5 Key Facts About Medicaid and Family Planning
Most women use contraception at some point in their lives and for low-income women in particular, Medicaid provides access to family planning services which include contraceptives as well as many preventive and primary care services related to sexual and reproductive health. Congress is considering changes to Medicaid that would reduce federal spending on the program and lead to an estimated 7.6 million people losing Medicaid coverage and becoming uninsured. As the largest public payer for family planning services in the US, changes to Medicaid, including reductions in enrollment, benefits, or the type of providers that can participate in the program could have a large impact on access to contraception and other family planning care for low-income individuals. Amid debates to limit federal Medicaid support, this brief presents five facts to know about Medicaid’s role for family planning.
1. Medicaid plays an outsize role providing coverage for low-income women of reproductive age.
Medicaid, the nation’s health coverage program for poor and low-income people, provides access to health and long-term care services for millions of low-income women across the nation. Nationally, Medicaid covers one in five adult women of reproductive age (18 to 49 years old), and more than four in ten (44%) with low incomes (Figure 1). Medicaid coverage of adult reproductive age women with low incomes ranges across the country, from roughly one in five in Texas (22%) to six in ten (61%) in New York and New Mexico.
The ACA’s Medicaid expansion plays a major role in the program’s coverage of reproductive age women. Nearly four in ten (38%) adult women of reproductive age who are enrolled in Medicaid are covered through the expansion pathway. Ten states have not expanded Medicaid under the ACA.

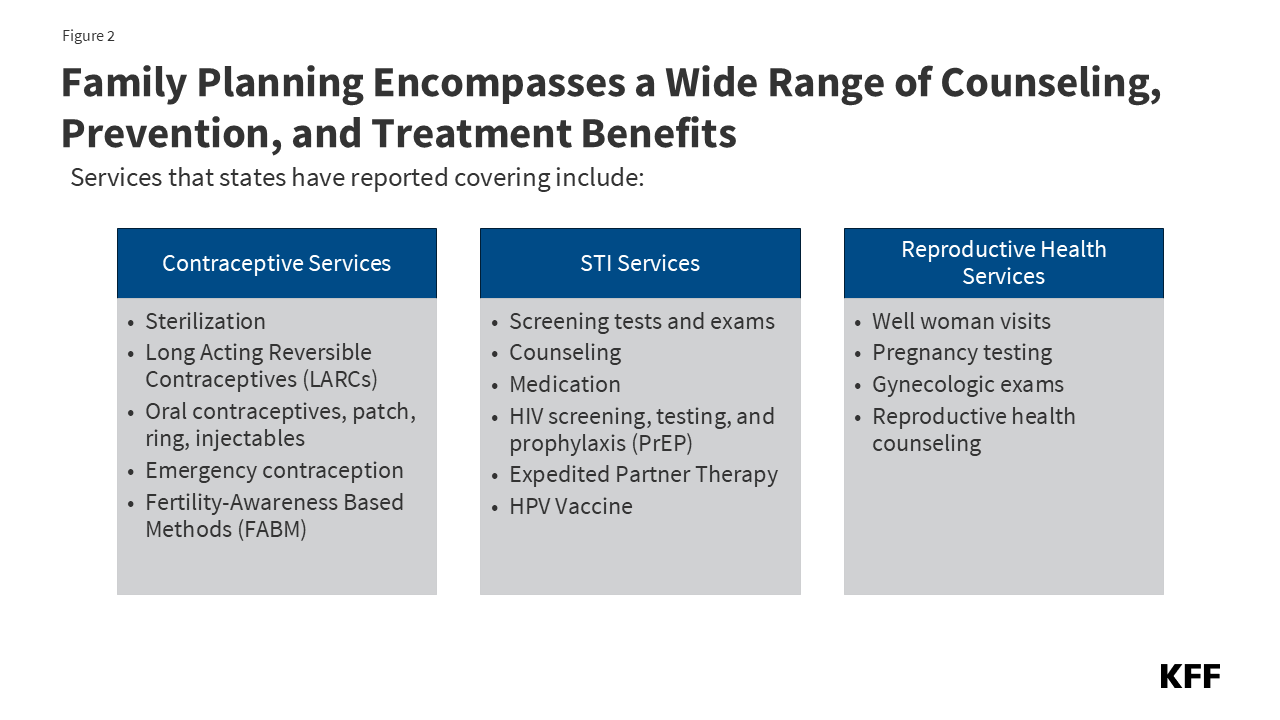
2. All state Medicaid programs cover family planning benefits, which include contraception as well as a broad range of preventive health services.
The Medicaid program has a long history of covering family planning as part of a comprehensive set of preventive services, and the federal government pays a higher federal match rate of 90% for family planning services than it does for other health care services. Federal Medicaid law classifies family planning services and supplies as a “mandatory” benefit category that states must cover, but it does not formally define the specific services that must be included, giving states flexibility in how they design the coverage. States routinely cover prescription contraceptives and related services such as gynecologic exams and testing and treatment for sexually transmitted infections (Figure 2).
Research has found that the ACA’s Medicaid expansion is associated with an increased use of the most effective long-acting contraceptives as well as use of contraception after having a baby.
3. Medicaid coverage supports access to consistent contraceptive care which reduces unintended pregnancies and alleviates cost barriers for women with low incomes.
Federal law prohibits states from imposing out-of-pocket charges for family planning care in Medicaid, an important cost protection for women with low incomes. According to a national survey on contraceptive experiences, one in five (20%) reproductive age women who were uninsured reported that they had to stop using contraception in the past year because of the cost, compared to 5% of women covered by Medicaid.
Nationally, about half of reproductive age women with Medicaid coverage obtained family planning services in 2021, and in some states (Figure 3), it is higher (59% in Ohio and 60% in Louisiana). The family planning benefit most commonly accessed by women with Medicaid was oral contraceptives, which are also the most used reversible contraceptive among women in the general population. Medicaid also covers intrauterine devices, contraceptive implants, sterilization procedures, and injectable contraceptives along with follow up care.

4. Many Medicaid enrollees seek family planning services at specialized family planning clinics that also offer abortion services, such as Planned Parenthood.
Congress is considering a proposal to ban Planned Parenthood and other Medicaid essential community providers from participating in the Medicaid program. The federal Medicaid statute allows Medicaid enrollees to seek care from any provider that is qualified and willing to participate in the program, and for family planning services specifically, federal law allows enrollees to seek services outside of managed care provider networks if they desire. Some Medicaid providers, including many Planned Parenthood clinics, offer both family planning services and abortion care. Medicaid reimburses these clinics for the family planning services they provide but does not pay for abortion care because of the Hyde Amendment’s ban on the use of federal funds for abortions (except in the cases of rape, incest, or life endangerment). The current reconciliation bill under consideration in Congress (and passed by the House) would prohibit Planned Parenthood and some other family planning clinics that also provide abortion services from participating in the program and getting reimbursed for serving Medicaid patients. While the reconciliation bill seeks to reduce federal spending, the restriction on Medicaid payments to Planned Parenthood is a priority of Republican leaders and has been included in the reconciliation bill despite the fact that the Congressional Budget Office projects the provision would raise federal spending by $300 million.
Medicaid accounts for a major share of Planned Parenthood clinics’ financing. Excluding these clinics from Medicaid would likely result in many clinic closures and could lead to provider shortages in areas where they have a larger presence. Nationally, one in ten (11%) female Medicaid enrollees ages 15 to 49 who received family planning services went to a Planned Parenthood clinic in 2021, with larger shares in some states – as high as 29% in California (Figure 4). In some areas, there may not be other safety-net providers to absorb the patients Planned Parenthood currently serves. In other areas, existing clinics may not have the capacity to provide the same scope of care that family planning clinics, like Planned Parenthood, offer. KFF research has found that specialty reproductive health care clinics such as Planned Parenthood clinics offer a broader range of services to their patients compared to non-specialized clinics. In 2013, Texas replaced its Medicaid family planning program with a state-funded program that excluded Planned Parenthood as a participating provider. Following the change, there was a sizable drop in Medicaid claims for contraceptives and an increase in Medicaid-funded births.

5. More than half of states have established programs that use Medicaid coverage to pay for family planning services for people who are uninsured.
To help address gaps in coverage, several states extend Medicaid coverage for family planning services to people who do not qualify for full Medicaid benefits (usually because their incomes exceed the state income eligibility thresholds or they do not otherwise qualify for Medicaid). States can establish these family planning programs as a State Plan Amendment or through a Section 1115 waiver (Figure 5). States have the latitude to decide which services they cover in these limited scope family planning programs, though pharmacy coverage is restricted to family planning and related services. Nationally, 31 states provide family planning coverage to individuals who do not qualify for full Medicaid benefits. In 26 states, eligibility for the program is based solely on meeting certain income requirements, while eligibility in four states is limited to people who lose Medicaid for any reason (1 state) or lose Medicaid postpartum coverage (3 states). Most of the states (23) provide coverage to men as well as women.

