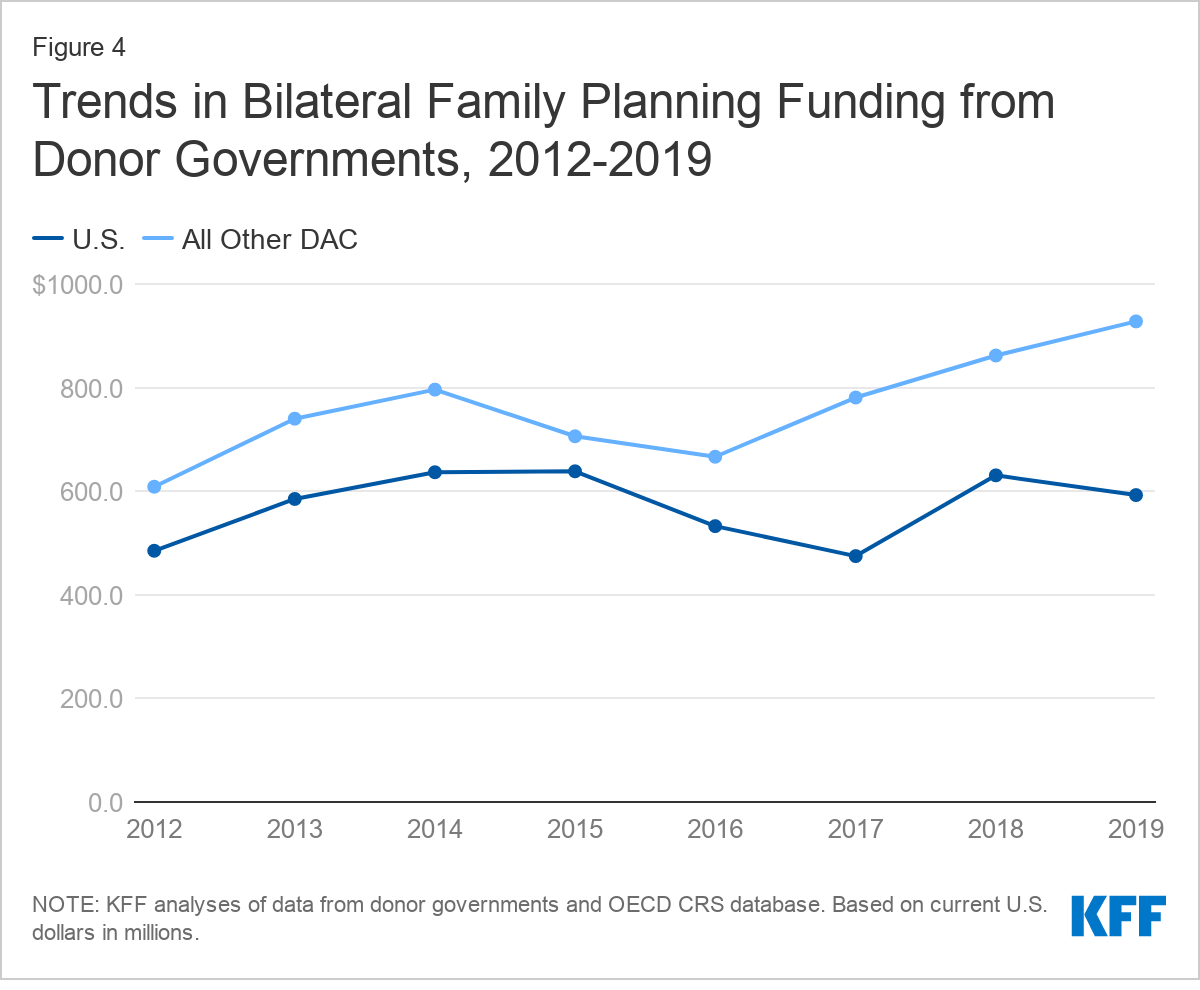
Donor government funding for family planning has generally risen since the London Summit in 2012, although totals have fluctuated over the period. Funding in 2019 (US$1.5 billion) was more than US$400 million above the 2012 level (US$1.1 billion) and includes increases from seven of the ten donors: Canada, Denmark, the Netherlands, Norway, Sweden, the U.K. and the U.S. If the U.S. is excluded, funding from all other donors rose from US$608.6 million to US$927.8 million, a more than US$300 million (52%) increase (see Figure 4).
Donor Contributions to UNFPA
While the majority of donor government assistance for family planning is provided bilaterally, donors also provide support for family planning activities through contributions to the United Nations Population Fund (UNFPA). Most of UNFPA’s funding is from donor governments, which provide funding in two ways: 1) donor directed or earmarked contributions for specific activities (e.g. donor contributions to the UNFPA Supplies), which are included as part of bilateral funding above; and 2) general contributions to “core” activities that are untied and meant to be used for both programmatic activities (e.g. family planning, population and development, HIV/AIDS, gender, and sexual and reproductive health and rights) and operational support as determined by UNFPA.
In 2019, the donor governments profiled provided US$367.6 million in core contributions to UNFPA, essentially flat compared to the 2018 level (US$374.1 million), even without U.S. support.10,11 Three donors increased funding (Denmark, France, and Germany), five remained flat (Australia, Canada, the Netherlands, Norway, and the U.K.), and one declined (Sweden). For the third year in a row, the Trump administration withheld funding from UNFPA.12
Norway provided the largest core contribution to UNFPA in 2019 (US$62.0 million), followed by Sweden (US$61.7 million), Denmark (US$45.3 million), Germany (US$37.0), and the Netherlands (US$36.7 million) (see Figure 5 and Table 2). Two donors – Demark and Norway - provided larger contributions to UNFPA’s core resources than their total bilateral funding for family planning.
Looking Ahead
While donor government funding for family planning has generally increased since the London Summit, and more recently held steady, future levels could depend on the fall-out from the COVID-19 pandemic, including how significantly the pandemic affects donor budgets as well as needs on the ground. At the same time, the Biden Administration has expressed support for global family planning efforts and may seek additional funding for these efforts, though any funding request would need to be approved by Congress. Given that the U.S. is the largest donor to global family planning efforts, any changes would have an outsized impact.
Methodology
Bilateral and multilateral data on donor government assistance for family planning (FP) in low- and middle-income countries were collected from multiple sources. The research team collected the latest bilateral assistance data directly for 10 governments: Australia, Canada, Denmark, Germany, France, the Netherlands, Norway, Sweden, the United Kingdom, and the United States during 2020. Data represent the fiscal year 2019 period. Direct data collection from these donors was desirable because they represent the preponderance of donor government assistance for family planning and the latest official statistics – from the Organisation for Economic Co-operation and Development (OECD) Creditor Reporting System (CRS) (see: http://www.oecd.org/dac/stats/data) – which are from 2018 and do not include all forms of international assistance (e.g., funding to countries such as Russia and the Baltic States that are no longer included in the CRS database). In addition, the CRS data may not include certain funding streams provided by donors, such as FP components of mixed-purpose grants to non-governmental organizations. Data for all other OECD DAC member governments – Austria, Belgium, Czech Republic, the European Union, Finland, Greece, Hungary, Iceland, Ireland, Italy, Japan, Korea, Luxembourg, New Zealand, Poland, Portugal, the Slovak Republic, Slovenia, Spain, and Switzerland – which collectively accounted for approximately 2 percent of bilateral family planning disbursements, were obtained from the OECD CRS and are from calendar year 2018.
For purposes of this analysis, funding was counted as family planning if it met the OECD CRS purpose code definition: “Family planning services including counselling; information, education and communication (IEC) activities; delivery of contraceptives; capacity building and training.” Where it was possible to identify funding amounts, family-planning-related activities funded in the context of other official development assistance sectors (e.g. education, civil society) are included in this analysis. Project-level data were reviewed for Canada, Denmark, France, Germany, the Netherlands, Norway, and Sweden to determine whether all or a portion of the funding could be counted as family planning. Family-planning-specific funding totals for the United States were confirmed through communication with government representatives. Funding attributed to Australia and the United Kingdom is based on a revised Muskoka methodology as agreed upon by donors at the London Summit on Family Planning in 2012. Funding totals presented in this analysis should be considered preliminary estimates based on data provided by representatives of the donor governments who were contacted directly.
It was difficult in some cases to disaggregate bilateral family planning funding from broader population, reproductive and maternal health totals, as the two are sometimes represented as integrated totals. In addition, family-planning-related activities funded in the context of other official development assistance sectors (e.g. education, civil society) have in the past remained largely unidentified. For purposes of this analysis, we worked closely with the largest donors to family planning to identify such family-planning-specific funding where possible. In some cases (e.g. Canada), specific FP percentages were recorded for mixed-purpose projects. In other cases, it was possible to identify FP-specific activities by project titles in languages of origin, notwithstanding less-specific financial coding. In still other cases, detailed project descriptions were analyzed (see Appendix for detailed data table).
Bilateral funding is defined as any earmarked (FP-designated) amount and includes family planning-specific contributions to multilateral organizations (e.g. non-core contributions to UNFPA Supplies). UNFPA contributions from all governments correspond to amounts received during the 2019 calendar year, regardless of which contributor’s fiscal year such disbursements pertain to.
With some exceptions, bilateral assistance data were collected for disbursements. A disbursement is the actual release of funds to, or the purchase of goods or services for, a recipient. Disbursements in any given year may include disbursements of funds committed in prior years and in some cases, not all funds committed during a government fiscal year are disbursed in that year. In addition, a disbursement by a government does not necessarily mean that the funds were provided to a country or other intended end-user. Enacted amounts represent budgetary decisions that funding will be provided, regardless of the time at which actual outlays, or disbursements, occur. In recent years, most governments have converted to cash accounting frameworks, and present budgets for legislative approval accordingly; in such cases, disbursements were used as a proxy for enacted amounts.
U.S. totals represent disbursements during the fiscal year (October 1 – September 30) for the period between 2012-2018. In FY 2019, a comparable figure for funding disbursed was not available due to adjustments made in USAID’s accounting system. Instead, the FY 2019 total is based on Congressionally appropriated amounts, which include US$575.0 million in funding for family planning as well as US$17.5 million transferred to family planning from the Congressional appropriation to UNFPA.13
UNFPA core contributions were obtained from United Nations Executive Board documents. UNFPA estimates of total family planning funding provided from both core and non-core resources were obtained through direct communications with UNFPA representatives. Other than core contributions provided by governments to UNFPA, un-earmarked core contributions to United Nations entities, most of which are membership contributions set by treaty or other formal agreement (e.g., United Nations country membership assessments), are not identified as part of a donor government’s FP assistance even if the multilateral organization in turn directs some of these funds to FP. Rather, these would be considered as FP funding provided by the multilateral organization, and are not considered for purposes of this report.
The fiscal year period varies by country. The U.S. fiscal year runs from October 1-September 30. The Australian fiscal year runs from July 1-June 30. The fiscal years for Canada and the U.K. are April 1-March 31. Denmark, France, Germany, the Netherlands, Norway, and Sweden use the calendar year. The OECD uses the calendar year, so data collected from the CRS for other donor governments reflect January 1-December 31. Most UN agencies use the calendar year and their budgets are biennial.
All data are expressed in US dollars (USD). Where data were provided by governments in their currencies, they were adjusted by average daily exchange rates to obtain a USD equivalent, based on foreign exchange rate historical data available from the U.S. Federal Reserve (see: http://www.federalreserve.gov/) or in some cases from the OECD. Data obtained from UNFPA were already adjusted by UNFPA to represent a USD equivalent based on date of receipts.
Appendix
Endnotes
Totals represent funding specifically designated by donor governments for family planning as defined by the OECD DAC (see methodology), and include: standalone family planning projects; family planning-specific contributions to multilateral organizations (e.g., contributions to UNFPA Supplies); and, in some cases, projects that include family planning within broader reproductive health activities. ↩︎
In FY 2019, a comparable figure for funding disbursed was not available due to adjustments made in USAID’s accounting system. Instead, the FY 2019 total is based on Congressionally appropriated amounts, which include US$575.0 million in funding for family planning as well as US$17.5 million transferred to family planning from the Congressional appropriation to UNFPA (see Donor Contributions to UNFPA section for additional details). It is important to note that U.S. appropriations for a given year may be disbursed over a multi-year period. Appropriations have remained relatively flat for several years while disbursements have fluctuated largely due to the timing of payments. ↩︎
Includes core-contributions from members of the OECD DAC only; core contributions from non-DAC donors are not included in this total. ↩︎
In FY17, FY18, and FY19, the U.S. administration invoked the Kemp-Kasten amendment to withhold funding – both core and non-core contributions – to UNFPA. In each of these years, Congress required that funding withheld from UNFPA “shall be made available for family planning, maternal, and reproductive health activities.” See KFF “UNFPA Funding & Kemp-Kasten: An Explainer” for additional details. ↩︎
Includes funding from 29 DAC member countries and the European Union (EU). ↩︎
Totals represent funding specifically designated by donor governments for family planning as defined by the OECD DAC (see methodology), and include: standalone family planning projects; family planning-specific contributions to multilateral organizations (e.g., contributions to UNFPA Supplies); and, in some cases, projects that include family planning within broader reproductive health activities. ↩︎
Funding amounts specified by Congress are for a given fiscal year (the U.S. fiscal year is from October 1 to September 30), but may be spent over a multi-year period. Because funding may be spent over a multi-year period, disbursements may lag or vary from appropriations due to a variety of factors including a realignment of the program or the timing of reimbursement requests from an implementing partner, but will eventually be spent. ↩︎
In FY 2019, a comparable figure for funding disbursed was not available due to adjustments made in USAID’s accounting system. Instead, the FY 2019 total is based on Congressionally appropriated amounts, which include US$575.0 million in funding for family planning as well as US$17.5 million transferred to family planning from the Congressional appropriation to UNFPA (see Donor Contributions to UNFPA section for additional details). It is important to note that U.S. appropriations for a given year may be disbursed over a multi-year period. Appropriations have remained relatively flat for several years while disbursements have fluctuated largely due to the timing of payments. ↩︎
Includes core-contributions from members of the OECD DAC only; core contributions from n ↩︎
In FY17, FY18, and FY19, the U.S. administration invoked the Kemp-Kasten amendment to withhold funding – both core and non-core contributions – to UNFPA. In each of these years, Congress required that funding withheld from UNFPA “shall be made available for family planning, maternal, and reproductive health activities.” See KFF “UNFPA Funding & Kemp-Kasten: An Explainer” for additional details. ↩︎
In FY17, FY18, and FY19, the U.S. administration invoked the Kemp-Kasten amendment to withhold funding – both core and non-core contributions – to UNFPA. In each of these years, Congress required that funding withheld from UNFPA “shall be made available for family planning, maternal, and reproductive health activities.” See KFF “UNFPA Funding & Kemp-Kasten: An Explainer” for additional details. ↩︎
The COVID-19 pandemic has resulted in administrative challenges for state Medicaid agencies from staff transitions to telework due to social distancing requirements, increased applications during the economic downturn, and the need to modify policies and procedures to facilitate access to coverage and care in response to the public health crisis. As a result, states have faced increased enrollment while having fewer staff and resources available for routine eligibility and enrollment processing. At the same time, Maintenance of Eligibility (MOE) provisions require states to keep beneficiaries enrolled until the end of the month when the COVID-19 public health emergency (PHE) ends and prohibit states from adopting more stringent eligibility criteria or increasing premiums, as conditions of receiving temporary increased federal Medicaid funding under the Families First Coronavirus Response Act. Consequently, states will need to address a backlog of Medicaid eligibility renewals and redeterminations as well as continue to process new applications after the PHE ends.
In addition, many states have adopted temporary policy changes through various Medicaid emergency authorities to expand eligibility and/or streamline enrollment processes to connect individuals to coverage more quickly during the pandemic. States also have used emergency authorities to adopt other policies such as relaxing cost sharing and prior authorization requirements, increasing provider payments, and adding new benefits. States will have to decide whether to continue these policy changes after the PHE ends. If states return to pre-PHE eligibility and enrollment rules, they will need to redetermine eligibility for impacted enrollees. They also will need to notify beneficiaries and providers about any payment or benefit changes.
On December 22, 2020, CMS released a state health official letter outlining how states are expected to unwind emergency authorities and resume normal eligibility and enrollment processing after the end of the PHE. The current PHE declaration expires on April 21, 2021, but the Biden Administration has indicated the PHE will likely remain in place throughout 2021 and that states will receive 60 days notice before the end of the PHE to prepare for the end of emergency authorities and the resumption of pre-PHE rules. The change in Presidential administration could have implications for state planning and decisions at the end of the PHE, as the Biden Administration could revise the December 2020 guidance as well as the Trump Administration’s interim final rule (IFR) governing the MOE provisions. Because the Trump Administration did not finalize the IFR following the end of the comment period in January, the Biden Administration will have the opportunity to review comments and could make modifications in response to comments before finalizing the rule. This brief highlights key issues from the new CMS guidance to states as issued in December 2020.
What actions does CMS expect states to take during the PHE?
CMS expects states to process applications, redeterminations and renewals to the extent possible during the PHE, even though they cannot terminate coverage for most enrollees due to the MOE. CMS emphasizes prioritizing actions to ensure that individuals can enroll in and retain coverage, such as determining eligibility for new applications, during the PHE.1 Table 1 summarizes the circumstances that may result in state backlogs and the actions that CMS expects states to take during the PHE to address pending eligibility and enrollment actions. CMS also encourages states to conduct CHIP and Basic Health Plan (BHP) redeterminations and renewals during the PHE. Because the MOE does not apply to those programs, CMS notes that states can process CHIP and BHP actions now, which could allow them more time to focus on clearing Medicaid backlogs after the PHE and MOE conditions end.
Table 1: State Eligibility and Enrollment Backlogs and Expected State Actions During the PHE
Type of Action
Circumstances That May Contribute to Backlog When PHE Ends
Actions CMS Expects States to Take During PHE
Applications
The economic downturn has led to increased applications, and states may not have finished processing all applications received during the PHE by the time the PHE ends.
States also need to continue to process new applications received post-PHE.
States should make every effort to make timely eligibility determinations for new applicants.
Verifications
States that determine eligibility based on self-attested information must complete post-enrollment verification.
States should begin processing pending post-enrollment verifications to the extent possible and resume checking data sources to verify eligibility criteria for those enrolled based on self-attested information.
Redeterminations
Some individuals may have gained eligibility due to state-adopted emergency authorities that expanded eligibility (such as increased income/asset disregards). States will have to redetermine eligibility for these enrollees if they revert to prior rules after the PHE ends.
Enrollees also may have reported changes in circumstances during the PHE, but MOE rules required states to continue coverage.
States should make every effort to process changes in circumstances that may expand coverage, and process other changes in circumstances to the extent possible.
Renewals
States may have delayed processing eligibility renewals that were due during the PHE due to the need to focus on pandemic response.
States should process overdue renewals to the extent possible and initiate renewals based on electronic data/information available to the state.
To help ensure that future workloads are manageable, states can take action to evenly distribute renewals throughout the year. When completing renewals that were delayed during the PHE on an ex parte basis (using information available to the state and not requiring information from the individual), states have the option to retain the individual’s original eligibility period (effective when the renewal was due) instead of beginning a new eligibility period on the date the renewal actually is completed. This may help states distribute workloads in future years by staggering renewal dates but may also result in renewal periods for enrollees that are shorter than 12 months.
How quickly does CMS expect states to clear eligibility and enrollment backlogs after the PHE ends?
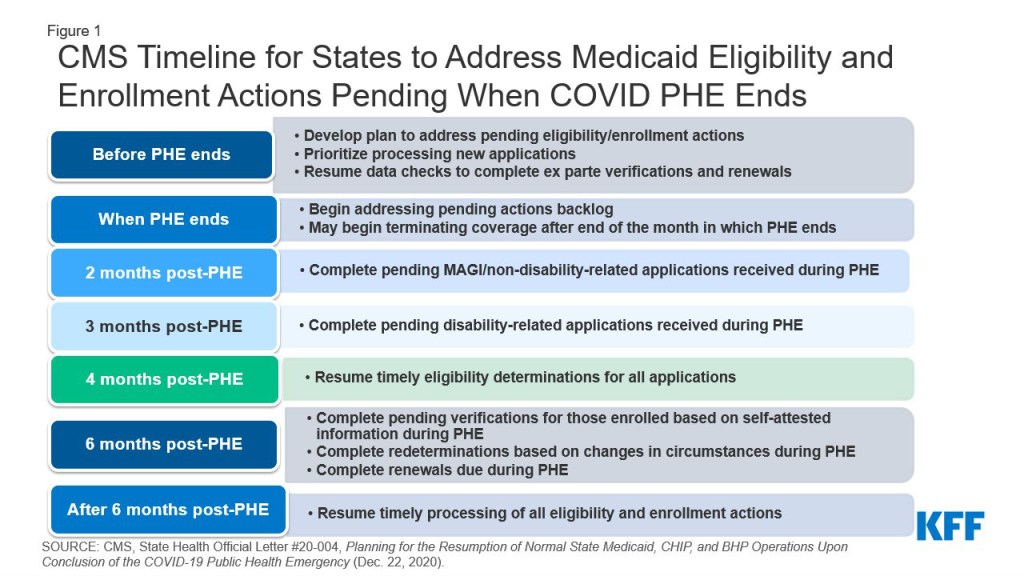
CMS expects states to complete all pending eligibility and enrollment actions and clear any backlogs within six months after the PHE ends. The guidance sets timelines for states to return to normal operations for eligibility determinations on new applications as well as eligibility verifications, redeterminations based on changes in circumstances, and renewals that are pending when the PHE ends (Figure 1). Initial milestones focus on processing applications, followed by completing pending verifications, redeterminations, and renewals.
Figure 1: CMS Timeline for States to Address Medicaid Eligibility and Enrollment Actions Pending When COVID PHE Ends
States need to adopt a methodology for prioritizing which pending eligibility and enrollment actions to complete first, focused on individuals “most likely” to no longer be eligible (Table 2).2 States have discretion about whether to adopt one of CMS’s methodologies or to develop their own approach. The state’s methodology will be part of the operational plan that it must develop to set out how it will process pending actions within CMS-required timeframes after the PHE ends. CMS will not approve state operational plans but may request them from states that are not meeting the required timeframes. States must submit baseline data about pending eligibility and enrollment actions at the end of the PHE and submit updates quarterly thereafter to show progress toward the timeframes. If states meet these timeframes, CMS will not consider eligibility and enrollment actions delayed due to the PHE as untimely for Program Error Rate Measurement (PERM) purposes.3
Table 2: State Options for Methodology to Prioritize Pending Eligibility and Enrollment Actions
Methodology
Description
Population-based approach
Prioritizes eligibility and enrollment actions for individuals in groups who are most likely to be no longer eligible (e.g., those who aged out of group, expansion adults who became Medicare-eligible).
Time-based approach
Prioritizes actions based on the length of time the action has been pending (state completes oldest pending actions first).
Hybrid approach
Combines the population and time-based approaches (e.g. use time-based approach to prioritize post-enrollment verifications and changes in circumstances and use population-based approach to prioritize renewals; or use population-based approach for first wave of pending actions and then switch to time-based approach).
State-developed approach
Develop another approach that prioritizes actions for individuals who are most likely to be no longer eligible or that pose a greater risk for ineligible individuals remaining enrolled longer.
The guidance reiterates existing policies states can adopt to streamline eligibility and enrollment processes and reduce administrative workload. For MAGI populations (whose eligibility is based solely on low income), these options include renewing coverage for 12 months when processing changes in circumstances and a data check shows continued eligibility, relying on income determinations made by SNAP or TANF, as well as Express Lane Eligibility and 12-month continuous enrollment for children. States can also streamline eligibility and renewal processes for non-MAGI enrollees (whose eligibility is based on old age or disability) by adopting 12 month renewal periods, using prepopulated renewal forms, offering renewal reconsideration periods, and modifying verification policies to accept self-attestation, among other policies.4
After the PHE ends, what do states need to do before terminating coverage?
States cannot terminate coverage until the end of the month in which the PHE ends, due to the MOE requirements. After the MOE and any temporary emergency authorities end, states must follow regular program rules that require sending 10 day advance notice and providing the opportunity for a fair hearing prior to terminating coverage. If states are ending emergency authorities and redetermining eligibility under more restrictive pre-PHE rules, states must provide enrollees with a reasonable timeframe, at least 30 days, to provide information to establish their continued eligibility.5 States also must ensure a smooth transition to other insurance affordability programs for those who lose Medicaid eligibility but may be eligible for Marketplace or other coverage.
After the PHE and MOE requirements end, states do not have to repeat redeterminations or renewals before terminating coverage for individuals who have been determined ineligible within six months of the date the state sends an advance notice of coverage termination. To adopt this option, states must inform the enrollee at the time of the ineligibility determination that coverage will end after the month in which PHE ends, and the state will redetermine their eligibility based on any changes in circumstances that they report prior to termination. The state then must send a second notice in advance of the termination date. In cases where the state requests information to establish continued eligibility, states must allow individuals to respond through the end of the PHE, regardless of when the request was sent. If an individual has not responded to a request that was sent within six months of the date on which the state intends to terminate coverage after the PHE ends, the state may send advance notice of termination without attempting a repeated verification or redetermination.
What do states need to do if they want to continue or end policies adopted through emergency authorities?
The various Medicaid emergency authorities adopted during the PHE will end automatically (when the PHE ends or on a specified end date), unless a state takes action to extend them. States are not subject to public notice requirements for returning to pre-PHE rules. However, CMS strongly encourages states to communicate about changes with providers, enrollees, and managed care plans. And, states must provide advance notice to enrollees of any actions that result in a loss of eligibility, a reduction in benefits, or an increase in cost-sharing; this includes changes due to ending an emergency authority that temporarily expanded eligibility or benefits. Although some states already have sent notices during the PHE informing enrollees of changes that will take effect after the PHE or MOE ends (such as increased cost-sharing), states must send a second advance notice at the end of the PHE prior to implementing these changes.6
CMS encourages states to consider whether some emergency authorities should end before the PHE ends. For example, many states paused Preadmission Screening and Resident Review (PASRR) assessments, which prevent unnecessary nursing facility stays and facilitate community transitions, for people with intellectual or developmental disabilities or mental illness entering nursing homes during the pandemic. Given PASRR’s role in preventing unnecessary institutionalization, CMS encourages states to re-start PASRR before the PHE ends.7
States may want to continue some policies adopted under emergency authorities after the PHE ends, though not all policies can be continued. For example, states can amend their state plans or HCBS waivers to continue service delivery via telehealth. States also can update their verification plans to continue streamlined eligibility and enrollment options. CMS specifically encourages states to identify any temporary authorities that increased access to HCBS and make these changes permanent. However, states that used Section 1135 waiver authority to relax provider screening requirements and/or temporarily enroll providers who participate in other state Medicaid programs or Medicare must return to regular program rules. States have six months from the end of the PHE to complete screenings of these provisional providers and to stop payments to any providers not fully enrolled.
CMS is also now allowing states to extend HCBS waiver emergency authorities adopted under Appendix K up to six months after the PHE ends. Appendix K allows states to make temporary changes to HCBS waivers in response to emergencies, such as modifying or expanding eligibility or benefits, modifying or suspending service planning and delivery requirements, and adopting policies to support providers. Appendix K approvals to date were scheduled to expire after one year, with the first expirations to occur in late January 2021. Given the pandemic’s longevity and uncertainty about how long the PHE ultimately will last, CMS is now allowing states to submit requests to extend existing Appendix K approvals up to six months after the PHE ends and will apply this end date to new Appendix K requests going forward.8 After six months post-PHE, states can continue many Appendix K policies by amending their HCBS waivers.9
CMS, State Health Official Letter #20-004, Planning for the Resumption of Normal State Medicaid, Children’s Health Insurance Program (CHIP), and Basic Health Program (BHP) Operations Upon Conclusion of the COVID-19 Public Health Emergency at p. 23-24 (Dec. 22, 2020), https://www.medicaid.gov/federal-policy-guidance/downloads/sho20004.pdf↩︎
CMS will issue future guidance on how states are expected to resume regular program integrity operations. The guidance will account for changes that occurred due to state adoption of emergency authorities during the PHE. Id. at p. 35. ↩︎
CMS specifies an exception for enrollees in the COVID-19 uninsured testing group: states may send a notice at the time of initial enrollment informing enrollees that their coverage will end after the PHE. The state does not have to redetermine eligibility (unless the enrollee submits an application for full Medicaid benefits) but must send a 10-day advance notice prior to terminating coverage after the PHE and MOE end. CMS, COVID-19 Frequently Asked Questions (FAQs) for State Medicaid and Children’s Health Insurance Program (CHIP) Agencies (last updated Jan. 6, 2021), https://www.medicaid.gov/state-resource-center/downloads/covid-19-faqs.pdf. ↩︎
States that used emergency authorities to extend the timeframe for individuals to request a fair hearing during the PHE must honor those timeframes after the PHE ends for notices that already have been sent, even if the state is reverting back to its former shorter timeframes after the PHE ends. CMS, State Health Official Letter #20-004, Planning for the Resumption of Normal State Medicaid, Children’s Health Insurance Program (CHIP), and Basic Health Program (BHP) Operations Upon Conclusion of the COVID-19 Public Health Emergency at p. 17 (Dec. 22, 2020), https://www.medicaid.gov/federal-policy-guidance/downloads/sho20004.pdf. ↩︎
All Appendix K authorities expire on the specified end date, except that individuals whose level of care renewals are extended for 12 months receive this full time period, regardless of the Appendix K end date. Id. at 17. ↩︎
Examples of Appendix K changes that can continue after the PHE ends include authorizing service delivery via telehealth, adding services like home-delivered meals, increasing payment rates, providing 30-day retainer payments, and including family caregivers as paid providers. Appendix K changes that cannot continue after the PHE ends include expanded timeframes for level of care re-evaluations, waivers of home and community-based settings and conflict of interest requirements, extensions of due dates for submitting data and reports to CMS, and changes approved under Section 1135 emergency authority such as extending timeframes for recertifying person-centered service plans and accepting verbal signatures for service plans. Id. at 7. ↩︎
Even before the COVID-19 pandemic began, signing up for health coverage and applying for financial assistance was often challenging. A 2020 KFF survey found half (51%) of consumers who looked for coverage during the 2020 open enrollment encountered difficulties, and nearly 5 million consumers sought in-person help but couldn’t get it. During the 2021 open enrollment, challenges compounded as consumers unfamiliar with the process needed to find replacement marketplace or Medicaid coverage for the first time, in-person assistance shifted to remote, and other pandemic-related complexities arose. Last year, nearly all state based marketplaces (SBM) re-opened marketplace enrollment in response to the pandemic, and SBMs are beginning to announce COVID re-openings this year. President Biden has said he favors providing a COVID-19 special enrollment period in the federal marketplace for people who are uninsured. (People who lose job-based insurance already qualify for a 60-day special enrollment period, but people who are already uninsured do not.)
Earlier this month, KFF convened a discussion with Navigators and other consumer assistance professionals from federal- and state-based marketplace states.1 They offered observations about the 2021 Open Enrollment period, discussed general and pandemic-specific challenges facing consumers seeking coverage, and offered suggestions to improve enrollment outcomes. This brief summarizes those observations.
In addition, this brief reviews information about federal marketplace resources and spending priorities contained in Trump Administration budget documents. Federal marketplace spending on consumer assistance, marketing, and other consumer assistance activities has declined during the Trump administration, even while revenue from user fees – which finance most of federal marketplace expenses – has held steady. It appears that more than $1 billion in unspent federal user fee revenue has accumulated and could be used to invest in changes that would make it easier for consumers to enroll in health coverage.
Available Marketplace Revenue
Unspent marketplace user fee revenue has accumulated. The Trump Administration substantially reduced spending on key activities that support marketplace enrollment, including navigator consumer assistance, marketing and outreach, the HealthCare.gov marketplace website, and the federal marketplace call center. At the same time, according to budget documents, the Administration did not spend all of the user fee revenue paid by marketplace health plans. Unused funds appear to have accumulated to more than $1 billion over fiscal years 2018-2020. Table 1 summarizes budget data from Fiscal Years 2013 and 2016, the first and last years of marketplace operations under the Obama Administration and from Fiscal Years 2017-2020 under the Trump Administration.
Table 1: Trends in Federal Marketplace Spending and User Fee Revenue, FY 2013-2020($ in thousands)
Activity
FY 2013
FY 2016
FY 2017
FY 2018
FY 2019
FY 2020
Eligibility and Enrollment
275,501
445,249
484,144
392,660
348,488
358,938
Consumer Information and Outreach
701,075
805,833
640,232
591,948
579,088
529,635
· Call Center
505,466
563,638
540,197
525,326
499,053
442,700
· Navigator, enrollment assisters
107,513
99,677
51,166
12,720
19,499
20,835
· Consumer education/outreach
77,436
101,048
16,599
10,744
11,231
11,600
Information Technology
402,553
664,083
710,867
767,413
504,283
612,358
Health plan management and payment, oversight, federal payroll, other admin activities
In addition to user fee revenue, CMS uses agency discretionary appropriations to fund certain cross cutting expenses that support Medicare and Medicaid as well as the marketplace.
Spending cuts on consumer assistance and outreach activities, even as revenue held steady, contributed to the user fee carryover. Most spending for federal marketplace operations is for consumer information and outreach activities (navigator enrollment assistance, marketing and outreach, and the federal call center) and for information technology (HealthCare.gov). Spending on these, as well as other eligibility and enrollment activities declined precipitously under the Trump administration and accounts for most of the reduction in overall spending for marketplace operations during that time. Because of these spending reductions, marketplace expenses were cut below the level of user fee revenue collected. From Trump Administration budget documents, it appears that for three years, FY 2018-2020, roughly $400 million per year in available user fee revenue was not spent, resulting in a cumulative carryover of revenue of more than $1.2 billion.2 Additional unused revenue likely accumulated during the current fiscal year, though that cannot be seen from budget documents released to date3 . A final regulation issued by the Trump Administration in its closing days would reduce the federal marketplace user fee rate from 3% to 2.5% starting in 2022. Unless changed by the new Administration, this reduction in the user fee rate would make it difficult for the federal marketplace to reverse cuts in spending on consumer information, outreach, and assistance activities.
Supporting Enrollment During the Pandemic
Following the close of the 2021 open enrollment period in, Navigators stressed the importance of reopening the federal marketplace for enrollment in 2021. For the first time in several years, marketplace enrollment increased in a number of states. Nevertheless, Navigators noted address unresolved problems that hindered access for some consumers during the regular open enrollment period. They also pointed to the importance of making every effort to get people covered during the pandemic. Navigators offered several recommendations for ensuring a successful COVID-19 special enrollment period.
Navigators urged that an emergency COVID enrollment period extend for longer than the 6-week federal open enrollment period that just concluded. They noted that time will be needed not only to sign up new consumers, but to follow up with those who experienced difficulties during the regular open enrollment. As the pandemic took off in March 2020, 11 of the 12 SBMs reopened marketplaces for enrollment, most – initially – for a period of 6 to 8 weeks. As the year progressed, however, most SBMs extended the enrollment opportunity, some into the summer, and several to year end. (Table 2)
Table 2 : Initial and Final Dates for COVID-related SBM Re-openings in 2020
State-Based Marketplace
Initial End Date for COVID Marketplace Re-Opening
Final End Date
California
June 30
August 31
Colorado
April 30
April 30
Connecticut
April 17
April 17
District of Columbia
June 15
December 31
Maryland
June 15
December 15
Massachusetts
May 25
July 23
Minnesota
April 21
April 21
Nevada
April 15
May 15
New York
April 15
December 31
Rhode Island
April 15
April 30
Vermont
April 17
August 14
Washington
May 8
May 8
Navigators also stressed the importance of investing substantially in publicizing a COVID re-opening of marketplace enrollment. As KFF Tracking Polls have found for years, most consumers are unaware of marketplace open enrollment deadlines. The KFF tracking poll for December 2020 found that fewer than 1 in 5 respondents knew the then-upcoming deadline to sign up for 2021 coverage through the marketplace. Greater publicity will be required to inform people when and how to sign up for a special, COVID-related enrollment opportunity. Navigators also suggested the federal government could spend more on marketing and advertising, funding that had been cut by 90% by the Trump administration. At the same time, SBM navigators urged that federal marketing efforts be carried out in consultation with SBMs, whose timing and other rules for COVID-19 enrollment periods may differ from those of the federal marketplace.
Navigators noted the importance of targeted outreach strategies to reach some consumers, including those who do not speak English, non-citizens, and those who have been uninsured for a longer period of time. These groups are typically more difficult to reach and may be less aware of extended enrollment periods. The 2020 KFF survey found that 71% of uninsured individuals did not even try to find coverage for 2020. The perceived high cost, lack of awareness about subsidies, fear of how getting coverage subsidies could affect their immigration status, and other factors discourage millions of uninsured consumers from even looking into coverage options. Outreach from trusted individuals and community based organizations could be undertaken to reach such consumers, particularly during a special enrollment period.
As part of any marketing efforts, federal Navigators advised against describing the reopening of marketplace enrollment as a COVID-19 special enrollment period or SEP, and instead recommended it be characterized as a new open enrollment period. They noted that the term SEP can be confusing to for consumers, who may not realize the “special” enrollment opportunity applies to them, or who may have had difficulty applying for SEPs in the past. Navigators also pointed out that while the Trump Administration revised rules during the pandemic, giving consumers more time to apply for a SEP following coverage loss, consumers still had to provide documentation of that coverage loss before they could enroll using the COVID-SEP.
To be effective, federal Navigators indicated they will need additional resources to provide consumer assistance during a COVID enrollment period. Current year funding awards to federal marketplace navigators ($10 million) are less than 10% of the amount the Obama Administration invested in enrollment assistance during the first open enrollment period ($108 million). While a few federal navigator programs have been able to find supplemental funding resources from their states or foundations, others have had to substantially reduce capacity as a result of federal funding cuts. For example one statewide program that used to employ 30 full time navigators now has 6. In addition, most navigator programs now “front load” their annual award, using most resources during the 6-week open enrollment period, and maintaining only skeleton capacity to help consumers during the rest of the year. Currently operating federal navigator programs said, with enhanced funding, they could respond immediately if a COVID enrollment period is established, but they noted it will take time to ramp up the number of people they can help as they re-hire and train staff, and hoped decisions about the length of a federal COVID enrollment period would take that into account.
Addressing problems that arose during the 2021 open enrollment period
Navigators described several issues that surfaced during the most recent open enrollment period, some related to the economic upheaval caused by the coronavirus pandemic. These issues included difficulties in estimating income for the year due to job loss or receipt of unemployment benefits, receipt of failure to file notices due to IRS backlogs in processing income tax returns, and policies discouraging enrollment among eligible immigrants. They suggested policy changes in conjunction with a COVID enrollment period anticipate and try to respond to problems that affected consumer’s ability to enroll during the last Open Enrollment.
Navigators reported an increase in consumers facing difficulties in estimating annual income this year because of job loss, reductions in hours, or because of receipt of unemployment benefits which varied in availability and amount during 2020. Marketplace subsidies are based on a consumer’s estimated income for the coming calendar year and when consumers apply for subsidies, the marketplace conducts real-time verification of their income estimate, comparing it to their most recently filed federal tax return. Pandemic-related job loss or reductions in hours after years of steady employment can lead to problems verifying income. In these cases, consumers may receive a notice of data match inconsistency (DMI) that requests further documentation. Although subsidies will be temporarily approved based on the consumer’s estimated income, they will be reduced or terminated 90 days later unless required DMI documentation is received and approved. Navigators expressed concern that DMI-related subsidy terminations could start happening in February-March for consumers who cannot successfully complete the verification process. Navigators also heard from clients who worried they may have to repay some or all of the premium tax credit that they received during the pandemic if they their income increases later in the year. In response to these concerns, Navigators suggested the marketplace could target outreach and assistance to consumers who received DMI notices during open enrollment. Additionally, the federal government could waive repayment of excess premium tax credits during the pandemic.
Because of backlogs at the Internal Revenue Service (IRS), Navigators also reported that some consumers who filed their income taxes nevertheless received failure to file notices, putting their current subsidies at risk. Recipients of marketplace premium tax credits in a year are required to file a federal tax return for that year if they want to continue receiving subsidies in the subsequent year. Because of the pandemic, the 2019 tax filing deadline was extended to July 2020 and the IRS experienced delays processing returns. As a result, some consumers were notified they were at risk of losing marketplace subsidies even though they had filed their income taxes as required. The notice did not clearly indicate what steps to take next, leaving many consumers unsure of how to address the issue. Navigators said providing targeted outreach and assistance for consumers who received failure to file notices could help ensure they are covered and subsidies continue.
Navigators are concerned about actions that have discouraged enrollment by immigrants. Navigators reported that a series of Trump Administration policy actions, including recent changes to the “public charge” policy, have instilled fear and deterred enrollment in public coverage among immigrants. Although the public charge policy does not apply to marketplace subsidies, Navigators said this policy has suppressed enrollment in marketplace coverage and Medicaid. The Biden Administration has vowed to rescind the public charge rule changes. Navigators also suggested targeted outreach to immigrants during a COVID enrollment period.
While the Medicaid maintenance of eligibility (MOE) requirements tied to enhanced federal Medicaid funding for states during the public health emergency (PHE) have helped consumers maintain Medicaid, Navigators worried about potential loss of coverage when the PHE ends. Under the MOE requirements, states must provide continuous coverage through the end of the month in which the PHE ends for people enrolled in Medicaid. Navigators said this policy has enabled consumers to maintain their Medicaid coverage during the pandemic. However, they expressed concern that when the PHE ends and Medicaid redeterminations resume, some consumers could lose their Medicaid and need help finding new coverage. Consumers who lose Medicaid coverage mid-year are eligible for a 60-day special enrollment period (SEP) during which they can sign up for marketplace coverage, although Trump Administration policy changes made this process more difficult for consumers. Navigators suggested the marketplace could coordinate with state Medicaid programs as they resume redeterminations and refer people for enrollment assistance if they need to transition to new coverage.
Navigators raised other concerns – some of them longstanding – that could be addressed to support in-person enrollment assistance and make the enrollment process more efficient and easier for consumers. The federal marketplace could begin to invest in improvements using some carryover funding, although investments will likely be needed beyond the time of any COVID-enrollment period.
Beyond additional funding during an emergency COVID-related enrollment period, navigators spoke to the restoration of federal funding for consumer assistance. Federal navigators said increased funding is necessary to rebuild a diminished workforce. They stressed it will take time to rebuild after years of funding cuts but agreed immediate improvements could be achieved. Federal navigators also noted the importance of re-establishing navigator services that have been eliminated altogether under the Trump Administration. Currently no navigator services are offered in two federal marketplace states (South Carolina and Utah), and none are offered in most of the counties of six other states (Texas, Michigan, Ohio, Illinois, Kansas and Nebraska). The Trump Administration also eliminated the requirement to have at least two navigator programs serving each state; in 2016 there were 100 federal navigator grantees, today there are 30. In addition, the requirement for federal navigators to maintain a physical presence in the state they serve was eliminated. While much more help was provided remotely during the pandemic, a small number of current federal navigator grantees only maintain web and phone services in the states they serve.
Federal navigators expressed frustration with the quality of the assistance provided by the federal marketplace call center. Concerns about the effectiveness and reliability of help from the federal marketplace call center date back years. In a 2015 KFF survey, most marketplace assisters said help from the call center was rarely or only sometimes effective. Current federal navigators noted some call center staff lacked the training and experience to provide adequate assistance. They also said that the call center lacks an effective system for escalating complex cases to more highly trained specialists. By contrast, navigators in several SBM states reported more positive experiences with their call centers. Several said SBM call centers make dedicated lines and specially trained staff available for Navigators. In some SBMs, the call centers also directly refer consumers to navigators when those consumers are in need of in-person assistance.
Federal navigators also raised concerns about the federal marketplace website and offered ideas for improvement they felt would streamline the enrollment process. Some concerns related to the Find Local Help tool – the Trump Administration redesigned this tool to steer consumers to brokers instead of marketplace assisters. The tool also no longer identifies navigator programs, but rather lists them among other volunteer assister programs that the marketplace does not fund. Other concerns related to design of the online application. For example, when consumers need to correct or update information in their online application, they cannot go directly to the specific screen, but must scroll through each application question in order. Federal navigators also noted that the federal government’s training program does not include access to the online application, making it harder for them to learn the flow of questions and required information and to identify changes in the online application from one year to the next. Navigators in SBM states had few complaints about their marketplace websites and felt they were well-designed and included needed functionality. In particular, the New York marketplace has created a secure portal for certified navigators so they can access their clients’ online accounts, input information, review the application status, and handle other basic administrative tasks, such as password changes. Federal navigators said having this type of portal on healthcare.gov would enable them to help consumers more efficiently and reduce reliance on the call center.
Navigators reported ongoing challenges with coordination between the marketplace and Medicaid. While most SBM states have integrated marketplace websites that determine eligibility for marketplace coverage and Medicaid, the process for determining eligibility for Medicaid in FFM states is less streamlined. Eight states that use healthcare.gov have delegated authority to the federal marketplace to make eligibility determinations for the Medicaid programs. In the remaining states on the healthcare.gov platform, the marketplace makes an initial assessment of eligibility for Medicaid, then refers the applicant’s information to the state Medicaid agency to make a final eligibility determination. How well this handoff operates in practice can vary. Delays in processing Medicaid applications in some states can mean that some consumers initially assessed as eligible for Medicaid but ultimately determined ineligible cannot complete their marketplace application during the open enrollment period and instead must apply for an SEP to finish the application and enroll.
Navigators reported that some consumers who signed up during open enrollment are already experiencing post-enrollment problems, such as not receiving their first premium invoice, having claims denied, or trouble learning to use new coverage. While Navigators provide some post-enrollment assistance, by law, they are required to refer such problems to statewide consumer assistance programs (CAPs), established under the ACA. The ACA provided an initial appropriation for CAPs, but Congress has not provided further appropriations, and CAP programs have received no federal funding since 2012. Navigators urged that CAP funding should also be a priority.
Discussion
As he takes office, President Biden faces a daunting list of challenges as he endeavors to make progress on the health reform proposals he made during the campaign. Some, such as proposals to expand ACA subsidies, will require an act of Congress. Others, including re-opening enrollment in the federal marketplace, require only executive action. To make the enrollment process simpler and enable more people to enroll, additional investments would also be needed. Beyond just reversing Trump Administration cuts, there are opportunities to make the make the marketplace more responsive to consumer needs and to work with Navigators to identify and address problems as they emerge. The availability of unspent, carryover user fee revenue could make possible immediate investments in marketing and outreach, support for enrollment assistance, and other improvements.
A reopened ACA enrollment period has the potential to get more people covered during a public health emergency and in the midst of massive economic dislocation. There are, however, challenges and trade-offs involved. Without any increase in federal subsidies, many people who are uninsured may still find coverage unaffordable. A new enrollment period could also provide an opportunity for people who have recently developed health conditions to sign up, which would provide them greater access to care but could also worsen the risk pool and lead to an increase in premiums. A concerted outreach effort could help get more people covered, including those who are currently healthy, thus improving the risk pool and reducing the number who are uninsured.
Participants in the discussion were from Arizona, Colorado, District of Columbia, Florida, Indiana, Maine, New York, Pennsylvania, Texas, Virginia, and Wisconsin. ↩︎
Data on user fee revenue was not published during the Obama Administration. Disclosed detail on marketplace spending and revenue began in 2017, with inclusion of the Health Insurance Exchanges Transparency table in Trump Administration budget documents. In addition to user fee revenue, a portion of marketplace operations expenses are financed through discretionary appropriations to the Centers for Medicare and Medicaid Services (CMS), recognizing that some activities also provide cross-cutting support to Medicare, Medicaid and CHIP. ↩︎
The Trump Administration’s FY 2021 budget justification shows proposed spending levels, which are not necessarily achieved, while budget documents show actual spending and revenue amounts for prior years. ↩︎
Here’s our recap of the past week in the coronavirus pandemic from our tracking, policy analysis, polling, and journalism.
This week marked the one-year anniversary since the first patient with COVID-19 was hospitalized in the United States. At this point, coinciding with President Joe Biden’s inauguration and a new administration leading the federal response, the country has surpassed 24.6 million COVID-19 total cases and roughly 410,100 total deaths as of January 21.
On his first day in office, President Biden signed several executive orders including requiring masks and physical distancing in federal buildings and on other federal properties. On Thursday, the President signed an executive order mandating masks for interstate travel in the U.S. and released a national strategy responding to the pandemic. KHN outlines what President Biden promised during the presidential campaign and will be tracking the administration’s actions on health and COVID-19 related promises.
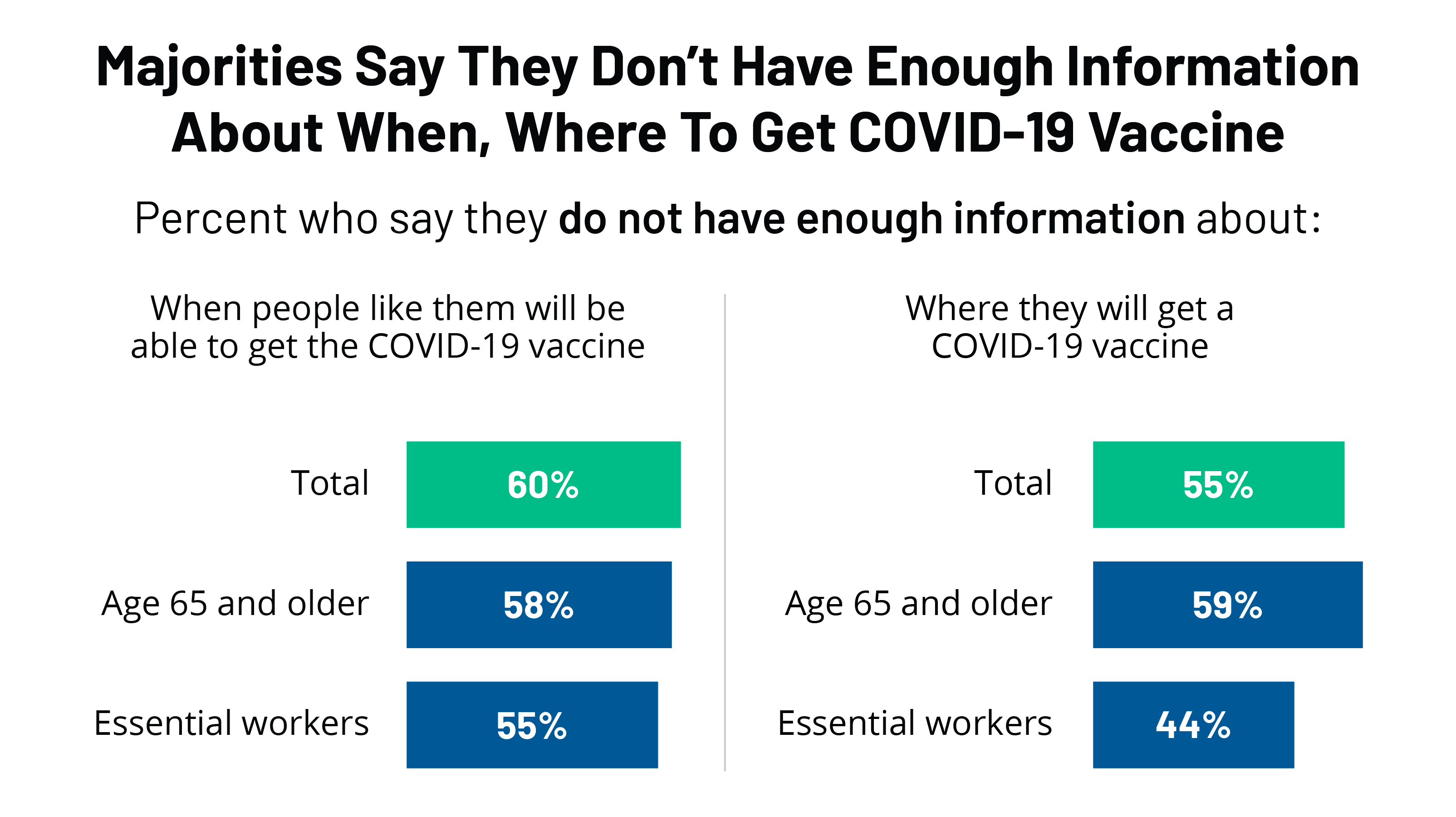
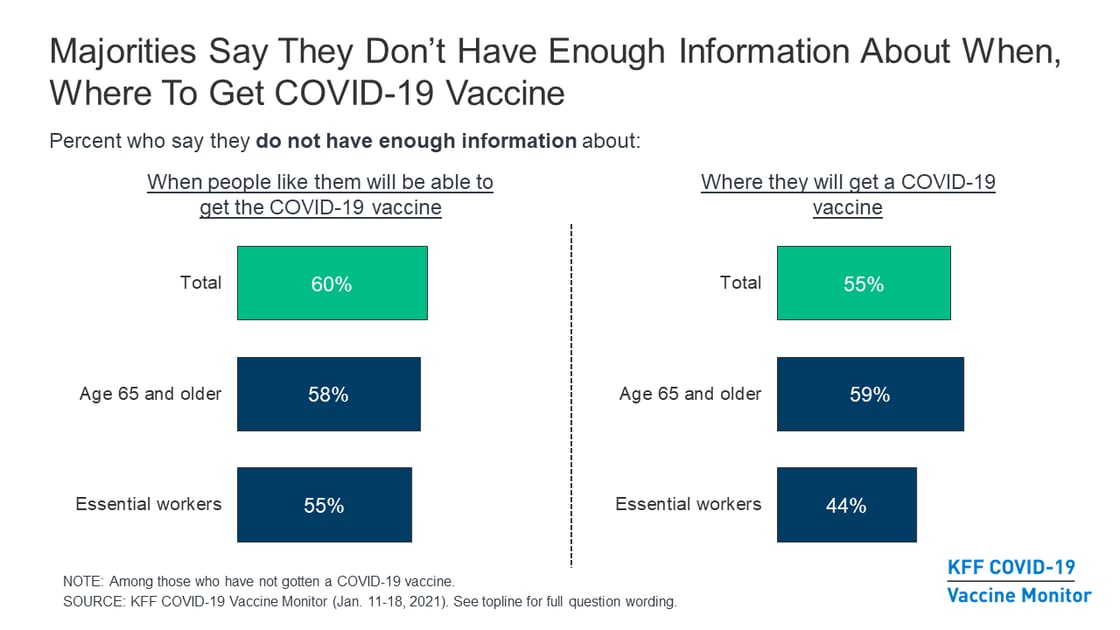
The latest COVID-19 Vaccine Monitor reports that half the public expect the vaccine rollout to get better under President Biden. The new report also highlights that a majority of the public, including prioritized groups like older adults and essential workers, say they don’t have enough information about where and when to receive a vaccine.
Meanwhile, an update to January 19 data on states’ COVID-19 vaccine priorities shows 12 states have moved to redefine their priority populations or open vaccine availability to people 65 and older, bringing the total number of states placing this population in the 1a or 1b category to 28. Six states moved those under age 65 with high risk medical conditions up in line as well.
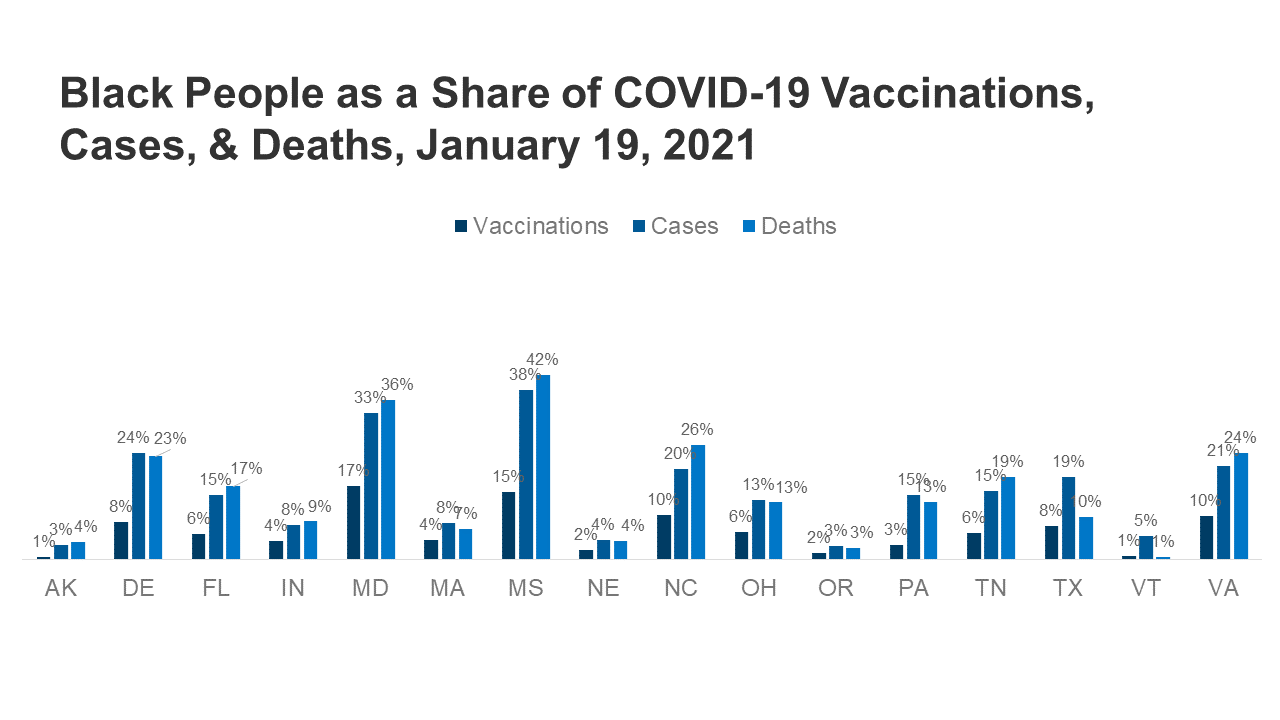
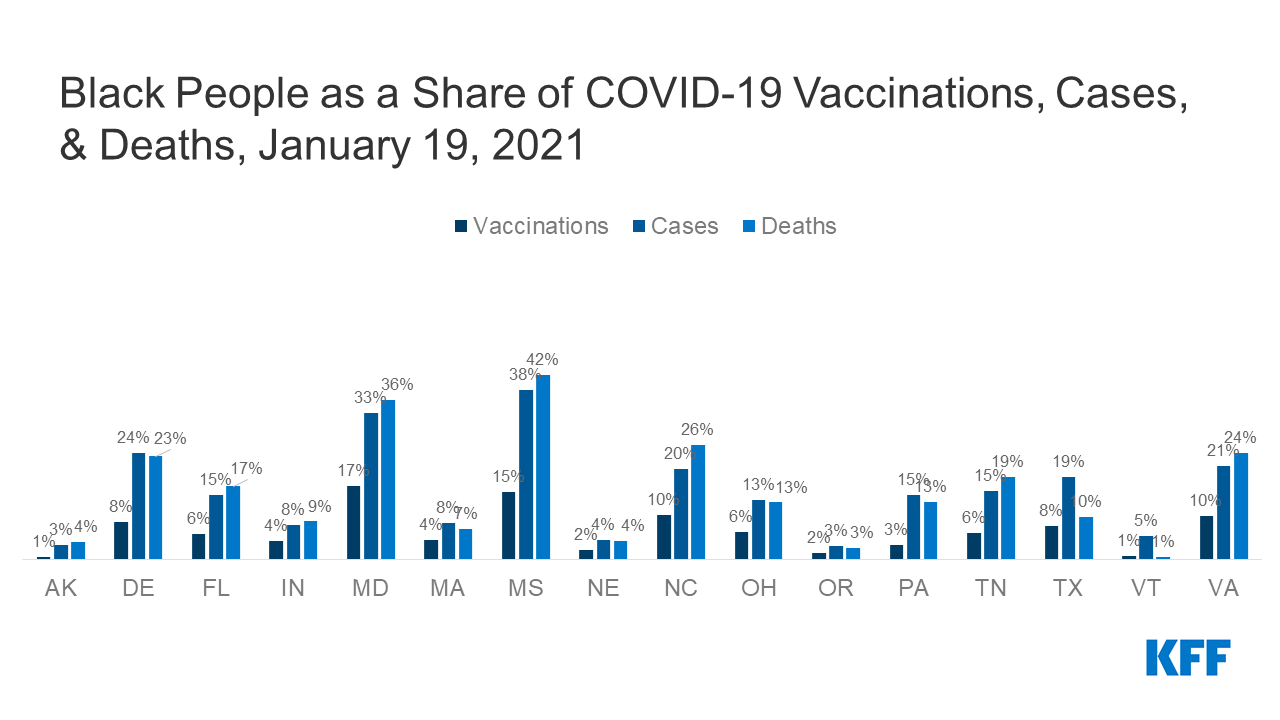
A new analysis explores state-reported data on vaccination by race/ethnicity and will be regularly updated and available on KFF’s COVID-19 state data and policy tracker. While it is still early in the vaccine distribution timeline for the general public, the preliminary data provided by 16 states indicate Black and Hispanic people’s share of vaccinations is smaller than their share of cases and deaths in most of these reporting states. The data and our news reporting at KHN have also shown that vaccination is lagging by various measures for people of color.
Media reports indicate some health workers are opting not to be vaccinated, particularly among those working in long-term care facilities. A new data note examines the makeup (by race/ethnicity, income level, age, gender, education, and citizenship status) and health insurance coverage of the estimated 15.5 million health care workers with direct patient contact.
Here are the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: Total cases worldwide stand at 97.5 million this week – with an increase of nearly 4.4 million new confirmed cases in the past seven days. There were approximately 95,400 new confirmed deaths worldwide, bringing the total for confirmed deaths to nearly 2.1 million.
U.S. Cases and Deaths: Total confirmed cases in the U.S. reached 24.6 million this week. There was an increase of about 1.3 million confirmed cases between Jan. 14 and Jan. 21. Approximately 21,400 confirmed deaths in the past week brought the total in the United States to 410,100.
Factors Associated With COVID-19 Cases and Deaths in Long-Term Care Facilities: Findings from a Literature Review (News Release, Issue Brief)
Patterns in COVID-19 Cases and Deaths in Long-Term Care Facilities in 2020 (Issue Brief)
January 14 Web Event: A Shot in the Arm For Long-Term Care Facilities? Early Lessons from the COVID-19 Vaccine Rollout to High Priority Populations (Archived Recording)
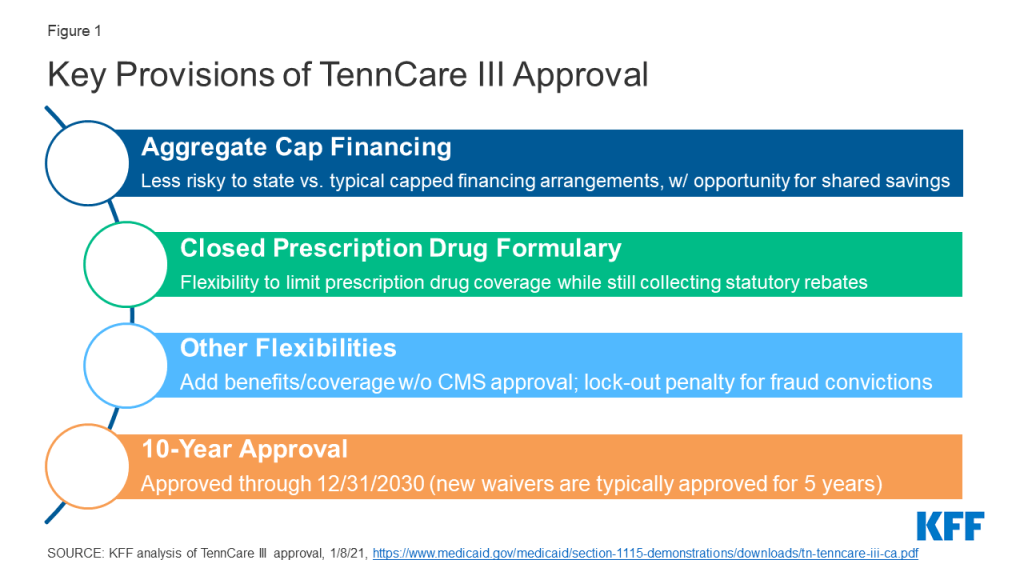
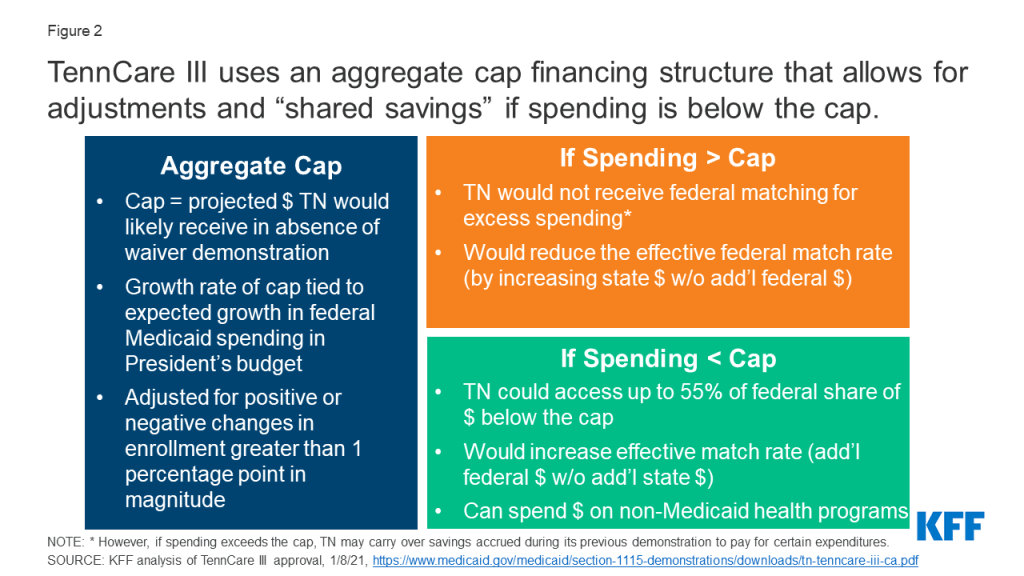
Section 1115 waiver activity has been a key area of interest in the final weeks of the Trump Administration. Section 1115 authority allows the HHS Secretary to waive certain provisions of federal law in state Medicaid programs to test policies that are likely to promote program objectives. These waivers generally reflect administration priorities, although the Secretary’s discretion is not unlimited. The incoming Biden Administration could rescind existing waiver guidance (such as guidance related to work requirements and capped financing) and/or issue new guidance. It could also review provisions in currently approved waivers and renewal requests and move to withdraw or not renew waivers that do not promote program objectives. Although CMS generally reserves the right to withdraw approved waiver and/or expenditure authorities at any time, precedent for withdrawing approved waivers is limited.
In its final days, the Trump Administration has approved controversial waivers that had been pending (most recently for Tennessee), extended other waivers more than a year before expiration, and took steps to try to prolong the process for withdrawing or amending approved waivers. This issue brief takes a closer look at this recent activity to understand implications for the Biden Administration.
Tennessee Approval
On January 8, 2021, CMS approved a waiver request from Tennessee that would transition nearly all of the state’s Medicaid program currently covered by its long-standing TennCare II waiver into a new TennCare III program. This waiver includes most TennCare enrollees, including children, parents, and pregnant women as well as many seniors and people with disabilities. This complex approval is particularly significant nationally due to provisions related to financing, drug coverage, and the duration of the waiver (Figure 1). These factors make Tennessee’s waiver a prime candidate for review by the Biden Administration.
Figure 1: Key Provisions of TennCare III Approval
Financing: The TennCare III waiver sets an aggregate cap on federal spending and provides an opportunity for the state to keep a portion of any federal savings (Figure 2). Both of these features differ from the way Medicaid financing works under current law where costs and savings are shared by the states and the federal government due to the formula that guarantees federal matching dollars at a rate set in statute without a pre-set limit. While Section 1115 waivers must be budget neutral to the federal government, that budget neutrality is typically determined on a per enrollee basis rather than an aggregate basis. In the past, capped demonstrations have been approved in Rhode Island, Vermont, and Virginia (for a limited population), but they are no longer in place in these states. CMS is explicit that its approval of Tennessee’s waiver is not a part of the Trump Administration’s Healthy Adult Opportunity (HAO) initiative, which allows for capped financing. The match rate is an area of Medicaid that may not be changed under Section 1115 waiver authority. Key financing elements of TennCare III include:
Setting the Cap. The aggregate cap would be adjusted each year to reflect the expected growth in federal Medicaid spending in the President’s budget and adjusted for positive or negative changes in enrollment that are greater than one percentage point in magnitude.
Spending Above the Cap. Typically, capped financing would pose fiscal risks to states and could lower a state’s effective match rate because any state spending above the cap would not receive federal matching funds, as is the case with capped financing for Puerto Rico and the other Territories. However, adjustments to Tennessee’s cap tied to the growth rate for Medicaid in the President’s budget (which has historically been higher than inflation and higher than the Tennessee’s historic growth) and to increased enrollment mitigate the risk of this capped financing model to Tennessee. If Tennessee’s expenditures do exceed the cap, the state may carry over savings accrued during the final five years of TennCare II to pay for certain expenditures. While Tennessee must submit an amendment to reduce the level of benefits or covered populations below what was in place at the end of 2020, the TennCare III approval does not prohibit such changes.
Spending Below the Cap. If expenditures are below the cap in a given demonstration year, Tennessee may access up to 55% of the federal share of savings to reinvest in state health programs (including those not eligible for Medicaid funding) if the state meets certain quality metrics (to be determined by Tennessee and CMS in the coming months), in addition to retaining 100% of the savings the state would normally get under Medicaid matching formula. Under this provision, Tennessee could see a higher effective match rate than statutory levels since this opportunity for shared savings allows the state to receive additional federal Medicaid dollars without additional state spending. Prior CMS guidance related to the use of federal Medicaid funds for non-Medicaid state programs has been mixed. Guidance from 2017 noted that CMS would no longer allow federal matching funds for designated state health programs (DSHP); however, in its approval of TennCare III CMS explained that it would allow for federal funds for non-Medicaid state health programs in line with policy principles established in its Health Adult Opportunity (HAO) guidance.
Figure 2: TennCare III uses an aggregate cap financing structure that allows for adjustments and “shared savings” if spending is below the cap.
Closed Formulary: Under federal rules, in exchange for significant rebates on prescription drugs, state Medicaid programs must cover nearly all drugs approved by the FDA, essentially requiring an “open formulary” (unlike private insurers, who can enter into negotiations with manufacturers about whether or not to include drugs on the insurers’ formularies). The TennCare III approval would allow Tennessee to instead cover the greater of either one drug per therapeutic class or the same number of drugs per class as a selected Essential Health Benefits benchmark plan in the Affordable Care Act exchange, with an exceptions process for coverage of non-formulary drugs. Tennessee could still collect statutory rebates for covered drugs. CMS previously rejected a similar proposal in Massachusetts.
10-Year Approval: In November 2017 guidance, CMS indicated it would consider approving “routine, successful, non-complex” Section 1115 extension requests for up to 10 years. Since then, CMS has approved 10-year waiver extensions for three non-family planning demonstrations (WI, ME, and IN). CMS approved TennCare III for 10 years even though it does not appear to meet the conditions in the 2017 guidance: it was approved as a new waiver (not an extension), received 6,186 comments (of which “the vast majority” opposed the waiver), and contains complex financing and provisions.
Other Key Waiver Issues to Watch
Other recent activity under the Trump Administration may hamper the Biden Administration’s efforts to review certain waivers.
Expedited and Early Approval of Waivers. On January 15, 2021 CMS approved a ten-year extension for the Texas Healthcare Transformation and Quality Improvement Program (THTQIP) waiver following a “fast track” extension process which allowed the state to waive public notice and comment requirements (citing the immediacy of the COVID-19 public health emergency). The THTQIP waiver had been set to expire on September 30, 2022. On the same day, CMS renewed Florida’s Managed Medical Assistance waiver (which had been set to expire in June 2022) through June 2030. These renewals include provisions that the Biden Administration may review, including uncompensated care pools which provide funding for people who could be covered through the Medicaid expansion. Early approvals of these requests under the Trump Administration may make it more difficult for the Biden Administration to modify or withdraw these provisions subsequently.
Process to Withdraw Waiver Authorities. Outgoing CMS Administrator Seema Verma has encouraged states to sign a “letter of agreement” that specifies that any future CMS determination suspending, terminating, or withdrawing a waiver must have an effective date no sooner than nine months after the initial determination. The letter also specifies timelines for hearings and a briefing schedule for states to challenge these determinations. These agreements could make it more difficult for the Biden Administration to amend or withdraw waivers that it determines to be inconsistent with Medicaid program objectives, depending upon how they are construed. Congressional Democrats have noted that these “letters of agreement” conflict with existing regulations that require CMS to establish such a process as part of each waiver’s terms and conditions and requested that CMS rescind them immediately.
Pending Litigation. The Supreme Court is reviewing appeals court decisions setting aside work requirement waivers in Arkansas and New Hampshire, with the opening briefs filed by the Trump Administration and states on January 19, 2021. Although the Biden Administration is likely to rescind guidance related to Medicaid work requirements and could move to withdraw other currently approved work requirement waivers, a Supreme Court ruling in favor of the HHS Secretary’s authority to approve work requirements could still leave these waivers open to future administrations.
As of January 19, 2021, 17 states were reporting some vaccination data by race/ethnicity, including 16 states reporting the distribution of vaccinations by race/ethnicity.
Black Americans’ share of vaccinations is smaller than their share of cases in 16 reporting states and smaller than their share of deaths in 15 of the states. The trend is similar for Hispanic Americans with them accounting for a smaller share of vaccinations compared to cases and deaths in most states reporting data.
White Americans’ share of vaccinations is larger than their share of cases in 13 of the 16 reporting states and larger than their share of deaths in 9 states.
Asian Americans are experiencing fewer and smaller gaps between their share of vaccinations and cases in reporting states. Data on Asians’ share of deaths is limited and data gaps also exist for American Indian and Alaska Native and Native Hawaiian and Other Pacific Islander people.
Vaccines are not yet broadly available and states are prioritizing specific groups before the general public, so vaccination patterns may change as more data is available. However, data and our news reporting at KHN have shown that vaccination is lagging by various measures for people of color. KFF will regularly update the data by race/ethnicity to track racial disparities in access and administration of COVID-19 vaccines.
Also available is a new data note examining the makeup (by race/ethnicity, income level, age, gender, education, and citizenship status) and health insurance coverage status of the estimated 15.5 million health care workers with direct patient contact. Health and long-term care workers were among the first groups prioritized for the COVID-19 vaccination based on federal guidelines, which states have tailored and implemented.
Some key findings in the data note include:
Overall, 59% of health care workers are White and 41% are people of color (including 17% who are Black, 14% who are Hispanic, and 8% who are Asian). However, the majority (52%) of workers in long-term care settings are people of color (including 28% who are Black, 15% who are Hispanic, and 6% who are Asian) while 48% are White.
A large majority (77%) of health care workers are women, and the number rises to 84% in long-term care settings.
17% of health care workers are low-income (household income less than 200% of the federal poverty level), with 5% having household income below the poverty level. One-third (33%) of workers in long-term care settings are low-income, including 11% who have household income below poverty.
14% of health workers in long-term care are uninsured and about one in five (21%) have Medicaid coverage. Overall, less than one in ten (7%) health care workers are uninsured.
Eight in ten of health care workers have completed at least some college, while 4% have not completed high school. Among those working in long-term care, six in ten have completed some college, with 10% having less than a high school education.
Media reports indicate some health workers are opting not to be vaccinated, particularly among those working in long-term care facilities, and recent KFF COVID-19 Vaccine Monitor data show that roughly three in ten health care workers (29%) express hesitancy about getting a COVID-19 vaccine. A better understanding of the health care workforce in direct contact with patients can better inform educational efforts and messages about the vaccine to ensure equity in its distribution. Read Key Characteristics of Health Care Workers and Implications for COVID-19 Vaccination for the full findings and discussion.
Nearly 6 in 10 Older Americans Don’t Know When or Where They Can Get a COVID-19 Vaccine; Black and Hispanic Adults among the Groups Least Likely to Have Enough Information
Two Thirds of the Public Give the Federal Government Low Marks for the Vaccine Rollout Under the Trump Administration; Half Expect the Situation to Get Better Under President Biden
Despite Optimism about COVID-19 Vaccines in the Future, Half Say They are Frustrated with the Current Situation and Nearly a Quarter are Angry
While older Americans are a high-priority group for getting a COVID-19 vaccine, the latest KFF COVID-19 Vaccine Monitor report finds that, among those who have not yet been vaccinated, most people ages 65 and older say they do not have enough information about when (58%) and where (59%) they will be able to get vaccinated.
Most essential workers, another high-priority group, say they have enough information about where to get a vaccine (55%) but do not have enough information about when they will be able to get vaccinated (55%). This includes some health care workers who have not yet gotten vaccinated and say they don’t have enough information about when they will be able to get vaccinated (21%).
“The Biden administration has been left with a huge challenge on vaccine administration. Most Americans don’t know when or where they can get a vaccine, including older Americans, who are already eligible to get a vaccine in a growing number of states,” KFF President and CEO Drew Altman said. “Understandably large numbers of people are frustrated, angry and confused.”
The findings highlight a key challenge facing public health authorities seeking to get their limited supplies of vaccine into the arms of priority populations. While the priorities differ across states, older Americans and at least some essential workers are high priorities for early phases of distribution across states.
Among the broader public, most who have not yet been vaccinated say they do not have enough information about when people like them will be able to get a vaccine (60%) or about where they can get a vaccine (55%).
Black and Hispanic adults, as well as low-income households, are among the groups least likely to say they have enough information. Within each group, at least two thirds say that they do not have enough information about when they can get vaccinated, and at least 6 in 10 say they don’t have enough information about where to get vaccinated.
Based on the latest Monitor survey fielded during the last days of the Trump administration, the Monitor report finds that about two thirds (65%) of the public rate the federal government’s distribution efforts so far as “fair” or “poor.”
There is a wide gap in how partisans grade the federal government’s performance. Republicans are more than twice as likely as Democrats to say the federal government is doing an “excellent” or “good” job (43% v. 17%), and Democrats are much more likely than Republicans to give negative marks (80% v. 46%). Independents fall in the middle with two-thirds giving the federal government negative marks.
Most Americans also rate their state government’s performance as only fair or poor (60%), though without a partisan divide, as majorities of Democrats, Republicans and independents hold this view.
About half (48%) of the public expects vaccine distribution to “get better” under President Biden’s administration, while most others expect the situation to “stay about the same” (36%). Relatively few (12%) expect distribution to “get worse.”
Democrats overwhelmingly expect improvements under President Biden (83%), as do a plurality of independents (45%). While few (12%) Republicans expect the situation to “get better” under President Biden, most (57%) expect it to stay about the same.
With millions of health care workers, long-term care residents and staff, and older adults across the country already getting vaccinated against COVID-19, most (66%) of the public say they feel “optimistic” that things will get better.
At the same time, half (50%) say they are “frustrated,” a third (33%) say they feel “confused,” and nearly a quarter (23%) say they are “angry,” highlighting the difficulties ahead as the vaccine rollout continues.
While optimism crosses party lines, more Democrats (61%) than Republicans (42%) or independents (48%) say they are frustrated, reflecting their higher levels of concerns about the pandemic. The groups most likely to express confusion about the current situation includes at least four in ten Black adults (46%), those under age 30 (40%), and those with annual incomes under $40,000 (42%).
Other findings include:
Two thirds (65%) of the public, including most Democrats (70%), independents (64%), and Republicans (59%), are confident that vaccines are being distributed in a way that is fair, similar to the December KFF COVID-19 Vaccine Monitor which found 67% of adults were confident the vaccine would be distributed in a fair manner.
While most Black adults express confidence that vaccines overall are being distributed fairly, half (52%) say they lack confidence that the needs of Black people are being taken into account. Among Hispanic adults, a significant minority (44%) lacks confidence that the needs of Hispanic people are being taken into account.
Next week, KFF will release new findings on people’s willingness to get a vaccine.
Designed and analyzed by public opinion researchers at KFF, the KFF Vaccine Monitor survey was conducted from Jan. 11-18 among a nationally representative random digit dial telephone sample of 1,563 adults, including oversamples of adults who are Black (310) or Hispanic (306). Interviews were conducted in English and Spanish by landline (287) and cell phone (1,276). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and hesitancy, trusted messengers and messages, as well as the public’s experiences with vaccination.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and hesitancy, trusted messengers and messages, as well as the public’s experiences with vaccination.
Key Findings
With news reports about states lagging in their vaccine distribution efforts and concerns that the supply of available vaccines will not meet demand, the latest KFF COVID-19 Vaccine Monitor poll (conducted January 11-18) finds two-thirds of U.S. adults (65%) say the federal government is doing a “fair” or “poor” job of distributing vaccines to the states. About three in ten adults give the federal government a positive rating of “excellent” or “good”. Likewise, six in ten think their state government is doing a “fair” or “poor” job of distributing the vaccine to people in their state. Notably, while similar shares across partisans give their state government negative marks, nearly half of Democrats (45%) think the federal government is doing a “poor” job while Republicans are more divided in their assessment.
About half of the public think that efforts to distribute the vaccine will “get better” under a President Biden Administration, compared to about a third who think efforts will “stay about the same,” and one in ten who say it will “get worse”. Democrats overwhelmingly expect distribution efforts to improve under President Biden (83%) as do a plurality of independents (45%), while most Republicans (57%) say it will remain about the same.
Two-thirds of adults say they are confident that the COVID-19 vaccines in the U.S. are being distributed fairly, including most Black adults (58%). However, about half of Black adults say they are “not too” or “not at all” confident that the vaccine distribution efforts are taking into account the needs of Black people (52%).
Majorities of the public who have not yet gotten vaccinated (94% of all adults) say they do not have enough information about when people like them will be able to get the vaccine (60%) and about where they will be able to get the vaccine (55%). Notably, about six in ten Black and Hispanic adults say they do not have enough information about where to get the vaccine, compared to about half of White adults who say the same. Among adults 65 and over – a group that has higher priority for the vaccine – about six in ten say they do not have enough information about when (58%) and where (59%) they will be able to get the vaccine.
Despite some discontent with government vaccine distribution efforts, two-thirds of the public saying they feel “optimistic” about the current status of vaccinations in the U.S. Though amidst reports of delays in the vaccine rollout in some areas, half also say they feel “frustrated” by the state of the vaccination efforts – including six in ten Democrats (61%), nearly half of independents (48%), and four in ten Republicans (42%). Notably, a third of adults say they feel “confused” by the state of vaccinations in country, which is similar to share who say they feel “satisfied,” indicating there is room for improvement in the first weeks of the Biden Administration.
Most Give Negative Assessment of Federal, State Government Vaccine Distribution Efforts
With news that some statesand localities are lagging behind in their distribution efforts and reports that demand for COVID-19 vaccines is outstripping supply, about two-thirds of adults say the federal government is doing a “fair” (33%) or “poor” (31%) job of distributing the COVID-19 vaccines to the states. Just under three in ten give the federal government a positive rating of either “good” (21%) or “excellent” (8%).
State governments also get a negative rating from the public with a majority saying their state government is doing just a “fair” job (36%) or a “poor” job (25%) of distributing vaccines to people in their state while a third say they are doing a “good” (25%) or “excellent” (7%) job.
Figure 1: Majorities Say Federal Government And State Governments Are Doing Fair Or Poor Job Of Distributing COVID-19 Vaccines
Notably, Democrats and Republicans give their state governments similar ratings with about six in ten saying they are doing a “fair” or “poor” job distributing the vaccine to people in their state. However, with the survey fielded in the last days of the Trump Administration, partisan opinions are more split when rating the federal government. Eight in ten Democrats say the federal government is doing a “fair” or “poor” job of distributing the COVID-19 vaccines to the states, whereas Republicans are more divided in their rating of the federal government (43% say “excellent” or “good”, and 46% “fair” or “poor”).
Figure 2: More Than Four In Ten Democrats Say Federal Government Is Doing Poor Job Of Distributing Vaccines To The States
About half of adults (48%) think efforts to distribute the vaccine in the U.S. will “get better” under the new President Biden Administration. About a third (36%) say they think vaccine distribution efforts will “stay about the same” while 12% say it will stay “get worse.” An overwhelming majority of Democrats (83%) think vaccine distribution efforts will “get better” under the Biden Administration while a majority of Republicans (57%) think distribution efforts will remain “about the same.” About four in ten independents (45%) expect distribution efforts to improve under President Joe Biden while 38% think it will “stay about the same.”
Figure 3: About Half Say Vaccine Distribution In The U.S. Will Get Better Under Biden Administration, Including Vast Majority Of Democrats
Despite some discontent with the vaccine distribution efforts of the federal government and state governments, most adults (65%) – including majorities across Democrats (70%), independents (64%), and Republicans (59%) – are confident that vaccines are being distributed in a way that is fair. About a third of the public say they are “not too confident” (20%) or “not at all confident” (12%) that the COVID-19 vaccines are being distributed fairly. In the December KFF COVID-19 Vaccine Monitor, fielded before COVID-19 vaccinations began in the U.S., a similar share of adults (67%) expressed confidence that the vaccine would be distributed in a fair manner.
Figure 4: Majorities Across Partisans Are Confident COVID-19 Vaccines Are Being Distributed Fairly In The U.S.
Nonetheless, while the public overall expresses confidence that the vaccines are being distributed fairly, concerns remain about whether the needs of people of color are being taken into account in the vaccine distribution process. While most Black adults (58%) are at least “somewhat confident” that the vaccine is being distributed fairly in the U.S., just 9% are “very confident” that is the case. Indeed, about half of Black adults (52%) say they are “not too” or “not at all” confident that the distribution of a COVID-19 vaccine is taking the needs of Black people into account. While most about half of Hispanic adults (53%) express some confidence that the needs of Hispanic people are being taken into account in the distribution of the vaccine, a large share (44%) say they are “not too confident” or “not at all confident.”
In KFF’s December 2020 COVID-19 Vaccine Monitor, half of Black adults (49%) and six in ten Hispanic adults (60%) said they were confident that the development of the vaccine was taking into account the needs of Black and Hispanic people respectively.
Figure 5: Less Than Half Of Black Adults Are Confident COVID-19 Vaccine Distribution Is Taking Into Account The Needs Of Black People
Majorities Say They Do Not Have Enough Information About Where And When To Get Vaccine
Among those who have not yet gotten the COVID-19 vaccine (94% of all adults), six in ten say they do not have enough information about when people like them will be able to get the vaccine. Information on where to get a vaccine is also needed as a majority (55%) of those who are not yet vaccinated say they do not have enough information about where they will get a vaccine. Despite some states having slightly different vaccine priority criteria, most adults (55%) say they have enough information about how their state is deciding who gets priority for the COVID-19 vaccine, with four in ten (43%) saying they do not have enough information.
Figure 6: Majorities Say They Don’t Have Enough Information About When And Where To Get A COVID-19 Vaccine
Adults 65 and older are among the groups many states are prioritizing for vaccine distribution. However, among those older adults who have not yet been vaccinated, about six in ten say they do not have information about when people like them will be able to get the COVID-19 vaccine (58%) and about where they will be able to get it (59%). Notably, a majority of essential workers who have not yet gotten the vaccine say they have enough information about where to get the vaccine (55%), but most say they do not have enough information about when people like them will be able to get vaccinated (55%). This includes health care workers (one-fifth of essential workers work in a health care delivery setting) who have not yet gotten vaccinated and say they don’t have enough information about when they will be able to get vaccinated (21%). A similar share (18%) of health care workers haven’t gotten vaccinated and say they don’t have enough information about where to get vaccinated.
About six in ten Black (62%) and Hispanic (63%) adults say they do not have enough information about where to get a COVID-19 vaccine, compared to about half of White adults who say they do not enough information (51%). Six in ten lower income adults with a household income under $40,000 (61%) say they do not have enough information about where they will be able to get a vaccine, compared to about half of those with a household income of $90,000 or more (49%). Similarly, lower income adults are also less likely than their higher income counterparts to say do not have enough information about when people like them will be able to get the vaccine (66% vs. 54%).
Figure 7: Limited Information About When, Where To Get The Vaccine Is Particularly An Issue For Black, Hispanic, And Lower Income Adults
Public Is Optimistic About COVID-19 Vaccination Efforts, Though Some Concerns Remain
With millions of health care workers, long term care workers and residents, and older adults throughout the country getting vaccinated against COVID-19, two-thirds of the public (66%) say they feel “optimistic” about the current status of vaccinations in the U.S. Nonetheless, perhaps reflecting the negative ratings given to the federal and state government vaccine distribution efforts, half of the public (50%) say they feel “frustrated” with the current status of COVID-19 vaccinations in the country. Additionally, one-third of adults say they feel “confused” about the status of vaccinations, including about four in ten Black adults (46%), young adults ages 18 to 29 (40%), and those with a household income under $40,000 (42%). A third of the public say they feel “satisfied” about current status of vaccinations in the U.S. while about one in four say they feel angry (23%).
Figure 8: Two-Thirds Say They Feel Optimistic About U.S. COVID-19 Vaccinations, Half Are Frustrated
Table 1: Views of Current Status of Vaccine Distribution in U.S. by Age, Race/Ethnicity
Percent who say each of the following describes how they feel about current status of COVID-19 vaccination in the U.S.:
Age
Race/Ethnicity
18-29
30-49
50-64
65+
Black
Hispanic
White
Optimistic
64%
66%
63%
70%
65%
70%
65%
Frustrated
48
46
55
53
55
42
52
Confused
40
30
32
33
46
38
31
Satisfied
32
27
29
41
31
43
30
Angry
25
20
26
23
22
24
23
Optimism about vaccinations crosses party lines with about two-thirds of Democrats, independents, and Republicans saying they feel optimistic about the current status of vaccinations in the country. However, despite the shared optimism, about six in ten Democrats (61%) also say they are frustrated, compared to less than half of Republicans (42%) and independents (48%) who say the same.
Figure 9: Majorities Across Partisanship Say They Feel Optimistic, Six In Ten Democrats Say They Feel Frustrated
Vaccine Hesitancy
These additional findings were released January 27, 2021.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and hesitancy, trusted messengers and messages, as well as the public’s experiences with vaccination.
Key Findings
As millions of Americans get their first and second doses of a COVID-19 vaccine, the latest KFF COVID-19 Vaccine Monitor reports that a growing share of the public is open to getting vaccinated, but many of the same groups that were hesitant in December remain hesitant now. The share of U.S. adults who want to get the vaccine as soon as possible has increased since December among Black, Hispanic, and White adults alike, and the share who say they want to “wait and see” how it works for other people has declined. Similarly, vaccine enthusiasm has shifted among those living in urban, suburban, and rural communities, but rural residents continue to be among the most resistant to getting vaccinated.
Partisanship continues to be a factor in attitudes towards COVID-19 vaccination. While vaccine enthusiasm increased for both Democrats and independents, it has not shifted among Republicans, who remain the most resistant, with 33% saying they will definitely not get the vaccine or will get it only if required to do so for work, school or other activities.
Racial and economic equity remains at the forefront of the COVID-19 vaccine conversation. Black and Hispanic adults and those with lower incomes are less likely than their White and higher-income counterparts to say they have personally received at least one dose of the vaccine or that they know someone who has. Black and Hispanic adults are also among those most likely to say they want to “wait and see” how the vaccine is working for other people before getting vaccinated themselves.
Knowing someone who has been vaccinated for COVID-19 is correlated with vaccine hesitancy and enthusiasm. Among those who say they want the vaccine “as soon as possible,” about half (52%) know someone who has been vaccinated, while among those who say they’ll get it “only if required,” a much smaller share (29%) know someone who has received the vaccine.
Those who have not yet been vaccinated for COVID-19 have many concerns and information needs related to the new vaccines, particularly when it comes to side effects and the effectiveness of the vaccine. About half say they don’t have enough information about the vaccine’s side effects or effectiveness, with higher shares of younger, Black, and Hispanic adults citing these information needs.
When examining messages and information that might increase the public’s willingness to get vaccinated, the messages the public finds the most convincing emphasize the vaccine’s effectiveness at preventing illness, protection for those who are vaccinated, and the ability to return to normal life. On the other hand, hearing that some people experience short-term side effects from the vaccine or that a small number of people have experienced serious allergic reactions has the potential to decrease willingness to get vaccinated for a substantial share of people.
Reinforcing previous findings about trusted sources of information, the survey finds that doctors, nurses, and other health care providers are the sources that people say they’re most likely to turn to when making their own decisions about whether to get vaccinated. Still, these conversations have not started yet for many, with only about a quarter (26%) saying they have asked a health care professional for information about the vaccine so far.
COVID-19 Vaccine Hesitancy and Enthusiasm
Trends in Hesitancy and Enthusiasm
With millions of Americans having received at least one dose of a COVID-19 vaccine, the latest KFF COVID-19 Vaccine Monitor (fielded just before President Biden took office) reports that enthusiasm for getting vaccinated has increased markedly since December. Four in ten U.S. adults (41%) now say that when an FDA-approved vaccine for COVID-19 is available to them for free, they will get the vaccine “as soon they can,” up from 34% in December. An additional 6% say they have already received at least one dose of the vaccine1 , bringing the total in this “as soon as possible” group to nearly half the public (47%). About three in ten (31%) say they want to “wait until it has been available for a while to see how it is working for other people” before getting the COVID-19 vaccine themselves, down from 39% in December. One in five adults are more reluctant to get vaccinated, including 7% who say they will get the vaccine only “if they are required to do so for work, school, or other activities” and 13% who say they will “definitely not” get the vaccine.
Figure 1: Compared To December, Larger Share Now Want COVID-19 Vaccine “As Soon As Possible,” Fewer Want To “Wait And See”
The share of U.S. adults who want to get the vaccine as soon as possible has increased since December among Black, Hispanic, and White adults alike, and the share who say they want to “wait and see” how it works for other people has declined among Black and White adults. However, Black adults (43%) and Hispanic adults (37%) remain significantly more likely than White adults (26%) to say they want to “wait and see,” while White adults (53%) are more likely to say they have already been vaccinated or want the vaccine “as soon as possible” compared Black or Hispanic adults (35% and 42%, respectively).
Figure 2: Vaccine Enthusiasm Increased Across Racial/Ethnic Groups, But Black And Hispanic Adults Remain More Wary Than White Adults
Similarly, there has been a shift in COVID-19 vaccine enthusiasm across different types of communities, including in urban, suburban, and rural areas. Among rural residents, 42% now say they have either already been vaccinated or want the vaccine “as soon as possible” and 27% want to “wait and see” how it’s working, essentially reversed from December when 29% said “as soon as possible” and 38% said “wait and see.” Still, rural residents remain much more likely than those living in urban areas to say they will “definitely not” take the vaccine (21% vs. 8%).
Figure 3: COVID-19 Vaccine Enthusiasm Has Shifted Across Community Types, But Rural Residents Remain More Resistant
Politically, the shift in COVID-19 vaccine enthusiasm between December and January was driven almost entirely by Democrats (and to a lesser extent, independents). Nearly two-thirds of Democrats (64%) now say they have either already been vaccinated or want the vaccine as soon as possible, up from 47% in December, and the share of independents who fall into this group increased from 30% to 45%. Republicans remain the least enthusiastic group, with 32% saying they have already been vaccinated or want the vaccine as soon as they can, 33% saying they want to wait and see how it works for others, and 25% saying they will definitely not get the vaccine, similar to the December results.
Figure 4: Increase In Vaccine Enthusiasm Driven Entirely By Democrats And Independents; Republicans Remain Reluctant
Which Groups Are Most Enthusiastic/Hesitant/Resistant?
Who is most enthusiastic to get vaccinated against the novel coronavirus? Adults ages 65 and over (66%) and Democrats (64%) are among those most likely to say that they have already gotten the vaccine or that they will get it “as soon as they can.” Those who work in a health care delivery setting (58%), White adults (53%) and those who live in households where someone has a serious health condition (51%) are also more likely than their counterparts to say they have been vaccinated already or want the vaccine “as soon as possible.”
Figure 5: Older Adults, Democrats Most Enthusiastic To Get Vaccinated
Who is most likely to say they want to wait to see how vaccination goes for other people before getting vaccinated themselves? Young adults ages 18-29 (43%), Black adults (43%), Hispanic adults (37%), and those living in urban areas (37%) are the most likely to say they want to “wait and see” how the COVID-19 vaccine is working for other people before getting vaccinated themselves.
Figure 6: Young Adults, Black Adults Most Likely To Want To “Wait And See”
One in five U.S. adults overall say they will either “definitely not” get vaccinated or that they’ll get vaccinated “only if required” for work, school, or other activities. One-third (33%) of Republicans fall into one of these most reluctant categories, as do about three in ten rural residents (29%) and a similar share of essential workers in fields other than health care (28%).
Figure 7: Republicans And Rural Residents Most Reluctant To Get Vaccine
Health Care Workers and Other Essential Workers
One priority group for early COVID-19 vaccination is essential workers – those who are required to work outside their home during the pandemic – including those who work in health care delivery settings. Twelve percent of all essential workers, including 32% of health care workers and 5% of non-health essential workers, say they have received at least one dose of the vaccine. Still, substantial hesitation remains even among these priority groups. Three in ten non-health essential workers (31%), and a similar share of health care workers (28%) say they want to wait and see how the vaccine is working for other people before getting it themselves. Among essential workers in fields other than health care, 12% say they’ll get the vaccine only if required, and 16% say they will definitely not get it, though these shares are somewhat smaller among health care workers (5% and 9%, respectively).
Figure 8: Many Essential Workers, Including Some Health Care Workers, Remain Hesitant Or Reluctant To Get COVID-19 Vaccine
Personal Experiences With Vaccination
At the time the survey was fielded, access to the COVID-19 vaccine in most states was limited to health care workers and long-term care workers, and some states had begun to open up access to other groups including older adults, other front-line workers, and those with certain health conditions. While just 6% of U.S. adults say they have personally received at least one dose of the COVID-19 vaccine, an additional 41% say they know someone who has been vaccinated. However, this proximity to vaccination is unevenly distributed across demographic groups. White adults (51%) are more likely than their Black and Hispanic counterparts (38% and 37%, respectively) to say they’ve either been vaccinated or know someone who has. Further, those with household incomes of $90,000 or more are almost twice as likely as those with incomes under $40,000 to say that they or someone they know has been vaccinated (65% vs. 33%). These patterns are consistent with a recent KFF analysis that found that the shares of vaccinations among Black and Hispanic people were lower compared to their shares of the total population in most states where data were reported by race and ethnicity.
Figure 9: Almost Half Of Adults Have Been Vaccinated Or Know Someone Who Has, A Group That Is Disproportionately White, High-Income
Knowing someone who has been vaccinated for COVID-19 is also correlated with vaccine hesitancy and enthusiasm among those who have not yet been vaccinated themselves. Among those who say they want the vaccine “as soon as possible,” about half (52%) know someone who has been vaccinated, while among those who say they’ll get it “only if required,” a much smaller share (29%) know someone who has received the vaccine.
Figure 10: Knowing Someone Who Has Been Vaccinated For COVID-19 Is Correlated With Vaccine Enthusiasm
Concerns and Information Needs
Concerns About COVID-19 Vaccines
Understanding the concerns or reservations that people have about vaccines can be helpful for crafting effective messages to convince people to get vaccinated. Asked about a variety of things they might be concerned about, the most common concern among U.S. adults who have not yet been vaccinated is that “the long-term effects of the COVID-19 vaccines are unknown” (68% say they are “very” or “somewhat” concerned about this). Majorities are also concerned that they might experience serious side effects from the vaccine (59%), that the vaccines are not as safe as they are said to be (55%), or that they are not as effective as they are said to be (53%). Fewer (31%) say they concerned that they might get COVID-19 from the vaccine.
Figure 11: Many Express Concern About COVID-19 Vaccine’s Long-Term Effects, Side Effects, Safety, and Effectiveness
Concerns about safety and side effects are highest among those who want to wait and see how the vaccine is working for others as well as those who are more reluctant to get vaccinated. Among the “wait and see” group that is closely watching how things go for others during the initial vaccine rollout, nine in ten (89%) are concerned about the long-term effects of the vaccine, eight in ten are concerned they may experience serious side effects, three-quarters are concerned the vaccines are not as safe as they are said to be, and two-thirds (68%) are concerned they might not be as effective as claimed.
Still, concerns about the vaccine are not completely absent for those who are eager to get vaccinated, or even those who have already received at least one dose of the vaccine. Notably, about half of those who have already received at least one dose (49%) and a similar share of those who say they want the vaccine as soon as possible (48%) say they are at least somewhat concerned that the long-term effects of the COVID-19 vaccines are unknown.
Figure 12: Concerns About COVID-19 Vaccine Vary By Vaccine Enthusiasm
Echoing previous findings that different groups have different reasons for being hesitant to get vaccinated, the January KFF COVID-19 Vaccine Monitor reports that different groups express different levels of concern about side effects, safety, and effectiveness as well. For example, among those who have not yet been vaccinated, about half of Black (54%) and Hispanic adults (50%) say they are concerned they might get COVID-19 from the vaccine, compared to a much smaller share of White adults (20%). Black and Hispanic adults are also more likely than White adults to express nearly every concern measured in the survey, with large shares of Black adults saying they are concerned that the long-term effects of the vaccine are unknown (86%), that they might experience serious side effects (75%), and that the vaccines may not be as safe (75%) or effective (71%) as they are said to be. Those with lower incomes and those who have not graduated from college are also more likely to express each of these concerns compared to their higher-income and more educated counterparts, and larger shares of women than men are concerned about each of these things.
Table 1: Concerns About A COVID-19 Vaccine Among Those Who Have Not Yet Been Vaccinated By Income, Race/Ethnicity, Education And Gender
Percent who say they are very or somewhat concerned about each of the following:
Total
Household income
Race/Ethnicity
Education
Gender
>$40K
$40K- >$90K
$90K+
Black
Hisp.
White
Less than College
College+
Men
Women
The long-term effects of the COVID-19 vaccines are unknown
68%
77%
72%
55%
86%
74%
63%
73%
58%
63%
74%
They might experience serious side effects from the COVID-19 vaccine
59
69
62
44
75
68
52
64
47
51
67
The COVID-19 vaccines are not as safe as they are said to be
55
66
59
37
75
61
49
60
42
47
64
The COVID-19 vaccines are not as effective as they are said to be
53
68
51
36
71
66
46
59
40
47
60
They might get COVID-19 from the vaccine
31
45
27
15
54
50
20
36
18
23
39
NOTE: Based on those who say they have not yet been vaccinated (94% of adults).
Information and Misinformation
Echoing the public’s concerns about side effects and effectiveness, nearly six in ten (57%) of those who have not been vaccinated against COVID-19 say they don’t have enough information about the potential side effects of the vaccine, and about half (49%) say they don’t know enough about the vaccine’s effectiveness. Notably, these information needs are substantially higher among those who say they are waiting to see how the vaccine works for others and those who say they will get vaccinated only if required. Just over three-quarters in both these groups say they don’t have enough information about the vaccine’s side effects, and about seven in ten say they don’t know enough about its effectiveness.
Figure 13: Large Shares Say They Don’t Have Enough Information About COVID-19 Vaccine Side Effects, Effectiveness
Information needs about COVID-19 vaccine side effects and effectiveness are higher among younger adults and those who are Black or Hispanic. Among Black and Hispanic adults who have not been vaccinated, about two-thirds say they don’t have enough information about the side effects of the vaccine and about six in ten say the same about the vaccine’s effectiveness. Among those under age 50, roughly six in ten say they don’t know enough about side effects and more than half need more information about effectiveness.
Figure 14: Majorities Of Younger, Black, Hispanic Adults Say They Don’t Have Enough Information About Vaccine Side Effects Or Effectiveness
Information needs also vary by education and income. Among adults with a high school education or less, 63% say they don’t know enough about the COVID-19 vaccine side effects and 57% say they lack information about its effectiveness. Similarly, among those with household incomes under $40,000, two-thirds say they don’t have enough information about side effects and six in ten (61%) don’t know enough about effectiveness.
Figure 15: Lower-Income Adults And Those Without College Degrees More Likely To Say They Don’t Have Enough Information About Vaccine
The Vaccine Monitor also reports that some of those who have not yet been vaccinated have heard misinformation about the COVID-19 vaccines and either believe it to be true or are unsure whether it is true or false. Most commonly, 8% of those who haven’t been vaccinated believe the vaccines currently being distributed contain the live virus that causes COVID-19, and an additional 11% say they’ve heard this and are unsure if it’s true. Small shares also believe or are unsure whether the COVID-19 vaccines have been shown to cause infertility (13%) or whether getting vaccinated requires paying an out-of-pocket cost (12%). Overall, one-third (34%) of those who have not been vaccinated believe or are unsure about at least one of these things.
Figure 16: One-Third Of The Unvaccinated Believe Or Are Unsure About Some Common COVID-19 Vaccine Myths
Notably, the share who believe or are unsure about at least one of these vaccine “myths” (that the vaccine contains the live coronavirus, that it causes infertility, or that an out-of-pocket cost is required to get vaccinated) is higher among those who want to “wait and see” how the vaccine works for other people (41%) and those who say they will “definitely not” get vaccinated (53%). These shares also vary by education level; 37% of those without a college degree believe or are unsure about at least one of these things, compared with 28% of college graduates.
Figure 17: Those In “Wait And See” And “Definitely Not” Groups Are More Likely To Believe Or Be Unsure About COVID-19 Vaccine Myths
On the other hand, about half (47%) of those who have not been vaccinated know that people will still need to wear face masks after getting vaccinated to help limit the spread of coronavirus, though this level of awareness is somewhat lower among the groups that are move hesitant to get vaccinated (36% in both the “wait and see” and “only if required” groups and 35% in the “definitely not” group).
Figure 18: About Half Are Aware That Face Masks Are Still Required After Vaccination, Fewer Among More Vaccine-Hesitant Groups
How Messages And Information Affect Willingness To Get Vaccinated For COVID-19
Messages and Information That Might Convince People To Get Vaccinated
The latest COVID-19 Vaccine Monitor tested different messages and information that might make people more likely to get vaccinated for COVID-19, and found that the messages the public finds the most convincing emphasize the vaccine’s effectiveness, protection from illness, and the ability to return to normal life. Among those who have not yet been vaccinated, majorities say they would be more likely to get a vaccine if they heard it was “highly effective” in preventing illness from COVID-19 (57%), that getting vaccinated offers protection from getting sick (56%), and that the vaccine offers “the quickest way for life to return to normal” (54%). Over four in ten say they would be more likely to get vaccinated if they heard that “millions of people have already safely been vaccinated” (46%) and that vaccination is needed to “get the U.S. economy back on track” (45%). Somewhat fewer said that knowing the vaccine is free (36%) or hearing that a doctor or health care provider they trust (38%) or a close friend or family member (32%) got vaccinated would make them more likely to get vaccinated themselves.
Figure 19: Most Convincing Messages Emphasize Vaccine Effectiveness, Protection From Illness, And Return To Normal Life
Among the important “wait and see” group that is the best target for converting from vaccine hesitant to vaccine enthusiastic, the most convincing messages are similar to those for the public overall. Two-thirds (67%) of this group says hearing that the vaccine will help protect them from getting sick would make them more likely to get vaccinated, and 64% say the same thing about hearing that the vaccines are highly effective. The same share (64%) say they would be more likely to get vaccinated after hearing that vaccination offers the quickest return to normal live. Few in the “definitely not” group say they’d be convinced by any of the messages tested, reflecting the daunting challenge of addressing reluctance to get vaccinated among this group.
Table 2: Responses To Pro-Vaccine Messages And Information By COVID-19 Vaccine Enthusiasm
Percent who say that hearing each of the following would make them more likely to get vaccinated:
Total
Get it as soon as you can
Wait and see
Get it only if required
Definitely will not get
The vaccines have been shown to be highly effective in preventing illness from COVID-19
57%
64%
66%
54%
18%
The vaccine will help protect you from getting sick from COVID-19
56
67
62
41
14
The quickest way for life to return to normal is for most people to get vaccinated
54
64
62
48
12
Millions of people have already safely been vaccinated for COVID-19
46
55
51
43
8
We need people to get vaccinated to get the U.S. economy back on track
45
55
48
47
11
A doctor or health care provider you trust has gotten the vaccine
38
49
38
34
7
There is no cost to get the vaccine
36
46
38
32
3
A close friend or family member got vaccinated for COVID-19
32
39
37
29
3
NOTE: Asked among those who say they have not yet been vaccinated (94% of adults).
Whether people find pro-vaccine messages and information convincing also varies by demographic group and by partisan identification. For example, larger shares of Black and Hispanic adults compared to White adults say they would be more likely to get vaccinated after hearing most messages tested in the survey. In particular, Hispanic adults are much more likely than White adults to report increased likelihood of getting vaccinated after hearing that there is no cost to get vaccinated (54% vs. 32%) or that a friend or family member (53% vs. 26%) or a health care provider they trust (51% vs. 34%) got the vaccine. Young adults ages 18-29 are also more likely than their older counterparts to say they’d be more likely to get vaccinated after hearing there is no cost (48%) or that a close friend or family member got vaccinated (41%).
Republicans are less likely than Democrats and independents to say that each message tested would make them more likely to get vaccinated. Despite many polls showing Republicans are concerned about reviving the U.S. economy, 30% of Republicans say they would be more likely to get vaccinated after hearing that getting people vaccinated will help get the economy back on track, compared to 57% of Democrats and 47% of independents.
Table 3: Responses To Pro-Vaccine Messages And Information By Race/Ethnicity, Age, Party Identification
Percent who say that hearing each of the following would make them more likely to get vaccinated:
Total
Age
Race/Ethnicity
Party ID
18-29
30-49
50-64
65+
Black
Hisp.
White
Dem.
Ind.
Rep.
The vaccines have been shown to be highly effective in preventing illness from COVID-19
57%
67%
57%
49%
55%
58%
69%
53%
67%
59%
43%
The vaccine will help protect you from getting sick from COVID-19
56
62
56
49
57
61
71
50
67
57
42
The quickest way for life to return to normal is for most people to get vaccinated
54
62
52
46
60
61
69
49
67
55
37
Millions of people have already safely been vaccinated for COVID-19
46
55
46
41
42
50
65
39
57
48
29
We need people to get vaccinated to get the U.S. economy back on track
45
50
43
41
49
51
63
40
57
47
30
A doctor or health care provider you trust has gotten the vaccine
38
44
41
31
36
43
51
34
48
40
24
There is no cost to get the vaccine
36
48
36
32
28
33
54
32
44
39
21
A close friend or family member got vaccinated for COVID-19
32
41
34
29
26
35
53
26
42
33
20
NOTE: Asked among those who say they have not yet been vaccinated (94% of adults).
Messages and Information That Might Deter People From Getting Vaccinated
Just as messaging can help convince people to get vaccinated, the public may also hear things that would make them less eager to get a COVID-19 vaccine. In the Monitor we report on a few of these messages and find that hearing about rare allergic reactions and short-term side effects may increase vaccine hesitancy for some. Overall, 39% of those who have not yet been vaccinated say that hearing that “a small number of people have experienced a serious allergic reaction” to the vaccine would make them less likely to get vaccinated, and 33% say the same after hearing that some-people experience “short-term side effects like pain or fever.” Fewer say they would be deterred after hearing that masks and social distancing will still be required after getting vaccinated (20% say this would make them less likely) or that two vaccine doses are required (18%).
Figure 20: Some Say Hearing About Rare Allergic Reactions And Short-Term Side Effects Would Make Them Less Likely To Get Vaccinated
Of particular concern, six in ten of those who want to “wait and see” how the vaccine is working say hearing about rare allergic reactions would make them “less likely” to get vaccinated, and half of this group says the same about hearing of short-term side effects.
Figure 21: “Wait And See” Group Particularly Affected By Hearing About Side Effects, Rare Allergic Reactions
About half of Black and Hispanic adults also say that hearing about short-term side effects and rare allergic reactions to the COVID-19 vaccine would make them less likely to get vaccinated. While one in five adults overall (18%) say that learning they would need to receive two doses of the vaccine several weeks apart would make them less likely to get vaccinated, about a quarter of Hispanic adults (28%), Black adults (26%), and those with household incomes under $40,000 (26%) say this is the case.
Table 4: Response To Negative Vaccine Messages And Information By Race/Ethnicity And Income
Percent who say that hearing each of the following would make them less likely to get vaccinated:
Total
Race/Ethnicity
Household Income
Black
Hispanic
White
>$40K
$40K- >$90K
$90K+
A small number of people have experienced a serious allergic reaction to the COVID-19 vaccine
39%
49%
50%
32%
48%
38%
27%
Some people were experiencing short-term side effects like pain or fever from the COVID-19 vaccine
33
46
46
23
43
32
17
You will need to continue to wear a mask and practice social distancing even after getting vaccinated
20
26
27
16
27
19
15
You had to receive two doses of the vaccine several weeks apart
18
26
28
12
26
17
7
NOTE: Asked among those who say they have not yet been vaccinated (94% of adults).
Who Will The Public Turn To When Making Decisions About Whether To Get Vaccinated?
Echoing previous findings about trusted sources of information on COVID-19 vaccination, the latest survey finds that 79% of U.S. adults who have not yet been vaccinated say they would be likely to turn to a doctor, nurse, or other health care provider when deciding whether to get a vaccination, including almost half (46%) who say they would be “very likely.” About six in ten say they’d be likely to turn to other sources such as the U.S. Centers for Disease Control and Prevention (CDC) (60%), family or friends (58%), their state or local health department (57%), or a pharmacist (54%). Few say they’d turn to a religious leader such as a priest, rabbi, or minister (17%).
Despite the fact that health care providers are the source people say they are most likely to turn to for vaccine information, relatively few (24%) of those who have not yet been vaccinated say they have already asked a doctor or other health care professional for information about the vaccine, a share that rises to 32% among those who say they want to get vaccinated “as soon as possible.”
Figure 22: 8 in 10 Say They’ll Turn To Doctors, Nurses, And Other Health Providers When Deciding Whether To Get COVID-19 Vaccination
Health care providers are the top source that Americans say they’ll turn to for help with vaccine decision-making across demographic groups. However, there are some differences in how different groups plan to use other sources in making this decision. For example, larger shares of Black and Hispanic adults, as well as young adults ages 18-29, say they’re likely to turn to the CDC or their state and local health department, reflecting partisan differences in how these sources of information are viewed. Further, a larger share of Black adults (33%) and Hispanic adults (29%) say they will turn to a religious leader for help with this decision compared to White adults (11%), suggesting a potential pathway for information delivery that could be productive with some communities of color.
Table 5: Likely Sources of COVID-19 Vaccine Information By Age. Race/Ethnicity And Party Identification
Percent who say that, when deciding whether to get a COVID-19 vaccine, they are very or somewhat likely to turn to each of the following for information:
Total
Age
Race/Ethnicity
Party ID
18-29
30-49
50-64
65+
Black
Hisp.
White
Dem.
Ind.
Rep.
A doctor, nurse, or other health care provider
79%
82%
80%
77%
79%
84%
81%
77%
85%
80%
72%
The Centers for Disease Control and Prevention (CDC)
60
78
64
51
46
71
69
55
74
64
39
Family or friends
58
62
56
57
58
61
63
56
64
57
54
Their state or local public health department
57
68
57
50
55
71
73
51
73
59
37
A pharmacist
54
56
55
51
55
65
57
52
63
54
48
A religious leader such as minister, pastor, priest, or rabbi
17
12
17
18
22
33
29
11
17
17
16
NOTE: Asked among those who say they have not yet been vaccinated (94% of adults).
Recent Sources Of Information
These additional findings were released February 3, 2021.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and hesitancy, trusted messengers and messages, as well as the public’s experiences with vaccination.
Key Findings
Adults with differing levels of enthusiasm towards getting the COVID-19 vaccine also report different media sources of information. Among those who say they want to get the COVID-19 vaccine as soon as they can, about half say they have gotten at least a fair amount of information about the vaccine from cable news (51%) and network television news (48%) in the past two weeks compared to about a third of adults who say they definitely will not get the vaccine (37% and 32% respectively) or who want to “wait and see” (37% and 36% respectively).
Adults who are hesitant about the COVID-19 vaccine and say they want to “wait and see” before getting it or who say they definitely will not get it are more likely to say they have gotten information about the vaccine from social media (37% and 40% respectively) than those who are more enthusiastic about getting the vaccine (25%). This likely reflects the higher levels of enthusiasm for the vaccine among older adults – who are more likely to say they have gotten information from cable news – and reflects vaccine hesitancy among younger adults, who are more likely to say they have gotten information from social media.
The public is also turning to more personal sources of information, as nearly four in ten adults say they have gotten vaccine information from family and friends. Notably, those who say they want the vaccine as soon as possible are more likely than those most resistant to the vaccine to say family and friends have been an information source.
Adults who say they want to get the vaccine “as soon as they can” are most likely to say they have gotten information about the vaccine from CNN (41%) and MSNBC (31%) while those who say they will definitely not get the vaccine are most likely to say they have gotten information from Fox News (33%). This split reflects both the fractured media environment and the partisan differences in enthusiasm for getting the COVID-19 vaccine.
Facebook is a key social media source of information with at least one in five adults across levels of vaccine enthusiasm and hesitancy saying they got information about the vaccine from Facebook, including more than a third of those who say they definitely will not get the vaccine.
Recent Sources Of COVID-19 Vaccine Information
The KFF COVID-19 Vaccine Monitor, conducted January 11-18, 2021, reports that majorities of the public say they do not have enough information about when they can get a COVID-19 vaccine and where to get their vaccine once it is time. As public health officials are tasked with making sure accurate and timely COVID-19 vaccination information is reaching the public, television news, social media, and family and friends are likely to be key mediums. Currently, many adults report getting information about the COVID-19 vaccine from television, including about four in ten who say that in the past two weeks they have gotten at least a fair amount of information about the vaccine from cable news (43%), network news (41%), and local TV news (40%). This includes a majority of adults 65 and older (54%) who say they have gotten at least a fair amount of information about the COVID-19 vaccine from cable news in the past two weeks. Notably, about two-thirds of Black adults – a group that is more likely to report they do not have enough information about where and when to get a COVID-19 vaccine – say they have gotten at least a fair amount of information about the vaccine from cable news (65%) and network news (68%) in the past two weeks.
Three in ten adults (31%) say they have gotten at least a fair amount of information about the vaccine from social media in the past two weeks while about one in five have gotten information from national newspapers (23%), radio (20%), and local newspapers (19%). Large shares of adults 18 to 29 (42%), Hispanic adults (40%), and Black adults (39%) report getting at least a fair amount of information about the vaccine from social media.
When it comes to more personal and direct sources of information, four in ten adults (40%) say they have gotten at least at a fair amount of information about the vaccine from family and friends. Though nearly eight in ten adults say they will turn to doctors, nurses and other health care providers when deciding whether to get vaccinated for COVID-19, currently most of the public is not getting recent information about the vaccine from these medical professionals as just three in ten (31%) report getting information from a doctor, nurse or other health care provider in the past two weeks. One in five adults (20%) say they have gotten information about the vaccine from an employer while fewer have gotten vaccine information from a health insurance provider (15%) or from a place of worship (9%). Though notably, Black (19%) and Hispanic adults (14%) are more likely than their White counterparts (7%) to say they have gotten a lot or a fair amount of vaccine information from a place of worship in the past two weeks.
Figure 1: TV News Tops Media Sources For COVID-19 Vaccine Information, Friends And Family Top Personal Sources Of Information
Table 1: Sources Of Information By Age, Race/Ethnicity, And Community Type
Age
Race/Ethnicity
Community type
Percent who say they got a lot or a fair amount of information about the COVID-19 vaccine from each of the following in the past two weeks:
18-29
30-49
50-64
65+
Black
Hispanic
White
Urban
Suburban
Rural
Media sources:
Cable news
34%
40%
45%
54%
65%
44%
40%
42%
44%
42%
Network TV news
34
38
40
52
68
47
36
41
40
41
Local TV news
28
37
43
53
59
54
35
42
40
36
Social media
42
37
28
16
39
40
27
34
30
28
National newspapers
31
27
16
20
28
28
21
25
24
16
Radio
18
20
22
19
29
27
17
22
21
13
Local newspapers
18
17
14
27
24
20
17
20
18
15
Personal sources:
Friends and family
41%
38%
40%
41%
48%
44%
37%
41%
39%
37%
A doctor, nurse, or other health care provider
35
31
30
29
38
30
30
32
31
30
An employer
27
23
20
8
20
24
18
22
20
13
A health insurance provider
12
12
15
25
28
20
13
15
16
14
A place of worship
5
8
11
13
19
14
7
9
8
14
Adults with differing levels of enthusiasm towards getting the COVID-19 vaccine report different media sources of information. Among the 41% of adults who say they want to get the COVID-19 vaccine as soon as they can, about half say they have gotten “a lot” or a “fair amount” of information about the vaccine from cable news (51%) and network television news (48%) in the past two weeks. Smaller shares of those who say they definitely will not get the vaccine and those who say they want to “wait and see” before getting the vaccine say they have gotten at least a fair amount of information about it from cable news or network news. Indeed, those who say they want to “wait and see” or who say they definitely will not get the vaccine are somewhat more likely to say they have gotten information about the vaccine from social media (37% and 40% respectively) than those who are more enthusiastic about getting the vaccine (25%).
Table 2: Media Sources Of Information By COVID-19 Vaccine Enthusiasm
Percent who say they got a lot or a fair amount of information about the COVID-19 vaccine from each of the following in the past two weeks:
Get it as soon as you can
Wait and see
Get it only if required
Definitely will not get vaccinated
Cable news
51%
37%
44%
37%
Network TV news
48
36
34
32
Local TV news
42
41
40
28
Social media
25
37
26
40
National newspapers
31
16
15
20
Radio
22
17
31
14
Local newspapers
22
15
17
15
NOTE: Among those who have not gotten the COVID-19 vaccine
One-third (33%) of the public believe or are unsure about at least one vaccine myth including that the vaccines currently being distributed contain the live virus that causes COVID-19, that it causes infertility, or that getting vaccinated requires paying an out-of-pocket cost. Despite concerns that vaccine misinformation may be spreading, particularly through social media, the KFF COVID-19 Vaccine monitor finds that overall, similar shares of both those who believe or are unsure about at least one of the these myths and those who do not believe this misinformation say they have gotten information from television news and social media.
Figure 2: Sources Of Information Are Similar For Both Those Who Believe Vaccine Misinformation And Those Who Do Not
While sizeable shares of adults across levels of vaccine enthusiasm say they have gotten information about the vaccine from friends and family in the past two weeks, those who say they want the vaccine as soon as possible are more likely than those most resistant to the vaccine to say family and friends have been an information source (44% vs. 34%). On the other hand, the most vaccine resistant group is at least twice as likely as those most enthusiastic for the vaccine to say they have gotten at least a fair amount of information from a place of worship (15% vs. 6%).
Table 3: Personal Sources Of Information By COVID-19 Vaccine Enthusiasm
Percent who say they got a lot or a fair amount of information about the COVID-19 vaccine from each of the following in the past two weeks:
Get it as soon as you can
Wait and see
Get it only if required
Definitely will not get vaccinated
Friends and family
44%
40%
28%
34%
A doctor, nurse, or other health care provider
32
25
21
31
An employer
17
18
23
14
A health insurance provider
16
13
13
16
A place of worship
6
10
7
15
NOTE: Among those who have not gotten the COVID-19 vaccine
Specific Cable News Information Sources
Reflecting the fractured media environment and the partisanship that has characterized the U.S. COVID-19 response, people with different levels of vaccine enthusiasm report different sources of COVID-19 vaccine information when it comes to cable news. Those who say they want to get the vaccine as soon as possible are most likely to say they have gotten information about the vaccine from CNN (41%) and MSNBC (31%), while those who say they will definitely not get the vaccine are most likely to say they have gotten information from Fox News (33%). Notably, those who say they definitely will not get the vaccine are about twice as likely to say they have gotten information from Newsmax (13%) than those who want to get the vaccine as soon as possible (5%) or who want to “wait and see” (6%). Among adults who say they want to “wait and see” before getting the vaccine or who say they will only get the vaccine if required, one in four say they have gotten information from CNN and Fox News.
Figure 3: Specific Cable News Source Varies By Vaccine Enthusiasm And Hesitancy
When thinking about what is said in the news, adults who say they think the seriousness of COVID-19 is generally underestimated or generally accurate are most likely to say they have gotten information about the vaccine from CNN (43% and 36% respectively). On the other hand, those who say the seriousness of COVID-19 is exaggerated are most likely to say Fox News was their cable news source for information about the vaccine (29%). Similarly, those who say the seriousness of COVID-19 is exaggerated are three times as likely as those who say the seriousness of the virus has been presented accurately or has been underestimated to say they have gotten information from Newsmax. Given that people self-select their news sources, these data do not necessarily prove a causal relationship; it may be that those who believe the seriousness of COVID-19 is exaggerated are more likely to select specific news sources, rather than the news sources being the origin of the belief that the seriousness of COVID-19 is exaggerated.
Figure 4: Specific Cable News Source Varies By Perception Of Seriousness Of COVID-19
Specific Social Media Information Sources
Facebook is a key social media source of information with at least one in five adults across levels of vaccine enthusiasm and hesitancy saying they got information about the vaccine from Facebook in the past two weeks. It emerges as a particularly important media source for those most reluctant to get the vaccine with 36% of those who say they will definitely not get the vaccine saying they have gotten information from Facebook.
Figure 5: At Least One in Five Got Information About The Vaccine From Facebook, Including More Than A Third Of Those Most Reluctant
Irrespective of whether people think the seriousness of COVID-19 has been exaggerated, accurately presented, or underestimated, Facebook maintains a dominant position as a social media source of information.
Figure 6: Facebook Is The Top Social Media Information Source Across Perceptions Of The Seriousness Of COVID-19
Methodology
This KFF COVID-19 Vaccine Monitor was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted January 11- 18, 2021, among a nationally representative random digit dial telephone sample of 1,563 adults ages 18 and older (including interviews from 306 Hispanic adults and 310 non-Hispanic Black adults), living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). Phone numbers used for this study were randomly generated from cell phone and landline sampling frames, with an overlapping frame design, and disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification was based on incidence of the race/ethnicity subgroups within each frame. Specifically, the cell phone frame was stratified as: (1) High Hispanic: Cell phone numbers associated with rate centers from counties where at least 35% of the population is Hispanic; (2) High Black: Cell phone numbers associated with remaining rate centers from counties where at least 35% of the population is non-Hispanic Black; (3) Else: numbers from all remaining rate centers. The landline frame was stratified as: (1) High Black: landline exchanges associated with Census block groups where at least 35% of the population is Black; (2) Else: all remaining landline exchanges. The sample also included 246 respondents reached by calling back respondents that had previously completed an interview on the KFF Health Tracking Poll at least nine months ago. Another 197 interviews were completed with respondents who had previously completed an interview on the SSRS Omnibus poll (and other RDD polls) and identified as Hispanic (n = 75; including 24 in Spanish) or non-Hispanic Black (n=122). Computer-assisted telephone interviews conducted by landline (287) and cell phone (1,276, including 931 who had no landline telephone) were carried out in English and Spanish by SSRS of Glen Mills, PA. To efficiently obtain a sample of lower-income and non-White respondents, the sample also included an oversample of prepaid (pay-as-you-go) telephone numbers (25% of the cell phone sample consisted of prepaid numbers) Both the random digit dial landline and cell phone samples were provided by Marketing Systems Group (MSG). For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s 2019 U.S. American Community Survey (ACS), on sex, age, education, race, Hispanic origin, and region, within race-groups, along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the January- June 2019 National Health Interview Survey. The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample, and design modifications, namely, the oversampling of prepaid cell phones and likelihood of non-response for the re-contacted sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Group
N (unweighted)
M.O.S.E.
Total
1,563
± 3 percentage points
Total who have not gotten a COVID-19 vaccine
1,454
± 3 percentage points
Race/Ethnicity
White, non-Hispanic
823
± 4 percentage points
Black, non-Hispanic
310
± 7 percentage points
Hispanic
306
± 7 percentage points
Party Identification
Democratic
555
± 5 percentage points
Republican
301
± 7 percentage points
Independent
484
± 5 percentage points
Vaccine Uptake
Already got vaccinated/Will get vaccine as soon as they can
798
± 4 percentage points
Wait and see
464
± 6 percentage points
Only if required/Definitely not getting vaccine
282
± 7 percentage points
Cross-tabs
Appendix
These additional findings were released February 3, 2021.
Appendix Table 1: Cable News Information Sources By Age, Race/Ethnicity, And Community Type
Percent who say they got information about the COVID-19 vaccine from each of the following:
Total
Age
Race/Ethnicity
Community type
18-29
30-49
50-64
65+
Black
Hispanic
White
Urban
Suburban
Rural
CNN
31%
33%
31%
29%
32%
58%
34%
26%
34%
32%
22%
Fox News
24
18
20
25
36
28
27
23
21
26
26
MSNBC
22
18
18
24
29
41
19
20
22
24
17
One America News
11
8
9
13
14
12
15
10
10
10
15
Newsmax
7
3
7
9
8
7
7
8
4
8
9
Appendix Table 2: Social Media Information Sources By Age, Race/Ethnicity, And Community Type
Percent who say they got information about the COVID-19 vaccine from each of the following:
Total
Age
Race/Ethnicity
Community type
18-29
30-49
50-64
65+
Black
Hispanic
White
Urban
Suburban
Rural
Facebook
26%
26%
36%
23%
14%
29%
32%
5%
25%
27%
27%
YouTube
12
22
15
9
3
16
22
9
12
15
6
Twitter
9
20
10
5
2
9
11
7
11
9
5
Instagram
8
19
10
3
2
16
16
4
12
7
3
Endnotes
Estimates of the number of people vaccinated from this or any survey may vary from government statistics due to survey timing or margin of sampling error. ↩︎