KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
In this column for the JAMA Health Forum, Larry Levitt explores what President-elect Biden might do to advance his health care vision both through legislation and through executive orders and waivers and demonstrations in spite of a narrowly divided Congress.
With President-elect Joe Biden and a new Congress taking office next month, newly updated KFF briefs examine two women’s health policy issues awaiting federal policymakers in 2021.
President-elect Biden campaigned on reversing the Trump Administration’s regulations for the Title X family planning program, which require complete financial and physical separation from abortion services, including referrals, for family planning providers funded by the program. The Current Status of the Title X Network and the Path Forward brief provides a narrative with maps and charts illustrating the Title X changes made by the Trump Administration and the resulting impact. Over 25% of participating providers left the program, with six states and at least half of providers in eight other states exiting the program. The brief also reviews the pending litigation on the regulations, and what steps the Biden Administration would have to take to reverse the Trump regulations.
Improving maternal health has captured the attention of federal and state policymakers in recent years. The updated brief, Expanding Postpartum Medicaid Coverage, discusses one focus area of improving maternal health. While all states must provide health coverage to pregnant women on Medicaid with incomes up to at least 138% (about $30,000 for a family of three) of the federal poverty level through 60 days after they give birth, gaps remain in coverage beyond that timeframe in many states. The brief explains existing state variation in Medicaid postpartum coverage and explains state and federal options to extend coverage beyond 60 days postpartum.
When Congress convenes next year and President-elect Biden and Vice-President-elect Harris are sworn-in, they are likely to take up previous legislative efforts to address maternal health care. This table summarizes pending bills on maternal health introduced in the 116th Congress.
This slideshow examines trends in U.S. health spending over time, including the share of household budgets devoted to health expenses and comparisons of out-of-pocket expenditures to money spent on insurance. The data shows that U.S. heath spending outpaced the country’s economic growth before slowing in recent years, and that health insurance represents a growing share of total health expenditures, particularly public programs.
The slideshow is part of the Peterson-Kaiser Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.
In the midst of the coronavirus pandemic, community health centers are serving as public health responders, especially for medically underserved populations. Health centers are a national network of safety net primary care providers who provided care to nearly 30 million patients in 2019, and disproportionately serve patients who are low-income, persons of color, uninsured, or publicly insured – groups that have been especially hard hit by the pandemic. Based on focus group interviews conducted in September and October 2020 with informants from 16 state and regional Primary Care Associations (PCAs) representing 750 health centers and a supplemental questionnaire completed by PCAs following focus group interviews, this brief examines how health centers have adapted their service delivery models during the pandemic response and the current challenges they face continuing to meet patients’ needs.
Key Findings
Health centers are providing testing in underserved communities, but PCAs report there is still unmet need. In the week ending December 4th alone, health centers provided over 335,000 tests. Respondents described a range of efforts by health centers to increase testing capacity, such as testing in parking lots, creating temporary testing sites, and deploying mobile testing units. Despite these efforts, some of the participating PCAs said that health centers in their state or region cannot provide tests to all patients who need them, identifying long wait times, shortages of PPE, and staff shortages as the most common barriers to adequate testing.
Health centers are coordinating with state and local public health agencies on response efforts. Respondents reported that health centers in their states have been working with public officials to conduct testing and contact tracing, secure reimbursement for telehealth visits, and ensure access to services for vulnerable populations. These efforts have helped provide continued access to care and have been important to health centers’ financial stability.
Rapidly pivoting to telehealth was key for health centers to continue seeing patients amid the pandemic and helped to keep health centers financially solvent. Despite the success in shifting to telehealth services, respondents noted both technological and cultural barriers for some patients. While respondents agreed telehealth would likely remain an important service delivery mode, they also described health center efforts to create safer environments for in-person care, such as upgrading HVAC systems and reconfiguring space for “sick” and “well” clinics.
Many health centers are meeting patients “where they are” by taking medical care outside the clinic – while also addressing non-medical needs like food insecurity. Respondents reported health centers’ use of mobile vans and other strategies to reach agricultural workers where they work and live, American Indian reservations, and other underserved communities hard-hit by the pandemic. Depending on the need, health centers are providing COVID-19 testing, handwashing stations, and flu immunizations, among other services. Additionally, respondents described health centers partnering with local organizations to distribute food and assess needs for housing and other social supports.
Health centers face ongoing shortages of testing supplies and PPE. Respondents reported that the competition among hospitals and large health systems for PPE often made acquiring the supplies more difficult. Many health centers have relied on consortia or PCAs for group buying power, though PCAs indicated that health centers continue facing difficulty getting adequate testing supplies and PPE.
PCAs reported that staff layoffs due to the pandemic have been relatively limited, but the pandemic’s impact on staff morale is a concern for the workforce and health care accessibility. Most respondents reported that the length and uncertainty of the pandemic were impacting staff morale. They noted several other factors impacting morale, including the challenging pivot to telehealth for staff providing services that are difficult to perform virtually, balancing work with obligations at home as schools moved online, and the ramifications of staff becoming infected with the coronavirus.
Health centers are facing financial uncertainty on several fronts following the drop in patient volume during the pandemic. PCAs expressed concerns about the expiration of temporary provisions and authorizations related to Medicaid coverage and telehealth reimbursement when the public health emergency ends. They noted these provisions have been key to making telehealth viable for health center finances during the pandemic. On the other hand, Congress recently voted to reauthorize federal funding for the Community Health Center Program ($5.7 billion in FY 2021) and, if signed into law, would add much needed stability for health centers during the pandemic, although financial challenges remain going forward.
Questions remain about health centers’ role in administering a COVID-19 vaccine to medically underserved communities. Several PCA respondents reported that health centers are involved in vaccine distribution planning with states, but at the time of interviews, major questions remained about where vaccines would be shipped and stored, how frontline health center staff would be immunized, whether staff should be deployed to state-run vaccination sites, and how staff would track multiple doses of the vaccines. Most respondents also expressed the need for targeted messaging to encourage patients to get the COVID-19 vaccine, especially because populations served by health centers may be more reluctant to get a vaccine due to mistrust of the health care system.
Health centers have made major adaptations to their service delivery models to address health care needs in the most vulnerable communities during the pandemic, but they still face many challenges. Most immediate will be undertaking a massive vaccination campaign as the country continues to struggle with rising COVID-19 cases. Still, with the end of the pandemic potentially in sight, shifting focus from the immediate response to longer-term recovery will help ensure health centers remain able to care for historically underserved communities during the pandemic and after its resolution.
Key Findings
Introduction
In the midst of the COVID-19 pandemic, almost 1,400 community health centers can serve as public health responders for medically underserved populations. Operating in nearly 13,000 community locations, community health centers cared for nearly 30 million patients in 2019, including many high-need populations such as people who are homeless, low-income elderly individuals, and those with complex medical, behavioral, and social needs. Because of their location, scope of care, and experience in serving at-risk populations, community health centers continue to serve these populations not only for ongoing health care but also for COVID-19-related care. In response to the COVID-19 pandemic, nearly all community health centers are providing diagnostic testing for the COVID-19 virus, despite facing significant losses in operational capacity. Early in the outbreak, health centers experienced a heavy loss of visits and revenue and a large number of site closures. By the week of December 4th, health centers had made a significant recovery but still reported a 17% decline in visits compared to normal rates and closure of 1 in 20 sites.
In order to understand how community health centers have been able to serve their patients during the COVID-19 pandemic and the challenges they face in doing so, we interviewed respondents from 16 state and regional Primary Care Associations (PCAs) representing community health centers. In addition to the interviews, participating PCAs were asked to complete a supplemental questionnaire, with 14 out of 16 participating PCAs completing the questionnaire. Together, the 16 PCAs represent over 750 health centers (54 percent of all federally-funded health centers in operation during 2019, the latest year available) across 19 states and one U.S. territory. Community health centers in these states account for 63 percent of all health center patients served in 2019 and span inner-city and frontier areas. To maintain confidentiality of PCA discussants while providing some geographic context for the quotes, PCAs are identified as being located in one of four Census regions rather than identifying each by state. Additional detail on the methods underlying this analysis are in the Methods box at the end of the brief.
Key Findings
COVID-19 Testing, Contact Tracing, and Vaccine Distribution
Nearly all health centers are providing COVID-19 testing, focusing on vulnerable communities with limited testing resources. When the coronavirus pandemic hit, health centers quickly pivoted to providing COVID-19 testing in their communities. According to data from the Health Resources and Services Administration (HRSA), health centers provided over 335,000 tests in the week ending December 4th. Testing capacity has increased since the early weeks of the pandemic in April 2020, from 80% to 98% of responding health centers as of December 4th, 2020. PCA respondents described multiple efforts to increase capacity, including by setting up drive-thru testing sites in parking lots, creating temporary testing sites, some of which were in tents so that tests could be conducted outside, and deploying mobile testing units to target hard-to-reach populations, such as people who are homeless and migrant workers. Despite these efforts, several of responding PCAs said they were able to provide tests to all patients who need them, while a small share said they were uncertain if their members were able to meet all need (Appendix Table 1).
We have dozens of mobile units across the state and they have been mobilizing them just dramatically. It’s setting up the mobile pop-up test sites in random neighborhoods through the state or taking them to a homeless encampment to be able to make sure they’re also being taken care of for COVID reasons. Going out to migrant farms to be able to take care of those special populations that they kind of already had always done, but they kind of took it to the next level.
– PCA in the South
Barriers to meeting testing needs remain. Respondents cited several barriers to meeting the testing needs in their communities. Reflecting supply-chain issues reported across the country, the most common barriers reported were long waits for test results, shortages of PPE, and shortages of testing supplies and equipment (Appendix Table 2). In one case, a PCA respondent described two health centers that purchased their own testing equipment due to long wait times for results but, because of supply shortages on cartridges for the machine, the health centers were never able to activate the onsite testing equipment. In addition, several PCA respondents reported staff shortages as a concern for providing testing. Other barriers were a lack of clarity and/or communication on who should be tested, a lack of space to conduct testing, and an inability to cover all community locations, reflecting the diverse challenges reported by health centers to PCA respondents.
We’re having enormous issues getting PPE for our health centers to be able to perform testing. So that has been extremely problematic as well. The PCA reached out and took an inventory of all the needs of our health centers… But we’re still short on gowns, gloves, those kinds of things.
– PCA in the West
Health centers are coordinating with state and local public health agencies on COVID-19 response efforts. Since the beginning of the pandemic, respondents reported working closely with states and local health departments on a variety of issues from conducting COVID-19 testing and contact tracing to providing treatment for patients with COVID-19. For example, one PCA respondent described how the health care for the homeless project in their state helped to staff a temporary field hospital during the height of the crisis in the state. Additionally, some health centers have received funding to assist the state’s efforts to conduct contact tracing.
I think it was really key in the first week or so that we got in there with the state and painted this picture for them of a COVID response without health centers and they responded, I think pretty heroically, [with] immediate Medicaid advances to keep the doors open in the opening days. A lot of our health centers had negative margins…and they were just thinking, it’s game over. But the state provided advances and then worked with us very, very rapidly on a supplemental payment plan…Because that was provided, we’ve had real stabilization
– PCA in the Northeast
Health centers are preparing for a vaccine, but questions remain about their role in administering the vaccine within their communities. Most respondents indicated that health centers are involved in vaccine distribution planning with their states, but at the time of the interviews, they felt many questions remained unanswered. Several respondents noted they had been told health center staff would be vaccinated in the first phase of essential health care workers, though some were still unclear about how those vaccines would be administered. Although health centers are registered vaccine providers in their states, most respondents did not expect individual health centers to receive early doses of the Pfizer vaccine because of the cold storage requirements. While most anticipated receiving vaccines to administer to patients and community members in the coming months, one respondent noted the state was planning for large vaccination sites and was uncertain what role health centers might play in those events. Even as they prepare to administer the vaccine, respondents worried about the need to track multiple doses and multiple vaccines and the challenge of engaging in a large vaccination campaign at the same time staff are stretched thin responding to the current surge in COVID-19 cases.
Respondents also expressed the need for targeted messaging to encourage patients to get the COVID-19 vaccine. The Advisory Committee on Immunization Practices (ACIP) is now recommending people age 75 and older and frontline essential workers be vaccinated in phase 1b and adults ages 65-74, high-risk younger adults, and other essential workers be included in phase 1c. However, states will make the final decisions about vaccine prioritization and may vary from the ACIP. A recent report estimated that nearly half (47%) of health center patients would qualify for Phase 1b or 1c COVID-19 vaccination under the ACIP recommendations because they are adults of advanced age or with underlying health conditions that put them at higher risk of serious COVID-19 illness and many more are essential workers. PCA respondents noted that many of their patients may be more reluctant to get a vaccine due to mistrust of the health care system. Given health centers’ focus on underserved communities and their long-standing role in encouraging and providing immunizations, they can help garner trust among their patient communities, especially among communities of color who make up a disproportionate share of health center patients
If we’ve got 30 million patients that we’re seeing, we want to be a part of this distribution of the vaccinations, because we have these relationships.
– PCA in the Northeast
Shift to Telehealth
A rapid shift to telehealth helped health centers continue serving patients while observing social distancing measures. PCA respondents reported that when lockdowns were first implemented, health centers quickly transitioned to providing patient visits via telehealth. Working closely with state Medicaid agencies, respondents noted they were able to get emergency authorization for telehealth approved, which was critical for the viability of telehealth at health centers given that the bulk of patients (48% as of 2019) are enrolled in Medicaid. As a result, health centers were much better equipped than in the past to continue seeing patients and providing non-COVID-19 related care. For example, most PCA respondents reported that, prior to the pandemic, less than 5% of total visits were conducted virtually (Appendix Table 3); in a separate survey of health centers conducted by HRSA, health centers reported that three in ten visits (30%) were conducted virtually for the week ending on December 4th, 2020, down from as much as 54% in April. However, respondents noted that the shift to telehealth required new workflows and a shift in staff resources. While most respondents agreed that telehealth is “here to stay,” some expressed concern that shifting to telehealth will disengage health centers from their communities and their patients and could result in care that is less effective than face-to-face encounters.
Telemedicine/telehealth has just been a lifesaver for us, and the centers have adapted really quickly. Before COVID, about 3% of our centers were using virtual visits in some capacity, now about 95% of them are.
– PCA in the South
The shift to telehealth presents challenges for medically underserved communities, such as technological and cultural barriers. Respondents noted that health centers faced a number of challenges in making the transition to telehealth. Technological issues, including internet access, particularly in rural areas, and smartphone data plan limits present barriers for some patients. Health centers have developed creative solutions to address these problems, including installing WIFI boosters in their parking lots and providing tablets to patients who participate in telehealth visits from their cars. They have also redeployed some staff to walk patients though the process of setting up for telehealth visits. Other concerns, though, are harder to address. Many patients do not feel comfortable using telehealth, and others living in crowded housing situations face privacy concerns. Several respondents also mentioned safety issues for patients at risk of or facing domestic violence.
Domestic abuse situations in a telehealth encounter don’t work well especially when the abuser is sitting in the room with you. And also in terms of other mental health visits, a lot of our patients live in apartments with six or seven other family members there and don’t feel comfortable having a tele-mental health visit with their family members or others in the room as well.
– PCA in the Midwest
Despite ongoing challenges, telehealth services have improved access for some hard-to-reach populations and for some services. Nearly all respondents noted that one benefit of telehealth has been improved access to care for some populations. One respondent reported that no-show rates had declined because patients did not have to deal with transportation, child care issues, or taking time off from work. The ability to provide visits over the phone has helped to engage certain groups, according to some respondents, including patients in early recovery from substance use disorder and Latino men. The phone visits allow these individuals to more easily fit appointments into their schedules. Across the board, respondents said access to mental health visits had increased because of telehealth.
I think the biggest thing with telehealth is we realized how much of a difference it makes with so many of our patients in terms of addressing some of the determinants of health. The no-show rates are down into the single digits. But that’s because patients don’t have to worry about transportation, child care, taking off from a job that they probably don’t have sick leave to take off from and you’re meeting them where they are.
– PCA in the Northeast
Managing Ongoing Health Needs
PCAs reported that following the initial shutdowns in March and April, visits for some services had rebounded to close to pre-pandemic levels by October while visits for other services remain low. In particular, most PCA respondents reported that preventive services for adults and dental visits showed the biggest drops at the time of the study compared to pre-pandemic levels (Appendix Table 4). Other services with the greatest declines according to respondents included well-child visits, child immunizations, and chronic conditions management. While health centers saw a large increase in telehealth utilization beginning in March, virtual visits were not enough to offset declines for most services, and respondents expressed concern that visits could drop again amid rising cases. Respondents attributed the decline in these visits to patients’ fear of infection when coming into the health centers for services; however, respondents noted the situation presents challenges to preventing and managing illness and could have long-term consequences for patients.
It is still a challenge of getting patients in. Something that people are working on is an outreach program, an informational campaign for the community this fall to begin to get our chronic patients back into the facilities because we are prepared to do that and it is necessary, particularly in our urban communities.
– PCA in the Midwest
Health centers have increased telehealth availability, moved services outside the clinic, and made physical adaptations to ensure patient safety and to encourage patients to continue to seek regular care, but also fear a return to indoor services. At the time of the focus groups, respondents said health centers were focused on creating safe environments for the patients to return to in-person visits. Some health centers have reconfigured their space to have a “sick” clinic and a “well” clinic for both children and adults while others have designated age-specific locations – one site for pediatrics only and another for adults. Health centers that cannot set up separate spaces for sick and well patients have instead established time blocks for sick patients followed by an intensive decontamination before seeing well patients. Similar to drive-up COVID-19 testing, some health centers also have set up drive-up pharmacies to facilitate access to medications. Finally, some health centers are upgrading HVAC systems and building more walls to close off internal spaces. At the same time, while respondents noted that health centers remain focused on getting patients to return for in-person visits, PCA respondents from colder-climate states, in particular, were uniform in their concern about what would happen when the warm weather ended and they would no longer have the option of serving patients outdoors. All PCA directors were aware of the threat that fully returning indoors would carry for patients and staff alike, and the extent to which moving operations back inside could create barriers to accessing care for some patients.
Health centers [are] doing work such as having a “sick” clinic and a “well” clinic – “sick” entrance and “well” entrance. We have one health center that has reported really great results, they said that the patients feel safer by that approach.
– PCA in the West
Health centers are finding other creative solutions to help patients manage their ongoing health needs. Respondents described health centers’ use of mobile vans to provide certain services, such as flu vaccinations. Noting the limitations of telehealth visits for preventive and chronic disease management visits, respondents reported that some providers were teaching patients how to take their pulse or check their blood pressure or blood sugar so that maintenance visits could be conducted through telehealth rather than in person. They also discussed conducting home visits for certain populations, including high-risk elderly patients.
Certain staff are working remotely and certain staff are working at the center and so we’re doing a combination of in-person, telehealth, and actually at-home visits, particularly for our elderly, at-risk patients, or patients that have significant underlying conditions.
– PCA in the South
Targeting At-Risk Communities and Addressing Non-Medical Needs
Many health centers are taking services outside the clinic and into communities that are underserved and at elevated risk for contracting COVID-19. The threat of COVID-19 has made it even more difficult for some populations to access care out of fear of exposure to the virus and because of more limited capacity at health center sites, both for ongoing health needs as well as testing and treatment for COVID-19. Respondents described ways health centers are serving populations, including migrant farmworkers, American Indians, and people experiencing homelessness, outside of the clinic setting. According to respondents, given the longstanding relationships health centers have built with their communities, they are uniquely positioned to reach underserved populations. Using mobile vans, health center staff have gone into communities, sometimes outside of their service area, to provide COVID-19 testing and other services. Respondents noted that in addition to testing, health center staff are making sure these communities have masks, hand washing stations, and hand sanitizer so they can protect themselves against COVID-19. Some have also set up isolation camps or secured quarantine housing for migrant workers who test positive. One respondent noted that “taking health care to the community where it’s needed as opposed to a defined site” is something health centers see as a new opportunity to improve care and to offset the closing of some health center sites.
Our Indian Health Centers on the reservation…really joined forces to do this, it wasn’t just providing testing but also getting PPE to the residents in those areas. So it was up to our health centers to make sure there are hand washing stations, PPE, sanitizer, food, it was all in an effort to try to protect them…In fact, there was another entity that actually provided planes to drop off the PPE, not only to remote rural areas…They also did that with the Navajo reservation and many of our health centers helped to disperse those supplies.
– PCA in the West
Health centers have expanded non-medical services that affect health, such as food distribution, in response to economic instability during the pandemic. The economic crisis caused by the coronavirus pandemic led to increased needs for food and other social services among health center patients, as well as the continued need for health centers to provide traditional enabling services such as outreach and enrollment assistance. Respondents reported that health centers partnered with food pantries and played a more active role in food distribution than before the pandemic. In Boston, health centers partnered with city officials to receive food deliveries that they then distributed in their communities. Health centers also stepped in to fill in gaps in providing food when schools closed. Beyond the pandemic, health centers in Minnesota were involved in distributing food after the civil unrest following the death of George Floyd. In addition, respondents also described adopting a trauma-informed care model to reassess the social needs of their patients, including needs for housing or other supports.
So, we have a number of places where you can go through a drive-thru for food distribution and get a COVID test at the same time. Or places where the health centers are offering services alongside their food pantry and then some food pantries that are doing distributions at health centers because it’s a place where people are coming already just to limit transportation.
– PCA in the Midwest
Operational Challenges to Continuing Care
Health centers face ongoing shortages of testing supplies and PPE. As with many other health care providers, respondents reported that acquiring PPE and testing supplies has been a challenge for health centers since the pandemic began. With these items in high demand across the country, respondents reported having to compete with hospitals and large health systems for key protective gear. In addition, acquiring PPE in the different sizes that fit staff (for example, small gloves) has been a challenge. Many health centers have relied on consortia or PCAs for group buying power and for the ability to purchase supplies from the state or large health systems, although respondents indicated that health centers face continuing challenges acquiring testing supplies and PPE.
The reality of the situation is that hospitals get first dibs and we’re at the bottom of the food chain there.
– PCA in the South
Although layoffs have been relatively limited, the pandemic’s impact on staff morale is a concern for the workforce and health care accessibility. According to respondents, health centers have managed to avoid large staff layoffs; most respondents reported either none or fewer than 10% of staff have been laid off or furloughed since March. Only one respondent estimated that more than 10% of clinical staff had been laid off at the health centers they represent, although no PCAs reported that more than 10% of administrative or enabling services staff had been laid off (Appendix Table 5). However, most respondents were concerned about how the uncertainty surrounding the pandemic was impacting staff morale and how the shift to telehealth had been more difficult for certain staff. For example, several PCAs reported that some providers, such as mental health and substance use disorder providers, have generally been able to transition from in-person visits to telehealth with few disruptions. However, other services have had greater difficulty transitioning to telehealth, such as dental or group nutrition classes. Another major concern among many PCAs was the staff with children who are balancing work demands along with virtual schooling at home. Some respondents reported staff leaving their jobs to support their children at home or reported increased risk of burnout among staff. Another concern raised by some respondents was that some providers who contracted COVID-19 and have since recovered are facing long-term conditions from the virus, such as fatigue, that have affected their ability to perform duties after returning to work. The range of staffing challenges related to the pandemic adds pressure on health centers that already faced challenges recruiting and retaining staff before the pandemic, and could affect health care accessibility even after the pandemic is over.
We’ve had a lot of sites have staff quit because they had to be at home with their kids because they’re in a position where they’re not able to work at home. Our behavioral health providers are thriving in a virtual environment. And they are able to put all of their services as virtual but for our staff members that aren’t able to work virtually, I think they’re struggling and I think that struggles are starting to trickle down to morale and burnout.
– PCA in the South
Financial Challenges
Health centers are facing a decline in revenue and increased operating costs, compared to finances before the pandemic. Due to social distancing measures and site closures, health centers have seen declines in visits, which has led to an estimated $4 billion in patient revenue losses since April, or roughly 13% of total 2019 revenue. When asked to estimate how current patient revenue had changed since before the pandemic, nearly all the PCAs estimated that revenues from patient visits were down either between 1% to 25% or down by roughly 26% to 50% (Appendix Tables 6). At the same time, however, health centers are facing increased operating costs during the pandemic related to increased costs for PPE, testing supplies, and implementing and operating telehealth programs (Appendix Table 7).
I think it’s important to recognize the revenue reduction, loss of revenue for the health centers. Some of our health centers lost over 50% of their revenue. This is not going to be made up in three or four or even six months. It’s going to take a while. And so that’s something that we are looking at – to find ways of how do we augment what’s been lost and cannot be replaced.
– PCA in the South
Federal financial relief has helped to limit revenue losses, but some health centers were ineligible for key federal funding programs or were concerned about meeting complex funding requirements. All federally-funded health centers received a total of nearly $2 billion in rapid response grants from HRSA to improve COVID-19 testing capacity, purchase PPE, and to maintain health center capacity generally. Health centers did not need to apply for these grants, and the award was determined by the size of the health center patient population and the number of uninsured patients reported in the Uniform Data System. In addition to the rapid response grants, health centers were also eligible for other federal funding made available through coronavirus recovery legislation, including the Paycheck Protection Program (PPP), the Provider Relief Fund, and the Uninsured Claims Fund. These funds had more restrictive application and awarding processes and had more limitations in how the funds could be spent. While respondents reported that smaller and rural health centers were generally able to access needed federal funding and loans, they were more concerned about larger health centers, generally located in urban areas, which also saw larger drops in patient visits compared to rural health centers due to more strict social distancing measures. They noted that some of these health centers could not apply for PPP loans because they exceeded the 500-employee limit for a non-profit to qualify. An estimated 93 health centers are ineligible for PPP loans because of their size; collectively, these health centers serve 28% of health center patients nationwide. PCAs also reported that some health centers expressed concerns with limitations on how some federal grants can be spent. In some cases, respondents reported that some health centers are not applying for more grants due to the complexity of spending restrictions.
And our big health centers weren’t eligible for PPP forgiveness, they’re really struggling. We’ve seen this pattern that you’re in a worse financial spot than if you’re a smaller organization or rural health center.
– PCA in the Midwest
Health centers are relying heavily on telehealth to supplement lost revenue, but uncertainty remains over whether states will roll back temporary telehealth payment policies. Respondents reported that many state Medicaid agencies temporarily increased payments for many services conducted via telehealth to be comparable to in-person visits, which they felt was critical to keeping health centers solvent as well as making telehealth more widely available. However, state Medicaid agencies have not authorized the telehealth reimbursements permanently, and most respondents identified the uncertainty of future telehealth reimbursement as a concern for health centers’ finances. They were especially concerned that state Medicaid agencies could eliminate or reduce the temporary telehealth reimbursement rates if states seek budget cuts to make up for lost revenues during the pandemic.
I think for us a big concern is not getting the full reimbursement rate for telehealth. I think there’s an assumption from policymakers and a lot of education that’s needed that it costs less to run telehealth, where if anything the IT infrastructure, the liability; you know all that costs more, or at least equal. …[W]hen we think about sustainability and just making it through the end of the pandemic whenever that is, that is a big concern for people right now.
– PCA in the South
Respondents also expressed concerns about the eventual end of the temporary Medicaid continuity of coverage provisions and the potential loss of coverage for Medicaid patients that could result when states resume Medicaid redeterminations. As part of the Families First Coronavirus Response Act, states are eligible to receive an increase in the federal match rate for certain Medicaid spending if they meet maintenance of eligibility (MOE) requirements that include ensuring continuous coverage for current enrollees. The MOE requirements are tied to the end of the public health emergency (PHE), at which point state Medicaid agencies cannot be penalized for removing Medicaid enrollees who are no longer eligible due to changes in circumstances that are identified or reported during redeterminations. Several respondents raised concerns that patients currently covered by Medicaid could lose coverage when the MOE requirements end. They also noted that confusion over how states will handle redeterminations may result in otherwise eligible individuals losing coverage if they have trouble completing redetermination processes or providing verification. The potential for a decline in Medicaid enrollment and an increase in uninsured individuals seeking care could impact health center finances, and it would come as health centers attempt to recover from revenue losses during the pandemic.
The state announced that in September they have been doing administrative renewals, they have just been extending [coverage]. But now they are starting to send renewal packets out to their patients at the same time as sending out letters saying you’re okay under the emergency waiver. So [the letters] created a tremendous amount of confusion among our patients.
– PCA in the South
Congress recently voted to reauthorize continued federal funding for the Health Center Program and, if signed into law, could add stability to health center finances through FY 2023, though it is unlikely to be a panacea for health center finances during the pandemic. In total, Congress voted to appropriate $5.7 billion to the Health Center Program for FY 2021, most of which ($4 billion) comes from the Community Health Center Fund (CHCF) that provides an additional $4 billion per fiscal year until FY 2023. PCA respondents described the CHCF as an ongoing source of stability for health centers, especially as health centers manage a number of other financial uncertainties during the pandemic. While the three-year funding of the CHCF will help to stabilize health center finances, they will likely face more financial challenges going forward as their role in vaccine distribution ramps up, as well as when they reconfigure their services, staffing, and clinics back to normal operations following the resolution of the pandemic.
Conclusion
Community health centers play a key role in addressing COVID-19 outbreaks, particularly in communities with high poverty and high health care needs. They have quickly adapted to the emergency situation with new models of care, responded to both medical and nonmedical needs, and moved care into new locations and configurations. Health centers’ history of reaching medically underserved communities and populations has made them core members of many states’ coronavirus response.
Health centers are expected to be involved in administering the COVID-19 vaccine in the coming months. As states finalize their vaccine distribution plans, health center staff and many of their patients will be among the priority groups to receive early doses of the vaccine. Although health centers have experience providing vaccines for other diseases, they will face unique challenges with the COVID-19 vaccine, including cold storage requirements and the need to track multiple doses from multiple vaccines. At the same time, they can serve as a trusted source of information to overcome concerns about getting the vaccine among at-risk and other vulnerable patients.
As health centers seek to continue serving their patients, numerous difficulties remain. Although the shift to telehealth has helped to restore access to primary care, there are still barriers to managing ongoing health needs and addressing the increased need for social services and supports among health center patients. At the same time, health centers face cumulative revenue shortfalls and uncertainty surrounding various revenue streams. Failure to address these challenges may undermine their ability to provide care to vulnerable and historically underserved communities.
The health center experience also shows a need to focus on the pandemic aftermath. Reviving effective preventive and primary care services that were set aside in order to mount the pandemic response will be a challenge. In addition to restoring services, providers will also need to re-establish the trust relationship that has enabled community health centers to succeed in ensuring that hard-to-serve populations have access to culturally competent care. If the nation is to fully move back to normal, designing and implementing long-term recovery policies will be as important as the initial response.
This brief was prepared by Bradley Corallo and Jennifer Tolbert of KFF and Sara Rosenbaum, Jessica Sharac, Peter Shin, and Charmi Trivedi of the Geiger Gibson/RCHN Community Health Foundation Research Collaborative at the George Washington University.
Additional funding support for this brief was provided to the George Washington University by the RCHN Community Health Foundation.
Methods
Findings in the brief are based on focus groups conducted with 16 Primary Care Association (PCAs) representing 19 states and one U.S. territory in late September and early October 2020. A later focus group and interviews focused on COVID-19 vaccine distribution were conducted in November and December 2020. Participating PCA respondents were also asked to complete a supplemental data request. Fourteen PCAs responded to the supplemental data request, with one regional PCA providing a separate response for each of two member states, for a total of 15 survey responses. Invitations to focus groups and the supplemental data request were sent to PCA directors and were either completed by the director or their designee.
We selected PCAs for interviews based on a mix of characteristics corresponding to the health centers they represent, including region of the United States, urban vs. rural areas, number of health center organizations in a state, and whether the states were considered hotspots for the coronavirus in early 2020. Together, the 16 PCAs represent over 750 health centers (54 percent of all federally-funded health centers in operation during 2019) across 19 states and one U.S. territory. Community health centers in these states account for 63 percent of all health center patients served in 2019, the latest year that these data are available.
Primary Care Associations are state and regional non-profit organizations that support health centers to meet the key goals of the Health Center Program. Some of the key tasks performed by PCAs include: providing training and technical assistance to health centers, creating economies of scale for purchasing power, monitoring policy and regulatory changes affecting health centers, assisting health centers to adapt to changing health care needs for patients, and facilitating collaboration with other health centers and key government agencies.
Appendix
Appendix Table 1: Health Centers’ Capacity to Provide COVID-19 Diagnostic Testing to All Patients Who Need Tests
Among member health centers providing COVID-19 diagnostic tests, are health centers generally able to provide tests for all patients who need them? (14 Responses)
Yes
7
No
6
Don’t Know
1
NOTE: Figure based on 14 responses to a supplemental questionnaire from PCAs that participated in focus group discussions. In total, the PCAs responding to this question represent 596 federally-funded health center organizations (43% of all health center organizations) across 14 states.SOURCE: KFF and Geiger Gibson/RCHN Community Health Foundation Study of Primary Care Associations on Community Health Centers’ Response to the COVID-19 Pandemic.
Appendix Table 2: Barriers to Adequate COVID-19 Diagnostic Testing Provided by Health Centers
Please identify all applicable barriers to adequate COVID-19 diagnostic testing provided by health centers, if any, that member health centers are reporting. (15 Responses)
Member health centers have not reported any barriers to adequate diagnostic testing at their health centers (if selected, please do not check another type of barrier)
0
Member health centers have not reported any barriers because other providers in the community provide adequate COVID-19 testing
1
Long waiting times for test results
14
Shortage of testing supplies and equipment
13
Shortage of personal protective equipment (PPE) to protect staff
13
Shortage of staff
10
Inability to provide tests to all patients who need a test
9
Inability to coverall all of the community locations where patients need to get their tests
7
Lack of space to conduct testing
7
Lack of clarity/communication regarding who should receive testing
7
Initial HRSA funding to provide testing has run out
4
Other barrier to adequate testing
7
NOTE: Figure based on 15 responses to a supplemental questionnaire from PCAs that participated in focus group discussions. In total, the PCAs responding to this question represent 694 federally-funded health center organizations (50% of all health center organizations) across 18 states.SOURCE: KFF and Geiger Gibson/RCHN Community Health Foundation Study of Primary Care Associations on Community Health Centers’ Response to the COVID-19 Pandemic.
Appendix Table 3: Share of All Health Center Visits That Were Virtual Before March 1, 2020
Before March 1, 2020, approximately what share of all visits at your member health centers were virtual visits (e.g., telehealth/telephonic)? Please consider all virtual visits regardless of service type (e.g., medical, dental, behavioral health, etc.), but do not include calls to patients for such things as appointment confirmations or pharmacy reminders. (15 Responses)
Few or none
5
1%-5%
5
6%-10%
2
11%-15%
0
16%-20%
2
Greater than 20%
0
Don’t know
1
NOTE: Figure based on 15 responses to a supplemental questionnaire from PCAs that participated in focus group discussions. In total, the PCAs responding to this question represent 694 federally-funded health center organizations (50% of all health center organizations) across 18 states.SOURCE: KFF and Geiger Gibson/RCHN Community Health Foundation Study of Primary Care Associations on Community Health Centers’ Response to the COVID-19 Pandemic.
Appendix Table 4: Health Center Services with the Greatest Declines in Visits Currently Compared to Visit Levels Before March 1, 2020
Thinking about your member health centers overall, which services, if any, are currently experiencing the greatest declines in visits compared to visit levels before March 1, 2020? Please select up to but no more than 3 services. (15 Responses)
No services are currently experiencing a decline in visits compared to visit levels before March 1, 2020 (if checked, please do not select another type of service)
0
Preventive services for adults (such as routine exams and immunizations
Cancer screenings (such as cervical cancer screenings, colorectal cancer screenings, and mammograms)
1
Prenatal care services
1
Family planning services
0
Mental health services
0
Substance use disorder services
0
Vision services
0
Pharmacy services
0
Services for patients receiving in-home care
0
NOTE: Figure based on 15 responses to a supplemental questionnaire from PCAs that participated in focus group discussions. In total, the PCAs responding to this question represent 694 federally-funded health center organizations (50% of all health center organizations) across 18 states.SOURCE: KFF and Geiger Gibson/RCHN Community Health Foundation Study of Primary Care Associations on Community Health Centers’ Response to the COVID-19 Pandemic.
Appendix Table 5: Share of Health Center Staff Laid Off or Furloughed Since March 1, 2020 and Not Returned or Rehired
Thinking about your member health centers overall, approximately what percentage of the following staff have been laid off or furloughed since March 1, 2020 and have not since returned to work or been rehired? (15 Responses)
Administrative Staff
Clinical Staff
Enabling Services Staff
None or very few
5
6
5
10% or less
8
5
6
11%-25%
0
1
0
26%-50%
0
0
0
More than 50%
0
0
0
Don’t know
2
3
3
NOTE: Figure based on 15 responses to a supplemental questionnaire from PCAs that participated in focus group discussions. In total, the PCAs responding to this question represent 694 federally-funded health center organizations (50% of all health center organizations) across 18 states.SOURCE: KFF and Geiger Gibson/RCHN Community Health Foundation Study of Primary Care Associations on Community Health Centers’ Response to the COVID-19 Pandemic.
Appendix Table 6: Changes in Health Centers’ Operating Costs Since March 1, 2020
Thinking about your member health centers overall, have operating costs generally increased, decreased, or stayed about the same since March 1, 2020? (15 Responses)
Operating costs have increased
10
Operating costs have stayed about the same
1
Operating costs have decreased
1
Don’t know
3
NOTE: Figure based on 15 responses to a supplemental questionnaire from PCAs that participated in focus group discussions. In total, the PCAs responding to this question represent 694 federally-funded health center organizations (50% of all health center organizations) across 18 states.SOURCE: KFF and Geiger Gibson/RCHN Community Health Foundation Study of Primary Care Associations on Community Health Centers’ Response to the COVID-19 Pandemic.
Appendix Table 7: Changes in Health Centers’ Patient Revenue Since March 1, 2020
Thinking about your member health centers overall, roughly how much has current patient revenue (i.e., insurance reimbursement and self-pay revenue) changed for your member health centers as a whole compared to patient revenue before March 1, 2020? (15 Responses)
Patient revenue is roughly the same or greater compared to patient revenue before March 1, 2020
0
Patient revenue has decreased by 1-25%
8
Patient revenue has decreased by 26%-50%
6
Patient revenue has decreased by more than 50%
0
Don’t know
1
NOTE: Figure based on 15 responses to a supplemental questionnaire from PCAs that participated in focus group discussions. In total, the PCAs responding to this question represent 694 federally-funded health center organizations (50% of all health center organizations) across 18 states.SOURCE: KFF and Geiger Gibson/RCHN Community Health Foundation Study of Primary Care Associations on Community Health Centers’ Response to the COVID-19 Pandemic.
While millions have recently lost their jobs or income and face new stresses, many who have been working during the pandemic also face new pressures. Almost overnight, the COVID-19 pandemic presented many workers with a whole host of concurrent risk factors for poor mental health and substance use problems, including generally high levels of uncertainty and fear, an overload of news and information, changes to workplace processes and demands, changes in household dynamics, financial and job security concerns, potential worsening of existing health conditions, and difficulties linked to caregiving. People working during the pandemic face unique threats to mental health and well being depending on which sector they work in and their potential exposure to the coronavirus. Generally speaking, surveys conducted during the pandemic have found that many workers have been experiencingburnout (which results from chronic workplace stress and can impact an individual’s motivation and productivity) and adverse mental health outcomes. (more…)
Both Remote and On-Site Workers are Grappling with Serious Mental Health Consequences of COVID-19
While millions have recently lost their jobs or income and face new stresses, many who have been working during the pandemic also face new pressures. Almost overnight, the COVID-19 pandemic presented many workers with a whole host of concurrent risk factors for poor mental health and substance use problems, including generally high levels of uncertainty and fear, an overload of news and information, changes to workplace processes and demands, changes in household dynamics, financial and job security concerns, potential worsening of existing health conditions, and difficulties linked to caregiving. People working during the pandemic face unique threats to mental health and well being depending on which sector they work in and their potential exposure to the coronavirus. Generally speaking, surveys conducted during the pandemic have found that many workers have been experiencingburnout (which results from chronic workplace stress and can impact an individual’s motivation and productivity) and adverse mental health outcomes. (more…)
While millions have recently lost their jobs or income and face new stresses, many who have been working during the pandemic also face new pressures. Almost overnight, the COVID-19 pandemic presented many workers with a whole host of concurrent risk factors for poor mental health and substance use problems, including generally high levels of uncertainty and fear, an overload of news and information, changes to workplace processes and demands, changes in household dynamics, financial and job security concerns, potential worsening of existing health conditions, and difficulties linked to caregiving. People working during the pandemic face unique threats to mental health and well being depending on which sector they work in and their potential exposure to the coronavirus. Generally speaking, surveys conducted during the pandemic have found that many workers have been experiencingburnout (which results from chronic workplace stress and can impact an individual’s motivation and productivity) and adverse mental health outcomes. (more…)
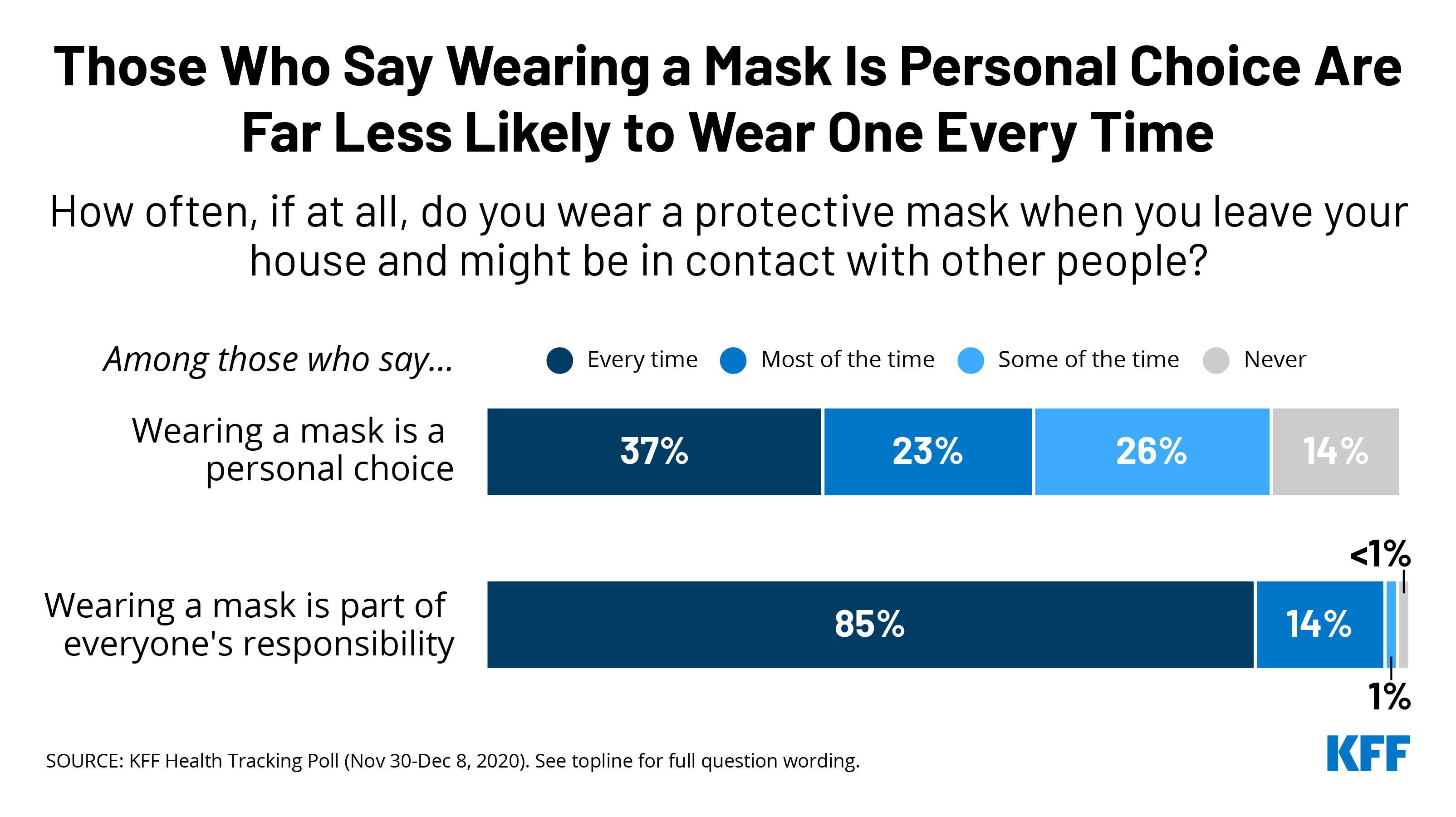
When People See Wearing a Mask as Part of Everyone’s Responsibility, They Are More Likely to Do So
A new KFF Health Tracking Poll finds that the use of protective face masks varies depending on whether people view it as a personal choice or collective responsibility. Among those who say that wearing a mask is part of everyone’s responsibility, 85% say that they wear a mask every time they leave their house and might be in contact with other people, and less than 1% say they never wear a mask. Among those who say that wearing a mask is a personal choice, just 37% report wearing a mask every time they leave the house and 14% say they never wear a mask.
The results highlight that adherence to public health guidance is likely affected by the public framing of the issue. The Trump Administration has promoted mask wearing as a personal choice and has opposed the idea of a nationwide mask mandate. President-elect Joe Biden has promised that he will urge all Americans to wear masks for the first 100 days of his presidency and has framed the issue as part of people’s “patriotic duty.”
Source
KFF Health Tracking Poll – December 2020: COVID-19 and Biden’s Health Care Agenda
President-elect Joe Biden campaigned on restoring the Title X family planning program that has been diminished under the Trump Administration. The Biden Administration will likely take executive action to reverse the Trump Administration regulations and restore access to Title X funded services to parts of the country that have lost federal support as a result of the regulations. This executive action could also restore the standards of care that were previously required by the Title X program, including provision of abortion referrals when requested and non-directive pregnancy options counseling, as well as allowing family planning sites to provide abortion services with non-federal funding. New regulations would also have an impact on the ongoing litigation challenging the Trump Administration regulations.
This analysis reviews the impact the Trump Administration regulations have had on the Title X network and discusses the likely impact and limitations of the Biden Administration’s potential actions.
In the United States, approximately 700 women die each year as a result of pregnancy or delivery complications. An additional 50,000 women each year face short or long-term severe consequences to their health as an outcome of pregnancy or labor. Both maternal mortality and severe morbidity have been steadily increasing over the past years, prompting a federal response to maternal health issues. There has been growing attention to wide racial and ethnic disparities in maternal health outcomes as well as gaps in maternity care services in many communities, particularly rural areas. There has also been growing emphasis on improving care in the postpartum period, such as recommendations to expand care beyond the traditional one postpartum visit.
Medicaid pays for more than four in ten births nationally and is the focus of some of the pending bills in Congress as well as some state efforts to improve maternity care. Federal law requires that all states extend Medicaid eligibility to pregnant women with incomes up to 138% of the federal poverty level ($29,435 annually for a family of three). Pregnancy-related coverage for the woman must last through 60 days postpartum. In the states that have expanded eligibility for Medicaid under the Affordable Care Act (ACA), many low-income women can remain on Medicaid after the 60 days postpartum period or qualify for federal subsidies to purchase coverage through ACA Marketplace plans. However, in the states that have not adopted the ACA’s Medicaid expansion, postpartum women need to requalify for Medicaid as parents to stay on the program, but eligibility levels for parents are much lower than for pregnant women. As a result, many women in non-expansion states become uninsured after pregnancy-related coverage ends 60 days postpartum because, even though they are poor, their income is still too high to qualify for Medicaid as parents.
The 115th Congress passed the Preventing Maternal Deaths Act of 2018 (H.R. 1318), which authorized the CDC to increase support for state and tribal maternal mortality review committees (MMRCs). A number of other bills, focusing on maternal health, have been introduced in the Congress in the 2019-2020 session. These pending bills address a number of related maternity care issues, including extending Medicaid postpartum coverage from 60 days to one year, funding for clinical training on health equity and implicit bias, developing broader networks of maternity care providers in rural areas, and research on the potential benefits of Medicaid coverage for doula care. Below, are summaries of several bills on maternal health currently pending in Congress.
The recent election of former Vice President Joe Biden as well as the on-going effects of the coronavirus pandemic and related economic downturn are the key issues that will substantially shape Medicaid policy over the next year. The President-elect has supported the Medicaid expansion under the Affordable Care Act (ACA) and has proposed broader coverage expansions using a federal public option to cover more low-income Americans, including those in states that have not expanded. Such proposals require Congressional Action that will likely be difficult to pass in a closely divided Senate, and particularly so without Democratic control. Barring major legislative initiatives, there are a number of more targeted actions that the new Administration could implement to expand Medicaid coverage. While these approaches have the potential to reduce the number of people uninsured, they could also increase federal and state spending, which could pose particular challenges at the state level during a period of tight revenues and increasing needs.
Revise Section 1115 Waiver Policy to Support Coverage
The Biden Administration can revise current demonstration waiver policy to focus on expanding coverage and rescind or reverse waiver policies that limit coverage, including work requirements and other restrictive provisions. Section 1115 waiver priorities may change from one presidential administration to another. While each administration has some discretion over which types of waivers to approve and encourage, that discretion is not unlimited: the HHS Secretary must determine that the waiver will promote program objectives as set out by Congress. The Biden Administration could revise the Section 1115 waiver approval criteria to include expanding coverage, a provision removed by the Trump Administration. The Biden Administration also could rescind CMS guidance that invites state waivers to condition Medicaid eligibility on work requirements; stop defending waiver approvals involving work requirements and other restrictive provisions in lawsuits in AR, NH, IN, and MI; and reject pending work requirement waivers. The Biden Administration will face these issues as soon as it takes office, because the Supreme Court is hearing cases involving the Arkansas and New Hampshire work requirement waivers this term. In addition, the Biden Administration could review provisions, such as work requirements, in currently approved waivers and renewal requests and move to withdraw or not renew waivers that are not promoting program objectives.
The Biden Administration can approve or encourage waivers that would expand coverage to targeted groups or help make Marketplace coverage more affordable. For example, the Biden Administration could approve pending waivers and encourage additional waivers to extend the postpartum coverage period beyond 60 days, or encourage waiver proposals to extend coverage to incarcerated individuals prior to release, and to allow 12-month continuous eligibility for adults. Massachusetts and Vermont were able to leverage existing Medicaid Section 1115 waivers to secure federal Medicaid matching funds to help finance enhanced premium subsidies for Marketplace coverage. Some states had debated and Washington state enacted a public plan option designed to spur competition and lower costs for Marketplace enrollees, but without any type of waiver from the federal government. While the Trump administration has discouraged use of waivers under Section 1332 to expand public coverage, the Biden administration could provide guidance to states on using Medicaid 1115 waivers in combination with Section 1332 waivers to advance these public plan proposals or other strategies, along with the potential flexibility to reinvest any federal savings from lower costs for ACA premium subsidies to improve affordability for consumers and expand coverage.
The Biden Administration could encourage states to adopt certain waiver policies by establishing a template with options to expand coverage and with streamlined approval. One constraint in using waivers to expand coverage is that it has been longstanding federal policy to require that waivers be budget neutral for the federal government, meaning federal costs under a waiver must not exceed what federal costs would have been for that state without the waiver. Unlike before the ACA, states do not need to find savings to extend coverage to adults without dependent children.
Extend the Public Health Emergency (PHE)
The Biden Administration can extend the COVID-19 public health emergency (PHE) declaration, which will extend access to the temporary increase in the Medicaid match rate as well as Maintenance of Eligibility (MOE) requirements including continuous coverage. The PHE currently is set to expire on January 20, 2021. The Families First Coronavirus Response Act provided a 6.2 percentage point increase in the federal share for non-expansion Medicaid spending with requirements to maintain eligibility and provide continuous coverage for all Medicaid enrollees. The enhanced match is in place until the end of the quarter in which the PHE ends, while the continuous coverage requirement of the MOE is in place until the end of the month in which the PHE ends. The enhanced FMAP provides broad fiscal relief states and also supports increases in enrollment tied to the MOE and the economic downturn. Under the MOE, states cannot make eligibility standards or enrollment procedures more restrictive or increase premiums while they are receiving enhanced federal funds.
States are using emergency authorities to adopt a number of policy options to facilitate Medicaid coverage that are also tied to the PHE. Beyond the MOE requirements, nearly all (47) states are making changes to streamline eligibility and/or enrollment to help connect people to coverage more quickly during the pandemic. States are also using emergency authorities to expand eligibility for individuals who need long-term services and supports. Over half of states have expanded eligibility criteria for seniors and people with disabilities, while a few states have increased the total number of home and community-based waiver enrollees served. Nearly all states have streamlined enrollment processes, and over one-third of states have eased premium and/or cost-sharing requirements for seniors and people with disabilities. Extending the PHE would also extend use of many of these emergency authorities.
The Biden Administration could also expand the use of Section 1115 waivers during the PHE. The Trump Administration released a waiver template for COVID-19 related changes that were primarily focused on allowing states to adopt certain LTSS policies, and approvals to date have been related to requests made under the template. For example, CMS did not approve Washington’s request to establish a temporary eligibility group to provide additional Marketplace subsidies for individuals with incomes at or below 200% FPL. CMS also has not yet approved Washington’s request to use Medicaid waiver authority create a Disaster Relief Fund to cover costs associated with the treatment of uninsured individuals with COVID-19, housing, nutrition supports and other COVID related expenditures. Historically, states have used Section 1115 authority to expand coverage and/or reimburse uncompensated care to address the direct impact of natural disasters and public health emergencies.
Remove Barriers to Coverage Post PHE
A Biden Administration can work with states to help support coverage after the PHE ends. The Biden Administration can help and encourage states to transition policies that expand eligibility and streamline enrollment adopted under emergency authorities to permanent authorities after the PHE. In addition, the Biden Administration can develop guidance to ensure that those who are eligible stay enrolled in Medicaid at the end of the PHE. When states were implementing updated enrollment systems and processes to comply with the ACA, CMS worked with states to delay and stagger renewal and redetermination processes and also to suspend Payment Error Rate Measurement (PERM) reviews.
A Biden Administration could issue guidance to encourage states to take up existing options to support coverage. Such options include removing the 5-year coverage ban for recent pregnant women or children immigrants, using presumptive eligibility for one or more groups to expedite enrollment in Medicaid or CHIP, providing 12-month continuous eligibility to children in Medicaid or CHIP, and taking into account reasonably predictable changes in income when determining eligibility. In addition, states can adopt processes to improve communications with enrollees such as taking proactive steps to update enrollee address information and following up on returned mail by calling and/or sending email or text notifications. Many of these options could play an even more significant role as states resume renewals and redeterminations post PHE.
A Biden Administration can reverse current policies that impose enrollment barriers making it more difficult for those who are eligible for Medicaid to maintain coverage. While current rules require states to act when enrollees report a change in circumstances that may affect their continued eligibility, the Trump Administration has encouraged use of periodic eligibility checks as a program integrity strategy and has encouraged states to conduct enhanced eligibility verification and more closely monitor changes in enrollee circumstances. While such measures were encouraged to reduce instances of ineligible people being enrolled in the program and other eligibility errors, they also have resulted in creating greater enrollment barriers for people who remain eligible for the program. Research and experience show that increased requirements associated with eligibility determinations and renewals can lead to decreases in coverage among eligible people due to difficulties completing administrative processes and providing documentation. Such policies were likely a factor contributing to declines in Medicaid enrollment prior to the pandemic.
The Biden Administration can reverse proposed changes to Supplemental Security Income (SSI) disability review rules, which could impact Medicaid eligibility for people with disabilities. The Trump Administration proposed changes to Social Security regulations that would increase the number and frequency of “continuing disability reviews” for children and adults who receive SSI benefits. SSI is federal cash assistance for people with low incomes, limited assets, and significant disabilities. SSI is an important Medicaid eligibility pathway for people with disabilities. Increasing the frequency of SSI continuing disability reviews could result in some enrollees losing Medicaid coverage for which they remain eligible, due to difficulty navigating the administrative process.
Expand Outreach Efforts
A Biden Administration can increase outreach and enrollment efforts for Medicaid and Marketplace coverage. Since taking office, the Trump Administration has dramatically reduced funding for federal marketplace Navigators that were created to provide outreach, education, and enrollment assistance to consumers eligible for Marketplace and Medicaid coverage and now requires that they be funded by the marketplaces. Compared to 2016, federal Navigator funding for FY 2020 was reduced by 84% on average. Outreach under the ACA was also reduced by 90%. A Biden Administration could restore federal spending for navigators and on marketing and outreach. The new administration could also provide funding to states for outreach and enrollment assistance in Medicaid. Recent analysis suggests that there is a shortage of consumer assistance resources, even as lack of knowledge of ACA coverage options among the public persists. With the coronavirus crisis causing record job losses, increased investment in outreach and enrollment assistance could ensure people losing their job-based health coverage understand other coverage options and can get needed help applying for and enrolling in other coverage.
Propose More Targeted Legislative Changes
Narrow legislative proposals could encourage states to adopt the ACA Medicaid expansion. If Congressional support for more sweeping health care proposals is lacking – including a public option that would cover poor adults in states that have not expanded Medicaid — the Biden Administration may consider more targeted legislative changes to Medicaid to encourage Medicaid expansion, such as legislation to allow 100% federal matching funds for states that newly adopt the expansion for a period of time. Under the ACA, states that adopted the Medicaid expansion received 100% federal matching funds for three years (from 2014-2016) and the match has gradually phased down to 90% where it remains. Without a change in the law, states that newly expand would be eligible for the 90% match rate for expansion coverage. Twelve states have not adopted the Medicaid expansion, leaving many poor adults in a coverage gap, not eligible for Medicaid or Marketplace subsidies.
Legislative proposals could focus on extending coverage for specific populations including postpartum women, those needing community based long-term care, those ready to transition out of the criminal justice system and recent immigrants. There has been bi-partisan support for legislation that would allow states to extend postpartum Medicaid coverage from the current 60 days to 12 months. Other targeted legislative bi-partisan legislative proposals include the Medicaid Reentry Act (included in the House passed COVID-relief package) would allow Medicaid to cover services for Medicaid beneficiaries who are incarcerated during the 30 days preceding their release from prison or jail which could facilitate coverage and access post-release. The Health and Economic Recovery Omnibus Emergency Solutions (HEROES) Act also includes a provision offering states a time-limited 10% enhanced FMAP for activities to increase HCBS during and after the PHE period ends, including increasing the number of individuals receiving HCBS. Finally, the Biden Administration could work with Congress to allow states the options to allow coverage for recent immigrants (eliminating the 5 year coverage bar) for groups other than pregnant women and children.
Additional fiscal relief can bolster states’ ability to support and sustain increases in Medicaid coverage. President-elect Biden has indicated support for further increasing the FMAP and may try to work with Congress to enact legislation though Republican leaders have generally been opposed to substantial increases in state and local assistance during the pandemic and economic crisis. The Medicaid and CHIP Payment and Access Commission (MACPAC) at the December 2020 meeting announced moving toward a recommendation calling for an automatic Medicaid countercyclical financing model based on earlier recommendations from the General Accountability Office (GAO). The HEROES Act passed by the House in May and then updated and passed again in October would increase the enhanced FMAP to 14% effective through September 2021 to support states as the COVID-19 pandemic continues providing states with an estimated $55.5 billion in federal support according to the Congressional Budget Office. Congress could also consider alternative options to target the relief to states experiencing higher enrollment increases. However, it remains unclear if Congress will provide additional relief through the FMAP or if they will revisit the MOE requirements as part of another coronavirus relief package.
Here’s our recap of the past week in the coronavirus pandemic from our tracking, policy analysis, polling, and journalism.
The U.S. surpassed 17.2 million total cases this week, and set records on three days this week for the highest number of new cases and deaths daily during the pandemic. This is all as the Pfizer COVID-19 vaccine began distribution across the country and an independent advisory panel recommended that the Food and Drug Administration move forward with emergency authorization for the Moderna COVID-19 vaccine.
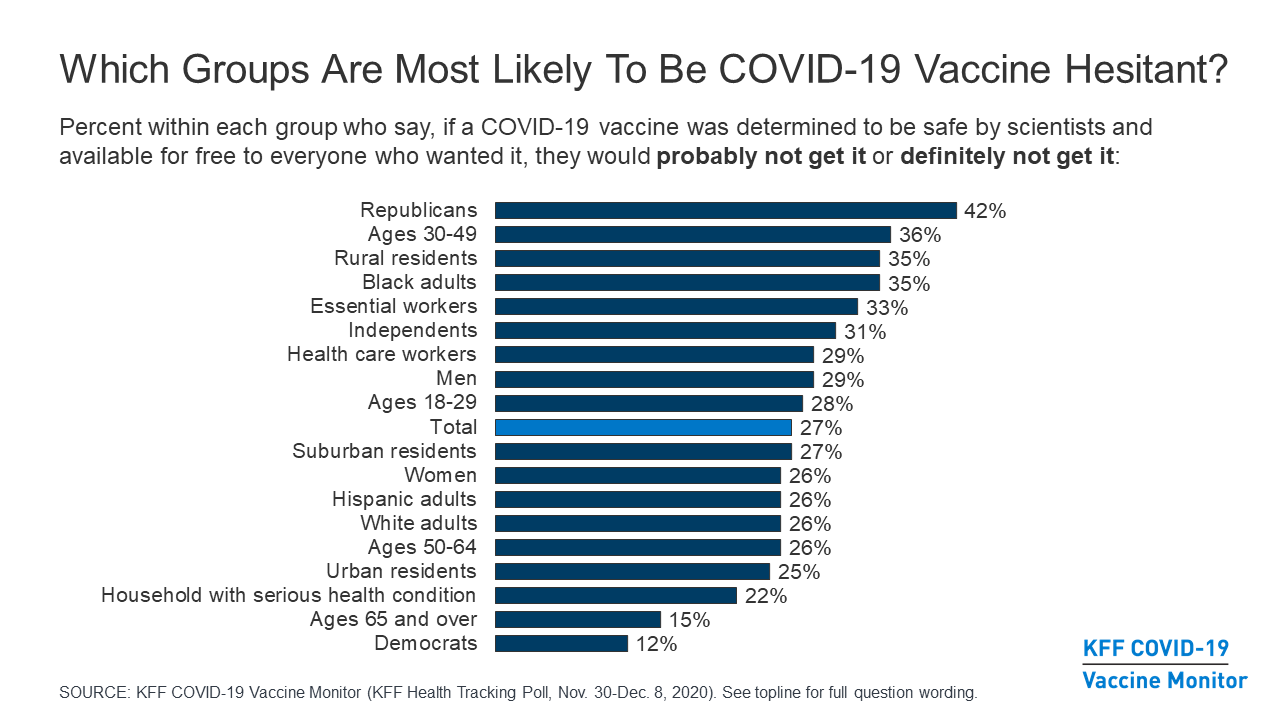
This week at KFF, we launched the COVID-19 Vaccine Monitor to track the public’s confidence in the vaccine and experiences for the duration of the pandemic. The first data from the project shows Americans’ enthusiasm for getting a COVID-19 vaccination varies substantially across groups, with Republicans and Black Americans among those most hesitant.
KFF President Drew Altman reviewed the new data to assess where the country stands. He finds reasons for optimism in his latest column.
Meanwhile, this month’s health tracking poll finds large majorities now say they wear masks every time they leave the house and can continue social distancing for at least six months if needed, with differences by partisan affiliation.
KFF analysts’ review of the latest releases and statements from state officials finds most states are following the Centers for Disease Control and Prevention’s (CDC) Advisory Committee on Immunization Practices’ (ACIP) recommendations for who qualifies as the highest priority group (health care workers and long-term care residents). Some states, though, are choosing to start with one of the populations in the first weeks as they await more supply. Most states are still developing plans for their later priorities, but according to our review several already differ from what the CDC is likely to recommend.
In a new brief KFF experts highlight the laws and regulations that are in place to ensure access to free COVID-19 vaccines for individuals regardless of their insurance status and explain how vaccine administration costs will be covered in private insurance, Medicare and Medicaid, and for the uninsured.
As the year winds down, KHN and Politifact’s Health Check on the collection of claims downplaying and denying of the coronavirus was chosen as the lie of the year. This comes as the nation has posted new daily records in cases and deaths and available hospital intensive care unit beds are in short supply.
Here are the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: Total cases worldwide reached 75 million this week – with an increase of nearly 4.5 million new confirmed cases in the past seven days. There were approximately 80,100 new confirmed deaths worldwide, bringing the total for confirmed deaths to nearly 1.7 million.
U.S. Cases and Deaths: Total confirmed cases in the U.S. passed 17.2 million this week. There was an increase of over 1.5 million confirmed cases between Dec. 11 and 17. Approximately 18,400 confirmed deaths in the past week brought the total in the United States to 310,700.
Who Didn’t Get a Second Shingrix Shot? Implications for Multidose COVID-19 Vaccines (Issue Brief)
Delivering HIV Care and Prevention in the COVID Era: A National Survey of Ryan White Providers (Issue Brief)
How Might Internet Connectivity Affect Health Care Access? (Chart Collection)
Updated: Coronavirus Puts a Spotlight on Paid Leave Policies (Issue Brief)
KFF Health Tracking Poll – December 2020: COVID-19 and Biden’s Health Care Agenda (News Release, Poll Findings)
Gaps in Cost Sharing Protections for COVID-19 Testing and Treatment Could Spark Public Concerns About COVID-19 Vaccine Costs (News Release, Issue Brief)
Updated: COVID-19 Coronavirus Tracker – Updated as of December 18 (Interactive)
Updated: State Data and Policy Actions to Address Coronavirus (Interactive)
U.N. SG Guterres Warns Against ‘Vaccinationalism,’ Spread Of Misinformation On COVID-19 In Address, Remarks In Germany (KFF Daily Global Health Policy Report)