A Closer Look at the Work Requirement Provisions in the 2025 Federal Budget Reconciliation Law
Note: This analysis was updated to include the Congressional Budget Office’s (CBO) latest cost estimates for the reconciliation package that was enacted on July 4, 2025, as well as new provisions in the law.
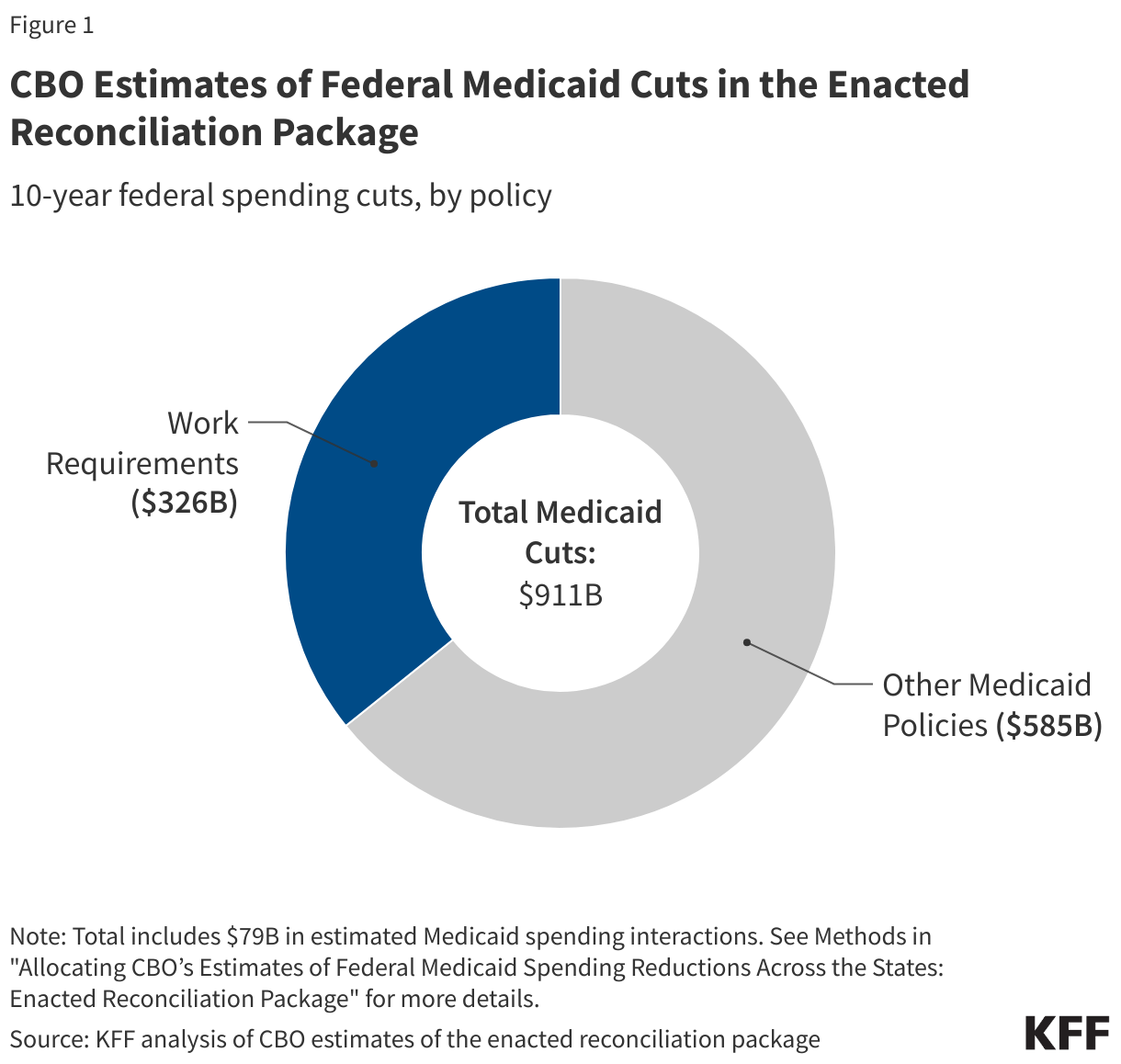
On July 4, President Trump signed into law a budget reconciliation package once called the “One Big, Beautiful Bill” that includes significant changes to the Medicaid program. The Congressional Budget Office (CBO) estimates the Medicaid work requirement provisions in the passed budget reconciliation law will be the largest source of Medicaid savings, reducing federal spending by $326 billion over ten years and cause millions to become uninsured.
Implementing work requirements on a national scale, requiring states to verify individuals’ monthly work status (at least every 6 months) and implement a long list of exemptions are policies that proved challenging for Arkansas and Georgia to operationalize and led to 18,000 people losing coverage in Arkansas. KFF analysis shows most Medicaid adults under age 65 are working already (without a requirement) or face barriers to work. Many Medicaid adults who are working low-wage jobs are employed by small firms and in industries that have low employer-sponsored insurance offer rates. In previous analysis, CBO found that a Medicaid work requirement would not have any meaningful impact on the number of Medicaid enrollees working, and cited research from Arkansas indicating that “many participants were unaware of the work requirement or found it too onerous to demonstrate compliance,” resulting in coverage loss.
The law will require states to condition Medicaid eligibility for adults in the Affordable Care Act (ACA) Medicaid expansion group at application and following enrollment on meeting work requirements starting January 1, 2027, with the option for states to implement requirements earlier. Currently, 41 states (including DC) have expanded their Medicaid programs under the ACA to nearly all adults up to 138% FPL ($21,597 for an individual in 2025). As of June 2024, over 20 million people were enrolled through Medicaid expansion, representing nearly a quarter of total Medicaid enrollment across all states and 31% of total enrollment in expansion states. The Medicaid expansion population includes adults without dependents as well as many parents and people with disabilities or chronic conditions who do not receive SSI.
Key takeaways include:
- CBO estimates. Of the Medicaid provisions included in the law, CBO estimates implementing work requirements will account for the largest share of federal Medicaid savings. Earlier CBO estimates found work requirements will cause the largest increase in the number of people without health insurance.
- Verification requirements. The law requires states to verify at application and at renewal that individuals in the ACA expansion group meet work requirements (80 hours of work activities per month) or exemption criteria. States can also require verification more frequently.
- Implementation timeline. The law requires HHS to release an interim final rule by June 2026 leaving states with limited time to develop or change implementation plans, protocols, and systems (and to test systems changes) before the January 2027 work requirement implementation deadline.
- State implementation choices. State choices to impose more stringent requirements than the minimum federal requirements outlined in the law (e.g., requiring more frequent verification or imposing longer “look-back” periods when verifying coverage) as well as state effectiveness in using existing data to automate verification processes, will affect the number of individuals at risk of losing coverage.
- Comparison to other waivers and proposals. The Medicaid work requirement policies included in the law are more stringent than previous policies considered by Congress and work requirements implemented under state Medicaid demonstration waivers; for example, the law makes it harder to gain coverage and to re-enroll and does not exempt older adults from requirements
What does CBO say?
Of the Medicaid provisions included in the enacted reconciliation package, CBO estimates implementing work requirements will account for the largest share of federal Medicaid savings; earlier CBO estimates also found work requirements will cause the largest increase in the number of people without health insurance. Over ten years, work requirements are estimated to reduce federal Medicaid spending by $326 billion, representing the largest share of the estimated $911 billion in total Medicaid cuts included in the law (Figure 1). (CBO also projects indirect effects from the work requirement provision will decrease federal revenues by $8.65 billion over a decade.) The savings will largely stem from coverage losses. CBO has not published updated estimates of the number of people who will lose Medicaid under the reconciliation package previously referred to as the “One Big, Beautiful Bill.” Earlier CBO analysis of the House-passed version of the reconciliation bill estimated 18.5 million people will be subject to the requirements each year and by 2034 federal Medicaid coverage will decrease by an estimated 5.2 million adults, with work requirements ultimately increasing the number of people without health insurance by 4.8 million in 2034. CBO expects few of those disenrolled to have access to employment-based coverage and that no one will be eligible for Marketplace premium tax credits (as the law makes those losing or denied Medicaid coverage due to work requirements ineligible for premium tax credits to purchase coverage through the ACA Marketplaces).
What does the law require?
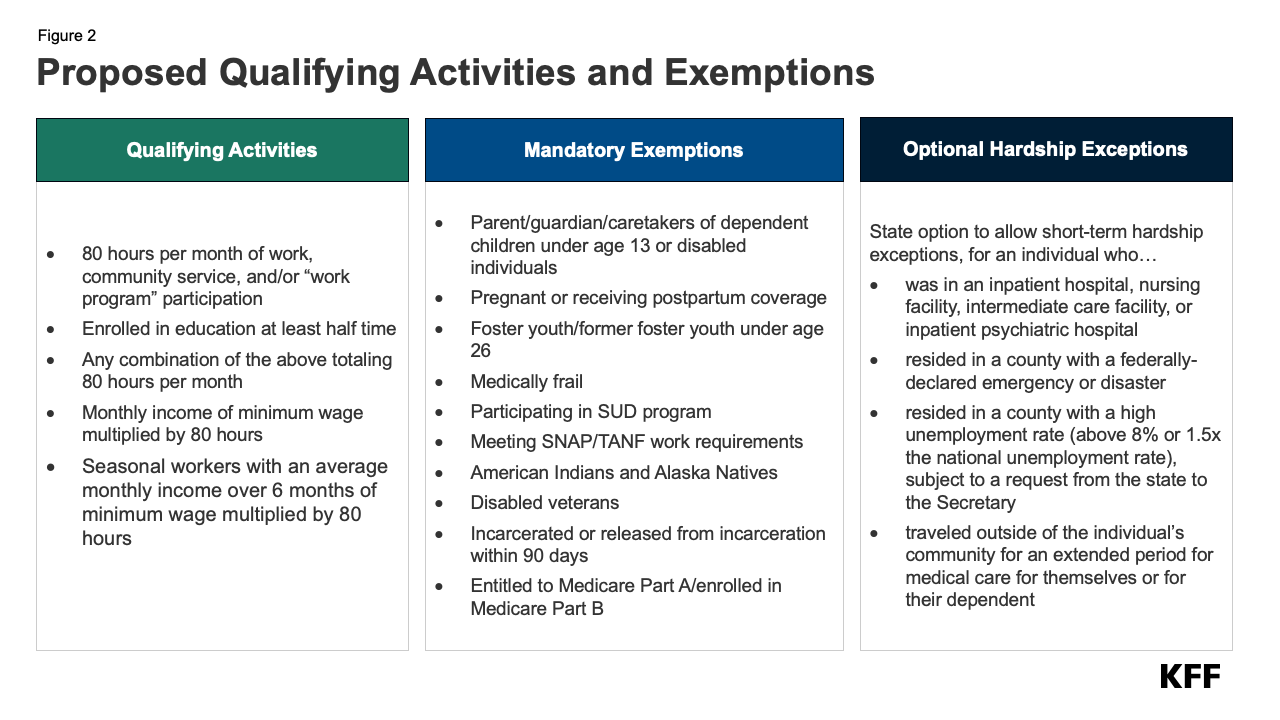
Expansion adults will be required to complete 80 hours of work or community service activities per month or meet exemption criteria to enroll in and maintain coverage (Figure 1). (Work requirements will also likely apply to states like Wisconsin and Georgia that have partial adult coverage expansions under 1115 waivers.) Individuals applying for coverage and those enrolled in coverage will need to work or engage in specified “qualifying activities” for at least 80 hours per month. States will be required to verify qualifying activities or exemptions in (at least) the month before application and (at least) one month between eligibility redeterminations (see Figure 2 and additional discussion below). The law specifies mandatory exemptions including parents and caretakers with children ages 13 and under, individuals who are “medically frail,” and individuals who are pregnant or postpartum, among others (Figure 1). The “medically frail” designation includes individuals who are blind or disabled, individuals with physical, intellectual, or developmental disabilities, individuals with substance use disorder or a “disabling” mental disorder, and those with “serious or complex” medical conditions. States may allow short-term hardship exceptions from work requirements, for enrollees (or applicants) experiencing certain extenuating circumstances (Figure 2).
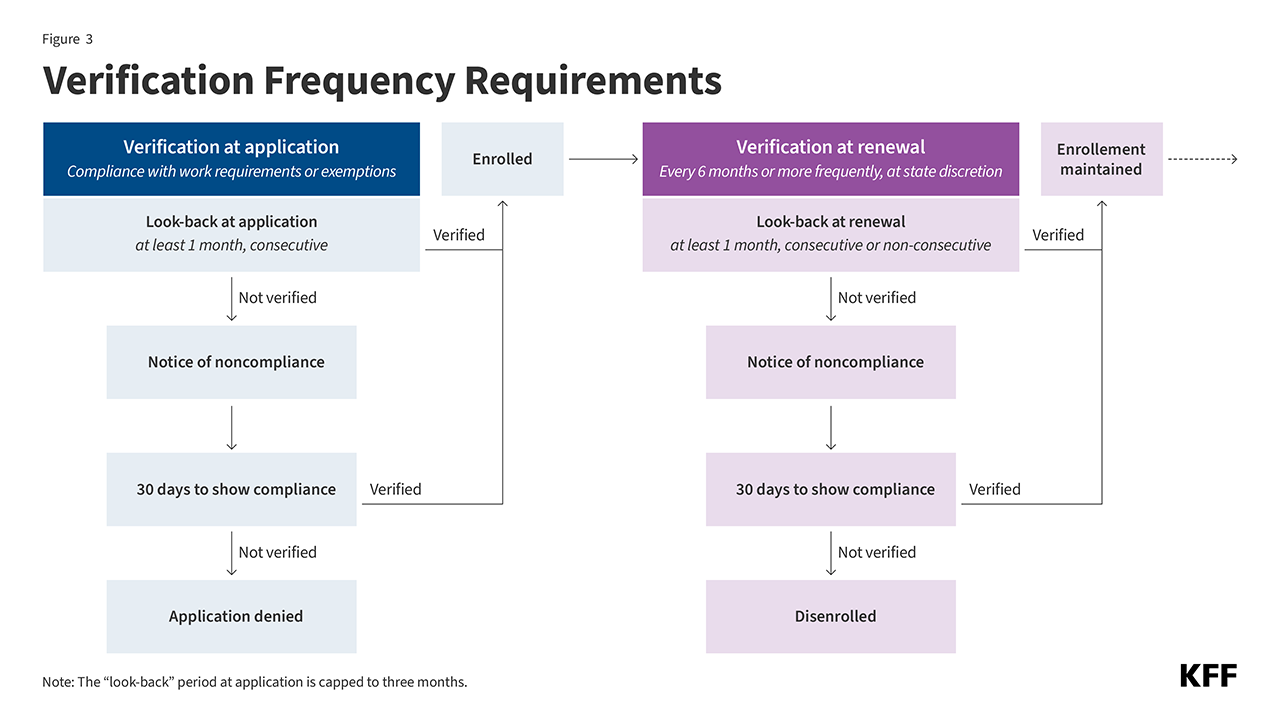
At a minimum, states will be required to verify individuals’ work or exemption status when individuals apply for coverage and at eligibility renewal (Figure 3). At application, states will be required to “look back” one or more consecutive months (immediately preceding the application month, up to three total months) to confirm compliance with the requirements. Every six months when eligibility is redetermined (or more frequently as determined by states), states will be required to “look back” one or more months (consecutive or non-consecutive) to verify compliance. In effect, states could require individuals to comply with work requirements for multiple months before they can enroll in coverage or for multiple months within any six-month eligibility period (or more frequently than every six months). The law directs states to use available information (e.g., payroll data) “where possible” to verify compliance with work activities or exemption status, without requiring additional documentation from individuals.
When a state is unable to verify compliance with the requirements or that an individual meets exemption criteria, it must issue a “notice of noncompliance” and deny the application or disenroll the individual from coverage if the individual is unable to show compliance (Figure 3). Individuals will have 30 days to show compliance (coverage will be maintained during this period if already enrolled). After 30 days, if an individual is unable to demonstrate compliance with the requirements or show they are exempt, the state will be required to deny the application or disenroll the individual from coverage (no later than the end of the month following the 30-day period). States will be required to follow standard Medicaid termination processes, including determining whether an individual qualifies for Medicaid coverage on another basis and provide written notice and opportunity for a fair hearing. To regain Medicaid coverage, individuals will need to reapply (triggering another compliance check at application). Individuals will also be barred from receiving subsidized Marketplace coverage, as the law makes those losing (or denied) Medicaid coverage due to work requirements ineligible for premium tax credits to purchase coverage through the ACA Marketplaces.
What is the timeline for implementation?
The law specifies key work requirement implementation and compliance dates (Figure 4). The law directs the Secretary of HHS to issue an interim final rule on implementing work requirements by June 1, 2026 (the law specifies the interim rule will not be subject to public notice or public comment). States will be required to condition Medicaid expansion eligibility and coverage on meeting work requirements by January 1, 2027, with an option to implement requirements sooner. States must begin outreach to notify individuals of the new requirements at least three months before the start of the first compliance “look-back” period and notify individuals “periodically thereafter.” The law allows the Secretary to exempt states from compliance with the new requirements until no later than December 31, 2028, if the state is demonstrating a “good faith” effort to comply.
Figure 4
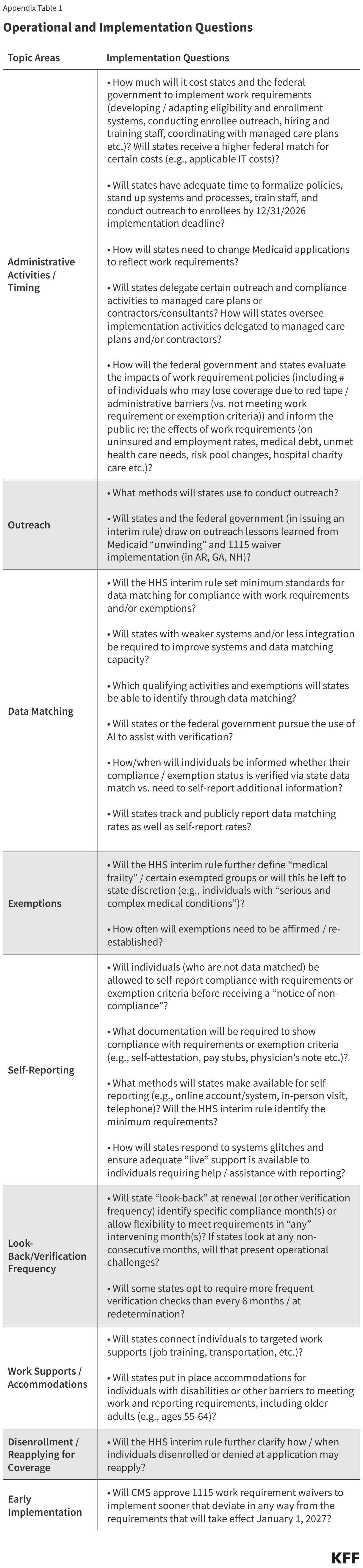
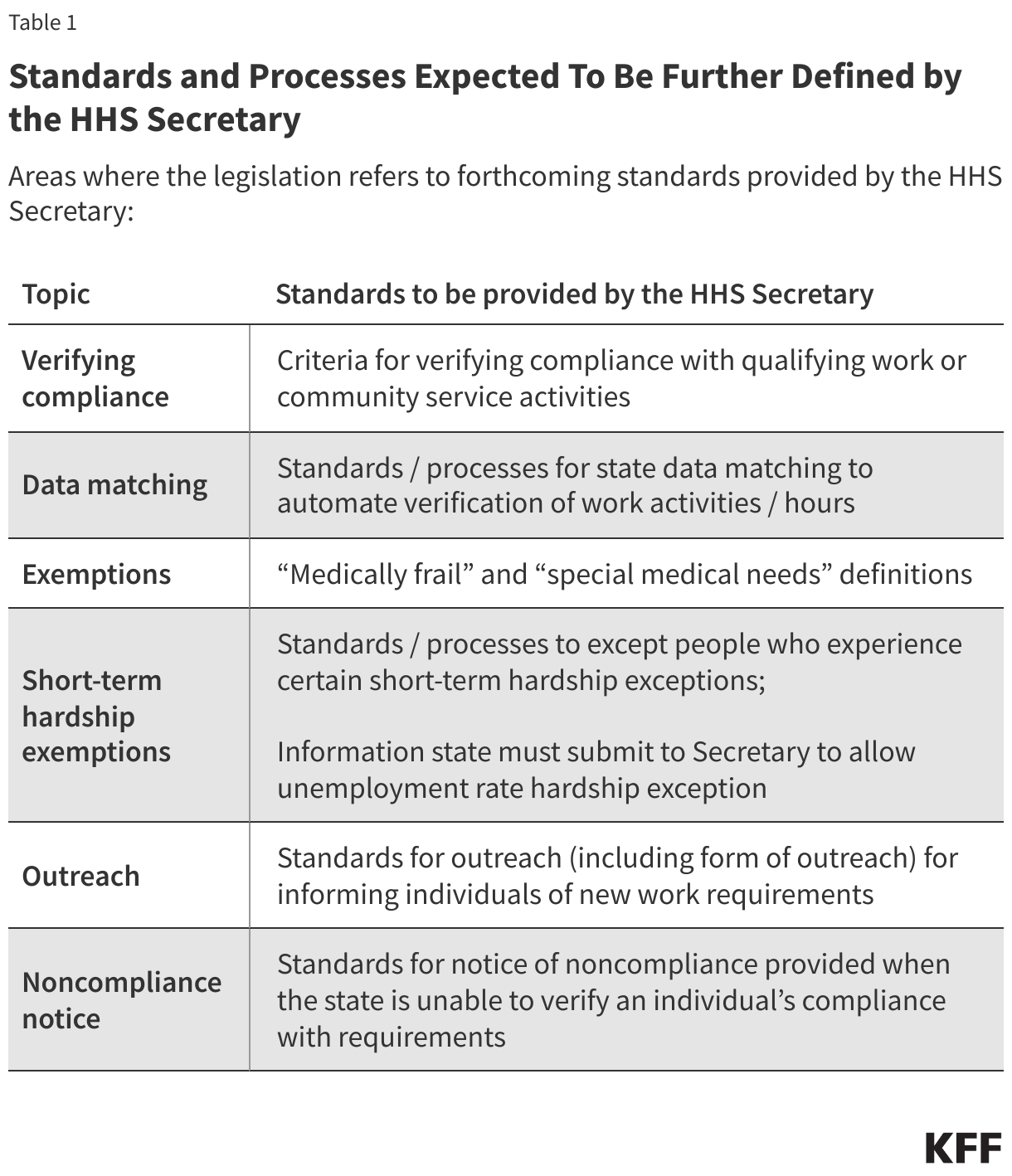
A forthcoming HHS interim rule may identify implementation parameters and additional state requirements; however, if the rule is slated to be released by June 2026, states will have limited time to develop or change implementation plans, protocols, and systems (and to test systems changes). The work requirement provisions outlined in the law raise many operational and implementation questions (Appendix Table 1). The law includes references to areas where additional HHS guidance may further define standards and processes for states (Table 1). Implementing work requirements will involve complex systems changes (e.g., developing or adapting eligibility and enrollment systems), enrollee outreach and education, staff training, and coordination with managed care plans, providers, and other stakeholders. The law allows states flexibility to impose more stringent requirements than the minimum requirements specified (e.g., requiring more frequent verification or imposing longer “look-back” periods when verifying coverage) and allows states to implement requirements sooner than January 2027.
How could implementation vary across states?
States will have flexibility to impose more stringent requirements than the minimum federal requirements outlined in the law. For example, states will have flexibility to determine how many months to “look back” at application (up to three months) and redetermination to verify compliance (and whether to verify compliance more frequently than at redetermination). In effect, states could choose to require compliance with work requirements for multiple months prior to the application month and for every month following enrollment (Box 1).
Box 1
The impact of choosing different “look-back” periods
John lost his job and was out of work in April and May. In June, he started in a new seasonal position and worked 80 hours during the month. In July, John applies for Medicaid in an expansion state, as he qualifies for Medicaid on the basis of his income.
- State A uses a 1-month look-back period when determining compliance with work requirements at application. John would be able to enroll in Medicaid (provided he meets all other program requirements).
- State B uses a 3-month look-back period when determining compliance with work requirements at application. John would not qualify for Medicaid, as he was out of work in two of the three months.
State data matching process decisions and how effective states are with data matching will affect how many individuals will need to submit proof of work hours or exemption status, and ultimately the number of individuals at risk of losing coverage. States with older or weaker systems or less integration (e.g., with SNAP or TANF) may be less effective. But even with effective systems, not all work can be verified through existing data sources, including, for example, community service and self-employment. As noted earlier, the law directs states (“where possible”) to data match work activities and automate the verification of exempted individuals/groups. Some exemptions may be easier to identify with existing data including parent/caretaker status, recent incarceration, and compliance with SNAP/TANF work requirements. Others may be more difficult such as participation in SUD program or meeting the “medically frail” definition (e.g., individuals with SUD, individuals with physical, intellectual, or developmental disabilities, those with “serious or complex” medical conditions).
How does this law compare to state waivers and previous proposals?
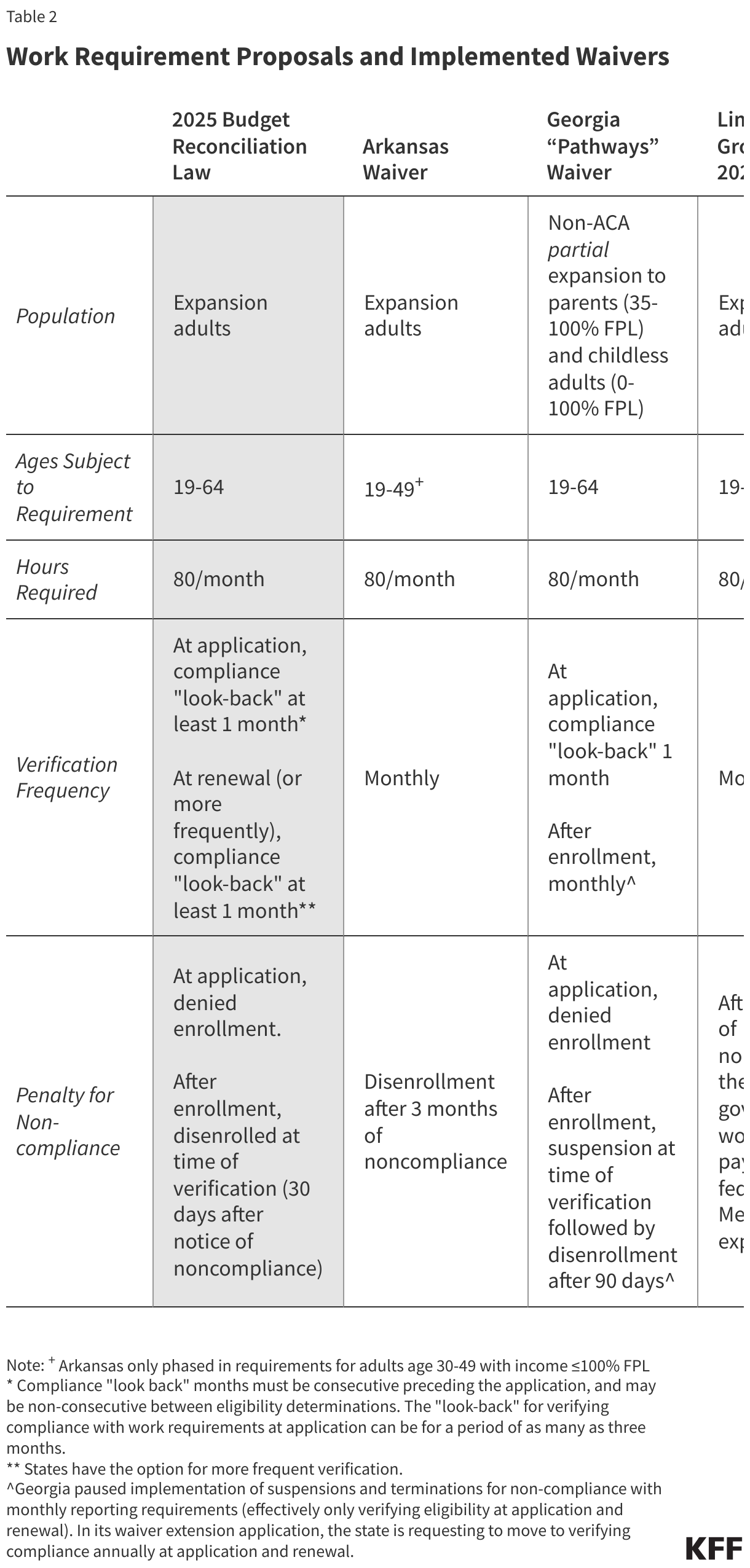
The Medicaid work requirement policies included in the law are more stringent than previous policies considered by Congress and work requirements implemented under state Medicaid demonstration waivers (Table 2). The law shares some similarities in structure to other federal legislative proposals and waivers, including requiring 80 hours per month of qualifying activities such as employment, community service, or work programs, and allowing exemptions for parents and individuals with certain health conditions (although Georgia’s waiver currently offers no exemptions). However, the law will condition eligibility at initial application and after enrollment on meeting work requirements, making it harder to gain coverage and to re-enroll (than in Arkansas or under the Limit, Save, Grow Act considered by Congress in 2023). Individuals lost coverage after three months of noncompliance in Arkansas and under the Limit, Save, Grow proposal, while under the law individuals could lose coverage more quickly (if the state chooses to verify monthly). The policy in the law will also extend to older age, through age 64 (unlike Arkansas’s waiver and the Limit, Save, Grow Act). In Georgia where the work requirement extends through age 64, the state’s interim evaluation found that work requirements have had a significant impact on lowering program enrollment, particularly for adults ages 50-64. For more on lessons learned from Arkansas’ and Georgia’s experience implementing work requirements (under demonstration waivers), see KFF’s previous explainers.
Appendix