KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
The Kaiser Health Policy News Index is designed to help journalists and policymakers better understand which health policy-related news stories Americans are following, and what the public knows about health policy issues covered in the news. It also looks at how attention to health policy news stories compares to other national news stories.
Health Policy Stories v. National News Stories
Table 1 below presents the top news stories of 2016, as determined by the percent of Americans who said they followed news coverage related to each story “very” or “fairly” closely in monthly Kaiser tracking polls. The major news stories that dominated this past year and captivated Americans’ attention range from multiple conflicts involving police officers to the various scripted and unscripted events of the 2016 presidential election.
As seen in the table, health policy news stories were never the most closely followed news stories. Across the ten Kaiser Health Tracking Polls conducted between January and November 2016, the presidential campaign was the top news story in more than half of these surveys. On average, more than seven in ten Americans said they were closely following news about the election each month.
Table 1: Most Closely Followed Stories in 2016 by Month
Month
Story
Percent who say theyfollowed the story closely
January
Conflicts involving ISIS and other Islamic militant groups in Iraq and Syria
76%
February
2016 presidential campaigns
Conflicts involving ISIS and other Islamic militant groups
73
73
March
2016 presidential campaigns
81
April
Terrorist attacks in Brussels and other conflicts involving ISIS
80
June
The attack at a LGBT night club in Orlando, Florida
85
July
2016 presidential campaigns
83
August
Conflicts involving ISIS and other Islamic militant groups
Republican candidate Donald Trump’s presidential campaign win
82
NOTE: In May 2016, no tracking poll was conducted. The December tracking poll will be released in January 2017.
Although the election was certainly the biggest national story of 2016, there were several major health policy stories that made news this year, including the unsafe levels of lead in Flint, Michigan’s water supply and the Zika virus outbreak. The year was bookended by stories about Republican lawmakers and the Affordable Care Act, with January’s top health story being President Obama vetoing repeal of the law and November’s top health story being Republican lawmakers’ plans to repeal the law once President-elect Trump is in office.
Table 2: Most Closely Followed Health Policy Stories in 2016 by Month
Month
Health Policy Story
Percent who say theyfollowed the story closely
January
Congressional efforts to repeal the 2010 health care law and President Obama’s veto
48%
February
Unsafe levels of lead found in the drinking water in Flint, Michigan
64
March
Unsafe levels of lead found in the drinking water in Flint, Michigan
63
April
Unsafe levels of lead found in the drinking water in Flint, Michigan
70
June
Reports about rising health insurance premiums
61
July
The Zika virus outbreak
The ongoing heroin and prescription painkiller addiction epidemic in the U.S.
52
52
August
The Zika virus outbreak
60
September
The Zika virus outbreak
61
October
The Zika virus outbreak
64
November
Republican plans to repeal the 2010 health care law
70
NOTE: In May 2016, no tracking poll was conducted. The December tracking poll will be released in January 2017.
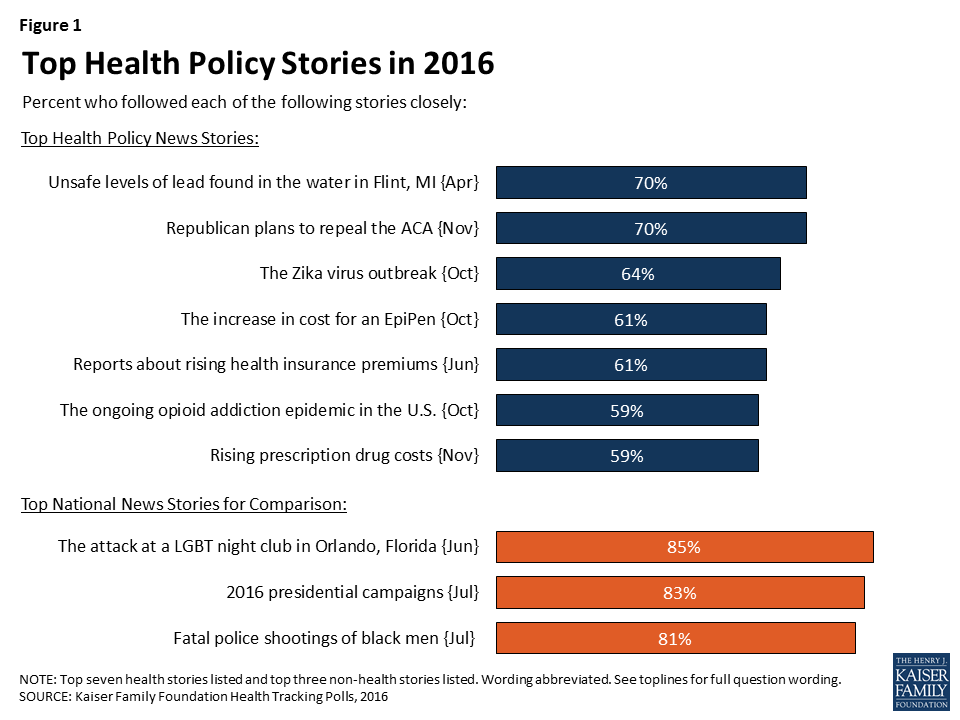
Overall, the top three most closely-followed news stories in 2016 were the attack at an LGBT night club in Orlando, Florida (85 percent reported following this story closely in June), the 2016 presidential campaign (83 percent in July), and the fatal police shootings of black men (81 percent in July). The top three most closely followed health policy news stories in 2016 were the unsafe levels of lead in Flint, Michigan’s drinking water (70 percent in April), Republicans post-election plans to repeal the Affordable Care Act (70 percent in November), and the Zika virus outbreak (64 percent in October).
Figure 1: Top Health Policy Stories in 2016
A Closer Look at Some of the Top Health Policy News Stories
In addition to tracking which health policy-related news stories Americans are following, the Kaiser Health Tracking Polls also examines what the public knows about health policy issues covered in the news. In 2016, we examined Americans’ awareness of and attitudes towards several of the health policy stories in the news.
Flint, Michigan Water Crisis
While Flint, Michigan began using the Flint River as its water source in April 2014, serious concerns about the level of lead in the city’s drinking water supply did not emerge until 2015. The Kaiser Family Foundation began tracking Americans’ attention to news about the unsafe levels of lead in Flint’s water supply in February 2016, and the story ranks as one of the top health policy news stories of the year. One of the main findings from our survey work during this time was the lack of confidence that Americans had in their state governments to ensure the safety of public services; in April, about three in ten (29 percent) reported being ‘extremely’ or ‘very’ confident that their state government can ensure the safety of public water supplies over the next five years while seven in ten reported being either “somewhat confident” or “not all confident.”
Figure 2: Majority of the Public Not Very Confident in State Government’s Ability to Ensure Safety of Public Services
News about the Affordable Care Act
The year began with Republican lawmakers voting to repeal the Affordable Care Act (ACA), only to have President Obama veto the bill.1 And with the election of Republican presidential candidate Donald Trump, the year is ending with reenergized efforts to repeal this legislation and accompanying uncertainty about the future of the U.S. health care system. Throughout 2016, Americans have paid varying degrees of attention to news stories about different aspects of the ACA, with news about Republican post-election plans to repeal the law (70 percent reported following this story closely in November), reports about rising health insurance premiums (61 percent in June), and the number of Americans without health insurance (58 percent in September), having the largest share of individuals who reported following news about these stories closely.
Figure 3: Americans Vary in How Closely they Follow ACA-Related News
Partisans Vary In Perceptions of How Media Cover the ACA
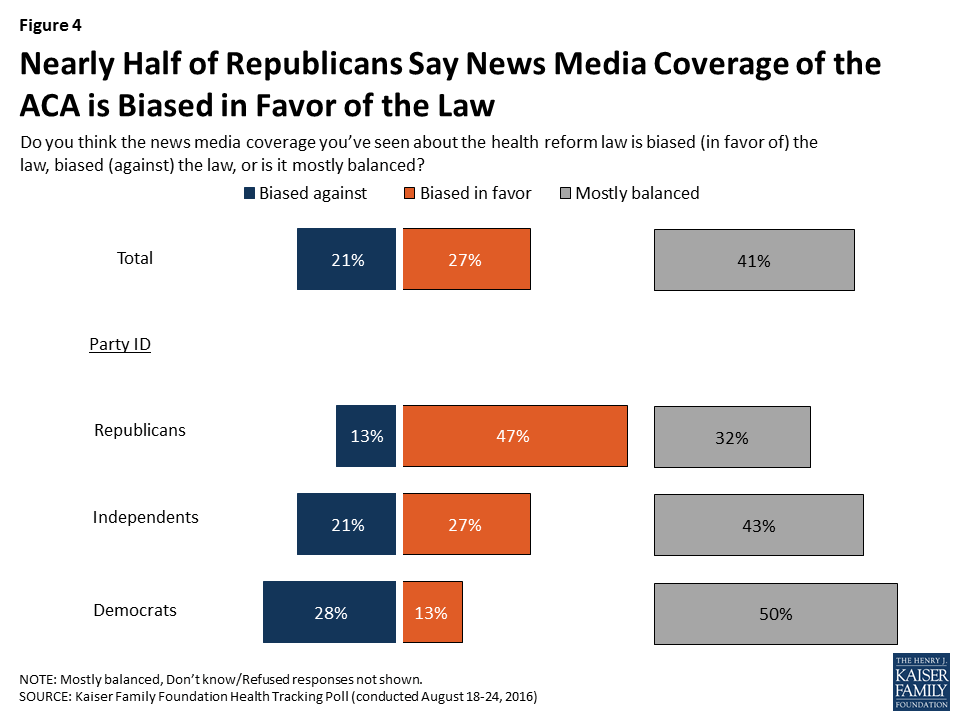
As with almost everything associated with the ACA, Americans’ attitudes of how the news media cover the law are largely dependent on party affiliation. As seen in August, not only do Republicans, Democrats, and independents have very different views towards the law – they also have different views on how the media cover the law. Nearly half (47 percent) of Republicans said the coverage was biased in favor of the law while half of Democrats and 43 percent of independents said the news coverage was mostly balanced.
Figure 4: Nearly Half of Republicans Say News Media Coverage of the ACA is Biased in Favor of the Law
Zika Virus Outbreak
The Kaiser Family Foundation started tracking Americans’ attention to the Zika virus outbreak beginning in February 2016, when the World Health Organization first declared the virus to be an international public health emergency.2 Throughout 2016, the Zika virus outbreak was one of the most followed health stories, with about six in ten of the population from February through October saying they followed news about the virus closely.
Our polls this year have also measured overall knowledge of the ways the virus spreads, the effects of the virus, and support for Congressional funding aimed at reducing the impact of the virus. Overall, the surveys found that although Americans said they were paying close attention to the virus (especially during the summer months), very few reported that they were personally affected. The September Kaiser Health Tracking Poll found that while a vast majority of Americans have heard or read about the Zika virus, very few (2 percent) said they personally knew anyone whose health had been affected by the virus.
Figure 5: Nine in Ten Americans Have Heard at Least a Little About Zika; Two Percent Know Someone Whose Health Is Affected
For more findings from our survey research on Zika, visit our Zika slideshow.
The U.S. Heroin and Prescription Painkiller Epidemic
Throughout 2016, the news media has covered stories about the increase in Americans’ use of heroin and prescription painkillers, and the increase in overdose deaths related to these drugs. News stories about the opioid epidemic included specific events such as the announcement of the Centers for Disease Control and Prevention’s new guidelines for prescribing prescription painkillers in March3 and more general stories about how the epidemic is affecting individuals and communities. The Foundation began tracking Americans’ attention to the epidemic in June. Since then, with the exception of one month, at least half of the public have reported closely following news stories related to the epidemic.
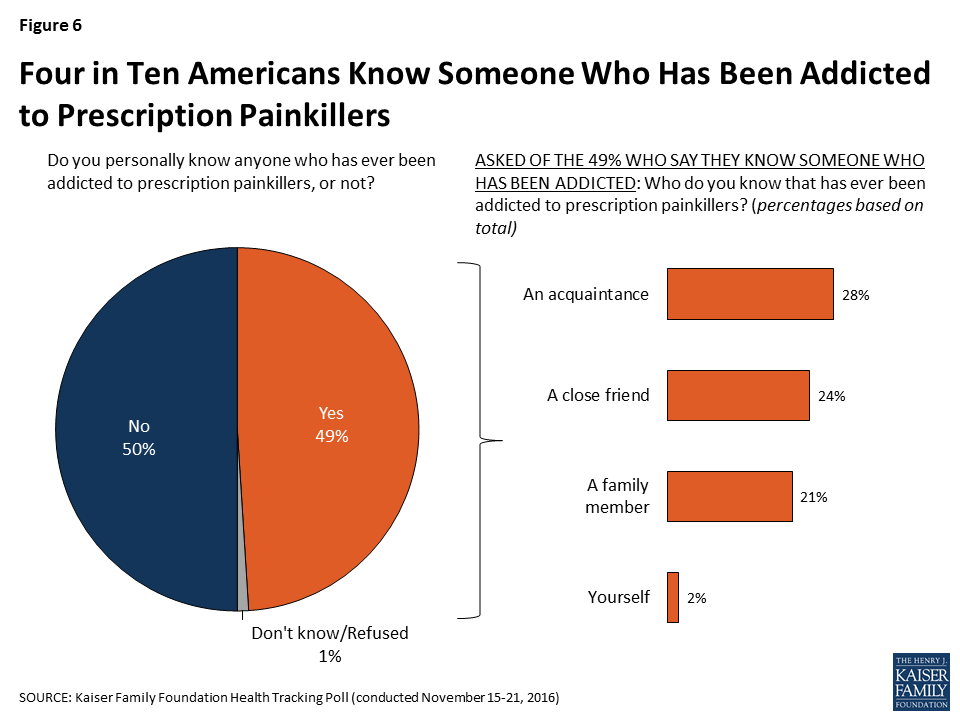
In addition to tracking attention to these stories, several of our surveys examined the public’s attitudes toward, and experiences with, the prescription painkiller epidemic, including the November Kaiser Health Tracking Poll, which found that nearly half of Americans said they knew someone who had been addicted to prescription painkillers, including 2 percent who said it was themselves who was addicted.
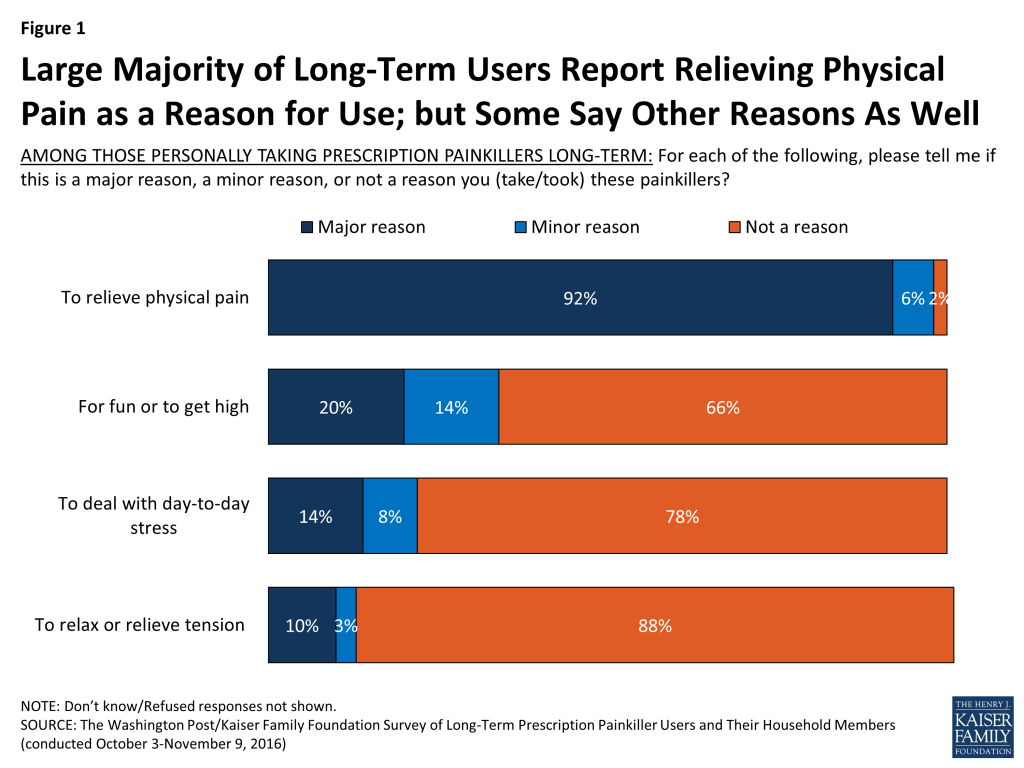
Figure 6: Four in Ten Americans Know Someone Who Has Been Addicted to Prescription Painkillers
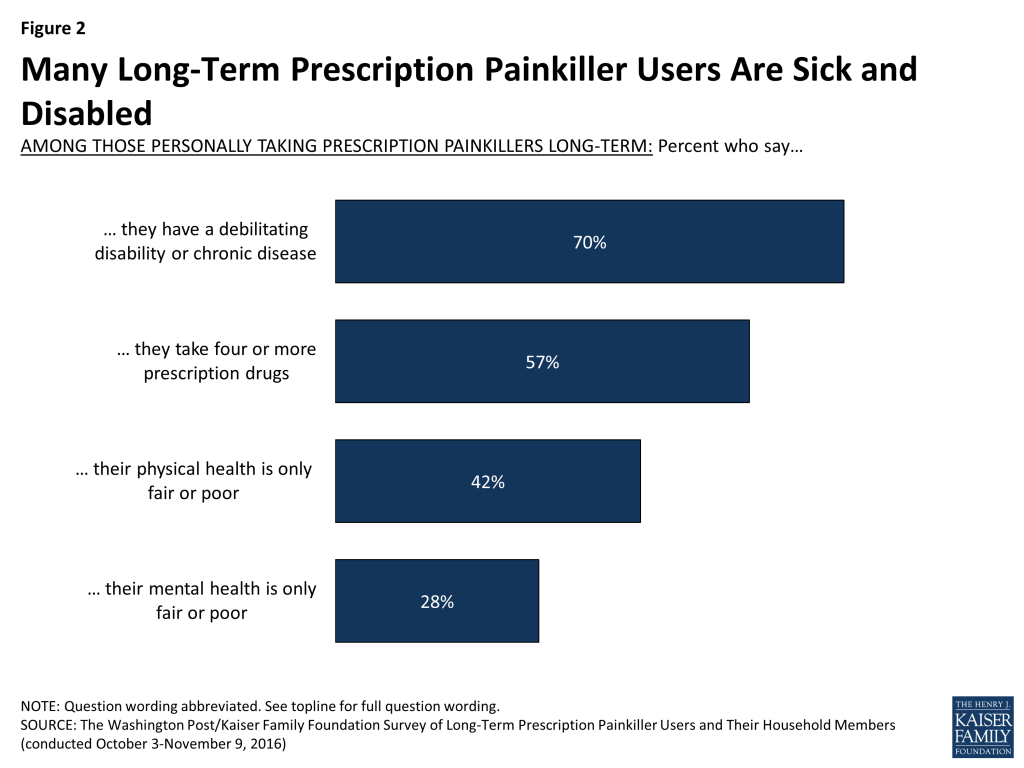
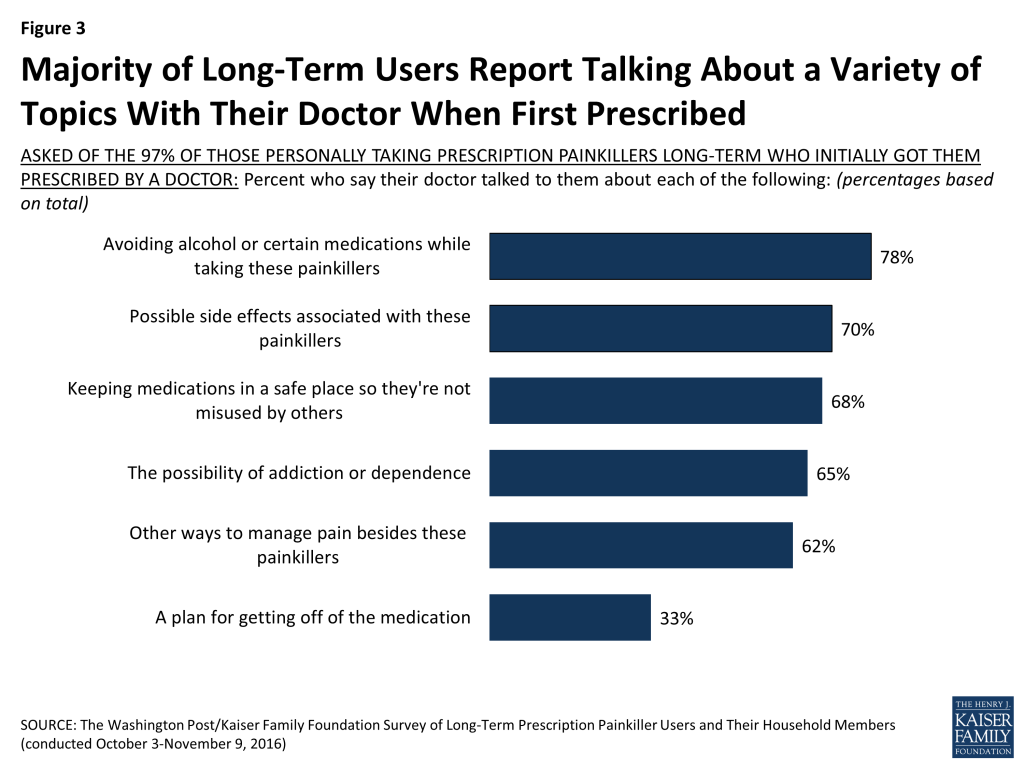
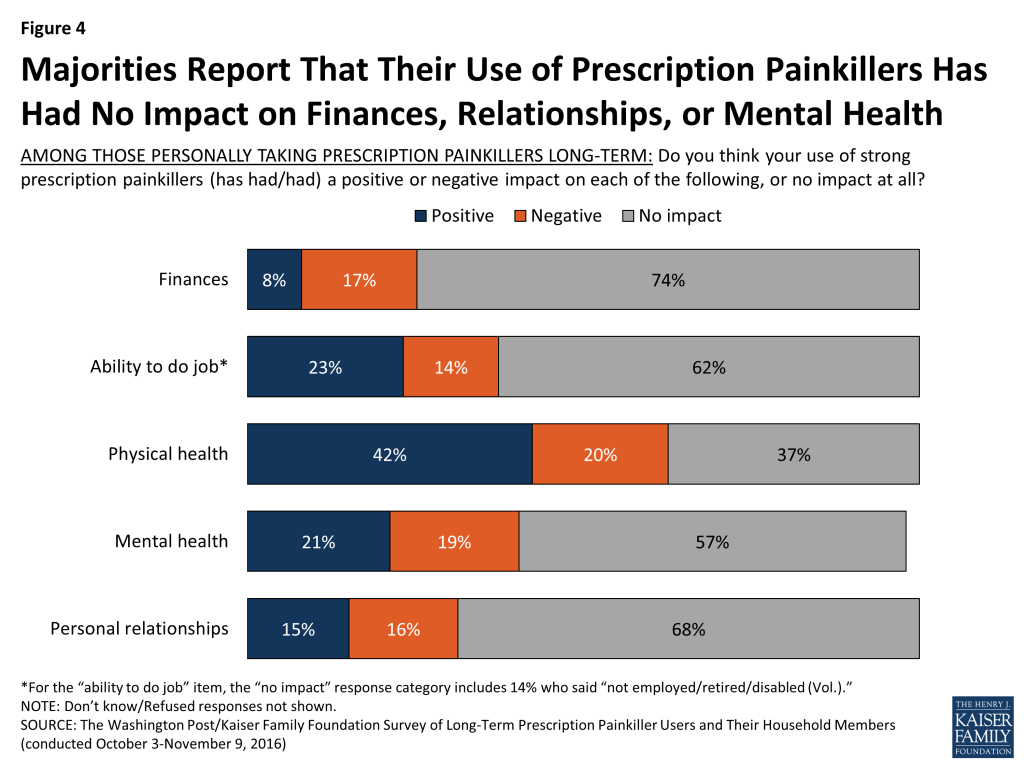
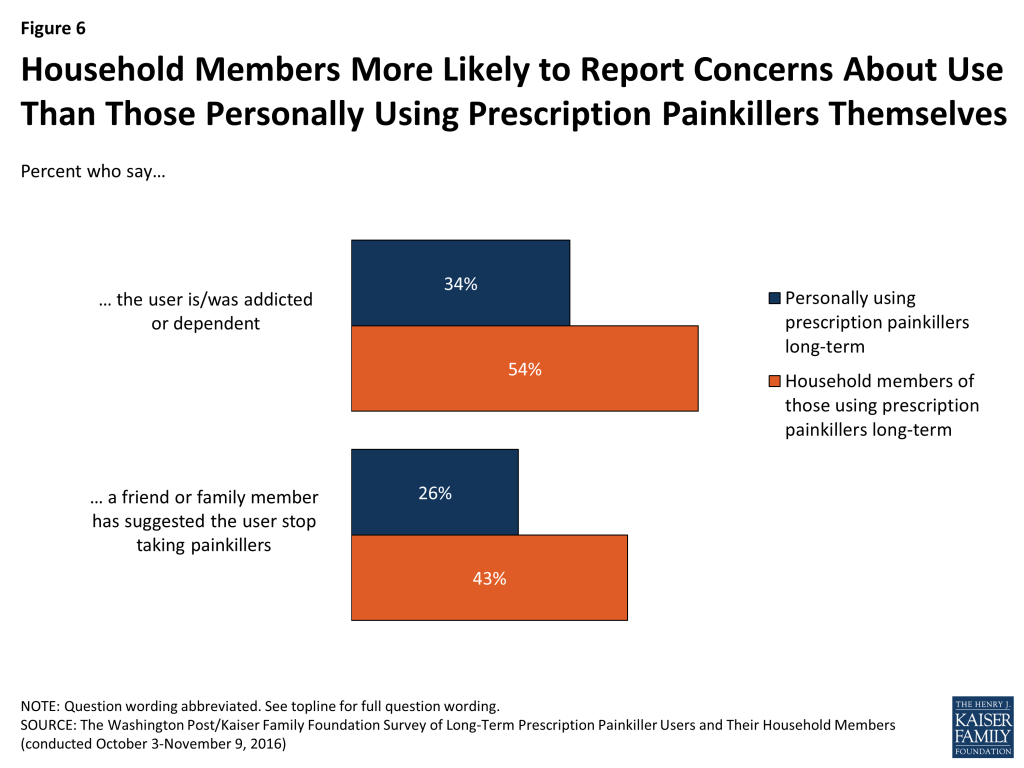
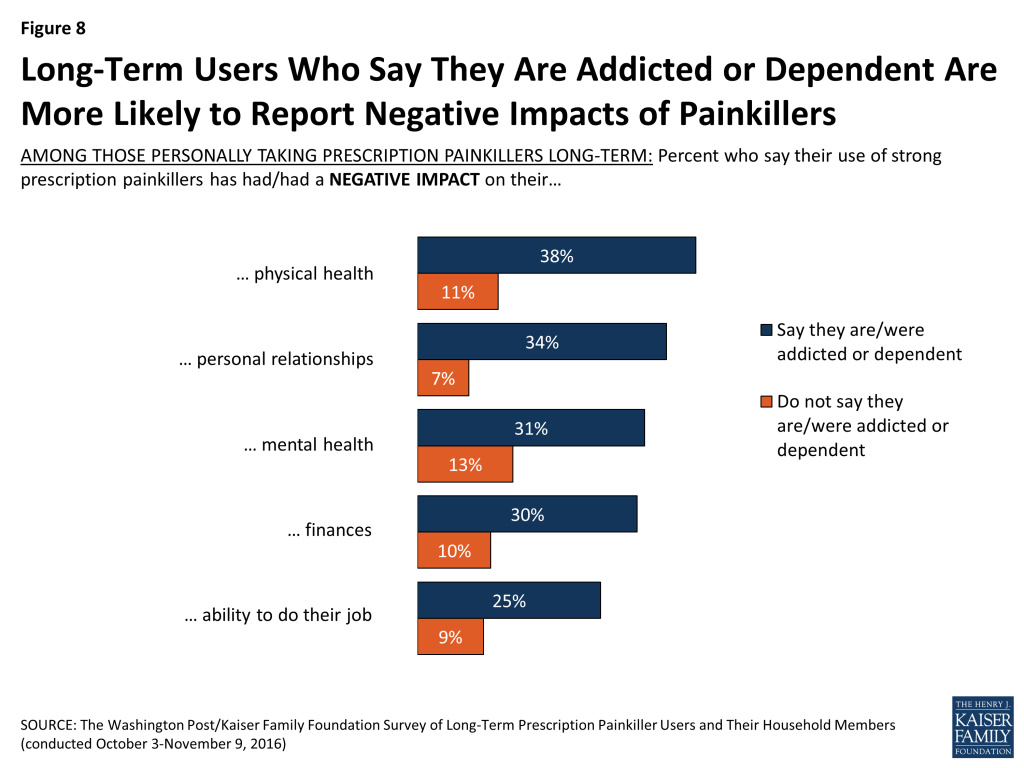
In addition, a partnership survey with The Washington Post took a closer look at U.S. adults who were long-term users of prescription painkillers and found that one in three (34 percent) long-term opioid users reported being physically dependent or addicted.
Prescription Drug Prices
Another major health story, followed by most Americans this year, has been news about the rising costs of prescription drugs – most notably, coverage about an increase in cost for the EpiPen. The October Kaiser Health Tracking Poll found that about six in ten Americans reported following news about the increase in cost for the EpiPen, which was similar to the share who reported following more general news about the rise in prescription drug costs in the November Kaiser Health Tracking Poll.
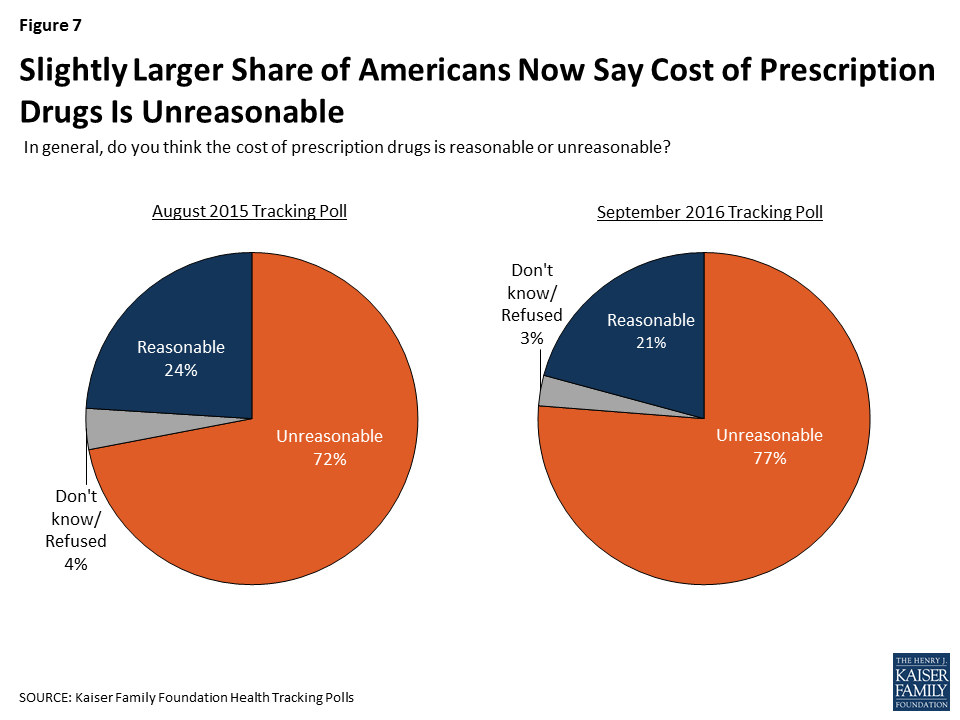
In light of the recent media attention on rising prescription drug costs, we have also been tracking Americans’ perceptions of prescription drug costs and find that these perceptions have changed over time. For example, in September 2016, we found a larger share of Americans said they think prescription drug prices were unreasonable compared to those who said they were unreasonable a year earlier.
Figure 7: Slightly Larger Share of Americans Now Say Cost of Prescription Drugs Is Unreasonable
More data on public opinion on prescription drugs and their prices is available in a summary slideshow.
Methodology
The Kaiser Family Foundation tracks the public’s attention to and awareness of the top health policy stories using the Health Policy News Index (HPNI) in each month’s tracking poll. To develop the HPNI, researchers track the top news stories and top health policy news stories on a daily basis over a one-month period to assess which are the top news stories. The top news stories and top health policy news stories are measured separately. In order to gather the top news stories during the month, data is collected daily on the top five news stories as determined by GoogleNews. The top health policy news stories are gathered using the Morning Briefing produced by Kaiser Health News, an editorially independent program of the Foundation. Each weekday during the month, Foundation researchers tally the number of stories appearing in the Morning Briefing from 5 news organizations (TheAssociated Press, The Washington Post, USA Today, TheNew York Times, and TheWall Street Journal). All news and related stories are coded by researchers to reflect the basic type of news story and the subject the story addresses. Those topics that were covered in the largest number of stories are tallied and the most common stories of the month are then included in the HPNI. The number of stories included in the HPNI vary each month depending on the number of stories that have garnered national news attention.
Following the news-tracking period, a question about how closely the public followed each of the stories in the HPNI is included on the monthly Kaiser Health Tracking Poll, a nationally representative dual frame telephone survey (landline and cell phone) of U.S. adults ages 18 and over, conducted in English and Spanish. Each tracking poll interviews a minimum of 1,200 respondents. Detailed methodological information about each month’s poll is available at https://www.kff.org/tag/tracking-poll/.
Endnotes
The U.S. Senate passed the legislation on December 3, 2015 and the House passed the legislation on January 6, 2016. President Obama vetoed the legislation on January 8, 2016. ↩︎
A key provision of the Affordable Care Act (ACA) is the requirement that private insurance plans cover recommended preventive services for women without any patient cost-sharing.1 On December 20, 2016, the Health Resources and Services Administration updated the preventive services for women by accepting the recommendations of the Women’s Preventive Services Initiative, convened by the American College of Obstetricians and Gynecologists (ACOG), and comprised of representatives of national groups with expertise in women’s health. The committee reaffirmed the services for women that were recommended in 2011 and added one new one for mammography.
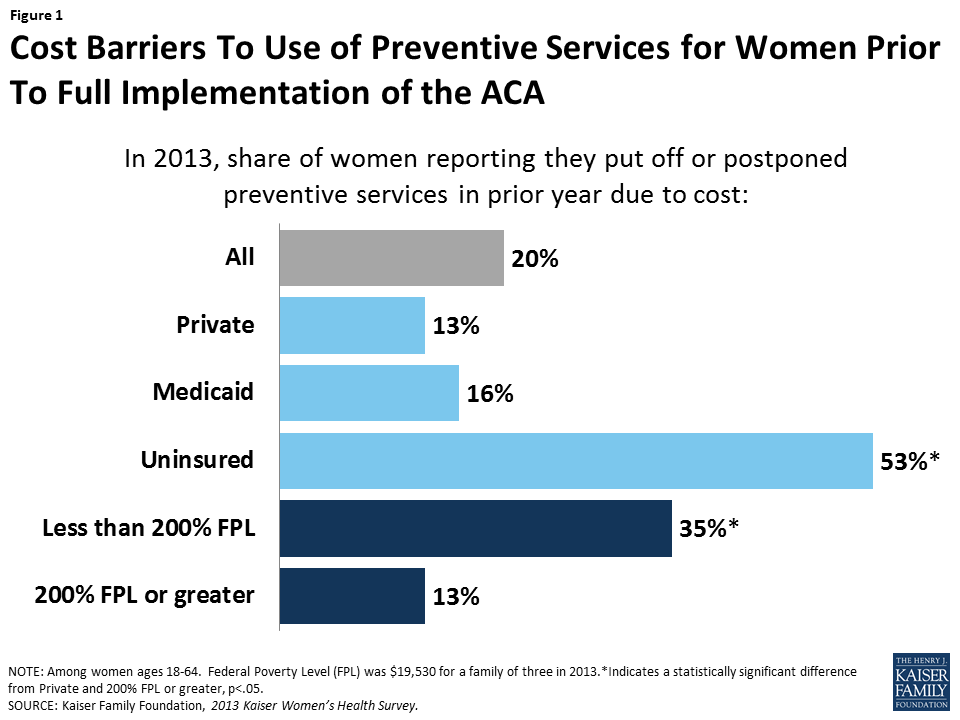
Prior to the ACA’s full implementation, one in five women reported they postponed or went without preventive care because of cost, a much greater barrier for low-income and uninsured women (Figure 1). This factsheet summarizes the ACA preventive services policy’s impact on women, with a focus on the women’s services that are promulgated by HRSA.
Figure 1: Cost Barriers To Use of Preventive Services for Women Prior To Full Implementation of the ACA
ACA Preventive Services That Affect Women
Under Section 2713 of the ACA, private health plans must provide coverage for a range of preventive services for adults and children and may not impose cost-sharing (such as copayments, deductibles, or co-insurance) on patients receiving these services. These requirements apply to most private plans – including individual, small group, large group, and self-insured plans in which employers contract administrative services to a third party. The policy also applies to beneficiaries covered under the ACA’s Medicaid expansion. For children and adolescents, plans must cover the services recommended by the Health Resources and Services Administration’s Bright Futures Project. The required preventive services for adults2 are based on evidence-based recommendations issued by the following three different federal organizations: the United States Preventive Services Task Force (USPSTF), the Centers for Disease Control and Prevention Advisory Committee on Immunization Practices (ACIP), and for women, the Health Resources and Services Administration (HRSA). The preventive services that HRSA requires for women were initially based on recommendations from an expert committee convened by the Institute of Medicine (now the National Academy of Medicine).3 This subset of services for women was just updated by HRSA, and is based on recommendations from the Women’s Preventive Services Initiative (WPSI), a committee convened by ACOG. Table 1 summarizes all of the preventive services affecting women recommended by these three committees that the ACA requires plans to cover without cost sharing.
Table 1: ACA Requires Private Plans to Cover Recommended Preventive Services Free of Cost Sharing for Women
Highlights on the Updated HRSA-Defined Preventive Services for Women
The newly updated services for women from HRSA are designed to identify gaps in services for women that are not recommended by the other expert committees. They include:
Contraceptive coverage
The contraceptive coverage recommendation has been updated. This policy requires that all private plans must cover without cost sharing all 18 distinct prescribed methods used by women (Table 2), as outlined by the Food and Drug Administration (FDA). Insurers may continue to limit coverage in these categories to generic drugs and can impose cost-sharing for equivalent branded drugs. The WPSI reiterates that contraceptive care should include counseling, initiation of contraceptive use, and follow-up care (e.g. management and evaluation as well as changes to and removal or discontinuation of the contraceptive method).
Of all the preventive services, contraception has gained the most attention, with some employers suing the federal government and seeking an exemption from the rule based on the premise that by including contraception in their plans they were being forced to violate their religious beliefs. This litigation reached the US Supreme Court in two cases: Burwell v Hobby Lobby and Zubik v Burwell.4
Table 2: FDA Approved Contraceptive Methods that must be Covered in Private Plans and Medicaid Expansion Programs
The updated HRSA preventive services coverage rules now require that average-risk women be covered for mammography screening. Coverage may begin between ages 40 and 50 and continue through at least age 74, every 1-2 years. HRSA recommends that an individual woman decide on timing and frequency of mammography in consultation with her health care provider. Additionally, the USPSTF recommends that women with family history of breast, ovarian, or peritoneal cancer should be screened for BRCA-related cancer, and those with positive results should receive genetic counseling and genetic testing when appropriate. The USPSTF also recommends that some women with higher risk for breast cancer take prophylactic medications, such as tamoxifen or raloxifene, which must be covered without cost sharing under the ACA.5
Cervical cancer
The HRSA services include cervical cancer screening for women ages 21 to 65. Depending on age and risk, a combination of Pap and HPV testing may be used.
Pregnancy
HRSA recommends screening all pregnant women for gestational diabetes. Prenatal visits are also covered without cost sharing as part of the HRSA recommendation for well woman visits, discussed further below. This is in addition to a number of screening tests recommended by the USPSTF for pregnant women, plus folic acid supplements and substance abuse counseling and cessation (Table 1).
Breastfeeding services and supplies
Both the USPSTF and HRSA recommend breastfeeding education and lactation consultations for pregnant and postpartum women. The HRSA recommendation goes further by recommending coverage without cost sharing for rental of breast pumps and breastfeeding supplies during the antenatal, perinatal, and postpartum periods.
Counseling on Sexually Transmitted Infections (STIs)
HRSA recommends behavioral counseling for women at increased risk for STIs.
Screening for human immunodeficiency virus (HIV)
The HRSA services include HIV counseling, at least one HIV test during a woman’s lifetime and more if needed, for women at higher risk for contracting HIV.
Screening for Interpersonal and Domestic Violence
The committee recommends that providers screen adolescents and women for violence and provide or refer to interventional services when needed. This can include counseling, education, and other support services.
Well-woman visits
The HRSA services for women include coverage for at least one annual well-woman visit that women can use to obtain all of the preventive services that are recommended, including prenatal care. They note that for some women, more than one visit may be needed to cover all the preventive and counseling services they need.
Conclusion
A repeal of the ACA as proposed by President-elect Trump would end the requirement that recommended preventive services be covered by private plans without cost sharing, unless this provision is included as part of replacement legislation. The specific preventive services for women that were updated and promulgated by HRSA, however, could also be eliminated or scaled back by administrative action, without the need for Congressional action because HRSA can accept or reject any of the women’s services recommended by the WPSI.
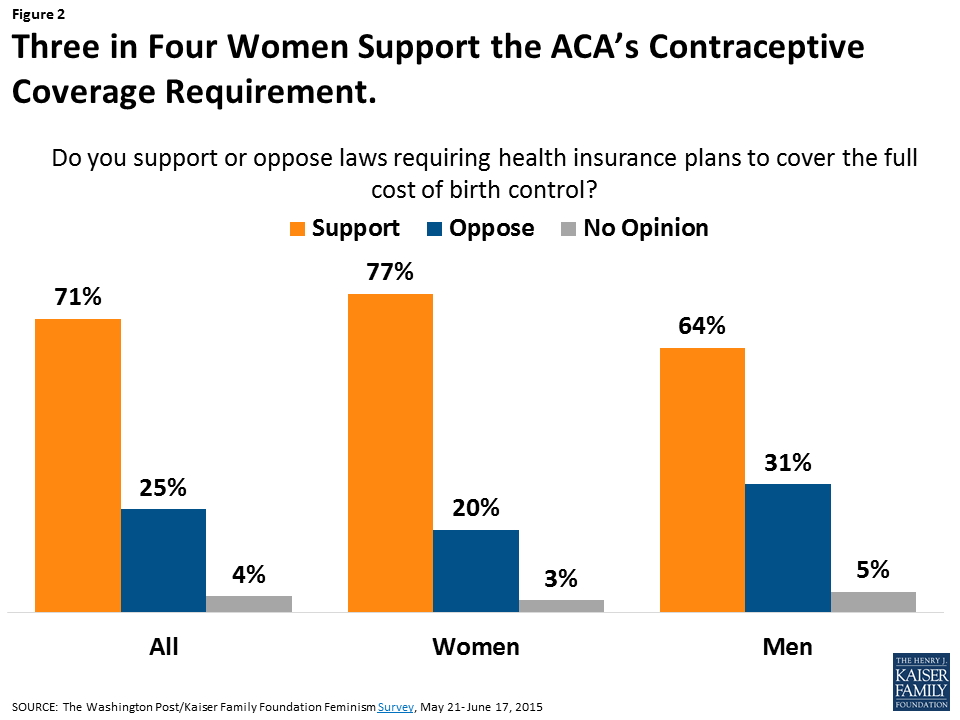
As the Trump administration transitions to the White House, it remains to be seen how or whether the new administration and 115th Congress will specifically address preventive services for women more broadly. The administration and Congress, however, have signaled that they will address the accommodation for employers claiming religious objections to the contraceptive coverage provision.6 Although the contraceptive coverage provision has been controversial among certain employers, among the public, and especially among women, there has been widespread support for the requirement (Figure2). Research has also documented that women’s out-pocket-spending on contraceptives has dropped significantly as a result of the law.7 Given that more than 90% of women use contraceptives at some point in their lives,8 this is a benefit that affects millions of women.
Figure 2: Three in Four Women Support the ACA’s Contraceptive Coverage Requirement.
The 2010 Affordable Care Act (ACA) included many provisions affecting the Medicare program and the 57 million seniors and people with disabilities who rely on Medicare for their health insurance coverage. Such provisions include reductions in the growth in Medicare payments to hospitals and other health care providers and to Medicare Advantage plans, benefit improvements, payment and delivery system reforms, higher premiums for higher-income beneficiaries, and new revenues.
President-elect Donald Trump, Speaker of the House Paul Ryan, Health and Human Services (HHS) Secretary-nominee and current House Budget Committee Chairman Tom Price, and many other Republicans in Congress have proposed to repeal and replace the ACA, but lawmakers have taken different approaches to the ACA’s Medicare provisions. For example, the House Budget Resolution for Fiscal Year 2017, introduced by Chairman Price in March 2016, proposed a full repeal of the ACA. The House Republican plan, “A Better Way,” introduced by Speaker Ryan in June 2016, proposed to repeal some, but not all, of the ACA’s Medicare provisions.
This brief explores the implications for Medicare and beneficiaries of repealing Medicare provisions in the ACA. The Congressional Budget Office (CBO) has estimated that full repeal of the ACA would increase Medicare spending by $802 billion from 2016 to 2025.1 Full repeal would increase spending primarily by restoring higher payments to health care providers and Medicare Advantage plans. The increase in Medicare spending would likely lead to higher Medicare premiums, deductibles, and cost sharing for beneficiaries, and accelerate the insolvency of the Medicare Part A trust fund. Policymakers will confront decisions about the Medicare provisions in the ACA in their efforts to repeal and replace the law.
What are the key Medicare provisions in the ACA and how would repeal affect Medicare spending and beneficiaries?
The following discussion highlights several of the key Medicare provisions in the ACA and assesses how repeal of these provisions could affect Medicare spending and beneficiaries.2
Payments to Health Care Providers
The ACA reduced updates in Medicare payment levels to hospitals, skilled nursing facilities, hospice and home health providers, and other health care providers. The ACA also reduced Medicare Disproportionate Share Hospital (DSH) payments that help to compensate hospitals for providing care to low-income and uninsured patients, with the expectation that hospitals would have fewer uninsured patients as a result of the ACA’s coverage expansions.
Repealing the ACA’s sustained reductions in provider payments would be expected to:
Increase Part A and Part B spending. CBO has estimated that roughly $350 billion3 of the total $802 billion in higher Medicare spending over 10 years could result from repealing ACA provisions that changed provider payment rates in traditional Medicare. Repealing these provisions would increase payments to providers in traditional Medicare. Additionally, some hospitals would receive higher DSH payments, if these payments were restored to their pre-ACA levels.
Increase the Part A deductible and copayments and the Part B premium and deductible paid by beneficiaries. The Part A deductible and copayments would be expected to increase due to an increase in Part A spending that would likely occur if payment reductions are repealed. This is because the Part A deductible for inpatient hospital stays is indexed to updates in hospital payments, and the copayment amounts for inpatient hospital and skilled nursing facility stays are calculated as a percentage of the Part A deductible. Similarly, the Part B premium and deductible would be expected to increase if payments to Part B service providers are restored. This is because Part B premiums are set to cover 25 percent of Part B spending, and the Part B deductible is indexed to rise at the same rate as the Part B premium.
Payments to Medicare Advantage Plans
Prior to the ACA, federal payments to Medicare Advantage plans per enrollee were 14 percent higher than the cost of covering similar beneficiaries under the traditional Medicare program, according to the Medicare Payment Advisory Commission (MedPAC).4 The ACA reduced payments to Medicare Advantage plans over six years, which brought these payments closer to the average costs of care under the traditional Medicare program. In 2016, federal payments to plans were 2 percent higher than traditional Medicare spending (including quality-based bonus payments to plans).5
Repealing the ACA’s Medicare Advantage payment changes would be expected to:
Increase total Medicare spending as a result of increasing payments to Medicare Advantage plans relative to spending under traditional Medicare. CBO has estimated that repealing the Medicare Advantage-related provisions in the ACA would increase Medicare spending by roughly $350 billion6 (out of the $802 billion total increase) over 10 years.
Increase the Part B premium and deductible paid by beneficiaries. The Part B premium and deductible would likely increase if the payment reductions for Medicare Advantage plans are repealed because the Part B premium is set to cover 25 percent of Part B spending, and the Part B deductible is indexed to rise at the same rate as the Part B premium.
Improve benefits and lower out-of-pocket costs for beneficiaries enrolled in Medicare Advantage plans. Payments that Medicare Advantage plans receive in excess of their costs to provide Part A and Part B benefits are required to be used to provide benefits not covered by traditional Medicare, to reduce cost sharing, premiums, or limits on out-of-pocket spending, or both. Thus, if the ACA’s reductions in Medicare Advantage plan payments were repealed, plans could provide extra benefits to Medicare Advantage enrollees and/or reduce enrollees’ costs.
Medicare Benefit Improvements
The ACA included provisions to improve Medicare benefits by providing free coverage for some preventive benefits, such as screenings for breast and colorectal cancer, cardiovascular disease, and diabetes, and closing the coverage gap (or “doughnut hole”) in the Part D drug benefit by 2020. These benefit improvements increased Medicare Part B and Part D spending.
Repealing the ACA’s Medicare benefit improvements would be expected to:
Reduce Medicare Part B spending for preventive services and reduce Part D spending on costs in the coverage gap.
Increase beneficiary cost sharing for Part B preventive benefits.
Increase beneficiary cost sharing by Part D enrollees who have drug spending high enough to reach the coverage gap. According to MedPAC, in 2013, roughly 25 percent of the 37.8 million Part D enrollees (or around 9 million beneficiaries) had drug spending high enough to reach the coverage gap.7 ,8
Reduce Part D premiums, on average, since Part D premiums are set to cover 25.5 percent of program costs, and reinstating the Part D coverage gap would lower Part D spending.
Revenues to the Medicare Trust Funds
The ACA established new sources of revenue dedicated to the Medicare program, including a 0.9 percentage point increase in the Medicare Part A payroll tax on earnings of higher-income workers (incomes more than $200,000/individual and $250,000/couple), and a fee on the manufacturers and importers of branded drugs, which has generated additional revenue for the Part B trust fund, including $3 billion in 2015 alone.9
Repealing the ACA’s Medicare revenue provisions would be expected to:
Reduce revenues to Medicare’s Part A and Part B trust funds.
Reduce Part A payroll taxes for Medicare beneficiaries (and other taxpayers) with earnings greater than $200,000/individual or $250,000/couple.
Medicare Part B and Part D Premiums for Higher-Income Beneficiaries
The ACA froze the income thresholds for the Part B income-related premium beginning at $85,000/individual and $170,000/couple through 2019, which subjected a larger share of Medicare beneficiaries to the higher Part B income-related premium over time.10 The law also added a new surcharge to Part D premiums for higher-income enrollees, using the same income thresholds as Part B premiums.
Repealing the ACA’s income-related premium provisions would be expected to:
Reduce the number of higher-income Part B enrollees paying income-related premiums.
Reduce Part D premiums for beneficiaries with incomes above $85,000/individual and $170,000/couple.
Payment and Delivery System Reforms and New Quality Incentives
Through a new Center for Medicare & Medicaid Innovation (CMMI, or Innovation Center) within the Centers for Medicare & Medicaid Services (CMS), the ACA directed CMS to test and implement new approaches for Medicare to pay doctors, hospitals, and other providers to bring about changes in how providers organize and deliver care. The ACA authorized the Secretary of Health and Human Services to expand CMMI models into Medicare if evaluation results showed that they either reduced spending without harming the quality of care or improved the quality of care without increasing spending. CMMI received an initial appropriation of $10 billion in 2010 for payment and delivery system reform model development and evaluation, and the ACA called for additional appropriations of $10 billion in each decade beginning in 2020.
The ACA also created incentives for hospitals to reduce preventable readmissions and hospital-acquired conditions, and established new accountable care organizations (ACO) programs. Research has shown declines in Medicare patient readmissions since the Hospital Readmission Penalty Program provisions were introduced.
Repealing these ACA’s payment and delivery system reform provisions would be expected to:
Increase Medicare spending due to elimination of CMMI and other quality incentive programs. On net, CBO has estimated that CMMI’s operations will generate savings of $34 billion over the 2017-2026 period, with gross savings of $45 billion over this period. These savings are attributed to the expansion of successful payment and delivery system reform models into Medicare. In addition to eliminating the savings generated from CMMI, Medicare spending could also increase if the incentives to reduce preventable readmissions and hospital-acquired conditions are included in proposals to repeal and replace the ACA.
Independent Payment Advisory Board
The ACA authorized a new Independent Payment Advisory Board (IPAB), a 15-member board that is required to recommend Medicare spending reductions to Congress if projected spending growth exceeds specified target levels, with the recommendations taking effect according to a process outlined in the ACA. To date, no members have been appointed to the Board. Many policymakers have expressed opposition to IPAB, and there have been several legislative attempts to eliminate it. The CMS Office of the Actuary has estimated that the IPAB process will first be triggered in 2017, based on its most recent Medicare spending growth rate projections.11
Repealing IPAB would be expected to:
Increase Medicare spending over time, in the absence of the Board’s cost-reducing actions. CBO projects Medicare savings of $8 billion as a result of the IPAB process between 2019 and 2026.12
How would ACA repeal affect the solvency of the Medicare Hospital Insurance trust fund?
Fully repealing the ACA would accelerate the projected insolvency of the Medicare Hospital Insurance (HI) trust fund, out of which Part A benefits are paid. This would result from higher spending for Part A services due to higher payments to Part A service providers (such as hospitals) and Medicare Advantage plans for services provided under Part A, along with reduced revenues, if the additional 0.9 percent payroll tax on high earners is repealed. As a result, Medicare would not be able to fulfill its obligation to pay for all Part A-covered benefits within a shorter period of time if the ACA is repealed than if the law is retained.
Prior to enactment of the ACA in 2010, the Medicare Trustees projected that the Part A trust fund would not have sufficient funds to pay all Part A benefits beginning in 2017. Following enactment of the law, the insolvency date was extended. The current insolvency date is projected to be 2028. Repealing the ACA is expected to push up the insolvency date.
Discussion
The Medicare provisions of the ACA have played an important role in strengthening Medicare’s financial status for the future, while offsetting some of the cost of the coverage expansions of the ACA and also providing some additional benefits to people with Medicare. Savings were achieved in part by reducing payments to providers, such as hospitals and skilled nursing facilities. Medicare provider payment changes in the ACA were adopted in conjunction with the ACA’s insurance coverage expansions, with the expectation that additional revenue from newly-insured Americans would offset lower revenue from Medicare payments. In addition, Medicare savings were achieved through lower payments to Medicare Advantage plans.
Congressional action to repeal the ACA appears imminent, but it is not yet clear whether Congress will repeal the ACA in its entirety or keep certain provisions in place. Previous Congressional proposals have taken different approaches. For example, the House Budget Resolution for Fiscal Year 2017, introduced by Chairman Price in March 2016, proposed a full repeal of the ACA. The House Republican plan, “A Better Way,” introduced by Speaker Ryan in June 2016, proposed to repeal some of the ACA’s Medicare Advantage payment changes, along with repealing IPAB and CMMI, the additional Medicare payroll tax on high earners, and certain other tax and revenue provisions, but appears to retain other Medicare provisions, including changes to provider payment updates and the benefit improvements.13
A majority of Americans have expressed support for some of the ACA provisions that affect Medicare, including the elimination of out-of-pocket costs for many preventive services, closing the Part D coverage gap, and the higher Medicare payroll tax for higher-income workers.14 Some industry stakeholders have expressed concern about the implications of retaining the ACA’s savings provisions, yet repealing the ACA’s coverage expansions.
Aside from uncertainty about whether any of the ACA’s Medicare provisions will be retained, questions have arisen as to what changes policymakers could advance through the legislative process known as “reconciliation.” Policymakers are considering repealing the ACA as part of budget reconciliation legislation, which requires only a simple majority in the Senate to pass. Senate rules (the so-called “Byrd Rule”) limit the scope of reconciliation legislation to provisions with budgetary effects, including spending and revenues. Most of the Medicare provisions in the ACA have budgetary effects, according to CBO, so would likely be considered in order in the context of a reconciliation bill.
As a result of the Medicare provisions included in the ACA, Medicare spending per beneficiary has grown more slowly than private health insurance spending; premiums and cost-sharing for many Medicare-covered services are lower than they would have been without the ACA; new payment and delivery system reforms are being developed and tested; and the Medicare Part A trust fund has gained additional years of solvency. Full repeal of the Medicare provisions in the ACA would increase payments to hospitals and other health care providers and Medicare Advantage plans, which would likely lead to higher premiums, deductibles, and cost sharing for Medicare-covered services paid by people with Medicare. Full repeal would also reduce premiums for higher-income beneficiaries, and reduce payroll tax contributions from beneficiaries (and other taxpayers) with high earnings. Repealing the ACA would have uncertain effects on evolving payment and delivery system reforms. Partial repeal of the law could also have implications for Medicare spending, the Part A trust fund solvency date, and beneficiaries’ costs. Policymakers who seek to repeal the ACA may need to address the implications for Medicare, beneficiaries, and other stakeholders.
Endnotes
Congressional Budget Office, “Budgetary and Economic Effects of Repealing the Affordable Care Act,” June 2015, available at https://www.cbo.gov/publication/50252. ↩︎
This discussion does not include the ACA provision to eliminate the tax deductibility of the 28 percent federal subsidy, known as the retiree drug subsidy (RDS), for employers who provide creditable prescription drug coverage to Medicare beneficiaries. Repealing this provision would not have a direct effect on Medicare spending but, in allowing for the tax deductibility of RDS payments, would be accounted for as a federal tax expenditure. ↩︎
This $350 billion estimate is calculated from CBO’s statement that roughly one-half of the net increase in direct spending ($715 billion, between 2016 and 2025) would stem from repealing provisions that changed payment rates in the fee-for service sector. Congressional Budget Office, “Budgetary and Economic Effects of Repealing the Affordable Care Act,” June 2015, available at https://www.cbo.gov/publication/50252. ↩︎
This $350 billion estimate is calculated from CBO’s statement that roughly one-half of the net increase in direct spending ($715 billion, between 2016 and 2025) would stem from repealing provisions that changed the rules for setting payment rates for Medicare Advantage plans. Congressional Budget Office, “Budgetary and Economic Effects of Repealing the Affordable Care Act,” June 2015, available at https://www.cbo.gov/publication/50252. ↩︎
According to CMS estimates, more than 11 million Medicare Part D enrollees have received a total of $23.5 billion in savings and discounts in the coverage gap since the enactment of the ACA, with savings averaging $2,127 per enrollee over five years. See Centers for Medicare & Medicaid Services, “Medicare Advantage Premiums Remain Stable in 2017; Beneficiaries Have Saved over $23.5 Billion on Prescription Drugs,” September 22, 2016, available at https://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2016-Press-releases-items/2016-09-22.html. ↩︎
The Part B income-related premium was established by the Medicare Modernization Act of 2003 and took effect in 2007. The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) made further changes to Medicare’s income-related premiums requiring beneficiaries with incomes above $133,500 ($267,000 for married couples) to pay a larger percentage of Part B and Part D program costs than they currently pay, beginning in 2018. MACRA also included a provision to index the thresholds to inflation based on their levels in 2019. ↩︎
As Republican policymakers consider how to repeal and replace the Affordable Care Act (ACA), they are likely to face a number of decisions about whether to retain any of the law’s changes to Medicare. Repealing the ACA has potential implications for Medicare spending, beneficiaries, and other stakeholders, according to a new Kaiser Family Foundation brief.
A full repeal of the ACA would undo all of the law’s changes to Medicare and would increase Medicare spending, primarily by restoring higher payments to health care providers and Medicare Advantage plans. The increase in Medicare spending would likely lead to higher Medicare premiums, deductibles, and cost sharing for beneficiaries, and accelerate the insolvency of the Medicare Part A trust fund. It also would eliminate coverage in the “doughnut hole” of the Medicare Part D drug benefit, a coverage gap that is closing by 2020 under the ACA.
Full repeal of the Medicare provisions in the ACA would increase Medicare spending by $802 billion from 2016 to 2025, according to the Congressional Budget Office.
Ever since the Affordable Care Act became law, critics have warned that it would cause a “death spiral” in the individual health insurance market. Those fears were unfounded, but if Republicans in Congress repeal the ACA without immediately replacing it, they might just cause one.
The ACA prohibits insurers from denying access to coverage based on pre-existing conditions and also prohibits them from charging different premiums to individuals based on their health. Everyone is in one big insurance pool, sharing in the average cost. Critics worry that in such a system, people who are sick buy coverage because they know they need it, but healthy people hold out, raising the average cost of doing business for insurers and leading them to raise premiums on everyone. That, in turn, could cause yet more healthy people to drop insurance because they no longer see it as a good value, again requiring insurers to increase premiums, and so on, resulting in a death spiral.
To prevent this from happening, the ACA encourages healthy people to get insurance through a carrot (premium subsidies for low- and middle-income people) and a stick (the so-called individual mandate, which generally requires people to be insured or pay a penalty).
It hasn’t worked out perfectly, with more sick people enrolled than insurers expected when they initially set their premiums in 2014. That’s a big reason why premiums are rising more quickly for 2017 — with benchmarks increasing 22% on average nationally and 8% in California. Some insurers have exited the market, and Obamacare consumers face fewer choices. But the hope is that these higher premiums represent a one-time market correction rather than a sign of worsening trends to come.
Of course, the election of Donald Trump and continued Republican control of Congress have put the future of the ACA itself in doubt. Republicans have consistently promised to repeal and replace the health law, and they now have the ability to fulfill that promise — though, according to recent news reports, they will seek to repeal the law before they figure out how to replace it.
Judging from the GOP’s strategy during the Obama administration (when it was understood that the president would veto any legislation that hurt his signature law), Republicans may use a budget maneuver known as a reconciliation bill to repeal major parts of the ACA. The advantage of such a bill is that it cannot be filibustered in the Senate, meaning it can be passed with 51 votes instead of 60. The disadvantage is that it can be used only to make changes that have a direct effect on federal spending or taxes. So, for example, a reconciliation bill cannot repeal the ACA’s insurance market regulations, including protections for people with pre-existing conditions. But it can repeal the law’s premium subsidies and the individual mandate.
If that’s what GOP lawmakers decide to do — as many informed observers suspect they will — there’s a high likelihood that they would, in fact, produce a death spiral. With guaranteed insurance for people with pre-existing conditions but no subsidies or individual mandate, premiums could skyrocket. Or, more likely, insurers simply would exit the market. Why risk losses when the whole law is getting repealed anyway? The upshot would be canceled coverage with no other options for people buying in the ACA’s marketplaces (like healthcare.gov or Covered California), as well as those buying directly from insurers, where the same rules apply.
Even if the GOP eliminates only the individual mandate — while leaving other aspects of the ACA in place for a period of time — this could happen very quickly.
But there are ways to avoid this potential chaos.
One approach would be to hold off on voting to repeal the ACA until the Republicans settle on a replacement. That could put Republicans in a difficult position because they have promised to repeal the ACA quickly and have not yet reached consensus on an alternative.
Another approach would be to leave the individual mandate in place and extend temporary mechanisms included in the ACA to stabilize the insurance market, providing subsidies to insurance companies that enroll high-cost patients and those that experience financial losses. This approach, too, poses political challenges because Republicans strongly oppose the individual mandate and some have opposed the ACA’s stabilization mechanisms as a “bailout” of insurers.
President-elect Trump said recently that he wanted to keep the ACA’s prohibition against denying coverage for people with pre-existing conditions. It’s understandable that Republicans would want to keep the popular stuff in the ACA while getting rid of the unpopular stuff (the individual mandate and increased taxes). Unfortunately, there’s no magic pixie dust to make that easy or avoid difficult trade-offs.
A new Kaiser Family Foundation analysis finds that 52 million adults under 65 – or 27 percent of that population — have pre-existing health conditions that would likely make them uninsurable if they applied for health coverage under medical underwriting practices that existed in most states before insurance regulation changes made by the Affordable Care Act.
In eleven states, at least three in ten non-elderly adults would have a declinable condition, according to the analysis: West Virginia (36%), Mississippi (34%), Kentucky (33%), Alabama (33%), Arkansas (32%), Tennessee (32%), Oklahoma (31%), Louisiana (30%), Missouri (30%), Indiana (30%) and Kansas (30%).
States with the most people estimated to have the conditions include: California (5,865,000), Texas (4,536,000), and Florida (3,116,000).
Using data from two large government surveys, the analysis estimates the total number of nonelderly adults in each state with a health condition that could lead to a denial of coverage in the individual insurance market, based on pre-ACA field underwriting guides for brokers and agents. The results are conservative because the data don’t include some declinable conditions. The estimates also don’t include the number of people with other health conditions that wouldn’t necessarily cause a denial, but could lead to higher insurance costs based on underwriting.
While most people with pre-existing health conditions have coverage through an employer or public program, such as Medicaid, they may intermittently seek insurance in the individual market during times when they’re ineligible for other coverage, such as following a job loss or divorce. People who are self-employed, early retirees, or lower-wage workers in jobs that don’t provide health benefits often are covered by individual plans for longer periods.
Before ACA protections took effect in 2014, private insurers in the individual health insurance market could use applicants’ health status, health history and other risk factors to determine whether and under what terms to issue coverage. Some examples of conditions which could have led to automatic denial of coverage include cancer, diabetes, epilepsy, heart disease, and pregnancy.
In the post-election health policy debate, both political parties have expressed a desire to continue protecting people with pre-existing conditions.
UPDATE: An updated version of this analysis based on 2018 data is now available. It includes estimates for non-elderly adults and households, with some breakouts by state, age and gender.
Before private insurance market rules in the Affordable Care Act (ACA) took effect in 2014, health insurance sold in the individual market in most states was medically underwritten.1 That means insurers evaluated the health status, health history, and other risk factors of applicants to determine whether and under what terms to issue coverage. To what extent people with pre-existing health conditions are protected is likely to be a central issue in the debate over repealing and replacing the ACA.
This brief reviews medical underwriting practices by private insurers in the individual health insurance market prior to 2014, and estimates how many American adults could face difficulty obtaining private individual market insurance if the ACA were repealed or amended and such practices resumed. We examine data from two large government surveys: The National Health Interview Survey (NHIS) and the Behavioral Risk Factor Surveillance System (BRFSS), both of which can be used to estimate rates of various health conditions (NHIS at the national level and BRFSS at the state level). We consulted field underwriting manuals used in the individual market prior to passage of the ACA as a reference for commonly declinable conditions.
Estimates of the Share of Adults with Pre-Existing Conditions
We estimate that 27% of adult Americans under the age of 65 have health conditions that would likely leave them uninsurable if they applied for individual market coverage under pre-ACA underwriting practices that existed in nearly all states. While a large share of this group has coverage through an employer or public coverage where they do not face medical underwriting, these estimates quantify how many people could be ineligible for individual market insurance under pre-ACA practices if they were to ever lose this coverage. This is a conservative estimate as these surveys do not include sufficient detail on several conditions that would have been declinable before the ACA (such as HIV/AIDS, or hepatitis C). Additionally, millions more have other conditions that could be either declinable by some insurers based on their pre-ACA underwriting guidelines or grounds for higher premiums, exclusions, or limitations under pre-ACA underwriting practices. In a separate Kaiser Family Foundation poll, most people (53%) report that they or someone in their household has a pre-existing condition.
A larger share of nonelderly women (30%) than men (24%) have declinable preexisting conditions. We estimate that 22.8 million nonelderly men have a preexisting condition that would have left them uninsurable in the individual market pre-ACA, compared to 29.4 million women. Pregnancy explains part, but not all of the difference.
The rates of declinable pre-existing conditions vary from state to state. On the low end, in Colorado and Minnesota, at least 22% of non-elderly adults have conditions that would likely be declinable if they were to seek coverage in the individual market under pre-ACA underwriting practices. Rates are higher in other states – particularly in the South – such as Tennessee (32%), Arkansas (32%), Alabama (33%), Kentucky (33%), Mississippi (34%), and West Virginia (36%), where at least a third of the non-elderly population would have declinable conditions.
Table 1: Estimated Number and Percent of Non-Elderly People with Declinable Pre-existing Conditions Under Pre-ACA Practices, 2015
State
Percent of Non-Elderly Population
Number of Non-Elderly Adults
Alabama
33%
942,000
Alaska
23%
107,000
Arizona
26%
1,043,000
Arkansas
32%
556,000
California
24%
5,865,000
Colorado
22%
753,000
Connecticut
24%
522,000
Delaware
29%
163,000
District of Columbia
23%
106,000
Florida
26%
3,116,000
Georgia
29%
1,791,000
Hawaii
24%
209,000
Idaho
25%
238,000
Illinois
26%
2,038,000
Indiana
30%
1,175,000
Iowa
24%
448,000
Kansas
30%
504,000
Kentucky
33%
881,000
Louisiana
30%
849,000
Maine
29%
229,000
Maryland
26%
975,000
Massachusetts
24%
999,000
Michigan
28%
1,687,000
Minnesota
22%
744,000
Mississippi
34%
595,000
Missouri
30%
1,090,000
Montana
25%
152,000
Nebraska
25%
275,000
Nevada
25%
439,000
New Hampshire
24%
201,000
New Jersey
23%
1,234,000
New Mexico
27%
332,000
New York
25%
3,031,000
North Carolina
27%
1,658,000
North Dakota
24%
111,000
Ohio
28%
1,919,000
Oklahoma
31%
706,000
Oregon
27%
654,000
Pennsylvania
27%
2,045,000
Rhode Island
25%
164,000
South Carolina
28%
822,000
South Dakota
25%
126,000
Tennessee
32%
1,265,000
Texas
27%
4,536,000
Utah
23%
391,000
Vermont
25%
96,000
Virginia
26%
1,344,000
Washington
25%
1,095,000
West Virginia
36%
392,000
Wisconsin
25%
852,000
Wyoming
27%
94,000
US
27%
52,240,000
SOURCE: Kaiser Family Foundation analysis of data from National Health Interview Survey and the Behavioral Risk Factor Surveillance System.NOTE: Five states (MA, ME, NJ, NY, VT) had broadly applicable guaranteed access to insurance before the ACA. What protections might exist in these or other states under a repeal and replace scenario is unclear.
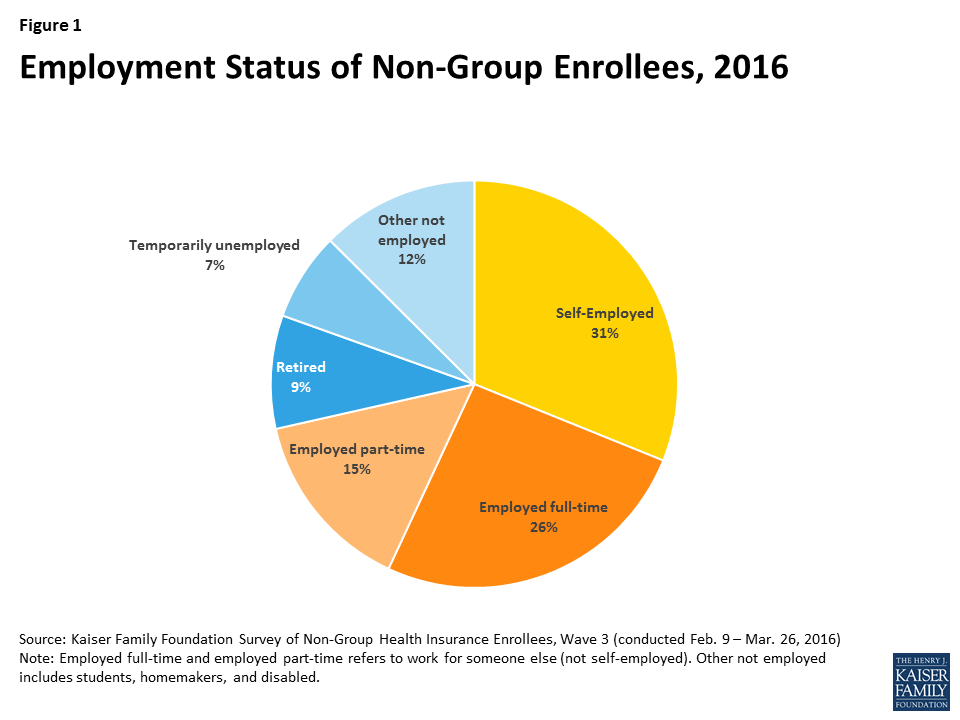
At any given time, the vast majority of these approximately 52 million people with declinable pre-existing conditions have coverage through an employer or through public programs like Medicaid. The individual market is where people seek health insurance during times in their lives when they lack eligibility for job-based coverage or for public programs such as Medicare and Medicaid. In 2015, about 8% of the non-elderly population had individual market insurance. Over a several-year period, however, a much larger share may seek individual market coverage.2 This market is characterized by churn, as new enrollees join and others leave (often for other forms of coverage). For many people, the need for individual market coverage is intermittent, for example, following a 26th birthday, job loss, or divorce that ends eligibility for group plan coverage, until they again become eligible for group or public coverage. For others – the self-employed, early retirees, and lower-wage workers in jobs that typically don’t come with health benefits – the need for individual market coverage is ongoing. (Figure 1 shows the distribution of employment status among current individual market enrollees.)
Prior to the ACA’s coverage expansions, we estimated that 18% of individual market applications were denied. This is an underestimate of the impact of medical underwriting because many people with health conditions did not apply because they knew or were informed by an agent that they would not be accepted. Denial rates ranged from 0% in a handful of states with guaranteed issue to 33% in Kentucky, North Carolina, and Ohio. According to 2008 data from America’s Health Insurance Plans, denial rates ranged from about 5% for children to 29% for adults age 60-64 (again, not accounting for those who did not apply).
Figure 1: Employment Status of Non-Group Enrollees, 2016
Medical Underwriting in the Individual Market Pre-ACA
Prior to 2014 medical underwriting was permitted in the individual insurance market in 45 states and DC. Applications for individual market policies typically included lengthy questionnaires about the health and risk status of the applicant and all family members to be covered. Typically, applicants were asked to disclose whether they were pregnant or contemplating pregnancy or adoption, and information about all physician visits, prescription medications, lab results, and other medical care received in the past year. In addition, applications asked about personal history of a series of health conditions, ranging from HIV, cancer, and heart disease to hemorrhoids, ear infections and tonsillitis. Finally, all applications included authorization for the insurer to obtain and review all medical records, pharmacy database information, and related information.
Once the completed application was submitted, the medical underwriting process varied somewhat across insurers, but usually involved identification of declinable medical conditions and evaluation of other conditions or risk factors that warranted other adverse underwriting actions. Once enrolled, a person’s health and risk status was sometimes reconsidered in a process called post-claims underwriting. Although our analysis focuses on declinable medication conditions, each of these other actions is described in more detail below.
Declinable Medical Conditions
Before the ACA, individual market insurers in all but five states maintained lists of so-called declinable medical conditions. People with a current or past diagnosis of one or more listed conditions were automatically denied. Insurer lists varied somewhat from company to company, though with substantial overlap. Some of the commonly listed conditions are shown in Table 2.
Table 2: Examples of Declinable Conditions In the Medically Underwritten Individual Market, Before the Affordable Care Act
Condition
Condition
AIDS/HIV
Lupus
Alcohol abuse/ Drug abuse with recent treatment
Mental disorders (severe, e.g. bipolar, eating disorder)
Alzheimer’s/dementia
Multiple sclerosis
Arthritis (rheumatoid), fibromyalgia, other inflammatory joint disease
Muscular dystrophy
Cancer within some period of time (e.g. 10 years, often other than basal skin cancer)
SOURCE: Kaiser Family Foundation review of field underwriting guidelines from Aetna (GA, PA, and TX), Anthem BCBS (IN, KY, and OH), Assurant, CIGNA, Coventry, Dean Health, Golden Rule, Health Care Services Corporation (BCBS in IL, TX) HealthNet, Humana, United HealthCare, Wisconsin Physician Service. Conditions in this table appeared on declinable conditions list in half or more of guides reviewed. NOTE: Many additional, less-common disorders also appearing on most of the declinable conditions lists were omitted from this table.
Our analysis of rates of pre-existing conditions in this brief focuses on those conditions that would likely be declinable, based on our review of pre-ACA underwriting documents. Our analysis is limited – and our results are conservative – because NHIS and BRFSS questionnaires do not address some of the conditions that were declinable, and in some cases the questions that do relate to declinable conditions were too broad for inclusion. See the methodology section for a list of conditions included in the analysis.
In addition to declinable conditions, many insurers also maintained a list of declinable medications. Current use of any of these medications by an applicant would warrant denial of coverage. Table 3 provides an example of medications that were declinable in one insurer prior to the ACA. Our analysis does not attempt to account for use of declinable medications.
Table 3: Declinable Medications
Anti-Arthritic Medications
Adalimumab/Humira
Cyclosporine/Sandimmune
Methotrexate/Trexall
Ustekinumab/Stelara
others
Anti-Diabetic Medications
Avandia/Rosiglitazone
Glucagon
Humalog/Insulin products
Metformin HCL
others
Medications for HIV/AIDS or Hepatitis
Abacavir/Ziagen
Efavirenz/Atripla
Interferon
Lamivudine/Epivir
Ribavirin
Zidovudine/Retrovir
others
Anti-Cancer Medications
Anastrozole/Arimidex
Nolvadex/Tamoxifen
Femara
others
Anti-Psychotics, Autism, Other Central Nervous System Medications
Abilify/Ariprazole
Aricept/Donepezil
Clozapine/Clozaril
Haldol/Haldoperidol
Lithium
Requip/Ropinerole
Risperdal/Risperidone
Zyprexa
others
Anti-Coagulant/Anti-Thrombotic Medications
Clopidogrel/Plavix
Coumadin/Warfarin
Heparin
others
Miscellaneous Medications
Anginine (angina)
Clomid (fertility)
Epoetin/Epogen (anemia)
Genotropin (growth hormone)
Remicade (arthritis, ulcerative colitis)
Xyrem (narcolepsy)
others
SOURCE: Blue Cross Blue Shield of Illinois, Product Guide for Agents
Some individual market insurers also developed lists of ineligible occupations. These were jobs considered sufficiently high risk that people so employed would be automatically denied. In addition, some would automatically deny applicants who engaged in certain leisure activities and sports. Table 4 provides an example of declinable occupations from one insurer prior to the ACA. Our analysis does not attempt to account for declinable occupations.
Table 4: Ineligible Occupations, Activities
Active military personnel
Iron workers
Professional athletes
Air traffic controller
Law enforcement/detectives
Sawmill operators
Aviation and air transportation
Loggers
Scuba divers
Blasters or explosive handlers
Meat packers/processors
Security guards
Bodyguards
Mining
Steel metal workers
Crop dusters
Nuclear industry workers
Steeplejacks
Firefighters/EMTs
Offshore drillers/workers
Strong man competitors
Hang gliding
Oil and gas exploration and drilling
Taxi cab drivers
Hazardous material handlers
Pilots
Window washers
SOURCE: Preferred One Insurance Company Individual and Family Insurance Application Form
Other Adverse Underwriting Actions
Beyond the declinable conditions, medications and occupations, underwriters also examined individual applications and medical records for other conditions that could generate significant “losses” (claims expenses.) Among such conditions were acne, allergies, anxiety, asthma, basal cell skin cancer, depression, ear infections, fractures, high cholesterol, hypertension, incontinence, joint injuries, kidney stones, menstrual irregularities, migraine headaches, overweight, restless leg syndrome, tonsillitis, urinary tract infections, varicose veins, and vertigo. One or more adverse medical underwriting actions could result for applicants with such conditions, including:
Rate-up – The applicant might be offered a policy with a surcharged premium (e.g. 150 percent of the standard rate premium that would be offered to someone in perfect health)
Exclusion rider – Coverage for treatment of the specified condition might be excluded under the policy; alternatively, the body part or system affected by the specified condition could be excluded under the policy. Exclusion riders might be temporary (for a period of years) or permanent
Increased deductible – The applicant might be offered a policy with a higher deductible than the one originally sought; the higher deductible might apply to all covered benefits or a condition-specific deductible might be applied
Modified benefits – The applicant might be offered a policy with certain benefits limited or excluded, for example, a policy that does not include prescription drug coverage.
In some cases, individuals with these conditions might also be declined depending on their health history and the insurer’s general underwriting approach. For example, field underwriting guides indicated different underwriting approaches for an applicant whose child had chronic ear infections:
One large, national insurer would issue standard coverage if the child had fewer than five infections in the past year or ear tubes, but apply a 50% rate up if there had been more than 4 infections in the prior year;
Another insurer, which used a 12-tier rate system, would issue coverage at the second most favorable rate tier if the child had just one infection in the prior year or ear tubes, at the fifth rate tier if there had been 2-3 infections during the prior year, and at the seventh tier if there had been 4 or more infections; for some conditions, this company’s rating might depend on the plan deductible – applicants with history of ear infections would be offered the second rating tier for policies with a deductible of $5,000 or higher;
Another insurer would issue standard coverage if the child had just one infection in the prior year or if ear tubes had been inserted more than one-year prior, apply a rate up if there were two infections in the prior year, and decline the application if there were three or more infections;
Another insurer would issue standard coverage if the child had fewer than 3 infections in the past year, but issue coverage with a condition specific deductible of $5,000 if there had been 3 or more infections or if ear tubes had been inserted.
In a 2000 Kaiser Family Foundation study of medical underwriting practices, insurers were asked to underwrite hypothetical applicants with varying health conditions, from seasonal allergies to situational depression to HIV. Results varied significantly for less serious conditions. For example, the applicant with seasonal allergies who made 60 applications for coverage was offered standard coverage 3 times, declined 5 times, offered policies with exclusion riders or other benefit limits 46 times (including 3 offers that excluded coverage for her upper respiratory system), and policies with premium rate ups (averaging 25%) 6 times.
Pre-existing Condition Exclusion Provisions
In addition to medical screening of applicants before coverage was issued, most individual market policies also included more general pre-existing condition exclusion provisions which limited the policy’s liability for claims (typically within the first year) related to medical conditions that could be determined to exist prior to the coverage taking effect.3
Example of pre-existing condition exclusion
Jean, an Arizona teacher whose employer provided group health benefits but did not contribute to the cost for family members, gave birth to her daughter, Alex, in 2004 and soon after applied for an individual policy to cover the baby. Due to time involved in the medical underwriting process, the baby was uninsured for about 2 weeks. A few months later, Jean noticed swelling around the baby’s face and eyes. A specialist diagnosed Alex with a rare congenital disorder that prematurely fused the bones of her skull. Surgery was needed immediately to avoid permanent brain damage. When Jean sought prior-authorization for the $90,000 procedure, the insurer said it would not be covered. Under Arizona law, any condition, including congenital conditions, that existed prior to the coverage effective date, could be considered a pre-existing condition under individual market policies. Alex’s policy excluded coverage for pre-existing conditions for one year. Jean appealed to the state insurance regulator who upheld the insurer’s exclusion as consistent with state law.
The nature of pre-existing condition exclusion clauses varied depending on state law. In 19 states, a health condition could only be considered pre-existing if the individual had actually received treatment or medical advice for the condition during a “lookback” period prior to the coverage effective date (from 6 months to 5 years). In most states, a pre-existing condition could also include one that had not been diagnosed but that produced signs or symptoms that would prompt an “ordinarily prudent person” to seek medical advice, diagnosis or treatment. In 8 states and DC, conditions that existed prior to the coverage effective date – including those that were undiagnosed and asymptomatic – could be considered pre-existing and so excluded from coverage under an individual market policy. For example, a congenital condition in a newborn could be considered pre-existing to the coverage effective date (the baby’s birth date) and excluded from coverage. About half of the states required individual market insurers to reduce pre-existing condition exclusion periods by the number of months of an enrollee’s prior coverage.
Example of policy rescission
Jennifer, a Colorado preschool teacher, was seriously injured in 2005 when her car was hit by a drug dealer fleeing the police. She required months of inpatient hospitalization and rehab, and her bills reached $185,000. Jennifer was covered by a non-group policy which she had purchased five months prior to the accident. Shortly after her claims were submitted, the insurer re-reviewed Jennifer’s application and medical history. Following its investigation, the insurer notified Jennifer they found records of medical care she had not disclosed in her application, including medical advice sought for discomfort from a prolapsed uterus and an ER visit for shortness of breath. The insurer rescinded the policy citing Jennifer’s failure to disclose this history. Jennifer sued the insurer for bad faith; four years later a jury ordered the insurer to reinstate the policy and pay $37 million in damages.
Unlike exclusion riders that limited coverage for a specified condition of a specific enrollee, pre-existing condition clauses were general in nature and could affect coverage for any applicable condition of any enrollee. Pre-existing condition exclusions were typically invoked following a process called post-claims underwriting. If a policyholder would submit a claim for an expensive service or condition during the first year of coverage, the individual market insurer would conduct an investigation to determine whether the condition could be classified as pre-existing.
In some cases, post-claims underwriting might also result in coverage being cancelled. The investigations would also examine patient records for evidence that a pre-existing condition was known to the patient and should have been disclosed on the application. In such cases, instead of invoking the pre-existing condition clause, an issuer might act to rescind the policy, arguing it would have not issued coverage in the first place had the pre-existing condition been disclosed.
Discussion
The Affordable Care Act guarantees access to health insurance in the individual market and ends other underwriting practices that left many people with pre-existing conditions uninsured or with limited coverage before the law. As discussions get underway to repeal and replace the ACA, this analysis quantifies the number of adults who would be at risk of being denied if they were to seek coverage in the individual market under pre-ACA rules. What types of protections are preserved for people with pre-existing conditions will be a key element in the debate over repealing and replacing the ACA.
We estimate that at least 52 million non-elderly adult Americans (27% of those under the age of 65) have a health condition that would leave them uninsurable under medical underwriting practices used in the vast majority of state individual markets prior to the ACA. Results vary from state-to-state, with rates ranging around 22 – 23% in some Northern and Western states to 33% or more in some southern states. Our estimates are conservative and do not account for a number of conditions that were often declinable (but for which data are not available), nor do our estimates account for declinable medications, declinable occupations, and conditions that could lead to other adverse underwriting practices (such as higher premiums or exclusions).
While most people with pre-existing conditions have employer or public coverage at any given time, many people seek individual market coverage at some point in their lives, such as when they are between jobs, retired, or self-employed.
There is bipartisan desire to protect people with pre-existing conditions, but the details of replacement plans have yet to be ironed out, and those details will shape how accessible insurance is for people when they have health conditions.
Gary Claxton, Cynthia Cox, Larry Levitt, and Karen Pollitz are with the Kaiser Family Foundation. Anthony Damico is an independent consultant to the Kaiser Family Foundation.
Methods
To calculate nationwide prevalence rates of declinable health conditions, we reviewed the survey responses of nonelderly adults for all question items shown in Methods Table 1 using the CDC’s 2015 National Health Interview Survey (NHIS). Approximately 27% of 18-64 year olds, or 52 million nonelderly adults, reported having at least one of these declinable conditions in response to the 2015 survey. The CDC’s National Center for Health Statistics (NCHS) relies on the medical condition modules of the annual NHIS for many of its core publications on the topic; therefore, we consider this survey to be the most accurate means to estimate both the nationwide rate and weighted population.
Since the NHIS does not include state identifiers nor sufficient sample size for most state-based estimates, we constructed a regression model for the CDC’s 2015 Behavioral Risk Factor Surveillance System (BRFSS) to estimate the prevalence of any of the declinable conditions shown in Methods Table 1 at the state level. This model relied on three highly significant predictors: (a) respondent age; (b) self-reported fair or poor health status; (c) self-report of any of the overlapping variables shown in the left-hand column of Methods Table 1. Across the two data sets, the prevalence rate calculated using the analogous questions (i.e. the left-hand column of Methods Table 1) lined up closely, with 20% of 18-64 year old survey respondents reporting at least one of those declinable conditions in the 2015 NHIS and 21% of 18-64 year olds in the 2015 BRFSS. Applying this prediction model directly to the 2015 BRFSS microdata yielded a nationwide prevalence of any declinable condition of 28%, a near match to the NHIS nationwide estimate of 27%.
Methods Table 1: Declinable Medical Conditions Available in Survey Microdata
Declinable Condition Questions Available in both the 2015 National Health Interview Survey and also the 2015 Behavioral Risk Factor Surveillance System
Declinable Condition Questions Available in only the 2015 National Health Interview Survey
Ever had CHD
Melanoma Skin Cancer
Ever had Angina
Any Other Heart Condition
Ever had Heart Attack
Crohn’s Disease or Ulcerative Colitis
Ever had Stroke
Epilepsy
Ever had COPD
Difficulty Due to Mental Retardation
Ever had Emphysema
Difficulty Due to Cerebral Palsy
Chronic Bronchitis in past 12 months
Difficulty Due to Senility
Ever had Non-Skin Cancer
Difficulty Due to Depression
Ever had Diabetes
Difficulty Due to Endocrine Problem
Weak or Failing Kidneys
Difficulty Due to Blood Forming Organ Problem
BMI > 40
Difficulty Due to Drug / Alcohol / Substance Abuse
Pregnant
Difficulty Due to Schizophrenia, ADD, or Bipolar Disorder
In order to align BRFSS to NHIS overall statistics, we then applied a Generalized Regression Estimator (GREG) to scale down the BRFSS microdata’s prevalence rate and population estimate to the equivalent estimates from NHIS, 27% and 52 million. Since the regression described in the previous paragraph already predicted the prevalence rate of declinable conditions in BRFSS by using survey variables shared across the two datasets, this secondary calibration solely served to produce a more conservative estimate of declinable conditions by calibrating BRFSS estimates to the NHIS. After applying this calibration, we calculated state-specific prevalence rates and population estimates off of this post-stratified BRFSS sample.
The programming code, written using the statistical computing package R v.3.3.2, is available upon request for people interested in replicating this approach for their own analysis.
Endnotes
In 2013, five states – Maine, Massachusetts, New Jersey, New York, and Vermont – required all non-group health insurance policies to be offered on a guaranteed issue basis (meaning applicants could not be denied based on health status) with community rating (meaning premiums could not vary based on health status). ↩︎
Under the Health Insurance Portability and Accountability Act of 1996 (HIPAA), eligible individuals who had at least 18 months of continuous prior coverage, who were leaving group health plan coverage, and who met other requirements, had to be offered non-group policies on a guaranteed issue basis with no pre-existing condition exclusions. HIPAA gave insurers flexibility to limit the number of guaranteed issue policies to two. In addition, HIPAA gave states flexibility to offer eligible individuals an alternative source of individual market coverage, such as high-risk pool coverage, which most states elected to do. See Kaiser Family Foundation State Health Facts.
↩︎
As the nation struggles with an ongoing epidemic of prescription painkiller abuse, misuse, and overdoses, a new Washington Post/Kaiser Family Foundation survey finds that one in three (34%) of those who recently used such drugs for at least two months report being addicted or dependent.
Most long-term users are battling significant health problems, including seven in ten who say they have a debilitating disability or chronic disease. Almost all (98%) long-term painkiller users cite relieving pain as a reason for using the medications, but some also report other reasons:
One third (34%) say they take the painkillers for fun or to get high;
One in five (22%) say they take them to deal with day-to-day stress; and
One in ten (12%) say they take them to relax or relieve tension.
Nearly all (97%) long-term users say they started taking the painkillers through a prescription from a doctor, and most say they discussed with their doctor the possibility of addiction or dependence and alternative ways to manage pain. However, only a third (33%) say their doctor discussed a plan for getting off of the medication.
Some long-term users also report misuse of prescribed medications, including:
20 percent say that they have known or suspected that someone else was using, taking, or selling their painkillers;
17 percent report taking painkillers not prescribed for them; and
14 percent say they’ve shared their painkillers with a family member or friend.
Given the recent attention to prescription opioid abuse, two thirds (67%) of long-term users say they are concerned that efforts to reduce the number of people abusing prescription painkillers will make it harder for them to obtain their medication.
The new Post/Kaiser Survey of Long-Term Prescription Painkiller Users and Their Household Members is the 30th in a series of surveys over the past 20 years conducted as part of The Washington Post/Kaiser Family Foundation Survey Project. The poll was conducted by cellular and landline telephone October 3 – November 9, 2016, among a random national sample of 809 adults age 18 and older who they themselves (n=622), or a household member (n=187) have taken strong prescription painkillers for a period of two months or more at some time in the past two years other than to treat pain from cancer or terminal illness. The margin of sampling error is plus or minus 4 percentage points for the full survey and plus or minus 5 percentage points for those personally taking prescription painkillers long-term. A report with full survey results is available on the Foundation’s website. The Washington Post articles on the survey findings are available at washingtonpost.com. The survey was designed and analyzed jointly by researchers at Kaiser and The Washington Post.
This partnership poll from The Washington Post and the Kaiser Family Foundation examines the long-term use of prescription painkillers by exploring the views and experiences of adults 18 and over who they themselves have taken strong prescription painkillers for a period of two months or more at some time in the past two years, other than to treat pain from cancer or terminal illness. The survey, conducted at a time when the nation is struggling to address the ongoing prescription painkiller and heroin epidemic, takes a closer look at long-term users of prescription painkillers to better understand how they started taking these drugs, their interactions with medical providers, their concerns and experiences with addiction, and their views of efforts to stem the abuse of painkillers. In addition, the survey also included household members of long-term users in order to capture their unique insight into how the drug use has impacted the individual.
This survey is the 30th in a series of surveys dating back to 1995 that have been conducted as part of The Washington Post/Kaiser Family Foundation Survey Project.
As the nation struggles to address the ongoing prescription painkiller and heroin abuse and overdose epidemic, The Washington Post and Kaiser Family Foundation Survey of Long-Term Prescription Painkiller Users and Their Household Members takes a closer look at those who are long-term users of prescription painkillers to better understand from their perspective what some of the drawbacks and benefits of the drugs are, as well as how they have impacted their lives. The survey explores how these long-term users started taking the drugs, their interactions with medical providers, their concerns and experiences with addiction, and their views of efforts to stem the abuse of painkillers. The survey was conducted among adults 18 and over who they themselves have taken strong prescription painkillers for a period of two months or more1 at some time in the past two years, other than to treat pain from cancer or terminal illness. In addition, the survey also included household members of long-term users in order to capture their unique insight into how the drug use has impacted the individual. Some of the key findings from this survey are noted below.
Long-Term Users Say They Started for Medical Reasons and Discussed Risks with Providers
Nearly all long-term users of prescription painkillers say they started the painkillers with a prescription from a doctor and that they started taking them for chronic pain (44 percent), for pain after a surgery (25 percent) or for pain after an accident or injury (25 percent).
Majorities say their doctor talked to them about the possibility of addiction or dependence, avoiding alcohol or other medications, and other ways to manage pain, but 61 percent say there was no discussion about a plan for getting off the painkillers. Still, a large majority (75 percent) say they think their doctor provided enough information on the risk of addiction and other side effects associated with prescription painkillers.
Disability and Poor Health Are Common Among Long-Term Users, Most Say Drugs Have Improved Life and Are Concerned About Crackdown
They are a group that reports significant health issues such as a debilitating disability or chronic disease (70 percent), only fair or poor physical health (42 percent), or taking four or more prescription drugs (57 percent).
A majority of long-term prescription painkiller users (57 percent) say it has made their quality of life better, but one in six (16 percent) say it has made it worse.
With the recent attention prescription painkillers have received in light of the epidemic of abuse and overdose, two-thirds (67 percent) of long-term users say they are concerned that efforts to decrease the number of people abusing prescription painkillers will make it more difficult for them to access them.
Some Report Non-Medical Use, Addiction or Dependence, or Other Misuse
While nearly all long-term users say they use the drugs to relieve pain, some also report that a major reason they take them is “for fun or to get high” (20 percent), “to deal with day-to-day stress” (14 percent), or “to relax or relieve tension” (10 percent). Only three percent of long-term users say that when they started, it was for recreational reasons.
Sizeable shares also report:
being physically dependent or addicted to the painkillers (34 percent) (a group explored in detail in Section 2),
they have taken prescription painkillers that were not prescribed specifically for them since starting on painkillers (17 percent),
they have given their painkillers to a family member or friend (14 percent), and
they have known or suspected someone was using, taking, or selling their painkillers (20 percent).
Household Members Generally Report More Negative Impacts
Interviews with people living in the same household as a long-term prescription painkiller user provide another angle of insight into these individuals, be it their spouse, parent, or another household member.
Household members are more likely to report they think the user is or was addicted or dependent and that their use has had a negative impact on their finances, personal relationships, and their health.
Views of the Painkiller Epidemic
Majorities of people personally using prescription painkillers as well as people in their household say that people who use painkillers and doctors who prescribe painkillers deserve at least some of the blame for the painkiller addiction epidemic.
When asked about a number of efforts what would be effective in reducing the abuse of prescription painkillers, long-term users point to efforts such as increasing pain management training for medical students and doctors (82 percent), increasing access to addiction treatment programs (80 percent), and increasing research about pain and pain management (81 percent).
Report: Introduction
Currently, the nation is struggling with an ongoing epidemic of prescription painkiller and heroin abuse and overdose, driven at least in part by a recent increase in the number of prescriptions written.2 Recognizing the role physicians play in prescribing strong painkillers, the Centers for Disease Control and Prevention recently released guidelines for prescribing these medications and note the limited evidence of the efficacy of long-term use of prescription painkillers and concerns that the risks of addiction and adverse effects may outweigh their benefits.3 However, many people rely on prescription painkillers to provide relief from acute or chronic pain. As policymakers, medical professionals, and families weigh how to handle the ongoing epidemic and in order to better understand how long-term users came to use these drugs and their experiences while taking them, The Washington Post and the Kaiser Family Foundation conducted a survey of adults who they themselves, or a household member, have taken strong prescription painkillers for a period of two months or more at some time in the past two years, other than to treat pain from cancer or terminal illness. A time period of two months or more was selected to focus on those whose use may be at odds with current government guidelines around prescription painkiller use. We estimate that about 7 percent of adults in the U.S. fall into this category (5 percent), or have a household member who does (2 percent). What follows is a close look at their views and experiences with these painkillers, and how they view ongoing efforts to quell the epidemic.
Report: Section 1: Views And Experiences Of Long-term Users Of Prescription Painkillers
Why Did They Start Taking Strong Prescription Painkillers?
The vast majority of those taking strong prescription painkillers for two months or more report starting them with a prescription from a doctor (97 percent). More than four in ten of long-term users say they started taking them for chronic pain (44 percent), while 25 percent say they started due to pain after a surgery and another 25 percent say they started for pain after an accident or injury. Very few say they initially got the painkillers some way other than a doctor (3 percent) or that they started for recreational use (3 percent).
Many have been taking the painkillers for quite some time. Half (52 percent) of those personally using prescription painkillers say they have taken them for two years or more, but there are big differences depending on if they are still taking them or not. Most of those who say they no longer take them say they took them for 6 months or less (48 percent) and that they started them for pain after surgery (34 percent) or an accident or injury (27 percent). Seven in ten of those currently taking them have been on them for two years or more, and most started taking them for chronic pain (55 percent).
Table 1: Length of Use and Reason for Starting Varies by Current Usage
AMONG THOSE PERSONALLY USING PRESCRIPTION PAINKILLLERS LONG-TERM:
Total
Currently taking prescription painkillers (55%)
No longer taking prescription painkillers (45%)
How long (have you been taking/did you take) these painkillers?
6 months or less
28%
12%
48%
More than 6 months but less than 1 year
7
4
10
At least 1 year but less than 2 years
13
14
12
2 years or more
52
70
30
Which of the following comes closest to the reason you began taking painkillers?
Pain after surgery
25%
18%
34%
Pain after an accident or injury
25
23
27
Chronic pain
44
55
32
Recreational use
3
2
4
NOTE: Started for some other reason (vol.) and Don’t know/Refused responses not shown.
Those no longer personally taking them point to a number of different reasons why they stopped, including that they no longer needed them for pain (60 percent of those not currently taking them), they were worried about becoming addicted (50 percent), they didn’t like the side effects (45 percent), and their prescription ended (34 percent).
Reasons for Taking Prescription Painkillers
While about nine in ten long-term prescription painkiller users report that relieving physical pain is a ‘major reason’ why they take the painkillers, some report taking the painkillers for other reasons as well. One in five say a major reason they take them is “for fun or to get high,” followed by 14 percent who say “to deal with day-to-day stress” and 10 percent who say “to relax or relieve tension.”
Figure 1: Large Majority of Long-Term Users Report Relieving Physical Pain as a Reason for Use; but Some Say Other Reasons As Well
Many Users Report a Disability and Multiple Prescriptions
Many personally taking prescription painkillers report being sick and disabled, such as saying they have a debilitating disability or chronic disease (70 percent) or that their physical health is only fair or poor (42 percent). More than half (57 percent) also say they take four or more prescription drugs, including 32 percent who report taking seven or more. These shares are significantly larger than for the general public. For example, 19 percent of the public reports having a chronic disease or disability4 and 18 percent say they are in fair or poor health.5
Figure 2: Many Long-Term Prescription Painkiller Users Are Sick and Disabled
Compared to the general public, long-term users skew middle aged (59 percent between 40-64 versus 43 percent). Relatively few long-term users report working full-time (23 percent) or part time (8 percent) with more long-term users saying they are on disability (33 percent) or retired (20 percent). In comparison, six in ten of the general public report being employed, 18 percent say they’re retired, and 7 percent say they are on disability and can’t work.6
Interactions with Doctors
Most personally taking prescription painkillers long-term report that when their doctor first prescribed these medications, their doctor talked to them about:
avoiding alcohol or certain medications while taking painkillers (78 percent);
possible side effects associated with these painkillers (70 percent);
keeping the medications in a safe place so they’re not misused by others (68 percent);
the possibility of addiction or dependence (65 percent); and
other ways to manage pain besides these painkillers (62 percent).
On the other hand, 61 percent say there was no discussion about a plan for getting off the painkillers when the doctor first prescribed them, while a third (33 percent) say there was.
Figure 3: Majority of Long-Term Users Report Talking About a Variety of Topics With Their Doctor When First Prescribed
In addition, 75 percent of long-term prescription painkiller users say they think their doctor provided enough information on the risk of addiction and other side effects associated with prescription painkillers. Still, one in five (19 percent) say their doctor did not provide enough information. For the most part, long-term users say that their doctor has not changed their dose (56 percent) or how often they take them (71 percent) since they started taking them. However, about two in ten (21 percent) say a doctor has increased their dose, and one in ten (10 percent) say their doctor has told them to take them more frequently.
Impact on Life
Overall, long-term users report mostly positive effects of using painkillers. Virtually all long-term users (92 percent) say the painkillers have reduced their pain at least somewhat well. And, a majority of long-term prescription painkiller users (57 percent) say their use of the medications has made their quality of life better, particularly those who say they started the painkillers for chronic pain (69 percent), but one in six (16 percent) say it has made it worse.
In terms of the impact their use of the painkillers has had on certain aspects of their lives, most long-term users report that their use of the drugs has had no impact on their finances (74 percent) however more say the impact has been negative than say positive (17 percent versus 8 percent). But when it comes to their impact on their physical health or their ability to do their job, more say the impact has been positive than say negative (42 percent vs. 20 percent and 23 percent vs. 14 percent, respectively). Most say there has been no impact on their mental health or personal relationships, but for those that do, similar shares say the impact has been positive as say negative.
Figure 4: Majorities Report That Their Use of Prescription Painkillers Has Had No Impact on Finances, Relationships, or Mental Health
Reports of Addiction, Dependence and Misuse
In addition to some reporting negative impacts on their lives, 34 percent report that they think they are or were physically dependent or addicted to the painkillers (this group is profiled in Section 2). Few (9 percent) say they have sought treatment for addiction and 2 percent say they have considered seeking addiction treatment. Additionally, a quarter (26 percent) say that a friend or family member has suggested they stop taking them.
There are also a number of indications of misuse among long-term users, including 17 percent who say they have taken prescription painkillers that were not prescribed specifically for them since starting on painkillers and 14 percent who say they have given their painkillers to a family member or friend. In addition, 20 percent say they have known or suspected someone was using, taking, or selling their painkillers, rising to nearly three in ten (28 percent) of long-term users in rural areas, compared to 10 percent of those in urban areas.
Figure 5: One in Three Long-Term Prescription Painkiller Users Think They Are Addicted or Dependent; Some also Report Misuse
Risky Use
Many are taking other drugs that could put them more at risk for an overdose or other complications. About half (52 percent) of long-term users say that while taking their prescription painkillers they were taking other prescription medications for anxiety, depression, or sleep problems. And, 18 percent say that while taking their prescription painkillers they have consumed alcohol.
Perceptions of Risk
Two-thirds (68 percent) of those personally using prescription painkillers long-term say that the benefits of pain relief outweigh the risk of addiction. However, nearly half (46 percent) acknowledge that using them makes a person more likely to use heroin or other illegal drugs and 40 percent say prescription painkillers are as addictive as heroin.
Compared to those personally using strong painkillers, the general public is more split on the risks and benefits of using prescription painkillers for more than a week, and are more likely than those personally using to say prescription painkiller use makes a person more likely to use heroin or other illegal drugs or that prescription painkillers and heroin are equally addictive.
Table 2: Long-Term Users’ and General Public’s Perceptions of Prescription Painkiller Risk
Which comes closer to your view on using prescription painkillers for more than a week to treat pain?
The risk of addiction outweighs the benefits of pain relief
25%
47%
The benefits of pain relief outweigh the risk of addiction
68
44
Don’t know/Refused
6
9
Do you think prescription painkiller abuse makes a person more likely or less likely to use heroin or other illegal drugs, or do you think it doesn’t make much of a difference?
More likely
46%
58%
Less likely
4
2
Doesn’t make much of a difference
43
36
Don’t know/Refused
7
4
Which do you think is more addictive, prescription painkillers or heroin, or do you think they are about equally addictive?
Prescription painkillers
3%
6%
Heroin
45
29
Equally addictive
40
60
Don’t know/Refused
12
6
SOURCE: National comparison of U.S. adults from Kaiser Health Tracking Poll (conducted November 15-21, 2016)
Access to Prescription Painkillers: Users’ Troubles and Concerns
Reports of Problems Accessing Painkillers
Some of those personally using prescription painkillers long-term report trouble accessing them, including trouble affording them (18 percent), getting a pharmacy to fill a prescription (16 percent), getting refill from doctors (16 percent), and getting insurance to cover it (12 percent). Overall, 41 percent of long-term users report at least one of these issues. With the recent attention prescription painkillers have received in light of the epidemic of abuse and overdose, two-thirds (67 percent) of long-term users say they are concerned that efforts to decrease the number of people abusing prescription painkillers will make it more difficult for them to access them; a share that increases to nearly eight in ten (78 percent) of those who started to treat chronic pain, including 56 percent who say they are very concerned.
Six in ten (60 percent) long-term users say it is easy for people to get painkillers that were not prescribed to them, while a similar share (59 percent) say it is difficult for people who need the drugs for medical purposes to get them. Majorities of the general public say it is easy to get drugs in both scenarios, although a larger share say it’s easy for people to get drugs not prescribed to them than say the same about those who need them for medical purposes.
Table 3: Perceptions of Prescription Painkiller Accessibility Among Long-Term Users and the General Public
How easy or difficult do you think it is for people…
… to get access to prescription painkillers that were NOT prescribed to them?
Easy (NET)
60%
71%
Very easy
36
37
Somewhat easy
24
33
Difficult (NET)
27
27
Somewhat difficult
14
17
Very difficult
14
10
Don’t know/Refused
13
3
… who need prescription painkillers for medical purposes to get access to them?
Easy (NET)
36%
62%
Very easy
16
28
Somewhat easy
20
34
Difficult (NET)
59
35
Somewhat difficult
30
24
Very difficult
29
12
Don’t know/Refused
5
3
SOURCE: National comparison of U.S. adults from Kaiser Health Tracking Poll (conducted November 15-21, 2016)
Side Effects
Prescription painkillers are known for causing certain side effects, and among long-term users, reports of side effects are quite common. Seven in ten (72 percent) of those personally using prescription painkillers report experiencing at least one of the following side effects: constipation (55 percent), indigestion, dry mouth, or nausea (50 percent) or breathing problems (15 percent). While many have experienced side effects, half (50 percent) say they have not taken medications specifically to treat side effects. However, one in five (21 percent) say they have.
Half (49 percent) of those personally using painkillers say they are at least somewhat concerned about side effects, including one in four (27 percent) who say they are very concerned, and nearly half of those who no longer take the painkillers say that the side effects are at least a minor reason they stopped (45 percent, or 20 percent of long-term users overall). Still, large majorities say their doctor discussed possible side effects when they initially prescribed the painkillers (70 percent) and feel their doctor provided enough information about the risk of addiction and other side effects (75 percent).
Views and Experiences from Household Members of Prescription Painkiller Users
Interviews with people living in the same household as a long-term prescription painkiller user provide another angle of insight into this group. For most, the user is a spouse (43 percent), followed by a parent (25 percent), a child (9 percent), or some other person in their household (21 percent).
Household Members Report Negative Impacts, Concerned About Addiction
In general, household members are more likely to report issues with addiction or dependence and negative experiences than those who are personally taking the painkillers. For example, 54 percent of household members say they think the person is or was addicted or dependent and 43 percent report that a friend or family member has suggested the user stop.
Figure 6: Household Members More Likely to Report Concerns About Use Than Those Personally Using Prescription Painkillers Themselves
In addition, household members are roughly twice as likely as those personally using prescription painkillers to say the drugs have had a negative impact on the user’s finances (37 percent versus 17 percent), the user’s personal relationships (34 percent versus 16 percent), the user’s physical health (39 percent versus 20 percent), the user’s mental health (39 percent versus 19 percent), and the user’s ability to do their job (27 percent versus 14 percent).
Report: Section 2: A Focus On Those Reporting They Are Physically Dependent Or Addicted
Of those personally using prescription painkillers, about a third (34 percent) say they think they are or were addicted or physically dependent on them,7 which accounts for about 2 percent of adults in the U.S. This section examines their views and experiences more closely. Like long-term prescription painkiller users generally, many who say they are or were addicted or dependent say they started for chronic pain (47 percent), a quarter (25 percent) say they started for pain after a surgery, and 19 percent say they started after an injury or accident. Six percent say they started using recreationally.
Nearly all (95 percent) of those saying they’re addicted or dependent say that relieving physical pain is a reason they’re taking the drugs. However, they are much more likely than others to say they’re taking them for other reasons as well, such as for fun or to get high (47 percent versus 27 percent), to deal with day-to-day stress (38 percent versus 14 percent), or to relax or relieve tension (30 percent versus 3 percent).
Figure 7: Long-Term Users Who Say They Are Addicted or Dependent Are More Likely to Report Taking Painkillers for Other Reasons
Not surprisingly, those who say they are or were dependent or addicted also are more likely than others to report being concerned about addiction (49 percent versus 25 percent) and to report misuse, such as taking painkillers not prescribed to them (30 percent versus 10 percent) or giving them to a family member or friend (21 percent versus 11 percent). They are also more likely than others to say they know or suspect someone has taken their pills (28 percent versus 15 percent) and to report that a family or friend has suggested they stop taking the medication (40 percent versus 18 percent).
About a quarter (24 percent) of those who report being addicted or dependent say they think their quality of life is worse after taking these medications, compared to 12 percent of those who do not say they are addicted or dependent. They’re also more likely than those not reporting addiction or dependence to say it’s had a negative impact on their finances, their personal relationships, their employment, their physical health, and their mental health.
Figure 8: Long-Term Users Who Say They Are Addicted or Dependent Are More Likely to Report Negative Impacts of Painkillers
Among those who say they are or were addicted or dependent, three in ten (31 percent) feel their doctor did not provide enough information about the risk of addiction and other side effects, but they are similar to others in terms of reporting that their doctor talked to them about the possibility of addiction or dependence or a plan to get off medications. They’re more likely than others to say they have had trouble with at least one of the following: getting a prescription written or filled, affording the drugs, or getting insurance to pay for them (58 percent versus 33 percent). Eight percent say they have a prescription for Narcan or Naloxone at home, a drug that can reverse the effects of prescription painkillers and prevent overdose.
Controlling for factors such as income and region, younger adults (18-39), Hispanics, and those who report taking the painkillers for two or more years are more likely than their counterparts to report being addicted or dependent on the drugs.
Report: Section 3: Views Of Prescription Painkiller Epidemic
Prescription Painkiller Abuse Is One of Many Serious Health Issues
For those personally using prescription painkillers long-term, the abuse of painkillers ranks last on a list of health issues facing the country today. Those personally using in the South (73 percent) are more likely to say opioid abuse is a very serious problem than those in the Midwest (60 percent) or West (41 percent).
Table 4: Abuse of Prescription Painkillers Ranks Low Among Several Health Issues, But Majorities Say Abuse Is a Very Serious Problem
Percent who say each health issue is a VERY SERIOUS problem in this country:
NOTE: Some items asked of half samples. Question wording abbreviated. See topline for full question wording.SOURCE: National comparison of U.S. adults from Kaiser Health Tracking Poll (conducted November 15-21, 2016)
Who’s To Blame For Epidemic?
Majorities of people personally using prescription painkillers as well as people in their household say that people who use painkillers and doctors who prescribe them deserve at least some of the blame for the ongoing epidemic. In addition, two-thirds (65 percent) of opioid users’ household members say they blame drug companies and half (49 percent) say they blame the government. Ranking lower on the list for both groups are law enforcement and pharmacies and pharmacists.
Table 5: Views of Long-Term Users, Their Household Members, and the General Public onWho Is to Blame for the Prescription Painkiller Addiction Epidemic
Percent who say each of the following deserve A LOT or SOME blame for the prescription painkiller addiction epidemic:
Household members of those using prescription painkillers long-term
U.S. Adults
People who use painkillers
61%
65%
68%
Doctors who prescribe painkillers
54
66
69
Drug companies
47
65
60
The government
40
49
44
Hospitals
27
44
43
Law enforcement
17
14
28
Pharmacies and pharmacists
15
19
28
NOTE: Some items asked of half samples of the general public.SOURCE: National comparison of U.S. adults from Kaiser Health Tracking Poll (conducted November 15-21, 2016)
Effective Strategies for Combatting the Epidemic
When asked what would be effective in reducing the abuse of prescription painkillers, eight in ten of those personally taking opioids say increasing pain management training for medical students and doctors (82 percent), increasing research about pain and pain management (81 percent), and increasing access to addiction treatment programs (80 percent). Large majorities also say encouraging people who were prescribed painkillers to dispose of any extras once they no longer medically needed them (73 percent), public education and awareness programs (72 percent), and monitoring doctors’ prescribing habits (69 percent) would be effective. Roughly half say reducing the social stigma around addiction (54 percent), putting warning labels about addiction on drug bottles (50 percent), and government limits on the amount of drugs that can be produced (47 percent). These responses are generally similar to what the public feels would be effective. The general public is somewhat more likely than those personally using to say the following would be effective: public education and awareness programs (86 percent vs. 72 percent), monitoring doctors’ prescription painkiller prescribing habits (83 percent vs. 69 percent), and increasing pain management training for medical students and doctors (89 percent vs. 82 percent).
Methodology
The Washington Post/Kaiser Family Foundation Survey Project is a partnership combining survey research and reporting to better inform the public. The Post-Kaiser Survey of Long-Term Prescription Painkiller Users and Their Household Members, the 30th in this series was conducted by telephone October 3 – November 9, 2016, among a representative random national sample of 809 adults age 18 and over who they themselves, or a household member, have taken strong prescription painkillers for a period of two months or more8 at some time in the past two years, other than to treat pain from cancer or terminal illness. Interviews were administered in English and Spanish, combining random samples of both landline (n=266) and cellular telephones (n=543).
Sampling, data collection, weighting and tabulation were managed by SSRS in close collaboration with The Washington Post and Kaiser Family Foundation researchers.
The SSRS Omnibus survey (detailed below) estimates that about seven percent of adults in the U.S. have either themselves used strong prescription painkillers in the past two years for two months or more, other than to treat pain from cancer or terminal illness (five percent), or have a household member that has (two percent). Due to the low-incidence of this study population, the sampling was designed to increase efficiency in reaching this group by using the following sample sources:
Cell and Landline Phone Random Digit Dialing (RDD) (n=354): The dual frame landline and cellular phone sample was generated by Marketing Systems Group (MSG) using RDD procedures. Interviewers calling landline phone numbers asked to speak with an adult currently at home on a random rotation. Interviews calling cellular phones interviewed the person answering the phone after verifying eligibility.
Respondents Previously Completing Interviews on the SSRS Omnibus Survey (n=455). Weekly, RDD landline and cellular phone surveys of the general public were used to identify eligible respondents. Individuals who had previously indicated on the SSRS omnibus survey that they fit the eligibility criteria for this study were re-contacted.
Regardless of the sample source, all respondents were screened to verify that they have taken a strong prescription painkiller for a period of two months or more in the past two years or have a household member who has, other than to treat pain from cancer or terminal illness. If a respondent indicated that both themselves and a household member qualified, they completed the questionnaire about their own personal use. The screening questions are identified at the beginning of this document as S3 through S5.
A multi-stage weighting design was applied to ensure an accurate representation of the population of long-term strong prescription drug users and their household members. The first stage of weighting involved corrections for sample design, including accounting for non-response for the re-contact sample. In the second weighting stage, demographic adjustments were applied to account for systematic non-response along known population parameters. No reliable administrative data were available for creating demographic weighting parameters for this group. Therefore, demographic benchmarks were derived by compiling a sample of all respondents interviewed on the SSRS Omnibus survey between August 18, 2016 and November 9, 2016 (N=15,944) and weighting this sample to match the national adult population based on the 2016 U.S. Census Current Population Survey March Supplement parameters for age, gender, education, race/ethnicity, region, phone status, and population density. This sample was then filtered to include respondents qualifying for the current survey (N=1,122), and the weighted demographics of this group were used as post-stratification weighting parameters for the total sample (including age by gender, education, race/ethnicity, region, population density, self or household member prescription painkiller user, and phone status).
All sampling error margins and tests of statistical significance have been adjusted to account for the survey’s design effect, which is 1.6 for this survey. The design effect is a factor representing the survey’s deviation from a simple random sample, and takes into account decreases in precision due to sample design and weighting procedures. Sample sizes and margin of sampling errors for key groups are shown below; other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll.
Table 6: Sample Size and Margin of Sampling Error
Group
N (unweighted)
Margin of sampling error (percentage points)
Total
809
±4
Interview type
Personal user
622
±5
Household interview
187
±9
Among personal users
Report being addicted or dependent
200
±9
Do not report being addicted or dependent
422
±6
This questionnaire was administered with the exact questions in the exact order as appears in this document. If a question was asked of a reduced base of the sample, a parenthetical preceding the question identifies the group asked. Current users were asked the questions in the present tense, indicated where applicable in the first part of the parenthetical text within the question. Past users were asked the questions in the past tense and read the language in the second half of the parentheses. In addition, those personally using were asked the questions directly about their use, whereas household members were asked about the user in most cases, as indicated in the questions.
Since some of the questions could be sensitive and due to the nature of the survey content, interviewers were given specific instructions on how to cope with respondents who seemed agitated or distressed by the questions, including offering resources to which respondents could turn for support.
The Washington Post and the Kaiser Family Foundation each contributed financing for the survey, and representatives of each organization worked together to develop the survey questionnaire and analyze the results. Each organization bears the sole responsibility for the work that appears under its name. The project team from the Kaiser Family Foundation included: Mollyann Brodie, Ph.D., Bianca DiJulio, and Bryan Wu. The project team from The Washington Post included: Scott Clement and Emily Guskin. Both The Washington Post and the Kaiser Family Foundation public opinion and survey research are charter members of the Transparency Initiative of the American Association for Public Opinion Research.
Endnotes
A time period of two months or more was selected to focus on those whose use may be at odds with current government guidelines around prescription painkiller use. ↩︎
We use a combined measure of those who say they are or were addicted OR physically dependent on prescription painkillers. We chose to use this combined measure given people’s potential for misunderstanding ‘dependence’ or their potential unwillingness to say they’re addicted due to social desirability reasons. The 34 percent who say they are addicted or dependent is comprised of 21 percent who say they are both addicted and dependent, 11 percent who say they’re only dependent, and 2 percent who say they’re only addicted. Overall, responses are similar for those saying they’re addicted and those saying they’re dependent. ↩︎
A time period of two months or more was selected to focus on those whose use may be at odds with current government guidelines around prescription painkiller use. ↩︎
To date, Minnesota and New York are the only states to have adopted a Basic Health Program (BHP), an option in the Affordable Care Act (ACA) that permits state-administered coverage in lieu of marketplace coverage for those with incomes below 200% of the federal poverty level (FPL) who would otherwise qualify for marketplace subsidies. BHP covers adults with incomes between 138-200% of FPL and lawfully present non-citizens with incomes below 138% FPL whose immigration status makes them ineligible for Medicaid. States implementing BHP receive 95% of what the federal government would have spent on subsidies if BHP enrollees had received marketplace coverage. Both states covered much of the BHP-eligible population prior to the ACA, which facilitated their adoption of BHP. Minnesota, in particular, adopted BHP to retain this prior coverage while saving state dollars. Based on semi-structured interviews with key stakeholders and policymakers in each state as well as reviews of policy documents and reports, this brief examines implementation of the BHP as of Summer 2016. It assesses the impact of BHP on consumers, the marketplaces, and state costs and financing. Although the 2016 election results create uncertainty around the future of the ACA (including BHP), BHP implementation provides important lessons about structuring coverage programs for low-income uninsured consumers for consideration in future reforms. Key findings include the following.
BHP programs in both Minnesota and New York provide coverage with lower premiums and cost-sharing compared to subsidized marketplace coverage. In New York, BHP enrollees with incomes at or below 150% FPL do not pay premiums while those with incomes between 150 and 200% FPL pay $20 per month. Sliding-scale premiums in Minnesota are higher than in New York but lower than for subsidized marketplace plans. According to stakeholders, an important feature of both programs is the absence of deductibles. Copayments are also generally lower than for QHPs. Both programs cover services in addition to essential health benefits for all or some BHP enrollees.
More affordable coverage led to increased enrollment in New York. When New York adopted the BHP in 2016, enrollment rose by 42% among those whose eligibility shifted from federally-subsidized QHPs to BHP. Enrollment increased by only 4% among subsidy-eligible adults unaffected by BHP implementation. Officials and stakeholders attributed the enrollment growth to BHP’s lower premiums and out-of-pocket cost-sharing compared to subsidized QHP coverage. Minnesota officials and stakeholders reached similar conclusions about the impact of affordability on enrollment. In both states, new enrollees attracted by more affordable coverage were described as relatively young and healthy. According to stakeholders, consumers also reported preferring the greater simplicity and predictability of BHP, compared to the marketplace.
BHP did not appear to affect marketplaces’ stability. New York officials reported that BHP implementation did not affect marketplace stability or carrier interest. Minnesota officials felt that the instability experienced in the state’s marketplace resulted from factors other than BHP; however, carriers suggested that BHP may have contributed by shrinking the marketplace’s size.
Most BHP insurers also participated in Medicaid and/or the marketplace. Minnesota conducted a joint procurement for Medicaid and BHP; carriers wishing to participate in one program had to join both, and many offered QHPs as well. In New York, 11 of 13 BHP plans participated in all three programs. This overlap helped consumers retain continuous coverage arrangements when income changes moved them between programs.
BHP enrollees whose incomes rose above 200% FPL experienced steep cost increases when they moved to QHPs. BHP’s more affordable coverage for enrollees ended at 200% FPL, so costs increased for those whose income rose above 200% FPL. Minnesota is exploring ways to smooth this “cliff” by expanding BHP eligibility above 200% FPL. Advocates in New York have called for a similar discussion of policy options.
Both states experienced fiscal gains from BHP, but state financing was needed. Both states achieved administrative efficiencies by using existing state agencies to run BHP. Both states also realized significant net savings by using BHP to fund populations previously covered with state funds—lawfully present immigrants in New York, who had been receiving Medicaid funded entirely by the state; and the general BHP population in Minnesota, which previously covered them through a Medicaid waiver with standard federal matching rates. However, the federal BHP payments did not fully cover program costs in either state, requiring the states to finance a share of the costs. For fiscal year 2017, Minnesota expects to pay 26% of BHP costs while New York will fund 15%.
While the outcome of the 2016 election has created uncertainty around the future of the ACA, including BHP, the experiences of Minnesota and New York with BHP suggest broader lessons about coverage for low-income consumers. Chief among these lessons is the importance of affordability, both in terms of premiums and out-of-pocket costs. New York’s natural experiment shows with particular clarity that affordability improvements can yield significant enrollment gains and risk-pool improvements among the lowest-income consumers qualifying for marketplace subsidies. In addition, stakeholders reported that many consumers preferred the simplicity of state-administered coverage that offered consistency in premiums, cost-sharing, and benefits across participating plans over the complexity of marketplace plans. Encouraging a common set of plans and providers to participate across programs, including public programs and the private market, can promote continuity of coverage and care for consumers who move between programs when household circumstances change. Finally, relying on existing infrastructure to administer new coverage programs creates efficiencies and can help to avoid duplication.
Issue Brief
Introduction
The Basic Health Program (BHP) gives states the option of providing state-administered coverage in lieu of coverage through health insurance marketplaces to certain individuals with incomes at or below 200% of the federal poverty level (FPL). Soon after the enactment of the Affordable Care Act (ACA), the BHP was broadly viewed as giving states the flexibility to provide more affordable coverage to low-income consumers and providing consumers with incomes up to 200% FPL with access to the same set of health plans. Because federal BHP regulations were delayed, states could not implement BHP until 2015. To date, two states, Minnesota and New York, have adopted BHP.
To learn about these states’ experiences with BHP, in Spring and Summer 2016 the Kaiser Family Foundation and the Urban Institute conducted semi-structured phone interviews with policymakers and stakeholders in Minnesota and New York. Interviewees included Medicaid and marketplace officials, consumer advocates, in-person assisters, and representatives from health plans and community health centers (CHCs). We also reviewed state policy documents and reports. This work builds on previous analyses that described federal regulations for the BHP and provided a roadmap to states interested in implementing the BHP for estimating the number of BHP-eligible people and approximate federal BHP payments.
This brief reviews Minnesota’s and New York’s approaches to BHP and assesses BHP’s impact on consumers, marketplaces, and state costs. Although there is uncertainty around the future of the ACA (including BHP) following the 2016 election, BHP implementation offers important lessons for consideration in future reforms about structuring coverage programs for low-income uninsured consumers.
Background
Federal BHP Rules
States can adopt the BHP to cover consumers with incomes up to 200% FPL who would otherwise qualify for subsidies in the marketplace. BHP is available to two groups of such consumers: those with incomes between 138-200% FPL; and lawfully present non-citizens with incomes at or below 138% FPL whose immigration status disqualifies them from federally-funded Medicaid (often because of lawful residence for less than five years). Coverage through BHP must be as comprehensive and affordable as subsidized coverage in the marketplace, though states can provide coverage beyond the essential health benefits and lower consumer costs. States implementing BHP receive 95% of what the federal government would have spent to subsidize BHP enrollees had they received marketplace coverage. While the ACA authorized states to implement BHP beginning January 2014, delays in issuing BHP regulations prevented states from implementing the program until January 2015.
Prior State Coverage in Minnesota and New York
In New York and Minnesota, state health programs predating the ACA made BHP a particularly appealing option. Before the ACA, both Minnesota and New York had health programs, funded in whole or in part by state dollars, that served much of the BHP-eligible population. These programs furnished more affordable and, in some cases, more comprehensive coverage than what federally subsidized qualified health plans (QHPs) offer in health insurance marketplaces under the ACA. BHP let states maintain such pre-ACA coverage while achieving fiscal gains by replacing state dollars with federal BHP funds.
Minnesota’s pre-existing coverage program, MinnesotaCare (MNCare), was originally created in 1992 to provide working people with access to affordable health coverage.1 By 2011, the program served children, parents, and pregnant women up to 275% FPL and childless adults with incomes up to 250% FPL through a Medicaid Section 1115 waiver.2 Prior to 2015 the program was funded by a state tax on medical providers and health plans (covering 48% of costs in 2012), federal medical assistance matching dollars (44%), and sliding-scale premiums paid by enrollees (8%).3 Anticipating a switch to BHP, the state authorized changes to the program in 2013. These changes included limiting adult’s eligibility to 200% FPL and adding lawfully present non-citizens with incomes below 138% FPL as well as eliminating asset limits and a cap on covered hospital services.4 BHP implementation meant that, instead of standard federal matching funds, the state would receive 95% of the amount that BHP consumers would otherwise have received in marketplace subsidies, which was expected to yield significant state budget savings.
New York provided state-funded coverage to lawfully present immigrants ineligible for federal Medicaid. The 2001 New York Court of Appeals decision in Aliessa v. Novello required the state to provide Medicaid to otherwise eligible lawfully present immigrants for whom the state was denied federal Medicaid funds. Some had been lawful residents for less than five years, others were Permanently Residing Under Color of Law in categories outside those qualifying for federal Medicaid funding.5 New York covered this population with state-only dollars before it implemented BHP. Following the implementation of BHP, the federal government, through BHP payments, assumed much of the cost of covering this population.6 These savings were anticipated to provide significant state budget gains even as BHP offered coverage substantially more affordable than subsidized QHPs to adults with incomes between 138% and 200% FPL.
Overview of BHP in Minnesota and New York
Minnesota was the first state to adopt the BHP. Minnesota converted MNCare to BHP effective January 1, 2015. The primary effect was financial—the source of federal funding shifted from Medicaid to BHP. Consumers were able to remain in the same plans and received the same benefits and cost-sharing protections as before. Regardless of the health plan they choose, MNCare enrollees pay premiums and cost-sharing on the same sliding scale, beginning at 35% FPL, and all enrollees receive the same benefits.
New York provided BHP, termed “the Essential Plan (EP),” to immigrants starting in April 2015, adding adults between 138-200% FPL effective January 1, 2016. New York offers four EP products—known as EPs 1, 2, 3, and 4. EP 1 and 2 are for those with incomes 151%-200% FPL (EP 1) and 139%-150% FPL (EP 2). EP 3 and 4 serve immigrants between 100-138% FPL (EP 3) and under 100% FPL (EP 4).7 Benefits and cost-sharing vary across the four EP categories, though within each category all health plans offer the same coverage at the same cost to consumers. For immigrants, the 2015 move to EP involved financial accounting, without affecting consumers’ coverage. In 2016, benefits and cost-sharing remained largely unchanged, but immigrants were moved from Medicaid to EP plans. In some cases, immigrants needed to choose a new health plan. Adults with incomes 138%-200% FPL who were previously enrolled in QHPs transitioned into EP during the 2016 open enrollment period (OEP).
Table 1 describes key aspects of BHP in each state.
Table 1: Key BHP Features in Minnesota and New York
Minnesota (MinnesotaCare)
New York (Essential Plan)
Overall Approach
Program Structure
Single product, regardless of income or immigration status
Premiums and cost sharing above 35% FPL, with exceptions
4 products: EP 1 and 2 for 138-200% FPL; EP 3 and 4 for immigrants at or below 138% FPL
Benefits, premium, and cost-sharing requirements vary between EP programs, but within each program are the same for all health plans
Premiums, Cost-sharing, and Benefits
Premiums
Premiums on a sliding scale, 35-200% FPL: $4/month to $80/month
No premiums for those under age 21, American Indians and family members, military members completing a tour of active duty within last 24 months
No premiums at or below 150% FPL
$20/month premium for between 151% and 200% FPL
Cost-sharing
No deductible; (statutory $2.95 monthly deductible waived by all insurers)
Modest co-payments
No copays for those under age 21 and American Indians
No deductibles
Modest co-payments above 100% FPL
Benefits
Essential health benefits
Dental care, vision, and enhanced behavioral health services covered
EP 1 and 2: Essential health benefits covered
Enrollees in EP 1 and 2 can purchase dental and vision coverage at full cost
EP 3 and 4: Additional benefits approximate Medicaid coverage
Enrollment/Disenrollment
Enrollment Policy
Enrollment open year round
Enrollees must report changes in circumstance within 30 days
Enrollment open year round
Enrollees must report changes in circumstance
Grace Period
30-day grace period; can avoid coverage gap by paying past-due and current premiums by the end of the grace month
90-day lock-out period if enrollees fail to pay past-due and current premiums; after 90 days, can re-enroll without penalty
30-day grace period; can avoid coverage gap by paying past-due and current premiums by the end of the grace month
Health Plan Contracting
Approach to contracting
Joint procurement with Medicaid
Marketplace issues Invitation to Participate to insurers; rates set by Medicaid agency (> Medicaid rates)
Health plan overlap
Plans must serve both Medicaid and MNCare
At least one Medicaid/MNCare plan in each county also participates in the marketplace
1 of 13 plans offering EP coverage also participate in Medicaid and the marketplace
Provider networks
Provider networks broader in MNCare compared to QHPs
Generally, 85% overlap between EP and QHP provider networks.
In some areas, EP provider networks narrower than Medicaid
Program Administration
Administration
Administered by Medicaid agency; some responsibilities shared with marketplace
Program operations shared between Medicaid and the marketplace
Financing
Costs
Projected FY2017 costs: $608 million
Projected FY2017 costs: $2,461 million
Source of funding
Federal BHP payments: 68%; State funds: 26%; Consumer premiums: 6%
Federal BHP payments: 85%; State funds: 15%
Key Findings
Program Design
Premiums, Cost-Sharing, and Benefits
BHP programs in Minnesota and New York provide coverage without deductibles and with lower premiums than what consumers would pay for subsidized marketplace plans. In New York, EP premiums were set by the state legislature at $20 per individual for those with incomes above 150% FPL and at or below 200% FPL. Enrollees with incomes up to 150% FPL do not pay premiums.8 In contrast, enrollees in MNCare pay premiums on a sliding scale from 35% FPL to 200% FPL,9 except for specified exempt groups.10 In both states, BHP premium payments are less than what consumers would have paid for the second-lowest-cost silver plan in the marketplace (Table 2).11 BHP enrollees face no deductibles in either state. Although the Minnesota statute provides for a $2.95 monthly MNCare deductible, all BHP plans waive the deductible. Stakeholders noted that consumers greatly valued the absence of deductibles in both states’ BHP programs.
Table 2: 2016 Monthly Premiums for BHP and QHPs
Income
MinnesotaCare
Essential Plan
QHP Benchmark Planwith Premium Tax Credits
35% FPL
$4
$0
$7
140% FPL
$25
$0
$48
151% FPL
$37
$20
$61
200% FPL
$80
$20
$126
SOURCE: Minnesota Department of Human Services, MinnesotaCare Premium Estimator Table, (Minnesota Department of Human Services, 2015); New York State of Health, Attachment F – BHP Product Offering and Cost-Sharing (New York State of Health, 2015); Kaiser Family Foundation, 2016 Health Insurance Marketplace Calculator (QHP premiums calculated based on US average premium for single-person household).NOTE: BHP is called “MinnesotaCare” and “Essential Plan” in Minnesota and New York, respectively.
In New York, other BHP cost-sharing is also lower than for subsidized marketplace plans. EP plans 1 and 2 have actuarial values (AV) above 95% while EP plans 3 and 4 mirror cost-sharing in Medicaid. A plan’s AV is the percentage of the cost of covered services the plan is expected to pay on average for a typical group of enrollees. Thus, a higher AV plan will lower the share of costs borne by enrollees. Consumers with income at or below 250% FPL are eligible for cost-sharing reductions (CSR) in the marketplaces, which raise the AV of standard QHPs. However, BHP coverage in New York pays a higher proportion of out-of-pocket costs than QHPs with these CSRs. For consumers with incomes up to 150% FPL, QHPs with CSRs offer 94% AV, and for those with incomes between 151-200% FPL, QHPs with CSRs provide 87% AV. Stakeholders noted that when consumers with incomes between 138% and 200% FPL enrolled in New York QHPs, they were charged copayments above BHP levels for office visits, hospital utilization, and prescription drugs, and those with incomes between 150% and 200% FPL also faced $250 deductibles (Table 3). New York advocates pushed hard for low cost-sharing in BHP and were happy with the state’s decisions.
Table 3: For New York Consumers Between 138-200% FPL, Cost-Sharing in BHP vs. QHPs with CSRs
138-150% FPL
151-200% FPL
BHP
QHP with CSRs
BHP
QHP with CSRs
Deductible (single)
$0
$0
$0
$250
Max out-of-pocket limit (single)
$200
$1,000
$2,000
$2,000
Copayments
PCP
$0
$10
$15
$15 (after deductible)
Specialist
$0
$20
$25
$35 (after deductible)
Inpatient hospital
$0
$100 per admission
$150 per admission
$250 per admission (after deductible)
ER Visit
$0
$50
$75
$75
Tier 1 drugs
$1
$6
$6
$9
Tier 2 drugs
$3
$15
$15
$20
Tier 3 drugs
$3
$30
$30
$40
SOURCE: 2017 Invitation for Participation in New York State of Health, Attachment F – BHP Product Offering and Cost-Sharing, NY State of Health, 2015.NOTE: New York refers to BHP as the “Essential Plan,” or EP. Cost-sharing and premiums vary between EP 1, which serves consumers between 151-200% FPL, and EP 2, which covers consumers at 138-150% FPL. QHPs with CSRs are from the 2015 New York marketplace.
Minnesota increased BHP premiums and cost-sharing in 2015, but the resulting amounts are still lower than what consumers would have faced in the marketplace. In 2015, the Minnesota legislature increased MNCare premiums for enrollees with incomes 150%-200% FPL. The amount of the increase was scaled to income, with a 28% rise for those with incomes between 150%-159% FPL increasing to a 60% boost for those with incomes at 200% FPL. However, as shown in Table 2, these amounts are still lower than the premiums consumers would have been charged in the marketplace for subsidized QHPs with benchmark premiums. The legislature also lowered the AV of MNCare plans from 98% to 94%, bringing cost-sharing in line with marketplace coverage for those with incomes at or below 150% FPL. The resulting cost-sharing remained under the amounts charged in the marketplace for those between 150% FPL and 200% FPL, who in non-BHP states are offered QHPs with 87% AV.12 Minnesota’s premium and cost-sharing increases went into effect in August 2015 and January 2016, respectively, and were expected to yield an estimated $27.8 million in additional revenue over 23 months.13
Table 4: MinnesotaCare Premium and Cost-Sharing Changes
Cost-Sharing Changes
Through Dec. 31, 2015
Effective Jan. 1, 2016
Deductible
$0
$0
Nonpreventive office visits
$3
$15
Mental health visits
$0
$0
ER visits (does not apply if admitted)
$3.50
$50
Inpatient hospital admission
$0
$150
Prescription drugs (generic)
$3
$6
Prescription drugs (brand name)
$3
$20
Prescription drug OOP monthly maximum
None
$60
SOURCES: Minnesota Department of Human Services, Bulletin: Legislative Changes to Medical Assistance and MinnesotaCare, Minnesota Department of Human Services, July 2015, http://www.dhs.state.mn.us/main/groups/publications/documents/pub/dhs16_195870.pdfRandall Chun. MinnesotaCare Information Brief, Research Department of the Minnesota House of Representatives, updated January 2016, http://www.house.leg.state.mn.us/hrd/pubs/mncare.pdfNOTE: Minnesota statute provides for $2.95 monthly deductibles in MNCare, but all plans waive those deductibles. BHP is called “MinnesotaCare” in Minnesota.
For many BHP enrollees, benefits are broader than with QHPs. MNCare consumers receive, in addition to what QHPs offer, oral health services, vision services, and enhanced behavioral health coverage. In New York, EP 1 and 2 offer the same benefits as QHPs. EP 3 and 4 approximate Medicaid benefits by covering non-prescription drugs, orthotic devices, orthopedic footwear, adult vision care, adult dental care, and non-emergency transportation (administered by the Department of Health), in addition to QHP services.14 EP 1 and 2 do not cover adult vision and dental care as part of the standard benefit package; to obtain those benefits, consumers must pay the additional premium from insurers that offer coverage for such services.15
Contracting with Health Plans
Most BHP insurers also participate in Medicaid and/or the marketplace. In both states, officials sought to have the same plans and provider networks available in Medicaid, BHP, and QHP. Such an overlap promotes continuity of care when consumers’ income changes and they move between programs. In Minnesota, the state conducted a joint procurement for Medicaid and BHP; plans wishing to join one program had to participate in both. In each county, consumers can choose between two or three Medicaid/MNCare plans, at least one of which also offers marketplace coverage.16 In New York, 13 insurers offer EP, 11 of which participate in all three programs.17 State officials reported that, in 2016, EP consumers have a choice of plans in all but two rural counties. For 2017, state officials indicated that all counties will have a choice of plans.
BHP health plan payments were based on Medicaid rates then adjusted for the BHP population. State officials in Minnesota reported that the capitation rates for Medicaid and MNCare were similar in 2016. However, the joint procurement for both programs included rebidding prior managed care contracts. By leveraging Medicaid participation, and because BHP enrollees proved healthier than the historical MNCare population, the state was able to negotiate MNCare capitation rates that were 15% lower than expected. In New York, the rates for EP 3 and 4 were set at the Medicaid rate, while rates for EP 1 and 2 were based on the Medicaid rates then adjusted to reflect differences between Medicaid and EP utilization patterns, covered benefits, and cost-sharing rules. These adjustments raised rates for EP 1 and 2 20% above Medicaid levels.
Provider Networks
In Minnesota, provider networks are broader in BHP than the marketplace; the picture is more varied in New York. According to state officials, despite lower provider payments in BHP than the marketplace, Minnesota’s BHP plans offered broader networks; BHP plans included all Medicaid providers, while QHPs used narrow networks to restrain premiums. The greater breadth of Medicaid/BHP networks over QHP networks was particularly significant with dental care, behavioral health care, and Mayo Clinic providers. In New York, the picture was more complex; some consumers who moved from QHPs to BHP lost access to previous providers. In most cases, New York insurers used their Medicaid provider networks for BHP; however, some insurers’ BHP networks were more limited than their Medicaid provider networks. A number of stakeholders saw this as a transitional effect that would likely diminish or disappear over time.
Having similar provider networks across the three coverage programs facilitated New York consumers’ transition to EP. Beginning in January 2016, consumers previously enrolled in QHPs were transitioned to new EP plans. State officials reported that consumers could automatically renew in “sister” EP plans, those that were offered by the same carrier and that had at least 85% of their providers participating in both plans. Consumers had the option to change insurers for the 2016 plan year, rather than auto-renew. Some consumers whose QHPs were not offered by an EP-participating carrier could not auto-enroll and had to affirmatively select an EP plan.
Impact on Consumers
BHP enrollment
Enrollment increased substantially following BHP implementation in New York. Implementation of EP in New York in 2016 provided a natural experiment testing the impact of increased affordability on enrollment. Among adults with incomes 150-200% FPL—all of whom moved from federally-subsidized QHPs to EP—enrollment grew by 42% between 2015 and the end of the 2016 open enrollment period (OEP), an increase of 52,000 enrollees. By contrast, enrollment increased by only 4% among adults with incomes 200-400% FPL, whose subsidy eligibility was unaffected by BHP implementation (Figure 1).18 Overall, enrollment among those with incomes from 138% – 200% FPL, who moved from the marketplace into BHP, rose 35% (from 166,000 to 224,000). Compared to those with incomes 150%-200% FPL, enrollment growth among BHP enrollees with incomes 138%-150% FPL was less pronounced. In 2015, nearly half of those in the latter group (19,000 out of 40,000) were parents who received supplemental state subsidies that paid the full QHP premium.19 As a result, the affordability improvements from moving to BHP were much lower in magnitude for many in this group than for those with incomes between 150%-200% FPL.
Figure 1: New York Subsidized QHP and Essential Plan Enrollment, 2015-2016
In New York, those eligible for BHP were more likely to enroll than those determined eligible for subsidized QHP coverage. Among people who applied for 2016 coverage and qualified for BHP in New York, 98% continued through the enrollment process to select a plan.20 Only 58% did so among applicants who were found eligible for subsidized and unsubsidized QHPs, combined.21 Stakeholders reported that BHP increased participation because of both reduced premiums and the absence of deductibles. Lower out-of-pocket cost-sharing in BHP also appeared to improve consumers’ receipt of primary care, according to some stakeholders. According to state analyses, consumers enrolled in BHP averaged $1,100 in savings compared to what they would have paid for subsidized QHP coverage.22 Similar estimates were not available for Minnesota.
Stakeholders reported that MNCare’s greater affordability increased enrollment. Minnesota did not offer a comparable natural experiment to New York, since eligibility for BHP and subsidized QHP coverage did not change from 2014 through 2016. However, stakeholders believed that BHP’s lower premiums and out-of-pocket cost-sharing, compared to subsidized QHP coverage, contributed to enrollment growth following ACA implementation. Monthly MNCare enrollment increased from 79,000 in September 2014 to nearly 101,000 in September 2016.23 State officials noted that enrollment dipped slightly from 2015 to 2016 as systems issues that had delayed the renewal process were resolved and those who were no longer eligible transitioned off coverage.
BHP enrollees were reportedly younger and healthier than those in QHPs. Although detailed data enabling a comparison of demographic characteristics were not publicly available, carriers in New York reportedly were pleased that younger and healthier members signed up for EP, though officials noted that one year’s experience is a limited basis for generalization. Minnesota officials described BHP members as younger and healthier than both the Medicaid population and QHP enrollees. Officials in both states attributed these effects to the greater affordability of BHP compared to subsidized marketplace coverage.
Year-round BHP enrollment improved consumers’ access to coverage without harming the risk pool. Because of BHPs’ low premiums, stakeholders observed that consumers had little or no incentive to delay enrollment until illness or injury created a need for coverage. Carriers in both states thus report that year-round enrollment has not led to detectable adverse selection. The impact of year-round enrollment on total coverage levels may be significant. For example, New York State officials project that, between the end of the 2016 OEP and 2017, BHP enrollment will grow from nearly 380,000 to roughly 600,000.
Stakeholders reported that consumers valued the increased predictability and simplicity of BHP coverage, compared to marketplace plans. According to consumer groups and enrollment assisters, consumers appreciated the greater predictability and understandability of premiums, cost-sharing, plan networks, and benefits offered by BHP’s state-defined coverage, which remained constant from plan to plan. Consumers had no need to reengage with a rapidly changing and complex marketplace at open enrollment each year. That said, changes occur in state-administered systems, as illustrated by Minnesota’s increases in 2016 premiums and cost-sharing.24 Stakeholders noted that while some consumers complained about these changes, particularly increased out-of-pocket costs, coverage remained relatively affordable and understandable; enrollment thus did not decline.
Coverage Transitions
The two states varied in the integration of their eligibility systems. In both New York and Minnesota, the marketplace provides an online enrollment pathway for Medicaid, CHIP, BHP, and the marketplace. New York’s system determines eligibility for all programs and lets consumers complete the enrollment process online, preventing breaks in coverage both following the initial application and when consumers move between programs. However, a few thousand immigrants who were still in the state’s “legacy” Medicaid system had to be transferred manually. Minnesota’s marketplace system also provides eligibility determinations for Medicaid and MNCare; however, if verification or further follow-up is needed, the application is sent to counties to complete Medicaid enrollment or the state Department of Human Services (DHS) to complete MNCare enrollment. Stakeholders expressed concern that breakdowns can occur with the information transfer, leading to enrollment delays for some consumers and the possibility of some consumers not getting coverage. They noted that problems and delays are more likely to occur for families in which some members are eligible for Medicaid and others qualify for MNCare.
BHP enrollees whose incomes rise above 200% FPL experience steep cost increases when they move to QHPs. In federally subsidized QHPs, these enrollees face both higher premiums and higher cost-sharing, including deductibles, which BHP plans do not charge. Compared to Minnesota, the cliff is steeper in New York because BHP coverage is less costly to consumers; but in both states, stakeholders indicated that the combination of higher premiums along with deductibles of $1,500 or more for consumers moving into QHPs poses real financial challenges. They further noted that the cliff existed prior to BHP implementation when consumers moved from Medicaid to QHP coverage; however, it was not as steep because the marketplace subsidies are more generous at 139% FPL than 200% FPL. While stakeholders expressed concern over this cliff, they felt that this highlighted the importance of BHP as a more affordable coverage option.
Minnesota is exploring ways to expand BHP coverage beyond the current eligibility levels. To address affordability concerns above 200% FPL and to lessen the severity of the current “cliff,” a multi-stakeholder task force in Minnesota recommended expanding BHP to 275% FPL. Advocates in New York have called for a similar discussion of options to improve affordability for higher income marketplace enrollees.
Impact on the Marketplace
BHP did not appear to harm administrative funding for marketplaces. In Minnesota, financing for the state’s marketplace, MNsure, comes from a 3.5% assessment on QHP premiums sold through the marketplace.25 By covering consumers with incomes under 200% FPL who would have otherwise enrolled in the marketplace, BHP reduced this assessment revenue. However, Minnesota applies standard federal cost-allocation principles to marketplace activities, including eligibility determination, application assistance, and public education, that benefit Medicaid and BHP. As a result, MNsure receives payments from DHS to support marketplace operations. State officials reported that these cost-allocation payments for Medicaid and BHP consumers provided the marketplace with adequate and stable administrative funding. New York finances its marketplace through a broad-based assessment on plans inside and outside the marketplace. Consequently, adopting the BHP did not affect New York marketplace revenues.
BHP did not appear to affect marketplace stability. In New York, officials who worried about marketplace effects before program implementation reported that, after implementation, those worries proved unwarranted as marketplace stability remained unaffected. In Minnesota, the marketplace has experienced significant upheaval, with many carriers reporting losses, some high-profile plan exits, and significant premium increases (particularly for 2017). State officials and most stakeholders believed that BHP was not responsible for those problems. They attributed the marketplace’s challenges to carriers’ initial underpricing of QHP premiums; the state’s high-risk pool ending in 2015, which shifted many high-cost consumers to QHPs; federal underfunding of risk-corridor payments; and other causes unrelated to BHP. However, carriers suggested that the reduced size of the marketplace due to BHP may have made its risk pool more vulnerable to enrollment by relatively few high-cost consumers. In New York and Minnesota, BHP had a minimal impact on overall risk levels and premiums in the individual market, according to officials.
Impact on State Administration and Financing
BHP Administration
Existing state agencies administer BHP in both states. In both New York and Minnesota, the Medicaid program assumes most administrative responsibilities for BHP, with the marketplace taking on some tasks. According to stakeholders, because MNCare was once a Medicaid waiver program, the Medicaid agency assumes overall programmatic responsibility for BHP. In New York responsibilities are shared between Medicaid and the marketplace, both of which are housed in the state’s Department of Health. For example, Minnesota’s Medicaid agency both contracts with BHP plans and sets BHP rates; and in New York the marketplace contracts with plans, while the Medicaid program sets payment rates. Relying on existing infrastructure for BHP administration reduced administrative costs. Stakeholders in New York also noted that using existing agencies helped create a smoother launch with BHP than had been observed with other new health programs. According to stakeholders, neither state covered BHP administrative costs through premium assessments on BHP plans. Based on guidance from the Centers for Medicare and Medicaid Services, such assessments can be funded through federal BHP allotments, since fees and taxes are absorbed into BHP premiums.26
Coordination among state agencies is generally effective in both states, though there have been some challenges. Given the shared responsibilities for BHP program administration between Medicaid and the marketplaces, stakeholders noted that strong communication and coordination between the agencies was essential. Officials in both states reported having good working relationships with their sister agencies and felt the administrative structure supported effective program administration. Operationally, stakeholders in Minnesota noted some challenges related to the state’s multiple eligibility systems. They felt that better coordination around business processes might help to lessen enrollment delays some consumers face as they move between programs.
BHP Costs and Financing
The study states achieved significant savings by moving individuals from older coverage programs into BHP. According to state officials, New York saved an estimated $1 billion in state fiscal year (SFY) 2016 by using federally-funded BHP to cover approximately 250,000 lawfully present immigrants who had previously received state-funded Medicaid. Even though the state incurred new costs for non-immigrant BHP enrollees, the state still realized more than $800 million in net savings. Minnesota likewise anticipated fiscal gains from transitioning consumers out of a Medicaid waiver program, for which the state paid nearly 50% of all costs, into BHP. However, the state did not experience anticipated financial relief in 2015. Federal BHP payments are based on QHP premium levels, and the state’s unexpectedly low initial QHP premiums reduced 2015 federal BHP funding below projected levels. Higher QHP premiums in 2016 increased federal BHP funding. In addition, legislatively-mandated increases in premium and cost-sharing requirements along with a healthier-than-expected BHP population, both of which are discussed above, lowered BHP program expenditures. As a result of these combined factors, Minnesota’s BHP provided budget gains in 2016 that were greater than originally anticipated.
State contributions are required to cover a portion of BHP costs in both states. For several reasons, including federal BHP payments provide only 95% of what the federal government would have spent on subsidies had BHP enrollees received marketplace coverage; BHP coverage in both Minnesota and New York is more generous than federally-subsidized QHP coverage; and BHP pays plans more than Medicaid, federal financing does not fully cover BHP program costs. In New York, projected EP costs for FY 2017 are $2,461 million. Federal BHP payments are expected to pay 85% of the costs, and state general operating funds will cover 15%, or $377 million.27 In Minnesota, projected costs for MNCare for FY 2017 are $608 million. Federal BHP payments are projected to cover 68% of these costs; consumer premium contributions will finance 7%; and the state will contribute 26% (Figure 2).28 Stakeholders in Minnesota expressed concern about future funding for BHP. The state relies on a 2% provider tax to finance BHP, among other programs. Originally, the provider tax paid many costs, such as for the state’s high-risk pool, that are no longer needed following ACA implementation. In 2014, the state legislature repealed the provider tax effective December 2019, but did not establish an alternative financing mechanism for BHP. While near-term funding will be available, and BHP enjoys widespread support among policymakers and stakeholders, the long-term implications for the program are unclear. Stakeholders in both Minnesota and New York believed that stable funding sources for both the marketplace and BHP were critical to ensuring the programs’ future. An important open question is how much the rise in QHP premiums for 2017 and beyond, which will increase federal BHP payments, will lower state BHP costs.
Figure 2: Projected Sources of BHP Financing in Minnesota and New York, Fiscal Year 2017
Lessons Learned
Following the outcome of the 2016 elections, the future of BHP and other Affordable Care Act provisions is unclear. Despite this uncertainty, the experiences of Minnesota and New York with BHP suggest broader lessons about effective coverage programs for low-income consumers.
Substantial enrollment gains and an improved risk pool can result when low-income consumers are offered coverage much more affordable than federally subsidized marketplace plans. New York’s “natural experiment” with BHP demonstrates the significant enrollment gains, including among the relatively young and healthy, that can be achieved by reducing this group’s premiums below subsidized QHP levels and eliminating deductibles.
Many consumers preferred the stability and simplicity of state-defined coverage to the marketplace’s complexity and unpredictability. Stakeholders reported that many low-income consumers found marketplace coverage confusing and hard to negotiate, preferring the consistency of state-administered coverage in which premiums, cost-sharing, and benefits were the same across participating plans. Consumers likewise appreciated the ability to stay in the same BHP plan without the need to “shop” each year to avoid large premium increases.
Encouraging plans and providers to participate across all coverage programs can promote continuity of care. Overlap of plans and networks promotes continuity of provider relationships and care when consumers move between programs because of changing household circumstances. In addition, Minnesota found that conducting joint procurement for Medicaid and BHP achieved savings in both public programs, broadened BHP provider networks beyond QHP levels, and increased the state’s leverage to implement delivery-system and payment reforms.
Relying on existing infrastructure to administer new coverage programs can create efficiencies and avoid duplication. Both Minnesota and New York administered BHP primarily through the Medicaid agency, thereby lowering BHP administrative costs. Neither state created new administrative structures to run BHP.
Conclusion
When federal officials announced that regulatory delays prevented states from implementing BHP until 2015, all states considering BHP put that option aside, except for Minnesota and New York. The latter states’ experiences highlight the potential for BHP to make coverage more affordable for those with incomes between 138-200% FPL. Both states set premiums and cost-sharing levels below those in the marketplace. Significant enrollment gains resulted when New York transitioned consumers from subsidized QHPs to BHP. Moreover, notwithstanding marketplace instability in Minnesota that most observers attribute to other factors, BHP does not appear to be a major factor undermining marketplace viability in either state.
Although the 2016 election results create uncertainty around the future of the ACA (including BHP), BHP implementation provides important lessons about structuring coverage programs for low-income uninsured consumers for consideration in future reforms. Significant enrollment gains and risk-pool improvements can result when low-income consumers are offered insurance that is substantially more affordable than federally subsidized marketplace coverage. Moreover, many consumers prefer the simplicity and predictability of a state-administered program, with uniform costs and benefits, to the changing, complex coverage offered in a health insurance marketplace.
New York requires insurers to follow the BHP naming convention in naming their products to ensure that consumers can easily identify BHP plans. “Essential Plan 1” is the product for individuals with incomes between 150 and 200% FPL, “Essential Plan 2” is the product for individuals with incomes between 138 and 150% FPL, “Essential Plan 3” is the product for individuals with incomes between 100 and 138% FPL who are not eligible for Medicaid due to immigration status, and “Essential Plan 4” is the product for individuals with incomes at or below 100% FPL who are not eligible for Medicaid due to immigration status. ↩︎
Individuals under age 21, American Indians and Alaska Natives and their family members are exempt from premiums, and members of the military who have completed a tour of active duty within 24 months and their family members are exempt from premiums for 12 months. Medicaid.gov, Minnesota’s Basic Health Program Blueprint, (Medicaid.gov, April 2016), https://www.medicaid.gov/basic-health-program/downloads/minnesota-bhp-blueprint.pdf↩︎
Because neither Minnesota nor New York enrolled BHP individuals into the marketplace in 2016, a direct comparison of what those individuals would have paid in premiums is not possible. The estimates included in the Table are based on a household size of 1. While the estimates were calculated based on the US average premium for a single adult age 40, the actual consumer costs at the applicable income levels are based entirely on family income when consumers purchase benchmark-priced coverage. Source: Kaiser Family Foundation, 2016 Health Insurance Marketplace Calculator, https://modern.kff.org/interactive/subsidy-calculator-2016/↩︎
Peter Newell and Nikhita Thaper. New York’s Temporary Premium Subsidies: Meeting Immediate Goals and Yielding Useful Lessons. United Health Fund, June 2016. https://www.uhfnyc.org/assets/1492↩︎
Centers for Medicare and Medicaid Services. “Basic Health Program: State Administration of Basic Health Programs; Eligibility and Enrollment in Standard Health Plans; Essential Health Benefits in Standard Health Plans; Performance Standards for Basic Health Programs; Premium and Cost Sharing for Basic Health Programs; Federal Funding Process; Trust Fund and Financial Integrity.” Federal Register. Vol. 79, No. 48 (March 12, 2014): 14112-14151 at 14133, http://www.gpo.gov/fdsys/pkg/FR-2014-03-12/pdf/2014-05299.pdf, as discussed in Stan Dorn and Jennifer Tolbert, The ACA’s Basic Health Program Option: Federal Requirements and State Trade-Offs, (Kaiser Commission on Medicaid and the Uninsured and the Urban Institute, November 2014), https://modern.kff.org/health-reform/report/the-acas-basic-health-program-option-federal-requirements-and-state-trade-offs/↩︎