A Continuing Saga: Ending Abortion Restrictions in States with Constitutional Protections
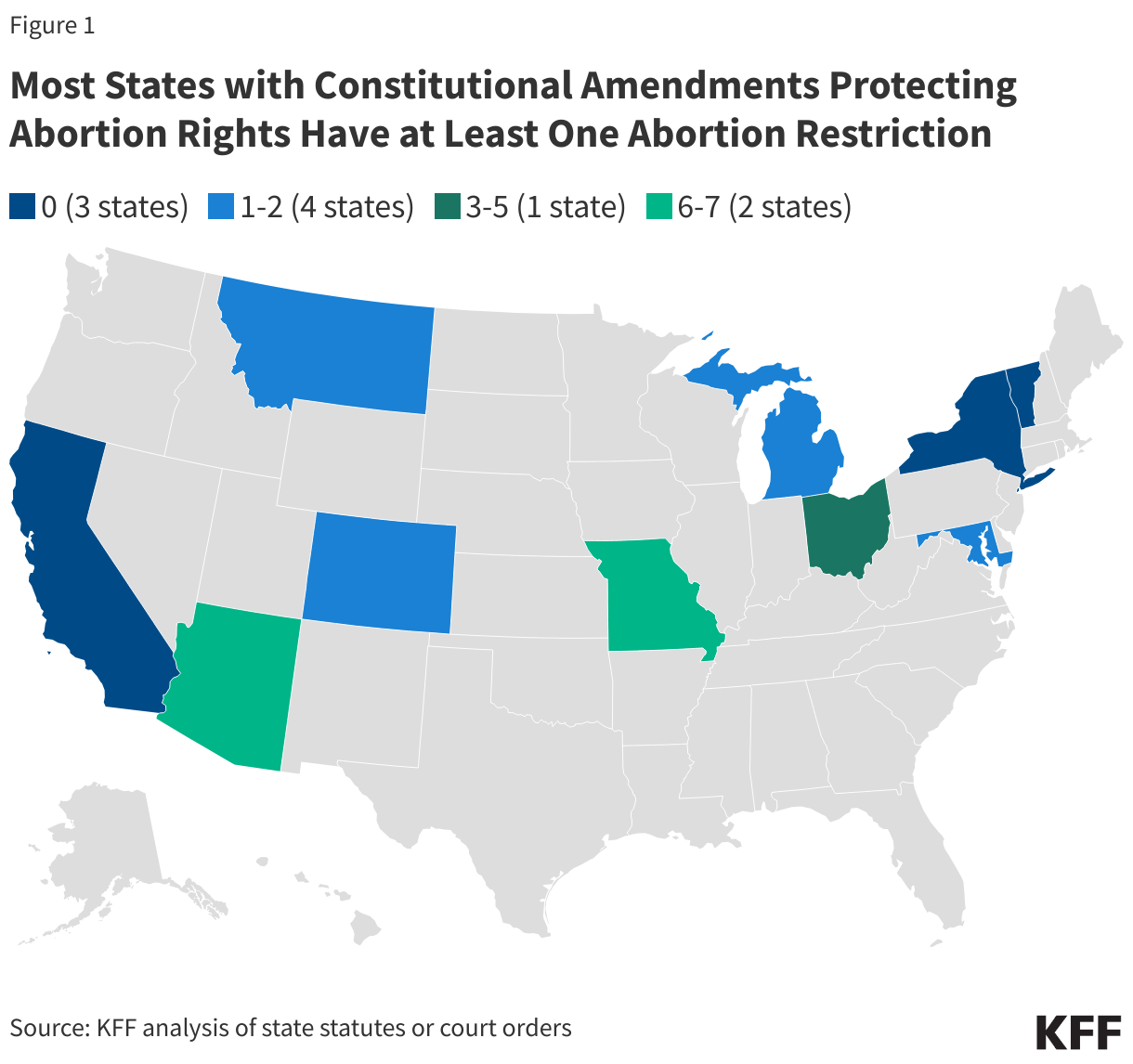
Since the Supreme Court overturned Roe v. Wade in June 2022, states have been able to set policy that defines abortion access across this nation. In the past three years, voters in 10 states have passed constitutional amendments to protect abortion rights. These amendments, however, do not automatically invalidate the states’ laws restricting abortion such as waiting periods, coverage bans, and ultrasound requirements. The restrictions need to be challenged in court before they can be invalidated. This process can take years, and in states with new constitutional protections, people seeking abortion care may still face access restrictions while the litigation proceeds. Additionally, in some instances, after courts have blocked restrictions, conservative state legislatures have passed laws enacting very similar restrictions, lengthening the process to block these laws, since advocates have to challenge multiple state laws or amend already-existing challenges to block the newly passed laws. This policy watch provides an update on the status of abortion restrictions in states that passed a constitutional amendment protecting abortion, or where a state court previously interpreted the state constitution as protecting abortion access.
Status of Litigation Based on Recent Constitutional Amendments
In four states with recently passed constitutional amendments protecting the right to abortion or a broader right to reproductive freedom — Arizona, Michigan, Missouri, and Ohio – advocates have filed lawsuits seeking to block abortion restrictions, alleging that these restrictions violate the newly passed constitutional amendments. These lawsuits test the reach of these constitutional amendments beyond pre-viability gestational limits. In Montana, another state that recently passed a constitutional amendment, abortion providers are also challenging prior abortion restrictions, but because this challenge was filed before the state’s constitutional amendment passed, they are relying on previous state supreme court precedent to make their arguments. Advocates in Alaska and Kansas, where there is no specific constitutional amendment protecting abortion, have challenged restrictions based on state supreme court cases finding abortion is protected in the state constitution.
Whether or not the restrictions that are being challenged will be permanently blocked depends on how each respective state’s supreme court interprets the state constitution’s right to abortion. The language of the constitutional amendments varies and some might provide greater protections than others (Table 9). States that rely on state supreme court precedent protecting a right to abortion—as opposed to a constitutional amendment explicitly protecting this right—may provide protections today, but future courts may overturn that precedent, much like the U.S. Supreme Court did with Roe v. Wade.
The following section provides an overview of the status of legal challenges to abortion restrictions in states with recently passed constitutional amendments or litigation that has found that the state constitution protects abortion rights.
Arizona
The Arizona constitutional amendment – passed in November 2024 – protects a fundamental right to abortion and forbids the state from enacting, adopting, or enforcing any law that “denies, restricts or interferes with that right before fetal viability unless justified by a compelling state interest that is achieved by the least restrictive means.” Currently, the gestational limit in the state is fetal viability. However, there are other restrictions that are still in effect.
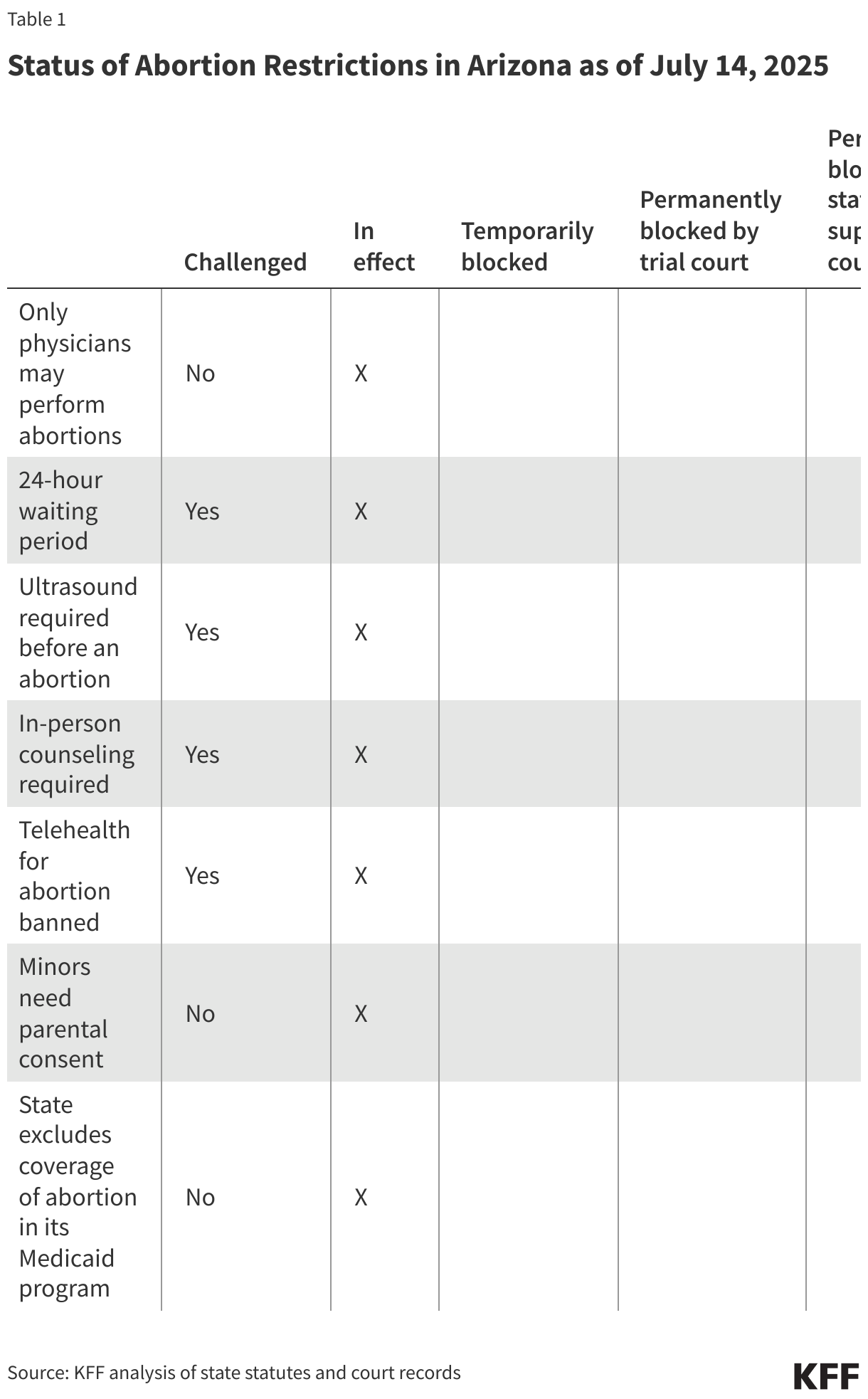
Abortion rights advocates in Arizona filed a lawsuit in May 2025 challenging the in-person counseling requirement, 24-hour waiting period, ultrasound requirement, and ban on the use of telehealth for abortion care. The state court where this challenge was filed is yet to issue a ruling.
Michigan
In November 2022, voters passed a constitutional amendment in Michigan that protects a fundamental right to reproductive freedom, the right to make decisions regarding pregnancy, including the right to abortion, among others. It states that “[a]n individual’s right to reproductive freedom shall not be denied, burdened, nor infringed upon unless justified by a compelling state interest achieved by the least restrictive means.”
The state has no gestational limit on abortion, however, a state funding ban on abortion funding for Medicaid enrollees and a parental consent requirement are still in effect.
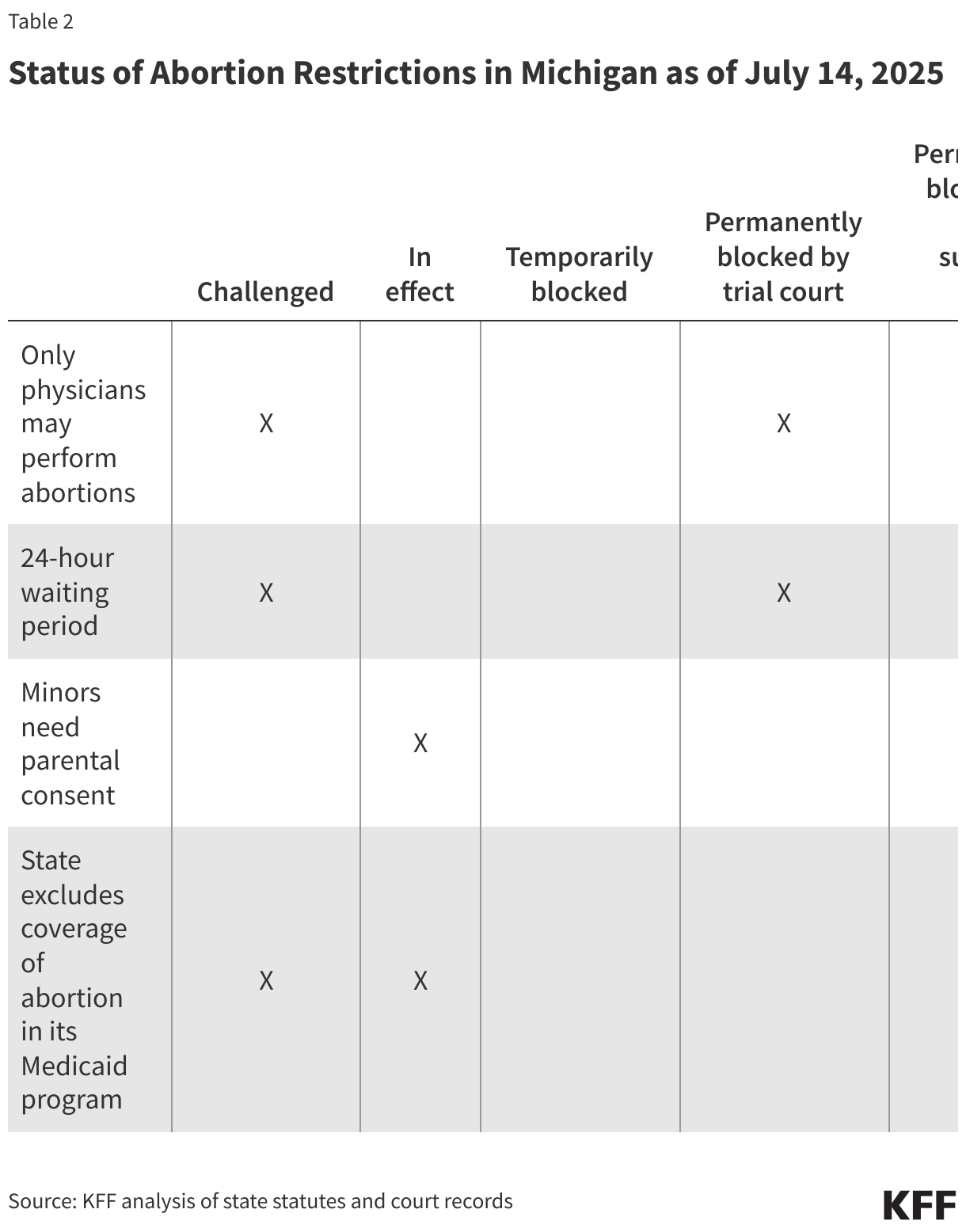
In two separate lawsuits, advocates in Michigan are challenging the exclusion of abortion coverage from the state’s Medicaid program and laws requiring a 24-hour waiting period and limiting abortion provision to physicians. A trial court recently ruled that the latter two requirements are unconstitutional and blocked them permanently. However, the state’s supreme court is yet to rule on these restrictions.
Missouri
In November 2024, voters in Missouri passed a constitutional amendment protecting a fundamental right to reproductive freedom, including the right to make decisions about abortion care. The amendment states that this right “shall not be denied, interfered with, delayed, or otherwise restricted unless the Government demonstrates that such action is justified by a compelling governmental interest achieved by the least restrictive means. Any denial, interference, delay, or restriction of the right to reproductive freedom shall be presumed invalid.” Currently, the gestational limit in the state is fetal viability, but other restrictions are still in effect.

Several clinics in Missouri filed a lawsuit alleging that the state’s pre-viability bans as well as many restrictions violate the state’s newly granted constitutional right to reproductive freedom. In December 2024, a Missouri state trial court sided with the clinics, and blocked the state’s pre-viability abortion bans, as well as many of the restrictions, while the litigation continues. However, in late May 2025, the Missouri Supreme Court lifted the preliminary injunction for the restrictions, and ordered the trial court to use a more strenuous test to determine if the plaintiffs meet the bar for a preliminary injunction. When restrictions went back into effect, clinics stopped providing abortion care, even though the total ban was not in effect. The case went back before the trial court, where the judge reviewed the request for a preliminary injunction using the standard set forth by the state supreme court and in response issued an order on July 3, 2025 blocking once again the state’s pre-viability ban and some restrictions, including the 72-hour waiting period. The state has appealed this order to the Missouri Supreme Court.
Ohio
The Ohio constitution was amended by voter initiative in November 2023 protecting the right to make and carry out reproductive decisions, including decisions about abortion care. Per the amendment, “[t]he State shall not, directly or indirectly, burden, penalize, prohibit, interfere with, or discriminate against… the exercise of this right, unless the State demonstrates that it is using the least restrictive means to advance the individual’s health in accordance with widely accepted and evidence-based standards of care.”
Currently, the gestational limit in the state is 22 weeks LMP (last menstrual period), however, are other restrictions are still in effect or temporarily blocked.
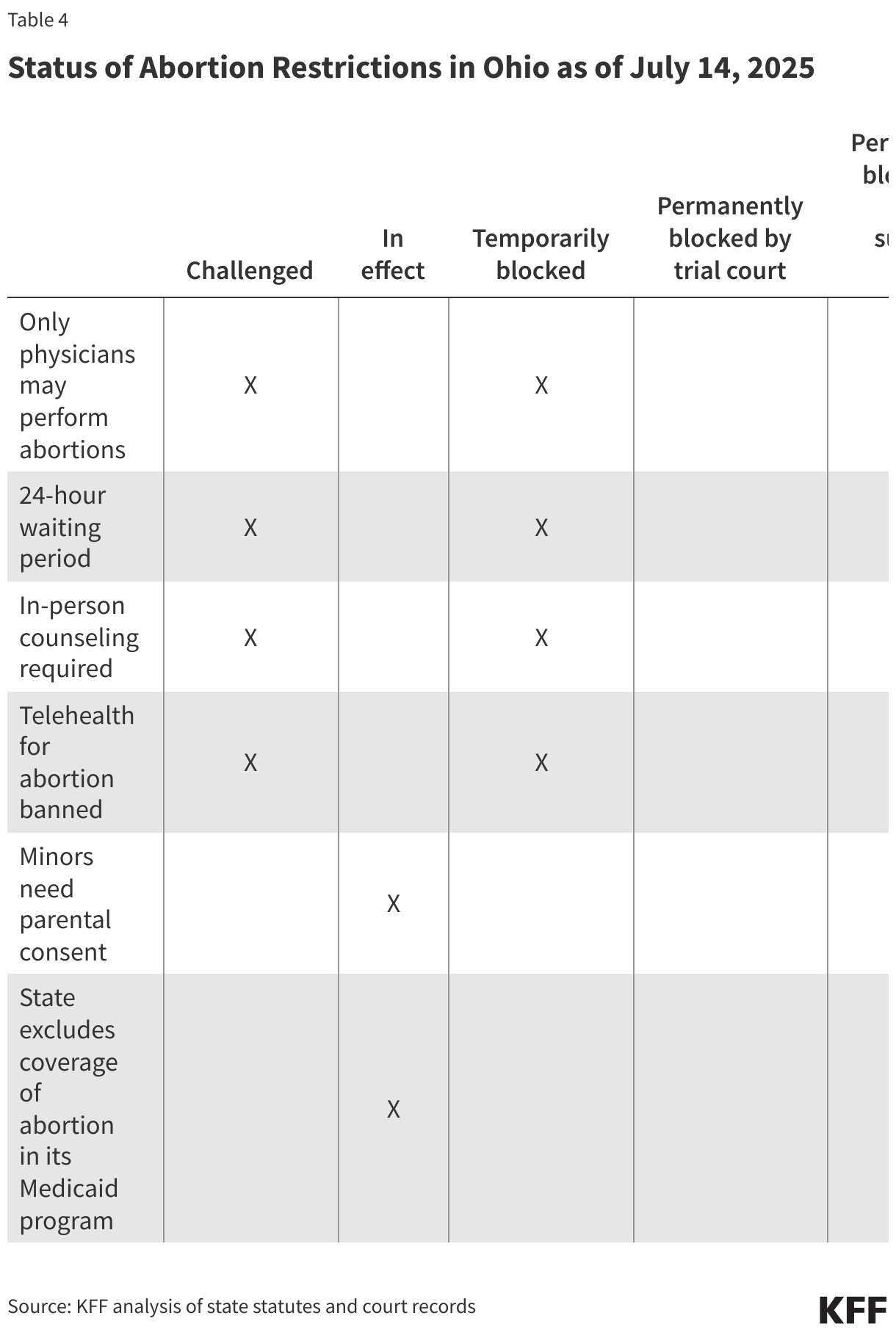
In two different lawsuits, abortion providers in Ohio challenged the 24-hour waiting period, the in-person counseling appointment, the telehealth abortion ban, and a law that limits the provision of abortion care to physicians. Abortion providers used the state’s constitutional amendment as the basis for these challenges. In both of these lawsuits, the trial courts have temporarily blocked the challenged restrictions while litigation proceeds. After the constitutional amendment was passed by voters, some Ohio legislators sought to curtail judges’ ability to block these laws and interpret the constitutional amendment, but these efforts did not progress.
Status of Litigation in States with State Supreme Court Precedent Protecting the Right to Abortion
Alaska
In 1997, the Alaska Supreme Court found that the state constitutional right to privacy protects the right to abortion. The state has no gestational limit on abortion, however, other restrictions are still in effect.

Advocates in Alaska are challenging a law that limits abortion provision to physicians, using previous state supreme court precedent as the basis for their challenge. This requirement was originally blocked by a preliminary injunction in 2021 and in September 2024, a state trial court ruled that the requirement violates the constitutional protection for the right to abortion.
Kansas
In 2019, the Kansas Supreme Court found that the Kansas Bill of Rights includes the right to abortion. The gestational limit in the state is 22 weeks LMP (last menstrual period), other restrictions are still in effect.

In Kansas, advocates are challenging a 24-hour waiting period law that is temporarily blocked due to a court order while litigation proceeds and a law banning advanced practice registered nurses from providing medication abortion care. Advocates in Kansas have also used Kansas Supreme Court precedent to successfully challenge laws that limit the provision of abortion care to physicians and require ultrasounds before an abortion, as well as in-person dispensing of medication abortion.
Montana
In 1999, the Montana Supreme Court found that the state constitution protects the right to abortion. In 2024, the Montana Supreme Court reaffirmed this protection.
In addition, voters approved an amendment in November 2024 recognizing an individual’s right to make decisions about pregnancy, including the right to abortion. It states that “[t]his right shall not be burdened unless justified by a compelling government interest achieved by the least restrictive means.”
The gestational limit in the state is fetal viability, however, a state parental consent law is still in effect.
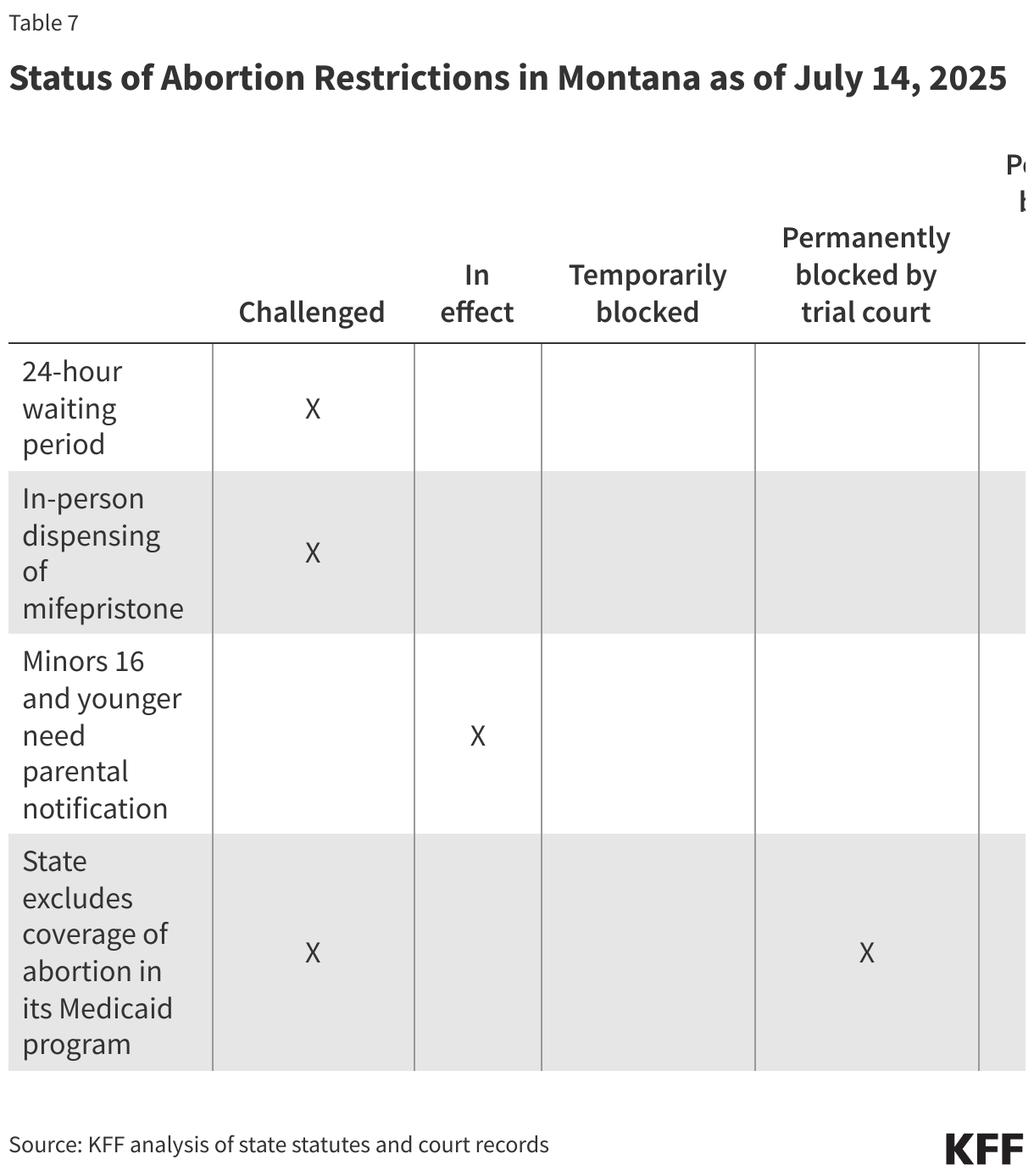
Abortion providers in Montana are challenging a law that excluded abortion coverage from the state’s Medicaid program, relying on previous Montana Supreme Court precedent that held that the state constitutional protection for privacy includes a protection for the right to abortion, instead of relying on the state’s newly passed constitutional amendment, since the challenge was underway before the constitutional amendment passed. In March 2025, a trial court ruled that this restriction is unconstitutional and permanently blocked it. Additionally, the Montana Supreme Court recently concluded in a different case that was also brought by abortion providers, that restrictions including an in-person dispensing requirement, a 24-hour waiting period, and a ban on telemedicine for abortion were unconstitutional. These restrictions are no longer in effect.



