KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Health Affairs Article: Comparing the Assets of Uninsured Households to Cost Sharing Under High Deductible Health Plans
Relatively few uninsured households have enough financial assets to cover the cost-sharing in consumer-driven health plans tied to Health Savings Accounts (HSAs), according to this study by Kaiser Family Foundation researchers published as a Health Affairs Web Exclusive on April 15, 2008.
Consumer-driven plans generally require enrollees to pay for most health-care expenses themselves until they reach the plan’s relatively high deductible. At that point, the plan begins to pay at least some of the costs of additional health-care expenses. The plans also permit tax-free contributions to savings accounts that can be used to cover out-of-pocket costs, with unused funds rolling over from one year to the next.
The new study analyzes the asset levels of households with two or more uninsured members in 2004 and compares it to the range of cost-sharing features in HSA-qualified health plans in that year. Assets are an important consideration because low- and moderate-income families may not have adequate income to pay the potentially high cost-sharing under these policies and would have to dip into any savings to pay their bills.
This Medicare Part D Data Spotlight examines the variation in 2008 Part D plan coverage, cost sharing and utilization management tools for the 10 prescriptions most commonly used by Medicare beneficiaries, including treatments for cholesterol, cardiovascular health, osteoporosis, dementia, gastrointestinal reflux and ulcers.
It looks at data from the 47 stand-alone prescription drug plans available nationwide in 2008. This data spotlight is one in a series analyzing key aspects of the 2008 Medicare Part D prescription drug plan choices. The analysis was conducted jointed by Jack Hoadley of Georgetown University, Elizabeth Hargrave and Katie Merrell of NORC at the University of Chicago, and Juliette Cubanski of the Kaiser Family Foundation.
This Medicare Part D Data Spotlight focuses on the availability of drug plans for beneficiaries receiving the Part D low-income subsidy in 2008 and changes since 2006.
It looks at data from the 47 stand-alone prescription drug plans available nationwide in 2008. This is one in a series analyzing key aspects of the 2008 Medicare Part D prescription drug plan choices. The analysis was conducted jointed by Jack Hoadley of Georgetown University, Elizabeth Hargrave of NORC at the University of Chicago, and Juliette Cubanski of the Kaiser Family Foundation.
This synthesis of key findings from analysis presented in a series of eight Medicare Part D 2008 Data Spotlights describes key features of stand-alone prescription drug plans offered in 2008 and trends since 2006.
The synthesis covers a range of topics, including premiums, the coverage gap, benefit design, cost sharing, specialty tiers, formularies, utilization management, the top 10 brand-name prescription drugs, and the availability of low-income subsidy plans. The analysis was conducted jointed by Jack Hoadley of Georgetown University, Elizabeth Hargrave of NORC at the University of Chicago, and Juliette Cubanski and Tricia Neuman of the Kaiser Family Foundation.
The National ADAP Monitoring Project Annual Report provides the latest data on state AIDS Drug Assistance Programs (ADAPs). ADAPs, part of the Ryan White Program, provide HIV medications to low-income people with HIV/AIDS who have limited or no prescription drug coverage. ADAPs operate in all 50 states, the District of Columbia, and U.S. territories and associated jurisdictions.
The report, the 12th in an annual series, was released by the Kaiser Family Foundation and the National Alliance of State and Territorial AIDS Directors (NASTAD) at a policy forum on April 8, 2008.
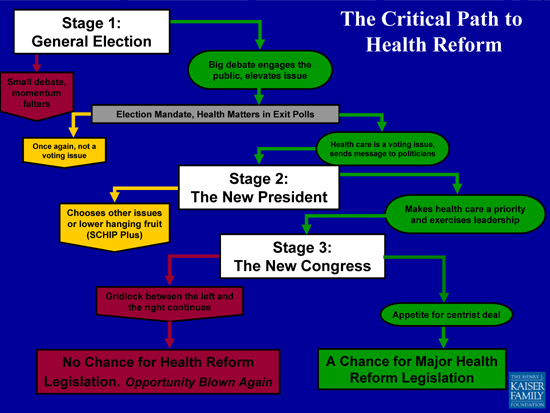
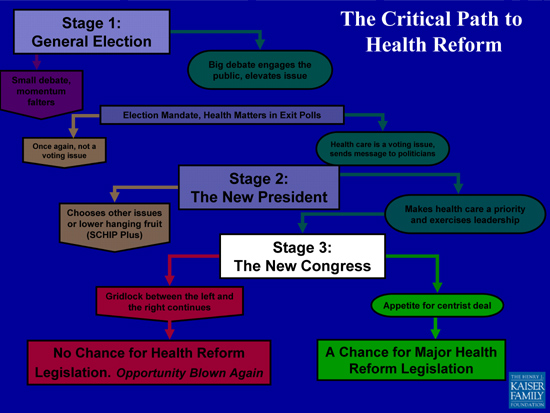
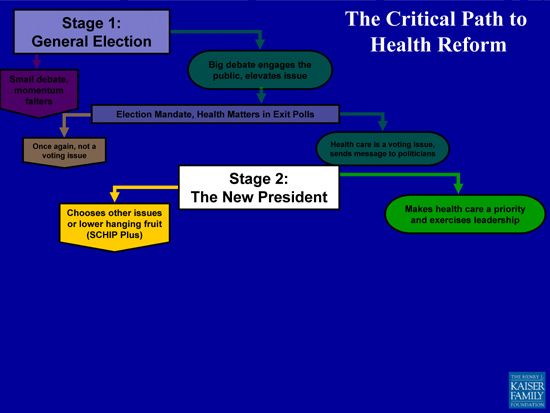
Finally, it bears mentioning for organizations like Kaiser that do research and analysis and are committed to public education on complex health policy issues, that the kinds of activities that will be most useful will vary depending on what stage we are at on the “critical path.” At this early stage, education about the problems and the issues is critically important to establish the facts and dispel myths. What are the public’s concerns and experiences with the health care system? How do insecurities about health care affordability and coverage relate to growing economic worries? This is also the time to develop policy ideas that could be a basis for broader agreement in 2009. Later, when we get to a legislative debate in 2009, the details of health reform plans will become all important, as will the challenge of analyzing them and explaining what different plans and proposals could mean for average people. But the main point is simply this: We are only at the beginning of this debate, indeed the real debate has not yet begun, and there are key decision points — in effect different mini health reform debates — still to come.
If there is a debate in the new Congress in 2009 about comprehensive health reform legislation, a major question is: Will there be an appetite for a bipartisan, centrist deal? No matter who is in the White House or what the margins are in the Senate, it is very unlikely that the deep divisions about how to reform our health care system between left and right will have been transformed enough to support passage of legislation that will entirely satisfy either liberals or conservatives. Health care’s ideological divide is too deep. It will therefore take a compromise somewhere in the middle, shading left if there is a Democratic president or more right if there is a Republican one, to get legislation passed, but there will be a centrist compromise or no compromise at all on health reform in 2009. Of course other challenges will present themselves as well. Health care’s famous interest groups will become active in the process. And the challenge of paying for expanding coverage, always a major hurdle, will be exacerbated by the pressure to balance the budget in what may still be a shaky or recovering economy.
Will the new president make health a top early priority and exercise real leadership on the issue? One of the big lessons of the health reform debate of the early nineties is that the Congress needs to be fully engaged in the process early on. Nevertheless, for health reform legislation to stand a chance, a new President will have to make it an early and top priority and exercise real leadership. Given the history of failure on health reform and the chances of failure again, making comprehensive health reform a top early priority will not be a small decision for any President. No doubt advisors will argue both sides of the question. A tempting easier road, even for Democrats who have made universal coverage a cornerstone of their election campaigns, will be to attend to unfinished business first, and lead with a reauthorization of the SCHIP program, plus perhaps some additional incremental reforms. Let’s call this the SCHIP Plus scenario. In a world where progress has been hard to come by in health reform, this result will be satisfying to many. However, it will not be perceived as having accomplished comprehensive reform by many more (whether of a Democratic or Republican flavor). An SCHIP Plus strategy could be pursued as a first in a series of steps on health reform and might in fact play out that way. But there is only so much time in a presidential term before the focus on reelection takes over and only so much energy to devote to health care issues over other priorities.