Recent Efforts to Extend Medicaid Postpartum Coverage and What to Watch Looking Ahead
Medicaid is a key source of coverage for low-income pregnant people in the United States, covering more than four in ten births nationally, but many people who qualify for Medicaid because they are pregnant lose that coverage 60 days postpartum, especially if they live in a state that has not expanded Medicaid. In recent years there has been a growing interest among state and federal policymakers in extending Medicaid postpartum coverage beyond the 60-day mark to help address racial disparities and improve maternal and infant health. Earlier this year, federal legislation was enacted that gives states a temporary option to extend postpartum coverage beyond 60 days, and Congress is currently considering additional legislation to require such extended coverage.
Federal law requires that all states cover pregnant individuals with incomes at least up to 138% of the federal poverty level (FPL), although many states have set higher income eligibility levels, and they must extend coverage for 60-days postpartum. Some people lose that coverage after the postpartum period because they have no eligibility pathway even though they have incomes below the federal poverty level. Following the 60-day postpartum period, in states that have adopted the Affordable Care Act (ACA)’s Medicaid expansion, individuals with incomes below 138% FPL have a continued pathway to Medicaid coverage and those with higher incomes may qualify for subsidized coverage through the ACA marketplace plans; however, individuals in non-expansion states may become uninsured because Medicaid eligibility levels for parents are much lower than for pregnant people. For example, in Alabama, which has not sought a postpartum coverage extension, the Medicaid eligibility level for parents is 18% FPL, which is approximately $4,000/year for a family of three.
The federal American Rescue Plan Act (ARPA) enacted in March 2021 gives states the option to extend postpartum coverage to pregnant individuals to a full year. The coverage option is available for five years starting on April 1, 2022 and states must provide a full scope of benefits without limitations on coverage during the extension. Prior to ARPA’s enactment, states had to seek permission from the Centers for Medicare and Medicaid Services (CMS) by applying for a Section 1115 waiver to extend the postpartum period beyond 60 days, although none of these applications were approved until April 2021. Even though the new option under ARPA will not be effective until April 2022, postpartum coverage has been continuous since the start of the coronavirus pandemic because Medicaid disenrollment has been suspended during the public health emergency.
Largely in response to the new federal option, at least 25 states have taken steps to extend Medicaid postpartum coverage. To date, most of these are expansion states, but actions in non-expansion states will ensure continued coverage following the current postpartum period. Prior to the enactment of ARPA, California and Texas had limited state-funded postpartum coverage in place and a few states had submitted waivers to CMS to extend postpartum coverage through Medicaid, although, in some cases, targeted to narrow groups, such as those with a diagnosed substance use disorder, or for less than 12 months. States often seek approval of a demonstration waiver to do something they cannot do under current law. A few states are still seeking waivers to implement prior to April 2022 or to extend postpartum coverage in ways more limited than the new ARPA option.
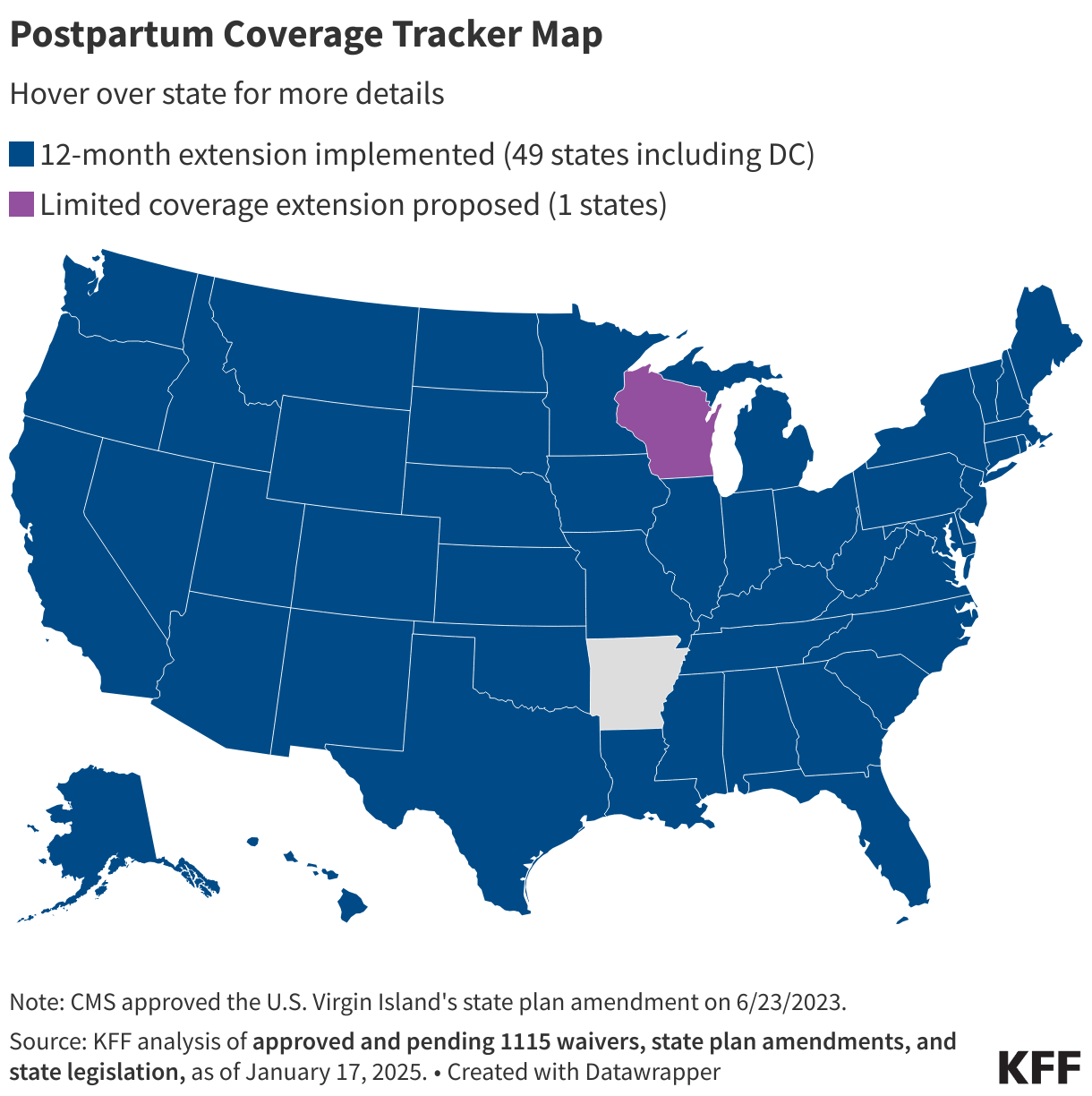
Recent state actions to extend postpartum coverage for 12 months include:
- Thirteen states (California, Colorado, Connecticut, DC, Maine, Maryland, Minnesota, New Jersey, Ohio, South Carolina, Tennessee, Washington, and West Virginia) enacted legislation, a first step to implementing a coverage extension;
- New York and North Carolina are debating proposed legislation;
- Two states (Indiana and Pennsylvania) announced plans to adopt the new option using existing authority; and
- Illinois received approval to extend postpartum coverage for 12 months through a waiver (waivers are pending in three states—Florida, Massachusetts, and Virginia).
Although recent federal action has prompted many states to consider extending postpartum coverage, some states still won’t have a pathway for coverage beyond the current 60-day postpartum period, and Congress is currently considering proposals to require such coverage. Uneven adoption of the ARPA option means postpartum individuals in many states remain at risk of losing Medicaid coverage just two months after giving birth. Postpartum people with household incomes below the poverty level in non-expansion states often do not have another coverage option and become uninsured when they lose Medicaid coverage. Currently, Congress is considering a provision in the Build Back Better Act that would require all states to extend Medicaid postpartum coverage from 60 days to 12 months, ensuring continuity of Medicaid coverage for postpartum individuals in all states to more broadly reduce disparities and improve maternal and infant health outcomes. However, there is a push to lower the overall amount of spending in the package, and the extension of postpartum coverage could be forced to compete against other priorities.
To track updated state-by-state activity on Medicaid postpartum coverage, please visit our Medicaid Postpartum Coverage Extension Tracker.