KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
A new KFF brief looks at where COVID-19 falls as a leading cause of death in the U.S. compared to similarly large and wealthy countries. The analysis finds that COVID-19 mortality rates are the third leading cause of death in the U.S., a ranking shared by only one peer country, Belgium. In several other peer countries, including Australia and Germany, COVID-19 is not close to breaking into the top 10 leading causes of death.
The brief also addresses high per capita excess deaths in the U.S. – the number of deaths exceeding what is expected in a typical year.
The analysis is available on the Peterson-KFF Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.
In this perspective published by the Washington Post, KFF Executive Vice President for Health Policy Larry Levitt explains why the popular Affordable Care Act provisions that ensure people with pre-existing conditions can access affordable health insurance can’t easily be preserved if other related provisions are overturned.
As the 2020 Election Day approaches, many candidates continue to focus on health care issues, including on the public health and economic response to COVID-19, the future of the Affordable Care Act, health care costs and abortion.
To help reporters understand and cover these issues, KFF offers independent, non-partisan policy analysis, polling and other research and has experts who can provide context, explain trade-offs and provide key data points on health care issues that may arise in the debates and broader campaign. Some key resources:
Overview
This overview slideshow compares President Trump’s record and Democratic nominee Biden’s positions across a wide range of key health issues. This JAMA Health Forum column also summarizes key differences.
This brief reviews the Trump administration’s record on a wide range of health issues.
The October KFF Health Tracking Poll assesses voters’ views of the presidential candidates on key health care issues. The KFF/Cook Political Report’s Sun Belt Voices Project polls voters in Arizona, Florida and North Carolina, three critical battleground states.
These health care snapshots provide state-specific health policy data on costs, Medicaid, Medicare, private insurance, the uninsured, women’s health, health status, and access to care.
COVID-19
This overview and detailed side-by-side compares President Trump and Democratic nominee Biden on their records, actions and proposals related to the COVID-19 pandemic.
Our September poll examines the public’s knowledge and views of the coronavirus outbreak, and their trust in public health experts and institutions, including concerns about how political pressure may affect vaccine development.
KFF President and CEO Drew Altman’s essay in The BMJ examines two fundamental policy decisions made by the Trump administration that set the U.S. on the controversial and highly criticized course it has taken on COVID-19.
This topic page highlights several pieces on how people of color have fared worse during the pandemic and also provides data on underlying health care disparities and racial inequities.
The post looks at how insurers could treat COVID as a pre-existing condition if the federal protections in the ACA were overturned as a result of a pending case before the Supreme Court.
Affordable Care Act and Coverage Expansions
This explainer examines the potential impact of the Texas v. California case, supported by the Trump administration, that aims to overturn the ACA. The U.S. Supreme Court is scheduled to hear the case on Nov. 10, a week after the election. This analysis examines key provisions of the law and how they impact nearly every American, with national, state, and public opinion data.
This analysis estimates the number and share of people by state with pre-existing conditions that would have prevented them from buying health insurance based on the underwriting practices in place in most states prior to the ACA. This post looks at variation by age, gender and in and outside metro areas.
This analysis examines the impact of expanding ACA premium subsidies as Democratic nominee Biden has proposed on the cost of Marketplace coverage.
This post looks at what we know about recent trends in health insurance coverage. This report assesses the effects of the ACA’s Medicaid expansion on coverage, access to care, state budgets, and the economy.
This brief provides key public opinion data about the public’s views and knowledge about the ACA.
Prescription Drug and Health Costs
This slideshow explains the similarities and differences among major proposals to lower prescription drug costs introduced by the Trump Administration, members of Congress, and the Biden campaign.
This explainer examines key issues regarding importation of drugs from Canada and other countries.
This brief looks at Medicare negotiation of drug prices.
This analysis estimates how often consumers receive surprise medical bills when getting emergency room and hospital care, and describes key proposals to protect consumers. This brief looks at the chance of getting an unexpected out-of-network medical bill for different health conditions, including heart attacks and mastectomies.
This slideshow captures key polling data on Americans’ views and experiences with prescription drug costs, and this data note looks at Americans’ experiences with surprise medical bills.
Abortion and Reproductive Health
This brief looks at the potential implications of the presidential election on women’s health issues, while this one summarizes four state ballot initiatives related to abortion, sex education and paid leave.
This poll explores the public’s views and knowledge about abortion and reproductive health issues, including Roe v. Wade, state-level restrictions, and family planning services.
This analysis examines the likely impact of Trump administration regulations, currently blocked by court orders, for abortion coverage in ACA marketplace plans.
This slideshow looks at the impact of state abortion policies on clinical practice.
If you have questions about any of these resources or want to talk to a KFF expert, please contact Rakesh Singh, Craig Palosky or Chris Lee for assistance.
On June 12th, the Trump Administration released a final regulation implementing Section 1557 of the Affordable Care Act, and revising an Obama era rule. In it, the administration removed explicit nondiscrimination protections based on gender identity and sexual orientation in health care. In light of a recent Supreme Court decision, and based on other legal grounds, five lawsuits are currently challenging the Trump Administration rule and blocking its implementation. If the explicit protections provided under the Obama era rule are lifted, it could be easier for health care providers to refuse to see individuals who are transgender or who do not conform to traditional sex norms.Explicit protections on the basis of sexual orientation and gender identity could have significant and lasting implications for LGBTQ people, including the estimated 1.4 million transgender adults living in the US.
This analysis seeks to better understand the experiences of transgender people in the US health care system. We examine the demographic characteristics of transgender adults ages 18 and over and their access to health care. We analyzed pooled, cross-sectional data from a subset of the 2017 and 2018 Behavioral Risk Factor Surveillance System (BRFSS). We consider adults to be transgender based on their response to survey questions and define all other adults to be cisgender.
Key Takeaway
Our analysis finds that transgender adults are more likely to be uninsured (19% vs. 12%) and report cost-related barriers to care (19% vs. 13%) than cisgender adults. Transgender adults are also more likely to be non-Hispanic Black and low income than cisgender adults (Figure 1).
Findings
DEMOGRAPHICS
Age. A much larger share of transgender adults are under age 35 (44%) than cisgender adults (27%) with one in four (25%) transgender adults under age 25 (data not shown). At the other end of the age spectrum, 16% of transgender adults are 65 years old or older, compared to 22% of cisgender adults (Figure 2).
Education. Transgender adults report fewer years of education compared to cisgender adults, holding age constant (analysis not shown). Nearly one quarter of all transgender adults (23%) have less than a high school education compared to 13% of their cisgender peers. A smaller share of transgender than cisgender adults graduated from college or technical school (15% vs. 27%, respectively).
Race/Ethnicity. While a majority of transgender and cisgender adults are white, a larger share of transgender than cisgender adults are Black (16% vs. 12%, respectively).
Annual Household Income. A larger share of transgender than cisgender adults live on lower incomes: 25% of transgender adults report an annual household income under $20,000 compared to 15% of cisgender adults, based on income reported for 2017-2018 (Figure 3). Transgender adults are more likely to report an annual income under $20,000 holding age constant (analysis not shown).
Employment Status. Among adults still in the labor force, a higher share of cisgender adults report being employed compared to transgender adults (56% vs. 48%, respectively). Nearly one in ten (9%) of transgender adults report they were unemployed from 2017-2018, a share much higher than that of cisgender adults (5%).
HEALTH STATUS, INSURANCE COVERAGE, AND ACCESS TO CARE
Health Status. Transgender adults are more likely than cisgender adults to report being in poor health (10% vs. 5%, respectively).
Lifetime Depression. Transgender adults report lifetime depression at twice the rate of cisgender adults (38% vs. 19%, respectively) (Figure 4).
Health Insurance Coverage. A larger share of transgender than cisgender adults (19% vs. 12%, respectively) report that they were uninsured over the 2017-2018 period.
Cost-Related Barriers to Care. Nearly one in five (19%) transgender adults report experiencing barriers to care due to cost, more than the share reported by cisgender adults (13%).
Personal Doctor. A similar share of transgender (22%) and cisgender (21%) adults report that they do not have a personal doctor or health care provider.
Time Since Last Checkup. A similar share of transgender and cisgender adults report having gone more than one year since their last checkup (25% vs. 24%, respectively).
Discussion
Our analysis finds that transgender people differ from cisgender adults in a number of ways that could impact their health care, as a backdrop for understanding the potential implications of lifting anti-discrimination protections. Transgender adults are younger, less educated, have lower incomes, are in poorer health, with higher rates of lifetime depression, and are less likely to be white, employed and have health insurance. Transgender adults are also more likely than cisgender adults to experience barriers to care due to cost. In other ways, barriers to care faced by transgender people are similar to those faced by cisgender people.
Past research shows that younger adults report lower incomes, and that people of color are also more likely to be uninsured, which may explain some of the differences in demographic characteristics and insurance coverage. However, it has also been suggested that demographic differences alone do not completely explain why transgender adults experience more difficulty in accessing care in certain circumstances than their cisgender peers do.
Our analysis suggests that transgender adults experience barriers to care even with the Section 1557 health care protections based on gender identity in place. Removing these protections may exacerbate already-existing access problems, which may lead to increased barriers to care among these adults, at a time when access to health care is critical.
This work was supported in part by the Elton John AIDS Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods
This brief analyzes pooled, cross-sectional data from the 2017 and 2018 Behavioral Risk Factor Surveillance System (BRFSS). BRFSS is an ongoing, state-based, random-digit-dialed telephone survey of non-institutionalized civilian adults living in the community. The BRFSS core questionnaire does not include questions about sexual orientation or gender identity; however, both the 2017 and 2018 BRFSS offer an optional, unified module on sexual orientation and gender identity. In each survey wave, select states opted to add the sexual orientation and gender identity module to the survey (2017: 27 states and Guam; 2018: 28 states and Guam).
In the subset of states which administered the optional module, adults were asked if they considered themselves to be transgender. We defined adults as transgender if they considered themselves to be: 1) transgender female; 2) transgender male; or 3) transgender, gender non-conforming. Of adults who identify as transgender adults in this analysis, 23% (n=433) identified as gender non-conforming. We considered adults who did not identify as transgender to be cisgender. Our study population includes 1,872 transgender adults and 430,817 cisgender adults in the subset of states which opted to administer the module in 2017 and 2018. Our analysis excluded adults who responded that they did not know or were not sure (n=1,684) or adults who refused to answer (n=3,184).
We examined differences in demographics and access to care through questions administered in the core BRFSS questionnaire. Our estimates of transgender and cisgender adults use the BRFSS survey weights to account for the complex sampling design, and our analysis excludes missing values. Missing is included as a valid category for education (.3%), race/ethnicity (1.6%), employment status (.9%) and income (15.4%). We did not provide estimates of sex assigned at birth as severalstudies have shown that measurement of sex assigned at birth using BRFSS significantly misclassifies transgender adults. All reported differences in demographics and access to care between transgender and cisgender adults are statistically significant. Results from all statistical tests were reported with p< .05 considered statistically significant.
A new KFF issue brief examines the implications of a Supreme Court with a solid conservative majority. Two abortion cases have pending requests for Supreme Court review: Dobbs v. Jackson Women’s Health Organization and FDA v. ACOG. If the Court chooses to take these cases, abortion laws and who can legally challenge them could be affected in major ways, including:
The option for doctors and clinics to challenge laws regulating abortion on behalf of their patients could be eliminated, and only patients themselves could challenge the laws.
The constitutional right to an abortion established in Roe v. Wade could be overturned allowing states to ban or further restrict abortion.
The legal standard for evaluating abortion laws’ constitutionality could be changed.
The confirmation process for Judge Amy Coney Barrett, President Donald J. Trump’s appointment to fill the Supreme Court seat previously held by Justice Ruth Bader Ginsburg, began last week with the fate of the Affordable Care Act (ACA) firmly at the center of the hearings. With the Supreme Court set to hear arguments in California v. Texas only days after the election, the nomination of Judge Barret has placed heightened scrutiny on what President Trump’s administration would do to continue the ACA’s protections for people with pre-existing conditions if the Supreme Court invalidates the law.
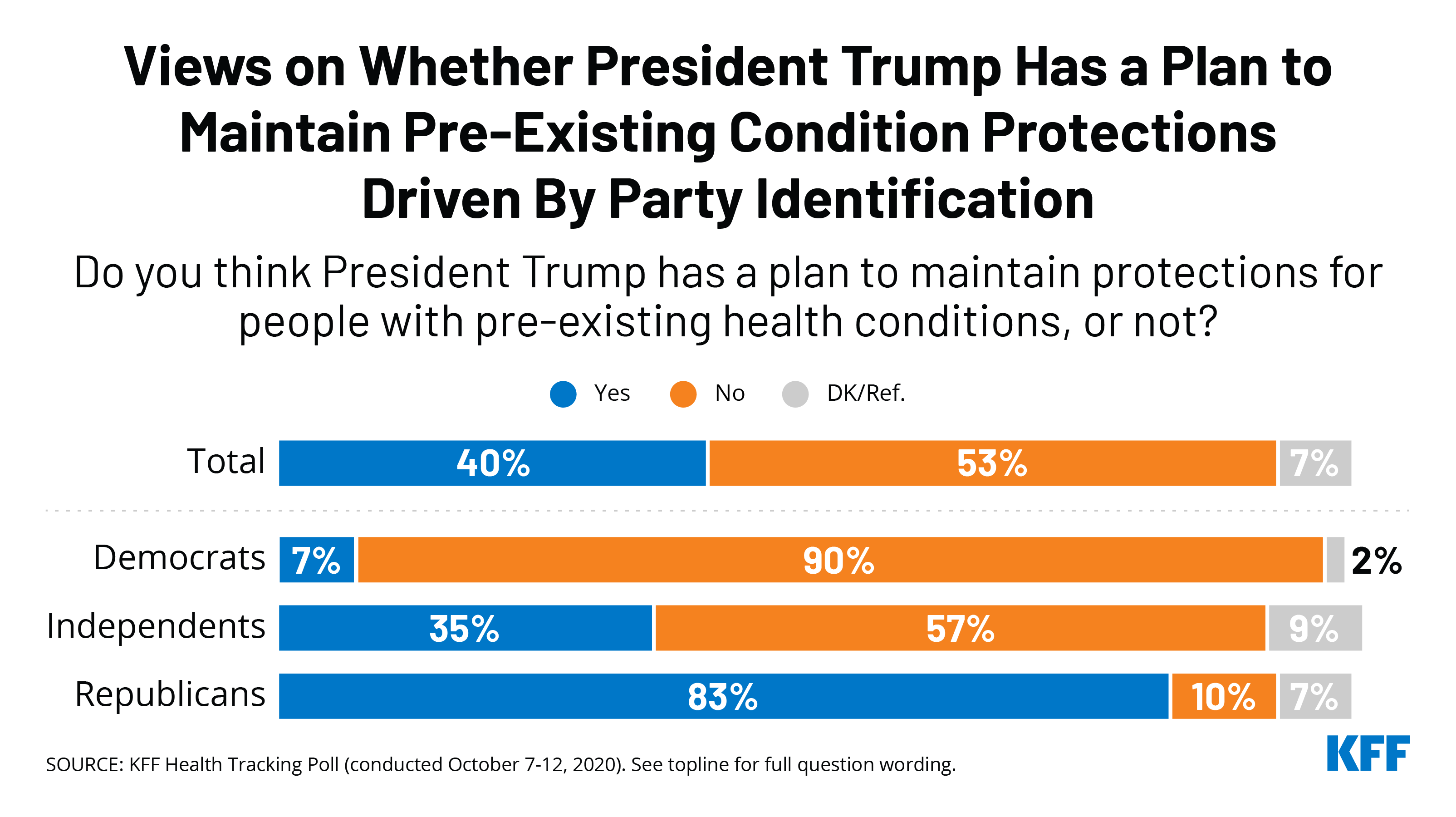
The October KFF Health Tracking Poll finds that a large majority of the public – including majorities of Democrats (91%), independents (81%), and Republicans (66%) – now say they do not want to see the Supreme Court overturn the ACA’s pre-existing condition protections. The share who do not want to see these protections overturned has increased by double digits from one year ago for each group. While both presidential candidates – President Trump and former Vice President Joe Biden – say they have plans to ensure pre-existing condition protections, more than half (53%) of the public say they “do not think President Trump has a plan to maintain protections for people with pre-existing health conditions,” including majorities of Democrats (90%) and independents (57%). On the other hand, a large majority of Republicans (85%) say President Trump “has a plan” to maintain these protections afforded by the ACA.
In 2020, Trump signed an executive order – a statement of goals — promising to protect people with pre-existing conditions, but has offered no plan to do so. This order is not a binding rule or law. President Trump has not provided further details.
Government officials hope to identify one or more safe and effective COVID-19 vaccines over the next few months as part of a multi-agency effort known as Operation Warp Speed. If and when they succeed, their focus will shift to making sure people across the country can access the vaccine.
A new issue brief lays out some of the key challenges with such a massive vaccination effort, which could require hundreds of millions of vaccine doses to be delivered across the country in a short period of time. The brief describes the leading vaccine candidates for the U.S. and what’s known about the federal government’s plans for distributing a successful vaccine or vaccines across the country and the challenges, including the potential need for billions of dollars in additional funding.
It also examines issues around supply, logistics and monitoring; the role of the federal, state and local governments; insurance coverage and out-of-pocket costs; racial and ethnic disparities; and building public confidence about the vaccine’s safety and effectiveness.
The brief is part of KFF’s broader portfolio examining the health and economic impacts of the COVID-19 pandemic, including original policy analysis, polling and journalism.
Poll: Most Americans Say President Trump is Intervening with the FDA’s and CDC’s Coronavirus Work, But Trust the Agencies at Least a Fair Amount to Do the Right Thing
Two-Thirds of the Public Worries They or Someone in Their Family Will Get Sick from Coronavirus, up 13 Percentage Points Since April
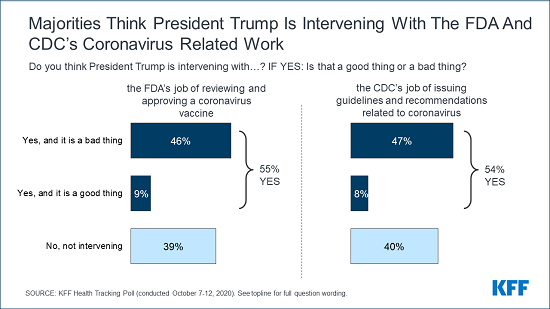
As COVID-19 cases rise across much of the country, most Americans think that the president is intervening with the public health agencies working to address the pandemic, the latest KFF Health Tracking Poll finds.
Similar majorities say both that President Trump is intervening with the Food and Drug Administration’s efforts to review and approve a coronavirus vaccine (55%) and that he is in intervening with the Centers for Disease Control and Prevention’s efforts to issue coronavirus guidelines and recommendations (54%). In each case, most of those who believe President Trump is intervening say it is a bad thing.
There are partisan differences. Most Republicans say the president is not intervening, while most Democrats think President Trump is intervening, and that it is a bad thing.
Majorities are also at least somewhat worried that political pressure from the White House will lead the FDA to rush to approve a vaccine without making sure it is safe and effective (62%).
In spite of these concerns, large majorities of the public have at least a fair amount of trust both in the FDA to ensure any vaccine is safe and effective (71%) and in the CDC to provide guidelines and recommendations based on scientific evidence (72%). In each case, majorities across party lines trust the agencies, though Democrats are more likely than Republicans to trust the CDC “a great deal.”
The poll also finds two thirds (66%) of the public are now worried that they or someone in their family will get sick from COVID-19, up 13 percentage points from April when slightly more than half (53%) were worried. Women are more likely than men (73% v. 58%) to worry about the risk. Among partisans, twice as many Democrats as Republicans (87% v. 42%) worry about this risk.
The poll also gauges the impact of President Trump’s recent COVID-19 diagnosis and treatment on the public’s willingness to engage in preventive measures.
About 3 in 10 say it has made them more likely both to practice social distancing (31%) and wear face masks (31%). About twice as many Democrats as Republicans say President Trump’s diagnosis makes the more likely to practice social distancing (44% vs. 20%) and wear face masks (40% vs. 20%).
“At a time when President Trump is aggressively downplaying the pandemic, his diagnosis and hospitalization appear to have had the opposite effect, scaring some Americans, including Republicans, to take more precautions such as wearing masks,” KFF President and CEO Drew Altman said.
About 4 in 10 adults (42%) think the worst of the coronavirus outbreak is yet to come, while a third say the worst is behind us (33%), and one in five don’t think it is a major problem. The share who say the worst is yet to come remains well below its peak in July (60%).
Designed and analyzed by public opinion researchers at KFF, the poll was conducted from Oct. 7-12 among a nationally representative random digit dial telephone sample of 1,207 adults. Interviews were conducted in English and Spanish by landline (290) and cell phone (917). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
A COVID-19 vaccine or vaccines may become available in the United States in the next several months, at which point the process of actually delivering vaccines to most, if not all, of the population will begin. Although the U.S. has some experience with mass vaccine distribution, including during an outbreak, COVID-19 represents an unprecedented challenge that will require a scale not previously undertaken. Planning has already been underway, including the release of a federal distribution strategy and the federal government’s advance purchase of millions of doses of COVID-19 vaccine candidates. Even so, numerous outstanding questions and challenges remain regarding vaccine distribution, including:
Funding for Vaccine Distribution. A critical and potentially limiting factor in the distribution of a COVID-19 vaccine is resource constraints faced by state and local health departments. Public health has long been underfunded in the U.S., and the health and economic impacts of the pandemic have further strained the public health infrastructure and reduced revenues. To date, just $200 million in federal emergency funds has been directed to state and local health departments for vaccine distribution.
Supply, Logistics, and Monitoring. Distributing potentially hundreds of millions of doses of COVID-19 vaccines rapidly, effectively, and equitably represents a public health logistics effort on a scale not seen in the U.S. before. In addition to the challenges of the sheer number of doses likely to be needed, other logistical issues include identifying and vetting a broad network of sites for administration, ensuring cold chain requirements are met, monitoring delivery of multiple doses, and tracking vaccine safety.
Federal, State, and Local Authority Over Vaccination Requirements. There remain outstanding issues concerning the relative roles and responsibilities of the federal, state and local governments in vaccine distribution in the context of a pandemic which crosses jurisdictional lines. A complicated patchwork of rules and regulations across jurisdictions could result in differential access to vaccines and varying levels of success in controlling COVID-19. Some policy considerations include whether or not vaccine mandates or changes in scope of practice regulations regarding who can administer a COVID-19 vaccine will be pursued.
Insurance Coverage and Out-of-Pocket Costs. Ensuring that COVID-19 vaccines are covered by insurance and available at no-cost to individuals would greatly enhance access. Both the Administration and Congress have taken steps to address this issue, including advance purchase of millions of doses of COVID-19 vaccine candidates and legislative requirements to provide no-cost COVID-19 vaccines under private insurance, Medicaid, and Medicare, building on existing protections under the Affordable Care Act (ACA). Despite these measures, limitations and gaps remain and some individuals may still face cost and access barriers.
Addressing Racial and Ethnic Disparities. COVID-19 has had a significant impact on communities of color in the U.S., and the pandemic threatens to further widen racial and ethnic disparities. People of color may face greater challenges in seeking and receiving Covid-19 vaccines due to cost and access issues and may be more reluctant to get a vaccine due to mistrust of the medical system. Taken together, these issues present formidable challenges not only to reaching people of color with a COVID-19 vaccine, but to the success of the overall national COVID-19 vaccine effort.
Communication and Trust. Except when individuals may be subject to a vaccine mandate, receiving a COVID-19 vaccine will be voluntary, so high vaccination rates will depend on the public’s willingness to be vaccinated. People will have to trust the vaccine, the authorities overseeing distribution, and the provider administering the vaccine. All vaccines face issues of public confidence to one extent or another, yet there are indications that distrust of COVID-19 vaccines may be greater than other vaccines, and concerns about politicization of vaccine approval and distribution. Overcoming this trust deficit will likely require robust communication and trust-building efforts.
Issue Brief
Introduction
A vaccine or vaccines for COVID-19, the disease caused by the SARS-CoV-2 virus, may become available for use in the U.S. over the next several months. At that point, officials will begin the process of actually delivering vaccines to states and localities and overseeing their administration to individuals. It will be a historically complex challenge to ensure that enough vaccines are distributed in a rapid, effective, and equitable way. The U.S. has some experience with mass vaccine distribution to build on and has faced some of the challenges before, but delivering COVID-19 vaccines will need to be at a much greater scale than past efforts, and will also bring new and unique challenges.
While there are still many unknowns, it is likely that hundreds of millions of COVID-19 vaccine doses will have to be administered to people across the country to achieve an adequate level of protection. For example, by one estimate, 462 to 660 million doses of a vaccine could be needed for a two-dose regimen, and potentially more over time depending on the strength and duration of immunity and dosing requirements. While initial planning documents have been released, numerous outstanding questions and challenges remain. These range from questions regarding the respective roles of the federal, state, and local governments, to financing and coverage of a vaccine, addressing racial and ethnic disparities and communication and public trust. This brief outlines what is currently known about the U.S. COVID-19 vaccine distribution plan and discusses key issues and challenges as well as outstanding questions.
COVID-19 Vaccine Candidates and Timeframe for Availability in the U.S.
The U.S. government, through a multi-agency, public-private partnership, known as Operation Warp Speed (OWS), which was publicly launched on May 15, has provided pharmaceutical companies with over $10 billion in funding to support research, development, manufacturing, and distribution of eight different candidate COVID-19 vaccines. Through these efforts, the federal government has already effectively purchased hundreds of millions of doses of these vaccines, from multiple manufacturers, even as clinical trials and federal regulatory review are ongoing (see Table 1).
Table 1: Characteristics of Known Operation Warp Speed COVID-19 Vaccine Candidates(as of October 15, 2020)
Supports advanced clinical studies, vaccine manufacturing technology transfer, process development, scaled-up manufacturing, and other development activities, to make available at least 300 million doses of a coronavirus vaccine.
Supports demonstration of large-scale manufacturing and delivery of 100 million doses of vaccine. By funding this effort, the federal government will own the 100 million doses. The government can also acquire additional doses up to a quantity sufficient to vaccinate 300 million people.
Supports accelerated development of an rVSV-SARS-CoV2 (recombinant) COVID-19 vaccine. Based on experience with the rVSV-based Ebola vaccine, a COVID-19 vaccine using the same rVSV platform has potential to provide a rapid and robust immune response.
Supports manufacturing and delivering of 100 million doses of vaccine candidate. By funding this effort, the federal government will own the 100 million doses. The government can also acquire up to an additional 400 million doses.
Supports large-scale production and nationwide delivery of 100 million doses of a vaccine. By funding this effort, the federal government will own the 100 million doses. The government can also acquire up to an additional 500 million doses.
Supports advanced development including clinical trials and large-scale manufacturing of 100 million doses. By funding this effort, the federal government will own the 100 million doses. The government can also acquire up to an additional 500 million doses.
NOTES:a The agreement between the federal government and AstraZeneca states that “at least 300 million doses will be made available” to the government.b Merck/IAVI and Sanofi/GlaxoSmithKline vaccine trials are testing 1 and 2 dose regimens.
It is possible that one or more of the OWS vaccine candidates will become available for public use over the next several months. Four candidates have already advanced to Phase 3 trials, undergoing study in large groups of volunteers to determine their safety and efficacy. Under the most optimistic scenarios, initial trial results for at least one vaccine candidate could be available as early as the end of October. However, it is more likely results will start to become available later in the year or next year, and companies have said they would not start to pursue authorization until late November at the earliest. Typically, vaccines are approved through the FDA’s Biologic License Application (BLA) process, but during a public health emergency the FDA can grant an Emergency Use Authorization (EUA) for a vaccine even before full approval if certain criteria are met. Access through an EUA is accelerated compared to a BLA because the requirements are less stringent and vaccine use under an EUA could be more limited to specific target groups. It is expected that even if an EUA is granted, companies will continue to pursue full regulatory approval through the BLA process, which could be completed for some vaccine candidates in 2021.
It is also expected that upon FDA authorization or approval there will already be a limited number, perhaps tens of millions of doses, of a given vaccine ready to be shipped. Manufacturing is expected to ramp up after FDA authorization or approval, which would allow for distribution of an increasing number of doses over time. Eventually there could be multiple, competing vaccines that have been approved or authorized, raising questions about how the government will identify the preferred vaccine(s) and how people will differentiate between the various vaccines’ effectiveness and safety. It is also important to note that these vaccine candidates have so far been tested in non-pregnant adults only, and at least initially will likely not be recommended for use in children. Additional trials looking at vaccine effectiveness in children are likely to come later.
Table 2: Key Terms/Entities Involved in the COVID-19 VaccineAuthorization and Approval Process
The federal government’s multi-agency, public-private partnership “to accelerate the development, manufacturing, and distribution of COVID-19 vaccines, therapeutics, and diagnostics”, with the goal producing and delivering 300 million COVID-19 vaccine doses in the United States. OWS is led by the Department of Health and Human Services (including CDC, FDA, NIH, and BARDA) and the Department of Defense.
The VRBPAC advises the FDA Commissioner “in discharging responsibilities as they relate to helping to ensure safe and effective– vaccines and related biological products for human use and, as required, any other product for which the Food and Drug Administration has regulatory responsibility.” It provides independent advice and recommendations. The VRBPAC may review a vaccine EUA request as well as BLA request.
Before formal vaccine approval by the FDA, a product must pass through three phases of clinical trials, starting with Phase 1 trials, with a small number of people and continuing to Phase 3 trials, large-scale, safety and effectiveness studies. After successful completion of all three trial phases (with specified endpoints met), a Biologics License Application (BLA) may be submitted. A BLA “is a request for permission to introduce, or deliver for introduction, a biologic product into interstate commerce”, that the FDA reviews to decide on approval.
The FDA released specific guidance for industry on the COVID-19 vaccine approval process in June 2020. The guidance recommends that a COVID-19 vaccine demonstrate evidence of being at least 50% effective, among other criteria, before seeking approval.
During a public health emergency, the FDA can use its EUA authority to “allow the use of unapproved medical products, or unapproved uses of approved medical products, to diagnose, treat, or prevent serious or life-threatening diseases when certain criteria are met.” An EUA may be granted based on interim analysis of clinical endpoint data from a Phase 3 trial, and before a manufacturer has submitted and/or FDA has completed a formal review of a BLA.
The Secretary of HHS first declared COVID-19 to be a public health emergency on January 31, 2020 and has renewed this designation several times since. The FDA’s most recent EUA guidance for COVID-19 was released on October 6, 2020. As part of this guidance, the FDA has specified that data from Phase 3 trials should include a median follow-up duration of at least two months after completion of the full vaccination regimen before an EUA may be requested.
The NIH and CDC sponsored a National Academies consensus study to assist policymakers in developing guidelines for the equitable allocation of COVID-19 vaccines, both domestically and globally. It is intended to inform a range of advisory groups and decision-making bodies, including the CDC’s Advisory Committee on Immunization Practices (ACIP). On October 2, the committee released its framework report. The framework identifies four risk-based criteria for prioritization– risk of acquiring infection; risk of severe morbidity and mortality; risk of negative societal impact; and risk of transmitting infection to others – and four allocation phases.
The ACIP was established under Section 222 of the Public Health Service Act (42 U.S.C. §2l7a), as amended. The ACIP provides advice and guidance to the Director of the CDC regarding use of vaccines for effective control of vaccine-preventable diseases in the United States. Recommendations made by the ACIP are reviewed by the CDC Director, and if adopted, are published as official CDC/HHS recommendations. This typically includes advice regarding vaccines already licensed for use in the U.S., but guidance can be issued for unlicensed vaccines, such as those authorized under an EUA.
Plans for U.S. Distribution of COVID-19 Vaccines
The federal government has released several documents addressing how vaccine distribution will proceed. On August 4, the Centers for Disease Control and Prevention (CDC) provided state and local health departments with interim vaccine planning assumptions and action steps to inform development of COVID-19 pandemic vaccination plans. Actual planning documents were provided to health authorities on August 27; at this time, CDC also sent a letter to governors asking them to ensure distribution sites in their states could be operational by November 1. OWS provided Congress with a federal vaccine distribution strategy, and CDC released an interim playbook for jurisdiction operations on September 16. In the playbook, CDC says jurisdictions are required to develop and submit vaccination plans by October 16, 2020. Finally, on September 23, HHS announced that it was providing $200 million to state and local jurisdictions specifically for vaccine preparedness. An OWS organization chart provides additional information on the leadership structure and respective roles of federal agencies.
Based on these documents, current U.S. distribution plans are as follows:
After FDA authorization or approval, the federal government and 64 state, local, and territorial jurisdictional immunization programs1 , that CDC funds and works with, will begin to oversee delivery of available vaccine doses to approved administration sites across the country. At first, there will be few vaccine doses available, so the federal government will determine the number of doses allocated to each jurisdiction. This allocation will depend on which vaccine(s) are approved, the number of doses available for those vaccines, the population of jurisdictions, and potentially other factors.
Distribution is expected to unfold in phases. Jurisdictions have been told to use the following assumptions in planning for each phase. In Phase 1, an initial limited supply of vaccine doses would be available, and therefore likely be prioritized for certain groups and distribution and administration more tightly controlled. In Phase 2, the vaccine supply would be increased and access expanded to include a broader set of the population, with additional providers involved in administration. In Phase 3, there would likely be sufficient supply to meet demand, and distribution would be integrated into routine vaccination programs. (Many of the distribution issues discussed in this brief refer to challenges faced especially during Phase 1 and Phase 2).
Pre-approved administration sites will make requests for vaccine doses to their jurisdiction’s immunization program, which will review and approve these requests according to its allocation of vaccines from the federal government. Jurisdictions’ immunization programs will submit orders to the federal government (initially to OWS, potentially later to CDC as well). Once reviewed by federal officials, vaccine doses will be delivered by a central distributor to administration sites within 48 hours of approval. This stands in contrast to the distribution system used for seasonal influenza where, outside of the CDC’s Vaccines for Children Program (VCP) and the Section 517 Immunization Program (described below), vaccine production and distribution are primarily handled by the private sector. For COVID-19, the federal government has selected McKesson Corporation as its central distributor. McKesson currently serves as the central distributor for the VCP and was the central distributor during H1N1 pandemic influenza in 2009-2010.
In addition to vaccines being delivered by the central distributor via orders received from jurisdictions’ immunization programs, the federal government may also ship doses to designated secondary vaccine depots and receive orders from and ship doses directly to some private partners with agreements in place such as large retailers and pharmacies, especially as more doses become available.
Federal, state, and local government officials will determine a prioritization schedule for how to allocate the initially limited vaccine doses to specific population groups. Federal agencies asked the National Academies of Medicine (NAM) to develop a framework for prioritization, which NAM released on October 2. The NAM findings will inform additional recommendations and policies to be developed by the CDC’s Advisory Committee on Immunization Practices (ACIP), the official federal advisory committee that informs CDC’s immunization policies, practices, and recommendations. The NAM framework and initial discussions at ACIP indicate that high-risk workers in health care facilities, first responders, and persons at elevated risk from COVID-19 disease such as the elderly, are likely to be among the groups prioritized for receipt of the early, limited number of vaccine doses.
Indications are that the administration of the vaccine to individuals will likely take place in a wide variety of locations, including: public and private hospitals and clinics (e.g., federally qualified health centers, rural health centers), medical practices, pharmacies, and potentially government-run mass vaccination locations. Jurisdictions’ immunization programs and the federal government will work together to identify and approve distribution sites and expect the need to expand the network of partner sites to reach all target populations.
While the U.S. military has been a key part of the OWS effort by supplying logistical, program management, and contracting expertise, current plans do not include a major role for the military in distributing Covid-19 vaccines to the general public.
Policy and Implementation Issues and Questions
Even with the release of these documents, many outstanding questions and a myriad of potential issues remain. Some of these are dependent on the specific characteristics of any vaccine that is authorized or approved (e.g., the number of doses needed, storage requirements, and the target recipient profile), and final decisions regarding an allocation framework. Others are due to the unprecedented scale and complexity of the COVID-19 pandemic, including its devastating health and economic impacts and disproportionate impact in some communities, particularly communities of color. Still others are due to existing policy barriers and challenges, resource constraints, and unresolved decisions on the part of federal, state, and local governments. Finally, the hyper-partisan nature of the COVID-19 response in the U.S. has contributed to growing public mistrust and skepticism of a COVID-19 vaccine, presenting particular challenges for vaccine adoption. We examine some of these key issues below. This list is not meant to be exhaustive; for example, we do not examine in detail the issues around the prioritization of the potentially limited supply of vaccines, which is the subject of the NAM committee and will also be addressed by ACIP.
Funding for Vaccine Distribution
A critical and potentially limiting factor in the distribution of a COVID-19 vaccine is resource constraints faced by state and local health departments, who will have the main responsibility for managing vaccine distribution. Public health has long been underfunded in the U.S., and the health and economic impacts of the pandemic have further strained state and local public health infrastructure and reduced state revenues upon which they depend. Many have yet to meet the testing and contact tracing needs they already face, let alone be ready to distribute a new vaccine. To date, Congress has appropriated approximately $2.45 billion across two of the four emergency COVID-19 relief bills2 to states, localities, and territories for a range of COVID-19 public health activities that, while not specific to vaccines, could include vaccine-related activities. Thus far, of these amounts, CDC has awarded $200 million from CARES Act funds to jurisdictions for vaccine preparedness, well below what is likely needed for such a large scale effort. At a September 16 hearing of the Senate Appropriations Subcommittee Hearing on Coronavirus Response, CDC Director Redfield stated that state and local jurisdictions needed $6 billion to support COVID-19 vaccine distribution, while the National Association of City and County Health Officers estimates the need at $8.4 billion. The Association of Immunization Managers, which represents the 64 state, local, and territorial immunization programs, has said that additional funds are needed for shoring up the health care workforce, opening new vaccine administration sites, adapting information systems, purchasing personal protective equipment, and combating disinformation and vaccine hesitancy, among other areas. Concerns about funding challenges have also been raised by the National Governors Association. Negotiations between Congress and the Administration on a fifth COVID-19 relief bill, which would have included billions for vaccine distribution (the House Democratic bill, the Heroes Act, included $7 billion and the Senate Republican bill included $6 billion), are stalled, so it is unclear when additional funding will be made available to states for this purpose.
Government-led vaccine distribution in the timeframe and at the scale being contemplated for COVID-19 has never before been done in the U.S., with hundreds of million doses needing to be distributed, over as short period of time as possible, in order to vaccinate most of the U.S. population. In contrast, in a typical year, CDC distributes about 75 million vaccine doses to health departments and private providers. In the context of the H1N1 pandemic during 2009-2010, the government distributed 124 million doses of the H1N1 pandemic influenza vaccine over the course of several months. In recent years, over 150 million doses of seasonal influenza vaccines have been delivered in the U.S. per year, though, as mentioned above, outside of the VCP and 317 programs, these vaccines are primarily distributed via the private sector, not by the government. In addition to the sheer number of doses likely to be needed, there are a host of logistical issues and supply challenges that come with the effort to distribute COVID-19 vaccines, including:
The actual set of sites where vaccines will be administered, especially for the earliest phases of distribution, remains unclear. Federal guidance and operational plans indicate that it will be a mix of providers (such as hospitals and medical practices), pharmacies, state and local public health departments, and potentially government-run mass vaccination sites. Thousands of specific partners and site locations will have to be identified (and in some cases created), vetted, and approved before vaccine doses can be distributed to them. The accessibility of these sites will have implications for equitable access to the vaccine, given that lower income individuals and people of color are more likely to face transportation/location-based barriers to health care.
Existing state and local governmental distribution networks are primarily focused on delivering childhood, but not adult vaccines. Especially early on, adults will likely be the focus for COVID-19 vaccine distribution, and mass distribution of vaccines to adults has, in the past, proven more challenging than delivering to children. This is because there are fewer pre-existing relationships and networks through state and local governments for adult vaccinations. During 2009-2010, for example, state and local vaccine programs had to triple the number of providers they had a relationship with to be able to distribute 2009-H1N1 vaccines. Governments at all levels will likely have to significantly expand their distribution channels and partnerships for vaccine administration to reach target groups with a COVID-19 vaccine.
There will be a need to account for flexibility in planning and implementation of distribution. As the CDC and HHS plan distribution plans already recognize, there will be few doses available early on in the distribution process, with the supply of vaccine extremely limited compared to the demand. This will mean the first doses will be rationed, and that roll out will occur with unpredictable timing, as vaccine doses become available as production expands. Therefore, it will be important to set realistic expectations on initial supply. The effort to roll-out the 2009 H1N1 pandemic influenza vaccine lost credibility among state and local officials and the public alike when the amount of vaccine available to the public in October 2009 did not meet the earlier expectations that had been set by federal officials.
Several of the likely COVID-19 vaccine candidates need to be preserved at extremely cold temperatures, which will require specialized equipment not currently available in many distribution sites. Urban areas, where specialized equipment is more likely to be present, will likely be able to manage cold chain supply processes more easily than rural areas where the equipment may not be available, which could introduce inequities in distribution. The federal government has stated it would likely not require jurisdictions to procure additional equipment but could implement a distribution approach that involved distributed networks of federally managed cold chain sites and use of mass vaccination to reach target populations.
Several leading vaccine candidates will require two doses for immunization, with the second dose given several weeks after the first, which raises additional challenges. Vaccines with two-dose regimens will require careful tracking of doses and follow up with each individual receiving the vaccine to ensure they receive the same vaccine, with the second dose given at the proper time. This kind of two-dose schedule has not been required for other mass-distributed vaccines such as seasonal influenza or during the 2009-H1N1 pandemic influenza. The CDC and local jurisdictions are in the process of implementing a new vaccine tracking system to monitor COVID-19 vaccine administration and help with multiple dose tracking, but it is unclear if, or how, the new system will integrate with existing immunization information systems (IIS). There is already great variation in IIS across jurisdictions, and many have gaps and face other challenges including low provider participation rates and lack of interoperability of immunization records with patients’ electronic health records and across jurisdictional borders.
Vaccines may be released on an accelerated schedule, and some may be administered under an EUA without having gone through a full safety review initially, so the government is planning on implementing enhanced safety monitoring to track vaccine adverse events. Close tracking of safety and adverse events is yet another layer of planning and administration falling primarily on state and local health authorities. Tracking adverse events closely will be important not only to determine the safety of the vaccines, but also to establish evidence of harm in individuals for potential compensation purposes. Under the liability protections outlined in the Public Readiness and Emergency Preparedness (PREP) Act manufacturers cannot be held liable for damages caused by their vaccines (except where there has been willful misconduct). However, individuals who die or suffer serious injuries directly caused by the administration of an approved vaccine under conditions of a public health emergency could receive compensation from the government through the Countermeasures Injury Compensation Fund (CICF), although there are some limitations to the CICF.
Given that demand will be high and supply low during the initial phase of distribution, vaccine doses will be seen as highly valuable and therefore vulnerable to theft, fraud or corruption. This means physical security and close tracking of the shipments of doses will be required to ensure that vaccine doses get to delivered and administered properly, a level of planning and oversight beyond what is normally needed for vaccine distribution.
Federal, State, and Local Authority Over Vaccine Requirements
There remain outstanding issues concerning the relative roles and responsibilities of the federal, state and local governments in distributing a vaccine, as well as those of private actors. While much of the responsibility in the U.S. for delivering public health services, including support for vaccination, lies at the state and local levels, other considerations may be warranted in the midst of a pandemic that has been declared a national emergency. Federalism has benefits for public health, particularly the ability to localize responses, but raises unique challenges in a pandemic, with the potential for a complicated patchwork of different rules and regulations to navigate across jurisdictions, which could result in different timetables for receiving and shipping vaccines to providers, different levels of success in reaching target outcomes across the country, and differential access by geography, which could exacerbate existing inequalities in access and care and ultimately have implications for public health and broader population immunity. As one example, adult coverage rates for seasonal influenza, an ACIP-recommended vaccine that is free for most with insurance, vary by state, ranging from a low of 25% in Nevada to a high of 51% in Rhode Island (among those ages 18-64).
More specifically, some of the policy considerations around federal and state responsibilities include:
Vaccine mandates: Governmental vaccine mandates play a role in the distribution and uptake of many vaccines, but the extent to which mandates can and will be used by federal, state, and local authorities to encourage COVID-19 vaccinations remains an open question. There are potential mechanisms by which federal authority could impose vaccine requirements such as though conditioning some forms of federal funding on vaccination, but there is a debate about how far federal powers extend here and whether the government should use these authorities for COVID-19 vaccines. On the other hand, state and local jurisdictions commonly impose vaccine mandates and could use their authorities to impose COVID-19 vaccination mandates, but this might mean requirements would vary greatly across jurisdictions.
All states have immunization requirements in one form or another for child-care and school-age children, although there is significant variation across states (see Table 3). In many cases states mandate a set of vaccinations for children, allowing exemptions from this requirement only under certain circumstances. For example, some states allow only medical exemptions from vaccine requirements, while others allow medical as well as non-medical exemptions under some circumstances.
Seasonal influenza vaccinations are typically not mandated by states, though some have taken steps toward such mandates. In August, Massachusetts announced it would require children in daycares and schools to receive a seasonal influenza vaccination this year; other states could follow. In 2009-2010 there were no state-level mandates requiring that children or adults receive a 2009-H1N1 influenza vaccine.
Some states also mandate vaccines for certain types of health care workers, such as those working in hospitals or long-term care facilities. State laws vary considerably in terms of which vaccines are required, which types of workers the mandates cover, and what types of exemptions from these mandates are allowed. In the future, similar mandates could be developed by states for COVID-19 vaccines.
States have additional authorities to mandate vaccinations during public health emergencies and outbreaks, often with the power to order such actions resting with the governor of the state or with a state health officer. For example, following a measles outbreak in 2019, New York City declared a public health emergency and used its expanded authority to requirethat individuals in certain zip codes to be vaccinated for measles. The differential application of these expanded authorities by states could introduce further inequities in vaccine coverage.
Finally, in some cases, the private sector may mandate vaccination as a condition of employment, such as a hospital mandating vaccination for its health care workers. More generally, the U.S. Occupational Safety and Health Administration (OSHA) has taken the position that employers can require employees to be vaccinated for influenza, though exemptions may be provided. The U.S. Equal Employment Opportunity Commission (EEOC) states that employers should consider encouraging, rather than requiring, vaccination and, if vaccination is required, employees may be entitled to exemptions. Given the gravity of COVID-19, it is possible that employers will seek to mandate vaccination in some cases.
Table 3: State Mandates for ACIP-Recommended Pediatric Vaccines
Vaccine
Number of States with Mandate
Influenza
5 states*
DTaP/Tdap
50 states and DC
MMR
50 states and DC**
Polio
50 states and DC
Chicken pox
50 states and DC
Hepatitis A
17 states and DC
Hepatitis B
46 states and DC
HPV
3 states and DC
Meningococcal
29 states and DC
NOTES: DTaP/Tdap: tetanus, diphtheria, and pertussis; MMR: measles, mumps, rubella; HPV: human papillomavirus*CT, NJ, PA, and RI only require annual flu shots in childcare settings; MA requires of all children.**IA does not require a mumps vaccineSOURCE: KFF analysis of Information from state statutes and immunization websites.
Scope of practice regulations for vaccine administration. A key issue to consider concerns regulations around who can administer vaccines. Licensing of providers who can administer vaccines is determined at the state level, and therefore varies across the country. Expanding this scope of practice is one avenue for increasing distribution channels and uptake. Medical providers, such as physicians and nurses, commonly administer vaccines, but pharmacists can also administer many vaccines. State requirements around pharmacist administration of vaccines vary, particularly around which vaccines can be administered, what kind of training is needed to be licensed, and what for what ages pharmacists can vaccinate. During a public health emergency states can expand scope of practice laws, as several states did during the H1N1 pandemic in 2009-2010, but this can lead to differences across states. During a public health emergency, the federal government also has authority to expand scope of practice regulations under the PREP Act, and HHS has already done so to authorize pharmacists to order and administer childhood vaccines to individuals ages three through 18 years and to procure and administer COVID-19 vaccines when they become available. The COVID-19 vaccine authorization specifically preempts any state or local law that would prohibit these providers from administering vaccines, if the providers satisfy the requirements laid out in the guidance. States, and the federal government, could consider further expansions of scope of practice to accommodate the scale of COVID-19 vaccination requirements, if needed.
Ensuring that COVID-19 vaccines are available at no-cost to individuals would greatly enhance access. Both the Administration and Congress have taken steps to address this issue. The OWS strategy states that the Administration’s advance purchase of millions of doses of COVID-19 vaccines candidates from multiple manufacturers is intended to ensure that no American will be charged for the vaccine or its administration (although it is possible that some vaccine providers may still charge an administration fee). The Families First Coronavirus Response Act and the CARES Act put specific requirements in place for no-cost COVID-19 vaccine access under private insurance, Medicaid, and Medicare. These build on existing protections provided under the Affordable Care Act (ACA). However, despite these measures, limitations and gaps related to a COVID-19 vaccine remain, and some individuals, particularly adults, may still face cost and access barriers. Some of the key provisions and outstanding issues include:
Private Insurance: Under federal legislation, most private insurers will be required to cover COVID-19 vaccines at no-cost. The ACA requires private health insurers to cover any vaccine recommended by ACIP at no-cost, although insurers have up to one year from the time of recommendation to implement coverage. The CARES Act specifically requires group health plans and health insurance issuers (those subject to ACA requirements for preventive services, but not including short-term limited duration or association health plans) to cover any ACIP-recommended COVID-19 vaccine without cost-sharing, including the cost of administration. Such coverage must begin 15 business days after an ACIP recommendation, which eliminates the usual up to one-year timeframe. However, these cost protections are not necessarily available if a patient seeks a vaccine from an out-of-network provider.
Medicaid. All children and some adults in Medicaid have coverage for vaccines at no cost, and Congress has temporarily addressed the gap for other adults to ensure coverage for a COVID-19 vaccine. The ACA requires Medicaid coverage of all ACIP-recommended vaccines at no-cost for adults in the Medicaid expansion population. However, for adults covered through traditional Medicaid pathways, immunizations are an optional Medicaid benefit and, when covered, cost-sharing may be imposed. Currently, less than half of states cover all ACIP-recommended adult immunizations. The Families First Act addressed this by authorizing a 6.2 percentage point increase in federal Medicaid matching funds to help states respond to COVID. As a condition of receiving these enhanced funds, states must cover COVID-19 vaccines without cost-sharing, during the public health emergency. When the public health emergency declaration ends, however, adults in traditional Medicaid could face cost-sharing or may not have coverage for the vaccine. For children, Medicaid covers vaccines at no-cost through the Vaccines for Children Program (VCP), a 100% federally funded entitlement program created by Congress in 1993. The VCP also provides no-cost vaccine coverage for American Indian and Alaskan Native children, uninsured children, and children who meet the program’s criteria for being underinsured. In addition, the Children’s Health Insurance Program (CHIP) also provides vaccine coverage for its enrollees, uninsured children who have incomes above Medicaid eligibility levels.
Medicare. Vaccines are covered through Medicare, but some beneficiaries may face cost-sharing or delayed access for a COVID-19 vaccine, depending on the process used by FDA to make a vaccine available for use. Medicare covers vaccines under Parts B and D, with most vaccines covered under Part D. Part D plans must cover all FDA-approved vaccines, although they may impose cost-sharing. The CARES Act requires Medicare Part B to cover a COVID-19 vaccine and its administration without cost-sharing upon licensure by the FDA; this applies to beneficiaries in both traditional Medicare and Medicare Advantage plans. It does not, however, require such coverage upon issuance of an EUA, which could limit access to vaccines for the more than 60 million people covered by Medicare if a vaccine first becomes available via an emergency authorization.
Uninsured and underinsured adults: There is no federal entitlement vaccination program for uninsured and underinsured adults. Instead, existing federal programs that support vaccination for the uninsured and underinsured are discretionary and rely on annual Congressional appropriations for funding. These include Section 317 of the Public Health Service Act, which authorizes the federal purchase of vaccines for uninsured or underinsured adults (as well as children and adolescents), and can be used during an outbreak, and funding for FQHCs, which provide vaccinations regardless of ability to pay. During H1N1, the federal government purchased the vaccine and funded public health authorities to ensure that uninsured and underinsured adults received it free of charge, as long as they were vaccinated at a public health clinic or other designated site. Similarly, it is expected that the federal government’s purchase of COVID-19 vaccines will be used to support free vaccination of adults who are uninsured and underinsured. Funds to providers to cover vaccine administration costs will be available through a “COVID-19 claims reimbursement program”, part of a new Provider Relief Fund created and funded through the CARES Act and the Paycheck Protection Program and Health Care Enhancement Act. Despite these measures, it is not yet known if the existing advance purchase of COVID-19 vaccines or the claims reimbursement program will be sufficient to support vaccination for all those who are uninsured and underinsured, and whether additional funding or other remedies might be needed.
COVID-19 has had a significant impact on communities of color in the U.S., who account for a disproportionate share of COVID-19 cases, hospitalizations, and deaths. Data also indicate that the pandemic is taking a larger economic toll on communities of color, and that COVID-19 threatens to further widen racial and ethnic disparities that already exist in the U.S. Moreover, the medical system’s historic mistreatment of people of color and ongoing racism and discrimination contribute to greater distrust among communities of color that may contribute to increased reluctance to be vaccinated. A new KFF/The Undefeated survey, for example, found that half of Black adults say they would not want to get a coronavirus vaccine even if deemed safe by scientists and freely available, with safety concerns and distrust cited as the top reasons (see Figure 1). By contrast, most White adults say they would get vaccinated, and those who wouldn’t are more likely to say they don’t think they need it. In addition, the survey found that majorities of Black adults lack confidence that the vaccine development process is taking the needs of Black people into account, and that when a vaccine becomes available it will have been properly tested and will be distributed fairly. Already, there are significant disparities in adult vaccine coverage rates for racial and ethnic minorities in the context of routine immunization. For example, coverage rates for seasonal influenza, which is available at no-cost to those with insurance, are lower for adults of color compared to Whites. Coverage rates by race/ethnicity also vary by state. Taken together, these issues present formidable challenges not only to reaching people of color with a COVID-19 vaccine, but to the success of the overall national COVID-19 vaccine effort. Ultimately, effective outreach strategies developed in partnership with and directed toward communities of color will be critical to building public trust and willingness to get vaccinated.
Figure 1: Black Americans Less Likely To Say They Would Get COVID-19 Vaccine Even If It Was Free And Determined Safe By Scientists
Except when individuals may be subject to a vaccine mandate, receiving a COVID-19 vaccine will be voluntary. Therefore, achieving high vaccination rates and sufficient population-level protection from the virus will depend on the public’s willingness to be vaccinated: people will have to trust the vaccine, the authorities overseeing distribution, and the provider administering the vaccine. All vaccines face issues of public confidence to one extent or another, yet there are indications that distrust of COVID-19 vaccines (despite the fact that no vaccine has been approved yet) may be even greater than for other vaccines. This presents a significant challenge for authorities at the federal, state, and local levels, and will require robust communication and trust-building efforts to address.
The most common reasons given by adults for not receiving seasonal influenza vaccines are concerns about the safety and efficacy of the vaccine and a belief the vaccine itself can make a person ill.
Polling on COVID-19 vaccines has indicated an increasing level of mistrust about the vaccines and decreasing willingness among Americans to receive one. In May, 72 percent of U.S. adults said they would definitely or probably get a vaccine to prevent COVID-19 if it were available but in September only 51 percent said the same (a 21 percent decline in four months). Partially driving this growing distrust among Americans is an increasing concern with politicization of the vaccine approval process: a majority of the public (62 percent) is worried political pressure will lead the FDA to rush to approve a coronavirus vaccine without making sure that it is safe and effective. As noted above, Black adults in particular have expressed some of the highest levels of mistrust of COVID-19 vaccines even as this group has been disproportionately affected by the pandemic.
Reducing mistrust about COVID-19 vaccines would involve a multi-pronged communication approach, including efforts to counter the growing public perception that politics is driving the vaccine approval process for COVID-19 to ensure Americans have confidence that when a vaccine is approved that they believe it is indeed safe and effective. A recent letter from the HHS National Vaccine Advisory Committee to the Assistant Secretary for Health included recommendations for building public confidence, including through a unified, proactive, and highly visible, communication structure and community and stakeholder engagement. Transparency and avoiding conflicts of interest helps in reducing mistrust. In addition, having clear, consistent, and culturally-relevant messages about COVID-19 vaccines and their benefits to individuals, communities, and the country will be important, as will building partnerships in advance with individuals and groups that can serve as trusted sources for delivering such messages for different communities. Given that safety of vaccines has been the number one concern both in past vaccination campaigns and regarding COVID-19 vaccines, a particular emphasis on assuring safety will be important.
There is no doubt that distributing COVID-19 vaccines will be a massive, complicated effort for the U.S., and an unprecedented challenge for officials at the federal, state, and local levels. While planning for distribution has been underway for months and progress has been made, there are still numerous questions about how the U.S. will plan to overcome the many challenges. An undertaking of this magnitude also means that no plan will unfold exactly as expected and there will inevitably be substantial learning and the need to make adjustments made as implementation unfolds. Adding further uncertainty to this effort is the fact the U.S. is currently in the midst of election season, and its possible there might be significant changes in federal, state, and local government leadership just as the distribution of COVID-19 vaccines gets underway. Successfully addressing the barriers and challenges identified here will be important in the effort to ensure the greatest health benefit accrues from administering COVID-19 vaccinations.
Endnotes
These include: all 50 states and DC; 8 U.S. territories and freely associated Pacific states and five cities. ↩︎
The Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 (P.L. 116-123), enacted March 6, specified that not less than $950 million “shall be provided for grants to or cooperative agreements with States, localities, territories, tribes, tribal organizations, urban Indian health organizations, or health service providers to tribes, to carry out surveillance, epidemiology, laboratory capacity, infection control, mitigation, communications, and other preparedness and response activities.” The Coronavirus Aid, Relief, and Economic Security (CARES) ACT (P.L. 116-136), enacted March 27, specified that “not less than $1.5 billion for grants to or cooperative agreements with states, localities, territories, tribes, tribal organizations, urban Indian health organizations, or health service providers to tribes, including to carry out surveillance, epidemiology, laboratory capacity, infection control, mitigation, communications, and other preparedness and response activities.” ↩︎
Approximately seven months after the coronavirus sparked social distancing measures and concerns about hospital capacity, new medical records data help shed light on the magnitude of the drop in hospital admissions and the more recent rebound in hospitalizations. These new data provide additional information to help assess the economic impact of the COVID-19 pandemic on hospitals and insurers and also provide more information to help assess the extent to which people are still delaying or forgoing care. We analyze trends in total hospital admissions and then separately analyze non-COVID-19 admissions by patient sex, age, and region. We calculate actual admissions as a share of total predicted admissions in 2020 based on trends from past years. Key findings include:
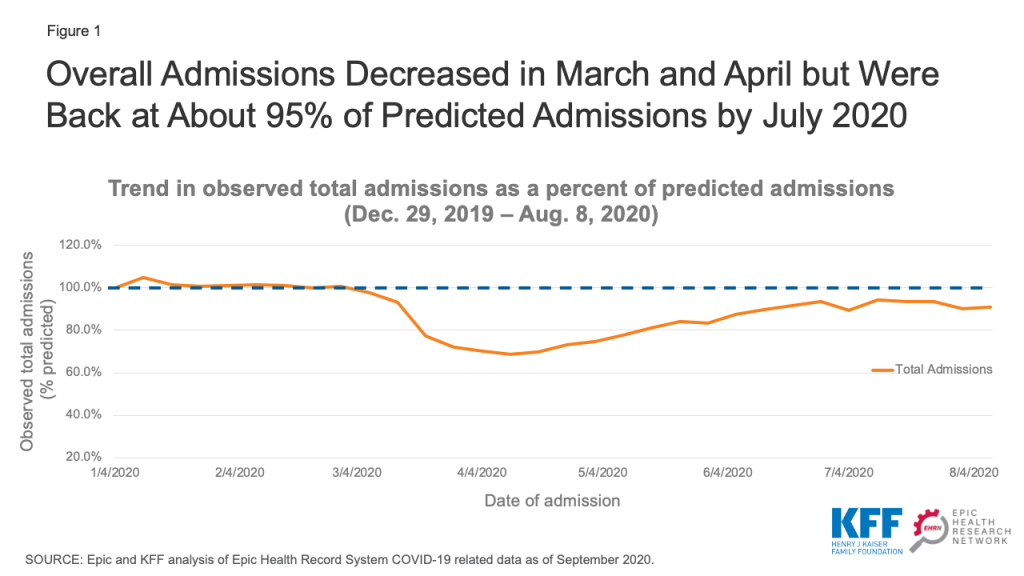
Total hospital admissions dropped to as low as 68.6% of predicted admissions during the week of April 11, 2020 and then increased to a high of 94.3% of predicted levels by the week of July 11, 2020. As of August 8, 2020, admission volume has dipped slightly to 90.8% of predicted levels.
Overall, the number of hospitalizations lost due to declines in admissions between March 8 and August 8, 2020, represent 6.9% of the total expected admissions for 2020.
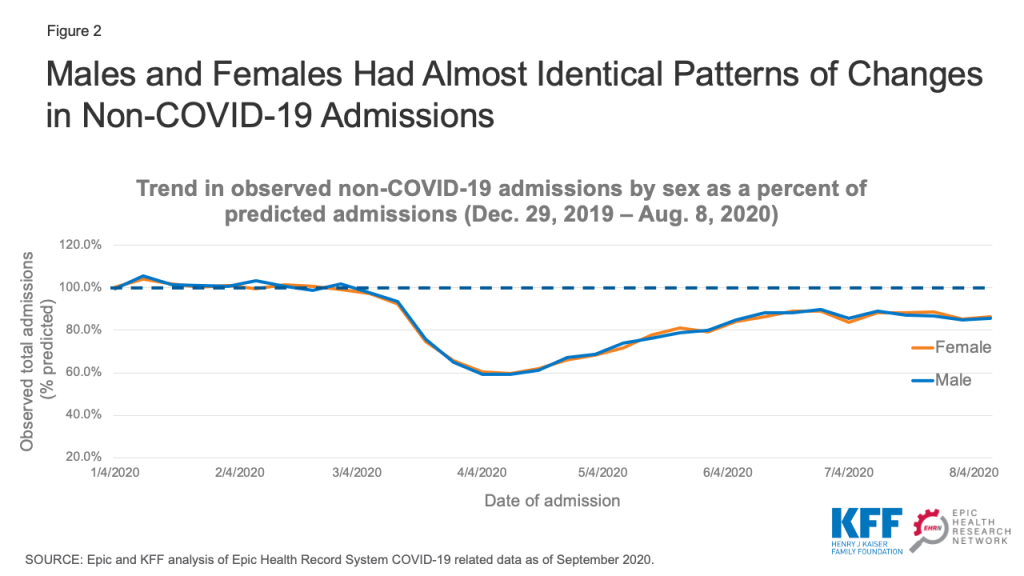
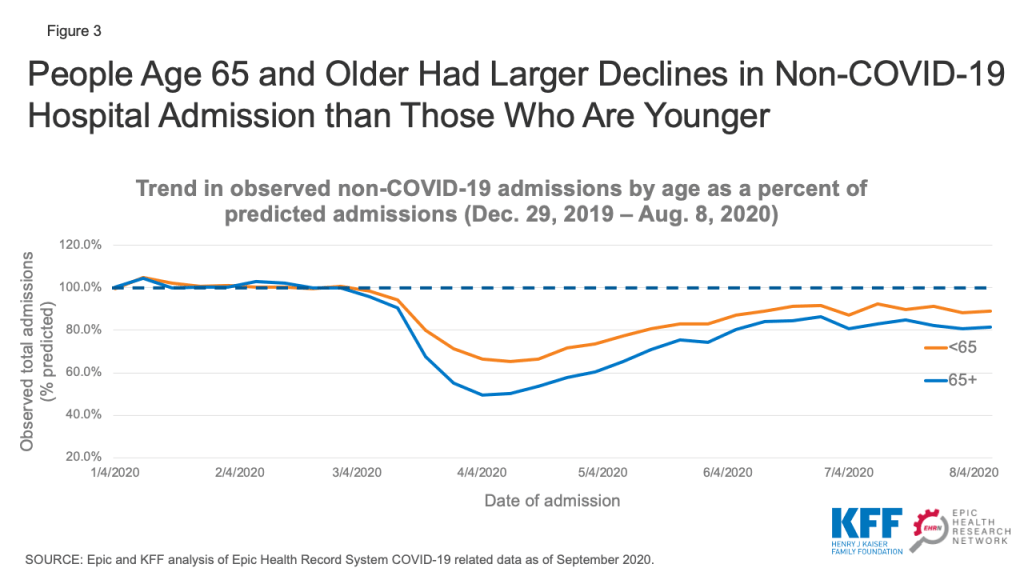
When looking specifically at non-COVID-19 admissions, people age 65 and older had about half as many admissions in late March and April compared to what was predicted. While their admissions have increased somewhat, they stabilized at approximately 80-85% of their predicted level in late July and early August—while admissions for people under age 65 were at about 90% of predicted levels during the same period.
This new analysis is based on electronic medical record (EMR) data from Epic Health Research Network (EHRN) and includes all inpatient hospital admission volume from Dec 31, 2017 to August 8, 2020, involving patients who either were discharged or died, as of September 13, 2020. Data are aggregated weekly and pooled from 27 health care organizations in the United States, representing 162 hospitals that span 21 states and cover 22 million patients. These states represent 67.0% of COVID-19 cases as of September 23, 2020 and also represent 66.5% of the U.S. population.1 Predicted volume was calculated using historical data from Dec 31, 2017 to Jan 25, 2020.2 COVID-19 admissions were identified as admissions with either a documented COVID-19 diagnosis (U07.01) or other respiratory diagnosis involving a patient who either had tested positive or presumptive positive for COVID-19 or received a COVID-19 diagnosis within 14 days of the admission.
Background and prior studies on 2020 health care trends
Several recent studies show that, beginning in March 2020, social distancing measures, concerns over hospital capacity, and fears of contracting COVID-19 led to sharp declines in health care spending.3 Across all health care services, not including pharmaceutical drugs, expenditures were down 38% in April 2020, compared to April 2019. More recently, overall spending on health care has started to rebound and, by June, spending was only 10% lower than the previous year.4
An earlier EHRN analysis of EMR data found similar patterns for emergency department visits for acute myocardial infarctions and stroke, with sharp declines followed by increases that brought those emergency department visits roughly back to expected rates. In late March to early April, the incidence of these conditions as reported in hospital emergency department records was down by 45% for AMIs and 38% for strokes.5 By the end of May, the weekly incidence of acute myocardial infarction admissions had returned to approximately 92% of the pre-pandemic trend (prior to March 13, 2020). Similarly, the incidence of emergency department visits for stroke returned to approximately 87% of the historical trend.6 Analysis of EMR data for breast, cervical, and colon cancer screenings showed an even sharper decline beginning in early March followed by an increase in screenings; even so, screening rates have remained far below 2019 levels.7 By mid-June, weekly volumes for these cancer type screenings remained roughly 30-35% lower than their pre-COVID-19 levels.
A recent analysis of outpatient office visits published by the Commonwealth Fund found that visits fell nearly 60% by early April and then increased, plateauing as of July at 10% below the pre-pandemic baseline.8 Another analysis of outpatient visits that included data through May 15, 2020 found that non-COVID-19 outpatient visits dropped by almost 40 percent by mid-April and then started to increase by mid-April.9 An analysis of data from 18 states that was published by the Health Care Cost Institute found similar patterns for childhood vaccinations and cancer screenings.10 A study published in September in Health Affairs used data from a national medical group specializing in hospital medicine to analyze hospital admissions.11 That study reported similar patterns to ours—with all medical admissions in April having declined by 34.1%, and by June/July they were 8.3% lower relative to baseline volume.
Trends in overall hospital admissions
Our analysis of EMR data shows a precipitous drop in hospital admissions starting the week of March 14, 2020, falling to a low of roughly 70% of predicted admissions by the week of April 11 (Figure 1)—just four weeks after the March 13, 2020 national emergency proclamation. Admissions gradually began to increase soon after that date and, by July 11, admissions were back to approximately 95% of their predicted level. More recently, total admissions dipped slightly and are now at about 90% of predicted levels.
Figure 1: Overall Admissions Decreased in March and April but Were Back at About 95% of Predicted Admissions by July 2020
The “lost” admissions between March 8 and August 8, 2020 account for 6.9% of the total number of admissions predicted during the 2020 calendar year. If the number of admissions remains at about 90% of predicted admissions (as they were on August 8) through the end of the year, total admissions will be 10.5% below predicted volume for the entire year. If there are new restrictions on non-emergency procedures in the latter part of 2020, the share of “lost” admissions likely will be higher.
Implications for hospital finances
This drop in admissions was not something that hospitals could have anticipated at the beginning of the year and suggests revenue losses that may be difficult for some hospitals to weather. Hospitals’ financial strength differs widely. One recent study found that the median hospital had enough cash on hand to pay its operating expenses for 53 days in 2018, but the 25th percentile hospital only had enough cash on hand for 8 days.12 Smaller hospitals and rural hospitals are among those most likely to face financial challenges in the wake of revenue loss related to COVID-19. These hospitals may be more likely to close or merge if they do not have the financial resources to make up for declines in revenue caused by the declines in admissions shown in our data.
Hospitals and other health care providers have qualified for various types of federal assistance during the coronavirus pandemic. However, much of this money was not targeted to safety net hospitals operating on narrow margins.13 Most notably, hospitals and other Medicare and Medicaid providers received grants from the $175 billion provider relief fund that is being distributed by the Department of Health and Human Services (HHS). Hospitals qualified for grants that were the equivalent to a minimum of 2% of revenue and on average received grants that amounted to about 5.6% of revenue.14 Hospitals that qualified for additional grants either qualified by seeing a high number of COVID-19 inpatients by June 10 or were children’s hospitals, rural hospitals and/or safety net hospitals. About $30 billion remains available for future grant allocations as of October 8, 2020.15 It is unclear how the Department of Health and Human Services will allocate that money. How declines in admissions translates into lost hospital revenue depends on the type of admissions that were missed and which insurers paid for those admissions. Private insurers typically reimburse at higher rates than Medicare or Medicaid, and reimbursement widely varies by type of admission.16
Hospitals and other providers that participate in traditional Medicare were also eligible for loans through the Medicare Accelerated and Advance Payment Programs, which are designed to help hospitals facing cash flow disruptions during an emergency. About 80% of the $100 billion in loans went to hospitals.17 Repayment for the loans was originally set to begin in August, but Congress later delayed when repayments would begin and extended the period for repayment.18
Hospitals are also receiving a 20% increase in inpatient reimbursement for COVID-19 patients during the current public health emergency. The Congressional Budget Office estimated that this change will increase Medicare spending by about $3 billion.19 Hospitals may also be eligible for loans being distributed by the Treasury department, the Federal Reserve, and Small Business Administration.
Implications for insurer finances
Health insurers, in contrast, may be benefiting financially from this decline in hospital admissions. Many insurers have been reporting large profits despite voluntarily eliminating cost sharing for patients with COVID-19.20 The Affordable Care Act’s (ACA) Medical Loss Ratio limits the share of premiums that insurers can keep for overhead and profit. This means that beneficiaries get a refund check from their insurer if it did not spend a sufficient share of premiums on health care costs for beneficiaries. Using preliminary data reported by insurers to state regulators and compiled by Market Farrah Associates, KFF estimated insurers will be issuing a total of about $2.7 billion in rebates across all markets in 2020—nearly doubling the previous record high of $1.4 billion last year.21
Trends in non-COVID-19 admissions
We used EMR data from EHRN to look specifically at non-COVID-19 admissions by patient sex, age and region. By looking specifically at non-COVID-19 admissions, we can more easily assess declines in the use of health care due to voluntary and mandatory delays in non-emergency care. This analysis does not include specific diagnoses or procedures to assess which types of admissions had the steepest declines. Declines in certain types of admissions—such as car crashes—may be explained by changes in habits due to the coronavirus pandemic. However, as discussed earlier in this paper, declines in cancer screenings suggest that the overall decline in admissions is also a sign of patients delaying or foregoing preventive care and therefore not starting necessary treatments. Some cancer treatments were also delayed earlier in the pandemic,22 although those treatments may now have resumed in many cases.
Non-COVID-19 admissions by sex
Non-COVID-19 admissions for both male and female patients dropped to about 60% of predicted admissions in April 2020 and then increased to roughly 85-90% of predicted admissions by the summer (Figure 2). On an absolute level, admissions for female patients remained about 20% higher than for male patients (data not shown). Much of this differential is likely due to women’s admissions for childbirth.
Figure 2: Males and Females Had Almost Identical Patterns of Changes in Non-COVID-19 Admissions
Non-COVID-19 admissions by age
We stratified the EHRN admissions data by age to assess trends in non-COVID-19 admissions for patients age 65 and older compared to younger patients. We found that admissions for patients age 65 and older was just 50-55% of predicted levels in April 2020, compared to 65-70% of predicted levels for younger patients (Figure 3). Admissions among patients age 65 and older have not rebounded as quickly as younger patients. Admissions for patients age 65 and older were at roughly 80% of their predicted level in late July and early August, while admissions for patients under age 65 were at approximately 90% of predicted levels during the same time period. Individuals age 65 and older may be more reluctant to schedule non-emergency procedures given that they are at higher risk of serious illness if infected with the coronavirus.23
The slower return to normal among older patients may lead to a change in hospitals’ payer mix. While patients age 65 and older typically have Medicare, the majority of younger patients have private insurance, which typically reimburses at a higher rate than Medicare.24 If hospitals experience an increase in the share of patients with private insurance, that could help mitigate some of the revenue declines they are likely to see from a drop in overall admissions.
Figure 3: People Age 65 and Older Had Larger Declines in Non-COVID-19 Hospital Admission than Those Who Are Younger
Non-COVID-19 admissions by region
We next examined how non-COVID-19 admission trends differed across geographic regions, using the regions defined by the U.S. Census Bureau. To give a sense of the geographic distribution of our dataset, admissions from the Northeast, Midwest, South, and West regions account for 22%, 37%, 28%, and 13% of overall admissions, respectively. Hospitals in the Northeast experienced the steepest decline in non-COVID-19 admissions, with those admissions decreasing to a low of roughly 50% of predicted admissions the week of April 11 (Figure 4). Admissions in the Northeast have since increased and were at 87% of predicted levels in early August. Hospitals in the Midwest followed a similar pattern but did not experience quite as steep an initial decline in admissions. In the South, where the number of cases increased in some states during the summer, there has been less of a rebound in non-COVID-19 admissions and those admissions were about 82% of predicted levels in early August. Hospitals in the West did not experience as large a decline in admissions, but also have not experienced as large of a rebound. By early August, admissions in the West were at about 83% of predicted levels.
Figure 4: Hospitals in the Northeast Experienced Steepest Initial Decline in Non-COVID-19 Admissions
Implications
This new analysis from the Epic Health Research Network provides additional insights into patterns of hospital admissions during the COVID-19 pandemic. This adds to a body of research showing the steep decline in admissions in the spring followed by a more recent rebound in admissions. By looking at the patterns in non-COVID-19 admissions, we can see how changes in behavior had a differential impact by region, age, and sex. If overall hospital admissions remain at or above 90% of predicted admissions, hospital revenues may stabilize at a somewhat sustainable level. However, if the coronavirus begins to spread more rapidly later in the fall and non-emergency procedures are once again delayed, it could have serious consequences both for hospitals’ financial stability and the health of patients.
Tyler Heist, Ph.D., and Sam Butler, M.D., are with the Epic Health Research Network. Karyn Schwartz, M.P.H., is with KFF.
The predictive model was based on data through Jan 25, 2020 because that was the first week with a reported COVID-19 case in the United States. We used a generalized additive model and fit it to weekly admission volume, combining long term trend, yearly seasonal, and holiday effects. Forecasts were then obtained for Jan 26, 2020 through Dec 26, 2020. ↩︎
Cynthia Cox, Rabah Kamal, and Daniel McDermott, “How have healthcare utilization and spending changed so far during the coronavirus pandemic?” Peterson-KFF Health System Tracker, Aug. 6, 2020.
↩︎
Cynthia Cox, Rabah Kamal, and Daniel McDermott, “How have healthcare utilization and spending changed so far during the coronavirus pandemic?” Peterson-KFF Health System Tracker, Aug. 6, 2020.
↩︎
Jeff Trinkl, and Owen Sizemore, “Return to Near Average Number of ED Visits for Acute MI and Strokes 12 Weeks Post COVID-19 Emergency Declaration,” Epic Health Research Network, July 7, 2020.
↩︎
Jeff Trinkl, and Owen Sizemore, “Return to Near Average Number of ED Visits for Acute MI and Strokes 12 Weeks Post COVID-19 Emergency Declaration,” Epic Health Research Network, July 7, 2020.
↩︎
Christopher Mast and Alejandro Munoz del Rio, “Delayed Cancer Screenings—A Second Look,” Epic Health Research Network, July 17, 2020.
↩︎
Ateev Mehrotra, Michael Chernew, David Linetsky, Hilary Hatch, David Cutler, and Eric C. Schneider, “The Impact of the COVID-19 Pandemic on Outpatient Visits: Changing Patterns of Care in the Newest COVID-19 Hot Spots,” Commonwealth Fund, August 13, 2020
↩︎
Engy Ziedan, Kosali I. Simon and Coady Wing, “Effects of State Covid-19 Closure Policy on Non-Covid-19 Health Care Utilization,” National Bureau of Economic Research, July 2020.
↩︎
Katie Martin, Daniel Kurowski, Phillip Given, Kevin Kennedy, Elianna Clayton, “The Impact of COVID-19 on the Use of Preventive Health Care,” Health Care Cost Institute, Sept. 9, 2020 ↩︎
John D. Birkmeyer, Amber Barnato, Nancy Birkmeyer, Robert Bessler, and Jonathan Skinner. “The Impact Of The COVID-19 Pandemic On Hospital Admissions In The United States.” Health Affairs September 24, 2020.
↩︎
Dhruv Khullar, Amelia M. Bond and William L. Schpero. “COVID-19 and the Financial Health of US Hospitals.” JAMA. 2020;323(21):2127–2128.
↩︎
Karyn Schwartz and Anthony Damico, “Distribution of CARES Act Funding Among Hospitals,” KFF, May 13, 2020.
↩︎
This was calculated using 2019 National Health Expenditure data to estimate total revenue. We assumed that hospitals received 50% of the $10.2 billion allocated to rural providers and assumed that hospitals did not get any of the $20 billion in Phase 3 funding.
↩︎
Karyn Schwartz and Jennifer Tolbert, “Limitations of the Program for Uninsured COVID-19 Patients Raise Concerns,” KFF, Oct. 8, 2020.
↩︎
Eric Lopez, Gary Claxton, Karyn Schwartz, Matthew Rae, Nancy Ochieng, and Tricia Neuman, “Comparing Private Payer and Medicare Payment Rates for Select Inpatient Hospital Services,” KFF, July 7, 2020; Eric Lopez, Tricia Neuman, Gretchen Jacobson and Larry Levitt, “How Much More Than Medicare Do Private Insurers Pay? A Review of the Literature,” KFF, April 15, 2020; MACPAC, “Medicaid Hospital Payment: A Comparison across States and to Medicare,” MACPAC, April 2017.
↩︎
Juliette Cubanski, Karyn Schwartz, Jeannie Fuglesten Biniek and Tricia Neuman, “Medicare Accelerated and Advance Payments for COVID-19 Revenue Loss: Time to Repay?” KFF, Aug. 7, 2020.
↩︎
CBO, “Preliminary Estimate of the Effects of H.R. 748, the CARES Act, Public Law 116-136, Revised, With Corrections to the Revenue Effect of the Employee Retention Credit and to the Modification of a Limitation on Losses for Taxpayers Other Than Corporations,” CBO, April 27, 2020.
↩︎
Reed Abelson, “Major U.S. Health Insurers Report Big Profits, Benefiting From the Pandemic,” New York Times, Aug. 5, 2020; KFF, “When Cost-Sharing Waivers for COVID-19 Treatment Expire for People with Private Insurance Plans,” KFF, Aug. 24, 2020.
↩︎
Rachel Fehr and Cynthia Cox, “Data Note: 2020 Medical Loss Ratio Rebates,” KFF, April 17, 2020.
↩︎
Eric Lopez, Gary Claxton, Karyn Schwartz, Matthew Rae, Nancy Ochieng, and Tricia Neuman, “Comparing Private Payer and Medicare Payment Rates for Select Inpatient Hospital Services,” KFF, July 7, 2020. ↩︎