Interest in Using Over-the-Counter Oral Contraceptive Pills: Findings from the 2022 KFF Women’s Health Survey
Issue Brief
Introduction
In July 2022, Perrigo’s HRA Pharma submitted an application to the Food and Drug Administration (FDA) to make its progestin-only oral contraceptive (Opill) available over the counter (OTC). The typical review period is 10 months. If approved, it would be the first daily oral contraceptive pill approved for OTC use available in the U.S. Although it is farther behind in the process, another pharmaceutical company, Cadence, is working toward FDA approval of an OTC version of its combined oral contraceptive pill (Zena).
Oral contraceptives are the most commonly used method of reversible contraception in the U.S., and studies suggest that OTC access would increase use of contraception and facilitate continuity of use in addition to saving time spent on travel, at a doctor’s office, and off work. The American Medical Association and the American College of Obstetricians and Gynecologists support efforts to make an oral contraceptive pill available OTC, without age restrictions.
This brief presents data from the 2022 KFF Women’s Health Survey (WHS) about reproductive age (18-49) females’ preferences for an OTC contraceptive pill (N = 4,088). The KFF WHS is a nationally representative survey that includes 5,201 females1 , conducted primarily online from May 10, 2022, to June 7, 2022. The survey covers several topics related to reproductive health and well-being. See the Methodology section for details.
Findings
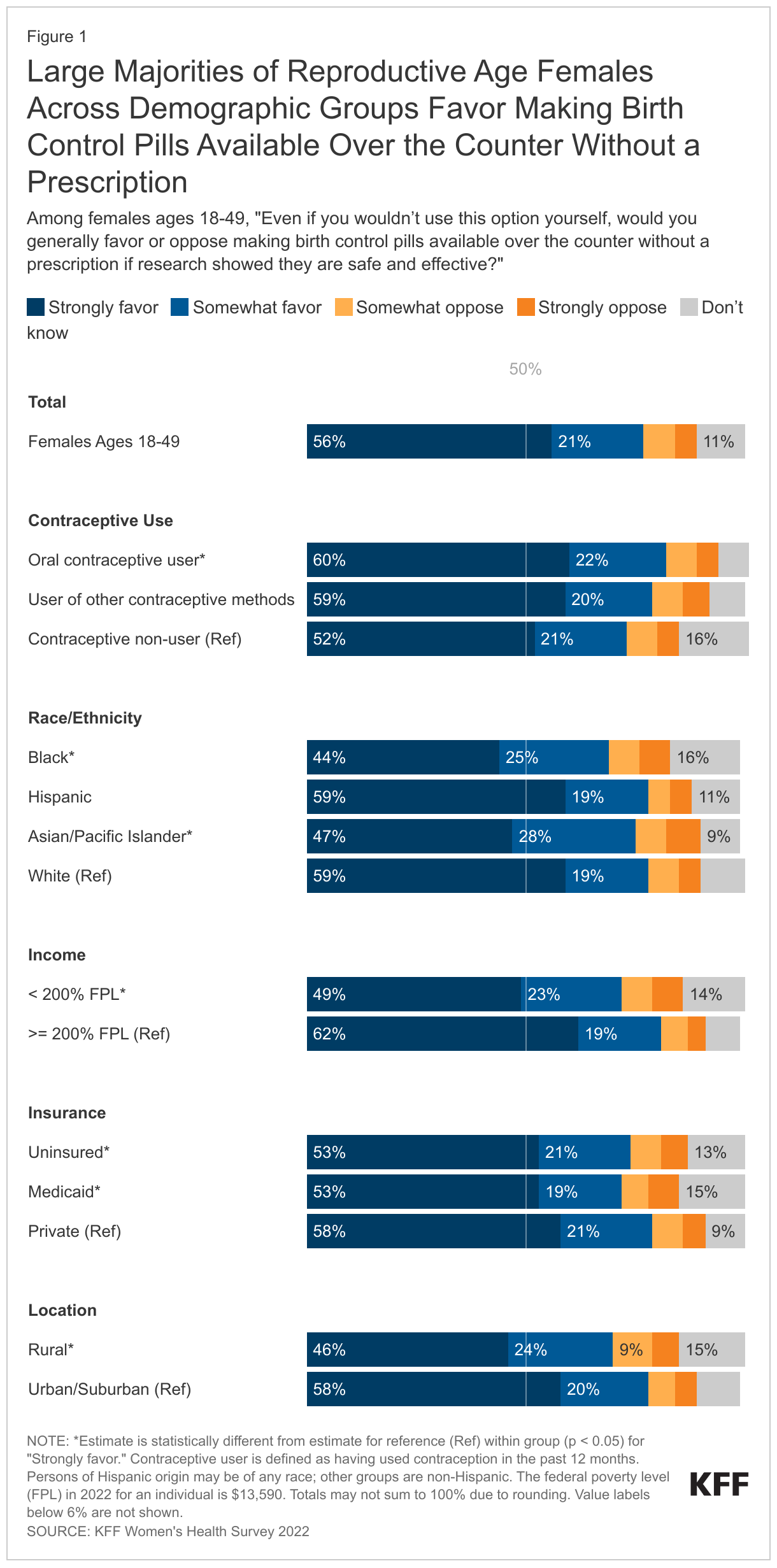
More than three-quarters (77%) of reproductive age females favor making birth control pills available over the counter without a prescription if research showed they are safe and effective (Figure 1). Fifty-six percent strongly favor this policy and 21% somewhat favor it, even if they would not use this option themselves. Twelve percent of females either somewhat or strongly oppose this policy and 11% did not know whether they favor or oppose it.
Larger shares of recent oral contraceptive users (60%) strongly favor making birth control pills available OTC compared to those who have not used contraception in the past 12 months (52%).
About six in ten (59%) White and Hispanic reproductive age females strongly favor making a birth control pill available OTC if research showed it is safe and effective compared to less than half of Black (44%) and Asian/Pacific Islander females (47%). Higher-income (>= 200% FPL) females (62%) are more likely than low-income (< 200% FPL) females (49%) to say that they strongly favor making birth control pills available OTC.2
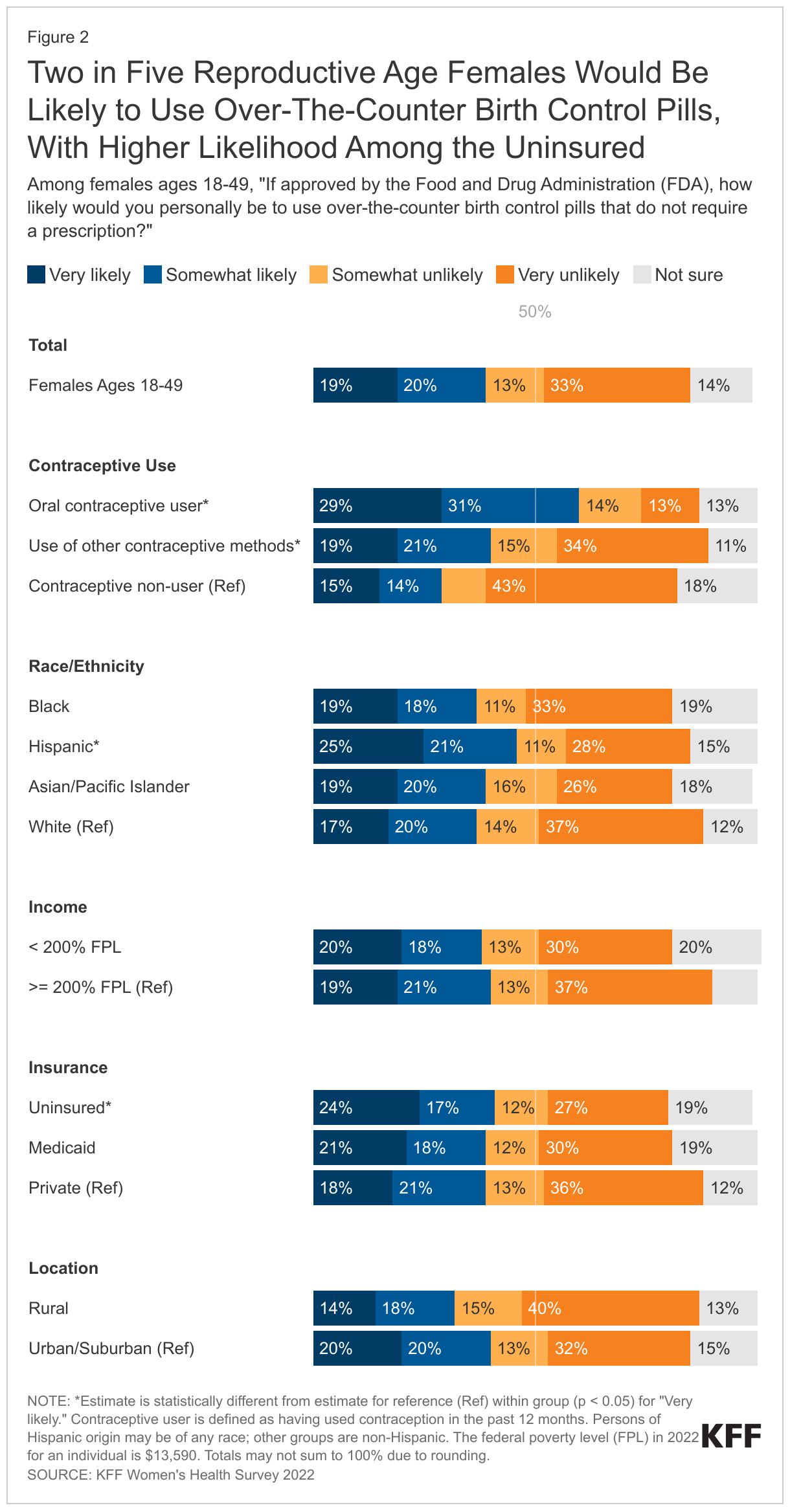
Two in five (39%) reproductive age females would be likely to use OTC birth control pills that do not require a prescription if approved by the FDA (Figure 2). One in five would be very likely (19%) or somewhat likely (20%) to use them. Almost half (46%) say they would be somewhat or very unlikely to use them and 14% do not know.
Interest is significantly higher among females who currently use oral contraceptives. Sixty percent of reproductive age females who have used birth control pills in the past 12 months said they would be likely or very likely to use OTC birth control pills compared to 40% of other contraceptive users and 29% of contraceptive non-users.
A higher share of reproductive age Hispanic females (25%) say they would be very likely to use OTC birth control pills if approved by the FDA than their White counterparts (17%). The share of low-income females who would be very likely to use OTC birth control pills is similar to the share of higher-income females (20% and 19%, respectively). One in four (24%) uninsured reproductive age females would be very likely to use them compared to about one in five (18%) of those with private health insurance. A higher share of females living in urban/suburban (20%) are very likely to use OTC birth control pills than rural females (13%).
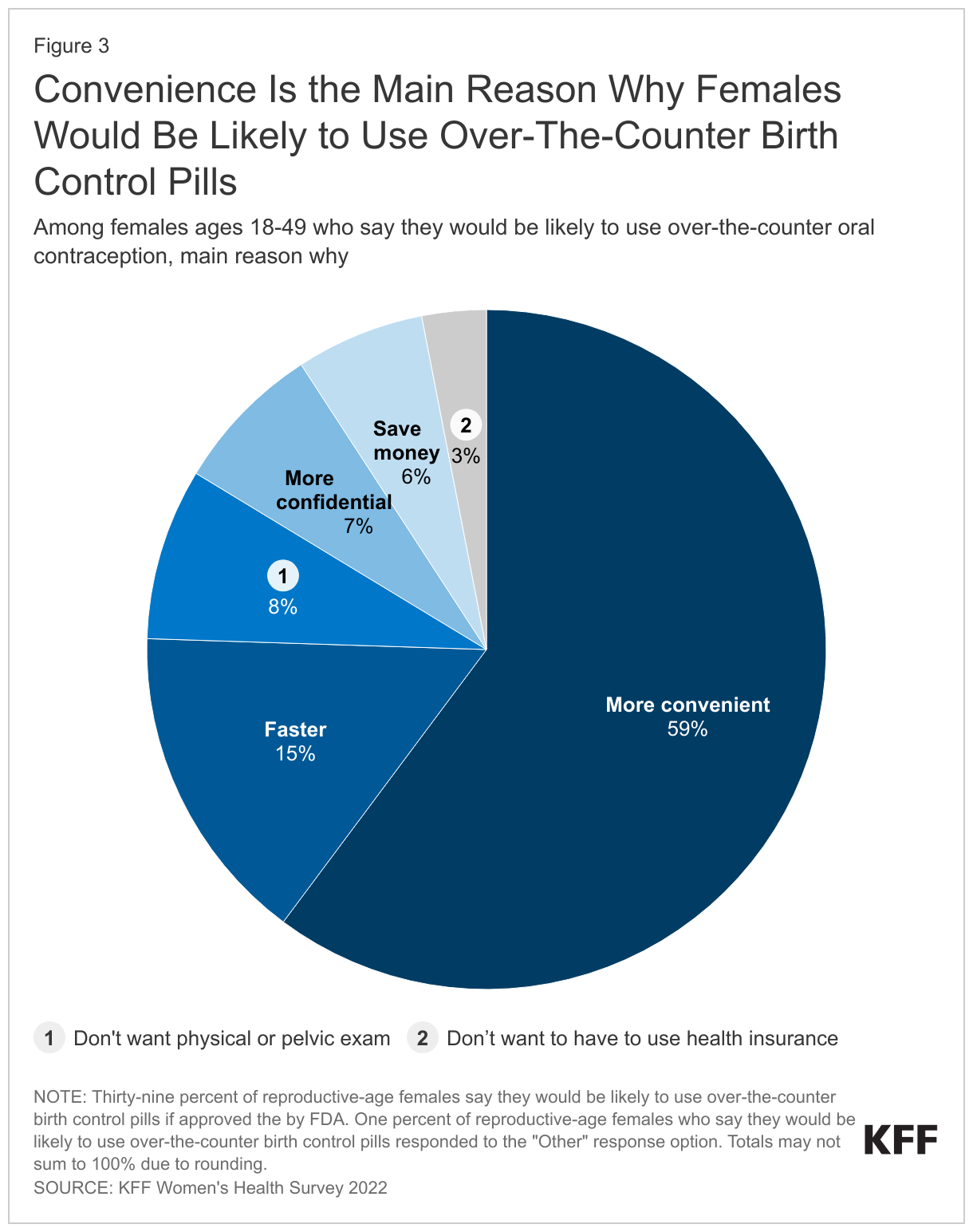
Convenience is the leading reason that reproductive age females say they would be somewhat or very likely to use OTC birth control pills (59%) (Figure 3). Fifteen percent believe it would be faster; 8% do not want to have to have a physical or pelvic exam; 7% say it would be more confidential; 6% think it would save money; and 3% do not want to use their health insurance to buy birth control pills.
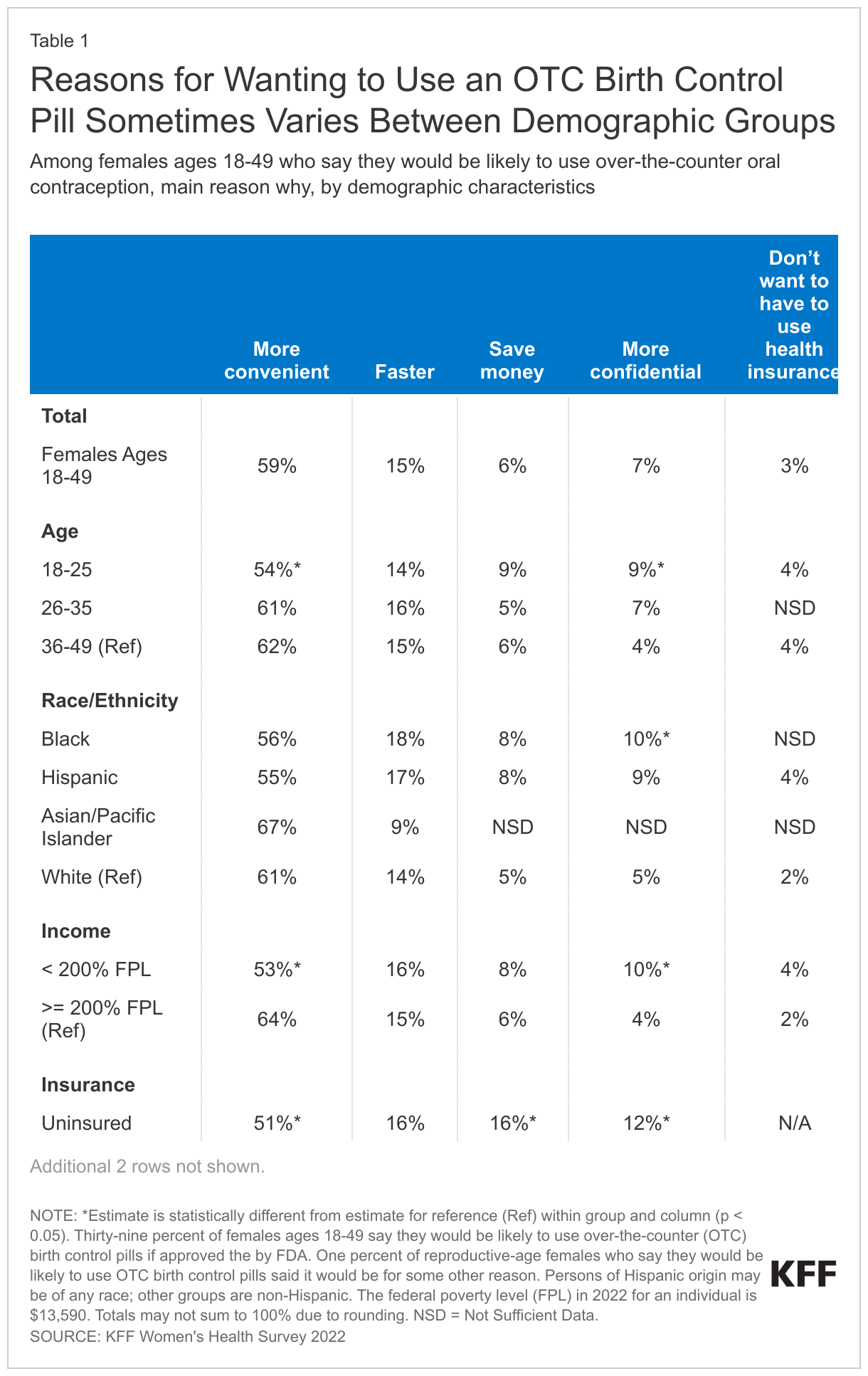
While convenience is the leading reason for wanting to use an OTC birth control pill across demographic groups, there are some differences within groups. Nearly two-thirds (64%) of higher-income (>= 200% FPL) reproductive age females who say they would be likely to use OTC birth control pills cite convenience as their main reason (Table 1). One in ten Black females (10%) and those ages 18 to 25 (9%) say their main reason is confidentiality, compared to 5% of White females and 4% of females ages 36-49. Sixteen percent of uninsured females say they would be likely to use OTC birth control pills mainly because they think it would save money, compared to 5% of those with private health insurance. Among reproductive age females likely to use OTC birth control pills, one in five (20%) with Medicaid say that it would be faster, compared to 13% of those with private insurance.
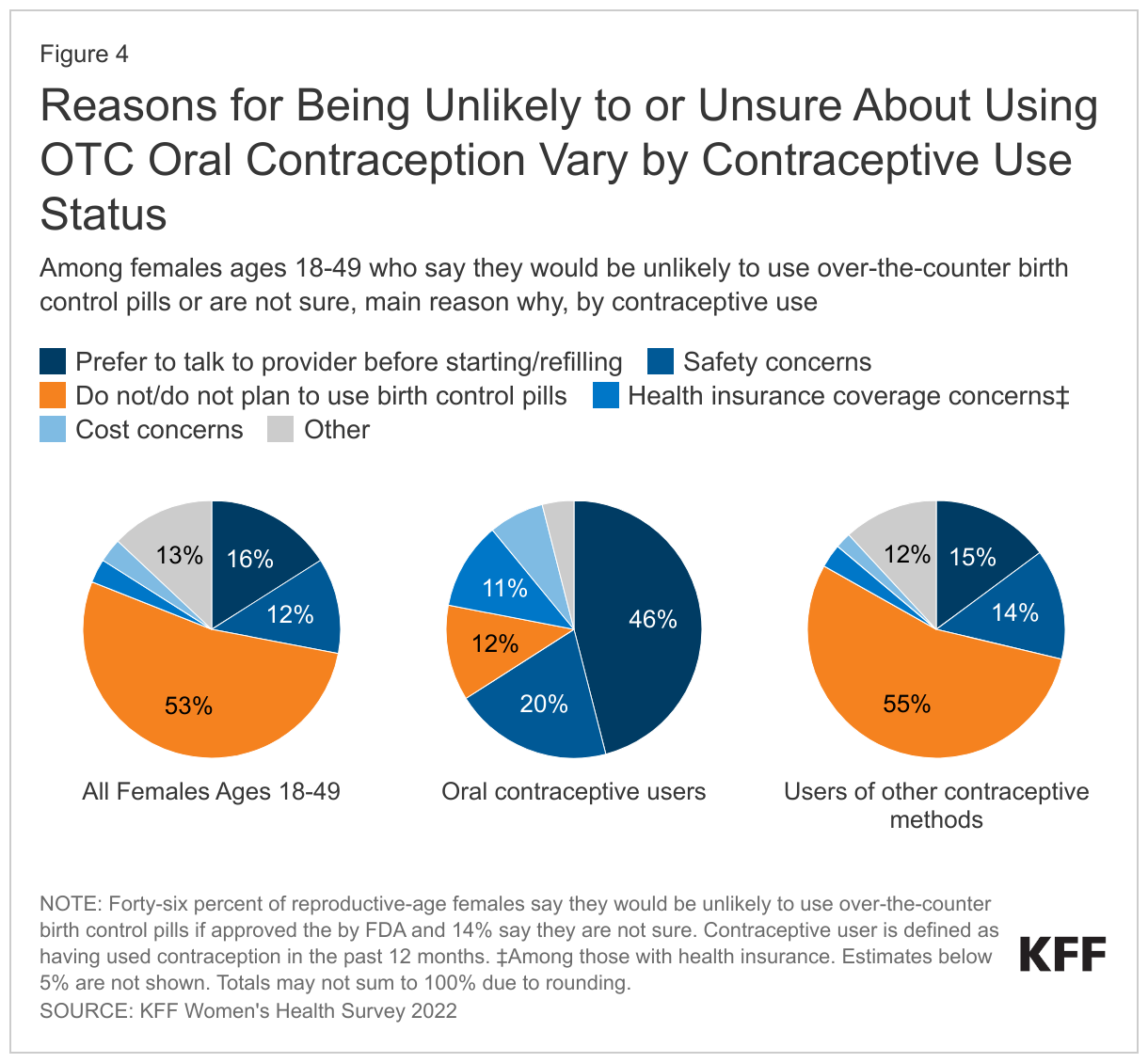
Among reproductive age females who say they would be somewhat or very unlikely to use OTC birth control pills without a prescription, or who are not sure, the majority (53%) say that the main reason is because they do not currently use birth control pills or do not plan to use them in the future (Figure 4). Sixteen percent say that they would prefer to talk to a health care provider before starting or refilling birth control pills; 12% cited safety concerns as the main reason they would be unlikely to use them; 3% said they would be concerned about the cost; and 3% would be concerned about whether their health insurance would cover them.
Thirteen percent of reproductive age females who are unlikely to or not sure if they would use OTC birth control pills without a prescription report that they are unlikely to use them for some other reason; common reasons include that they or their partner have had a sterilization procedure or that they prefer another method.
These estimates change, however, when looking at reproductive age females who have used oral contraceptives in the past 12 months and those who have used other methods of contraception. Among oral contraceptive users who say that they would be unlikely to use an OTC oral contraceptive or are not sure, the main reason is that they prefer to talk to a provider before starting or refilling birth control pills (46%), followed by safety concerns (20%). Among users of other contraceptive methods who say that they would be unlikely to use an OTC oral contraceptive or are not sure, the main reason is that they do not use or plan to use birth control pills (55%), followed by a preference for talking to a provider before starting or refilling birth control pills (15%).
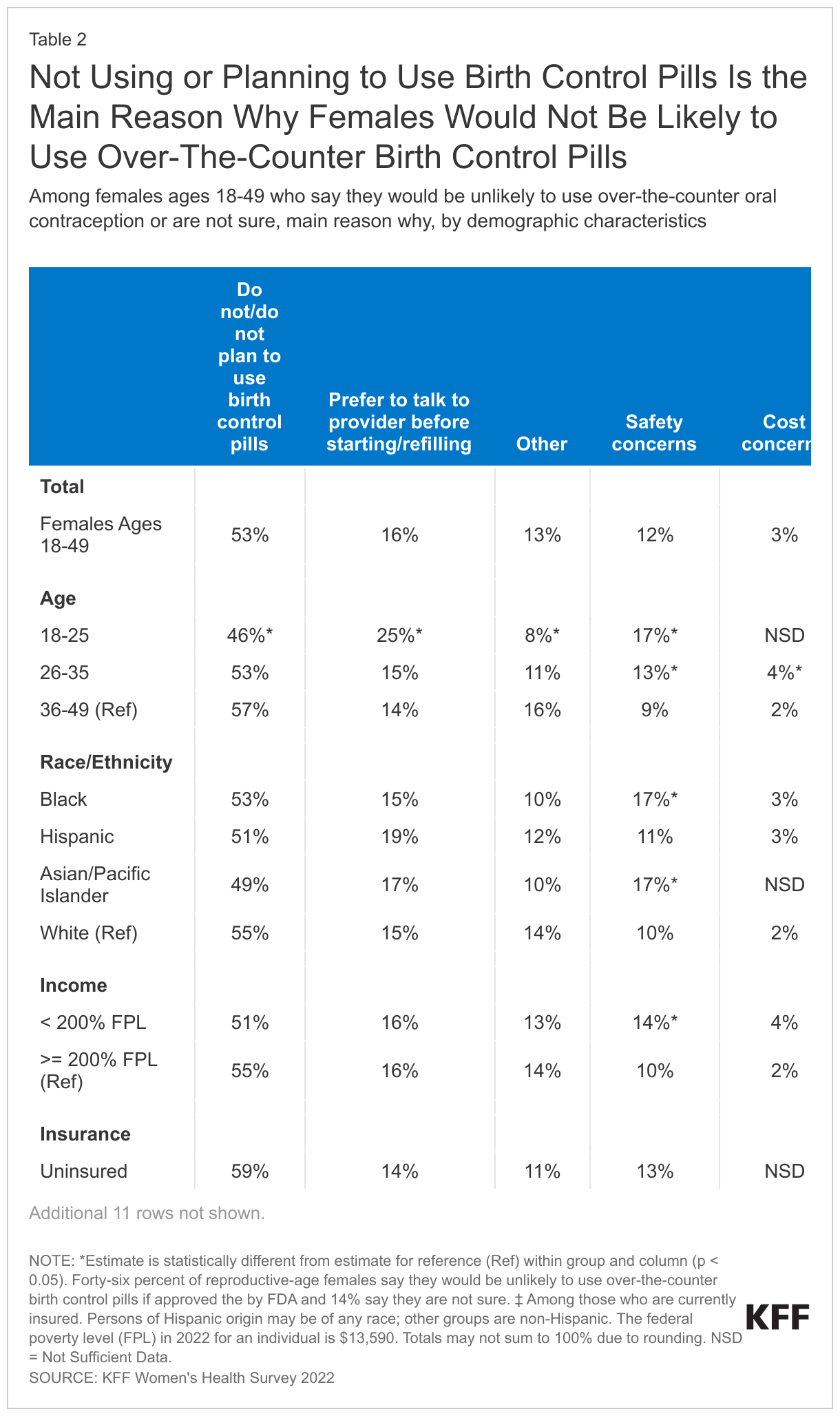
Among reproductive age females who say they would be unlikely to use OTC birth control pills without a prescription, or who are not sure, 17% of those ages 18-25 cite safety concerns as the main reason compared to 9% of those ages 36-49 (Table 2). A larger share of those ages 18 to 25 (25%) cites a preference to talk to a health care provider before starting or refilling birth control than those ages 36-49 (14%). Seventeen percent of Black and Asian/Pacific Islander females say that they have safety concerns, higher than the share of White females (10%) who have the same concern.
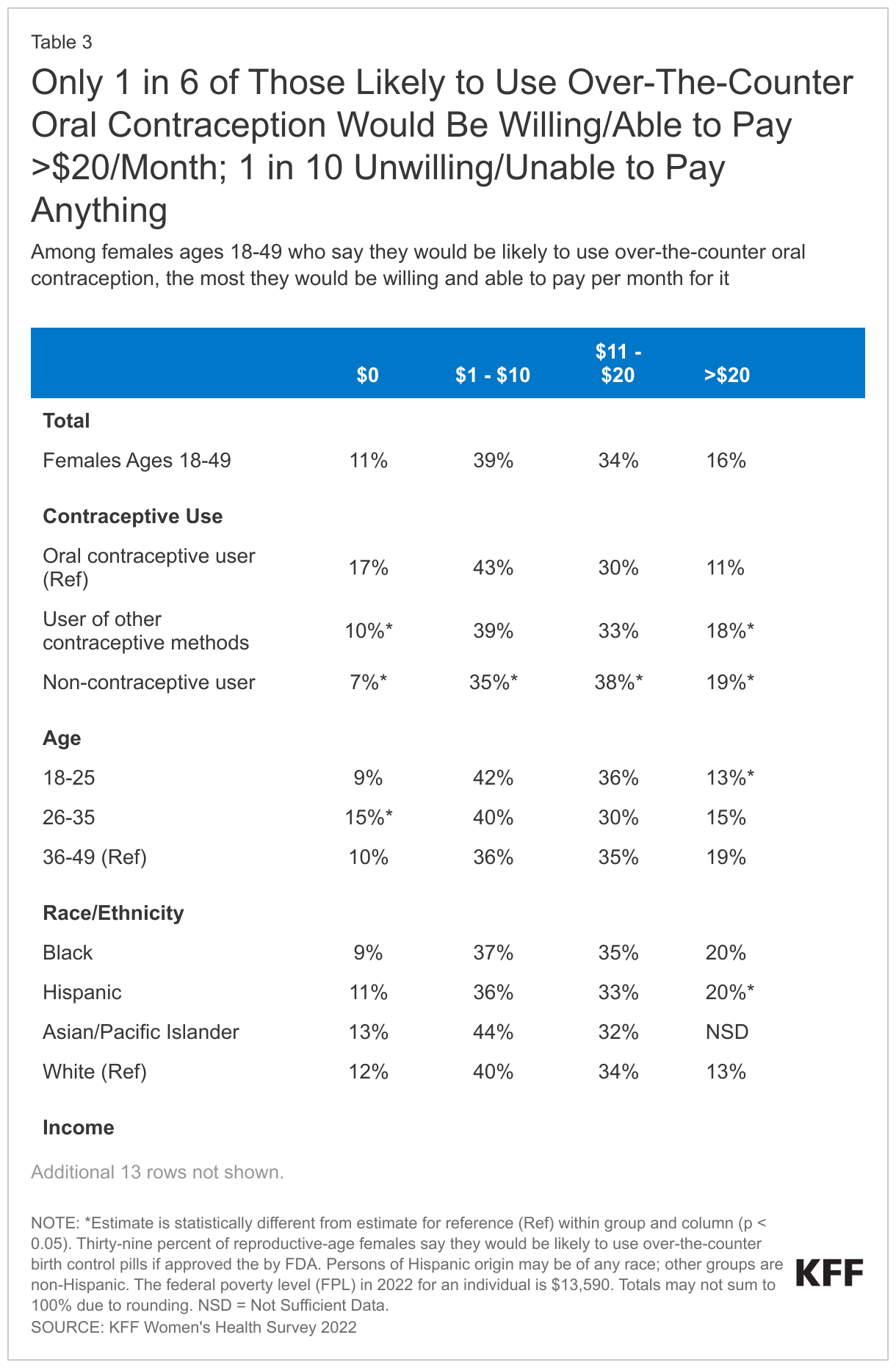
Among reproductive age females who report being likely to use OTC birth control pills, two in five (39%) would be willing and able to pay $1-$10 per month for them (Table 3). One-third (34%) would be willing and able to pay $11-$20 per month and 16% would pay more than $20. One in ten (11%) say they are unwilling or unable to pay anything for OTC birth control pills. Currently, most private insurance plans and Medicaid are required to cover the full cost of prescribed contraceptives.
Among those who say they are likely to use OTC birth control pills, 17% of oral contraceptive users say they would be unwilling or unable to pay anything for them, compared to 7% of contraceptive non-users. Nearly one in five (21%) uninsured females would pay more than $20 per month. Notably, there are no statistically significant differences by income level.
Looking Forward
There is broad support among females for an OTC oral contraceptive pill, and many are likely to use it. However, likely users are cost-sensitive, with only one in six willing and able to pay more than $20 per month for it and one in ten not willing or able to pay anything for it.
At the federal level, the Affordable Care Act requires most private health insurance plans to cover FDA-approved contraception for women; however, it must be prescribed in order for it to be covered. The most recent guidance about ACA implementation, issued by the Departments of Labor and Health and Human Services, and the Treasury in July 2022, states that plans and issuers are encouraged to cover OTC emergency contraceptive products with no cost sharing when they are purchased without a prescription, but the guidance does not currently require it.
At the state level, nine states currently require health plans regulated by the state, including fully-insured employer plans and individual plans, to cover OTC contraceptive medications without cost sharing, and without a prescription from a health care provider (three of those state laws apply to emergency contraception only). While no-cost coverage of prescription contraceptives has been required under Medicaid for decades, only six states and DC report covering OTC emergency contraception without a prescription in their Medicaid programs.
The pharmaceutical company that submitted an FDA application to switch from prescription-to-OTC status has not yet made price information publicly available. In addition to the retail cost, which will be an important consideration for those not using insurance, should a daily oral contraceptive pill become available OTC, accessibility and uptake will also depend on whether private health insurance and Medicaid cover it without a prescription.
Aside from the cost issues, many reproductive age women say they would still prefer to talk to a health care provider before starting or refilling birth control and others say they would still have safety concerns. These findings indicate that outreach and education will also play an important role in helping women understand their options in using an OTC oral contraceptive pill should the FDA approve the change in status.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methodology
Overview
The 2022 KFF Women’s Health Survey is a nationally representative survey of 6,442 people ages 18 to 64, including 5,201 females (self-reported sex at birth) and 1,241 males, conducted from May 10, 2022, to June 7, 2022. The objective of the survey is to help better understand respondents’ experiences with contraception, potential barriers to health care access, and other issues related to reproductive health. The survey was designed and analyzed by researchers at KFF (Kaiser Family Foundation) and fielded online and by telephone by SSRS using its Opinion Panel, supplemented with sample from IPSOS’s KnowledgePanel.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Questionnaire design
KFF developed the survey instrument with SSRS feedback regarding question wording, order, clarity, and other issues pertaining to questionnaire quality. The survey was conducted in English and Spanish. The survey instrument is available upon request.
Sample design
The majority of respondents completed the survey using the SSRS Opinion Panel (n=5,202), a nationally representative probability-based panel where panel members are recruited in one of two ways: (1) through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Group through the U.S. Postal Service’s Computerized Delivery Sequence. (2) from a dual-framed random digit dial (RDD) sample provided by Marketing Systems Group.
In order to have large enough sample sizes for certain subgroups (females ages 18 to 35, particularly females in the following subgroups: lesbian/gay/bisexual; Asian; Black; Hispanic; Medicaid enrollees; low-income; and rural), an additional 1,240 surveys were conducted using the IPSOS KnowledgePanel, a nationally representative probability-based panel recruited using a stratified ABS design.
Data collection
Web Administration Procedures
The majority of surveys completed using the SSRS Opinion Panel (n=5,056) and all of the surveys completed using the KnowledgePanel (n=1,240) were self-administered web surveys. Panelists were emailed an invitation, which included a unique passcode-embedded link, to complete the survey online. In appreciation for their participation, panelists received a modest incentive in the form of a $5 or $10 electronic gift card. All respondents who did not respond to their first invitation received up to five reminder emails and panelists who had opted into receiving text messages from the SSRS Opinion Panel received text message reminders.
Overall, the median length of the web surveys was 13 minutes.
Phone Administration Procedures
In addition to the self-administered web survey, n=146 surveys were completed by telephone with SSRS Opinion Panelists who are web reluctant. Overall, the median length of the phone surveys was 28 minutes.
Data processing and integration
SSRS implemented several quality assurance procedures in data file preparation and processing. Prior to launching data collection, extensive testing of the survey was completed to ensure it was working as anticipated. After the soft launch, survey data were carefully checked for accuracy, completeness, and non-response to specific questions so that any issues could be identified and resolved prior to the full launch.
The data file programmer implemented a “data cleaning” procedure in which web survey skip patterns were created in order to ensure that all questions had the appropriate numbers of cases. This procedure involved a check of raw data by a program that consisted of instructions derived from the skip patterns designated on the questionnaire. The program confirmed that data were consistent with the definitions of codes and ranges and matched the appropriate bases of all questions. The SSRS team also reviewed preliminary SPSS files and conducted an independent check of all created variables to ensure that all variables were accurately constructed.
As a standard practice, quality checks were incorporated into the survey. Quality control checks for this study included a review of “speeders,” reviewing the internal response rate (number of questions answered divided by the number of questions asked) and open-ended questions. Among all respondents, the vast majority (97%) answered 96% or more of the survey questions they received, with no one completing less than 91% of the administered survey (respondents were informed at the start of the survey that they could skip any question).
Weighting
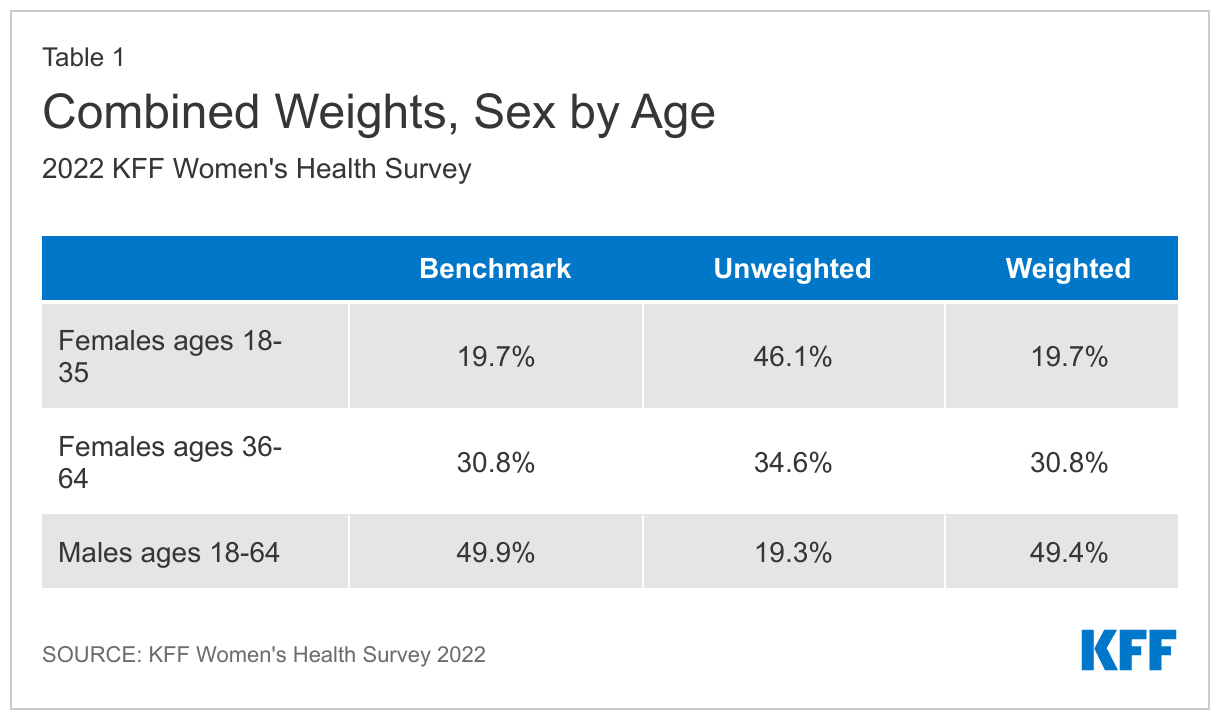
The data were weighted to represent U.S. adults ages 18 to 64. The data include oversamples of females ages 18 to 35 and females ages 36 to 64. Due to this oversampling, the data were classified into three subgroups: females 18 to 35, females 36 to 64, and males 18 to 64. The weighting consisted of two stages: 1) application of base weights and 2) calibration to population parameters. Each subgroup was calibrated separately, then the groups were put into their proper proportions relative to their size in the population.
Calibration to Population Benchmarks
The sample was balanced to match estimates of each of the three subgroups (females ages 18 to 35, females ages 36 to 64, and males ages 18 to 64) along the following dimensions: age; education (less than a high school graduate, high school graduate, some college, four-year college or more); region (Northeast, Midwest, South, West); and race/ethnicity (White non-Hispanic, Black non-Hispanic, Hispanic-born in U.S., Hispanic-born Outside the U.S., Asian non-Hispanic, Other non-Hispanic). The sample was weighted within race (White, non-Hispanic; Black, non-Hispanic; Hispanic; and Asian) to match population estimates. Benchmark distributions were derived from 2021 Current Population Survey (CPS) data.
Weighting summaries for females ages 18 to 35, females ages 36 to 64, and males ages 18 to 64 are available upon request.
Finally, the three weights were combined, and a final adjustment was made to match the groups to their proper proportions relative to their size in the population (Table 1).
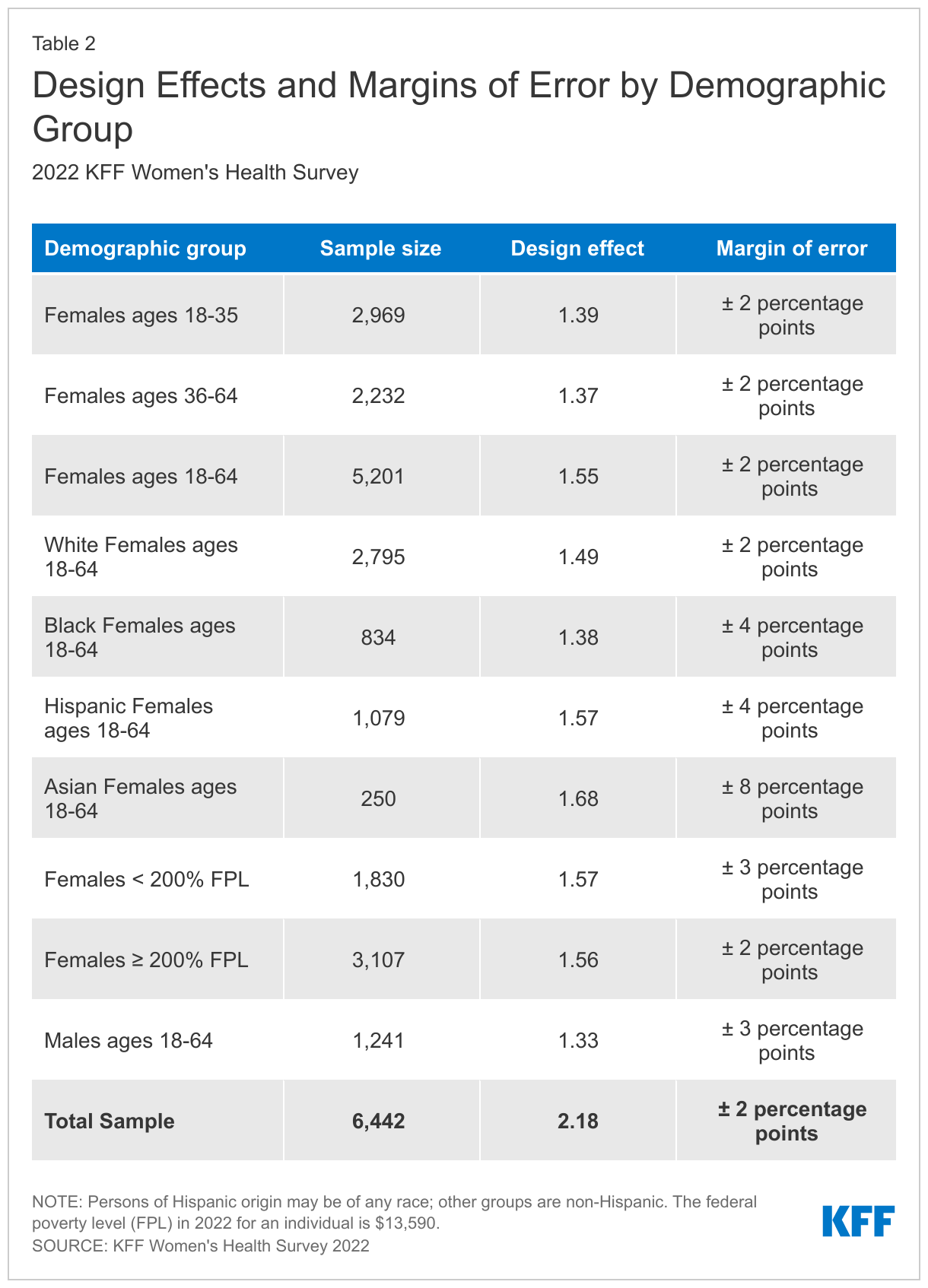
Margin of Sampling Error
The margin of sampling error, including the design effect for subgroups, is presented in Table 2 below. It is important to remember that the sampling fluctuations captured in the margin of error are only one possible source of error in a survey estimate and there may be other unmeasured error in this or any other survey.
KFF Analysis
Researchers at KFF conducted further data analysis using the R survey package, including creating constructed variables, running additional testing for statistical significance, and coding responses to open-ended questions. The survey instrument is available upon request.
Rounding and sample sizes
Some figures in the report do not sum to totals due to rounding. Although overall totals are statistically valid, some breakdowns may not be available due to limited sample sizes or cell sizes. Where the unweighted sample size is less than 100 or where observations are less than 10, figures include the notation “NSD” (Not Sufficient Data).
Statistical significance
All statistical tests are performed at the .05 confidence level. Statistical tests for a given subgroup are tested against the reference group (Ref.) unless otherwise indicated. For example, White is the standard reference for race/ethnicity comparisons and private insurance is the standard reference for types of insurance coverage. Some breakouts by subsets have a large standard error, meaning that sometimes even large differences between estimates are not statistically different.
A note about sex and gender language
Our survey asked respondents which sex they were assigned at birth, on their original birth certificate (male or female). They were then asked what their current gender is (man, woman, transgender, non-binary, or other). Those who identified as transgender men are coded as men and transgender women are coded as women. While we attempted to be as inclusive as possible and recognize the importance of better understanding the health of non-cisgendered people, as is common in many nationally representative surveys, we did not have a sufficient sample size (n >= 100) to report gender breakouts other than men and women with confidence that they reflect the larger non-cisgender population as a whole. The data in our reproductive health reports use the respondent’s sex assigned at birth (inclusive of all genders) to account for reproductive health needs/capacity (e.g., ever been pregnant) while the data in our other survey reports use the respondent’s gender.
Endnotes
- Respondents were asked their sex assigned at birth as well as their gender identity. This brief presents data on respondents who said they were assigned female at birth and includes all gender identities, including transgender, non-binary, and others. ↩︎
- The federal poverty level (FPL) in 2022 for an individual is $13,590. ↩︎