Five Key Facts About Spending and Enrollment for People with Medicare and Medicaid (Dual-Eligible Individuals)
Introduction
There are approximately 12 million people enrolled in both Medicare and Medicaid, who are also known as dual-eligible individuals. Compared with people who are only covered by Medicare or Medicaid, this group is more likely to report being in fair or poor health and require assistance with activities of daily living and often experiences more fragmented or disjointed health care on account of having two sources of coverage.
For dual-eligible individuals, Medicare is the primary payer and covers medical and post-acute care, while Medicaid wraps around Medicare coverage by paying Medicare premiums and in most cases, cost-sharing. Among the approximately 12 million dual-eligible individuals, 8.6 million are “full-benefit” dual-eligible individuals, meaning they are eligible for Medicaid benefits that are not covered by Medicare, including long-term care, vision, and dental. The remaining 3.5 million dual-eligible individuals are “partial-benefit” dual-eligible individuals, who are eligible only for assistance with Medicare premiums, and in many cases, cost sharing through the Medicare Savings Programs (see Appendix, “How do Medicare Beneficiaries Become Eligible for Medicaid?”).
This issue brief analyzes linked Medicare and Medicaid administrative and claims data from 2022 and 2023 to provide a profile of enrollment and spending on dual-eligible individuals, drawing on new analysis of data on chronic conditions to show how higher rates of chronic conditions contribute to higher average spending among this population (see Methodology). The analysis finds that dual-eligible individuals comprise disproportionately high shares of spending in Medicare and Medicaid relative to their enrollment shares because of higher per-person costs than people who are not dual-eligible individuals. Those high per-person costs to some extent reflect higher rates of chronic conditions than other people with Medicare or Medicaid, and per person spending among dual-eligible individuals increases with the number of chronic conditions.
Key Facts
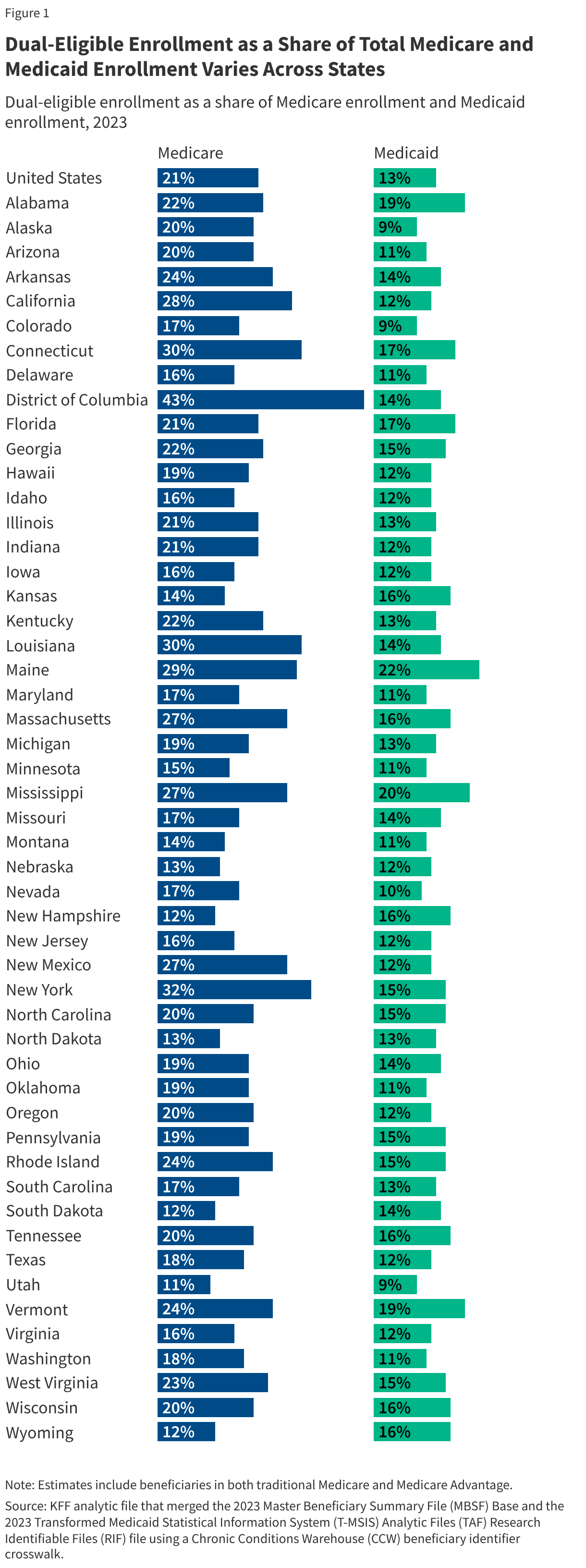
1. Dual-eligible individuals represent 21% of Medicare beneficiaries and 13% of Medicaid enrollees nationally, although state shares vary.
Dual-eligible individuals comprise 21% of the total Medicare population (including beneficiaries in both traditional Medicare and Medicare Advantage) and 13% of the total Medicaid population, but the shares vary widely across states. Dual-eligible individuals comprise 30% or more of all Medicare beneficiaries in the District of Columbia, New York, Connecticut, and Louisiana, but only 11% in Utah. Dual-eligible individuals comprise 20% or more of all Medicaid enrollees in Maine and Mississippi, but less than 10% in Utah, Colorado, and Alaska. Variation across states reflects an array of factors including the distribution of income and wealth among the state populations, the age distribution of state populations, and Medicaid eligibility criteria.
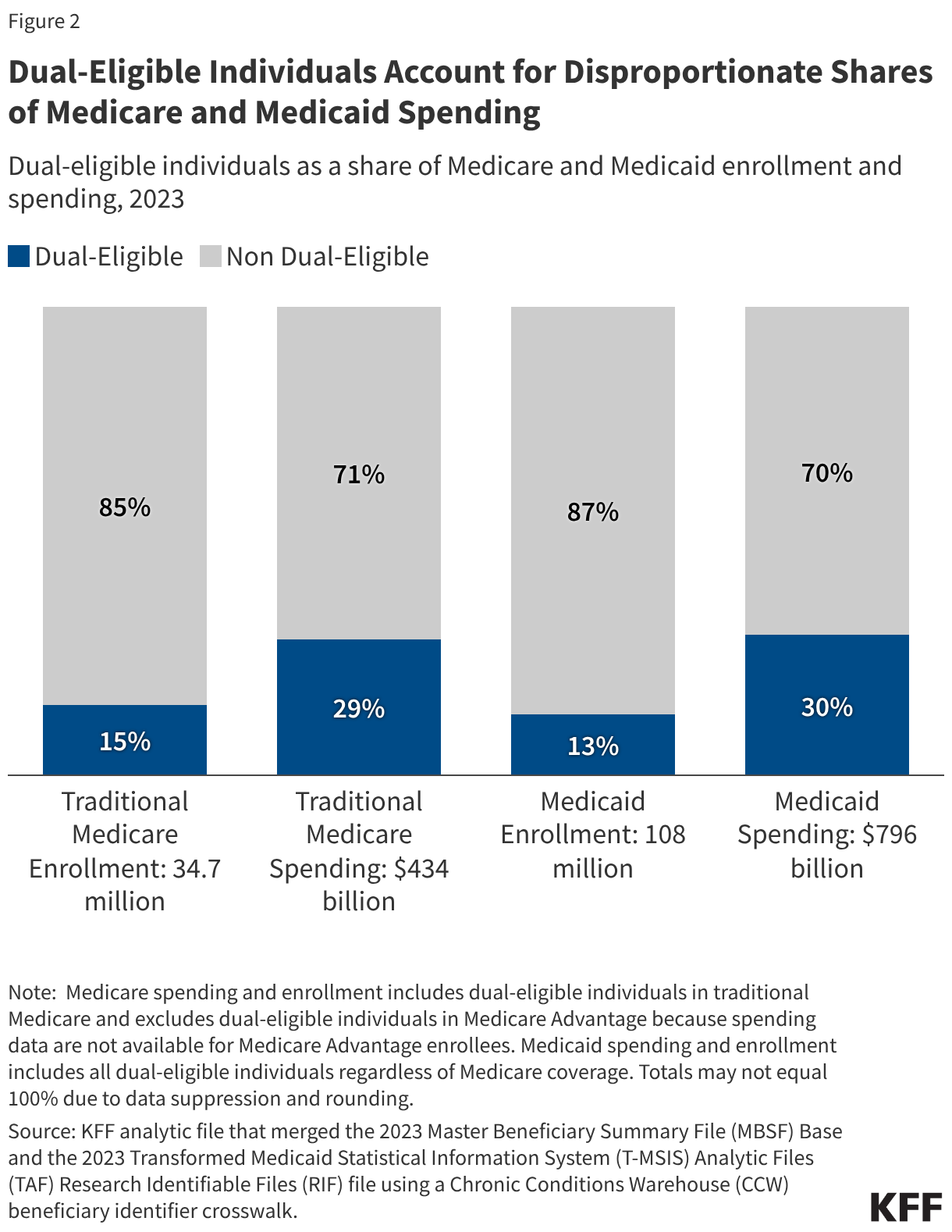
2. Dual-eligible individuals account for disproportionate shares of Medicare and Medicaid spending.
Dual-eligible individuals account for a larger share of spending in each program than their respective shares of Medicare and Medicaid enrollment. Dual-eligible individuals comprise 15% of the traditional Medicare population but account for 29% of traditional Medicare spending (or $127 billion of $434 billion). (Those estimates include spending for the 5.3 million dual-eligible individuals in traditional Medicare only, excluding the 9.2 million dual-eligible individuals who had Medicare Advantage coverage in the year because Medicare spending data are not available for beneficiaries enrolled in Medicare Advantage plans). Dual-eligible individuals comprise 13% of Medicaid enrollment but 30% of federal and state Medicaid spending (or $241 billion of $796 billion).
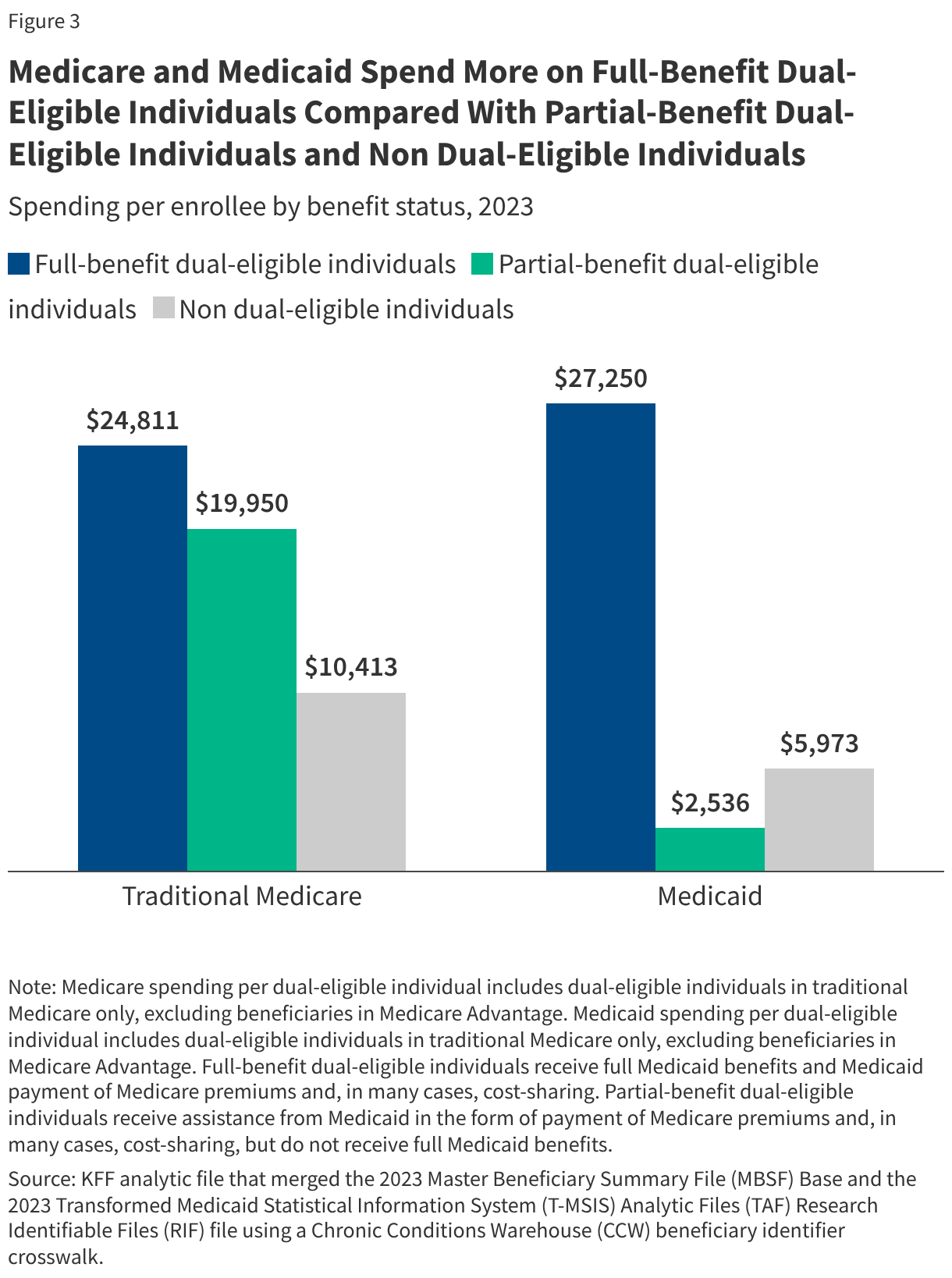
3. Medicare and Medicaid spend more per person on full-benefit dual-eligible individuals compared with other enrollees.
Traditional Medicare spending per person averages $24,811 for full-benefit dual-eligible individuals, $19,950 for partial-benefit dual-eligible individuals, and $10,413 for beneficiaries without Medicaid. Higher average Medicare per person spending among full-benefit dual-eligible individuals reflects greater use of medical care among this population, which could be related to their higher rates of chronic conditions (see below). Higher Medicare spending among full-benefit dual-eligible individuals may also reflect their ability to access health care services without substantial financial barriers associated with cost sharing, since most full-benefit dual-eligible individuals receive Medicaid coverage of Medicare cost sharing. In addition, this group has access to certain Medicaid benefits, such as non-emergency medical transportation and case management, which could ease access barriers and increase use of Medicare-covered services.
Per person Medicaid spending averages $27,250 for full-benefit dual-eligible individuals, $2,536 for partial-benefit dual-eligible individuals, and $5,973 for Medicaid enrollees without Medicare. Medicaid only pays for premiums and, in many cases, cost sharing for partial-benefit dual-eligible individuals. Even though Medicare is the primary payer for acute care, Medicaid per person spending for full-benefit dual-eligible individuals is several times larger than for Medicaid enrollees without Medicare. That difference likely reflects several factors: increased use of long-term care and other services not covered by Medicare; higher rates of chronic conditions among dual-eligible individuals, which is associated with higher spending (or greater use of services); and the fact that most other Medicaid enrollees are children, parents, and others under age 65 who tend to have lower per enrollee spending.
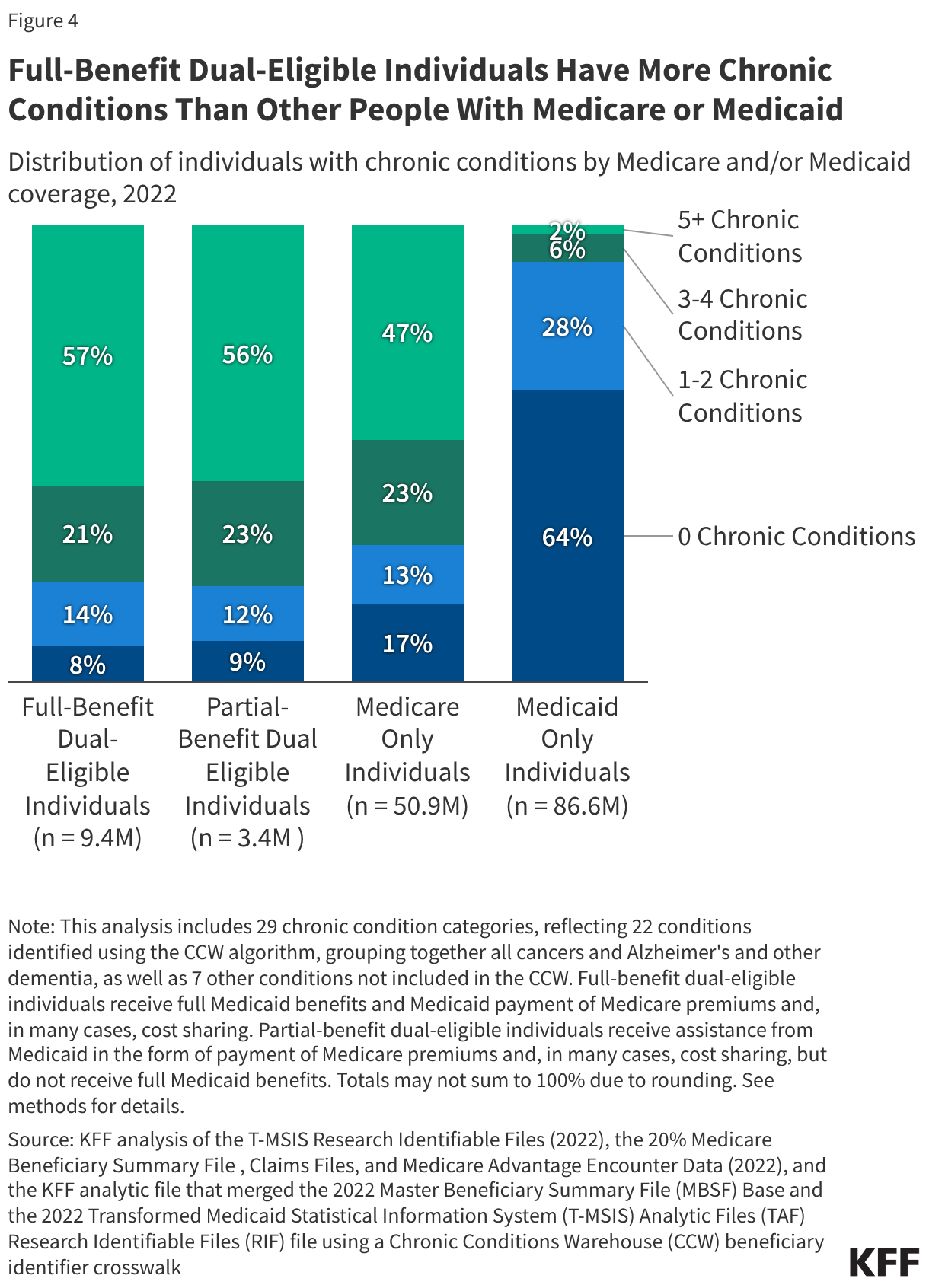
4. Full-benefit dual-eligible individuals have more chronic conditions than other people with Medicare or Medicaid.
Rates of chronic conditions are higher among full-benefit and partial-benefit dual-eligible individuals compared with other people with Medicare or Medicaid coverage. Fifty seven percent of full-benefit and 56% of partial-benefit dual-eligible individuals have five or more chronic conditions, compared with less than half (47%) of all other Medicare beneficiaries and just 2% of enrollees with Medicaid only. The relatively high rates of Medicare beneficiaries with multiple chronic conditions reflects that the Medicare population consists primarily of adults ages 65 and older, where chronic conditions such as hypertension, hyperlipidemia, and arthritis are more common than among younger adults. Medicaid-only enrollees are less likely than dual-eligible individuals to have chronic conditions, which reflects the fact that most Medicaid enrollees are children, parents, and others under age 65. Nearly two-thirds of Medicaid-only enrollees (64%) have no chronic conditions, compared with 17% of non-dual Medicare beneficiaries, and just 8% of full- and 9% of partial-benefit dual-eligible individuals.
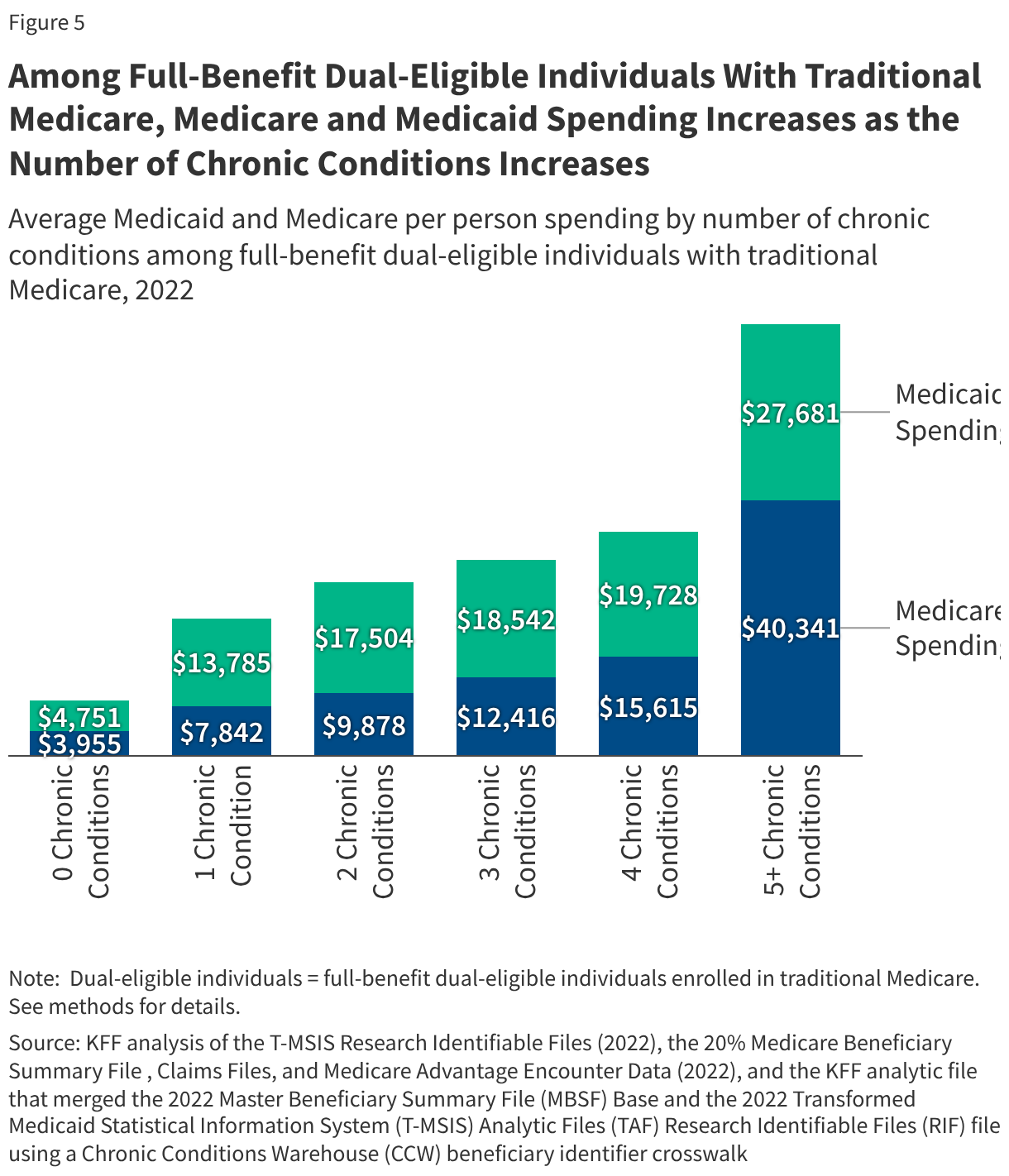
5. Among full-benefit dual-eligible individuals with traditional Medicare, Medicare and Medicaid spending increase with the number of chronic conditions.
Among full-benefit dual-eligible individuals enrolled in traditional Medicare, Medicare and Medicaid spending increase with the number of chronic conditions. For a full-benefit dual-eligible individual without any chronic conditions, traditional Medicare spending averages $3,955 and Medicaid spending averages $4,751. In comparison, among those with five or more chronic conditions, traditional Medicare spending averages $40,341 (over 10 times higher) and Medicaid spending averages $27,681 (almost 6 times higher). Although Medicare is the primary payer for dual-eligible individuals’ acute care, Medicaid spending on dual-eligible individuals is often higher than that of Medicare. This outcome likely occurs because Medicare generally doesn’t cover long-term care, which can be extremely expensive, and accounts for nearly one-third of all Medicaid spending. Spending on Medicaid enrollees who use long-term care is eight times higher than that of enrollees who don’t use long-term care, and over 60% of enrollees who use long-term care are dual-eligible individuals.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Appendix
How do Medicare Beneficiaries Become Eligible for Medicaid?
- States are required to cover Medicare beneficiaries who receive Supplemental Security Income and may choose to cover an array of additional groups such as people with significant disabilities and income less than the federal poverty level, those with high medical spending, and those who need long-term care.
- Most, but not all, full-benefit dual-eligible individuals are also eligible for Medicare premium and cost-sharing assistance covered under the Medicare Savings Programs, which are administered by states.
- Federal law defines minimum income and resource limits for each of the Medicare Savings Programs, which are updated annually by the Centers for Medicare and Medicaid Services (CMS).
- Income and asset limits can also vary by state; generally, Medicare beneficiaries must have income below $1,861 each month for an individual ($2,455 for a couple) and resources below $9,500 for an individual ($14,910 for a couple) in 2026. States can raise those limits above the federal floor to provide coverage to individuals who qualify based on the higher eligibility criteria for the Medicare Savings Programs.
Methodology
Data: This analysis uses data available from various data sources to identify dual-eligible individuals’ enrollment, spending, and chronic conditions. Data sources include:
- Dual-eligible enrollment and spending: KFF analytic files that merge the Centers for Medicare & Medicaid Services Chronic Conditions Data Warehouse 2022-2023 research-identifiable Master Beneficiary Summary File (MBSF) Base and the 2022-2023 Transformed Medicaid Statistical Information System (T-MSIS) Analytic Files (TAF) Research Identifiable Files (RIF) file using a Chronic Conditions Warehouse (CCW) beneficiary identifier crosswalk.
- Chronic condition counts for Medicare-only and dual-eligible individuals: 20% sample of Centers for Medicare & Medicaid Services Chronic Conditions Data Warehouse research-identifiable Master Beneficiary Summary File (MBSF) Base, Claims, and Medicare Advantage Encounter Data, 2022 (merged with T-MSIS data for dual-eligible individuals).
- Chronic condition counts for Medicaid-only and dual-eligible individuals: Transformed Medicaid Statistical Information System (T-MSIS) Analytic Files (TAF) Research Identifiable Files (RIF) file, 2022 (merged with MBSF and Medicare Advantage Encounter Data for dual-eligible individuals).
Identifying Dual-Eligible Individuals Using Medicare and Medicaid Administrative Data
- Preparing Medicaid data: Enrollee-level T-MSIS data for the 50 states and D.C. are stacked to create a national file. Enrollees are assigned to a Medicaid state using STATE_CD. Enrollees with missing national identifiers (BENE_ID) are dropped. In some cases, multiple unique records (MSIS_ID) in a state are assigned to the same national identifier (BENE_ID). To handle duplicates within a state, one unique record is selected based on non-missing key variables, and spending for all records associated with the national identifier (BENE_ID) are summed to determine total Medicaid spending on behalf of the enrollee in the state in the year.
- Preparing Medicare data: Using the MBSF, enrollees are identified using unique national identifiers (BENE_ID). Enrollees are assigned to a Medicare state using STATE_CODE.
- Merging prepared Medicaid and Medicare data: The prepared Medicaid and Medicare data files are merged using the CCW beneficiary identifier crosswalk which links an enrollee’s unique national identifier in T-MSIS to the enrollee’s unique national identifier in MBSF. All enrollees with a record in both files are kept. For enrollees with T-MSIS records in multiple states, KFF assigned the state that matched the Medicare state is selected. If no states match, the state with the highest spending is selected. Medicaid spending for all records associated with the national identifier (BENE_ID) are summed to determine total Medicaid spending on behalf of the enrollee in the year.
- Classifying dual-eligible individuals using merged file: Individuals are categorized as dual-eligible if they have matching records in both the MBSF and T-MSIS files. Dual-eligible individuals are assigned to full- or partial-benefit status as follows:
- Enrollees with at least one month of full Medicaid (defined as Medicare monthly DUAL_STUS_CD_MM values of 02,04,08), are assigned as full-benefit status.
- Enrollees have at least one month of partial Medicaid (defined as Medicare monthly DUAL_STUS_CD_MM values of 01,03,05,06), are assigned partial-benefit status.
- Dual-eligible enrollees that do not have full-benefit or partial-benefit status from the Medicare monthly DUAL_STUS_CD_MM, are assigned using the Medicaid monthly DUAL_ELGBL_CD_MM from T-MSIS (values 02,04,08 indicate full benefits and 01,03,05,06 indicate partial benefits). Similar to above, individuals with any months of full Medicare are full-benefit.
- Dual-eligible enrollees that are not assigned using either the Medicare or Medicaid dual status indicators, are classified using the monthly code RSTRCTD_BNFTS_CD_MM from T-MSIS (at least one month with RSTRCTD_BNFTS_CD_MM with values of 1,A,D,4,5,7 indicates full-benefit status, and all others are assigned partial-benefit status).
Enrollment and Spending for Dual-Eligible Individuals, based on Medicare Claims
- Enrollment Used to Calculate Shares: For dual-eligible enrollment as a share of total Medicare enrollment nationally and by state, we included beneficiaries in both traditional Medicare and Medicare Advantage.
- Spending: Medicare beneficiaries included in spending analyses had to meet the enrollment sample requirements and have no Medicare Advantage coverage during the year. Total Medicare spending was calculated as the sum of all Medicare Part A, Part B, and Part D service category payments in the MBSF Cost and Utilization Segment. Medicare spending (total and per person) does not include beneficiary cost-sharing liability.
Enrollment and Spending for Dual-Eligible Individuals, based on Medicaid Claims
- Enrollment Used to Calculate Shares: Dual-eligible individual enrollment and spending are reported as a share of total Medicaid enrollment and spending.
- Spending: Medicaid spending is derived from two data sources. T-MSIS spending includes Medicaid spending on fee-for-service spending on health care and payments to managed care plans. Data on Medicare premiums (which are not in T-MSIS) for Part A and Part B are estimated for dual-eligible individuals based on months of Medicare enrollment as a Medicaid beneficiary. Premiums change slightly year-to-year and are based on the amounts reported by CMS.
- Assigning Medicare Premiums to Medicaid Individuals: Data on Medicare premiums (which are not in T-MSIS) for Part A and Part B are estimated for dual-eligible individuals based on months of Medicare enrollment as a Medicaid beneficiary. Part A premiums were assigned to every month a dual-eligible individual had a monthly dual eligibility code of 05 and Part B premiums were assigned each month for which individuals had codes of 01, 02, 03, 04, or 06. Premiums change slightly year-to-year and are based on the amounts reported by CMS. For 2023, the Centers for Medicare & Medicaid Services reported monthly Part A premiums were $506 and monthly Part B premiums were $164.90.
Chronic Conditions for Dual-Eligible Individuals, based on Medicare and Medicaid claims
- Medicare and Medicaid Claims Data Used to Identify Chronic Conditions: Medicare fee-for-service and Medicare Advantage encounter data were used. Fee-for-service claims and encounters across all service types—inpatient, outpatient, carrier, home health, and skilled nursing facility—are included. Durable medical equipment encounters are excluded. The analysis incorporates Part D prescription drug event data, which provides information on fills of prescription drugs. Medicare Advantage encounters that were chart reviews, as identified using the Chart Review Switch and in-home health risk assessments, identified using HCPCS codes (GO438, GO402, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99350) and place of service codes (12, 13, 14, 16) were removed. T-MSIS inpatient, other, long-term care, and pharmacy data were used.
- Inclusion Criteria: All Medicaid enrollees were included in this analysis. Additional criteria was used to limit the sample of Medicare-only and dual-eligible individuals included in counting chronic conditions:
- Medicare-only Inclusion Criteria: Medicare enrollees were included if they are in the MBSF 20% sample. Medicare Advantage enrollees enrolled in plans where over 80% individuals did not have any utilization were removed from the sample.
- Dual-Eligible Individuals Inclusion Criteria: Dual-eligible individuals were included if (1) they were in both the MBSF and TMSIS files using the CCW crosswalk, (2) they were included in the MBSF 20% sample, (3) and they had full Medicaid benefits for at least one month throughout 2022.
- Medicare Advantage: Individuals who had at least one month of Medicare Advantage coverage in the year are considered Medicare Advantage enrollees.
- Defining Chronic Conditions: This analysis used the CCW algorithm for identifying chronic conditions in the Medicare Advantage Encounter data 20% sample in 2022, the Medicare fee-for-service data 20% sample in 2022, and the 2022 Transformed Medicaid Statistical Information System (T-MSIS) Analytic Files (TAF) Research Identifiable Files (RIF) file. This analysis also included in its definition of chronic conditions substance use disorder, mental health, obesity, HIV, hepatitis C, and intellectual and developmental disabilities. The counts of chronic conditions are higher than reported using other data, such as the Medicare Current Beneficiary Survey, because a larger set of conditions are included. In total, 29 chronic conditions were included:
- Behavioral health conditions: Any mental health condition and any substance use disorder. See KFF’s brief, “5 Key Facts About Medicaid Coverage for Adults with Mental Illness,” KFF brief “SUD Treatment in Medicaid: Variation by Service Type, Demographics, States and Spending,” and the Urban Institute, Behavioral Health Services Algorithm for additional details (Victoria Lynch, Lisa Clemans-Cope, Doug Wissoker, and Paul Johnson. Behavioral Health Services Algorithm. Version 4. Washington, DC: Urban Institute, 2024).
- Physical health conditions: Hypertension, transient ischemic attack, acute myocardial infarction, hyperlipidemia, ischemic heart disease, atrial fibrillation, heart failure, obesity, chronic obstructive pulmonary disease, pneumonia, asthma, diabetes, arthritis, hip fracture, osteoporosis, cataracts, glaucoma, chronic kidney disease, cancer (colorectal, endometrial, urologic, breast, prostate, or lung), benign prostatic hyperplasia, hepatitis, HIV, anemia, hypothyroidism.
- Cognitive impairment conditions: Alzheimer’s and/or dementia, intellectual and developmental delay, and Parkinson’s.