- Health centers served 32.4 million patients in 2024, an increase of over a million from 31.3 million patients in 2023. Nine in ten health center patients live in low-income households, over six in ten are patients of color, and three in ten live in rural areas.
- About half of health center patients are covered by Medicaid while 22% have private insurance (including ACA Marketplace coverage) and 18% are uninsured. Despite an increase in the number of privately insured patients, the number of uninsured health center patients increased in 2024, likely due to the unwinding of the Medicaid continuous enrollment provision that led to a decline in the number of Medicaid patients, following several years in which the number of Medicaid patients increased.
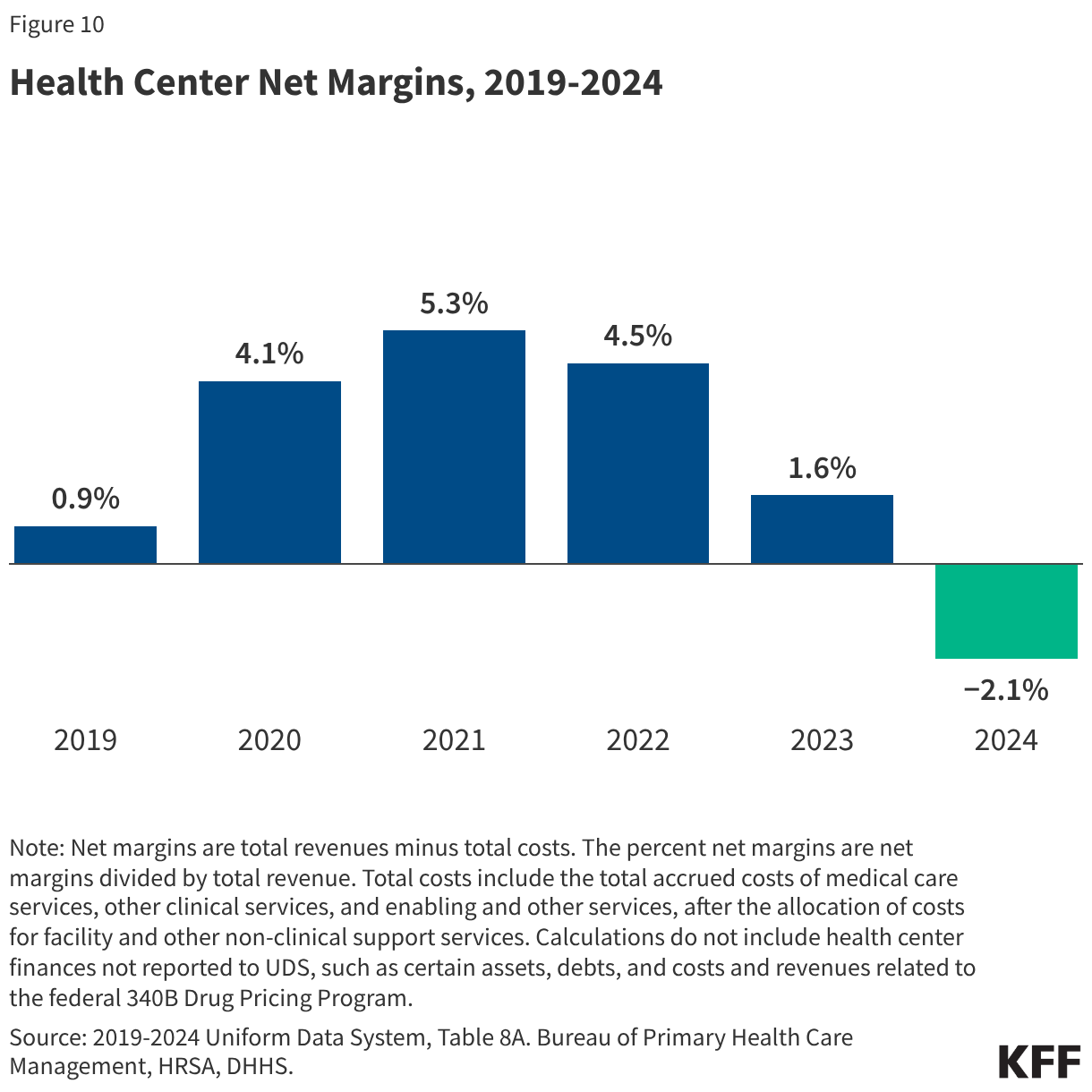
- Medicaid was the largest revenue source for health centers, accounting for 45% of the $49.8 billion in total health center revenue in 2024. Health center revenue increased in 2024 due to growing patient volume and revenue from payers, but net margins that account for revenue and costs fell from 1.6% in 2023 to -2.1% in 2024.
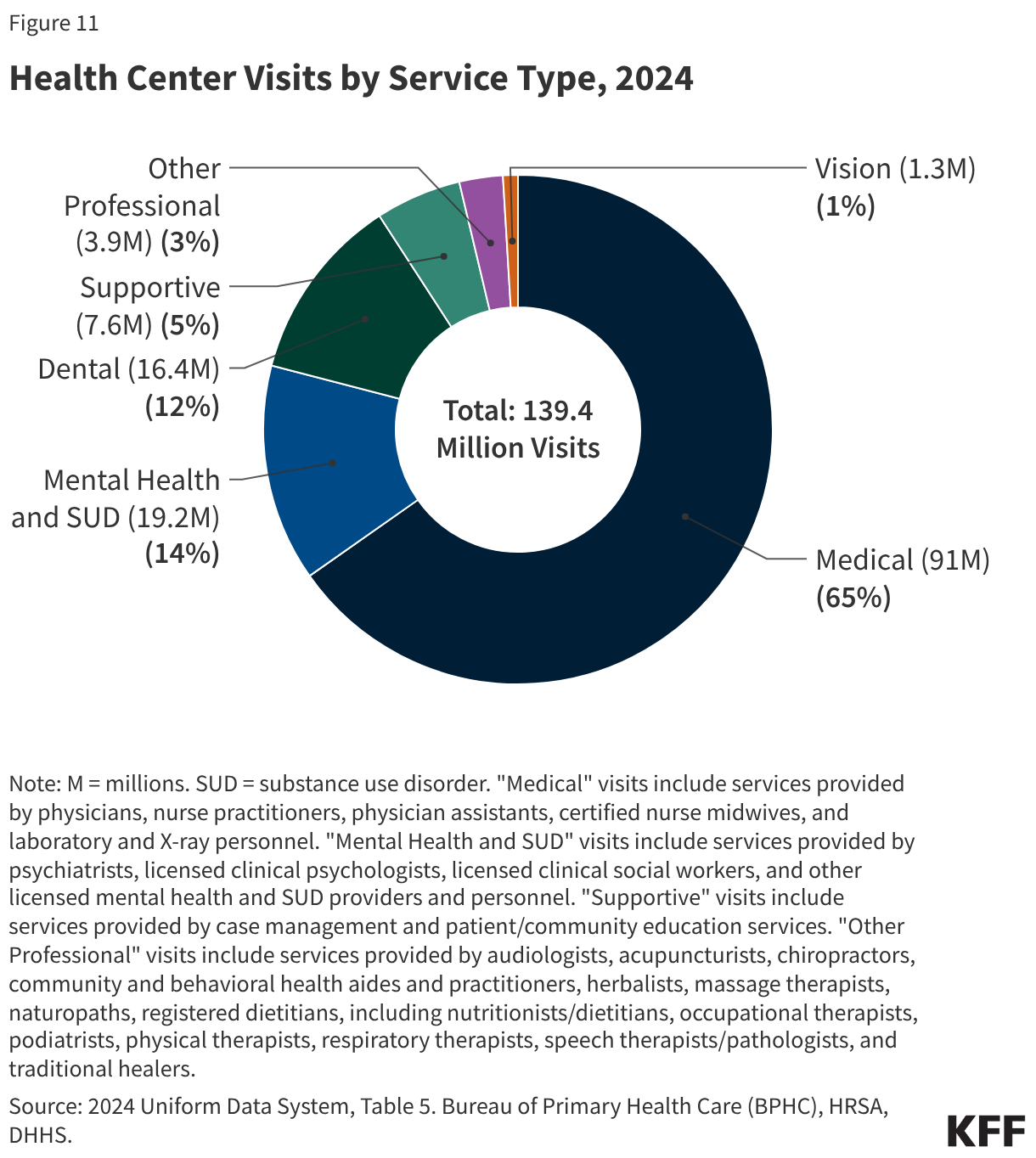
- Of the more than 139 million patient visits in 2024, 65% were for medical services, 14% were for mental health and substance use disorder (SUD) services, and 12% were for dental care. The share of health center visits conducted via telehealth remained steady from 2023, with 17.7 million telehealth visits (13%) in 2024.
- Amid significant federal policy changes and funding uncertainty, health centers face a number of challenges. Changes to Medicaid and the ACA Marketplace included in the 2025 reconciliation law and the expiration of ACA Marketplace enhanced premium tax credits at the end of 2025 are likely to increase the number of uninsured patients and patients who cannot afford out-of-pocket costs, placing new financial burdens on health centers. In addition, increased immigration enforcement in health care settings along with proposed changes to federal immigration policies may sow confusion and fear of using health center services among immigrant patients. At the same time, health centers face ongoing financial uncertainty amid federal funding stand-offs in Congress. The 2026 Consolidated Appropriations Act increases slightly health center funding to $4.6 billion for fiscal year 2026, but only extends funding through December 2026, including for the Community Health Center Fund, which was designed to provide more stable, longer-term funding.
Community Health Center Patients, Financing, and Services
Community health centers are a national network of nearly 1,400 safety-net primary care providers that served more than 32 million patients in 2024. They are located in medically underserved urban and rural communities and provide comprehensive primary care services to patients regardless of their ability to pay, providing a range of medical, behavioral, and supportive services. This brief reports on health center patients, services, and financing in 2024 and analyzes changes over time using national data from the Uniform Data System (UDS), to which all health centers are required to report annually, though variation exists across states. An upcoming brief will focus on health center patients, services, and financing specifically among rural health centers.
Editorial Note: This brief was updated on February 11, 2026 to clarify what the data on reported usual source of care for immigrant adults represent.
Introduction
Key Takeaways
Health Center Patients
Health Center Organizations
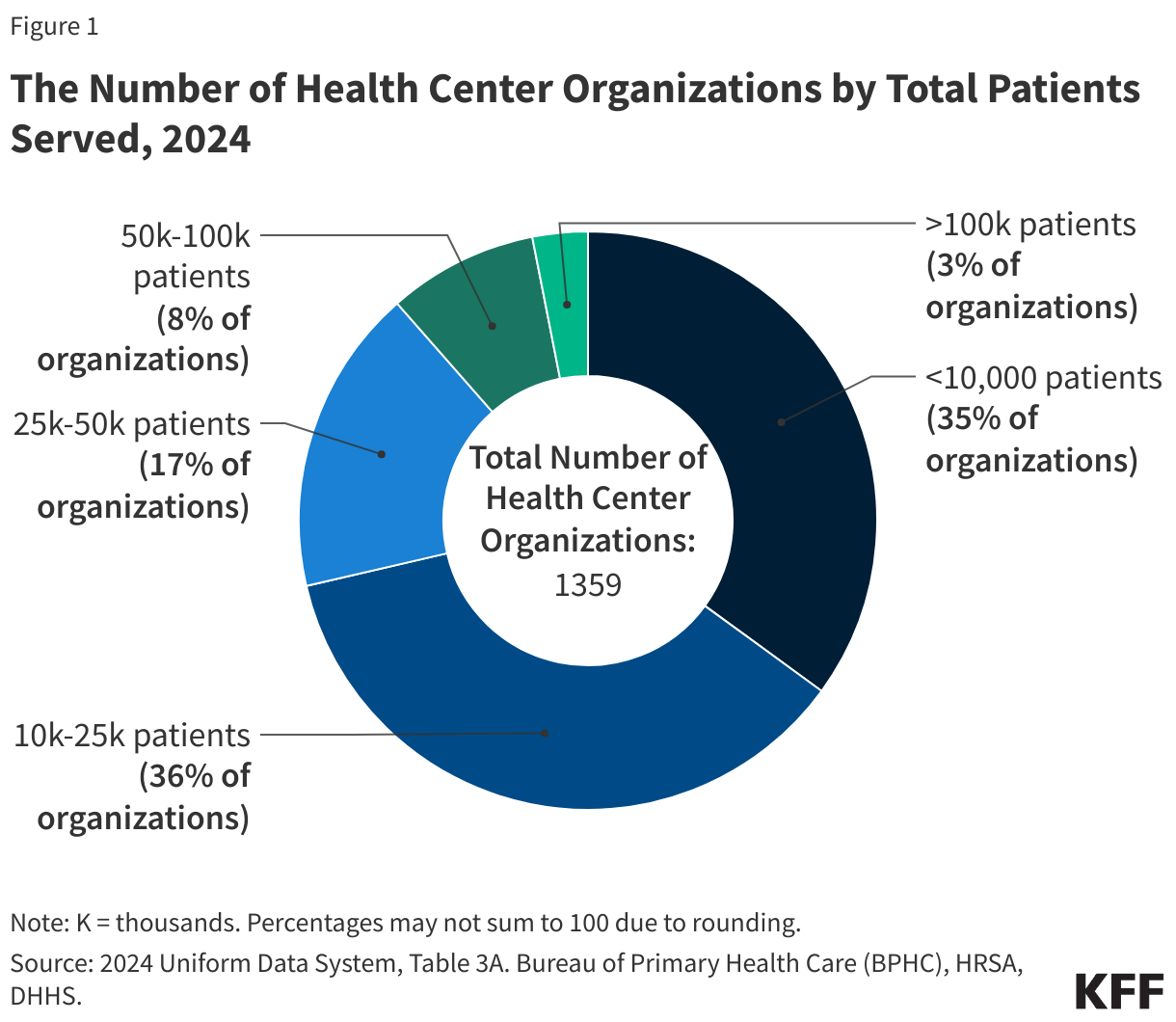
In 2024, 1,359 health center organizations provided care at over 16,300 service delivery sites (Figure 1). Roughly six in ten health centers served patients in medically underserved urban areas, while four in ten served rural communities. Seven in ten (71%) health centers provided care to 25,000 or fewer patients while 3% of health centers served 100,000 or more patients in 2024. Generally, smaller health centers are located in rural areas or focus services on certain neighborhoods or populations, while larger health centers tend to serve more urban areas and operate multiple clinic locations. In addition to traditional locations, health center sites include those located at schools, homeless shelters, and mobile sites, and some sites may operate seasonally.
Patient Demographics
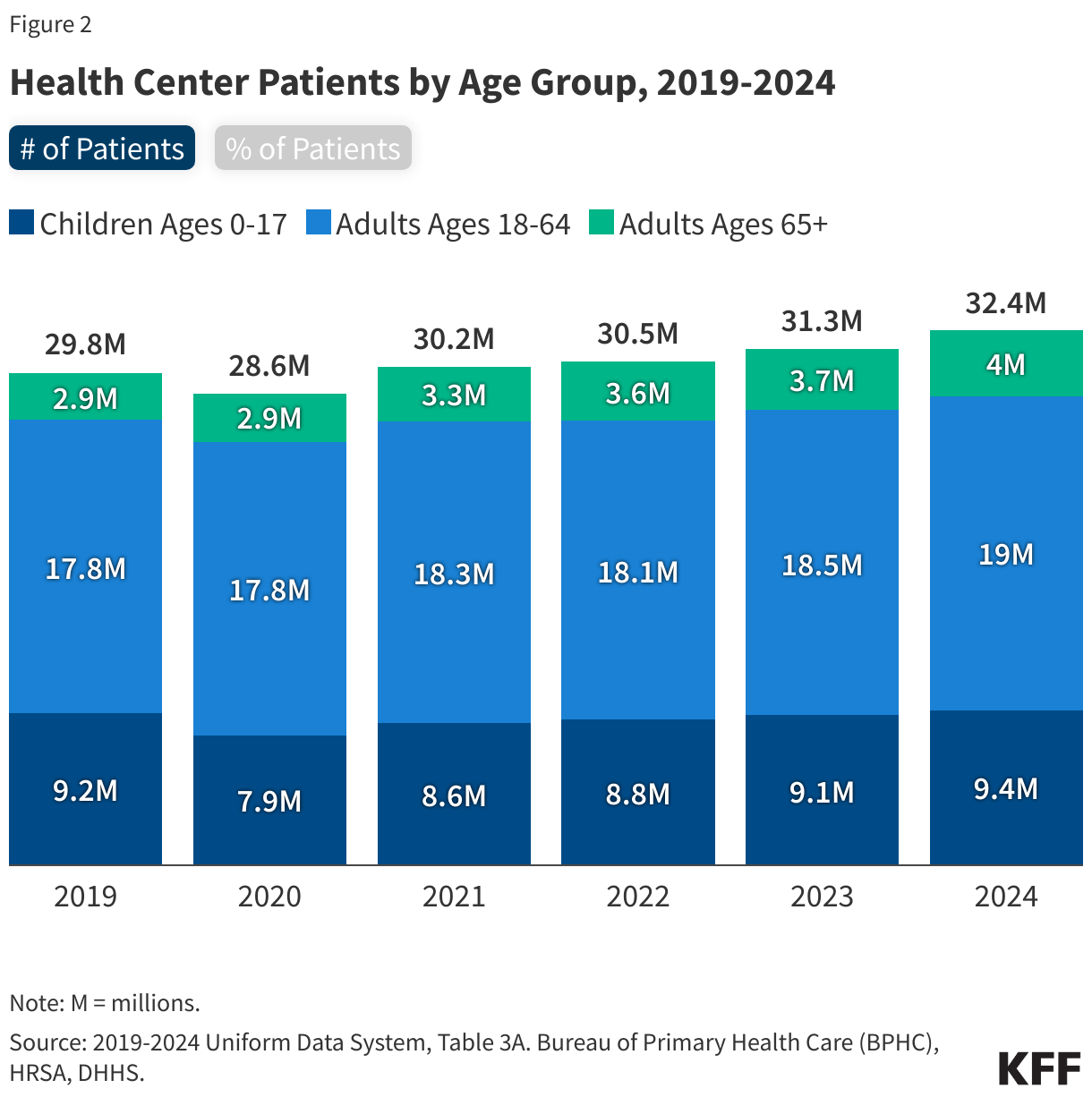
The number of patients served by health centers increased by over a million from 31.3 million in 2023 to 32.4 million in 2024, with increases across all age groups (Figure 2). Health centers served 9.4 million children in 2024, representing 29% of health center patients. Adults ages 18-64 comprised 59% of health center patients while adults ages 65+ made up 12%. The number of children served by health centers dropped during the pandemic and has been slow to rebound. Although still a small share of the total patient population, the number of adult patients ages 65+ served at health centers grew by 38%, or over one million, from 2019-2024, compared to 2% among children and 7% among adults ages 18-64 in the same period.
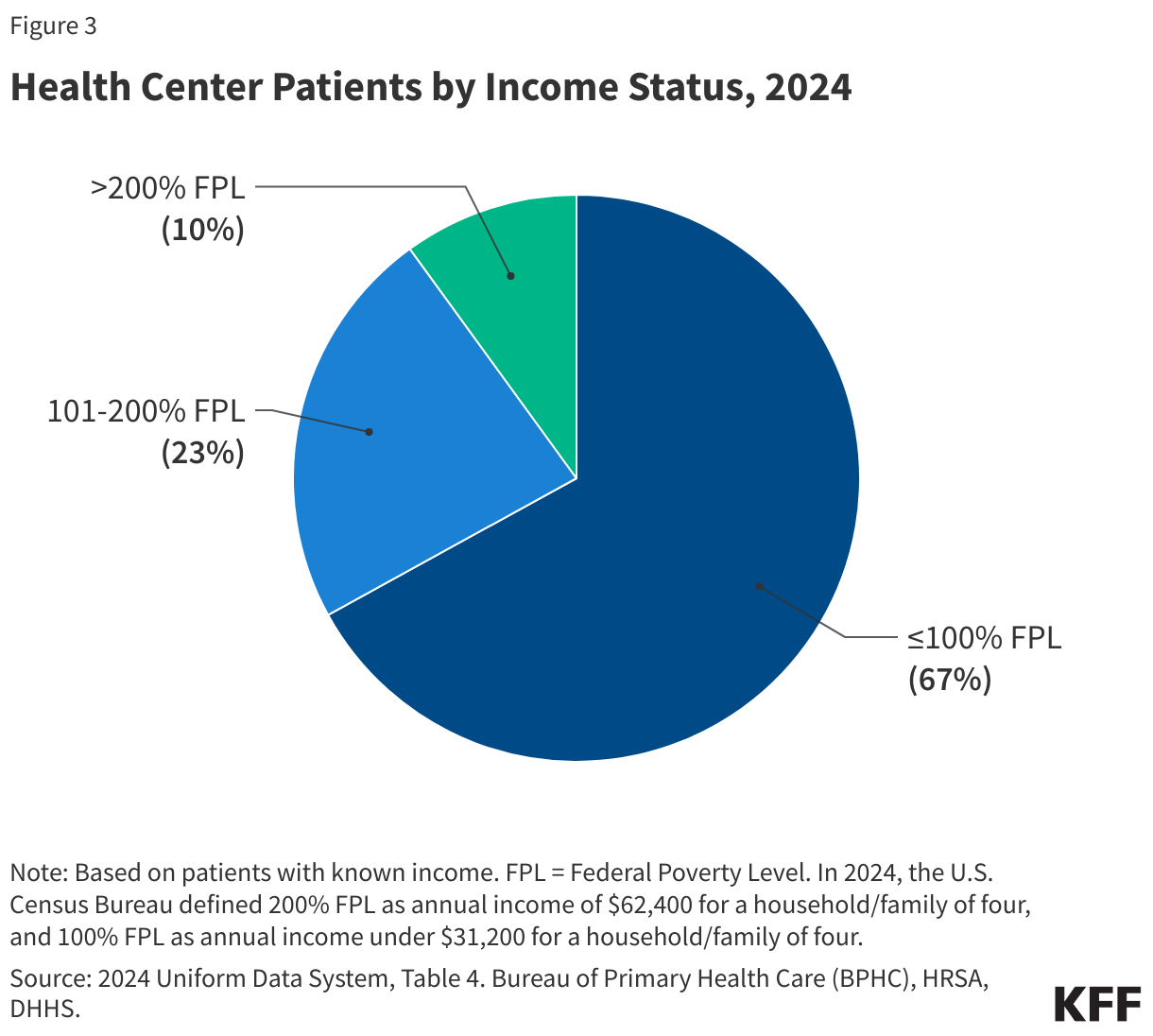
A majority of health center patients live in low-income households (Figure 3). Reflecting the mission of health centers to serve anyone regardless of ability to pay, nine in ten (90%) patients served at health centers had incomes that were at or below 200% of the federal poverty level (FPL) and two-thirds of patients (67%) had incomes at or below the poverty level in 2024 (the poverty level was $31,200 for a family of four in 2024). The share of low-income patients served at health centers is over three times that of the U.S. population, in which 27% of individuals lived in households earned under 200% FPL in 2024.
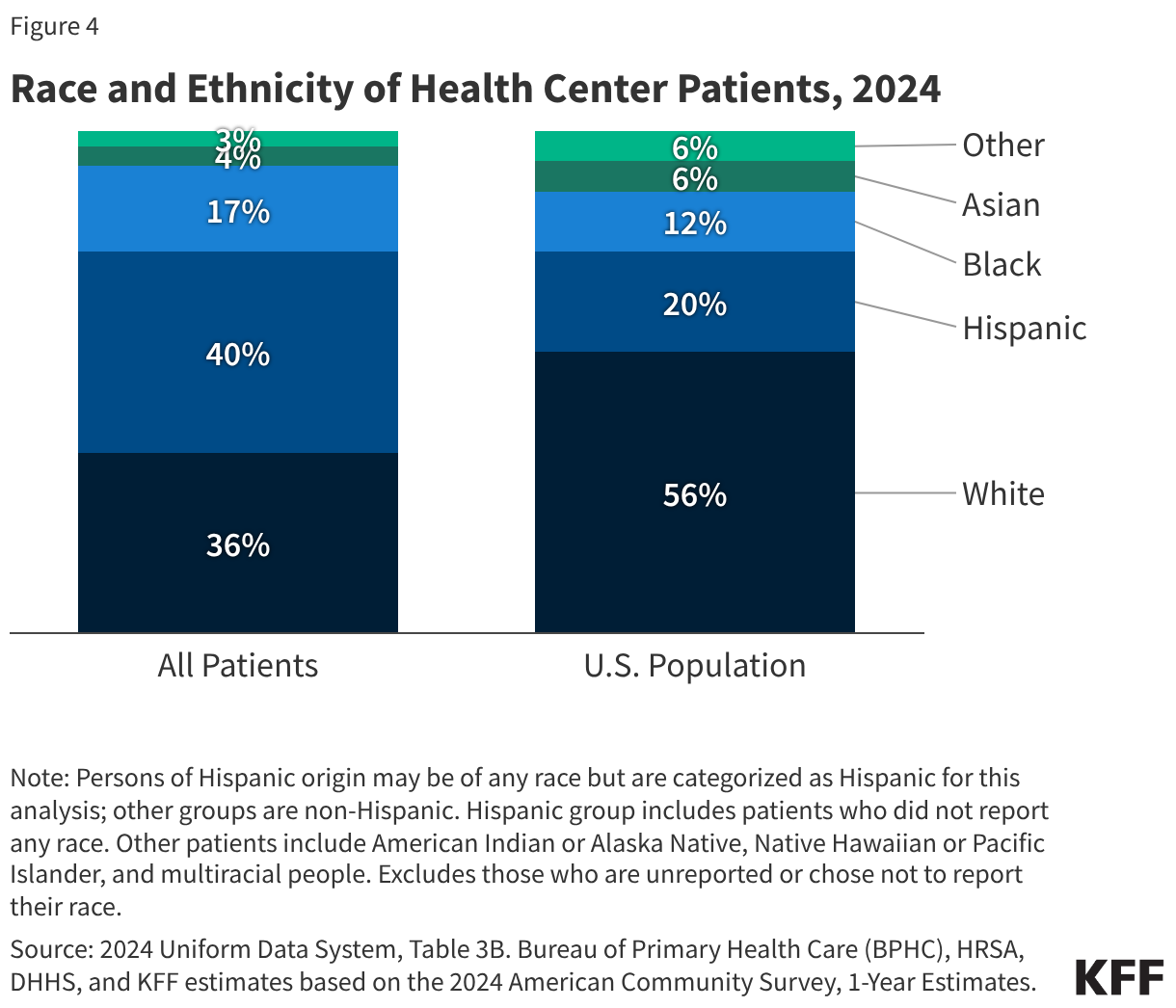
Most health center patients (64%) are people of color, greater than their share of the total U.S. population in 2024 (Figure 4). Across all health centers, Hispanic patients comprised the largest share of patients at 40%, followed by White patients (36%), Black patients (17%), Asian patients (4%), and all other patients (3%).
Special Patient Populations
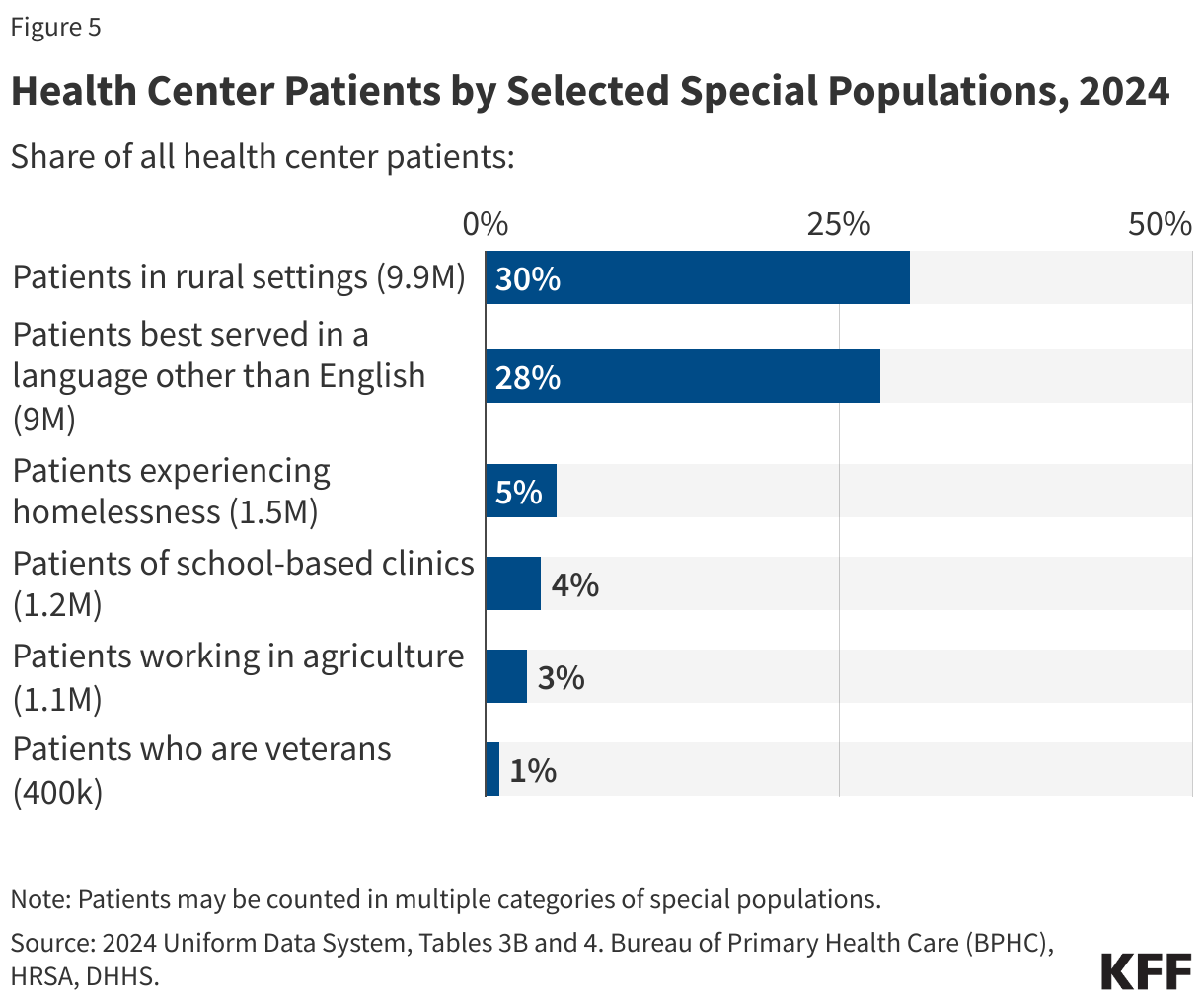
Health centers served millions of patients who were part of special populations with distinct health needs in 2024 (Figure 5). The Health Resources and Services Administration (HRSA), which administers the health center program, provides targeted funding for health centers that serve certain populations identified as underserved by the federal government, including people experiencing homelessness and migratory agricultural workers. In 2024, health centers served 1.5 million patients experiencing homelessness (5% of all patients), 1.2 million patients in school-based health centers (4% of all patients), 1.1 million agricultural workers (3% of all patients), and 400k patients who were veterans (1% of all patients). In addition, health centers are also required to report data on other populations with known challenges accessing primary care. For example, three in ten patients (30% or 9.9 million) were rural residents, which is higher than the 20% of the U.S. population living in rural areas, and nearly three in ten patients (28% or 9 million) are best served in a language other than English.
Health Coverage of Health Center Patients
Overall Health Coverage
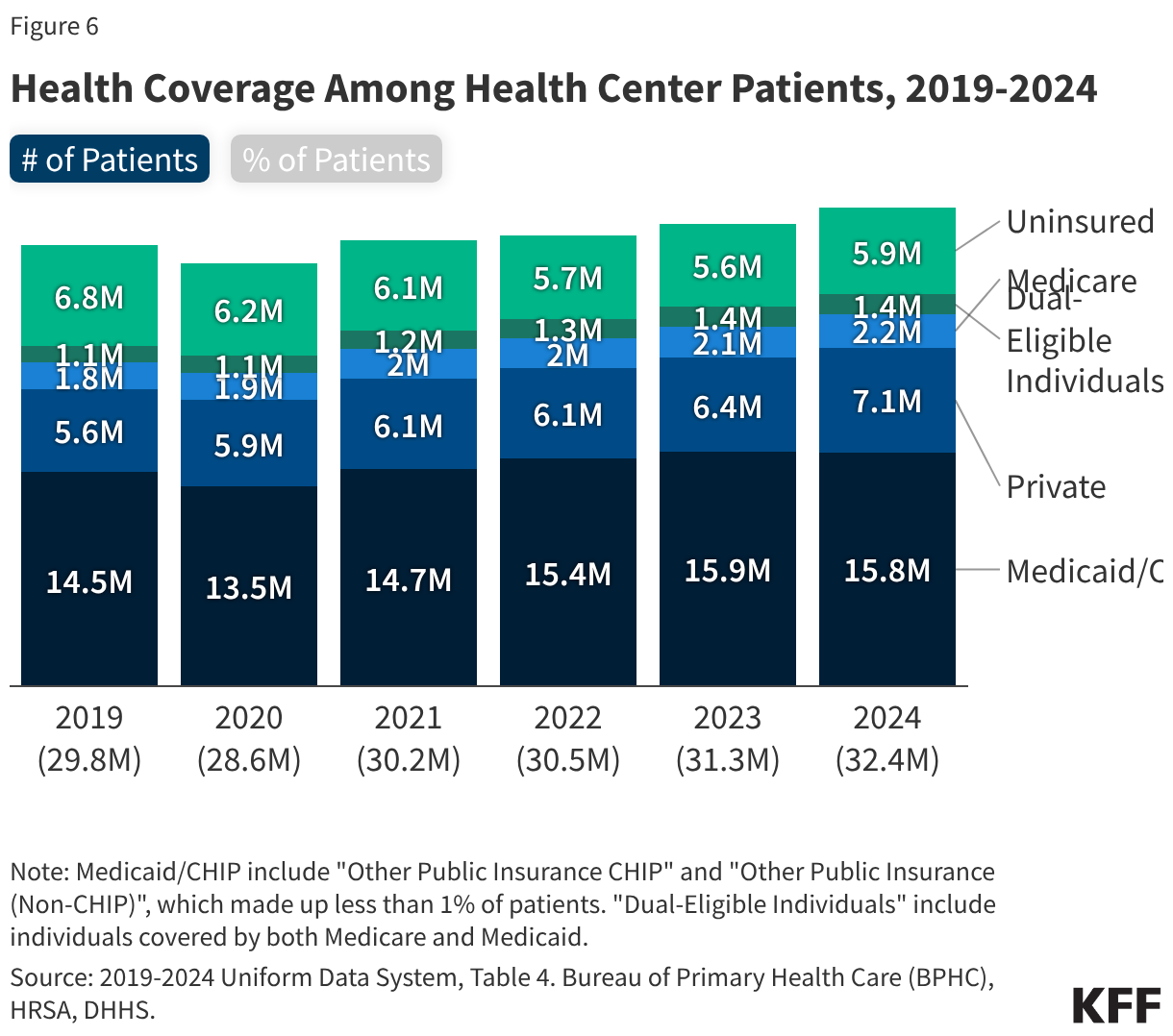
Over eight in ten (82%) health center patients had health insurance coverage in 2024 (Figure 6). Nearly half (49%) of health center patients were covered by Medicaid while 22% of patients had private insurance (including ACA Marketplace coverage), 7% were covered by Medicare, and 4% were dual-eligible patients who had both Medicare and Medicaid coverage. Medicare is likely the primary payer for health center services among dual-eligible patients, but Medicaid may cover the costs for dental services and some mental health or substance use disorder services. Nearly one in five (18%) health center patients were uninsured. The share of health center patients who were uninsured varied widely by state, ranging from 9% in several states to as high as 43% in Utah. This variation likely reflects a mix of factors such as the types of health centers in the state, characteristics of the health center patient populations, and state Medicaid expansion status.
Change in Uninsured Patients
After several years of decline, the number of health center patients who were uninsured increased in 2024. From 2023 to 2024, the number of uninsured health center patients increased by over 250,000 from 5.6 million to nearly 5.9 million (Figure 6). At the same time, the number of privately insured patients increased by over 11% (716,000) while the number of Medicaid patients dropped by 43,000 or less than 1% from 2023. The drop in Medicaid patients in 2024 after several years of increases is likely attributable to the end of the Medicaid continuous enrollment provision, which temporarily halted Medicaid disenrollments from March 2020 through March 2023. Starting in April 2023, states resumed disenrollments as part of the unwinding of continuous enrollment in Medicaid, and national Medicaid/CHIP enrollment has since declined. Enhanced premium tax credits for Marketplace coverage, adopted in 2021 and extended through December 2025, drove a record increase in Marketplace enrollment that likely led to the increase in health center patients with private insurance.
Medicaid Coverage of Health Center Patients by State
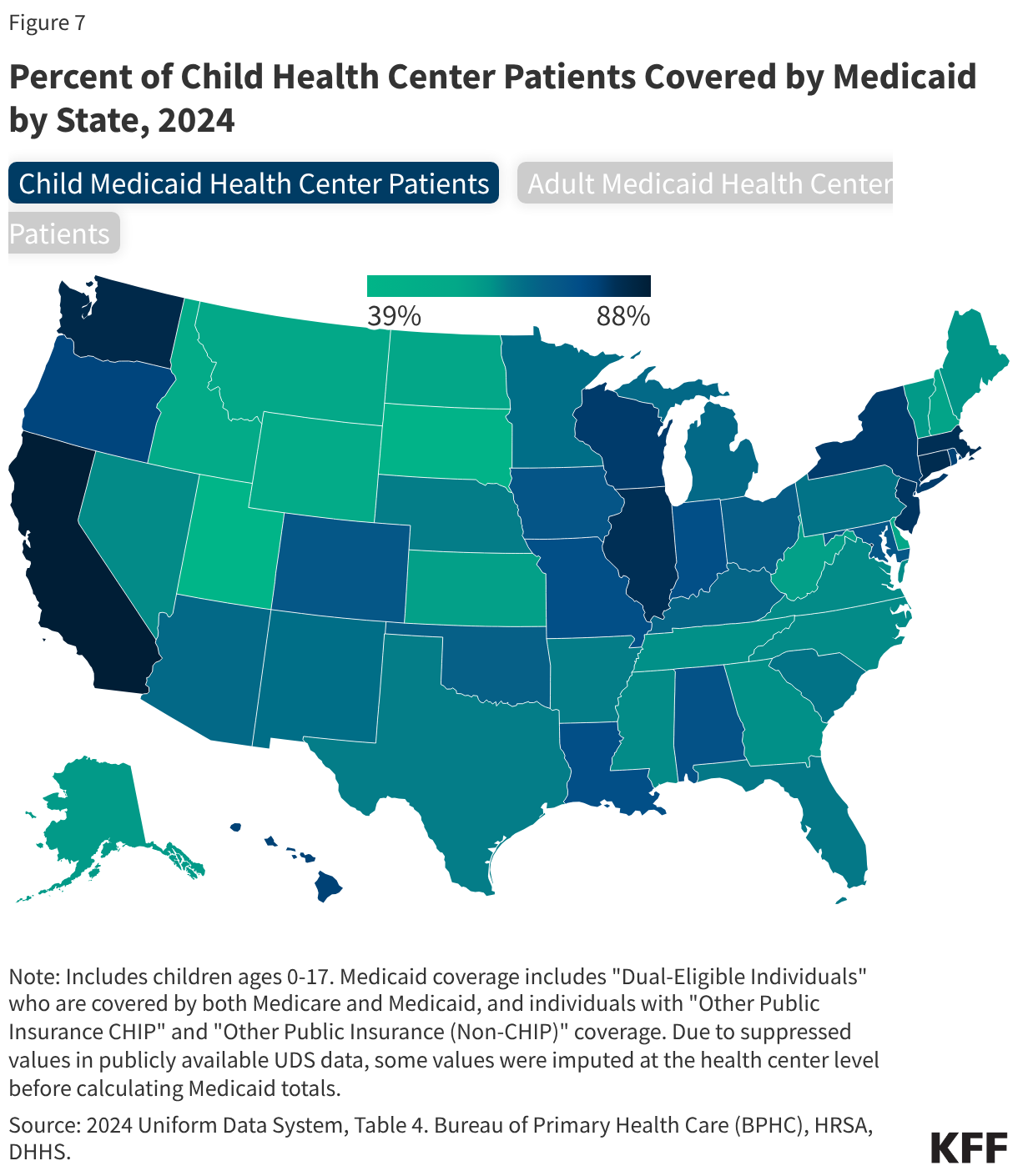
While Medicaid is an important source of coverage for health center patients, the share of child and adult health center patients covered by Medicaid varied widely by state (Figure 7). Nationwide, about 6.9 million (74%) child health center patients ages 0-17 and 10.3 million (45%) adult health center patients ages 18 and older were covered by Medicaid and CHIP, including dual-eligible health center patients who had both Medicare and Medicaid coverage. The share of child health center patients covered by Medicaid ranged from less than 50% in two states to 80% or more in nine states and DC, while the share of adult health center patients covered by Medicaid was less than 20% in six states and more than half in eight states and DC.
Health Center Financing and Costs
Health Center Revenue
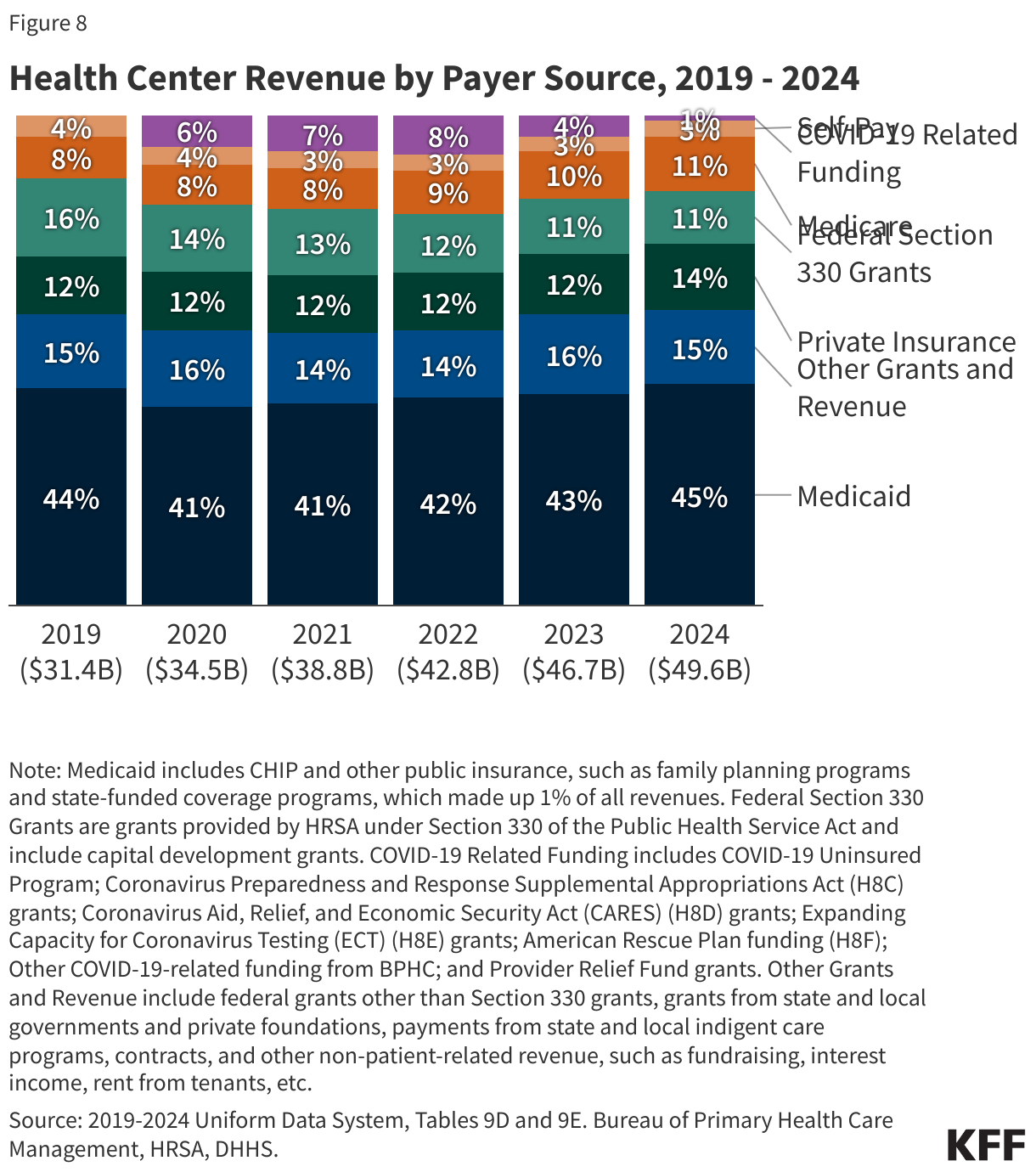
Despite the expiration of most COVID-19 funding and other supplemental funding provided during the pandemic, health center revenues continued to increase in 2024 due to growing patient volume and revenue from payers. In 2024, total health center revenue was $49.6 billion, an increase of 6% from $46.7 billion in 2023 (Figure 8). Nearly three quarters (73%) of health center revenue came from payments from Medicaid, private insurance, Medicare and self-pay patients, with Medicaid accounting for over 60% of patient care revenue and 45% of total revenue. Federal Section 330 grant funding, which supports health centers’ role as safety net providers, made up 11% and other grants and contracts were 15% of total revenue. COVID-19 funding largely expired after 2023 and accounted for just 1% of total revenue in 2024. From 2019 to 2024, patient care revenue increased as a share of total revenue from 68% to 73%. At the same time, Federal Section 330 grants decreased as a share of total revenue from 16% in 2019 to 11% in 2024.
Per Patient Revenue
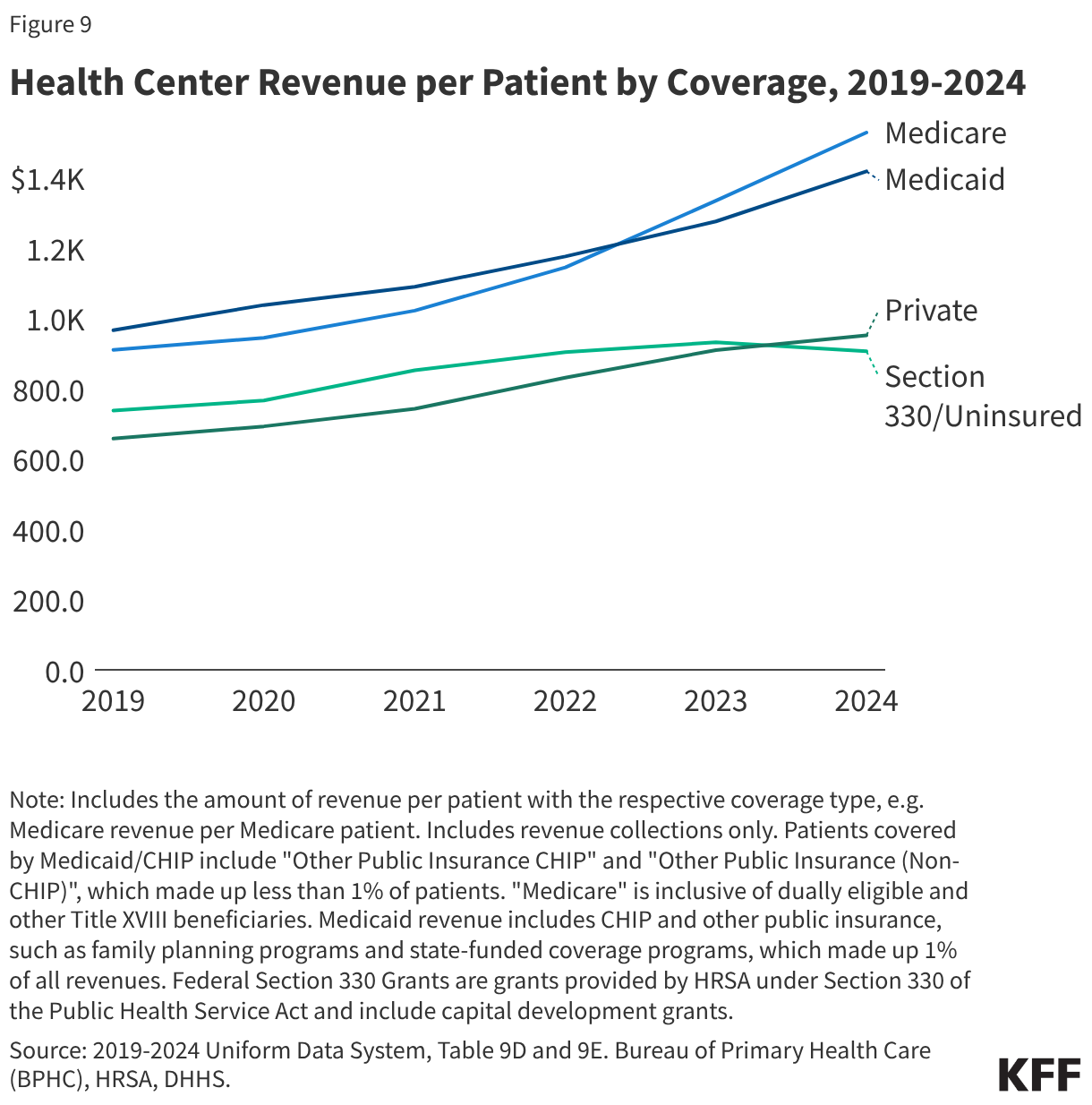
Federal Section 330 funding per uninsured patient is lower than per patient revenue from other payers (Figure 9). Federal section 330 grants support ongoing care to the uninsured, although section 330 grants are not tied directly to the number of uninsured patients health centers serve and may vary widely between health centers. In 2024, federal section 330 funding per uninsured patient ($906) was lower than per patient revenue from Medicare ($1,528), Medicaid ($1,418), and private insurance ($951). Section 330 funding per uninsured patient increased 26% from 2019 to 2023 but dropped 3% from 2023 to 2024 as the number of uninsured patients increased. From 2019 to 2024, growth in Section 330 funding per uninsured patient was lower than the growth in per patient revenue from Medicare (68%), Medicaid (47%), and private insurance (45%) during the same time period.
Health Center Costs
Rising operating costs outstripped increases in revenues in 2024, causing the national health center net margins to fall to -2.1% (Figure 10). Net margins account for both costs and revenue and are reported as a percentage of revenue. The strong positive net margins from 2020 through 2022 were driven primarily by the increase in COVID-related and other supplemental funding during the pandemic. The negative net margin in 2024 reflects higher costs, which increased 62% from 2019-2024 due to inflation, as well as reduced revenue from the expiration of COVID-19 funding. Net margins will vary by health center depending on factors such as their share of uninsured patients, operating costs, the amount of competitive federal grant funding they are awarded, and other sources of revenue.
Health Center Services and Workforce
Health Center Visits
Health centers provided more than 139 million visits in 2024 (Figure 11). Most visits (65%) were for medical services, though health centers also provided a wide range of other clinical and supportive services, including mental health and substance use disorder (SUD) services (14%), dental services (12%), vision services (1%), and other professional services (3%), which include services such as nutrition counseling, physical therapy, and traditional healing. Enabling or supportive services, which are non-clinical services like case management, transportation, and health education that facilitate access to care, represented 5% of all visits. Health centers are required by federal law to provide primary care and supportive services, and they may offer dental, vision, or other services depending on patient need and organizational capacity.
Telehealth
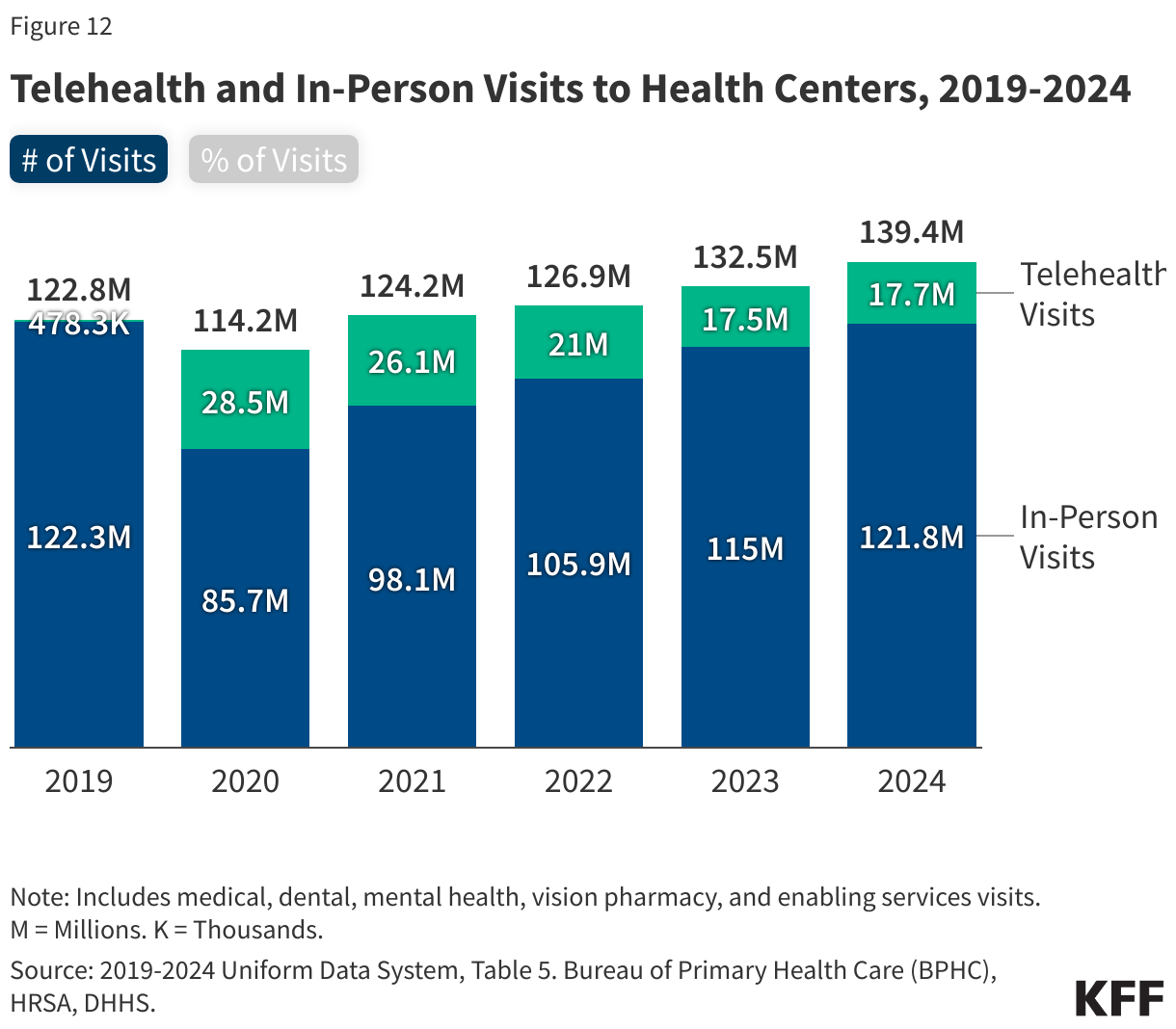
The share of health center visits conducted via telehealth remained steady from 2023 after several years of decline. In 2024, health centers provided 17.7 million telehealth visits, which represented 13% of all visits (Figure 12). The number of telehealth visits peaked in 2020 at the start of the coronavirus pandemic when 28.5 million visits (25%) were conducted via telehealth but declined from 2021 through 2023 before increasing slightly in 2024. Telehealth represents an important way for patients to access health center services, particularly since some patients face geographic and transportation barriers that can make it more difficult for them to attend in-person visits.
Health Center Workforce
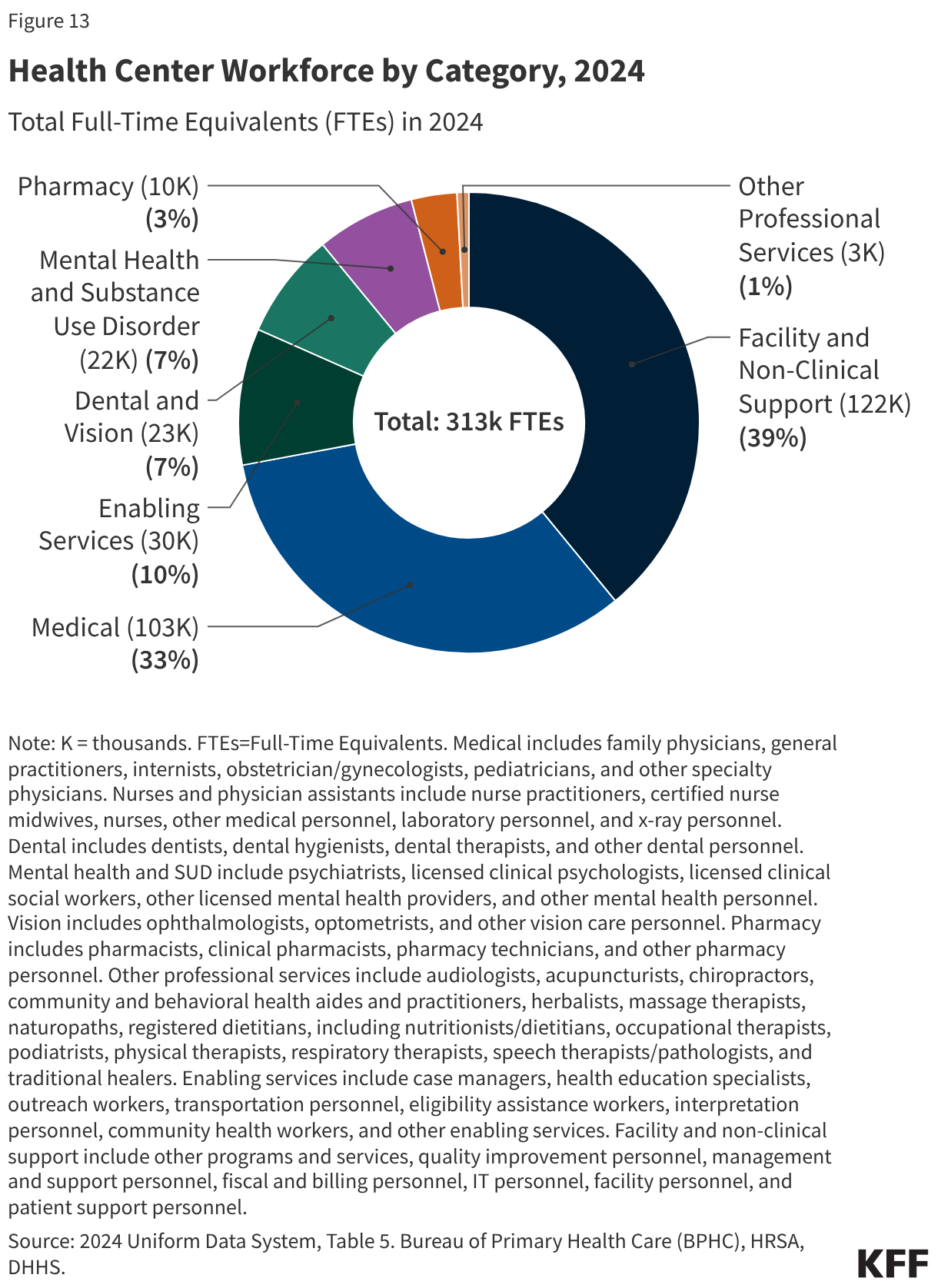
Health centers employed over 313,000 full-time equivalents (FTE) in 2024 (Figure 13). Most (61%) health center staff provide patient care or enabling services, including medical (33%), enabling (10%), dental and vision (7%), mental health and substance use disorder (7%), pharmacy (3%), and other professional services (1%). The remaining 39% of health center staff work in facility and non-clinical support. Health centers are important employers in their communities; however, they consistently report workforce shortages as one of their main challenges. Research indicates those shortages have worsened over time. Ongoing funding challenges and delays may further exacerbate these challenges.
Impact of Federal Policy Changes
Medicaid and Marketplace Changes in the 2025 Reconciliation Law
Changes to Medicaid and the ACA Marketplace included in the 2025 reconciliation law are estimated to increase the number of people without health insurance in 2034 by 10 million, which may have an outsized impact on the health center patient population. These coverage losses will be driven primarily by new Medicaid policies like mandatory work requirements for the ACA adult expansion population and the requirement for states to conduct eligibility redeterminations every six months rather than annually, and Marketplace changes, including the elimination of auto renewal and the special enrollment period for people with income less than 150% FPL. These changes are likely to lead to some health center patients losing coverage, even as many health centers provide assistance to patients to help them navigate the new Medicaid and Marketplace rules. Furthermore, changes to Medicaid financing, such as limits on states' ability to use provider taxes and caps on federal funding for state directed payments to managed care organizations, reduce the federal share of funding, and limit state flexibility in setting provider rates and expanding coverage given ongoing state budget challenges.
Health centers are a primary source of care for immigrant adults, but the 2025 reconciliation law includes eligibility restrictions and make many lawfully present immigrants ineligible for Medicaid and CHIP, ACA Marketplace subsidies, and Medicare. While health centers do not publicly report patient immigration status, data from the 2025 KFF/New York Times Survey of Immigrants show that three in ten (30%) immigrant adults say a health center is their usual source of care, with this share rising to nearly half (45%) of likely undocumented immigrant adults and nearly four in ten (37%) among immigrant adults with limited English proficiency. These data reflect shares of immigrant adults who report they use a health center when they are sick or need health advice but do not reflect use of care over any specified time period and cannot be used to estimate the share of health center patients who are immigrants in a given year. The law limits eligibility for Medicaid and CHIP, subsidized Marketplace coverage, and Medicare, eliminating coverage for many groups of lawfully present immigrants, including refugees, asylees, and people with Temporary Protected Status, among others. Some states have also reduced or eliminated state-funded coverage designed to fill gaps in federally funded coverage for immigrants due to funding challenges, further reducing coverage options for immigrant health center patients. Reliance on health centers may increase among immigrants who become uninsured as their affordable health care provider options become more limited.
The 2025 reconciliation law also stripped federal Medicaid funding for one year to Planned Parenthood clinics, which may increase demand for family planning services at health centers. This follows actions by the Trump Administration and a Supreme Court ruling that restricted funding to some providers of reproductive and sexual health care services. The share of female Medicaid enrollees who received their last contraceptive visit at a health center across the U.S. was 18% in 2023, with wide variation across states. Health centers may face difficulties in ramping up the availability of family planning services to meet the higher demand if other clinics close.
Expiration of the Enhanced Marketplace Tax Credits
The expiration of ACA Marketplace enhanced premium tax credits at the end of 2025 has increased premium payments for many enrollees and will likely increase the number of uninsured health center patients. Because the enhanced subsidies were allowed to expire at the end of 2025, premium payments for enrollees receiving subsidies increased by 114% on average. While some Marketplace enrollees likely shifted to lower cost plans in response to the reduction in financial assistance, some have been forced to drop coverage. High marketplace enrollment helped keep the uninsured rate low in 2024, but expiration of the enhanced tax credits may reverse recent increases in the number of health center patients with private coverage. Additionally, the shift to lower-cost bronze plans by health center patients could lead to more uncompensated care costs for health centers if patients are unable to afford the higher out-of-pocket costs.
Trump Administration Immigration Policies and Enforcement Actions
New federal policies could require health centers to verify patient immigration status. The U.S. Department of Health and Human Services (HHS) issued a notice of a policy change to update the definition of “federal public benefits” as outlined in the Personal Responsibility and Work Opportunity Reconciliation Act of 1996 (PRWORA) to add the Health Center Program, among others, to a list of programs considered “federal public benefits” that are restricted to individuals with a “qualified” immigration status. The policy change bars many lawfully present and undocumented immigrants from accessing care at health centers. However, while the notice limits the health center program to “qualified immigrants,” it does not change the underlying statutory requirements for health centers to serve patients regardless of immigration status, and it remains to be seen how enforcement of the guidance will affect health centers’ ability to provide care. The policy faces legal challenges and in September 2025, a court blocked implementation of the policy as it relates to the Health Center Program in 20 states and DC.
Changes in public benefit policies along with increased federal immigration enforcement actions may have a chilling effect on enrollment in health coverage and access to care among a broad group of immigrant families utilizing health center services, including citizen children in those families. Data from the KFF/New York Times 2025 Survey of Immigrants show that about one in ten immigrant adults say they stopped participating or avoided applying for an assistance program that helps pay for food, housing, or health care because they didn’t want to draw attention to their or a family member’s immigration status. Increased immigration enforcement in health care settings, federal data sharing used for immigration enforcement, proposed changes to federal public charge policy and policies requiring health centers to check immigration status can have negative impacts on the health and well-being of immigrant families due to more limited access to services as well as confusion and fear about using health center services.
Financial Challenges
Health coverage changes in the 2025 reconciliation law and expiration of the ACA enhanced premium tax credits will likely increase financial pressures for health centers. Research has estimated that health centers could experience over $3 billion in revenue reductions from a drop in the number of patients covered by Medicaid and an increase in the number of uninsured patients resulting from the 2025 reconciliation law’s health provisions. While many provisions in the new law, including some of the largest sources of federal Medicaid savings such as work requirements and financing changes, do not take effect until 2027 or later, other policy changes, such as changes to immigrant eligibility for Medicaid and Marketplace coverage and expiration of ACA enhanced premium tax credits, can impact health center finances earlier. An increase in uncompensated care costs would exacerbate financial challenges at health centers, which experienced negative net margins nationwide in 2024 amid rising operating costs.
Federal funding delays contribute to financial uncertainty for health centers. While Congress previously insulated health centers from funding lapses by authorizing the Community Health Center Fund for five years, the most recent two-year authorization was temporarily extended from September 30, 2025 to January 30, 2026 as part of the continuing resolution that reopened the federal government after a 43-day shutdown. On February 3, 2026, Congress passed the 2026 Consolidated Appropriations Act, which slightly increases health center funding to $4.6 billion for fiscal year 2026, but only extends funding through December 2026. The funding delays create significant challenges for health centers, which rely on federal funding to maintain operations and provide care to uninsured patients. Funding gaps earlier in 2025 caused health center closures, and the funding lapse due to the government shutdown led several states to allocate additional funds for health centers.