Key Findings
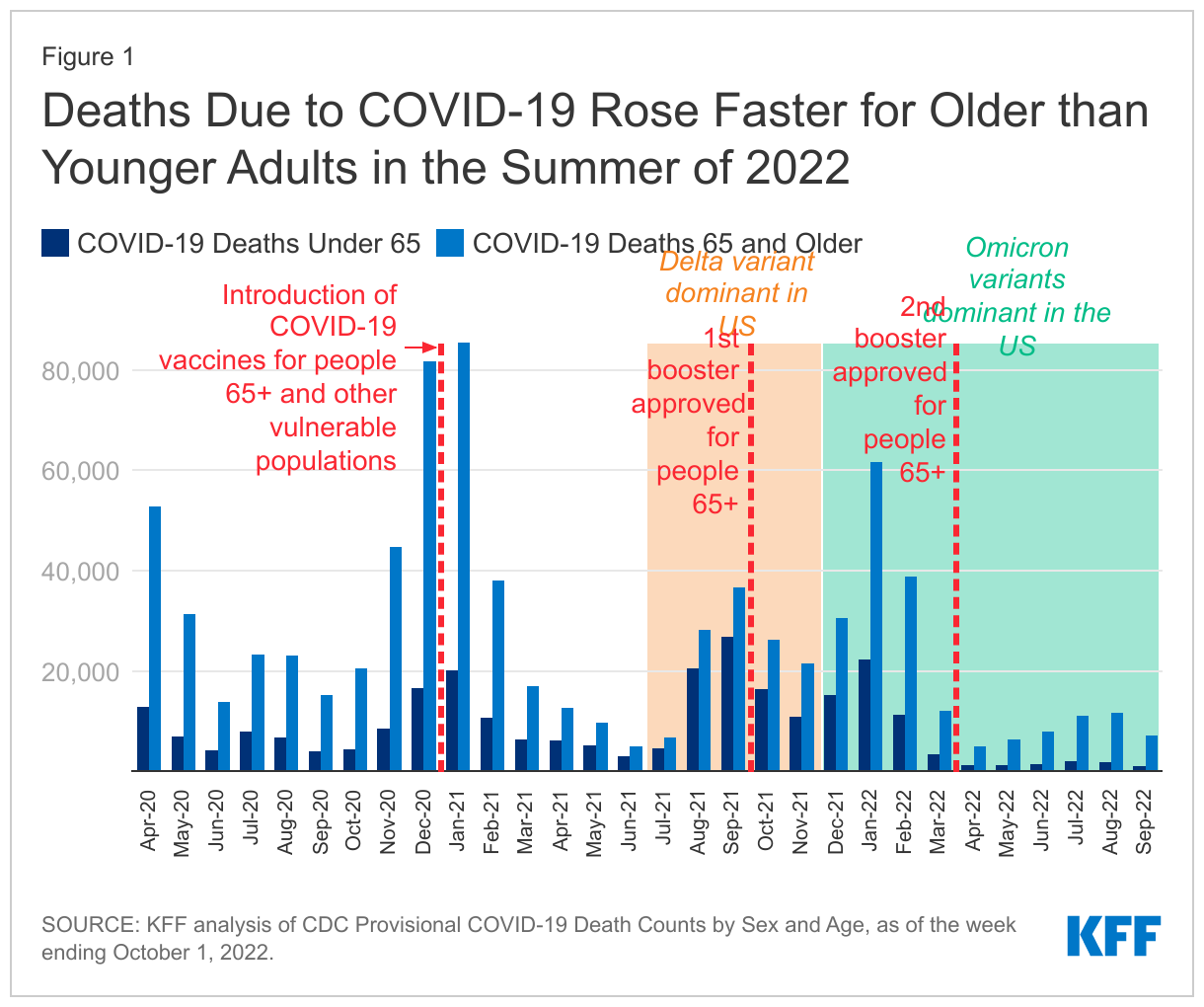
- In the upcoming midterm elections, many races will be decided by marginal changes in turnout with a few voters making a difference. The latest KFF Health Tracking Poll examines what health care issues may be motivating small groups of voters that could shift some key races. Abortion access and reproductive health is motivating majorities of Democratic women, women of reproductive age, and Democratic and Democratic-leaning voters in states where abortion is currently illegal. This is also the issue that these voters want to hear candidates talk about during the next month of the campaign. Moreover, state action on abortion seems to be a particularly motivating issue for Democrats in states that have a full abortion ban. The other health care issue that is resonating with a group of voters – older voters – is reducing the cost of prescription drugs for people with Medicare. Majorities of voters ages 65 and older say they are more likely to vote for a candidate who supports the Inflation Reduction Act provisions aimed at capping costs and allowing the federal government to negotiate prices for people with Medicare. These provisions were also motivating, to a lesser extent, Republican voters.
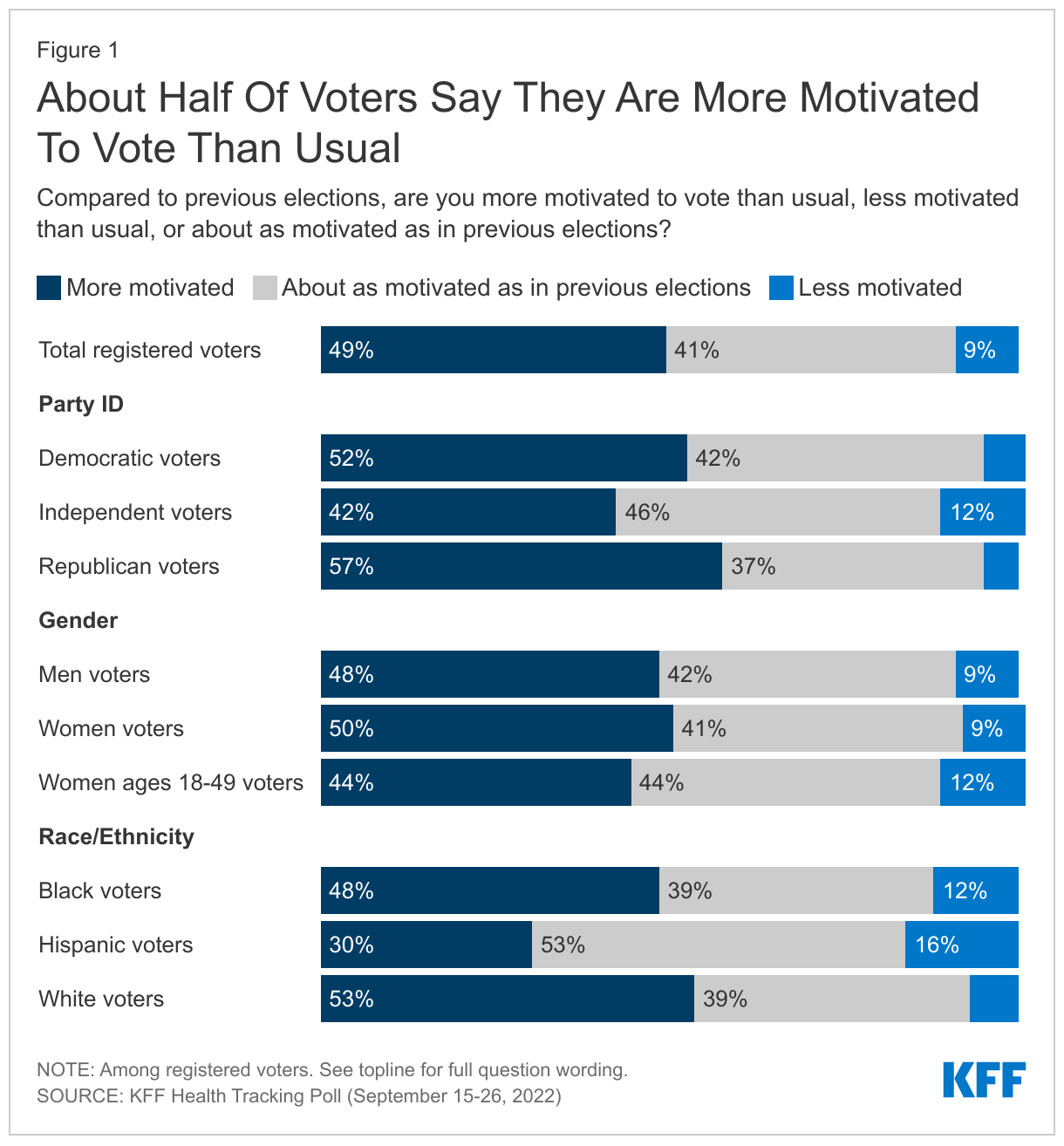
- With about a month before the 2022 midterm election, half of registered voters say they are more motivated to vote in this upcoming election compared with past elections. A single party doesn’t hold a distinct advantage – with more than half of both Republican and Democratic voters saying they are more motivated – but the issues motivating each group of voters differ. When asked to say in their own words why they are more motivated to vote now, the top issue provided by Republicans is the economy, while Democratic voters are more likely to offer abortion as their motivation for being more eager to vote. Independent voters are divided between the two issues. Large shares of voters also offer partisan reasons like keeping the other party out of office for the main reason why they are motivated to vote.
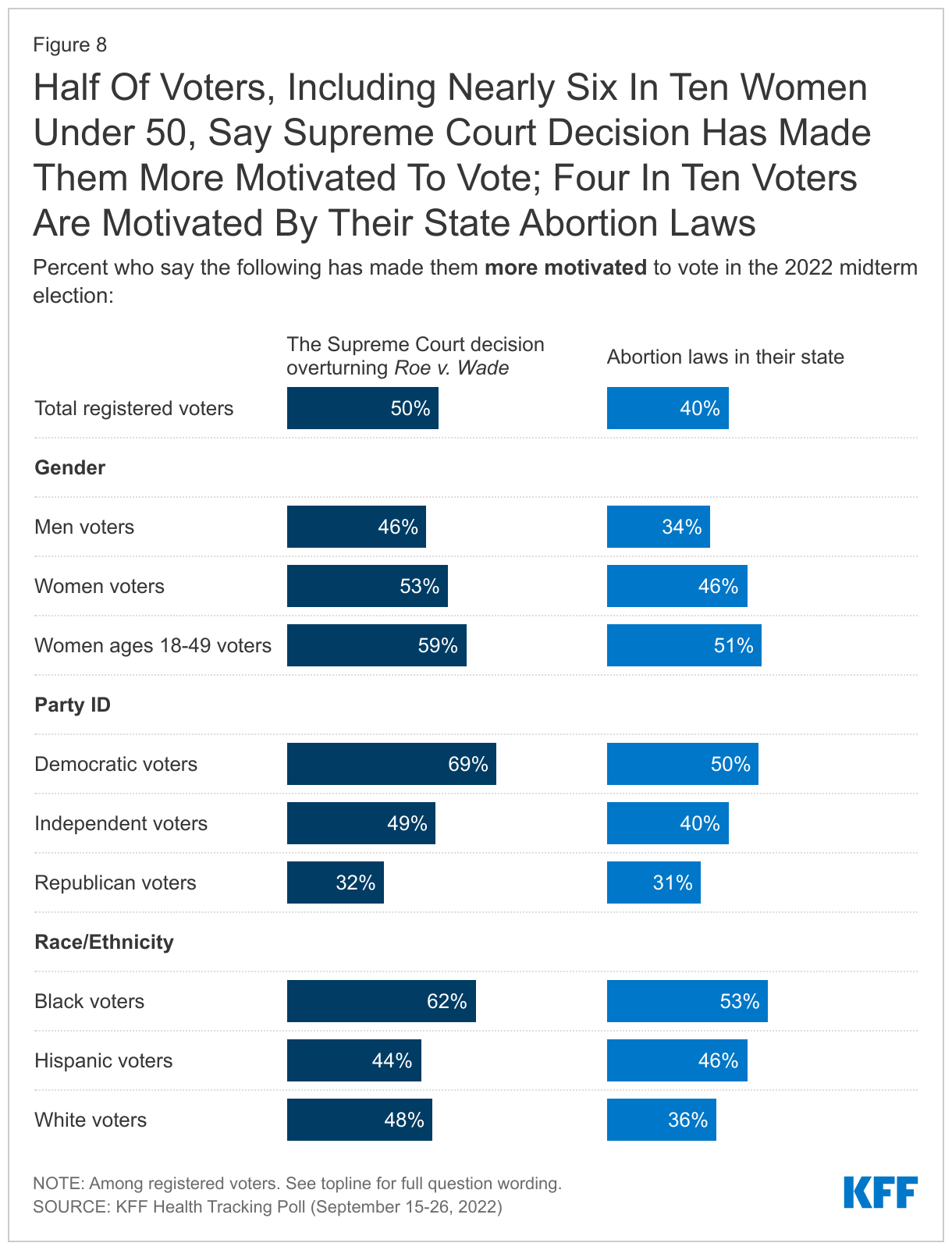
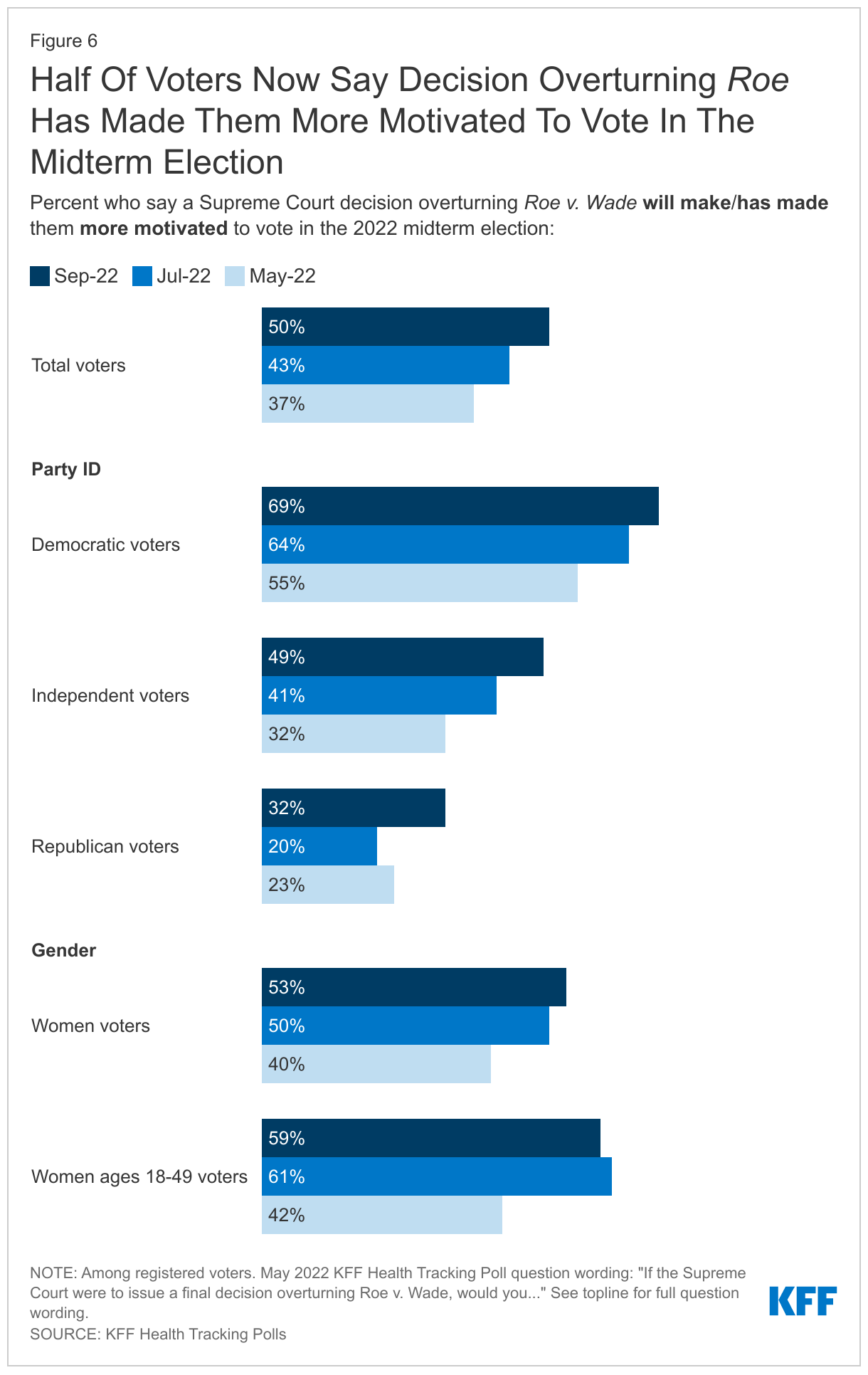
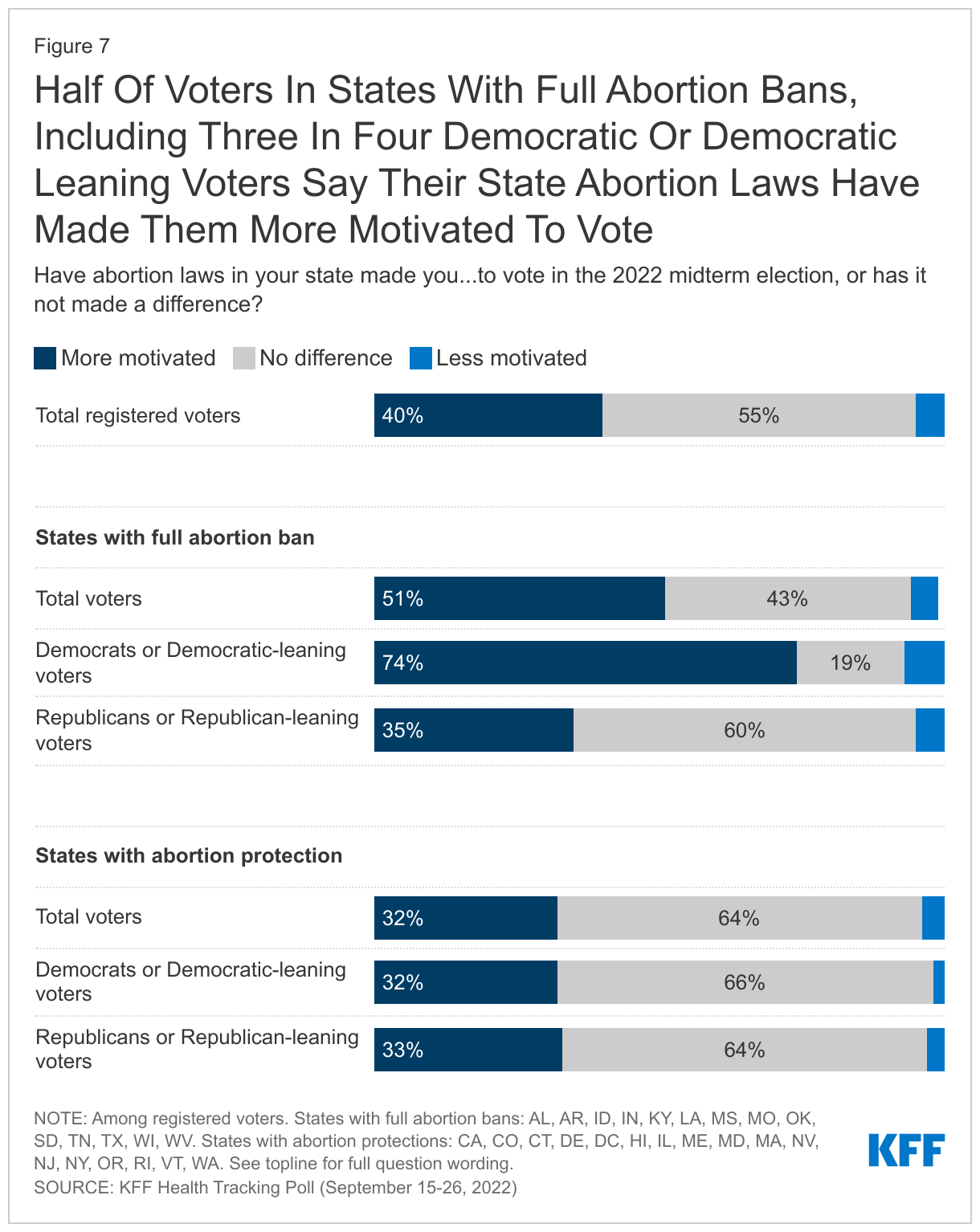
- The Supreme Court’s decision overturning Roe v. Wade is continuing to motivate some voters as half of voters (50%) now say the Court’s decision has made them more motivated to vote, up from 43% who said the same in July and an increase of 13 percentage points from a similar question in May. In addition, state actions on abortion are also motivating voters, particularly in the states where full abortion bans are now in place. Overall, four in ten voters say their state’s abortion laws have made them more motivated to vote, but this increases to 51% among voters living in states with full abortion bans. In addition, three in four Democratic or Democratic leaning independent voters (74%) living in states with full abortion bans in place say their state abortion laws have made them more motivated to vote.
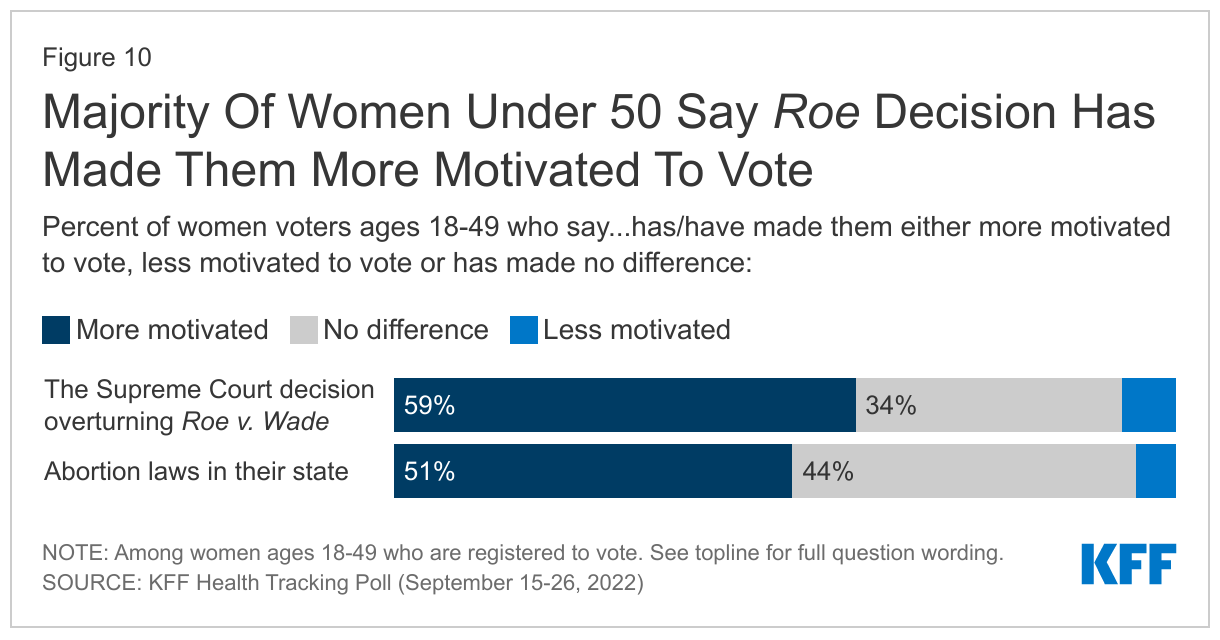
- The legality of abortion in the wake of the Dobbs decision also continues to resonate with women voters, ages 18 to 49. More than four in ten (44%) women voters, ages 18-49, say they are more motivated to vote this year compared to previous elections, and most of them (59%) say the Supreme Court decision overturning Roe v. Wade has made them more motivated to vote. In addition, when asked to say in their own words why they are more motivated to vote, one in seven of this group offers reasons related to the Supreme Court decision, such as the issue of abortion and reproductive rights (9%) and protecting women’s rights (4%).
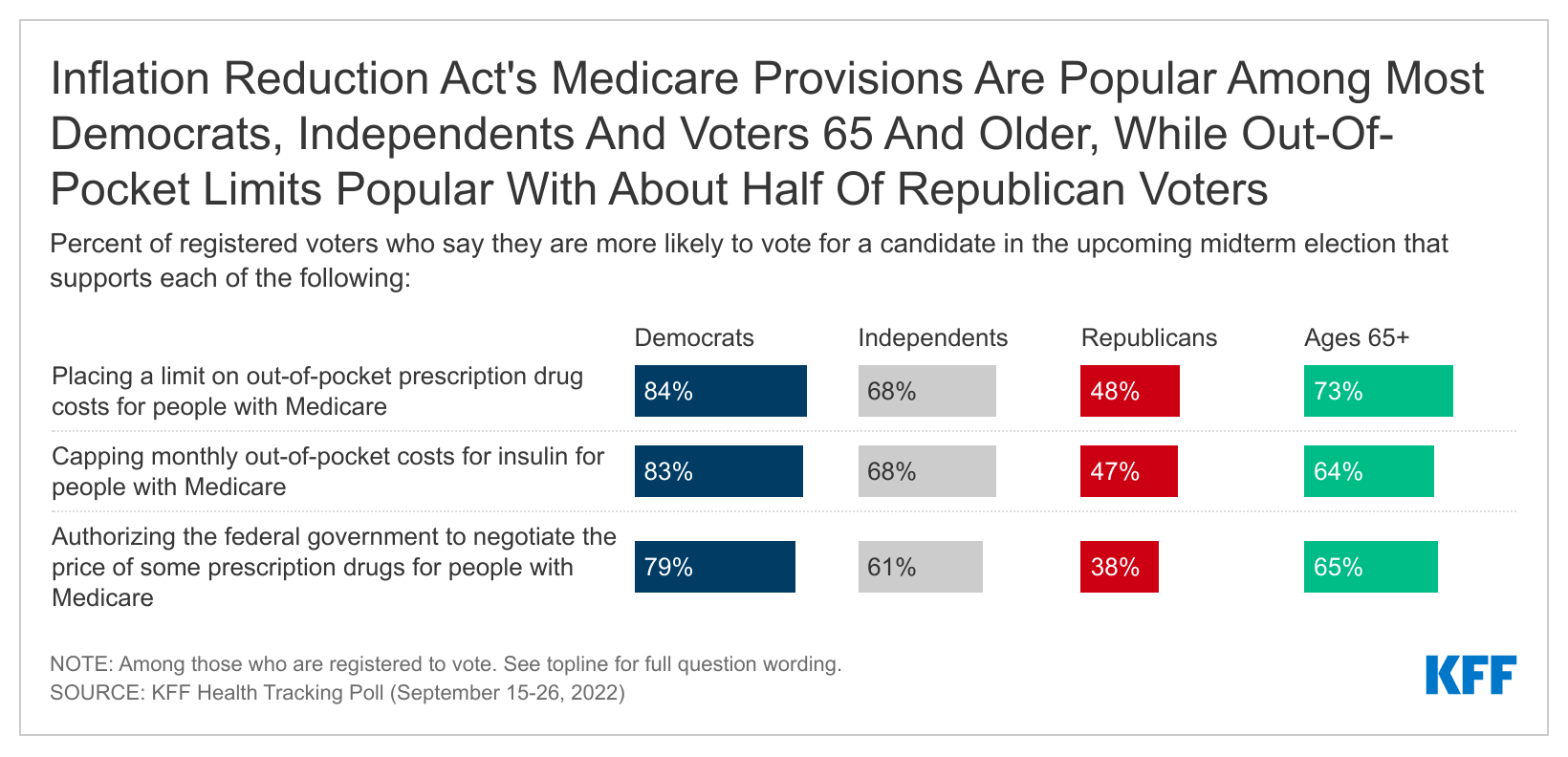
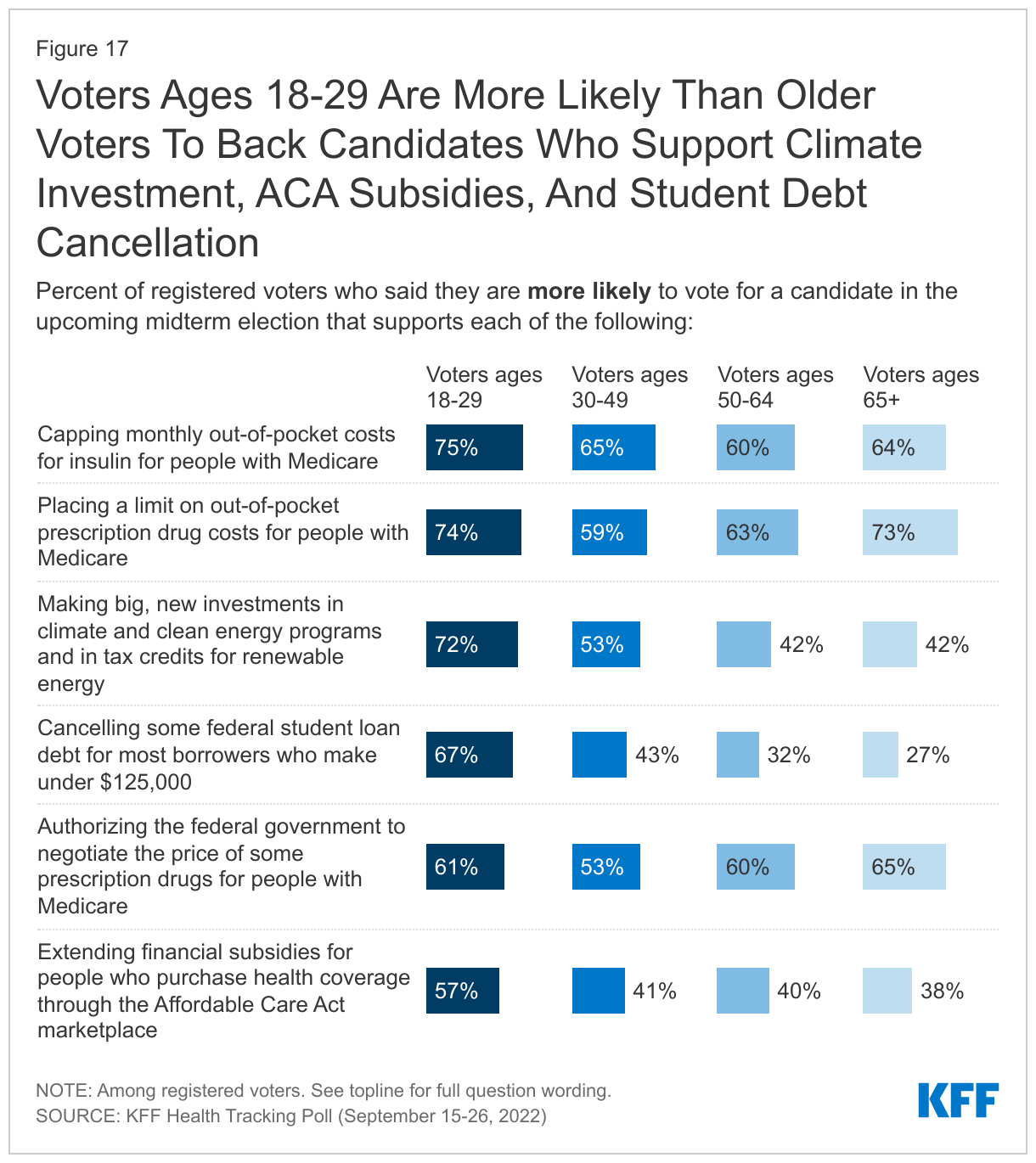
- With abortion dominating the issue of health care so far in the 2022 midterm election, the KFF Health Tracking Poll also examines whether the health care provisions in the Inflation Reduction Act are resonating with certain groups of voters. While adults are aware of some of the key health provisions that are included in the law, some of the provisions aimed at lowering the cost of prescription drugs for people with Medicare are resonating with some voters, including those ages 65 and older. About two-thirds of voters ages 65 and older say they are more likely to vote for a candidate who supports capping out-of-pocket costs for insulin for people with Medicare (64%) or authorizing the federal government to negotiate the price of some prescription drugs for people with Medicare (65%), and three-fourths of older voters (73%) say they are more likely to vote for a candidate who supports placing a limit on out-of-pocket drug costs for people with Medicare.
What Is Motivating Voters Ahead of the Midterm Elections?
With the upcoming midterm election only a month away, about half of registered voters (49%) say they are more motivated to vote compared to previous elections. About four in ten (41%) say they are about as motivated as they have been in past elections and one in ten (9%) say they are less motivated to vote. No party holds a motivation advantage at this point in the election with similar shares of Republican voters (57%) and Democratic voters (52%) saying they are motivated to vote. Older voters have historically had higher rates of voter turnout than younger voters and the 2022 midterm election looks to be no exception with nearly six in ten adults ages 65 and older say they are more motivated to vote, compared to slightly less than half of their younger counterparts.
Across racial and ethnic groups, Hispanic voters seem to have more tepid levels of motivation to vote in the 2022 midterm election. While about half of White voters (53%) and Black voters (48%) say they are more motivated to vote, just three in ten Hispanic voters (30%) say the same. Indeed, about one in six Hispanic voters (16%) say that compared to previous elections, they are less motivated to vote.
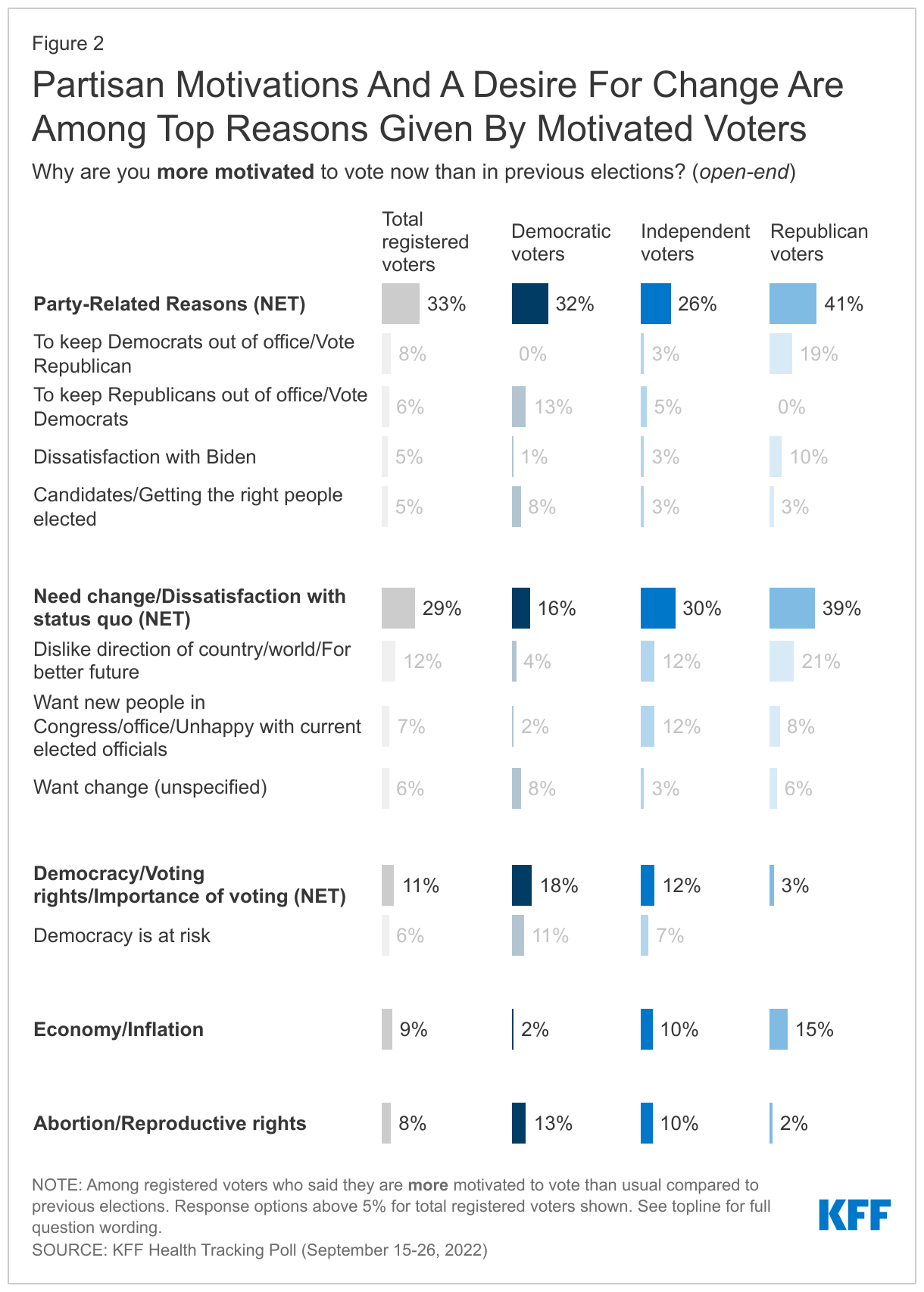
When motivated voters are asked to say in their own words why they are more motivated to vote now than in previous elections, about one in ten say they are more motivated to vote due to the economy and inflation (9%) and a similar share say their increased motivation is due to the issue abortion and reproductive rights (8%). However, reflecting the polarized state of politics in the nation, significant shares of more motivated voters give partisan reasons (33%) for their increased motivation to vote. About three in ten cite the desire for change (29%) and about one in ten motivated voters mention democracy, voting rights, and the importance of voting as a reason why they are more motivated to vote now than in previous elections.
The top issue provided by motivated Republican voters for their increased motivation is the economy (15%), while Democratic voters are more likely to offer abortion (13%) than the economy (2%) as the issue making them more eager to vote. Independent voters are divided between the two issues with similar shares offering the economy (10%) and abortion (10%) as their motivating issue. Unsurprisingly, partisanship also seems to be a key driver for both Republican and Democratic voters, with large shares of motivated voters from both parties citing party-related reasons for their increased motivation. Four in ten motivated Republicans (41%) give partisan reasons for their increased motivation including 19% who say they are more motivated to vote to either to keep Democrats out of office or to vote for Republicans, and an additional 10% mention dissatisfaction with President Biden. Among motivated Democratic voters, about a third (32%) name party-related reasons for their increased motivation, including 13% who mention wanting to keep Republicans out of office or wanting to vote for Democrats.
In Their Own Words: Why are you more motivated to vote now than in previous elections?
“We all need to vote blue. Abortion needs to be legal in all states.” – 72-year-old Democratic woman in Oregon
“Because women's rights are being threatened now more than ever and I'll be damned if I stand by and let it happen.” – 29-year-old Democratic woman in Alabama
“Personal Investments have plummeted, my grocery bill is astronomical, fuel cost is out of control, bail reform in NYS and criminals across the country are not being punished!” – 48-year-old Republican man in New York
“To vote out them Dems that are destroying the country.” – 58-year-old Republican woman in Connecticut
“To help protect women's rights.” – 40-year-old Democratic man in Georgia
Among voters who say they are less motivated to vote now compared to previous elections, 16% cite not believing in the election process as a reason why they are less motivated and similar shares mention disliking the candidates (15%) and not thinking their vote matters or will count (12%).
In Their Own Words: Why are you less motivated to vote now than in previous elections?
“Voting really does not matter. It is all rigged.” – 55-year-old Republican woman in Minnesota
“Because I don't believe in the promises that the candidates are making.” – 44-year-old Democratic woman in New York
“The candidates are all disappointing. No matter who is in office they all work for the same government. Things are getting worse and worse”. – 49-year-old Democratic woman in Texas
“I don't believe in either side anymore. I am through with politics.” – 61-year-old independent man in California
“Because our votes don't matter.” – 37-year-old Republican man in Kansas
“I would never vote republican but I'm not always happy to vote democrat.” – 24-year-old Democratic man in Texas
The Top Issues For Voters
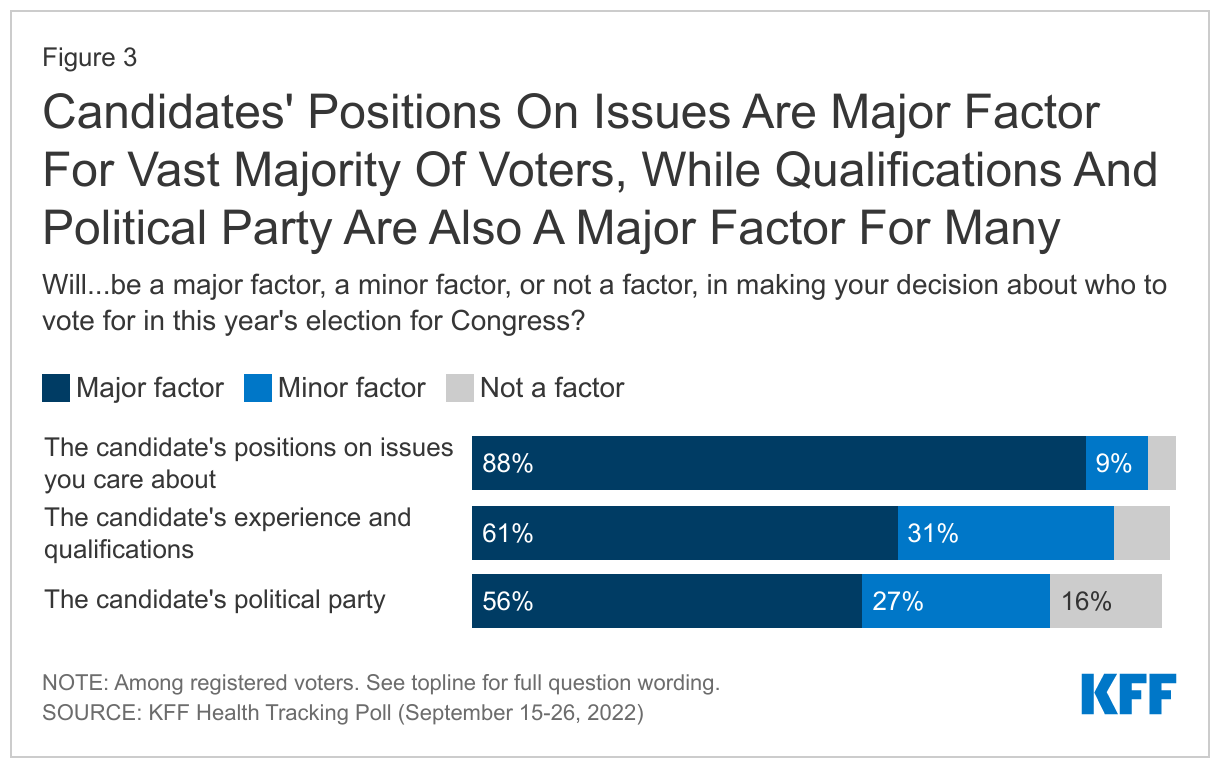
An overwhelming majority (88%) of voters say that a candidate’s positions on issues they care about will be a “major factor” in deciding how they vote for Congress this year, highlighting the importance of how candidates talk about the top issues for voters over the next few weeks. Most voters also say the candidate’s experience (61%) and political party (56%) is a “major factor” in their voting decision.
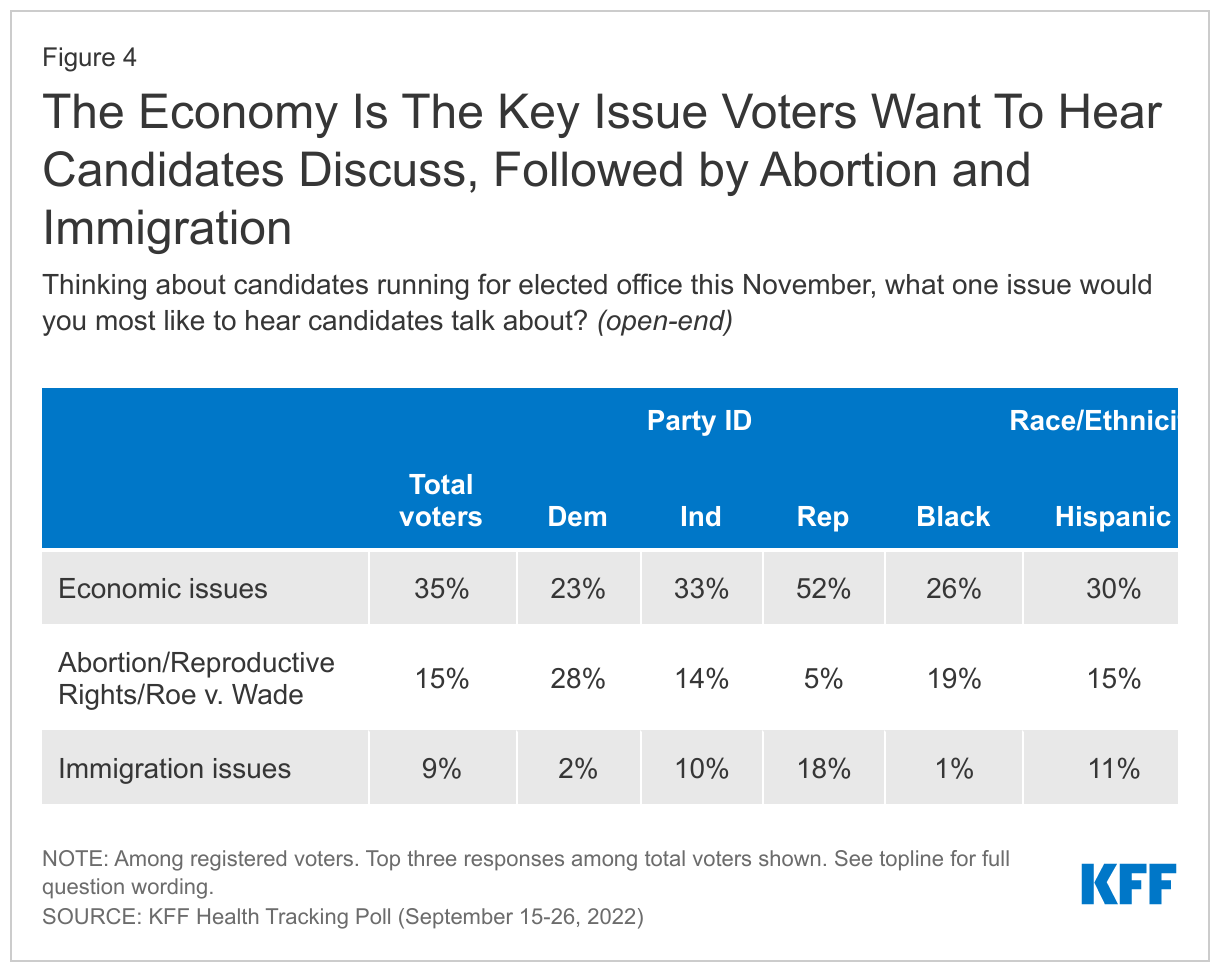
Given the overwhelming majority of voters who say a candidate’s positions on issues will be major factor in their vote, the latest KFF Health Tracking poll asked voters to name in their own words the one issue they would most like to hear candidates talk about. Economic issues, including inflation, emerge as the key issue ahead of the November midterm election with 35% of voters saying that is what they want to hear candidates talk about. Beyond economic issues, notable shares of voters say they would like to hear candidates talk about abortion, Roe v. Wade, and reproductive rights (15%), and about immigration (9%).
Across partisans, the economy is clearly the top issue for Republicans and for independents. Half of Republican voters (52%) and one-third of independent voters say they want to hear candidates talk about economic issues, including inflation. Immigration is the second most mentioned issue by Republican voters (18%) whereas among independent voters, 14% say they want candidates to discuss abortion and reproductive rights, while one in ten (10%) want to hear about immigration. Democratic voters are somewhat divided on what they want to hear candidates discuss, with nearly three in ten (28%) who say they want to hear about abortion and reproductive rights, while a quarter of Democratic voters (23%) want to hear about candidates talk about the economy.
The economy also stands as the most prominent issue across racial and ethnic groups with nearly four in ten White voters (39%), three in ten Hispanic voters (30%), and a quarter of Black voters (26%) saying they want to hear candidates talk about economic issues ahead of the election. However, abortion also emerges as a key issue, particularly for Black voters as nearly one in five say they want to hear candidates talk about it.
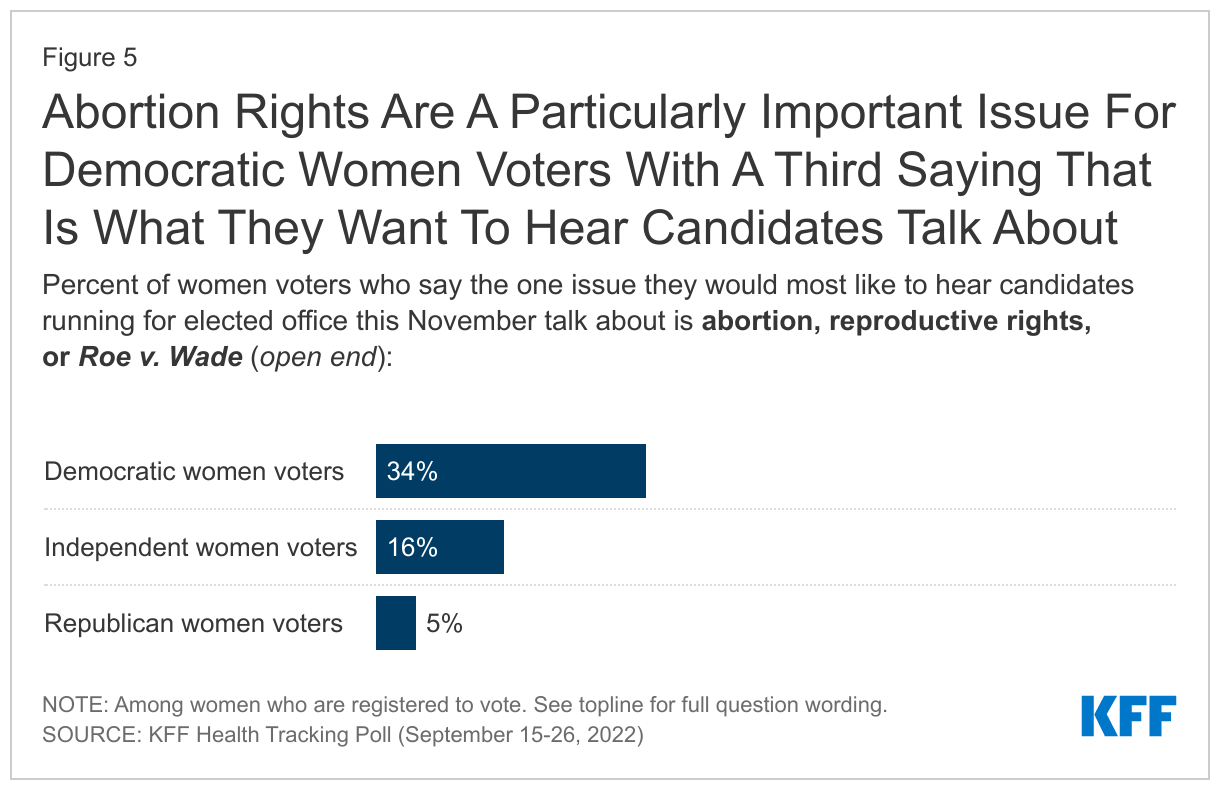
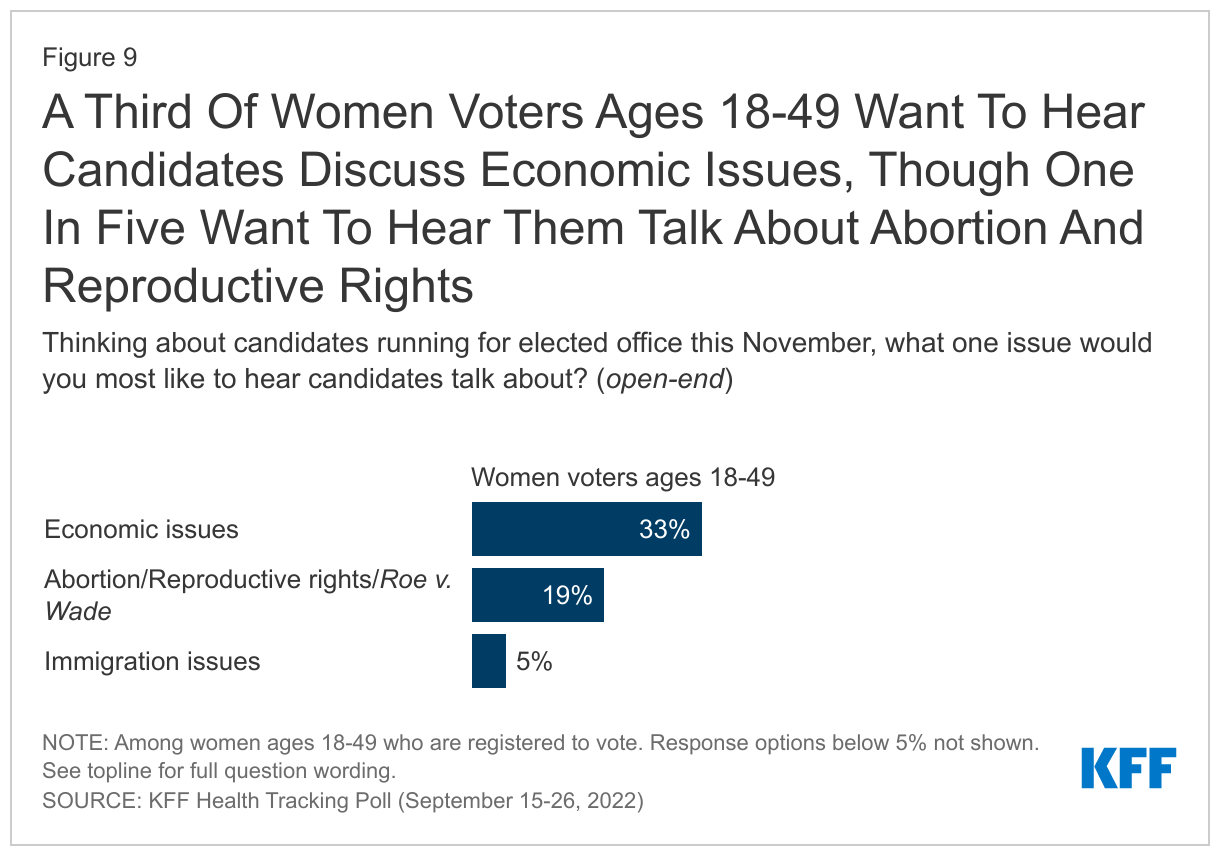
Women voters are more likely than men to say they want to hear the candidates discuss abortion, reproductive rights and Roe v. Wade (19% vs. 11%), though the economy is the top issue for both groups (34% and 37% respectively). Abortion rights are particulalrly important among Democratic women – a third of Democratic women (34%) say they want to hear candidates talk about abortion, more than twice the share of independent women (16%) and nearly seven times the share of Republican women (5%) who say the same.
How Changes In Abortion Policies Are Motivating Midterm Voters
In the wake of the Dobbs decision overturning Roe v. Wade and a number of states taking legislative action to restrict abortion, the latest KFF poll finds that half of voters (50%) say the Supreme Court’s decision has made them more motivated to vote, up from 43% who said the same in July and an increase of 13 percentage points from a similar question in May, before the Court had issued its decision but after a draft of the forthcoming decision was leaked. A majority of women voters, ages 18 to 49, (59%) continue to say the Supreme Court decision overturning Roe v. Wade has made them more motivated to vote, relatively unchanged from the July KFF poll.
The Dobbs decision seems to be motivating voters who want to vote for candidates who support abortion access more than those voters who want candidates to limit access. Voters who say they are more motivated to vote in this election compared to previous ones are about twice as likely to say they plan on voting for candidates who want to protect access to abortion (58%) than for candidate who want to limit abortion access (27%).
In addition, among those who say the Supreme Court decision itself has made them more motivated, three in four (76%) say they plan on voting for candidates who want to protect access to abortion compared to 17% who say they plan on voting for candidates who want to limit abortion access.
Similarly, with abortion laws being determined at the state level, many voters (40%) say their state’s abortion laws have made them more motivated to vote in the 2022 midterm election. Notably, voters in states with an abortion ban1 in place (51%) are more likely than those in states with protections for abortion access (32%) to say their state abortion laws have made them more motivated to vote. State abortion bans appear to be particularly motivating for Democrats as three in four Democratic or Democratic-leaning voters in states that have full abortion bans say their state abortion laws have made them more motivated to vote in the midterm election.
On both, the Supreme Court decision and recent state actions, larger shares of Democratic voters say each has made them more motivated to vote than Republican voters. Similarly, Black voters are more likely than their White counterparts to say both Supreme Court’s decision and their state abortion laws have made them more motivated to vote. About half of women voters say the Court’s decision overturning Roe (53%) and their state abortion laws (46%) have increased their motivation to vote. Notably, Republican women voters are somewhat more likely than their Republican male counterparts to say the abortion laws in their state have made them more motivated to vote (36% vs. 24%), though half of both Republican women (50%) and men (50%) say they plan to vote for candidates who want to limit access to abortion.
How The Dobbs Decision Is Motivating Women Voters Of Reproductive Age
KFF polling from July 2022 found that more than seven in ten women voters under the age of 50 said the issue of abortion access would be very important in making their decision about who to vote for in the midterm election. The latest KFF Health Tracking poll finds that large shares of women voters under 50 remain more motivated to vote due to the Supreme Court’s decision overturning Roe v. Wade, and that most are planning to vote for candidates who will protect abortion access.
Several months since the Supreme Court overturned Roe, the issue of reproductive rights remains salient for women voters ages 18 to 49, the group most directly impacted by the Court’s decision. While a third of women voters under age 50 say they want to hear candidates discuss economic issues, one in five (19%) say the issues they most want to hear them talk about are abortion, reproductive rights, and Roe v. Wade.
Overall, 44% of women voters under age 50 say, compared to previous elections, they are more motivated to vote in November. The issue of abortion and reproductive rights resonated with these younger women voters as about six in ten women voters ages 18 to 49 (59%) say the Supreme Court decision overturning Roe v. Wade has made them more motivated to vote, and half (51%) say their state abortion laws have increased their motivation to go to the polls.
Similar to overall voters who say they are motivated by the Dobbs decision, women voters 18 to 49 who are now more motivated to vote also are more likely to vote for candidates who support abortion access. Eight in ten women voters 18-49 who say they are more motivated to vote because of the Supreme Court decision on Roe say they will vote for a candidate who wants to support abortion access (79%).
State Abortion Restrictions
Following the Dobbs decision, fourteen states now have full bans on abortion. For the latest breakdown of key facts about abortion access in the U.S., see the KFF Abortion in The U.S. Dashboard.
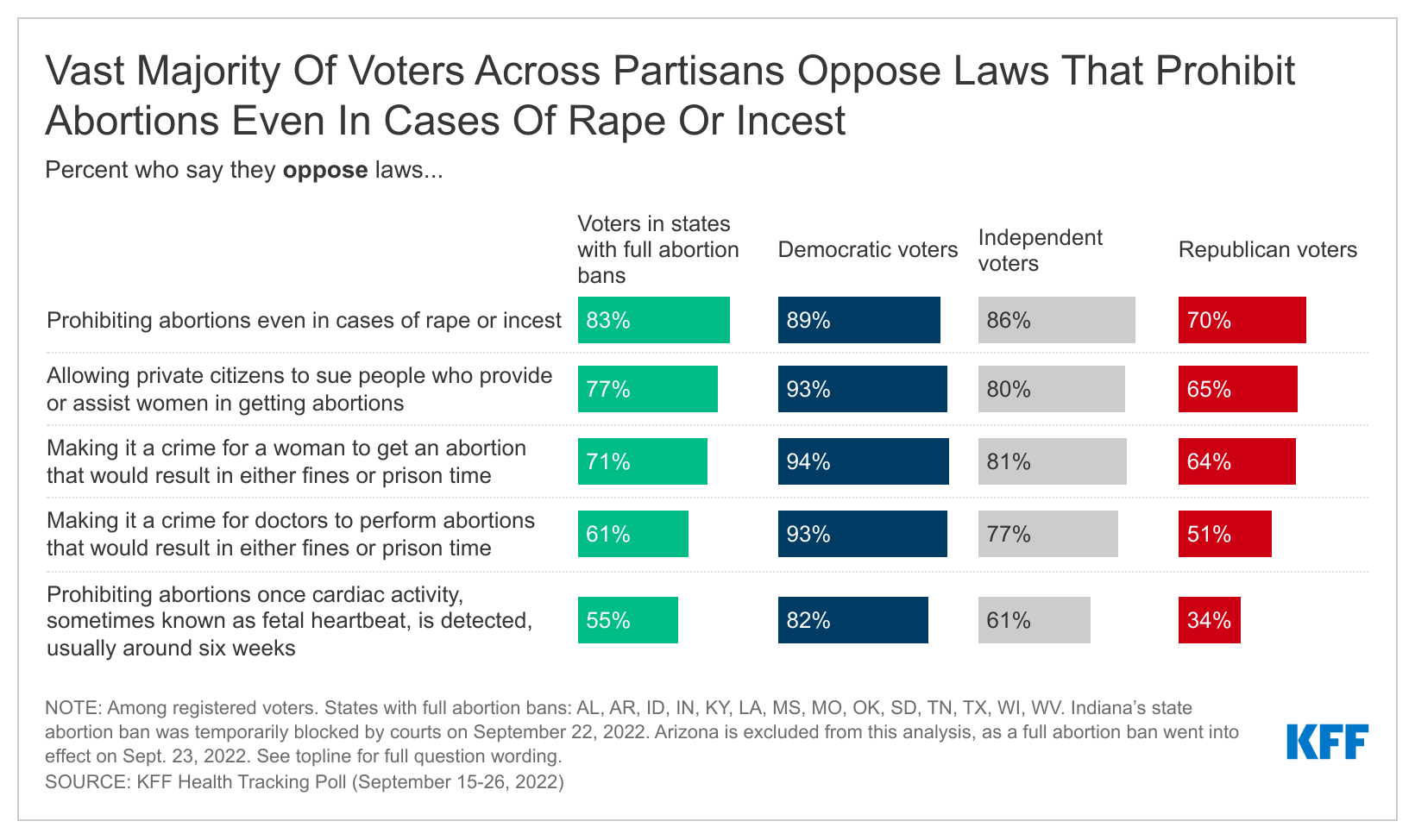
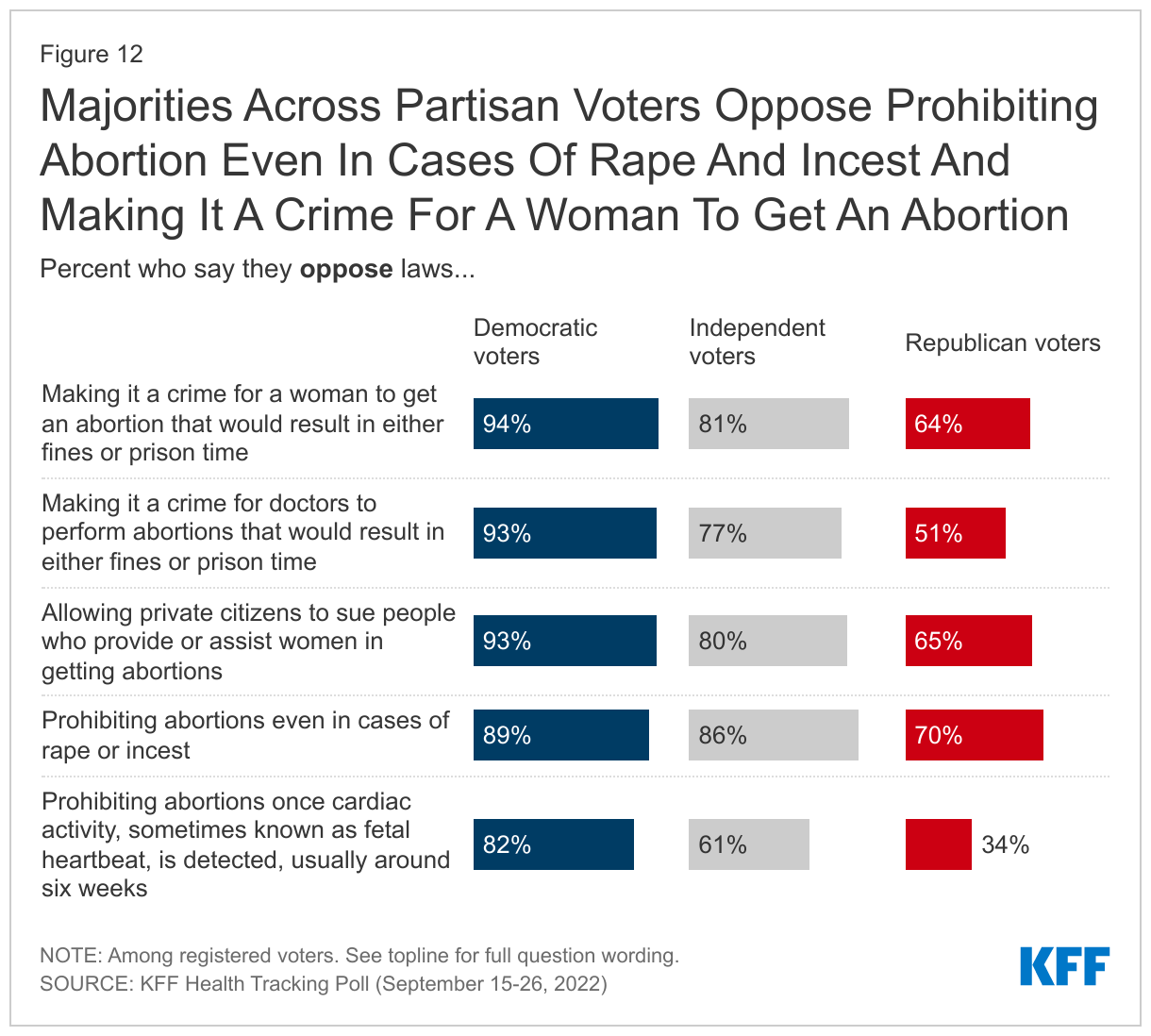
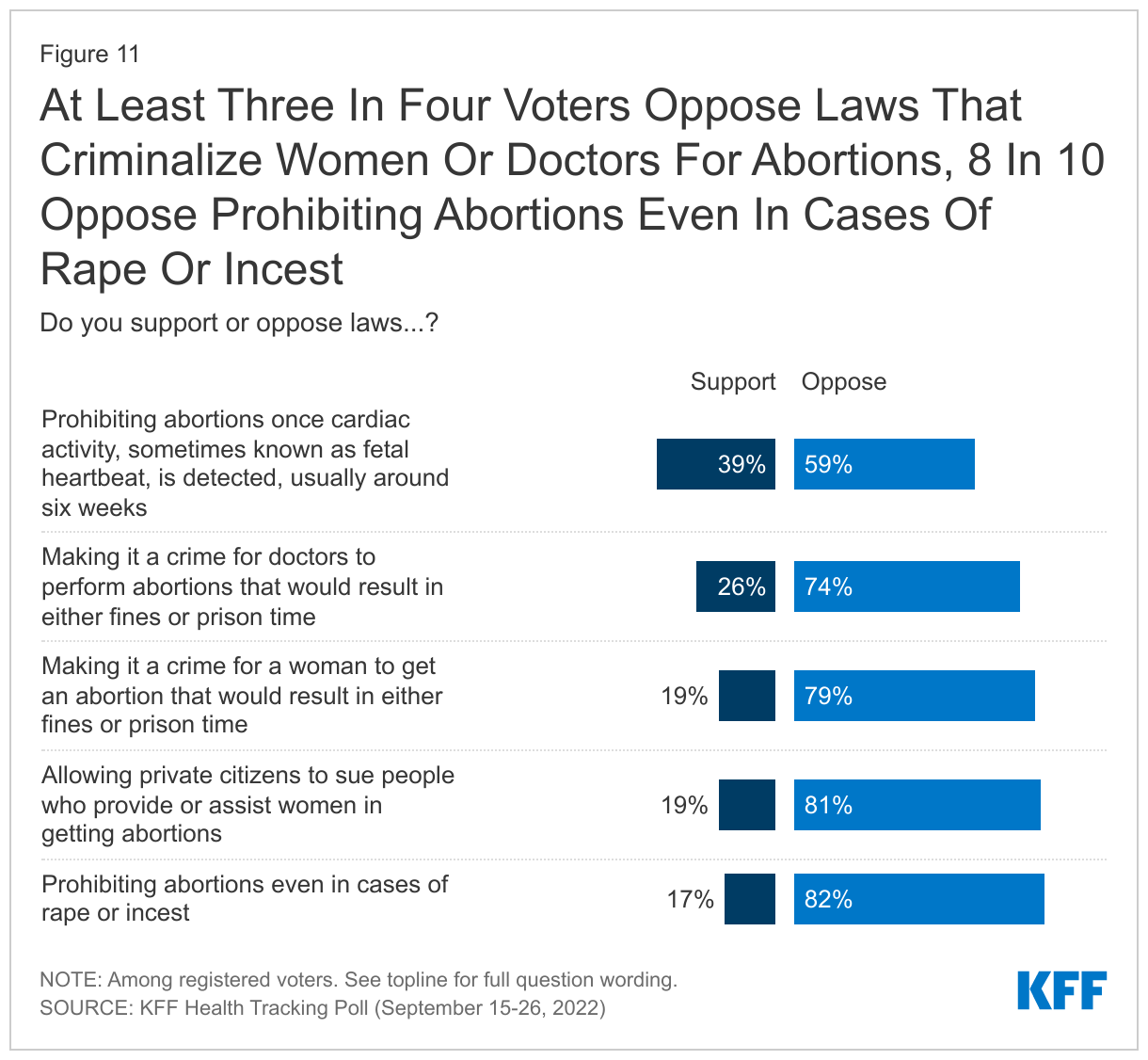
Most voters remain opposed to punitive abortion restrictions, with more than seven in ten voters opposed to making it a crime for doctors to perform abortions (74%) or for women to get abortions (79%) or allowing private citizens to sue people who provide or assist in abortions (81%). Six in ten voters (59%) oppose prohibiting abortions after a fetal heartbeat is detected and eight in ten (82%) oppose prohibiting abortion even in cases of rape or incest – a restriction that is currently in-place in states such as Texas, Tennessee, South Dakota, Missouri, Louisiana and Kentucky among others.
Though a majority of Republican voters (70%) approve of the Supreme Court’s decision overturning Roe v. Wade, majorities across partisan voters – including most Republicans – are opposed to laws prohibiting abortion even in cases of rape or incest, laws making it a crime for women to get an abortion that would result in either fines or prison, and laws allowing private citizens to sue people who provide or assist women in getting abortions.
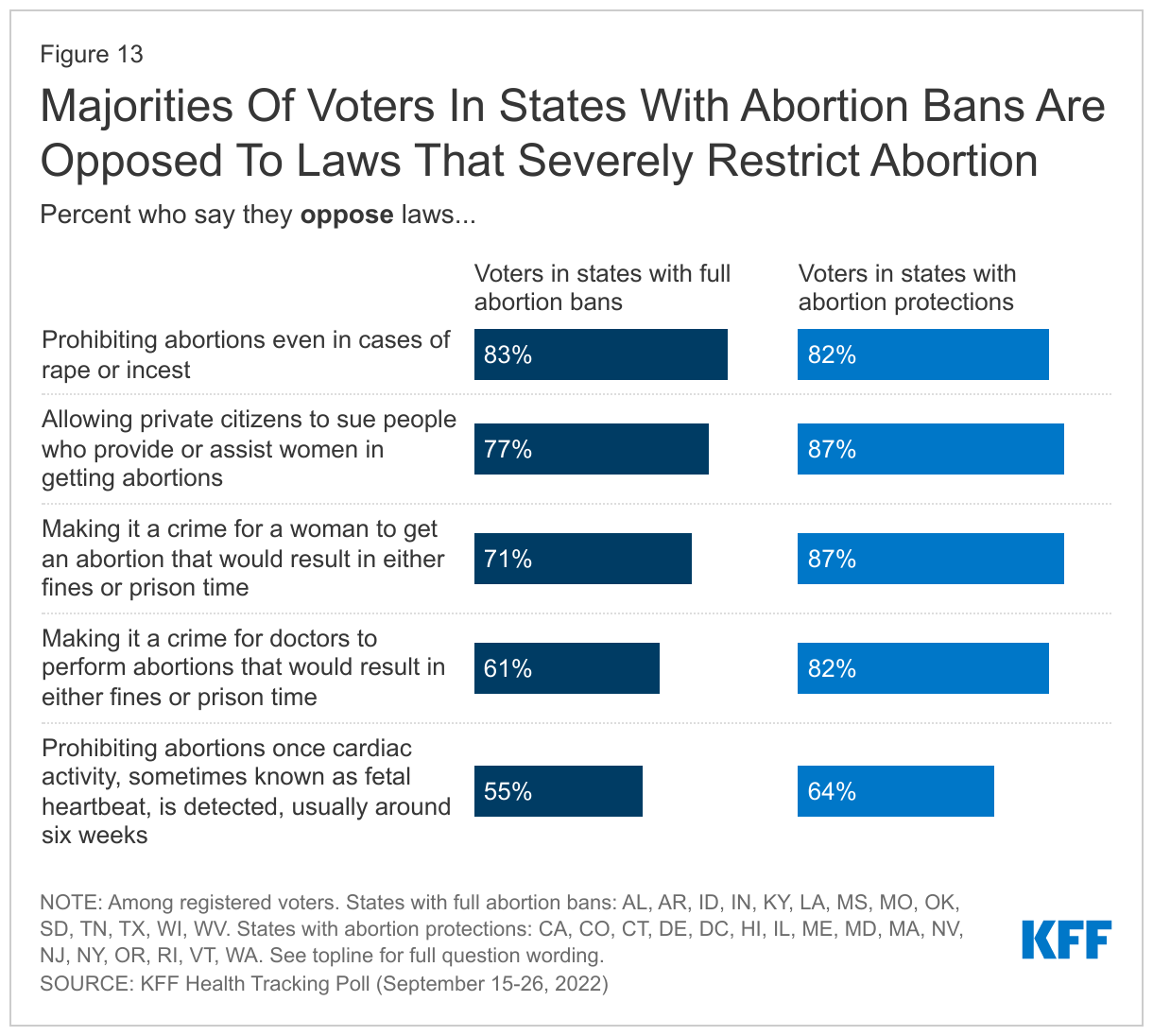
Large shares of voters living in states with abortion bans oppose many of the restrictions surveyed. More than eight in ten voters (83%) in states with full abortion bans say they oppose laws prohibiting abortion even in cases of rape and incest – which is currently the case in most of these states with full abortion bans. However, there is some support for prohibiting abortions once cardiac activity is detected among voters in states with full bans (45% support vs. 55% oppose).
Inflation Reduction Act Health Care Provisions And Student Loan Cancellation As Voting Issues
In the months leading up to the midterm election, which is historically viewed as a referendum on the president and their party, President Biden signed into effect the Inflation Reduction Act (IRA), a new law containing provisions related to health care and prescription drug costs, climate, and tax policy. In addition, he announced student loan debt forgiveness for many adults in the U.S. The KFF Health Tracking Poll examined how these recent Biden actions may be impacting voters ahead of the midterm elections.
The Inflation Reduction Act
Just over one month after President Biden signed the IRA into law, most of the public (77%) say they have heard or read at least a little about the new law, including majorities of adults across partisans, age groups, and racial and ethnic groups. About eight in ten adults ages 65 and older (82%), many of whom may be affected by the new law’s Medicare provisions, say they have heard at least a little about the new law and they are twice as likely as adults under age 65 to say they have heard “a lot” about it (25% vs. 12%).
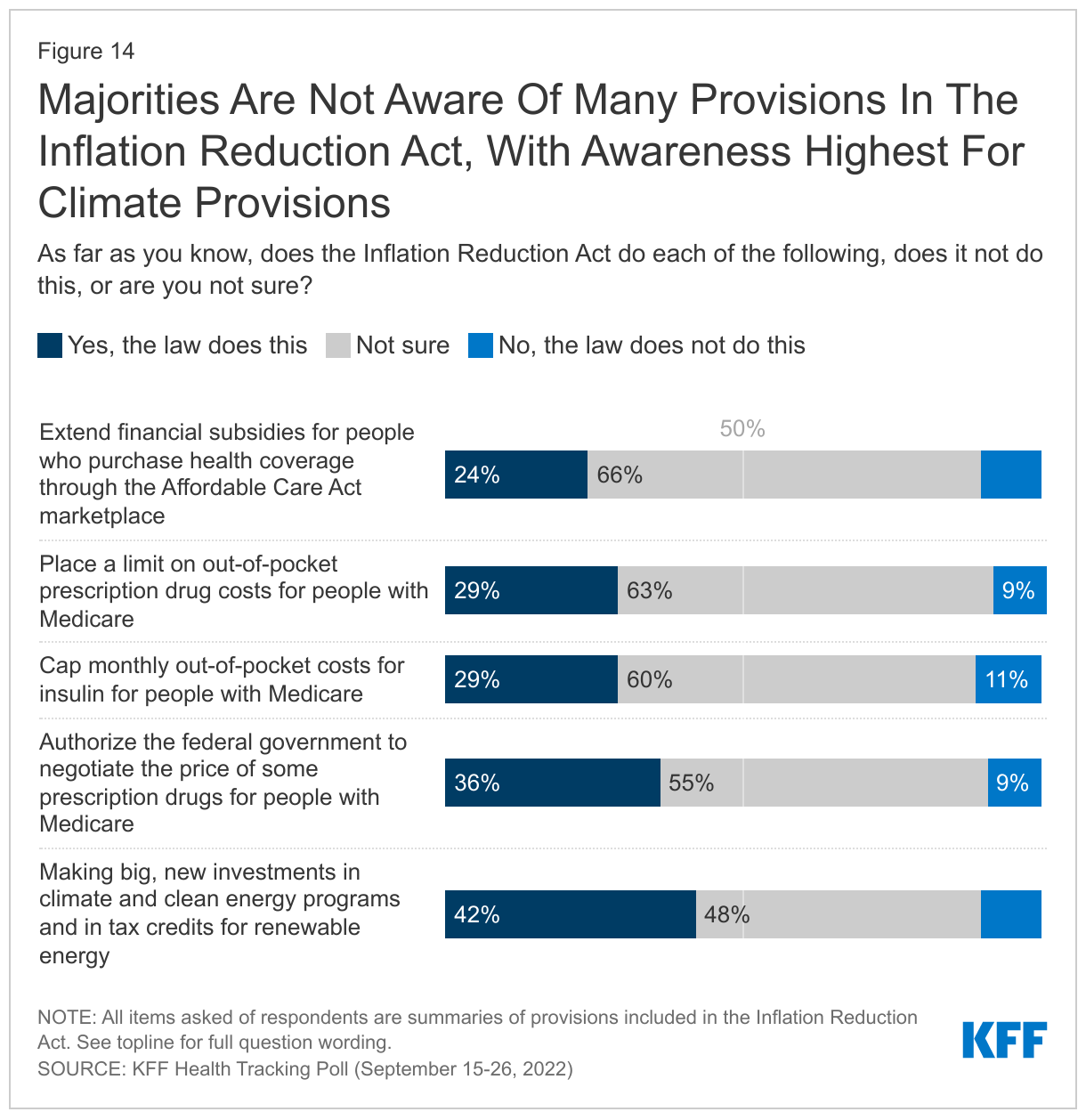
Yet, despite the fact that three in four adults have heard at least a little about the new law, few know what the law does. In fact, most adults are unaware of the law’s key health provisions. Most say they are unsure if the law extends financial subsidies for people who purchase health coverage through the Affordable Care Act marketplace (66%), places a limit on out-of-pocket prescription drug costs for people with Medicare (63%), caps monthly out-of-pocket costs for insulin for people with Medicare (60%) or authorizes the federal government to negotiate the price of some prescription drugs for people with Medicare (55%).
Awareness of the climate provisions in the new law, however, is higher compared to some of the health care elements of the law. While about half of adults (48%) say they are “not sure” if the new law makes big, new investments in climate and clean energy programs and in tax credits for renewable energy, about four in ten adults (42%) are aware the IRA does this.
Adults who say they have heard or read “a lot” or “some” about the Inflation Reduction Act are more likely than those who have only heard or read a little to know that each of the IRA provisions asked about in the survey were indeed part of the new law.
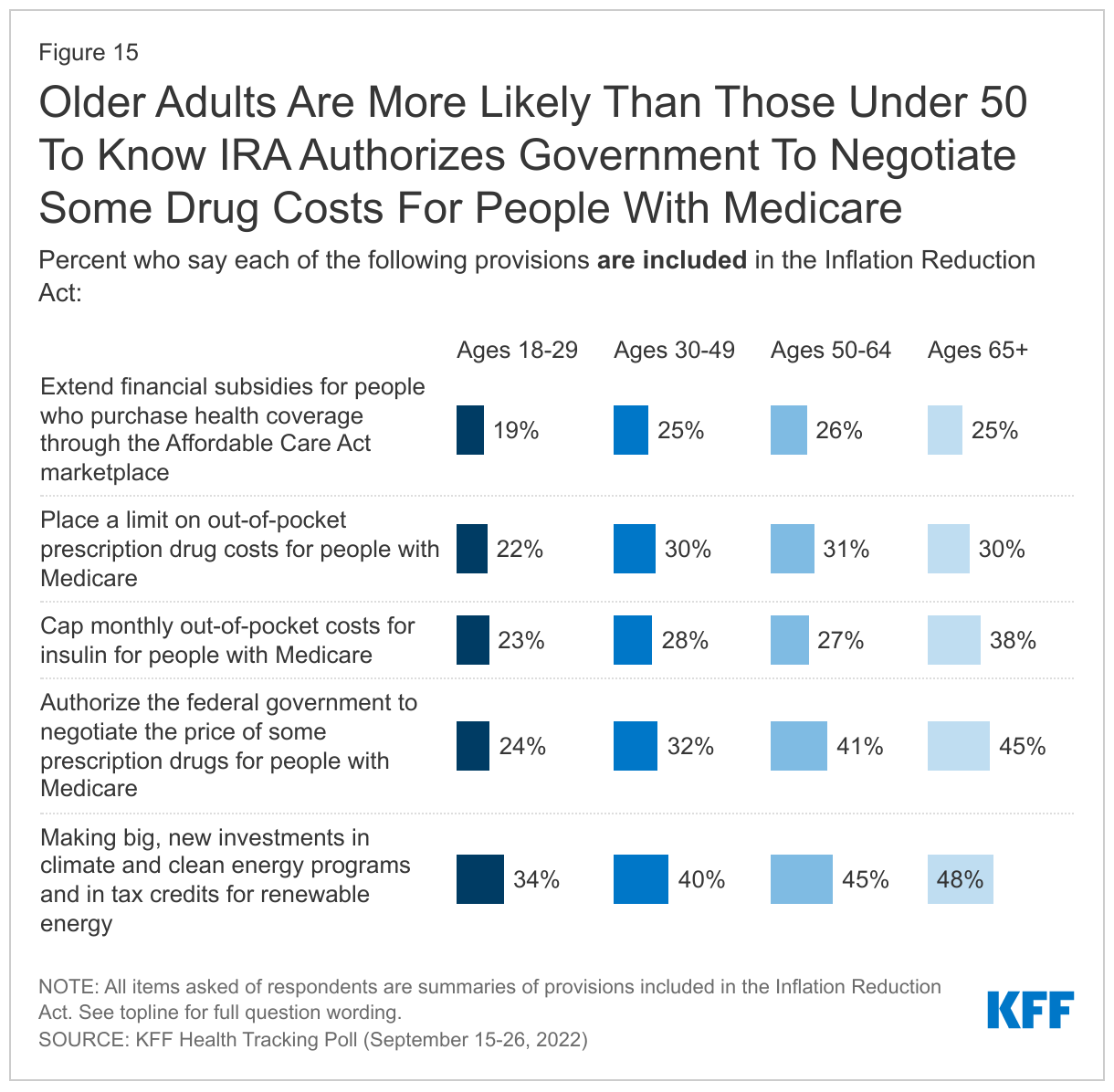
Adults ages 65 and over, a group that largely benefits from the Medicare prescription drug provisions of the law, are more likely than their younger counterparts to know that the IRA authorizes the federal government to negotiate the prices of some prescription drugs for people with Medicare (45% vs. 33% of adults 18 to 64) and to know that the bill caps monthly costs for insulin for people with Medicare (38% vs. 26% of adults 18 to 64).
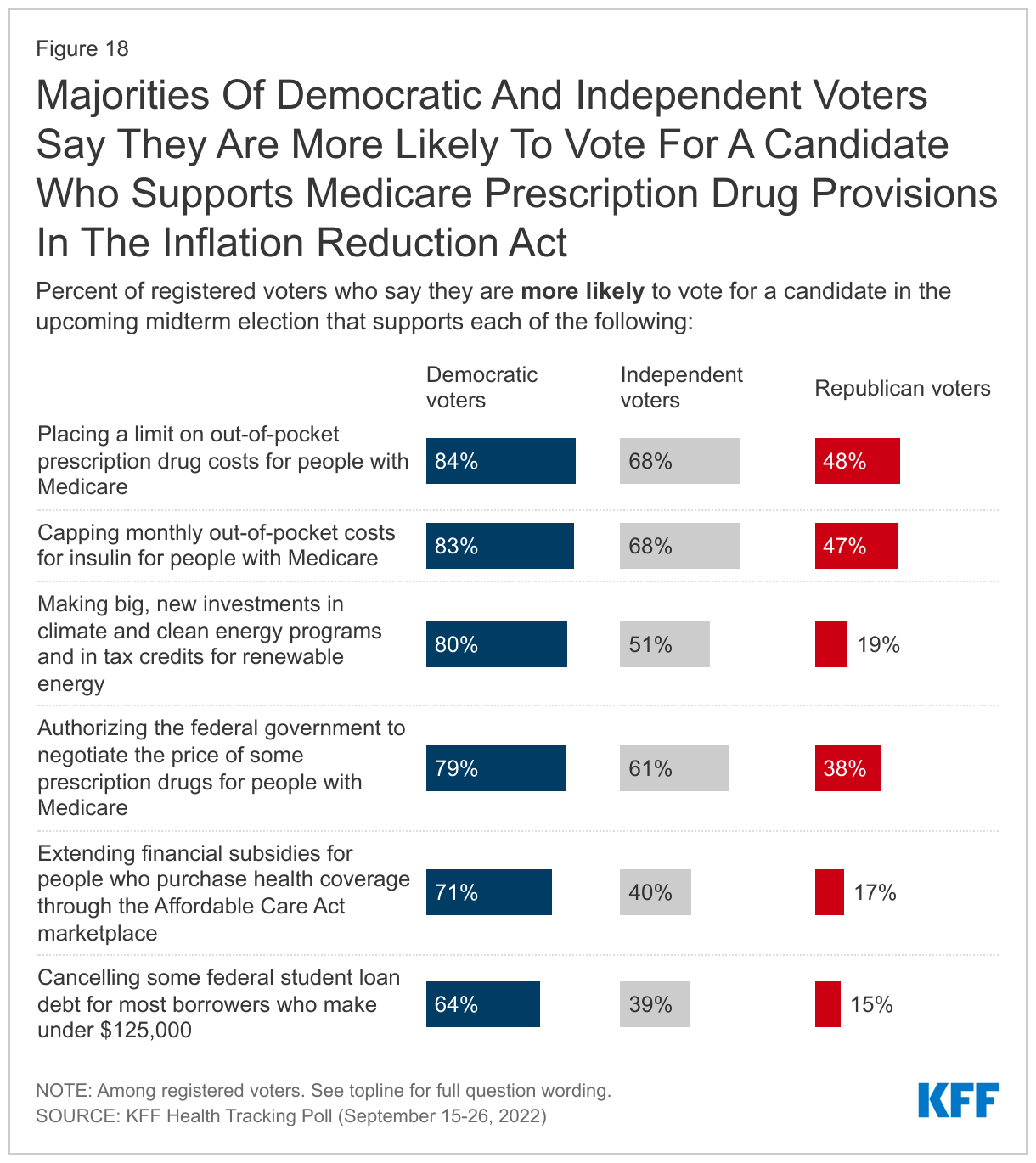
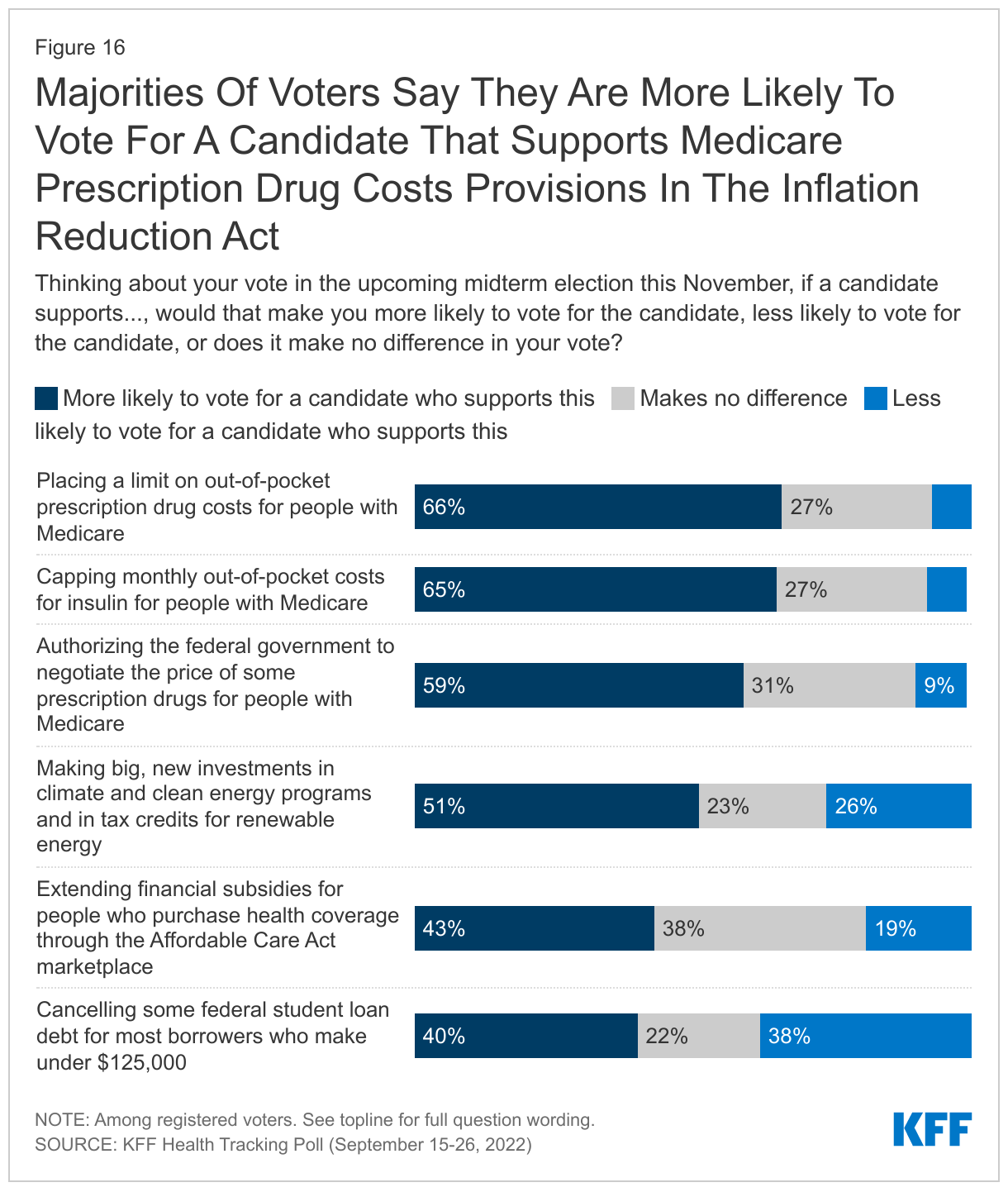
Though few adults are aware of the specific provisions included in the Inflation Reduction Act, many of these provisions are popular among voters. Majorities of voters say they would be more likely to vote for a candidate who supports placing a limit on out-of-pocket prescription drug costs for people on Medicare (66%), capping monthly out-of-pocket insulin costs for people with Medicare (65%) and authorizing the federal government to negotiate the price of some prescription drugs for people on Medicare (59%).
Voters are more divided on provisions related to climate and clean energy and extending subsidies under the Affordable Care Act. About half of voters (51%) say they would be more likely to vote for a candidate who supports making big, new investments in climate and clean energy programs and provide tax breaks for renewable energy, while less than half (43%) say they would be more likely to vote for a candidate who supports extending financial subsidies for people who purchase coverage through the Affordable Care Act marketplace.
Additionally, just a week after the passage of the IRA, the Biden Administration announced a plan to cancel up to $10,000 in federal student loans for most borrowers with incomes under $125,000. Notably, student loan cancellation appears to be particularly polarizing with four in ten voters (40%) saying they are more likely to vote for a candidate who supports cancelling some federal student loan debt for most borrowers who make under $125,000 while a similar share (38%) say they would be less likely to vote for a candidate who supports this.
These new policies could motivate different segments of voters. Majorities of voters ages 65 and older say they are more likely to vote for a candidate who supports the Medicare provisions in the Inflation Reduction Act, though fewer say the same about a candidate who supports clean energy investment, the extending ACA subsides, or cancelling some student loans. On the other hand, student loan cancellation may resonate among younger voters as those ages 18 to 29 are more than twice as likely as voters over 65 to say they are more likely to vote for a candidate who supports cancelling some student loans.
At least six in ten Democratic voters say they are more likely to vote for a candidate who supports each of the policies asked about, with the policies aimed at addressing prescription drug costs for people with Medicare being among the most popular. At least six in ten independent voters say they are more likely to vote for candidates who support these Medicare prescription drug provisions, though these policies are less popular among Republican voters. Eight in ten Democratic voters and half (51%) of independent voters also are motivated to vote for candidates who support climate investments, compared to just one in five Republicans (19%) who say the same.