Most Trump Voters Say Nothing Would Change Their Vote, 3 in 10 Can Name a Policy Position That Would
The independent source for health policy research, polling, and news.
Although premiums for Affordable Care Act Marketplace benchmark silver plans are decreasing on average across the U.S. in 2020, changes vary widely by geographic location and plan type, including premium increases in a number of counties and plans, according to a new KFF analysis of county-level data.
The analysis of premium data from insurer rate filings to state regulators, state exchange websites and healthcare.gov shows how premiums are changing next year at the county level, both before and after accounting for the federal subsidies that are available to some consumers depending on their income. An interactive map illustrates changes in premiums for the lowest-cost bronze, silver and gold plans by county.
The analysis finds that unsubsidized premiums for benchmark silver plans – which are the basis for determining federal financial help – are dropping by 3.5 percent, on average, and by just under 3 percent for the lowest-cost bronze, silver and gold plans. However, whether consumers will see their premium payments rise or fall will depend on their income, preferred metal level plan and how specific plan premiums are changing at the county level.
Other key findings of the analysis, How ACA Marketplace Premiums are Changing by County in 2020, include:
The ACA open enrollment period for the federal marketplace and most state marketplaces began Nov. 1 and ends on Dec. 15.
With KFF’s updated Health Insurance Marketplace Calculator, consumers can generate estimates of their health insurance premiums and the federal subsidies they may be eligible for when purchasing insurance on their own in the ACA marketplaces. Consumers also can search our collection of more than 300 Frequently Asked Questions about open enrollment, the health insurance marketplaces and the ACA.
Our look at how ACA Marketplace premiums are changing by county in 2021 is now available.
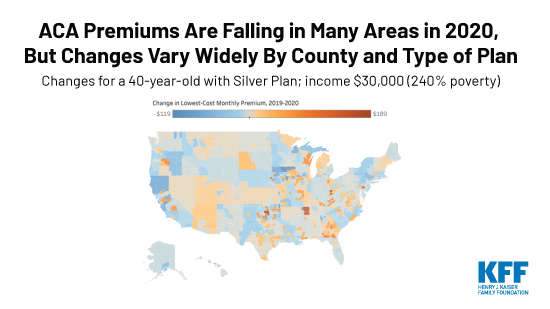
Premiums for ACA Marketplace benchmark silver plans are decreasing on average across the U.S. in 2020. However, premium changes vary widely by location and by metal level, including premium increases in a number of counties and plans. Additionally, the amount an exchange enrollee actually pays in premiums depends largely on their income – as most enrollees receive significant premium subsidies – and the difference in cost between the benchmark (second-lowest silver plan) and the premium for the plan they choose.
ACA premiums are falling in many areas of the U.S in 2020. This analysis has interactive maps with county-level data illustrating changes for the lowest-cost bronze, silver & gold plans across the country.
We analyzed premium data from insurer rate filings to state regulators, state exchange websites, and healthcare.gov to see how premiums are changing at the county level both before and after subsidies in 2020. The map below illustrates changes in premiums for the lowest-cost bronze, silver, and gold plans by county. Results are shown for a 40-year-old paying the full premium and for a 40-year old with an income of $20,000 (160% of poverty), $25,000 (200% of poverty), $30,000 (240% of poverty), $35,000 (280% of poverty), and $40,000 (320% of poverty), who would be eligible for a premium tax credit.
Nationally, the average unsubsidized premium for the lowest-cost bronze, silver, and gold plans are decreasing by just under 3% from 2019 to 2020, and the average benchmark silver premium – on which subsidies are calculated – is dropping by somewhat more, about 3.5%. (Table 1).
| Table 1: Change in the Average Lowest-Cost Premium by Metal Level Before Tax Credit, 2019-2020 for a 40-year-old | |||
| 2019 | 2020 | % Change | |
| Lowest Cost Bronze Premium | $340 | $331 | -2.6% |
| Lowest Cost Silver Premium | $454 | $442 | -2.7% |
| Lowest Cost Gold Premium | $516 | $501 | -2.9% |
| Benchmark Premium | $478 | $462 | -3.5% |
| SOURCE: Kaiser Family Foundation analysis of premium data from Healthcare.gov and review of state rate filings. | |||
In general, this could mean the tax credit covers somewhat less of the premium for subsidized enrollees who enroll in the lowest-cost plans. However, premium changes vary by geography, so whether enrollees will see their premium payments increase or decrease for 2020 will depend on how benchmark premiums are changing and how premiums for plans at their preferred metal level are changing in their county:
Premium changes for people eligible for subsidies will also be affected by changes in the amount they are expected to pay for a benchmark plan at any given income level, which is decreasing slightly in 2020.
| Table 2: Change in the Average Lowest-Cost Premium by Metal Level After Tax Credit, 2019-2020 | |||
| 40-year-old with $20,000 income (160% of poverty) | 2019 | 2020 | % Change |
| Lowest Cost Bronze Premium | $3 | $2 | -43.1% |
| Lowest Cost Silver Premium | $60 | $60 | +0.1% |
| Lowest Cost Gold Premium | $121 | $118 | -2.2% |
| 40-year-old with $25,000 income (200% of poverty) | |||
| Lowest Cost Bronze Premium | $26 | $25 | -5.3% |
| Lowest Cost Silver Premium | $118 | $117 | -0.8% |
| Lowest Cost Gold Premium | $180 | $177 | -1.8% |
| 40-year-old with $30,000 income (240% of poverty) | |||
| Lowest Cost Bronze Premium | $76 | $75 | -1.4% |
| Lowest Cost Silver Premium | $183 | $180 | -1.7% |
| Lowest Cost Gold Premium | $245 | $239 | -2.3% |
| 40-year-old with $35,000 income (280% of poverty) | |||
| Lowest Cost Bronze Premium | $142 | $140 | -1.2% |
| Lowest Cost Silver Premium | $253 | $249 | -1.7% |
| Lowest Cost Gold Premium | $315 | $308 | -2.2% |
| 40-year-old with $40,000 income (320% of poverty) | |||
| Lowest Cost Bronze Premium | $191 | $197 | +2.8% |
| Lowest Cost Silver Premium | $304 | $307 | +0.8% |
| Lowest Cost Gold Premium | $366 | $366 | 0.0% |
| SOURCE: Kaiser Family Foundation analysis of premium data from Healthcare.gov and review of state rate filings. | |||
As was the case in 2018 and 2019, insurers generally loaded the cost from the termination of federal cost-sharing reduction payments entirely onto the silver tier (a practice sometimes called “silver loading”). The relatively higher price for silver plans due to silver loading means subsidy-eligible Marketplace enrollees will continue to receive relatively large premium tax credits, although the dollar amount may be somewhat smaller than in past years based on decreases in the underlying benchmark silver premiums. These subsidies continue to make gold plans more easily attainable and make bronze plans cheaper (or even more likely to be available for $0) than before cost-sharing reduction payments were terminated. Subsidized premiums for bronze plans may be particularly attractive to many people eligible for premium tax credits (Table 3). For example, the tax credit for a 40-year-old individual making $20,000 covers the full cost of the premium for the lowest-cost bronze plan in 85% of counties (2,661 out of 3,142 counties in the U.S.). This is similar to 2019, when the tax credit has covered the full cost of the lowest-cost bronze plan for a low-income enrollee in 81% of counties (2,547 counties).
| Table 3: Number of Counties Where an Individual’s Tax Credit Covers the Full Premium of the Lowest-Cost Bronze Plan,for a 40-year-old | ||
| Example Age and Income | 2019 | 2020 |
| 40-year-old with $20,000 income (160% of poverty) | 2,547 (81% of counties) | 2,661 (85% of counties) |
| 40-year-old with $25,000 income (200% of poverty) | 2,028 (65%) | 1,736 (55%) |
| 40-year-old with $30,000 income (240% of poverty) | 661 (21%) | 608 (19%) |
| 40-year-old with $35,000 income (280% of poverty) | 410 (13%) | 287 (9%) |
| 40-year old with $40,000 income (320% of poverty) | 120 (4%) | 135 (4%) |
| SOURCE: Kaiser Family Foundation analysis of premium data from Healthcare.gov and review of state rate filings. | ||
However, even if subsidized silver premiums are higher than bronze premiums it is still important for low-income enrollees to consider the significant cost-sharing assistance that is only available if they enroll in a silver plan. In order to qualify for a plan with a cost-sharing reduction (CSR), low-income enrollees must sign up for a silver plan. CSR plans lower the amount an enrollee spends out-of-pocket by setting a lower out-of-pocket maximum, which also translates to lower deductibles, copayments, and coinsurance. For example, a single individual making between 100-200% of the poverty level can qualify for a silver plan with an out-of-pocket maximum of no more than $2,700, and the deductible would be significantly lower than that. If the same individual instead signs up for a bronze plan, the out-of-pocket maximum and deductible could be upwards to $8,150. If this person is sick or expects to have high health spending, it may be better to pay a relatively higher premium for a silver plan even if a bronze plan is available for a $0 premium.
The map below shows where an individual’s tax credit covers the full premium of the lowest-cost bronze plan for a 40-year-old with an income of $20,000 (160% of poverty), $25,000 (200% of poverty), $30,000 (240% of poverty), $35,000 (280% of poverty), and $40,000 (320% of poverty).
For subsidized enrollees, a gold plan may actually be available at no cost after tax credits are applied as well (Table 4). For example, the tax credit for a 40-year-old individual making $20,000 covers the full cost of the premium for the lowest-cost gold plan in 240 counties (out of 3,142 counties in the U.S.). This is a decrease from 2019, when the tax credit covered the full cost of the lowest-cost gold plan in 392 counties.
| Table 4: Number of Counties Where an Individual’s Tax Credit Covers the Full Premium of the Lowest-Cost Gold Plan, for a 40-year-old | ||
| Example Age and Income | 2019 | 2020 |
| 40-year-old with $20,000 income (160% of poverty) | 392 (12% of counties) | 240 (8% of counties) |
| 40-year-old with $25,000 income (200% of poverty) | 153 (5%) | 207 (7%) |
| 40-year-old with $30,000 income (240% of poverty) | 39 (1%) | 87 (3%) |
| 40-year-old with $35,000 income (280% of poverty) | 12 (0.4%) | 35 (1%) |
| 40-year old with $40,000 income (320% of poverty) | 12 (0.4%) | 12 (0.4%) |
| SOURCE: Kaiser Family Foundation analysis of premium data from Healthcare.gov and review of state rate filings. | ||
The map below shows counties where the unsubsidized premium for the lowest-cost gold plan has a lower or comparable premium to the lowest-cost silver plan in 2020, before tax credits are applied.
With news of average benchmark premiums dropping a bit on average in 2020, consumers may expect to pay less for any plan on the ACA Marketplaces. In reality, there is wide variation in premium changes, including premium increases for some consumers. What a given consumer actually pays depends on income, location, and differences in pricing between their plan and the benchmark silver plan. For consumers to know how much they will pay, they must return to Healthcare.gov or their state’s exchange each year and carefully consider their options.
As benchmark silver plans in 2020 continue to have relatively higher costs compared to bronze plans, low-income enrollees in many parts of the country will qualify for “free” (zero-premium) bronze plans. Most insurers are continuing to load the cost of offering reduced cost sharing plans onto silver premiums. The benchmark (second-lowest cost) silver plan is the basis for determining the amount of financial assistance consumers receive. When silver premiums are high in comparison to bronze plans, the large tax credit may cover all or most of the cost of a bronze plan. While “free” bronze or gold plans will be available to subsidized enrollees in many counties in 2020 it is still important for low-income enrollees, particularly those in need of more medical care, to consider the significant cost-sharing assistance that is only available if they enroll in a silver plan.
Although the federal government discontinued payments to insurers for reducing cost sharing for lower-income enrollees, insurers remain obliged to provide reduced cost sharing policies to eligible Marketplace enrollees. Silver plans with reduced cost sharing generally have higher actuarial values than gold plans and much higher value than bronze plans for enrollees with incomes below 200% of poverty. Low-income consumers will need to consider whether it makes sense to purchase a metal level other than silver, as a lower premium plan may come with significantly higher deductibles, copays, or coinsurance.
We analyzed data from the 2019 and 2020 Individual Market Medical files to determine premiums and the benchmark amounts to calculate premium tax credits for the scenarios presented. These files are available at data.healthcare.gov. Premiums for the 13 state-based marketplaces are from a review of insurer rate filings and state plan finders. For most states running their own exchange, premiums presented in this analysis are at the rating area level. Premiums for California and Massachusetts were collected at the zip code level, and premiums for Washington and Nevada were collected at the county level. All premiums are displayed as the full price, rather than just the portion that covers essential health benefits.
The average changes in plan costs were weighted by county using 2019 plan selections obtained from the 2019 Marketplace Open Enrollment Period County-Level Public Use file provided by CMS, available here. In states running their own exchanges, we gathered county-level plan selection data where possible and otherwise estimated county plan selections based on the county population in the 2010 Census and total state plan selections in the 2019 OEP State-Level Public Use File provided by CMS, available here.
[1] The map legend shows premium changes in dollars rather than the percent change because, at the county level, percent changes may appear to overstate premium increases and understate decreases, particularly for those who qualify for relatively large premium subsidies. For example, a change from $60 to $2 is a -97% change but a change from $2 to $60 is a +2900% change. This issue is less prevalent when calculating the percent change in national average premiums, since outlier premiums are not given as much weight. The percent change in premiums by county can be viewed by hovering over the map.
The Kaiser Family Foundation and Cook Political Report have embarked on a new project examining the attitudes and experiences of voters in several key battleground states leading up the 2020 presidential election. The Blue Wall Voices Project is a unique state-based polling project that relies on an innovative probability-based approach to conducting public opinion polls using a combination of telephone and online methodologies. Drawing from voter registration lists, KFF and Cook Political Report have conducted interviews with 3,222 voters in the four states constituting the “Democratic Blue Wall” – the area in the Upper Midwest that was previously considered a Democratic stronghold, and where state polls performed poorly in 2016 and underestimated support for President Trump. The data analyzed is from 767 voters in Michigan, 958 voters in Minnesota, 752 voters in Pennsylvania, and 745 voters in Wisconsin. For more details, please see the methodology section of this report.
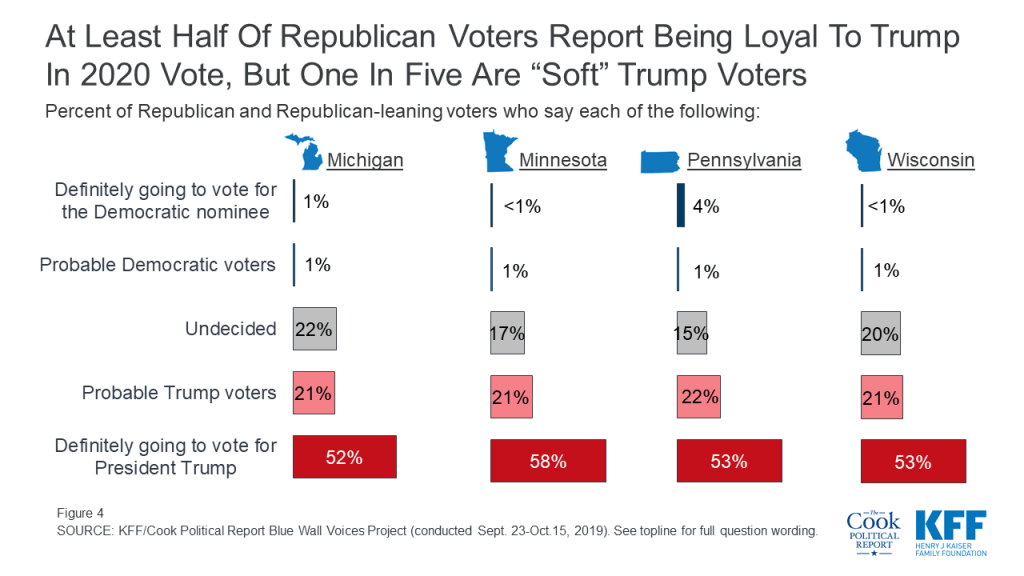
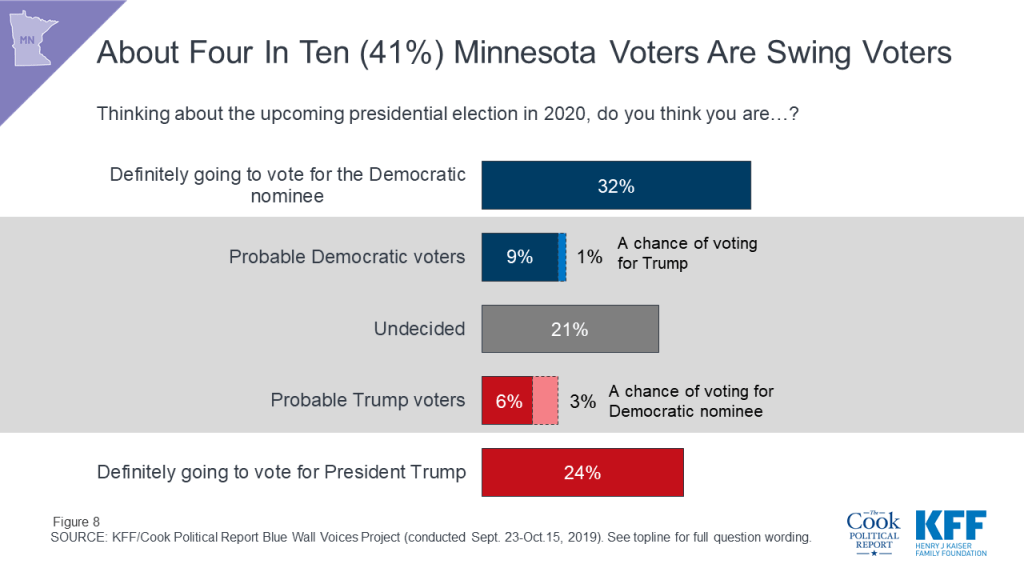
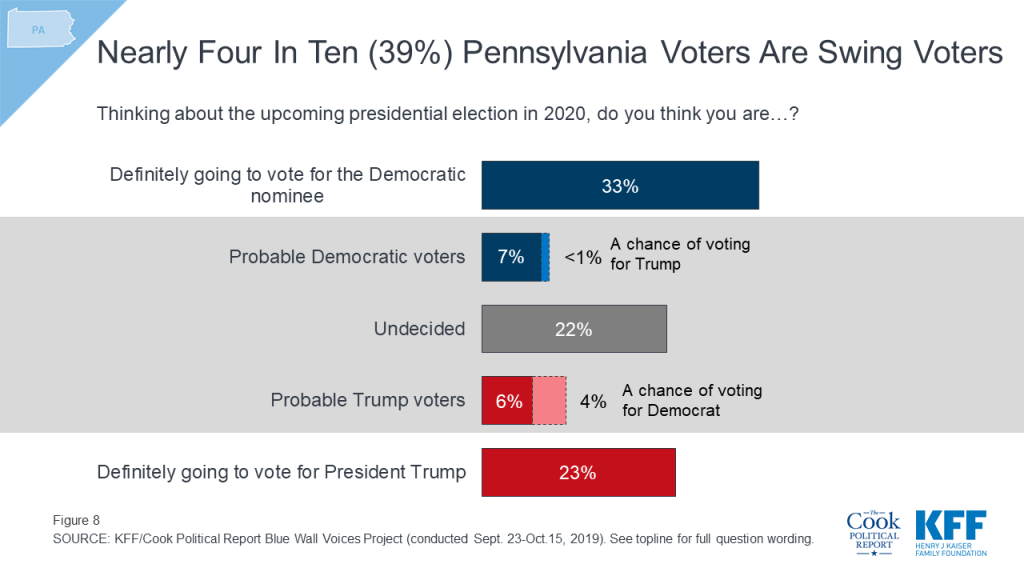
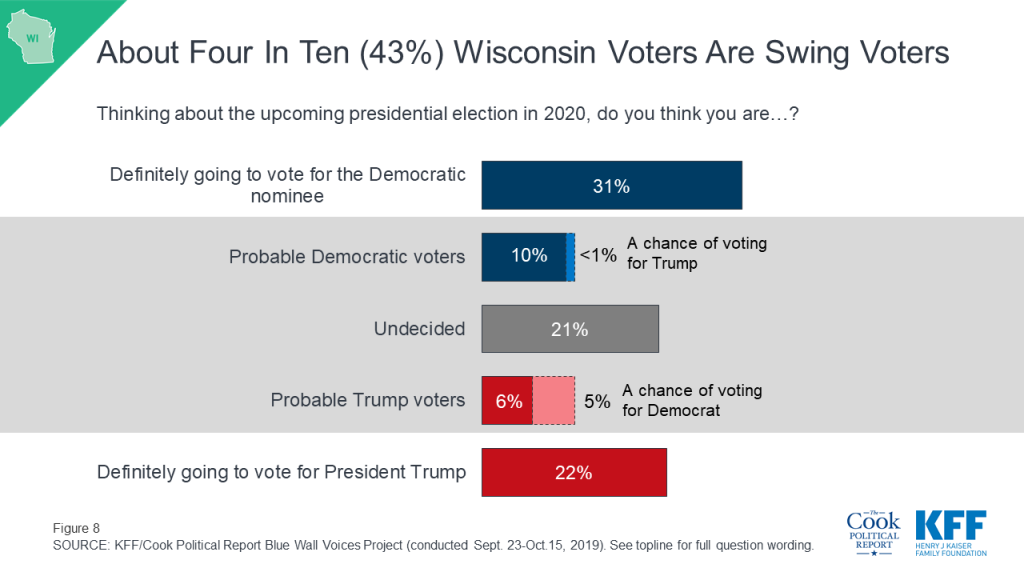
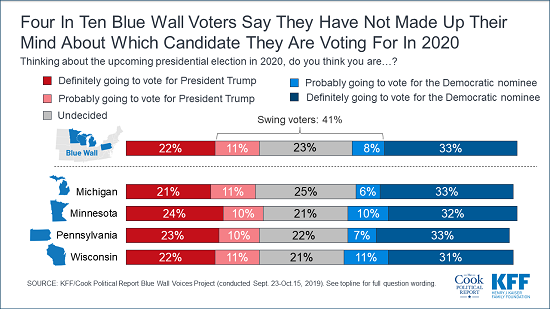
More than half of voters in Michigan, Minnesota, Pennsylvania, and Wisconsin say they have already made up their minds about which candidate they plan to vote for. One-third of voters say they are “definitely going to vote for the Democratic nominee” while one-fifth (22%) say they are “definitely going to vote for President Trump.” The share who say they are “definitely going to vote for President Trump” in these states is slightly lower than the share of voters nationally who reported the same in our national KFF Health Tracking Poll analysis earlier this year. It is important to note that while there are currently a larger share of voters in each state who say they are “definitely going to vote for the Democratic nominee” than “definitely going to vote for President Trump,” it is unclear how this could change once the Democrats choose a nominee and President Trump and other Republicans start attacking a single candidate rather than the entire field of candidates.
This leaves four in ten voters (41%) as the crucial voting block known throughout this report as “swing voters.” This group of voters either say they are “probably going to vote for President Trump” (11%), “probably going to vote for the Democratic nominee” (8%), or say they are “undecided” about how they will vote (23%).

There are not significant differences across the states, with similar shares of voters in Michigan (43%), Minnesota (41%), Pennsylvania (39%), and Wisconsin (43%) saying they are either “probably” going to vote for a candidate or are “undecided.”
It is important to note that not all “swing voters” could potentially change their vote to support the other party’s candidate. While nearly half of those who say they are probably going to vote for President Trump say there is “a chance” they will vote for the Democratic nominee (4% of all voters), on the other side of the ballot almost none of those who say they are probably going to vote for the Democratic nominee say that there is “a chance” they will vote for President Trump (less than 1%).

This is similar to what we found in our national analysis earlier this year, with few voters who say they are probably going to vote for either President Trump or the Democratic nominee saying there is “a chance” they will vote for the other party’s candidate. This is also similar across the four states included in this analysis with few voters saying there is “a chance” they would vote for the other party’s candidate.
A majority of Democratic voters and Republican voters in each state say they aren’t going to cast a vote for the other party’s candidate. About seven in ten (72%) Democratic and Democratic-leaning independent voters in Michigan say they are definitely going to vote for the Democratic nominee as do two-thirds of Democratic voters in Minnesota (68%), Wisconsin (66%), and Pennsylvania (65%).

A smaller share, but still a majority, of Republican and Republican-leaning independent voters say they are definitely going to vote for President Trump (58% in Minnesota, 53% in Wisconsin and Pennsylvania, and 52% in Michigan). Nearly twice as many Republican and Republican-leaning voters in Michigan and Wisconsin are undecided about their 2020 presidential vote choice as the Democratic counterparts in the states.1
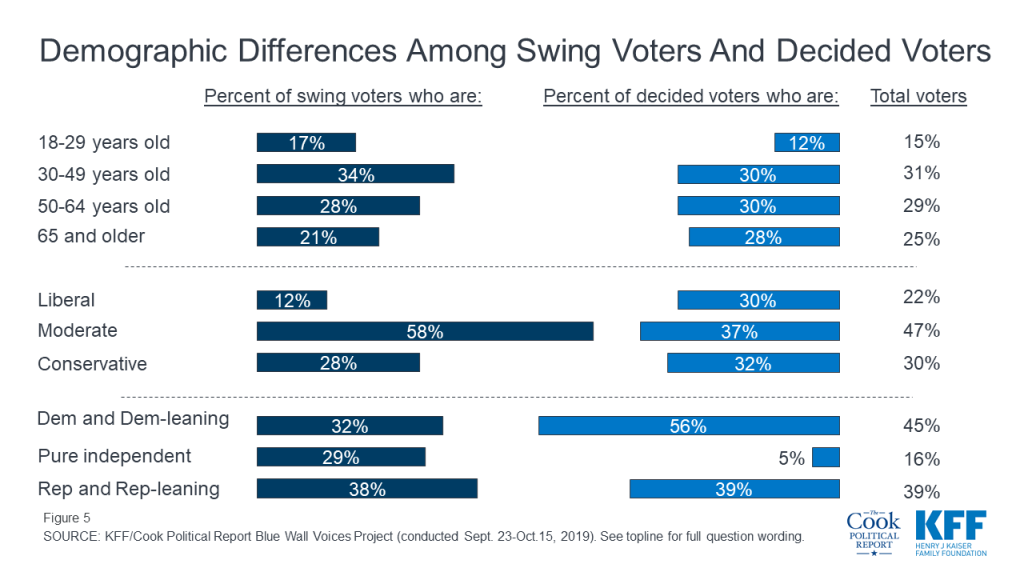
On most demographics, swing voters look very similar to their counterparts (voters who say they have already decided who they are going to vote for in the 2020 election), but they differ on three key variables: age, party identification, and ideology. Swing voters generally are more likely to say they are moderate in terms of their ideology (58%) and a larger share identify as political independents (29%) than their decided counterparts (5%). In addition, swing voters are slightly younger as a whole with about half (51%) under the age of 50 compared to 42% of decided voters.
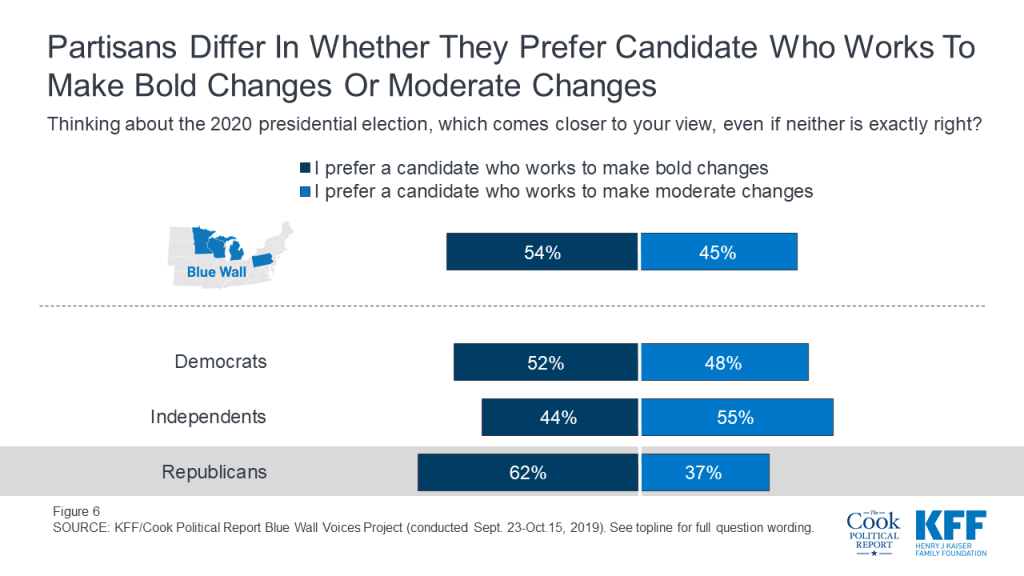
During the 2016 election, President Trump ran as an unconventional candidate who was going to work to implement bold changes in this country and deliver a shock to business as usual in Washington, D.C. One year out from the 2020 election, a slightly larger share of voters – including a majority of Republican voters – still prefer to vote for a candidate who wants to make bold changes rather than moderate changes. A slightly larger share of voters in Michigan, Minnesota, Pennsylvania, and Wisconsin say they prefer to vote for a candidate in 2020 who wants to make bold changes (54%) rather than a candidate who works to make moderate changes (45%).
Six in ten Republican voters (62%) say they prefer a candidate who works to make bold changes rather than a candidate who works to make moderate changes (37%). Democratic voters are more divided on their preference with half (52%) preferring a candidate who works to make bold changes and a similar share preferring a candidate who works to make moderate changes (48%). A majority of independent voters (55%) prefer a candidate who works to make moderate changes.
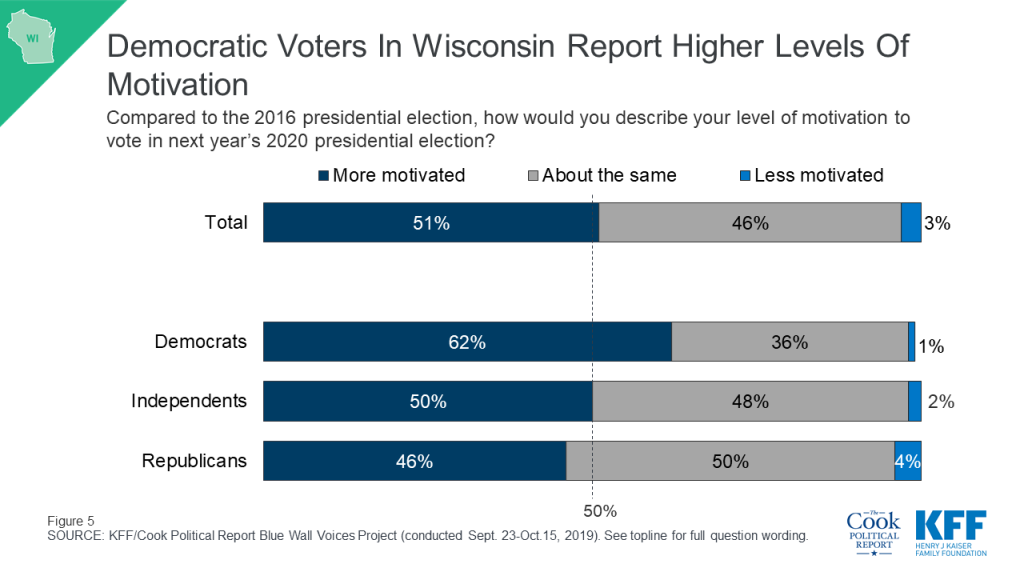
Democratic voters appear to have the edge in motivation one year out from the 2020 general election with a larger share of Democratic voters (64%) saying they are “more motivated” about voting in next year’s presidential election than either independent voters (55%) and Republican voters (53%).

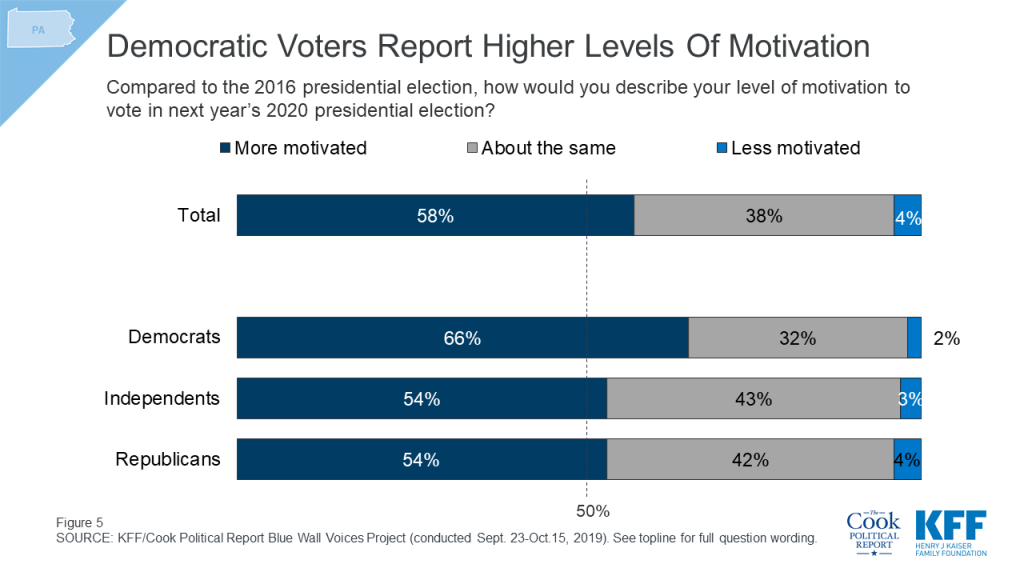
About two-thirds of Democratic voters in Pennsylvania (66%) and Michigan (65%) and six in ten Democratic voters in Wisconsin (62%) say they are “more motivated” to vote in next year’s election. This is compared to less than half of Republican voters in Wisconsin (46%) and slightly more than half of Republican voters in Pennsylvania (54%) Michigan (53%) who say they are more motivated to vote than in the previous presidential election. Partisan voters in Minnesota are both “more motivated” to vote in next year’s election. To see more on this, check out the individual state reports.
| Table 1: The Democratic Party has the Enthusiasm Edge in Michigan, Pennsylvania, and Wisconsin | ||||
| Percent who say they are more motivated to vote in next year’s election than in the 2016 election: | Michigan | Minnesota | Pennsylvania | Wisconsin |
| Total | 55% | 52% | 58% | 51% |
| Democratic voters | 65 | 57 | 66 | 62 |
| Independent voters | 61 | 47 | 54 | 50 |
| Republican voters | 53 | 59 | 54 | 46 |
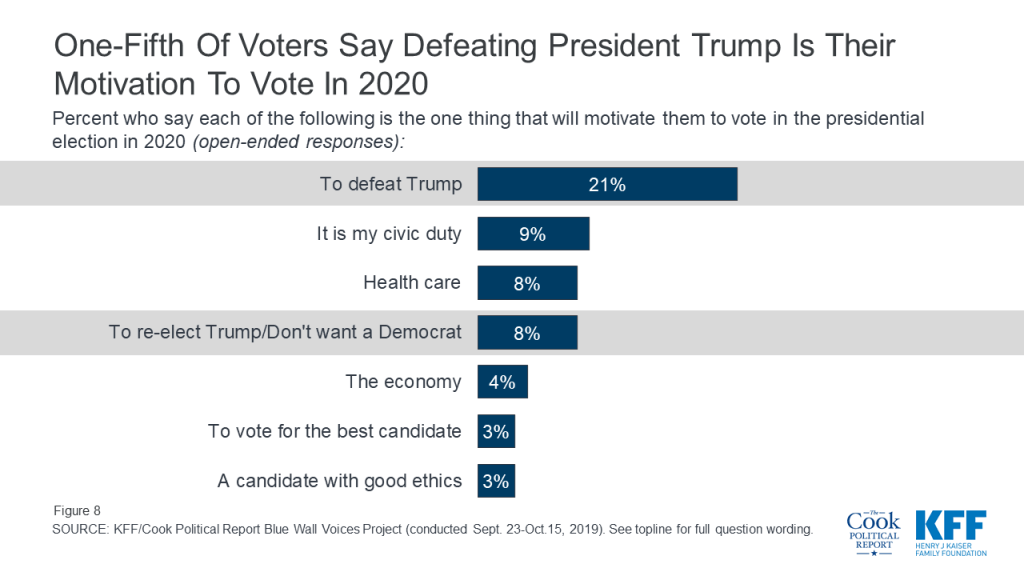
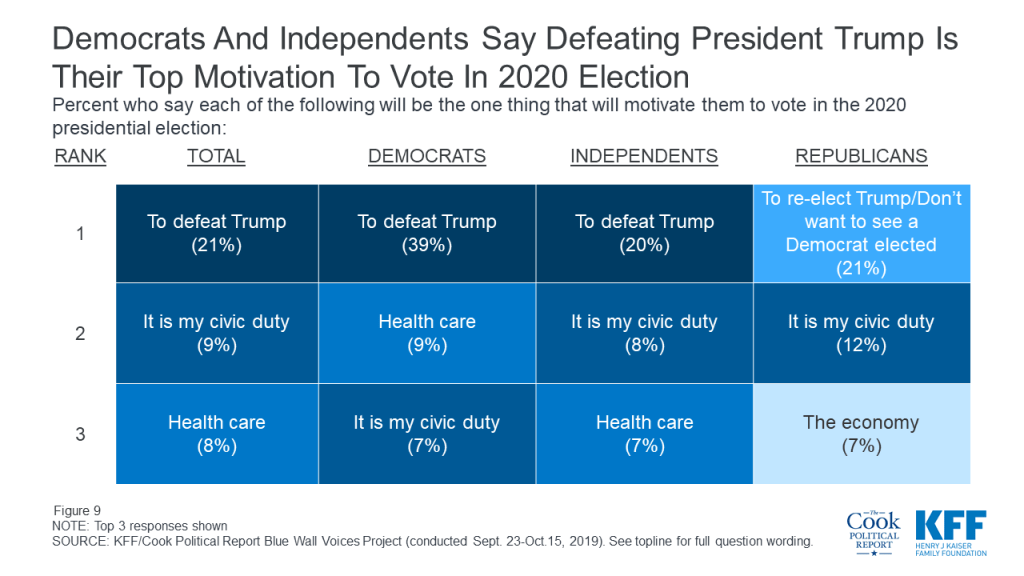
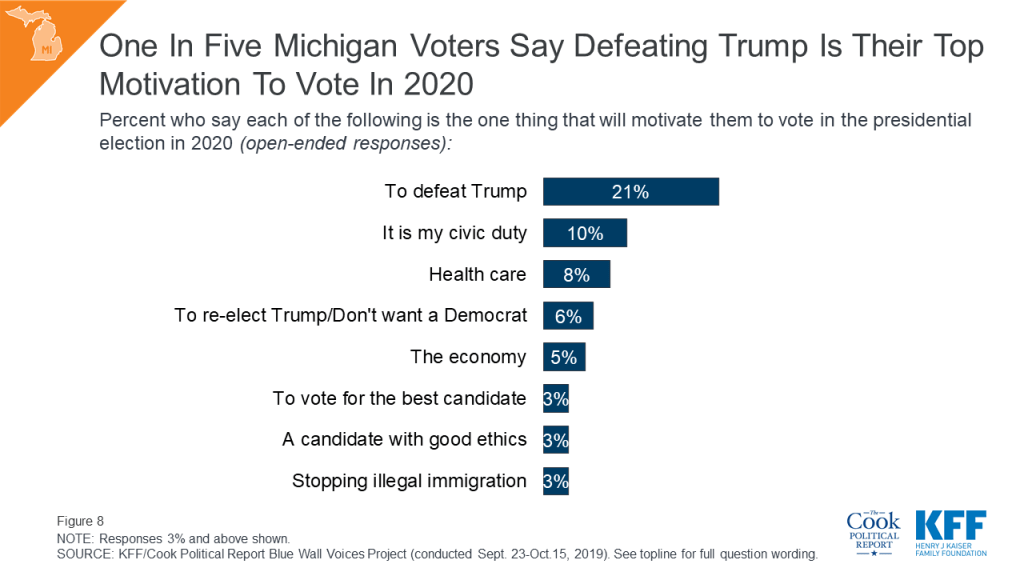
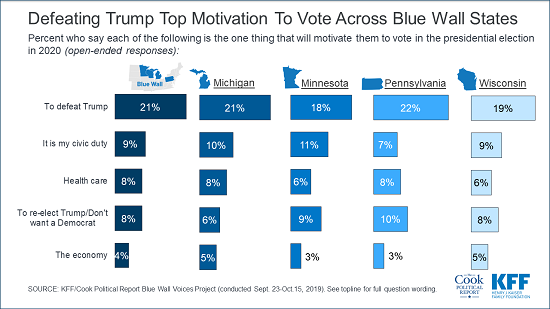
When asked to offer in their own words what one thing will motivate them to vote in the 2020 presidential election, one-fifth of all Blue Wall voters offer responses related to defeating President Trump (21%). This is followed by those who say voting is their civic duty (9%), health care (8%), re-electing President Trump or not wanting to elect a Democrat (8%), and the economy (4%) is their top motivation. Overall, one-fourth (23%) of voters offer issues such as health care, the economy, and immigration, as their motivation for voting in the 2020 presidential election.
Defeating President Trump is offered as the top motivation to vote in 2020 by four in ten Democratic voters (39%) and one-fifth of independent voters, while responses related to re-electing President Trump or not wanting to elect a Democrat was offered by 21% of Republican voters – followed by those who say that their civic duty is their top motivation to vote in 2020 (12%).
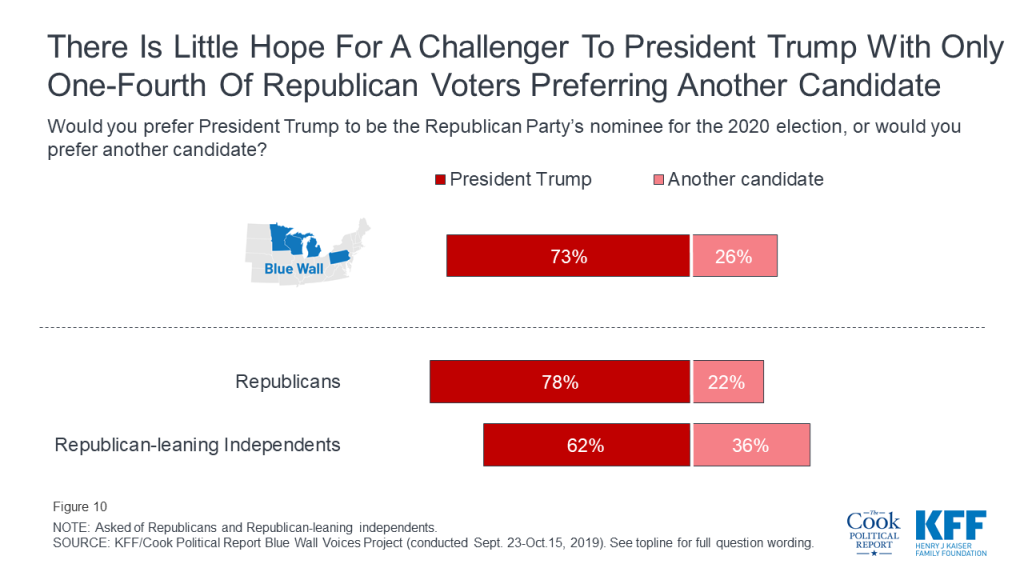
Most Republican and Republican-leaning independent voters (73%) also say they prefer President Trump to be the Republican Party’s nominee for the 2020 election with about one-fourth (26%) saying they prefer another candidate to be the Republican Party’s nominee. Those who self-identify as Republicans are more tied to President Trump with nearly eight in ten (78%) saying they prefer President Trump be the nominee compared to about six in ten (62%) independents who lean Republican in their views.
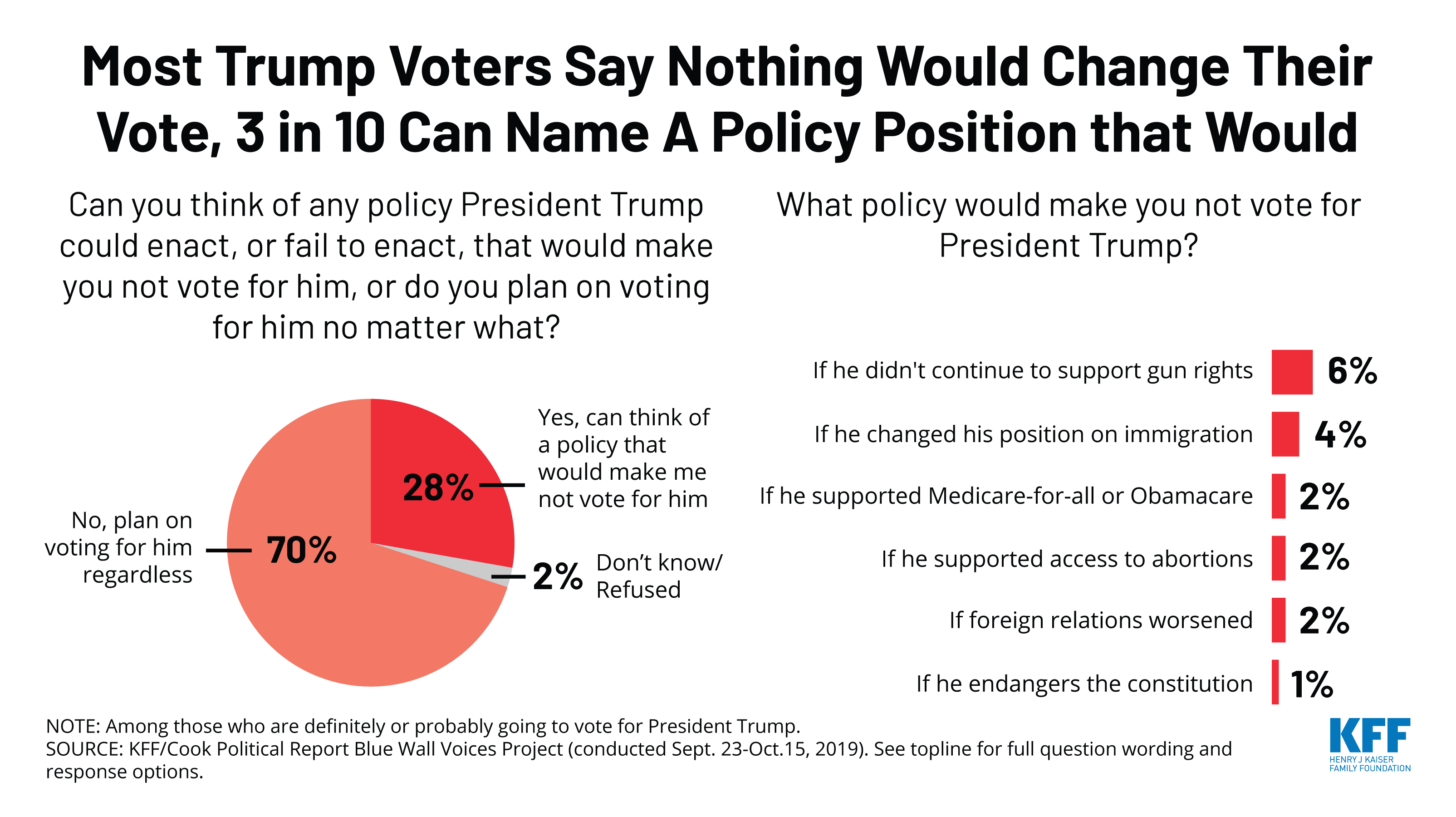
Most voters who say they are going to vote for President Trump in 2020 do not see a scenario in which he would no longer have their vote. Seven in ten Trump voters say there is not a policy he could enact or fail to enact that would make them no longer vote for him while three in ten (28%) say they can think of a scenario that would make them no longer vote for President Trump.
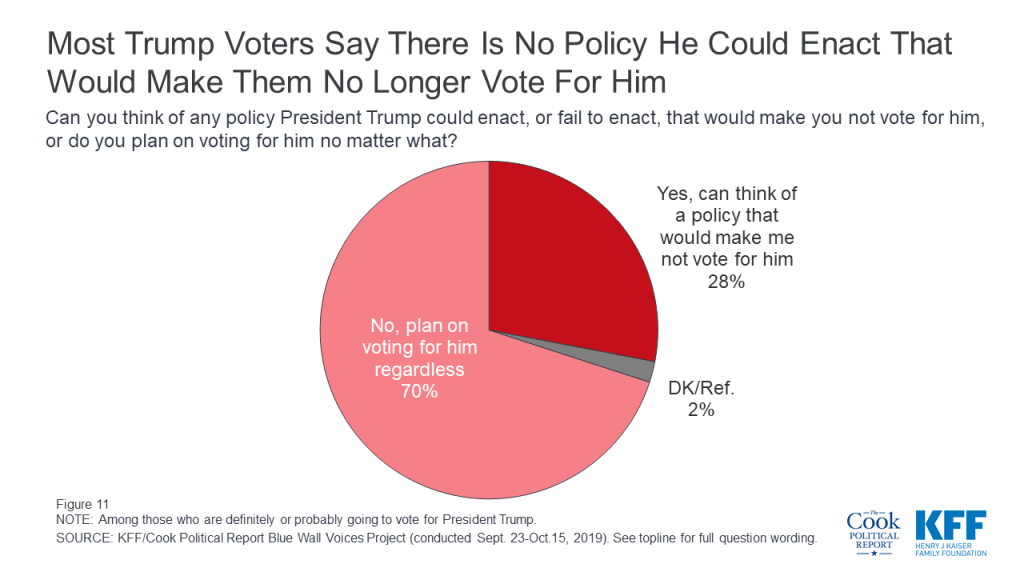
When asked to offer in their own words what policy President Trump could enact, or fail to enact, that would make them no longer vote for him, one-fifth (6% of all 2020 Trump voters) say that if he no longer continued to support gun rights they would no longer vote for him. This is followed by one in six (4% of all 2020 Trump voters) who offered that if he changed his position on immigration, they would no longer vote for him. Other issues that were offered include supporting Medicare-for-all (2%), supporting access to abortions (2%), or if foreign relations worsened (2%). Few Trump voters said they would not vote for President Trump if he endangered the constitution (1%).2
Democratic voters in the Blue Wall are divided in what is most important to them when selecting a candidate for president. Four in ten voters (42%) say it is more important that the Democrats select a candidate who “has the best chance to defeat President Trump” while a similar share (40%) say it is more important to select a candidate who “comes closest to their views on the issues.” Fewer (13%) voters say it is more important to select a candidate who “is the most authentic” and even fewer (4%) say it is most important to select a candidate who “can most disrupt the current system.”

A larger share of Democratic and Democratic-leaning independent voters in Minnesota say it is more important that the eventual nominee be able to defeat President Trump (48%) than come closest to their views on the issues (33%).
| Table 2: Minnesota Democratic Voters Prioritize Defeating President Trump | |||||
| In selecting a presidential nominee for the Democratic Party, which of the following is most important to you? | Total | Michigan | Minnesota | Pennsylvania | Wisconsin |
| Has the best chance to defeat President Trump | 42% | 42% | 48% | 40% | 39% |
| Comes closest to your views on the issues | 40 | 45 | 33 | 38 | 42 |
| Is the most authentic | 13 | 11 | 16 | 13 | 17 |
| Can most disrupt the current system | 4 | 2 | 3 | 7 | 2 |
| NOTE: Among Democratic and Democratic-leaning independents. | |||||
Yet, despite this, significant shares of Democratic voters in each of the states say they do not plan to vote in the Democratic primary in their state and instead plan to wait to vote until the 2020 general election. One-third of Democratic and Democratic-leaning voters in Minnesota say they plan to wait to vote until the 2020 general election as do one-fourth of Democratic voters in Michigan, one-fifth of Democratic voters in Wisconsin, and 17% of Democratic voters in Pennsylvania.
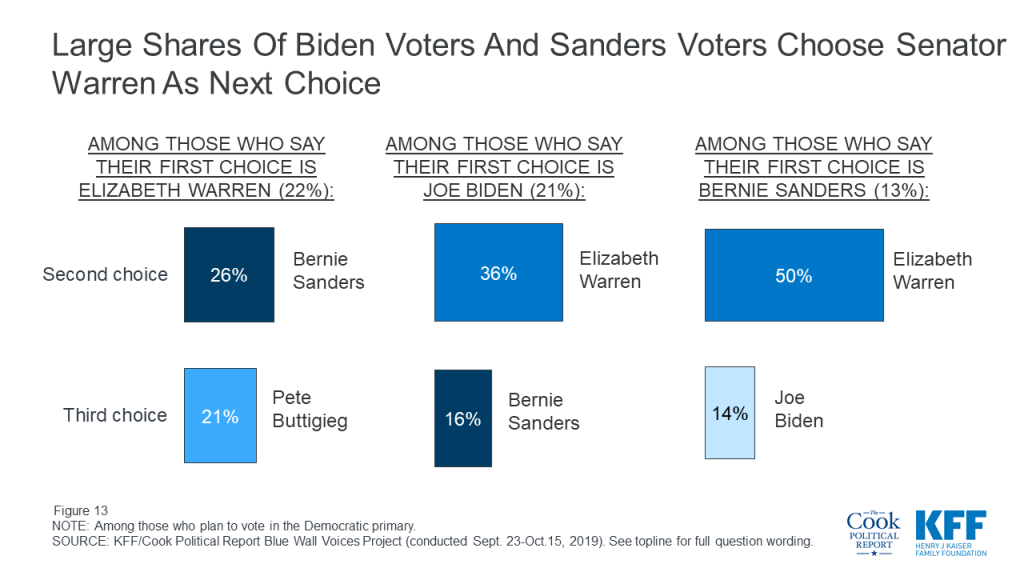
Among those primary election voters, Senator Elizabeth Warren and former Vice President Joe Biden have the edge over the other major Democratic presidential candidates. One-fifth of Democratic primary voters say Sen. Warren (22%) is the candidate they plan to support which is similar to the share who say Vice President Biden is the candidate they plan to support (21%). While Senator Warren and Vice President Biden garner similar shares of top choice votes among Democratic primary voters across the Blue Wall, four in ten Democratic primary voters choose Sen. Warren as either their first or second choice in the Democratic primary. This is followed by 29% who choose Vice President Biden, one-fourth who choose Sen. Sanders, and 14% who choose Mayor Pete Buttigieg. Most of the shift over to Sen. Warren is from Sen. Sanders supporters with half of Sen. Sanders supporters choosing Sen. Warren as their second choice of candidates. For more information about how voters in each of the states rank the candidates, check out the individual state reports.
The 2020 Democratic candidates are garnering support from slightly different voting groups throughout Michigan, Minnesota, Pennsylvania, and Wisconsin. Across the four states, a larger share of voters who chose Senator Sanders as their first choice are men (50%) compared to those who chose Senator Warren (35%) or Vice President Biden (43%) as their first choice candidate. Sen. Sanders also has an edge among younger voters with eight in ten of his supporters under the age of 50. Sen. Warren’s supporters, on the other hand, are more likely to be women (65%), and have at least a college degree (65%) compared to less than half of Sen. Sanders’ supporters or Vice President Biden’s supporters. About one in five of Vice President Biden’s supporters are African-American compared to smaller shares of Sanders’ supporters (9%) or Warren’s (7%).
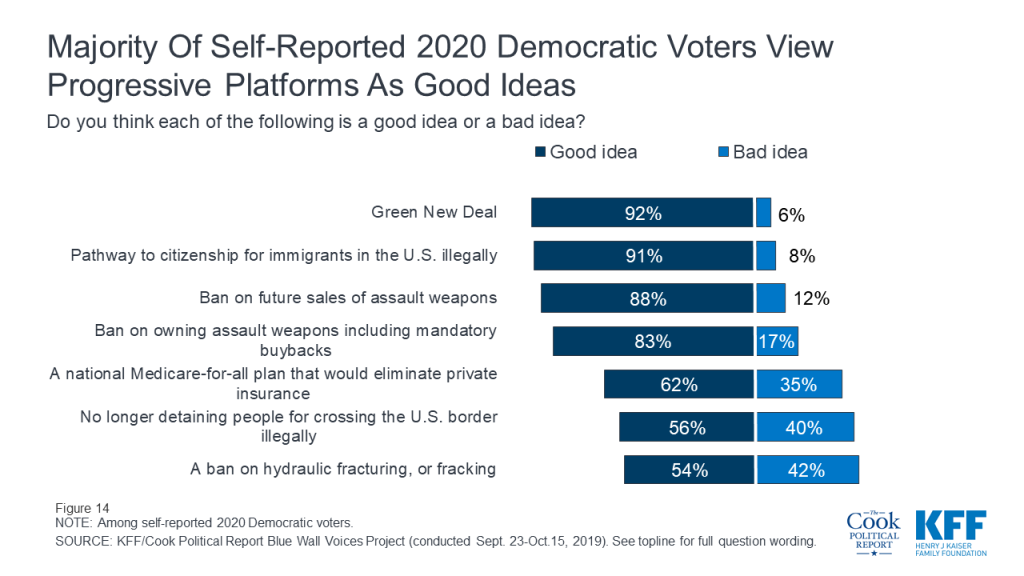
The Blue Wall Voices Project also seeks to find out how voters view many of the progressive positions being discussed by some of the Democratic nominees for president. Overall, a majority of voters in the Blue Wall who say they are either “definitely” or “probably” going to vote for the Democratic nominee view the progressive platforms asked about in this survey as “good ideas.” This includes majorities of these self-reported likely 2020 Democratic voters in each of the four states.
Nine in ten self-reported 2020 Democratic voters (92%) say the Green New Deal, the plan to address climate change through new regulations and increases in government spending on green jobs and energy-efficient infrastructure is a “good idea.” This is closely followed by large majorities who say a pathway to citizenship for immigrants in the U.S. illegally (91%), a ban on the future sale of assault weapons (88%), and a ban on the ownership of assault weapons and military-style rifles like the AR-15 including a mandatory buyback program for current owners (83%) are “good ideas.” Fewer, but still a majority (62%), say a national health plan in which all Americans would get their health coverage through a single government plan, Medicare-for-all, is a “good idea.” Slightly more than half of self-reported 2020 Democratic voters say stopping U.S. detainments for people crossing the border illegally or a ban on fracking are “good ideas” (56% and 54%, respectively). These three issues rank at the bottom of progressive platforms for self-reported 2020 Democratic voters in each of the four states.
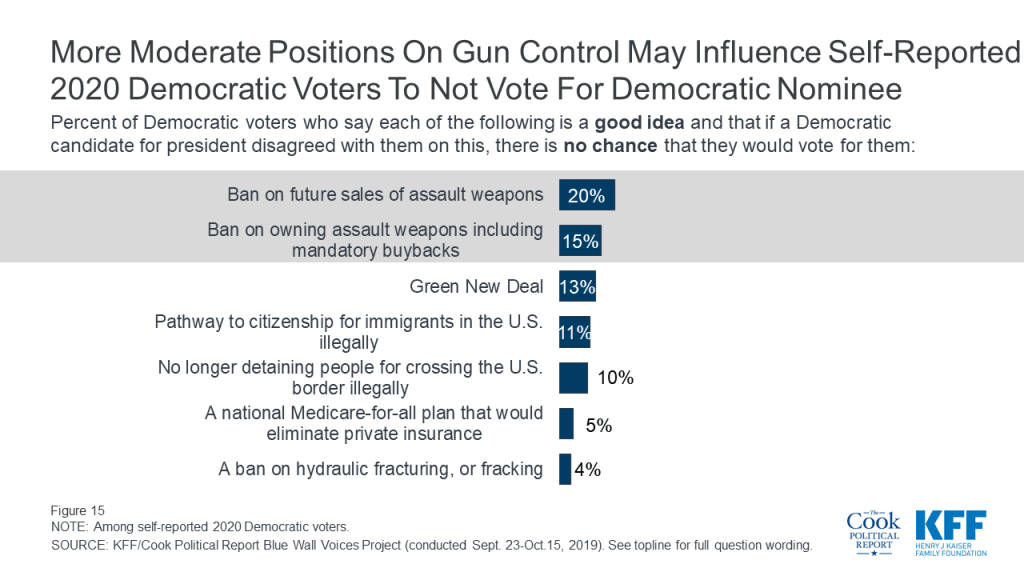
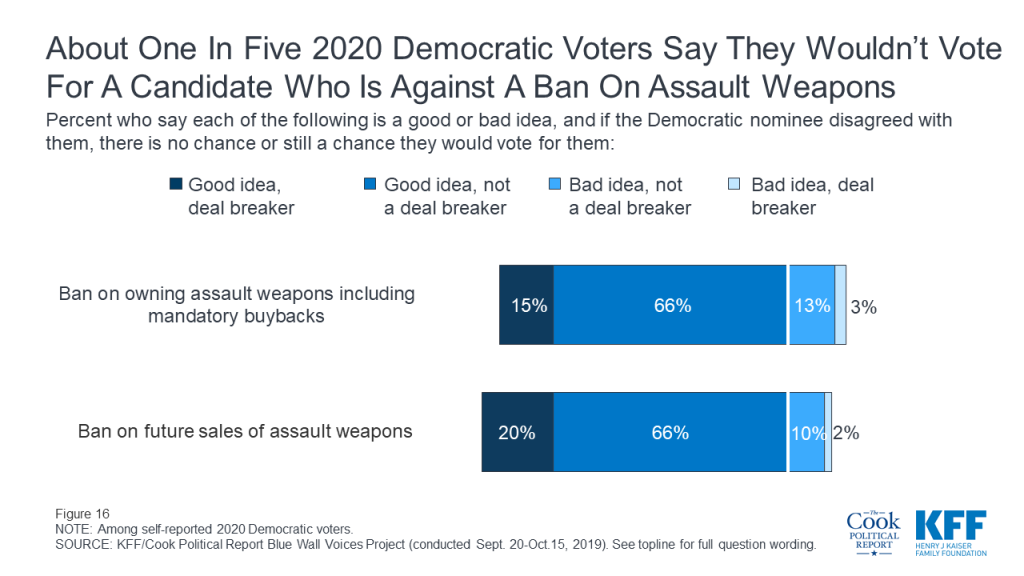
Yet, none of these issues are “deal breakers” with small shares of voters saying there is no chance they would vote for a candidate who disagreed with them on the issue. The positions that solicit that largest share of voters saying there is “no chance” they would vote for them are if a candidate was against a ban on future sales of assault weapons (20%), against a ban on ownership of assault weapons (15%), or against the Green New Deal (13%).
Few self-reported 2020 Democratic voters view any of the progressive ideas as deal breakers with less than 10% of Democratic voters saying the platforms are “bad ideas” and if a Democratic candidate disagreed with them on this, there is no chance they would vote for them.
Many likely 2020 Democratic voters see more moderate positions on assault weapon bans as possible deal breakers. One-fifth of self-reported 2020 Democratic voters say there is “no chance” they would vote for a candidate who was against a ban on the future sales of assault weapons and about one in eight (15%) 2020 Democratic voters say there is “no chance” they would vote for a Democratic nominee who was against a ban on owning assault weapons, including a mandatory buyback program.
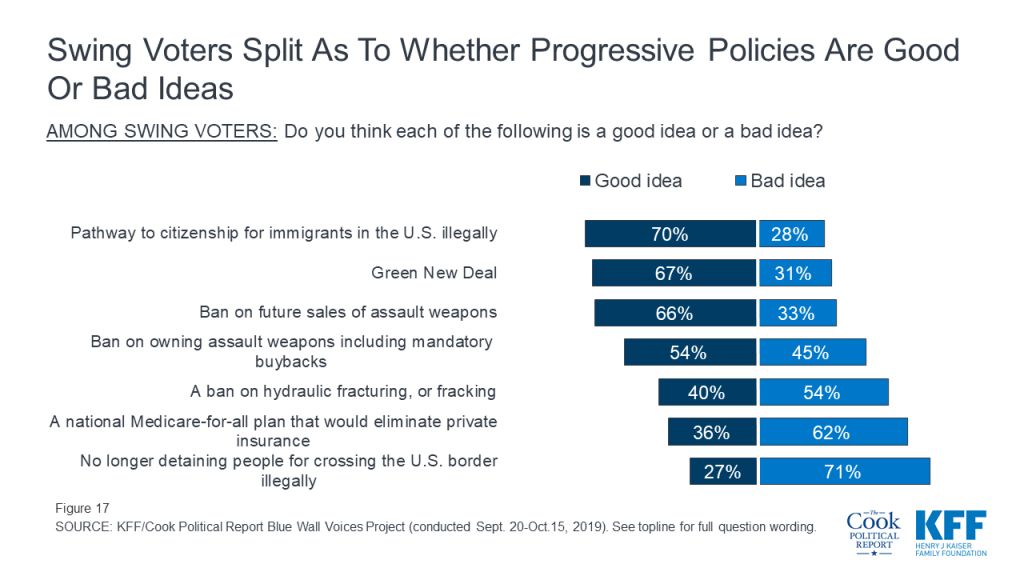
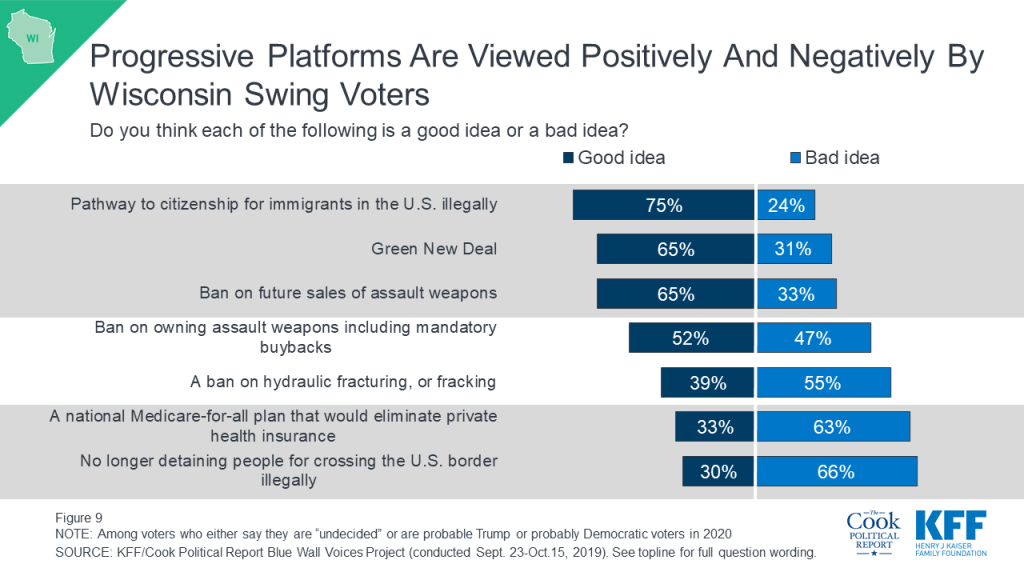
Majorities of swing voters, a crucial voting block in 2020, view a pathway to citizenship for immigrants in this country illegally (70%), the Green New Deal (67%), a ban on the future sale of assault weapons (66%), and a ban on the ownership of assault weapons including a mandatory buyback program (54%) as good ideas. Yet, many of these voters see three progressive platforms as “bad ideas.” Majorities of these voters view a ban on fracking (54%), a national Medicare-for-all plan (62%), and stopping border detainments of people coming into the country illegally (71%) as bad ideas.
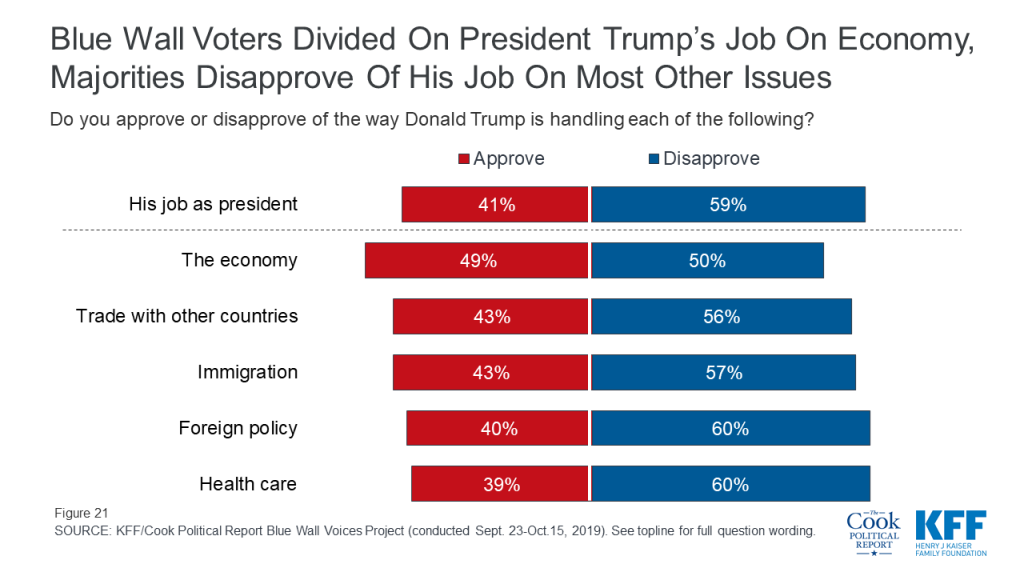
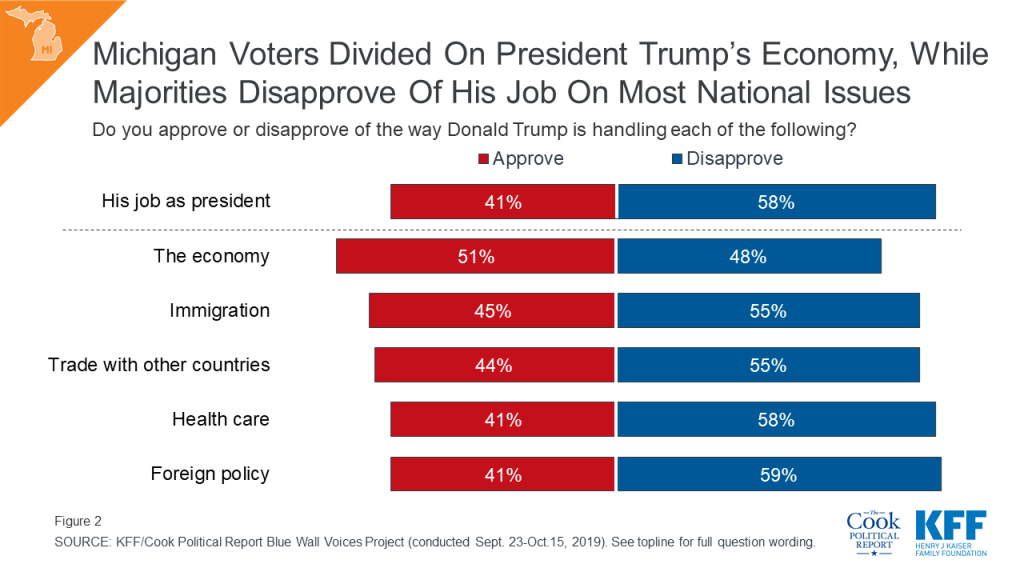
Health care and the economy are the top issues for voters in these states leading up to the 2020 presidential election but they are also two issues on which voters give President Trump very different marks. Voters give President Trump a somewhat positive rating (-1 percentage points) on the way he is handling the economy while a larger share of voters disapprove than approve of the way President Trump is handling health care (-21 percentage points net approval). Health care is one of the only issues in which President Trump’s approval is lower than his overall job approval (-18 percentage points). This report also examines the role of other key issues in the 2020 election such as immigration and international trade.
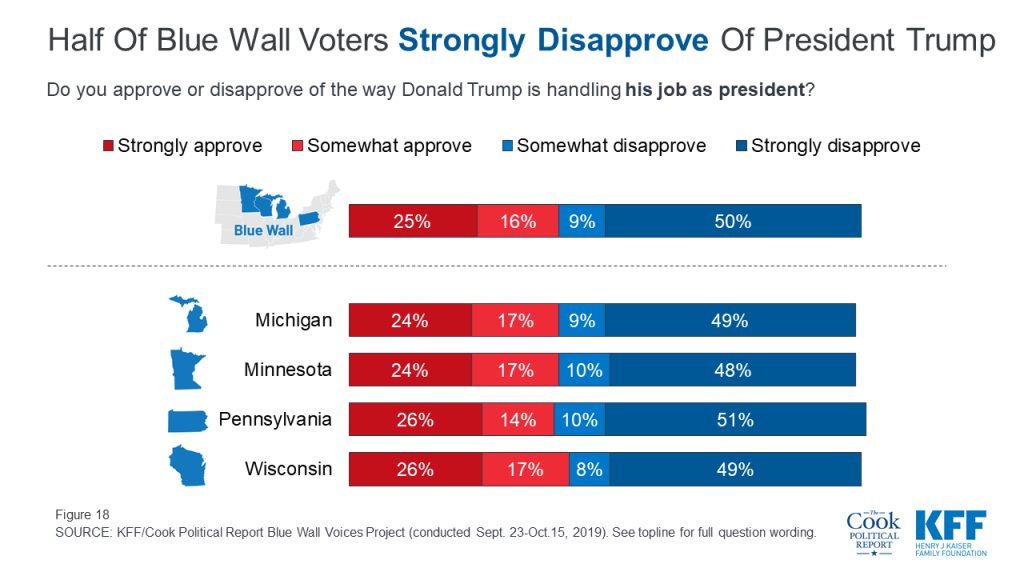
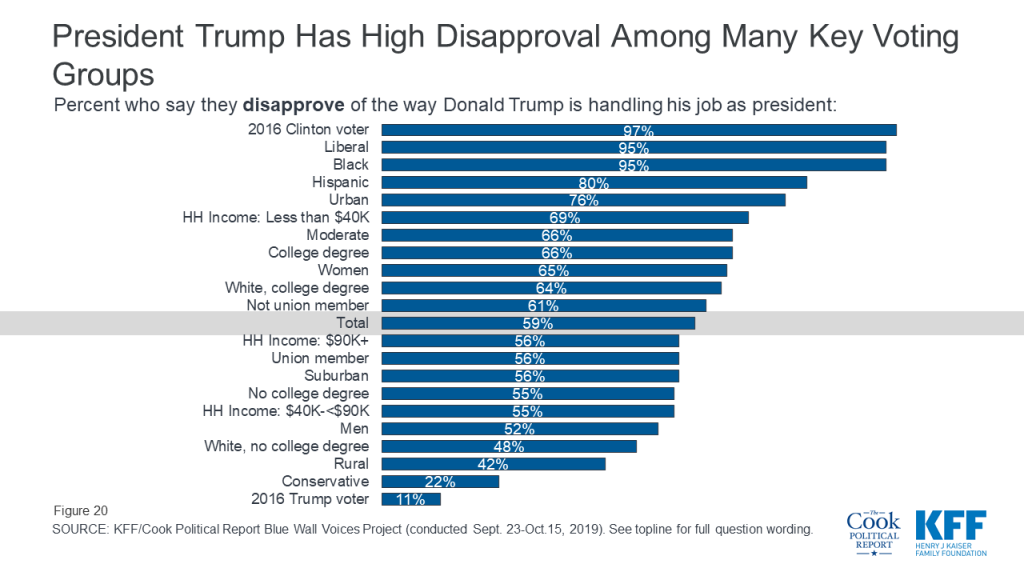
President Trump’s approval in each of the states as well as the Blue Wall overall is similar to what we see in national polls with about four in ten voters (41%) in the Blue Wall saying they either “strongly approve” or “somewhat approve” of the way Donald Trump is handling his job as president, while six in ten (59%) disapprove. If we look at the strongest opinions, twice as many voters “strongly disapprove” of the job President Trump is doing than “strongly approve” (50% v. 25%). About half of voters in each of the four states strongly disapprove of the way Donald Trump is handling his job as president.
Support for President Trump runs highest among his base including voters who voted for him in 2016 (89%), conservative voters (78%), and rural voters (57%).
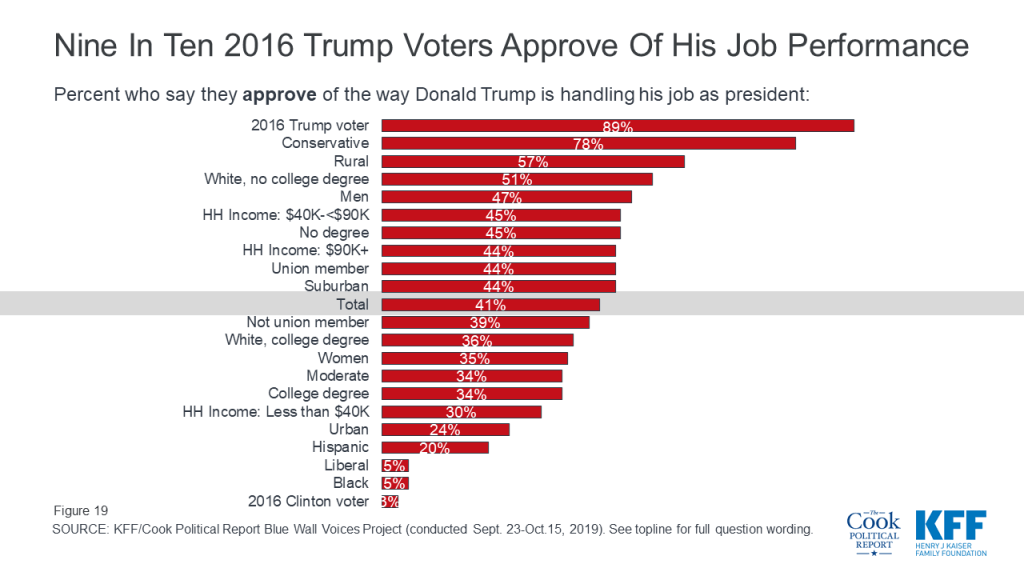
On the other hand, vast majorities of 2016 Clinton voters (97%) and liberal voters (95%) disapprove of his job performance. As do non-white voters across education groups, urban voters, voters earning less than $40,000 annually, moderate voters, and many more.
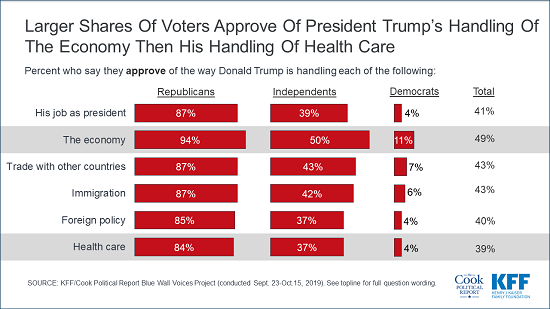
Voters in the Blue Wall states rank President Trump’s job performance most positively on the economy with about half of voters (49%) approving of the way Donald Trump is handling the economy. About four in ten voters approve of the job he is doing on the other issues including trade with other countries (43%), immigration (43%), foreign policy (40%), and health care (39%). There are no differences across the four states with similar shares of voters in Michigan, Minnesota, Pennsylvania, and Wisconsin approving of President Trump’s job on each of these key issues.
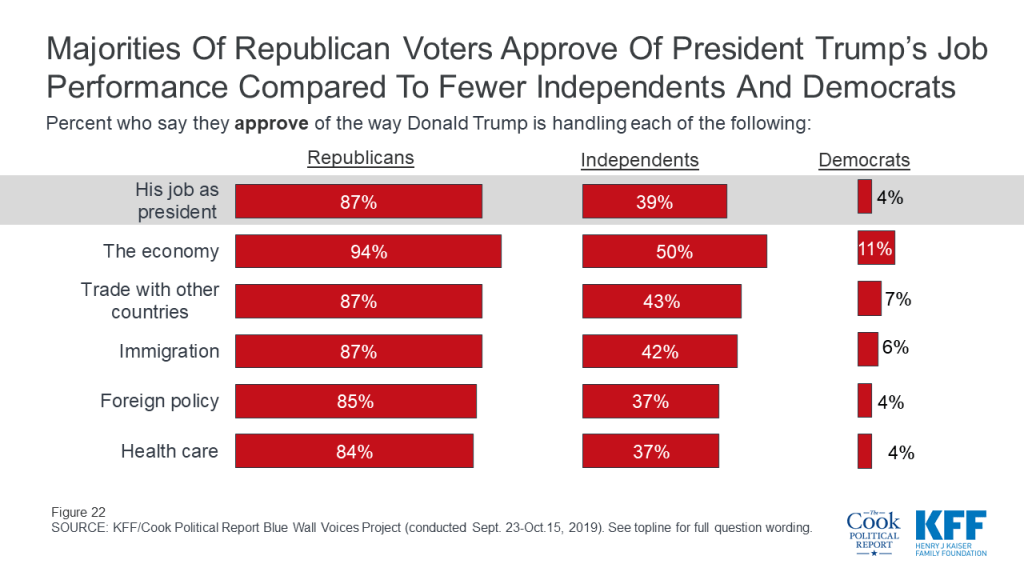
There are, however, unsurprisingly strong partisan differences. Large majorities of Republican voters approve of the job President Trump is doing on all of the issues while independent voters lean more negative in their assessments of President Trump’s job performance. Few Democratic voters approve of his job performance on any of the national issues included in the survey. Across the issues, President Trump ranks best in his handling of the economy with 94% of Republicans approving of the way he is handling the nation’s economy, as do half of independent voters and 11% of Democratic voters.
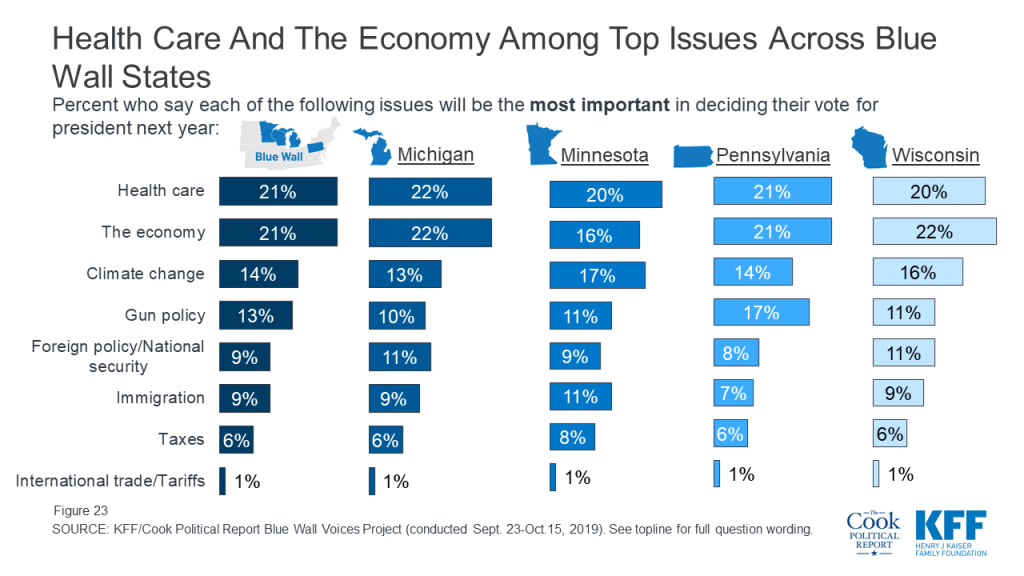
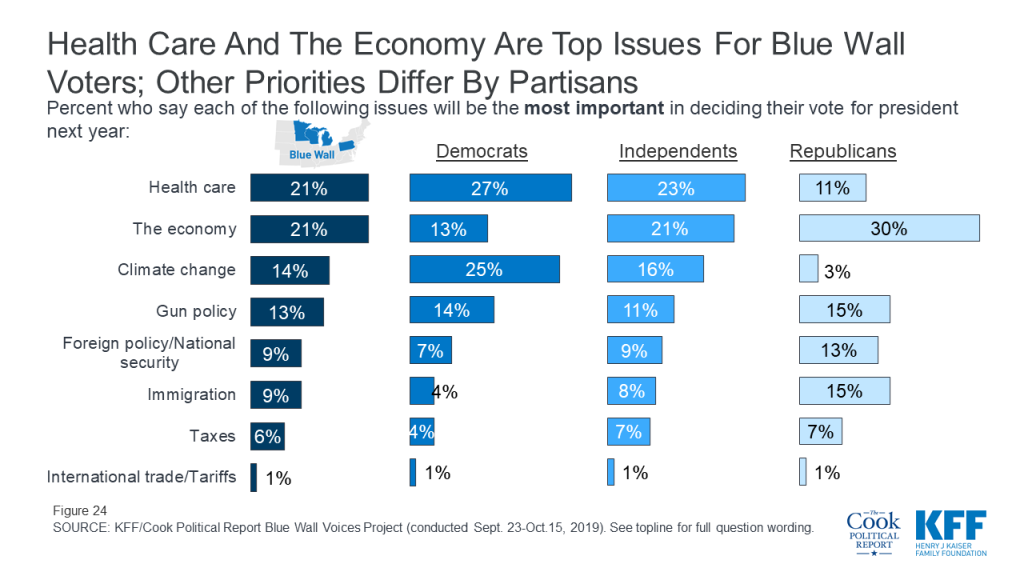
One year out from the 2020 general election, health care and the economy are the top two issues for voters. About one-fifth of voters say health care (21%) or the economy (21%) will be the most important issue in deciding their vote for president next year. These are followed by climate change (14%), gun policy (13%), foreign policy (9%), immigration (9%), taxes (6%), and international trade and tariffs (1%).
An Increased Interest in Foreign Policy?
The Blue Wall Voices Project was conducted September 23rd – October 15th, 2019. Two major foreign policy news stories happened during the field period including the U.S. House of Representatives’ impeachment inquiry and the Turkish invasion into Syria. While news regarding President Trump’s phone call with the Ukrainian President was released prior to the field period, House Speaker Nancy Pelosi announced a formal impeachment inquiry into Trump on September 24th. The news regarding his interactions with foreign leaders remained the top news for the weeks following as testimonies began before House committees. In addition, on October 12th President Trump’s administration announced that U.S. troops would be pulling back from northern Syria, subsequently allowing for Turkey forces to move into a region controlled by the Kurdish forces. Almost immediately, Turkey began assaults against Kurdish fighters and civilians in Syria. This lead to the U.S. to call on Turkey to stop the invasion and announce sanctions aimed at restraining the Turks’ assault. All of these events have led to an increase in the importance of foreign policy among voters in Michigan, Minnesota, Pennsylvania, and Wisconsin. Foreign policy and national security now rank alongside gun policy and immigration as the issues voters say will be the most important in deciding their vote for president next year.
Health care and the economy are the top issues across the Blue Wall states with Minnesota voters also selecting climate change as one of their top issues (17%). To see more about how partisans rank these issues in each state, check out the individual state reports.
The ranking of issues is largely driven by partisanship. Twice as many Republican voters say the economy will be the most important issue in deciding their vote for President next year than any other issue. Republicans rank the economy (30%), gun policy (15%), and immigration (15%) as the top issues in the presidential election. Democrats rank health care (27%) and climate change (25%) as the top issues. Independent voters choose health care (23%) and the economy (21%) as their top two issues.
Voters who are still undecided about their 2020 vote choice or haven’t made up their minds yet, our swing voters, rank the issues very similarly with health care and the economy as the top issues they say will be the most important in deciding their vote for president next year. In addition, health care and the economy are the top issues among swing voters in Michigan (23% and 25%), Minnesota (19% and 20%), Pennsylvania (19% and 24%), and Wisconsin (21% and 23%).
Health Care
Lowering prescription drug costs and making sure the ACA’s protections for people with pre-existing health conditions continue are the top health care priorities that voters want to see Congress take on next year. About two-thirds of voters (across states) say lowering prescription drug costs for as many Americans as possible should be a top priority for Congress which is similar to the share who say making sure the ACA’s protections for people with pre-existing conditions should be a top priority. These are the top health care priorities across voters in Michigan, Minnesota, Pennsylvania, and Wisconsin.

Lowering prescription drug costs ranks at the top of the list of health care priorities among all partisans (74% of Democratic voters, 69% of independent voters, and 62% of Republican voters). Making sure the ACA’s protections for people with pre-existing conditions continue is a top priority for both Democrats (83%) and independent voters (65%) while more than half of Republican voters (54%) say repealing and replacing the ACA is a top priority for Congress.

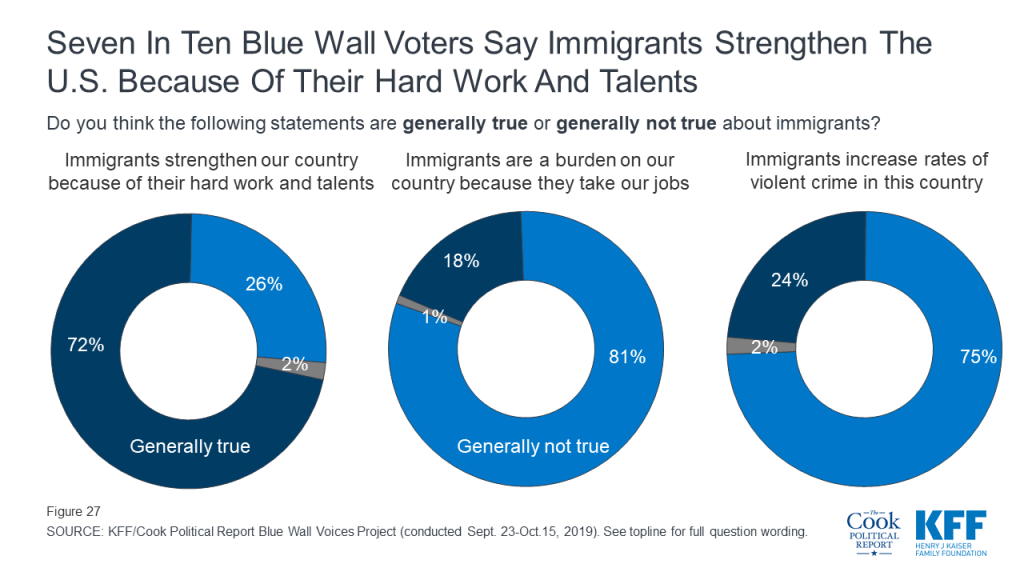
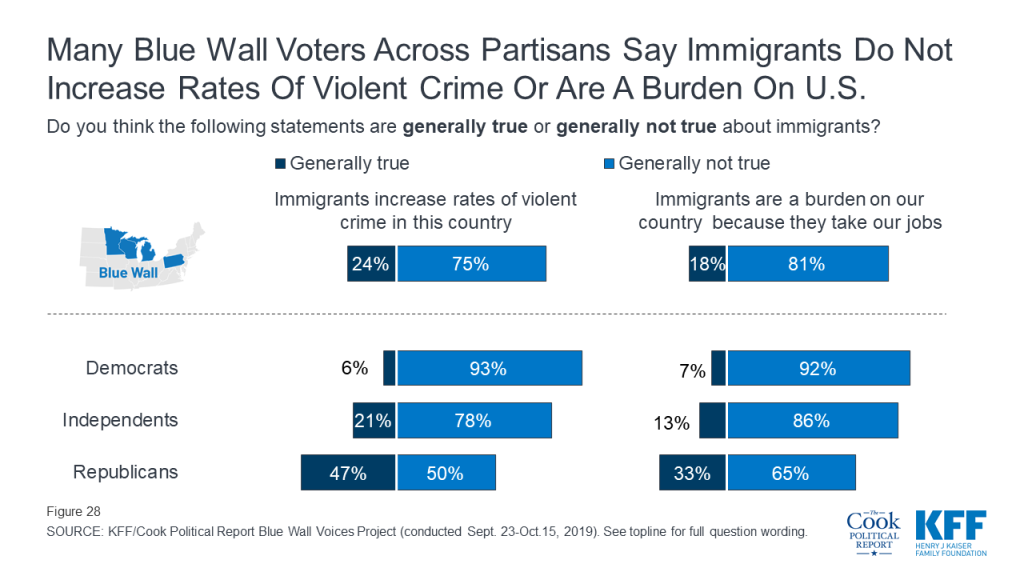
Overall, majorities of voters in each of the four states have positive views of immigrants in this country. Most say it is generally true that “immigrants strengthen our country because of their hard work and talents” (72%) and that it is generally not true that “immigrants are a burden on our country because they take their jobs” (81%) or “increase rates of violent crimes in this country” (75%).
While most Republican voters in Michigan, Minnesota, Pennsylvania, and Wisconsin say that it is generally not true that “immigrants are a burden because they take our jobs,” they are more divided on whether they think “immigrants increase rates of violent crime in this country.” Half of Republican voters say this is generally not true which is similar to the share who say it is generally true (47%).
While the economies of each of the states included in the Blue Wall Voices Project are distinct, the views of the economic outlook for the next year as well as views towards the fairness of the economic system are largely similar. The major differences in voters’ perceptions of the U.S. economy are mostly driven by party identification.
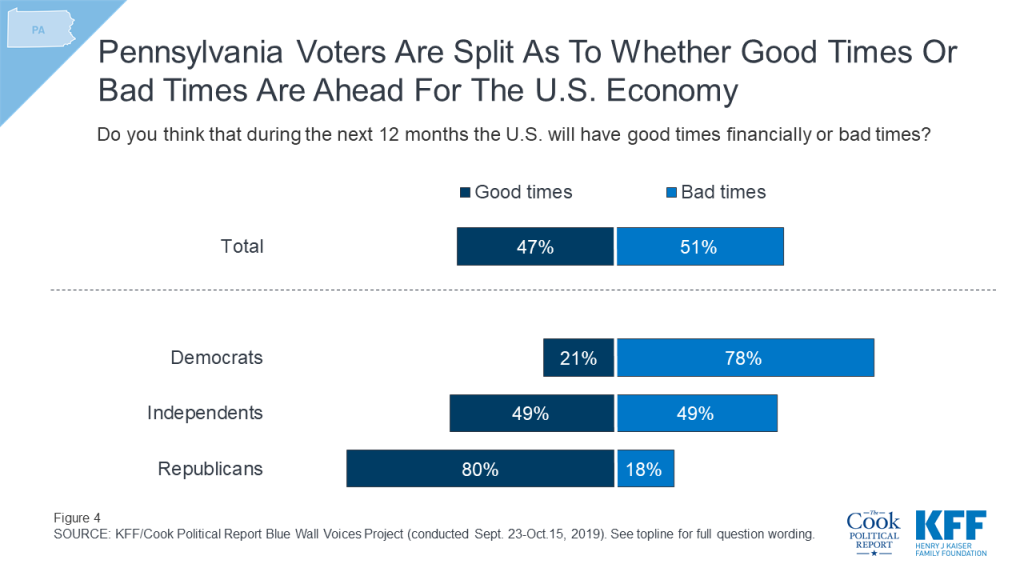
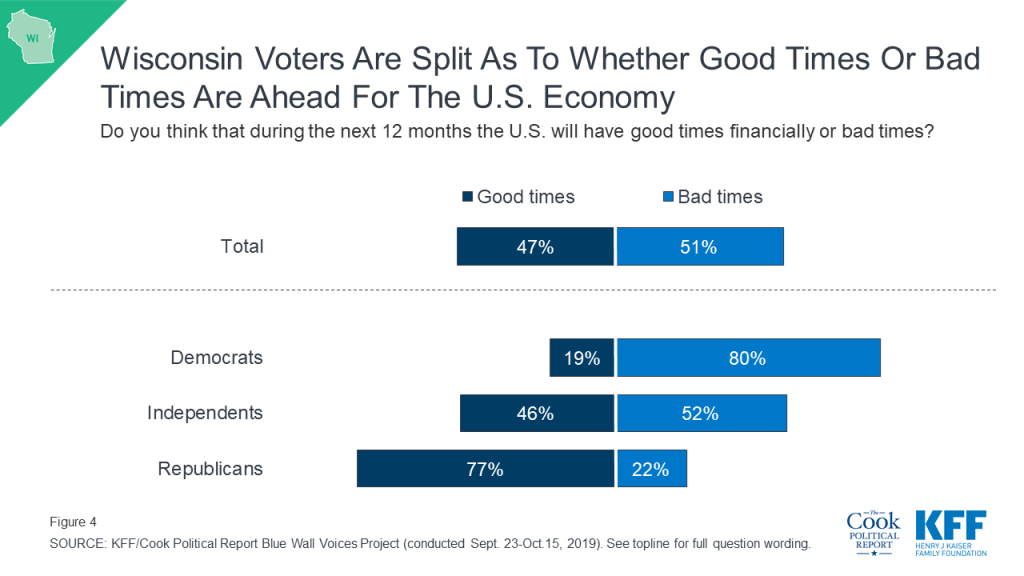
Voters are divided along party lines in their economic outlook for the next year with three-fourths (77%) of Democratic voters (across states) saying they expect that during the next 12 months the U.S. will have “bad times” while eight in ten Republicans (81%) say they expect the U.S. will have “good times.” Independent voters are split with similar shares saying they expect that during the next 12 months the U.S. will have good times financially (47%) as bad times (51%).

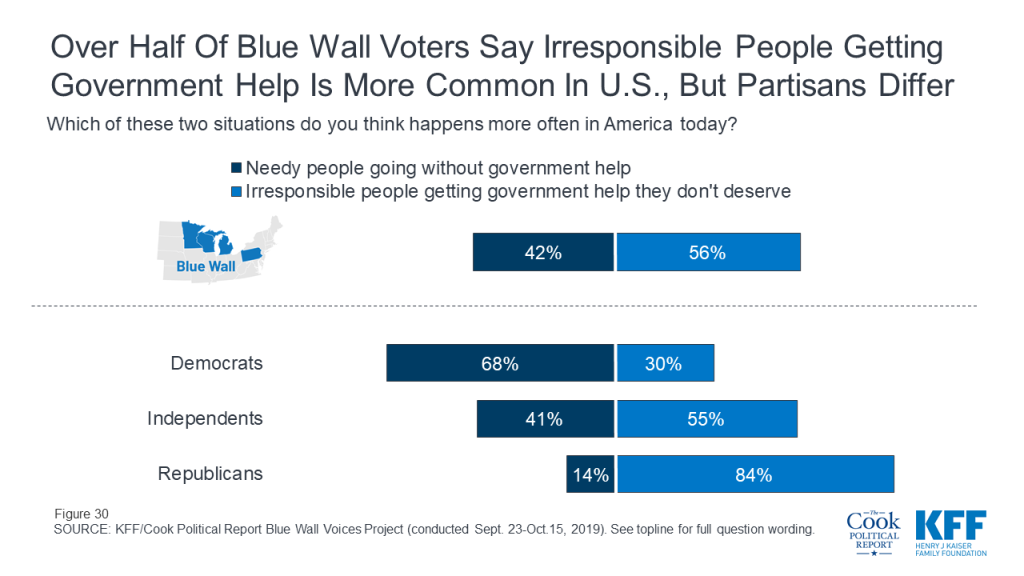
Views of the fairness current economic system are also largely partisan with larger shares of Democratic voters saying it is more often that “needy people go without government help in American today” (68%) than say it is more often that “irresponsible people get government help they don’t deserve” (30%). Republican voters view the system differently with the vast majority saying it is more often that “irresponsible people get government help they don’t deserve” (84%). A larger share of independent voters also say “irresponsible people getting government help they don’t deserve” happens more often in America today (55%).
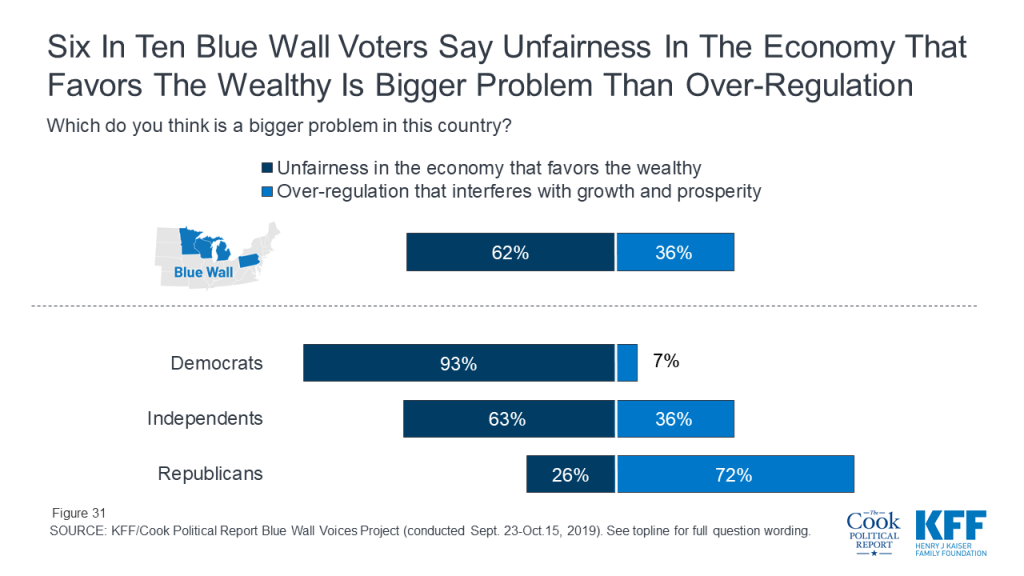
Six in ten voters (62%) say that “unfairness in the economy that favors the wealthy” is a bigger problem in this country while one-third of voters (36%) say “over-regulation that interferes with growth and prosperity” is a bigger problem. Nine in ten Democratic voters (93%) say unfairness in the economy is a bigger problem while seven in ten Republican voters (72%) say over-regulation is a bigger problem. Six in ten (63%) independent voters say unfairness in the economy is a bigger problem while 36% say over-regulation is a bigger problem.
With the U.S. engaged in a trade dispute with China and other countries, the Blue Wall Voices project sought to examine voters’ opinions of the possible impacts of the tariffs in Michigan, Minnesota, Pennsylvania, and Wisconsin.
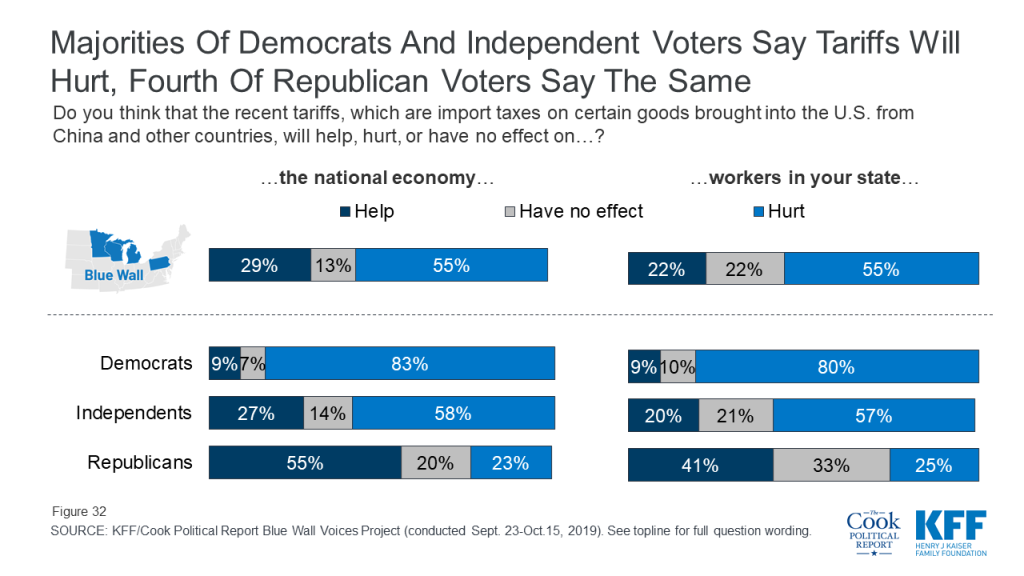
More than half of voters in the Blue Wall say the recent import taxes on certain goods brought into the U.S. from China and other countries will hurt both the national economy (55%) and workers in their state (55%). While these views are largely partisan, about one-fourth of Republican voters say the recent tariffs will hurt both the national economy (23%) and workers in their state (25%).
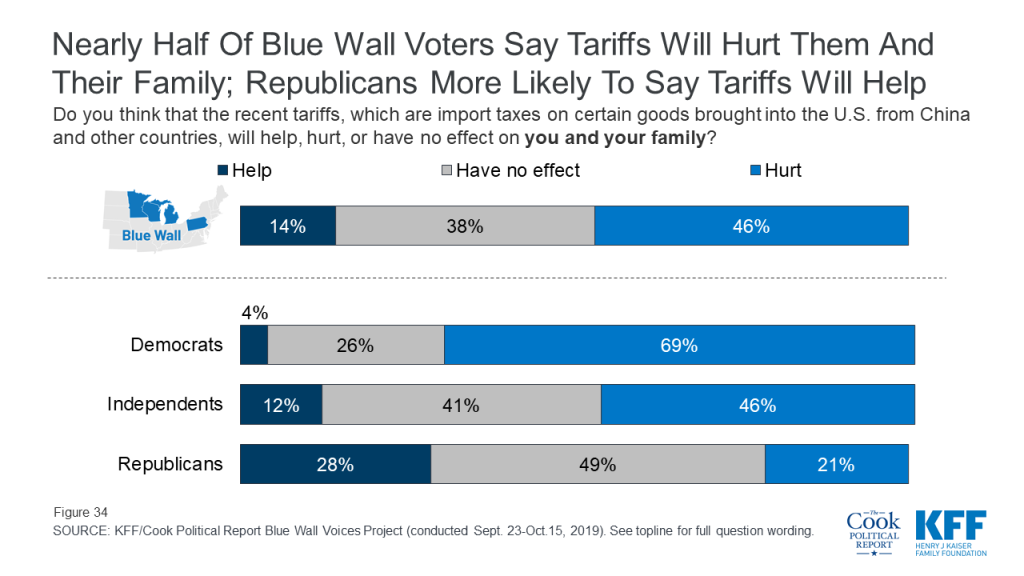
Overall, a larger share of voters in the Blue Wall say the recent tariffs will hurt rather than help them and their families, but a considerable share also say they expect the import taxes to have no effect. More than four in ten voters say the recent tariffs will hurt them and their family including roughly half of voters in Pennsylvania and Wisconsin.

Partisanship plays a large role in views of recent tariffs with seven in ten Democrats (69%) saying the tariffs will hurt them and their families compared to 46% of independent voters and 21% of Republican voters.
One key group that President Trump needs to retain support from in 2020 are rural voters. The poll indicates that currently President Trump has the support of rural voters in Michigan, Minnesota, Pennsylvania, and Wisconsin with larger shares of rural voters in each of the states saying they are either “definitely” or “probably” going to vote for President Trump than the Democratic nominee.
| Table 3: President Trump Currently Has Support Among Rural Voters In Upper Midwest | |||||
| TotalRural Voters | MichiganRural Voters | MinnesotaRural Voters | PennsylvaniaRural Voters | WisconsinRural Voters | |
| Definitely voting for President Trump | 32% | 29% | 38% | 35% | 28% |
| Probably going to vote for President Trump | 12 | 13 | 10 | 11 | 13 |
| Undecided | 27 | 29 | 24 | 27 | 27 |
| Probably going to vote for Democratic nominee | 6 | 4 | 7 | 4 | 10 |
| Definitely voting for Democratic nominee | 18 | 18 | 20 | 15 | 20 |
A key issue for this group is the economy with large shares of rural voters in each of the states saying the economy is among the most important issues when deciding their vote next year. And most rural voters approve of the way President Trump is handling the economy with about two-thirds of rural voters in Michigan (66%), Minnesota (65%), Pennsylvania (66%), and Wisconsin (61%) saying they either “strongly approve” or “somewhat approve.” In addition, majorities of rural voters in each state say they expect the U.S. will have good times financially during the next 12 months.
Rural voters are currently less negative in their assessment of how the recent tariffs will hurt workers in their state, the national economy, or their family than suburban and urban voters. But still about half of rural voters say the recent tariffs will hurt workers in their state (47%) and the national economy (45%), while about four in ten (39%) say the recent tariffs will hurt them and their families.
The Blue Wall Voices Project examines voters in the state of Michigan to get their perspectives on key issues and aspects of the 2020 election, including the role that health care and the economy may play in voters’ decisions. In addition, it gauges enthusiasm and vote choice leading up to the 2020 presidential election.
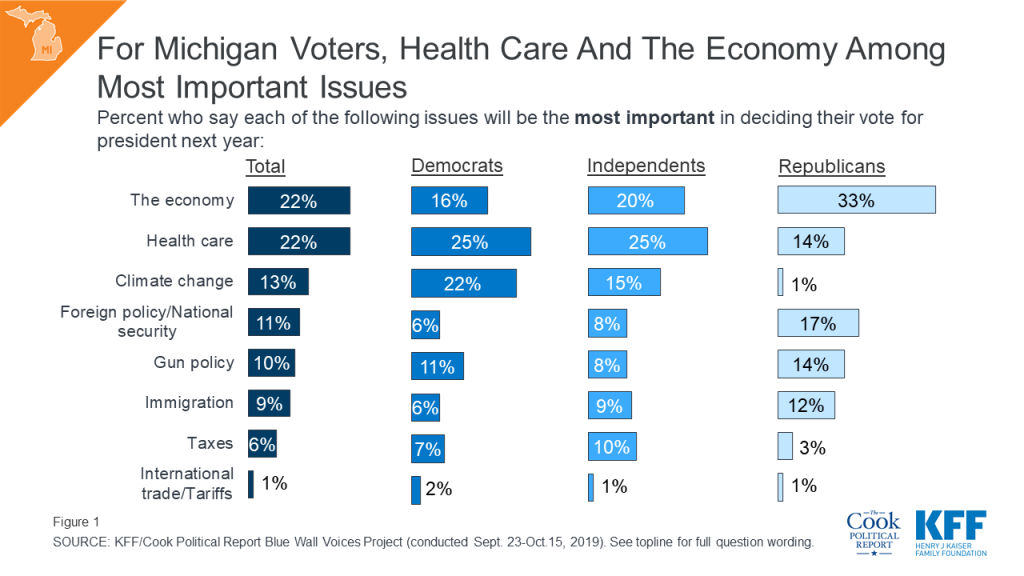
Overall, a larger share of Michigan voters say health care and the economy are the most important issues in deciding their vote for president in 2020. About one in five Michigan voters say health care (22%) and the economy (22%) are the most important issues to their vote, with smaller shares saying issues like climate change (13%), foreign policy and national security (11%), gun policy (10%), immigration (9%), taxes (6%), and international trade and tariffs (1%). Partisans are divided in their priorities, with one in four Democrats and independents choosing health care as their top issue, and one-third of Republicans choosing the economy as the most important issue.
With health care and the economy ranking above all other issues for Michigan voters, it is important to note that Michigan voters give President Trump very different marks on both of these issues. Half (51%) of Michigan voters approve of the way President Trump is handling the economy compared to four in ten (41%) who approve of the way he is handling health care.
While voters do not rank international trade as one of the most important issues in deciding their vote next year, Michigan is a state expected to be most affected by the ongoing trade disputes with China and other countries. Overall, about half of voters – including majorities of Democrats and independents – say they think the recent tariffs will hurt both the national economy (54%) and workers in Michigan (53%). However, this opinion is only shared by about one-fourth of Republican voters (21% and 26%, respectively) compared to majorities of Democrats (80% and 78%, respectively) and independent voters (58% and 57%, respectively). Six in ten Republican voters in Michigan (61%) say the recent tariffs will “help” the national economy and about four in ten (41%) say the tariffs will “help” Michigan workers.

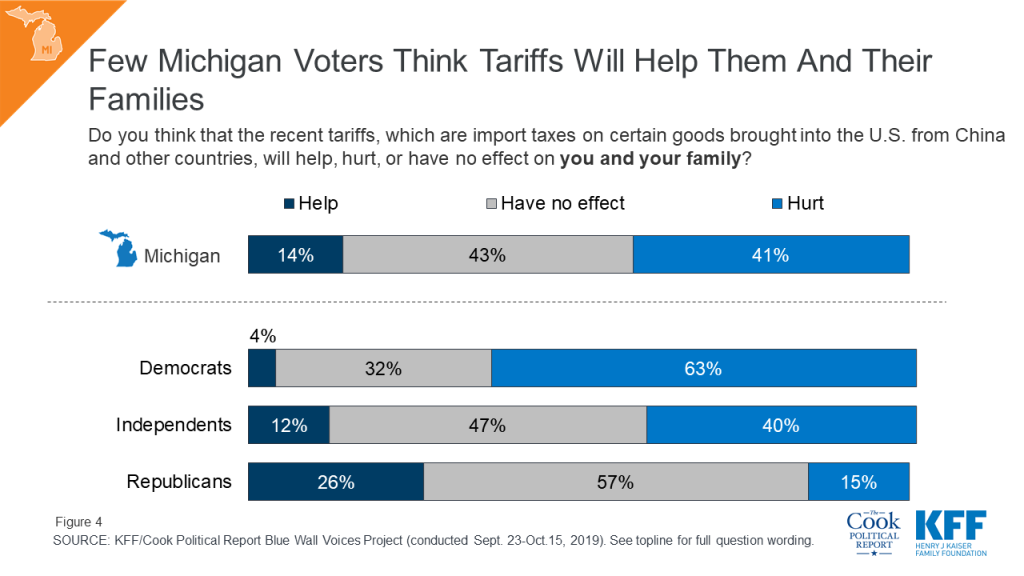
Partisans also differ in how they perceive the recent tariffs will impact them and their families. More than six in ten Democratic voters in Michigan (63%) say the recent tariffs will hurt them and their families while about half of independent voters (47%) and a majority of Republican voters (57%) in the state say they will “have no effect.” Overall, few voters (14%) say the recent tariffs will help them and their families.
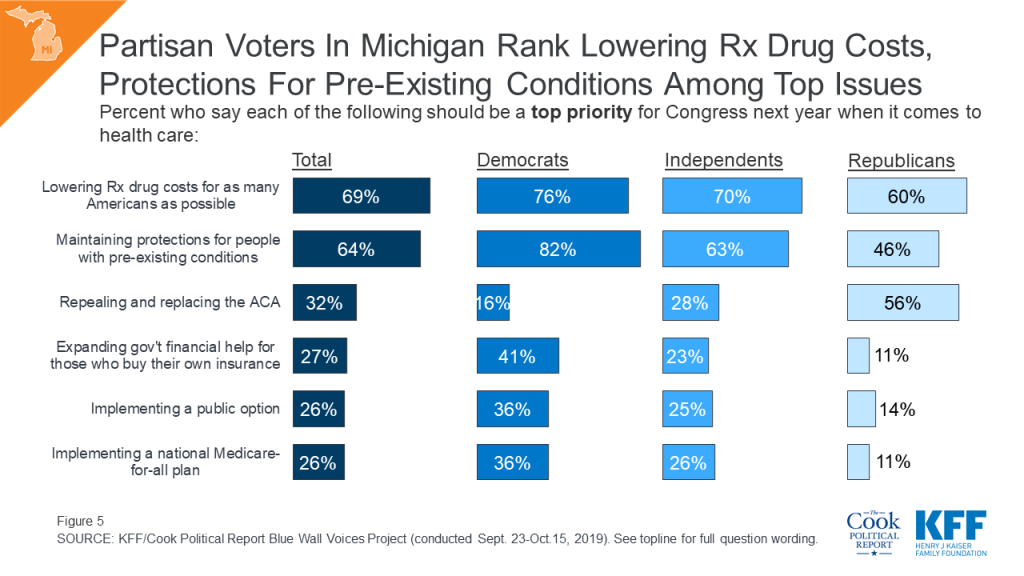
When asked specifically about health care priorities that Congress should work on next year, over six in ten say that lowering prescription drug costs (69%) and maintaining protections for people with pre-existing conditions (64%) should be the top priority for Congress. These priorities substantially outrank other policy proposals such as repealing and replacing the ACA, expanding government aid for people who buy their own health insurance, and implementing a public option or national Medicare-for-all plan. These top two priorities persist across partisans, with large shares of Democratic voters, independent voters, and Republican voters naming lowering prescription drug costs and maintaining pre-existing condition protections as top priorities. However, over half of Republican voters (56%) also say that repealing and replacing the ACA should be a top priority. Implementing a national Medicare-for-all plan, a topic that has dominated health care discussions in the 2020 Democratic primary, is not a top issue for all voters or for Democratic voters, specifically.
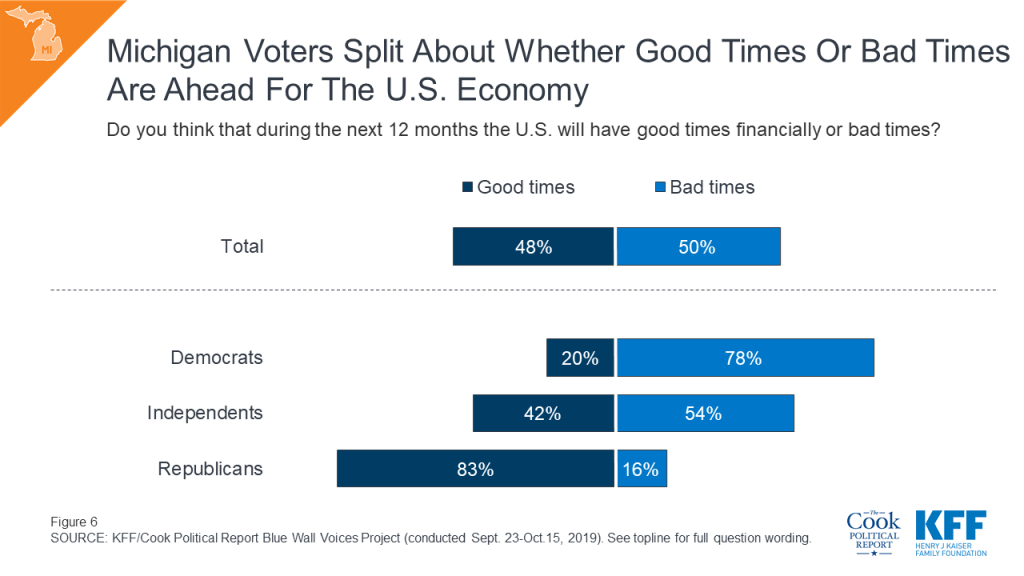
Turning to the economy, the other top issue for voters during the 2020 election, voters in Michigan are split about what they think the economic forecast will be like for the next 12 months. Similar shares of Michigan voters say that during the next 12 months, the U.S. will have bad times (50%) and good times (48%). Views on the economic outlook are largely partisan with roughly eight in ten Democrats (78%) saying bad times are ahead and roughly eight in ten Republicans saying good times are ahead (83%). Independent voters are more divided, with four in ten saying the U.S. will experience “good times” while 54% say they expect “bad times” ahead.
More than half of Michigan voters say they are more motivated (55%) to vote in next year’s election than in the previous presidential election. This includes a majority of Democrats (65%), independents (61%) and Republicans (53%) saying they feel more motivated than they did in 2016. Yet, similar to other states included in this analysis, a larger share of Democratic voters say they are “more motivated” than the share of Republican voters who said the same.

Given the high levels of motivation as the next presidential election approaches, the Blue Wall Voices survey explored what could be motivating voters. When asked specifically what the one thing is that will motivate them to vote in the 2020 election, voters offer an array of open-ended responses, with the most frequently volunteered response relating to defeating President Trump (21%), followed by those who offered responses related to civic duty (10%) and health care (8%). Small shares of voters cited reasons such as wanting to re-elect Trump and not wanting to elect a Democrat (6%), or the economy (5%).
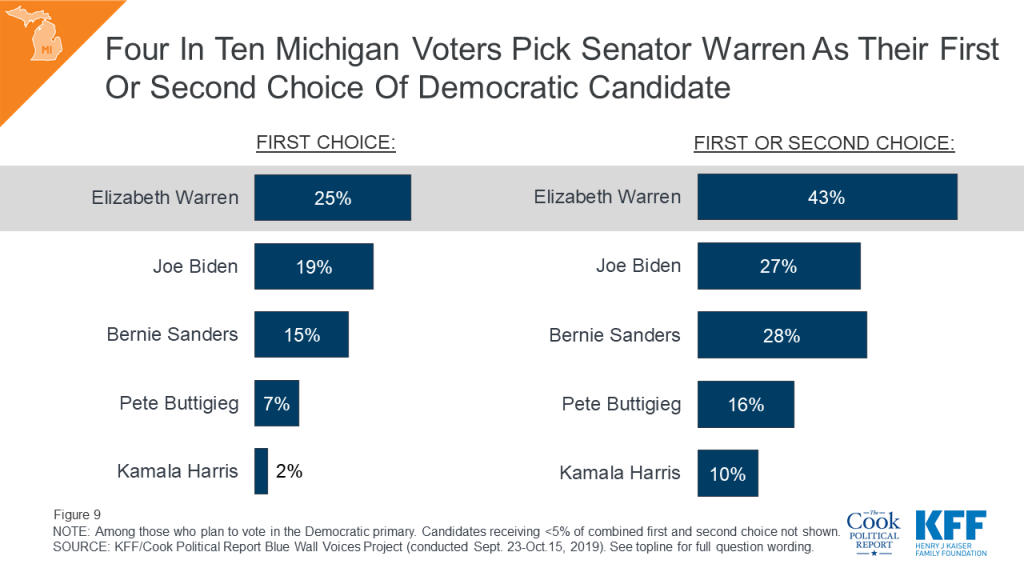
With more than four months before the 2020 Michigan Democratic primary, Senator Elizabeth Warren garners the most support among likely Democratic primary voters followed by Vice President Joe Biden and Senator Bernie Sanders. One-fourth of Michigan Democratic primary voters say Senator Warren is their first choice for the 2020 Democratic ticket and a combined 43% of voters say she is their first choice or second choice.
Overall, many voters (43%) in the state remain uncertain about who they will support in the 2020 election. One-third of Michigan voters say they are definitely voting for the Democratic nominee and about one-fifth (21%) say they are definitely voting for President Trump. In contrast, one-fourth of voters say they are undecided, and few voters say they are either probably voting for the Democratic nominee (6%) or for President Trump (11%). This poll finds there are few persuadable Michigan voters meaning that, while they currently support one candidate, they could be convinced to support the other party’s candidate.

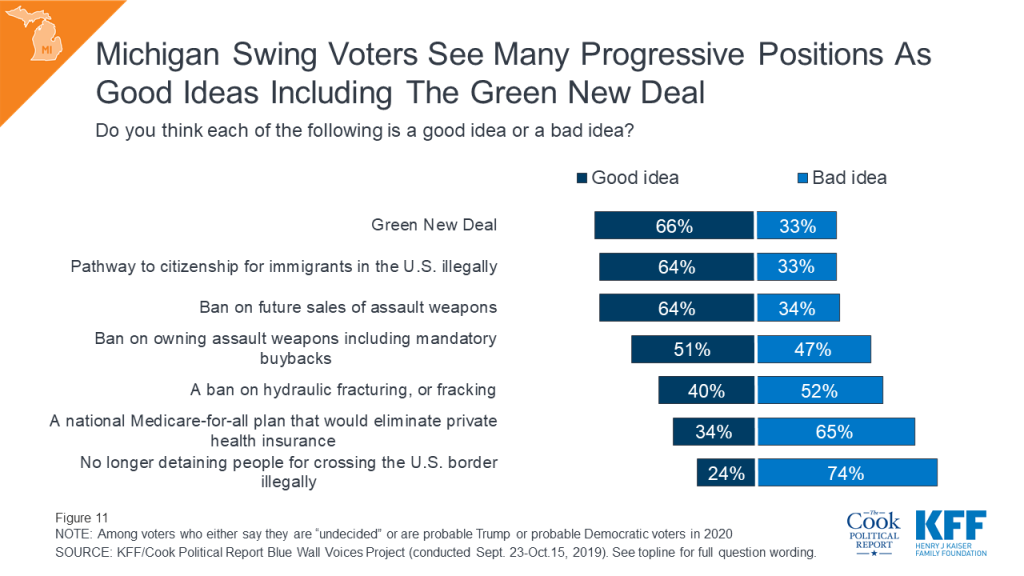
Michigan swing voters (those who are either undecided voters or say they are probable but not definite Trump or Democratic voters) are supportive of three progressive platforms: the Green New Deal, a pathway to citizenship for immigrants, and a ban on future sales of assault weapons. But, on the other progressive platforms included in this project, Michigan voters are either split or a majority say they are a bad idea. This includes two-thirds of Michigan swing voters (65%) who say a national Medicare-for-all plan is a “bad idea.”
The Blue Wall Voices Project examines voters in the state of Minnesota to get their perspectives on key issues and aspects of the 2020 election, including the role that health care and the economy may play in voters’ decisions. In addition, it gauges enthusiasm and vote choice leading up to the 2020 presidential election.
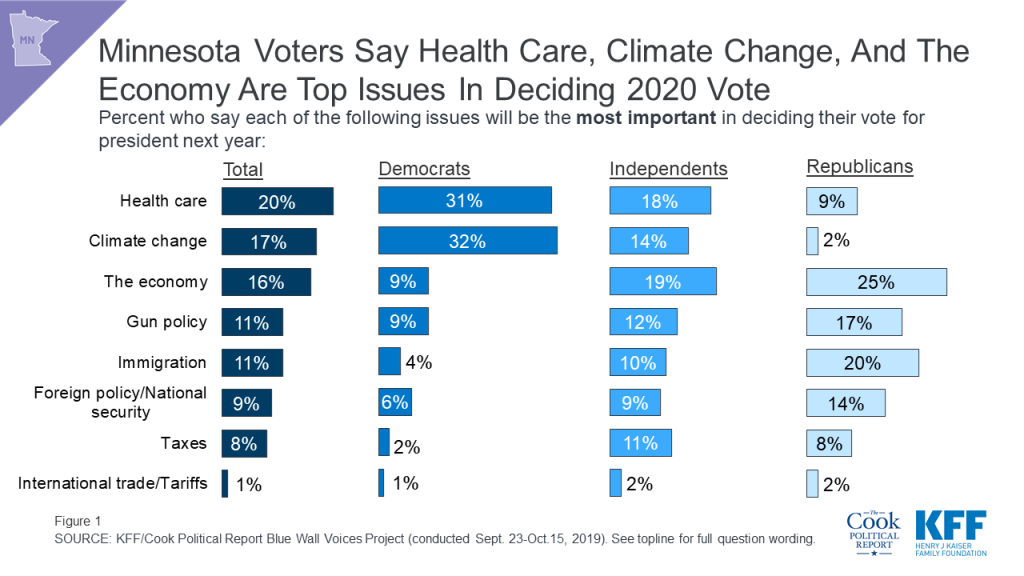
Overall, Minnesota voters say that a number of issues will be the most important in deciding their vote for president in 2020, with health care, the economy, and climate change emerging as the top issues. About one in five Minnesota voters say health care (20%), climate change (17%), and the economy (16%), are the most important issues to their vote, with smaller shares naming issues like gun policy (11%), immigration (11%), foreign policy and national security (9%), taxes (8%), and international trade and tariffs (1%). Partisans are divided in their priorities with three in ten Democrats ranking health care and climate change as their top issues, about two in ten independents ranking health care and the economy as their top issues, and one-fourth of Republicans ranking the economy as the most important issue and one in five saying immigration will be the most important issue in deciding their 2020 vote choice.
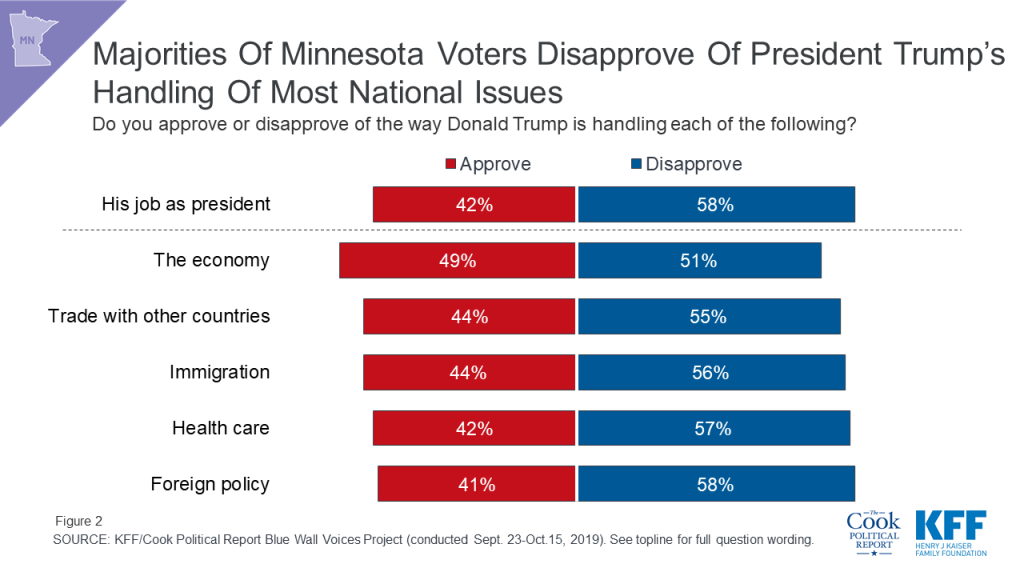
Overall, a majority of Minnesota voters disapprove of President Trump’s job performance (58%) while four in ten voters approve (42%). In addition, most Minnesota voters also disapprove of the way he is handling foreign policy (58%), health care (57%), immigration (56%), and trade with other countries (55%). Minnesota voters are more divided in their views of how President Trump is handling the economy with 49% of voters saying they approve compared to 51% who disapprove.
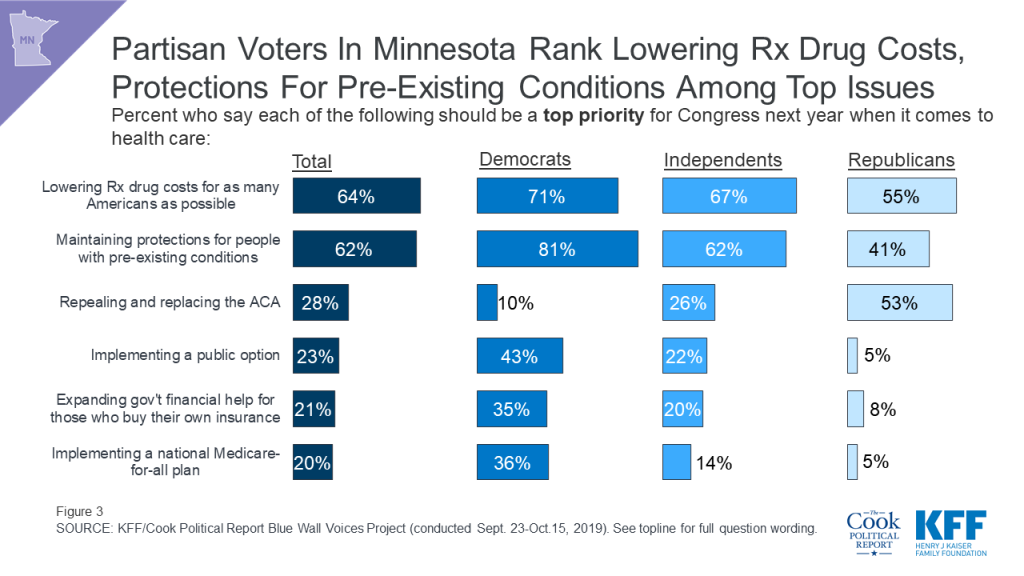
When asked specifically about health care priorities that Congress could work on next year, over six in ten say lowering prescription drug costs (64%) and maintaining protections for people with pre-existing conditions (62%) should be the top priority for Congress. These priorities substantially outrank other policy proposals such as repealing and replacing the Affordable Care Act (28%), expanding government financial help for people who buy their own health insurance coverage on the ACA marketplace to include more people (21%), and implementing a public option (23%) or national Medicare-for-all plan (20%). These top two priorities persist across partisans, with large shares of Democratic, independent, and Republican voters naming lowering prescription drug costs and maintaining pre-existing condition protections as top priorities. However, over half of Republican voters (53%) also say that repealing and replacing the ACA should be a top priority. Implementing a national Medicare-for-all plan, a topic that has dominated health care discussions in the 2020 Democratic primary, is not a top priority for a majority of voters or for Democratic voters, specifically.
Turning to the economy, the other top issue for voters during the 2020 election, Minnesota voters are optimistic about the U.S. economic forecast over the next 12 months. About half of Minnesota voters say that during the next 12 months, the U.S. will have “good times” (53%), compared to a slightly smaller share who say the U.S. will experience “bad times” (44%). Views towards the U.S. economy are largely partisan with two-thirds of Democrats (68%) saying bad times are ahead, while over eight in ten Republicans (84%) say the U.S. will experience “good times” financially. Independent voters are more divided, but lean positive with 54% saying they expect “good times,” while 44% say the U.S. economy will experience “bad times” over the next year.

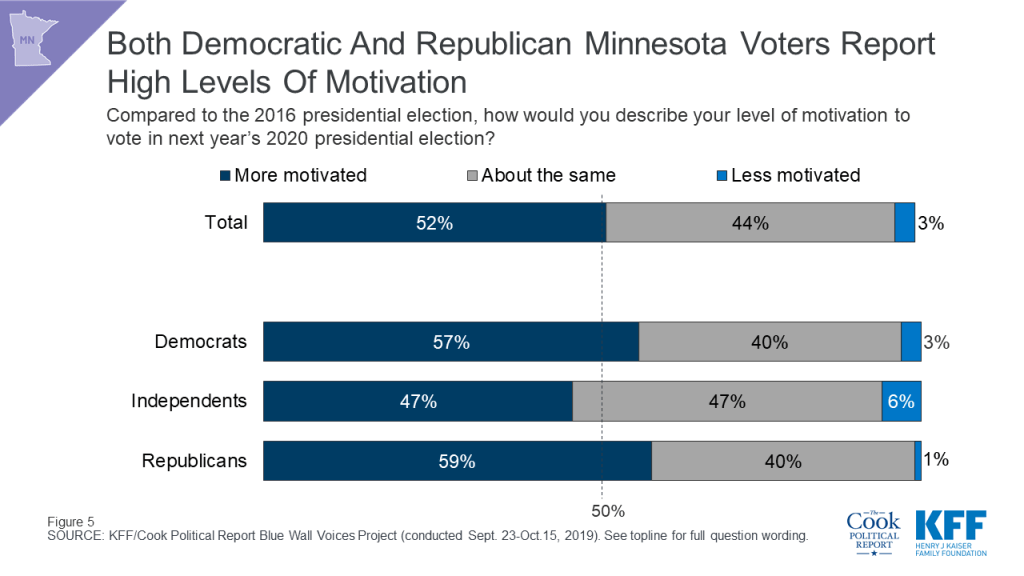
Slightly over half of Minnesota voters say they are more motivated (52%) to vote in next year’s election than in the previous presidential election. This includes majorities of Democrats (57%) and Republicans (59%) and nearly half of independents (47%) saying they feel more motivated than they did in 2016.
Given the high levels of motivation as the next presidential election approaches, the Blue Wall Voices survey explored what could be motivating voters. When asked specifically what the one thing is that will motivate them to vote in the 2020 election, voters offer an array of responses, with the most frequently volunteered response related to defeating Trump (18%), followed by those who offered responses related to civic duty (11%). Smaller shares cite reasons such as to re-elect Trump or not wanting a Democrat (9%), health care (6%), a candidate with good ethics (4%), and the environment or climate change (4%).

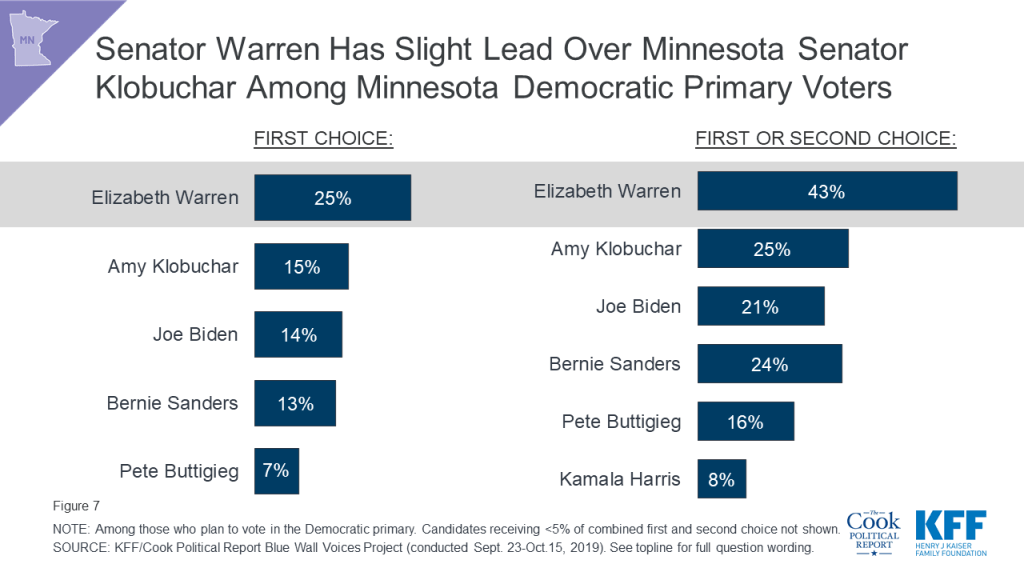
With more than four months left before the 2020 Minnesota Democratic primary, Senator Elizabeth Warren garners the most support among likely Democratic primary voters followed by Minnesota Senator Amy Klobuchar, Vice President Joe Biden, and Senator Bernie Sanders. One-fourth of Minnesota Democratic primary voters say Senator Warren is their first choice for the 2020 Democratic ticket and a combined 43% of voters say she is their first choice or second choice.
About one-third of Minnesota voters say they are “definitely voting for the Democratic nominee” (32%) and about one-fourth (24%) say they are “definitely voting for President Trump.” Many voters (41%) in the state remain uncertain about who they will support in the 2020 general election. Of that 41%, two in ten voters say they are “undecided” (21%), and about one in ten say they are either “probably voting for the Democratic nominee” (10%) or “probably voting for President Trump” (10%). This poll finds few persuadable Minnesota voters, meaning that, while they currently support one candidate, they could be convinced to support the other party’s candidate. Three percent of all Minnesota voters say that they are probably going to vote for President Trump, but there is “a chance” they will vote for the Democratic nominee. On the other side, 1% of Minnesota voters say that they are probably voting for the Democratic nominee, but there is “a chance” they will vote for President Trump.
Minnesota swing voters (those who are undecided or say they are probably going to vote for either President Trump or the Democratic nominee) have very different views on two key immigration issues. While three-fourths of Minnesota swing voters (76%) think a pathway to citizenship for immigrants who are in the country illegally is a “good idea,” two-thirds think stopping detainments at the U.S. border for people who are coming into the country illegally is a “bad idea.”
On other progressive platforms, Minnesota swing voters have positive views towards a ban on future sales of assault weapons (68%) and a Green New Deal that would address climate change through new regulations and increases in government spending on green jobs and energy-efficient infrastructure (64%), but say a national Medicare-for all plan is a “bad idea” (63%). Minnesota swing voters are more divided in their views towards a ban on owning assault weapons including a mandatory buyback program (54% say it is a “good idea,” while 46% say it is a “bad idea”) and a ban on fracking (42% say it is a “good idea,” while 50% say it is a “bad idea”).

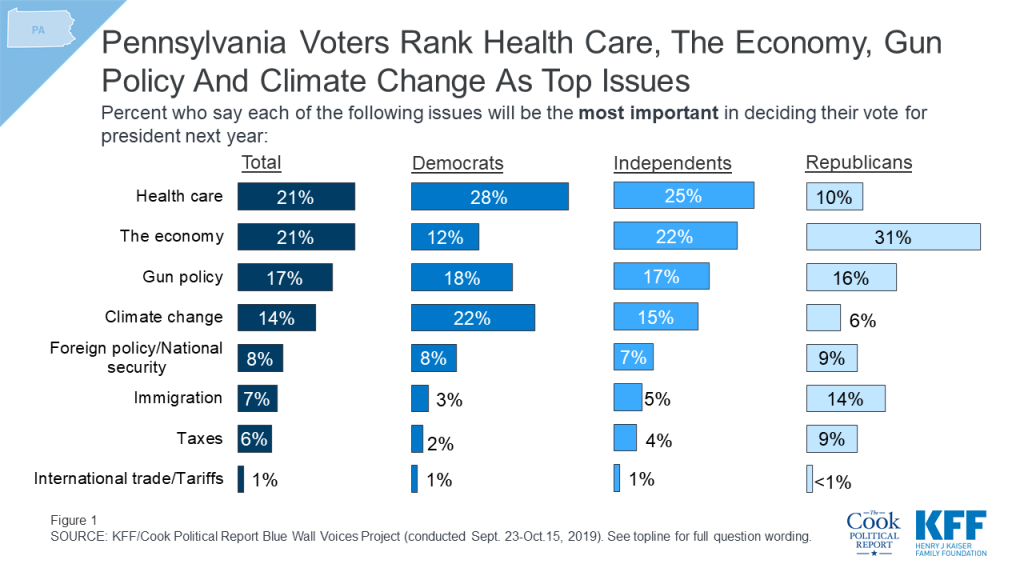
The Blue Wall Voices Project examines voters in Pennsylvania, a state that President Trump won by less than one percentage point (approximately 44,000 votes) over Democratic candidate Hillary Clinton in 2016. This poll finds that health care is among the top issues for voters more than one year out from the general election and examines enthusiasm and vote choice leading up to the 2020 presidential election.
Health care ranks among the top issues for voters leading up to the 2020 presidential election along with the economy, gun policy, and climate change. Health care is the top issue for Democratic voters (28%) and ranks among the top issue for independent voters (25%), but ranks lower among Republican voters. In fact, among Republican voters, health care ranks below the economy (31%), gun policy (16%), and immigration (14%), and alongside foreign policy or national security (9%) and taxes (9%), with one in ten Republican voters saying health care will be the most important issue in deciding their vote next year.
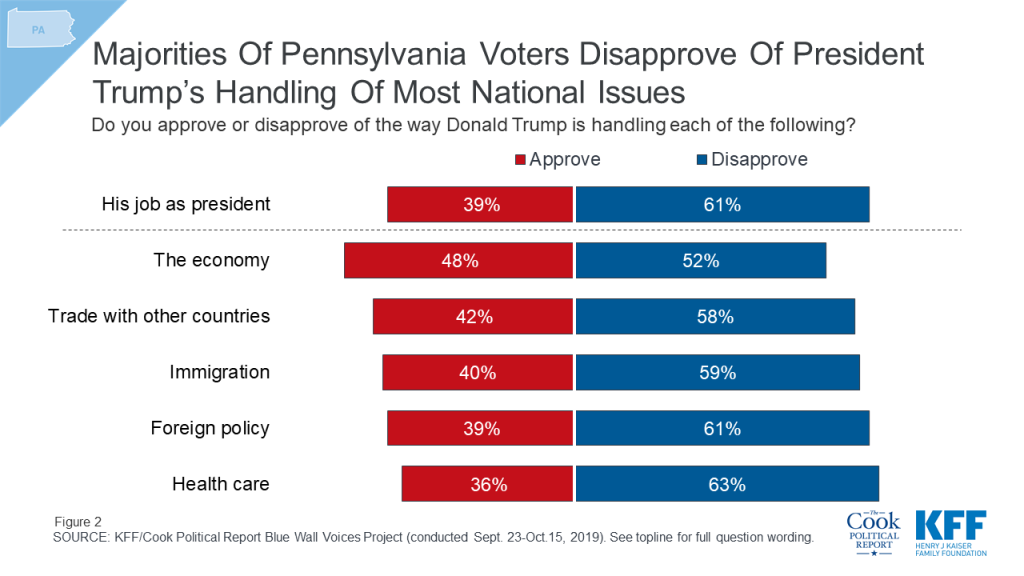
Similar to the overall Blue Wall, Pennsylvania voters are most positive in their views of the way President Trump has handled the economy with nearly half (48%) of Pennsylvania voters saying they approve of his job performance on this issue. On the other hand, more than six in ten Pennsylvania voters (63%) say they disapprove of the way he has handled health care. Both of these issues appear to be key issues leading up to the 2020 presidential race.
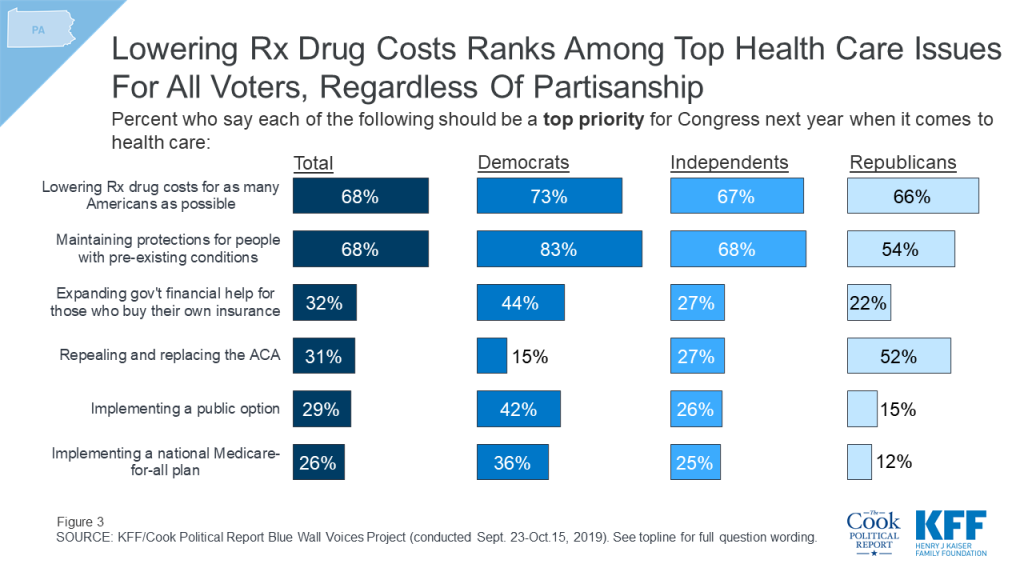
While Medicare-for-all has dominated most of the health care discussions on the 2020 Democratic campaign trail, it ranks low among the priorities that the public has for Congress next year. One-fourth (26%) of Pennsylvania voters say implementing a national Medicare-for-all plan is a “top priority” for Congress compared to nearly seven in ten who say the same about lowering prescription drug costs for as many Americans as possible (68%) as well as maintaining the Affordable Care Act’s protections for people with pre-existing medical conditions (68%). Implementing a national Medicare-for-all plan is not even a top priority among Democratic voters (36%).
The economy is another top issue for Pennsylvania voters but views of how the economy will fare over the next 12 months are largely driven by partisanship. Overall, voters in Pennsylvania are divided with similar shares saying they think that the U.S. will experience “good times” (47%) and “bad times” (51%) over the next 12 months. Eight in ten (78%) Democratic voters say the U.S. will have bad times financially over the next year while 80% of Republicans say the U.S. will have good times. Independents are evenly divided (49% v. 49%).
Two-thirds of Democratic voters say they are more motivated to vote in next year’s 2020 presidential election than they were in 2016 compared to slightly more than half of independent voters (54%) and Republican voters (54%). This is similar to the overall Blue Wall findings, which finds the Democratic Party has a slight enthusiasm edge over their Republican counterparts.
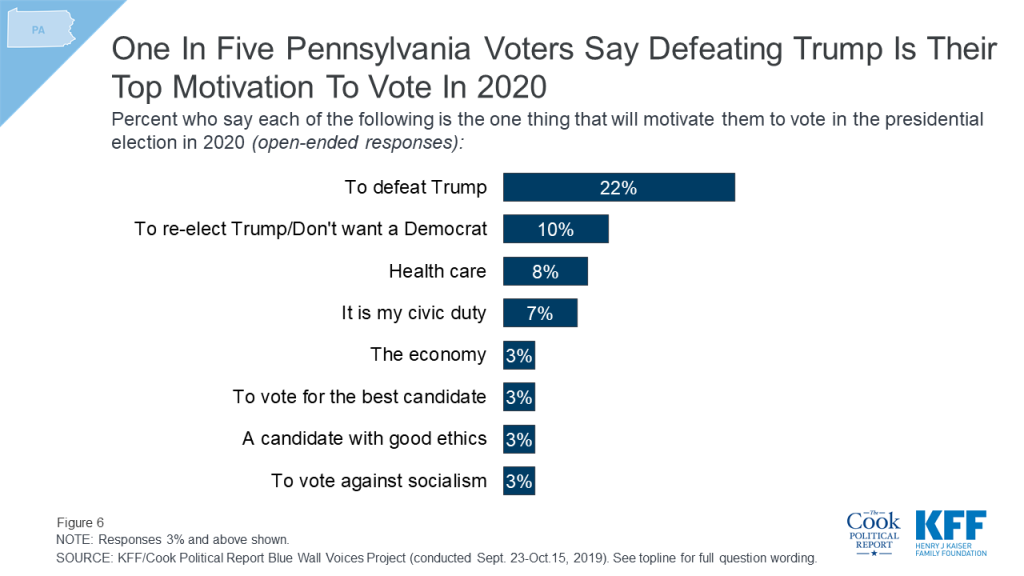
When asked to say in their own words what will be the one thing that will motivate them to vote in the 2020 presidential election, a larger share of voters offer responses related to defeating President Trump than any other thing. One-fifth of voters say defeating President Trump (22%) is the one thing that will motivate them to vote next year, followed by those who say they are motivated by re-electing President Trump or not wanting to elect a Democrat (10%), the issue of health care (8%), or their civic duty (7%).
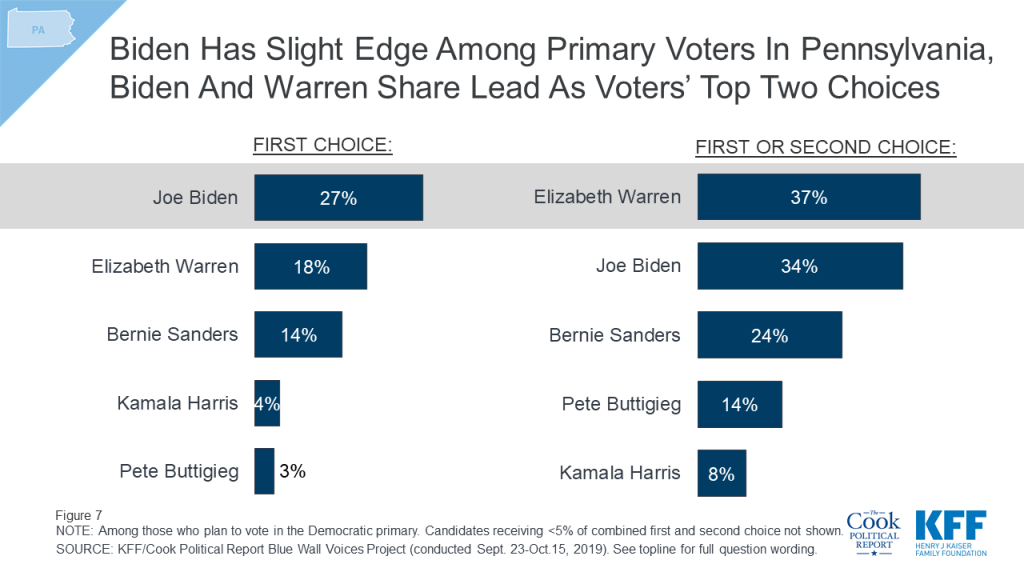
With more than six months before the Pennsylvania Democratic primary, Vice President Joe Biden, a Pennsylvania native, is the first choice among Democratic primary voters. One-fourth (27%) of Democratic primary voters chose Vice President Biden as their first choice of 2020 Democratic candidates followed by 18% of Democratic primary voters who chose Senator Elizabeth Warren and 14% who chose Senator Bernie Sanders. Senator Warren and Vice President Biden have a relatively similar share of first choice and second choice votes with more than one-third of voters selecting either candidate as their first or second choice.
Nearly four in ten (39%) Pennsylvania voters are still either undecided (22%) about their 2020 vote choice, or say they are “probably” voting for either President Trump (10%) or the Democratic nominee (7%) but have not made up their minds yet. This is compared to one-third of voters who say they are “definitely voting” for the Democratic nominee and one-fourth who are “definitely voting” for President Trump (23%).
With four in ten Pennsylvania votes still up for grabs, the poll finds that majorities of Pennsylvania swing voters (those who either say are still undecided or are either probable but not definite Trump or Democratic voters) say many of the progressive platforms currently being discussed in the Democratic primary are good ideas, but these voters are less positive in their views of three important policy positions, including Medicare-for-all. More than half of Pennsylvania swing voters say a pathway to citizenship for immigrants in the country illegally (72%), the Green New Deal (69%), a ban on future sales of assault weapons (67%), and a ban on owning assault weapons (57%) are good ideas. On the other hand, Pennsylvania swing voters are more negative in views of a national Medicare-for-all plan, fracking, and no longer detaining people for crossing the U.S. border illegally. Majorities of Pennsylvania swing voters say all three of these progressive platforms, a national Medicare-for-all plan (56%), a ban on fracking (57%), and stopping U.S. border detainments (72%), are “bad ideas.”

The Blue Wall Voices Project examines voters in Wisconsin, a state that President Trump won by less than one percentage point over Democratic candidate Hillary Clinton in 2016. This poll finds the economy and health care are among the top issues for voters more than one year out from the general election and examines enthusiasm and vote choice leading up to the 2020 presidential election.
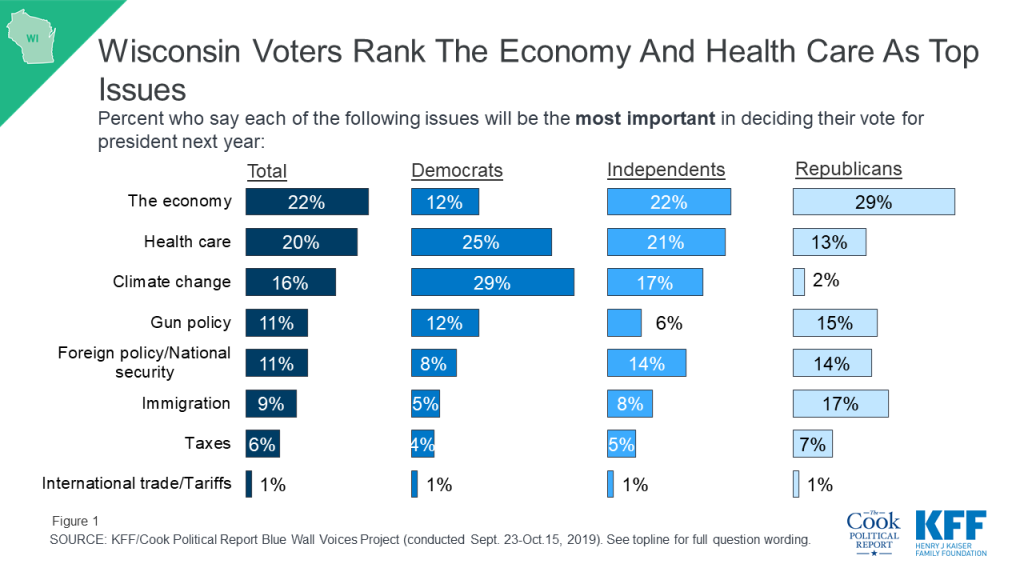
With approximately one year before the 2020 presidential election, the economy (22%) and health care (20%) emerge as the top issues for Wisconsin voters. Smaller shares name climate change (16%), gun policy (11%), foreign policy or national security (11%) and immigration (9%) as the issue which will be most important in deciding their vote. However, there are notable partisan differences on which issues are most important in deciding their vote. Among Democrats, climate change emerges as a top issue with nearly three in ten (29%) saying it will be the most important issue in deciding their vote, while among Republicans, only 2% say climate change is the most important issue. Nearly three in ten Republicans (29%) say the economy is the most important issue, compared to 22% of independents and 12% of Democrats. Larger shares of Democratic voters and independent voters say health care is the most important issue in deciding their vote (25% and 21%, respectively) than Republican voters (13%).
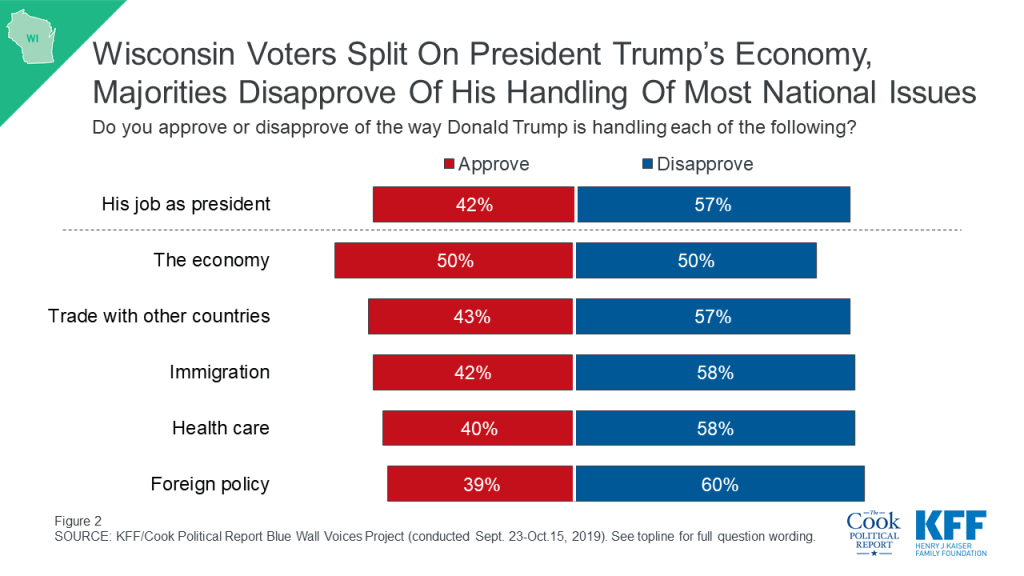
While Wisconsin voters are evenly divided in their views of how President Trump is handling the economy (50% v. 50%), a larger share of Wisconsin voters give President Trump negative marks on all other issues included in this poll including foreign policy (60%), health care (58%), immigration (58%), and international trade (57%).
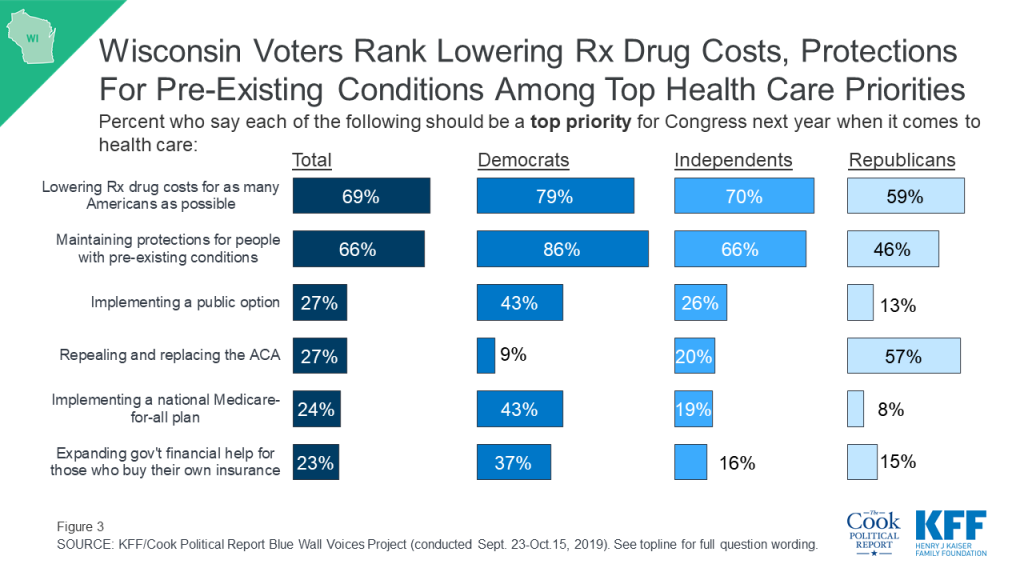
When asked about specific health care priorities for Congress to work on next year, nearly seven in ten Wisconsin voters say lowering prescription drug costs (69%) and maintaining protections for people with pre-existing conditions (66%) should be “a top priority.” Majorities of Democrats (79%), independents (70%), and Republicans (59%) say lowering prescription drug costs should be a top priority for Congress. A majority of Republicans (57%) say repealing and replacing the ACA should be a top priority while a smaller share (46%) say maintaining protections for people with pre-existing conditions should be a top priority for Congress. With discussions about Medicare-for-all dominating the health care conversation in the recent Democratic primary debates, equal shares of Wisconsin Democratic voters say implementing a national Medicare-for-all plan and implementing a public option should be a top priority for Congress next year (43% each), mirroring the policy divide on this issue among the leading Democratic candidates.
Wisconsin voters are divided in their economic outlook for the country in the next 12 months. About half (51%) think the U.S. will have “bad times” financially in the next year while 47% expect “good times.” There is a stark partisan divide with eight in ten Democrats expecting bad economic times in the next year, whereas three in four Republicans (77%) expect good times financially for the country. Similar shares of independent voters expect bad economic times (52%) and good times financially (46%).
About half of Wisconsin voters (51%) say they are more motivated to vote in 2020 than they were in the 2016 presidential election. Democrats seem to have the edge when it comes to motivation with more than six in ten Democrats (62%) saying they are “more motivated” to vote in 2020 than they were last election compared to less than half of Republicans (46%) who say they are more motivated.
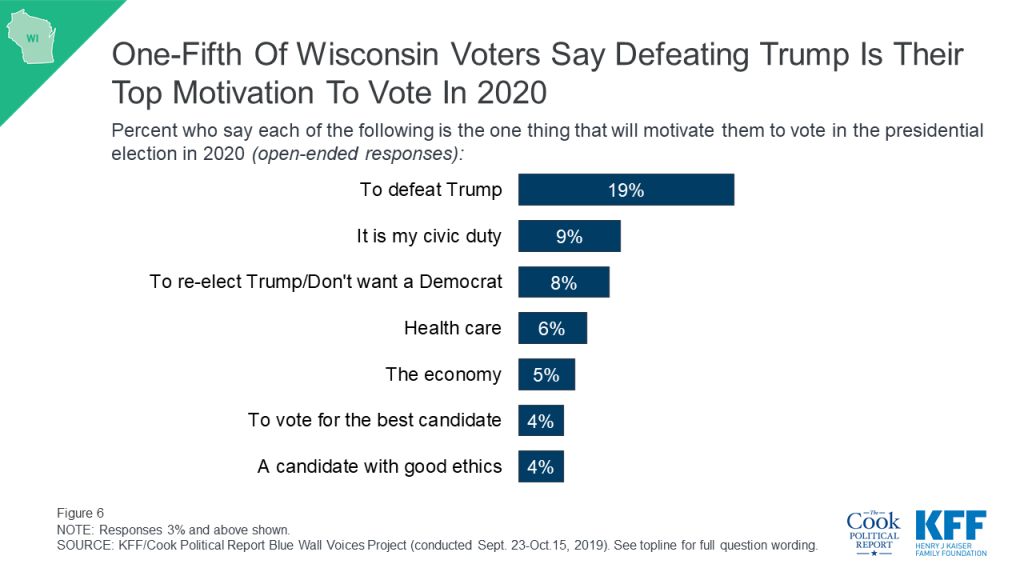
When asked specifically what one thing will motivate them to vote in the 2020 election, the most frequently volunteered response was defeating President Trump (19%). Smaller shares cited reasons such as a sense of civic duty (9%), re-electing President Trump or not wanting to elect a Democrat (8%), health care (6%), the economy (5%), and to vote for the best candidate (4%) or a candidate with good ethics (4%).
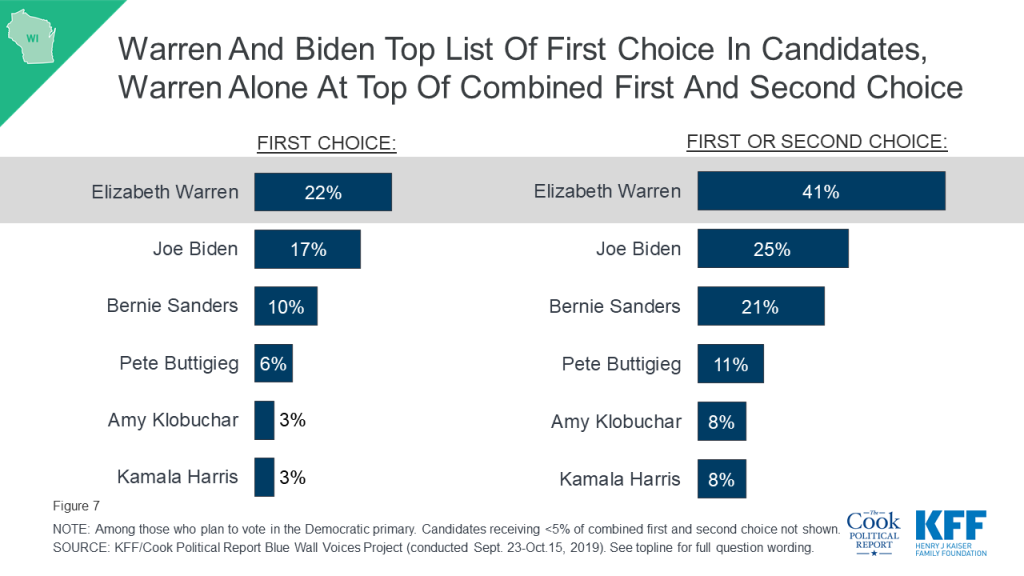
With about five months before Wisconsin’s 2020 primary election, about one in five Democratic voters say Senator Warren (22%) and Vice President Biden (17%) are who they plan to support during the Democratic primary. Vermont Senator Bernie Sanders, who won the Wisconsin primary in 2016 when he challenged former Senator Hillary Clinton for the nomination, is currently garnering 10%. Notably, about four in ten (41%) Wisconsin Democratic primary voters select Senator Warren as their first or second choice compared to one in four Democratic primary voters who select Vice President Joe Biden as their first or second choice while one in five (21%) say Senator Sanders is their first or second choice.
About four in ten (43%) Wisconsin voters are either undecided (21%) about their 2020 vote choice or say they are “probably” voting for either President Trump (11%) or the Democratic nominee (10%) but have not made up their minds yet. About three in ten voters say they are “definitely voting” for the Democratic nominee (31%) and about one in five say they are “definitely voting” for President Trump (22%).
Majorities of Wisconsin swing voters (those who are either undecided or say they are probably going to vote for either president Trump or the Democratic nominee) say many of the progressive platforms are “good ideas” including a pathway to citizenship for immigrants in the U.S. illegally (75%), a Green New Deal (65%), and a ban on future sales of assault weapons (65%). But most Wisconsin swing voters say a ban on fracking (55%), a national Medicare-for-all plan (63%), and stopping detainments at the U.S. border (66%) are bad ideas.
The Blue Wall Voices Project was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF) in collaboration with the Cook Political Report. The survey was conducted September 23rd – October 15th, 2019, among a representative random sample of 3,222 registered voters in four states (767 in Michigan, 958 in Minnesota, 752 in Pennsylvania, and 745 in Wisconsin) constituting the “Democratic Blue Wall” – the area in the Upper Midwest that were previously considered Democratic strongholds, and where state polls performed poorly in 2016 and underestimated support for President Trump. All registered voters included in the sample were sent an invitation letter including a link to complete the survey online, a toll-free number that respondents could call to complete the survey with a telephone interviewer, and $2 pre-incentive. Respondents who were living in Census block-groups identified as low-education and respondents identified as likely Hispanic were offered $10 post-incentive if they completed the survey. A random half of respondents received a QR code on their invitation letters. All respondents were then sent a reminder postcard, which included a QR code for all respondents. Respondents who were flagged in the voter file as both a) speaking Spanish and b) speaking either primarily or only their native language, received bilingual mailings, including text in both English and Spanish.
The sample was designed to reach respondents less likely to complete surveys online, by oversampling areas with a relatively low percentage of college graduates. Sample that could be matched to telephone numbers and that had not yet completed the survey online or by inbound computer-assisted telephone interview (CATI) were called by CATI interviewers to attempt to convert this sample to completed interviews. A total of 2,763 respondents completed the questionnaire online, 255 by calling in to complete, and 204 were completed as outbound CATI interviews. Data collection was carried out in English and Spanish by SSRS of Glen Mills, PA. The registered voter sample was provided by Aristotle. KFF paid for all costs associated with the survey.
A series of data quality checks were run on the final data, which resulted in 40 completes being removed from the data. Weighting involved multiple stages: First, each state sample was weighted to account for the sampling methodology including the oversampling of low-educational attainment areas and to the proportions of the voter file reachable or unreachable by outbound phone-call. Second, each state’s sample was weighted to match the voter file distribution of 2016 voter status, party identification, gender, race/ethnicity, home-ownership, Metropolitan status, state region, as well as the 2018 CPS Voter Supplement for age-by-gender, educational attainment and race. To address non-response among partisans not accounted for by demographics, the weight was adjusted so that the self-reported 2016 vote in each state matched the actual state outcome. The final weight combined each state’s weight and balanced the combined total sample to state distributions. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 2 percentage points. Numbers of respondents and margins of sampling error for each state are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Progressive Stances on Fracking, Medicare-for-all and Border Detainments May Turn Off Swing Voters
A year ahead of the 2020 presidential election, President Trump is the biggest defining factor for voters in Michigan, Minnesota, Pennsylvania, and Wisconsin – more often in a negative than a positive direction, finds a new partnership survey from KFF and The Cook Political Report of more than 3,000 voters across the four previously considered “Blue Wall” states, including at least 745 in each state.
More than twice as many voters in these states mention defeating President Trump (21%) as the one thing that will motivate them to vote in 2020 than offer responses related to re-electing him (8%).
Voters across the “Blue Wall” states – the area in the Upper Midwest that were previously considered Democratic strongholds and where 2016 state polls underestimated President Trump’s support – are more likely to mention President Trump as their main motivation than any issue including health care (8%) and the economy (4%), which top voters’ list of key national issues for the 2020 campaign. Overall, one-fourth (23%) of voters name any issue as their main motivation for voting in 2020.
As the 2020 race heats up, health care and the economy are the top issues for voters but these issues may pull voters, especially independents, in opposite directions. President Trump garners a higher approval rating on the economy (49% approve, 50% disapprove) than on any other issue, while he garners his lowest marks on health care (39% approve, 60% disapprove). And while half of independent voters approve of the way President Trump is handling the economy, most (61%) disapprove of the way he is handling health care.
Most voters (59%) in the four states also disapprove of his job performance overall, compared to 41% who approve. Yet, the poll isn’t all bad news for President Trump, as he retains solid support among his base across the Blue Wall states. Large majorities of Republican voters approve of his job performance overall (87%) and on every specific issue tested, including the economy (94%) and health care (84%).
At this stage, nearly two thirds (64%) of Democratic voters across the four states say they are more motivated to vote in 2020 than they were in 2016, compared over half of independents (55%) and Republicans (53%). On a state-by-state basis, Democrats have a clear enthusiasm advantage over Republicans in Michigan, Pennsylvania and Wisconsin, while in Minnesota voters in both parties are about equally enthusiastic.
Republicans’ loyalty to President Trump runs high. Most Republican and Republican-leaning voters (73%) say they want President Trump to be the Republican nominee in 2020, but small shares (28%) of his supporters can imagine a scenario in which he enacts a policy, or fails to enact a policy, that would result in them changing their vote.
A Year Out, President Trump Trails the Democratic Nominee, But 4 in 10 Say Their Mind Isn’t Made Up
Nearly one-fourth of voters in each of the states say they are “definitely” going to vote for President Trump in 2020, and an additional one in ten saying they are “probably” going to vote for him. However, more voters overall say they definitely or probably will vote for the Democratic nominee (40%) than say they definitely or probably will vote for President Trump (33%).
While many voters across the Blue Wall states say they have made up their mind about who they will vote for in the 2020 general election, about four in 10 say they either are undecided (23%) or are probably going to vote for either President Trump or the Democratic nominee but haven’t completely made up their minds yet. This crucial group of “swing voters” make up both those voters who may choose to stay home next year and a small share of voters who may still be persuadable to vote for the other party’s candidate (5%).
While Democrats Support Progressive Platforms, Some May Turn Off Crucial Swing Voters
Voters who say they are going to vote for the Democratic nominee in 2020 overwhelmingly think the progressive policy positions included in this survey are good ideas, including the Green New Deal (92%), a pathway to citizenship for immigrants in the country illegally (91%), a ban of future assault weapon sales (88%) and a ban and mandatory buyback of assault weapons (83%). Fewer, but still a majority, also say a ban on fracking (54%), stopping U.S. border detainments (56%), and a national Medicare-for-all plan (62%) – a hot-button issue in the Democratic primary race – are good ideas.
While few self-reported 2020 Democratic voters say they wouldn’t vote for a candidate who disagreed with them on any of these issue in the general election, there is some evidence that some of these progressive stances are not popular among swing voters.
Majorities of swing voters across the four states view three as bad ideas: not detaining border crossers (71%), Medicare-for-all (62%) and a fracking ban (54%). In Pennsylvania, 57% of swing voters say a fracking ban is a bad idea.
The Blue Wall poll also explores voters’ views on other issues, including tariffs and trade. Most voters across the four states say recent tariffs imposed on goods from China and other countries are hurting the national economy (55%) and workers in their state (55%). In addition, voters are about three times more likely to say the tariffs are hurting their families (46%) than are helping their families (14%). These shares are similar in each of the four states.
Voter Preferences in the Democratic Primaries
The four state polls also test Democratic voters’ primary preferences and finds former Vice President Joe Biden and Sen. Elizabeth Warren are voters’ top choices. Specifically:
METHODOLOGY
Designed and analyzed by public opinion researchers at KFF in collaboration with Cook Political Report, the poll was conducted September 23rd – October 15th, 2019, among a representative random sample of 3,222 registered voters in four states (767 in Michigan, 958 in Minnesota, 752 in Pennsylvania, and 745 in Wisconsin) constituting the Democratic “Blue Wall.” The poll relies on an innovative probability-based methodology designed to address shortcomings with telephone-only surveys based on either voter-registration rolls or random-digit dialing. Voters were contacted via mailing address using registration-based sampling and encouraged to participate in the survey either online or by telephone and follow-up contacts were made using outbound telephone calls. Interviews were conducted in English and Spanish either online (2763), by calling in to complete (255), or throughout outbound telephone interviews (204). The margin of sampling error is plus or minus 2 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
Since Medicaid’s inception, federal law has generally prohibited states from using Medicaid funds for services provided to nonelderly adults in “institutions for mental disease” (IMDs).1 The IMD payment exclusion was intended to leave states with the primary responsibility for financing inpatient behavioral health services.2 However, the lack of federal funding may limit access to needed inpatient services and contribute to high levels of unmet need. In recent years, the federal government has provided new mechanisms for states to finance IMD services for nonelderly adults through Medicaid in certain situations. There are now four options for states to cover these services: Section 1115 demonstration waivers, managed care “in lieu of” authority, disproportionate share hospital payments, and the SUPPORT Act state plan option.
This report provides new data to understand current patterns of Medicaid enrollees’ use of inpatient and outpatient substance use disorder (SUD) and mental health treatment services; explains the options for states to access federal Medicaid funds for enrollees receiving IMD services; analyzes current waiver activity; and draws on interviews with policymakers in two states and one county using IMD waivers to examine successes and challenges. Appendix Tables contain state-level data. Key findings include:
As states continue to seek Medicaid IMD payments, key issues to watch include capacity and utilization of treatment services across the care continuum, IMD day limits, discharge planning and care transitions, and the continued evolution of evidence-based best practices for SUD and mental health treatment.
Medicaid covers many behavioral health services, though there is not a specifically defined category of Medicaid benefits dedicated to behavioral health. Some behavioral health services fall under mandatory Medicaid benefit categories that all states must cover. For example, psychiatrist services are covered under the required “physician services” category. States also cover behavioral health services through optional benefit categories that states may choose to include in their Medicaid programs, such as case management or prescription drugs (which all states do). One important benefit category for behavioral health is the rehabilitative services option, through which states commonly cover non-clinical behavioral health services such as peer support and community residential services. In addition, under waiver or state plan authority, states can provide home and community-based long-term care behavioral health services that support independent community living, such as day treatment and psychosocial rehabilitation services. While all states that participate in Medicaid must cover inpatient services, federal law prohibits payment for services provided in IMDs, as further described below. Box 1 provides examples of behavioral health services that may be covered by Medicaid. A glossary defining key Medicaid behavioral terms is included in the Appendix.
Medicaid coverage of behavioral health services is sometimes more comprehensive than private insurance coverage. While many private insurance plans cover psychiatric hospital visits, in some states, Medicaid is more likely to cover additional services, such as case management, individual and group therapy, detoxification, and medication management. Medicaid is the primary payer for long-term services and supports on which many people with disabilities, including those with mental health needs, rely to live independently in the community.
Box 1: Examples of Medicaid Behavioral Health Services
Most nonelderly Medicaid adults receiving behavioral health treatment do so in an outpatient setting, without any inpatient services. In 2017, inpatient services were used by just under half (46%) of nonelderly Medicaid adults with SUD who received drug or alcohol treatment in the past year (Figure 1). A smaller share (17%) of Medicaid enrollees with mental illness who received treatment used inpatient services. The data do not distinguish services provided in IMDs from those provided in other inpatient settings such as a general inpatient hospital.
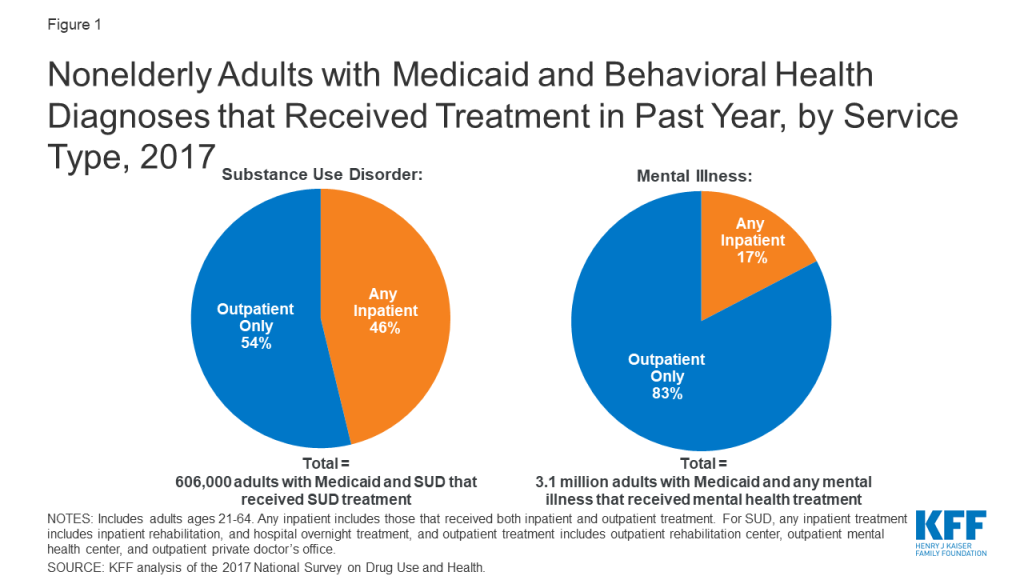
Though nonelderly Medicaid adults with behavioral health needs are significantly more likely than those who are privately insured to have used inpatient and outpatient treatment services in the past year, treatment rates are low across all payers. Among nonelderly adults with SUD, those with Medicaid are more likely have used inpatient treatment services compared to those with private insurance (8% vs. 3%, Figure 2). Similarly, among nonelderly adults with any mental illness, those with Medicaid are more likely to have used inpatient treatment, compared to those with private insurance (6% vs. 2%). Nevertheless, treatment utilization rates (use of treatment services in past year by those with a behavioral health diagnosis), particularly for inpatient treatment, remain low across payers. Inpatient treatment rates are low even for private insurers who, unlike Medicaid, are not subject to the IMD payment exclusion.
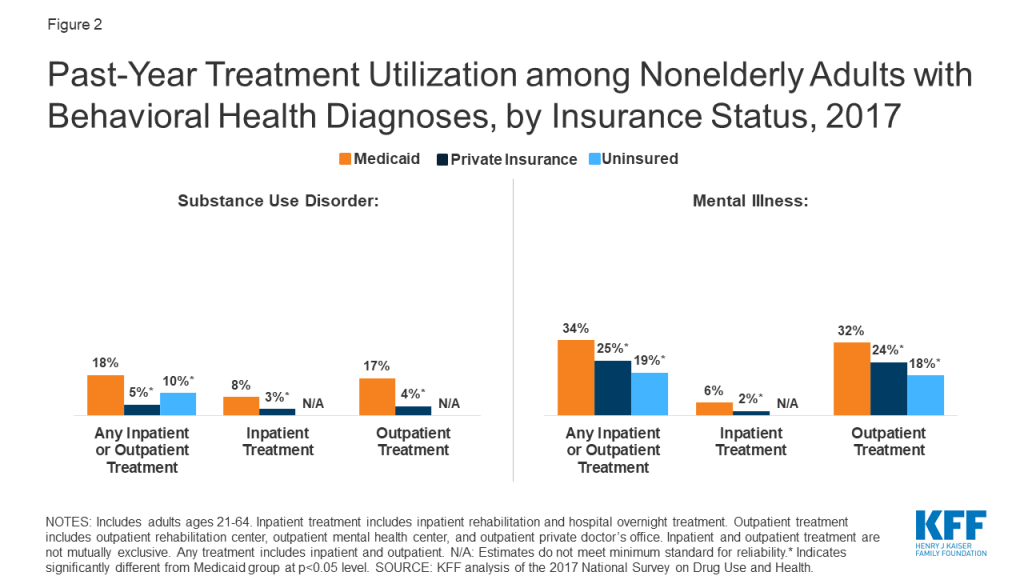
Many people with behavioral health diagnoses report unmet treatment needs. Substantial shares of nonelderly adults with SUD and any mental illness report an unmet need for drug or alcohol treatment, with those with private insurance significantly more likely to have an unmet SUD treatment need compared to those with Medicaid (91% vs. 80%, Figure 3). The share of nonelderly Medicaid adults with SUD and any mental illness reporting an unmet need for mental health treatment is similar to those with private insurance (36% vs. 34%).
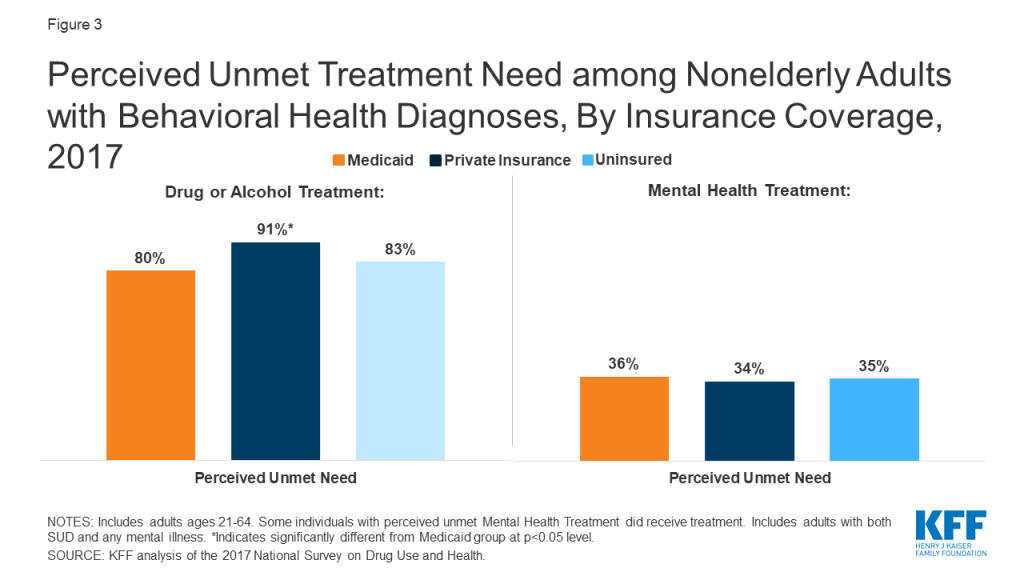
Administrative data shows wide state variation in use of inpatient services among nonelderly Medicaid adults who receive mental health or substance use disorder services. In FY 2013, the share of nonelderly Medicaid adults receiving any behavioral health treatment who received any inpatient SUD services ranged from 10% in Alaska to 57% in West Virginia. The share of those receiving any inpatient mental health services ranged from 9% in Alaska to 31% in Alabama and New York (Appendix Table 1). Like the national data discussed above, the state-level data do not separately identify IMD services from other inpatient services. In addition, this data – which is the most recently publicly available – predates the Affordable Care Act’s Medicaid expansion and the opioid epidemic’s impact over the last six years, and consequently may understate the number of enrollees now utilizing these services in states that have implemented the expansion since 2014.3
Federal law generally bars states from receiving “any [Medicaid] payments with respect to care or services for any individual who has not attained 65 years of age and who is a patient in an [IMD].”4 The payment exclusion applies to services provided within an IMD as well as to services provided outside an IMD to nonelderly adult IMD patients. An IMD is a “hospital, nursing facility, or other institution of more than 16 beds, that is primarily engaged in providing diagnosis, treatment, or care of persons with mental diseases [sic], including medical attention, nursing care, and related services” (Figure 4).5 Whether a particular facility is an IMD is determined by the state. Figure 4 lists factors considered in this determination. While all states that choose to participate in the Medicaid program must cover inpatient hospital services, those services specifically exclude care provided in IMDs.6 The IMD payment exclusion applies to Medicaid enrollees ages 21 through 64. States have the option to cover inpatient psychiatric hospital services for those under age 217 and IMD inpatient hospital and nursing facility services for those age 65 and older.8
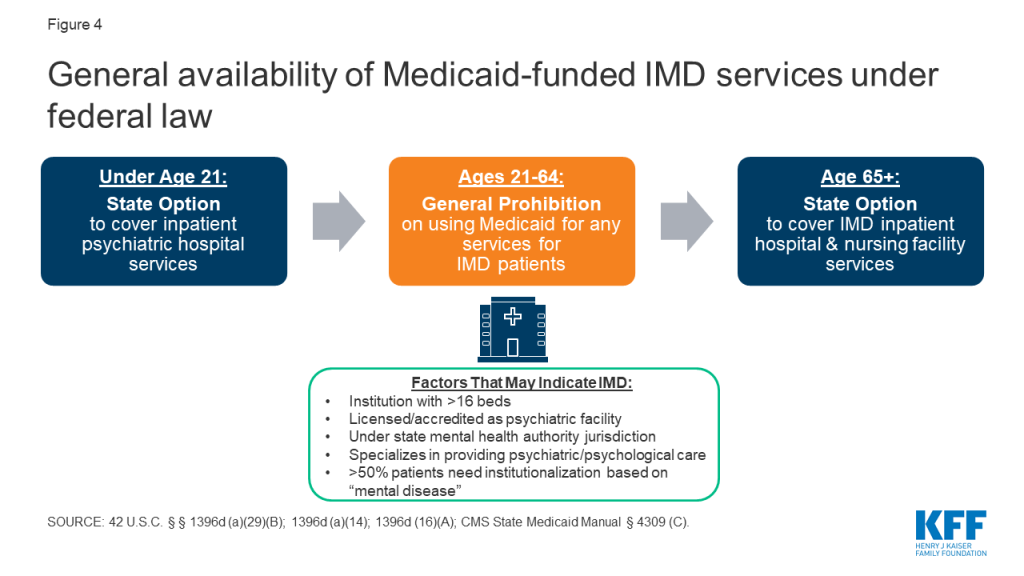
There are four ways that states can receive federal Medicaid funds for IMD services for nonelderly adults. These include Section 1115 demonstration waivers, Medicaid managed care “in lieu of” authority, disproportionate share hospital (DSH) payments, and the SUPPORT Act9 state plan option (beginning in October 2019) (Figure 5). Box 2 discusses considerations for providing institutional services under the Americans with Disabilities Act, separate from Medicaid.
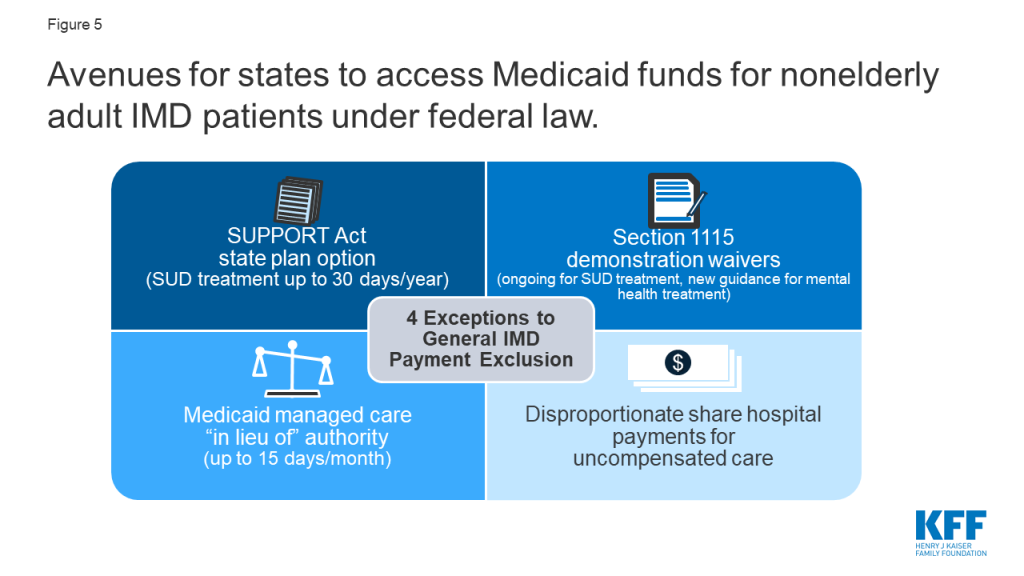
Box 2: Institutional Services and Community Integration
Waiving the IMD payment exclusion and expanding institutional services without also ensuring adequate access to community-based services could have implications for states’ community integration obligations under the Americans with Disabilities Act (ADA) if people with disabilities are inappropriately institutionalized.10 The Supreme Court’s Olmstead decision found that the unjustified institutionalization of people with disabilities violates the ADA. The ADA’s community integration mandate is separate from federal Medicaid law. However, states rely on Medicaid funding to help meet their ADA obligations, because Medicaid is the primary payer for long-term services and supports, including home and community-based services.11 Medicaid also is an important source of financing for behavioral health services, paying for 21% of SUD services and 25% of mental health services as of 2014.12 Consequently, even when providing IMD services to the extent permitted under federal Medicaid law or a waiver, states still separately must meet their independent community integration obligations under the ADA.
With the opioid epidemic increasing, CMS has been inviting states to apply for Section 1115 IMD SUD waivers,13 with guidance released in 2015,14 and revised in 2017.15 These waivers allow states to test using federal Medicaid funds to provide short-term inpatient and residential SUD treatment services in IMDs. Some of the requirements for these waivers have evolved over time (Figure 6). For example, unlike waivers approved under the 2015 guidance,16 waivers approved under the 2017 guidance do not explicitly limit the length of individual IMD stay.17 In addition, waivers under the 2015 guidance were contingent on states covering community-based SUD treatment services at the time of approval,18 while the 2017 guidance allows states up to two years after waiver approval to cover “critical levels of care.”19 As discussed in more detail below, more than half of states have an approved or pending IMD SUD payment waiver as of November 2019.
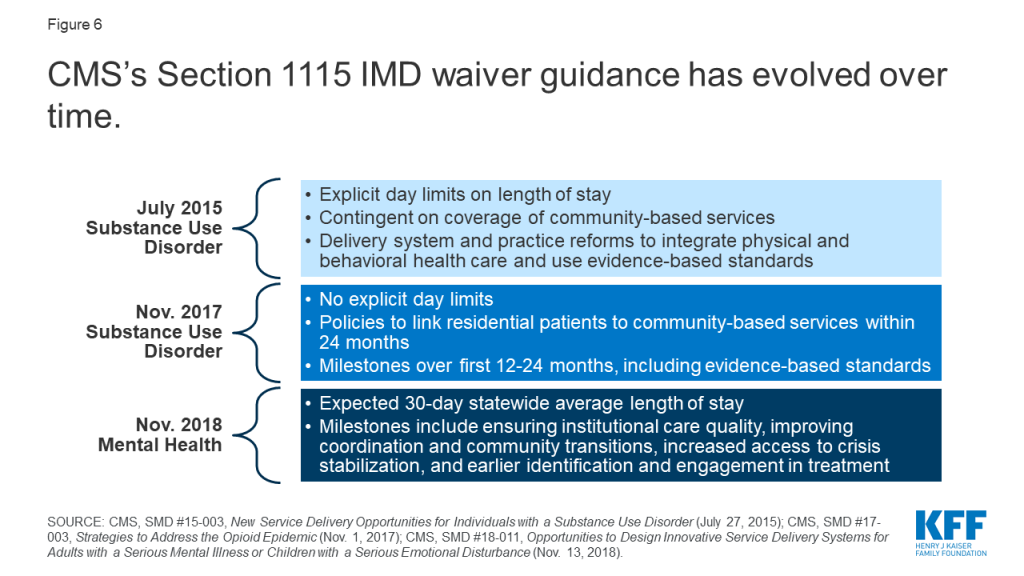
In addition to covering certain levels of care, the 2017 guidance incorporates other milestones that states must achieve during the term of an IMD SUD waiver (Figure 7).20 These include using evidence-based patient placement criteria; applying nationally recognized provider qualification standards; implementing prescribing guidelines and other strategies to address opioid abuse; and improving care coordination and transitions between levels of care.21 CMS’s 2019 IMD SUD waiver evaluation design guidance identifies SUD treatment access and utilization,22 health outcomes,23 and opioid-related overdose deaths as three key areas to assess.24
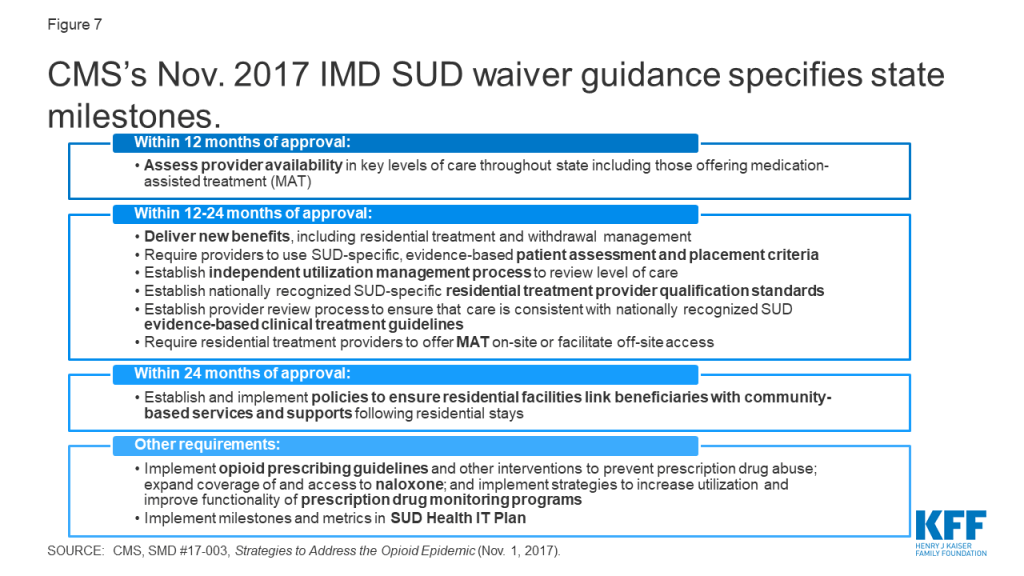
CMS also reversed long-standing policy and issued new guidance inviting states to apply for Section 1115 IMD payment waivers for mental health services in November 2018 (Figure 6).25 Until this point, CMS had not approved IMD mental health waiver requests in Illinois,26 Massachusetts,27 or North Carolina,28 citing its former policy not to allow Medicaid payments for individuals who receive only mental health treatment in IMDs.29 Under the new guidance, states will have to achieve a set of milestones over the term of these waivers, including ensuring institutional care quality, improving coordination and community transitions, increasing access to crisis stabilization, and earlier identification and engagement in treatment. States that previously had IMD mental health waiver requests that were not approved, as well as states with new requests, can apply for waivers under the 2018 guidance. As of November 2019, only one state (Vermont) has an approved Section 1115 IMD mental health waiver.
States with capitated managed care delivery systems can use “in lieu of” authority to cover IMD SUD and mental health services for up to 15 days per month.30 Specifically, states can use federal Medicaid funds for capitation payments to managed care plans that cover IMD inpatient or crisis residential services for nonelderly adults instead of providing other services, such as non-IMD inpatient or outpatient services, that are covered in the state plan benefit package.31 The IMD services must be medically appropriate and cost-effective, and enrollees cannot be required to accept IMD services instead of state plan services. This regulation took effect in July 2016,32 although it codified pre-existing long-standing federal sub-regulatory guidance that allowed federal Medicaid payments for IMD services. However, unlike the regulation, the former guidance did not subject IMD services covered under “in lieu of” authority to a day limit. Of the 41 states using comprehensive risk-based managed care organizations, 31 use Medicaid managed care “in lieu of” authority to cover IMD SUD and/or mental health services in both FY 2019 and FY 2020, and two (MS and NC) report plans to begin doing so in FY 2020.33 Two states reported using the authority in FY 2019 only (Appendix Table 3).34
States can spend a portion of their Medicaid DSH funds on IMD services.35 States must make these payments to offset uncompensated care costs incurred by hospitals that serve a disproportionate number of low-income patients. In FY 2018, 33 states made DSH payments totaling $2.9 billion to mental health treatment facilities including IMDs. These payments ranged from 0.0003% of total DSH payments to mental health facilities in Minnesota to 18% in New York (Appendix Table 4).
The SUPPORT Act partially lifts the IMD payment exclusion by allowing states to use federal Medicaid funds for nonelderly adults receiving IMD SUD services up to 30 days a year,36 from October 2019 through September 2023.37 IMD coverage under the SUPPORT Act option is in addition to IMD services covered under managed care in lieu of authority38 and Section 1115 waivers.39 To receive Medicaid payments under the SUPPORT Act option, IMDs must follow “reliable, evidence-based practices” and offer at least two forms of medication-assisted treatment (MAT) on-site40 for opioid use disorder. Separately, the SUPPORT Act also authorizes Medicaid payments for services provided outside IMDs for pregnant and post-partum women receiving IMD SUD services, as of October 2018.41
States must satisfy five criteria to qualify for Medicaid funds under the SUPPORT Act option (Figure 8). First, states have to maintain annual state and local funding levels42 for both IMD services and a specific list of community-based outpatient services43 provided to nonelderly adults who become eligible for Medicaid-funded IMD services under the new option. Additionally, states must ensure that nonelderly adults receive “appropriate evidence-based clinical screening” prior to receiving IMD SUD services.44 States also must confirm that IMDs receiving Medicaid payments can provide outpatient services, either themselves or through an established relationship with another facility or provider accepting Medicaid patients, to allow for successful community transitions.45 Finally, states electing the SUPPORT Act option must cover Medicaid SUD treatment services at four outpatient levels of care46 and at least two of five inpatient levels of care47 (Figure 9).
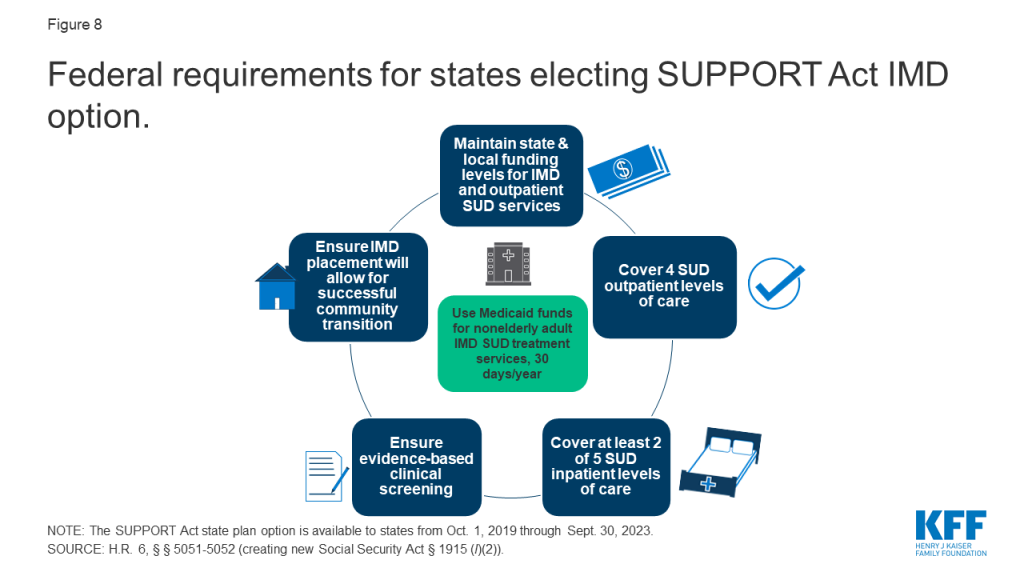
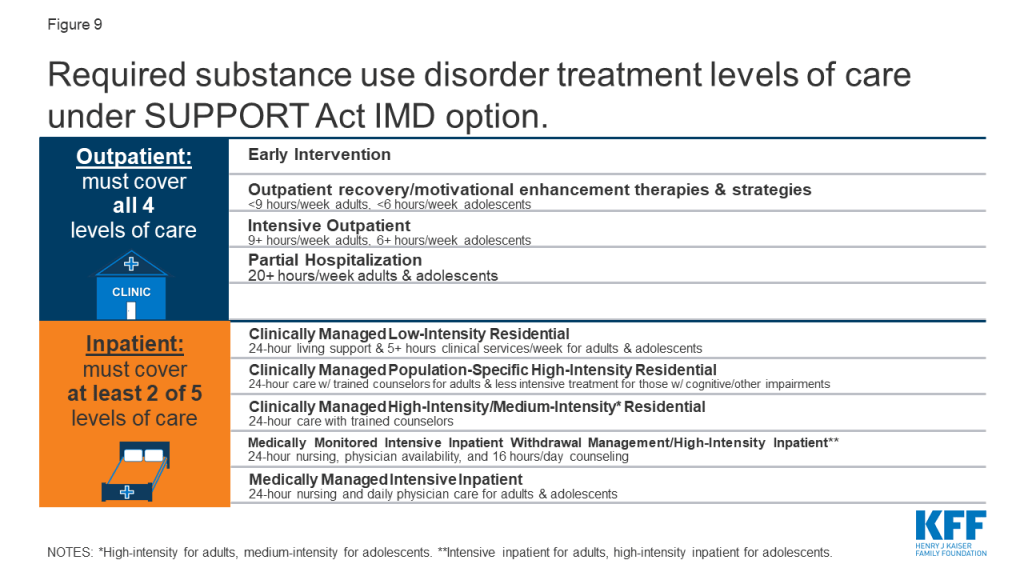
According to a KFF survey, five states report plans to pursue the SUPPORT Act option in FY 2020.48 These states include Idaho, Indiana, New Hampshire, South Dakota, and Tennessee.49 Twenty-one states report that they have not yet determined if they will pursue the SUPPORT Act option,50 and 24 states indicate that they do not plan to pursue this option.51 In explaining the rationale for not pursuing this option, many states noted that they already had a Section 1115 waiver in place or were pursuing such a waiver to allow IMD funding.52 Several states also felt that their Section 1115 waiver would provide more flexible limits on length of IMD stays compared to the 30-day cap on IMD services under the SUPPORT Act option.53 Table 1 compares key elements of Section 1115 IMD waivers with the SUPPORT Act.
| Table 1: Key Elements of Section 1115 Waivers vs. SUPPORT Act Option for IMD Payment | ||
| Program Element | Section 1115 Waiver | SUPPORT Act |
| Type of authority | Waiver | State plan option |
| Length of authority | Initial waivers usually granted for 5 years. States can apply for renewals, usually for 3 years. | Available from October 2019 through September 2023. |
| Type of IMD services allowed | SUD and/or mental health | SUD only |
| Length of stay | Varies by waiver: some numeric day limits, some unspecified, some require 30-day statewide average. | 30 days per year |
| Covered inpatient levels of care | Must cover intensive residential/inpatient and medically supervised withdrawal management within 24 months of waiver approval. | Must cover at least 2 of 5 inpatient levels of care. |
| Covered outpatient levels of care | Must cover outpatient and intensive outpatient services within 24 months of waiver approval. | Must cover all 4 outpatient levels of care. |
| Institutional to community transitions | Must develop policies to link residential patients to community-based services. | Must ensure that IMD placement will allow for successful community transition. |
| Evidence-based practices | Must use evidence-based patient assessment and placement criteria and provide access to MAT. | Must follow evidence-based practices, including clinical screening and MAT. |
| Maintenance of effort | For SUD waivers, CMS encourages states to maintain current funding levels for a continuum of services; waivers should not reduce or divert state spending on behavioral health services. For mental health waivers, CMS will consider a state’s commitment to on-going maintenance of effort on funding outpatient community-based services when approving waivers. | Must maintain state and local funding levels for IMD and outpatient services. |
The number of Section 1115 IMD SUD waiver approvals has markedly increased since January 2017. Four states had IMD SUD waivers approved by CMS as of December 31, 2016, and another 22 states have had IMD SUD payment waivers approved since then. Three more states have these waiver requests pending with CMS as of November 2019 (Figure 10 and Appendix Table 2).54 To date, Vermont remains the only state with an existing IMD mental health waiver, the current terms of which require those payments to phase out between 2021 and 2025.55 Vermont recently submitted a request to transition its existing mental health authority to the terms of the new guidance. Additionally, DC and Indiana have submitted pending waiver requests for IMD mental health services under the new guidance, with more states expected to follow. Idaho, Massachusetts, New Hampshire, New Jersey, North Carolina, and Rhode Island report plans to pursue an IMD mental health waiver in FY 2020, while Alaska, Connecticut, Virginia, and Washington report plans to do so after FY 2020.56
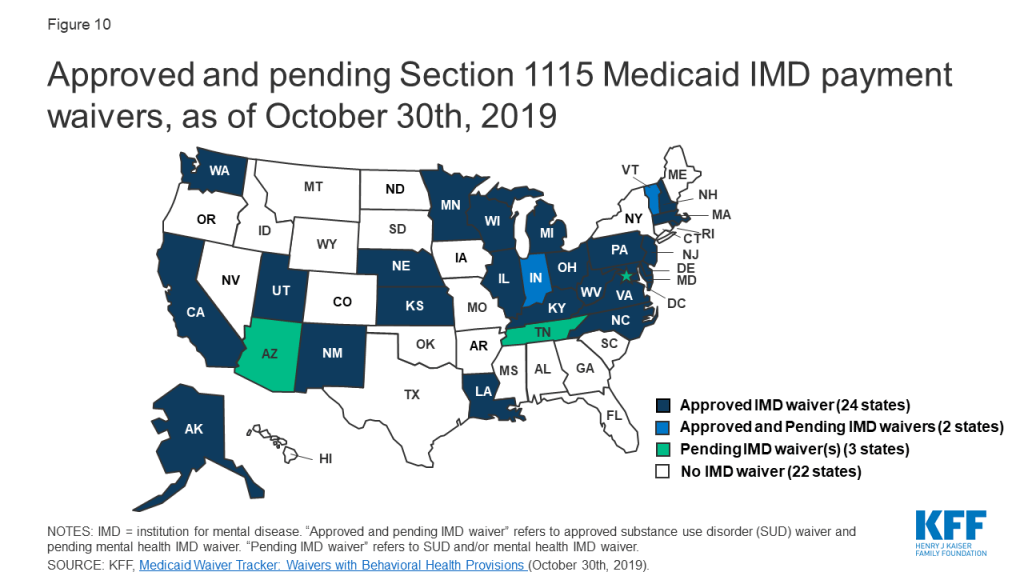
While waiver evaluations are still underway, news reports, interim evaluations, and feedback directly from states can inform the ongoing implementation of IMD waivers. While some waiver evaluation results are emerging, most are not expected until 2024 or 2025 (Appendix Table 2).57 Given the attention to state efforts to combat the opioid epidemic and emerging focus on mental health, states are moving forward with waiver implementation. State experience with these initiatives can help inform policy choices and design as other states consider similar waivers. To make some of this information available in advance of formal waiver evaluations, we conducted case studies in two states and one county. Table 2 summarizes the waivers in the three case study areas, and Box 3 describes the case study methodology.
| Table 2: Key Components of Approved 1115 Waivers for California, Virginia, and Vermont | |||
| State | California | Virginia | Vermont |
| Waiver/Program Name | Drug Medi-Cal Organized Delivery System (DMC-ODS) | The Virginia GAP and ARTS Delivery System Transformation | Vermont Global Commitment to Health |
| Approval Date | 8/13/2015 | 12/15/2016 | 1/1/199658 |
| IMD Authority Begins | 1/1/2016 (San Diego County implanted 7/2018) | 4/01/2017 | 1/1/199659 |
| IMD Authority Expires | 12/31/2020 | 12/31/2019 (Submitted amendment to extend) | 12/31/2021 for SUD; mental health to phase-out by 2025 (pending mental health waiver submitted to CMS) |
| SUD Authority | ✓ | ✓ | ✓ |
| Mental Health Authority | ✓ | ||
| Day Limit | 30-day statewide average; 90 day max. | 30-day statewide average | 30-day statewide average |
| SOURCE: KFF analysis of Section 1115 waivers for the IMD Payment Exclusion | |||
Box 3: Overview of Case Study Areas
Because waiver evaluations are ongoing and there is limited information about states’ experiences and outcomes with IMD waivers to date, we conducted case studies in Vermont; San Diego County, California; and Virginia, to provide a snapshot of how these three areas are using IMD waivers and identify common themes and lessons learned. In July 2019, we interviewed state and county officials by phone. We also reviewed publicly available waiver approval, reporting, and evaluation documents. Because San Diego County’s program is part of the California waiver, we also include relevant findings from the overall California waiver evaluation and other California waiver documents as relevant. In addition to considering geographic and political diversity, we chose case study regions to enable us to examine state experiences based on the type of IMD waiver authority (SUD and/or mental health), whether the waiver was approved under the 2015 or 2017 CMS guidance, and duration of implementation (Table 2).
Vermont has long-standing experience with using federal Medicaid funds for both IMD SUD and mental health services, through a Section 1115 waiver dating back to 1996. Vermont’s SUD authority is currently authorized under CMS’s 2017 guidance. Although the current waiver requires Vermont to phase-out IMD mental health funding between 2021 and 2025,60 the state has applied for IMD mental health waiver authority under the 2018 guidance. San Diego County began offering IMD SUD services in July 2018, and is one of the 40 counties participating in California’s Section 1115 waiver Drug Medi-Cal Organized Delivery System pilot program, which was approved under the 2015 guidance.61 Virginia added the Addiction and Recovery Treatment Services (ARTS) Delivery System Transformation Demonstration program, which includes IMD SUD services, to its Section 1115 waiver effective April 2017. Virginia’s waiver initially was approved under the 2015 CMS guidance, although the state subsequently came into compliance with the 2017 guidance.62
Interviews with case study areas implementing IMD waivers reveal that some expanded community-based treatment services in addition to IMD services. Notably, Virginia used state funds that previously went to IMD services to finance additional community-based SUD services to complement the IMD SUD services authorized by its waiver. Specifically, Virginia used state plan authority to add recovery supports and expanded medication-assisted treatment to the intensive outpatient, partial hospitalization, and residential levels of care. In addition to IMD residential services, California’s waiver adds enhanced SUD community-based services in the participating counties, including case management, withdrawal management, recovery services, physician consultation, and at county option, additional MAT drugs and partial hospitalization. Without the waiver, the California Medicaid state plan benefit package is limited to outpatient, intensive outpatient, perinatal residential (non-IMD), and opioid treatment program services. Other states not included as case studies for this report similarly expanded community-based services either under or in conjunction with their waivers authorizing payment for IMD services, such as West Virginia,63 Kansas,64 Illinois,65 Alaska,66 Indiana,67 and Wisconsin.68 However, at least one state (Kentucky) has restricted access to some community-based services (methadone) while funding IMD services under its waiver.69
While states believe that newly added community-based services are essential to achieving their waiver goals, utilization of some of the new services during initial implementation has not been as high as expected. Respondents noted that use of recovery supports (Virginia and California)70 and case management (California)71 has been low. As waiver implementation continues, these states are focused on additional provider training to increase new service utilization and improve treatment continuity as enrollees transition among care settings.
States are making efforts to address transitions between inpatient and outpatient care settings. California’s managed care external quality review report recommends that SUD providers at both residential and outpatient levels of care be allowed to bill for services provided to an individual on the same day to align with evidence-based best practices that call for introducing a patient to new treatment staff at least twice before residential discharge.72 This practice is intended to smooth care transitions and increase the rate of community-based treatment engagement after residential discharge. Having implemented bundled payments for episodes of care in 2019, Vermont is transitioning to value-based payments for IMD SUD services by January 2021, seeking to eliminate incentives for longer residential stays resulting in higher provider payments. The model is designed to encourage providers to engage in effective discharge planning, with payment disincentives for rapid readmissions. Virginia requires providers to include comprehensive transition plans and coordination of current care and post-discharge plans related to community services in their treatment plan to ensure continuity of care upon discharge with the individual’s family, school and community.
In addition to covering new services, states took steps to expand or maintain IMD residential provider networks for SUD services. San Diego County has worked to develop its residential provider network, while Vermont is focused on maintaining its long-standing network. One challenge in San Diego and other California counties has been helping residential providers establish the record keeping and quality improvement initiatives needed to successfully bill for Medicaid services.73 San Diego’s initiatives in this area include “gentle” reimbursement withholding incentives, in which a portion of provider payment is delayed until certain performance standards are met. San Diego also has spent substantial county staff time offering technical assistance to providers and introduced advance payments so that providers had funding available upfront to establish the needed administrative infrastructure.
States also worked to expand their community-based provider networks and increase payment rates. Virginia has been able to use state funds to fund “significant” provider rate increases for intensive outpatient and partial hospitalization services intended to build the Medicaid provider network. California’s waiver broadens the range of approved SUD treatment providers and allows counties to pay providers at higher than state plan rates to account for geographic differences and encourage providers to add capacity.74
All three areas also have initiatives to improve care coordination across providers to help ensure that enrollees remain connected to care as required under waiver guidance and milestones. For example, Virginia added a new office-based treatment program benefit, which co-locates a buprenorphine waivered provider and a licensed mental health provider, and includes reimbursement for care coordination. Virginia also changed its policy to allow both medical and SUD providers to bill for services for the same patient on the same day. This change was identified as a lesson learned to incentivize engaging patients in SUD treatment when they come in for other needed care. For example, a pregnant woman may see both an obstetrician and an MAT provider on the same day. San Diego County is including peer advocates and social work staff alongside doctors in emergency departments to help connect patients to community-based treatment after discharge.
Evaluation results in all three areas show increased treatment service utilization and provider participation. Results from the first year (April 2017 to March 2018) of waiver implementation in Virginia found that the number of outpatient providers billing for ARTS services increased by 173%;75 the number of Medicaid enrollees who used SUD treatment services increased by 57%;76 and more than 40% of enrollees with SUD received treatment, up from 24% in the prior year.77 In the seven counties that began service delivery in 2017, California’s waiver evaluation found that the number of people accessing treatment increased by about 7%.78 In the three counties included in the California waiver’s managed care external quality review report, the number of enrollees receiving SUD services nearly tripled in the first year of waiver implementation, compared to pre-waiver baseline claims data.79 While not yet included in California’s waiver evaluation findings, San Diego County anecdotally reports a 40 to 50% increase in the number of patients receiving SUD treatment services on both an inpatient and outpatient basis since waiver implementation in July 2018, compared to the corresponding month in the prior year. Vermont’s evaluation for 2013 to 2016 found that rates of initiation and engagement in community-based treatment post inpatient discharge for enrollees who had received IMD services exceeded both the general Vermont Medicaid rate and the national rate for both SUD and psychiatric services.80
California’s waiver evaluation found notable gains in access to residential treatment that could not have been financed by Medicaid without the waiver.81 Additionally, the California waiver’s managed care external quality review report notes that without the IMD payment authority, “[a]pproximately 80 percent of the residential facilities in California would not have qualified for [Medicaid] reimbursement, thus severely limiting treatment options.”82 As of March 2019, San Diego County reported adding 67 IMD beds, which has reduced the number of patients waiting for services.83
Evaluation results also have found decreases in emergency room visits and inpatient hospitalizations. From 2013 through 2016, Vermont’s interim waiver evaluation found that emergency room use within 30-days post-IMD discharge declined compared to emergency room use prior to the IMD admission for both mental health services (with declines ranging from 23 to 44%)84 and SUD services (with declines ranging from 39 to 56%).85 Psychiatric IMD readmission rates averaged 8% after 30 days over the four years, while SUD readmission rates were under 15% across settings (general hospital detox, IMD detox, and IMD residential) during this period.86 During the first 10 months of waiver implementation in Virginia, the number of emergency department visits related to SUD decreased by 14%, and the number of Medicaid enrollees with an acute inpatient admission related to SUD decreased by 4%.87
States report that existing IMD authority and policy may limit their efforts to address unique needs of special populations, such as pregnant women and individuals in the criminal justice system. With Vermont’s transition from its older waiver authority to waivers under the more recent CMS guidance, the state will no longer be able to use federal Medicaid funds for a specialized residential treatment facility that serves pregnant women and new mothers and infants. That care delivery model is based on a length of stay of 12 to 18 months, with an average length of stay of six months from 2013 through 2016.88 As a result, including this one program would cause the statewide average length of stay to exceed the 30 days approved in Vermont’s waiver. San Diego County and Virginia both reported unexpected challenges where the courts were ordering defendants to residential SUD treatment instead of incarceration, without regard to the evidence-based placement criteria adopted under the waiver that instead called for outpatient treatment.89 In both cases, Medicaid staff had to educate the courts about the need to order a medical evaluation to determine the appropriate level of care instead mandating residential care in all circumstances.
States report that waiver terms about IMD lengths of stay may not align with current evidence-based or state practices. California’s external quality review report found that the waiver’s limit of two IMD stays per year may be too restrictive because patients often do not complete their initial residential treatment visits, instead leaving in the first week to 10 days, but then later return when they are ready to commit to treatment.90 The report notes that current clinical criteria call for residential treatment to stabilize SUD issues, followed by partial hospitalization or intensive outpatient services, but do not limit residential treatment to two stays per year. In contrast, Virginia’s waiver initially included a 90-day maximum IMD stay, but CMS subsequently removed that provision, recognizing that stays tend to be longer at the lower levels of residential care where the focus is more on supportive services and less on clinical care. While Vermont finds that a 30-day average statewide length of stay is appropriate for SUD treatment, it believes that this limit will be too limiting for mental health treatment, especially with CMS’s newly cited position that federal Medicaid funds will be limited to individual IMD stays that do not exceed 60 days. Vermont’s state hospital serves patients with the most severe needs that can take “substantially longer to stabilize;” the average length of stay there is 120 days. Vermont will be able to meet CMS’s 30-day statewide average requirement by averaging that facility’s stays with another IMD that has more beds and serves patients with less acute needs. However, Vermont is concerned that its ability to use federal Medicaid funds for most of its state hospital patients will be limited because CMS has newly proposed that Medicaid cannot fund individual IMD stays that exceed than 60 days.
States are considering non-waiver exemptions to the IMD waivers, in part due to the time limited nature of waivers. For example, while Vermont reports that its IMD SUD waiver is working well, it also is considering pursuing the SUPPORT Act state plan option. While “largely redundant” of its existing waiver, the state sees the state plan option as more of a “long-term assurance” to have IMD payment authority in place. Virginia noted that it decided to add SUD community-based services using state plan rather than waiver authority as a way of “securing” those services as waivers are not permanent.
States are drawing on their experience with IMD SUD waivers to inform their consideration of whether to pursue and how to design an IMD mental health waiver. Before applying for an IMD SUD waiver, Virginia reviewed its existing Medicaid SUD benefits to determine what was working well and whether there were other evidence-based services that could be added to the benefit package to establish a robust community-based continuum of care. Now, Virginia is similarly assessing its Medicaid-covered mental health services. The state plans to establish a solid community-based services foundation first and then pursue a future IMD mental health waiver. After largely deinstitutionalizing its mental health services over the past 30 years,91 Vermont is working to retain a minimum capacity for patients with the most acute needs.92 The state is concerned that losing its current IMD mental health capacity under the existing federal funding phase-out plan will strain its community-based providers, who would be challenged by having to serve patients with more severe needs and as a result have less capacity to serve those with less severe needs. In Vermont’s experience, providing institutional care for the most acute patients reserves community-based services for those who do not need institutional care.
Many people with behavioral health diagnoses report unmet treatment needs, with substantial shares of nonelderly adults with SUD and any mental illness reporting an unmet need for drug or alcohol treatment. Though treatment utilization among nonelderly Medicaid adults with behavioral health needs is greater than the privately insured, treatment rates are low across all payers. Enabling states to access federal Medicaid funds for inpatient SUD and mental health treatment could help to address some of this unmet need and help states to cover services that reflect current evidence-based treatment standards. Additionally, providing federal matching funds for IMD services can free up state dollars previously spent on inpatient treatment to instead fund corresponding expansions in community-based services across the behavioral health care continuum. By law, state initiatives to expand behavioral health services cannot solely focus on inpatient services and instead also must consider community-based services, given states’ community integration obligations under the Americans with Disabilities Act. Thus, state expansion of behavioral health services under efforts to fund IMDs may also address demonstrated unmet treatment needs for outpatient behavioral health services.
The number of states with Section 1115 IMD SUD payment waivers has increased dramatically since 2017, now comprising over half the states. DC, Indiana, and Vermont have submitted applications seeking an IMD mental health payment waiver under the new guidance to date, other states have expressed interest, and more applications are likely to follow. In addition, the SUPPORT Act option for IMD SUD services is newly available to states in October 2019, with a few states expressing interest to date. All three case study areas in this report reported overall positive experiences with their waivers, supported by early evaluation findings, along with some implementation challenges that had to be resolved. Notably, all three areas had devoted substantial time and resources to expanding and strengthening a robust network of community-based SUD treatment services in addition to IMD services. Policymakers reported that receiving federal Medicaid funds for IMD services under the waivers can allow state and local funds to be used to expand community-based service options, increase provider payment rates, and develop other necessary program features that Medicaid does not fund, such as housing.
Given the widespread use of SUD waivers, and the notable policy change now allowing mental health waivers, states, health plans, providers, and enrollees will be interested in evaluation results assessing the waivers’ impact. Key questions include how allowing states to use federal Medicaid funds for IMD services affects access to and utilization of inpatient and outpatient care, health outcomes, care quality, costs, IMD day limits, discharge planning and care transitions, and the continued evolution of evidence-based best practices for SUD and mental health treatment. States may draw on their IMD SUD waiver experience to inform their design and implementation of IMD mental health waivers, and many enrollees have co-occurring SUD and mental health conditions. Still, it is not entirely clear how states’ IMD SUD experience will translate to IMD mental health waivers, given differences in providers and different requirements in CMS guidance. CMS and states may implement policy changes that represent lessons learned based on states’ mid-point assessments toward their waiver milestones. While some waiver evaluation results are emerging, most are not expected until 2024 or 2025. In the meantime, states’ quarterly and annual waiver reports to CMS and interim evaluation findings can provide important information about the waivers’ impact to inform whether CMS makes further Medicaid IMD policy changes and/or whether Congress acts to amend the statute.
This work was supported in part by the Milbank Memorial Fund. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The authors appreciate the time that public officials in Vermont; San Diego County, California; and Virginia, as well as members of the Fund’s Reforming States Group Inpatient Mental Health Financing Workgroup (Nick Macchione, San Diego County; Becky Pasternik-Ikard, Oklahoma; Sue Birch, Washington; Duane Mayes, Alaska; Judy Lee, North Dakota; Kate McEvoy, Connecticut; and Tom Alexander, South Carolina), spent sharing their experience and expertise.
–
Care Continuum: An integrated system of care that guides and tracks patients over time through a comprehensive array of health services spanning all levels of care.93
Community-based care: Healthcare provided in the home or another community setting and that typically allows the person to stay in their home rather than moving them to a facility to receive care. Examples include home health aides, case management services, and personal care services.94
Disproportionate Share Hospital (DSH) payments: Payments required by federal law from state Medicaid programs to qualifying hospitals that serve a large number of Medicaid and uninsured individuals.95
Inpatient Treatment: Healthcare provided upon admission to a facility, such as a hospital. Typically treats more severe diagnoses, provides 24-hour medical and emotional support, and involves the patient staying in the facility for an extended period of time.
Institution of Mental Disease: Hospital, nursing facility, or other institution of more than 16 beds, that is primarily engaged in providing diagnosis, treatment, or care of persons with mental diseases, including medical attention, nursing care, and related services.96
Institutional Care: Healthcare provided in an institutional setting such as a nursing facility, mental health institution, or an intermediate care facility for individuals with intellectual disability.
Medicaid Managed Care: Delivery system for Medicaid covered services by health plans that accept a set capitated payment for these services through a contract with the state Medicaid agency.97
Olmstead case: 1999 Supreme Court decision that found that the unjustified institutionalization of people with disabilities is illegal discrimination. Requires states to eliminate unnecessary segregation and ensure that persons with disabilities receive services in the most integrated setting appropriate to their needs.98
Outpatient Treatment: Healthcare provided in a part-time setting that allows the patient to continue their day-to-day activities outside of treatment. Typically allows the patient to maintain a more normal daily routine and relies more heavily on social circle support.
Section 1115 Demonstration Waiver: Authority by which HHS Secretary can allow states to test new approaches in Medicaid that differ from what is required by federal statute.99
Serious Emotional Disturbance: Someone under the age of 18 with a diagnosable mental, behavioral, or emotional disorder in the past year, which resulted in functional impairment that substantially interferes with or limits their role or functioning in family, school, or community activities.100
Serious Mental Illness: Someone over the age of 18 with a diagnosable mental, behavior, or emotional disorder that causes serious functional impairment that substantially interferes with or limits one or more major life activities.101
Substance Use Disorder: Recurring use of alcohol or drugs that causes significant clinical and functional impairment.102
SUPPORT Act: Federal law partially lifting the IMD payment exclusion by allowing states to use federal Medicaid funds for nonelderly adults receiving IMD SUD services up to 30 days a year, from October 2019 through September 2023.103
(Back to top)–
(Back to top)–
(Back to top)–
The average person with traditional Medicare coverage paid $5,460 out of their own pocket for health care in 2016, according to a new KFF analysis and interactive tool.
This $5,460 includes about $1,000 in out-of-pocket spending for long-term care facility services, averaged across all traditional Medicare beneficiaries. Such services are used by only 5 percent of beneficiaries in traditional Medicare. For the 95 percent of beneficiaries living in the community, average out-of-pocket spending on health care was $4,519 in 2016. But some groups of beneficiaries spent substantially more than others.
According to the analysis – based on the most current public data — beneficiaries who were likely to spend more out of pocket include women, people in older age groups, those who had been hospitalized, people in poorer self-reported health, and those with multiple chronic conditions.
The analysis comes at a time when some policymakers and presidential candidates are discussing proposals to expand coverage through programs modeled in some respects on Medicare, and improve financial protections and lower out-of-pocket costs for people currently covered by Medicare. Current Medicare-for-all proposals would largely eliminate premiums and out-of-pocket costs, including for those now covered by Medicare.
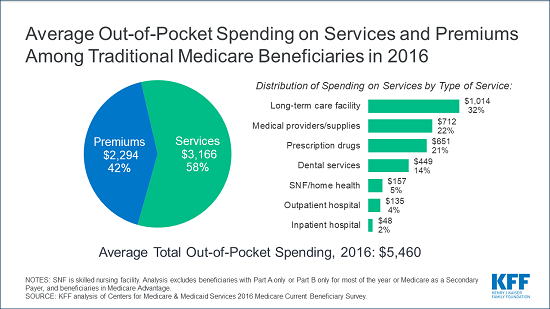
The analysis includes three interactive graphics that allow users to explore out-of-pocket spending data for different subgroups of Medicare beneficiaries, such as age, gender, and income, to see:
The analysis is based on the most current year of out-of-pocket spending data available from the Medicare Current Beneficiary Survey, a nationally representative survey of Medicare beneficiaries. It does not include spending by beneficiaries in Medicare Advantage plans, due to a lack of publicly available data for beneficiaries enrolled in the private Medicare plans.
Many policymakers and presidential candidates are discussing proposals to build on Medicare in order to expand insurance coverage and reduce health care costs, and improve financial protections and lower out-of-pocket costs for people currently covered by Medicare. More than 60 million people ages 65 and older and younger people with long-term disabilities currently rely on Medicare to help cover their costs for health care services, including hospitalizations, physician visits, prescription drugs, and post-acute care. However, Medicare beneficiaries face out-of-pocket costs for their insurance premiums, cost sharing for Medicare-covered services, and costs for services that are not covered by Medicare, such as dental care and long-term services and supports.
In 2016, the average person with Medicare coverage spent $5,460 out of their own pocket for health care (Figure 1). This average includes spending by community residents and beneficiaries residing in long-term care facilities (5% of all beneficiaries in traditional Medicare). Among community residents alone, average out-of-pocket spending on premiums and health care services was $4,519 in 2016. But some groups of beneficiaries spent substantially more than others. Current Medicare-for-all proposals in Congress and from presidential candidates would largely eliminate out-of-pocket costs for premiums and patient cost sharing, including for people now covered under Medicare.
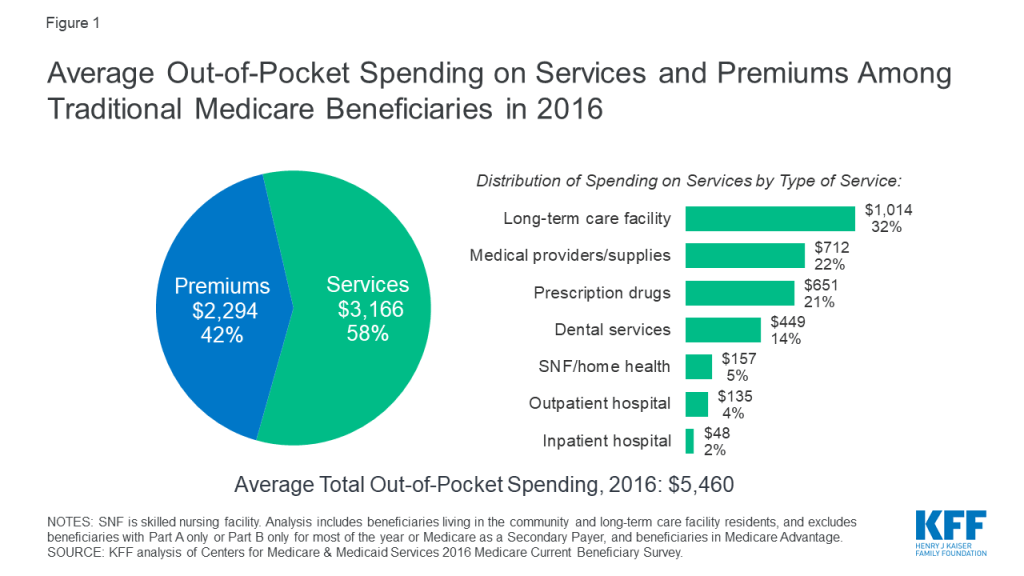
This analysis presents the most current data on out-of-pocket health care spending by Medicare beneficiaries, both overall and among different groups of beneficiaries. The analysis addresses three main questions:
The analysis is based on the most current year of out-of-pocket spending data available (2016) from the Medicare Current Beneficiary Survey (MCBS), a nationally representative survey of Medicare beneficiaries. The analysis includes beneficiaries living in the community and long-term care facility residents, and excludes beneficiaries enrolled in Medicare Advantage due to unverified reporting of events and spending for these beneficiaries in the MCBS. (See Methodology for details). All results presented in the text are statistically significant (see Appendix to access a downloadable table of results).
The graphic below shows how much the average person with traditional Medicare spent out of pocket for health care in 2016. Total out-of-pocket spending includes spending on medical and long-term care facility services and insurance premiums, with comparisons across different groups of beneficiaries.
Our analysis shows that Medicare beneficiaries spent $5,460 out of their own pockets for health care in 2016, on average, with more than half (58%) spent on medical and long-term care services ($3,166), and the remainder (42%) spent on premiums for Medicare and other types of supplemental insurance ($2,294). This average includes spending by community residents and beneficiaries residing in long-term care facilities (5% of all beneficiaries in traditional Medicare). Among community residents alone, average out-of-pocket spending on premiums and health care services was $4,519 in 2016.
Average total out-of-pocket spending varies considerably across different groups of beneficiaries.
The graphic below shows average out-of-pocket spending for specific health and long-term care services by traditional Medicare beneficiaries in 2016, with comparisons across different groups of beneficiaries.
Of the total average per capita spending on health and long-term care services in 2016 ($3,166), Medicare beneficiaries spent the most on long-term care (LTC) facility services, which are not covered by Medicare ($1,014, or 32% of average out-of-pocket spending on services), followed by medical providers and supplies ($712; 22%), prescription drugs ($651; 21%), and dental services ($449; 14%). These estimates are averaged across all traditional Medicare beneficiaries including users and non-users of each service; average spending among users would be higher than the averages presented here.
Average out-of-pocket spending by service varies across different groups of beneficiaries. For example:
The graphic below shows out-of-pocket spending on health-related services as a share of total per capita income, at the median, with comparisons across different subgroups of beneficiaries.
Our analysis shows that half of all beneficiaries in traditional Medicare spent at least 12% of their income on out-of-pocket health care costs in 2016. One quarter of all beneficiaries spent at least 23% of their incomes on health-related services in 2016, while 10% spent nearly half of their income (data not shown).
The median out-of-pocket health care spending burden varies by beneficiary subgroups. For example:
In 2016, people with traditional Medicare spent an average of $5,460 out of pocket for health care expenses, including premiums, cost sharing, and costs for services not covered by Medicare. Half of all traditional Medicare beneficiaries spent at least 12% of their total per capita income on health care. Although Medicare has helped make health care more affordable for people with Medicare, many beneficiaries face high out-of-pocket costs for care they receive, including costs for services that are not covered by Medicare—in particular, long-term care services. Some groups of beneficiaries face substantially higher out-of-pocket costs than others, including women, those ages 85 and over, those who are in poorer self-reported health and who have multiple chronic conditions, and those with no supplemental coverage.
The fact that traditional Medicare does not have an annual out-of-pocket limit and does not cover certain services that older adults are more likely to need may undermine the financial security that Medicare provides, especially for people with significant needs and limited incomes. Addressing these gaps would help to alleviate the financial burden of health care for people with Medicare, although doing so would also increase federal spending and taxes.
Juliette Cubanski, Wyatt Koma, and Tricia Neuman are with KFF.Anthony Damico is an independent consultant.
This interactive analysis is based on data from the Centers for Medicare & Medicaid Services (CMS) Medicare Current Beneficiary Survey (MCBS) Cost Supplement for 2016, the most recent year available. The MCBS is a survey of a nationally-representative sample of the Medicare population, including both aged and disabled enrollees who are living in the community as well as facility residents. The dataset integrates survey information reported directly by beneficiaries with Medicare administrative data. Survey-reported data includes the demographics of respondents, such as sex, age, race, living arrangements, income, health status, and physical functioning, the use and costs of health care services, and supplementary health insurance arrangements.
The survey also collects information on inpatient and outpatient hospital care, physician and other medical provider services, home health services, durable medical equipment, long-term and skilled nursing facility services, hospice services, dental services, and prescription drugs. Survey-reported information is matched to and supplemented by administrative records and billing and claims-level data when possible. Extensive efforts are made to verify the accuracy of survey reports and to reconcile discrepancies using administrative bill data to produce a more complete and reliable dataset.
Our analysis includes beneficiaries in traditional Medicare for most of their enrollment in 2016, and excludes beneficiaries enrolled in Part A or Part B only, those with Medicare as a Secondary Payer, and those enrolled in Medicare Advantage plans for most of their enrollment in 2016. For Medicare Advantage enrollees, it is not possible to verify survey-reported events in the MCBS with administrative claims data, as is done for beneficiaries in traditional Medicare. This has the effect of biasing downward survey-reported out-of-pocket spending amounts for Medicare Advantage enrollees compared to beneficiaries with traditional Medicare. It is not possible to determine whether observed differences are real or due to underlying differences in the data collection, verification, and imputation process for out-of-pocket spending by beneficiaries in traditional Medicare and Medicare Advantage. Therefore, we exclude Medicare Advantage enrollees (unweighted n=2,726) to avoid introducing bias associated with underreporting of events and spending for this population.
We also excluded beneficiaries who were enrolled in only Part A or Part B (unweighted n=298) and those with Medicare as a Secondary Payer (unweighted n=231) for most of their Medicare enrollment in 2016 Because Medicare is typically not the primary payer for those who are enrolled in only Part A or Part B but not both programs, beneficiaries with only Part A or Part B also have significantly lower average total out-of-pocket spending relative to those enrolled in both Part A and B, which is the rationale for excluding them from the analysis of out-of-pocket spending.
After excluding these groups of enrollees, our sample for the analysis of spending as a share of total income included 5,369 respondents in traditional Medicare (32.7 million weighted) in 2016. We analyze out-of-pocket spending among all traditional Medicare beneficiaries and by specific beneficiary subgroups, including age (under 65, 65-74, 75-84, 85 and over), gender (female, male), age by gender, race (white non-Hispanic, black non-Hispanic, Hispanic), race by gender, race by age, marital status (married, divorced/separated, widowed, single (never married)), education level (less than high school, high school graduate, some college, college graduate), per capita income categories (increments of $10,000), self-reported health status (excellent, very good, good, fair, poor), number of chronic conditions (none, 1-2, 3-4, 5 or more), Census region (Northeast, Midwest, South, West), metropolitan area (metropolitan, rural micropolitan, rural adjacent or nonadjacent), type of residence (community, facility), supplemental coverage (employer-sponsored insurance (ESI), Medicaid, Medigap, none), hospital use (no inpatient stay, any inpatient stay, one inpatient stay, two or more inpatient stays), and specific chronic conditions.
Out-of-pocket spending for medical and long-term care services reported in the MCBS is not the same as beneficiary liability or the Medicare cost-sharing amount for services used. Instead, out-of-pocket spending amounts are net of payments by any third-party payers, such as payments by Medicaid, Medigap, or employer-sponsored insurance. Survey-reported out-of-pocket payments are those payments made by the beneficiary or their family, including direct cash payments or in the form of Social Security or Supplemental Security Income (SSI) checks to a nursing home.
Out-of-pocket spending on premiums is derived from administrative data on Medicare Part A, Part B, and Part D premiums for each sample person along with survey-reported estimates of premium spending for other types of health insurance beneficiaries may have (including Medigap, employer-sponsored insurance, and other public and private sources). Part B premium amounts reported in the MCBS include income-related premiums paid by beneficiaries with higher incomes (more than $85,000 per individual/$170,000 per married couple). The administrative data reflect liability, not the actual payments made by beneficiaries for their premiums, which overstates actual premiums paid for certain groups of beneficiaries who are not responsible for paying their Medicare premiums. People who are dually-eligible for Medicaid are generally not liable for their Part A, Part B, or Part D premiums; those who receive the Part D low-income subsidy are eligible for full or partial coverage of their Part D premium. For these groups of beneficiaries, we adjusted the premium estimates reported in the MCBS to reflect the premium subsidies they receive. For beneficiaries reported as receiving the Part D low-income subsidy but who were not enrolled in benchmark plans (based on Part D contract IDs in the MCBS), we assigned premiums based on plan-specific data from the 2016 Part D landscape file.
The medical and long-term care services included in this analysis are:
The MCBS includes a measure of total income for individual respondents and their spouses, if applicable. However, the MCBS does not report all sources of income that some beneficiaries may have. As in many other surveys, income is self-reported, with beneficiaries asked to report total annual income for themselves and their spouses (where applicable) from all sources, including earnings, Social Security, pensions, and asset income. However, beneficiaries are not asked to report specific income amounts by source, and some types of income may go unreported or may be underestimated. Therefore, this measure results in an overall underreporting of income, particularly for those with relatively high incomes. This conclusion is based on a comparison of MCBS income estimates to income estimates from DYNASIM3, in which we measured the divergence of MCBS and DYNASIM income estimates at each percentile of per capita income.
We used the results of this comparison to derive adjustment factors for each percentile with which to rescale each MCBS respondent’s income. In general, this produced estimates of MCBS respondents’ income that are higher than self-reported values and that we believe are a more accurate representation of income among people on Medicare. We then combined this adjusted income estimate with per capita out-of-pocket spending estimates in the MCBS to derive a more reliable estimate of Medicare beneficiaries’ per capita out-of-pocket health care spending as a share of total income than one based on MCBS self-reported income data alone.
To estimate total out-of-pocket spending per beneficiary in traditional Medicare, we calculate for each sample person aggregate estimates of out-of-pocket spending on both insurance premiums for Medicare Parts A, B, and D and supplemental insurance coverage, and medical and long-term care services reported in the MCBS. These amounts are averaged across the entire sample of traditional Medicare beneficiaries and weighted to be representative of the traditional Medicare beneficiary population or specific subgroups of beneficiaries. Analysis of spending by type of service includes beneficiaries who did and did not use each type of service. References to “total out-of-pocket spending” in this analysis always include both premiums and service spending. We also often refer to the separate components of total spending (either out-of-pocket spending on services or premiums) in presenting results. For some beneficiary subgroups, estimates of out-of-pocket spending by service type may not add up to the total for all services due to missing data related to small sample size.
To measure per capita out-of-pocket health care spending as a share of per capita total income, we computed for each individual a ratio of out-of-pocket spending to total per capita income, arrayed the individual ratios of annual out-of-pocket spending to annual income from low to high and computed the median for the entire group of traditional Medicare beneficiaries, and by beneficiary subgroups.
Due to missing data related to small sample size, we are unable to show the median out-of-pocket spending as a share of income for beneficiaries who had Medicaid for part of the year and lived in the community. Similarly, we are unable to show the median out-of-pocket spending as a share of income for Medicare beneficiaries who are black and under the age of 65.
Ahead of the annual Affordable Care Act (ACA) open enrollment period, the time during which consumers can shop for health plans or renew existing coverage, KFF has updated and expanded its searchable collection of more than 300 Frequently Asked Questions about open enrollment, the health insurance marketplaces and the ACA.
Designed to help consumers and the navigators, brokers and others who assist them, the FAQs cover a wide range of topics including eligibility for subsidies, requirements for health coverage and information about health plans offered through state ACA marketplaces.
The updated collection includes a new section addressing the sale of Marketplace plans on private websites, sometimes described as “direct enrollment” sites or “certified enrollment partner” sites, as well as new answers to questions about immigration status and enrollment options for those affected by Hurricane Dorian.
More than 180 of the FAQs in the collection are available in Spanish.
Open enrollment for the Federal and most state marketplaces begins Friday, Nov. 1, 2019 and ends on Sunday, Dec. 15, 2019. Organizations assisting consumers are encouraged to link to the FAQ web page. Each question and answer may be shared individually by direct link, via Twitter and Facebook.
In addition to the FAQs, KFF also offers short, printable fact sheets on four common scenarios for consumers shopping for health plans:
KFF’s Health Insurance Marketplace Calculator will soon be updated with 2020 premium data. Visit https://www.kff.org/understanding-health-insurance for KFF’s most current resources for consumers looking for answers about open enrollment, the marketplaces and health insurance in general.
Since taking office, the Trump Administration has implemented a range of policies to curb immigration and enhanced immigration enforcement efforts. Amid this policy and political climate, immigrant families are reporting growing fears and challenges which are affecting their and their children’s health and well-being and have implications for organizations serving immigrant families and their broader local communities. This brief presents findings from discussions with service providers across sectors (including health, legal, and education), local officials, and parents in immigrant families in the San Francisco Bay Area and San Diego about issues facing immigrant families and providers in the current environment, how the local communities have responded to growing needs, and key priorities and opportunities identified for serving immigrant communities. It is based on roundtable discussions and interviews with service providers and local officials (referred to as providers throughout this brief) and focus groups with parents in immigrant families that were conducted by the Kaiser Family Foundation in Summer 2019. It finds:
Providers and families reported that the shifting policy and political environment has substantially increased fear and uncertainty among immigrant families, leading to negative effects on families and growing pressures on local organizations and communities. They noted that families, including children, have increased mental health needs, such as anxiety and depression, and are facing growing economic pressures that are compounded by fears of accessing public programs and services. Providers expressed concerns about the long-term negative consequences of the current environment for families and the potential implications of worsened health conditions and unrealized potential among the youth for the broader community. They also pointed to growing pressures on service providers and local communities, including stress and secondary trauma among staff serving families and increased challenges providing services, particularly legal support, to families in light of ongoing and uncertain policy changes. Providers and families noted that organizations and communities have shifted some resources and efforts away from longstanding immigrant populations to address needs of new migrants, who are often in crisis and need immediate support.
“I don’t understand how they get by day-by-day. Being traumatized and re-traumatized over and over….I mean these kids are always fearful, always thinking their parents are going to be deported, constantly in trauma.” Legal Services Provider, San Diego
“The crisis today—we’re going to see the effects from it ten years from now, five years from now.” Health Provider, San Francisco Bay Area
“It’s a lot of just having to be in crisis mode and reactionary mode that is really not sustainable. Unhealthy for the people affected, unhealthy for the staff…” Community-based Organization, San Diego
Families are decreasing use of programs and services due to fears. Families and providers pointed to a range of concerns among families about using programs and services, including increased risk of deportation, potential negative impacts on ability to adjust status and/or sponsor relatives, and being required to pay back benefits. Providers indicated that the administration’s changes to public charge and housing assistance policies have amplified fears. Providers and families reported that families are disenrolling themselves and their children from Medi-Cal (the Medicaid program in California) and other programs, and declining to renew or enroll themselves or their children in programs despite being eligible.
“…they’re scared to apply for certain much needed funding whether it’s Calfresh [food assistance] or it’s Medi-Cal, to get them the health insurance.” Family Services Provider, San Francisco San Francisco Bay Area
“…what we’re seeing is a lot of women are very hesitant to now enroll in medical services…They’re getting care here in the very last stages of their pregnancy and…the health of the mom and the child are impacted.” Health Provider, San Diego
Providers described how the San Francisco Bay Area and San Diego communities have responded to growing needs among immigrant families by strengthening cross-sector relationships and enhancing services and supports. They highlighted a range of strategies including strengthening existing or developing new cross-sector relationships, expanding capacity in other sectors to provide mental health screenings and services, increasing services and supports in schools, identifying trusted individuals and organizations to communicate with and assist families, and providing support for staff in service organizations. Providers and families indicated that actions by state and local leaders and certain state and local policies have underpinned the community response.
“I do think that if it wasn’t for building this cross-sector, multi-disciplinary, multi-agency network…we wouldn’t have been able to do some of the good things that we’ve been able to do.” Legal Services Provider, San Diego
“The other component that we are working with…is really building out mental health services and supports to our schools. …how do we provide trainings to teachers to identify depression, identify anxiety and how do we react and what resources do we have in place?” Educator, San Diego
“I live in California. I can go wherever here, and I feel protected because, thank God, we have people who support us and we are a sanctuary city, and that comforts me.” Parent, San Francisco Bay Area
Looking ahead, providers identified a range of priorities, including continuing to integrate and coordinate services and filling gaps in mental health care and legal support. They suggested continuing to strengthen cross-sector partnerships so they are sustainable over time; addressing gaps in mental health and legal services by facilitating connections to existing services and increasing the supply of providers over the long-term; and providing resources to meet the increased demands on non-profit organizations and local governments. Other key priorities they identified included maintaining access to health care as people disenroll from Medi-Cal; addressing shifting demographics and growing needs in underserved areas; educating and informing families, service providers, and legislators about ongoing policy changes; increasing access to data; and developing philanthropic approaches that respond to evolving needs. Providers also pointed to the role state leaders can play in framing public discussion of immigration issues and supporting efforts to address family needs and fill service gaps moving forward.
“…the model of intervention has to be a wraparound model. It has to be a comprehensive set of services that wraps around rather than siloed service…” Family Services Provider, San Francisco Bay Area
“…funding for legal services is critical. Building up the…army of immigration attorneys. …it’s a most complex area of the law, and it’s changing by the minute.” Legal Services Provider, San Diego
“We have seen a great number of people disenrolled in programs for which they are eligible… This does translate to greater burdens on our nonprofit community and our CBOs [community-based organizations], but also on local government to cover all the gaps.” Local Official, San Francisco Bay Area
In sum, families and providers report that the shifting policy and political environment is leading to increased fears and uncertainty among immigrant families that have wide-ranging negative effects on families’ daily lives and health. The growing fears and challenges among families also are increasing pressures on service providers and local communities. The San Francisco Bay Area and San Diego communities have responded to growing family needs in many ways that center on strengthening cross-sector partnerships and relationships and enhancing services and supports for families and service providers. Looking ahead, providers view continuing to support cross-sector collaborations and addressing gaps in services, particularly mental health and legal services, as key priorities. Providers also highlighted an ongoing need for trusted information and education about policy changes for families and service providers. Providers pointed to varied ways state and local leaders and philanthropy can support efforts to address families and service organizations moving forward, and stressed that addressing these needs is key for preventing erosion of California’s progress advancing health.
Since taking office, the Trump Administration has implemented policies to curb immigration and enhanced immigration enforcement efforts. Amid this policy and political climate, immigrant families have reported increased levels of fear and anxiety and challenges affecting their and their children’s daily lives, health, and well-being. Families’ growing fears and needs also have implications for organizations serving immigrant families as well as their broader local communities. This brief presents findings from service providers across sectors (including health, legal, and education), local officials, and parents in immigrant families in the San Francisco Bay Area and San Diego about challenges facing families and providers in the current environment, how the local communities have responded to growing needs, and key priorities and opportunities identified for serving immigrant communities in the future. It is based on policy roundtable discussions and interviews with service providers and local officials (referred to as providers throughout this brief) and focus groups with parents in immigrant families conducted by the Kaiser Family Foundation in Summer 2019 (see Methods box for more information). Blue Shield of California Foundation supported this work.
Growing levels of fear and uncertainty. Providers and families reported that families are fearful of raids and deportation and being separated from their children. They noted that these fears extend to children who worry about being separated from their parents as well as to people of varied immigration statuses, including legal immigrants. Fears are leading some families to limit daily activities such as driving and social interaction. Some individuals also are fearful of interacting with the police, leading to concerns among providers and families that individuals may be less willing to report crimes, including incidences of domestic violence. Providers pointed out that the fears among families are not new, but have become more intense in the current environment. Families and providers also described how increased discrimination and bullying in schools is leading some children to feel isolated and disconnected from the local community and noted that Muslim communities have been particularly affected by these issues.
“If something happens…who am I going to leave them with? Is it very hard, and they get sad because in TV they show they separate the kids from the parents, they take the parents and leave the kids here.” Parent, San Francisco Bay Area
“I try not to talk as much with others…if someone greets me, I greet them back, but I try not to have a conversation with them. I am fearful.” Parent, San Diego
“As many of you have talked about the situations in the school districts or in the school sites—there definitely has been a higher rate of anxiety….Also what we see is the increase of bullying.” Educator, San Diego
“We have a lot of fear about deportation, not just from our undocumented population, but from our longtime immigrants.” Local Official, San Francisco Bay Area
Economic pressures. Providers and families described how many immigrant families have faced challenges paying their monthly expenses, especially as costs of basic needs continue to increase. They indicated that the current climate has exacerbated these economic challenges because it has led some individuals to lose jobs, resulted in more limited job options, and made some individuals scared to seek a job or go to work.
“I get anxious because we don’t have enough for the rent….We are making sacrifices to be better financially, but some things are affecting us.” Parent, San Diego
“Sometimes I work 12 hours, 4 days per week. I have to work….I am very worried about making enough for the rent and for my daughter– and food.” Parent, San Francisco Bay Area
“I tell my husband, ‘I rather only you go to work, and I stay home with the kids. I won’t go to work; the situation is not safe.’” Parent, San Diego
Housing challenges. Providers and families reported that continually rising housing costs in these communities are pushing families into crowded living situations and/or out of communities. Providers emphasized that families often have unequal housing relationships with landlords and landlords sometimes use threats of immigration enforcement to intimidate families, leaving them vulnerable to unfair and/or unsafe housing situations. They also stressed that the administration’s recent proposed changes to housing assistance policies would limit access to assistance for mixed immigration status families, further amplifying the housing challenges they face.
“…it’s no longer doubling up…it really is an acute health issue where families are living in garages, closets, single residency occupancy, hotels–and I’m not talking about one family, but multiple families.” Local Official, San Francisco Bay Area
“…the lack of affordable housing in San Diego is very much a driver of this. And some landlords believe that they need to get their current tenants out so that they can raise rents and have people come in that are not immigrants, and so they perform illegal evictions.” Legal Services Provider, San Diego
Increased mental health needs. Families, including children, are experiencing high levels of stress, anxiety, and depression due to increased fear and uncertainty, according to providers and families. Moreover, they described effects on behavior and health, such as problems sleeping or eating; psychosomatic symptoms, such as headaches and stomachaches; and worsened chronic conditions, such as asthma and diabetes. Providers noted that, for many individuals, these issues compound existing mental health needs stemming from histories of violence and trauma. Families recognized that they and their children might benefit from mental health care but pointed to stigma, cost, and lack of providers as barriers to care. Similarly, providers highlighted the large gap in available mental health services to meet growing needs, especially providers who can offer linguistically and culturally appropriate care.
“My 12-year-old daughter was affected the most; she has deep feelings about this. Every day she says she is praying for me so I can arrive safely home….sometimes I find her in her room reading and crying.” Parent, San Francisco Bay Area
“I don’t understand how they get by day-by-day. Being traumatized and re-traumatized over and over….I mean these kids are always fearful, always thinking their parents are going to be deported, constantly in trauma.” Legal Services Provider, San Diego
“…they went through a very traumatic journey to get here…And then, living here is traumatic for lots of reasons just because it’s a new place and you don’t speak the language and you’re afraid of the government, so the mental health needs are really very extreme and we are not good at serving those. That is our biggest gap by far.” Health Provider, San Francisco Bay Area
Potential long-term consequences. Providers expressed significant concerns about the long-term negative physical and behavioral health consequences of the fears and growing mental health needs among families. They are worried that the current environment will contribute to worsened physical and mental health outcomes and limit potential future contributions, particularly among youth. They noted that these consequences would not only affect immigrant families but also their broader communities.
“I’ve always wanted to finish my engineering career… but I also have the fear. My wife says, go and study, but there is also the fear that I am undocumented, how am I going to study?” Parent, San Diego
“…We have a mental health team at this school, but we’ve gotten a lot more referrals just in the past year…kids that are academically not doing well, they were doing well and they’re not. The kids have a lot of anxiety. They are losing sort of like ‘what’s my goal?’” Health Provider, San Diego
“The crisis today—we’re going to see the effects from it ten years from now, five years from now. Attachment issues…infant-parent attachment—but more important is community attachment—that’s been disrupted….” Health Provider, San Francisco Bay Area
Fears of accessing programs and services. Providers said that proposed changes to housing assistance policies as well as proposed changes to public charge policy (which were finalized after the roundtables, interviews, and focus groups were conducted and recently halted under a court order) have made families increasingly wary of enrolling in programs or seeking services for themselves and their children. Families have a range of concerns about participating in programs stemming from confusion and uncertainty about the changes, including fear of increased risk of deportation, negative consequences on ability to adjust status or sponsor other family members, and being required to pay back benefits. Providers reported that an increasing number of families are disenrolling themselves and their children from programs, including Medi-Cal (California’s Medicaid program), and not renewing or not enrolling in programs even though they or their children are eligible and are not directly affected by the policy changes.
“In my case, when I got WIC some years ago, the situation was different, it wasn’t as intense as now. If I had to request WIC now, I wouldn’t do it.” Parent, San Diego
“…they’re scared to apply for certain much needed funding whether it’s Calfresh [food assistance] or it’s Medi-Cal, to get them the health insurance.” Family Services Provider, San Francisco Bay Area
“…when they do adjust and they are eligible for all these public benefits, a lot of them, they don’t even want to apply for it anymore. And they waited years, months to be eligible for these benefits, but they’re just so afraid that the public charge will hurt them…..” Legal Services Provider, San Francisco Bay Area
“…we had hundreds of calls from people, mostly in mixed families status who called and said, ‘Get my son off Medi-Cal right now.’ ‘Why? He’s a U.S. citizen and so are you.’ ‘Just do it. Just do it. I don’t want anybody looking at my family.’” Legal Services Provider, San Diego
“…a patient that needed to be discharged with dialysis in place…absolutely refused to accept Medi-Cal coverage because he was concerned about public charge and so the decision that he made instead was to go across the border to Mexico every day.” Health Provider, San Diego
Health and economic impacts of decreased program use. Providers noted that families’ decreased participation in programs further increases the economic challenges they face. The also pointed to negative effects on health resulting from decreased participation in Medi-Cal and other support programs, such as increased risk of food insecurity and worse health outcomes due to delayed prenatal care, lack of access to specialty care, and less continuity of care.
“…it feels like there’s two destabilizing factors, public charge and families’ willingness to enroll or rely on those systems…because it [moves] families into greater poverty and alienates them even more from the local safety net, including legal aid.” Legal Services Provider, San Francisco Bay Area
“…sometimes we screen and we find things that are wrong with them and we want to refer and do a lot of things and then it just stops there. So, our health outcomes are severely impacted by this sort of fear….” Health Provider, San Diego
“…we had a patient who had a breast mass. Our physician had told her to go see a specialist. And because she had heard about public charge, she did not want to go see the specialist….” Health Provider, San Francisco Bay Area
“…what we’re seeing is a lot of women are very hesitant to now enroll in medical services. …They’re getting care here in the very last stages of their pregnancy and…the health of the mom and the child are impacted.” Health Provider, San Diego
Increased pressures on service providers. Providers noted that staff in service organizations often come from shared backgrounds and experiences of the families they serve and experience secondary or vicarious trauma working with families in the current environment. Moreover, addressing families’ growing needs has strained organizational capacity, especially since organizations were typically operating at full capacity before needs increased. Providers said they are operating in a reactive, crisis-response mode, leaving them little time or opportunity to strategize and plan. Moreover, they described how the constantly shifting legal and policy environment makes it difficult for staff to stay up-to-date on changes and leaves them feeling uncertain about how to advise families on some topics. Providers also pointed out that many staff in service organizations face their own economic challenges living in high-cost areas, making it difficult to retain staff.
“…I think we’re beyond secondary trauma and I think it’s been so intense that it’s now just primary trauma for the advocates, especially if they have lived experience…and the fact that people can’t keep up as attorneys and advocates with the shifts in the law…So it’s both the legal environment in which they’re trying to practice, and the face-to-face work with their clients.” Legal Services Provider, San Francisco Bay Area
“It’s a lot of just having to be in crisis mode and reactionary mode that is really not sustainable. Unhealthy for the people affected, unhealthy for the staff…” Community-based Organization, San Diego
“…we’re also losing a lot of the workforce in human services because they can’t afford to live here either.” Local Official, San Francisco Bay Area
Growing complexity and challenges associated with providing legal support. Legal services providers noted that they have experienced major increases in case volume over the last few years. At the same time, the length of time to process cases has increased, often extending beyond the duration of funding available to support the work. They also noted that the constantly shifting legal environment has made it increasingly difficult to stay up-to-date on policies and determine legal strategies, even for experts. Other challenges they pointed to included changes in fee waiver programs that have created new cost barriers to avenues of immigration relief and lack of sufficient mental health resources to conduct psychological assessments often required to support cases. Providers noted that, while there have been substantial increases in resources for direct legal support in recent years, many of these resources cannot be used to support operations or infrastructure development, making it difficult for organizations to expand capacity to address growing needs. They stressed that, overall, legal services capacity remains insufficient to meet current needs, and pointed to a particularly large gap in availability of bilingual providers.
“I think we’re all facing concerns about the increasing length of time on asylum cases. …The funding no longer syncs up with the duration of the case. So you get funded to do asylum work and the cases now take so long that the funding is likely gone, but you’re continuing to work on the case…” Legal Services Provider, San Francisco Bay Area
“The other real destabilizing factor is…that it’s going to become harder for people to access fee waivers…very few people in the population that we’re working with can afford those fees.” Legal Services Provider, San Francisco Bay Area
“So there are many areas of relief for immigration services…where you have a psychological evaluation or a mental health screening to support the legal case. None of those areas are funded.” Legal Services Provider, San Diego
“But really having to adapt and educate ourselves as things are changing….we’re constantly having to shift and reeducate ourselves and then create a new legal strategy. So that’s been difficult.” Legal Services Provider, San Francisco Bay Area
Addressing needs of new migrants. Providers and families noted that organizations and communities have shifted some resources and efforts away from longstanding immigrant populations to address needs of new migrants, particularly in border regions. Because newcomer populations are in crisis, organizations have focused on providing protection and crisis management for these groups. In addition, legal services providers have redirected some support to newcomers because they may have pathways to legal status, for example, through asylum, while opportunities for longstanding immigrants to naturalize or adjust status have become more limited due to declines in fee waivers and other policy changes.
“…this newcomer population if we gain their asylum, if we win their asylum cases they will have a work permit and they will eventually qualify to become permanent residents and citizens. And so we feel that the social return on investment is critical in investing in this newcomer population.” Family Services Provider, San Francisco Bay Area
“…the whole emphasis of the work that we did was to get folks citizenship. And that’s pretty much gone away…the work has completely changed.” Legal Services Provider, San Diego
Immigration enforcement in border areas. San Diego providers noted that, because they are close to the border, deportation can happen rapidly leaving little time for intervention or defense. Moreover, they indicated that the presence of interior checkpoints and controls and visible presence of Immigration and Customs Enforcement (ICE) and Department of Homeland Security (DHS) agents in the community increases fears among families and leads some to limit their activity and travel within the region. They emphasized that when agents bring individuals in custody to hospitals for care it raises fears among other patients and creates challenges for health providers, who lack clarity on their and their patients’ rights and health privacy rules in these situations. Providers further noted that federal officials have enhanced authority in border regions, such as being able to enter private property and interrogate without a warrant. Providers also pointed to the unique needs and challenges of binational families in border areas and indicated that it has become increasingly stressful for these families to cross the border, including children who cross the border daily for school.
“It also means that the speed of deportation is fast. If you are a Mexican national, you are deported by sundown. That is fast.” Community-Based Organization, San Diego
“If there’s a border patrol out there, there is a lot of panic and distress it does trigger.” Health Provider, San Diego
“…families that cross the border…they have that set of stress about crossing every day–is there going to be a day where they close the borders? …that kind of like constant worry and threat…” Health Provider, San Diego
Strengthening cross-sector partnerships and collaborations. Providers described a range of new cross-sector partnerships and relationships that have developed in recent years to provide more coordinated and integrated services to meet families’ needs. Some examples they cited included health care and legal services partnerships, a legal services provider working with a social worker to enhance support for families, a dental health clinic adding an on-site mental health counselor, and a legal services provider hiring a psychologist. Providers stressed that building on existing organizational strengths and capacities and existing partnerships or collaborations helps prevent duplication of efforts. They noted that public-private partnerships can be particularly effective since supportive local agencies can facilitate access to funding and communicate needs to the state, and community-based organizations have strong connections with the community. In San Diego, providers pointed to development of the rapid response network—a coalition of human rights and service organizations, attorneys, and community leaders—as key to supporting the community response, which has included creating a new shelter and providing health care and other services to asylum-seekers. Providers further noted that the rapid response network has facilitated the ability of local legal services providers to coordinate and prioritize their legal support to families, which has contributed to more efficient and effective use of funds.
“I think that we clearly need more social workers on staff, but I think…the work of our attorneys is way more effective having me on staff there…I am the plan person who educates providers, guardians, parents…to help build bridges between the barriers that are ongoing related to whether it’s health or other immigration issues.” Legal Services Provider, San Francisco Bay Area
“I do think that if it wasn’t for building this cross-sector, multi-disciplinary, multi-agency network…we wouldn’t have been able to do some of the good things that we’ve been able to do, not just on the sheltering side but on the improving access to legal services side.” Legal Services Provider, San Diego
Expanding capacity in other sectors to screen for and address mental health needs. As noted, one of the key challenges identified by providers and families is lack of sufficient mental health services to meet family needs. To help address this gap, some providers in other sectors have expanded their focus on and capacity to address mental health needs. For example, one provider described participating in a training for health care providers, including primary care providers and pediatricians, to provide mental health screenings and basic mental health treatment as part of their scope of care. It was noted that expanding health care providers’ ability to provide mental health screenings and treatment increases access to care for families and frees up capacity of behavioral health providers to address more complex and severe cases. Providers also reported that a growing number of teachers and staff in schools are being trained to screen for and identify mental health needs and link families to services. Further, providers pointed to cross-sector training in how to provide trauma-informed care and recognizing a broad scope of services as mental health care, including indigenous forms of healing and community support groups, as strategies to help address mental health needs.
“…one opportunity would be for the medical community—primary care, pediatricians, family practice doctors—to think about broadening scope of practice to include basic mental health services. I think it unburdens our mental health pipeline so that the psychiatrists, psychologists can treat some of the more complicated conditions.” Health Provider, San Francisco Bay Area
“…a lot of our healing mechanisms are different and so we… we talk about herbal healing, we talk about history, storytelling—that’s how we heal. And, so how can we collaborate with Western and then indigenous forms of healing….” Family Services Provider, San Francisco Bay Area
“…we have provider training sessions where we bring in our legal advocacy units to help them to see and to maybe learn how to question or ask questions in a way that’s a little more culturally sensitive or impactful.” Health Provider, San Diego
Enhancing services and supports in schools. Providers described a number of ways schools have responded to growing fears and uncertainties among families. For example, some schools have added signage and messaging designed to create a safe and welcoming space and trained staff on how to respond if enforcement agents come on-site or if a student reports detention of a family member. Providers also indicated that teachers and staff in schools are increasingly recognizing stressors and factors that may be causing students to be late or tired and responding to these issues by linking students to mental health and other services rather than punishing them. Providers pointed to movement within some schools to offer more services “inside” (i.e. school-based clinics) rather than referring students out to services since having services available on-site reduces barriers to care. However, they recognized that schools face financial and resource constraints that limit their ability to expand their services.
“We have not been successful referring students offsite to mental health services. So, as a result, we keep bringing more mental health right into the [school] clinic because they will come to the clinic, but they won’t go offsite….” Health Provider, San Diego
“The other component that we are working with…is really building out mental health services and supports to our schools. …how do we provide trainings to teachers to identify depression, identify anxiety and how do we react and what resources do we have in place?” Educator, San Diego
“…we can’t educate our students if we’re not addressing the nonacademic barriers to their academic success. So our role has increasingly expanded to understanding what are those barriers to students being in school, staying in school, thriving in school, and making sure that we are partnering, if not directly resourcing our work to address their needs.” Educator, San Francisco Bay Area
“All of our schools have been trained and are prepared to respond to ICE activity at the school, which generally wouldn’t happen, but if a family member or a student comes and says that a family member has been detained, our schools are prepared in addressing that….” Educator, San Francisco Bay Area
Identifying trusted individuals and organizations. Amid growing fears and uncertainties, providers and families noted that families trust few individuals and organizations. They indicated that churches and schools remain key trusted resources and described how clergy and faith leaders have assumed new roles helping families respond to and navigate different experiences, including detention or deportation of a family member. They recognized that health care providers and schools also serve as trusted resources for families, although, in some cases, families feel wary about sharing information about their family’s immigration status with their health care provider or children’s school.
“…we have to be on school campuses, we have to be in community clinics, we have to have better partnerships with the churches. We have to do more home visiting because of people’s fears and also who we employ is very, very important.” Family Services Provider, San Francisco Bay Area
“…people come to congregations when they feel unsafe. They come not just wanting prayer and healing spaces, but wanting to be led and accompanied really through the navigation of whether to deportation, whether it’s a health scare, whatever is happening in their life.” Community-Based Organization, San Diego
Increasing support for staff in service organizations. Given the growing intensity and stress associated with serving immigrant families, providers reported it has become increasingly important to provide support to staff in service organizations. For example, some have implemented wellness initiatives and are providing counseling support for staff. Providers also described challenges retaining staff, particularly in high-cost areas, and some indicated they are focusing on increasing wages and enhancing equity in organizational leadership to increase retention.
“…the organization was no longer saying we give you permission to focus on self-care but we’re building self-care into the fabric of what it means to work here.” Legal Services Provider, San Francisco Bay Area
“We got a bilingual, bicultural therapist to…do some work with our staff around vicarious trauma and compassion burnout…” Legal Services, San Diego
“One thing that we’ve done is we created a wellness strategy internally. We’re sort of in the nascent stages of that, but we’re looking at equity across the organization, increasing to living wage for own staff.” Legal Services Provider, San Francisco Bay Area
State and local policies and leaders supporting families and providers. Providers and families described how certain state and local policies have underpinned the community response. For example, they noted that state and local sanctuary policies help families feel safe in their local communities and policies that protect people’s privacy and minimize requested information can facilitate access to services. Providers also explained how state and local leaders have taken supportive actions. For example, they noted that Governor Gavin Newsom has supported the community through symbolic actions, such as visiting the border, as well as through direct actions, by increasing state funding for services. Providers in San Diego described how leadership by a local council member was instrumental for establishing the new shelter for asylum-seeking families.
“I live in California. I can go wherever here, and I feel protected because, thank God, we have people who support us and we are a sanctuary city, and that comforts me.” Parent, San Francisco Bay Area
“…we have more protection and inclusion in funding…in local governments to send a message to migrants that their work is appreciated and that they’re equal members of our communities.” Local Official, San Francisco Bay Area
“…and noting that our city and county don’t have any funding for the legal services, the state has really been the government agency that has stepped up.” Legal Services Provider, San Diego
Continued development of cross-sector partnerships and collaborations. Looking ahead, providers suggested building on networks and collaborations to expand integrated support for families. They noted that this entails identifying mechanisms and resources to make partnerships and collaborations sustainable over time and continuing to identify systems and structures to facilitate referrals and connections across sectors. For example, one provider suggested creating multi-sector resource centers that could serve as a central point to direct resources and for families to obtain a diverse range of services. Another suggestion was to expand training of community workers, such as promotoras and community health workers, to provide a broader array of multi-sector supports and linkages.
“…the model of intervention has to be a wraparound model. It has to be a comprehensive set of services that wraps around rather than siloed service…” Family Services Provider, San Francisco Bay Area
“…but my big dream is that we combine it…and we serve as a gateway to primary care…and a gateway to mental health care, to legal support for families that need it.” Health Provider, San Francisco Bay Area
“But being able to be armed to talk about food, mental health, immigration… I think it’s too fragmented. I would like to see funding to bring together a group of disseminators.” Legal Services Provider, San Diego
Addressing gaps in mental health and legal services. Providers highlighted the need to implement long-term strategies to expand the supply of mental health providers and immigration attorneys, particularly those that can provide linguistically and appropriate care. In the short-term, they pointed to strategies such as creating inventories of available services within a local area to assist with linking families to assistance, expanding capacity in other sectors to conduct basic mental health screenings and treatment, and incorporating more mental health services into schools. Providers also noted that, as border policies continue to evolve, they are examining how to provide legal representation to people being required to wait on the other side of the border.
“So I would say, as an immigration attorney, that funding for legal services is critical. Building up the…army of immigration attorneys. …it’s a most complex area of the law, and it’s changing by the minute.” Legal Services Provider, San Diego
“We’re having a hard time attracting bilingual immigration attorneys. We’re having a hard time attracting bilingual mental health providers, social workers, etc. …so how can we partner with universities to nurture those leaders of the future? How can we boost the sector so that it becomes attractive to future professionals and then how do we also sustain funding beyond one year cycles or two year cycles?” Family Services Provider, San Francisco Bay Area
“…we need an inventory of mental health care providers across the Bay Area so we can support families through system navigation and reaching and accessing those programs.” Family Services Provider, San Francisco Bay Area
“…it’s really important to start thinking creatively on how legal representation is going to look like for those who are waiting on the other side of the border for months. And how they’re going to be able to access those services before they get to court….” Legal Services Provider, San Diego
Meeting increased demands on non-profit organizations and local resources. As family needs have evolved and increased, providers noted that non-profits have stepped in to meet new challenges and fill gaps, often without readily available funding. They further noted that, although there have been increases in funding for some services, funding often is tied to direct services, leaving non-profits without resources to support infrastructure development or operating costs. They suggested that flexible funding that meets organizations’ evolving needs, including resources to support infrastructure development and operating costs, would help in sustaining their ability to serve families. Providers also emphasized that local government is facing new demands, including responding to needs of new migrants and increased use of local resources and services as families disenroll from public programs.
“…Our biggest challenge right now in this institution is space. We could get two million dollars tomorrow and I have nowhere to sit attorneys.” Family Services Provider, San Francisco Bay Area
“…it was all nonprofits and the two community clinics — responded right away [to meet the needs of migrant families] and they put their mobile units there and provided healthcare consistently. They did it without any funding.” Health Provider, San Diego
“We have seen a great number of people disenrolled in programs for which they are eligible… This does translate to greater burdens on our nonprofit community and our CBOs, but also on local government to cover all the gaps.” Local Official, San Francisco Bay Area
Maintaining access to health care to prevent erosion of progress advancing health. Providers described how families are increasingly turning to informal support services as they disenroll from public programs. They stressed that maintaining families’ access to health care despite their disenrollment from programs would help prevent erosion of progress achieved advancing health through the state’s earlier coverage initiatives, such as its Medi-Cal expansion to pregnant women and children regardless of immigration status. Providers also noted that the state will likely face challenges implementing its new Medi-Cal expansion to young undocumented immigrant adults due to families’ fears about participating in public programs. They suggested that continuing education and messaging in the community could help promote enrollment and minimize disenrollment due to fears, but recognized that overcoming fears is challenging in the current environment.
“Our main concern is always to mitigate any kind of further damage, like direct damage. Like a child doesn’t have milk because their mom can’t afford when they could be getting it with WIC. Or a mom’s not taking her child who has a fever to General Hospital because she’s afraid that ICE is going to catch her….” Family Services Provider, San Francisco Bay Area
“…we’ve mobilized our informal food safety net, so when a family says they’re not as interested in CalFresh, I’ll move on to talking about our food bank…So really trying to talk about making it…two lanes instead of one…” Health Provider, San Francisco Bay Area
Addressing shifting demographics and growing needs in underserved areas. Providers indicated that communities have emerging language needs, for example among a growing Mayan community, for whom they do not have sufficient language resources to meet. They also discussed how the displacement of families due to continually increasing housing and living costs has resulted in a growing number of families living in areas with a dearth of services to meet their needs.
“Economically at baseline, it’s always been hard to live here. I’ve never known a time when our families haven’t been struggling, but I would say now many families have in our area have moved …we’ve had a huge exodus of families….” Health Provider, San Francisco Bay Area
“We have a multitude of different cultures coming in and at some point you know we’ve had families that were nodding their heads responding as yes, and we would ask another question and find out that’s a whole different dialect.” Health Provider, San Diego
“…the landscape and the picture of who we’re serving and what that means is very different than I think many of even our service providers and certainly our educators are accustomed to.” Educator, San Francisco Bay Area
Continuing to educate and inform families and service providers about policy changes. Families and providers said it is difficult to stay up-to-date on and understand continually evolving policies. They want more access to information about changing policies and their rights. Providers pointed to the ongoing need to educate staff in various organizations (e.g., health care providers, hospitals, schools, etc.) about their rights and how to respond if immigration agents come on site as well as to equip service providers with tools and information to communicate with families. In San Diego, providers stressed that legal analysis to provide increased clarity on how federal border enforcement authorities interact with state laws and health-related rules and rights would be helpful for health care providers.
“…there’s a lot of confusion and a lot of rumors around these things and we do a certain amount to try to convince them or to tell them that what is going to be safe or not; and the bottom line is we often don’t have a good answer for that. We have what we think is the current law today…but it is a little bit touch and go and things are changing….” Health Provider, San Francisco Bay Area
“What kind of resources, what kind of people do we bring in, what kind of training do we have to put in place so we can support the needs of our communities? It’s a challenging environment, internally as well as externally.” Health Provider, San Diego
Utilizing data to document needs and impacts of policy changes. Providers pointed to the need for more local and disaggregated data to understand different population needs and how the shifting legal and policy environment is affecting groups. They noted that non-profits generate data but often lack capacity to analyze it and suggested that community-based organizations can collaborate with universities or other research organizations to enhance analytic capacity. They emphasized that when community-based organizations engage in these types of partnerships, they have an opportunity to identify return benefits they might realize from engaging in the research—for example, one organization was able to increase screenings for patients through participation in a research project. They also emphasized the value of utilizing a community-based framework for research that allows community-based organizations to serve as equal partners in the research.
“…we have made a strategic decision that we will only engage in participatory research that has a return for us—to the community.” Family Services Provider, San Francisco Bay Area
Recognizing the role of philanthropy, state and local leaders, and communications strategies to address needs and frame public discussion. Providers suggested it is helpful for funders to recognize the full cost of projects by taking into account operations and administrative costs of grantees. They indicated that some funders are shifting toward multi-year operating grants to allow for more flexibility and responsiveness among grantees. Providers pointed to a number of areas where funding could be directed beyond direct services, including community building, communication strategies, data collection and research, and transnational work across the border. It was also noted that having a funding collaborative focused on issues affecting immigrant families facilitates a coordinated philanthropic response. Providers also pointed to the role state leaders can play in framing public discussion of immigration issues and supporting efforts to address family needs and fill service gaps moving forward. They also suggested that it will be important to continue to foster leadership development within the affected communities and discussed the value of focusing on the strengths and resiliency of immigrant families. They suggested incorporating voices from directly impacted groups into communications strategies and noted that funders could support these efforts through funding for ethnic and social media.
“There’s been a shift in the foundation world it seems to move towards multiple year funding…it means I don’t have to be reapplying every year for the same grant and I can focus more of my time on policy advocacy and strengthening our programs…” Family Services Provider, San Francisco Bay Area
“…So thinking about, how do you lift people up? …we have many needs and we have many things that we need help with, but you also have assets in the community. Don’t forget the assets and the voices and the stories, because data will inform planning, but it’s those human stories that will move people to action.” Local Official, San Francisco Bay Area
In sum, the findings from these roundtables, interviews, and focus groups illustrate that the shifting policy and political environment has substantially increased fears and uncertainty among immigrant families. As described by providers and families, these fears are having broad negative effects on families’ daily lives and health and well-being and increasing pressures on local organizations and communities. The San Francisco Bay Area and San Diego communities have responded to growing family needs in multiple ways, including developing cross-sector partnerships and relationships, expanding the focus on and capacity to provide mental health care in other sectors, enhancing services and supports in schools, identifying trusted individuals and organizations, and increasing support for staff in service organizations. Providers and families also indicated that state and local leaders and policies have underpinned the community response.
Providers identified a range of priorities to sustain and enhance support for families looking ahead, including continued development of cross-sector partnerships and collaborations; addressing gaps in mental health and legal services; meeting increased demands on non-profit organizations and local resources; maintaining access to health care; addressing shifting demographics and growing needs in underserved areas; educating and informing families and service providers about ongoing policy changes; increasing access to data; and developing philanthropic approaches that respond to evolving needs. They also pointed to the importance of messages that focuses on the strengths, resiliency, and benefits of immigrant families for their communities and the nation as priorities moving forward. As the ongoing national debate over immigration policy and enforcement continues, these discussions with service providers and families illustrate the effect it is having on immigrants themselves and the organizations that serve them.
Methods
The Kaiser Family Foundation, working with Donna Cohen Ross and PerryUndem Research/Communication, conducted policy roundtable discussions and structured individual interviews with individuals from organizations across various sectors serving immigrant families in the Bay Area and San Diego. We conducted two policy roundtable discussions in July 2019, one in San Francisco with 19 participants and one in San Diego with 16 participants, as well as 11 individual interviews in June 2019. Participants in the roundtable discussions and interviews included health and behavioral health providers, educators, legal services providers, community-based organizations, faith-based organizations, funders, and local officials who we identified as key service providers for immigrant families in the community.
In addition, we conducted two focus groups with Spanish-speaking parents in immigrant families in the Bay Area and San Diego in June 2019. Local focus group facilities recruited participants, and PerryUndem Research/Communication moderated the groups in Spanish. There were eight participants in each group. Participants included low-income adults with family incomes at or below 250% FPL who were parents or guardians of a minor in the household and who had at least one immediate family member in the household who was a noncitizen.
| The authors thank Blue Shield of California Foundation for its support for this work. They also extend their deep appreciation to the families and organizations who shared their time and experiences to inform this brief. |