Medicaid Changes in House and Senate Reconciliation Bills Would Increase Costs for 1.3 Million Low-Income Medicare Beneficiaries
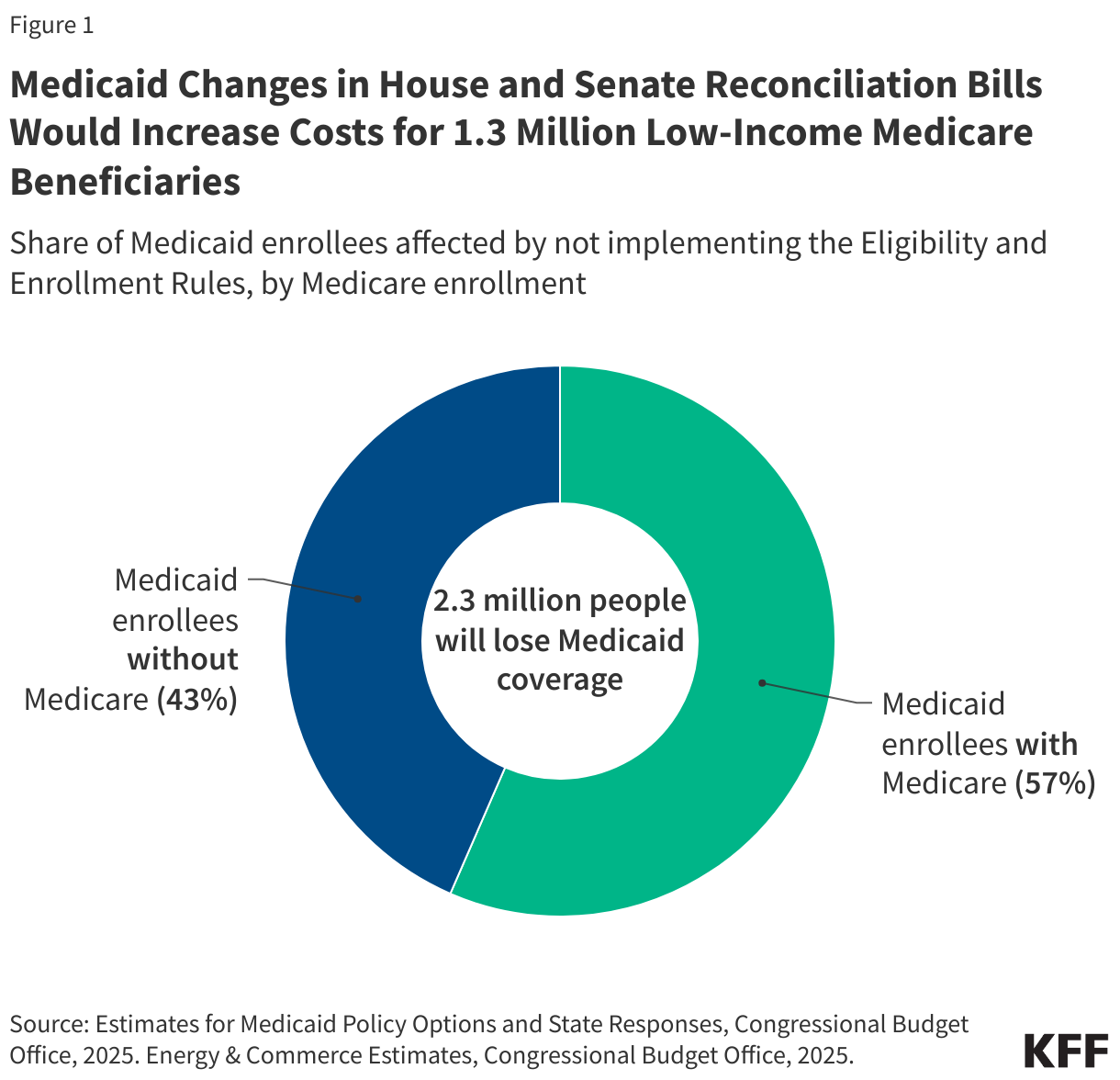
On May 22, the House passed a reconciliation bill, the One Big Beautiful Bill Act, which would partially pay to extend expiring tax cuts by cutting Medicaid. The Congressional Budget Office (CBO) estimates that the bill would reduce federal Medicaid spending by $793 billion over ten years and 10.3 million fewer people would be enrolled in Medicaid in 2034, including 1.3 million people with Medicare, otherwise known as “dual-eligible individuals”. The loss of Medicaid coverage for Medicare beneficiaries stems from delaying implementation of two rules that aimed to streamline the enrollment process and make it easier for people to maintain Medicaid coverage by reducing administrative barriers. Dual-eligible individuals would be disproportionately impacted by these provisions, comprising nearly 60% of the 2.3 million Medicaid enrollees who are estimated to lose coverage as a result of delaying these rules under the House reconciliation bill (Figure 1). Instead of placing a moratorium on implementation of the rules, the recently released Senate reconciliation language would prohibit nearly all of the provisions in the rules from ever being implemented.
Dual-eligible individuals have low incomes and modest savings. The 1.3 million people that would no longer have Medicaid if the eligibility and enrollment rules were not implemented would retain their primary health insurance coverage under Medicare, but lose Medicaid coverage of Medicare premiums, and in most cases, cost sharing, which are provided through Medicare Savings Programs (MSPs) administered by state Medicaid programs. Many would also lose coverage of Medicaid benefits that supplement their Medicare coverage, such as long-term care, dental services, and non-emergency medical transportation.
The loss of Medicaid coverage for Medicare beneficiaries stems from provisions in the House bill that would delay implementation of two Biden administration rules until 2035. The two rules that would be delayed under the House reconciliation bill were intended to make it easier for people to enroll in and maintain Medicaid coverage by minimizing administrative burden in the following ways.
- One rule aimed to reduce barriers to enrollment in the Medicare Savings Programs (MSPs), under which Medicaid pays Medicare premiums, and in most cases, cost sharing for low-income Medicare beneficiaries. Among other changes, the rule would automatically enroll Medicare beneficiaries with Supplemental Security Income (SSI) into the MSPs and would more closely align the MSP application to the application for Medicare’s Part D prescription drug Low-Income Subsidy (LIS).
- The second rule would more broadly streamline application, enrollment, and renewal processes in Medicaid. Among the changes most relevant for dual-eligible individuals are new requirements for states to assist applicants with procuring appropriate documentation to validate income and assets, a requirement to renew Medicaid coverage only once per year, and a prohibition on requiring in-person interviews as part of the application process
CBO estimates that delaying these two rules would reduce federal spending by $167 billion over 10 years, making this the second largest source of cuts to federal Medicaid spending in the bill. Illustrating why administrative burdens may make it hard for dual-eligible individuals to maintain Medicaid, prior KFF research finds that among people who newly become eligible for both Medicare and Medicaid, 28% lose Medicaid coverage within the first year despite living on fixed incomes.
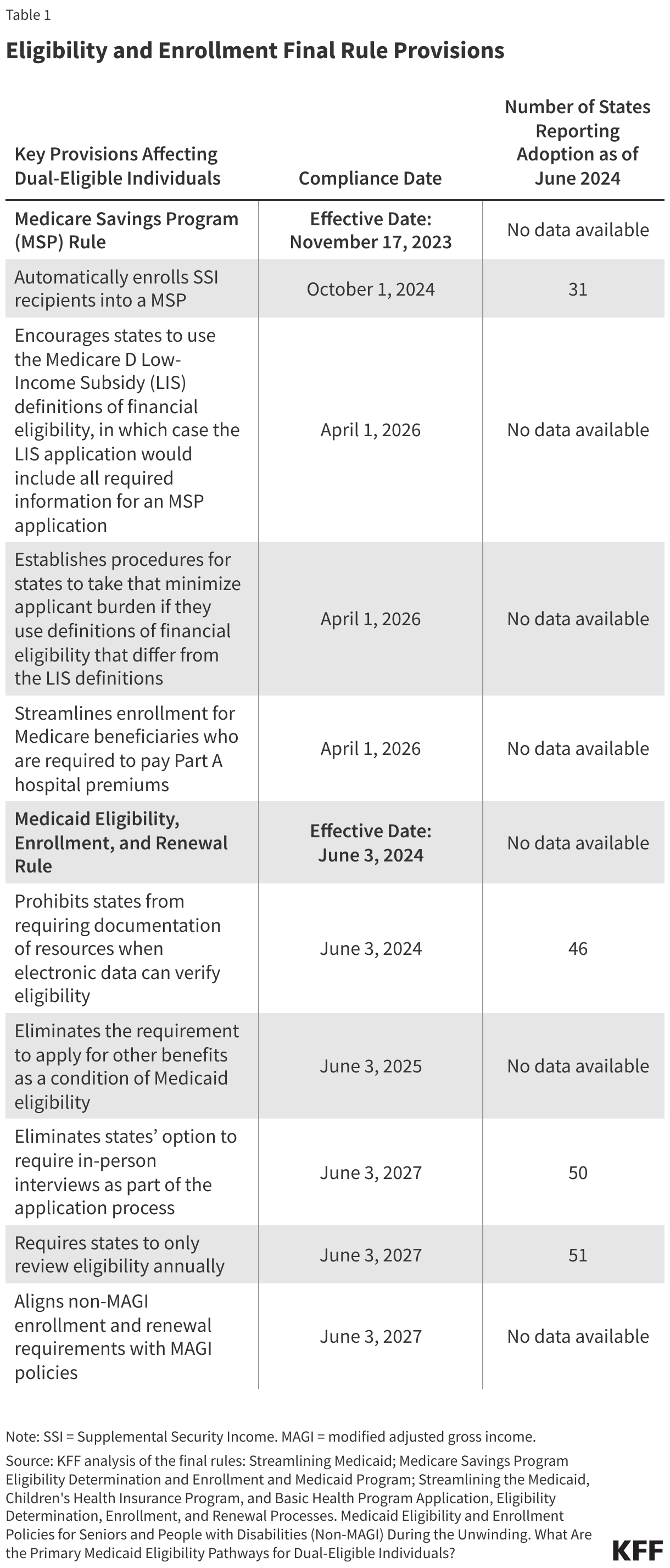
Although states have already implemented some of the rules’ provisions (Table 1), if the rules are delayed, it is expected that further implementation will cease and states may resume some practices that were prohibited under the rules. For example, 38 states report sending pre-populated renewal forms to Medicaid enrollees who qualify because they are ages 65 and older or have a disability, a practice they may discontinue if the rules are delayed. Alternatively, it’s possible that some states will reinstate requirements for applicants to submit paper documentation or report for in-person interviews. In a few cases, states will be required to reinstate application requirements or be prohibited from using more streamlined application processes.
Losing Medicaid coverage would substantially increase out-of-pocket costs for low-income Medicare beneficiaries. Because Medicare beneficiaries who qualify for Medicaid typically have very low incomes and little to no savings, the loss of Medicaid payment for the costs of Medicare’s premiums and cost sharing could make their Medicare coverage unaffordable. For example, the first rule would automatically enroll low-income Medicare beneficiaries who receive Supplemental Security Income (SSI) into a MSP. Without the MSP, such people must pay 20% of the $967 SSI monthly benefits for the $185 Medicare Part B monthly premium in 2025. (In order to qualify for SSI, individuals must have low incomes, limited assets, and either be over age 64 or have a qualifying disability.) This same individual would have additional out-of-pocket costs if they went to the doctor or were admitted to the hospital. Those additional out-of-pocket costs could discourage low-income beneficiaries from using health care and is the reason for CBO’s estimate that delaying implementation of the rules would reduce Medicare spending by $11 billion over 10 years.
Additionally, some of the 1.3 million Medicare beneficiaries expected to lose Medicaid under the House reconciliation bill may also lose subsidies that help pay for prescription drug premiums and cost sharing. Medicare beneficiaries with Medicaid are automatically enrolled in the Medicare Part D Low-Income Subsidy (LIS), which provides assistance with Part D prescription drug premiums and cost sharing. Illustrating the connection between Medicaid enrollment and LIS coverage, between December 2024 and January 2025, the number of LIS recipients decreased by 1 million, following Medicaid disenrollments that stemmed from the unwinding of the Medicaid continuous enrollment provision. Before the decline, LIS enrollment had been slowly but steadily growing over time.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
