Racial and Ethnic Health Inequities and Medicare
Executive Summary
This chart collection draws on primary and secondary data analyses by KFF and other sources to examine the characteristics, experiences, and outcomes of the Medicare population by race and ethnicity (see Methods for details on data and analysis). It includes data from a variety of sources to describe demographics, health status and disease prevalence, health coverage, access to care and service utilization, and health outcomes, including the most current data available pertaining to disparities related to COVID-19 within the Medicare population. It also documents disparities in income and wealth among people on Medicare.
Key Takeaways
- Life expectancy at age 65 has improved since the enactment of Medicare among all older adults but is lower for Black adults than White or Hispanic adults (18.0, 19.4, and 21.4 years, respectively) and higher for Hispanic adults than Black or White adults.
- Overall, Black and Hispanic Medicare beneficiaries have fewer years of formal education and lower median per capita income, savings, and home equity than White beneficiaries.
- Among Medicare beneficiaries, people of color are more likely to report being in relatively poor health, have higher prevalence rates of some chronic conditions, such as hypertension and diabetes than White beneficiaries; they are also less likely to have one or more doctor visit, but have higher rates of hospital admissions and emergency department visits than White beneficiaries.
- While the vast majority of Medicare beneficiaries across all racial and ethnic groups have some source of supplemental coverage to help fill in Medicare’s benefit gaps and cost-sharing requirements, the share of beneficiaries with different types of coverage varies by race and ethnicity. A smaller share of Black and Hispanic Medicare beneficiaries than White beneficiaries have private supplemental coverage through Medigap or retiree health plans, while a larger share have wrap-around coverage under Medicaid; a larger share of Black and Hispanic than White beneficiaries are enrolled in Medicare Advantage plans
- While relatively few Medicare beneficiaries overall report problems with access to care, a larger share of Black and Hispanic beneficiaries report trouble getting needed care than White beneficiaries.
- The COVID-19 pandemic has further highlighted stark racial/ethnic health inequities among Medicare beneficiaries, with Black, Hispanic, and American Indian/Alaska Natives accounting for disproportionate rates of COVID-19 cases and hospitalizations. Among adults ages 65 and older, people of color bear disproportionate rates of COVID-19 deaths relative to older White adults.
Report: Overview
Medicare is a national health insurance program that provides coverage to more than 60 million people ages 65 years and older and younger adults with long-term disabilities, including 15 million beneficiaries who are people of color. Medicare covers a broad range of health services, including hospital and physician services, preventive services, skilled nursing facility and home health care, hospice, and prescription drugs. While Medicare has been instrumental in providing adults access to medical care, racial disparities in diagnoses, treatment, and outcomes among beneficiaries persist and have been exacerbated by the coronavirus pandemic.
Medicare has helped to mitigate racial and ethnic inequities in health care in its role as both a regulator and the largest single purchaser of personal health care in the U.S. Prior to the establishment of Medicare, half of older adults lacked health insurance. Soon after its enactment in 1965, Medicare facilitated the integration of hospitals by enforcing Title VI of the Civil Rights Act, which prohibits the distribution of federal funds to institutions that practice discrimination.1 Before then, many hospitals were segregated, and in many parts of the country, Black physicians were unable to practice in hospitals in their community.2 As Dorothy Height, an American civil and women’s rights activist, observed, “the combination of Medicare, Medicaid and the civil rights legislation changed the health care landscape forever for Black Americans and minorities of all ages. Everyone benefited from these policies.”
However, as the coronavirus pandemic has laid bare, racial and ethnic inequities in health and health care persist, including among people with Medicare. Among adults ages 65 and over, COVID-19 related mortality rates for Black and Hispanic adults are nearly double the rate for White adults. In the Medicare population, which includes both older adults and younger adults with long-term disabilities, Black, Hispanic, and American Indian and Alaska Native beneficiaries have borne a disproportionate burden of COVID-19 cases and hospitalizations.
Long before the COVID-19 pandemic, numerous studies documented health inequities among Medicare beneficiaries by race and ethnicity, even after controlling for multiple factors, such as age, sex, and comorbidities. For example, Black Medicare beneficiaries have higher hospital readmission rates than White beneficiaries even after controlling for multiple patient-level factors,3 , 4 , 5 and in some studies, these disparities persist even within the same hospital or skilled nursing facility,6 ,7 suggesting that systemic-level factors are driving forces behind these disparities. Moreover, studies have documented racial/ethnic disparities in cancer survival rates and receipt of optimal treatments.8 , 9 , 10 , 11 ,12
Health inequities among Medicare beneficiaries are attributed to broader structural, socioeconomic, political, and environmental factors that are rooted in years of systemic racism. Socioeconomic disadvantages associated with structural racism shape health outcomes among people of color long before the age of Medicare eligibility is reached and have a cumulative effect over the course of a lifetime, contributing to ongoing or greater inequities in older ages.13 ,14
This chart collection draws on primary and secondary data analyses by KFF and other sources to examine the characteristics, experiences, and outcomes of the Medicare population by race and ethnicity (see Methods for details on data and analysis). It includes data from a variety of sources to describe demographics, health status and disease prevalence, health coverage, access to care and service utilization, and health outcomes, including the most current data available pertaining to disparities related to COVID-19 within the Medicare population. It also documents disparities in income and wealth among people on Medicare.
While the collection of race and ethnicity data in administrative and survey data has improved over time, sample size and data collection limitations, including limitations related to completion, accuracy, and classifications of race/ethnicity data, preclude analysis of certain racial and ethnic groups consistently across data sources. Further, gaps in data reporting and collection standards, such as the reporting of COVID-19 cases and deaths in nursing homes by race and ethnicity, impede the complete identification of racial and ethnic disparities. These data limitations affect our ability to display results for a consistent set of racial and ethnic groups in this chart collection, especially for Asian, American Indian and Alaska Native, and Native Hawaiian and Other Pacific Islander beneficiaries, and beneficiaries who identify as two more races in some of our analyses. Moreover, due to these data limitations, we are unable to present more nuanced and disaggregated data that reflect the heterogeneity within different racial and ethnic groups. For example, researchers have documented differences in health outcomes within Hispanic subgroups, such as those identifying as Mexican, Cuban, Puerto Rican, Dominican, and Central/South American, that would otherwise be masked.15 ,16 Throughout this brief, individuals of Hispanic origin may be of any race, but are classified as Hispanic for the analysis; all other groups are non-Hispanic.
Report: Demographics
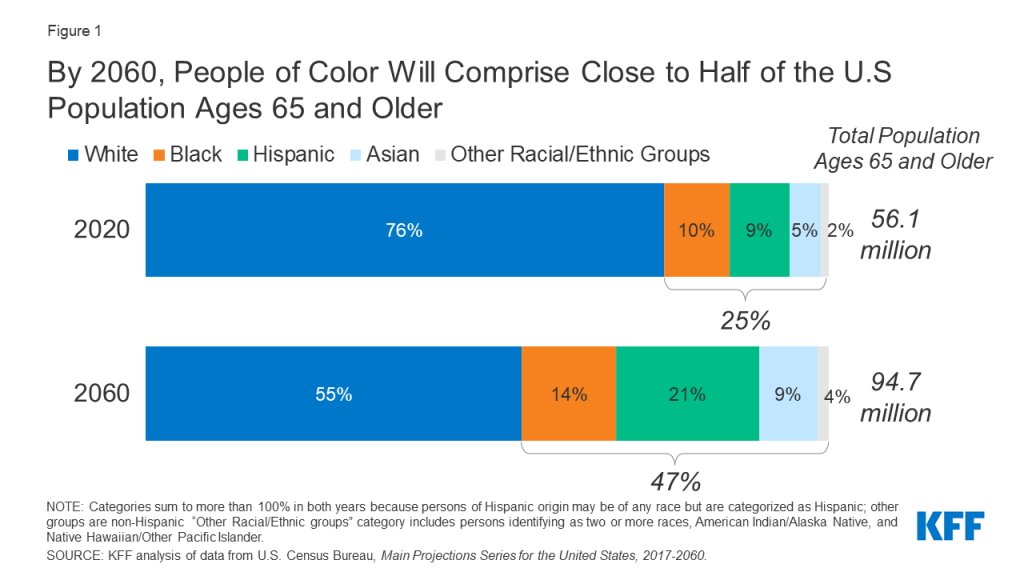
By 2060, People of Color Will Comprise Close to Half of the U.S Population Ages 65 and Older
The population of the United States ages 65 and older is projected to grow from 56 million in 2020 to 95 million in 2060, accounting for nearly a quarter of the nation’s total population in 2060.
The U.S population ages 65 and over is also expected to become more diverse over time. Between 2020 and 2060, White adults are projected to account for a decreasing share of adults ages 65 and older, with their population declining from 76% to 55%, while the share of adults ages 65 and older who are people of color is projected to nearly double, from 25% to 47%. Much of this increase reflects growth in the older Hispanic adult population, with the share of adults ages 65 and older who are Hispanic projected to more than double over the next four decades, from 9% in 2020 to 21% in 2060 (Figure 1).
The Average Number of Years of Life Remaining at Age 65 Is Substantially Lower for Black Adults Than for White or Hispanic Adults
In 2018, adults in the U.S who reached age 65 were expected to live an additional 19.5 years on average –reflecting a 5-year gain in life expectancy since 1960, prior to the enactment of Medicare.17
However, life expectancy at age 65 is lower among Black adults (18 years) than among White adults (19.4 years) and Hispanic adults (21.4 years) (Figure 2). Among adults in all three groups, life expectancy at age 65 is higher for women than men.
Notably, Hispanic male and female adults have the highest life expectancy at age 65, despite being socioeconomically disadvantaged compared to White adults. Research has, in part, attributed this advantage (i.e., “Hispanic paradox”18 ) to lower smoking rates and other positive health behaviors among Hispanic adults relative to other groups, as well as immigration-related processes that indirectly select healthier immigrants.19 However, these findings are still not fully understood. Researchers have also projected that among Hispanic adults born in the United States, this life expectancy advantage is expected to diminish due to increasing prevalence of obesity.20
The Majority of Medicare Beneficiaries Are White Adults, While 24% Are People of Color
In 2018, there were 60.9 million Medicare beneficiaries in total, including adults ages 65 and older and younger adults living with a long-term disability. A majority of Medicare beneficiaries are White, while 24% are people of color. This includes 10% (6 million) Black beneficiaries, 8% (5.1 million) Hispanic beneficiaries, and 6% (3.7 million) beneficiaries in other racial and ethnic groups, including Asian, Native Hawaiian or Other Pacific Islander, and American Indian or Alaska Native people as well as people identifying two or more races (Figure 3).
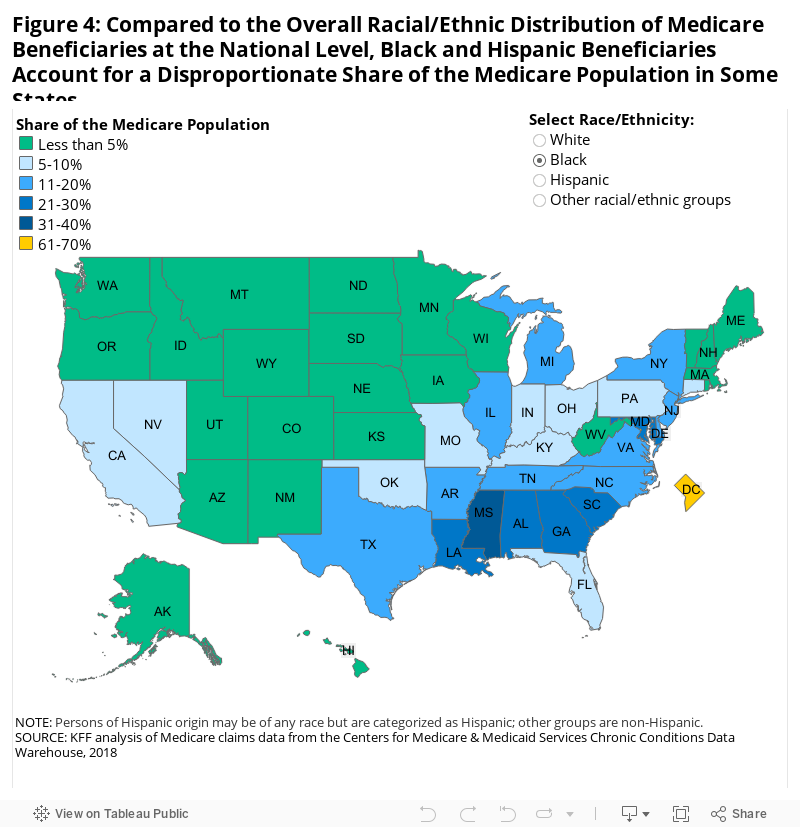
Compared to the Racial/Ethnic Distribution of Medicare Beneficiaries at the National Level, Black and Hispanic Beneficiaries Account for a Disproportionate Share of the Medicare Population in Some States
While the Medicare population in all states is predominantly White, Black and Hispanic beneficiaries account for a disproportionate share of the Medicare population in some states, relative to the racial/ethnic distribution of Medicare beneficiaries at the national level (Table 1, Figure 4). Black adults account for 11% of the Medicare population nationally, but a larger share in 14 states and the District of Columbia, and less than 5% in 22 states. Notably, the share of Black adults in the Medicare population in the District of Columbia (63%) is nearly six times higher than the national average (Table 1). Hispanic adults account for 8% of the Medicare population nationally, but a larger share in nine states, and less than 5% in 35 states and the District of Columbia. In large part, these distributions of Medicare beneficiaries by race and ethnicity reflect the variation in the racial and ethnic composition of the U.S population across states.
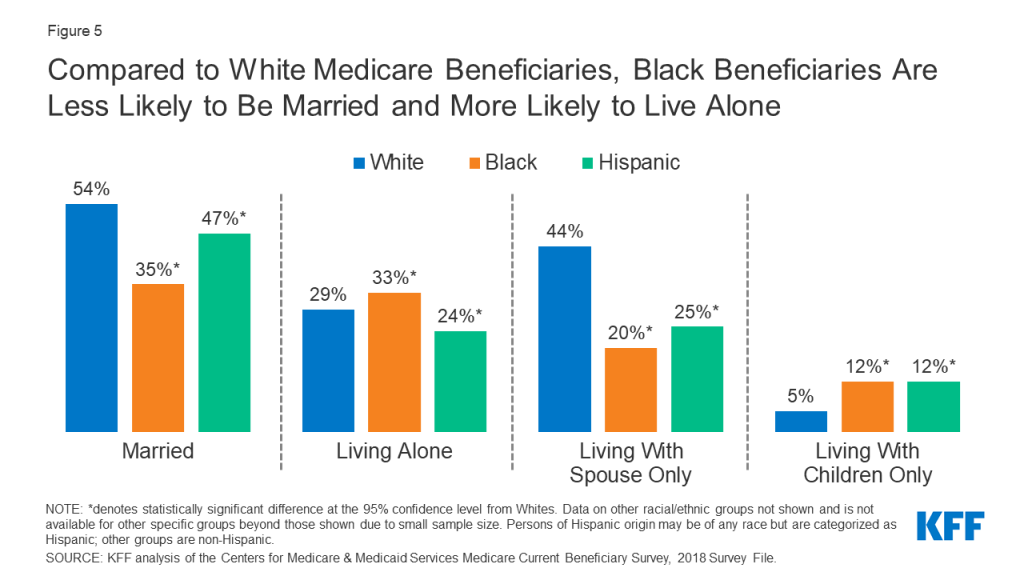
Compared to White Medicare Beneficiaries, Black Beneficiaries Are Less Likely to Be Married and More Likely to Live Alone
Household living arrangements of Medicare beneficiaries differ by race and ethnicity. Researchers have considered living alone as a potential predisposing factor for social isolation, which is a risk factor for poor health outcomes.21
Compared to White beneficiaries, Black beneficiaries are more likely to live alone (54% versus 33%, respectively) (Figure 5). Conversely, smaller shares of Black and Hispanic beneficiaries are married than White beneficiaries (35%, 47%, and 54%, respectively), with Black and Hispanic beneficiaries being less likely to be living with just their spouse compared to White beneficiaries.
Larger Shares of Black and Hispanic Medicare Beneficiaries Are Under Age 65 and Living with a Long-Term Disability Compared to White Beneficiaries
The vast majority (86%) of Medicare beneficiaries are ages 65 and older, while 14% are under age 65 and qualify for Medicare due to a long-term disability.
Larger shares of Black (25%) and Hispanic (19%) beneficiaries are under age 65 compared to White beneficiaries (12%) (Figure 6). Beneficiaries under age 65 are more likely than older adults to have lower incomes, report fair or poor health status, and have a cognitive or mental impairment, regardless of race/ethnicity.

Report: Education, Poverty, And Wealth
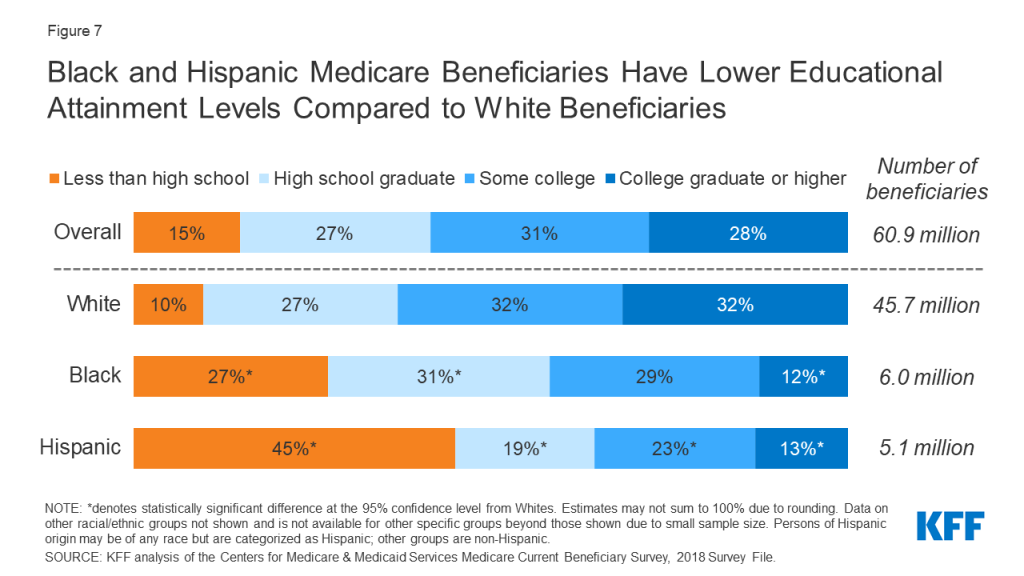
Black and Hispanic Medicare Beneficiaries Have Lower Educational Attainment Levels Compared to White Beneficiaries
Educational attainment, one of the key social determinants of health, varies by race and ethnicity, with Black and Hispanic beneficiaries having fewer years of education compared to White beneficiaries.
More than one quarter of Black (27%) Medicare beneficiaries and nearly one half (45%) of Hispanic beneficiaries have less than a high school education, compared to 10% of White beneficiaries (Figure 7). Conversely, a much smaller share of Black (12%) and Hispanic (13%) beneficiaries than White beneficiaries (32%) have a college degree or higher.
Nearly Half of Older Hispanic and Black Adults Have Family Incomes Below 200% of the Poverty Threshold—Nearly Double the Rate Among Older White Adults
Among people ages 65 and older, Black and Hispanic adults are more likely than older White adults to have family income below poverty, based on both the official poverty measure and the Supplemental Poverty Measure (SPM).
Based on the official poverty measure, nearly half of older Black and Hispanic adults (51% and 49%, respectively) have family incomes below 200% of poverty, compared to just over one quarter (29%) of older White adults (Figure 8).
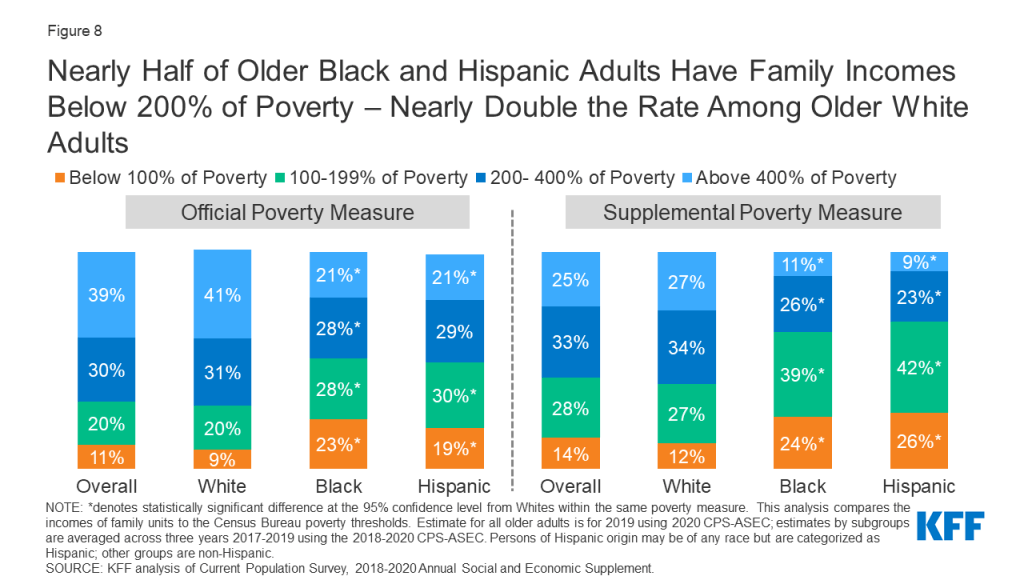
The share of Black and Hispanic adults with family income below poverty is higher based on the SPM than under the official poverty measure. The SPM differs from the official poverty measure in that it takes into account several additional financial resources, including in-kind government benefits (e.g., food stamps, housing subsidies), tax credits, out-of-pocket medical expenses, work expenses, homeownership, and geographic variation in housing costs. The SPM also deducts medical out-of-pocket expenses from financial resources, which is an especially important factor in calculating income for older adults. Based on the SPM, 63% of older Black adults and 68% of older Hispanic adults have incomes below 200% of poverty, compared to 39% of older White adults.
Median Per Capita Income, Savings, and Home Equity are Higher for White Beneficiaries Than for Black or Hispanic Beneficiaries
In 2019, half of all Medicare beneficiaries had incomes below $29,655 per person, savings below $73,819 per person, and home equity below $75,346 per person (Figure 9).
Median per capita income among White beneficiaries ($33,718) was double that of Hispanic beneficiaries ($15,611) and 1.5 times higher than median per capita income among Black beneficiaries ($23,050).
The wealth gap, based on median per capita home equity and savings, was notably wider. Median per capita savings among White beneficiaries ($117,803) was more than eight times higher than savings among Black beneficiaries ($14,523) and about twelve times higher than savings among Hispanic beneficiaries ($9,634). Median per capita home equity was more than five times higher among White beneficiaries ($95,001) than among Black beneficiaries ($18,454) or Hispanic beneficiaries ($16,494). Lower savings and home equity among people of color on Medicare than among White Medicare beneficiaries, in part, reflects fewer opportunities among Black and Hispanic adults to accumulate wealth and transfer wealth from one generation to the next.22 ,23 ,24
A Wide Racial and Ethnic Disparity in Per Capita Savings Persists Even Among People on Medicare With a College Degree
While educational attainment has been considered by some as a pathway to improving wealth attainment, large racial and ethnic wealth gaps among Medicare beneficiaries persist even among beneficiaries who have attained the highest level of formal education.
Among beneficiaries with a college degree or higher, median per capita savings among White beneficiaries ($328,348) were four times higher than among Black beneficiaries ($82,050) and almost five times higher than among Hispanic beneficiaries ($67,777) (Figure 10). The persistence of the racial wealth gap even at the highest education level reinforces the role of other factors, including structural racism, in generating inequities in Medicare beneficiaries’ financial security.
Report: Health Status And Disease Prevalence
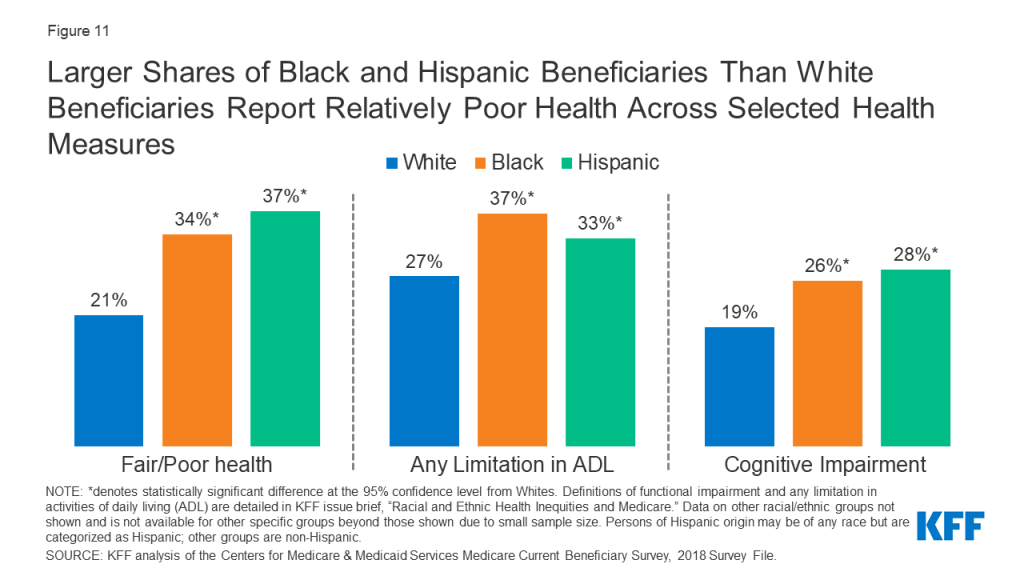
Larger Shares of Black and Hispanic Beneficiaries Than White Beneficiaries Report Relatively Poor Health Across Selected Health Measures
More than a third of Black and Hispanic beneficiaries (34% and 37%, respectively) report being in fair or poor health, compared to 21% of White beneficiaries (Figure 11). Black and Hispanic beneficiaries are more likely than White beneficiaries to have any limitation in activities of daily living (37%, 33%, and 27%, respectively), which is defined as difficulty performing any activities of daily living (e.g., bathing, eating). Limitations in activities of daily living are associated with increased risk of hospitalization, admission to a long-term care facility, and mortality among Medicare beneficiaries.25 ,26 Additionally, a larger share of Black (26%) and Hispanic (28%) beneficiaries than White beneficiaries (19%) have a cognitive impairment.
Black and Hispanic Beneficiaries have Higher Prevalence Rates of Certain Chronic Conditions Than White Beneficiaries
The prevalence of certain diseases and chronic conditions varies by race and ethnicity among Medicare beneficiaries. Hypertension is highly prevalent among all Medicare beneficiaries (63%); however, Black and Hispanic beneficiaries have higher rates of hypertension than White beneficiaries (79%, 65%, and 60%, respectively) (Figure 12, Table 3). Additionally, close to half of Black and Hispanic beneficiaries have diabetes, compared to 30% of White beneficiaries. Research has shown that among Medicare beneficiaries with diabetes, Black and Hispanic beneficiaries have the highest amputation rates.27 While the prevalence of stroke is low among all Medicare beneficiaries, the rate is higher among Black beneficiaries than White beneficiaries.
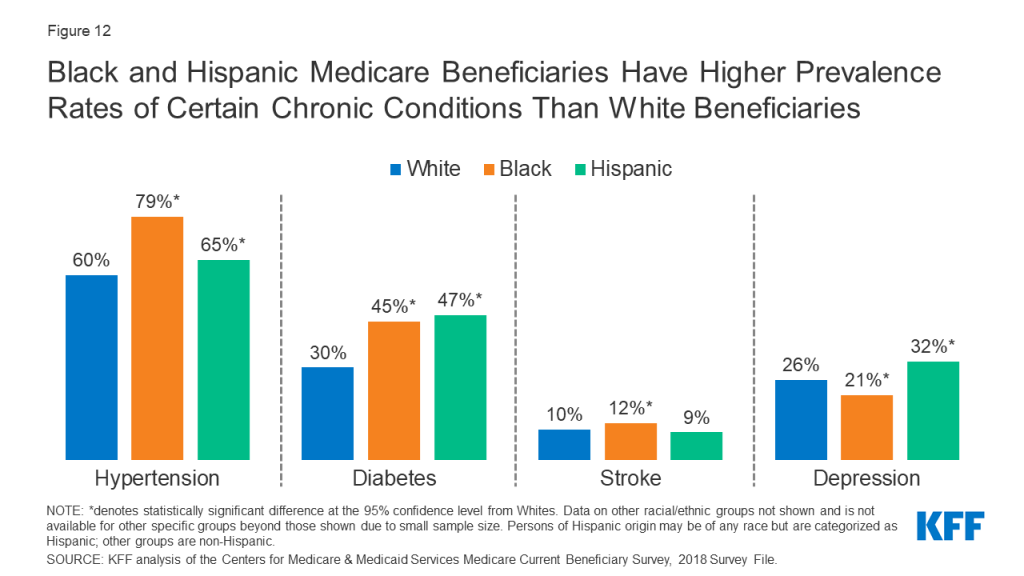
For other conditions, Black and/or Hispanic beneficiaries have lower prevalence rates than White beneficiaries, including cancer, where prevalence rates are 15% for both Black and Hispanic beneficiaries and 19% for White beneficiaries (Table 3). While a larger share of Hispanic beneficiaries (32%) than White (26%) beneficiaries report depression, a smaller share of Black beneficiaries (21%) report depression compared to White beneficiaries. Hispanic beneficiaries have lower prevalence rates of heart disease (25%) and pulmonary disease (16%) than White beneficiaries (33% and 20%, respectively) (Table 3).
Report: Sources Of Coverage Among Medicare Beneficiaries
Black and Hispanic Medicare Beneficiaries Are Less Likely Than White Beneficiaries to Have Private Supplemental Insurance, but More Likely to Have Wrap-Around Medicaid coverage or Be Enrolled in Medicare Advantage
The vast majority of Medicare beneficiaries across all racial and ethnic groups have some source of supplemental coverage. However, sources of supplemental coverage in Medicare vary by race and ethnicity. While a quarter of White beneficiaries have Medigap, also known as Medicare Supplement Insurance, only 5% of Black beneficiaries and 7% of Hispanic beneficiaries do so (Figure 13, Table 2). Medigap helps to fill in the gaps in traditional Medicare by fully or partially covering Part A and Part B cost-sharing requirements. Black and Hispanic beneficiaries are also less likely than White beneficiaries to have employer or union-sponsored retiree health benefits to supplement Medicare.
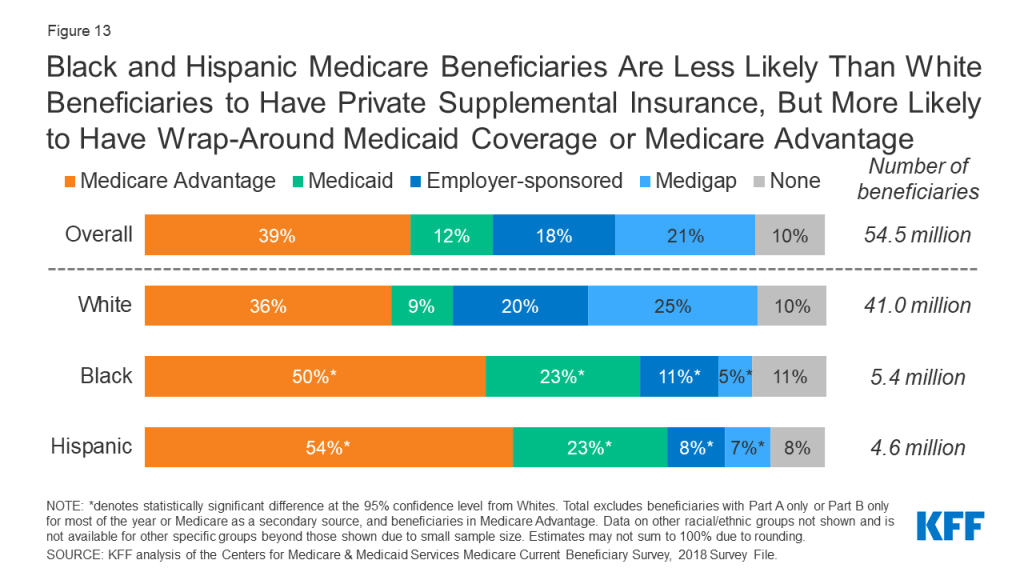
Medicaid provides supplemental coverage to nearly a quarter (23%) of Black and Hispanic beneficiaries, the federal-state program that provides coverage to low-income people, compared to just 9% of White beneficiaries. Additionally, half of Black (50%) and Hispanic (54%) beneficiaries were enrolled in a Medicare Advantage plan in 2018, as compared to just over one third of all White beneficiaries (36%).
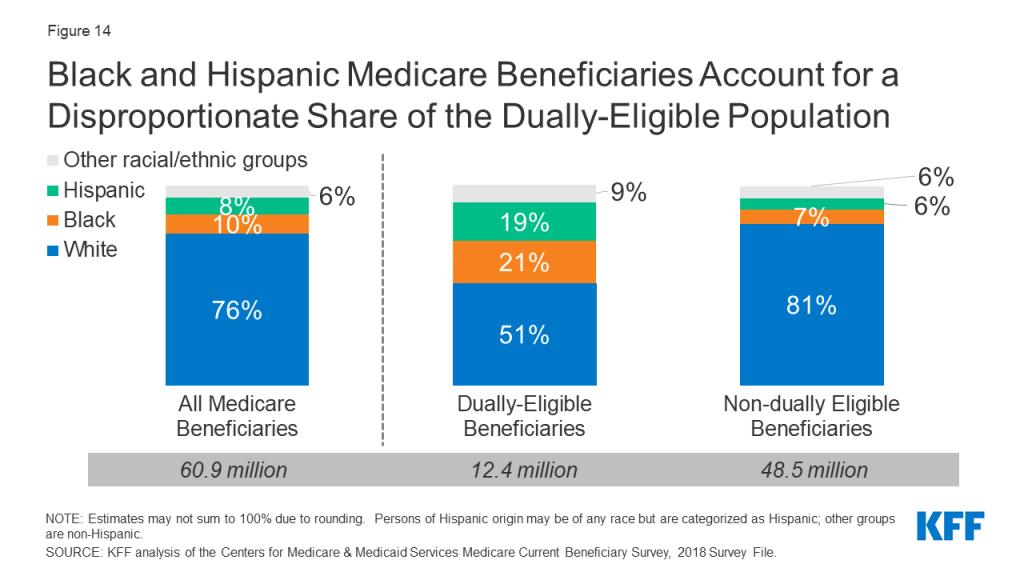
Black and Hispanic Beneficiaries Account for a Disproportionate Share of Beneficiaries Dually Eligible for Both Medicare and Medicaid
Medicaid, the federal-state program that provides coverage to low-income people, is a source of supplemental coverage for Medicare beneficiaries with low incomes and modest assets. Most dually eligible beneficiaries receive both full Medicaid benefits, including long-term services and supports, and payment of their Medicare premiums and cost sharing. Others do not qualify for full Medicaid benefits, but Medicaid covers their Medicare premiums and/or cost sharing through the Medicare Savings Programs.
Together, Black and Hispanic beneficiaries account for 18% of the total Medicare population, but 40% of the Medicare-Medicaid dually eligible population (Figure 14). Compared to all traditional Medicare beneficiaries, dual-eligible beneficiaries are more likely to report poor/fair health status, have lower income, and qualify for Medicare due to a permanent disability.
Black and Hispanic Medicare Beneficiaries With Part D Prescription Drug Coverage Are More Likely Than Their White Counterparts to Receive Low-Income Subsidies
The Medicare Part D program provides outpatient prescription drug coverage to Medicare beneficiaries. The majority (70%) of Medicare beneficiaries were enrolled in a Part D drug plan in 2018, with rates of Part D enrollment higher among Black (72%) and Hispanic (75%) beneficiaries than White beneficiaries (70%) (Figure 15).
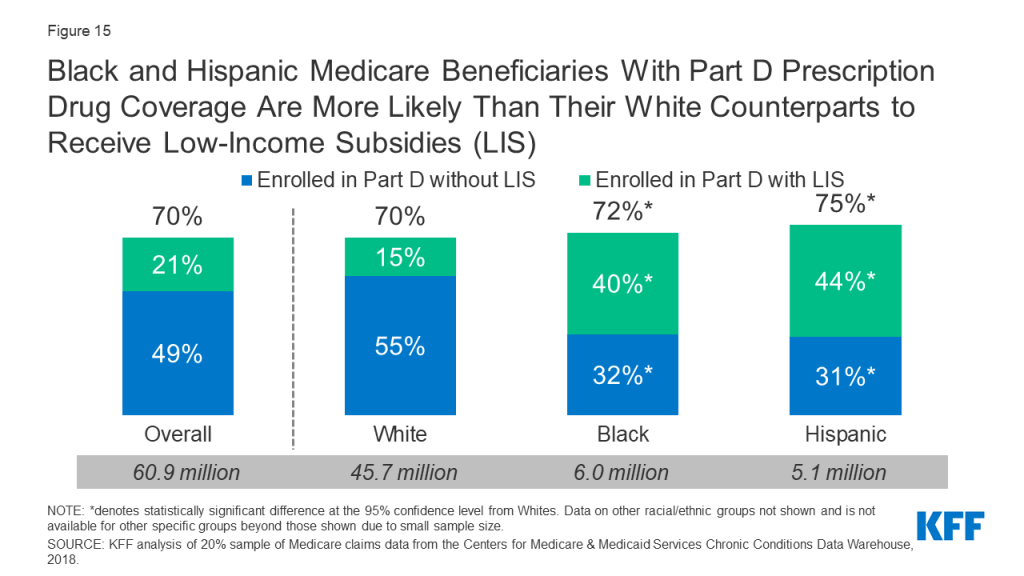
This may be partly a function of higher rates of enrollment in Medicaid among Black and Hispanic Medicare beneficiaries than among White beneficiaries, since dual-eligible beneficiaries are automatically enrolled in the Part D program and the Part D Low-Income Subsidy (LIS) program, which provides assistance with Part D premiums and cost sharing. Substantially larger shares (40% and 44%, respectively) of all Black and Hispanic beneficiaries were enrolled in Part D and received premium and cost-sharing assistance through the LIS program, compared to 15% of White beneficiaries.
Report: Access To Care And Service Utilization
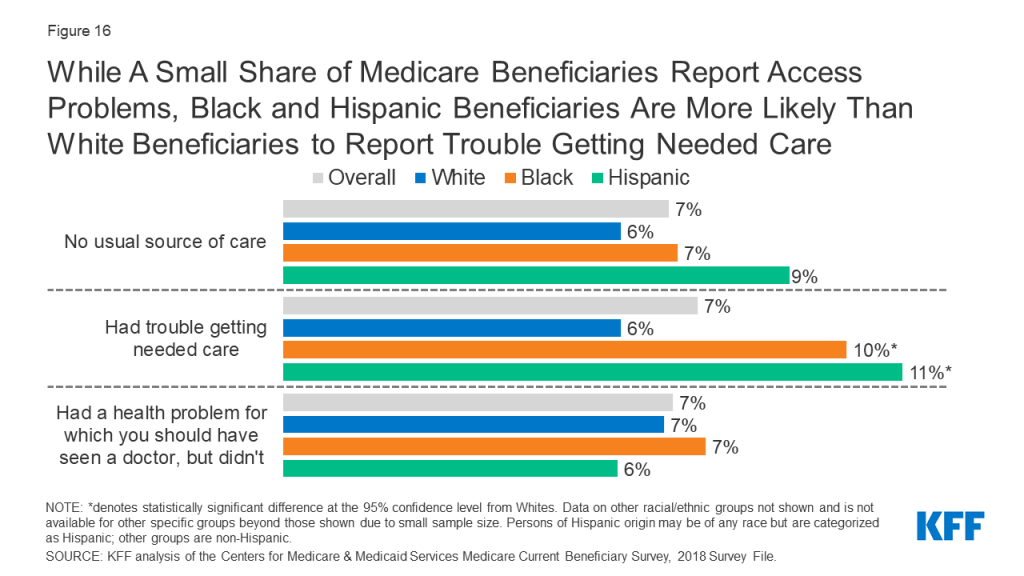
While a Small Share of Medicare Beneficiaries Overall Report Access Problems, Black and Hispanic Beneficiaries are More Likely than White Beneficiaries to Report Trouble Getting Needed Care
Overall, relatively few Medicare beneficiaries report problems with access to care, with no significant differences across racial and ethnic groups in the share of beneficiaries without a usual source of care or in the share of beneficiaries delaying needed care. These findings illustrate the importance of health insurance coverage in ensuring access to care and mitigating racial and ethnic disparities in some measures of access.
However, a larger share of Black (10%) and Hispanic (11%) beneficiaries than White beneficiaries (6%) report trouble getting needed care (Figure 16). Recent analysis by the Medicare Payment Advisory Commission (MedPAC) found that in 2019, among Medicare beneficiaries ages 65 and older, people of color were more likely than White beneficiaries to report unwanted delays in getting an appointment and problems finding a new specialist. This pattern was also observed among privately insured adults ages 50-64.
Black Medicare Beneficiaries Are More Likely to Report Cost-Related Barriers to Care Compared to White Beneficiaries
A larger share of Black and Hispanic beneficiaries than White beneficiaries report problems paying medical bills (21%, 13%, and 9%, respectively) and delaying care due to cost (14%, 12%, and 10% respectively). Among those with problems paying medical bills, a larger share of Black beneficiaries report debt to collection agencies due to medical bills than White beneficiaries (13% versus 4%, respectively) (Figure 17).

Among Beneficiaries in Traditional Medicare, Black and Hispanic Beneficiaries Were Less Likely Than White Beneficiaries to Report a Physician or Dental Visit in the Last Year
The majority of all beneficiaries in traditional Medicare saw at least one physician in 2018. However, the rate was lower among Black and Hispanic beneficiaries than among White beneficiaries (70% and 67%, respectively, compared to 79%). (Figure 18).
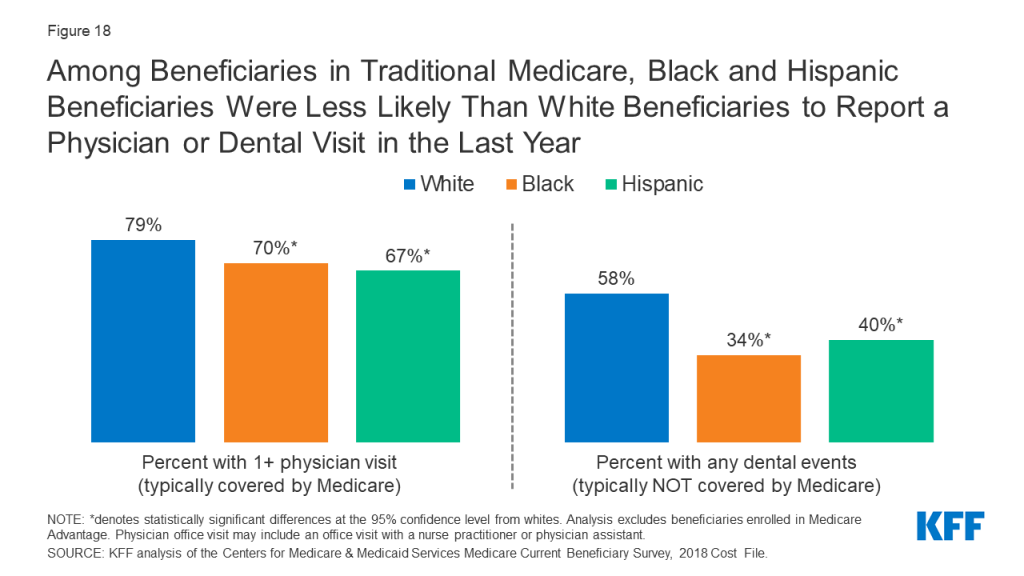
While traditional Medicare provides coverage for an array of medical services, it does not cover routine dental care. Consequently, in 2018, just over half (54%) of the Medicare population saw a dentist in the past year, with lower rates among Black beneficiaries (34%) and Hispanic beneficiaries (40%) than among White beneficiaries (58%) (Table 5).
Among Beneficiaries in Traditional Medicare, a Larger Share of Black Beneficiaries Had One or More Inpatient Stays and Emergency Department Visits Than White Beneficiaries
Among beneficiaries in traditional Medicare, a larger share of Black beneficiaries had an inpatient hospital stay than White beneficiaries (22% versus 15%, respectively) (Figure 19). The share of beneficiaries reporting at least two inpatient stays was also higher among Black beneficiaries (7%) than among White beneficiaries (4%) (Table 5). Racial/ethnic differences in inpatient stays (1+ days and 2+ days) did not differ significantly by self-reported health status.

A larger share of Black beneficiaries had one or more emergency department (ED) visits compared to White beneficiaries (41% versus 27%, respectively). In contrast to inpatient hospital stays, racial differences in ED visit rates by self-reported health status were observed. Specifically, Black beneficiaries in fair/poor health status were more likely than White beneficiaries of similar health status to report any emergency department visit (59% versus 43%, respectively). But even among Medicare beneficiaries in relatively better health (defined as excellent, very good, or good self-reported health status), Black beneficiaries were more likely than White beneficiaries to have an emergency department visit (30% vs. 21%, respectively). Additionally, the share of Black beneficiaries with two or more ED visits (24%) was twice as large as the share among White beneficiaries (12%).
Emergency Department Visit Rates for Hypertension, Diabetes, Stroke, and Heart Failure were Higher among Black Medicare Beneficiaries than Beneficiaries in Other Racial and Ethnic Groups
Among Medicare beneficiaries diagnosed with hypertension, the rate of ED visits among Black beneficiaries (53 per 1,000 people) was at least double the rates among White and Asian beneficiaries (22 and 21 visits per 1,000 people, respectively) and nearly double the rates among Hispanic and American Indian and Alaska Native beneficiaries (Figure 20). Among beneficiaries diagnosed with diabetes, ED visit rates among Black, Hispanic, and American Indian and Alaska Native beneficiaries (22, 17, and 20 visits per 1,000 beneficiaries, respectively) were at least double the rates among White and Asian beneficiaries (8 visits per 1,000 beneficiaries). Asian and Pacific Islander beneficiaries had lower ED visit rates for hypertension, diabetes, stroke, and heart failure compared to beneficiaries in other racial and ethnic groups.
Hospital Readmission Rates are Higher among Black Medicare Beneficiaries than Beneficiaries in Other Racial and Ethnic Groups
The Hospital Readmissions Reduction Program (HRRP), which has been in place since 2012, aims to reduce avoidable hospital readmission rates and improve quality of care by imposing payment penalties on hospitals with excess readmission rates for certain health conditions. In 2018, 30-day readmission rates among Medicare beneficiaries in traditional Medicare were higher among Black beneficiaries (19%) than among White beneficiaries (14%), Hispanic beneficiaries (17%), Asian/Pacific Islander beneficiaries (14%), and American Indian/Alaska Native beneficiaries (16%) (Figure 21). Black beneficiaries had higher odds of being readmitted to a hospital than White beneficiaries, regardless of diagnosis during the first hospitalization or discharge setting.
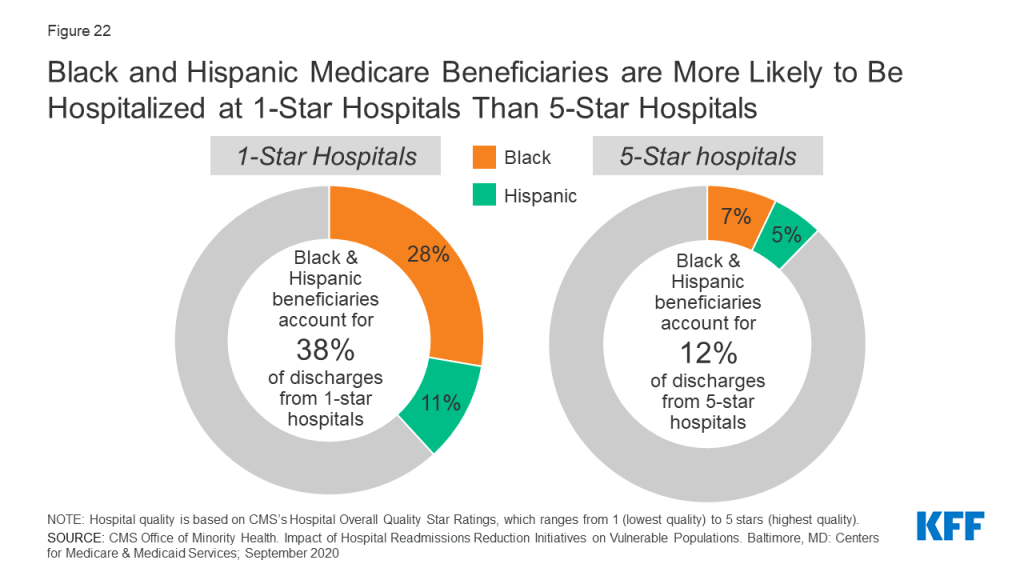
Black and Hispanic Medicare Beneficiaries are More Likely to be Hospitalized at 1-Star Hospitals than 5-Star Hospitals
CMS’s overall hospital quality star rating summarizes hospital performance on various measures, such as rates of readmissions, healthcare-associated infections, and value of care for certain health conditions (e.g., pneumonia) into a single star rating for each hospital, which ranges from 1 star (lowest quality) to 5 stars (highest quality). In 2018, Black and Hispanic beneficiaries accounted for 28% and 11% of discharges from 1-star hospitals, respectively, but only 7% and 5% of discharges from 5-star hospitals, respectively (Figure 22).
Black and Hispanic Beneficiaries Report Lower Utilization Rates Than White Beneficiaries of Some Prevention Services
Medicare provides coverage for a wide range of preventive and screening services, including a “Welcome to Medicare” physical exam during the first year of Medicare enrollment, immunization for various conditions (including influenza), and screening exams for cancers.
Overall, less than a quarter (21%) of male beneficiaries ages 50 and older reported receiving a prostate cancer screening, with no statistically significant differences by race or ethnicity (Figure 23). Less than half (43%) of all female beneficiaries ages 40 and older reported receiving a mammogram in the past year, with Black and Hispanic beneficiaries being more likely than White beneficiaries to receive a mammogram in the past year (51%, 49%, 42%, respectively).
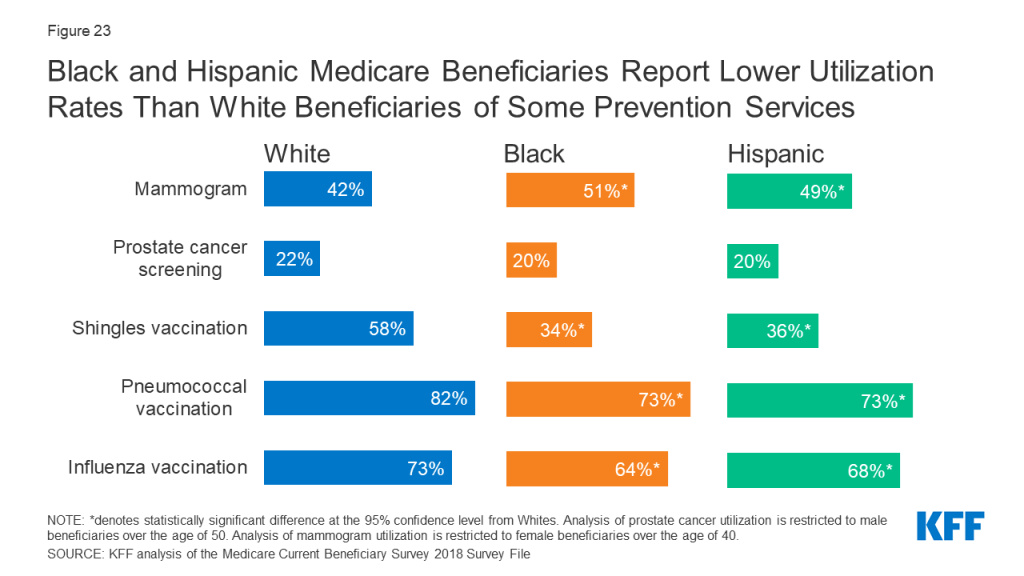
Notable racial and ethnic disparities in immunization rates were also observed among Medicare beneficiaries. Smaller shares of Black and Hispanic beneficiaries reported receiving a flu vaccination than White beneficiaries (64%, 68%, and 73%, respectively). Research has shown that the gap in flu vaccination is even greater when it comes to receipt of high-dose influenza vaccine,28 which is specifically targeted to adults ages 65 and older. Additionally, compared to White beneficiaries, Black and Hispanic beneficiaries had lower rates of pneumococcal vaccination and shingles vaccination. Several potential factors may contribute to racial and ethnic disparities in vaccination uptake, including, but not limited to, differential access to and use of preventive health care services, concerns or misconceptions about vaccine safety, and persistent medical mistrust rooted in a history of racial discrimination and mistreatment in the health care sector.
Report: Covid-19
COVID-19 Death Rates Among Hispanic, American Indian/Alaska Native, and Black Adults Ages 65 and Older are Nearly Double the Rate Among Older White Adults
People of color have experienced disproportionate rates of COVID-19 cases, hospitalizations, and deaths. Specifically, among adults ages 65 and older, the mortality rates per 100,000 people were higher for older Hispanic adults (1,050 deaths per 100,000), older American Indian/Alaska Native adults (966 deaths per 100,000), and older Black adults (900 deaths per 100,000) than for older White adults (561 deaths per 100,000) (Figure 24).
Among Adults Ages 65 and Older, COVID-19 Represents a Larger Share of Deaths Among People of Color than White People Since January 2020
Among older Hispanic adults, COVID-19 deaths account for 25% of all causes of death—2.3 times higher than the share among older White adults (11%) (Figure 25). For older American Indian/Alaska Native, Asian, Black, and Native Hawaiian or Other Pacific Islander adults, COVID-19 deaths account for 23%, 17%, 16%, and 16% of deaths from all causes, respectively.
COVID-19 Cases Are Higher Among American Indian/Alaska, Hispanic, and Black Beneficiaries Than Among White Beneficiaries
From January 1 to November 21, 2020, COVID-19 cases among American Indian and Alaska Native, Black, and Hispanic Medicare beneficiaries (4,598, 4,343, and 4,243 cases per 100,000 respectively) were 1.7, 1.6, and 1.6 times higher, respectively, than among White beneficiaries (2, 655 cases per 100,000) (Figure 26).
COVID-19 Hospitalization Rates Are Higher Among American Indian/Alaska Native, Black, and Hispanic Beneficiaries Than Among White Beneficiaries
From January 1, 2020 to November 21, 2020, hospitalization rates for American Indian/Alaska Native, Black, and Hispanic Medicare beneficiaries were 2.9 times, 2.7 times, and 2.1 times respectively, higher than White beneficiaries (592 hospitalizations per 100,000) (Figure 27).
Analysis of patient data from health records shows that in addition to having higher rates of infections, hospitalizations, and mortality, people of color have been more likely to require more intensive level of treatment at the time of COVID-19 diagnosis, such as inpatient hospitalization or the use of oxygen and ventilation. Further, the COVID-19 pandemic has exacerbated mental health outcomes among older Hispanic adults, with older Hispanic adults reporting higher rates of depression or anxiety (33%) than older White (23%), Black (26%), and Asian (17%) adults.
The CARES Act includes a provision requiring Medicare Part B to cover a vaccine for COVID-19 at no cost to Medicare beneficiaries. However, 35% of Black adults ages 18 and older say they would definitely or probably not get a vaccine even if it was deemed safe by scientists and offered at no cost, with about half (48%) saying they are not confident that the needs of Black people are being accounted for in the COVID-19 vaccine development process. This finding reflects well-founded medical mistrust among African Americans, based on a history of racial abuse and malpractice within the medical system, as exemplified by the Tuskegee syphilis experiment, involuntary medical experimentation of Henrietta Lacks,29 and ongoing forms of medical racism, such as under prescribing of pain medications for Black people due to racial bias.
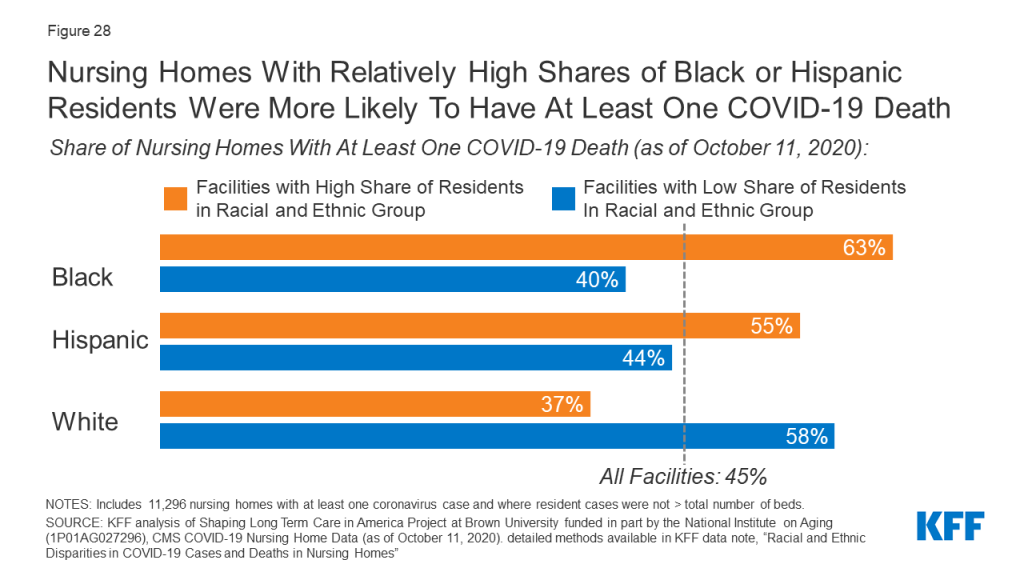
Nursing Homes with Relatively High Shares of Black or Hispanic Residents Were More Likely to Have At Least One COVID-19 Death
Older adults in long-term care facilities, such as nursing homes, have also been disproportionately impacted by the COVID-19 pandemic, with long-term facilities accounting for 7% of total cases and 40% of total deaths in the U.S. More than half of nursing homes with a high share (defined as 20% or more of residents) of Black residents (63%) and Hispanic residents (55%) reported at least one COVID-19 death, compared to 37% of nursing homes with a high share of White residents (Figure 28).
Nancy Ochieng, Juliette Cubanski, Tricia Neuman, and Samantha Artiga are with KFF. Anthony Damico is an independent consultant.
Methods
Data Sources Used in Analysis
The Centers for Medicare & Medicaid Services (CMS) 2018 Chronic Conditions Data Warehouse (CCW) was used to provide state-level estimates of the Medicare population, by race and ethnicity.
The CMS Medicare Current Beneficiary Survey (MCBS) 2018 Survey File was used to describe Medicare beneficiary characteristics, supplemental coverage, and access to care. The analysis on supplemental coverage was limited to beneficiaries enrolled in Part A and Part B for most months of the year, excluding those with Part A or Part B only and Medicare as a Secondary Payer for most months of the year. The MCBS 2018 Cost Supplement File was used to describe service utilization among Medicare beneficiaries in fee-for-service (FFS).
Analysis on Medicare Part D enrollment was based on prescription drug event claims data from a sample of Medicare beneficiaries (20% sample for 2018) from the CMS Chronic Conditions Data Warehouse (CCW).
The CMS Office of Minority Health’s Mapping Medicare Disparities Tool, which uses 2018 administrative claims data from the Chronic Conditions Warehouse, was used to describe emergency department visit rates. This data was limited to Medicare beneficiaries enrolled in FFS. Medicare Advantage enrollees were excluded from this analysis because claims data are not available for these beneficiaries.
The CMS Office of Minority Health’s report, Impact of Hospital Readmissions Reduction Initiatives on Vulnerable Populations, which uses 2016 administrative claims data from the CCW, was used to describe 30-day hospital inpatient readmissions in Medicare FFS beneficiaries.
Urban Institute’s Dynamic Simulation of Income Model (DYNASIM4) was used to describe Medicare beneficiaries’ income and assets in 2019. Detailed methodology is previously discussed here.
The 2018-2020 Current Population Survey March Annual Social and Economic Supplement (CPS ASEC) was used to provide subgroup estimates of poverty under the official and supplemental poverty measure over the period of 2017-2019. The 2020 CPS-ASEC was used to produce poverty rates for all older adults in 2019 The poverty rates presented in this analysis apply to the non-institutionalized Medicare population. The CPS ASEC poverty thresholds are different from the Health and Human Services (HHS) poverty guidelines (sometimes referred to as the “federal poverty level”). Detailed methodology is previously discussed here.
Data from the U.S Census Bureau’s 2017 National Population Projection Main Series was used for U.S population estimates among people ages 65 and over.
Elizabeth Arias and Jiaquan Xu, “United States Life Tables, 2018” National Vital Statistics Reports 69, no. 12 (November 2020) was used to describe life expectancy at age 65 by race and gender.
Data on COVID-19 cases and hospitalization rates among Medicare beneficiaries were obtained from CMS’ Preliminary Medicare COVID-19 Data Snapshot ( https://www.cms.gov/research-statistics-data-systems/preliminary-medicare-covid-19-data-snapshot).
Data on COVID-19 deaths among adults ages 65 and over were obtained from the Centers for Disease Control and Prevention, “Deaths involving coronavirus disease 2019 (COVID-19) by race and Hispanic origin group and age, by state” as of February 3, 2021 ( https://data.cdc.gov/NCHS/Deaths-involving-coronavirus-disease-2019-COVID-19/ks3g-spdg). The CDC WONDER online database was used to obtain 2019 U.S Census Bureau single-race population estimates in order to calculate death rates per 100,000 people.
Tables
Endnotes
- David Barton Smith, The Power to Heal: Civil Rights, Medicare, and the Struggle to Transform America’s Health Care System (Nashville: Vanderbilt University Press, 2016). ↩︎
- Emily A. Largent, “Public Health, Racism, and the Lasting Impact of Hospital Segregation,” Public Health Reports 133, no. 6 (2018): 715–20, https://doi.org/10.1177/0033354918795891. ↩︎
- Anouk Lloren et al., “Measuring Hospital-Specific Disparities by Dual Eligibility and Race to Reduce Health Inequities,” Health Services Research 54, no. February (2019): 243–54, https://doi.org/10.1111/1475-6773.13108. ↩︎
- Nicholas S. Downing et al., “Association of Racial and Socioeconomic Disparities With Outcomes Among Patients Hospitalized With Acute Myocardial Infarction, Heart Failure, and Pneumonia: An Analysis of Within- and Between-Hospital Variation,” JAMA Network Open 1, no. 5 (2018): e182044, https://doi.org/10.1001/jamanetworkopen.2018.2044. ↩︎
- Yue Li et al., “Medicare Advantage Associated With More Racial Disparity Than Traditional Medicare For Hospital Readmissions,” Health Affairs 36, no. 7 (2017): 1328–35, https://doi.org/10.1377/hlthaff.2016.1344. ↩︎
- Downing et al., “Association of Racial and Socioeconomic Disparities With Outcomes Among Patients Hospitalized With Acute Myocardial Infarction, Heart Failure, and Pneumonia: An Analysis of Within- and Between-Hospital Variation.” ↩︎
- Maricruz Rivera-hernandez et al., “Racial Disparities in Readmission Rates among Patients Discharged to Skilled Nursing Facilities,” Journal of the American Geriatrics Society 67, no. 8 (2019): 1672–79, https://doi.org/10.1111/jgs.15960.Racial. ↩︎
- Jolyn Taylor et al., “Disparities in Treatment and Survival among Elderly Ovarian Cancer Patients,” Gynecologic Oncology 151, no. 2 (2018): 269–94, https://doi.org/10.1016/j.ygyno.2018.08.041. ↩︎
- Jeffrey H. Silber et al., “Disparities in Breast Cancer Survival by Socioeconomic Status Despite Medicare and Medicaid Insurance,” Milbank Quarterly 96, no. 4 (2018): 706–54, https://doi.org/10.1111/1468-0009.12355. ↩︎
- Ikumi Suzuki et al., “Racial Disparities in Outcome among Head and Neck Cancer Patients in the United States: An Analysis Using SEER-Medicare Linked Database.,” Journal of Clinical Oncology 37, no. 15 (2018): 6051–6051, https://doi.org/10.1200/JCO.2019.37.15_suppl.6051. ↩︎
- Clara Lam et al., “Differences in Cancer Survival among White and Black Cancer Patients by Presence of Diabetes Mellitus: Estimations Based on SEER-Medicare-Linked Data Resource,” Cancer Medicine 7, no. 7 (2018): 3434–44, https://doi.org/10.1002/cam4.1554. ↩︎
- Sikander Ailawadhi et al., “Racial Disparities in Treatment Patterns and Outcomes among Patients with Multiple Myeloma: A SEER-Medicare Analysis,” Blood Advances 3, no. 20 (2019): 2986–94, https://doi.org/10.1182/bloodadvances.2019000308. ↩︎
- Arline T Geronimus, “The Weathering Hypothesis and the Health of African-American Women and Infants: Evidence and Speculations.,” Ethn Dis. 2, no. 3 (1992): 207–21. ↩︎
- Arline T. Geronimus et al., “‘Weathering’ and Age Patterns of Allostatic Load Scores among Blacks and Whites in the United States,” American Journal of Public Health 96, no. 5 (2006): 826–33, https://doi.org/10.2105/AJPH.2004.060749. ↩︎
- Dinorah Martinez Tyson et al., “Unpacking Hispanic Ethnicity—Cancer Mortality Differentials Among Hispanic Subgroups in the United States, 2004–2014,” Frontiers in Public Health 6, no. August (2018): 1–11, https://doi.org/10.3389/fpubh.2018.00219. ↩︎
- Fatima Rodriguez et al., “Disaggregation of Cause-Specific Cardiovascular Disease Mortality Among Hispanic Subgroups,” JAMA Cardiology 2, no. 3 (2017): 240–47, https://doi.org/10.1001/jamacardio.2016.4653. ↩︎
- Robert Grove and Alice Hetzel, Vital Statistics Rates in the United States: 1940-1960 (Washington, DC: U.S Government Printing Office, 1968); Elizabeth Arias, Brian L. Rostron, and Tejada-Vera Betzaida, “United States Life Tables, 2005,” National Vital Statistics Reports 58, no. 10 (2010); Jiaquan Xu et al., “Deaths: Final Data for 2007,” National Vital Statistics Reports 58, no. 19 (2010), available at https://www.cdc.gov/nchs/data/hus/2010/022.pdf. ↩︎
- Jennifer Van Hook, Michelle Frisco, and Carlyn Graham, “Signs of the End of the Paradox? Cohort Shifts in Smoking and Obesity and the Hispanic Life Expectancy Advantage,” Sociological Science 7 (2020): 391–414, https://doi.org/10.15195/v7.a16. ↩︎
- Michelle L. Frisco, Jennifer Van Hook, and Robert A. Hummer, “Would the Elimination of Obesity and Smoking Reduce U.S. Racial/Ethnic/Nativity Disparities in Total and Healthy Life Expectancy?,” SSM – Population Health 7 (2019): 100374, https://doi.org/10.1016/j.ssmph.2019.100374. ↩︎
- Van Hook, Frisco, and Graham, “Signs of the End of the Paradox? Cohort Shifts in Smoking and Obesity and the Hispanic Life Expectancy Advantage.” ↩︎
- National Academies of Sciences, Engineering, and Medicine, Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System (Washington, DC: The National Academies Press, 2020). ↩︎
- Alexandra Killewald and Brielle Bryan, “Falling Behind: The Role of Inter- and Intragenerational Processes in Widening Racial and Ethnic Wealth Gaps through Early and Middle Adulthood,” Social Forces 97, no. 2 (2018): 705–40. ↩︎
- Tyson H. Brown, “Diverging Fortunes: Racial/Ethnic Inequality in Wealth Trajectories in Middle and Late Life,” Race and Social Problems 8, no. 1 (2016): 29–41, https://doi.org/10.1007/s12552-016-9160-2. ↩︎
- Raj Chetty et al., “Race and Economic Opportunity in the United States: An Intergenerational Perspective” (Cambridge, MA, 2018), https://www.nber.org/system/files/working_papers/w24441/w24441.pdf. ↩︎
- Ling Na et al., “Activity Limitation Stages Are Associated With Risk of Hospitalization Among Medicare Beneficiaries,” PM and R 9, no. 5 (2017): 433–43, https://doi.org/10.1016/j.pmrj.2016.09.008. ↩︎
- Jibby E. Kurichi et al., “Predicting 3-Year Mortality and Admission to Acute-Care Hospitals, Skilled Nursing Facilities, and Long-Term Care Facilities in Medicare Beneficiaries,” Archives of Gerontology and Geriatrics 73 (2017): 248–56, https://doi.org/10.1016/j.archger.2017.08.005. ↩︎
- Bjoern Suckow et al., “Hemoglobin A1c Testing and Amputation Rates in Black, Hispanic, and White Medicare Patients,” Annals of Vascular Surgery 36 (2016): 208–17, https://doi.org/10.1016/j.avsg.2016.03.035. ↩︎
- Laura L. Hall et al., “A Map of Racial and Ethnic Disparities in Influenza Vaccine Uptake in the Medicare Fee-for-Service Program,” Advances in Therapy 37, no. 5 (2020): 2224–35, https://doi.org/10.1007/s12325-020-01324-y. ↩︎
- Rebecca Skloot, The Immortal Life of Henrietta Lacks (Crown Publishing Group, 2010). ↩︎