An Overview of Medicaid Work Requirements: What Happened Under the Trump and Biden Administrations?
Issue Brief
The Trump Administration aimed to reshape the Medicaid program by newly approving Section 1115 demonstration waivers that imposed work and reporting requirements as a condition of Medicaid eligibility. However, courts struck down many of these approvals and the Supreme Court recently dismissed pending challenges in these cases. The Court dismissed pending litigation in Arkansas and New Hampshire due to the expiration of Arkansas’ waiver as well as the Biden Administration’s earlier withdrawals of these approved work requirement waivers. The Biden Administration had concluded that these provisions reduce coverage and thus do not promote the objectives of the Medicaid program. States could have appealed these withdrawal decisions to the HHS Departmental Appeals Board, and Georgia has challenged the withdrawal of its work requirements in court. An initial decision in the Georgia case is currently pending.
Although few Medicaid work and reporting requirements were implemented due to litigation, state withdrawals, and/or pauses during the COVID-19 pandemic, available implementation data from Arkansas suggests that these requirements were confusing to enrollees and result in substantial coverage loss, including among eligible individuals. This recent history of Medicaid work requirements illustrates the tensions between states, changing presidential administrations, and the courts. This issue brief answers key questions about these provisions:
- What is the history of Medicaid and work requirements?
- What do we know about the impacts of Medicaid work requirements?
- What is the current status and future of Medicaid work requirements?
Although the Biden Administration has concluded that it does not believe work requirements further Medicaid program objectives, a future presidential administration could revisit these waiver provisions. To survive an expected legal challenge, the administrative record in any future approvals would likely have to support the conclusion that such waivers would further Medicaid program objectives, including promoting affordable coverage for low income people.
What is the history of Medicaid and work requirements?
Prior to the Trump Administration, no states had received waiver approvals to condition Medicaid coverage on work and reporting requirements, and legislative attempts to incorporate work requirements into Medicaid statute failed. Policy arguments for and against Medicaid work requirements are grounded in views about whether Medicaid is akin to a public assistance program, like Temporary Assistance for Needy Families (TANF), or one that provides health insurance, in line with the Affordable Care Act (ACA) expansion of the program as one of several routes to increasing access to affordable health care for uninsured Americans. Adults who receive TANF cash assistance generally are required to participate in work, as one of the express purposes of TANF enumerated in statute is to “end the dependence of needy parents on government benefits by promoting job preparation, work, and marriage.” In contrast, Congress has not identified work as an objective for the Medicaid program. The ACA aimed to make Medicaid available to low-income adults through its Medicaid expansion, regardless of whether a person also met categorical eligibility requirements such as being pregnant, a parent, senior, or person with a disability. After implementation of the ACA’s Medicaid expansion, the Obama Administration signaled it would not approve state waiver requests to require work as a condition of Medicaid eligibility, concluding in its denial of Arizona’s request that work requirements “could undermine access to care and do not support the objectives of the [Medicaid] program.” In an effort to reframe Medicaid to a program akin to “public assistance”, unsuccessful Republican attempts to repeal and replace the ACA in 2017 proposed allowing states to require work as a condition of Medicaid eligibility.
In ways other than work requirements, Medicaid supports employment by providing affordable health coverage as well as voluntary employment referral and/or work support programs in some states. Research shows that being in poor health is associated with increased risk of job loss, while access to affordable health insurance has a positive effect on the ability to obtain and maintain employment. Medicaid coverage helps low-wage workers get care that enables them to remain healthy enough to work; across states enrollees report that this coverage helps them to manage chronic conditions and supports their ability to work jobs that may be physically demanding. While most Medicaid adults who qualify through non-disability pathways are already working, some states have launched initiatives to support employment for Medicaid enrollees without making employment a condition of eligibility. A couple of states (including AR and IN) have offered voluntary employment referral programs relying on general enrollee notices rather than targeted outreach. Other states (including LA, ME, and MT) have incorporated intensive targeted outreach and case management services into their voluntary work support programs.
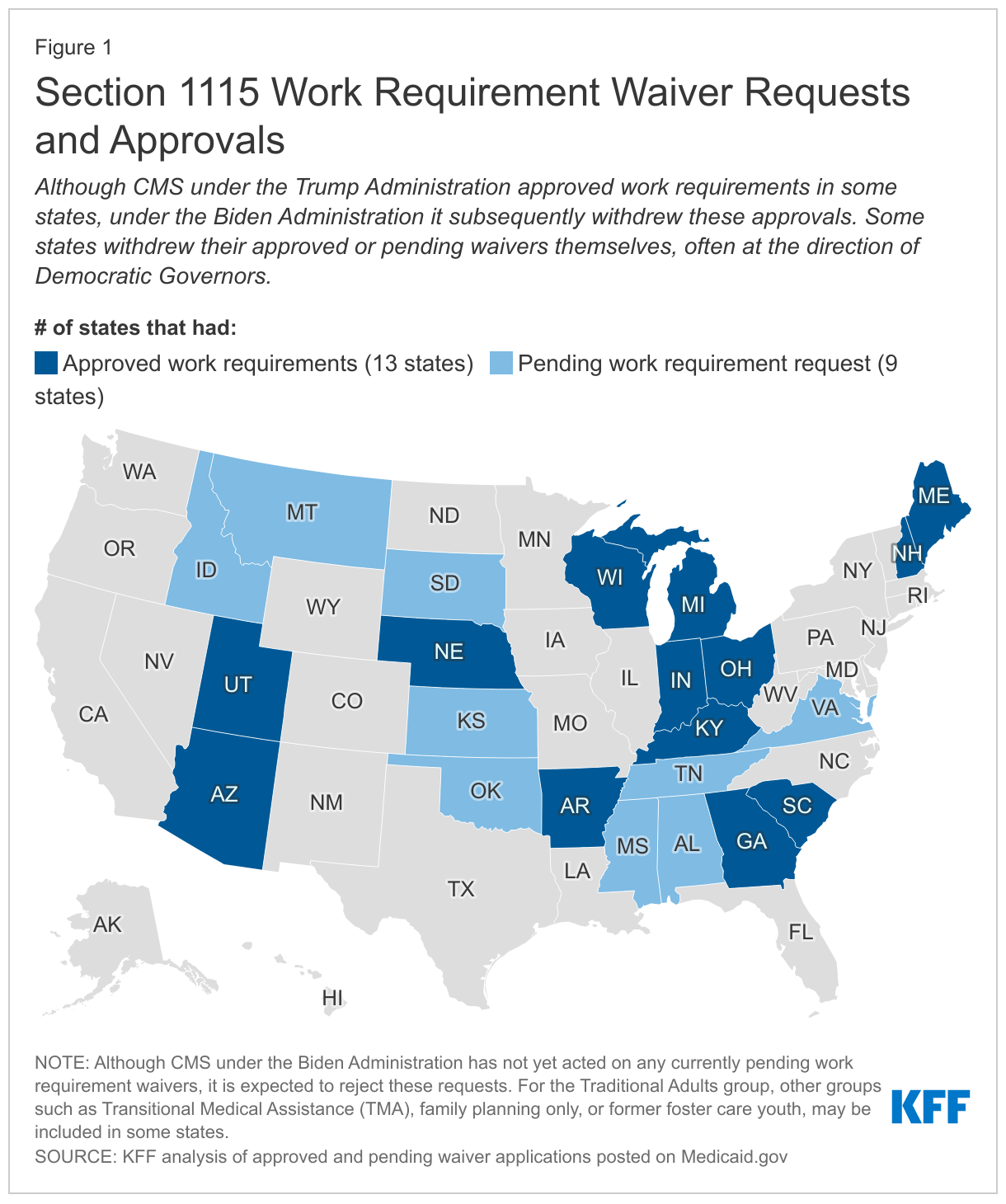
In a departure from previous administrations, the Trump Administration encouraged and approved Section 1115 waivers that conditioned Medicaid coverage on meeting work and reporting requirements in 13 states (Figure 1). Under Section 1115 of the Social Security Act, the Secretary of HHS can allow states to use federal Medicaid funds in ways that federal rules do not otherwise allow, as long as the initiative is an “experimental, pilot, or demonstration project” that “is likely to assist in promoting the objectives of [the program].” In January 2018, CMS issued guidance inviting states to request Section 1115 waivers that impose work and reporting requirements (referred to as “community engagement”) as a condition of Medicaid eligibility for non-elderly, non-pregnant adult beneficiaries who are eligible on a basis other than disability. The guidance asserted that such provisions would promote program objectives by helping states “in their efforts to improve Medicaid enrollee health and well-being through incentivizing work and community engagement.” In contrast to voluntary work support programs discussed above, the guidance was explicit that state initiatives to condition Medicaid eligibility on meeting work and reporting requirements could not use federal Medicaid funds for supportive services to help people overcome barriers to work, such as childcare or transportation. The next day, CMS approved the first Medicaid work requirement in Kentucky’s waiver. In total, CMS under the Trump Administration approved waivers with work requirements in 13 states. Across states, work requirement waivers were generally similar in conditioning Medicaid coverage for certain adults on reported employment or other qualifying activities, with some variation in technical details. For example, waivers varied by:
- population, with most applying to expansion adults, a couple applying to both expansion and traditional adults, such as low-income parents, in expansion states, and some later approvals applying to low-income parents and some limited other populations in non-expansion states;
- exemptions, such as for older age or medical frailty (although the work requirement guidance excluded people who are eligible for Medicaid based on a disability, many Medicaid adults with disabilities do not receive SSI benefits and are eligible due to low income rather than disability status, so they would be subject to work requirements unless the state makes an exemption and they are able to successfully navigate the exemption process);
- qualifying activities in addition to employment (such as education, community service, and job search or training);
- number of hours of qualifying activities required per week or month and how to report these (such as through an online account); and
- consequences for noncompliance (typically disenrollment, though two states (GA and SC) required compliance to be established prior to enrollment and one state (NE) conditioned access to certain benefits, rather than eligibility, on compliance with work requirements).
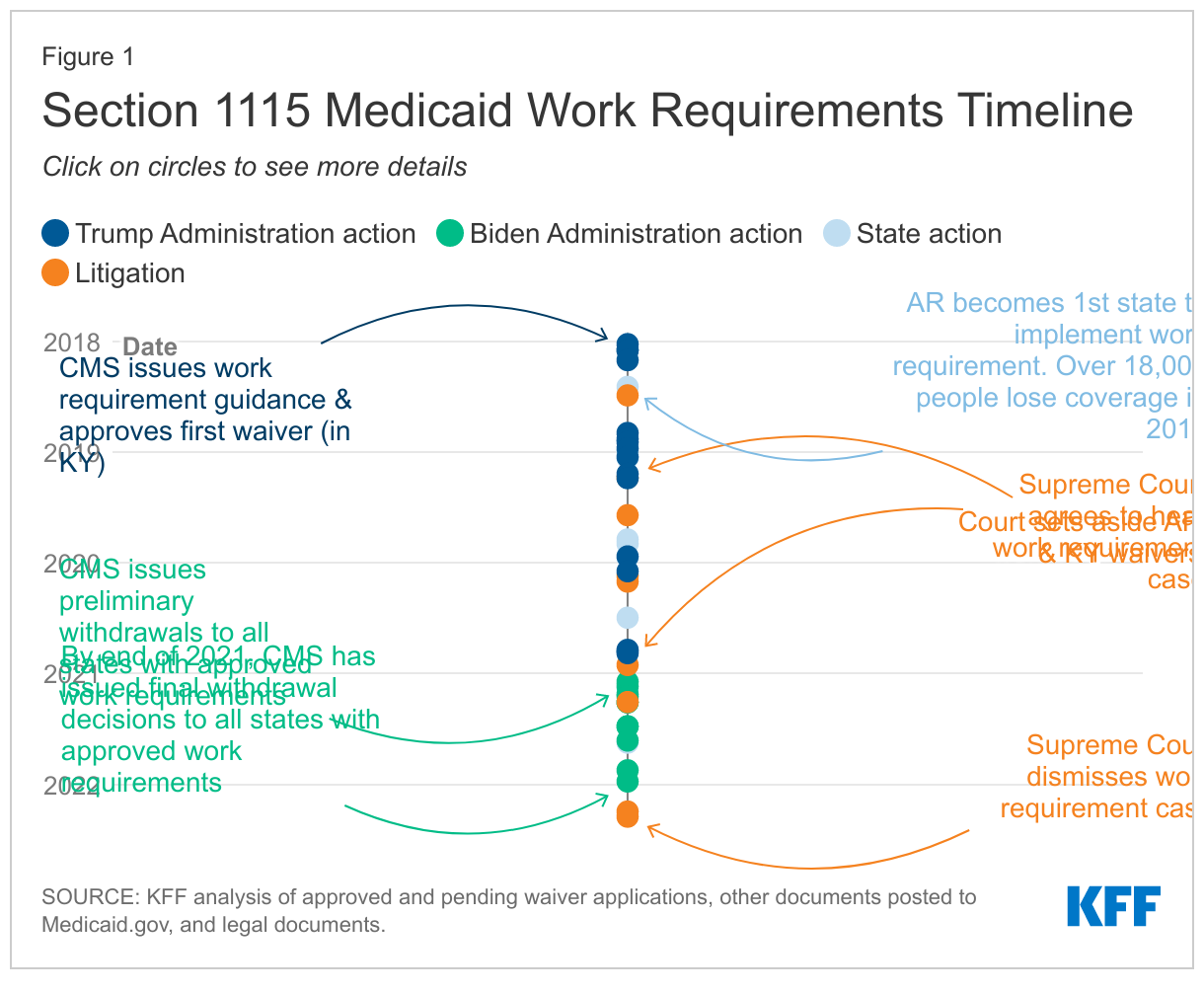
Of the 13 states that had approved work requirements, only Arkansas implemented such requirements with consequences for noncompliance. Other states that began implementation did not disenroll those who did not comply and instead paused implementation due to litigation and/or the COVID-19 pandemic. For state-level detail on these approved waivers as well as additional requests that were not approved by the end of the Trump Administration, see Figure 1 and Appendix Table 1. For more information on the timing of work requirement approvals, as well as subsequent legal challenges and withdrawals (as discussed in the section below), see Appendix Figure 1.
What do we know about the impacts of Medicaid work requirements?
Research on the relationship between work and health, including experience with AFDC, TANF, and SNAP, suggest that the effects of work requirements on health and employment may be limited. In the 1990s, states used Section 1115 waivers in attempts to increase work among enrollees in the Aid to Families with Dependent Children (AFDC) program; however, an analysis suggested that a significant part of the AFDC targeted population faced obstacles to work including disability. Similarly, research finds that work requirements in TANF—the program that replaced AFDC—have had little impact on increasing employment over the long-term, as most TANF enrollees are either already working or face significant employment barriers that work requirements do not address. Studies also find that SNAP work requirements do not significantly increase employment but result in large reductions in SNAP participation. Finally, a review of research on the relationship between work and health found that although there is strong evidence of an association between unemployment and poorer health outcomes, there is limited evidence on the effect of employment on health.
As most Medicaid enrollees are already working or face barriers to work, work and reporting requirements may cause coverage loss among eligible enrollees without increasing employment. Prior to the pandemic, the majority (63%) of non-dual (i.e., not also enrolled in Medicare), non-SSI, nonelderly Medicaid adults were already working full or part-time. Among those not working, most were not working due to caregiving (12%), illness or disability (10%), or school attendance (7%). Many of these reasons would likely qualify as exemptions from work requirement policies in most states, leaving just 7% of Medicaid adults (who reported that they were retired, unable to find work, or were not working for another reason) to whom work requirement policies could be directed. A 2018 analysis suggests that if all states were to implement Medicaid work requirements, between 1.4 and 4.0 million Medicaid adults could lose coverage, with the majority of disenrollment occurring among individuals who comply with the requirements (i.e., are working enough hours to satisfy requirements) and remain eligible but lose coverage due to new administrative reporting burdens or red tape. Research suggests work requirements could have particular adverse effects on certain Medicaid populations, such as women, people with HIV, and adults with disabilities including those age 50 to 64. Finally, the one in four Medicaid enrollees living in homes with limited internet access may face particular challenges meeting work and reporting requirements, as many states disseminated information about these requirements online and/or required enrollees to report compliance online.
Available implementation data suggests that Medicaid work and reporting requirements were confusing to enrollees and result in substantial coverage loss, including among eligible individuals. As noted above, few states implemented approved Section 1115 waivers with work requirements due to litigation, state withdrawals, and/or the COVID-19 pandemic. However, Arkansas’ waiver was in effect from June 2018 through March 2019 (when it was set aside by a federal court), with evidence from this period suggesting that more than 18,000 people (about 25% of those subject to the requirement) lost coverage in 2018. While enrollees who lost coverage in 2018 could reapply for coverage in January 2019, the vast majority of those who lost coverage (89%) remained unenrolled in early 2019. Although Arkansas’s program included safeguards intended to protect coverage for people with disabilities and others who should not have been subject to the requirements from losing coverage (including “medically frail” and “good cause” exemptions and “reasonable accommodations” to assist with meeting the requirements), few people used these safeguard measures relative to the number who lost coverage. Among those who accessed “good cause” exemptions, the vast majority did so due to disability/other health issues or technical issues, primarily related to reporting. This difficulty with reporting underscores that Arkansas’ administrative processes presented barriers to eligible people retaining coverage including and beyond those with disabilities. Lack of computer literacy and internet access among enrollees created barriers to setting up online accounts as well as ongoing reporting. Research indicates that enrollees in Arkansas were unaware of or confused by the new work and reporting requirements, which did not provide an additional incentive to work beyond economic pressures.
What is the current status and future of Medicaid work requirements?
The Biden Administration began the process to withdraw Section 1115 work requirements in February 2021 and has since issued final withdrawals for all states that had approvals. CMS generally reserves the right to withdraw approved waiver authorities at any time it determines that these authorities are no longer in the public interest or promote Medicaid objectives. A January 2021 executive order from President Biden directed HHS to review waiver policies that may undermine Medicaid. CMS subsequently withdrew Medicaid work requirement waivers in all states that had approvals. These withdrawal letters cited evidence from Arkansas (described above) as well as additional data indicating that about 40% of those subject to work requirements (or 17,000 beneficiaries) in New Hampshire and 33% (or 80,000 beneficiaries) in Michigan were at risk of coverage loss, prior to implementation pauses. The letters also highlighted that job and income loss among the low-income population during the COVID-19 pandemic were likely to exacerbate the risks of coverage loss under work requirements. No states were implementing work requirements at the time of withdrawal, either due to the pandemic, litigation (see Appendix Table 2), or prior termination by the states themselves (see Figure 1).
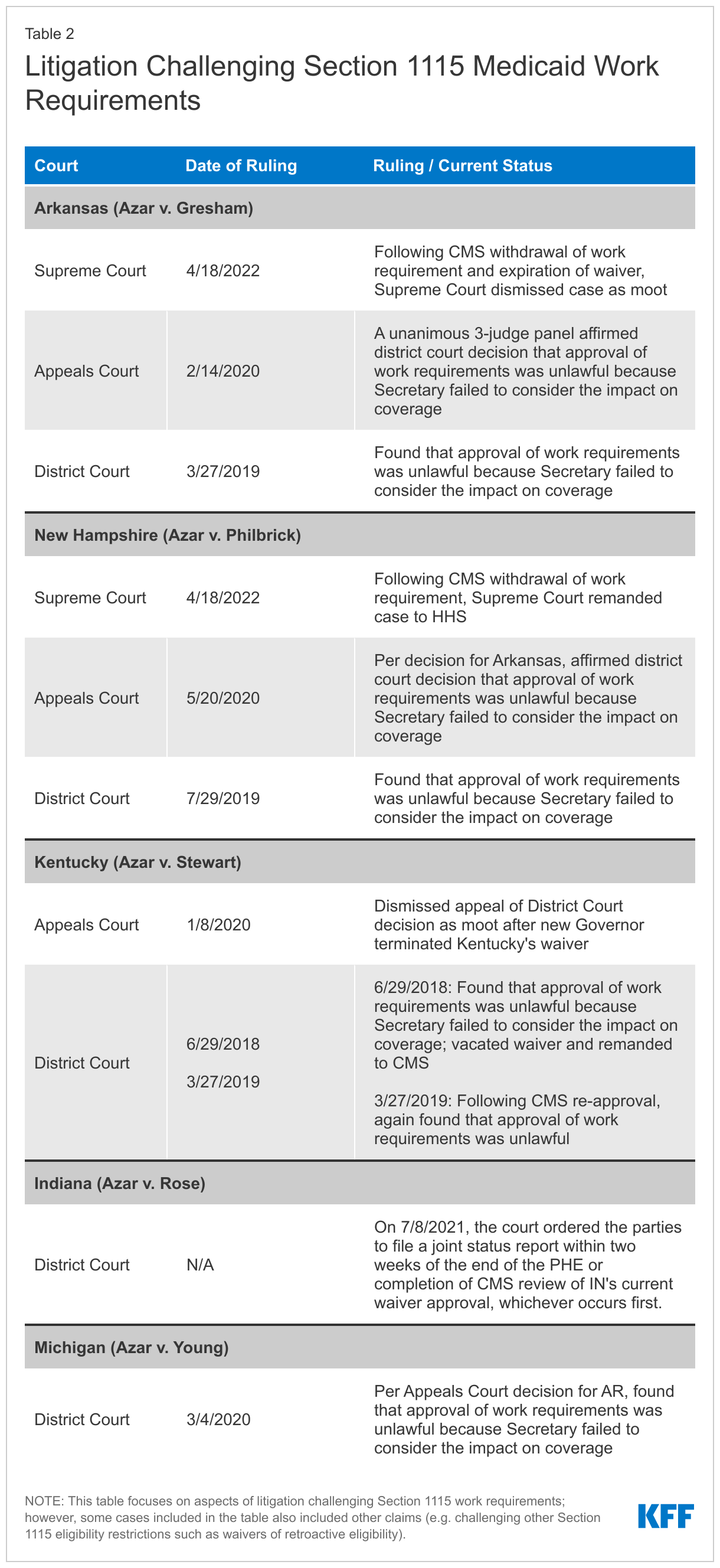
Following the Biden Administration’s withdrawals, in April 2022 the Supreme Court dismissed pending appeals in cases that had found work requirement approvals unlawful. Previously, in February 2020 a DC Circuit Court of Appeals panel affirmed in a unanimous opinion that the HHS Secretary’s approval of Medicaid work requirements in Arkansas was unlawful because the Secretary failed to consider the impact on coverage. The DC appeals court subsequently affirmed that the Secretary’s New Hampshire approval also was unlawful. Before leaving office, the Trump Administration asked the Supreme Court to reverse these appeals court decisions and the Court agreed to hear the cases in December 2020. However, following the Biden Administration’s withdrawals of the Arkansas and New Hampshire work requirements, in April 2021 the Supreme Court removed the cases from its oral argument calendar. In April 2022, the Biden Administration asked the Court to vacate the lower court decisions and dismiss the Arkansas case as moot (as that waiver had expired) and remand send the New Hampshire case back to HHS (as New Hampshire had not asked the Court to review the case involving its waiver). In April 2022, the Court granted this motion, effectively putting an end to the pending litigation. (For more information on work requirement litigation across states, see Appendix Table 2 and Figure 1.)
The Supreme Court’s dismissal does not preclude future presidential administrations from approving new Section 1115 work requirements. Each case challenging work requirements (see Appendix Table 2) has centered on the administrative record of the underlying waiver approvals under the Trump Administration, with courts finding that these approvals were unlawful because they were unsupported by the administrative records. Specifically, the courts found that the Secretary did not consider impacts on coverage contained in the administrative records. Although the Biden Administration has concluded that it does not believe work requirements further Medicaid program objectives, CMS under future presidential administrations could issue new guidance encouraging work requirement waivers and approve such waivers based on a different interpretation of program objectives—though these would likely face legal challenges. For example, although Arkansas removed its work requirement in its new waiver, the state noted that should federal law or regulations permit the use of a work requirement as a condition of eligibility in the future, it would seek to amend the demonstration accordingly. Separately, states had the opportunity to appeal the Biden Administration’s withdrawals of work requirement waivers to the HHS Departmental Appeals Board and Georgia has challenged the withdrawal of its work requirements (which would have been part of a limited coverage expansion) in court. Georgia’s challenge remains pending, with an initial decision expected later this summer.
Conclusion
As a health coverage program, Medicaid can support employment by providing health coverage and access to care and medications that enable people to work, and it can also provide voluntary employment referral and/or work support programs. In a departure from previous administrations, the Trump Administration encouraged and approved Section 1115 waivers that conditioned Medicaid coverage on meeting work and reporting requirements. Though few of these work requirements were implemented due to legal challenges, state withdrawals, and/or the COVID-19 pandemic, available data suggests that such requirements can result in substantial coverage loss, including among eligible individuals, as evidenced by the more than 18,000 individuals who lost coverage in seven months under Arkansas’ work and reporting requirement. Based in part on this data, the Biden Administration withdrew all approved work requirement waivers by the end of 2021; Georgia has since challenged the withdrawal of its work requirements in court. Following these withdrawals and the expiration of Arkansas’ waiver, the Supreme Court dismissed pending appeals in cases that had found work requirement approvals unlawful. Though the Court’s action does not preclude future presidential administrations from approving new Section 1115 work requirements, these would likely face legal challenges.
Appendix