Medicare Part D Enrollment, Premiums, and Cost Sharing in 2026
Introduction
The Medicare Part D program provides an outpatient prescription drug benefit to 56 million older adults and people with long-term disabilities in Medicare who enroll in private plans, including stand-alone prescription drug plans (PDPs) to supplement traditional Medicare and Medicare Advantage prescription drug plans (MA-PDs) that include drug coverage and other Medicare-covered benefits. This brief analyzes Medicare Part D enrollment and costs in 2026 and trends over time, based on data from the Centers for Medicare & Medicaid Services (CMS).
Highlights for 2026
- Enrollment in Medicare Part D stand-alone PDPs increased for 2026 to 24.9 million, up from 23.2 million in 2025, mainly due to growth in employer group plans. But Medicare Advantage continues to be the primary source of Part D drug coverage for people with Medicare, with 31.4 million enrollees. Enrollment in the Part D Low-Income Subsidy (LIS) increased in 2026, from 13.1 million to 13.6 million, offsetting a similarly sized decrease in enrollment in 2025.
- Overall, Part D enrollment is concentrated in a handful of large plan sponsors, with the top 5 firms (UnitedHealth, Humana, Centene, CVS Health, and Health Care Service Corporation) covering nearly three-fourths of Part D enrollees. Centene is the top firm in the PDP market, with more than one-third (35%) of all PDP enrollees, while UnitedHealth is the top firm in the MA-PD market, with 26% of all MA-PD enrollees.
- The temporary Part D premium stabilization demonstration for stand-alone PDPs continues to work as intended to help stabilize PDP premiums. The average monthly premium for Part D coverage decreased for PDPs in 2026 (from $39 to $36), while increasing modestly for MA-PDs (from $7 to $8). The average monthly premium for Part D coverage in 2026 is more than 4 times higher for PDPs than for MA-PDs, with most MA-PD enrollees in zero-premium plans, which reflects the ability of Medicare Advantage plan sponsors to reduce their Part D premiums using rebates that are not available to PDP sponsors. Nearly 8 in 10 MA-PD enrollees without low-income subsidies pay no monthly premium for Part D coverage in 2026 (not including premiums they may pay for medical benefits), compared to around 3 in 10 PDP enrollees in zero-premium plans.
- Cost pressures for Part D plan sponsors under the redesigned Part D benefit are likely one factor in higher costs being passed along to both PDP and MA-PD enrollees in the form of higher deductibles and greater use of coinsurance. In 2026, most Part D enrollees pay either the standard $615 Part D deductible or a partial amount. The share of MA-PD enrollees in a plan that charges a deductible for drug coverage in 2026 is 82%, a sharp increase from 2024 when 23% of MA-PD enrollees were in a plan charging a drug deductible. The share of Part D enrollees in a plan charging no drug deductible decreased between 2025 and 2026, from 40% to 18% among MA-PD enrollees and from 15% to 4% among PDP enrollees.
- Median cost-sharing amounts for covered drugs across different formulary tiers are the same or similar in PDPs and MA-PDs in 2026, but there is some variation in the share of PDPs and MA-PDs charging flat dollar copayments versus coinsurance (a percentage of the drug’s price) for preferred brands and non-preferred drugs. Virtually all PDP enrollees pay coinsurance for preferred brands (97%) and non-preferred drugs (100%), compared to 56% and 89% of MA-PD enrollees. But the use of coinsurance has increased on MA-PD formularies compared to 2025, when 27% of MA-PD enrollees faced coinsurance for preferred brands and 56% faced coinsurance for non-preferred drugs.
Part D Enrollment
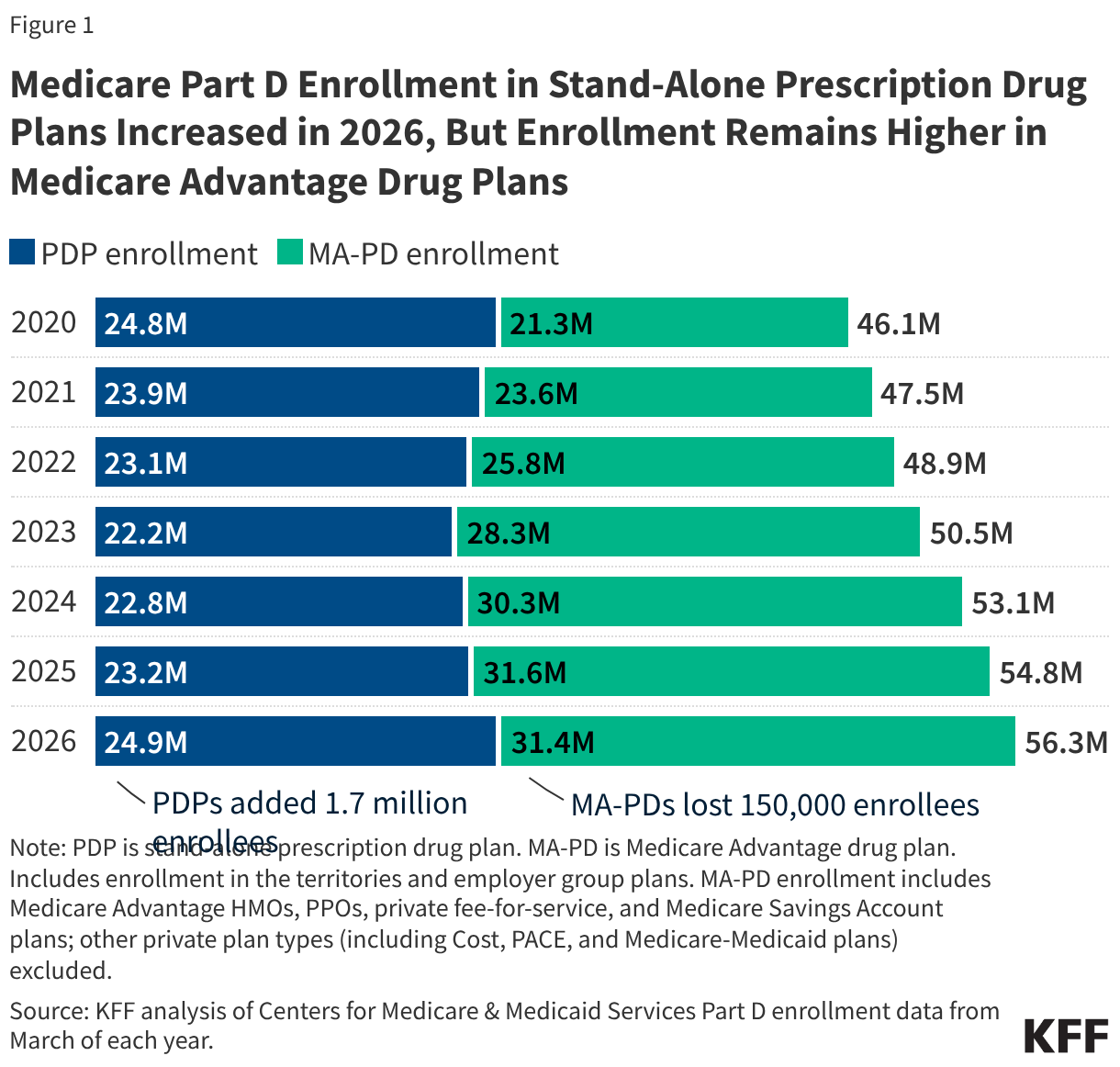
The number of Medicare Part D enrollees in stand-alone prescription drug plans increased in 2026, but enrollment remains higher in Medicare Advantage drug plans
More than half (56%) of all Part D enrollees in 2026 are in Medicare Advantage drug plans, continuing a trend of increasing enrollment in Medicare Advantage (Figure 1). At the same time, the overall number of PDP enrollees increased for the third year in a row and is up by 1.7 million since 2025, with most of the growth in employer group PDPs. The modest reduction in overall MA-PD enrollment between 2025 and 2026 (from 31.6 million to 31.4 million) reflects a shift in enrollment among employer group plan enrollees from group MA-PD plans to group MA-only plans with separate PDPs. (These enrollment trends are discussed in greater details in a separate KFF analysis, “Analyzing Changes in Medicare Part D Enrollment for 2026.”)
An even larger share of Part D Low-Income Subsidy enrollees is in Medicare Advantage drug plans than Part D enrollees overall
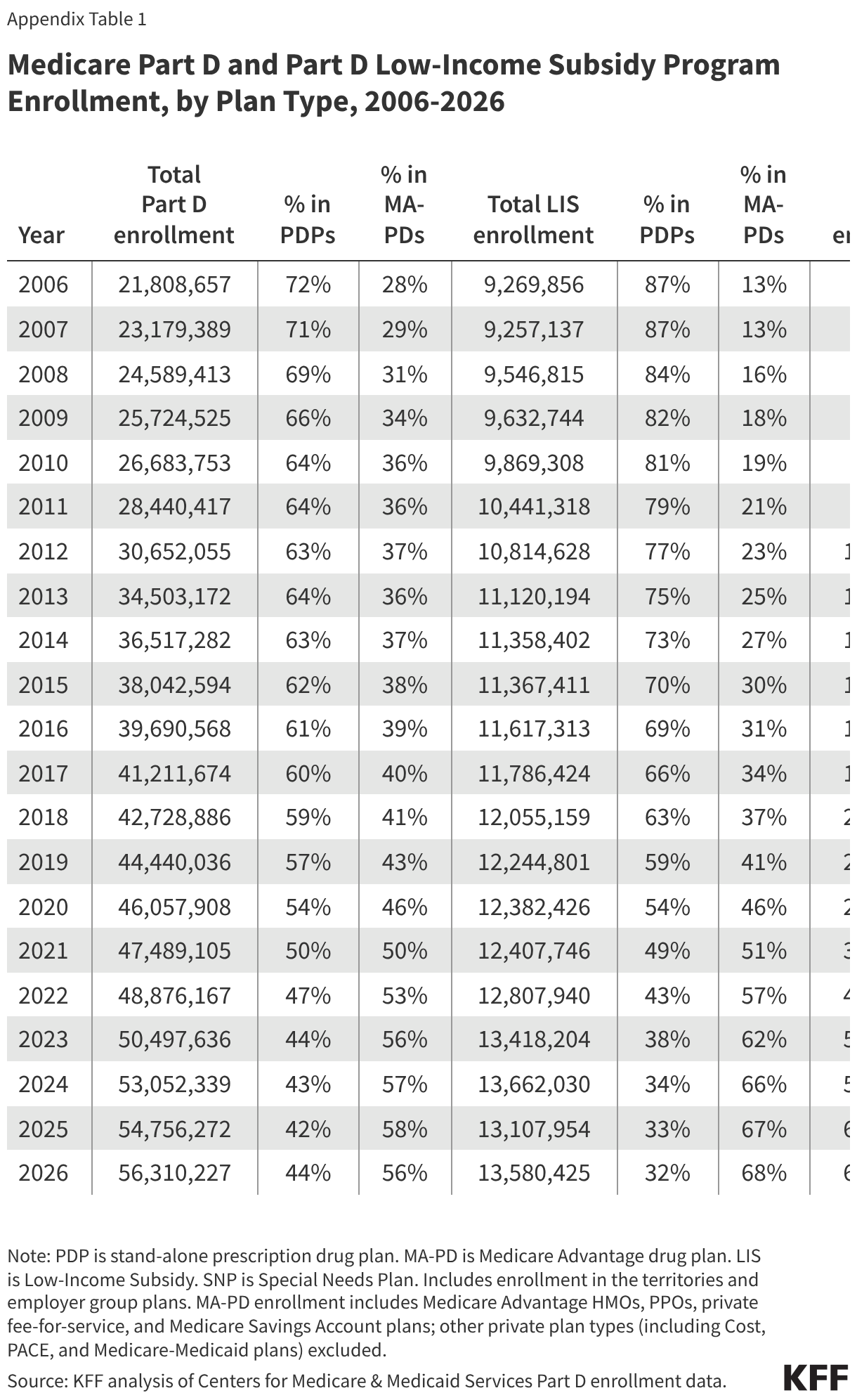
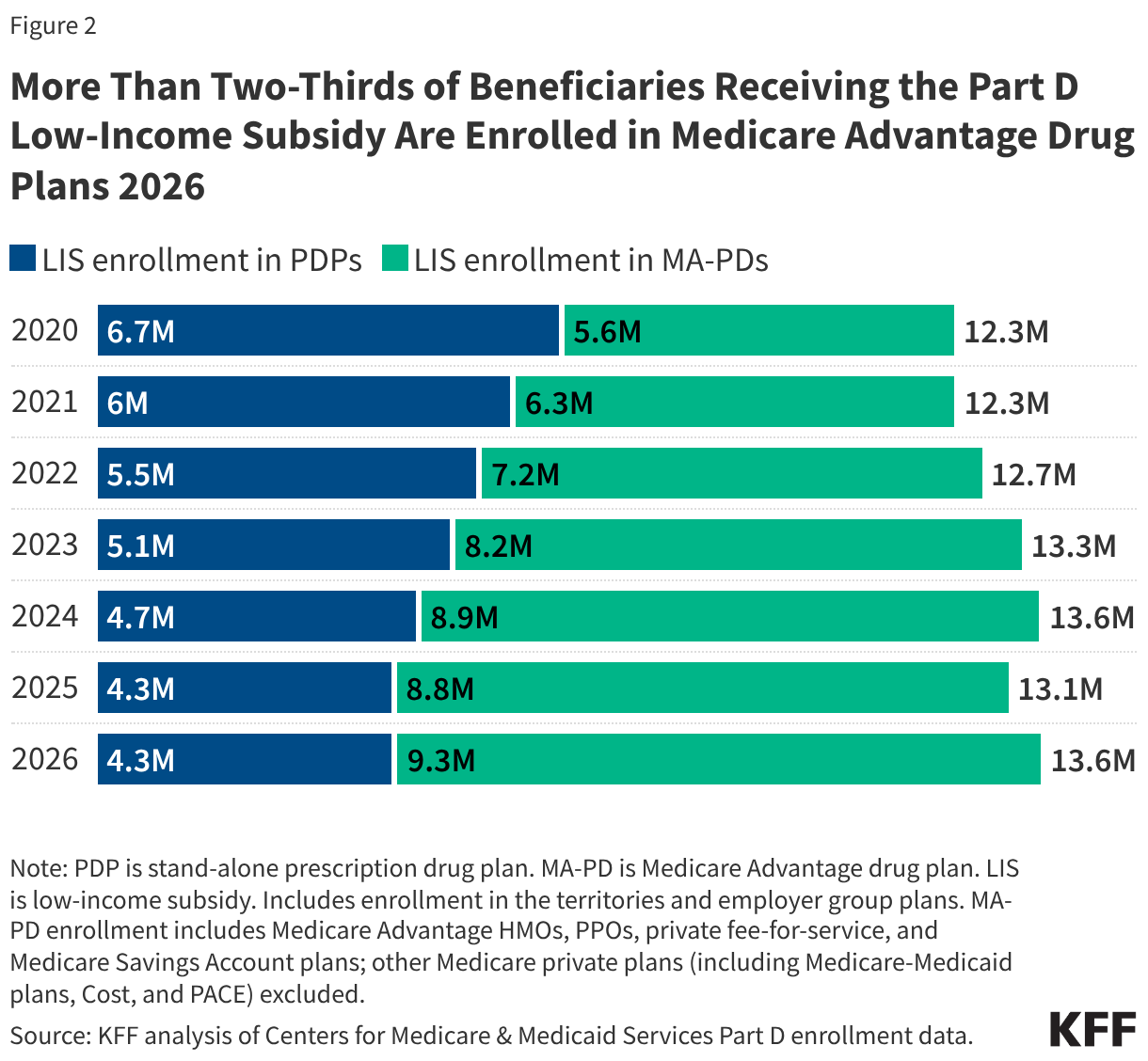
The Medicare Part D Low-Income Subsidy (LIS) provides financial assistance with drug plan premiums and cost sharing for low-income enrollees. More than two-thirds (68%) of LIS enrollees—9.3 million out of 13.6 million—are enrolled in Medicare Advantage drug plans in 2026 (Figure 2). Nearly half of all LIS enrollees (6.7 million or 49%) are enrolled in Medicare Advantage Special Needs Plans (SNPs), nearly all of whom are in plans designed specifically for dual-eligible individuals (Appendix Table 1). LIS enrollment in MA-PDs has increased over time in tandem with overall enrollment of Medicare beneficiaries in Medicare Advantage plans generally and SNPs specifically.
Part D LIS enrollment overall increased modestly by 0.5 million in 2026, from 13.1 million to 13.6 million, offsetting a similar decrease in LIS enrollment in 2025. This decrease was likely due to Medicaid disenrollment among dual-eligible individuals that stemmed from the unwinding of the Medicaid continuous enrollment provision in place during the COVID-19 pandemic. Medicare beneficiaries with Medicaid coverage (dual-eligible individuals) automatically qualify for LIS, meaning a loss of Medicaid coverage would lead to a loss in LIS unless eligible individuals apply and enroll separately.
Five firms cover nearly three-fourths of Part D enrollees in 2026
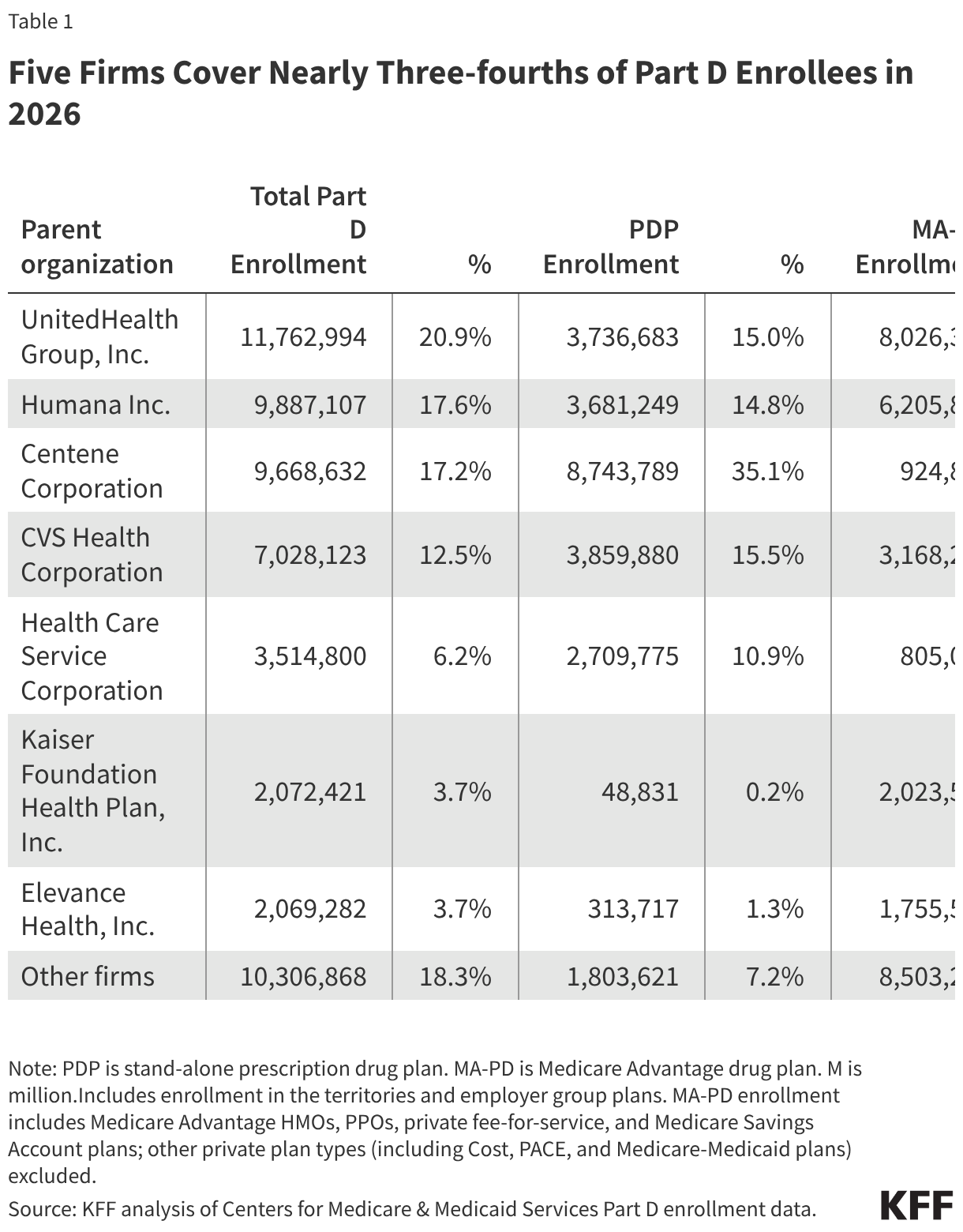
Part D enrollment is concentrated in a handful of top plan sponsors, with 5 firms covering 74% of all Part D enrollees in 2026, or 41.9 million out of 56.3 million enrollees (Table 1). One in 5 enrollees (11.8 million) are in Part D plans sponsored by UnitedHealth, including both stand-alone PDPs and MA-PDs, followed by Humana and Centene, each with around 10 million enrollees across both types of Part D plans.
Centene is the top firm in the PDP market, with more than one-third (35%) of all PDP enrollees, followed by CVS Health (16%) and UnitedHealth (15%). UnitedHealth is the top firm in the MA-PD market, with 26% of all MA-PD enrollees, followed by Humana (20%) and CVS Health (10%).
More than 6 million PDP enrollees—one-third of the total—are enrolled in the lowest-premium PDP in 2026
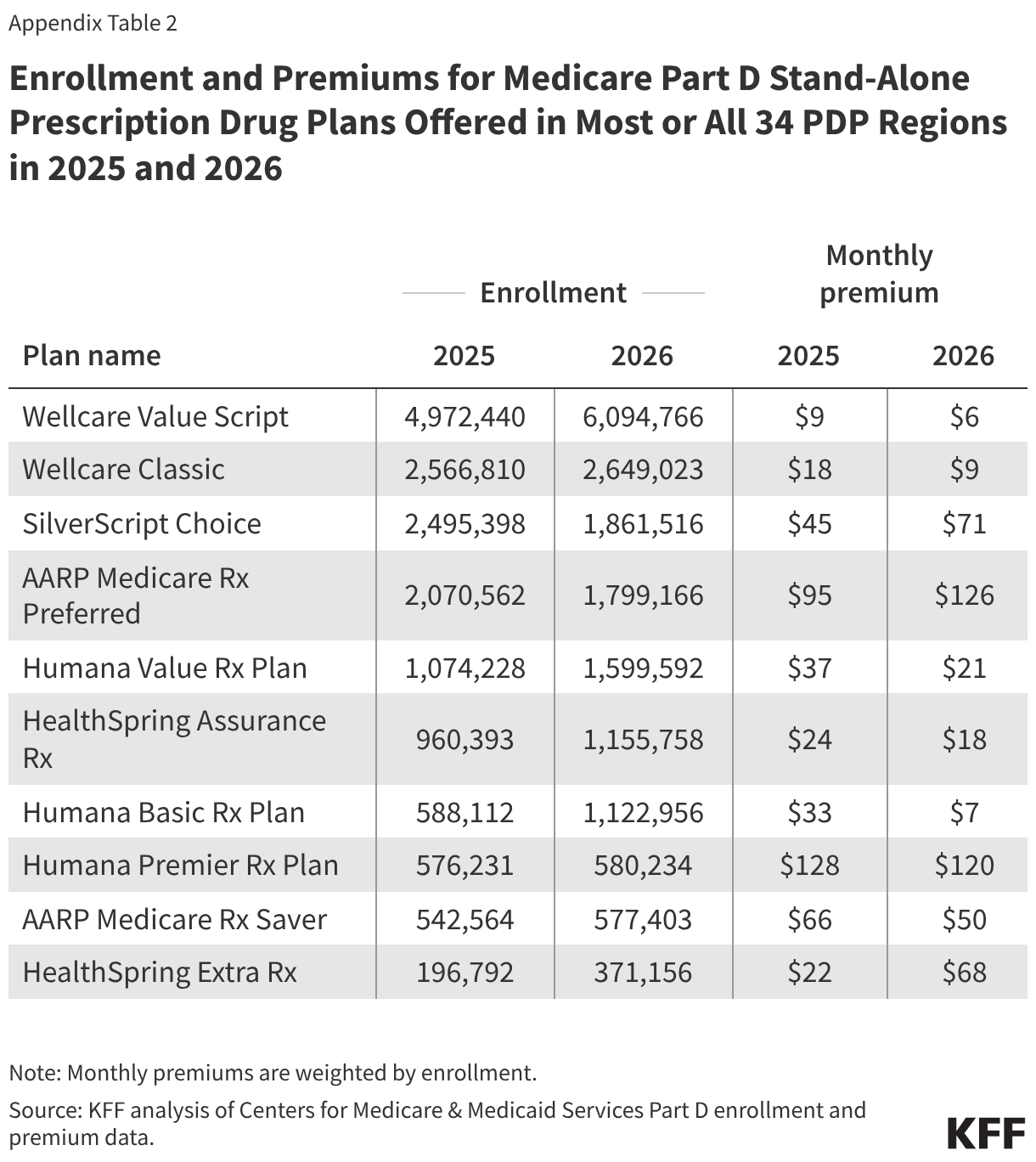
Among the 10 national PDPs available in 2026, the PDP with the lowest average monthly premium—Wellcare Value Script, at just under $6—has attracted a substantial share of all PDP enrollees, with one-third of PDP enrollees in non-group plans (6.1 million) (Figure 3). Between 2025 and 2026, Wellcare Value Script gained 1.1 million PDP enrollees, as several other national PDPs experienced smaller increases and some PDPs lost enrollment (Appendix Table 2).
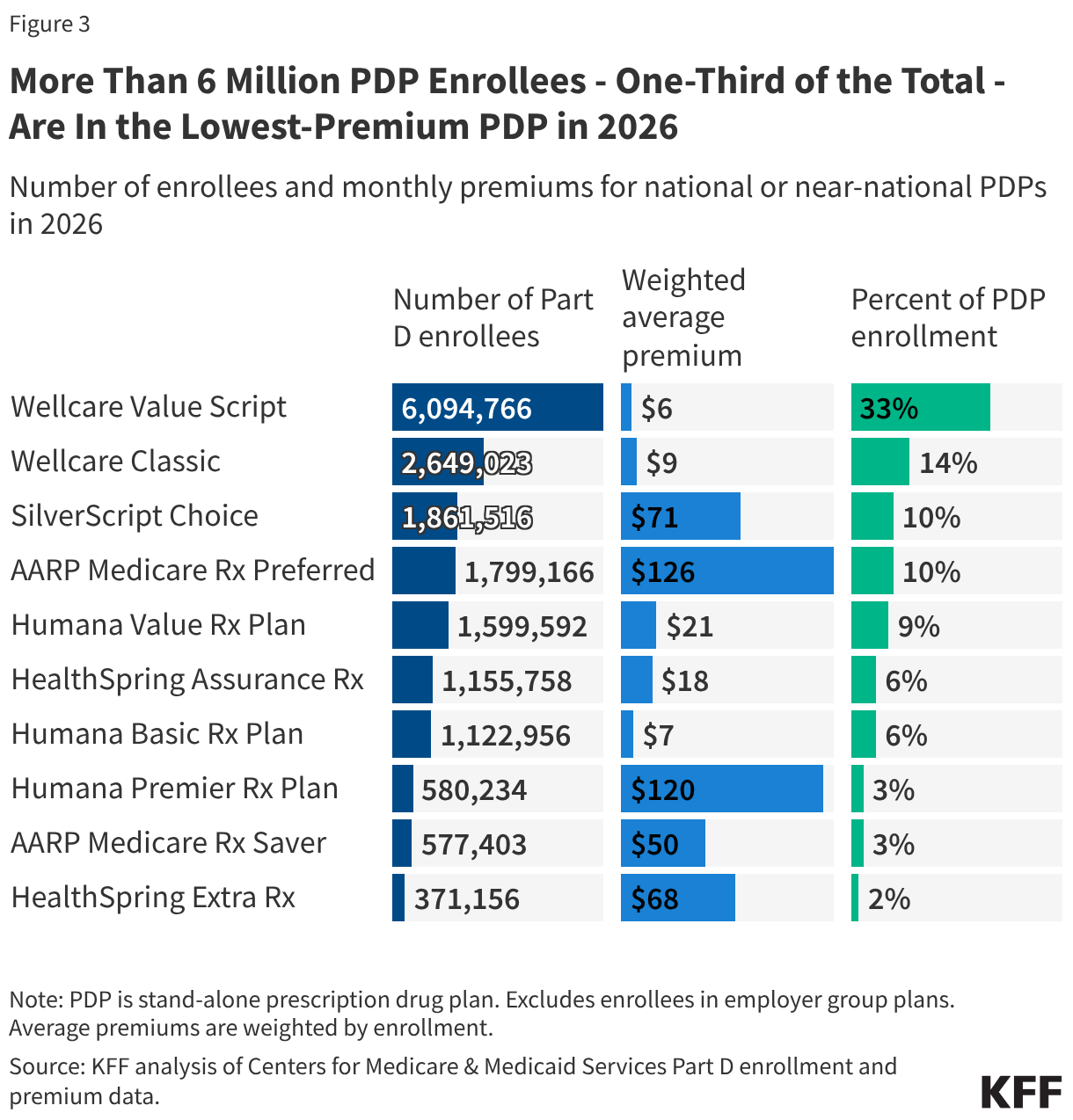
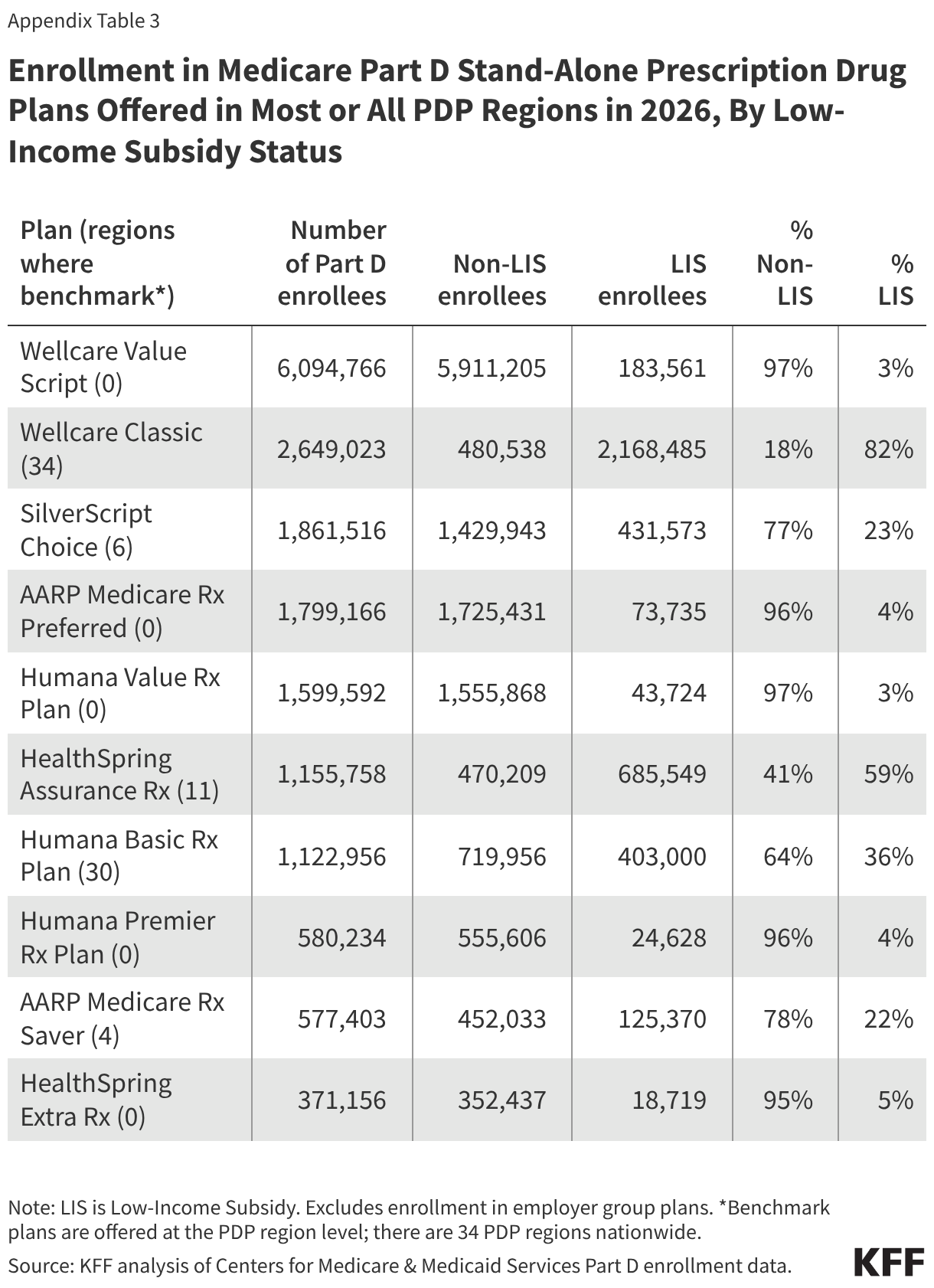
The number and share of LIS enrollees in national PDPs vary considerably, which is related to the fact that only 1 of these 10 plans (Wellcare Classic) is a benchmark PDP in all 34 PDP regions, meaning it is available to all Part D enrollees receiving LIS for no premium (4 other PDPs are benchmark plans in some but not all regions) (Appendix Table 3). A majority of all enrollees in Wellcare Classic (82% or 2.2 million) are receiving LIS, along with 60% of enrollees (0.7 million) in HealthSpring Assurance Rx, a benchmark plan in 11 regions, and 36% of enrollees (0.4 million) in Humana Basic Rx Plan, a benchmark plan in 30 regions. In contrast, only 3% of the 6.1 million enrollees in Wellcare Value Script are LIS enrollees; despite its low average premium, this is an enhanced PDP and therefore does not qualify to be a benchmark plan.
Overall, 14% (0.6 million) of the 4.2 million PDP enrollees receiving LIS in 2026 (excluding those in employer group plans) are enrolled in non-benchmark PDPs. LIS enrollees in non-benchmark plans are required to pay a portion of the plan’s premium for the cost of basic benefits that exceeds the LIS benchmark amount in their region or if their plan charges a premium for enhanced benefits.
Part D Premiums
The average monthly premium decreased for PDPs in 2026, but the premium for Part D coverage is still substantially higher for PDPs than for MA-PDs
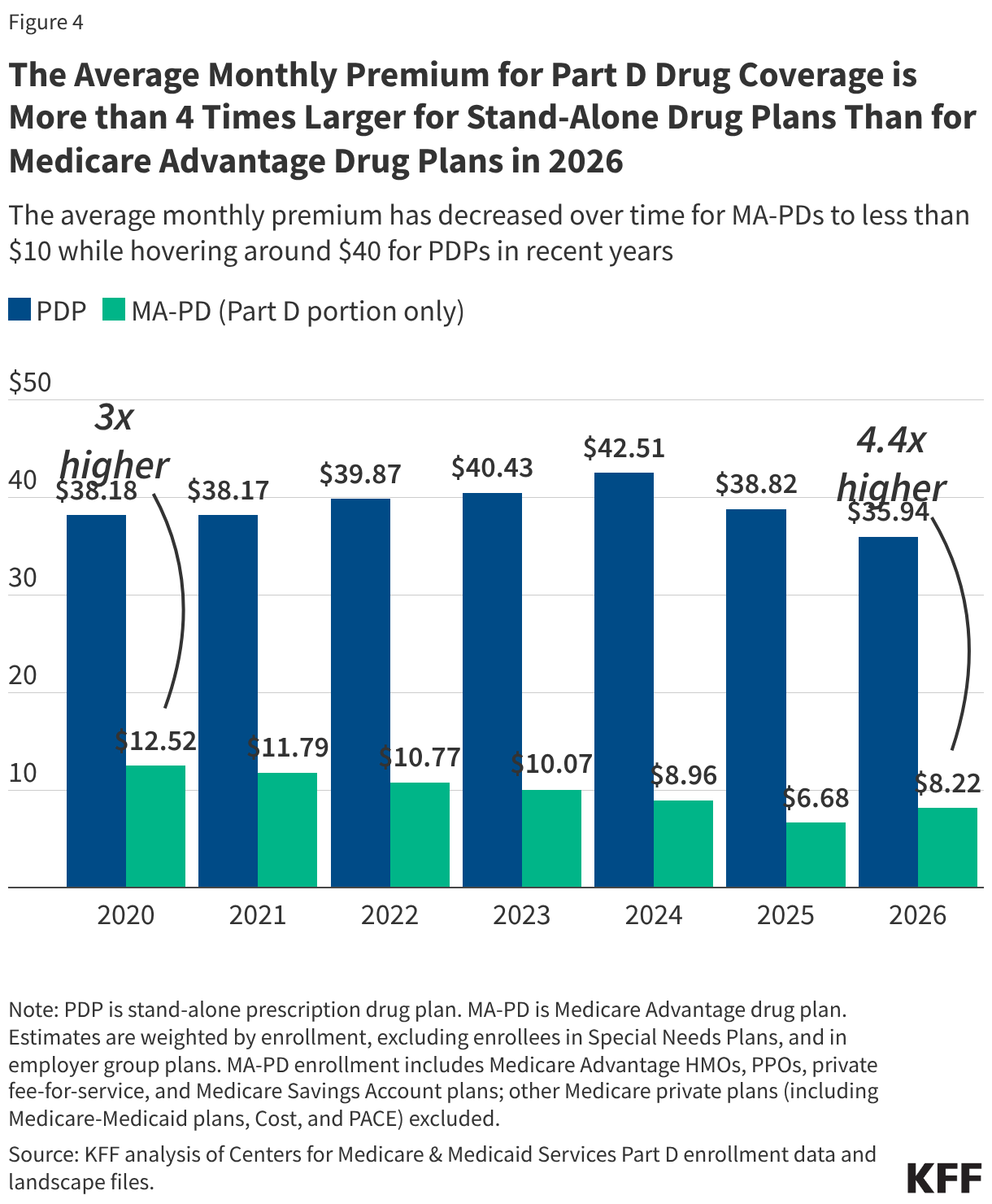
The temporary Part D premium stabilization demonstration for stand-alone PDPs established by the Biden administration in 2024 and renewed for a second year by the Trump administration in 2025 continues to work as intended to help stabilize PDP premiums, with the average monthly PDP premium decreasing 7% between 2025 and 2026, from $39 to $36. This is despite monthly premium increases in some PDPs of up to $50, the maximum increase allowed in 2026 for plans participating in the premium stabilization demonstration.
On average, PDP enrollees continue to pay substantially more each month for their Part D drug coverage than enrollees in MA-PDs. The $36 average monthly PDP premium is more than 4 times higher than the $8 average monthly premium for drug coverage in MA-PDs (weighted by enrollment) (Figure 4). (The total average premium for MA-PDs, including all Medicare-covered benefits, is $15 per month in 2026.) The weighted average MA-PD premium for Part D coverage increased modestly between 2025 and 2026 (up from $7 to $8). (These estimates are based on enrollment in March 2026 and factor in new plans for 2026, plan changes during open enrollment, and new enrollees, and therefore differ from other estimates published in a separate KFF brief, which are based on MedPAC’s projection of average monthly Part D premiums in 2026 using 2025 enrollment and not factoring in new plans, plan switching, or new enrollees.)
The average premium for drug coverage in MA-PDs is heavily weighted by zero-premium plans because MA-PD sponsors can use rebate dollars from Medicare payments to lower or eliminate their Part D premiums. Rebates to Medicare Advantage plans have tripled since 2015 and now exceed $2,600 per year per beneficiary.
Within the PDP market, average monthly premiums vary by the generosity of Part D coverage offered by a given plan—namely, whether they are basic or enhanced plans, and the amount of the drug deductible. Enhanced Part D plans offer a more generous benefit than basic plans through lower cost sharing, a lower (or no) drug deductible, or better formulary coverage. In 2026, 58% of PDP enrollees (10.8 million) are in enhanced PDPs, and they face an average monthly premium of $39, 27% higher than the average $31 premium faced by the 42% of PDP enrollees (7.8 million) in basic plans. Only 4% of PDP enrollees are in a plan charging zero deductible, but they face an average monthly premium of $127, while the 78% of PDP enrollees in a plan charging the standard $615 deductible face an average monthly premium of $22. Among MA-PD enrollees, there is considerably less variation in monthly premiums by these measures of plan generosity, which reflects both the large share of MA-PD enrollees in zero premium plans (as described below) and the fact that 94% of MA-PD enrollees are in enhanced plans.
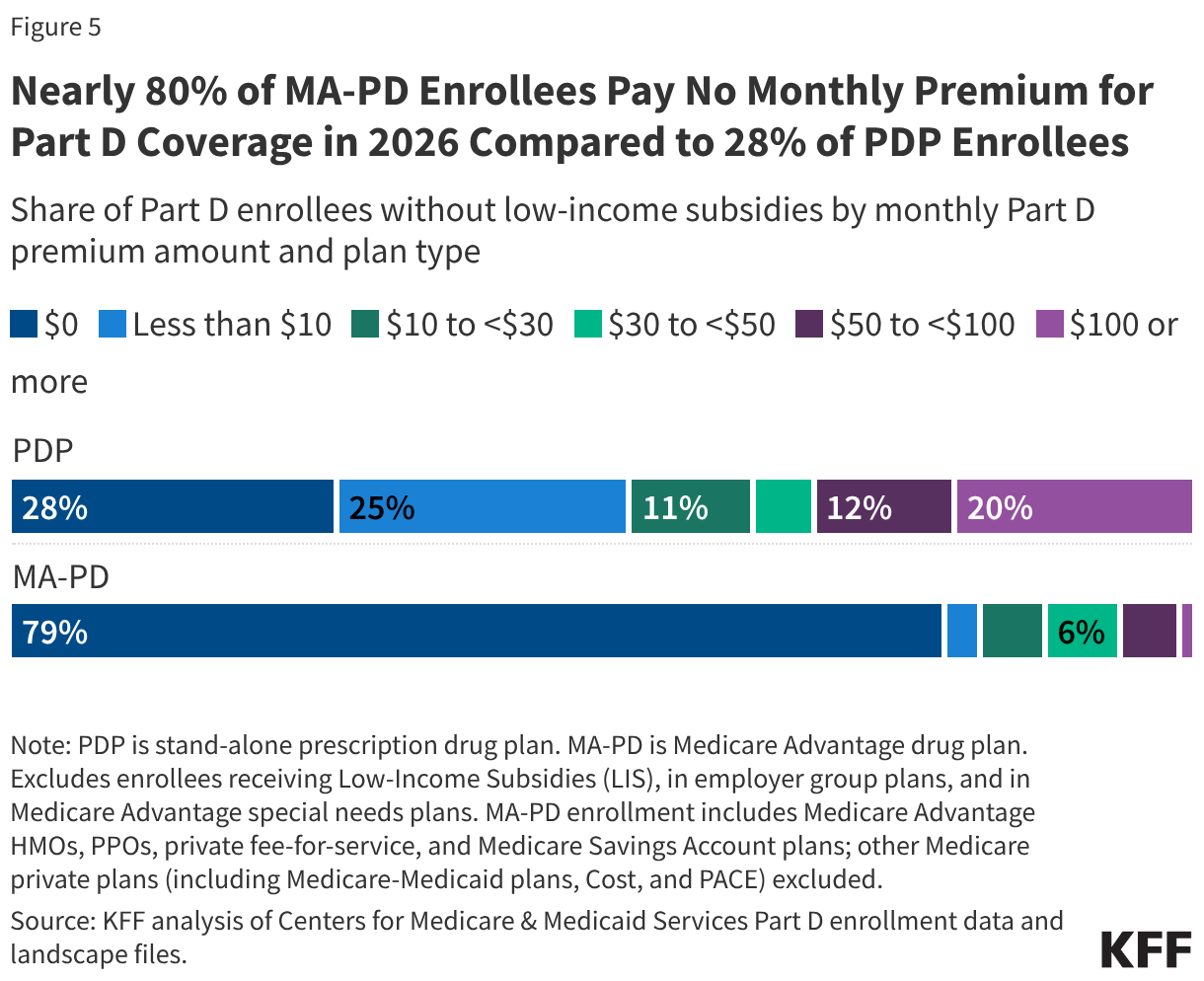
Nearly 8 in 10 MA-PD enrollees without low-income subsidies pay no monthly premium for Part D coverage, while around 3 in 10 PDP enrollees pay no premium
Nearly 80% of MA-PD enrollees without low-income subsidies (79% or 14.3 million) pay no monthly premium for Part D coverage in 2026, compared to 28% of PDP enrollees without LIS (4.0 million) (Figure 5). For the average Medicare beneficiary in 2026, 21 out of their 32 MA-PD options charge no premium for drug coverage, while 2 out of their 11 PDP options charge no premium.
Of the 4.0 million non-LIS PDP enrollees paying zero premium, 62% (2.5 million) were enrolled in Wellcare Value Script, which was available for zero premium in 14 out of 34 PDP regions, 10% (0.4 million) in Humana Basic Rx, which was available for zero premium in 21 regions, and another 10% in Humana Value Rx, available for zero premium in 5 regions.
While 79% of non-LIS MA-PD enrollees pay no premium for drug coverage, among the 21% who do, the average monthly premium for drug coverage is $40 per month. Among the 72% of PDP enrollees who pay a monthly premium, their average monthly premium is $57.
Roughly one-third of PDP enrollees without LIS (35%, or 5.1 million) pay premiums above zero but less than $30 per month, but 1 in 5 (20%, or 2.9 million) pay at least $100 per month for their Part D plan (Figure 6). In contrast, less than 1% of non-LIS MA-PD enrollees pay $100 per month or more in Part D premiums.
Out-of-Pocket Costs
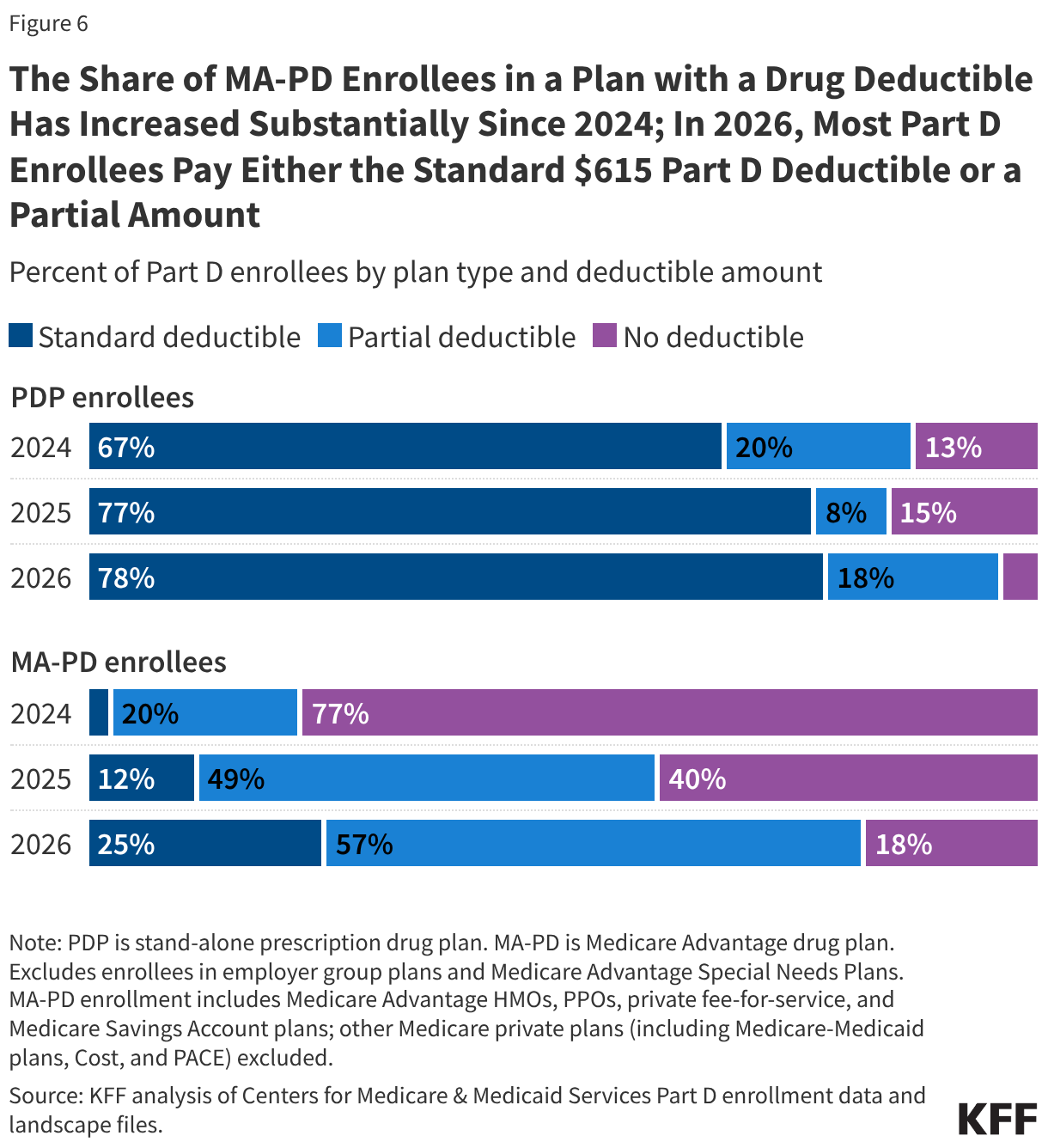
The share of MA-PD enrollees in a plan with a drug deductible has increased substantially since 2024; in 2026, most Part D enrollees pay either the standard $615 Part D deductible or a partial amount
Increasing cost pressures for Part D plan sponsors under the redesigned Part D benefit are a likely factor in higher costs being passed along to both PDP and MA-PD enrollees in the form of higher deductibles and greater use of coinsurance (as described below). Among MA-PD enrollees, 82% (16.8 million) are in a plan that charges a deductible for drug coverage in 2026 – a sharp increase from 2024 when 23% of MA-PD enrollees were in a plan charging a deductible (increasing to 60% in 2025) (Figure 6). In 2026, 25% of MA-PD enrollees are in a plan that charges the standard deductible of $615 (up from 3% in 2024 and 12% in 2025) and 57% face a partial deductible. The share of MA-PD enrollees in a plan charging no drug deductible has fallen from 77% in 2024 to 18% in 2026.
There have been comparatively fewer changes in the distribution of PDP enrollees facing different drug deductible levels since 2024. Nearly all PDP enrollees (96% or 18 million) are in a plan that charges a drug deductible in 2026, including more than three-fourths (78%) in a plan that charges the standard deductible of $615 and 18% facing a partial deductible. The share of PDP enrollees facing no drug deductible in 2026 has fallen to 4%, down from 15% in 2025 and 13% in 2024. (These estimates include Part D enrollees receiving Low-Income Subsidies, who do not pay a deductible regardless of whether their plan charges one.)
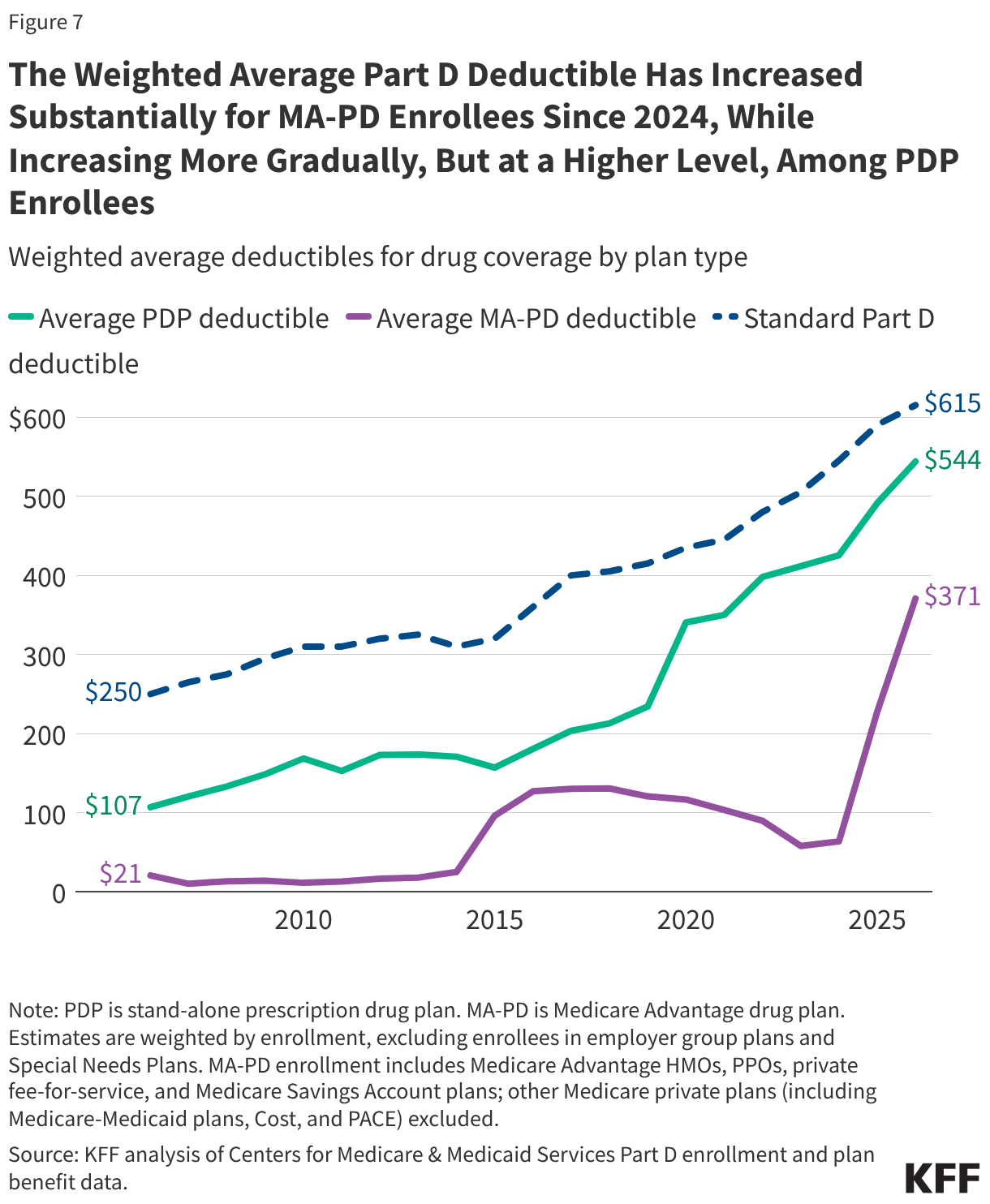
The weighted average drug deductible has increased substantially for MA-PD enrollees since 2024. In 2026, the average Part D deductible is $371 in MA-PDs, up 63% since 2025 ($228) and 481% since 2024 ($64) (Figure 7). For PDP enrollees, the weighted average Part D deductible has increased more gradually but has remained higher than the average Part D deductible for MA-PD enrollees. In 2026, the average Part D deductible is $544, up 11% since 2025 ($491) and 23% since 2024 ($425).
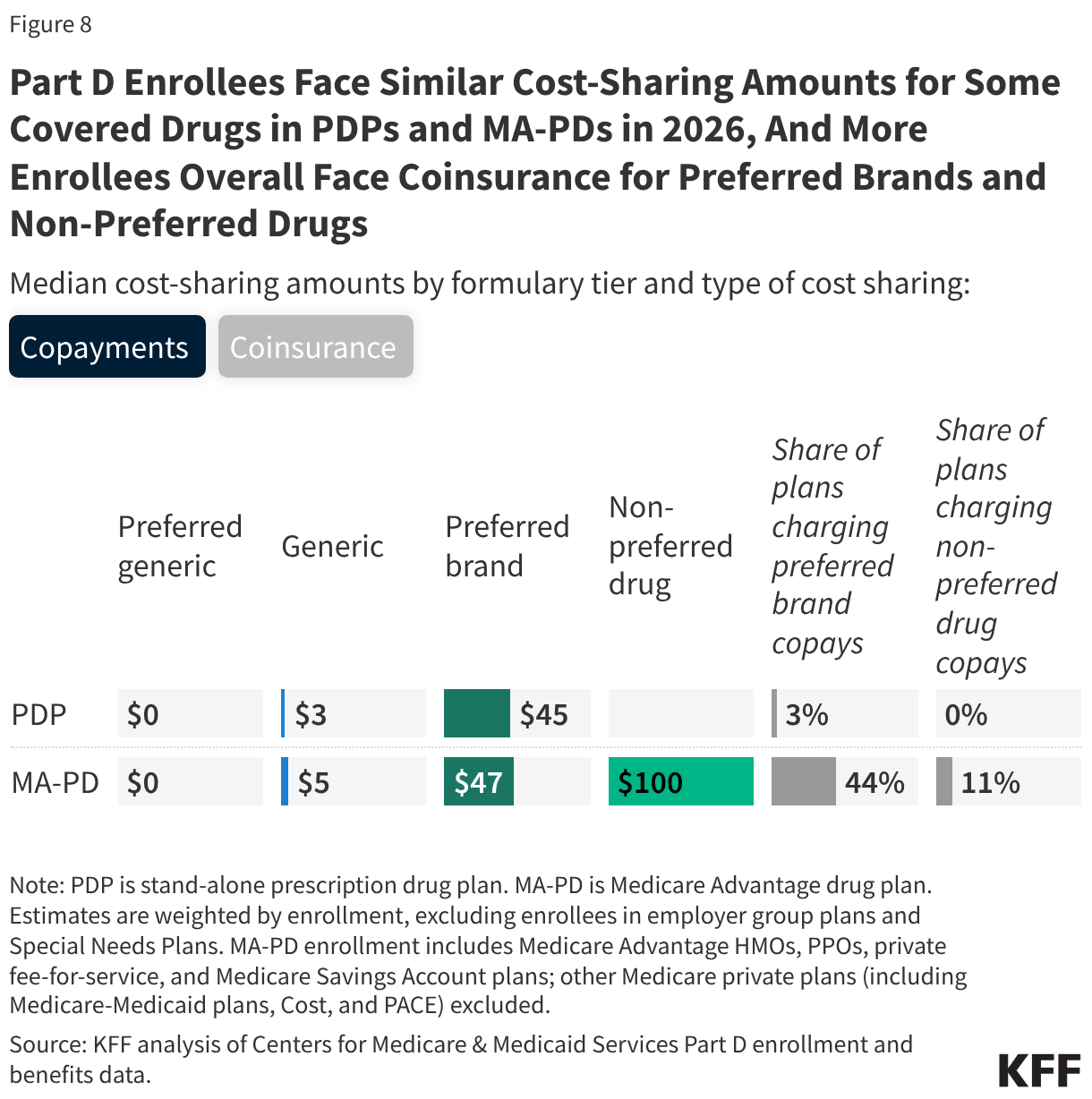
In 2026, more Part D enrollees overall face coinsurance rather than copayments for preferred brands and non-preferred drugs
As in previous years, Part D enrollees face low copayments for generic drugs and higher cost-sharing amounts for preferred brands, non-preferred drugs, and specialty drugs regardless of whether they are in PDPs or MA-PDs (Figure 8). Median cost-sharing amounts for drugs covered on preferred generic, generic, and preferred brand tiers are the same or similar in PDPs and MA-PDs, but there is some variation in the share of PDPs and MA-PDs charging flat dollar copayments versus coinsurance (a percentage of the drug’s price) for preferred brands and non-preferred drugs.
Virtually all PDP enrollees pay coinsurance for preferred brands (97%) and non-preferred drugs (100%); among MA-PD enrollees, these shares are 56% and 89%, respectively. However, these rates have increased compared to 2025, when 27% of MA-PD enrollees faced coinsurance for preferred brands and 56% faced coinsurance for non-preferred drugs. The median coinsurance rate for preferred brands is 25% in PDPs and 21% in MA-PDs, and for non-preferred drugs, 34% in PDPs and 38% in MA-PDs.
Median coinsurance for specialty tier drugs (those that cost over $950 in 2026) is higher for MA-PD enrollees than PDP enrollees—28% vs. 25%. Plans that waive some or all of the standard deductible, which most MA-PDs do, are permitted to set the specialty tier coinsurance rate above 25%.
These cost-sharing amounts apply when beneficiaries fill prescriptions in the initial coverage phase of the Part D benefit. Under a provision in the Inflation Reduction Act, beneficiaries no longer face cost sharing in the catastrophic coverage phase of the Part D benefit. In 2026, Medicare beneficiaries pay no more than $2,100 out of pocket for prescription drugs covered under Part D.
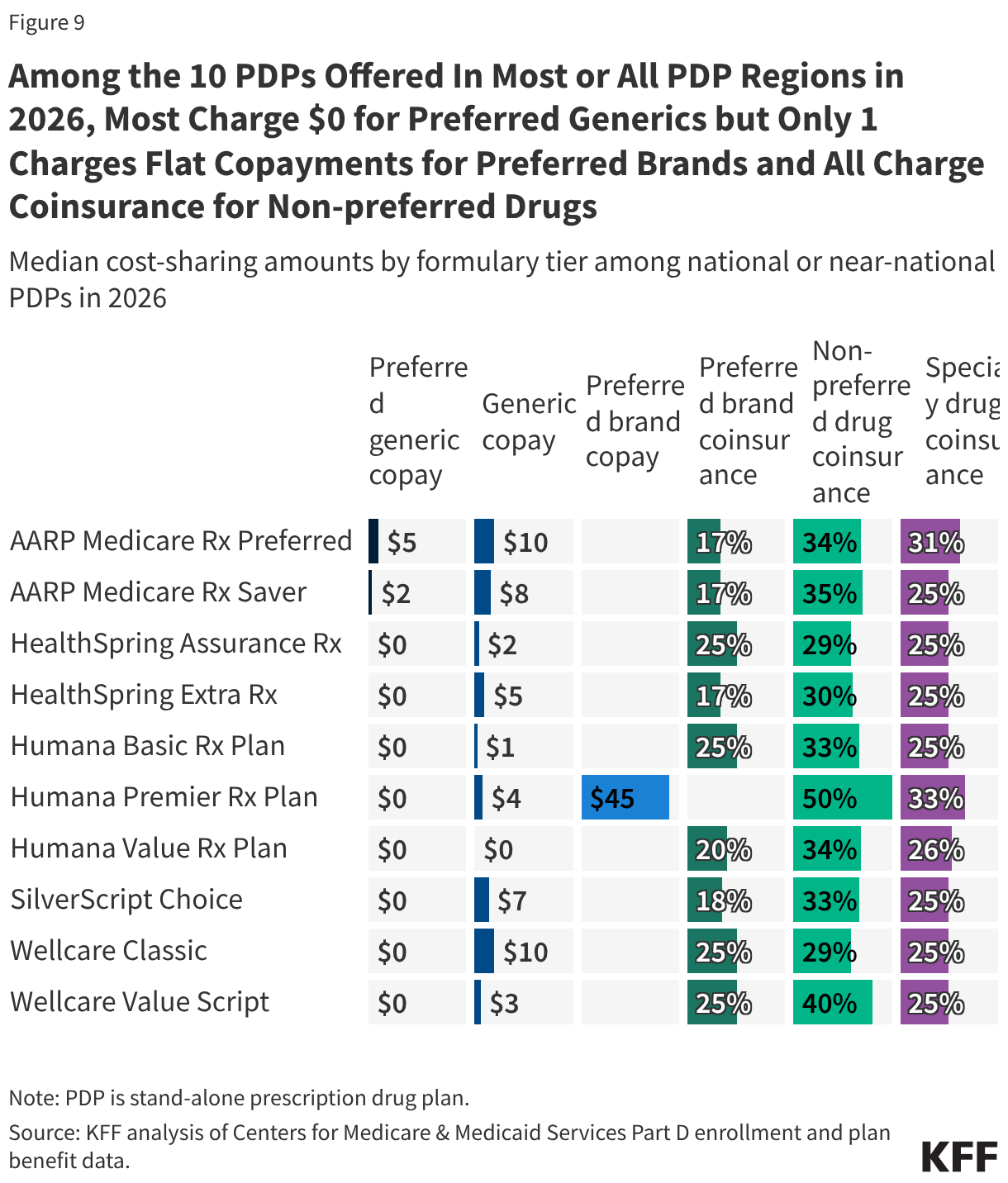
Among the 10 PDPs offered in most or all PDP regions, most charge $0 for preferred generics but only 1 PDP charges flat copayments for preferred brands and all charge coinsurance for non-preferred drugs
Part D enrollees in 8 of the 10 national or near-national PDPs face a median copayment of $0 for preferred generics, while median copays for drugs on the standard generic tier range from $0 to $10 (Figure 9). For preferred brands, 9 of the 10 PDPs charge coinsurance, with median amounts ranging from 17% to 25%, and only 1 national PDP (Humana Premier Rx) charges a copay. All 10 national or near-national PDPs charge coinsurance for non-preferred drugs, ranging from 29% to 50% at the median, and coinsurance for specialty tier drugs ranging from 25% to 33%.
Appendix