KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Medicaid’s Money Follows the Person (MFP) demonstration provides states with enhanced federal matching funds for services and supports to help seniors and people with disabilities move from institutions to the community. Over 90,000 people have participated in MFP from 2007 through June 2018.
With a short-term funding extension set to expire on December 31, 2019, MFP’s future remains uncertain for the 44 states participating in the program, without a longer-term reauthorization by Congress. Twenty percent of MFP states will have exhausted their current funds by the end of 2019, and the vast majority of the remaining states expect to do so during 2020.
Over one-third of MFP states identified a range of services that they expect to discontinue if federal funding expires, with community transition services most often cited. States also expect that they will not be able to maintain staff and activities focused on enrollee outreach and community housing, which are financed with enhanced federal matching funds.
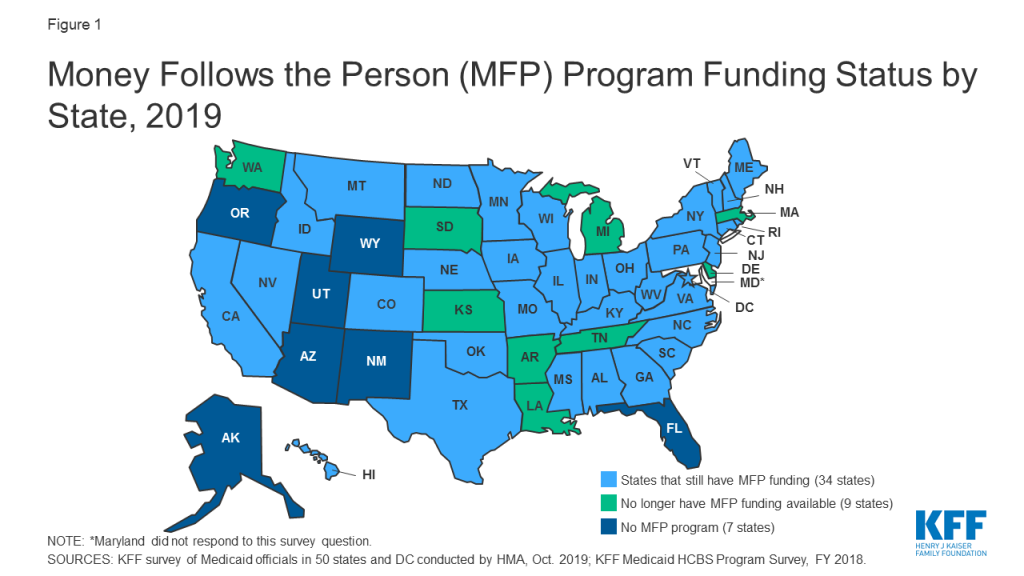
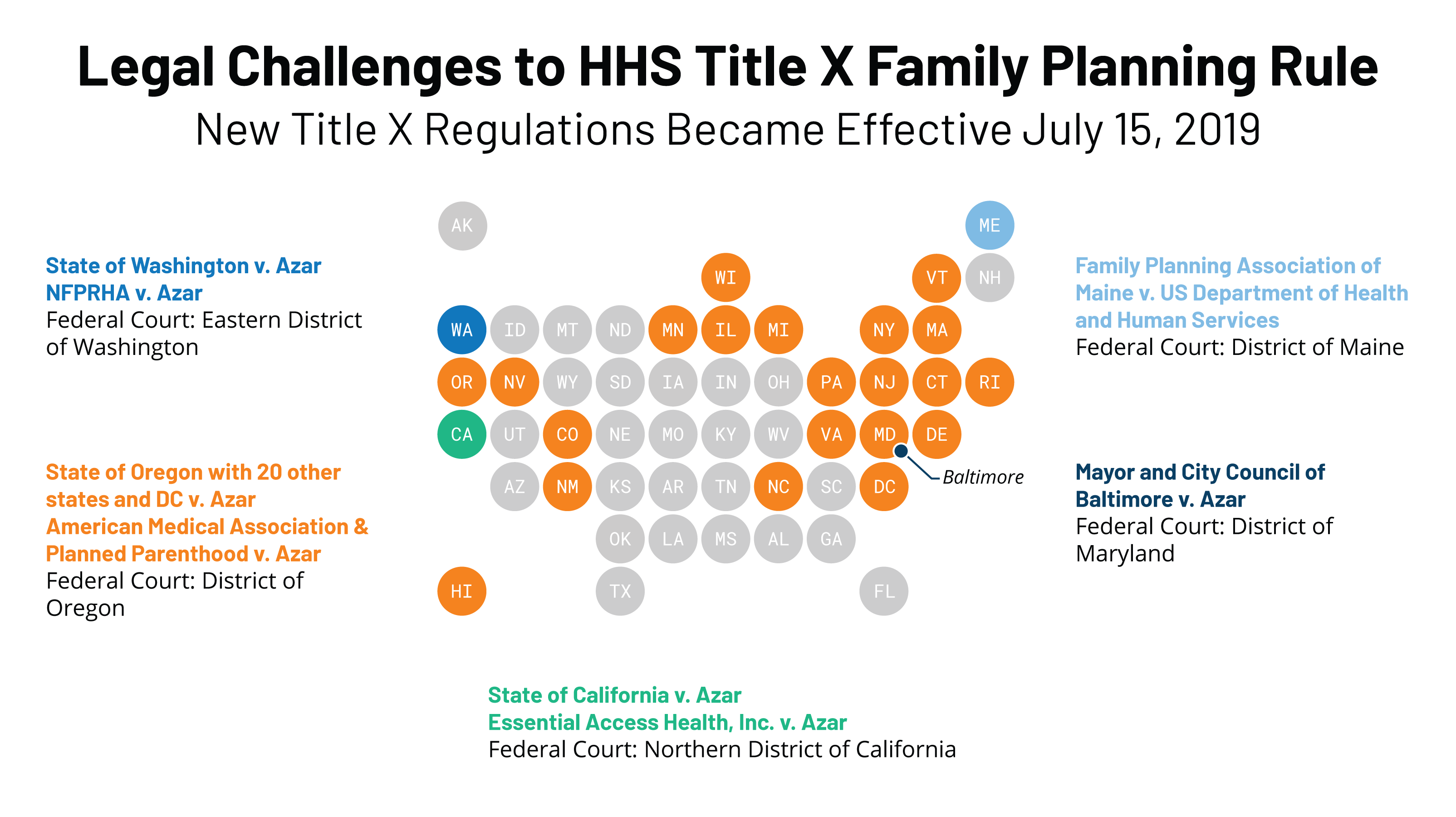
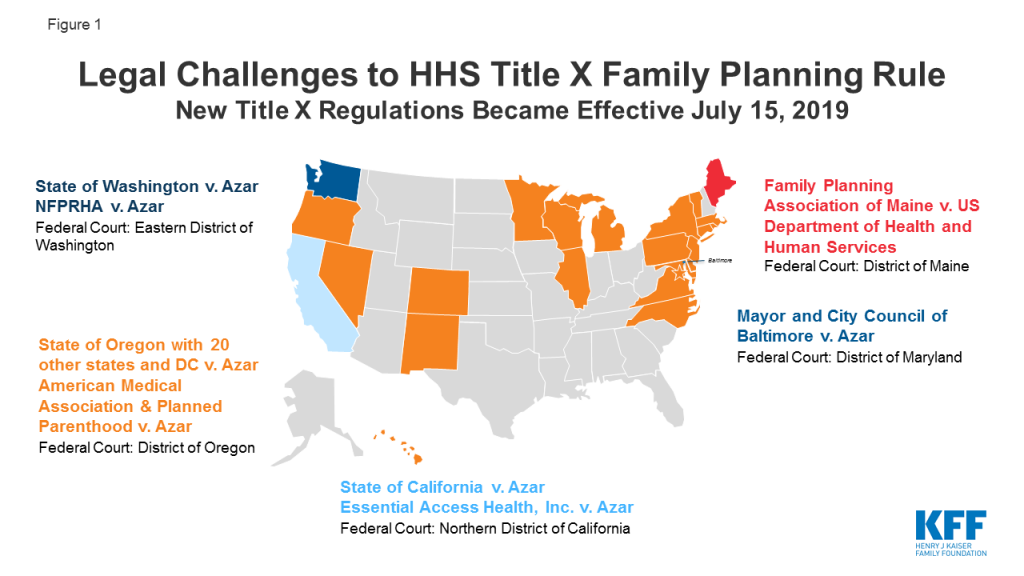
Medicaid’s Money Follows the Person (MFP) demonstration has helped seniors and people with disabilities move from institutions to the community by providing enhanced federal matching funds to states since 2007.1 The program operates in 44 states (Figure 1 and Table 1), and has served over 90,000 people as of June 2018.2 Box 1 below provides more information about the MFP population, services, and financing. MFP seeks to reduce the Medicaid program’s institutional bias, which exists because nursing facility services must be covered, while most home and community-based services (HCBS) are provided at state option. The program is credited with helping many states establish formal institution to community transition programs that did not previously exist by enabling them to develop the necessary service and provider infrastructure.3 It also has been a catalyst for states to develop housing-related activities as states have used MFP funds to offer housing-related services and hire housing specialists to help beneficiaries locate affordable accessible housing, which is routinely cited as a major barrier to transitions.4
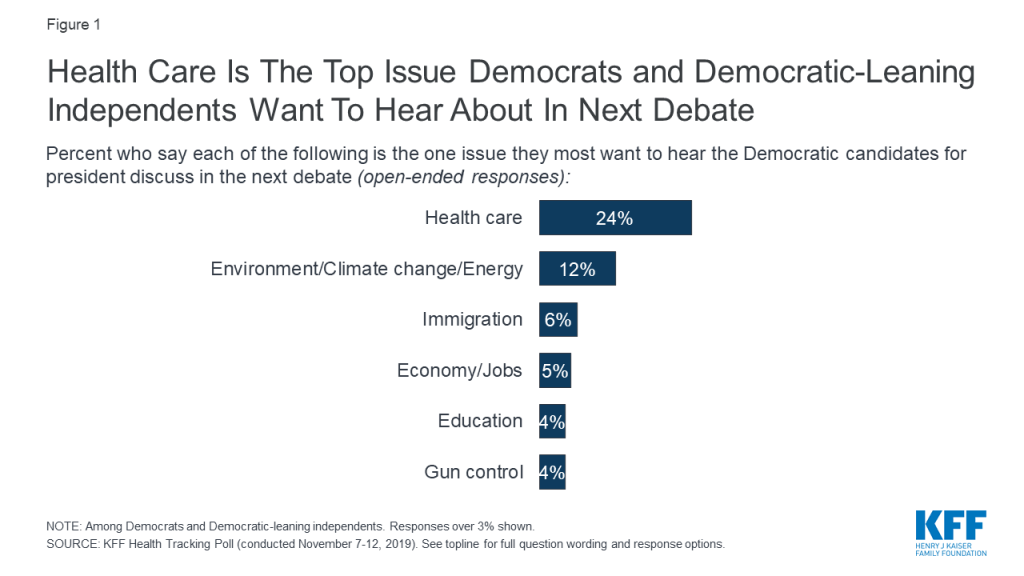
Figure 1: Money Follows the Person (MFP) Program Funding Status by State, 2019
With a short-term funding extension set to expire on December 31, 2019, MFP’s future remains uncertain without a longer-term reauthorization by Congress. MFP is a federal grant program created as part of the Deficit Reduction Act of 2005, and subsequently extended by the Affordable Care Act, with total funding increased to $4 billion.5 Although states were set to fully phase-out their MFP programs in federal fiscal year 2020, Congress has provided $254.5 million in additional funds in three short-term extensions of the program through December 2019.6 This issue brief highlights new data about the status of states’ MFP funding and the services and activities that would be affected if the program is not reauthorized. The brief draws on data from the Kaiser Family Foundation’s most recent 50-state Medicaid home and community-based services (HCBS) survey and 50-state Medicaid budget survey.
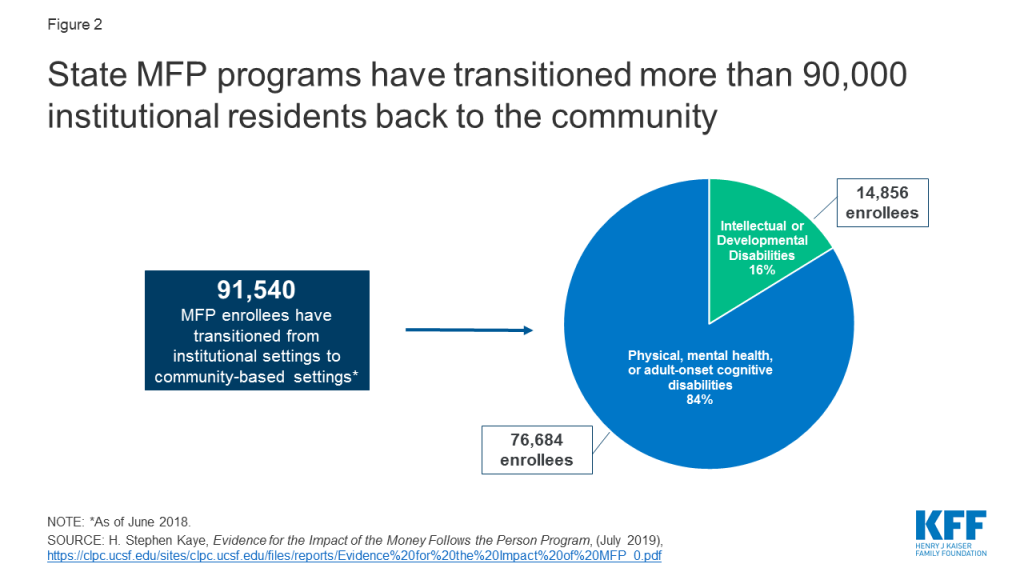
Figure 2: State MFP programs have transitioned more than 90,000 institutional residents back to the community
Box 1: MFP Enrollees, Services, and Financing
Over 90,000 people have moved from institutions to the community with support provided by MFP from 2007 through June 2018. Over 80 percent of MFP enrollees are people with physical, mental health, or adult-onset cognitive disabilities, and less than 20 percent are people with intellectual or developmental disabilities (I/DD) (Figure 2). While people with mental health disabilities comprise a small share of all MFP enrollees, states increasingly have focused on meeting this population’s typically greater needs as MFP programs became more established. One study shows a 77 percent increase in cumulative transitions for people with mental health disabilities in less than two years (1,790 in 2013 to 3,174 in mid-2015).7
MFP’s enhanced matching funds are available for HCBS to support beneficiaries during their first year in the community, after residing in an institution for more than 90 consecutive days. States receive an enhanced matching rate (within a range of 75% to 90%8 ) during the first year that an enrollee lives in the community for Medicaid HCBS that are covered through the state plan benefit package or a waiver. These services typically include personal care, adult day health, case management, homemaker, habilitative, and respite. States also receive the enhanced matching rate for “demonstration services,” which are additional HCBS provided during the enrollee’s first year in the community and in a manner or amount not otherwise available to Medicaid enrollees, such as transition coordination services or additional personal care hours. Enhanced matching funds are drawn down from the state’s MFP grant. From 2007 through 2016, states were awarded MFP grants ranging from nearly $6 million in South Dakota to nearly $400 million in Texas.9 Through MFP, states also provide services to help beneficiaries overcome barriers to returning to community living after residing in an institution for an extended period. These “supplemental services,” such as security and utility deposits and household set up costs, are not necessarily long-term care in nature and are reimbursed at the state’s regular matching rate.
States must use their enhanced matching funds for initiatives to shift their long-term care spending in favor of HCBS over institutional care. The activities most frequently financed by enhanced matching funds include expanding HCBS waiver capacity, providing access to transition services, improving access to affordable accessible housing, engaging in outreach, training direct care workers and medical providers, developing enrollee needs assessments, and supporting administrative data and tracking systems.10
Key Findings
Twenty percent (9 of 44) of MFP states will have exhausted their current funds by the end of 2019, and the vast majority of the remaining states expect to do so during 2020. Seven states (KS, LA, MA, MI, SD, TN, and WA) already have exhausted their MFP funds, and two more (AR and DE) expect to do so by December 2019 (Figure 1 and Table 1). Thirty-four states report they have not yet expended all of their MFP funds, although the vast majority of this group anticipates that their current funding will be exhausted during 2020.11
Over one-third (15 of 44) of MFP states identified a range of services and other program activities and staff positions that they expect to discontinue if federal funding expires (Table 1). Community transition services were most often cited as being at risk of discontinuing once MFP funds are exhausted. Other services that states expect to discontinue include community case management, housing relocation assistance, and family caregiver training. Program staff positions and activities that states expect to discontinue without additional federal funding include outreach specialists, housing specialists, and training for care coordinators and providers, among other activities. States use their enhanced matching funds to finance initiatives to expand HCBS, as described in Box 1 above, and may not be able to continue these activities if federal funding is lost.
Just over one-quarter (12 of 44) of MFP states already have added new services to existing HCBS waivers in anticipation of federal funding expiring (Table 1). These include 12 waivers serving seniors and people with physical disabilities, 11 waivers serving people with I/DD, three waivers serving people with brain injuries, and one waiver serving people with mental health disabilities. All of these states have added transition services (CO, DE, GA, ID, IN, MA, ND, OH, SD, VA, WA, and WV) to support individuals in the community up to a year after leaving an institution. In addition, Michigan has a Section 1915 (i) HCBS state plan amendment awaiting CMS approval to add transition services for seniors and adults with physical disabilities to replace MFP funding. Several states added other services to their waivers in addition to transition services. For example, Colorado added life skills training, home delivered meals, and peer mentorship to six waivers, Massachusetts added orientation and mobility services, Ohio added community integration services, and Washington added goods and services.
Eight states report plans to add new services to an existing HCBS waiver in anticipation of MFP funds expiring (Table 1). Among these states, four already have added some services to an existing waiver (described in the prior paragraph, GA, ID, IN, OH) and also now plan to add other services, while four states are making these plans for the first time (IA, NE, NJ, SC). Georgia plans to add transition services to its two waivers that do not already include these services. Iowa plans to add three new services, including crisis response, behavioral programming, and mental health outreach, to its waiver serving people with I/DD. Nebraska is exploring adding tenancy services to its waiver serving seniors and adults with physical disabilities. South Carolina plans to add expanded goods and services and transition coordination services to three waivers serving people with HIV/AIDS, seniors, and people with physical disabilities. Ohio is planning to add coaching support services and community integration support services to two waivers serving seniors and people with physical disabilities. NJ is seeking to expand community transition services to add one-time clothing purchase and one-time pantry stocking.
Looking Ahead
With the help of MFP enhanced federal matching funds, states have invested in building and maintaining their transition programs, serving over 90,000 seniors and people with disabilities who have received the services and supports to move from institutions to the community. The national MFP evaluation found that enrollees experienced significant increases in quality of life measures after leaving an institution, and these increases were sustained two years after moving to the community.12 HHS’s report to Congress on MFP noted that “any dollar value placed on these improvements would not adequately reflect what it means for people with significant disabilities when they can live in and contribute to their local communities.”13
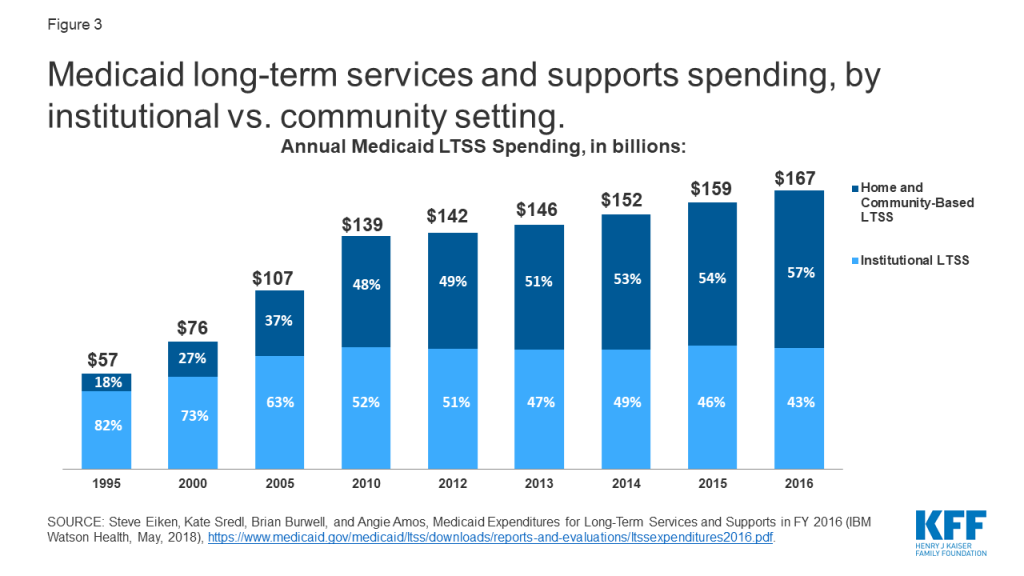
The national MFP evaluation found that some individuals would not have transitioned without MFP. After five years of program operation, about 25 percent of older adult MFP enrollees and half of those with I/DD in 17 states would have remained institutionalized without MFP.14 Additionally, MFP enrollees were less likely to return to an institution compared to those who transitioned without MFP.15 Other research has found declines in nursing home occupancy rates and reductions in the number of nursing home residents who never expect to return to the community in states with “robust” MFP programs compared to states without MFP or with a “minimal” program.16 All of these findings show that MFP has contributed to tipping the balance of long-term services and supports (LTSS) spending, with spending on HCBS surpassing spending on institutional care for the first time in 2013, and comprising 57% of total Medicaid LTSS spending as of 2016.17 MFP also has helped states control per enrollee spending, as providing enrollees with HCBS typically costs less than institutional care.18 The national MFP evaluation found that state Medicaid programs realized $978 million in savings during the first year after transition for MFP enrollees through 2013, though all of these savings could not be attributed to MFP. 19
MFP’s future remains uncertain, with current funding exhausted by the end of 2019 in 20 percent of MFP states and most of the remaining states expecting to run out of funds during 2020. While some states have added certain HCBS funded by MFP to other Medicaid authorities in anticipation of the funding expiration, over one-third of MFP states report that some HCBS funded by MFP as well as staff positions to support transitions, such as outreach and housing coordinators, are at risk of ending when federal funding for the program expires. While MFP has contributed to state progress in rebalancing LTSS to date, support would need to be ongoing for states to maintain this progress, especially as the demand for LTSS is expected to grow as the population ages. States continue to report that lack of access to affordable and accessible housing and an inadequate supply of direct care workers are major barriers to serving more people in the community. While there are always competing demands on federal budget funding that could disrupt MFP, there is not a substantive debate over it as there is with many other health programs. However, if Congress does not reauthorize MFP, it could hinder state efforts to help beneficiaries move from institutions to the community.
Table 1: States’ Money Follows the Person (MFP) Program Funding and Future Plans
State
Has MFP Program
Exhausted MFP Funds
Plans to discontinue MFP services and/or program activities if federal funding not reauthorized
Already added MFP services to existing waiver
Plans to add MFP services to existing waiver
Alabama
X
Alaska
N/A
Arizona
N/A
Arkansas
X
X
California
X
X
Colorado
X
X
X
Connecticut
X
Delaware
X
X
DC
X
Florida
N/A
Georgia
X
X
X
Hawaii
X
Idaho
X
X
X
Illinois
X
X
Indiana
X
X
X
Iowa
X
X
Kansas
X
X
Kentucky
X
Louisiana
X
X
X
Maine
X
Maryland
X
NR
Massachusetts
X
X
X
Michigan
X
X
X
*
Minnesota
X
Mississippi
X
TBD
Missouri
X
X
Montana
X
X
Nebraska
X
X
Nevada
X
X
New Hampshire
X
New Jersey
X
X
New Mexico
N/A
New York
X
X
North Carolina
X
North Dakota
X
X
Ohio
X
X
X
Oklahoma
X
X
Oregon**
N/A
Pennsylvania
X
Rhode Island
X
South Carolina
X
X
X
South Dakota
X
X
X
Tennessee
X
X
X
Texas
X
Utah
N/A
Vermont
X
TBD
Virginia
X
X
X
Washington
X
X
X
West Virginia
X
X
X
Wisconsin
X
Wyoming
N/A
TOTAL:
44
7
15
12
8
NOTES: N/A = not applicable. NR = no response to survey question. TBD = state’s plans to be determined. HCBS waivers include § 1915 (c) and § 1115. *Additionally, MI is adding services to a § 1915 (i) state plan amendment. **OR discontinued its MFP program in 2010.SOURCES: KFF survey of Medicaid officials in 50 states and DC conducted by HMA, Oct. 2019; KFF Medicaid HCBS Program Survey, FY 2018.
Endnotes
To qualify for MFP, individuals must reside in an institution for more than 90 consecutive days and move to a house, apartment, or group home with less than four residents. ↩︎
The MFP enhanced federal matching rate is determined by subtracting the state’s regular matching rate from 100%, dividing the result in half, and then adding that number of percentage points to the state’s regular matching rate. The MFP enhanced matching rate is capped at 90%. ↩︎
The majority of MFP states consistently reported per enrollee spending for MFP enrollees receiving HCBS to be lower than those in institutions, and no state reported that institutional costs were lower than HCBS in KFF surveys of MFP states in 2008, 2010, 2011, 2012, 2013, and 2015. A couple of states using capitated managed care reported that HCBS and institutional costs were comparable due to a blended capitation rate. KFF, Money Follows the Person: A 2015 State Survey of Transitions, Services, and Costs (Oct. 2015). ↩︎
To financially qualify for Medicaid long-term services and supports (LTSS), an individual must have low income and limited assets. In response to concerns that these rules could leave a spouse without adequate support when a married individual needs LTSS, Congress created the spousal impoverishment rules in 1988. These rules required states to protect a portion of a married couple’s income and assets to provide for the “community spouse’s” living expenses when determining nursing home financial eligibility, but gave states the option to apply the rules to home and community-based services (HCBS) waivers.
Section 2404 of the Affordable Care Act (ACA), which is set to expire on December 31, 2019, changed the spousal impoverishment rules to treat Medicaid HCBS and institutional care equally. Applying more stringent Medicaid financial eligibility rules to HCBS than to nursing homes could slow or begin to reverse states’ progress in expanding access to HCBS, while reauthorizing the rules would provide stability for enrollees and states. This issue brief answers key questions about the spousal impoverishment rules, presents 50-state data from a 2019 Kaiser Family Foundation survey about state policies and future plans, and considers the implications if Congress does not extend Section 2404. Key findings include:
Some states may stop applying the spousal impoverishment rules to HCBS if Section 2404 expires. Forty of 51 states plan to continue applying the rules to at least some HCBS waiver populations. Two of 11 states plan to continue applying the rules to Section 1915 (i) state plan HCBS enrollees, while none of the eight states electing Community First Choice HCBS option plan to continue applying the rules to those enrollees.
Fourteen states expect that the expiration of Section 2404 would affect HCBS enrollees. The most frequently cited outcome was fewer individuals eligible for waiver services. Without Section 2404, the spousal impoverishment rules will revert to a state option for most HCBS waiver enrollees and will no longer apply to HCBS provided under other Medicaid authorities, unless states obtain a Section 1115 waiver, as of January 1, 2020.
Eight states report that the repeated temporary extensions of Section 2404 to date have resulted in confusion among enrollees and/or increased staff workload or administrative burdens.
Issue Brief
Introduction
Seniors and people with disabilities or chronic illnesses may need long-term services and supports (LTSS) for help with self-care tasks (such as eating, bathing, or dressing) and household activities (such as preparing meals, managing medication, or housekeeping). Medicaid is the primary payer for LTSS, covering over half of national spending on nursing home care and home and community-based services (HCBS) as of 2017.1 To financially qualify for Medicaid LTSS, an individual must have low income and limited assets. When one spouse in a married couple needs LTSS, Medicaid spousal impoverishment rules protect some income and assets to support the other spouse’s living expenses, in an effort to prevent her “financial devastation from paying the high cost of [her spouse’s] nursing home care.”2
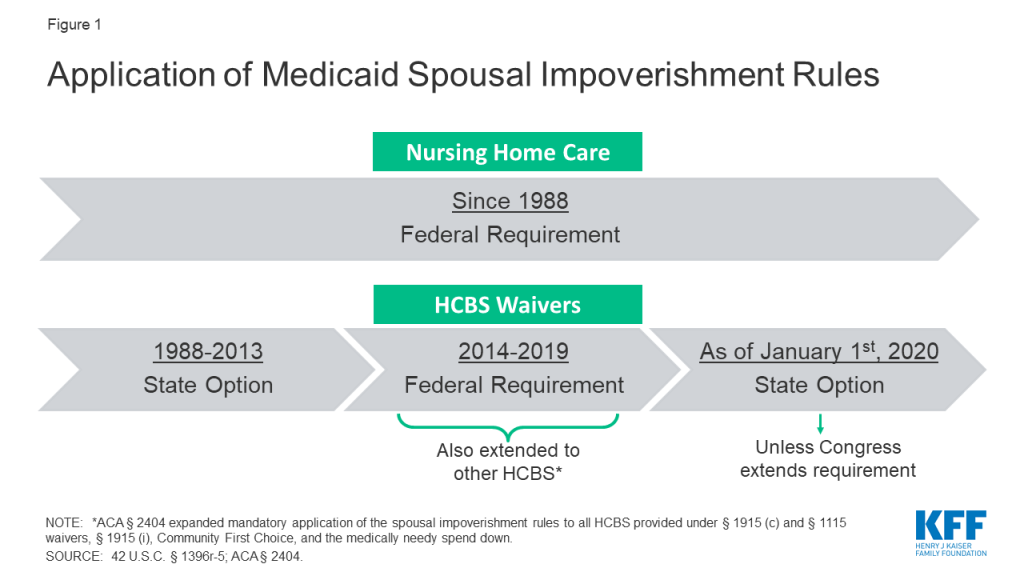
Since Congress enacted the spousal impoverishment rules in 1988, federal law has required states to apply them when a married individual seeks nursing home care.3 Prior to 2014, states had the option to apply the rules when a married individual sought home and-community based waiver services.4 However, from January 1, 2014 through December 31, 2019, Section 2404 of the Affordable Care Act (ACA) has required states to apply the spousal impoverishment rules to HCBS waivers.5 Section 2404 also expanded the spousal impoverishment rules to the Section 1915 (i) HCBS state plan option, Community First Choice (CFC) attendant care services and supports, and individuals eligible through a medically needy spend down. If Congress does not reauthorize Section 2404, the spousal impoverishment rules will revert to a state option for HCBS waivers and will not apply to other HCBS, as of January 1, 2020 (Figure 1).
This issue brief answers key questions about the spousal impoverishment rules,6 presents new data from a 2019 Kaiser Family Foundation (KFF) 50-state survey about state policies and future plans in this area, and considers the implications if Congress does not extend Section 2404.
Figure 1: Application of Medicaid Spousal Impoverishment Rules
Key Questions About Medicaid LTSS Spousal Impoverishment Rules
1. What are the general Medicaid LTSS financial eligibility rules?
Federal law limits Medicaid LTSS eligibility to people with low incomes and limited assets. At minimum, states generally must cover nursing home care for people who have qualifying functional needs and receive federal Supplemental Security Income (SSI) benefits7 ($771 per month for an individual, and $1,157 for a couple in 2019).8 States can choose to adopt the “special income rule,” to increase the Medicaid nursing home income limit to 300% of SSI ($2,313 per month for an individual in 2019),9 and 43 states do so in 2018.10 States also can choose to apply the “special income rule” when determining Medicaid financial eligibility for people receiving HCBS under a waiver, and all but one of the states using the “special income rule” elect this option to expand HCBS financial eligibility; this eligibility pathway known as the “217-group.”11 Additionally, people who qualify for Medicaid institutional LTSS or HCBS under the “special income rule” typically are subject to an asset limit, and most states apply the SSI asset limits of $2,000 for an individual, and $3,000 for a couple.
Once eligible for Medicaid LTSS, individuals generally must contribute a portion of their monthly income to the cost of their care. These “post-eligibility treatment of income” (PETI) rules apply to both nursing home services and HCBS waivers. For those in nursing homes, a small “personal needs allowance” is permitted to pay for items not covered by Medicaid, such as clothing;12 the federal minimum personal needs allowance is $30 per month and the state median was $50 per month in 2018.13 Individuals in the “217-group” are subject to PETI under HCBS waivers and may have a higher “maintenance needs allowance,” recognizing that individuals living in the community must pay for room and board. There is no federal minimum for HCBS maintenance needs; instead, states may use any amount as long as it is based on a “reasonable assessment of need” and subject to a maximum that applies to all enrollees under the waiver.14
2. What policy considerations led Congress to enact the spousal impoverishment rules?
Congress created the spousal impoverishment rules in 1988, to protect a portion of a married couple’s income and assets to support the “community spouse’s” living expenses when the other spouse sought Medicaid LTSS. The spousal impoverishment rules supersede rules that would otherwise require eligibility determinations to account for a spouse’s financial responsibility for a Medicaid applicant or beneficiary.15 They were enacted “in response to evidence that at-home spouses – typically elderly women with little or no income of their own – faced poverty and a radical reduction in their standard of living before their spouses living in a nursing home could qualify for Medicaid.”16 Prior to the spousal impoverishment rules, “married individuals requiring Medicaid-covered LTSS were commonly faced with either forgoing services or leaving the spouse still living at home with little income or resources.”17
Concerns about potentially financially devastating LTSS costs that motivated Congress to add the spousal impoverishment rules to Medicaid 30 years ago remain relevant today. LTSS costs are difficult for most people to afford out-of-pocket, and private insurance coverage of LTSS is limited. In 2019, a year of nursing home care averages over $90,000; average annual home health aide services cost over $52,000; and average annual adult day health care services total nearly $20,000.18 As in 1988, the high cost of LTSS “can rapidly deplete the lifetime savings of elderly couples”19 today. The spousal impoverishment rules “help ensure. . . that community spouses are able to live out their lives with independence and dignity.”20 While the amounts protected under the rules (discussed below) might be considered “quite modest or even inadequate to sustain the at-home spouse’s accustomed standard of living, they far exceed the income and asset levels that may be retained in the case of unmarried recipients of Medicaid long-term care services”21 (described above, e.g., typically $2,000 in countable assets and a minimum of $30 monthly personal needs allowance for nursing home enrollees).
3. How do the spousal impoverishment rules affect Medicaid LTSS financial eligibility?
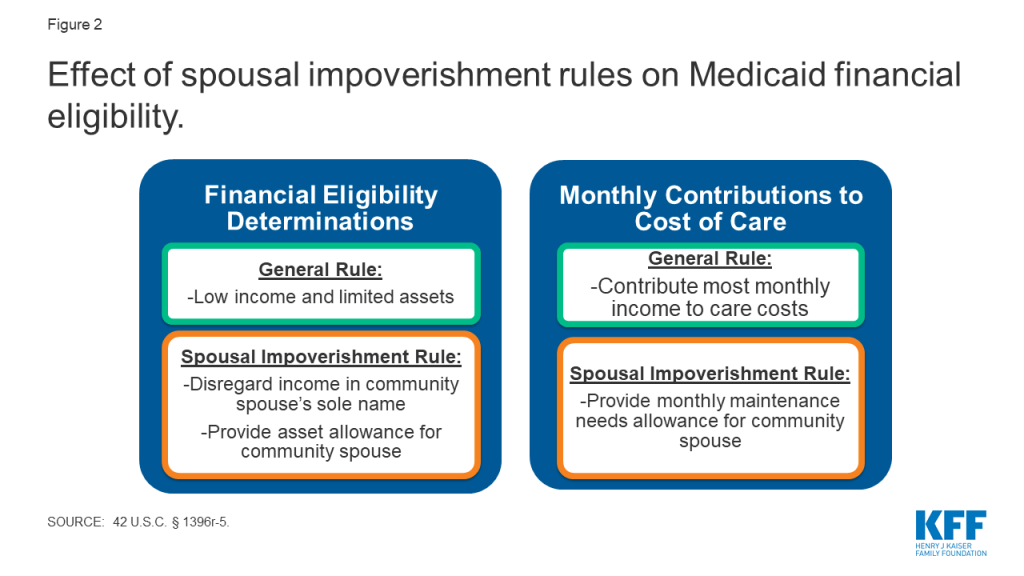
Since 1988, Congress has required states to apply the spousal impoverishment rules to long-term nursing home services to provide financial support for the “community spouse.”22 Specifically, states must disregard a portion of income and assets at two points when a married individual is seeking nursing home services: (1) when determining and renewing the individual’s Medicaid financial eligibility; and (2) when determining the individual’s monthly required contribution to his care costs under the PETI rules (Figure 2). The rules apply to long-term nursing home stays, which are those expected to last at least 30 consecutive days.23 The spousal impoverishment rules apply when a married individual seeks or receives Medicaid LTSS, and his spouse is not in a nursing home or other medical institution.24 The rules do not apply when both spouses seek long-term Medicaid nursing home care.25 The amounts protected under the spousal impoverishment rules are updated annually and are in addition to the general Medicaid LTSS income and asset limits described above. Box 1 provides additional detail about how protected amounts are determined under the rules.
Figure 2: Effect of spousal impoverishment rules on Medicaid financial eligibility.
Box 1: General Application of Medicaid Spousal Impoverishment Rules26
Income. When determining financial eligibility for a married individual seeking Medicaid LTSS,27 and when determining his required contribution from monthly income to the cost of care,28 any income in the “community spouse’s” sole name is not deemed available to the Medicaid spouse. Additionally, when determining the required contribution from monthly income to the cost of care, the starting point is that half of any income in the couple’s joint name is deemed available to the Medicaid spouse.29 The rules also provide for a “monthly maintenance needs allowance” (MMNA) for the community spouse, subject to both minimum and maximum limits.30 If the “community spouse’s” sole income, plus half of the couple’s joint income, is less than the minimum MMNA, the “community spouse” can retain additional income, enough to reach the minimum. The minimum MMNA is 150% FPL ($2,057.50 per month for a household of two in 2019).31 The “community spouse’s” MMNA cannot exceed a maximum limit ($3,160.50 in 2019).32
Assets. When determining Medicaid LTSS financial eligibility, the starting point is that half of the couple’s assets (including any countable assets in which either or both spouses have an ownership interest at the time of the Medicaid spouse’s most recent period of continuous institutionalization33 ) potentially can be retained by the “community spouse.34 The rules also provide for a “community spouse resource allowance” (CSRA), subject to minimum and maximum limits.35 If the “community spouse’s” half of the assets is less than the minimum CSRA ($25,284 in 2019; and higher at state option), the Medicaid spouse can transfer to her enough assets to reach the minimum CSRA. If the “community spouse’s” half of the assets exceeds the maximum CSRA ($126,420 in 2019), she can retain only the amount up to the maximum, with remaining assets considered available to the Medicaid spouse.36 After Medicaid eligibility is established, none of the “community spouse’s” assets are deemed available to the Medicaid spouse.37
From the rules’ creation in 1988, until ACA Section 2404 took effect in January 2014, states had the option to apply the spousal impoverishment rules to HCBS waivers.38 Specifically, states could choose whether to apply the rules to HCBS waivers in two instances: first, states could decide whether to apply the rules when determining and renewing financial eligibility under HCBS waivers for the “217-group.” These are individuals for whom states have opted to expand the minimum Medicaid LTSS financial eligibility limits under the “special income rule” (described above), who would be eligible under the Medicaid state plan if institutionalized, meet an institutional level of care, and would be institutionalized if not receiving waiver services. The option to apply the spousal impoverishment rules to HCBS waivers is specifically limited to the 217-group, even though states also can include people eligible through other Medicaid eligibility pathways in their HCBS waivers.39 Second, if states apply the spousal impoverishment rules when determining and renewing Medicaid financial eligibility for the 217-group under HCBS waivers, they also can opt to apply the rules to this group when determining any required monthly contribution from income to their cost of care under the PETI rules (described above). The 217-group is the only Medicaid HCBS population subject to PETI.
Prior to Section 2404 taking effect in 2014, most, but not all states, opted to apply the spousal impoverishment rules to HCBS waivers. In 2009 (the most recent year for which data are available prior to 2014), five states (Alabama, Massachusetts, New Hampshire, New York, and West Virginia) chose not to apply the spousal impoverishment rules to HCBS waivers, and these data were not reported for one state (Illinois).40
4. How Did ACA Section 2404 change the Medicaid spousal impoverishment rules?
Section 2404 currently requires states to apply the spousal impoverishment rules to Medicaid HCBS waivers from January 1, 2014 through December 31, 2019. Under the ACA, Section 2404 was set to expire on December 31, 2018, but Congress has temporarily extended the provision first through March 31, 2019, then through September 30, 2019, and most recently through December 31, 2019. Section 2404 removes the state option for applying the rules to HCBS waivers and instead makes the rules mandatory for determining both financial eligibility and PETI when a married individual seeks Medicaid home and community-based waiver services.41
Additionally, Section 2404 expands the types of HCBS to which states must apply the spousal impoverishment rules from 2014 through 2019. First, Section 2404 applies the spousal impoverishment rules to all individuals under Section 1915 (c) HCBS waivers, not just the 217-group. Section 2404 also applies the spousal impoverishment rules to HCBS provided under Section 1115 waivers. Finally, Section 2404 requires states to apply the rules when determining Medicaid financial eligibility for HCBS provided through additional authorities, including the Section 1915 (i) state plan option, CFC attendant care services and supports, and medically needy/spend down pathways. Table 1 summarizes federal requirements and state options to apply the spousal impoverishment rules over time.
Table 1: Federal Requirements and State Options to Apply Medicaid Spousal Impoverishment Rules
LTSS Authority
1988-2013
2014-2019, under Section 2404
As of Jan. 1, 2020, unless Section 2404 reauthorized
Institutional care
Nursing homes
Required
Required
Required
Medical institutions
Required
Required
Required
HCBS
217-group in Section 1915 (c) waivers
State option*
Required
State option*
Other groups in Section 1915 (c) waivers
Not allowed**
Required
Not allowed**
HCBS under Section 1115 waivers
Not allowed**
Required
Not allowed**
Section 1915 (i) state plan HCBS
Not allowed**
Required
Not allowed**
Community First Choice
Not allowed**
Required
Not allowed**
Medically needy/spend down
Not allowed**
Required
Not allowed**
NOTES: *States opt whether to apply the rules to financial eligibility for the 217-group, and if so, separately opt whether to also apply the rules to that group’s PETI. **States may obtain § 1115 waivers to apply the rules to individuals other than the 217-group. SOURCE: 42 U.S.C. § 1396r-5; ACA § 2404.
5. What are the implications if ACA Section 2404 expires in December 2019?
If Congress does not extend Section 2404, application of the spousal impoverishment rules to HCBS waivers will return to a state option as of January 1, 2020,42 and will no longer apply to the other HCBS authorities (Table 1). Without Section 2404, states would have to obtain a Section 1115 waiver to apply the spousal impoverishment rules to HCBS waiver enrollees other than the 217-group, Section 1915 (i) state plan HCBS, CFC, or individuals eligible through a spend down.43 Facing impending expiration of the rules first in December 2018, and again in April 2019, September 2019, and December 2019, CMS has issued guidance directing states to take the following actions if Section 2404 expires: (1) redetermine financial eligibility, without applying the spousal impoverishment rules, for all individuals receiving HCBS under Section 1915 (i) and CFC, and for those eligible under HCBS waivers (other than the 217-group if the state elects the option); (2) recalculate PETI for individuals receiving services under HCBS waivers, (other than the 217-group if the state elects the option); and (3) stop applying the rules to new Medicaid HCBS applicants (other than the 217-group if the state elects the option.44
If Section 2404 expires, over three-quarters (40 of 51) of states plan to continue applying the spousal impoverishment rules to at least some HCBS waiver populations (the 217-group), while five states’ plans were unknown at the time of our survey.45 Among the 40 states with plans to continue the spousal impoverishment rules for 217 waiver groups, all will apply them to eligibility determinations, 30 states will apply them to PETI, and 29 states will apply them to both determinations. Some state responses varied by waiver program. For example, 14 states were uncertain of continuation plans for at least one HCBS waiver.46 If the Section 2404 requirement expires, states will have the option to continue to apply the rules to the 217-group covered under Section 1915 (c) HCBS waivers.
Thirteen states already have or will seek a Section 1115 waiver to allow them to continue to apply the spousal impoverishment rules to non-217-group HCBS waiver enrollees, while 14 states will not seek such a waiver. Specifically, three states (AL, NV, OK) will seek a new Section 1115 waiver to continue to apply the spousal impoverishment rules to non-217 group waiver enrollees, and 10 states with existing Section 1115 waivers noted that this authority is included under their current waivers and will continue.47 By contrast, 14 states will not seek a Section 1115 waiver to continue the policy for non-217-group waiver enrollees.48 Sixteen states’ plans in this area were undecided at the time of our survey.49
Two of 11 states plan to continue applying the spousal impoverishment rules to Section 1915 (i) state plan HCBS enrollees if Section 2404 expires. These states (IA and NV) will seek a Section 1115 waiver to authorize this policy. By contrast, five states do not plan to continue applying the spousal impoverishment rules to Section 1915 (i) state plan HCBS if Section 2404 expires (CA, CT, ID, IN, TX). One state’s plans in this area were undecided (OH).50
None of the eight states offering CFC attendant services reported plans to continue applying the spousal impoverishment rules to CFC enrollees if Section 2404 expires.51 If Section 2404 expires, states would have to obtain a Section 1115 waiver to continue applying the spousal impoverishment rules to CFC enrollees. California, Oregon, and Washington would not seek such a waiver, while Connecticut, Maryland, Montana, and Texas were undecided.
Fourteen states report that the expiration of Section 2404 would have an impact on financial eligibility for individuals currently enrolled under HCBS waivers.52 Among these states, 10 expected that fewer individuals would be eligible for waiver services;53 five expected that more individuals would have a higher share of cost requirement under the PETI rules;54 and five expected that at least some waiver enrollees potentially would have to move to institutions due to loss of HCBS eligibility.55 Michigan indicated that the expiration of spousal impoverishment protections would result in 3,000 fewer individuals eligible under an HCBS waiver serving seniors and adults with physical disabilities. Without Section 2404, the spousal impoverishment rules will revert to a state option for HCBS waivers and will no longer apply to HCBS provided under other Medicaid authorities, unless states obtain a Section 1115 waiver, as of January 1, 2020.
Eight states report that the repeated temporary extensions of Section 2404 to date have affected the state and/or HCBS waiver enrollees. Among these states, six indicated confusion among waiver enrollees,56 and five noted increased staff workload.57 One state reported that state staff were unable to focus on other priorities due to the need to redetermine waiver eligibility and PETI in advance of the expiration date,58 while two states reported other impacts.59 Each time that the date on which Section 2404 was set to expire approached, states must redetermine enrollees’ financial eligibility, and if applicable PETI, without applying the spousal impoverishment rules, and send notice of any changes to enrollees before the expiration date, according to the CMS guidance described above. At minimum, states must do this for non-217 waiver enrollees, Section 1915 (i) enrollees, and CFC enrollees. States also must do this for the 217-group if they do not elect the option to continue to apply the rules. Then, each time after Congress enacted another temporary extension, states had to notify enrollees that the anticipated changes would not take effect, redetermine financial eligibility and PETI, this time applying the spousal impoverishment rules, and again send enrollees notice of any changes. This cycle has been repeated for scheduled expirations in December 2018, April 2019, September 2019, and December 2019,
Applying the same financial eligibility rules to Medicaid nursing facility care and HCBS helps alleviate bias in favor of institutional care.60 If financial eligibility limits are less stringent for nursing home care than for HCBS, an individual in need of LTSS may qualify only for institutional care. Even if an individual financially qualifies for both nursing home care and HCBS, he may be incentivized to choose nursing home care if that option will protect additional income and assets to support his spouse at home, due to differential application of the spousal impoverishment rules.
Applying more stringent income and asset rules to HCBS, compared to nursing home care, could impact the progress that states have made in expanding access to HCBS. The share of Medicaid LTSS spending devoted to HCBS instead of institutional care has been steadily increasing in recent decades. A majority of Medicaid LTSS spending went to HCBS for the first time in 2013, and reached 57% in 2016 (Figure 3). Although not required by federal Medicaid law, states have an independent community integration obligation under the Americans with Disabilities Act (ADA) when administering services, programs, and activities.61 The Supreme Court’s Olmstead decision found that the unjustified institutionalization of people with disabilities is illegal discrimination under the ADA, and Medicaid plays a key role in helping states meet their community integration obligations.62 Applying financial eligibility rules to HCBS that are more restrictive than those for institutional care could be challenged under the ADA, even if permitted by Medicaid law.
Figure 3: Medicaid long-term services and supports spending, by institutional vs. community setting.
Looking Ahead
Congress could consider legislation to extend Section 2404 in the coming weeks, before the provision expires at the end of December 2019. There does not appear to be a substantive debate over the issue like with other health programs, but there are always competing demands for federal funding. Section 2404’s original expansion of the spousal impoverishment rules in the ACA likely was time limited due to an effort to control costs. The Congressional Budget Office (CBO) estimated the cost of the temporary extension of Section 2404 at $22 million for January through March 2019 at $22 million63 and $46 million for April through September 2019.64 CBO estimated that a longer-term extension, for 5 years from October 2019 through March 2024, would cost $331 million;65 Congress subsequently amended this bill to extend the rules from October through December 2019.
If reauthorized, the rules would provide stability and continuity for enrollees receiving HCBS and for states administering Medicaid eligibility determinations and renewals, while increasing federal and state budgetary costs over and above the current baseline. If Section 2404 expires, several states have indicated their plans to continue to apply the spousal impoverishment rules to some or all HCBS waivers are unknown. Though most states are planning to continue to apply the rules at this time, without Section 2404 or a similar requirement, states could stop doing so at any time by submitting an HCBS waiver amendment.66 Additionally, without Section 2404, states lack legal authority to apply the rules when determining financial eligibility for HCBS under other authorities, including waiver enrollees other than the 217-group, Section 1915 (i), CFC, and spend down pathways, and would have to devote time and resources to obtaining and administering a Section 1115 waiver to be able to treat financial eligibility for all HCBS equally.67 To date, few states plan to seek such a waiver. Applying different Medicaid financial eligibility rules to institutional LTSS and HCBS could affect states’ progress in expanding access to HCBS, rebalancing LTSS spending, and promoting community integration.
Table 2: States’ Application of Spousal Impoverishment Rules to Medicaid HCBS
State
Applied to Waivers in 2009
Plans To Apply After § 2404 Expires in Dec. 2019 To:
217 Waiver Groups
Non-217 Waiver Groups
§ 1915 (i) HCBS*
CFC*
Alabama
No
Yes
Yes
Alaska
Yes
Unknown
Undecided
Arizona
Yes
Yes
Yes
Arkansas
Yes
Yes
No
California
Yes
Yes
Undecided
No
No
Colorado
Yes
Yes
No
Connecticut
Yes
Yes
No
No
Undecided
Delaware
Yes
Yes
Yes
No response
DC
Yes
Yes
No response
No response
Florida
Yes
Yes
No
Georgia
Yes
Yes
No
Hawaii
Yes
Yes
Yes
Idaho
Yes
Yes
Undecided
No
Illinois
No response
No response
No response
Indiana
Yes
Yes
Undecided
No
Iowa
Yes
Yes
Yes
Yes
Kansas
Yes
Unknown
Undecided
Kentucky
Yes
Yes
Undecided
Louisiana
Yes
Yes
No
Maine
Yes
No response
No response
Maryland
Yes
Yes
No
Undecided
Massachusetts
No
No response
No response
Michigan
Yes
Unknown
Undecided
Minnesota
Yes
Yes
No response
Mississippi
Yes
Yes
No
No response
Missouri
Yes
Yes
Undecided
Montana
Yes
Yes
Undecided
Undecided
Nebraska
Yes
Yes
No
Nevada
Yes
Yes
Yes
Yes
New Hampshire
No
No response
No response
New Jersey
Yes
Yes
Yes
New Mexico
Yes
Yes
Yes
New York
No
No response
Undecided
No response
North Carolina
Yes
No response
No response
North Dakota
Yes
Yes
Undecided
Ohio
Yes
Yes
No
Undecided
Oklahoma
Yes
Yes
Yes
Oregon
Yes
Yes
No
No
Pennsylvania
Yes
Yes
Undecided
Rhode Island
Yes
Yes
Yes
South Carolina
Yes
Yes
Undecided
South Dakota
Yes
Yes
No
Tennessee
Yes
Yes
Yes
Texas
Yes
Unknown
Undecided
No
Undecided
Utah
Yes
Unknown
Undecided
Vermont
Yes
Yes
Yes
Virginia
Yes
Yes
No
Washington
Yes
Yes
Yes
No
West Virginia
No
Yes
No response
Wisconsin
Yes
Yes
Undecided
Wyoming
Yes
Yes
No
TOTAL ELECTING WAIVER/STATE PLAN OPTION
All 50 states and DC offer at least 1 waiver
11 states
8 states
APPLICATION OF SPOUSAL IMPOVERISHMENT
45 yes, 5 no, 1 no response
40 yes, 5 unknown, 6 no response
13 yes, 14 no, 16 undecided, 8 no response
2 yes, 5 no, 1 undecided, 3 no response
0 yes, 3 no, 4 undecided, 1 no response
NOTES: *Blank cell = state does not elect option. “Unknown” = state’s plans undetermined at time of survey.SOURCES: Julie Stone, Medicaid Eligibility for Persons Age 65+ and Individuals with Disabilities: 2009 State Profiles (Cong. Research Serv., June 2011); KFF Medicaid HCBS Program Surveys, FY 2018.
MaryBeth Musumeci and Priya Chidambaram are with KFF.Molly O’Malley Watts is with Watts Health Policy Consulting.
Endnotes
National LTSS expenditures totaled $364.9 billion, including spending on residential care facilities, nursing homes, home health services, HCBS waivers, ambulance providers, and some post-acute care. Medicare post-acute care spending ($81.5 billion) is excluded. LTSS payers include Medicaid (52%), other public and private insurance (20%), out-of-pocket spending (16%), and private insurance (11%). All HCBS waivers are attributed to Medicaid. KFF estimates based on 2017 National Health Expenditure Accounts data from CMS, Office of the Actuary. ↩︎
The rules also apply to long-term care in other medical institutions besides nursing homes. 42 U.S.C. § 1396r-5. The rules apply to stays of at least 30 consecutive days. 42 U.S.C. § (h)(1)(B). ↩︎
Specifically, states could opt to apply the rules to individuals who are eligible for Medicaid by reason of a Section 1915 (c) HCBS waiver, under 42 U.S.C. § 1396a (a)(10)(A)(ii)(VI) (describing individuals who would be eligible under the Medicaid state plan if institutionalized, meet an institutional level of care, and would be institutionalized if not receiving waiver services, sometimes referred to as the “217-group,” because they also are described in 42 C.F.R. 435.217). 42 U.S.C. § 1396r-5 (h)(1)(A). ↩︎
This brief is not an exhaustive discussion of Medicaid LTSS financial eligibility rules. Additionally, other topics such as asset transfers and estate recovery are beyond the scope of this brief. ↩︎
To be eligible for SSI, beneficiaries must have low incomes, limited assets, and an impaired ability to work at a substantial gainful level as a result of old age or significant disability. ↩︎
Section 209 (b) allows states to apply Medicaid eligibility rules that are more restrictive than the SSI rules, as long as the state’s rules are no more restrictive than they were in 1972, when SSI was created, and provided that the state allows SSI beneficiaries to establish Medicaid eligibility through a spend-down. 42 U.S.C. § 1396a (f). ↩︎
42 U.S.C. § 1396a (q); 42 U.S.C. § 1396r-5 (d)(1). When determining PETI under the spousal impoverishment rules, additional deductions are permitted for minor or dependent children, dependent parents, or dependent siblings of either spouse who reside with the community spouse, 42 U.S.C. § 1396r-5 (d)(1)(C), and expenses incurred for medical or remedial care for the institutionalized spouse, 42 U.S.C. § 1396r-5 (d)(1)(D), in addition to the community spouse monthly income allowance discussed in Key Question 2. ↩︎
42 U.S.C. § 1396r-5 (a)(1). The rules permit (and sometimes require) that a married individual seeking Medicaid LTSS whose spouse is not institutionalized is treated differently for financial eligibility purposes than other individuals seeking Medicaid LTSS. 42 U.S.C. § 1396r-5 (a)(2). ↩︎
The rules also apply to states providing Medicaid under a Section 1115 waiver, to the same extent that the rules would apply if the state instead used state plan authority, 42 U.S.C. § 1396r-5 (a)(4)(A), and to PACE programs, 42 U.S.C.§ 1396r-5 (a)(5). ↩︎
The minimum MMNA can be increased if either spouse establishes that it does not provide adequate income to the “community spouse,” “due to exceptional circumstances resulting in significant financial duress.” 42 U.S.C. § 1396r-5 (e)(2)(B). ↩︎
The “community spouse” may retain additional assets if either spouse establishes that the assets retained in the CSRA do not generate enough income to meet the minimum MMNA. 42 U.S.C. § 1396r-5 (e)(2)(C). ↩︎
42 U.S.C. § § 1396r-5 (c)(2)(B), (f)(2)(A). For additional explanation of these provisions, see U.S. Dep’t of Health & Human Servs., Office of the Asst. Sec’y for Planning & Evaluation, Spouses of Medicaid Long-Term Care Recipients (April 1, 2005), https://aspe.hhs.gov/basic-report/spouses-medicaid-long-term-care-recipients. ↩︎
For example, states may include in their HCBS waivers individuals eligible for Medicaid under the state plan option to cover seniors and people with disabilities up to 100% of the federal poverty level (FPL, $12,160 for an individual in 2018) to offer services that are not provided under the state plan benefit package. ↩︎
Section 2404 does not require actual receipt of HCBS waiver services and thus allows an individual to obtain state plan Medicaid eligibility, by applying the spousal impoverishment rules, if the individual qualifies for but will not actually receive HCBS waiver services upon enrollment due to a waiver waiting list. CMS Informational Bulletin, Sunset of Section 2404 of the Affordable Care Act, Relating to the Spousal Impoverishment Rules for Certain Home and Community-Based Services Applicants and Recipients (Nov. 9, 2018), https://www.medicaid.gov/federal-policy-guidance/downloads/cib110918-2.pdf. ↩︎
CMS notes that states providing HCBS under Section 1115 waivers who wish to continue to apply the spousal impoverishment rules after Section 2404 expires may need to seek a waiver amendment to do so. CMS Informational Bulletin, Temporary Extension of the Affordable Care Act’s Spousal Impoverishment Provision for Married Recipients of Home and Community-Based Services (Feb. 8, 2019), https://www.medicaid.gov/federal-policy-guidance/downloads/cib020819.pdf; see also CMS Informational Bulletin, Additional Temporary Extension of the Spousal Impoverishment Rules for Married Applicants and Recipients of Home and Community-Based Services (Sept. 4, 2019), https://www.medicaid.gov/federal-policy-guidance/downloads/cib090419.pdf; CMS Informational Bulletin, Additional Extension of the Spousal Impoverishment Rules for Married Applicants and Recipients of Home and Community-Based Services (May 8, 2019), https://www.medicaid.gov/federal-policy-guidance/downloads/cib050819.pdf; CMS Informational Bulletin, Sunset of Section 2404 of the Affordable Care Act, Relating to the Spousal Impoverishment Rules for Certain Home and Community-Based Services Applicants and Recipients (Nov. 9, 2018), https://www.medicaid.gov/federal-policy-guidance/downloads/cib110918-2.pdf. ↩︎
The 40 states include 38 responding yes for § 1915 (c) waivers and two states (AZ and VT) responding not applicable; these two states do not offer any § 1915 (c) waivers and instead provide all HCBS through a § 1115 waiver that already authorizes application of the spousal impoverishment rules. The five states with unknown plans are AK, KS, MI, TX, and UT. The remaining six states (IL, ME, MA, NH, NY, and NC) did not respond to this survey question. ↩︎
AK, CA, CT, FL, KS, MI, MO, ND, OR, PA, TX, UT, WA, and WI. ↩︎
AR, CO, CT, FL, GA, LA, MD, MS, NE, OH, OR, SD, VA, and WY. ↩︎
AK, CA, ID, IN, KS, KY, MI, MO, MT, ND, NY, PA, SC, TX, UT, and WI. The remaining 8 states (DC, IL, ME, MA, MN, NH, NC, and WV) did not respond to this survey question. ↩︎
The remaining three states (DE, DC, and MS) did not respond to this survey question. ↩︎
The remaining state (NY) did not respond to this survey question. ↩︎
CA, ID, LA, MI, MO, MT, NV, NH, NY, OH, OK, PA, TX, and UT. ↩︎
$9 million in FY 2019, $7 million in FY 2020, and $7 million in FY 2021. Congressional Budget Office, H.R. 259 Medicaid Extenders Act of 2019 cost estimate (Jan. 11, 2019), https://www.cbo.gov/system/files/2019-01/hr259.pdf. ↩︎
Congressional Budget Office, H.R. 3253 Empowering Beneficiaries, Ensuring Access, and Strengthening Accountability Act of 2019 Preliminary Cost Estimate (as introduced on June 13, 2019), https://www.cbo.gov/system/files/2019-06/hr3253.pdf. ↩︎
Since § 2404 took effect, CMS has asked states to indicate in their § 1915 (c) waiver applications and renewals whether they intend to apply the rules to the 217-group if § 2404 expires. CMS Informational Bulletin, Sunset of Section 2404 of the Affordable Care Act, Relating to the Spousal Impoverishment Rules for Certain Home and Community-Based Services Applicants and Recipients (Nov. 9, 2018), https://www.medicaid.gov/federal-policy-guidance/downloads/cib110918-2.pdf. ↩︎
CMS indicates that it will work with states to expedite these waiver approvals. States could seek waivers to apply the rules to some but not all of these populations. These waivers would be approved using expenditure authority and would be subject to federal budget neutrality rules. Id. ↩︎
Telemedicine holds the potential to expand access to contraceptives, STI testing and treatment, and abortion care, yet few individuals use this approach to obtain these services. A new KFF analysis examines the opportunities of telemedicine to expand access to sexual and reproductive health care as well as the policy barriers impeding its expansion. Because each state defines and regulates telemedicine differently, the availability and coverage of services is inconsistent across the country. While no state explicitly prohibits the use of telemedicine for contraception or STIs — 18 states have effectively banned telemedicine approaches to provide medication abortion. Many of the states that have recently passed abortion restrictions that have led to clinic closures have passed laws that block the use of telemedicine to distribute mifepristone, even though research finds it to be safe, effective and acceptable to patients when compared to in-person care.
The brief also outlines the growing use of telemedicine for contraception and STI care, including a discussion of insurance coverage of telemedicine services, the financial implications for providers and patiensti and its potential to improve access to reproductive health care across the United States.
Telemedicine technologies may help address unmet reproductive health needs in the U.S., particularly for rural populations and those with transportation and childcare barriers.
A wide range of reproductive health care services are provided via telemedicine, including hormonal contraception, medication abortions, and sexually transmitted infection (STI) care. These services could replace the need for in-person care in some cases, though most telemedicine services today still function as an adjunct to the existing health care system.
Despite its potential, telemedicine utilization by patients is low and significant barriers exist to its implementation. Initiating a telemedicine program entails significant investment in technology, and requires overcoming logistical challenges including privacy concerns, licensing of physicians and malpractice coverage.
Insurance coverage of telemedicine services varies widely based on the insurance plan and state policies. Insurers typically pay lower rates for telemedicine compared to in-person care, and patients may pay out-of-pocket for services normally covered in full in the clinical setting, including contraception and STI screening.
Introduction
The World Health Organization (WHO) defines telemedicine as the provision of health care services by health care professionals, utilizing technology to exchange information in the diagnosis, treatment and prevention of disease. While not yet broadly adopted across the U.S., telemedicine’s use in reproductive health care has shown promise in offering innovative solutions to unmet health needs, particularly in areas with few health care providers. Leading medicalgroups endorse telemedicine in bolstering reproductive health services and expanding access for rural women. This brief presents an overview of telemedicine’s current use in sexual and reproductive health care, and reviews considerations in its coverage, potential to improve access, and financial implications for providers and patients.
Telemedicine Background
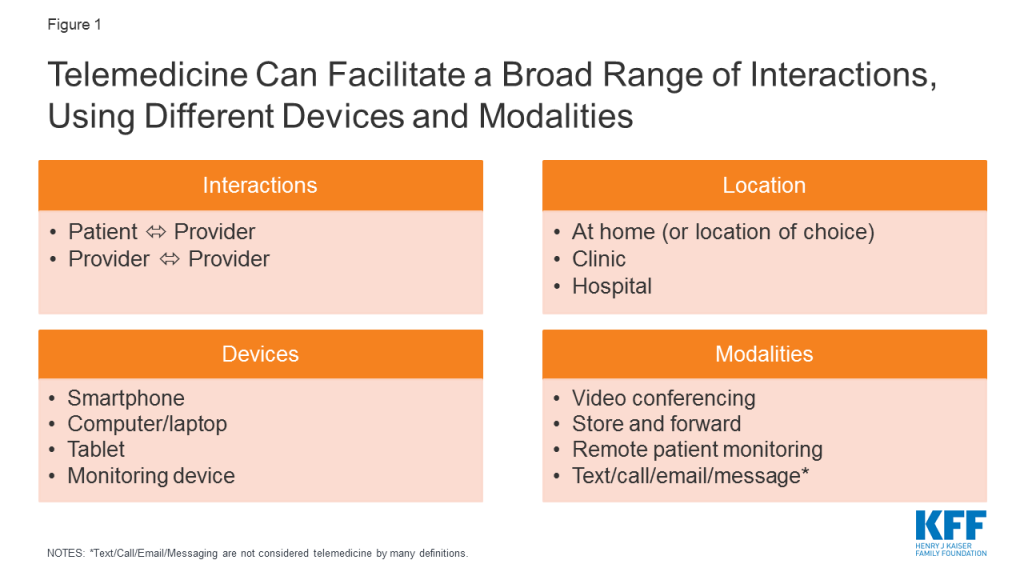
Varied definitions for telemedicine and telehealth exist. In the broadest definition, telemedicine can include basic telecommunication tools like phone calls, text messages, emails, faxes and online patient health portals that allow patients to schedule appointments, read appointment summaries, view lab results and communicate with their providers. Many health care organizations and insurers, however, adopt a narrower definition, typically involving three specific telemedicine modalities:
Videoconference: real-time exchange of information via video. Example: patient has an appointment on a web-based platform with a clinician.
Store and forward: an online consultation in which patient information is sent to a remote clinician, who later sends back diagnostic/treatment recommendations.
Remote patient monitoring: patient’s home monitoring device sends data to clinician for review. Example: home blood sugar data sent to doctor remotely.
Telemedicine facilitates remote interactions between patients and providers or between providers of different specialties, originating from health care facilities or a patient’s home (Figure 1). A patient may see their usual provider during a telemedicine visit, remaining within their existing health care system, or may interact with remote providers they have never met before, for example on a third party application.
Figure 1: Telemedicine Can Facilitate a Broad Range of Interactions, Using Different Devices and Modalities
Due to its diverse functions, telemedicine has long been touted as a method to increase health care access, focused on rural populations where clinicians are scarce. KFF’s 2017 Women’s Health Survey revealed many women, particularly low-income women, delay or forgo necessary health care due to problems obtaining transportation or childcare, indicating that telemedicine could be beneficial in low-income, urban populations as well.
Despite its potential, patient use of telemedicine appears small. An analysis of private insurance claims by FAIR Health reveals telemedicine use grew 14-fold for non-hospital patient-provider interactions from 2014-2018, but still represented only a small fraction of all medical claims (0.1%). Urban areas experienced more growth than rural, and the majority of utilizers were women (65%) and ages 31-40 (21%). Patients may be reluctant to adopt telemedicine, preferring in-person visits to videoconferencing, and establishing rapport via video poses challenges to patient engagement. In a study of health care consumers, 43% of respondents thought telehealth visits would be less personal than traditional services, and 49% perceived the quality of care to be lower. Since users may engage with different providers each time they utilize telemedicine, continuity of care may be disrupted as well.
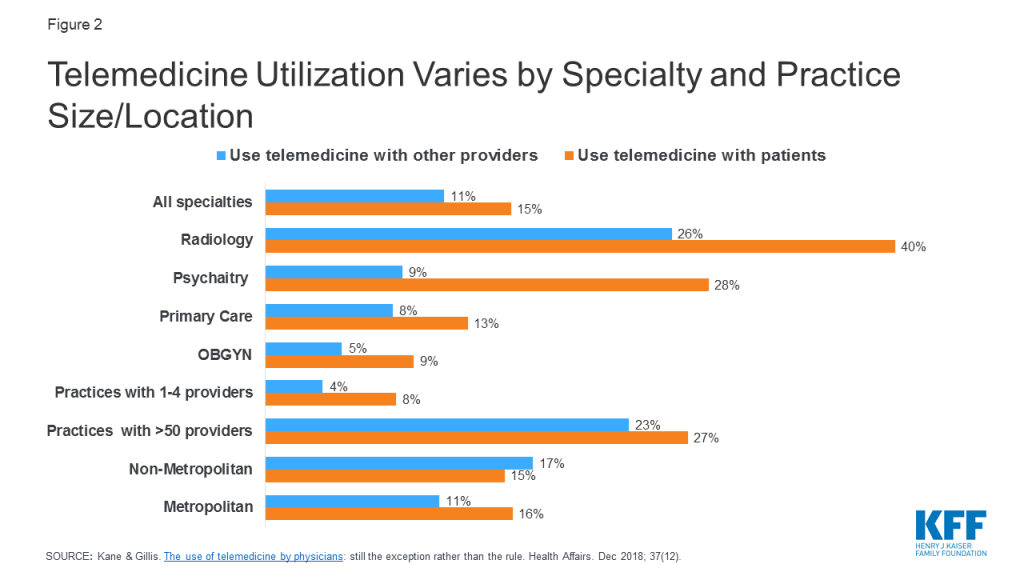
Among providers, a 2016 survey of physicians found just 15% of physicians worked in practices offering telemedicine services, with primary care providers and OBGYNs using telemedicine considerably less than specialties like radiology and psychiatry (Figure 2). Uptake for telemedicine was notably higher among larger practices, and in non-metropolitan areas for provider to provider interactions.
Figure 2: Telemedicine Utilization Varies by Specialty and Practice Size/Location
Reproductive Health Services in Telemedicine
A broad range of gynecologic and obstetric services can be offered via telemedicine, including contraception, medication abortions, STI care, prenatal care, and limited applications in OB-Psychiatry, men’s sexual health and care for sexual assault victims (Table 1). The modalities of delivery and levels of patient-provider interaction vary across these services.
Table 1: Scope of Reproductive Health Services in U.S. Offered via Telemedicine
UAMS, Mayo Clinic, BabyScripts (partnering with GWU, Penn Medicine, MedStar Health, UTHealth, Medical University of South Carolina, etc.)
Video consultation with specialists
University of Pittsburgh
Obstetrics & Mental Health
Prenatal OB-Psych care
University of Arkansas for Medical Sciences (UAMS)
Postpartum depression care
Chiron Health, Amwell
Men’s Sexual Health
Treatment for erectile dysfunction, premature ejaculation
Roman
Sexual Assault
Video consultation with forensic sexual assault nurse examiners
Penn State SAFE-T center
KFF Analysis of Outpatient Telemedicine Utilization in Reproductive Health Care
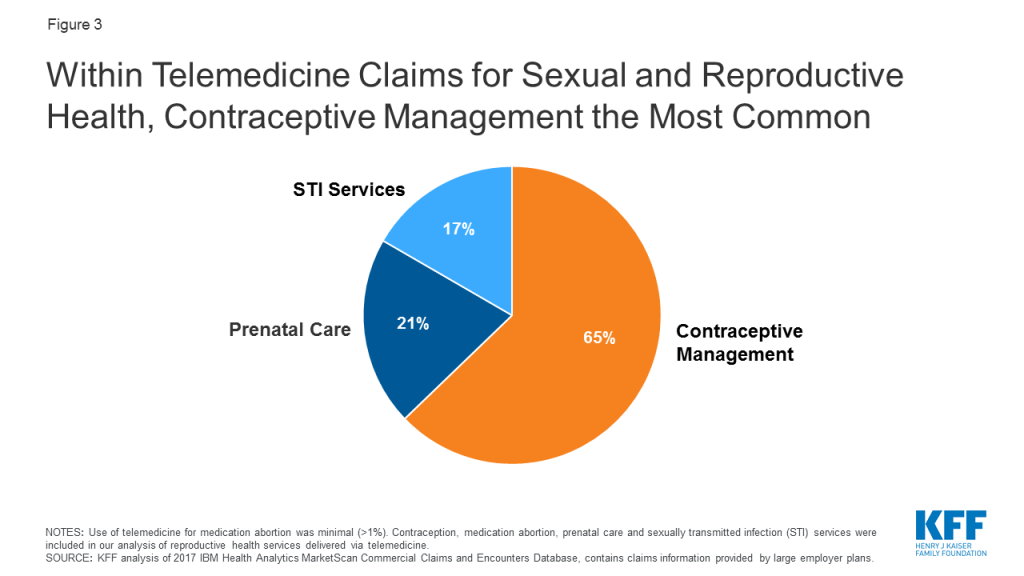
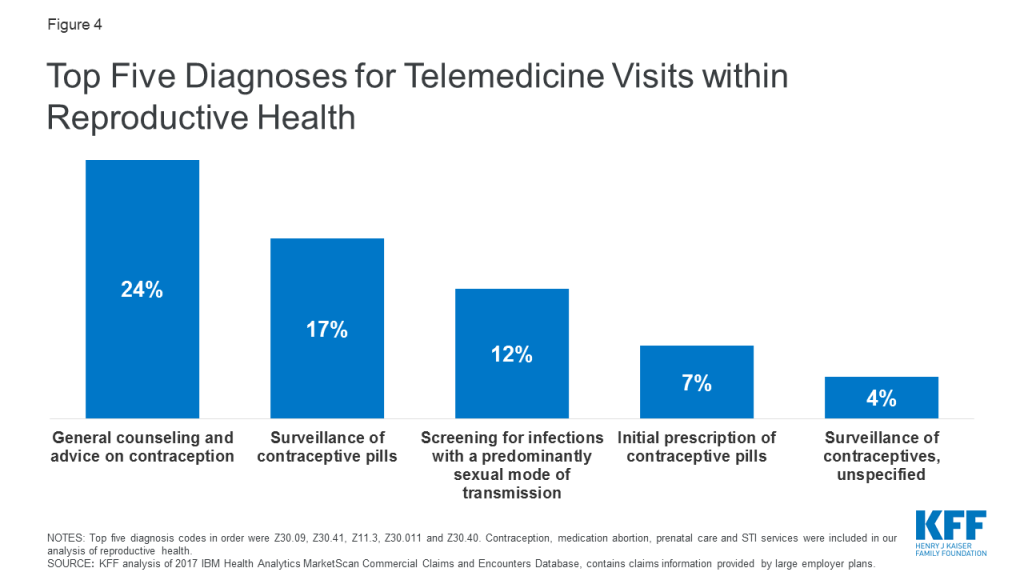
Use of telemedicine in reproductive health care is minimal. KFF analyzed outpatient telemedicine utilization among individuals with large employer sponsored health plans, using the 2017 IBM Health Analytics MarketScan Commercial Claims and Encounters Database. 51,758,413 weighted claims were analyzed within the reproductive health categories of contraceptive management, medication abortion, prenatal care, and STI testing and treatment. 11,089 of these claims were delivered via telemedicine, meaning telemedicine services accounted for just 0.02% of all reproductive health claims.1 Within telemedicine claims for reproductive health, visits for contraceptive management were the most common (65%), followed by prenatal care (21%) and STI services (17%). Use of telemedicine for medication abortion was minimal (<1%) (Figure 3). The most frequent reproductive health diagnosis codes for telemedicine claims are shown in Figure 4. These data do not capture use of telemedicine on platforms that do not accept private insurance, or by patients with public insurance or no insurance.
Figure 3: Within Telemedicine Claims for Sexual and Reproductive Health, Contraceptive Management the Most CommonFigure 4: Top Five Diagnoses for Telemedicine Visits within Reproductive Health
Contraception
The most effective forms of birth control, including long acting reversible contraceptives (LARCs), require in-person care, but providers can prescribe a variety of other contraceptive methods via telemedicine, including oral contraceptive pills (OCPs), the patch and vaginal ring. As of June 2019, 14 online OCP platforms existed in the U.S. All determine eligibility and prescribe OCPs in the same general manner:
Using a smartphone or computer, the patient provides a health history via a questionnaire or video consultation with a clinician.
The clinician reviews the information remotelyand determines eligibility for OCPs. The provider may be a doctor, nurse practitioner, physician assistant or certified nurse midwife, often depending on state law.
The patient receives the OCPs by pharmacy pick-up or mail. Prescriptions are valid for 3-12 months, with a 1-12 month supply at a time, depending on the platform and insurance provider.
Almost all risk factors precluding use of hormonal birth control can be assessed online; evaluations screen for age, smoking history, and conditions posing significant health risks including clotting disorders, heart disease, breast cancer, and migraines with aura. These platforms cannot measure blood pressure, typically a necessity before initiating OCPs, but most require the user input a reading from the last year; the CDC deems this method acceptable if a provider cannot measure the blood pressure.2 A study of 9 telecontraception platforms found OCPs were prescribed when contraindicated in 3 of 45 visits, but adherence to CDC Medical Eligibility Criteria actually may be higher than for in-person visits. This suggests telemedicine prescription of OCPs is safe, as compared to traditional care.
Select platforms offer emergency contraception (Table 1). While levonorgestrel (LNG)/Plan B One Step can be accessed over the counter, ulipristal acetate (UPA)/Ella, requires a prescription. UPA is more effective in preventing pregnancy than LNG, especially for overweight and obese individuals, and can be taken up to 120 hours after unprotected sex (LNG has a 72 hour limit). Telemedicine prescription of UPA could allow for quicker and broader access to this medication.
Cost and coverage
Out of pocket costs for OCPs via telemedicine includes the consult fee, contraceptive product and delivery fee. Across the available platforms, a patient can expect to pay anywhere from $0 to more than $170 for the OCP prescription and a 1 month supply. This can total an average $313 per year (range $67to $519) for an uninsured patient according to a recent study. Many platforms accept private insurance to cover the cost of the contraceptive product, but not necessarily the consult or delivery fee. Some platforms do not accept any insurance plans, and almost none accept Medicaid (Table 2). Limited information is available on the cost of other types of contraception (patch, ring).
Under the ACA, most private insurance plans are required to cover FDA-approved contraceptive services and supplies without cost-sharing to the patient, but the providers must be in-network which is not always the case for telemedicine. Medicaid programs are similarly required to cover family planning services without cost-sharing to the patient, but because many platforms do not accept insurance, particularly public insurance, insurers may not reimburse patients for these applications. Therefore, telemedicine users pay more for contraception out of pocket than those who have an in-person visit with an in-network provider, which most plans are required to cover in full.
Table 2: Estimated Out of Pocket Costs for Oral Contraceptive Pills Prescribed via Telemedicine
OCPs via telemedicine are available in all 50 states, D.C., Puerto Rico and the U.S. Virgin Islands, from at least two vendors per state. That said, most telemedicine platforms only operate in specific states, likely due to challenges expanding across state lines. For example, TwentyEight Health only prescribes to NY and NJ residents, while PRJKT RUBY is available in 49 states and Planned Parenthood Direct will operate in all 50 states by the end of 2020.
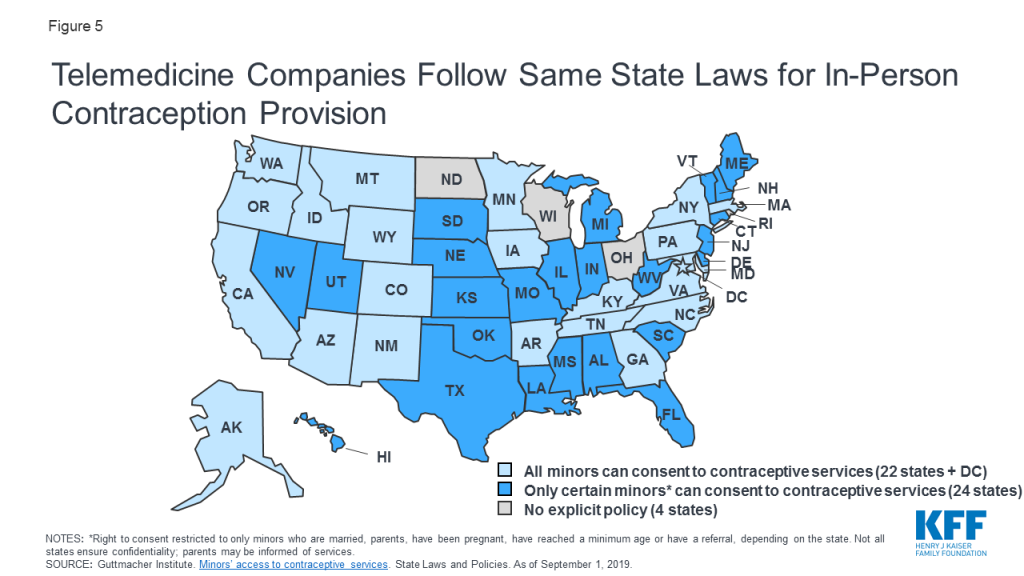
To date, no policies specifically prohibit the use of telemedicine for contraception. Rather, telemedicine services for contraception follow the same state laws as do in-person services. For example, many telemedicine platforms for contraception have an 18+ age requirement, often in accordance with state laws (Figure 5). Several platforms also impose upper age limits, typically from 35-50 years old, likely due to safety concerns.
Figure 5: Telemedicine Companies Follow Same State Laws for In-Person Contraception Provision
Abortion
Medication abortions use medications to terminate pregnancy, most commonly mifepristone and misoprostol. Medication abortions are FDA approved until 10 weeks gestation, are highly safe and effective and account for approximately 39% of all abortions. Due to the myriad of restrictions on abortion, many communities do have not have access to medication abortion, and even in places where it is available, some states require patients have at least two visits to obtain the pills.
Table 3: Delivery Models for Telemedicine Medication Abortion
Model
Example
Description
Availability
Safety & Efficacy
Site-to-site
Planned Parenthood (PP)
1. Patient goes to participating PP clinic for intake appointment and ultrasound.
2. Remote PP provider reviews history and imaging. If eligible, provider remotely unlocks medication drawer in patient’s room.
3. Patient takes mifepristone in clinic, misoprostol at home.
1. Patient goes to any nearby clinic for pre-treatment labs and ultrasound.
2. Patient sends results to TelAbortion study, provider determines eligibility.
3. If eligible, patient mailed medications.
4. Follow up via phone or videoconference.
8 states: CO, GA, HI, ME, NM, NY, OR, WA
Found to be safe, feasible and acceptable to patients (Raymond et al. 2019).
Fully Remote
Women on Web
1. Patient fills out online questionnaire.
2. Provider remotely reviews info.
3. If eligible, patient receives medications by mail.
Process may require in-person visits if determined to need ultrasound or RhoGAM.
Not available in U.S.
Studies in Ireland and across 33 countries finds method is effective, low rates of adverse events (Aiken et al. 2017, Gomperts et al. 2008). May increase surgical intervention risk (Gomperts et al. 2014).
To address limited access, Planned Parenthood pioneered the first telemedicine medication abortions in the U.S. in 2008. Their protocol is classified as a “site-to-site” model, whereby a clinician remotely prescribes medication abortions by collaborating with Planned Parenthood centers that do not have on-site abortion providers; the patient receives their labs, ultrasound and medications all from their local Planned Parenthood clinic (Table 3). Alternatively, the TelAbortion study, a FDA-approved clinical trial run by Gynuity Health Projects, uses a “direct-to-patient” model. In this model the patient consults with a remote clinician, obtains labs and an ultrasound from any nearby clinic, and if deemed eligible, receives their medications by mail. While in-person services are still required, the difference between this and “site-to-site” is the freedom for patients to obtain pre-treatment tests from any convenient medical facility, rather than only partnering sites. Both the TelAbortion and the Planned Parenthood protocols have been shown to be safe, effective and acceptable to patients when compared to in-person care, but are only available in certain states.
Efforts are underway to provide telemedicine abortions without ever visiting a health care facility. In this “fully remote” model, the patient completes an online questionnaire to assess (1) confirmation of pregnancy, (2) gestational age and (3) blood type. If determined eligible by a remote clinician, the patient is mailed the medications. This model does not require an ultrasound for pregnancy dating if the patient has regular periods and is sure of the date of their last menstrual period (in line with ACOG’s guidelines for pregnancy dating). If the patient has irregular periods or is unsure how long they have been pregnant, they must obtain an ultrasound to confirm gestational age and rule out an ectopic pregnancy3 and send in the images for review before receiving their medications. If the patient does not know their blood type or has Rh negative blood, the provider may prompt the patient to visit a nearby clinic for an injection to prevent adverse reactions between maternal and fetal blood (RhoGAM), if indicated.
Women on Web successfully implements this model in multiple countries outside of the U.S. Multiple studies find their service is safe and effective, but may lead to small increased need for surgical intervention. AidAccess started offering this model in the U.S, using a remote physician in Europe and a pharmacy in India. This delivery system blends into the concept of “at-home” or “self-managed” abortions, however in telemedicine abortions, a clinician is always involved in the safe prescribing of these medications. The FDA issued a cease and desist letter to AidAccess as this service is not currently legal in the U.S.
Cost and coverage
Cost estimates for telemedicine abortions are not readily found. Per TelAbortion’s website, costs will depend on the patient’s state, required tests and insurance coverage, but the study will provide a cost estimate before enrolling. Similarly, patients must call their nearest Planned Parenthood for telemedicine abortion cost estimates. For in-person care, the Turnaway study found the average out of pocket cost to be $461 for a first trimester medication abortion across 30 U.S. sites; women also spent from $0 to $2200 (mean of $54) on related travel costs. Telemedicine abortions may cost similar to those in-person, but patients may save on transportation, childcare and lost wages.
Insurance coverage for abortion can be limited. The Hyde Amendment prohibits use of federal funds for abortion except in cases of rape, incest or endangerment to the woman’s life. This limits abortion funding for Medicaid enrollees, federal employees, and those covered by the military, Veterans Affairs, and Indian Health Service. In addition, several states restrict abortion coverage in private insurance plans (though most people with employer-provided health coverage are in self-insured plans, outside the reach of state restrictions). This means many people who obtain abortions incur out of pocket fees, regardless of their insurance plan. Should telemedicine abortions become more widely available, these limitations would apply.
Access and policy
Telemedicine services must abide by the same regulations as those for equivalent in-person services. Therefore, the multitude of laws enforced for in-person abortion services, including physician and hospital requirements, gestational limits, waiting periods, and age restrictions, all apply to telemedicine abortions. Telemedicine abortions are then subject to additional prescribing barriers described below.
Prescribing Barriers
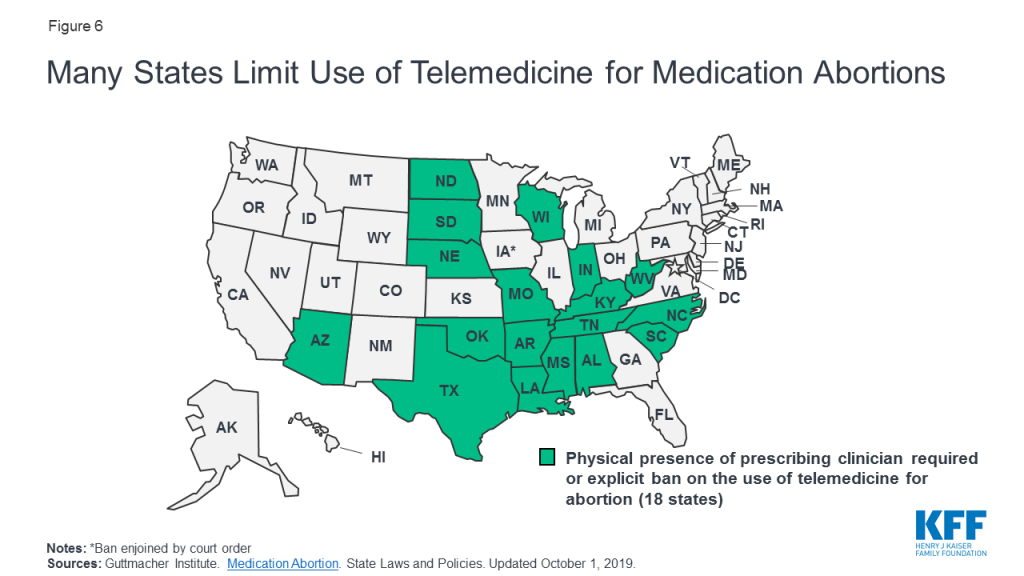
A few states explicitly prohibit use of telemedicine in abortions (AZ, KY), while 18 states require the prescribing clinician be physically present with the patient for a medication abortion. This effectively prohibits all telemedicine abortions in those states (Figure 6). Indiana also prohibits prescription of medication abortions if the prescriber has not previously examined the patient in-person.
Figure 6: Many States Limit Use of Telemedicine for Medication Abortions
Telemedicine abortions are further limited by the FDA Risk Evaluation and Mitigation Strategy (REMS) on mifepristone, despite its exceedingly low rate of adverse events. Mifepristone’s REMS means it may only be dispensed by certified providers in clinics and hospitals, and is not available in commercial pharmacies or by mail like most other medications. The REMS also requires a prescriber and a patient agreement form before dispensing the medication, complicating remote provision of abortions. TelAbortion obtained a FDA waiver for their telemedicine study, allowing them to mail mifepristone directly to patients which is normally prohibited. If the REMS for mifepristone were lifted, the availability of medication abortions by telemedicine would likely increase.
What is a Risk Evaluation and Mitigation Strategy(REMS)? A REMS creates a strategy for medication prescribing, typically to decrease adverse events for drugs with safety concerns. 59 drugs currently require a REMS due to their life-threatening side effects, including several opioids, antipsychotics and cancer treatments. Mifepristone is associated with low rates of adverse events, and many urge for its REMS to be removed.
Scope of Practice
While not specific to telemedicine, 34 states only allow licensed physicians to prescribe medication abortions, excluding advanced practice clinicians (APCs) like nurse practitioners, certified nurse midwives and physicians assistants. For APCs trained in abortion care, multiple studies show their skills are safe and comparable to those of physicians. By reducing the number of providers allowed to offer abortions, the use of telemedicine abortion is indirectly limited.
STI Care
Several mobile apps and online services provide STI consultation, testing and treatment (Table 4). Most allow users to select a testing panel, which they then obtain through in-person lab centers like Quest or LabCorp. Some platforms offer at-home collection kits, where the consumer mails in self-collected samples to a lab for testing; this could involve self-collection of urine, a vaginal, rectal or oral swab or a finger prick blood sample. For positive results, several platforms offer provider consultation and prescribe treatment for select STIs (typically gonorrhea, chlamydia, trichomonas and herpes), with medications shipped home or ordered to a pharmacy. For some positive results, however, including HIV and syphilis, users would be prompted to seek in-person care for an exam and additional testing. Telemedicine STI testing may be ideal for individuals who are asymptomatic but may have been exposed to a STI after unprotected sex, but if the patient is showing symptoms, an in-person exam is still typically needed. Select platforms do not require testing before STI treatment, particularly for expedited partner therapy or acute flares of known herpes infections, and others prescribe PrEP (pre-exposure prophylaxis) for the prevention of HIV. Most platforms offer care to all genders, but Roman specializes in men’s sexual health.
Telemedicine has also been used to evaluate risk for cervical cancer. Nurx and Binx Health offer at-home HPV screening, to test for the strains of HPV that cause genital warts and cervical cancer; patients still require in-person pap smears to check the cervix for cancerous or pre-cancerous cells. For women with abnormal pap smears who need colposcopies, one study trialed transmitting live images of the cervix to a remote provider to determine the need for a biopsy or further testing. This study was limited by low quality images, and resulted in additional testing for patients.
Telemedicine care may be appealing to individuals who do not feel comfortable seeking in-person STI care due to stigma or privacy concerns; that said, not all mobile apps comply with the Health Insurance Portability and Accountability Act (HIPAA). Some consumers may doubt their ability to self-collect samples for testing, but studies show this collection method is feasible and acceptable to most patients, may increase uptake of testing by patients, and yields test results comparable in accuracy to clinician-collected samples for HPV, trichomonas, gonorrhea and chlamydia. The only FDA approved at-home HIV test requires the user collect an oral swab, test the sample and read the results at home; studies reveal false negative results are more common than for in-clinic testing using this method. More often however, telemedicine platforms have users mail in self-collected samples to a lab; the accuracy of this method compared to in-clinic testing remains unclear. False negatives may also occur if users order tests too soon after unprotected sex. To ensure quality results, users should look for platforms using FDA approved tests and labs accredited by the College of American Pathologists (CAP) and certified under the Clinical Laboratory Improvement Amendments (CLIA).
Table 4: Examples of STI Services Available via Telemedicine
NOTES: This is not an exhaustive list of all telemedicine platforms offering STI care.*The cost of STI testing panels varies based on the number of type of tests ordered.Abbreviations: CLIA: Clinical Laboratory Improvement Act. CAP: College of American Pathologists. HIPAA: Health Insurance Portability and Accountability Act
Cost and coverage
STI care via telemedicine can come with significant out of pocket costs to the patient (Table 4). While some platforms accept private insurance, most do not accept Medicaid, and many do not accept any insurance plans. Scant data exists comparing out of pocket costs for STI care using telemedicine to in-person care, however for most patients, telemedicine could cost more; this is because the ACA requires most private insurance plans and states with Medicaid expansion to cover recommended STI counseling and screening at no cost sharing to the patient. By 2021, state Medicaid programs and most private insurances will be required to cover the cost of PrEP for individuals at risk for HIV with no patient cost-sharing. For uninsured patients, STI services are often covered at no or low cost at publicly funded STI clinics, while these individuals would pay full price for telemedicine services. That said, insured individuals may not use their coverage to pay for STI care; in a study of U.S. STD clinics, 62% of patients with private insurance, 65% of patients on their parent’s insurance and 37% of patients on Medicaid were not willing to use their insurance for their visit, opting to pay out of pocket presumably due to privacy concerns. Individuals may be willing to pay more out of pocket for telemedicine in exchange for greater anonymity and forgoing in-person interactions.
Access and policy
Some telemedicine platforms for STIs operate in all 50 states, whereas others are restricted to certain regions (Table 4). Most platforms place age restrictions on its users; for example you must be ≥13 years old to access STI testing through Nurx and ≥18 for PlushCare. These limits are often more restrictive than state laws regarding minors and STI care; as of August 2019, minors in all 50 states and DC can consent to STI services, although 11 states require a minimum age (typically 12-14 years old). Most states do not mention STI care in their telemedicine reimbursement laws, but select states do. For example Texas and New Mexico specifically do not require in-person evaluation before expedited partner therapy, allowing telemedicine’s use for these cases.
Crosscutting Issues
State Regulation
All 50 states and D.C. define, regulate and reimburse for telemedicine differently. According to the Center for Connected Health Policy’s (CCHP) report on state telehealth laws, in 2018 over 160 telemedicine related bills were introduced, reflecting the field’s ever-changing policy landscape. This complexity creates challenges for patients in knowing what services are covered, and for providers who must ensure they comply with evolving state laws. Below we outline key issues related to the regulation and reimbursement of telemedicine. For the most up to date information, CCHP provides an interactive tracking tool for state and federal legislation regarding telehealth policy.
Licensing and Malpractice
Clinicians must be licensed to practice in states where they offer telemedicine services. For example, if a clinician is located in CA, but is providing services remotely to a patient in MA via telemedicine, the provider must be licensed in MA, the state where the patient is located. Nine states require special licenses specific to telemedicine (AL, LA, ME, NV, NM, OH, OR, TN, TX). Others participate in “compacts” that allow providers in participating states an expedited process to practice in other compact states. As of October 2019, 34 states participate in the enhanced Nurses Licensing Compact, and 29 states and D.C. participate in the Physician’s Interstate Medical Licensure Compact. Clinicians must also ensure their malpractice insurance covers telemedicine and services provided across state lines. Insurance premiums may be higher if covering telemedicine, and Hawaii is the only state to require malpractice carriers to offer telemedicine coverage.
Online prescribing
Most states require a patient-provider relationship be established before e-prescribing of medications. Many telemedicine platforms use an online health questionnaire to establish that relationship, but in at least 15 states, this method is considered inadequate (AR, CO, DE, FL, HI, ID, IA, KS, KY, LA, ME, MO, NM, WA, WI). Instead, a physical exam would be required before prescribing, either in-person, by live-video, or by a referring physician, depending on the state. Therefore, in certain states an app prescribing OCPs may need to establish the patient-provider relationship via live-video, rather than a questionnaire. Examples of online prescribing laws addressing telemedicine are shown below (Table 5).
Table 5: Examples of State Laws Addressing Prescribing Medications via Telemedicine
A patient completing a medical history online and forwarding it to a physician is not sufficient to establish the relationship, nor does it qualify as store-and-forward technology.
Pharmacists are prohibited from dispensing prescription drugs on the basis of an internet-based questionnaire or a telephone consultation, without a valid pre-existing patient-practitioner relationship.
Prohibits providers from issuing prescriptions without establishing an ongoing physician-patient relationship (exceptions apply).
NOTES: This table highlights common regulations but it not an exhaustive list of online prescribing laws.SOURCE: Center for Connected Health Policy. Current State Laws and Reimbursement Policies. Fall 2019.
Reimbursement and Coverage
Payment structures for telemedicine are relatively new and currently evolving; therefore, reimbursement and coverage vary by how each state chooses to regulate Medicaid and private insurance plans. Restrictions to telemedicine’s coverage often falls into one or more of the following categories:
Provider specialty: limiting reimbursement to specific medical specialties (example: covering psychiatry and radiology but not OBGYN).
Type of provider: limiting reimbursement to certain provider types (example: covering a visit with a physician, but not a nurse practitioner).
Type of modality: limiting reimbursement to specific modalities (example: live video reimbursed more often than store-and-forward or remote patient monitoring).
Patient condition: limiting reimbursement to certain conditions, like diabetes.
Location of patient/“originating” site: limiting the location a patient can be while engaging in the telemedicine service (example: excluding the patient’s home).
Medicaid
All states have laws determining which telemedicine services their Medicaid programs will cover, and for how much they will be reimbursed. These laws are not specific to reproductive health care, and may only cover certain specialties, providers, modalities, conditions and originating sites. While 50 states and D.C. reimburse for some forms of live videoconferencing, most limit coverage to certain specialties (typically behavioral health) and a few explicitly exclude OBGYN or abortion care (Appendix). Fewer states reimburse for store-and-forward services or remote patient monitoring, and often only certain services are covered like radiology or dentistry, or certain diagnoses like congestive heart failure. Eight states reimburse for some forms of all three modalities, but patients would still need to check with the specifics of their state’s plan to ensure coverage (Figure 7).
Figure 7: State Medicaid Policies Regarding Payment for Telemedicine Services Vary
Telemedicine has the potential to increase convenience and minimize travel by allowing patients to access services from their home. However, only 19 state Medicaid programs explicitly allow the patient’s home as the originating site. In the remaining states, telemedicine may not be covered if the patient is at home or a non-clinical site. The Centers for Medicare and Medicaid Services (CMS) has shown interest in expanding the use of telemedicine; while not as applicable to most reproductive-aged individuals, CMS will expand telehealth benefits to Medicare Advantage beneficiaries in 2020, allowing a patient’s home as the originating site. State telemedicine laws are evolving, and in the future, public insurance plans may cover more services as familiarity with how to pay for this care increases.
Private insurance
KFF’s Employer Health Benefits Survey reveals coverage for telemedicine by large employers has increased significantly in recent years; the share of large firms offering telemedicine health benefits grew from 27% in 2015 to 82% in 2019, indicating promising growth for the field. 41 states and D.C. have laws governing reimbursement for telemedicine services in private plans (although laws in GA are not currently in effect). As with Medicaid, private payer laws vary based on the services, specialties and providers they cover. In approximately half of states, if telemedicine services are shown to be medically necessary and meet the same standards of care as in-person services, private insurance plans must cover telemedicine services if they would normally cover the service in-person, called “service parity.” CCHP finds only 6 states (CA, DE, GA, HI, MN, NM) require telemedicine services to be reimbursed at the same rate as equivalent in-person services, called “payment parity;” our analysis of telehealth laws suggests an additional 4 states follow payment parity as well (AR, CO, KY, NJ). In the remaining states, telemedicine is typically reimbursed at lower rates than equivalent in-person care.
Low Uptake
Based on which definition of telemedicine is used, utilization estimates vary widely. In a study by Definitive Health Care, 44% of outpatient providers reported utilizing telehealth, including applications like video conferencing, online consults, RPM and patient portals for lab results, appointment notes and prescription instructions. Uptake of telehealth appears similarly robust in a recent report, Life in Rural America; of 695 women surveyed, 26% of participants reported ever receiving a diagnosis or treatment from a provider using email, text messaging, a mobile app, live video or telephone.
By contrast, most researchers analyzing insurance claims adopt a narrower definition of telemedicine, excluding applications like phone, email and patient portals, while focusing on videoconferencing, RPM and store and forward services. Using these parameters, telemedicine utilization appears minimal. In a KFF analysis of claims data among enrollees of large employer sponsored private health plans, less than 1% of people utilized outpatient telemedicine visits in 2016. Among Kaiser Permanente patients, <5% utilized video visits from 2015-2017, but those who did reported high patient satisfaction.
Telemedicine has yet to gain traction in underserved populations; a 2013-2016 analysis published in Health Affairs revealed utilization of telemedicine among Medicaid, low income and rural populations was significantly lower than individuals with private insurance, higher incomes and in suburban and urban settings, respectively, despite most of these individuals being willing to use telemedicine. These data suggest low income and rural communities are not currently reached by telemedicine to the degree its proponents may have intended.
Investment Costs in Telemedicine Technology:
Significant logistical and financial challenges come along with establishing a telemedicine program at a health center or as a third-party app. The telemedicine platform should be compliant with the Health Insurance Portability and Accountability Act (HIPAA) and often must integrate into an existing electronic health record. This represents a significant financial investment, and outpatient centers are divided regarding their interest in telemedicine; providers cite issues such as satisfaction with their current services without telehealth, lack of clarity in reimbursement and inability to justify the investment due to lack of financial return as reasons they are not interested in investing in telemedicine services. To help with investment costs for rural providers, the Federal Communications Commission’s Rural Health Care Program has recently approved a three-year program allocating $100 million for expanding telemedicine use in low-income rural areas, offering broadband and telecommunications services at discounted prices.
Beyond startup costs, the cost of telemedicine to the health system as compared to in-person care remains unclear. Certain studies show telemedicine visits are less costly than in-person care, particularly for emergency room visits. This cost savings may be offset by increases in new utilization of the health system; one study found 88% of telehealth visits represented new utilization of the health system by those who would otherwise not seek in-person care, leading to increased overall cost. By contrast, another study found decreased follow up visits among telemedicine users, contributing to overall cost savings to the health system. As telemedicine use expands, further analysis on this topic would help elucidate the cost of telemedicine to the health system, and to patients.
Looking Forward
Access to reproductive health care, including comprehensive contraception and abortion care, is being curtailed in many communities across the U.S. While telemedicine remains a promising tool to address this unmet need, utilization of telemedicine among patients remains low. For some services, including OCP prescriptions and self-collection STI testing, telemedicine can largely function separately from the existing health system. Meanwhile for other services, including abortion care and in-lab STI testing, users must still link to in-person care, making telemedicine an adjunct to the existing health system. Notably, in-person care is still required for more effective methods of contraception like LARCs, for confirmatory testing and treatment of HIV, and for many preventative services like pap smears and pelvic exams. Significant implementation barriers exist to telemedicine’s growth, including state policies limiting its use, variable insurance coverage and high start-up investment for health centers. The future of telemedicine will likely depend on increasing availability, expanding insurance coverage and increasing reimbursement, alignment of regulatory policies and broadening outreach efforts to underserved populations who could benefit from these technologies.
Appendix
Appendix 1
Reimbursement Requirements for Medicaid Programs and Private Payers Vary Widely State to State
Medicaid reimburses for the following telemedicine services…(Restrictions on services, conditions, providers and sites apply)
Private payers reimburse(Restrictions apply)
Live Video?
Store and Forward?
At-home Remote Patient Monitoring?
Email Phone Fax?
Home as originating site?
For some telemedicine services?
Telehealth at same rate as in-person care?
AL
✓
X
✓ Only for DM & CHF
X
X
X
X
AK
✓
✓
✓
X
X
X
X
AZ
✓ Includes OBGYN, excludes abortion
✓Excludes OBGYN & primary care
✓ For CHF
X
X
✓Excludes abortion
X
AR
✓Excludes abortion
X
X
X
X
✓Excludes abortion
✓
CA
✓
✓
X
Some
✓
✓
✓*
CO
✓
Dental
✓
X
✓
✓
✓
CT
✓Behavioral health only
✓Provider to provider only
X
Some
X
✓
X
DE
✓
X
X
X
✓
✓
✓
DC
✓
X
Xb
X
X
✓
X
FL
✓Behavioral health only
X
X
X
X
✓
X
GA
✓
✓ Ultrasound, X-ray, dentistry only
X
X
X
✓*
✓*
HI
✓
Xa
Xb
X
✓g
✓
✓
ID
✓Includes primary care
X
X
X
X
X
X
IL
✓
X
✓Uterine monitoring and BP in pregnancy
X
X
✓
X
IN
✓Excludes abortion
X
✓
X
X
✓Excludes abortion
X
IA
✓ Excludes abortion
X
Xc
Some
X
✓Excludes abortion
X
KS
✓Excludes abortion
X
✓
X
X
✓Excludes abortion
Xd
KY
✓
Radiology only
X
X
✓
✓
✓
LA
✓
X
✓
X
X
✓
X
ME
✓
X
✓
Some
X
✓
Xd
MD
✓
✓
✓
X
✓
✓
X
MA
✓Behavioral health only
X
X
X
X
✓
X
MI
✓
X
X
X
✓
✓
X
MN
✓
✓
✓
X
✓
✓
✓
MS
✓
Radiology only a
✓
X
X
✓
X
MO
✓
X
✓ Includes pregnancy
X
X
✓
X
MT
✓
X
X
X
✓
✓
X
NE
✓
Radiology only
✓
X
X
✓
X
NV
✓
✓
X
X
✓
✓
X
NH
✓
Xa,e
Xe
X
✓
✓
X
NJ
✓ Behavioral health only
X a
Xb
X
✓
✓
✓
NM
✓
✓
X
X
X
✓
✓
NY
✓
✓
✓
X
✓
✓
X
NC
✓
X
X
X
X
X
X
ND
✓
X
X
X
X
✓
Xd
OH
✓
X
X
X
✓
✓
Xf
OK
✓
X
X
X
X
✓
X
OR
✓
Dental
✓
Some
X
✓
X
PA
✓
X
X
X
X
X
X
RI
✓
X
X
X
X
✓
X
SC
✓
X
✓
X
✓
X
X
SD
✓
X
X
X
X
✓
X
TN
✓ Crisis-related only
✓
X
X
X
✓
X
TX
✓Excludes abortion
✓Only w/ real-time audio
✓Includes pregnancy
X
✓
✓ Excludes abortion
X
UT
✓
X
✓
X
X
✓
X
VT
✓
X
✓For CHF
X
✓
✓
X
VA
✓Includes OB ultrasound
✓Excludes OBGYN & primary care
✓Includes DM in pregnancy
X
X
✓
X
WA
✓Behavioral health & dentistry
✓Excludes OBGYN & primary care
✓
X
✓
✓
X
WV
✓
X
X
X
X
X
X
WI
✓
X
X
X
X
X
X
WY
✓
X
X
X
✓
X
X
Total states
50 + DC
14
22
5
19
41 + DC
10
NOTES: Telemedicine services must typically be shown to be equivalent to in-person services to meet reimbursement requirements.CHF= Congestive heart failure*Law exists but not currently in effect.|a HI, MS, NH, NJ have laws requiring reimbursement for store and forward in Medicaid, however are not in effect or do not have corresponding policy indicating enforcement.b DC, HI, NJ have laws requiring reimbursement for remote patient monitoring in Medicaid, however are not in effect or do not have corresponding policy indicating enforcement.c Iowa supposed to start remote patient monitoring program in July 2019 for Medicaid Managed Care plans.d Reimbursement has to be determined “in a manner consistent with” in-person services, but does not mention that the payment needs to be the same.e NH voted to expand Medicaid coverage to store and forward and remote patient monitoring, effective in 2020.f Ohio recently passed HB 166 recently passed on 7/18/19, telemedicine services be reimbursed at the same rate as equivalent in-person services, for health benefit plans issues or renewed as of 2021.g In statute, HI includes a patient’s home as eligible originating site, but not included in Administrative Rules.SOURCE: Center for Connected Health Policy. Current State Laws & Reimbursement Policies. Updated Oct 15, 2019.
Endnotes
KFF analyzed a sample of medical claims obtained from the 2017 IBM Health Analytics MarketScan Commercial Claims and Encounters Database, which contains claims information provided by large employer plans. We only included claims for women ages 15-44 who were enrolled in a plan for more than half a year. We defined outpatient telemedicine utilization to include any clinical interaction between a patient and health care provider (physician or non-physician), delivered via live-video, remote patient monitoring, store and forward technology or telephone. Telehealth claims were captured using procedure modifiers specific to telehealth, including GT and 95 for synchronous telecommunication and GQ for asynchronous telecommunication, and “place of service 2” to indicate delivery by telemedicine. We also analyzed the following procedure codes specific to telehealth: 99441-99444, 98966-98969, G2010, G2012, G9868-G9870, S9110, G0071. Inpatient and emergency department uses of telemedicine were excluded, as were provider-provider interactions. ↩︎
Per the CDC, OCPs can be safely provided after a thorough medical history and blood pressure measurement. Women with high blood pressure or vascular disease are generally not advised to use combined OCPs (estrogen and progesterone), due to increased risk of heart attack and stroke. Therefore, the CDC recommends a blood pressure measurement be taken before initiation of OCPs, but determines that in instances where a provider cannot take a measurement, the woman may report a prior measurement to her provider. However, studies have shown that women who do not have their blood pressure measured before starting OCPs are at a higher risk of heart attack and ischemic stroke than those who did have their blood pressure taken. ↩︎
Without an ultrasound, ectopic pregnancy cannot be excluded, however a study >16,000 women seeking medical abortions found the rate of ectopic pregnancy to be exceedingly low (1.3/1,000 pregnancies). ↩︎
KFF Brief Explains the Legal Challenges to New Title X Regulations
Attorneys General from 23 states, major family planning organizations, individual providers, and the American Medical Association have sued to block the new rules.
A new KFF brief provides an update on the legal challenges to the Trump Administration’s new Title X family planning regulations. These regulations make many changes to the program, notably they disqualify family planning providers who also offer abortion services with non-Title X funds from participating in the program and also ban Title X funded sites from referring patients to abortion services. Attorneys general from 23 states, major family planning organizations, individual providers, and the American Medical Association have sued HHS on the grounds that these regulations violate providers’ freedom of speech, create barriers to patients accessing care, impede timely access to services, as well as other constitutional and procedural arguments. The brief details the status of the litigation in different federal courts and explains the key positions of the plaintiffs and the Trump Administration.
On March 4, 2019, the Trump Administration issued new regulations that makes significant changes to Title X, the federal family planning grant program. The new regulations effectively block the availability of Title X grants to family planning clinics that offer abortion services with other funds, curtail counseling, ban Title X projects from making referrals to abortion services, and require all pregnant patients served by Title X clinics to be referred for prenatal services, regardless of their pregnancy intention. Shortly after the regulations were finalized, the attorneys general from 23 states, major family planning organizations and the American Medical Association filed legal challenges in federal courts to block the implementation of the final Title X regulations.
Box 1: Key Facts – Title X Federal Family Planning Program
Title X, enacted in 1970, is the only federal program specifically dedicated to supporting the delivery of family planning care.
Administered by the HHS Office of Population Affairs (OPA), and funded at $286.5 million for Fiscal Year 2018, the program served over 4 million low-income, uninsured, and underserved clients that year.
In 2017, nearly 4,000 clinics nationwide relied on Title X funding to help serve 4 million people. The sites include specialized family planning clinics such as Planned Parenthood centers, community health centers, state health departments, as well as school-based, faith-based, and other nonprofit organizations.
Title X grants made up about 19% of revenue for family planning services for participating clinics in 2017, providing funds to not only cover the direct costs of family planning services, but also pay for general operating costs such as staff salaries, staff training, rent, and health information technology.
Although the district courts in Washington, Oregon, California and Maryland initially issued preliminary injunctions blocking the implementation of the new regulations, the Courts of Appeals have blocked these preliminary injunctions, and the regulations are currently in effect pending the outcome of the litigation. The Trump Administration Title X regulations are similar to rules issued by the Reagan Administration that were also challenged by provider groups, but were ultimately upheld in 1991 by the Supreme Court in Rust v Sullivan. Ultimately, one or more of these cases may be appealed to the Supreme Court, to decide whether the Trump Administration regulations violate the federal statutes or the Constitution or are within their agency rights. This brief provides an overview of the legal challenges to the Trump Administration final regulations and summarizes the key positions of the plaintiffs and HHS.
What provisions of the final regulations are being challenged?
On March 4, 2019, new final regulations for Title X grants were published in the Federal Register. The Office of Population Affairs, the federal agency that administers the program announced that the regulations would become effective on July 15, 2019 with a full phase in on March 4, 2020. The regulations make many changes to the requirements for Title X projects that are already reshaping the program and provider network available to low-income people through Title X.
Specifically, the regulations:
Prohibit federal Title X funds from going to any family planning site that also provides abortion services: The Title X statute specifies that no federal funds appropriated under the program “shall be used in programs where abortion is a method of family planning.” While HHS has changed its interpretation of this provision over time, throughout most of the history of the program, the ban has generally been understood to mean that Title X funds cannot be used to pay for or support abortion, as was the policy under the prior regulations.
Require that Title X funded activities have full physical and financial separation from abortion-related activities: In addition to separate accounting (as has been the requirement prior to the new regulations), providers must have separate electronic and paper health records, treatment, consultation, examination and waiting rooms, office entrances and exits, workstations, signs, phone numbers, email addresses, educational services, websites, and staff. This new requirement essentially disqualifies any provider from receiving Title X funds if they also offer or refer patients to abortion services.
Ban referrals for abortion services, and mandate referrals to prenatal services: Under the regulations in place from 2000 to 2019, Title X grantees were required to provide nondirective pregnancy options counseling and referrals upon request. This requirement meant that Title X grantees provided complete, medically accurate and unbiased information and resources for all pregnancy options without steering patients to one option. The new final regulations interpret referrals for abortion to be activities that are considered providing “abortion as a method of family planning” and prohibit Title X grantees and subrecipients from providing, promoting, referring for, supporting, or presenting abortion services to patients. Under the new regulations, a Title X project is permitted—but not required—to provide pregnant people with a list of health care providers that offer comprehensive primary health services (including providers of prenatal care). The rules also stipulate that some—but not the majority—of providers on the list may also provide abortion, but neither the list nor the project staff may indicate which of the listed providers also offer abortion services. The regulations specify that all pregnant clients must be referred to prenatal care, regardless of their stated wishes.
Eliminate the requirement for nondirective pregnancy options counseling that also includes discussion of abortion as an option: Under the previous regulations, Title X grantees were required to offer pregnant women the opportunity to be provided information and counseling regarding prenatal care and delivery; infant care, foster care, or adoption; and pregnancy termination. If asked for information and counseling, providers were required to provide nondirective counseling on each of the options. Each Title X site can now decide whether or not to offer nondirective pregnancy options counseling to patients, but only a medical doctor or advanced practice provider (defined as including physician assistants and advanced practice registered nurses) is permitted to provide this counseling.
Report age and partners for minor clients: Title X grantees and subrecipients are required to maintain and report records indicating the age of minor clients and the age of their sexual partners as specified under state notification laws.
Who is challenging the Trump Administration regulations?
The attorneys general from 23 states, major family planning organizations, individual providers and the American Medical Association (Figure 1) have filed legal challenges in federal courts to block the implementation of the Trump Administration’s final Title X regulations claiming the new rules violate the Constitution and federal laws.
Figure 1: Legal Challenges to HHS Title X Family Planning RuleNew Title X Regulations Became Effective July 15, 2019
The plaintiffs in these lawsuits are challenging these regulations claiming that they would harm the four million low-income people who receive family planning services from Title X sites, would reduce the network of Title X sites, ban providing full medical information and referrals, and potentially decrease the provision of effective medically appropriate contraceptive services. In addition, the rules will create a financial strain on grantees and states that can longer accept the Title X funds, and potentially impact public health.
Although the district courts in Washington, Oregon, California and Maryland initially issued preliminary injunctions blocking the implementation of the new regulations, the Courts of Appeals have subsequently blocked these preliminary injunctions, and the regulations are currently in effect pending the outcome of the litigation. The plaintiffs in the Washington, Oregon and California cases appealed the 9th Circuit Court of Appeals decision (provided by a three Judge panel) staying the preliminary injunction, requesting an en banc hearing of a larger panel of Judges. This request was granted but the new regulations remain in effect pending the decision of the en banc hearing (which took place on September 23, 2019). The 4th Circuit Court of Appeals (in Maryland) also held a hearing on the appeal of the preliminary injunction issued by the district court on September 18, 2019.
Table 1: Plaintiffs Challenging the Legality of the Trump Administration’s Title X Regulations
Plaintiffs
Court
Judge
Status (as of Nov 1, 2019)
Essential Access Health Inc.; Melissa Marshall M.D.1
State of California by and through Attorney General Xavier Becerra
United States District Court Northern District of California
District Court issued preliminary injunction for CA that was stayed by 9th Circuit Court of Appeals.
District Court has stayed current motions and hearings until after the decision from the 9/23/2019 en banc hearing
OR, NY, CO, CT, DE, DC, HI, IL, MD, MA, MI, MN, NV, NJ, NM, NC, PA, RI, VT, VA, & WI2
American Medical Association, Oregon Medical Association, Planned Parenthood of Southwestern Oregon, Planned Parenthood Columbia Willamette, Thomas N. Ewing M.D,; Michele Megregian C.N.M.
United States District Court, District of Oregon, Eugene Division
District Court issued a preliminary injunction for MD which was stayed by the 4th Circuit Court of Appeals pending appeal.
4th Circuit Court of Appeals held hearing on September 18, 2019 on appeal of preliminary injunction.
District Court is continuing to consider the case, and hearing is scheduled for January 2020.
On what grounds are the plaintiffs suing the federal government?
The heart of the litigation is Section 1008 of Title X, which states that no federal funds appropriated under this program “shall be used in programs were abortion is a method of family planning.”
While the plaintiffs are claiming numerous violations of federal process and law, the interpretation of Section 1008 of the Title X statute is at the heart of this litigation. Section 1008 of specifies that no federal funds appropriated under the program “shall be used in programs where abortion is a method of family planning.” HHS has changed its interpretation of this provision over time, but throughout most of the history of the program, the ban has generally been understood to mean that Title X funds cannot be used to pay for or support abortion, as was the policy under the regulations in place before the Trump Administration issued new regulations. At that time, the program required that all clinics that also offered abortion services financially separate their operations but did not have a full physical separation requirement.
In the preamble to the regulation, HHS contends that these new regulations are necessary to enforce compliance with the statutory bar on the use of Title X funds for abortions. Many provisions in the Trump Administration’s regulation mirror those issued in 1988 by the Reagan Administration. Those regulations were challenged by Title X grantees and doctors in a lawsuit that ultimately reached the U.S. Supreme Court in Rust v. Sullivan. In 1991, the Supreme Court held that the regulations reflected one permissible interpretation of the statute and did not violate the First or Fifth Amendments. HHS believes that the Supreme Court ruling in Rust v. Sullivan is the controlling legal precedent and that Trump Administration regulations, like the Reagan Administration regulations, are an acceptable interpretation of the statute, and are constitutionally valid.
In Rust v Sullivan, the Supreme Court ruled that the government may favor childbirth over abortion and is within its rights to allocate funds consistent with this viewpoint—without violating a woman’s right to choose to terminate her pregnancy. After the Supreme Court’s decision, Congress voted to repeal the prohibitions on counseling and referring for abortion, but lacked the votes to override President George H.W. Bush’s veto.
The Reagan era regulations, however, were never fully implemented. The Clinton Administration issued regulations that have been in effect ever since, permitting Title X providers to refer for abortions and allow sites that also provide abortion services to participate in Title X, so long as there is financial separation between the Title X funds and funds used for abortion services.
While there are many plaintiffs represented in the cases against HHS, the cases present similar challenges. The plaintiffs contend that Title X funds have never been available for abortion services, and the defendant (HHS) fails to identify any evidence suggesting that any Title X funds are being used for abortion services.
The plaintiffs contend that the Administration violated the Administrative Procedures Act by not stating a valid reason for the rule or following proper notice and comment procedures. While Rust v. Sullivan held that the regulations were one acceptable interpretation of Section 1008 at that time, the plaintiffs argue that the applicable law has changed. Every year since 1996 (after Rust), Congress has passed an Appropriations Act for Title X requiring that all pregnancy counseling be nondirective. In particular, the plaintiffs contend that the requirement to refer all pregnant patients to pre-natal services and the ban on abortion referrals is violation of this section which requires all pregnancy counseling to be nondirective.
In addition, they are claiming that HHS has violated Section 1554 of the ACA (Box 2), which states that the agency shall not promulgate any regulations that creates any unreasonable barriers to the ability of individuals to obtain appropriate medical care or restricts communications between a doctor and a patient. They charge that these regulations create barriers to care by requiring physical and financial separation for clinics that provide abortion services with non-Title X funds, only permitting doctors and advanced practice providers to provide counseling, and requiring additional documentation for minors. They also claim that the regulations restrict the speech of doctors who work at Title X clinics by banning referrals to abortion services, and requiring referrals to pre-natal service even if that is not what the patient seeks.
Box 2: Section 1554 of the Affordable Care Act (ACA)
Section 1554 of the ACA provides that the Secretary “shall not promulgate any regulation that”
Creates any unreasonable barriers to the ability of individuals to obtain appropriate medical care;
Impedes timely access to health services;
Interferes with communications regarding a full range of treatment options between the patient and the provider;
Restricts the ability of health care providers to provide full disclosure of all relevant information to patients making health care decisions;
Violates the principles of informed consent and the ethical standards of health care professionals; or
Limits the availability of health care treatment for the full duration of a patient’s medical needs.
All of the lawsuits challenging the Title X final rule are based on similar legal arguments. Listed below are some of the common claims.
Table 2: Litigation Challenging Trump Administrations Final Title X Regulations:Summary of the Plaintiffs’ and Government’s Position
Claim: Violation of the Administrative Procedure Act (APA) which governs the process by which federal agencies develop and issue regulations. It includes requirements for notice, public comment, and standards for judicial review
Plaintiffs’ Position:
HHS exceeded the scope of its statutory authority and acted in a manner that is arbitrary and capricious
HHS did not comply with notice and comment requirements.
The final rule is significantly different from the proposed rule.
The final rule does not address any identified problem.
The final rule is contrary to law because it violates the Health and Human Services Appropriations Act Section 1554 of the Affordable Care Act (ACA), the First and Fifth Amendments of the U.S. Constitution. (See below for more on these claims.)
Government’s Position:
The regulations are necessary to enforce compliance with the statutory bar on the use of Title X funds for abortions.
Rust v. Sullivan confirmed that this rule is a valid exercise of HHS authority.
The final rule is a “logical outgrowth” of the proposed rule
Claim: Violation of Section 1554 of the Affordable Care Act (ACA) which states that the Secretary “shall not promulgate any regulation that”:
Creates any unreasonable barriers to the ability of individuals to obtain appropriate medical care;
Impedes timely access to health services;
Interferes with communications regarding a full range of treatment options between the patient and the provider;
Restricts the ability of health care providers to provide full disclosure of all relevant information to patients making health care decisions;
Violates the principles of informed consent and the ethical standards of health care professionals; or
Limits the availability of health care treatment for the full duration of a patient’s medical needs.
Plaintiffs’ Position:
The following provisions of the Final Rule violate Section 1554 of the ACA:
Prohibition on abortion counseling and referral
Requirement that nondirective counseling only be provided by a physician or advance practice provider
Physical and financial separation
Documentation for minors
Government’s Position:
The Plaintiffs have waived any argument based on Section 1554 because HHS did not receive any comments on the proposed rule about Section 1554 during the comment period.
Section 1554 does not apply to Title X; it only applies to provisions of the ACA.
Even if Section 1554 applies, the Title X regulations do not impede access to care.
Claim: Violation of Continuing Appropriations Act, 2019, Pub. L. 115–245, 132 Stat. 2981, 3070–71 (2018), “That amounts provided to said projects under such title shall not be expended for abortions, that all pregnancy counseling shall be nondirective. . .” Congress has consistently included this language with respect to Title X appropriations funding every year since 1996.
Plaintiffs’ Position:
The Title X requirement to refer all pregnant women to prenatal services and the ban on abortion referrals violates the Appropriations Act.
Counseling and referral are inextricably linked.
Government’s Position:
The rule requires all counseling to be nondirective. “Referral” is different from, and not a part of, “counseling.”
Claim: Violation of First Amendment (freedom of speech)4 “Congress shall make no law… abridging the freedom of speech.” The First Amendment applies equally to the actions and regulations of Executive agencies
Plaintiffs’ Position:
The ban on abortion referrals and the requirement to refer all pregnant women to prenatal appointments violates doctors’ and patients’ First Amendment rights. The ban on abortion referrals and requirement to refer pregnant patients to prenatal appointments is an impermissible viewpoint-based restriction and forces providers to speak a view they do not hold (that prenatal care is appropriate). In addition, the regulations imposes a speaker-based ban, only allowing medical doctors and advanced practitioners to provide pregnancy options counseling. Recent Supreme Court decisions have confirmed that medical speech is deserving of First Amendment protection of the highest order.
The final rule requires grantee states and other Title X grantees to infringe on the free speech rights of health care providers as a condition of securing Title X funds.
Government’s Position:
The Supreme Court upheld similar provisions in Rust v. Sullivan. Doctors are free to tell patients that abortion is not a method of family planning supported by Title X. The government is permitted to fund some activities and not others. The Supreme Court ruled in Rust v. Sullivan, “The Government can, without violating the Constitution, selectively fund a program to encourage certain activities it believes to be in the public interest, without at the same time funding an alternate program… In doing, the Government has not discriminated on the basis of viewpoint; it has merely chosen to fund one activity to the exclusion of the other.”
Claim: Violation of Fifth Amendment: The Due Process Clause of the Fifth Amendment prohibits the federal government from denying equal protection of the laws. when “vagueness permeates the text” of a law it violates the due process clause of the Fifth Amendment
Plaintiffs’ Position:
The Rule specifically targets and harms women because it discriminates based on pregnancy and gender. The Rule is not substantially related to an important government interest or rationally related to a legitimate government interest.
The Rule does not give Title X grantees and sub-recipients sufficient guidance and invites inconsistent or biased enforcement.
The physical and financial separation requirement provides the Secretary with excessive latitude to determine whether a Title X project has met this provision.
The Final Rule is ambiguous on whether Title X providers may refer patients for abortion in case of medical necessity, and what a Title X provider may discuss with respect to abortion if she provides nondirective pregnancy options counseling.
The Final Rule’s prohibition on actions that “encourage, promote or advocate abortion as a method of family planning” is vague and invites arbitrary and discriminatory enforcement by the Secretary.
Government’s Position:
The Rule is perfectly clear and just as specific as the materially identical provisions sustained in Rust v. Sullivan. The Due Process Clause tolerates greater imprecision when government subsidies are involved.
Looking Forward
Grantees were required to submit action plans to show compliance with the new regulations on August 19, 2019, and a certificate of compliance on September 19, 2019. Some of the nonprofits and states (IL, ME, OR, WA) challenging the regulations have decided to withdraw from Title X or put a hold on drawing down funds as the cases move through the federal district courts. In addition, Planned Parenthood, also a litigant in the cases, formally withdrew from the program. In addition to the 400 Parenthood sites, over 600 additional clinics, composed of state health departments, federally qualified health centers, and nonprofit organizations are no longer using Title X funds to support services for low-income and uninsured individuals. These decisions affect all of the Title X clinics in Hawaii, Maine, Oregon, Utah, Vermont, and Washington and the majority of Title X clinics in Alaska, Connecticut, Illinois, Maryland, Massachusetts, Minnesota, New Hampshire and New York.
The new regulations are currently in effect and the plaintiffs are awaiting the rulings from the 9th Circuit and 4th Circuit Court of Appeals regarding whether the regulations can be blocked until the cases make their way through the federal district courts. On March 4, 2020, Title X sites are required to physically separate the abortion services they provide with non-Title X funds. If this part of the regulations is implemented as scheduled in March 2020, it is expected that many more Title X grantees and sites will withdraw from the Title X network. While Supreme Court may eventually hear these cases, the 2020 presidential election may take place before these cases reach the Supreme Court.
Endnotes
Essential Access Health et al. and the State of California filed two separate lawsuits challenging the final regulations. These two cases have been related to one another at the district court. ↩︎
State of Oregon et al. and the American Medical Association et al. filed two separate lawsuits challenging the final regulations. These two cases have been consolidated for pretrial purposes. ↩︎
State of Washington and the National Family Planning & Reproductive Health et al. filed two separate lawsuits challenging the final regulations. These two cases have been consolidated for pretrial purposes. ↩︎
California does not include a violation of the First Amendment it its legal challenge. ↩︎
Poll: On Health Care, Democrats and Democratic-Leaning Independents Trust Sen. Sanders the Most, but Significantly More People Support a Public Option than Medicare-for-All
Democrats Want to Hear More about How Candidates’ Plans Affect Seniors, How They Will Pay for Them, How Middle-Class Taxes Might Change, and How Will They Get Congress to Pass Them
3 in 4 Americans Do Not Expect Congress to Take Action to Lower Drug Costs Before the 2020 Election
Ahead of tonight’s Democratic presidential debate, Sen. Bernie Sanders is the candidate most trusted on health care by Democrats and Democratic-leaning independents, though the Medicare-for-all plan he has championed is significantly less popular than the “public option” approach put forward by some other candidates, the latest KFF Health Tracking Poll finds.
Among the overall public, a narrow majority (53%) support the idea of a Medicare-for-all plan that would cover all Americans through a single government plan. At the same time, two-thirds (65%) say they support a government-run health plan that would compete with private insurance, often called a public option. Large majorities of Democrats support both a public option (88%) and Medicare-for-all (77%).
Most Republicans oppose both approaches to expanding coverage, but more of them favor a public option (41%) than Medicare-for-all (27%). Majorities of independents support both options, though a larger share favors a public option.
The poll also examines the public’s views towards Medicare-for-all when they are provided descriptions that include the trade-offs under consideration.
When a Medicare-for-all plan is described as requiring many employers and some individuals to pay more in taxes while eliminating both out-of-pocket costs and premiums for all Americans, the public is split with equal shares (48%) supporting and opposing it. The public is also divided when the plan is described as increasing taxes individuals will personally pay, but decreasing their overall costs for health care (47% in favor, 48% opposed).
In Primary Race, Sen. Sanders is Most Trusted by Younger Adults; VP Biden Leads among Seniors
The poll finds that Sen. Sanders, who has drawn national attention to his Medicare-for-all plan since his 2016 presidential run, has built a significant trust advantage among Democrats and Democratic-leaning independents.
When asked which candidate they trust the most to handle health care, nearly three in 10 (29%) name Sen. Sanders, with former Vice President Joe Biden (21%) and Sen. Elizabeth Warren (19%) not far behind. No other presidential candidate comes close.
Sen. Sanders is by far the most trusted candidate among those ages 18-34, named by nearly half (47%) of this group. Vice President Biden is the most trusted among seniors by a wide margin (33%, with Warren next at 18%). Sen. Sanders holds a clear advantage among independents who lean Democratic, with four in 10 (39%) naming his as their most trusted candidate on health care while pure Democrats are divided, with similar shares saying they trust Sen. Warren (26%), Vice President Biden (23%) and Sen. Sanders (22%).
Health care remains Democrats’ top issue, with one in four (24%) Democrats and Democratic-leaning independents offering it as the issue they most want to hear candidates discuss in the next debate. Smaller shares name the environment/climate change/energy (12%), immigration (6%), the economy and jobs (5%), education (4%) or gun control (4%).
Large shares of Democrats and Democratic-leaning independents say the candidates are spending too little time talking about how their health care plans will affect seniors on Medicare (50%), how to pay for proposed changes (47%), whether their plans would increase taxes on the middle class (45%), and how they will work with Congress to enact their plans (45%).
Most Say Washington Isn’t Doing Enough to Lower Drug Costs and Doubt Congress Will Pass Anything
In spite of White House and Congressional proposals to lower what people pay for prescription, the poll finds that large majorities believe President Trump and his administration (70%), Democrats in Congress (75%) and Republicans in Congress (77%) are not doing enough to lower drug costs.
Seven in 10 Americans (72%) say it’s unlikely that Congress will pass legislation to lower drug costs in the next year. Majorities of Democrats, Republicans and independents are pessimistic about the prospects for enacting drug-cost legislation.
Despite ACA Marketplace Premiums Falling, Few Think That Is the Case
The Affordable Care Act’s 2020 open enrollment period began this month, allowing people who buy their own coverage or are uninsured an opportunity to sign up for Marketplace coverage.
Premiums on average are somewhat lower this year than last year, though few people know it. The poll finds just 6% of the overall public believe premiums on average are lower this year, a fraction of the share (44%) who say premiums are up this year.
When assessing how well the health insurance marketplaces in the nation are working, the public is divided with similar shares saying they are working well (45%) as saying they are not working well (47%).
People are somewhat more positive about their state’s marketplace, with half (52%) saying it is working well. People living in states that run their own marketplaces are more likely to say their marketplace is working well (58%) than those living in states relying on the federal government’s HealthCare.gov marketplace (48%).
METHODOLOGY
Designed and analyzed by public opinion researchers at KFF, the poll was conducted November 7-12, 2019 among a nationally representative random digit dial telephone sample of 1,205 adults. Interviews were conducted in English and Spanish by landline (302) and cell phone (903). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
Filling the need for trusted information on national health issues, the Kaiser Family Foundation is a nonprofit organization based in San Francisco, California.
Health care has been a dominant issue throughout the 2020 Democratic presidential primary and the latest KFF Health Tracking Poll finds Democrats continuing to prioritize health care over other issues. Ahead of tonight’s Democratic presidential debate, when asked to state in their own words the one issue they most want to hear the Democratic presidential candidates discuss, about one in four (24%) Democrats and Democratic-leaning independents offer health care. Fewer mention other issues such as the environment (12%), immigration (6%), jobs and the economy (5%), education (4%), and gun control (4%).
Senator Bernie Sanders is the candidate most trusted on health care by Democrats and Democratic-leaning independents, though the Medicare-for-all plan he’s championed is significantly less popular than the “public option” approach put forward by some other candidates. Among adults overall, a narrow majority (53%) support the idea of a Medicare-for-all plan while a larger majority (65%) say they support a government-run public option that would compete with private insurance. Large majorities of Democrats support both a public option (88%) and Medicare-for-all (77%), and while most Republicans oppose both approaches to expanding coverage, more favor the public option proposal (41%) than a Medicare-for-all plan (27%).
Attitudes towards a Medicare-for-all plan shift moderately depending on how such a proposal is described. For example, if the plan is described as requiring many employers and some individuals to pay more in taxes, but eliminating both out-of-pocket costs and premiums for all Americans, overall favorability drops to 48%. Similarly, overall favorability drops (47%) when the plan is described as increasing taxes individuals will personally pay, but decreasing their overall costs for health care.
Senator Bernie Sanders leads the field when Democrats and Democratic-leaning independents are asked which Democratic presidential candidate they trust the most on health care. About three in ten (29%) say they trust Sen. Sanders, followed by about one-fifth who say they trust Vice President Joe Biden (21%) or Senator Elizabeth Warren (19%). Overall trust of Sanders on health care is largely driven by younger Democrats and Democratic-leaning independents as well as those who are not as connected to the Democratic Party. Nearly half (47%) of Democrats and Democratic-leaning independents between the ages of 18 and 34 prefer Sanders when it comes to health care, while Biden holds a sizeable edge over other candidates among adults 65 and older (33%). Among independents who lean Democratic, Senator Sanders is the preferred candidate (39%), while self-identified Democrats are split on which candidate they most trust to handle health care: Warren (26%), Biden (23%) and Sanders (22%).
The 2020 open enrollment period for people who purchase their own insurance on the ACA marketplaces began in most states on November 1st. The law’s seventh open enrollment period began with the announcement that premiums in many areas of the U.S. are decreasing. Yet a plurality of the public (44%) thinks premiums are higher than they were last year. Though ACA marketplace premiums are now on average lower than they were last year, just 6% think this is the case.
Health Care and the 2020 Election
This month’s KFF Health Tracking Poll continues our analysis of the role health care may be playing in the 2020 election with a look at what issues Democrats want to hear about in the next debate as well as which of the Democratic primary candidates they trust the most when it comes to handling health care.
Democratic Presidential Primary Debates
Health care has been and remains a top issue for Democrats during the 2020 Democratic presidential primary. Recent KFF Health TrackingPolls have found that health care consistently emerges as a top issue that Democrats and Democratic-leaning independents want to hear the 2020 Democratic presidential candidates discuss, and this month’s poll finds this continues to be true. When asked to say in their own words what issue they would most like to hear the Democratic presidential candidates discuss in the upcoming debate, one in four Democrats and Democratic-leaning independents (24%) offer health care. This is twice as many as say they want to hear more about any other issue such as the environment (12%), immigration (6%), jobs and the economy (5%), education (4%), and gun control (4%).1
Figure 1: Health Care Is The Top Issue Democrats and Democratic-Leaning Independents Want To Hear About In Next Debate
And while various Democratic candidates have put out their own health care proposals, Democrats are still wanting to know more. Large shares say Democratic candidates are spending too little time talking about how their health care plans will affect older adults on Medicare (50%), how they will pay for their plans (47%), whether they will require higher taxes on the middle class (45%), and how they will work with Congress to pass their health care proposals (45%). About four in ten say the candidates are spending too little time discussing how they will lower health care costs for individuals (41%) and whether their plans would cover all U.S. residents (40%); and about a third say the candidates are spending too little time talking about how their plans differ from President Trump’s approach to health care.
Figure 2: Half Want To Hear About How Democratic Candidates’ Health Care Proposals Will Affect Older Adults
Sanders, Biden, And Warren Are Most Trusted When It Comes To Health Care
When asked which candidate they trust the most when it comes to handling health care, nearly three in ten (29%) Democrats and Democratic-leaning independents say they are most trusting of Senator Bernie Sanders. About one in five say they are most trusting of former Vice President Joe Biden (21%) and Senator Elizabeth Warren (19%) when it comes to handling health care.
Figure 3: Democrats And Democratic-Leaning Independents Most Likely to Trust Sanders, Biden, And Warren To Handle Health Care
Notably, nearly half (47%) of younger Democrats and Democratic leaning independents, ages 18 to 34, say they have the most trust in Bernie Sanders when it comes to handling health care. However, among adults ages 65 and older, Joe Biden is the most trusted candidate to handle health care (33%).
Table 1: Candidate Trust On Health Care By Age
Percent who trust each of the following candidates the most when it comes to handling health care:
18-34year olds
35-54year olds
55-64year olds
65 andolder
Bernie Sanders
47%
26%
9%
16%
Joe Biden
12
20
31
33
Elizabeth Warren
14
25
21
18
Pete Buttigieg
3
4
7
9
Amy Klobuchar
1
7
7
3
Andrew Yang
10
1
1
2
Cory Booker
3
3
2
0
NOTE: Showing only candidates who received more than 2% among total Democrats and Democratic-leaning independents
When it comes to which candidate they most trust to handle health care, there are some notable differences between adults who identify as Democrats and those who identify as independents, but say they lean towards the Democratic party. Democrats are relatively divided with about one in four saying they most trust Elizabeth Warren (26%), Joe Biden (23%) and Bernie Sanders (22%). However, a larger share of Democratic-leaning independents (39%) choose Bernie Sanders as the most trusted candidate on health care than any of the other Democratic presidential candidates.
Figure 4: While Pure Democrats Are Divided; Four In Ten Democratic-Leaning Independents Trust Bernie Sanders The Most On Health Care
Medicare-for-all and Public Option
This month’s poll continues to find larger support for more incremental changes to the nation’s health care system than a major overhaul. Support for a “public option,” in which a government-administered plan would compete with private health insurance and be available to all Americans, has decreased slightly since last month. Two in three adults (65%) favor a public option, down from 73% in October. Levels of support for a public option were similar in July (65% support) and September (69%).
Following a narrowing of net support in recent months for Medicare-for-all, this month’s poll finds about half the public (53%) favors a national Medicare-for-all plan while 43% are opposed. Indeed, since July, support for Medicare-for-all has remained relatively steady with about half of adults in favor of the proposal.
Figure 5: About Half Of Adults Support A National Medicare-for-all Plan
Democrats and independents continue to be more likely than Republicans to favor both a public option and Medicare-for-all. Nonetheless, a public option that would compete with private health insurance plans garners more support among Republicans and independents than a proposed national Medicare-for-all plan. While large majorities of Democrats favor both proposals (77% Medicare-for-all, 88% public option), half of independents (52%) support a Medicare-for-all proposal compared to about seven in ten (69%) who support a public option. Among Republicans, 27% support a national Medicare-for-all plan while four in ten (41%) favor a public option.
Figure 6: Larger Shares Support A Public Option Than Medicare-for-all
Moderate Shifts in Support of a National Health Plan Depending On How The Plan Is Described
Previous KFF polling has found that attitudes towards a national Medicare-for-all plan are quite malleable when given counter-arguments. This month’s tracking poll finds more moderate shifts in the public’s views towards Medicare-for-all when they are provided descriptions that balance the trade-offs lawmakers are considering. When Medicare-for-all is described as eliminating private health insurance, but allowing people to choose their medical providers, support for Medicare-for-all remains relatively unchanged (54% favor v. 43% oppose). If the plan is described as requiring many employers and some individuals to pay more in taxes, but eliminating both out-of-pocket costs and premiums for all Americans, overall favorability drops and the public is equally divided (48% favor vs. 48% oppose) in their views. Similarly, the public is also divided when the plan is described as increasing taxes individuals will personally pay, but decreasing their overall costs for health care (47% favor vs. 48% oppose).
Figure 7: Some Moderate Shifts In Support For Medicare-for-all Depending On Description Of Plan
Additionally, about four in ten (39%) say a Medicare-for-all plan that would eliminate health insurance premiums, deductibles, and most out-of-pocket costs but would increase taxes on many employers and some individuals, will not have much financial impact on them. About a third of adults (34%) think they would be worse off under a Medicare-for-all plan while about one in five (22%) think they would be better off. Notably, half of adults 65 and older with Medicare coverage think they would not be financially impacted by a Medicare-for-all plan. Partisans have different expectations of how they would be financially impacted by a Medicare-for-all system which eliminated premiums and deductibles, but increased taxes on employers and some individuals. About half of Democrats (49%) and four in ten independents (40%) think they would not be impacted financially whereas half of Republicans (52%) think they would be worse off under a Medicare-for-all plan.
Figure 8: Nearly Four In Ten Think A Medicare-for-all Plan Would Not Have Much Financial Impact On Them
The Affordable Care Act’s Seventh Open Enrollment Period
Overall opinions of the Affordable Care Act (ACA) have remained relatively unchanged for the past two years since the Republican efforts to repeal the 2010 health care law. Half of the public (52%) this month hold favorable opinions of the ACA while four in ten (41%) hold a negative opinion of the law. Partisans remain divided on the ACA as eight in ten Democrats (83%) have a favorable view of the ACA compared to half of independents (52%) and about one in five Republicans (22%).
Figure 9: Public More Likely To View The ACA Favorably Than Unfavorably
With the ACA open enrollment underway, millions of Americans will be using state and federal health insurance marketplaces, established by the 2010 health reform law, to shop for health insurance plans to cover them and their families in 2020. Americans are divided on how well they think the health insurance marketplaces are working in their own state and in the nation overall. When assessing how well the health insurance marketplaces in the nation are working, about four in ten (45%) say they are working “very well” (7%) or “somewhat well” (38%) while a similar proportion (47%) say they are working either “not too well” (27%) or “not at all well” (19%). The public is slightly more positive about how health insurance marketplaces are working in their state with half (52%) saying they are working either “very well” (14%) or “somewhat well” (37%).
Figure 10: Public Divided On How Well ACA Health Insurance Marketplaces Are Working
Partisans are split on their views of how well the ACA health insurance marketplaces are working. Nearly six in ten Democrats (57%) say the marketplaces in the nation overall are working well and two-thirds (67%) say marketplaces in their state are working well. On the other hand, a majority of Republicans (56%) say marketplaces in the nation overall are not working well while about half (52%) say the marketplace in their state is not working well.
Notably, adults living in states that have developed their own state-based marketplace are more likely to say the health insurance marketplace in their own state is working well. About six in ten adults (58%) living in states with state-based marketplaces say the health insurance marketplace in their state is working well compared to half of those living in states that are using the federal marketplace (48%).
Figure 11: Views Of ACA Marketplaces Vary By Partisanship And Marketplace Type
A recent KFF analysis of ACA marketplace premium data for 2020 has indicated that on average, premiums are decreasing across the U.S., though premium changes vary widely by location. Yet few adults think premiums for health insurance plans available in the ACA marketplaces are lower than they were last year. A plurality of the public (44%) think premiums are higher than they were last year while 6% think ACA marketplace premiums are now lower. About three in ten (29%) think the ACA premiums are about the same as last year.
While few partisans think the premiums for ACA plans are lower this year compared to last year, Republicans are more likely than Democrats to say the premiums are higher. Nearly half of Republicans (48%) say premiums in the ACA marketplaces are higher than they were last year compared to 37% of Democrats.
Figure 12: About Four In Ten Think ACA Marketplace Premiums Are Higher Compared To Last Year
The Trump Administration’s Continuing Health Care Efforts
In December 2018, a federal district court judge in Texas issued a ruling siding with Republican state attorneys general that declared the Affordable Care Act invalid since Congress zeroed out the penalty for not having health insurance. The case is now with a panel of judges in the 5th Circuit Court of Appeals. A ruling is expected in the coming months and many expect the case to make its way to the U.S. Supreme Court.
Overall, 62% of the public do not want to see the Supreme Court overturn the ACA’s pre-existing condition protections; yet the public is more divided on whether they want the Supreme Court to overturn the entire law (45% would like to see it overturned and 48% would not). While 76% of Democrats and half of independents do not want to see the 2010 health care law overturned, seven in ten Republicans (71%) say they would like to see the Supreme Court overturn the law. However, far fewer Republicans (43%) want to see the ACA’s protections for people with pre-existing conditions overturned.
Figure 13: About Six In Ten Do Not Want Supreme Court To Overturn ACA Protections For People With Pre-Existing Conditions
Throughout 2019 lawmakers on both sides of the aisle have been working to address the cost of prescription drugs. Both the U.S. House of Representatives and the U.S. Senate have held hearings on this issue and both the Trump administration and House Speaker Nancy Pelosi have put forward proposals to address prescription drug costs. Despite these efforts to address the issue, majorities say that President Trump and his administration (70%), Democrats in Congress (75%) and Republicans in Congress (77%) are “not doing enough” to bring down the costs of prescription drugs.
Figure 14: Majorities Say President Trump And Congressional Republicans And Democrats Are Not Doing Enough To Lower Rx Drug Costs
Notably, partisans appear to be critical of their own parties as a majority of Democrats (65%) say Congressional Democrats are “not doing enough” to bring down the costs of prescription drugs and a majority of Republicans (56%) say Congressional Republicans are “not doing enough.” Partisans are polarized on President Trump’s efforts to address prescription drugs costs with an overwhelming majority of Democrats (94%) and about eight in ten independents (77%) saying the Trump administration is “not doing enough,” compared to one-third of Republicans who say the same.
Figure 15: Majorities Of Partisans Say Democrats And Republicans In Congress Are Not Doing Enough To Lower Rx Drug Costs
Seven in ten adults (72%) —including majorities across partisans—think it is “not too likely” or “not at all likely” that Congress will pass legislation to lower the costs of prescription drugs in the next year.
If the public’s pessimism about the prospects of legislation to address prescription drug costs proves to be true, blame for the lack of results will be shared. Three in ten (30%) say they would blame Republicans if Congress does not pass legislation to lower the costs of prescription drugs, and a similar proportion (30%) would blame Democrats in Congress. One in four (25%) would place the blame on President Trump.
Figure 16: Most Say It Is Unlikely That Congress Will Pass Legislation To Lower Prescription Drug Costs In The Next Year
Methodology
This KFF Health Tracking Poll was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted November 7th–12th 2019, among a nationally representative random digit dial telephone sample of 1,205 adults ages 18 and older, living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). The sample included 290 respondents reached by calling back respondents that had previously completed an interview on the KFF Tracking poll at least nine months ago. Computer-assisted telephone interviews conducted by landline (302) and cell phone (903, including 613 who had no landline telephone) were carried out in English and Spanish by SSRS of Glen Mills, PA. To efficiently obtain a sample of lower-income and non-White respondents, the sample also included an oversample of prepaid (pay-as-you-go) telephone numbers (25% of the cell phone sample consisted of prepaid numbers) as well as a subsample of respondents who had previously completed Spanish language interviews on the SSRS Omnibus poll (n=10). Both the random digit dial landline and cell phone samples were provided by Marketing Systems Group (MSG). For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s 2017 American Community Survey (ACS) on sex, age, education, race, Hispanic origin, and region along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the July-December 2018 National Health Interview Survey. The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample, and design modifications, namely, the oversampling of prepaid cell phones and likelihood of non-response for the re-contacted sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Group
N (unweighted)
M.O.S.E.
Total
1,205
±3 percentage points
Party Identification
Democrats
353
±6 percentage points
Republicans
340
±6 percentage points
Independents
390
±6 percentage points
Democrats/Democratic-leaning independents/Independents with no leaning
643
±5 percentage points
Democrats and Democratic-leaning independents
550
±5 percentage points
Endnotes
Fieldwork for this poll was concluded prior to the November 14th shooting at Saugus High School in Santa Clarita, California. ↩︎
An updated chart collection explores trends in health outcomes, quality of care, and spending on treatment for people with diabetes, the most common endocrine disease in the United States. The analysis finds that diagnosis rates and diabetes-related spending have continued to grow in the U.S., even as disease management has improved and the rate of associated complications has declined.
The slideshow is part of the Peterson-KFF Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.